Non-AIDS Kaposi's sarcoma in the head and neck area
Non-AIDS Kaposi's sarcoma in the head and neck area
Non-AIDS Kaposi's sarcoma in the head and neck area

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
CLINICAL REVIEW<br />
David W. Eisele, MD, Section Editor<br />
NON-<strong>AIDS</strong> KAPOSI’S SARCOMA IN THE<br />
HEAD AND NECK AREA<br />
Anna Patrikidou, MD, 1 Kostas Vahtsevanos, PhD, 1 Martha Charalambidou, PhD, 2<br />
Rosalia-Maria Valeri, PhD, 3 Persefoni Xirou, MD, 4 Kostas Antoniades, PhD 5<br />
1 Department of Maxillofacial Surgical Oncology, Theagenio Cancer Hospital, Thessaloniki,<br />
Greece. E-mail: a.patrikidou@uclmail.net<br />
2 Department of Radiation Oncology, Theagenio Cancer Hospital, Thessaloniki, Greece<br />
3 Department of Cytopathology, Theagenio Cancer Hospital, Thessaloniki, Greece<br />
4 Department of Histopathology, Theagenio Cancer Hospital, Thessaloniki, Greece<br />
5 Department of Oral <strong>and</strong> Maxillofacial Surgery, General Hospital ‘‘G. Papanikolaou,’’<br />
Thessaloniki, Greece<br />
Accepted 9 June 2008<br />
Published onl<strong>in</strong>e 28 October 2008 <strong>in</strong> Wiley InterScience (www.<strong>in</strong>terscience.wiley.com). DOI: 10.1002/hed.20945<br />
Abstract: Kaposi’s <strong>sarcoma</strong> is classified <strong>in</strong>to 4 types: classic<br />
(sporadic), African (endemic), iatrogenic (transplant recipients),<br />
<strong>and</strong> epidemic (acquired immunodeficiency syndrome [<strong>AIDS</strong>]-<br />
associated). This article aims to feature a comprehensive review<br />
of non-<strong>AIDS</strong> Kaposi’s <strong>sarcoma</strong>, <strong>in</strong>clud<strong>in</strong>g literature review <strong>and</strong><br />
report of 3 cases. Case material was from our hospital’s archive.<br />
Literature review was conducted via electronic <strong>and</strong> manual medical<br />
database searches. Biological aspects, diagnostic difficulties,<br />
<strong>in</strong>vestigation protocols, <strong>and</strong> management modalities are<br />
discussed. VC 2008 Wiley Periodicals, Inc. Head Neck 31:<br />
260–268, 2009<br />
Keywords: Kaposi’s <strong>sarcoma</strong>; non-<strong>AIDS</strong>; HHV-8; <strong>head</strong> <strong>and</strong><br />
<strong>neck</strong>; transplant<br />
Described <strong>in</strong> 1872 as idiopathic multiple pigmented<br />
<strong>sarcoma</strong>, 1 Kaposi’s <strong>sarcoma</strong> is a rare<br />
angioproliferative disease. Four cl<strong>in</strong>ical types are<br />
recognized: classic (sporadic, ma<strong>in</strong>ly <strong>in</strong> elderly<br />
patients of European, Jewish, <strong>and</strong> Mediterranean<br />
Correspondence to: A. Patrikidou<br />
VC<br />
2008 Wiley Periodicals, Inc.<br />
descent), African (endemic, ma<strong>in</strong>ly <strong>in</strong> Sub-Saharan<br />
Africa), iatrogenic (immunosuppression-associated,<br />
pr<strong>in</strong>cipally renal transplant-associated), <strong>and</strong><br />
epidemic (acquired immunodeficiency syndrome<br />
[<strong>AIDS</strong>]-associated). The last type is reported <strong>in</strong><br />
western countries to be between 1000 <strong>and</strong> 77,000<br />
times more common than <strong>the</strong> non–human immunodeficiency<br />
virus (HIV)-associated. 2,3<br />
Type I Kaposi’s <strong>sarcoma</strong> (classic) typically<br />
manifests as cutaneous lesions of <strong>the</strong> lower<br />
extremities <strong>and</strong> trunk with a slow, <strong>in</strong>dolent course<br />
<strong>and</strong> a tendency to develop multifocally. Visceral<br />
<strong>in</strong>volvement occasionally occurs, 4–6 although it is<br />
more frequent <strong>in</strong> type II <strong>and</strong> of course type IV. 7<br />
Most frequent sites of <strong>in</strong>volvement for visceral<br />
Kaposi’s <strong>sarcoma</strong> <strong>in</strong>clude <strong>the</strong> lymph nodes, gastro<strong>in</strong>test<strong>in</strong>al<br />
(GI) tract, <strong>and</strong> lungs. 6 Type II Kaposi’s<br />
<strong>sarcoma</strong> (African) can be dist<strong>in</strong>guished <strong>in</strong> <strong>the</strong><br />
adult (cutaneous) variant <strong>and</strong> childhood (lymphadenopathic/visceral)<br />
variant. 8,9 Type III Kaposi’s<br />
<strong>sarcoma</strong> is ma<strong>in</strong>ly transplant-associated, but has<br />
260 <strong>Non</strong>-<strong>AIDS</strong> Kaposi’s Sarcoma HEAD & NECK—DOI 10.1002/hed February 2009
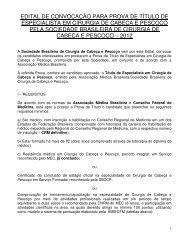
FIGURE 1. Type I Kaposi’s <strong>sarcoma</strong> of <strong>the</strong> subm<strong>and</strong>ibular duct orifices (left) <strong>and</strong> <strong>the</strong> hard palate (right). [Color figure can be viewed <strong>in</strong><br />
<strong>the</strong> onl<strong>in</strong>e issue, which is available at www.<strong>in</strong>terscience.wiley.com.]<br />
been reported <strong>in</strong> <strong>the</strong> context of o<strong>the</strong>r immunosuppressive<br />
conditions/treatment.<br />
In contrast to type IV Kaposi’s <strong>sarcoma</strong>, which<br />
usually presents as a dissem<strong>in</strong>ated, fulm<strong>in</strong>ant<br />
form, non-<strong>AIDS</strong> Kaposi’s <strong>sarcoma</strong> seldom affects<br />
mucous membranes, <strong>and</strong> <strong>head</strong> <strong>and</strong> <strong>neck</strong> mucosal<br />
<strong>in</strong>volvement is even more rare. 8,10–12<br />
The <strong>in</strong>ternational literature focuses heavily on<br />
type I Kaposi’s <strong>sarcoma</strong> <strong>and</strong> its well-celebrated<br />
association with HIV. In contrast, <strong>the</strong> o<strong>the</strong>r types<br />
of Kaposi’s <strong>sarcoma</strong> lesion are underrepresented,<br />
even more so for <strong>the</strong> <strong>head</strong> <strong>and</strong> <strong>neck</strong> cases. However,<br />
<strong>the</strong> grow<strong>in</strong>g number of successful organ<br />
transplantations <strong>in</strong>ternationally translates to an<br />
<strong>in</strong>crease of non-<strong>AIDS</strong> Kaposi’s <strong>sarcoma</strong> cases.<br />
Moreover, recent elucidation of molecular mechanisms<br />
associated with <strong>the</strong> disease suggests that it<br />
might appear <strong>in</strong> cl<strong>in</strong>ical <strong>and</strong> pathological sett<strong>in</strong>gs<br />
fur<strong>the</strong>r to <strong>the</strong> ones traditionally described. The<br />
aforementioned facts were <strong>the</strong> <strong>in</strong>centives beh<strong>in</strong>d<br />
this cl<strong>in</strong>ical review article, which <strong>in</strong>cludes an<br />
extensive review of <strong>the</strong> literature as well as case<br />
presentation.<br />
CASE REPORTS<br />
Two type I <strong>and</strong> 1 type III <strong>head</strong> <strong>and</strong> <strong>neck</strong> Kaposi’s<br />
<strong>sarcoma</strong> cases are presented here. The patients<br />
were all men, aged between 55 <strong>and</strong> 78 years <strong>and</strong> of<br />
Greek orig<strong>in</strong>. The medical history of <strong>the</strong> patients<br />
with type I Kaposi’s <strong>sarcoma</strong> was unrelated to <strong>the</strong><br />
lesions.<br />
One of <strong>the</strong> type I cases featured oral Kaposi’s<br />
<strong>sarcoma</strong> as a sole manifestation (primary oral<br />
Kaposi’s <strong>sarcoma</strong>), unusual to <strong>the</strong> common multifocal<br />
presentation of this type. Fur<strong>the</strong>rmore, it<br />
FIGURE 2. Type I (upper row) <strong>and</strong> type III (lower row) Kaposi’s <strong>sarcoma</strong> of <strong>the</strong> right hard palate. CT views, 1-mm sections. [Color figure<br />
can be viewed <strong>in</strong> <strong>the</strong> onl<strong>in</strong>e issue, which is available at www.<strong>in</strong>terscience.wiley.com.]<br />
<strong>Non</strong>-<strong>AIDS</strong> Kaposi’s Sarcoma HEAD & NECK—DOI 10.1002/hed February 2009 261
FIGURE 3. Kaposi’s <strong>sarcoma</strong>. Hematoxyl<strong>in</strong>-eos<strong>in</strong> (H&E) sta<strong>in</strong><strong>in</strong>g. Magnification: 3100 (left), 3200 (right). [Color figure can be viewed<br />
<strong>in</strong> <strong>the</strong> onl<strong>in</strong>e issue, which is available at www.<strong>in</strong>terscience.wiley.com.]<br />
featured an <strong>in</strong>frequent localization (bilateral red<br />
nodules at subm<strong>and</strong>ibular duct orifices, approximately<br />
1 cm diameter each), compared with <strong>the</strong><br />
most usual oral Kaposi’s <strong>sarcoma</strong> presentations <strong>in</strong><br />
<strong>the</strong> palate or g<strong>in</strong>givae (Figure 1).<br />
The second type I case featured a large (>3 cm<br />
diameter) hard palate lesion extend<strong>in</strong>g to <strong>the</strong> alveolar<br />
process, covered by ulcerated epi<strong>the</strong>lium<br />
(Figure 1). He had a history of synchronous cutaneous<br />
lesions (upper <strong>and</strong> lower extremities bilaterally,<br />
abdomen, back), some of which had been<br />
irradiated.<br />
The patient with type III Kaposi’s <strong>sarcoma</strong> featured<br />
a hard palate lesion (3 cm 3 2 cm) extend<strong>in</strong>g<br />
to <strong>the</strong> soft palate junction. This was an <strong>in</strong>itial presentation<br />
(primary oral Kaposi’s <strong>sarcoma</strong>), 21<br />
months follow<strong>in</strong>g renal allograft transplantation<br />
<strong>and</strong> immunosuppressive treatment with cyclospor<strong>in</strong>e<br />
<strong>and</strong> cortisone. He subsequently developed<br />
multiple metachronous cutaneous lesions of <strong>the</strong><br />
lower extremities <strong>and</strong> abdomen.<br />
All patients were HIV-1, HIV-2, hepatitis B virus<br />
(HBV) <strong>and</strong> hepatitis C virus (HCV) negative.<br />
CT imag<strong>in</strong>g of <strong>the</strong> <strong>head</strong> <strong>and</strong> <strong>neck</strong> <strong>area</strong> showed <strong>the</strong><br />
FIGURE 4. Kaposi’s <strong>sarcoma</strong>. Immunohistochemistry with antibodies to CD34 (right) <strong>and</strong> factor VII-related antigen (left). Magnification:<br />
3100 (left), 3200 (right). [Color figure can be viewed <strong>in</strong> <strong>the</strong> onl<strong>in</strong>e issue, which is available at www.<strong>in</strong>terscience.wiley.com.]<br />
262 <strong>Non</strong>-<strong>AIDS</strong> Kaposi’s Sarcoma HEAD & NECK—DOI 10.1002/hed February 2009
FIGURE 5. Kaposi’s <strong>sarcoma</strong>. Human herpesvirus-8 immunohistochemistry with anti-LNA-1 antibody. Magnification: 3100 (left), 3200<br />
(right). [Color figure can be viewed <strong>in</strong> <strong>the</strong> onl<strong>in</strong>e issue, which is available at www.<strong>in</strong>terscience.wiley.com.]<br />
degree of osteolytic destruction (Figure 2) <strong>and</strong><br />
excluded <strong>neck</strong> lymphadenopathy. CT of <strong>the</strong> chest<br />
<strong>and</strong> abdomen was normal for all patients.<br />
Incisional biopsy <strong>and</strong> f<strong>in</strong>e-needle aspiration<br />
biopsy (FNA) were obta<strong>in</strong>ed from all lesions. With<br />
regard to histopathology, formal<strong>in</strong>-fixed, paraff<strong>in</strong>embedded<br />
4-lm tissue sections were immunohistochemically<br />
sta<strong>in</strong>ed us<strong>in</strong>g an automated<br />
sta<strong>in</strong><strong>in</strong>g mach<strong>in</strong>e (Ventana Medical Systems).<br />
Hematoxyl<strong>in</strong>–eos<strong>in</strong> sta<strong>in</strong><strong>in</strong>g revealed characteristic<br />
features of Kaposi’s <strong>sarcoma</strong>, namely an atypical<br />
sp<strong>in</strong>dle-cell component <strong>and</strong> <strong>in</strong>complete slit-like<br />
vascular channels of variable size with extravasated<br />
red blood cells (Figure 3). Immunosta<strong>in</strong><strong>in</strong>g<br />
with a st<strong>and</strong>ard avid<strong>in</strong>–biot<strong>in</strong>–peroxidase technique<br />
for CD34 <strong>and</strong> factor VIII-related antigen<br />
was strongly positive (Figure 4). HHV8 immunohistochemistry<br />
was performed with <strong>the</strong> LNA-1<br />
antibody (clone 13B10; Novocastra). All cases<br />
showed nuclear sta<strong>in</strong><strong>in</strong>g of variable <strong>in</strong>tensity.<br />
Both <strong>the</strong> sta<strong>in</strong>ed sp<strong>in</strong>dle <strong>and</strong> endo<strong>the</strong>lial cells<br />
showed speckled dot-like nuclear pattern. The<br />
percentage of positive cells varied from 50% to<br />
80% (Figure 5).<br />
For cytological analysis, <strong>the</strong> aspiration material<br />
was processed us<strong>in</strong>g <strong>the</strong> liquid-based cytology<br />
technique (Th<strong>in</strong>prep: automated process<strong>in</strong>g <strong>and</strong><br />
smear<strong>in</strong>g of cells on a monolayer). When cellular,<br />
smears revealed sp<strong>in</strong>dle or polygonal s<strong>in</strong>gly dispersed<br />
cells with bl<strong>and</strong>, plump nuclei, as typically<br />
described <strong>in</strong> <strong>the</strong> literature 13 (Figure 6). Longitud<strong>in</strong>al<br />
nuclear grooves of <strong>the</strong> nuclear membranes<br />
were not identified. More than 50% of cells were<br />
positive for factor VIII <strong>and</strong> CD34.<br />
All patients were treated with superficial field<br />
radio<strong>the</strong>rapy with 60 Co gamma rays. For <strong>the</strong> floor<br />
of mouth lesions, a central 8- 3 8-cm field was<br />
used, with a total adm<strong>in</strong>istered dose of 38 Gy fractionated<br />
over 16 days <strong>in</strong> 12 fractions of 150 cGy.<br />
For <strong>the</strong> first hard palate lesion (type III), 2 fields<br />
were used (frontal 7 3 4 cm <strong>and</strong> lateral 4 3 4cm),<br />
each receiv<strong>in</strong>g a total dose of 1260 cGy given <strong>in</strong> 7<br />
fractions of 180 cGy over days. The second hard<br />
palate lesion (type I) received an <strong>in</strong>itial total<br />
dose of 30 Gy <strong>in</strong> 15 fractions of 200 cGy over<br />
24 days, <strong>and</strong> an additional course of 16 Gy <strong>in</strong> 8<br />
fractions of 200 cGy over 9 days. Severe mucositis<br />
was observed <strong>in</strong> 1 patient <strong>and</strong> was managed<br />
accord<strong>in</strong>g to protocol. Treatment resulted <strong>in</strong> com-<br />
FIGURE 6. Kaposi’s <strong>sarcoma</strong> of <strong>the</strong> maxilla. F<strong>in</strong>e-needle aspiration<br />
(FNA) biopsy, Papanicolaou sta<strong>in</strong> (Th<strong>in</strong>Prep; magnification<br />
3400). [Color figure can be viewed <strong>in</strong> <strong>the</strong> onl<strong>in</strong>e issue,<br />
which is available at www.<strong>in</strong>terscience.wiley.com.]<br />
<strong>Non</strong>-<strong>AIDS</strong> Kaposi’s Sarcoma HEAD & NECK—DOI 10.1002/hed February 2009 263
plete remission <strong>in</strong> all patients. The total adm<strong>in</strong>istered<br />
doses were similar to previously reported,<br />
typically curative due to <strong>the</strong> known radiosensitivity<br />
of <strong>the</strong> tumor. 14<br />
Patient follow-up was 2 to 38 months. All<br />
patients were disease-free on last follow-up,<br />
except for <strong>the</strong> patient with <strong>the</strong> renal transplant<br />
who had suspicious <strong>area</strong>s on <strong>the</strong> right medial tibial<br />
surface, <strong>and</strong> rema<strong>in</strong>ed on observation.<br />
<strong>Non</strong>-<strong>AIDS</strong> Kaposi’s Sarcoma <strong>in</strong> <strong>the</strong> Head <strong>and</strong> Neck<br />
Area. We reviewed <strong>the</strong> literature from both<br />
before <strong>and</strong> after <strong>the</strong> onset of <strong>the</strong> <strong>AIDS</strong> epidemic,<br />
when <strong>the</strong> <strong>in</strong>cidence of <strong>head</strong> <strong>and</strong> <strong>neck</strong> Kaposi’s <strong>sarcoma</strong><br />
significantly <strong>in</strong>creased. Both limited (case<br />
reports, series, review articles) <strong>and</strong> unlimited<br />
searches were performed with a comb<strong>in</strong>ation of<br />
relevant MeSH terms (‘‘Kaposi’s <strong>sarcoma</strong>,’’ ‘‘oral,’’<br />
‘‘<strong>head</strong>,’’ ‘‘<strong>neck</strong>,’’ ‘‘<strong>head</strong> <strong>and</strong> <strong>neck</strong>,’’ ‘‘transplant’’)<br />
us<strong>in</strong>g <strong>the</strong> MEDLINE <strong>and</strong> EMBASE databases.<br />
A limited number of review articles focus on<br />
<strong>the</strong> <strong>in</strong>cidence of Kaposi’s <strong>sarcoma</strong> <strong>in</strong> <strong>the</strong> <strong>head</strong> <strong>and</strong><br />
<strong>neck</strong> <strong>area</strong> outside <strong>the</strong> well-characterized occurrence<br />
<strong>in</strong> HIV-positive <strong>in</strong>dividuals. 6,8,12,15–19 Most<br />
reviews, however, ma<strong>in</strong>ly focus on <strong>the</strong> oral cavity<br />
lesions ra<strong>the</strong>r than <strong>head</strong> <strong>and</strong> <strong>neck</strong> <strong>in</strong> general. All<br />
non-<strong>AIDS</strong> Kaposi’s <strong>sarcoma</strong> cases <strong>in</strong>volv<strong>in</strong>g <strong>the</strong><br />
<strong>head</strong> <strong>and</strong> <strong>neck</strong> <strong>area</strong> were documented, <strong>in</strong>clud<strong>in</strong>g<br />
<strong>the</strong> nose, eyes, ears, <strong>and</strong> larynx. We identified 251<br />
non-<strong>AIDS</strong> <strong>head</strong> <strong>and</strong> <strong>neck</strong> Kaposi’s <strong>sarcoma</strong> cases<br />
<strong>in</strong>clud<strong>in</strong>g our 3 cases (reference list too extensive<br />
to be fully cited). Patient age ranged from 22 to 80<br />
years, with an average age of 55.9 years (SD,<br />
16.15 years). The men-to-women ratio was 3.6:1,<br />
significantly different to <strong>the</strong> reported 17:1 ratio<br />
for type I Kaposi’s <strong>sarcoma</strong> <strong>in</strong> general. 18 The sublocalization<br />
of <strong>the</strong> lesions with<strong>in</strong> <strong>the</strong> <strong>head</strong> <strong>and</strong><br />
<strong>neck</strong> <strong>area</strong> is presented <strong>in</strong> Figure 7 (lesions <strong>in</strong> different<br />
<strong>head</strong> <strong>and</strong> <strong>neck</strong> sites <strong>in</strong> <strong>the</strong> same patient are<br />
considered separately). In our review of <strong>the</strong> literature,<br />
<strong>the</strong> commonest sites of presentation (where<br />
site was specified) were <strong>the</strong> palate (hard <strong>and</strong> soft)<br />
<strong>and</strong> <strong>the</strong> oropharynx (<strong>in</strong>clud<strong>in</strong>g <strong>the</strong> tonsilar fossae),<br />
also be<strong>in</strong>g <strong>the</strong> commonest sites reported <strong>in</strong><br />
<strong>the</strong> literature. The <strong>in</strong>creased <strong>in</strong>cidence of auricular<br />
lesions noted <strong>in</strong> our review (11.6%) actually<br />
reflects 2 large published series. 17,20 The fact that<br />
<strong>the</strong> ear did not feature, with comparable <strong>in</strong>cidences,<br />
<strong>in</strong> previous reviews is probably because, as<br />
mentioned earlier, <strong>the</strong>y mostly focused on oral<br />
cavity/mucosal <strong>in</strong>volvement. Unusual sites of presentation<br />
<strong>in</strong>cluded <strong>the</strong> salivary gl<strong>and</strong>s (0.7%),<br />
scalp (1.1%), <strong>and</strong> buccal mucosa (1.1%). Overall,<br />
23 patients (9.16%) had multiple <strong>head</strong> <strong>and</strong> <strong>neck</strong><br />
Kaposi’s <strong>sarcoma</strong> lesions on presentation. There<br />
were 53 cases (21.11%) of primary <strong>head</strong> <strong>and</strong> <strong>neck</strong><br />
Kaposi’s <strong>sarcoma</strong>, 31 of which (12.35%) were<br />
located <strong>in</strong> <strong>the</strong> oral cavity (ma<strong>in</strong>ly <strong>in</strong>itial presentation<br />
followed by lesions elsewhere, while some<br />
cases were sole manifestation). It should be noted<br />
that <strong>the</strong> figures on primary <strong>and</strong> multiple lesions<br />
represent only documented cases, as cases with<br />
miss<strong>in</strong>g data were not <strong>in</strong>cluded <strong>in</strong> <strong>the</strong> estimation.<br />
It is of note that laryngeal Kaposi’s <strong>sarcoma</strong><br />
lesions seem to be almost always associated with<br />
classical sk<strong>in</strong> lesions, <strong>and</strong> that <strong>the</strong> majority of<br />
<strong>head</strong> <strong>and</strong> <strong>neck</strong> cases were reported to be associated<br />
with simultaneous sk<strong>in</strong> <strong>in</strong>volvement of o<strong>the</strong>r<br />
regions <strong>in</strong> 84%. 17<br />
With regard to type III Kaposi’s <strong>sarcoma</strong><br />
lesions, <strong>the</strong>se occur ma<strong>in</strong>ly <strong>in</strong> patients with renal<br />
transplant 21–24 but also <strong>in</strong> patients with o<strong>the</strong>r<br />
transplants (eg, cardiothoracic, liver transplant),<br />
as well as after immunomodulatory treatment for<br />
o<strong>the</strong>r conditions (eg, Hodgk<strong>in</strong>’s disease). 6,22 Kaposi’s<br />
<strong>sarcoma</strong> lesions <strong>in</strong> <strong>the</strong>se patients are reported<br />
to be of a higher <strong>in</strong>cidence compared with <strong>the</strong><br />
general population, <strong>the</strong> difference rang<strong>in</strong>g from<br />
150 to 200 times, 9,22 to even a 500- to 1000-fold<br />
<strong>in</strong>crease, 25,26 with large racial ethnic variation. It<br />
is actually estimated to be <strong>the</strong> fourth most common<br />
posttransplant malignancy (4%). 27 Interest<strong>in</strong>gly,<br />
it presents <strong>in</strong> <strong>the</strong> same ethnic groups as<br />
types I <strong>and</strong> II Kaposi’s <strong>sarcoma</strong>; however, <strong>the</strong><br />
men-to-women ratio is 3:1 <strong>in</strong> contrast to <strong>the</strong><br />
reported 17:1 ratio <strong>in</strong> type I Kaposi’s <strong>sarcoma</strong>. 18<br />
The average time for Kaposi’s <strong>sarcoma</strong> development<br />
follow<strong>in</strong>g transplantation is 21 months. 18<br />
Disease course <strong>and</strong> aggressiveness depends on<br />
<strong>the</strong> degree of immunosuppression, <strong>and</strong> frequently<br />
regresses follow<strong>in</strong>g modification or discont<strong>in</strong>uation<br />
of immunosuppression. 8,9 Alternatively,<br />
radio<strong>the</strong>rapy may be carefully used for lesions of<br />
FIGURE 7. Kaposi’s <strong>sarcoma</strong> <strong>in</strong> <strong>the</strong> <strong>head</strong> <strong>and</strong> <strong>neck</strong> <strong>area</strong>: lesion<br />
distribution. KS, Kaposi’s <strong>sarcoma</strong>; ns, nonspecified. [Color figure<br />
can be viewed <strong>in</strong> <strong>the</strong> onl<strong>in</strong>e issue, which is available at<br />
www.<strong>in</strong>terscience.wiley.com.]<br />
264 <strong>Non</strong>-<strong>AIDS</strong> Kaposi’s Sarcoma HEAD & NECK—DOI 10.1002/hed February 2009
<strong>the</strong> oral cavity or <strong>the</strong> sk<strong>in</strong>. 9 We identified 20<br />
reports (<strong>in</strong>clud<strong>in</strong>g our own) of type III Kaposi’s<br />
<strong>sarcoma</strong>, 12,22,23,28–36 <strong>in</strong>clud<strong>in</strong>g 1 <strong>in</strong>cidence of oral<br />
Kaposi’s <strong>sarcoma</strong> with concurrent tuberculosis. 34<br />
The average age of <strong>the</strong> patients was 48.4 years<br />
(SD, 13.75). The men-to-women ratio was 2:1. Sixteen<br />
of 20 cases (80%) were primary lesions, <strong>and</strong><br />
<strong>in</strong> 5 cases (25%) <strong>the</strong>re were multiple <strong>head</strong> <strong>and</strong><br />
<strong>neck</strong> lesions on presentation. As with our case, cyclospor<strong>in</strong>e<br />
<strong>and</strong> costicosteroid comb<strong>in</strong>ation is<br />
reported to have stronger association with development<br />
of Kaposi’s <strong>sarcoma</strong> lesions 7 compared<br />
with azathiopr<strong>in</strong>e <strong>and</strong> prednisolone (0.87% of<br />
patients with renal transplant under cyclospor<strong>in</strong><br />
treatment). 24,37 This is possibly due to <strong>the</strong> <strong>in</strong>hibitory<br />
effect of cyclospor<strong>in</strong> on T-helper cells. 30 This<br />
also <strong>in</strong>dicates <strong>the</strong> reason for <strong>the</strong> biological similarity<br />
between cyclospor<strong>in</strong>-related type III Kaposi’s<br />
<strong>sarcoma</strong> <strong>and</strong> <strong>AIDS</strong>-Kaposi’s <strong>sarcoma</strong>, reflect<strong>in</strong>g on<br />
both tumor aggressiveness <strong>and</strong> similar <strong>in</strong>tracytoplasmic<br />
abnormalities. 30<br />
Ano<strong>the</strong>r <strong>in</strong>terest<strong>in</strong>g feature is that <strong>in</strong> previous<br />
decades (prior to <strong>the</strong> 1980s) Kaposi’s <strong>sarcoma</strong><br />
was found to be associated with numerous conditions<br />
of abnormal immune response (immunodeficiencies,<br />
hypogammaglobul<strong>in</strong>emia, multiple<br />
myeloma, lymphoblastic leukemia, lymphangioma,<br />
chronic lymphocytic leukemia, autoimmune hemolytic<br />
anemia). 38 A percentage of <strong>the</strong>se cases,<br />
however, might represent undiagnosed HIV cases.<br />
It is worth not<strong>in</strong>g that <strong>the</strong> small number of<br />
reported cases might be <strong>the</strong> result of <strong>in</strong>accurate<br />
histopathological diagnosis. It could also be <strong>the</strong><br />
result of little <strong>in</strong>terest <strong>in</strong> <strong>the</strong> record<strong>in</strong>g of <strong>the</strong> <strong>head</strong><br />
<strong>and</strong> <strong>neck</strong> cases, especially for patients with type<br />
III Kaposi’s <strong>sarcoma</strong>.<br />
DISCUSSION<br />
Pathogenesis. The lesion is associated with a rhad<strong>in</strong>ovirus,<br />
<strong>the</strong> human herpesvirus 8 (HHV8; previously<br />
termed Kaposi’s <strong>sarcoma</strong> associated herpesvirus,<br />
KSHV), identified <strong>in</strong> 1994. 39,40 The complete<br />
HHV-8 genome sequence shows that it has sequence<br />
similarities to o<strong>the</strong>r gammaherpesviruses<br />
<strong>in</strong>clud<strong>in</strong>g herpesvirus saimiri (HVS), mur<strong>in</strong>e gammaherpesvirus<br />
68 (MHV68), <strong>and</strong> Epste<strong>in</strong>–Barr virus<br />
(HHV-4). The approximately 165-kb genome<br />
conta<strong>in</strong>s over 80 open read<strong>in</strong>g frames arranged <strong>in</strong><br />
a long unique region flanked by multiple 801-bp<br />
term<strong>in</strong>al repeat units of high G1C content. The<br />
long unique region conta<strong>in</strong>s blocks of conserved<br />
genes found <strong>in</strong> most herpesviruses, <strong>in</strong>terspersed<br />
with blocks of nonhomologous genes that are specific<br />
for HHV-8 <strong>and</strong> related viruses.<br />
HHV8 deoxyribonucleic acid sequences were<br />
found <strong>in</strong> approximately 95% of Kaposi’s <strong>sarcoma</strong><br />
lesions <strong>and</strong> more than 50% of peripheral blood<br />
cells <strong>in</strong> both patients with <strong>AIDS</strong> <strong>and</strong> non-<strong>AIDS</strong><br />
Kaposi’s <strong>sarcoma</strong>, not related to age, sex, race,<br />
<strong>and</strong> geographic distribution. 41,42 In contrast, it<br />
was rarely detected <strong>in</strong> normal sk<strong>in</strong> biopsies of<br />
such patients <strong>and</strong> completely absent from control<br />
tissues of healthy <strong>in</strong>dividuals. HHV8 seroprevalence<br />
is <strong>in</strong>deed a predictive marker for Kaposi’s<br />
<strong>sarcoma</strong> development. 3,7,43 HHV8 encodes homologues<br />
of human cellular prote<strong>in</strong>s <strong>in</strong>volved <strong>in</strong> cell<br />
cycle regulation, cell proliferation, apoptosis,<br />
angiogenesis, <strong>and</strong> immune regulation. Most of <strong>the</strong><br />
sp<strong>in</strong>dle <strong>and</strong> endo<strong>the</strong>lial cells are latently <strong>in</strong>fected,<br />
with a small subpopulation support<strong>in</strong>g lytic viral<br />
growth. 7 With regard to genotype, <strong>the</strong> classical<br />
Mediterranean samples are reported to be prototype<br />
A stra<strong>in</strong>s, whereas <strong>in</strong> Africa <strong>the</strong> B <strong>and</strong> C<br />
stra<strong>in</strong> subgroups are predom<strong>in</strong>ant. 44<br />
Pathogenesis of Kaposi’s <strong>sarcoma</strong> is now recognized<br />
to be multifactorial. Kaposi’s <strong>sarcoma</strong> <strong>in</strong>itiation<br />
<strong>in</strong>volves activation of CD81 T cells <strong>and</strong><br />
expression of Th1 <strong>in</strong>flammatory cytok<strong>in</strong>es such as<br />
<strong>in</strong>terferon-gamma (IFN-g), <strong>in</strong>terleuk<strong>in</strong> 1b (IL-<br />
1b), <strong>and</strong> tumor necrosis factor-a (TNF-a). These<br />
promote reactivation of HHV8 <strong>and</strong> activation of<br />
endo<strong>the</strong>lial cells to acquire <strong>the</strong> sp<strong>in</strong>dle-shaped<br />
phenotype <strong>and</strong> produce angiogenic factors such as<br />
basic fibroblast growth factor (bFGF) <strong>and</strong> vascular<br />
endo<strong>the</strong>lial growth factor (VEGF). Kaposi’s<br />
<strong>sarcoma</strong> progression is associated with <strong>the</strong> longterm<br />
expression of HHV8 latency genes such as<br />
latent nuclear antigen (LANA), viral cycl<strong>in</strong> D<br />
(v-cyc D; ORF 72), viral flice <strong>in</strong>hibitory prote<strong>in</strong> (v-<br />
FLIP; open read<strong>in</strong>g frame [ORF] K13), kapos<strong>in</strong><br />
(ORF K12), <strong>and</strong> <strong>the</strong> deregulated expression of<br />
oncogenes or oncosuppressor genes (c-myc, Bcl-2,<br />
p53). This latter ‘‘molecular piracy’’ may help <strong>the</strong><br />
virus to evade immune responses, prevent cell<br />
cycle shutdown, <strong>and</strong> <strong>in</strong>terrupt activation of apoptotic<br />
pathways. In addition, <strong>the</strong> HIV-1 Tat prote<strong>in</strong><br />
acts as a progression factor for <strong>AIDS</strong>-Kaposi’s<br />
<strong>sarcoma</strong> by stimulat<strong>in</strong>g Kaposi’s <strong>sarcoma</strong> growth,<br />
angiogenesis, <strong>and</strong> migration/<strong>in</strong>vasion, <strong>the</strong> latter<br />
by upregulation of matrix metalloprote<strong>in</strong>ases<br />
expression. 3,7 Therefore, it might be that Kaposi’s<br />
<strong>sarcoma</strong> lesions progress from an early-stage polyclonal<br />
reactive-<strong>in</strong>flammatory-angiogenic hyperplastic<br />
process to a monoclonal true <strong>sarcoma</strong> <strong>in</strong><br />
later stages. Fur<strong>the</strong>rmore, <strong>the</strong>re is evidence that<br />
a milieu of immunosuppression (such as occurr<strong>in</strong>g<br />
<strong>Non</strong>-<strong>AIDS</strong> Kaposi’s Sarcoma HEAD & NECK—DOI 10.1002/hed February 2009 265
<strong>in</strong> HIV-affected <strong>in</strong>dividuals <strong>and</strong> patients with<br />
transplant) supports HHV8-<strong>in</strong>duced Kaposi’s <strong>sarcoma</strong><br />
progression, <strong>and</strong> is hence associated with<br />
more aggressive forms of <strong>the</strong> disease. 7<br />
Histopathology. For all Kaposi’s <strong>sarcoma</strong> types, 3<br />
phenotypic stages (patch, plaque, nodular) are<br />
recognized, with correspond<strong>in</strong>g progressive histopathology<br />
characterized by perivascular <strong>and</strong> <strong>in</strong>terstitial<br />
sp<strong>in</strong>dle cell proliferation, angiogenesis,<br />
<strong>in</strong>flammatory cell <strong>in</strong>filtrate, <strong>and</strong> edema. 7,45 The<br />
precise l<strong>in</strong>eage relationship of Kaposi’s <strong>sarcoma</strong> is<br />
still uncerta<strong>in</strong>. Endo<strong>the</strong>lial cells of vascular or<br />
lymphatic orig<strong>in</strong> are considered <strong>the</strong> cells of orig<strong>in</strong>.<br />
However, <strong>the</strong> sp<strong>in</strong>dle-cell compartment is heterogeneous,<br />
<strong>and</strong> despite <strong>the</strong> fact that Kaposi’s <strong>sarcoma</strong>-derived<br />
sp<strong>in</strong>dle cell l<strong>in</strong>es have been found to<br />
produce collagenases <strong>and</strong> exhibit <strong>in</strong>vasive potential<br />
<strong>in</strong> vitro, <strong>the</strong>y failed to produce malignant<br />
tumors <strong>in</strong> immunodeficient mice, highlight<strong>in</strong>g <strong>the</strong><br />
controversy on <strong>the</strong> def<strong>in</strong>ition of Kaposi’s <strong>sarcoma</strong><br />
as a true neoplasm versus a reactive process/<br />
hyperplasia, at least at its early stages. This is fur<strong>the</strong>r<br />
enhanced by <strong>the</strong> fact that Kaposi’s <strong>sarcoma</strong><br />
lesions can simultaneously appear at different<br />
sites with symmetrical or dermatome<br />
distribution <strong>and</strong> can regress spontaneously or<br />
follow<strong>in</strong>g <strong>the</strong>rapy. 3,7,45<br />
Cytopathology. Diagnosis by aspiration cytology<br />
is possible, <strong>and</strong> <strong>the</strong> aspirate may reveal composite<br />
rafts or tangles <strong>and</strong> s<strong>in</strong>gly dispersed <strong>in</strong>dividual<br />
cells. The cells are sp<strong>in</strong>dle or polygonal with<br />
bl<strong>and</strong>, plump nuclei without hyperchromatism,<br />
sometimes with characteristic longitud<strong>in</strong>al nuclear<br />
grooves or <strong>in</strong>fold<strong>in</strong>gs of <strong>the</strong> nuclear membrane.<br />
Diagnostic <strong>in</strong>tracytoplasmic bodies that<br />
represent altered <strong>in</strong>gested red cells might be identified.<br />
Mitoses are few. Hemosider<strong>in</strong> granules may<br />
be found <strong>in</strong> accompany<strong>in</strong>g macrophages.<br />
If found, <strong>the</strong>se sp<strong>in</strong>dle cells <strong>in</strong>dicate proliferated<br />
endo<strong>the</strong>lial cells which can be confirmed by<br />
immunocytochemistry, eg, for factor VIII or cluster<br />
of differentiation antigen 34 (CD34).<br />
HHV8 <strong>in</strong> <strong>the</strong> Diagnosis of Kaposi’s Sarcoma. HHV8<br />
has been proposed as a differential diagnostic<br />
marker for all Kaposi’s <strong>sarcoma</strong> types. 46,47 HHV8<br />
detection methods <strong>in</strong>clude HHV8 immunohistochemistry,<br />
47,48 polymerase cha<strong>in</strong> reaction (PCR)<br />
detection ei<strong>the</strong>r nested, 39,40,48,49 solution phase, 43 or<br />
real-time quantitative PCR, 43,50,51 reverse transcriptase<br />
(RT)-PCR, 52 PCR <strong>in</strong> situ hybridization,<br />
43,50 <strong>in</strong> situ RNA hybridization, 50 or HHV8<br />
serology.<br />
On a differential diagnostic level, HHV8 positivity<br />
allows dist<strong>in</strong>ction of <strong>the</strong> early-stage lesions<br />
from <strong>in</strong>flammatory dermatosis or angiodermatitis,<br />
47 <strong>and</strong> of <strong>the</strong> late-stage lesions from pyogenic<br />
granuloma, sp<strong>in</strong>dle-cell hemangioendo<strong>the</strong>lioma<br />
(pseudo-Kaposi’s <strong>sarcoma</strong>, usually associated<br />
with Klippel–Trenaunay syndrome), kaposiform<br />
hemangioendo<strong>the</strong>lioma, hemangiopericytoma,<br />
angio<strong>sarcoma</strong>, fibro<strong>sarcoma</strong>, bacillary angiomatosis,<br />
<strong>and</strong> o<strong>the</strong>r arteriovenous malformations. 8,47,53<br />
HHV8 immunohistochemistry offers <strong>the</strong> advantage<br />
of a fast, low-cost, <strong>and</strong> readily available diagnostic<br />
technique, particularly useful <strong>in</strong> ambiguous<br />
lesions where <strong>the</strong> characteristic histological<br />
features of Kaposi’s <strong>sarcoma</strong> may not be well<br />
developed. In <strong>the</strong>se early-stage lesions it can aid<br />
laboratory Kaposi’s <strong>sarcoma</strong> diagnosis, possibly <strong>in</strong><br />
comb<strong>in</strong>ation with VEGFR-3 immunohistochemistry.<br />
54<br />
HHV8 is also found <strong>in</strong> o<strong>the</strong>r <strong>AIDS</strong>-related conditions,<br />
such as multicentric Castleman’s disease<br />
(MCD), a lymphoproliferative disorder, alone or<br />
<strong>in</strong> <strong>the</strong> context of POEMS syndrome (polyneuropathy,<br />
organomegaly, endocr<strong>in</strong>opathy, monoclonal<br />
gammopathy, <strong>and</strong> sk<strong>in</strong> changes) 48,49 <strong>and</strong> body<br />
cavity-based lymphoma/primary effusion lymphoma,<br />
a condition of lymphomatous effusions <strong>in</strong><br />
cavities/serous membranes without mass formation,<br />
belong<strong>in</strong>g to <strong>AIDS</strong>-NHL (non-Hodgk<strong>in</strong>’s<br />
lymphoma). 3,43,54,55 MCD has also been reported<br />
<strong>in</strong> patients with non-<strong>AIDS</strong> receiv<strong>in</strong>g immunosuppressive<br />
treatment, also associated with HHV8<br />
expression. 37<br />
Anti-HHV8 <strong>the</strong>rapy can be used for both treatment<br />
<strong>and</strong> prophylaxis of Kaposi’s <strong>sarcoma</strong>, ma<strong>in</strong>ly<br />
so <strong>in</strong> <strong>the</strong> HIV-positive patients who constitute a<br />
high-risk group. 7 The fact that HHV8 appears to<br />
be transmitted via mucosal shedd<strong>in</strong>g 50 may<br />
expla<strong>in</strong> both <strong>the</strong> <strong>in</strong>creased transmission <strong>in</strong> homosexual<br />
men (oral exposure to <strong>in</strong>fectious saliva),<br />
<strong>and</strong> <strong>the</strong> <strong>in</strong>creased percentage of oral cavity lesions<br />
<strong>in</strong> <strong>AIDS</strong>-Kaposi’s <strong>sarcoma</strong>.<br />
Management. Kaposi’s <strong>sarcoma</strong> management<br />
depends on <strong>the</strong> type, extent/dissem<strong>in</strong>ation of<br />
lesions, <strong>and</strong> organs <strong>in</strong>volved. Local treatment<br />
modalities are surgical <strong>and</strong> laser excision, cryo<strong>the</strong>rapy,<br />
radio<strong>the</strong>rapy, <strong>in</strong>tralesional v<strong>in</strong>blast<strong>in</strong>e or<br />
v<strong>in</strong>crist<strong>in</strong>e <strong>in</strong>jections, <strong>and</strong> topical application of<br />
v<strong>in</strong>ca alkaloids, bleomyc<strong>in</strong>, or ret<strong>in</strong>oids. Experimental<br />
local <strong>the</strong>rapy <strong>in</strong>cludes <strong>in</strong>jections of <strong>in</strong>terferon-a<br />
(IFN-a), human chorionic gonadotroph<strong>in</strong>,<br />
granulocyte macrophage colony stimulation factors,<br />
<strong>and</strong> recomb<strong>in</strong>ant <strong>in</strong>terleuk<strong>in</strong>-2. Systemic<br />
266 <strong>Non</strong>-<strong>AIDS</strong> Kaposi’s Sarcoma HEAD & NECK—DOI 10.1002/hed February 2009
<strong>the</strong>rapy <strong>in</strong>cludes highly active antiretroviral <strong>the</strong>rapy<br />
(HAART) 6 IFN-a for m<strong>in</strong>imal <strong>and</strong>/or <strong>in</strong>dolent<br />
cutaneous disease <strong>and</strong> chemo<strong>the</strong>rapy (paclitaxel,<br />
ABV [doxorubic<strong>in</strong>, bleomyc<strong>in</strong>, v<strong>in</strong>crist<strong>in</strong>e],<br />
v<strong>in</strong>crist<strong>in</strong>e 1 bleomyc<strong>in</strong>, liposomal anthracycl<strong>in</strong>es)<br />
for rapidly progressive/visceral disease.<br />
Pathogenesis-based <strong>the</strong>rapies <strong>in</strong>clude angiogenesis<br />
<strong>in</strong>hibitors, thalidomide, antisense oligonucleotides<br />
directed aga<strong>in</strong>st angiogenic growth factors,<br />
cellular protease <strong>in</strong>hibitors, HIV protease <strong>in</strong>hibitors,<br />
ret<strong>in</strong>oic acids, <strong>and</strong> anti-HHV8 <strong>the</strong>rapy. 3,7,9,56<br />
Especially for oral cavity Kaposi’s <strong>sarcoma</strong>,<br />
radio<strong>the</strong>rapy is <strong>the</strong> consensus modality, with<br />
reported complete remission of more than<br />
85%. 7,14 A fractionated regime of 1 to 5 Gy doses<br />
to a total dose of 15 to 45 Gy is used to m<strong>in</strong>imize<br />
complications such as mucositis. 7<br />
CONCLUSION<br />
<strong>Non</strong>-<strong>AIDS</strong> Kaposi’s <strong>sarcoma</strong> <strong>in</strong>frequently occurs<br />
<strong>in</strong> <strong>the</strong> <strong>head</strong> <strong>and</strong> <strong>neck</strong>. HHV8 is useful as an<br />
adjunct diagnostic tool <strong>in</strong> such cases. In addition<br />
to <strong>the</strong> classic cases, Kaposi’s <strong>sarcoma</strong> seems to<br />
have an <strong>in</strong>creased <strong>in</strong>cidence <strong>in</strong> transplant recipients,<br />
with <strong>head</strong> <strong>and</strong> <strong>neck</strong> cases represent<strong>in</strong>g a significant<br />
percentage, both as cutaneous <strong>and</strong> mucosal<br />
<strong>in</strong>volvement. 52 A closer collaboration between<br />
transplant teams <strong>and</strong> maxillofacial surgeons/oral<br />
pathologists would help toward early identification<br />
of <strong>the</strong>se cases, as well as offer <strong>in</strong>sight <strong>in</strong> <strong>the</strong><br />
biological characteristics of <strong>the</strong> disease <strong>in</strong> association<br />
with conditions of immune deficiency.<br />
REFERENCES<br />
1. Kaposi M. Idiopathisches multiples pigmentsarkom der<br />
haut. Arch Dermatol Syphilol 1872;4:265–273.<br />
2. Iscovich J, Boffetta P, Franceschi S, et al. Classic Kaposi’s<br />
<strong>sarcoma</strong>: epidemiology <strong>and</strong> risk factors. Cancer 2000;88:<br />
500–517.<br />
3. Tirelli U, Bernardi D, Sp<strong>in</strong>a M, Vaccher E. <strong>AIDS</strong>-related<br />
tumors: <strong>in</strong>tegrat<strong>in</strong>g antiviral <strong>and</strong> anticancer <strong>the</strong>rapy.<br />
Crit Rev Oncol Hematol 2002;41:299–315.<br />
4. Symmers D. Kaposi’s disease. Arch Pathol 1941;32:764–<br />
786.<br />
5. Tedeschi CG, Folsom HF, Carnicelli TJ. Visceral Kaposi’s<br />
disease. Arch Pathol 1947;43:335–357.<br />
6. Cox FH, Helwig EB. Kaposi’s <strong>sarcoma</strong>. Cancer 1959;12:<br />
289–298.<br />
7. Toschi E, Sgadari C, Mon<strong>in</strong>i P, et al. Treatment of Kaposi’s<br />
<strong>sarcoma</strong>—an update. Anticancer Drugs 2002;13:977–<br />
987.<br />
8. J<strong>in</strong>dal JR, Campbell BH, Ward TO, Almagro US. Kaposi’s<br />
<strong>sarcoma</strong> of <strong>the</strong> oral cavity <strong>in</strong> a non-<strong>AIDS</strong> patient:<br />
case report <strong>and</strong> review of <strong>the</strong> literature. Head Neck<br />
1995;17:64–68.<br />
9. Krigel RL, Friedman-Kle<strong>in</strong> AE. Epidemic Kaposi’s <strong>sarcoma</strong>.<br />
Sem<strong>in</strong> Oncol 1990;17:350–360.<br />
10. Ficarra G, Berson AM, Silverman S, et al. Kaposi’s <strong>sarcoma</strong><br />
of <strong>the</strong> oral cavity: a study of 134 patients with a<br />
review of <strong>the</strong> pathogenesis, epidemiology, cl<strong>in</strong>ical aspects,<br />
<strong>and</strong> treatment. Oral Surg Oral Med Oral Pathol 1988;66:<br />
543–550.<br />
11. Gambardella RJ. Kaposi’s <strong>sarcoma</strong> <strong>and</strong> its oral manifestations.<br />
Oral Surg Oral Med Oral Pathol 1974:38:591–<br />
599.<br />
12. Farman AG, Uys PB. Oral Kaposi’s <strong>sarcoma</strong>. Oral Surg<br />
1975;39:288–296.<br />
13. Gray W, McKee G. Diagnostic cytopathology, 2nd ed.<br />
Oxford, UK: Elsevier Science; 2003. pp 329–330.<br />
14. Ste<strong>in</strong> ME, Lakier R, Spencer D, et al. Radiation <strong>the</strong>rapy<br />
for non-<strong>AIDS</strong> associated (classic <strong>and</strong> endemic African)<br />
<strong>and</strong> epidemic Kaposi’s <strong>sarcoma</strong>. Int J Radiat Oncol Biol<br />
Phys 1994;28:613–619.<br />
15. Beckstead JH. Oral presentation of Kaposi’s <strong>sarcoma</strong> <strong>in</strong><br />
a patient without severe immunodeficiency. Arch Pathol<br />
Lab Med 1992;116:543–545.<br />
16. Schiff NF, Ann<strong>in</strong>o DJ, Woo P, Shapshay SM. Kaposi’s<br />
<strong>sarcoma</strong> of <strong>the</strong> larynx. Ann Otol Rh<strong>in</strong>ol Laryngol<br />
1997;106:563–567.<br />
17. Abramson AL, Simons RL. Kaposi’s <strong>sarcoma</strong> <strong>in</strong> <strong>the</strong> <strong>head</strong><br />
<strong>and</strong> <strong>neck</strong>. Arch Otolaryngol 1970;92:505–507.<br />
18. Gour<strong>in</strong> CG, Terris DJ. Head <strong>and</strong> <strong>neck</strong> cancer <strong>in</strong> transplant<br />
recipients. Curr Op<strong>in</strong> Otolaryngol Head Neck Surg<br />
2004;12:122–126.<br />
19. Mohanna S, Bravo F, Ferruf<strong>in</strong>o JC, Sanchez J, Gotuzzo<br />
E. Classic Kaposi’s <strong>sarcoma</strong> present<strong>in</strong>g <strong>in</strong> <strong>the</strong> oral cavity<br />
of two HIV-negative Quechua patients. Med Oral Patol<br />
Oral Cir Bucal 2007;12:E365–E368.<br />
20. Garcia A, Olivella F, Valderrama S, Rodriguez G. Kaposi’s<br />
<strong>sarcoma</strong> <strong>in</strong> Colombia. Cancer 1989;64:2393–2398.<br />
21. Siegel JH, Janis R, Alper JC, et al. Dissem<strong>in</strong>ated visceral<br />
Kaposi’s <strong>sarcoma</strong>. Appearance after human renal<br />
homograft operation. JAMA 1969;207:1493–1496.<br />
22. Harwood AR, Osoba D, Hofstader SL, et al. Kaposi’s <strong>sarcoma</strong><br />
<strong>in</strong> recipients of renal transplants. Am J Med<br />
1979;67:759–765.<br />
23. Qunibi W, Akhtar M, Sheth K, et al. Kaposi’s <strong>sarcoma</strong>:<br />
<strong>the</strong> most common tumor after renal transplantation <strong>in</strong><br />
Saudi Arabia. Am J Med 1988;84:225–232.<br />
24. Lessan-Pezeshki M, E<strong>in</strong>ollahi B, Khatami MR, et al.<br />
Kidney transplantation <strong>and</strong> Kaposi’s <strong>sarcoma</strong>: review of<br />
2050 recipients. Transplant Proc 2001;33:2818.<br />
25. Penn I. Kaposi’s <strong>sarcoma</strong> <strong>in</strong> transplant recipients. Transplantation<br />
1997;64:669–673.<br />
26. Moosa MR. Racial <strong>and</strong> ethnic variations <strong>in</strong> <strong>in</strong>cidence <strong>and</strong><br />
pattern of malignancies after kidney transplantation.<br />
Medic<strong>in</strong>e (Baltimore) 2005;84:12–22.<br />
27. Penn I. Cancers <strong>in</strong> renal transplant recipients. Adv Ren<br />
Replace Ther 2000;7:147–156.<br />
28. Howl<strong>and</strong> WJ, Armbrecht EC, Miller JA. Oral manifestations<br />
of multiple idiopathic hemorrhagic <strong>sarcoma</strong> of<br />
Kaposi’s: report of two cases. 1966;24:445–449.<br />
29. Pisanty S, Garfunkel A. Kaposi’s <strong>sarcoma</strong>. J Oral Med<br />
1970;25:89–92.<br />
30. Margolius L, Ste<strong>in</strong> M, Spencer D, Bezwoda WR. Kaposi’s<br />
<strong>sarcoma</strong> <strong>in</strong> renal transplant recipients. S Afr Med J<br />
1994;84:16–17.<br />
31. Bowie SA, Bach D. Oral Kaposi’s <strong>sarcoma</strong> <strong>in</strong> a non-<strong>AIDS</strong><br />
patient. Gen Dent 1999;47:413–415.<br />
32. Meyers AD, Barker C, Grossman R, Potsic WP, Jafek<br />
BW. Kaposi’s <strong>sarcoma</strong> of <strong>the</strong> oropharynx follow<strong>in</strong>g renal<br />
transplantation. Trans Sect Otolaryngol Am Acad Ophthalmol<br />
Otolaryngol 1976;82:560–562.<br />
33. Liao CH, Ko JY, Chueh SC, et al. Laryngeal Kaposi’s<br />
<strong>sarcoma</strong> <strong>in</strong> a renal-transplant patient. Transplantation<br />
2003;76:884–885.<br />
34. Wang ALM, Li PKT, To KF, Lai FM, Lai KN. Coexistence<br />
of Kaposi’s <strong>sarcoma</strong> <strong>and</strong> tuberculosis <strong>in</strong> a renal transplant<br />
recipient. Transplantation 1998;66:115–118.<br />
<strong>Non</strong>-<strong>AIDS</strong> Kaposi’s Sarcoma HEAD & NECK—DOI 10.1002/hed February 2009 267
35. Marsman WA, van Gelder T, Mulder AH, Ijzermans<br />
JNM, Zietse R, Weimar W. Successful treatment of<br />
Kaposi’s <strong>sarcoma</strong> <strong>in</strong> a renal allograft recipient. Nephrol<br />
Dial Transplant 1996;10:900–901.<br />
36. Benc<strong>in</strong>i PL, Marchesi L, Ca<strong>in</strong>elli T, Crosti C. Kaposi’s<br />
<strong>sarcoma</strong> <strong>in</strong> kidney transplant recipients treated with cyclospor<strong>in</strong>.<br />
Br J Dermatol 1988;118:709–714.<br />
37. Bollen JM, Polstra AM, van der Kuyl AC, et al. Multicentric<br />
Castleman’s disease <strong>and</strong> Kaposi’s <strong>sarcoma</strong> <strong>in</strong> a<br />
cyclospor<strong>in</strong>-treated, HIV-1 negative patient: case report.<br />
BMC Blood Disord 2003;3:3–8.<br />
38. W<strong>in</strong>dle-Taylor PC, Shah N. Oropharyngeal Kaposi’s <strong>sarcoma</strong>.<br />
Report of two cases <strong>and</strong> review of <strong>the</strong> literature. J<br />
Laryngol Otol 1983:97:1065–1071.<br />
39. Chang Y, Cesarman E, Pess<strong>in</strong> MS, et al. Identification of<br />
herpesvirus-like DNA sequences <strong>in</strong> <strong>AIDS</strong>-associated<br />
Kaposi’s <strong>sarcoma</strong>. Science 1994;266:1865–1869.<br />
40. Huang YQ, Li JJ, Kaplan MH, et al. Human herpesvirus-like<br />
nucleic acid <strong>in</strong> various forms of Kaposi’s <strong>sarcoma</strong>.<br />
Lancet 1995;345:759–761.<br />
41. Moore PS, Chang Y. Detection of herpesvirus-like DNA<br />
sequences <strong>in</strong> Kaposi’s <strong>sarcoma</strong> <strong>in</strong> patients with <strong>and</strong> those<br />
without HIV <strong>in</strong>fection. N Eng J Med 1995;332: 1181–1185.<br />
42. Moore PS, Gao SJ, Dom<strong>in</strong>guez G, et al. Primary characterization<br />
of a herpesvirus agent associated with Kaposi’s<br />
<strong>sarcoma</strong>. J Virol 1996;70:549–558.<br />
43. Kennedy MM, Cooper K, Howells DD, et al. Identification<br />
of HHV8 <strong>in</strong> early Kaposi’s <strong>sarcoma</strong>: implications for<br />
Kaposi’s <strong>sarcoma</strong> pathogenesis. J Cl<strong>in</strong> Pathol: Mol Pathol<br />
1998;51:14–20.<br />
44. Zong JC, Metroka C, Reitz MS, et al. Stra<strong>in</strong> variability<br />
among Kaposi’s <strong>sarcoma</strong>-associated herpes virus (human<br />
herpesvirus 8) genomes: evidence that a large cohort of<br />
United States <strong>AIDS</strong> patients may have been <strong>in</strong>fected by<br />
a s<strong>in</strong>gle common isolate. J Virol 1997;71:2505–2511.<br />
45. Simonart T, Hermans P, Sch<strong>and</strong>ene L, van Vooren JP.<br />
Phenotypic characteristics of Kaposi’s <strong>sarcoma</strong> tumor<br />
cells derived from patch-, plaque- <strong>and</strong> nodular-stage<br />
lesions: analysis of cell cultures isolated from <strong>AIDS</strong> <strong>and</strong><br />
non-<strong>AIDS</strong> patients <strong>and</strong> review of <strong>the</strong> literature. Br J<br />
Dermatol 2000;143:557–563.<br />
46. Courville P, Simon F, le Pessot F, et al. [Detection of<br />
HHV8 latent nuclear antigen by immunohistochemistry.<br />
A new tool for differentiat<strong>in</strong>g Kaposi’s <strong>sarcoma</strong> from its<br />
mimics.] Ann Pathol 2002;22:267–276.<br />
47. Hong A, Davies S, Lee CS. Immunohistochemical detection<br />
of <strong>the</strong> human herpes virus 8 (HHV8) latent nuclear antigen-1<br />
<strong>in</strong> Kaposi’s <strong>sarcoma</strong>. Pathology 2003;35:448–450.<br />
48. Bélec L, Mohamed AS, Authier FJ, et al. Human herpesvirus<br />
8 <strong>in</strong>fection <strong>in</strong> patients with POEMS syndromeassociated<br />
multicentric Castleman’s disease. Blood 1999;93:<br />
3643–3653.<br />
49. Tohda S, Murakami N, Nara N. Human herpesvirus 8<br />
DNA <strong>in</strong> HIV-negative Japanese patients with multicentric<br />
Castleman’s disease <strong>and</strong> related disorders. Int J Mol<br />
Med 2001;8:549–551.<br />
50. Pauk J, Huang ML, Brodie SJ, et al. Mucosal shedd<strong>in</strong>g<br />
of human herpesvirus 8 <strong>in</strong> men. N Engl J Med 2000;343:<br />
1369–1377.<br />
51. Polstra AM, van den Burg R, Goudsmit J, Cornelissen<br />
M. Human herpesvirus 8 load <strong>in</strong> matched serum <strong>and</strong><br />
plasma samples of patients with <strong>AIDS</strong>-associated Kaposi’s<br />
<strong>sarcoma</strong>. J Cl<strong>in</strong> Microbiol 2003;41:5488–5491.<br />
52. Nuovo M, Nuovo G. Utility of HHV8 RNA detection for<br />
differentiat<strong>in</strong>g Kaposi’s <strong>sarcoma</strong> from its mimics. J<br />
Cutan Pathol 2001;28:248–255.<br />
53. Fusetti M, Chitti-Batelli S, Eibenste<strong>in</strong> A, et al. Isolated<br />
oropharyngeal Kaposi’s <strong>sarcoma</strong> <strong>in</strong> non-<strong>AIDS</strong> patient:<br />
differences <strong>and</strong> similarities with sp<strong>in</strong>dle-cell haemangioendo<strong>the</strong>lioma.<br />
J Laryngol Otol 2001;115:330–332.<br />
54. Dup<strong>in</strong> N, Fisher C, Kellam P, et al. Distribution of<br />
human herpesvirus-8 latently <strong>in</strong>fected cells <strong>in</strong> Kaposi’s<br />
<strong>sarcoma</strong>, multicentric Castleman’s disease, <strong>and</strong> primary<br />
effusion lymphoma. Proc Natl Acad Sci U S A 1999;96:<br />
4546–4551.<br />
55. Nador RG, Cesarman E, Chadburn A, et al. Primary<br />
effusion lymphoma: a dist<strong>in</strong>ct cl<strong>in</strong>icopathologic entity<br />
associated with <strong>the</strong> Kaposi’s <strong>sarcoma</strong>-associated herpes<br />
virus. Blood 1988;2:645–656.<br />
56. Shibagaki R, Kishimoto S, Takenaka H, Yasuno H.<br />
Recomb<strong>in</strong>ant <strong>in</strong>terleuk<strong>in</strong> 2 mono<strong>the</strong>rapy for classic Kaposi’s<br />
<strong>sarcoma</strong>. Arch Dermatol 1998;134:1193–1196.<br />
268 <strong>Non</strong>-<strong>AIDS</strong> Kaposi’s Sarcoma HEAD & NECK—DOI 10.1002/hed February 2009