State PIP - STATE HEALTH SOCIETY-----BIHAR
State PIP - STATE HEALTH SOCIETY-----BIHAR
State PIP - STATE HEALTH SOCIETY-----BIHAR

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN<br />
Government of Bihar<br />
NATIONAL RURAL <strong>HEALTH</strong> MISSION<br />
2009-10<br />
February 2009
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
Abbreviations<br />
ANM<br />
ASHA<br />
AWC<br />
AWW<br />
BCC<br />
BPL<br />
BEmOC<br />
CBO<br />
CDR<br />
CEO<br />
CEmOC<br />
CMR<br />
DHS<br />
DPT<br />
GO<br />
GoB<br />
GoI<br />
HIV<br />
ICDS<br />
IEC<br />
IMR<br />
MMR<br />
NFHS I<br />
NFHS II<br />
NFHS III<br />
NGO<br />
O & M<br />
OP<br />
OPD<br />
RCH<br />
PHC<br />
PPP<br />
<strong>PIP</strong><br />
PRI<br />
RKS<br />
SHC<br />
SIHFW<br />
TB<br />
TFR<br />
Auxiliary Nurse Midwife<br />
Accredited Social Health Activist<br />
Aaganwadi Centre<br />
Aaganwadi Worker<br />
Behaviour Change Communication<br />
Population Below Poverty Line<br />
Basic Emergency Obstetric Care<br />
Community Based Organization<br />
Crude Death Rate<br />
Chief Executive Officer<br />
Comprehensive Emergency Obstetric Care<br />
Crude Mortality Rate<br />
Directorate of Health Services<br />
Diphtheria, Pertusis and Tetanus vaccine<br />
Government Order<br />
Government of Bihar<br />
The Government of India<br />
Human Immunodeficiency Virus<br />
Integrated Child Development Services<br />
Information Education Communication<br />
Infant Mortality Rate<br />
Maternal Mortality Rate<br />
National Family Health Survey I<br />
National Family Health Survey II<br />
National Family Health Survey III<br />
Non-Governmental Organizations<br />
Operation and Maintenance<br />
Out-Patient (section or department of a hospital)<br />
Out-Patient Department<br />
Reproductive and Child Health<br />
Primary Health Centre<br />
Public Private Partnership<br />
Program Implementation Plan<br />
Panchayati Raj Institutions<br />
Rogi Kalyan Samiti<br />
Sub Health Centre<br />
<strong>State</strong> Institute of Health & Family Welfare<br />
Tuberculosis<br />
Total Fertility Rate<br />
2
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
Preface<br />
National Rural Health Mission offers unprecedented opportunity to improve the health of<br />
the people of Bihar. The Public Health System of Bihar, through its more than 10000<br />
ANMs, 75000 of ASHAs, 70000 of Aaganwadi Workers and thousands of doctors<br />
reaches out to the people living in more than 80000 villages. The Public Health<br />
infrastructure, particularly PHCs/CHCs and other Government hospitals ought to be the<br />
institutions where people can put their trust for good and affordable quality health<br />
services as per needs.<br />
Though the role of Public Health system is primarily important, NRHM heralds a new<br />
beginning where the health of the people will be placed in their own hands and<br />
government will play a role of facilitator providing all round support and ensuring access<br />
to health services.<br />
The <strong>PIP</strong> has been prepared through consultation with block and district level<br />
functionaries. The plans have been prepared on the needs identified and has addressed<br />
lots of critical issues to implement the programme.<br />
The plan is aimed at improving the access to comprehensive quality health care by<br />
improving the public health infrastructure to desired standards and placing the health of<br />
the people in their hands. Government will play the role of a facilitator and undertake<br />
new initiatives.<br />
As planned here the capacity to manage the programme in the state is going to be<br />
significantly strengthened. The Programme Management Support Units at the block level,<br />
HMIS and the support systems shall also be strengthened. This year also a number of PPP<br />
initiatives is taken to reach out services to the people through varied channels.<br />
It is expected that for the state of Bihar, this will be the turning point for accelerated<br />
improvement in health.<br />
3
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
Table of Contents<br />
Chapter Content Page No.<br />
Preface 3<br />
1 Executive Summary 9-11<br />
2 Process of Plan Preparation 12<br />
3. Background and Current Status<br />
3.1 Demographic and Socio-Economic Features at <strong>State</strong> and District 12-16<br />
Levels<br />
3.2 Administrative Divisions 17-20<br />
3.3 RCH Outcome and Service Utilization 20-23<br />
3.4 Public Health Infrastructure 24-25<br />
3.5 Private and NGO Health Service 26<br />
3.6 Donor Assisted Programme in the <strong>State</strong> 26-27<br />
3.7 Institutional Arrangements and Organizational Development 27<br />
3.8 Program Finance 27<br />
Part A Reproductive & Child Health-II<br />
4 Situation Analysis<br />
4.1 Maternal Health 29-30<br />
4.2 Child Health 30-31<br />
4.3 Family Planning 31-33<br />
4.4 Adolescent Health 33-36<br />
4.5 District/Sub District Variations 36-39<br />
4.6 Health Infrastructure and Facilities 40-45<br />
4.7 Human Resource Development including Training 45-46<br />
4.8 Inequity/ Gender; Vulnerable Groups Including Urban Slums &<br />
Tribal<br />
4.8.1 Inequity and Gender 46-47<br />
4.8.2 Urban Slums 47<br />
4.9 Logistics 47-48<br />
4.10 HMIS and Monitoring & Evaluation 48-49<br />
4.11 Behaviour Change Communication 49<br />
4.12 Convergence/Coordination 49-50<br />
4.13 Finance 50<br />
5 Progress and Lessons learnt from RCH II Implementation of 05-<br />
4
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
08<br />
5.1 Major achievement during 2005-08 51-52<br />
5.2 Programme Management 52-53<br />
6 RCH II PROGRAMME OBJECTIVES AND STRATEGIES<br />
6.1 Vision <strong>State</strong>ment 54<br />
6.2 Technical Objectives, Strategies and Activities<br />
1 Maternal Health 55-61<br />
2 Child Health 61-70<br />
3 Family Planning 71-77<br />
4 Adolescent Reproductive and Sexual Health 78-81<br />
5 Urban Health 81-83<br />
6 Vulnerable Groups (Health Camps in Maha Dalit Tola) 84<br />
7 Tribal Health 84<br />
8 Innovations<br />
8.1 PNDT Act 85<br />
8.2 Muskaan Programme 86-87<br />
9 Strengthening of SIHFW 88<br />
9.1 Fast Track Training Cell in SIHFW 88<br />
9.2 Filling Vacant Position at SIHFW/Hiring Consultant at SIHFW 88<br />
10 Infrastructure and Human Resource 89<br />
11 Institutional Strengthening 90-92<br />
12 Training 93-97<br />
13 IEC/BCC 98-107<br />
14 Procurement of Equipments/ Instruments and Drugs/Supplies 108-109<br />
16. Programme Management 110-120<br />
17. Convergence and Coordination 121<br />
18. Role of <strong>State</strong>, District & Blocks 121<br />
19. Monitoring and Evaluation 121-126<br />
20. Synergie with NRHM Additionalities 127<br />
21. Sustainability 128<br />
22. Extra inclusions in RCH 129-130<br />
23. Work Plan (Annexure - 3d) 131<br />
24. Budget (Annexure- 3c & 3e) 131<br />
Part B NRHM Additionalities<br />
1. Decentralisation 133<br />
5
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
1.0 ASHA 134-145<br />
1.1 Untied Funds for Health Sub-Centre, APHC & PHCs 146<br />
1.2 Village Health & Sanitation Committee 147<br />
1.3 Seed Money for Rogi Kalyan Samiti 147-148<br />
2. Infrastructure Development<br />
2.1 Construction or establishment of Health Sub-Centre 149<br />
2.2 Construction of PHC 150<br />
2.3 Upgradation of Community Health Centre (CHC) 151<br />
2.4 Infrastructure & Service Improvement as per IPHS in 48 (District 152<br />
& Sub-Divisional) Hospitals for<br />
accreditation/ISO 9000 Certification of Health<br />
facilities<br />
2.5 Upgradation of Infrastructure of ANM Training Schools 152-154<br />
2.6 Annual Maintenance Grant 154<br />
3. Contractual Manpower<br />
3.1 Incentive, Contractual Salaries and Bonus 154-155<br />
3.2 Block Programme Management Unit 155-156<br />
3.3 Additional Manpower for <strong>State</strong> Health Society Bihar 156-157<br />
3.4 Additional Manpower under NRHM 157<br />
4. PPP Initiative in <strong>State</strong><br />
4.1 102- Ambulance Service 158<br />
4.2 Dial 1911 - Doctor on Call & Samadhan 158-159<br />
4.3 Additional PHCs Management by NGOs 159<br />
4.4 AAPIO 160<br />
4.5 <strong>State</strong> Health Resource Centre 160<br />
4.6 Services of Hospital waste treatment and Disposal in all 160-162<br />
Government Health facilities upto PHCs in Bihar<br />
(IMEP)<br />
4.7 Dialysis Unit in Government Hospital of Bihar 162-163<br />
4.8 Setting up of Ultra Modern Diagnostic Centre in RDCs and all 163-164<br />
Government Medical College Hospitals<br />
4.9 Providing Telemedicine Services in Government Health facilities 165-168<br />
4.10 Outsourcing Pathology & Radiology Services from PHCs to 168-169<br />
District Hospital<br />
4.11 Operationalising Mobile Medical Unit 169-171<br />
6
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
4.14 Monitoring and Evaluation 171-172<br />
4.15 Generic Drug Shop 173<br />
4.16 Nutrition Rehabilitation Centres (NRCs) for Treatment of sever 173-174<br />
and acute malnutrition<br />
4.17 Hospital Maintenance 174<br />
4.18 Providing Ward Management Services in Govt. Hospitals 175<br />
4.19 Provision of HR Consultancy Services 175-176<br />
4.20 Advanced Life Saving Ambulances (ALS) 176<br />
7. Mobilisation and Management support for Disaster Management 177-178<br />
8. Health Management Information System (HIMS) 178-181<br />
9. Strengthening of Cold Chain 182-183<br />
12 Main streaming AYUSH under NRHM 183-187<br />
Summary Budget of NRHM Part- B 188-190<br />
Part C Immunization<br />
1 Routine Immunization 191-225<br />
Part D National Disease Control Programmes<br />
1 IDSP 227-229<br />
2 IDD 230-236<br />
3 NPCB 237-251<br />
4 NLEP 252-285<br />
5 TB 287-319<br />
NVBDCP<br />
5 Kalazar 321-351<br />
6 Malaria 352-364<br />
7 Dengu & Chikungunya 366-368<br />
8. JE 369-371<br />
9. Filaria 372-380<br />
Part E Intersectoral Convergence<br />
1 Intersectoral Convergence 382-392<br />
BUDGET<br />
1 NRHM Part A RCH II 393<br />
2 NRHM Part B - Additionalities 394-396<br />
3 NRHM Part C - Immunization 397<br />
4 NRHM Part D NDCP 397<br />
5 NRHM Part E - Convergence 397<br />
7
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
6 Summary of Budget 398<br />
Annexures<br />
Annexure 3a Self Appraisal of <strong>State</strong> <strong>PIP</strong> against Appraisal Criteria<br />
Annexure 3b Targets for goals, outcomes, outputs and inputs<br />
Annexure 3d Work plan RCH<br />
Annexure 3e Details of Budget of RCH- II (Part-A)<br />
Annexure 4 IMNCI<br />
Annexure 5 IFA<br />
Annexure 6 IUD Training<br />
Annexure 7 MTP Training<br />
Annexure 8 CTP (Comprehensive Training Programme)<br />
Annexure 9<br />
Annexure 10<br />
Annexure 11<br />
Annexure 12<br />
Annexure 13<br />
Annexure 14<br />
Annexure 15<br />
Annexure 16<br />
Annexure 17<br />
Annexure 18<br />
Annexure 19<br />
Annexure 20<br />
Annexure 21<br />
Pilot Health Financing Scheme for Safe Maternity to BPL/SC/ST beneficiaries in<br />
accredited private facilities<br />
Incentive for Cesarean Section, Pregnancy testing, Safe Abortion & IUCD in<br />
Bihar<br />
Procurement<br />
School Health<br />
List of 27x7<br />
Pregency Kit<br />
MAPEDIR<br />
Training Details<br />
Mahadalit Tola Report<br />
IEC Budget Breakup<br />
NSV Kit<br />
Minilap Set<br />
FRU Report<br />
8
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
Executive Summary Chapter 1<br />
Executive Summary<br />
Introduction<br />
The <strong>State</strong> Health Society, Government of Bihar is committed towards promoting the right of<br />
every woman, man and child to enjoy a life of health and equal opportunity and is making all<br />
round efforts in this direction. SHSB under the aegis of Department has taken steps to bring about<br />
outcomes as envisioned in the Millennium Development goals, RCH II / NRHM programme and<br />
Vision 2010 Bihar. It aims at minimizing regional variations in the areas of Reproductive and<br />
Child Health including population stabilization through an integrated, focused and participatory<br />
programme. Meeting unmet demands of the target population, and provision of assured,<br />
equitable, responsive quality services are central to the programme strategies. Based on<br />
experience gained during the implementation of RCH II, the Department anticipates that current<br />
RCH programme implementation would produce equitable reproductive and child health<br />
outcomes and contribute to raising the status of the girl child.<br />
The Goal<br />
The goal is to improve quality of life of the people by:<br />
(Goals mentioned below are for the period of RCH-II i.e. to be achieved by 2010)<br />
ê reducing Maternal Mortality Ratio (MMR) from 371 to 100 per 1,00,000 live births,<br />
ê reducing Infant Mortality Rate (IMR) from 61 to 30 per 1000 live births,<br />
ê Reducing Total Fertility Rate (TFR) 1 from 4.3 to 2.1 for population stabilization with<br />
enhanced satisfaction of clients with medical services.<br />
The Department is making all out efforts to reduce the IMR and has initiated an innovative program<br />
‘MUSKAAN’ for the same cause and so as to also reach the poorest of the poor with effective,<br />
quality and equitable health services. Simultaneously taking steps to effectively implement national<br />
health programme while creating synergy and convergence with RCH II.<br />
1 NFHS-3<br />
9
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
Status and Situation<br />
Important RCH indicators such as MMR, IMR and TFR are showing declining trends whereas<br />
institutional deliveries, complete ANC, contraceptive use in the state has increased. The state has<br />
mapped poorly performing districts and is now extensively focusing on them.<br />
Status of Important RCH indicators in the state are as follows:<br />
Declined<br />
ê MMR has declined from 389 (1998) to 371 (SRS 2003-05)<br />
ê IMR has declined from 63 (Census 2001) to 61 per 1000 live births (SRS 2006-07)<br />
ê Total Fertility Rate (TFR) has decreased from 4.3 to 4.0 (NFHS III 2005-06) to 3.9 (SRS 8)<br />
ê Percentage of children under age 3 who are underweight has marginally declined from 48<br />
percent to 47 percent.<br />
Increased<br />
é Institutional deliveries have increased from 12.1 (NFHS-I 1992-93) percent to 22 percent<br />
(NFHS-III 2005-06) to 27.7 percent (DLHS-III 2007-08)<br />
é Antenatal Care has increased from 15.9 percent (NFHS-II 1998-99) to 16.9 percent (NFHS-<br />
III) to 45% (DLHS-III 2007-08)<br />
é % Full Immunization coverage has increased from 10.7 (NFHS-I 1992-93) percent to 41.4<br />
percent (DLHS-III 2007-08)<br />
é Contraceptive use has increased from 23.1 percent (NFHS-I 1992-93) to 34.1 percent (NFHS-<br />
III)<br />
é Sex ratio from 825 to 871 (CRS 2006-07)<br />
Strategic Direction<br />
The entire <strong>State</strong> Health Society Bihar team is working in a mission mode to achieve goals set-in<br />
for the state and is effectively dealing with the challenges. The Department has set the strategic<br />
direction that encompasses year wise objectives, technical strategies; interventions include<br />
program and services for improving maternal health, child health, family planning, adolescents'<br />
health etc. The complete programme has been bifurcated into institutional and cross cutting<br />
programme strategies as well as specific core programmatic strategies for taking effective actions.<br />
These institutional and cross cutting strategies have impact on all the components of RCH viz.<br />
maternal health, child health, family planning, adolescent health etc whereas specific core<br />
programme strategies have wider impact on the specific programme component. It has been<br />
recognized that all these strategies should converge and go hand-in-hand to achieve the<br />
programme outcome. The state considers that strengthening institutional mechanisms,<br />
infrastructural development, ensuring adequately trained human resources etc. are fundamental<br />
requirements for getting better programme outcomes. Accordingly, the document is presented with<br />
backward linkages from core programme strategies to institutional framework. Convergence of<br />
strategies and progress is as described below:<br />
i) Core Programme Strategies<br />
‣ Special schemes such as Muskaan, MAMTA addressing child health, incentives to health staff.<br />
ii) Cross Cutting Programmatic Strategies<br />
‣ Capacity building, PPP, quality assurance, gender mainstreaming, community participation,<br />
serving vulnerable community through mobile units etc. Resource planning for all the sectors<br />
will be also done.<br />
iii) Strengthening Institutional Framework and Governance Mechanisms<br />
‣ Recruitment and placement of qualified human resource<br />
‣ Structures: Functional, accountable <strong>State</strong>/District Health Mission with Governing and<br />
Executive Board; Integrated Organizational Structure of Department of Health; Functional<br />
10
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
SPMU, DPMU, BPMU; Constitution of RKS and Village Health and Sanitation Committee<br />
for bringing in transparency and accountability by involving the community.<br />
‣ Infrastructure Development and ensuring consistent logistics support.<br />
Strategies RCH Components Goals<br />
Maternal Health<br />
Reduction in MMR<br />
Institutional framework<br />
and Governance<br />
mechanism<br />
Cross Cutting<br />
Strategies<br />
Core Programme<br />
Strategies<br />
Child Health<br />
Family Planning<br />
Adolescent Health<br />
Vulnerable<br />
Community<br />
Reduction in IMR<br />
Reduction in TFR<br />
Services to each<br />
adolescent<br />
Ensuring equitable<br />
healthcare delivery<br />
SUMMARY of BUDGET<br />
PART<br />
HEAD<br />
BUDGET 2009-10<br />
(Rs. In lakhs)<br />
In Cr.<br />
%<br />
A RCH II 48495.00 484.95 37.89<br />
B NRHM Additionalities 43568.00 435.68 34.04<br />
C Immunization 3193.08 31.93 2.49<br />
D NDCP 7,133.84 71.34 5.57<br />
E Intersectoral Convergence 2172.70 21.72 1.70<br />
TOTAL 104562.62 1045.62 81.70<br />
PPI Operational Cost 76.97 6.01<br />
Infrastructure Maintenance<br />
(Treasury Fund) 157.22 12.28<br />
GRANT TOTAL 1279.81 100.00<br />
11
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
Process of Plan Preparation Chapter 2<br />
Information collected from the District and Block level is the key in preparing the <strong>State</strong><br />
<strong>PIP</strong>. At the block level, consultation was done which was further sent to the District. With<br />
the information gathered from the block, district has further held consultations and<br />
prepared their priorities and requirements, which are being reflected in the District Health<br />
Action Plans, still being prepared in the districts.<br />
The method of data collection is both primary and secondary in the preparation of the<br />
Plan. The secondary data were collected by reviewing records, registers and annual<br />
reports. The data were also collected from DLHS, SRS and NFHS surveys to support<br />
the background information. For primary data, the procedure involved focus group<br />
discussions, interactions and meetings in different districts. This was done to have<br />
opinion of all the programme officers, health staff, grass root workers and private<br />
partners.<br />
Based on the feedback received from the districts state programme officers have<br />
discussed and finalized the S<strong>PIP</strong> requirements. The state has considered the<br />
requirement of the district thoroughly and provision has been made in the <strong>PIP</strong> as per<br />
their need.<br />
The SPMU team was thoroughly involved in the process and their critical inputs were<br />
incorporated to make this plan more holistic, realistic and achievable. The Plan was<br />
further reviewed by the Executive Director, SHSB and the CEO-cum-Secretary, Health,<br />
Deptt.of Health, Govt. of Bihar.<br />
It should be mentioned that the plan has been prepared keeping in mind that private<br />
party can simultaneously complement the role of the Government machinery in<br />
delivering the health care services in the state.<br />
12
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
Background & Current Status Chapter 3<br />
3.1 Demographic and Socio-Economic Features at <strong>State</strong> and District Levels<br />
Bihar with a population of 82.9 million is the second most populous state in India, next only to<br />
Uttar Pradesh. Despite efforts in the last few decades to stabilise population growth, the states<br />
population continues to grow at a much faster rate (28.43%) than the national population<br />
(21.34%). The state is densely populated with 880 persons per square kilometre as against the<br />
country average of 324.The sex ratio of the state at 919 is also less favourable than the national<br />
average of 933.<br />
Table 3.1.1: Bihar: Demographic, Socio-Economic and Health Indices<br />
Characteristics Bihar India<br />
Area<br />
94,163 Sq. Km<br />
Demographic Indicators<br />
Population 828.8 Million 1027.0 Million<br />
Population Density (Population / km2) 880 324<br />
Sex Ratio 919 933<br />
% decadal growth rate 28.43% 21.34%<br />
Socio-Economic Indicators<br />
Per Capita Income (Rs.) for year 2003-04<br />
At constant1993-94 prices 3707 10964<br />
At current prices 6861 20292<br />
% decadal growth in Per capita Income ~ zero ~ 45%<br />
Proportion of population below poverty line 42% 26%<br />
Level of Urbanization 10.5% 27.8%<br />
Literacy 47.5% 65.4%<br />
Source: Census 2001, Ministry of Statistics and Program Implementation<br />
Among the 38 districts of the state, West Champaran is the largest in terms of area (5228.00 sq.<br />
km) while the smallest is Sheikhpura (605.96 sq. km). In terms of population, Patna is the largest<br />
at 4.72 millions followed by East Champaran that has a population of 3.94 millions. Sheohar and<br />
Sheikhpura have the smallest population of 0.52 millions and 0.53 millions respectively. In terms<br />
of Sex Ratio, while districts such as Siwan (1031) and Gopalganj (1001) have a favourable ratio,<br />
other districts like Munger (872), Patna (873) and Bhagalpur (876) have a less favourable ratio.<br />
13
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
Bihar has a total SC population of around 15.07%. However, SC population in certain districts<br />
like Gaya (29.6%) and Nawada (24.1%) is much higher than the state average. On the other hand,<br />
districts such as Kishanganj (6.6%) and Arwal (8.9%) have a relatively low proportion of SC<br />
population. After the bifurcation of the state in 2002, most of the areas with large ST population<br />
have been included in the state of Jharkhand. Therefore, the state has less than 1% ST population.<br />
In terms of key health indicators, Bihar is among the low performing states. Though the state<br />
fares reasonably well in terms of its Infant Mortality Rate (61) as against the national average<br />
(58), it continues to be among the poorer performing states in terms of other indicators such as<br />
TFR, MMR and NMR.<br />
In terms of socio-economic indices too the district level variation is obvious. For literacy rates,<br />
districts such as Arwal (26%), Jehanabad (29.3%), Kishanganj (31.1%), Araria (35%) and<br />
Katihar (35.1%) are much below the even state average of 46.4%. However, there are districts -<br />
Aurangabad (57%), Bhojpur (59%), Munger (59.5%), Patna (62.9%) and Rohtas (61.3%) -that<br />
have performed better than the state average with literacy rates close to 60%. Similarly<br />
performance of districts on percentage of people living below the poverty line is varied with<br />
districts such as Araria faring the worst at 80.3%. Other poor performing districts are Bhagalpur,<br />
Madhubani, Purnea, Sitamarhi, Supaul and Sheohar, where close to 70% of the population<br />
continues to live below the poverty line. Despite such a large number of districts having a<br />
significant proportion of their population living below poverty line, the state average of 46.2%<br />
(among the lowest in the country) is largely due to the fact that there are some districts such as<br />
Kaimur, Saharsa, Samastipur, Arwal, Jehanabad and Gopalganj where close to 80% of the<br />
population are living above the poverty line. (See table 2.1.2 for district-wise detailed data).<br />
14
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
Table 2.1.2: Bihar: Key Demographic and Socio-economic Indicators of Districts<br />
Sl No Districts<br />
Area in Sq. Population<br />
BPL SC ST Sex Literacy<br />
Km Rural Urban Total (%) (%) (%) Ratio Rates<br />
1 2 3 4 5 6 7 8 9 10 11<br />
1 Araria 2830.00 2026257 132351 2158608 80.3 13.6 1.4 913 35.0<br />
2 Aurangabad 3305.00 1842998 170057 2013055 61.7 23.5 0.1 934 57.0<br />
3 Arwal 761.12 659270 52458 711728 23.36 8.9 0.05 929 26.0<br />
4 Banka 3019.56 1552353 56420 1608773 63.4 12.4 4.7 908 42.7<br />
5 Begusarai 1918.00 2241743 107623 2349366 65.4 14.5 0.1 912 48.0<br />
6 Bhagalpur 2569.44 1970745 452427 2423172 70.2 10.5 2.3 876 49.5<br />
7 Bhojpur 2474.17 1930730 312414 2243144 55.3 15.3 0.4 902 59.0<br />
8 Buxar 1623.83 1273422 128974 1402396 46.6 14.1 0.6 899 56.8<br />
9 Champaran (E) 3968.00 3688687 251086 3939773 54.1 13.0 0.1 897 37.5<br />
10 Champaran (W) 5228.00 2733907 309559 3043466 47.4 14.3 1.5 901 38.9<br />
11 Darbhanga 2279.00 3028441 267348 3295789 60.0 15.5 0.0 914 44.3<br />
12 Gaya 4976.00 2997479 475949 3473428 69.8 29.6 0.1 938 50.4<br />
13 Gopalganj 2033.00 2022048 130590 2152638 37.6 12.4 0.3 1001 47.5<br />
14 Jehanabad 807.88 743433 59154 802587 26.34 10.0 0.05 929 29.3<br />
15 Jamui 3098.27 1295552 103244 1398796 63.4 17.4 4.8 918 42.4<br />
16 Kaimur 3361.90 1247299 41775 1289074 15.4 22.2 2.8 902 55.1<br />
17 Katihar 3057.00 2174361 218277 2392638 49.1 8.7 5.9 919 35.1<br />
18 Khagaria 1486.00 1204027 76327 1280354 48.8 14.5 0.0 885 41.3<br />
19 Kishanganj 1884.00 1167340 129008 1296348 58.0 6.6 3.6 936 31.1<br />
20 Lakhisarai 1299.01 684485 117740 802225 62.3 15.8 0.7 921 48.0<br />
15
<strong>State</strong> <strong>PIP</strong>, Bihar 2008-09<br />
National Rural Health Mission<br />
Sl.No.<br />
Districts<br />
Area<br />
sq.k.m<br />
in<br />
Population<br />
Rural Urban Total<br />
BPL (%) SC (%)<br />
ST<br />
(%)<br />
Sex<br />
Ratio<br />
Literacy Rate<br />
1 2 3 4 5 6 7 8 9 10 11<br />
21 Madhepura 1788.00 1458679 67967 1526646 55.4 17.1 0.6 915 36.1<br />
22 Madhubani 3501.00 3450736 124545 3575281 72.4 13.5 0 942 42.0<br />
23 Munger 1418.76 819950 317847 1137797 53.0 13.3 1.6 872 59.5<br />
24 Muzaffarpur 3372.00 3398361 348353 3746714 55.9 15.9 0.1 920 48.0<br />
25 Nalanda 2367.00 2016899 353629 2370528 53.8 20.0 0.0 914 53.2<br />
26 Nawada 2494.00 1671253 138443 1809696 62.0 24.1 0.1 946 46.8<br />
27 Patna 3202.00 2757060 1961532 4718592 48.1 15.5 0.2 873 62.9<br />
28 Purnia 3229.00 2321544 222398 2543942 70.0 12.3 4.4 915 35.1<br />
29 Rohtas 3851.10 2123942 326806 2450748 56.8 18.1 1.0 909 61.3<br />
30 Saharsa 1701.65 1383015 125167 1508182 14.2 16.1 0.3 910 39.1<br />
31 Samastipur 2904.0 3271338 123455 3394793 19.5 18.5 0.1 928 45.1<br />
32 Saran 2641.0 2950064 298637 3248701 54.1 12.0 0.2 966 51.8<br />
33 Sheikhpura 605.96 444189 81313 525502 59.5 19.7 0.0 918 48.6<br />
34 Sheohar 442.99 494699 21262 515961 69.8 14.4 0.0 885 35.3<br />
35 Sitamarhi 2200.01 2529407 153313 2682720 67.1 11.8 0.1 892 38.5<br />
36 Siwan 2219.0 2564860 149489 2714349 51.0 11.4 0.5 1031 51.6<br />
37 Supaul 2410.35 1644370 88208 1732578 74.6 14.8 0.3 920 37.3<br />
38 Vaishali 2036.00 2531766 186655 2718421 41.1 20.7 0.1 920 50.5<br />
<strong>State</strong> Total 94363.00 74316709 8681800 82998509 46.2 15.07 0.9 919 46.4<br />
16
3.2 Administrative Divisions<br />
Bound by Uttar Pradesh in the west, West Bengal on the east, Nepal on the north and Jharkhand<br />
on the south, Bihar covers an area of 94,363 square kilometers. The state has 38 districts divided<br />
into 9 administrative divisions. The number of districts in each division is detailed below -<br />
Table 3.2.1: Administrative Divisions<br />
Sl . Divisions Districts<br />
1 Patna Patna, Nalanda, Bhojpur, Rohtas, Kaimur, Buxar<br />
2 Magadh Gaya, Jehanabad, Arwal, Aurangabad, Nawada<br />
3 Tirhut Muzaffarpur, Sitamarhi, Vaishali, Champaran East, Champaran West, Sheohar<br />
4 Saran Saran, Siwan, Gopalganj<br />
5 Darbhanga Darbhanga, Madhubani, Samastipur<br />
6 Munger Begusarai, Jamui, Khagaria, Lakhisarai,Munger, Sheikhpura<br />
7 Kosi Saharsa, Madhepura, Supaul<br />
8 Bhagalpur Bhagalpur, Banka<br />
9 Purnea Purnia, Araria, Kishanganj, Katihar<br />
In addition, the state has 101 sub-divisions, 534 community development blocks, 9 urban<br />
agglomerations, 130 towns (125 statutory towns and 5 non-statutory census towns) and 37,741<br />
villages.<br />
Table 3.2.2: Community Development Blocks<br />
Sl.<br />
Districts<br />
Community Development Blocks<br />
Total<br />
Block Name<br />
1 Araria 9 Narpatganj, Forbesganj, Bhargama, Raniganj, Araria, Kursakatta, Sikti,<br />
Palasi, Jokihat<br />
2 Arwal 3 Karpi, Kurtha, Makhdumpur<br />
3 Aurangabad 11 Daudnagar, Haspura, Goh, Rafiganj, Obra, Aurangabad, Barun,<br />
Nabinagar, Kutumba, Deo, Madanpur<br />
4 Banka 11 Shambhuganj, Amarpur, Rajaun, Dhuraiya, Barahat, Banka, Phulidumar,<br />
Belhar, Chanan, Katoria, Bausi<br />
5 Begusarai 18 Khudabandpur, Chhorahi, Garhpura, Cheria Bariarpur, Bhagwanpur,<br />
Mansurchak, Bachhwara, Teghra, Barauni, Birpur, Begusarai, Naokothi,<br />
Bakhri, Dandari, Sahebpur Kamal, Balia, Matihani, Shamho Akha<br />
Kurha<br />
6 Bhagalpur 16 Narayanpur, Bihpur, Kharik, Naugachhia, Rangra Chowk, Gopalpur,<br />
Pirpainti, Colgong, Ismailpur, Sabour, Nathnagar, Sultanganj, Shahkund,<br />
Goradih, Jagdishpur, Sonhaula
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
7 Bhojpur 14 Shahpur, Arrah, Barhara, Koilwar, Sandesh, Udwant Nagar, Behea,<br />
Jagdishpur, Piro, Charpokhari, Garhani, Agiaon, Tarari, Sahar<br />
8 Buxar 11 Simri, Chakki, Barhampur, Chaugain, Kesath, Dumraon, Buxar, Chausa,<br />
Rajpur, Itarhi, Nawanagar<br />
9 E. Champaran 27 Raxaul, Adapur, Ramgarhwa, Sugauli, Banjaria, Narkatia, Bankatwa,<br />
Ghorasahan, Dhaka, Chiraia, Motihari, Turkaulia, Harsidhi, Paharpur,<br />
Areraj, Sangrampur, Kesaria, Kalyanpur, Kotwa, Piprakothi,<br />
Chakia(Pipra), Pakri Dayal, Patahi, Phenhara, Madhuban, Tetaria, Mehsi<br />
10 Champaran W 18 Sidhaw, Ramnagar, Gaunaha, Mainatanr, Narkatiaganj, Lauriya,<br />
Bagaha, Piprasi, Madhubani, Bhitaha, Thakrahan, Jogapatti, Chanpatia,<br />
Sikta, Majhaulia, Bettiah, Bairia, Nautan<br />
11 Dharbhanga 18 Jale, Singhwara, Keotiranway, Darbhanga, Manigachhi, Tardih,<br />
Alinagar, Benipur, Bahadurpur, Hanumannagar, Hayaghat, Baheri,<br />
Biraul, Ghanshyampur, Kiratpur, Gora Bauram, Kusheshwar Asthan,<br />
Kusheshwar Asthan Purbi<br />
12 Gaya 24 Konch, Tikari, Belaganj, Khizirsarai, Neem Chak Bathani, Muhra, Atri,<br />
Manpur, Gaya Town CD Block, Paraiya, Guraru, Gurua, Amas, Banke<br />
Bazar, Imamganj, Dumaria, Sherghati, Dobhi, Bodh Gaya, Tan Kuppa,<br />
Wazirganj, Fatehpur, Mohanpur, Barachatti<br />
13 Gopalganj 14 Katiya, Bijaipur, Bhorey, Pach Deuri, Kuchaikote, phulwaria, Hathua,<br />
Uchkagaon, Thawe, Gopalganj, Manjha, Barauli, Sidhwalia,<br />
Baikunthpur<br />
14 Jahanabad 12 Arwal, Kaler, Sonbhadra Banshi Suryapur, Ratni Faridpur, Jehanabad,<br />
Kako, Modanganj, Ghoshi, Hulasganj<br />
15 Jamui 10 Islamnagar Aliganj, Sikandra, Jamui, Barhat, Lakshmipur, Jhajha,<br />
Gidhaur, Khaira, Sono, Chakai<br />
16 Kaimur 11 Ramgarh, Nuaon, Kudra, Mohania, Durgawati, Chand, Chainpur,<br />
Bhabua, Rampur, Bhagwanpur, Adhaura<br />
17 Katihar 16 Falka, Korha, Hasanganj, Kadwa, Balrampur, Barsoi, Azamnagar,<br />
18 Khagaria<br />
Pranpur, Dandkhora, katihar, Mansahi, Barari, Sameli, Kursela,<br />
Manihari, Amdabad<br />
7 Alauli, Khagaria, Mansi, Chautham, Beldaur, Gogri, Parbatta<br />
18
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
19 Kishanganj 7 Terhagachh, Dighalbank, Thakurganj, Pothia, Bahadurganj,<br />
Kochadhamin, Kishanganj<br />
20 Lakhisarai 6 Barahiya, Pipariya, Surajgarha, Lakhisarai, Ramgarh Chowk, Halsi<br />
21 Madhubani 21 Madhwapur, Harlakhi, Basopatti, Jainagar, Ladania, Laukaha, Laukahi,<br />
Phulparas, Babubarhi, Khajauli, Kaluahi, Benipatti, Bisfi, Madhubani,<br />
Pandaul, Rajnagar, Andhratharhi, Jhanjharpur, Ghoghardiha, Lakhnaur,<br />
Madhepur<br />
22 Madhepura 13 Gamharia, Singheshwar, Ghailarh, Madhepura, Shankarpur,<br />
Kumarkhand, Murliganj, Gwalpara, Bihariganj, Kishanganj, Puraini,<br />
Alamnagar, Chausa<br />
23 Munger 9 Munger, Bariarpur, Jamalpur, Dharhara, Kharagpur, Asarganj, Tarapur,<br />
Tetiha Bambor, Sangrampur<br />
24 Muzaffarpur 17 Sahebganj, Baruraj (Motipur), Paroo, Saraiya, Marwan, Kanti, Minapur,<br />
Bochaha, Aurai, Katra, Gaighat, Bandra, Dholi (Moraul), Musahari,<br />
Kurhani, Sakra<br />
25 Nalanda 20 Karai Parsurai, Nagar Nausa, Harnaut, Chandi, Rahui, Bind, Sarmera,<br />
Asthawan, Bihar, Noorsarai, Tharthari, Parbalpur, Hilsa, Ekangarsarai,<br />
Islampur, Ben, Rajgir, Silao, Giriak, Katrisarai<br />
26 Nawada 14 Nardiganj, Nawada, Warisaliganj, Kashi Chak, Pakribarawan, Kawakol,<br />
Roh, Gobindpur, Akbarpur, Hisua, Narhat, Meskaur, Sirdala, Rajauli<br />
27 Patna 23 Maner, Dinapur-Cum-Khagaul, Patna Rural, Sampatchak, Phulwari,<br />
Bihta, Naubatpur, Bikram, Dulhin Bazar, Paliganj, Masaurhi, Dhanarua,<br />
Punpun, Fatwah, Daniawan, Khusrupur, Bakhtiarpur, Athmalgola,<br />
Belchhi, Barh, Pandarak, Ghoswari, Mokameh<br />
28 Purnia 14 Banmankhi, Barhara, Bhawanipur, Rupauli, Dhamdaha, Krityanand<br />
Nagar, Purnia East, Kasba, Srinagar, Jalalgarh, Amour, Baisa, Baisi,<br />
Dagarua<br />
29 Rohtas 19 Kochas, Dinara, Dawath, Suryapura, Bikramganj, Karakat, Nasriganj,<br />
Rajpur, Sanjhauli, Nokha, Kargahar, Chenari, Nauhatta, Sheosagar,<br />
Sasaram, Akorhi Gola, Dehri, Tilouthu, Rohtas<br />
30 Saharsa 10 Nauhatta, Satar Kataiya, Mahishi, Kahara, Saur Bazar, Patarghat,<br />
Sonbarsa, Simri Bakhtiarpur, Salkhua, Banma Itahri<br />
19
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
31 Samastipur 20 Kalyanpur, Warisnagar, Shivaji Nagar, Khanpur, Samastipur, Pusa,<br />
Tajpur, Morwa, Patori, Mohanpur, Mohiuddinagar, Sarairanjan,<br />
Vidyapati Nagar, Dalsinghsarai, Ujiarpur, Bibhutpur, Rosera, Singhia,<br />
Hasanpur, Bithan<br />
32 Saran 21 Mashrakh, Panapur, Taraiya, Ishupur, Baniapur, Lahladpur, Ekma,<br />
Manjhi, Jalalpur, Revelganj, Chapra, Nagra, Marhaura, Amnour, Maker,<br />
Parsa, Dariapur, Garkha, Dighwara, Sonepur<br />
33 Sheikhpura 6 Barbigha, Shekhopur Sarai, Sheikhpura, Ghat Kusumbha, Chewara,<br />
Ariari<br />
34 Sitamarhi 17 Bairgania, Suppi, Majorganj, Sonbarsa, Parihar, Sursand, Bathnaha,<br />
Riga, Parsauni, Belsand, Runisaidpur, Dumra, Bajpatti, Charaut, Pupri,<br />
Nanpur, Bokhara<br />
35 Sheohar 5 Purnahiya, Piprarhi, Sheohar, Dumri Katsari, Tariani Chowk<br />
36 Siwan 19 Nautan, Siwan, Barharia, Goriakothi, Lakri Nabiganj, Basantpur,<br />
Bhagwanpur Hat, Maharajganj, Pachrukhi, Hussainganj, Ziradei,<br />
Mairwa, Guthani, Darauli, Andar, Raghunathpur, Hasanpura,<br />
Daraundha, Siswan<br />
37 Supaul 11 Nirmali, Basantpur, Chhatapur, Pratapganj, Raghopur, Saraigarh,<br />
Bhaptiyahi, Kishanpur, Marauna, Supaul, Pipra, Tribeniganj<br />
38 Vaishali 16 Vaishali, Paterhi Belsar, Lalganj, Bhagwanpur, Goraul, Chehra Kalan,<br />
Patepur, Mahua, Jandaha, Raja Pakar, Hajipur, Raghopur, Bidupur,<br />
Desri, Sahdai Buzurg, Mahnar<br />
3.3 RCH Outcome and Service Utilization<br />
The government and its concerned agencies have initiated various programmes to address the<br />
health related issues of the state. However, there is considerable scope of improvement. One of<br />
the reasons for limited achievements of the programs has been the lack of quality of services. The<br />
<strong>State</strong> Health Society has paid special attention to the quality of services and aims at meeting the<br />
needs of the population leading to widespread acceptance of the services. The goal is to provide<br />
integrated reproductive health care services, including addressing the unmet need for<br />
contraception in order to improve the situation by the year 2012.<br />
The program has made positive impact on the indicators in the state but there is still a long way to<br />
go. The current situation of the selected indictors based on NFHS-3 shows that overall the state is<br />
moving towards achieving the goals. The recent NFHS-3 has shown the improvements in health<br />
indicators in the <strong>State</strong>. IMR has reduced from 78 to 62, MMR from 389 to 371. However TFR<br />
has risen from 3.7 to 4.<br />
20
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Important indicators reviewed during NFHS-3:<br />
Total Fertility Rate (TFR) has increased from 3.7 to 4<br />
Contraceptive use has increased from 24 % to 34 %<br />
Antenatal Care has not improved at all<br />
Institutional deliveries have increased from 15 % to 22%<br />
IMR has declined from 78 to 62 per 1000 live births<br />
Percentage of children under age 3 who are underweight has increased 54.3 to 58.4%<br />
Though the <strong>State</strong> has achieved some progress in terms of output indicators, the maternal<br />
mortality, child mortality and population growth continues to be a cause of serious concern to the<br />
state's development efforts. Moreover, floods in some parts of the state make the <strong>State</strong> vulnerable<br />
to communicable diseases. Besides, the health infrastructure is inadequate to cater to the needs of<br />
the people and the upkeep of the already existing facilities is quite challenging.<br />
Human resource is another major issue where the <strong>State</strong> health system is struggling. The paucity<br />
of medical professionals especially the specialists limits the public health facilities in providing<br />
much required higher level of care to the needy. A mismatch exists in the <strong>State</strong> between the<br />
available medical and Para medical professionals and the demand for their services. More<br />
medical graduates and Para medical professionals are required to fill up this gap. Moreover<br />
despite number of trainings held, rationalization of manpower is yet to take place. To overcome<br />
this, the <strong>State</strong> has initiated public private partnerships, out sourcing health facilities and<br />
programmes to private sector and NGOs, contracting specialists for specialized care, etc. There is<br />
also dearth of well-trained public health professionals and managers to effectively steer the public<br />
health and family welfare programs. Another issue which the state is encountering is a declining<br />
sex ratio. Several initiatives like advocacy, intensive IEC programs and enforcement of PNDT<br />
aimed at reversing the existing sex ratio will be initiated this year.<br />
In the coming years, the state envisions a system, which provides all the individuals specially the<br />
BPL population the ability to access health care at an affordable price by tackling the existing<br />
problems and build on its strengths and address its weaknesses.<br />
21
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
3.4 Public Health Infrastructure<br />
District wise Availability of Health Centres of Bihar <strong>State</strong><br />
Sl.<br />
Name of<br />
Districts<br />
No.<br />
of<br />
DH<br />
New<br />
Constr<br />
uction<br />
Total<br />
DH<br />
No. of Sub<br />
Divl<br />
Hospitals<br />
exist<br />
New<br />
Constr<br />
uction<br />
No. of<br />
Referral<br />
Hospital<br />
upgraded<br />
in Sub Div<br />
Hospitals<br />
Total<br />
Sub<br />
Div<br />
Hospi<br />
tals<br />
No. of<br />
Referral<br />
Hospitals<br />
exist<br />
previousl<br />
y<br />
No. of<br />
Referral<br />
Hospitals<br />
exist<br />
Presently<br />
No. of<br />
PHCs<br />
exist<br />
New<br />
Constr<br />
uction<br />
No. of<br />
APHCs<br />
upgrade<br />
d into<br />
PHCs<br />
Total<br />
No. of<br />
PHCs<br />
No. of<br />
APHCs<br />
exist<br />
previosly<br />
No. of<br />
APHCs<br />
exist<br />
presently<br />
No. of<br />
HSCs<br />
1 Araria 1 1 1 1 2 3 2 9 9 30 30 200<br />
2 Arwal 1 1 0 3 3 23 23 46<br />
3 Aurangabad 1 1 1 1 3 3 11 11 58 58 207<br />
4 Banka 1 1 1 1 3 3 10 1 11 24 24 227<br />
5 Begusrai 1 1 1 1 2 2 1 11 7 2 18 31 29 288<br />
6 Bhagalpur 1 1 1 1 2 2 2 11 5 2 16 46 44 280<br />
7 Bhojpur 1 1 1 1 2 2 12 2 1 14 20 19 284<br />
8 Buxar 1 1 1 1 2 7 4 1 11 20 19 158<br />
Champaran<br />
9 (E) 1 1 1 2 3 3 1 20 7 3 27 46 43 315<br />
Champaran<br />
10 (w) 1 1 1 1 2 2 2 16 2 18 25 25 389<br />
11 Darbhanga 1 1 2 2 13 6 4 19 51 47 261<br />
12 Gaya 1 1 1 1 2 2 1 19 6 4 25 49 45 439<br />
13 Gopalganj 1 1 1 1 3 3 10 4 2 14 22 20 186<br />
14 Jamuai 1 1 1 1 3 3 7 2 2 9 21 19 166<br />
15 Jhanabad 1 1 1 1 2 2 4 5 2 9 25 23 81<br />
16 Kaimur 1 1 1 1 2 2 1 9 2 1 11 40 39 107<br />
17 Katihar 1 1 2 2 3 1 11 5 2 16 32 30 257<br />
18 Khagaria 1 1 0 1 1 6 1 1 7 18 17 151<br />
19 Kishanganj 1 1 1 1 2 2 7 7 8 8 136<br />
20 Lakhisarai 1 1 1 1 1 1 4 2 6 13 13 102<br />
21 Madhapura 1 1 1 1 1 7 6 4 13 23 19 115<br />
22 Madhubani 1 1 1 1 1 3 2 1 19 19 76 76 430<br />
22
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
23 Munger 1 1 1 1 1 6 3 3 9 13 10 123<br />
24 Muzaffarpur 1 1 0 1 1 14 2 16 47 47 473<br />
25 Nalanda 1 1 1 1 2 3 2 12 8 7 20 36 29 302<br />
26 Nawada 1 1 1 1 2 2 10 4 3 14 27 24 129<br />
27 Patna 3 1 1 5 4 3 16 7 6 23 70 64 418<br />
28 Purniea 1 1 1 1 2 2 1 11 3 3 14 34 31 278<br />
29 Rohtas 1 1 1 1 2 1 1 13 6 5 19 17 12 186<br />
30 Saharsa 1 1 1 1 7 3 10 33 33 152<br />
31 Samastipur 1 1 3 1 4 1 1 14 6 4 20 59 55 354<br />
32 Saran 1 1 1 1 3 2 15 5 3 20 45 42 413<br />
33 Sheikhpura 1 1 1 1 1 1 3 3 6 18 18 74<br />
34 Sheohar 1 1 1 1 1 1 3 1 4 7 7 34<br />
35 Sitamarhi 1 1 1 1 1 1 13 5 2 18 38 36 213<br />
36 Siwan 1 1 1 1 2 2 15 4 2 19 34 32 370<br />
37 Supaul 1 1 1 1 2 1 1 9 2 1 11 28 27 178<br />
38 Vaishali 1 1 1 1 2 2 11 6 3 17 36 33 336<br />
Total 25 11 36 23 20 15 58 70 55 398 135 73 533 1243 1170 8858<br />
23
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Table : Bihar: Public Health Infrastructure – Personnel<br />
Sl.<br />
No<br />
Districts<br />
MO ANM LHV MHW Staff Nurse AWW<br />
Sanct. Working Sanct. Working Sanct Working Sanct. Working Sanct. Working Sanct. Working<br />
1 Araria 117 98 273 177 41 12 102 40 17 9 1778 1631<br />
2 Aurangabad 188 91 342 319 23 17 110 75 12 3 1430 1390<br />
3 Arwal 62 24 78 105 4 4 59 34 0 0 631 631<br />
4 Banka 97 84 275 213 45 25 124 49 12 6 1352 1044<br />
5 Begusarai 117 73 352 351 24 16 33 11 8 8 1314 1296<br />
6 Bhagalpur 162 127 387 385 48 27 34 32 8 8 1512 1347<br />
7 Bhojpur 132 105 370 368 26 20 106 42 8 1 1658 1646<br />
8 Buxar 89 77 212 212 15 11 42 19 2 2 1139 1139<br />
9 Champaran (E) 237 135 364 355 35 23 48 28 12 1 2901 2895<br />
10 Champaran (W) 145 74 427 308 43 19 60 5 19 15 2263 2252<br />
11 Darbhanga 172 152 363 296 29 19 131 96 8 5 2563 2315<br />
12 Gaya 231 197 575 563 41 33 245 159 8 1 2427 2385<br />
13 Gopalganj 106 95 250 249 20 8 30 3 12 2 1816 1592<br />
14 Jehanabad 119 92 59 56 5 5 31 18 13 8 604 599<br />
15 Jamui 85 61 222 222 25 12 70 31 12 8 1156 1138<br />
16 Kaimur 93 74 146 146 19 11 64 20 19 9 996 993<br />
17 Katihar 121 106 238 211 56 31 33 1 12 7 1716 1637<br />
18 Khagaria 73 61 190 191 31 18 18 5 4 2 967 965<br />
19 Kishanganj 56 37 169 115 31 15 64 27 11 5 1052 963<br />
20 Lakhisarai 72 51 131 131 20 14 40 28 10 9 671 608<br />
21 Madhepura 81 51 223 93 35 9 22 4 4 0 962 588<br />
22 Madhubani 233 124 487 380 37 15 54 43 34 16 3437 2852<br />
23 Munger 141 91 157 157 30 28 51 30 23 23 645 644<br />
24 Muzaffarpur 241 223 594 592 29 21 140 82 4 4 2822 2610<br />
25 Nalanda 178 167 402 402 30 30 36 21 0 0 1785 1761<br />
26 Nawada 115 87 207 207 24 11 30 21 25 17 1249 1235<br />
27 Patna 289 205 434 434 32 30 49 6 16 13 2481 2465<br />
28 Purnia 126 100 356 275 56 29 126 67 8 2 1464 1424<br />
29 Rohtas 158 129 286 270 29 12 136 48 20 10 1712 1628<br />
30 Saharsa 97 55 192 169 33 15 18 1 26 21 932 825<br />
31 Samastipur 192 183 475 470 30 20 29 18 4 4 2692 2512<br />
24
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
32 Saran 185 133 512 386 33 29 46 17 27 10 2455 2218<br />
33 Sheikhpura 53 36 109 109 16 6 18 4 4 1 357 339<br />
34 Sheohar 52 34 46 26 4 1 38 13 9 1 265 265<br />
35 Sitamarhi 147 127 299 289 27 9 130 82 17 13 2064 1920<br />
36 Siwan 151 126 465 298 31 25 102 56 13 9 2099 1934<br />
37 Supaul 85 70 206 111 44 8 60 34 2 0 1376 1230<br />
38 Vaishali 126 105 421 414 25 24 33 28 8 3 1844 1608<br />
5124 3860 11294 10055 1126 662 2562 1298 451 256 60587 56524<br />
25
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
3.5 Private and NGO Health Service<br />
The <strong>State</strong> has a wide network of private health facilities in the urban areas providing Health<br />
services. In general, these private health facilities are run either by individuals/organizations for<br />
profit or by Non-profit Charitable organization/NGOs. However, exact data on the number of these<br />
health facilities are not available with the <strong>State</strong> as in the <strong>State</strong>, the registration of private clinics and<br />
nursing homes has not yet started although the Clinical Establishment Act has been passed last year.<br />
Presently these health facilities are also not regulated by the DoH & F.W. However under PNDT<br />
Act, the private clinics and nursing homes undertaking ultra sonography have been regulated and<br />
these facilities are being monitored. There is an urgent need to create a comprehensive database for<br />
private health service providers and develop appropriate regulatory mechanism for them.<br />
NGOs<br />
The state has only 12 Mother NGOs (MNGOs) covering 22 of the 38 districts of Bihar. However<br />
the state does not have a structured procedure to assess the working of MNGOs. There is a need to<br />
improve coordination between the NGOs and the Government at all levels i.e. state, districts and<br />
sub-district levels in order to make them effective.<br />
Further analysis of information related to NGOs in the state revealed that there are many NGOs that<br />
are engaged in the health service delivery. Although no attempts have been made to assess the<br />
functioning of these NGOs, it is important to take initiative to develop efficient NGO network in the<br />
<strong>State</strong>.<br />
3.6 Donor Assisted Programmes in the <strong>State</strong><br />
UNICEF<br />
Unicef is supporting the state for immunization, maternal health, nutrition and trainings. Unicef has<br />
already initiated the implementation of IMNCI programme and is supporting the operationalization<br />
of Nutritional Rehabiltization Centres. Extensive support is provided by them in the health sector<br />
especially during flood seasons. Unicef is providing technical support in operationlising ANM<br />
training centres, procurement of equipments related to child health etc.<br />
NIPI - Norwegian India Partnership Initiative<br />
Under NIPIs Child Health Initiatives, a voluntary health worker called Mamta has been engaged at<br />
all the District Hospitals and Sub Divisional Hospitals. A District Training Resource Centre wil be set<br />
up in Nalanda district. In three NIPI focus districts namely Jehanabad, Nalanda and Sheikhpura for<br />
operationzation of SNCUs, technical support and training of doctors and paramedical staffs are<br />
26
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
being provided. Home Based Newborn Care is being implemented in three NIPI focus districts<br />
through ASHAs. SPMU, DPMU and Block Programme Management Units shall be supported by<br />
provision of consultants. At the <strong>State</strong> level Child Health Consultant, Finance Analyst and Data<br />
Assistant, at the district level District Child Health Managers, at District Hospitals and Sub<br />
divisional level Child Health Supervisors and Dy. Child Health Supervisors and at the block level<br />
Junior Child Health Managers shall be placed.<br />
The detailed fund allocation has been annexed.<br />
WHO-NPSP<br />
WHO is supporting the state in Pulse Polio Immunization Programme.<br />
UNFPA<br />
UNFPA is collaborating with SHSB from financial year 08-09 and is providing technical support in<br />
Maternal Health.<br />
3.7 Institutional Arrangements and Organizational Development<br />
Along with Health department the ICDS, PHED and Panchayat are helping in implementing the<br />
NRHM Programme. The coordination has been placed at <strong>State</strong> level, District Level and Block<br />
Level. At the Grassroot level linkage between ASHA, ANM with AWW has been strengthened.<br />
PHED department has taken up the training of ASHA.<br />
Trainings are being regularly conducted under different programmes in the state. The state has<br />
already started the trainings of IMNCIs. With the Unicef support the <strong>State</strong> has initiated to<br />
operationlise 22 ANM schools in 2009-10. Repair and renovation of these schools are already in<br />
progress and are expected to be operationalised in this year. Most of the districts have their own<br />
warehouse.<br />
The state has a unique system of collecting data from each PHC level. The state has established a<br />
data centre in the state and has centres in District and at PHC. These data centres collect data from<br />
each PHC through mobile phone and feed in the computer. The computerized data is later given to<br />
the respective Programme Officers.<br />
3.8 Program Finance<br />
Governments Of Indias funds are released to the state through two separate channels, i.e; through<br />
the state budget and directly through the <strong>State</strong> Health Society. Further the Departments outlay for<br />
the procurement of vaccines, drugs, equipments etc; is spent centrally and assistance to the state has<br />
been in the form of kind.<br />
27
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
PART- A<br />
RCH Flexible Pool<br />
2009-2010<br />
28
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Situational Analysis Chapter 4<br />
4.1 Maternal Health<br />
Improving the maternal health scenario by strengthening availability, accessibility and utilization of maternal<br />
health services in the state is one of the major objectives of RCH. However, the current status of maternal<br />
health in the state clearly shows that the programme has not been able to significantly improve the health<br />
status of women. There are a host of issues that affect maternal health services in Bihar. The important ones<br />
are listed below:<br />
· Shortage of skilled frontline health personnel (ANM, LHV) to provide timely and quality ANC and PNC<br />
services.<br />
· The public health facilities providing obstetric and gynecological care at district and sub-district levels<br />
are inadequate.<br />
· Mismatch in supply of essential items such as BP machines, weighing scales, safe delivery kits, Kit A<br />
and Kit B, etc and their demand.<br />
· Shortage of gynecologists and obstetricians to provide maternal health services in peripheral areas.<br />
· Inadequate skilled birth attendants to assist in home-based deliveries<br />
· Weak referral network for emergency medical and obstetric care services<br />
· Lack of knowledge about antenatal, perinatal and post natal care among the community especially in<br />
rural areas<br />
· Low mean age of marriage resulted in pregnancy and difficult deliveries.<br />
· Low levels of female literacy resulted unawareness on maternal health services.<br />
· High levels of prevalence of malnutrition (anemia) among women in the reproductive age group<br />
· Poor communication because of bad roads and a law and order situation.<br />
One of the very good things happen to maternal health is introduction JBSY.<br />
In 2008-09, 16 MOs trained in CEmOC and 59 MOs in Life Saving Anesthetic Skills who are now managing<br />
complicated cases at their respective place of postings. Bihar is the first state to have formally evaluated the LSAS<br />
examinees and issued certificates of practice for the obstetric anesthesia.<br />
29
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
A quality monitoring cell at the state level housed in <strong>State</strong> Institute of Health & Family Welfare is<br />
monitoring all the trainings. The cell has members drawn from SIHFW faculty, medical colleges,<br />
retired faculty members, officials from <strong>State</strong> Health Society and officials from partner agencies as<br />
its members. Their initial focus is to monitor the quality of various trainings being undertaken under<br />
NRHM like IMNCI, SBA, Minilap etc. In the year 2009-10, the role shall be expanded to include<br />
the monitoring of quality of critical care services. (details in annexure)<br />
4.2 Child Health<br />
The child health indicators of the state reveal that the state's IMR is lower than the national average but the<br />
NMR is disproportionately high. Morbidity and mortality due to vaccine-preventable diseases still continues<br />
to be significantly high. Similarly, child health care seeking practices in the case of common childhood<br />
diseases such as ARI and Diarrhoea are not satisfactory. The child health scenario is worse for specific<br />
groups of children, such as those who live in rural areas, whose mothers are illiterate, who belong to<br />
Scheduled Castes, and who are from poor households is particularly appalling.<br />
Issues affecting child health are not only confined to mere provision of health services for children, but other<br />
important factors such as maternal health and educational status, family planning practices and<br />
environmental sanitation and hygiene have enormous bearing on child health. This is more than evident in<br />
the case of Bihar where child health continues to suffer not only because of poor health services for children<br />
but due to issues such as significantly high maternal malnutrition, low levels of female literacy, early and<br />
continuous childbearing, etc. The specific issues affecting child health in the state are listed below.<br />
Maternal Factors<br />
· High levels of maternal malnutrition leading to increased risk pre-term and low -birth weight babies that<br />
in turn increase risk of child mortality.<br />
· Low levels of female literacy, particularly in rural areas.<br />
Family Planning Services<br />
· The Family Planning programme has partially succeeded in delaying first birth and spacing births<br />
leading to significantly high mortality among children born to mothers under 20 years of age and to<br />
children born less than 24 months after a previous birth.<br />
Child Health Services<br />
· The programme has not succeeded fully in effectively promoting colostrum feeding immediately after<br />
birth and exclusive breastfeeding despite almost universal breastfeeding practice in the state. In the <strong>State</strong><br />
majority of mother breast feed children beyond six months. However both <strong>State</strong> and Unicef have taken<br />
initiative to generate awareness among mothers for exclusive breast feeding.<br />
30
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
· High levels of child malnutrition, particularly in rural areas and in children belonging to disadvantaged<br />
socio-economic groups leading to a disproportionate increase in under five mortality.<br />
· Persistently low levels of child immunisation primarily due to non-availability of timely and quality<br />
immunisation services.<br />
· Lack of child health facilities, both infrastructure and human resource, to provide curative services for<br />
common childhood ailments such as ARI, Diarrhea, etc.<br />
· Inadequate supply of drugs, ORS packets, weighing scales, etc.<br />
· Lack of knowledge of basic child health care practices among the community.<br />
· Failure to generate community awareness regarding essential sanitation and hygiene practices that impact<br />
on the health of children.<br />
Since these factors are inter-linked and synergistic, any effort to improve the health of the children in the<br />
state needs to address child health issues in a holistic manner.<br />
IMNCI Training: IMNCI training has successfully started in the <strong>State</strong>. The Pilot project has also successfully<br />
completed in the district of Vaishali. The project is being monitored and managed by Unicef. In 2008-09<br />
IMNCI Training is being scaled up in thirteen districts. In phase wise rest of districts will be completed.<br />
In 2008-09, a pilot project done through SHSB on Nutritional Rehabilitation Centre. In this project special<br />
nutritious food provided to the severely malnutrition children.<br />
4.3 Family Planning<br />
RCH emphasizes on the target-free promotion of contraceptive use among eligible couples, the provision to<br />
couples a choice of various contraceptive methods (including condoms, oral pills, IUDs and male and female<br />
sterilization), and the assurance of high quality care. It also encourages the spacing of births with at least<br />
three years between births. Despite RCH and previous programmes vigorously pursuing family planning<br />
objectives, fertility in Bihar continues to decline at much lower rates than the national average. Although the<br />
total fertility rate has declined by about half a child in the six-year period between NFHS-1 and NFHS-2, it<br />
has increased in NFHS-3 and is far from the replacement level. Furthermore, certain groups such as rural,<br />
illiterate, poor, and Muslim women within the population have even higher fertility than the average.<br />
The persistently high fertility levels point to the inherent weakness of the state's family planning programme<br />
as well as existing sociodemographic issues. High TFR is reflected by a dismal picture of women in Bihar<br />
31
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
marrying early, having their first child soon after marriage, and having two or three more children in close<br />
succession by the time they reach their late-20s. At that point, about one-third of women get sterilized. Very<br />
few women use modern spacing methods that could help them delay their first births and increase intervals<br />
between pregnancies.<br />
The major issues affecting the implementation of the Family Planning programme in Bihar are as follows.<br />
· Lack of integration of the Family Planning programmes with other RCH components, resulting in<br />
dilution of roles, responsibilities and accountability of programme managers both at state and district<br />
levels.<br />
· Failure of the programme to effectively undertake measures to increase median age at marriage and first<br />
childbirth.<br />
· Inability of the programme to alter fertility preferences of eligible couples through effective behavior<br />
change communication (BCC).<br />
· Over emphasis on permanent family planning methods such as, sterilization ignoring other reversible<br />
birth spacing methods that may be more acceptable to certain communities and age groups. (Overall,<br />
sterilization accounts for 82 percent of total contraceptive use. Use rates for the pill, IUD, and condoms<br />
remain very low, each at 1 percent or less).<br />
· Due to high prevalence of RTI/STD, IUDs are not being used by majority of women.<br />
· Continued use of mass media to promote family planning practices despite evidently low exposure to<br />
mass media in Bihar, leading to lower exposure of family planning messages in the community,<br />
particularly among rural and socio-economically disadvantaged groups.<br />
· Weak public-private partnerships, social marketing to promote and deliver family planning<br />
services.(Public Private Partnership is improved since 2008-09. 102 Nursing homes in 20 districts are<br />
accredited to conduct Family planning operations . In 2008-09 accredited private Nursing homes are<br />
expected to conduct more than 50-60 thousand family planning operations in the state. From April,<br />
2008, 223000 sterilization conducted till Jan, 2009 of which 40,000 are conducted by the accredited<br />
private Nursing Homes. Details in Annexure)<br />
The issues mentioned above are closely interlinked with the existing sociodemographic conditions<br />
of the women, specially rural, poor and illiterate. Comprehensive targeted family planning<br />
programme as well as intersectoral co-ordination on an overall female empowerment drive is<br />
needed to address the factors responsible for persistently high fertility levels in Bihar.<br />
32
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
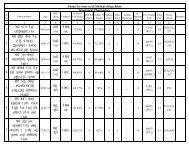
The state has quality assurance committee for family planning both at <strong>State</strong> and District level. The committee<br />
sits quarterly and report is sent to state. Also, 102 private hospitals and Clinics are accredited by the District<br />
Quality Assurance Committees for conducting sterilization in 20 districts.These private facilities are<br />
monitored by the QAC on sterilization conducted in the facilities. Family planning Insurance scheme is also<br />
being implemented in the state with ICICI Lombard . Most of the Sterilizations are conducted in the last<br />
two quarters due to existing sociodemographic and programmatic reasons as evident from the graph-<br />
Month wise comparison of Sterilization<br />
2007-08 & 2008-09<br />
100000<br />
90000<br />
80000<br />
88,000<br />
85473<br />
81105<br />
70000<br />
60000<br />
50000<br />
40000<br />
42008<br />
45673<br />
49750<br />
2007-<br />
08<br />
2008-<br />
09<br />
30000<br />
20000<br />
10000<br />
0<br />
6130<br />
7505<br />
2394<br />
1693<br />
3759<br />
3338<br />
7815<br />
9857<br />
1835<br />
1275<br />
2593<br />
13951<br />
4190<br />
6728 18210<br />
Apr May June July Aug Sep Oct Nov Dec Jan Feb Mar<br />
Efforts are being made<br />
to offer fixed day family planning services at District hospitals, Sub divisional<br />
hospitals, FRUs and accredited private facilities. Later on this will be extended to the PHCs.<br />
4.4 Adolescent Reproductive & Sexual Health<br />
The World Health Organization (WHO) defines adolescence as the period between 10 and 19 years of age,<br />
which broadly corresponds to the onset of puberty and the legal age for adulthood.<br />
33
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Commencement of puberty is usually associated with the beginning of adolescence. In some societies,<br />
adolescents are expected to shoulder adult responsibilities well before they are adults; in others, such<br />
responsibilities come later in life.<br />
Although it is a transitional phase from childhood to adulthood, it is the time that the adolescents experience<br />
critical and defining life events first sexual relations, first marriage, first childbearing and parenthood. It is<br />
a critical period which lays the foundation for reproductive health of the individuals lifetime. Therefore,<br />
adolescent reproductive and sexual health involves a specific set of needs distinct from adult needs.<br />
The reproductive health needs of adolescents as a group has been largely ignored to date by existing<br />
reproductive health services. Many adolescents in India face reproductive and other health risks. Poor<br />
nutrition and lack of information about proper diets increase the risk of iron-deficiency anemia for adolescent<br />
girls. Young women and men commonly have reproductive tract infections (RTIs) and sexually transmitted<br />
infections (STIs), but do not regularly seek treatment despite concerns about how these infections may affect<br />
their fertility.<br />
India also has one of the highest rates of early marriage and childbearing, and a very high rate of irondeficiency<br />
anemia. The prevalence of early marriage in India poses serious health problems for girls,<br />
including a significant increase of maternal or infant mortality and morbidities during childbirth. The<br />
following facts will help understand the situation objectively.<br />
· The median age of marriage among women (aged 20 to 24) in India is 16 years.<br />
· In rural India, 40 percent of girls, ages 15 to 19, are married, compared to only 8 percent of boys the<br />
same age.<br />
· Among women in their reproductive years (ages 20 to 49), the median age at which they first gave<br />
birth is 19.<br />
· Nearly half of married girls, ages 15 to 19, have had a least one child.<br />
· India has the worlds highest prevalence of iron-deficiency anemia among women, with 60 percent<br />
to 70 percent of adolescent girls being anemic.<br />
Underlying each of these health concerns are gender and social norms that constrain young people <br />
especially young womens access to reproductive health information and services.<br />
Motherhood at a very young age entails a risk of maternal death that is much greater than average, and the<br />
children of young mothers have higher levels of morbidity and mortality. Early child bearing continues to be<br />
an impediment to improvements in the educational, economic and social status of women in India. Overall<br />
for young women, early marriage and early motherhood can severely curtail educational and employment<br />
opportunities and are likely to have a long-term, adverse impact on their and their childrens quality of life.<br />
In many societies, adolescents face pressures to engage in sexual activity. Young women, particularly lowincome<br />
adolescents are especially vulnerable. Sexually active adolescents of both sexes are increasingly at<br />
high risk of contracting and transmitting sexually transmitted diseases, including HIV/AIDS; and they are<br />
typically poorly informed about how to protect themselves.<br />
To meet the reproductive and sexual health needs of adolescents, information and education should be<br />
provided to them to help them attain a certain level of maturity required to make responsible decisions. In<br />
particular, information and education should be made available to adolescents to help them understand their<br />
sexuality and protect them from unwanted pregnancies, sexually transmitted diseases and subsequent risk of<br />
34
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
infertility. This should be combined with the education of young men to respect womens self-determination<br />
and to share responsibility with women in matters of sexuality and reproduction.<br />
Information and education programs should not only be targeted at the youth but also at all those who are in<br />
a position to provide guidance and counseling to them, particularly, parents and families, service providers,<br />
schools, religious institutions, mass media and peer groups. These programs should also involve the<br />
adolescents in their planning, implementation and evaluation.<br />
Being a sensitive and often, controversial area, adolescent reproductive and sexual health issues and<br />
information are very often difficult to handle and disseminate. Furthermore, the contents do not only deal<br />
with factual and knowledge-based information but more importantly, need to deal with attitudinal and<br />
behavioral components of the educational process.<br />
Thus it can be conclusively stated that adolescents are a diverse group, and their diversity must be considered<br />
when planning programs.<br />
Adolescents, the segment of the population in the age group of 15 -19 years, constitute about 23% of the<br />
population of the state. This group is critical to the success of any reproductive and sexual health programme,<br />
as it would remain in the reproductive age group for more than two decades.<br />
Early marriages seem to be still a key problem. Percentage of boys who are married before attaining 21 years<br />
in consistently high in most districts. The mean age of marriage for girls is 16.9. 25% pregnant mothers in<br />
the state are in the age group of 15-19 years. This is due to the reason that most of the girls married before<br />
18 years.<br />
The various anecdotal evidences emerging from the community level participatory planning exercises and<br />
opinions voiced by the various levels of health officials during consultation exercise indicate that there is<br />
lack of a cohesive ARSH strategy at the state level. Possibility of bifurcating the total target into school<br />
going and out of school going adolescents have not been examined as a strategy option. Hence the current<br />
school health program by and large lacks any adolescent oriented interventions.<br />
In the consultations with the Bihar <strong>State</strong> AIDS Control Society, it had emerged that they have several<br />
adolescent targeted intervention including using special adolescent counselors currently going actively<br />
implemented. The possibility of convergence between the RCH II program priorities and NACP priorities<br />
require to be integrated.<br />
Specific capacity building initiatives to orient the health providers at various levels to specific necessities of<br />
the ARSH program like adolescent vulnerability to RTI/STI/HIV /AIDS, communication with adolescents,<br />
gender related issues, designing adolescent friendly health services, body and fertility awareness,<br />
35
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
contraceptive needs etc have not been actively taken up the state health department to prepare itself to tackle<br />
the problems / issues of this important segment.<br />
4.5 District/Sub District Variations<br />
Key indicators related to Maternal and Child Health (MCH) and Family Planning clearly show the poor<br />
status of RCH in Bihar. However, close examination of data reveals that there exist wide inter-district<br />
variations for almost all the key indicators.<br />
36
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
DLHS-3 Data for Bihar<br />
S.no.<br />
<strong>State</strong>/district<br />
% of households with low<br />
standard of living<br />
% girls marrying below legal<br />
18 age at marriage<br />
Birth order 3 and above<br />
Any Method<br />
Any Modern Method<br />
Female Sterilization<br />
Male Sterilization<br />
Unmet need for family<br />
planning<br />
% women received at least<br />
three visits for ANC<br />
Institutional Birth<br />
Delivery at home assisted<br />
by a doctor/nurse/LHV/ANM<br />
% of children (age12-23<br />
months) received full<br />
immunization<br />
Children breastfed within<br />
one hour of birth<br />
% women aware of HIV/AIDS<br />
1 Banka 92.0 59.9 50.4 25.0 22.7 20.4 0.0 39.2 31.5 24.7 12.6 32.9 15.1 42.3<br />
2 Aurangabad 85.4 38.7 46.9 34.5 31.0 29.4 0.3 37.9 18.9 30.6 5.0 56.5 14.4 48.3<br />
3 Araria 93.7 41.4 58.2 31.5 29.0 27.8 0.4 36.1 41.2 13.7 6.0 35.8 18.2 29.5<br />
4 Bhagalpur 74.0 27.8 53.1 40.3 35.0 29.3 0.5 36.4 20.4 30.4 14.7 49.6 22.6 57.5<br />
5 Muzaffarpur 81.4 35.7 50.5 33.1 32.2 28.9 0.1 36.9 20.4 23.0 3.3 57.4 15.5 46.0<br />
6 Nalanda 73.0 46.6 47.8 30.9 27.2 21.2 0.5 40.7 25.2 39.3 7.0 54.2 30.2 73.7<br />
7 Nawada 87.1 65.3 51.6 24.3 21.9 18.7 0.7 39.9 23.6 31.1 3.7 48.9 9.9 53.0<br />
8 Champaran W 89.2 57.8 58.7 32.3 27.8 26.3 0.2 36.9 32.4 24.9 2.4 30.2 9.8 36.6<br />
9 Patna 50.9 34.0 45.7 43.7 40.2 33.6 0.2 31.0 20.7 58.8 3.7 43.8 21.3 84.6<br />
10 Champaran E 88.0 54.9 48.1 27.7 23.6 20.8 0.7 34.7 36.0 27.1 1.7 41.3 7.2 19.9<br />
11 Buxar 78.0 49.8 47.9 31.2 26.9 23.7 0.2 36.8 22.1 48.0 4.8 27.7 23.4 65.0<br />
12 Begusarai 83.7 46.2 54.2 28.0 25.2 23.4 0.2 39.0 28.3 26.8 4.6 40.3 9.4 23.8<br />
13 Munger 61.7 30.5 42.6 41.4 33.9 30.3 0.4 31.6 36.8 48.6 10.5 36.3 19.3 79.0<br />
14 Madhubani 88.4 39.5 53.1 96.3 34.9 28.2 0.0 40.3 35.6 16.0 4.0 42.1 7.9 30.3<br />
15 Madhepura 90.6 55.3 53.5 35.0 31.0 29.2 0.4 35.9 20.0 17.7 3.9 39.7 11.1 39.4<br />
37
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
16 Lakhisarai 79.8 54.7 48.0 31.2 28.2 25.1 0.5 41.6 25.3 32.5 6.3 36.0 13.7 32.2<br />
17 Darbhanga 83.5 39.1 51.4 31.8 30.4 27.9 0.1 36.3 29.0 15.1 2.9 41.8 15.3 44.2<br />
18 Gaya 80.2 50.4 50.8 30.5 26.7 23.3 0.3 34.0 23.9 20.7 6.6 31.8 20.6 55.1<br />
19 Gopalganj 82.0 35.9 48.4 12.8 22.1 20.4 17.0 0.0 31.8 36.5 6.6 52.4 10.5 31.0<br />
20 Jamui 91.2 72.9 49.4 27.4 20.7 18.3 0.3 44.2 27.1 17.6 8.0 17.4 14.8 41.7<br />
21 Jehanabad 83.8 56.7 46.1 28.2 24.1 20.1 0.6 39.8 30.6 42.5 10.6 47.2 18.6 66.8<br />
22 Kaimur 84.4 56.1 51.5 29.9 24.8 21.3 0.2 34.9 23.7 42.6 6.8 21.9 30.9 60.2<br />
23 Katihar 88.1 43.7 53.0 26.0 20.3 16.6 0.0 43.7 32.5 12.4 3.9 32.6 13.4 37.6<br />
24 Khagaria 84.8 49.3 51.3 31.1 27.5 25.2 0.3 37.3 26.4 25.3 6.7 45.8 9.8 54.3<br />
25 Kishanganj 90.7 32.1 57.0 27.2 23.5 16.0 0.6 38.1 28.5 17.8 3.8 26.6 12.8 38.9<br />
26 Purnia 87.0 40.4 53.6 10.4 27.5 25.7 23.3 41.2 19.4 21.6 2.9 37.4 13.8 28.8<br />
27 Bhojpur 78.8 48.1 45.5 35.3 30.2 25.5 0.6 39.9 17.2 40.4 12.5 31.2 20.1 57.2<br />
28 Saharsa 87.3 54.4 47.9 32.6 29.8 27.8 0.2 37.5 13.9 20.0 8.8 43.4 15.8 46.3<br />
29 Samastipur 87.6 51.4 52.7 34.8 28.9 26.6 0.4 36.3 23.9 27.6 3.1 51.1 10.9 38.1<br />
30 Saran 81.9 31.0 51.5 29.1 25.2 20.9 0.3 43.7 22.7 22.4 6.1 65.1 15.4 59.8<br />
31 Sheikhpura 79.0 53.5 52.1 26.7 23.4 20.2 0.6 39.0 43.2 41.6 5.0 38.3 10.5 51.4<br />
32 Sheohar 89.0 54.8 57.0 27.4 22.3 20.4 0.1 42.6 18.9 11.9 3.4 28.3 8.3 31.8<br />
33 Sitamarhi 86.8 44.4 56.3 18.1 25.3 23.7 22.1 41.2 22.9 16.4 4.7 39.1 12.5 40.7<br />
34 Siwan 78.4 27.6 46.0 24.0 20.4 17.2 0.2 39.7 33.4 33.5 8.2 52.4 13.3 50.2<br />
35 Vaishali 81.3 41.2 46.9 43.6 39.8 35.0 0.6 32.7 16.0 28.2 9.6 53.3 33.8 81.5<br />
36 Supaul 92.0 44.2 51.5 43.1 41.6 40.1 0.1 29.8 21.2 23.2 2.4 39.5 13.3 38.2<br />
38
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Focus Districts:<br />
As per the guidelines issued by the Ministry of Minority Affairs, GoI regarding districts with higher<br />
percentage of the minority population, the S<strong>PIP</strong> for NRHM, attempts to provide adequate resources.<br />
Bihar has got seven districts Araria, Kishanganj, Purnia, Katihar, Sitamarhi, West Champaran, Darbhanga in<br />
category-A which have both socio-economic and basic amenities parameters below national average while<br />
allocating available resources to the districts, we've tried to give priority to these Category-A districts. The<br />
District Magistrates of 3 (three) of these districts i.e. Araria, Purnea and Katihar have been made members of<br />
<strong>State</strong> Health Mission headed by CM. This year the rest 4 will also be included, so that the specific problems<br />
of these districts may be brought into fore.<br />
39
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
4.6 Health Infrastructure and Facilities<br />
The delivery of services could only be improved if facilities are within reach and have minimum basic physical infrastructure to provide the basic<br />
services. There seemed a major challenge in construction of the health care facilities. Lack of clear guidelines sometimes delayed the process.<br />
To make the BEmOCs and CEmOCs functional, adequate staff, essential equipments and infrastructure (OT, Labour rooms, new born care area,<br />
blood storage and blood storage units) are to be taken up as a priority area.<br />
District wise Availability of Health Centres of Bihar <strong>State</strong><br />
No. of No. of No. of<br />
Referral Referra Referra<br />
No. of New<br />
Total<br />
No.<br />
No. of Total No. of No. of<br />
Hospital l l<br />
No.<br />
No. New Tota Sub Const<br />
Sub<br />
of New APHCs No. APHCs APHCs<br />
Sl Name of<br />
upgrade Hospit Hospit<br />
of<br />
of Constr l Divl r<br />
Div<br />
PHC Constr upgrad of exist exist<br />
. Districts<br />
d in Sub als als<br />
HSC<br />
DH uction DH Hospital uctio<br />
Hosp<br />
s uction ed into PHC previos present<br />
Div<br />
exist exist<br />
s<br />
s exist n<br />
itals<br />
exist<br />
PHCs s ly ly<br />
Hospital previou Present<br />
s<br />
sly ly<br />
1 Araria 1 1 1 1 2 3 2 9 9 30 30 200<br />
2 Arwal 1 1 0 3 3 23 23 46<br />
Aurangaba<br />
3 d 1 1 1 1 3 3 11 11 58 58 207<br />
4 Banka 1 1 1 1 3 3 10 1 11 24 24 227<br />
5 Begusrai 1 1 1 1 2 2 1 11 7 2 18 31 29 288<br />
6 Bhagalpur 1 1 1 1 2 2 2 11 5 2 16 46 44 280<br />
7 Bhojpur 1 1 1 1 2 2 12 2 1 14 20 19 284<br />
40
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
8 Buxar 1 1 1 1 2 7 4 1 11 20 19 158<br />
Champaran<br />
9 (E) 1 1 1 2 3 3 1 20 7 3 27 46 43 315<br />
1 Champaran<br />
0 (w) 1 1 1 1 2 2 2 16 2 18 25 25 389<br />
1<br />
1 Darbhanga 1 1 2 2 13 6 4 19 51 47 261<br />
1<br />
2 Gaya 1 1 1 1 2 2 1 19 6 4 25 49 45 439<br />
1<br />
3 Gopalganj 1 1 1 1 3 3 10 4 2 14 22 20 186<br />
1<br />
4 Jamuai 1 1 1 1 3 3 7 2 2 9 21 19 166<br />
1<br />
5 Jhanabad 1 1 1 1 2 2 4 5 2 9 25 23 81<br />
1<br />
6 Kaimur 1 1 1 1 2 2 1 9 2 1 11 40 39 107<br />
1<br />
7 Katihar 1 1 2 2 3 1 11 5 2 16 32 30 257<br />
1<br />
8 Khagaria 1 1 0 1 1 6 1 1 7 18 17 151<br />
1<br />
9 Kishanganj 1 1 1 1 2 2 7 7 8 8 136<br />
2 Lakhisarai 1 1 1 1 1 1 4 2 6 13 13 102<br />
41
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
0<br />
2<br />
1 Madhapura 1 1 1 1 1 7 6 4 13 23 19 115<br />
2<br />
2 Madhubani 1 1 1 1 1 3 2 1 19 19 76 76 430<br />
2<br />
3 Munger 1 1 1 1 1 6 3 3 9 13 10 123<br />
2 Muzaffarp<br />
4 ur 1 1 0 1 1 14 2 16 47 47 473<br />
2<br />
5 Nalanda 1 1 1 1 2 3 2 12 8 7 20 36 29 302<br />
2<br />
6 Nawada 1 1 1 1 2 2 10 4 3 14 27 24 129<br />
2<br />
7 Patna 3 1 1 5 4 3 16 7 6 23 70 64 418<br />
2<br />
8 Purniea 1 1 1 1 2 2 1 11 3 3 14 34 31 278<br />
2<br />
9 Rohtas 1 1 1 1 2 1 1 13 6 5 19 17 12 186<br />
3<br />
0 Saharsa 1 1 1 1 7 3 10 33 33 152<br />
3<br />
1 Samastipur 1 1 3 1 4 1 1 14 6 4 20 59 55 354<br />
3 Saran 1 1 1 1 3 2 15 5 3 20 45 42 413<br />
42
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
2<br />
3<br />
3 Sheikhpura 1 1 1 1 1 1 3 3 6 18 18 74<br />
3<br />
4 Sheohar 1 1 1 1 1 1 3 1 4 7 7 34<br />
3<br />
5 Sitamarhi 1 1 1 1 1 1 13 5 2 18 38 36 213<br />
3<br />
6 Siwan 1 1 1 1 2 2 15 4 2 19 34 32 370<br />
3<br />
7 Supaul 1 1 1 1 2 1 1 9 2 1 11 28 27 178<br />
3<br />
8 Vaishali 1 1 1 1 2 2 11 6 3 17 36 33 336<br />
Total 25 11 36 23 20 15 58 70 55 398 135 73 533 1243 1170 8858<br />
Table : Bihar: Public Health Infrastructure Personnel<br />
Sl.<br />
No<br />
Districts<br />
MO ANM LHV MHW Staff Nurse AWW<br />
Sanct. Working Sanct. Working Sanct Working Sanct. Working Sanct. Working Sanct. Working<br />
1 Araria 117 98 273 177 41 12 102 40 17 9 1778 1631<br />
2 Aurangabad 188 91 342 319 23 17 110 75 12 3 1430 1390<br />
3 Arwal 62 24 78 105 4 4 59 34 0 0 631 631<br />
4 Banka 97 84 275 213 45 25 124 49 12 6 1352 1044<br />
5 Begusarai 117 73 352 351 24 16 33 11 8 8 1314 1296<br />
6 Bhagalpur 162 127 387 385 48 27 34 32 8 8 1512 1347<br />
7 Bhojpur 132 105 370 368 26 20 106 42 8 1 1658 1646<br />
8 Buxar 89 77 212 212 15 11 42 19 2 2 1139 1139<br />
9 Champaran (E) 237 135 364 355 35 23 48 28 12 1 2901 2895<br />
43
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
10 Champaran (W) 145 74 427 308 43 19 60 5 19 15 2263 2252<br />
11 Darbhanga 172 152 363 296 29 19 131 96 8 5 2563 2315<br />
12 Gaya 231 197 575 563 41 33 245 159 8 1 2427 2385<br />
13 Gopalganj 106 95 250 249 20 8 30 3 12 2 1816 1592<br />
14 Jehanabad 119 92 59 56 5 5 31 18 13 8 604 599<br />
15 Jamui 85 61 222 222 25 12 70 31 12 8 1156 1138<br />
16 Kaimur 93 74 146 146 19 11 64 20 19 9 996 993<br />
17 Katihar 121 106 238 211 56 31 33 1 12 7 1716 1637<br />
18 Khagaria 73 61 190 191 31 18 18 5 4 2 967 965<br />
19 Kishanganj 56 37 169 115 31 15 64 27 11 5 1052 963<br />
20 Lakhisarai 72 51 131 131 20 14 40 28 10 9 671 608<br />
21 Madhepura 81 51 223 93 35 9 22 4 4 0 962 588<br />
22 Madhubani 233 124 487 380 37 15 54 43 34 16 3437 2852<br />
23 Munger 141 91 157 157 30 28 51 30 23 23 645 644<br />
24 Muzaffarpur 241 223 594 592 29 21 140 82 4 4 2822 2610<br />
25 Nalanda 178 167 402 402 30 30 36 21 0 0 1785 1761<br />
26 Nawada 115 87 207 207 24 11 30 21 25 17 1249 1235<br />
27 Patna 289 205 434 434 32 30 49 6 16 13 2481 2465<br />
28 Purnia 126 100 356 275 56 29 126 67 8 2 1464 1424<br />
29 Rohtas 158 129 286 270 29 12 136 48 20 10 1712 1628<br />
30 Saharsa 97 55 192 169 33 15 18 1 26 21 932 825<br />
31 Samastipur 192 183 475 470 30 20 29 18 4 4 2692 2512<br />
32 Saran 185 133 512 386 33 29 46 17 27 10 2455 2218<br />
33 Sheikhpura 53 36 109 109 16 6 18 4 4 1 357 339<br />
34 Sheohar 52 34 46 26 4 1 38 13 9 1 265 265<br />
35 Sitamarhi 147 127 299 289 27 9 130 82 17 13 2064 1920<br />
36 Siwan 151 126 465 298 31 25 102 56 13 9 2099 1934<br />
37 Supaul 85 70 206 111 44 8 60 34 2 0 1376 1230<br />
38 Vaishali 126 105 421 414 25 24 33 28 8 3 1844 1608<br />
5124 3860 11294 10055 1126 662 2562 1298 451 256 60587 56524<br />
44
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
District Hospitals: Out of 38 Districts 25 have district hospitals. Most of the district hospitals are not<br />
functioning up to the level due shortage of specialties and Staff Nurses. Construction of 11 District Hospitals<br />
are on full swing and expected to be completed by 2010.<br />
Sub District Hospitals: At present there are 23 Sub District Hospital, 20 new SDH are under construction and<br />
15 Referral Hospital are in the process of up gradation to SDH.<br />
Referral Hospitals: There are 55 referral Hospitals. These referral hospitals get patient from PHCs, APHCs<br />
and are covered by specialised services.<br />
Block PHCs: At present there are 398 PHCs, 135 new PHCs are under construction and will be<br />
operationalised by this year. 73 Adll PHCs will also be upgraded to PHCs. These PHCs require to be<br />
upgraded at CHC level for specialised Services.<br />
Adll PHCs: The total no. of Adll PHC is 1243. These adll PHCs only provide OPD services. All these PHCs<br />
require to functionalise the inpatient for providing deliver services and reduce the load of Block PHCs.<br />
HSCs: At present there are 8858 HSCs in the state. Half of the HSCs are running from the rented place or<br />
Panchayat office. Mostly these HSCs are manned by one ANM only.<br />
Infection Management and Environmental Plan:<br />
Bio medical waste management has emerged as a critical and important function within the ambit of<br />
providing quality healthcare in the country. It is now considered an important issue of environment and<br />
occupational safety. As per the Bio-Medical Waste (Management & Handling) Rules, 1998, all the waste<br />
generated in the hospital has to be managed by the occupier in a proper scientific manner. The GoI has also<br />
issued the IMEP guidelines for SCs, PHCs and CHCs. The state is in the process of outsourcing the Biomedical<br />
Waste Management system for all the hospitals.<br />
4.7 Human Resource Development including Training<br />
Human Resource Development forms one of the key components of the overall architectural corrections<br />
envisaged by both the RCH II and NRHM programs. The Government of Bihar also has spelt out the same as<br />
the number one priority. However the implementation of this vision has been fraught with various obstacles.<br />
Though the state has reasonable number of MBBS doctors, there is an acute shortage of specialized medical<br />
manpower. The shortage of specialists like obstetricians and Anesthetists are obstructing the state plans to<br />
operationalise all district hospitals as First Referral Units. The available specialists in the state cadre is<br />
45
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
concentrated at the state Referral Hospital and hence the same handle bulk of the institutional deliveries state<br />
wide and is the only center capable of providing comprehensive emergency obstetric care services. In 2008-<br />
09, there has been a continuous focus on the capacity building of the existing manpower in the state.<br />
Trainings as per GoI guidelines on Immunization, IMNCI, EmOC, LSAS, SBA and Minilap/MVA etc have<br />
been taken up with full vigour. It is proposed to continue these trainings in 2009-10. In addition, the state<br />
wide training on Immunization for Medical Officers, IPC skills for Breast feeding and basic training of<br />
neonatal resuscitation-shall also be taken up for various levels. (Details of training plan and Budget is given<br />
in the annexure)<br />
4.8 Inequity/ Gender; Vulnerable Groups Including Urban Slums & Tribal<br />
4.8.1 Inequity and Gender<br />
Ensuring Gender Equity<br />
One of the broad indicators for measuring gender disparity is the sex ratio. The sex ratio in Bihar is<br />
unfavorable to women. Analysis of other indicators on the basis of gender reveals widening gaps between the<br />
sexes. While NMR for females is marginally higher than that of males, it widens further for the IMR, and<br />
even further for the under-five Mortality Rate. In conditions of absolute poverty, where resources to food and<br />
health care are severely limited, preference is given to the male child, resulting in higher female malnutrition,<br />
morbidity and mortality.<br />
Gender discrimination continues throughout the life cycle, as well. Women are denied access to education,<br />
health care and nutrition. While the state's literacy rate is 47.5%, that for women in rural areas is as low as<br />
30.03%. Abysmally low literacy levels, particularly among women in the marginalised sections of society<br />
have a major impact on the health and well being of families. Low literacy rate impacts on the age of<br />
marriage. The demand pattern for health services is also low in the poor and less literate sections of society.<br />
Women in the reproductive age group, have little control over their fertility, for want of knowledge of family<br />
planning methods, lack of access to contraceptive services and male control over decisions to limit family<br />
size. According to NFHS data, for 13% of the births, the mothers did not want the pregnancy at all. Even<br />
where family planning methods are adopted, these remain primarily the concern of women, and female<br />
sterilization accounts for 19% of FP methods used as against male sterilization, which is as low as 1%. In<br />
terms of nutritional status too, a large proportion of women in Bihar suffers from moderate to severe<br />
malnutrition. Anemia is a serious problem among women in every population group in the state, with<br />
prevalence ranging from 50% to 87% and is more acute for pregnant women.<br />
46
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
In all the programmes efforts will be made to meet the needs of vulnerable groups and ensure equity. Gender<br />
sensitization shall be made part of each training. The monitoring system too will be geared for this so that we<br />
may get disaggregated data.<br />
The state of Bihar is implementing the PC- PNDT Act at right earnest. The MOs are being trained by the<br />
<strong>State</strong> Health and Family Welfare Institute. The Civil Surgeons are the nodal person in the district in this<br />
regard. However monitoring of the activity still a big problem and require to improve. The state has<br />
procedures for registering the diagnostic centres and hospitals which comply these institutes to follow the<br />
PC-PNDT Act.<br />
4.8.2 Urban Slums<br />
Urban health care has been found wanting for quite a number of years in view of the fast of urbanization<br />
leading to growth of slums and population as more emphasis is given in rural areas. Most of the Cities and<br />
Towns of Bihar have suffered due to lack of adequate primary health care delivery especially in the field of<br />
family planning and child health services.<br />
At present, there are 12 Urban Health Centres (UHC) in the state. However, as per the GoI guidelines, there<br />
should be one UHC for 50,000 population (outpatient). The Urban Health Centres should provide services of<br />
Maternal Health, Child Health and Family Planning and especially cater to the Urban slums. The<br />
infrastructure condition of the existing Urban Health Centres is not up to the mark and requires some major<br />
renovation work. The staff at each UHC should comprise of 1 Medical Officer (MO), 1 PHN/LHV, 2 ANMs,<br />
1 Lab Assistant and 1 Staff clerk with computer skills.<br />
4.9 Logistics<br />
Validation of equipments and drugs procurement is within the domain of state level decision making. The<br />
Districts generally purchase the requirements and distributed to the other Health institutes mostly Block<br />
PHCs. However stock out of drugs still a problem for concern and require insurability of drug availability in<br />
the health institutes.<br />
There is provision of contingency funds for emergency drugs at the district level and health facilities.<br />
Whenever PHCs/PHSCs run out of drugs, medicines are purchased through contingency fund and supplied to<br />
the PHCs/PHSCs. The general impression is supplies arrive too late and too little. However under NRHM<br />
there is scope for huge and rapid flow of materials from the MOHFW, GOI and the <strong>State</strong> level. Also under<br />
the decentralization process the CHC, PHCs and HSCs will have larger autonomy to purchase drugs and<br />
47
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
supplies locally as per procurement guidelines to be developed by the <strong>State</strong> Government under the NRHM.<br />
District and the peripheral institutions need to be strengthened through capacity building for enhancing their<br />
capabilities of indenting, procurement, inventory management and distribution of drugs and supplies and<br />
maintenance of medical equipment and transport.<br />
Cold Chain Vans are available in the districts for distribution of Vaccines to PHCs/ HSCs during vaccination<br />
programs and camps. Generally PHC vehicles are used to collect the drugs and supplies from the district<br />
store. Currently local purchase of drugs and supplies are not approved.<br />
Drugs, consumables, and vaccines are directly supplied by the state to districts for HSCs, PHCs and other<br />
facilities very irregularly. There is need to streamline the process for estimation and indenting of vaccines,<br />
drugs and supply of consumables. The supply system would ensure smooth flow of indented materials as per<br />
guidelines from state to all levels of utilization.<br />
A big leap has been taken in 2008-09 in the field of Procurement concerning Maternal and Child Health<br />
equipments and drugs. One of the key achievements has been the finalization of rate contracting for the state<br />
owned 26 Sick Newborn Care Unit, 533 Neonatal Stabilization Units and essential equipment for<br />
strengthening the labour rooms of the state hospitals. In addition, rate contracting of some important drugs<br />
like Misoprostol has also been ensured.<br />
4.10 HMIS and Monitoring & Evaluation<br />
The National Rural Health Mission has been launched with the aim to provide effective health care to rural<br />
population. The programme seeks to decentralize with adequate devolution of powers and delegation of<br />
responsibilities has to have an appropriate implementation mechanism that is accountable.<br />
In order to facilitate this process the NRHM has proposed a structure right from the village to the national<br />
levels with details on key functions and financial powers. To capacitate the effective delivery of the<br />
programme there is a need proper a proper HMIS system<br />
Regular monitoring, timely review of the NRHM activities should be carried out. The quality of MIES in<br />
<strong>State</strong> HQ and in districts is very poor. Reporting and recording of RCH formats (Plan and monthly<br />
reporting) are irregular, incomplete, and inconsistent and few districts are not reporting at all. Formats are<br />
not filled up completely at the sub center level. There information is not properly reviewed at the PHC level.<br />
No feedback is provided upon that information.<br />
For overall management of the programme, there is a Mission Directorate and a <strong>State</strong> Programme<br />
Management Unit in the state. The Unit is responsible for overall monitoring and evaluation of the<br />
48
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
programme in the state and the districts. The data gathering is being facilitated by the <strong>State</strong>, District and PHC<br />
Data Centres. The numerous formats being used have been reviewed and it is found that data needs to be<br />
compiled only as per RCH, NRHM programme and <strong>State</strong> needs. Hence the new MIES formats have been<br />
shared with all the health functionaries and it is expected that they shall be reporting in the new formats from<br />
the 3 rd quarter.<br />
At district level, there is a District Health Society who will be responsible for the data dissemination from the<br />
sub-district level to the district level. Data Manager/HMIS expert at the <strong>State</strong> level and Data Assistant at the<br />
district level will be responsible for management of HMIS.<br />
As such, there is a Monitoring Team constituted each at state and district level to monitor the implementation<br />
of the NRHM activities. The Team comprises of representatives from the Mission Directorate and<br />
Programme Committee for various health programmes. The Team also comprises of representatives from<br />
Govt. of India.<br />
There is a Hospital Management Committee/Rogi Kalyan Samiti at all PHCs and CHCs. The PHC / CHC<br />
Health Committee will monitor the performance of HSC under their jurisdiction and will submit the report<br />
and evaluate the HSC performance, and will be submitted to the District, which will compile and sent it to<br />
the <strong>State</strong>.<br />
4.11 Behaviour Change Communication<br />
The state does not have any comprehensive BCC strategy. All the programme officers implement the BCC<br />
activity as per their respective programmes.<br />
The IEC logistic is designed, developed and procured at the district level and distributed to the PHC in an ad<br />
hoc manner. However some activity is done at the state level.<br />
There is no credible study available to identify the areas / region specific knowledge, attitudes and practices<br />
pertaining to various focus areas of interventions like breast feeding, community & family practice regarding<br />
handling of infants, ARSH issues etc. At present there is no impact assessment of the IEC and BCC<br />
activities. Its very important to assess the impact of IEC/BCC activities, resources and methods to undertake<br />
mid way corrective measures.<br />
4.12 Convergence/Coordination<br />
Convergence with ICDS has been taken care of to cover immunization and ANC Service. ASHA, AWW and<br />
ANMs together hold monthly meetings with Mahila Mandals under MUSKAAN Programme. Government<br />
of Bihar has decided to merge Village Health and Sanitation Committee with Lok Swasthya Pariwar<br />
Kalyan and Gramin Swaschata Samiti constituted by Department of Panchayat Raj in Bihar. The PHED has<br />
49
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
been entrusted to train ASHAs as per GoI norm. Adolescent councilors are placed in each district from <strong>State</strong><br />
AIDS Control Society. The Health department is looking to cooperate with them by giving training to these<br />
councilors for implementing ARSH programme. The <strong>State</strong> PWD Department has taken care of the<br />
construction of Health Department. All the construction activity for Health Institutions under NRHM has<br />
already been handed over to the PWD department.<br />
4.13 Finance<br />
In 2008-09 the GoI had approved an amount of Rs. 978.61.47 Crores under RCH II.<br />
50
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
5. Progress and Lessons learnt from RCH II Implementation of 05-08<br />
5.1 Major achievements during 2005-09<br />
1. SHSB at <strong>State</strong> level and District Health Societies (in all 38 districts) formed & registered.<br />
2. ASHA: A total of 67506 ASHAs selected against the total revised target of 87,135.<br />
3. SPMU & DPM: The <strong>State</strong> Level consultants in SHSB and DPMU staff (3 in each district) have been<br />
recruited in 34 out of 38 districts. The orientation training for all has been completed.<br />
4. Free drug distribution of essential drugs started from 1st July 2006 and 24 hours presence of doctors<br />
ensured in all facilities up to PHC level resulting in unprecedented increase in OPD patients. 10-30<br />
times increase has been reported. Free drug list has been expanded to incorporate 33 OPD and 75<br />
IPD at MCH, 33 OPD and 107 IPD drugs at DH and 33 OPD and 37 drugs IPD at PHC.<br />
5. Routine Immunization: Full immunization percentage increased to 41.4% (DLHS). Use of AD<br />
Syringe increased to 95%.<br />
6. Against a total figure of 11000 posts of ANM (R), appointment of ANM (R) - 5800 posts of<br />
ANM(R) have been filled up.5200 new appointments have to be made.<br />
7. Rogi Kalyan Samitis formed in all health facilities till PHC level, registration of RKS completed rest<br />
in progress, so far 470 RKS have been registered.<br />
8. Training Programmes: Training of EmOC, Life Saving Anesthesia Training, IMNCI, ASHA,<br />
DPMUs, SBA training, Immunization and Neonatal resuscitation started. This includes the regular<br />
monitoring and corrective actions taken.<br />
9. ANM/GNM training Schools-Out of 22 ANM schools and 6 GNM schools, 20 ANM schools were<br />
restarted after a period of more than a decade. Currently approx. 600 students enrolled. In year 2009,<br />
it is being ensured that ANM and GNM schools train students up to their optimum capacity. Besides,<br />
efforts have been made to strengthen the overall structure of these schools in the state.<br />
10. Institutional delivery has increased manifold as evident from the bar diagram below-<br />
1000000<br />
900000<br />
800000<br />
700000<br />
600000<br />
500000<br />
400000<br />
300000<br />
200000<br />
100000<br />
0<br />
117062<br />
838481<br />
902667<br />
2006-07 2007-08 2008-09(till -Dec<br />
08)<br />
Series1<br />
51
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
11. Additionally in the year 2009-10, rate contracting of equipments for Child (SNCU & NSU) and<br />
Maternal Health (Labour room) for District, Sub-Divisional, CHC and PHC hospitals has been<br />
achieved, which will pave the way for procurement and availability of the same in the Districts.<br />
The <strong>State</strong> Programme Implementation Plan 2009-10 has been framed on the basis of strategies and activities<br />
which worked in last three years. The major bottlenecks have been identified and an attempt has been made<br />
to overcome them through alternative strategies.<br />
5.2 Programme Management<br />
Some of the things which didn't work in last three years are:-<br />
i. Construction & Renovation- Slow progress in Infrastructure<br />
ii. BCC strategy formulation.<br />
iii. High turnover of personnel in programmes.<br />
iv. The quality of training.<br />
v. Keeping up the motivational level of health staff at all levels.<br />
vi. Utilization of trained staff (It is sub optimal now).<br />
vii. Mismatch of personnel and equipment.<br />
viii. Lack of Proper monitoring and evaluation framework.<br />
ix. Quality issues in critical care services (timely use of referral transport by pregnant women,<br />
utilization of EmOC trained doctors )<br />
x. Acceptance of Private Partners t the district level<br />
Following strategies have been adopted to overcome the problem<br />
‣ Slow progress in infrastructure - To overcome the problem of slow progress in infrastructure, a<br />
separate infrastructure cell has been created in <strong>State</strong> Health Society, Bihar. This year, it is proposed<br />
that two more personnel may be added to this wing to strengthen it. Moreover all the DMs have been<br />
requested to designate an agency for their district that would carry out all infrastructure-related tasks.<br />
‣ Procurement of Equipment- Though essential drugs have been rate contracted so far, the rate contract<br />
of various equipments needed for carrying out RCH activities are still to be completed. Idea of a<br />
TNMSC model of Corporation is also taking shape in the Department to solve the logistic and<br />
procurement problem.<br />
‣ BCC strategy formulation- Even after two and half years of NRHM, Bihar lacks a consolidated BCC<br />
strategy in health due to lack of technical know how. Besides, some other initiatives are planned this<br />
year in areas like promotion of Breast feeding, PNDT and ARSH among others.<br />
52
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
‣ Quality Assurance committees in <strong>State</strong> and Districts- Quality assurance committees formed in 80 %<br />
of the districts as per Quality Assurance Manual of GoI and in rest of the districts, it will be formed<br />
by 2009 March end. <strong>State</strong> Quality Assurance Cell has been formed. Quarterly monitoring visits are<br />
planned at the state level and the divisional level to monitor quality of trainings and critical services<br />
including family planning.<br />
‣ Recruitment of Medical officers and paramedics- The process of recruitment is lengthy and takes<br />
about 04-06 months. The number of applicants is quite limited because of dearth of doctors and<br />
paramedics in the state. Moreover the consolidate remuneration is not lucrative enough. Hence from<br />
the previous year incentive for rural postings and specialist services have been provided in the S<strong>PIP</strong>.<br />
Similarly for ANMs, mobile phone facilities for all ANMs are being provided.<br />
‣ High turnover of Personnel- It is felt that the state needs to restrict the turnover of doctors on<br />
contract and also programme managers. It is proposed that a study may be undertaken to assess the<br />
situation and recommend remedies, however it is assumed that rural and specialist bonus will help to<br />
curb the turnover to same extent.<br />
‣ Quality of training - Monitoring cell has been constituted at the state level in <strong>State</strong> Institute of Health<br />
& Family Welfare. The trainings are being monitored at regular intervals.<br />
‣ Low motivational level of health staff - The motivational level of health staff at all levels is low.<br />
Continuous communication and feedback by state level programme officers is being done.<br />
‣ Sub optimal utilization of trained staff Regular evaluation and monitoring is being done and<br />
corrective steps are being taken. Placement of trained people at such facilities where infrastructure is<br />
in place. E.g. The government has taken up on priority the placement of the trained EMoC and LSAS<br />
doctors to the FRUs where there is no such facility. Poor monitoring and evaluation framework <br />
Regular monitoring visits by programme officers.<br />
‣ Pilot initiatives in two districts In 2009-10 Maternal and perinatal death enquiry and response is<br />
being initiated in two districts (Kishanganj and Jehanabad). In these districts referral transport money<br />
for JBSY is being linked for payment of referral transport arranged by the pregnant woman through<br />
PHC staff. as a pilot initiative. EmOc services, MTP services, Maternity complex, Newborn corner<br />
are also being strengthened in these two districts in intensive manner. Data collection on maternal<br />
and perinatal death will be done before and after the intervention. If the data collected after the<br />
intervention shows decline in MMR and IMR then the model will be replicated throughout the <strong>State</strong>.<br />
53
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
6. RCH II Programme Objectives and Strategies<br />
6.1 Vision <strong>State</strong>ment:<br />
The NRHM seeks to provide universal access to equitable, affordable and quality health care which is<br />
uncountable at the same time responsive to the needs of the people, reduction of child and maternal deaths as<br />
well as population stabilisation, gender and demographic balance in this process. The mission would help<br />
achieve goals set under the National Rural Health Policy and the Millennium Development Goals. To<br />
achieve these goals NRHM will:<br />
· Facilitate increased access and utilization of quality health services by all.<br />
· Forge a partnership between the Central, state and the local governments.<br />
· Set up a platform for involving the Panchayati Raj institutions and community in the management<br />
of primary health programmes and infrastructure.<br />
· Provide an opportunity for promoting equity and social justice.<br />
· Establish a mechanism to provide flexibility to the states and the community to promote local<br />
initiatives.<br />
· Develop a framework for promoting inter-sectoral convergence for promotive and preventive health<br />
care.<br />
54
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
6.2 Technical Objectives, Strategies and Activities<br />
1 Maternal Health<br />
Goals: Reduce MMR from present level 371 (SRS 2001-03) to less than 100<br />
Objectives:<br />
1. To increase 3 ANC coverage from 26.4% to 45% by 2009-10 and to 75% by 2010-11. (DLHS3)<br />
2. To increase the consumption of IFA tablets for 90 days from present level of 9.7% to 20% by 2009-10 and<br />
to 35% by 2010-11. (DLHS-3)<br />
3. To reduce anemia among pregnant mothers from 60.2% to 52% by 2009-10 and to 40% by 2010-11.<br />
4. To increase institutional delivery from 70% to 76% by 2009-10 and to 85% by 2010-11 (MIS data)<br />
5. To increase birth assisted by trained health personnel from 31.9% to 45%. (DLHS-3).<br />
6. To increase the coverage of Post Natal Care from 26% to 40% by 2009-10 and to 55% by 2010-11.<br />
(DLHS-3).<br />
7. To reduce incidence of RTI/STI cases<br />
8. To reduce the no of unsafe abortions<br />
Source of data: DLHS 3, NFHS 3 and MIS Data<br />
Objective No. 1: To increase 3 ANC coverage from 26.4% to 45% by 2009-10 and to 75% by<br />
2010-11.<br />
Strategies and Activities:<br />
1.1. Institutionalization of Village Health and Nutrition Days (VHND)<br />
1.1.1 In collaboration with ICDS, such that the Take Home Ration (THR) distribution and ANC Happens on<br />
the same day<br />
1.1.2 This will require minor changes in the microplans of Health and ICDS<br />
1.1.3 Policy decision and appropriate guideline under convergence between Health and ICDS need to happen<br />
as a priority<br />
1.2 Improved Access of ANC Care<br />
1.2.1 Provision for Additional ANMs in each Sub Centres (Refresher Training to ANMs on Full ANC to<br />
improve the quality of ANC)<br />
1.2.2 Setting up of New Sub Centres to cover more areas<br />
55
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
1.2.3 Micro planning: Identifying vulnerable groups, left out areas and communities having high percentages<br />
of BPL under each block and incorporating the same into the block micro plans to focus attention on them<br />
for providing Community and Home based ANC to them.<br />
1.2.4 Organizing Monthly Village Health and Nutrition Days in each Aaganwadi Centres<br />
1.2.5 Organizing RCH camp in Each Block PHC areas.<br />
1.2.6 Tracking of Pregnant mothers by ASHAs<br />
1.3 Ensure quality service and Monitoring of ANC Care<br />
1.3.1 Strengthen the monitoring system by checking of ANMs duty rooster and visits of LHVs and MOs.<br />
1.3.2 Involvement of PRIs in monitoring the ANMs service through convergence<br />
1.3.3 Refresher training of ANMs on ANC care<br />
1.3.4 Proper maintenance of ANC Register and Eligible couple register<br />
1.4 Strengthening of Health Sub Centres<br />
1.4.1 Repair and Renovation of Sub Centres<br />
1.4.2 Provide equipments like BP Apparatus, Weighing machines, Heamoglobinometer etc to the Sub<br />
Centers.<br />
1.4.3 Timely supply of Drug Kit A and Kit B<br />
1.5 Generate Awareness for ANC Service<br />
1.5.1 Convergences meeting with AWWs, ASHAs, PRI Members, NGOs at the Gram Panchayat level by<br />
ANMs. These meetings will also attended by MOs from Adll PHCs.<br />
1.5.2 Tracking of Pregnant mothers by ASHA, ANM and AWWs though organizing Mahila Mandals<br />
meeting. Incentive for ASHAs and ANMs to give for the initiative. This initiative is under MUSKAAN<br />
Programme. Incentive for ASHA will be taken care under Intersectoral Convergence.<br />
1.5.3 Counseling by ASHAs and ANMs to the pregnant mothers, mothers and Mother in Laws.<br />
Objective No. 2: To increase the consumption of IFA tablets for 90 days from present level of 9.7% to 20%<br />
by 2009-10 and to 35% by 2010-11. (DLHS-3)<br />
Strategies and Activities:<br />
2.1 Purchase and Supply of IFA Tablets<br />
2.1.1To include IFA under essential drug list<br />
2.1.2 Timely supply of IFA Tablets to the Health Institutions ( Ensuring no stock out of IFA at every level<br />
down to Sub-Centre Level)<br />
2.1.3 District to purchase IFA tablets in the case of stock out<br />
2.1.4 Convergence with ICDS and Education for regular supply of IFA tablets through AWWCs And<br />
Schools for the pregnant and lactating women, children 1-3 years and adolescent girls<br />
2.2 Awareness generation for consumption of IFA Tablets<br />
56
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
2.2.1 Pregnant mothers will be made aware for consumption of IFA tablets for 90 days<br />
2.2.2 ASHA and AWWs will generate awareness along with ANMs at the Village level<br />
2.2.3 Ensure utilizing the platform of Mahila Mandal meetings being held every third Wednesday<br />
Objective No.3: To reduce anemia among pregnant mothers from 60.2% to 52% by 2009-10 and to 40% by<br />
2010-11.<br />
3.1 Supplementing IFA tablets consumption with other clinical strategies.<br />
3.1.1 Half yearly de-worming of all adolescent girls.<br />
3.1.2 Training of ANM, AWW and ASHA on module on EDPT (Early Diagnosis and Prompt Treatment) of<br />
anemia.<br />
3.1.3 Activities for consumption of IFA tablets as per Objective No. 2<br />
3.2 Other strategies<br />
3.2.1 Refer severely Anemic Pregnant Mothers to referral centers<br />
3.2.2 IPC based IEC campaigns emphasizing on consumption of locally available iron rich foodstuff.<br />
Details given under Special Scheme on Anemia Control in Part B<br />
Objective No. 4: To increase institutional delivery from 70% to 76% by 2009-10 and to 85% by 2010-11<br />
(MIS data) and to increase facilities for Emergency Obstetric Care (EmOC)<br />
Strategies and Activities:<br />
The strategies will lead to up gradation and operationalization of the facilities to increase institutional<br />
deliveries along with providing EmOC and emergency care of sick children. These facilities will also provide<br />
entire range of Family Planning Services, safe MTPs, and RTI/STI Services.<br />
4.1 Upgrading Block PHCs/CHCs in to FRUs<br />
4.1.1 Provision of OT and lab facility by upgrading 76 FRUs<br />
4.1.2 Blood Bank and or Provision of Blood storage, OT and lab facility by upgrading 76 FRUs<br />
1. All district hospitals must have either its own Blood Bank, operational round the clock, or must have<br />
access to one that can be accessed in less than 30 minutes<br />
2. All CHC / PHCs have blood storage facility<br />
4.1.3 Training of MOs on Obs & Gynae and Anesthesia<br />
1. 18-week Life Saving Anesthetic Skills (LSAS) training for MBBS Doctors<br />
2. 16 week -Emergency Obstetric Skill training for MBBS doctors<br />
3. 3 days training of doctors and nurses posted at FRUs for the neonatal stabilization unit<br />
4.1.4 Repair and renovations of FRUs<br />
4.1.5 Appointment of Anesthetist, O&G specialist, Staff Nurses at the FRUs<br />
57
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
4.1.6 Incentivise the conduct of C section at FRUs @ Rs 1500 per C section for the staff involved at the<br />
FRUs.<br />
4.1.7 Accreditation of FRUs<br />
4.2 Operationalization of 24x7 facilities at the PHC level<br />
4.2.1 Training of MOs and Staff Nurses of PHCs in BEmOC<br />
4.2.2 Appointment of at least 3 Staff Nurse in each PHCs<br />
4.2.3 Repair and renovation of PHCs<br />
4.2.5 Availability of and timely supply of medical supplies and DDK & SBA kits<br />
4.2.5 Training of MOs, Staff Nurses on SBA<br />
4.3 Increase beneficiary choice for institutional delivery through IEC campaign complimented by network of<br />
link workers working on incentive basis for each institutional delivery achieved<br />
4.3.1 Strengthening JBSY Scheme<br />
1. Improving quality: Infrastructural support to high burden facilities to avoid early discharge<br />
following institutional deliveries<br />
2. Mapping of high burden facilities and proving them support for matching infrastructural up<br />
gradation to increase the hospital stay following delivery<br />
3. Identifying districts and blocks and communities within them, where the awareness and reach of<br />
JBSY scheme is poor and to ensure increased service utilization in these areas<br />
4.3.2 Design and implement an IEC campaign focusing on communicating the benefits of institutional<br />
delivery and benefits under JBSY scheme.<br />
4.3.3 Equip the ASHA network to reinforce the IEC messages through IPC interventions at village /<br />
community level.<br />
4.3.4 Provide incentives to ASHA for every institutional delivery achieved in her village / designated area.<br />
4.3.5 Involvement of PRIs for JBSY scheme to monitor and generate awareness for institutional delivery.<br />
4.4 Provision of Referral Support system<br />
4.4.1 Provision of a dedicated referral transport system for the newborns and pregnant women to refer them<br />
from home/HSCs/PHCs to referral centers.<br />
4.4.2 Monitoring of referral transport system<br />
4.4.3 Development of proper referral system between Health Institutions.<br />
4.4.4.Operationalising of Blood Storage Units in 76 FRUs<br />
58
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Lack of Blood Storage Units in the state make things complicated during emergency hence in 76 FRUs blood<br />
storage units has been proposed. Operationalising of at least one Blood Storage Units in 76 FRUs is proposed<br />
as per IPHS guidelines.<br />
Particulars Qty. Rate (Rs.) Months Amount<br />
Sl.<br />
(3x4x5=6)<br />
1 2 3 4 5 6<br />
1 Salary of One Medical Officer 76 20,000/- pm 12 1,82,40,000/-<br />
2 Salary of 3 Lab Technician @ Rs. 6500/- 228 6,500/- pm<br />
1,77,84,000/-<br />
12<br />
pm<br />
3 Diesel 76 5,000/- pm 12 45,60,000/-<br />
4 Service and Maintenance Charge 76 5,000/- pm 12 45,60,000/-<br />
5 Misc. and Others 76 2,000/-pm 12 18,24,000/-<br />
Total Operational Cost 4,69,68,000/-<br />
Objective No.5: To increase birth assisted by trained health personnel from 31.9% to 45%. (DLHS-3).<br />
Strategies and Activities:<br />
5.1 Ensure safe delivery at Home<br />
5.1.1 Provision of Disposable delivery kits with ANMs and LHVs - Establishing full proof Supply Chain of<br />
the DD Kits<br />
5.1.2 Training of ANMs on SBA<br />
1. Providing SBA with approved drug kits, in order to deal with emergencies, like post-partum<br />
hemorrhage, eclempsia, and puerperal sepsis<br />
2. Ensuring regular supply of these drugs to the SBA<br />
5.1.3 Supply of adequate DD Kits to ANMs, LHVs.<br />
5.2 Provision of delivery at HSC level<br />
5.2.1 Supply of DDkits to HSCs<br />
5.2.2 Delivery tables to be provided to the HSCs<br />
Objective No.6: To increase the coverage of Post Natal Care from 26% to 40% by 2009-10 and to 55% by<br />
2010-11. (DLHS-3).<br />
Strategies and Activities<br />
59
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
6.1 Ensuring proper practice of PNC services and follows ups at the health facility level.<br />
6.1.1 Refresher sessions for all ANMs on uniform guidelines to be followed for PNC care all delivery cases<br />
to remain at facility for minimum 6 hours after normal delivery and to be recalled to facility for check up<br />
with 4 days and after 42 days.<br />
6.1.2 Ensuring follow up PNC care through out reach services (ANM) for delivery cases where the patient<br />
does not return to facility for follow up check ups.<br />
6.1.3 Referral of all complicated PNC cases to FRU level.<br />
6.1.4 LHV and MO to monitor and report on PNC coverage during their field visits<br />
6.2 Utilizing the ASHA network to strengthen the follow up of PNC services through tracking of cases,<br />
mobilization to facilities and providing IPC based education / counseling.<br />
6.2.1 Utilize ASHA to ensure 3 PNC visits by the ANM for home delivery cases (1 st within 2 days, 2 nd within<br />
4 days and 3 rd within 42 days of delivery) and 2 follow up visits for institutional delivery cases.<br />
6.2.2 Counseling of all pregnant women on ANC and PNC during monthly meetings of MSS and during<br />
VHND.<br />
6.2.3 Linking of ASHAs incentives on institutional deliveries to completion of the PNC follow-ups.<br />
6.3 Basis Orientation of AWWs on identifying Post-partum and neonatal danger signs during her scheduled<br />
visits following delivery<br />
6.3.1 Basic orientation on IMNCI in order to be able to alert the beneficiary and coordinate with ASHA<br />
and ANM (to avoid undue delay)<br />
6.3.2 Basic orientation on identifying post-partum danger signs, specially, for home based deliveries, such<br />
that the she can alert ASHA, ANM or the local PHC towards avoiding undue delay<br />
Objective No. 7: Reduce incidence of RTI/STI<br />
Strategies and Activities<br />
7.1 Ensuring early detection through regular screenings and contact surveillance strategies.<br />
7.1.1 Early diagnosis of RTI / STI through early detection of potential cases through syndromic approach and<br />
referral by ANM and ASHA.<br />
7.1.2 Conducting VDRL test for all pregnant women as a part of ANC services.<br />
7.1.3 Implementing contact surveillance of at risk groups in convergence with Bihar AIDS Control Society.<br />
7.2 Strengthening the infrastructure, service delivery mechanism and capacity of field level staff for handling<br />
of RTI / STI cases.<br />
7.2.1 Conducting community level RTI / STI clinics at PHCs<br />
60
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
7.2.2 Training to all MOs at PHC / DH level in Management of RTI / STI cases in coordination with Bihar<br />
AIDS control Society.<br />
7.2.3 Training of frontline staff, LHV, ANM and ASHA in identifying suspected cases of RTI / STI in<br />
coordination with Bihar AIDS Control Society.<br />
7.2.4 Strengthening RTI / STI clinic of the District Hospitals<br />
Objective No. 8 Reduce incidence of unsafe abortion<br />
Strategies and activities<br />
8.1 Early diagnosis of pregnancy using Nischay pregnancy testing kits<br />
8.2 Counselling and proper referral for termination of pregnancy in 1st trimester if the woman wishes so<br />
8.2.1 Training of MOs and Nurses/LHV in MTP (MVA)<br />
8.2.2 Procurement and availability of MVA at the designated facilities.<br />
61
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
2. Child Health<br />
Goal: Reduce IMR from 61 (SRS 2005) to less than 30<br />
Objectives:<br />
1. To reduce low birth weight babys by supplementing nutritional support to pregnant mothers<br />
2. To increase exclusive breast feeding from 38.4% to 50% by 2009-10 and to 75% by 2010-11.<br />
3. To reduce incidence of underweight children (up to 3 years age) from 58.4% to 50% by 2009-10 and to<br />
40% by 2010-11.<br />
4. To strengthen neonatal care services in all PHCs/CHCs/SDHs by setting newborn care centers & having<br />
trained manpower therein.<br />
5. To reduce the prevalence of anaemia among children from 87.6% to 77% by 2008-09 and to 60% by 2009-<br />
10.<br />
6. To increase full immunization of Children from 41.4%% to 60% by 2009-10 and then to 70% by 2010-11.<br />
7. To reduce morbidity and mortality among infants due to diarrheoa and ARI<br />
Objective No.1: To reduce low birth weight babys by supplementing nutritional support to pregnant mothers<br />
Strategies and Activities:<br />
1.1 Convergence with ICDS, supplementary diet which is being given by AWW to pregnant mothers may be<br />
improved.<br />
1.1.1 A supplementary diet comprising of rice, dal and ghee will be provided to all pregnant women. This<br />
will be given for the last 3 months to all underweight pregnant BPL mothers. The Scheme will be<br />
implemented in convergence with ICDS.<br />
1.1.2 Joint Monitoring by Block MO i/cs with CDPO for implementation of the scheme.<br />
Objective No. 2: To increase exclusive breast feeding from 27.9% to 35% by 2008-09 and to 50% by 2009-<br />
10<br />
Strategies and Activities:<br />
2.1 Use mass media (particularly radio) to promote breastfeeding immediately after birth (colostrum feeding)<br />
and exclusively till 6 months of age.<br />
2.1.1 Production and broadcast of radio spots, jingles, folk songs and plays promoting importance of correct<br />
breastfeeding practices<br />
2.1.2 Production and broadcast of TV advertisements and plays on correct breastfeeding practices<br />
62
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
2.1.3 Publication of newspaper advertisements, booklets and stories on correct breastfeeding practices<br />
2.2 Increase community awareness about correct breastfeeding practices through traditional media<br />
2.2.2 Involve frontline Health workers, Aaganwadi Workers, PRIs, TBAs, local NGOs and CBOs in<br />
promoting correct breastfeeding and complementary feeding through IPC, group meetings, folk media and<br />
wall writing.<br />
2.2.3 Educate adolescent girls about correct breastfeeding and complementary feeding practices through<br />
school -based awareness campaign.<br />
3. To reduce incidence of underweight children (up to 3 years age) from 58.4% to 50% by 2008-09 and to<br />
40% by 2009-10<br />
Strategies and Activities:<br />
3.1. Growth monitoring of each child<br />
3.1.1 Supply of spring type weighing machine and growth recording charts to all ASHAs, AWWs. All<br />
ASHAs, Aaganwadi centers and sub centers will have a weighing machine and enough supply of growth<br />
recording charts for monitoring the weight of all children through Untied fund of S/Cs.<br />
3.1.1 Weighing and filling up monitoring chart for each child (0-6 years) every month during VHNDs<br />
Each child in the village will be monitored by weight and height and records will be maintained<br />
3.2 Referral for supplementary nutrition and medical care<br />
3.2.1 Training for indications of growth faltering and SOPs for referral to AWWC for nutrition<br />
supplementation and to PHC for medical care.<br />
3.2.2 Establishment of 10 Nutrition Rehabilitation Centres in Districts having severe problems of<br />
malnutrition and continue of 8 existing Centres (A Special Scheme taken up and put under NRHM B)<br />
Objective No.4: To strengthen neonatal care services in all PHCs/CHCs/SDHs by setting newborn care<br />
centers & having trained manpower therein.<br />
Strategies and Activities:<br />
4.1. Strengthen institutional facilities for provision of new born care<br />
4.1.1. It is planned to develop a model for comprehensive care of the newborn at all levels, from state to the<br />
community level.<br />
63
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
MODEL FOR COMPREHENSIVE CARE OF NEWBORN<br />
District Level<br />
Neonatal Stabilization Unit<br />
PHC Level<br />
Sick Newborn Care Unit (level 2)<br />
Village Level<br />
IMNCI trained worker, community initiatives (BCC<br />
approaches, involving PRI, Self Help groups etc.)<br />
Level Facility Services/Activities Training required Equipment<br />
1. District Level<br />
Near Level II Sick Newborn<br />
Care Unit ( (SNCU) to provide<br />
specialized care services to<br />
sick newborns<br />
2. PHC level<br />
Neonatal Stabilization Unit<br />
with basic care services in<br />
health facilities<br />
Special care of neonates 4 days training Equipment for<br />
SNCU and<br />
refurbishment.<br />
Delivery services<br />
Neonatal Resuscitation<br />
Warmth<br />
1 day training in<br />
essential newborn<br />
care<br />
Neonatal warmer<br />
Oxygen supply<br />
Ambu bag and<br />
Mask<br />
3. Village level<br />
IMNCI Trained workers in<br />
each village to provide<br />
essential child care and<br />
counseling services to<br />
community<br />
Post natal Visits, Counseling<br />
for breastfeeding and newborn<br />
care practices, immunization<br />
Timely identification,<br />
classification and treatment<br />
and referral, if needed<br />
8 days training in<br />
IMNCI<br />
IMNCI<br />
module<br />
Drug Kit<br />
training<br />
Plan of action:<br />
DISTRICT LEVEL: NEAR LEVEL II SICK NEWBORN CARE UNIT<br />
Neonatal mortality accounts for over 60% of Infant mortality. Further reduction in Infant and Child mortality<br />
is critically dependant upon significant decline in Newborn deaths. Although on average 41% of deliveries<br />
are conducted in the institutions, i.e., at P.H.C and district hospitals, there are no separate facilities to manage<br />
sick Neonates in the hospital and health centers, Even at district hospital, the sick Neonates (Home delivered<br />
and Institutional delivered) are generally treated along with the older sick children.<br />
64
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
It has been observed that near level II Neonatal care is<br />
· Needed for 15-20% of all the neonates<br />
· 5000 neonates need special care per million population per year<br />
· Need for 150 special care beds per million population<br />
Establishment of near leveI SNCU (sick newborn care unit) in 13 districts is proposed.<br />
REQUIREMENTS FOR ACCREDITATION<br />
1. Location of the SNCU:<br />
· Should be easily accessible from entrance of the hospital<br />
· Should not be located on top floor<br />
· For units catering both inborn and out born neonates: next to labor ward & delivery room<br />
· For units catering out born neonates only: near children ward<br />
2. Space Requirement:<br />
1200 sq ft area for a 12 bed near Level II SNCU @ 100 sq ft per patient of which:<br />
a. 50 sq ft would be patient care area and<br />
b. 50 sq ft would be added up for ancillary areas<br />
3. Equipments for individual patient care in the Sick Newborn Care Unit:<br />
Item<br />
Requirement for the unit<br />
1. Servo controlled radiant warmer 1 for each bed (essential) +2 Total=14<br />
2. Low reading digital thermometer (centigrade scale) 1 for each bed (essential) Total=14<br />
3. Neonatal stethoscope 1 for each bed (essential) Total=14<br />
4. Neonatal resuscitation kit: 1 set for each bed (essential) Total=14<br />
5. Electrically operated pressure controlled slow suction<br />
machine<br />
1 for 2 beds (essential)<br />
Total=7 (5 electrical, 2 foot operated)<br />
6. Oxygen hood (neonatal or infant size, unbreakable) 1 for each bed (essential) Total=14<br />
7. Non stretchable measuring tape (mm scale) 1 for each bed (essential) Total=14<br />
9. Infusion pump or syringe pump 1 for 2 beds (essential) Total=7<br />
10. Pulse oxymeter 1 for every two beds Total=7<br />
11. Double outlet oxygen concentrator 1 for every two beds Total=7<br />
65
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
12. Double sided blue light phototherapy 1 for every three beds Total=2<br />
13. Single side blue light phototherapy Total=3<br />
13. AC (1.5 ton) split 8<br />
14. Generator (15 KVA) 1<br />
4. Side Laboratory Equipments:<br />
Item<br />
Requirement for the unit<br />
Microscope with gram and Leishman staining facility 1 (essential)<br />
Microhematocrit centrifuge, capillary tubes and reader 1 (essential)<br />
Billirubinometer 1<br />
Multistix strips (in container) 1<br />
Glucometer with Dextrostix 3<br />
5. STAFF<br />
Manpower<br />
12 bed SNCU<br />
1. Pediatricians 2<br />
2. Medical Officer 4<br />
3. Sister-in-charge / PHN 1<br />
4. Staff Nurse 6<br />
5. ANMs 8<br />
6. Class IV 6<br />
6. Life Saving drugs for Emergency:<br />
This list is not exhaustive for an Emergency situation in any Sick Newborn Care Unit<br />
Item<br />
· Injection adrenaline, naloxone,<br />
· sodium bicarbonate, aminophylline,<br />
phenobarbitone, hydrocortisone,<br />
Requirement for the unit<br />
A stock of 1 set per bed per month<br />
should always be maintained in the<br />
unit<br />
· 10% dextrose,<br />
· normal saline,<br />
· ampicillin with cloxacillin, ampicillin and<br />
cefotaxime and gentamycin etc<br />
66
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Support establishment of Neonatal Stabilization Units in select 100 high-mortality blocks with personnel and<br />
equipment for neonatal resuscitation, Postnatal Care, Healthy Newborn Care , 35-37 weeks gestation,<br />
Stabilize neonates < 35 weeks<br />
FACILITIES FOR PHC LEVEL: NEONATAL STABLIZATION UNIT<br />
NEONATAL STABILIZATION<br />
· Adequate warming through radiant heat source.<br />
· Facilities for Resuscitation with self inflating resuscitation bag and well fitting neonatal face masks<br />
(at least two sizes).<br />
· Medicines of essential newborn care<br />
1. Supply of bucket type / spring type weighing machines to all sub centres and Anganwadi centres<br />
Many times new borns and infants are not weighed or incorrectly weighed using adult type weighing<br />
machines which are usually available at sub centres and Anganwadi centres. Provision of bucket type or<br />
spring type weighing instruments will improve weight monitoring.<br />
2. Pediatrician will be appointed on contract basis @ Rs.26000 pm.<br />
3. Training of MOs on Paediatrics<br />
4. Training of MOs, Staff Nurses on Facility Based New Born care<br />
Training and operationalization cost will be borne by the UNICEF.<br />
GRASSROOT LEVEL IMNCI TRAINING<br />
Details as per Annexure<br />
4.2 Generation of awareness on new born and infant care (home-based) in community through MSS<br />
4.2.1 Community Awareness on home-based care of new born (skin-to-skin contact, bathing after a week,<br />
not removing vermix, etc.); early recognition of danger signs - ARI, diarrhoea; proper weaning practice<br />
The ASHAs / MPWs / AWWs at every point of contact for ANC and PNC will reinforce tenets of homebased<br />
care of new born as per IMNCI guidelines. The training will be part of IMNCI.<br />
5. To reduce the prevalence of Aneamia among children from 87.6% to 77% by 2008-09 and to 60% by<br />
2009-10.<br />
Strategies and Activities<br />
Details in special programme for Controlling Iron Deficiency Anemia in Bihar under Part B NRHM<br />
Additionalities.<br />
67
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
6. To increase full immunization of Children from 32.8% to 40% by 2008-09 and then to 60% by 2009-10.<br />
Strategies and Activities<br />
6.1 Conduct fixed day and fixed-site immunization sessions according to district micro plans.<br />
6.1.1 Fill vacant ANM posts and appoint additional ANMs in a phased manner to achieve GoI norm of one<br />
ANM for 5000 population by the year 2009-10.<br />
6.1.2 Update district micro plan for conducting routine immunization sessions<br />
6.1.3 Ensure timely and adequate supply of vaccines and essential consumables such as syringes, equipment<br />
for sterilization, Jaccha-Baccha immunization cards, and reporting formats at all levels.<br />
6.1.4 Supply AD Syringes to conduct outreach sessions in select areas.<br />
6.1.5 Enlist help of AWW/ASHA in identification of new-borne and follow-up with children to ensure full<br />
immunization during sessions. New born tracking system to be implemented<br />
6.1.6 Replace all Cold Chain equipment, which is condemned, or more than five years old in a phased<br />
manner by the year 2007-08 and supply new Cold Chain equipment based on analysis of actual need of the<br />
health facilities<br />
6.1.7 Facilitate maintenance of Cold Chain equipment through Comprehensive annual maintenance contract<br />
with a private agency with adequate technical capacity. Tender already floated and decided.<br />
6.1.8 Provide POL support to <strong>State</strong> and Regional WIC/WIF facilities @ Rs. 15000 per month and @ Rs.<br />
5000 per PHC per month to each PHCs for running of Gensets and minor repair<br />
6.1.9 Issue necessary departmental instructions to re-emphasize provision of ANC services in the job<br />
description of Aaganwadi Workers and ANMs.<br />
6.2 Build capacity of immunization service providers to ensure quality of immunization services.<br />
6.2.1 Provide comprehensive skill up gradation training to immunization service providers (LHVs/ANMs),<br />
particularly in injection safety, safe disposal of wastes and management of adverse effects.<br />
6.2.2 Conduct training to build capacity of Medical Officers, MOICs and DIOs for effective management,<br />
supervision and monitoring of immunization services<br />
6.2.3 Train Cold Chain handlers for proper maintenance and upkeep of Cold Chain equipment<br />
6.3 Form inter-sectoral collaboration to increase awareness, reach and utilization of immunization services<br />
6.3.1 Develop working arrangements with ICDS and PRIs to ensure coordination at all levels<br />
6.3.2 Involve Aaganwadi Workers and PRIs to identify children eligible for immunization, motivate<br />
caregivers to avail immunization services and follow-up with dropouts.<br />
68
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
6.3.3 ASHA, AWW and ANM will hold meeting with Mahila Mandals at each village monthly for increasing<br />
the coverage of Immunization. Incentive to be provided to ASHA and ANM under RCH and AWW under<br />
intersectoral convergence.<br />
6.3.4 Involve ICDS and PRI networks in behavior change communication for immunization.<br />
6.4 Strengthen Supervision and monitoring of immunization services<br />
6.4.1 Build capacity of Medical Officers, MOICs and DIOs in supervision and monitoring of implementation<br />
of immunization services as per the micro-plan.<br />
6.4.2 Provide mobility support to MOICs and DIOs for supervision and monitoring of implementation of<br />
immunization services.<br />
6.4.3 Develop effective HMIS to support supervision and monitoring of implementation of immunization<br />
services.<br />
6.4.5 Coordinate with representatives of PRI to strengthen supervision and monitoring of immunization<br />
services.<br />
6.4.6 Details of Immunization have been incorporated in part- C of <strong>PIP</strong>.<br />
7. To reduce morbidity and mortality among infants due to Diarrhea and ARI<br />
Strategies and Activities:<br />
7.1 Increase acceptance of ORS<br />
7.1.1 Supply of ORS and ensure availability in all depots and supply of cotrimoxazole tablets.<br />
The ASHA drug kit will have ORS and cotrimoxazole tablets which should be replenished as per need.<br />
Aaganwadi centers should also be given ORS. In the absence of ORS, the use of home-based sugar and salt<br />
solution will be encouraged.<br />
7.1.2 Orientation of ASHA for diarrhea and ARI symptoms and treatment<br />
ASHAs will be specifically trained to identify symptoms of diarrhea and ARI and to provide home-based<br />
care. Danger signs prompting transportation to seek medical care will also be taught to ASHAs.<br />
7.1.3 Organize meetings for ASHAs/AWWs for dissemination of guidelines for Home based care<br />
ASHA and AWW will be trained and provide guidelines for Home based care. The meeting will be held at<br />
Block PHC level.<br />
A detail Action Plan for ORS submitted under Part B of NRHM Additionalities<br />
7.2 Strengthening of referral services for infants seeking care for life threatening diarrhoea and ARI<br />
7.2.1 Availability of referral money @ Rs.500 available for transporting of sick infants to the health institute.<br />
7.2.2 Blood slide examination of all febrile children with presumptive treatment<br />
69
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
In endemic areas, most children are anemic due to repeated bouts of malaria. Any febrile child needs to be<br />
checked for malaria compulsorily.<br />
7.2.1 Strengthening of PHCs/ referral centers<br />
School Health Programmes<br />
Counseling sessions will be organized in Govt. Schools in collaboration with BSACS. Story lines and<br />
slogans will be published in text books of schools in collaboration with the Education Deptt. Reference<br />
Books on Health Issues and Healthy Life-Style will be published for School libraries. Health Camps will be<br />
organized for health check-ups for school children. Innovative strategies will be adopted to orient school<br />
children about healthy practices.<br />
Details annexed<br />
70
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
3 Family Planning<br />
Goal: Reduce TFR by 2.1 from present level of 4.3<br />
Objectives:<br />
1. To reduce total unmet need for contraception from 23.1 % to 15%<br />
2. To increase Contraceptive Prevalence Rate (Any Modern Method) from 28.8% to 35% by 2008-09 and to<br />
45% by 2009-10<br />
3. To increase male participation in family planning<br />
4. To increase proportion of male sterilizations from 0.6% to 1.5%.<br />
5. Monitor the quality of service as per GoI guidelines for Sterilization<br />
Objective No.1: To reduce total unmet need for contraception from 23.1 % to 15%<br />
Strategies and Activities<br />
1.1 Plan to organize RCH camp in each PHC/CHC once in two months.<br />
1.1.1. Creating dedicated cadre of skilled manpower<br />
1. Training of MBBS doctors on Minilap and NSV<br />
2. Training of MBBS doctors on Anesthesia<br />
3. Training on IUCD: MOs, ANMs etc.<br />
1.1.2 One RCH camp will be organize in each PHC/CHC where Laparoscopic Ligation/Mini Lap will be<br />
done<br />
1.1.3 Incentive to acceptors Incentive for LL operations<br />
1.1.4 Training on LL operation, MTP and IUD Insertion<br />
1.1.5 ASHA and MPWs will publicize about the RCH in their area and motivate the eligible women to go for<br />
spacing & terminal methods of family planning.<br />
1.2 Motivate eligible couples who have had their first child for spacing for condoms, OCPs or IUDs<br />
1.2.1 Update EC register with help of ASHAs and AWW<br />
The eligible couple register is presently being updated once a year (usually in April) in a survey<br />
mode. It is done in a hurry and may not have complete information in many cases. With the<br />
involvement of ASHAs and AWWs, updates should be done each month preferably during VHNDs.<br />
This will result in less wastage of time and resources and better recording of information.<br />
1.2.2 Availability of FP services: IUCDs, OCPs, Emergency Pills, Condoms<br />
71
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
1.2.2.1 Each SDH/CHC/PHC should have static FP cell / corner, with earmarked ANM / LHV responsible,<br />
for providing these services daily as OPD services to clients<br />
1.2.2.2 Community Based Distribution (CBD) of Condoms and Pills: The OCPs and condoms can be<br />
provided to community based motivated volunteers, like members of Self Help Groups (for Pills) and<br />
Husbands of motivated ASHA, Satisfied NSV client, active PRI members etc. (for condoms) for community<br />
based distribution (CBD) of these. The availability of condoms and OCPs with the volunteers and their<br />
geographical responsibilities should be widely known to the potential clients / beneficiaries. Before they are<br />
made the community based distributors, they should be properly trained and mechanism developed to<br />
regularly monitor them and review their performance<br />
1.2.2.3 Public Private Partnership (Social marketing): This can be taken up on an experimental basis in a<br />
couple of districts, or a few blocks in these districts to pilot selling through entrusted community based<br />
institutions, volunteers, market mechanisms (like the popular pharmacist of the village, or grocery shop<br />
owner or the like) condoms and OCPs at normal or subsidized rates. This should be properly preceded by<br />
adequate awareness generation of the availability of these for price in the community itself and that the<br />
clients or the community members could buy these from specified vendors (volunteers etc.). The research has<br />
shown that the services, drugs, supplies etc. bought for fee are valued more by the user and they use them<br />
more.<br />
1.2.2.4 Organize monthly IUD Camps in PHCs/CHCs/SDHs IUD camps will be organize in each<br />
PHC/CHC/SDH every month. ANM and ASHA will be informed the dates on which the camp will be held<br />
in the concern HIs.<br />
1.2.3 Ensure follow up after IUD and OCP for side effects and treatment<br />
Many of the drop outs for IUD and OCP occur due to side effects and lack of proper attention to take care of<br />
these. Follow-ups after IUD insertion and starting of OCPs and provision of medical care to mitigate side<br />
effects will help in continuing with the service and also create further demand.<br />
1.2.4 Organize Contraceptive update seminars at the district level twice in a year.<br />
The seminar for contraceptive updates will be organized at the district level twice in a year. All the<br />
healthcare providers from the district will attend the seminar.<br />
1.3 Motivate eligible couples for permanent methods in post partum period specifically after second and third<br />
child<br />
Efforts will be made by the service providers to motivate parents to adopt permanent methods after the birth<br />
of the second or third child.<br />
1.3.1 Update EC register with help of ASHAs and AWW<br />
Every event will be recorded in the EC register and thus the register will be updated. This can be done after<br />
every event has occurred or reported to have occurred or during the VHNDs visit each month to a village.<br />
1.3.2 Motivate couple after second child in Post Partum period to go in for tubectomy / NSV<br />
72
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
After the second child is born, the couple will be motivated to adopt a permanent method of family planning<br />
preferably NSV. For this communication materials will be prepared and distributed.<br />
1.3.2 Follow up after tubectomy /NSV for side effects and treatment<br />
Each tubectomy / NSV will be followed up for side effects and their treatment. This will provide positive<br />
reinforcement and motivate others to adopt family planning.<br />
1.4 Making available MTP Services in all Health Institutions.<br />
Since 8% of maternal mortality continues to be attributed to unsafe abortion, therefore, availability of and<br />
accessibility to quality abortion services / MTP services acquire greater importance. There is a need to<br />
identify, map and train the providers, both in public and private sectors on abortions / MTP services. There is<br />
also a need to ensure availability of medical abortion drugs; this can be done by including these drugs into<br />
the state procurement list. The latest guidelines on this can be had from GoI. Revisions in MTP Act are<br />
underway; once done, systematic orientation of entire cadre of health personnel on this is required.<br />
1.4.1 MTP Services in the state is not fully operational in all the hospitals of the state. Training of MOs have<br />
been under taken during RCH-1. To further strengthen the skill of the doctors for MTP training, training shall<br />
be taken up during the year. 100 MOs will be trained in 2008-09.<br />
1.4.2 Plastic MVAs will utilize and state will made purchase for availability in health institutions.<br />
Objective No.2: To increase Couple Protection Rate<br />
Strategies and Activities<br />
2.1 Awareness generation in community for small family norm<br />
2.1.1 Preparation of communication material for radio, newspapers, posters<br />
Communication materials highlighting the benefits of a small family will be prepared for radio, TV and<br />
newspapers.<br />
2.1.2 Meetings with MSS, CBOs<br />
Communication materials to be used for monthly MSS/CBO meetings will be prepared and distributed for<br />
use.<br />
These meetings will be scheduled during or preceding the month family planning camps are scheduled to be<br />
held.<br />
2.2 Regularise supply of contraceptives in adequate amounts<br />
2.2.1 Indent and supply contraceptives for all depots and subcentre/ AWCs and social outlets: Each AWC<br />
and ASHA will have at least one months requirement of condoms and OCPs. Sub centres will have adequate<br />
supplies of IUDs also.<br />
73
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Objective No.3: To increase male participation in family planning<br />
Strategies and Activities<br />
3.1 Promote the use of condoms<br />
3.1.1 Counseling men in villages to demonstrate ease of use of condoms and for prevention of STDs<br />
Male workers will assist the MPWs in addressing the meetings of men in villages to demonstrate the use of<br />
condoms and its benefits in family planning and prevention of STDs. It should be stressed that condoms are<br />
easy to use and is a temporary method. Current methods of family planning which target women are not very<br />
easy to adopt while condoms can be very easily used.<br />
3.1.2 Regular supply of condoms and setting up depots which are socially accessible to all men<br />
It is very essential to supply condoms through depots which can be easily accessible to men and<br />
confidentiality will also be ensured. During the meetings, the sources of condoms in the village will be made<br />
known to all. It will be ensured that the clients identity will not be disclosed. The depot holder will be set up<br />
only on condition that he shall not reveal the identity of clients.<br />
3.2 Promote adopting NSV: as simple and convenient method of hassle free FP methods (however, it must be<br />
told that it doesnt protect from STI/RTI of HIV / AIDS)<br />
Objective No.4: To increase proportion of male sterilizations from 0.6% to 1.5%.<br />
4.1 Increase demand for NSVs (develop a cadre of satisfied NSV Client, who could be the advocates for<br />
NSV in their designated geographical areas. Orient and train them and give them specific geographical<br />
responsibility to give roster based talks etc to identified groups of probable clients. During these talks the<br />
probable clients can be registered and they could be escorted to the nearest static facility or the camp on<br />
designated days for NSV. Once completed the procedures, then these new clients can become advocates for<br />
the same. This entire process must be fully facilitated by respective PHCs and be provided with all logistics<br />
support along with some incentives for the work or activities undertaken by them)<br />
4.1.1 Village level meetings in which men who already underwent NSV share experiences to motivate men<br />
to undergo NSV<br />
All the GP/ADC Villages will be chosen in the district to hold meetings in which men who have undergone<br />
NSV will tell male members of the community about their experience and the benefits of NSV. These<br />
meetings will be repeated each month in the same batch of Gram Panchayat or ADC Villages. NSV will be<br />
conducted on the motivated men. The same men will then be requested to share their experiences in the next<br />
batch of five villages for the next three months.<br />
4.2 Increase capacity for NSV services<br />
4.2.1 Training of doctors for NSV<br />
While demand is being generated, a team of doctors should be trained at all the FRU level to conduct NSVs.<br />
4.2.2 Organize NSV camps at the Sub District Level<br />
74
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Objective No. 5: Monitor the quality of service as per GoI guidelines for Sterilization<br />
5.1 A quality assurance committee initiated in every district for monitoring the quality of sterilization in the<br />
respective district. The Civil Surgeon is the chairman of the committee with at least one Gynecologist.<br />
5.2 Streamline the contraceptive supply chain & Monitoring<br />
1. Identifications &Renovation of Warehouse <strong>State</strong> /District/ PHC<br />
2. Budget allocation for transportation at every level<br />
3. Provision for report format printing and their availability at every level<br />
Action Plan for Strengthening Sterilization Services<br />
The activities are segregated into short-term and long-term. They are separately spelled out for the state and<br />
the district.<br />
Short Term Activities<br />
<strong>State</strong> Level Activities:<br />
1. Service Availability<br />
STATIC SERVICES<br />
i. Ensure that district level facilities are fully equipped with manpower and equipments<br />
ii.Availability of Sterilization services everyday at district hospitals, separately for, Males and Females<br />
iii.Availability of Sterilization services at PHC level on at-least 3 fixed-days a week (these days could be<br />
fixed for the entire state, like the Immunization Days, which are Wednesday and Saturdays)<br />
iv. Demand generation activities: wide dissemination of information on the regular (daily and on fixed days)<br />
availability of the services<br />
1. prominent display<br />
2. workshop of key department functionaries, who in turn would disseminate the same to their line<br />
staff, who in turn will directly inform the public about the availability of services<br />
CAMPS<br />
v. The number of camps needs to be planned and based on the ELA of the districts<br />
a. Districts must plan camps in various PHCs and locations based on the need, in the beginning of the<br />
year; this should be based on the past years records etc., and these must be shared in the beginning of<br />
the year with the state<br />
b. These camps must be planned round the year, they must be evenly distributed through out the year<br />
and wide publicity on the venue and dates of the camps, well in advance must be disseminated<br />
through out the respective catchment areas<br />
75
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
c. Availability of Providers<br />
d. Line listing of available Providers by Geographical Areas (DHQ, PHCs, SDH etc.)<br />
‣ Gynecologist,<br />
‣ Surgeon<br />
‣ Anesthetist<br />
‣ Nursing Staff<br />
e. Roster for year long Static Services Providers: Based on the above line listing form Surgical Teams<br />
for male and female sterilization separately, the teams then must be provided with earmarked days of<br />
the week at static centres, like the rotation duties in Medical Colleges and big private Nursing<br />
Homes. For example Team 1 will perform on Mondays and Wednesdays; Team 2 on Tuesdays and<br />
Fridays; and Team 3 on Thursdays and Saturdays etc. and on rotation one Team can be on call for<br />
emergencies on holidays etc.<br />
f. Roster for year long Camp Services Providers Similarly, by camps the teams should be identified in<br />
the beginning of the year and their year-long roster be prepared and informed so to them in advance.<br />
The evenness in providers work load should be ensured such that it is not the situation that a few<br />
providers are doing all the surgeries while the remaining are doing none.<br />
g. Identification of Providers for Training: Line Listing of Providers for the same. It must be prepared<br />
for every district and every PHC in the district. Before the training begins for the identified future<br />
providers, their choice must sought as to the posting to the facility they would be interested in; as far as<br />
possible this should be respected. Based on this they should be trained and posted to the pre-identified<br />
facility in a time bound fashion. This exercise should be done in advance and proper notification<br />
regarding the same should be widely publicised and disseminated. This activity should be very closely<br />
monitored by the <strong>State</strong> Health Society, in order to ensure its full operationalization. Once done, the<br />
training in phased manner should happen in a time bound fashion.<br />
h. Equipping the facilities and keeping the sets of equipments ready for the camps<br />
i. This needs to be ensured as per the guidelines for the facilities: As per the<br />
guidelines, minimum numbers of sets must be available at district and sub-divisional<br />
hospitals<br />
ii. The same needs to be ensured for every camp in advance, such that the quality and<br />
hygiene are not compromised in the camps<br />
i. Monitoring System: Both for Static Services and Camps: To monitor provider out put and progress<br />
in static facilities and camps<br />
i. A check list needs to be developed at <strong>State</strong> Health Society to monitor the above<br />
ii. A mechanism needs to be developed on this and how the information so gathered<br />
could be used to improve the services and provider output<br />
76
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
j. Monthly Review of sterilization progress and performance by district and sub-district levels,<br />
specially focusing on high-burdened areas hard to reach areas<br />
i. A fixed agenda and points to be reviewed need to developed in order to make there<br />
review meetings focused and result oriented<br />
District Level Activities:<br />
1. Undertake block-wise analysis of service utilization and work out detailed service provisions: fixed day<br />
roster based static services, camps and their schedules<br />
2. Prepare block wise demand generation activities, separately for static services and camps<br />
3. Prepare a list of providers not providing sterilization services and orient and reorient them and place/post<br />
them as per defined roster to the services: static services and camps<br />
4. Finalize work plan with state to get specific need-based inputs<br />
5. Conduct monthly review of sterilization activities at district level<br />
Long Term Actions<br />
<strong>State</strong> Level Actions<br />
1. increased trained manpower<br />
2. create dedicated pool of providers exclusively for sterilization, develop a mechanism of incentives for<br />
the high achievers<br />
3. provide appropriate mix of services male and female sterilization at static facilities<br />
4. undertake state level NSV campaign<br />
5. gradually increase static facilities and popularize the availability of the same and similarly gradually<br />
reduce the number of camps proportionately<br />
6. organize state and regional level experience sharing<br />
District Level Actions<br />
1. saturate training of all available providers<br />
2. ensure presence of providers in all static facilities<br />
3. institutionalize sterilization services<br />
4. public private partnership<br />
a. line listing of the same<br />
b. dedicated pool of the same, MBBS doctors (ask them to perform surgeries at government<br />
facilities)<br />
5. orient block level MOs in using data for monthly review and stocktaking<br />
77
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
4. Adolescent Reproductive and Sexual Health<br />
Objective:<br />
1. To reduce incidence of teenage pregnancies from present 25% to 22% by 2008-09 and to 15% by 2009-10.<br />
2. To ensure the access to information on Adolescent Reproductive & Sexual Health (ARSH) through<br />
services at District Hospitals, SDH, CHCs, PHCs & HSC level.<br />
3. To increase awareness levels on adolescent health issues<br />
Objective No.1: To reduce incidences of teenage pregnancies from present 25% to 22% by 2008-09 and to<br />
15% by 2009-10.<br />
Strategies and Activities:<br />
1.1 Improve access to safe abortions<br />
1.1.1 MTP services made available at all the FRUs initially & at all SDHs in subsequent years, through<br />
training of select medical officers at DH/MC.<br />
MOs will be trained in MTPs<br />
1.1.2 Manpower (Training) & logistic support to private hospital doctors and will also be trained in<br />
conducting safe abortions.<br />
1.2 Ensure availability of condoms/OCPs/Emergency contraceptives<br />
1.2.1 Depot holders among adolescent groups/youth organizations<br />
In addition to the ASHA and the AWW, youth organizations such as football clubs and others will have<br />
depot holders who will provide condoms/OCPs and Emergency contraceptive pills and maintain<br />
confidentiality.<br />
Objective No.2: To ensure the access to information on Adolescent Reproductive & Sexual Health (ARSH)<br />
through services at District Hospitals, SDH, CHCs, PHCs & HSC level.<br />
Strategies and Activities<br />
2.1. Organize regular adolescent clinics/counseling camps at SC/PHC/CHC/SDH/DH<br />
2.1.1 Appointment of 5 nos. Adolescent Counselor for districts setting up Adolescent clinics.<br />
2.1.2 Adolescent health sessions/clinics will be held in each Sub Centre/ PHC / CHC/SDH and DH with<br />
service delivery & referral support<br />
2.1.3 Risk reduction counseling for STI/RTI<br />
78
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
During the monthly or weekly interactions through health sessions and clinics, counseling for preventing<br />
STI/RTI will be also be done. This will include single partner sex and use of condoms for safe sex.<br />
2.2 ASHA/AWW to act as nodal persons at village level for identifying & referring adolescents in need of<br />
such services.<br />
2.2.1 Training of AWW/ASHA in adolescent health issues<br />
All ASHAs and AWWs will be oriented on problems faced by adolescents, signs and symptoms of the<br />
problems and where to refer these cases.<br />
2.3 Referrals to de-addiction centers for treating alcoholism/drug addiction<br />
2.3.1 Identification of de-addiction centers in the state/district<br />
The state / district will identify NGOs or other de-addiction centres in the state and through the health<br />
workers will refer the cases in need to these centres for treatment.<br />
2.3.2 Circulate information on services provided at these centres and setup referral system<br />
The state/district will have an understanding with the de addiction centre on the process for referring patients<br />
to the de-addiction centres.<br />
Objective No.3: To increase awareness levels on adolescent health issues<br />
Strategies and Activities<br />
3.1 Organizing Behavioral Change Communication campaigns on specific problems of adolescents<br />
3.1.1 IEC activities along with take-home print material to be organized in coordination with MSS, Youth<br />
club<br />
One of the monthly theme meetings with the MSS / CBOs will be related to adolescent health problems,<br />
signs and symptoms, treatment and referrals.<br />
3.1.2 4 monthly health checkups under School Health Programme through PHC medical and paramedical<br />
staff<br />
School Health Programmes (Health Check up under MDM)<br />
As part of the School Health Programme, adolescents in schools will undergo health check ups thrice in a<br />
year. Some counseling related to common adolescent problems will also be given during these check ups.<br />
Children are the asset and future of the Nation. The progress of any country and state depends upon them for<br />
which they must remain healthy. In Bihar there are about 1.5 crore children of 6-14 years age reading in<br />
government primary & middle schools. The health check-up of these children are must atleast once in a year<br />
to detect any serious disease in the early stage, so that preventive and curative measures may be taken at the<br />
79
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
earliest. For this objective in mind government has decided to do medical health check-up of children<br />
reading in government primary and middle schools.<br />
OBJECTIVE :<br />
· Regular annual health check-up of Children registered in government primary and middle school.<br />
· To detect any defect in progress of health and nutritional deficiencies.<br />
· Early detection of serious illnesses and to refer them in the nearest specialized government health<br />
facilities.<br />
· To develop good habit for better health and hygiene to remain healthy.<br />
· To inculcate through the children habit to remain healthy among Family members and community.<br />
· To improve quality of food supplied to children by adding micronutrients.<br />
Additionally Counseling sessions will be organized in Govt. Schools in collaboration with BSACS. Story<br />
lines and slogans will be published in text books of schools in collaboration with the Education Deptt.<br />
Reference Books on Health Issues and Healthy Life-Style will be published for School libraries. Health<br />
Camps will be organized for health check-ups for school children. Innovative strategies will be adopted to<br />
orient school children about healthy practices.<br />
Details annexed<br />
3.1.3 Orientation of VHSC on adolescent issues<br />
The MPWs will during their routine interactions with the VHSC members apprise them of the<br />
problems and issues related to adolescents and what to do for treatment and referrals. (Budgeted in<br />
RCH Training along with maternal health, Child health and Family Planning)<br />
3.1.4 Premarital counseling of adolescent girls on reproductive health issues at PHC/RH/SDH/DH<br />
This will be part of the adolescent health session/clinics which will be regularly conducted at sub centres,<br />
PHCs and also at youth clubs.<br />
3.2 Dissemination of ARSH Guidelines and Trainings<br />
3.2.1 Organize dissemination of ARSH guidelines at <strong>State</strong> level.<br />
3.2.2 Training of TOTs on ARSH<br />
3.2.3 Training of MOs, ANMs on ARSH<br />
Proposed Strategies and Activities for Operationalization of ARSH<br />
1. ARSH service delivery through the public health system:<br />
80
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
a. Actions are proposed at the level of sub-centre, PHC, CHC, district hospitals through routine<br />
OPDs. Separate arrangements should be done for male and female adolescents.<br />
b. Fixed day, fixed time approach could be adopted to deliver dedicated services to adolescents<br />
and newly married couples. A fixed day across the state, either once a month or twice a<br />
month can be declared for ARSH, and the information regarding the same should be<br />
properly disseminated in the community and properly displayed at the facilities.<br />
c. A separate ARSH Cell, comprising of ANM, LHV, Health Educators etc. (perhaps on a<br />
rotatory basis) can be established at these Cells.<br />
d. A separate ARSH Cell can be constituted at every CHCs and Referral Units, with one MO as<br />
its nodal officer (on call, sort of) and two counselors.<br />
2. Interventions to operationalise ARSH<br />
a. Orientation of the service providers: Equipping the service providers with knowledge and<br />
skills is important. The core content of the orientation should be vulnerabilities of<br />
adolescents, need for services, and how to make existing services adolescent friendly.<br />
b. Environment building activities: this should include orienting broad range of gatekeepers,<br />
like district officials, panchayat members, womens group and civil society. Proper<br />
communication messages should be prepared for the same exercise. District, block and subblock<br />
level functionaries should be responsible for this.<br />
c. The MIS should at least capture information on teenage pregnancy, teenage institutional<br />
delivery and teenage prevention of STI.<br />
5 Urban Health<br />
Urban health care has been found wanting for quite a number of years in view of fast urbanization leading to<br />
growth of slums and population as more emphasis is given in rural areas. Most of the Cities and Towns of<br />
Bihar have suffered due to lack of adequate primary health care delivery especially in the field of family<br />
planning and child health services.<br />
Objectives:<br />
1. Improve delivery of timely and quality RCH services in urban areas of Bihar<br />
2. Increase awareness about Maternal, Child health and Family Planning services in urban areas of<br />
the state<br />
At present, there are 12 Urban Health Centres (UHC) in the state which are non-functional. However, as per<br />
the GoI guidelines, there should be one UHC for 50,000 population (outpatient). The Urban Health Centres<br />
are required to provide services of Maternal Health, Child Health and Family Planning. The infrastructure<br />
condition of the Urban Health Centres is not up to the mark and requires some major renovation work. The<br />
81
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
staff at each UHC should comprise of 1 Medical Officer (MO), 1 PHN/LHV, 2 ANMs, 1 Lab Assistant and 1<br />
Staff clerk with computer skills.<br />
Objectives No. 1: Improve delivery of timely and quality RCH services in urban areas of Bihar<br />
Strategies and Activities<br />
1.1 Identify health service providers of both public and private sectors (including NGOs) in urban areas<br />
and plan delivery of RCH services through them<br />
1.1.1 Mapping of Urban Slums and existing providers of RCH services of both public and private sectors has<br />
been completed<br />
1.1.2 Develop Micro-plans for each urban area for delivery of RCH services, both outreach and facility<br />
based.<br />
1.2 Strengthen facilities of both public and private sectors in urban areas<br />
1.2.1 Establish partnerships with select private health clinics for delivery of facility-based RCH services e.g.<br />
institutional delivery, permanent methods of FP, curative MCH service, etc.<br />
1.2.2 Collaborate with health facilities managed by large public sector undertakings such as Railways, ESIS,<br />
CGHS and Military to provide RCH services to general population from identified urban areas.<br />
1.3 Strengthen outreach RCH services in urban areas through involvement of both public and private<br />
sector service providers<br />
1.3.1 Deliver outreach services planned under RCH through reinforced network of frontline health service<br />
providers (ANMs, LHVs)<br />
1.3.2 Expand outreach of RCH services by adoption of identified under-served or un-served urban areas by<br />
facility-based providers (e.g. adoption of a particular slum by a medical college or private health institute)<br />
1.3.3 Establish 20 Urban Health Centres on a rental basis under PPP in this financial year especially in<br />
districts with DHs having heavy patient load<br />
Objective No. 2: Increase awareness about Maternal, Child health and Family Planning services in<br />
urban areas of the state<br />
Strategies and Activities<br />
2.1 Use Multiple channels for delivery of key RCH messages in urban areas<br />
2.1.1 Utililise various channels of mass media with extensive reach in urban areas such as TV, local cable<br />
networks, radio (particularly Vividh Bharti channels), cinema halls, billboards at strategic locations, etc to<br />
propagate messages related to key programme components of RCH.<br />
2.1.2 Extensive use of print media such as newspapers (particularly local newspapers), journals and<br />
magazines for dissemination of key RCH messages.<br />
82
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
2.2 Broad inter-sectoral coordination to increase awareness and knowledge of key messages under the<br />
RCH programme<br />
2.2.1 Involve representatives from Urban Local Bodies (municipal corporations and municipalities),<br />
commercial associations, sports bodies, voluntary and religious organisations for intensive inter-personal<br />
communication and community-based awareness campaigns.<br />
2.3. Use various channels of mass media for ensuring utilization of services of Urban Health Centres, private<br />
or Government<br />
83
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
6. Vulnerable Groups<br />
Health Camps in Maha-Dalit Tola<br />
Two camps shall be held in each Maha-Dalit tola where health check-up and counseling shall be done,<br />
followed by distribution of spectacles to reach out to the vulnerable sections of the Society<br />
Projected cost for larger districts Rs.500 x 30 districts x 100 tolas=15.00 lakhs<br />
Projected cost for smaller districts Rs.500 x 8 districts x 50 tolas=02.00 lakhs<br />
Projected cost for spectacles Rs.200 spectacles x 30 people x no. of villages<br />
7. Tribal Health - Deleted<br />
84
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
8. Innovations<br />
8.1 PNDT Act<br />
Implementation of Medical Termination of Pregnancy Act, 1971 and Pre-natal Diagnostic Techniques<br />
(prohibition) Act, 1994.<br />
In order to arrest the abhorrent & growing menace of illegal termination of pregnancies as well that of prenatal<br />
diagnostic test ascertaining sex-selection, the Medical Termination of Pregnancy Act, 1971 read with<br />
Regulations & Rules 2003 and the pre-natal Diagnostic Techniques (Prohibition of sex selection)Act were<br />
formulated.<br />
The misuse of modern science & technology by preventing the birth of girl child by sex determination before<br />
birth & thereafter abortion is evident also from the fact that, there has been a decline in sex ratio despite the<br />
existing laws.<br />
The Apex court has observed that:-<br />
We may state that there is total slackness by the Administration in implementing the Act. Some learned<br />
counsel pointed out that even though the Genetic Counselling Centre, Genetic Laboratories or Genetic<br />
Clinics are not registered, no action is taken as provided under Section 23 of the Act, but only a warning<br />
issued. In our view, those Centres which are not registered are required to be prosecuted by the Authorities<br />
under the provision of the Act and there is no question of issue of warning and to permit them to continue<br />
their illegal activities .The apex court accordingly directed the central as well as state Governments to<br />
implement the PNDT Act. In Bihar too the concerned authorities have been directed to implement the<br />
provisions of the both the Acts forcefully.<br />
Following actions have been taken and planned in this regard.<br />
A. <strong>State</strong>, District and block level workshops on PNDT has been planned.<br />
B. Create public awareness against the practice of prenatal determination of sex and female foeticide through<br />
advertisement in the print and electronic media by hoarding and other appropriate means<br />
C. A district wise task force to carry out surveys of clinics and take appropriate action in case of non<br />
registration or non compliance of the statutory provisions. Appropriate authorities are not only empowered to<br />
take criminal action but to search and sieze documents, records, objects etc.<br />
D. Beti Bachao Abhiyaan As female foeticide is a concern both in rural and urban areas, this year, Beti<br />
Bachao Abhiyan will be launched to sensitize people against this heinous practice. Massive awareness drive<br />
with the support of College students, womens organizations and other voluntary associations is planned this<br />
year. Human Chain, rallies, seminars, workshops and press conferences will be organized for the same.<br />
85
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
8.2 MUSKAAN Programme<br />
The state has started a New Programme called MUSKAAN Programme to track pregnant women and New<br />
Born Child. Under this programme ASHA, AWW and ANMs jointly track the pregnant mothers and New<br />
Born Child.<br />
This programme launch in October 2007. Under this programme ASHA, AWW and ANM will hold meeting<br />
with Mahila Mandals in AWWCs. The main objective is to cover ANC coverage and Immunization. A Data<br />
Centre also placed in all the 533 PHCs to monitor this programme.<br />
After the introduction of this programme it has been seen that the coverage of ANC and Immunization<br />
increased. The <strong>State</strong> wants to continue this programme and requested the GoI to fund the<br />
programme.Infrastructure is one of the important components for upgradation of facility to deliver the quality<br />
service. In the <strong>PIP</strong> it has been proposed a number of infrastructural corrections for upgrading the facilities.<br />
These are<br />
1. As per RCH Programme operationalisation of 76 First Referral Unit to provide emergency<br />
obstetric and newborn care 24 hrs. a day / 7 days a week. The aim is to ensure atleast two<br />
operational FRUs per district. There are 76 hospitals in the <strong>State</strong> which have been identified to be<br />
upgraded as FRUs. The main focus initially to provide remedial measures absolutely required to<br />
ensure proper functioning of the facility. Another important aims to provide appropriate specialist in<br />
each of these 76 Hospitals. It is proposed to upgrade 76 Health facilities to FRUs in 2007 2008.<br />
Unit cost of construction at the rate of average of 2 Crores as per RCH norm. The above hospital<br />
will be well equipped with OT, electric supply, water supply, toilet, telephone services, sewerage<br />
system and disposal system for hospital infectious waste.<br />
2. Anesthetist will be hire @ Rs.1000 per case for EmOC. A provision for 50000 cases included in the <strong>PIP</strong>.<br />
3. Neonatal Intensive care unit will be setup in 13 districts at the district hospitals. Each Neonatal unit will<br />
cost Rs. 39,36,000/-<br />
1 Civil & Electrical Works: Rs. 6,86,000/-<br />
2 Equipments for individual patient Care: Rs. 25,00,000/-<br />
3 General Equipments: Rs. 2,50,000/-<br />
4 Side Lab Equipments: Rs. 2,00,000/-<br />
5 Equipments for disinfection Rs. 1,50,000/-<br />
6 Data Collection & Recording Rs. 1,50,000/-<br />
Total Rs. 39,36,000/-<br />
86
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
The costs also include provision of equipments at these hospitals either as per IPHS or as required.<br />
4. Newborn Care Unit will be set up in all the 533 PHCs @ Rs. 1,57,400/- . This includes minor civil work<br />
and purchase of Equipments.<br />
87
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
9. Strengthening of SIHFW<br />
9.1 Fast-Track Training Cell in SIHFW<br />
It is also proposed in this budget to have a full time training experts/coordinator to spearhead various<br />
trainings under NRHM. Unless a dedicated Fast-Track Training cell is constituted at state level (at SIHFW),<br />
it will be very difficult to improve the quality of trainings and linkage training with performance. As training<br />
constitutes one of the largest single components of NRHM Budget allocation, this investment in creating the<br />
Fast-Track Training cell at the <strong>State</strong> level will be very cost effective intervention. Looking at the magnitude<br />
of the work under trainings, it is being proposed that under the training co-coordinator, there should be two<br />
training sub-coordinators, looking after 50% districts each. Additionally, one clerical staff is suggested. This<br />
training cell should be at the SIHFW and will eventually further strengthening SIHFW.<br />
Budget:<br />
(1.) One Training expert/coordinator<br />
= Monthly salary Rs. 30,000/- x 12 months = Rs. 3,60,000/- per annum<br />
(2.) Two Training sub-coordinators<br />
= Monthly salary Rs. 25,000/- x 2 individuals x 12 months = Rs. 6,00,000/- per annum<br />
(3.) One Clerk = Monthly salary Rs. 10,000/- x 12 months =Rs. 1,20,000/- per annum<br />
(4.) Office expenses = Monthly Rs. 5000/- x 12 months =Rs. 60,000/- per annum<br />
Total Annual Budget = Rs. 3,60,000/- + Rs. 6,00,000/- + Rs. 1,20,000/- + 60,000/- = Rs. 11,40,000/-<br />
9.2 Filling Vacant Position at SIHFW/Hiring Consultant at SIHFW<br />
AT the same time, the remaining vacancies of SIHFW can be filled. In order to fast-track the appointments<br />
of these faculties and support staff, the appointments can happen on a contractual basis such that trainings<br />
can be better organized and their quality improved. As part of strengthening SIHFW, a monitoring section<br />
needs to be created at SIHFW to use data on various aspects of training and to improve the quality of<br />
training, to make them need based, to assess if skill enhancement is happening, if program efficiency and<br />
effectiveness are increasing or if the trained staff are being rationally posted etc.<br />
Budget<br />
(1.) 10 consultant/faculties = Monthly<br />
Salary @ Rs. 30,000/- x 10 individuals x 12 months = Rs. 36,00,000/- per annum<br />
(2.) 4 Clerical Staff = Monthly salary Rs. 10,000/- x 4 individuals x 12 months = Rs.4,80,000/- per annum<br />
(3.) Office expenses = Monthly expenses Rs. 15,000/- x 12 months = Rs. 1,80,000/- per annum<br />
(4.) Monitoring Cell (additional expenses for regular reporting within the system = Rs. 5,000,00/- per annum<br />
Total annual budget= Rs. 47,60,000/- per annum<br />
88
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
10. Infrastructure and Human Resource<br />
Infrastructure is one of the important components for upgradation of facility to deliver the quality service. In<br />
the <strong>PIP</strong> it has been proposed a number of infrastructural corrections for upgrading the facilities. These are<br />
1. As per RCH Programme operationalisation of 76 First Referral Unit to provide emergency obstetric and<br />
newborn care 24 hrs. a day / 7 days a week. The aim is to ensure atleast two operational FRUs per district.<br />
There are 76 hospitals in the <strong>State</strong> which have been identified to be upgraded as FRUs. The main focus<br />
initially to provide remedial measures absolutely required to ensure proper functioning of the facility.<br />
Another important aims to provide appropriate specialist in each of these 76 Hospitals. It is proposed to<br />
upgrade 76 Health facilities to FRUs in 2007 2008. Unit cost of construction at the rate of average of 2<br />
crores as per RCH norm. The above hospital will be well equipped with OT, electric supply, water supply,<br />
toilet, telephone services, sewerage system and disposal system for hospital infectious waste.<br />
2. Anesthetist will be hire @ Rs.1000 per case for EmOC. A provision for 50000 cases included in the <strong>PIP</strong>.<br />
Similarly Gynecologists and Pediatrician will also be hired as per requirement.<br />
3. For follow up and monitoring RCH Coordinators will be hired at Commissionaire level and at SIHFW.<br />
4. Newborn Care Unit will be set up in all the 533 PHCs and DH. This includes minor civil work and<br />
purchase of Equipments.<br />
5. Setting up of Intensive Care Unit in all the District Hospitals<br />
An Intensive Care Unit (ICU) is a specialized department in a hospital that provides intensive care medicine.<br />
Many hospitals also have designated intensive care areas for certain specialties of medicine, as dictated by<br />
the needs and available resources of each hospital. The naming is not rigidly standardized.<br />
In most of the districts do not have Intensive Care Unit in any set up whether it is Private or Public. The<br />
patients have to shift either to the nearest medical colleges or to Patna for Intensive Care. In the process of<br />
transfer most of time it has been seen that patient die on transportation. The distance to the nearest ICU set<br />
up is long and most precious time waste for treatment of the patient.<br />
Setting up of Intensive Care Unit will help to avail patient the facility in all districts so that accessibility for<br />
intensive care can be addressed. The state has proposed to establish 4 bedded ICU in all the 36 District<br />
Hospitals.<br />
89
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
11. Institutional Strengthening<br />
For HRD, training of 10 regular Government doctors is being proposed in Public Health for improving their<br />
administrative skills.<br />
Multi - Skilled Specialist DNB (Family Physician) 3 years course for 20 service doctors from CHCs<br />
SHSB proposes to initiate DNB (Family Physician) 3 years course in select district hospitals. 20 Service<br />
doctors preferably from CHCs who want to undergo DNB courses run by National Board of Examinations<br />
shall be selected based on competitive examination. The course will run via distance education mode for one<br />
and half years followed by another 18 months for hands on experience. There is an option to complete the<br />
course in two parts. After 3 years training, these doctors shall be posted in the CHCs and referral hospitals to<br />
provide caesarean and anesthetist services. The permission of National Board of examination to commence<br />
the DNB Family Medicine course may have to be obtained. To select the suitable young doctors for the<br />
course who will give an undertaking to work in the government health system for 10 years in CHC upwards.<br />
Further more it is proposed that for Multi skilling of Doctors they can be sent to hospitals like Safdarjung etc<br />
in New Delhi for continuing medical education.<br />
Sub-centre rent shall be provided for 20% of the HSCs operational.<br />
Quality Assurance<br />
The state has Quality Assurance Committee for Sterilisation, Birth Control, Maternity Services,<br />
Child Survival Services, Immunization, and Case Management of Diseases in the district<br />
Quality of health care and reproductive health services consists of the proper performance<br />
(according to standards) of interventions that are known to be safe, that are affordable to the society<br />
in question and have the ability to produce an impact on client attraction & satisfaction, belief,<br />
population stabilization, inclination towards the continuation of method(s) etc.<br />
As per the guidelines lay down by the Honorable Supreme Court of India. The <strong>State</strong> Government is<br />
in the process of constituting Quality Assurance Committees (QACs) at the <strong>State</strong> and District levels<br />
to ensure that the standards for female and male sterilization and other health services are being<br />
90
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
followed in respect of preoperative measures, operational facilities and post-operative follow-ups<br />
and other ethical diagnostic and treatment protocols.<br />
The terms of reference for the <strong>State</strong> / District QAC are as follows:<br />
· The District QAC shall conduct medical audit of all deaths related to sterilization,<br />
maternity deaths and deaths arising out of suspected medical negligence and send reports<br />
to the <strong>State</strong> QAC office. The <strong>State</strong> QAC shall deliberate on the report.<br />
· Shall collect information on all hospitalization cases related to complications following<br />
sterilization as well as sterilization failure and maternity deaths and deaths arising out of<br />
suspected medical negligence.<br />
· Shall process all cases of failure, complications requiring hospitalization, and deaths<br />
following sterilization for payment of compensation and will pursue these cases with the<br />
insurance company or otherwise.<br />
· Shall review all static institutions i.e. Government and accredited private/NGOs and<br />
selected camps providing sterilization services and providing maternity, Child survival<br />
and other medical care for quality of care as per the standards laid down, and<br />
recommend remedial action for institutions not adhering to the standards.<br />
· A minimum of three members shall constitute the quorum.<br />
Presently the QAC also looking after the quality of all the trainings done under RCH.<br />
Monitoring of delivery of critical services & NRHM trainings (IMNCI, SBA, Immunization,<br />
EmOC, LSAS, NSU, BCC for promoting Breastfeeding, Minilap, MVA, ASHA).<br />
In Bihar state, there is a quality assurance cell housed in the <strong>State</strong> Institute of Health & Family<br />
Welfare. The key responsibility of this cell has been to coordinate with multiple stakeholders and<br />
keep a track on the trainings happening in the state. There are members from the SHSB, SIHFW,<br />
Faculty of various medical colleges, retired medical college faculty members, and health officials,<br />
members from the professional organizations, and officials from the development partners are on its<br />
panel. The monitoring visits are proposed to be undertaken by the members to different districts and<br />
sub districts for initial handholding and to ensure quality training. As a part of this, standard<br />
monitoring formats available with the state are to be used. The experience till now has been that<br />
many of the doctor members are reluctant to undertake field visits. This is more so when the<br />
91
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
trainings happen in such districts from where same day return is not feasible. The key underlining<br />
reason for this has been found out to be the implementation of RCH I TA and DA norms. As it is<br />
well known, these norms were defined more than ten years ago. The different monitors undertaking<br />
field visits tend to spend from their pockets for the monitoring visits. In the last ten years, the cost<br />
of living has gone up substantially and thus it is proposed to review the financial norms for the<br />
disbursement of TA and DA while on official duty.<br />
After discussions with the stakeholders, it is suggested that the following norms may be adopted by<br />
the SHSB/GoB pending more clear guidelines from the GoI.<br />
S No Category Description Honorarium Travel Cost per<br />
monitoring<br />
day<br />
1. <strong>State</strong>/Division<br />
Government officials<br />
and doctors<br />
With same day<br />
return<br />
2. <strong>State</strong>/Division<br />
With night stay<br />
Government officials involved<br />
and doctors<br />
3. Medical college With same day<br />
faculty/retired<br />
return<br />
professionals<br />
4. Medical college With night stay<br />
faculty/retired<br />
involved<br />
professionals<br />
5. Free lance professionals With same day<br />
(by invitation)<br />
return<br />
6. Free lance professionals With night stay<br />
(by invitation)<br />
involved<br />
800 per day AC Scorpio/Travera<br />
(@Rs 2000 per day)<br />
2800<br />
1500 per AC Scorpio/Travera 2750<br />
night (@Rs 2000 per day)<br />
800 per day AC Scorpio/Travera 2800<br />
(@Rs 2000 per day)<br />
1500 per<br />
night<br />
AC Scorpio/Travera<br />
(@Rs 2000 per day)<br />
2750<br />
1000 per day AC Scorpio/Travera 3000<br />
(@Rs 2000 per day)<br />
2000 per AC Scorpio/Travera 3000<br />
night (@Rs 2000 per day)<br />
In a month, on an average, 150 monitoring days would be involved for the training monitoring.<br />
92
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
12 Training<br />
Successful Implementation of any programme depends on the capacity building of the personnel engaged. In<br />
RCH II also ,human resource base will be created by enhancing the capacities through training .The<br />
sensitization of health personnel towards various RCH interventions is one of the major focus of the capacity<br />
building initiatives under RCH - II . Various trainings will be provided to <strong>State</strong> and district level managers,<br />
medical officers, nursing staff, ANMs, AWWs, ASHA and others.<br />
The training will be provided at the <strong>State</strong> Institute of H & FW , Regional training Institutes , ANM training<br />
schools , District hospital ,PHCs and also in Railways , ESI ,private sector hospitals where there is enough<br />
case load for a proper training. Some of the trainings will be contracted out to the NGOs and private players<br />
also, so that any limitation of <strong>State</strong> infrastructure is overcome easily. [Available in detail in NGO chapter].<br />
As BCC will be a major training aspect, it has been dealt in a separate chapter.<br />
All the technical training programmes will ensure that.along with the theoretical inputs, proper practical<br />
exposure is also provided. Apart from this each training programme will stress on the managerial aspect and<br />
on the communication with the clients.<br />
The TOTs will ensure that the trainers not only master the contents of the training topic but also aquire skills<br />
as teachers/trainers or facilitators and motivators.The state official, trainers, professionals and functionaries<br />
who excel in implementing training programmes will be recognized through awards and citations. A rational<br />
selection criterion will be used to select the trainees for the trainings where the no. of trainees are limited.<br />
Moreover promotion and posting policy will be linked to training and the functionary will have to undergo<br />
training to avail the promotion. There will be provision for proper rational posting so that the personnel<br />
trained, utilize their training in their day to day work.<br />
A feedback system will be developed to assess the quality of the training. From time to time, presence of<br />
state/regional observers will be ensured to assess the quality of district level trainings and workshops.<br />
Detailed Records and data about personnel undergone training should be available with all concerned at all<br />
levels. SIHFW will coordinate and monitor this with the help of district Data Officers<br />
93
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Training Institutes<br />
SIHFW<br />
The <strong>State</strong> Institute of Health and Family Welfare (SIHFW) is the premier training institute in the state of<br />
Bihar. SIHFW needs to be further strengthened as the apex institute in the state of Bihar for co-ordination<br />
and implementation of all capacity building initiatives under RCH II program. SIHFW has the required<br />
infrastructure and facilities, which need to be reinforced further so that it can conduct the various training<br />
programs on continuous basis.<br />
As the nodal agency for training activities in the <strong>State</strong>, SIHFW will have following major tasks:<br />
· To develop annual training calendars based on the district action plans in close co-ordination with<br />
RHFWTCs and ANMTCs.<br />
· To conduct clinical and non-clinical training programs for medical officers.<br />
· To support RHFWTCs and ANMTCs to conduct timely induction and refresher training programs for<br />
ANMs and LHVs.<br />
· To facilitate ongoing assessment of training needs of functionaries at all levels<br />
· Co-ordinate and implement integrated skill development and specialized skill development training<br />
programs.<br />
· Conducting TOTs with RHFWTCs and ANMTCs<br />
· To co-ordinate with SHSB for need based hiring of resource persons for the training programs<br />
In addition, adequate provisions will be made for the institute to hire need based services of electricians,<br />
plumbers, carpenters, etc. on contract basis.<br />
RHFWTCs<br />
There are Eight Regional Health and Family Welfare Training Centers (RHFWTCs) in the state Three for<br />
male and five for female health staff. All the sanctioned posts of trainers at these institutes are filled.<br />
However, functioning of all RHFWTCs is severely affected due to lack of proper infrastructure. The <strong>State</strong><br />
proposes to use the facility Survey to do a detailed assessment of the needs of these training centers. Based<br />
on the report of the facility survey, adequate resources will be provided to all RHFWTCs to upgrade their<br />
respective infrastructure and maintenance support.<br />
Location of the RHFWTCs in the <strong>State</strong>:<br />
RFWTC Male<br />
Patna (non residential)<br />
Muzaffarpur<br />
Bhagalpur<br />
RFWTC Female<br />
Patna<br />
Gaya<br />
Muzaffarpur<br />
Saran<br />
Purnea<br />
94
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
The Facility Survey will also assess the need for new Regional Health and Family Welfare Training Centers<br />
(RHFWTCs) in the state.<br />
ANMTCs<br />
There are 22 ANMTCs in Bihar; the training capacity of these institutes varies from 60 to 90 participants per<br />
batch. Most of these training centers were functioning sub-optiminaly in absence of proper infrastructure and<br />
other essential support but after the facility survey was completed with the help of UNICEF, GoB has been<br />
able to restart 20 ANM schools. Based on the report of the facility survey, adequate resources will be<br />
provided for all ANMTCs to upgrade their respective infrastructure and maintenance support. Further status<br />
of faculty positions/trainers and their requirements at ANMTCs would be assessed in course of facility<br />
survey and then adequate provisions will be made to address their needs.<br />
Key Training Activities<br />
The wide range of training activities to be conducted under RCH II program by various agencies and training<br />
institutes is outlined below. The trainings not mentioned in training plan would be taken up with the help of<br />
development partners .Adequate changes will be made to make all the trainings as per GOI guidelines.<br />
Maternal Health<br />
· Provide comprehensive skill up gradation training to frontline ANC service providers (ANMs<br />
and LHVs) to ensure delivery of quality ANC services<br />
· Conduct training to build capacity of LHVs for effective supervision and monitoring.<br />
· Train Aaganwadi Workers and PRI members would help in identification and motivation of<br />
pregnant women for healthy antenatal care practices and for utilization of ANC services.<br />
· Impart refresher training to Gynecologists and Obstetricians on safe delivery practices and<br />
referral procedures<br />
· Train all ANMs, LHVs, and Nurses in identification of danger signs during delivery, referral<br />
procedures and PNC services.<br />
· Train NGOs, Aaganwadi Workers and PRI members in raising community awareness and<br />
knowledge about importance of institutional delivery, safe delivery practices at home, referral<br />
and PNC services.<br />
Child Health<br />
· Train frontline Health workers, Aaganwadi Workers, PRIs, local NGOs and CBOs in correct<br />
breastfeeding and complementary feeding practices<br />
95
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
· Provide comprehensive skill up gradation training to immunization service providers<br />
(LHVs/ANMs), particularly in injection safety, safe disposal of wastes and management of<br />
adverse effects.<br />
· Conduct training to build capacity of Medical Officers, MOICs and DIOs for effective<br />
management, supervision and monitoring of immunization services<br />
· Train Cold Chain handlers for proper maintenance and upkeep of Cold Chain equipment<br />
· Train Aaganwadi Workers and PRI members in identification of children eligible for<br />
immunisation, in motivation of caregivers to avail immunisation services and in follow-up of<br />
dropouts<br />
· Identify key persons to join IMNCI master training pool<br />
· Train members of master trainer pool in national level course<br />
· Recruit and train district trainers (using state master trainer pool)<br />
· Train all health and ICDS staff in a phased manner<br />
· Train frontline health workers and Aaganwadi workers in health education techniques to build<br />
community capacity for early recognition of childhood illnesses, home-based care and careseeking<br />
Family Planning<br />
· Train partners such as NGO and civil society networks, religious organisations and leaders,<br />
PRIs, ICDS, Education, General Administration, Corporate Associations and Professional bodies<br />
(IAP, IMA) in promotion of Family Planning, at state, district and block levels<br />
· (Re) train frontline health workers, Aaganwadi Workers and PRIs as motivators and counselors<br />
for family planning services through IPC and counseling<br />
· Impart technical skill-enhancement training to existing and newly appointed frontline health<br />
workers on provision of various spacing (Oral contraceptive, condom, IUD insertion, emergency<br />
contraception) and terminal (female and male sterilization) methods of Family Planning.<br />
· Train doctors in various reversible and terminal FP procedures (MTP, Minilap, NSV and IUD).<br />
Adolescent Health<br />
· Conduct annual orientation and training of all health service providers on adolescent health<br />
needs at state, district and block levels<br />
· Train/sensitize community leaders, school teachers, PRIs, NGO networks, Anganwadi Workers,<br />
towards the health needs of the adolescents<br />
96
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
· Train NGO and civil society networks, religious organisations and leaders, PRI members and<br />
teachers in promotion of safe reproductive health practices and family planning among<br />
adolescents.<br />
· (Re) train frontline health workers and schoolteachers as motivators and counsellors for safe<br />
reproductive health practices and family planning among adolescents through IPC and<br />
counseling<br />
· (Re) train frontline health workers to provide RTI/STI curative services for adolescents<br />
97
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
13 IEC/BCC<br />
The Annual Action Plan 2009-10 for IEC/BCC has been prepared in the light of the number of<br />
initiatives taken by Dept. of Health, GoB, and <strong>State</strong> Health Society, Bihar, in the implementation of NRHM.<br />
It follows in essence, form and content, the National Communication Strategy. The National <strong>PIP</strong> for RCH<br />
and instructions and guidelines received from GoI and GoB from time to time has also been kept in mind.<br />
The selection and implementation of set of behavior change have been adopted with a view to<br />
improve a wide range of family care-giving and care-seeking practices, and enhance supportive<br />
environments for improved household health practices at community, institutional and policy level. The<br />
IEC/BCC Programme will focus on building an environment favoring health seeking practices, preferably<br />
through low cost and no cost interventions, especially for the disadvantaged and the marginalized sections of<br />
society. This outlook will set the tone and tenor of the mobilization process for effectuating a positive change<br />
in the existing socio-cultural mores, systems and processes.<br />
PUBLICITY:<br />
Print & Electronic Media Materials will be developed and publicized on different issues eg. Dial 102<br />
(Ambulance Service), Dial 1911 (Doctors Consultancy), ICU Service, JBSY, Promotion of Breast Feeding,<br />
Family Planning including Non Scalpel Vasectomy, Immunization, Urban Health, Adolescent and Sexual<br />
Reproductive Health, PNDT Act, Role of ASHA under NRHM, Role of Mamta, Importance of Super<br />
Speciality Hospitals and various PPP activities initiated by SHSB etc., through various print and electronic<br />
media. Health Materials will be publicized on Bihar Text Book & Different types of Certificates issued by<br />
Govt. of Bihar and others.<br />
Outdoor Media - Hoardings, Glow Signs, Laminated Board, Flex Banners, posters, etc., on issues related to<br />
RCH and NRHM will be put up at vantage points will be displayed at important locations like at District<br />
Offices, Block Offices, PHCs, Haat points, Bus Stands, Railway stations, etc. Monthly magazine brought out<br />
by the I & P.R. Dept. is being again sponsored by SHSB. Space has been allocated in the magazine for<br />
publicizing about health related programmes. Exhibitions, Melas, Nukkad Natak functions will be organized<br />
in each district from time to time to expand reach of different programmes. Folk Media will also be used as a<br />
tool for publicity. Health related Posters/Banners will be displayed on Mail Van.<br />
At the District/<strong>State</strong> level - Advocacy Programmes, workshops seminars, press conferences, etc., will be<br />
organised for different target groups including Politicians, Media Personnel, Bureaucrats, NGOs, School<br />
Children, etc.<br />
Mobility Support: Vehicles will be hired on rent on a monthly basis at the <strong>State</strong> to provide mobility support<br />
to the IEC component.<br />
98
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
BCC/IEC<br />
Bihar is a state with high cultural heterogeneity. It has been a challenging area to address for the issues of<br />
behaviour change in a heterogeneous population. Even if the language of communication in Bihar is<br />
Hindi/maithili/maghahi/angika/bhojpuri etc the use of words and styles differs from area to area. It indicates<br />
that no common strategy is going to work for the entire state as different areas have different dialects of<br />
communication. Use of BCC has been one of the key components in any health sector strategy. It is essential<br />
to modify risk prone life styles and practices to promote healthier lifestyles and practices. In past the state<br />
have had many major rounds of social mobilizations and awareness generation which have helped to take<br />
key health messages to even the most interior of the rural areas. But still there is a lot of space for the<br />
improvement. High prevalence rate of malaria, kalazar. TB, filaria and sickle cell anaemia indicates the<br />
magnitude of the problem in the state which can be reduced through behavior change approach. All these<br />
need area specific strategies for the positive change like to motivate the people through behavior change<br />
communication for the use of bed nets avoid water logging in and around habitation area and collection of<br />
garbage in a common place away from the habitation. The approach would be adopted to impart attention<br />
precise to the existing problems district wise focused manner.<br />
BCC strategy<br />
Development of a service oriented BCC strategy should be based on an assessment of the current status of<br />
knowledge, attitudes, beliefs and practices regarding issues concerned with MMR, IMR, TFR and ARSH;<br />
and factors likely to influence necessary change in behaviour. Creation of awareness of key aspects such as<br />
breast feeding and PNDT act is particularly important. Based on evidence, the strategy should aim to<br />
determine appropriate combination of messages and media and a mechanism for assessing impact at<br />
appropriate stages. The institutional arrangement including role of state and district and strengthening<br />
capacities for BCC is again important.<br />
Behaviour Change Communication:<br />
The Annual Action Plan for 2009-2010 for Behaviour Change Communication has been prepared in the light<br />
of the health priorities of the Government of Bihar and the programmes it is committed to implement under<br />
the NRHM. It draws its approach from the national communication strategy as well as NRHM and RCH<br />
guidelines.<br />
99
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Despite its third year of operation, the NRHM in the state has been implemented without a comprehensive<br />
communication strategy, which is largely due to lack of skilled human resource and professionals within the<br />
<strong>State</strong> Health Society and Health department to carry out this specialized function of strategic communication.<br />
The action plan therefore proposes certain initiatives that focus on institutional strengthening of the <strong>State</strong><br />
Health Society with human resource building consisting of communication professionals. It also lays<br />
emphasis on capacity building of the Programme Managers and the District Managers in strategic<br />
communication in order to ensure that communication activities do not merely remain adhoc interventions<br />
but are based on research, evidence; are local / region specific and are built on a strong monitoring &<br />
evaluation system.<br />
The strategic approach will also ensure that different elements of communication and channels are employed<br />
in a manner they complement and supplement one another leading to greater impact. The interventions will<br />
focus on :<br />
· Improving family care-giving and care-seeking practices<br />
· Enhance supportive environment for improved household practices at community, institution and policy<br />
level<br />
· Promote health seeking practices through low cost and no cost interventions<br />
· Pay attention to disadvantaged and marginalized sections of the society<br />
·<br />
Key Activities for the Year 2009-2010<br />
1. Establishment of BCC Cell in <strong>State</strong> Health Society<br />
In order to effectively manage the communication interventions for different programme under NRHM, a<br />
teams of experts and professionals need to be built. Under the Mission Director of NRHM i.e. The Executive<br />
Director, <strong>State</strong> Health Society, the following structure is proposed to be established.<br />
100
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Executive Director –<br />
<strong>State</strong> Health Society<br />
BCC Cell<br />
BCC Coordinator<br />
Training<br />
Coordinator<br />
Field<br />
Coordinator<br />
M & E<br />
Coordinator<br />
Designer /<br />
DTP Assistant<br />
IEC<br />
Logistics<br />
Assistant<br />
MIS<br />
Assistant<br />
<strong>State</strong> Health Society will set up the BCC Cell with development of terms of reference, job descriptions,<br />
identification and recruitment of suitable personnel with required skills and expertise as well their<br />
orientation.<br />
The BCC Cell under the leadership and over all direction of the Executive Director, <strong>State</strong> Health Society,<br />
will then be responsible to manage NRHMs communication activities in the state.<br />
101
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
2. Capacity Building of Programme Managers & District Managers<br />
Communication understanding and sensitivity is essential before any attempt to initiate activities to achieve<br />
goals of BCC under NRHM. Since this discipline is becoming more and more research and evidenced based,<br />
it is necessary for those to understand the concept, tools and advance techniques, who are supposed to<br />
undertake and supervise these activities in the state. It is a well recognized fact that accomplishment of<br />
NRHM goals largely depends upon quality of BCC inputs and its impact on behaviour and social change.<br />
To build the capacities of senior managers and mid-level managers of the health department and that of the<br />
<strong>State</strong> Health Society, a training workshop will be organiesd. Inputs from tools employed during capacity<br />
assessment of <strong>State</strong> Health Society and specific need assessment for this training will feed into the design of<br />
the training workshop. The capacity assessment exercise will aim to find :<br />
· individual capacity of officials of SHS to carry out / implement state wide IEC / BCC activitiesexperience<br />
& skill<br />
· capacity in designing and developing appropriate material & programme<br />
· training skill for the use of IEC / BCC material<br />
· capacity in communication monitoring- dissemination and tracking of progress<br />
· capacity for storage and appropriate distribution IEC / BCC material<br />
Besides this, it will contain topics such as<br />
· Understanding of communication as a process<br />
· Multistage thinking<br />
· Frame work and elements of communication research<br />
· Designing a communication campaign<br />
· Elements of an effective communication plan<br />
· Channels and tools for communicating the message<br />
· Multi channel approach<br />
· Skills to use communication material<br />
· Communication monitoring<br />
· Evaluation<br />
All these topics will be dealt in the light of new research and thinking in the area of development<br />
communication.<br />
3. Development of Health Communication Strategy<br />
The health communication strategy for the state will be developed through a participatory process involving<br />
experts, programme managers and government officers and will be consistent to the overall programme<br />
102
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
strategy for NRHM and RCH. It will aim to reposition different programmes and services under the NRHM<br />
in a health framework -that is, offering good health as the reward for families leading to other economic and<br />
social benefits. The communication strategy will attempt to cover the following :<br />
· Review the current status of NRHM programmes in the state<br />
· Identify potential communication strategies<br />
· Select the most appropriate approach<br />
· Identify primary, secondary and tertiary audience segments<br />
· Introduce the action plan with audience-media-message framework from which will evolve the<br />
communication plan for every programme<br />
The strength of any communication lies in it being is contextual and specific. It is essential to formulate<br />
a state specific communication strategy to reach to the masse with right kind of messages and through<br />
appropriate channels. Bihar is socially and economically backward but culturally very rich. It has many kinds<br />
of festivals associated with agriculture seasons, melas, huge religious congregations, community gathering<br />
etc which provide a unique opportunity to disseminate messages. Can this cultural and traditional richness<br />
become central theme of proposed communication strategy of Bihar? These are kind of questions for which<br />
experts will brainstorm.<br />
SHSB will lead the process of communication strategy development with technical inputs as well as<br />
formations of core groups of national and state level experts for development of Bihar specific<br />
communication strategy. SHSB will work in carrying out a comprehensive formative research and to pilot<br />
some concepts in the identified programme areas that will help in designing the strategy. This research will<br />
include :<br />
‣ review of existing state communication plan, if any,<br />
‣ social and cultural norms, practices & customs,<br />
‣ opportunities for entertainments and festivals, occupation-livelihood, daily life style<br />
‣ socio-economic indicators<br />
‣ available and popular means of communication.<br />
The core group will provide strategic communication recommendations and guidelines. Broadly out come of<br />
this strategy development initiative will be<br />
· Strategic Communication positioning for the state of Bihar<br />
· Communication goals of the state<br />
· Means to achieve communication goals - resources<br />
· SHS's preparedness to accomplish these goals - infrastructure, allocations and capacities<br />
This communication strategy will help the state health planners to<br />
· Increase impact of communication drives / campaigns initiated by the state<br />
103
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
· Use time, people and resources more efficiently<br />
· Exploit opportunities - use of cultural and traditional richness of Bihar<br />
· Prevent potential problems<br />
4. Communication Plans for Different Programmes under NRHM<br />
While the institutional strengthening and communication strategy development process will be carried out,<br />
communication plans for different programmes under NRHM will be prepared and implemented under the<br />
2009-2010 <strong>PIP</strong> with technical support from different internal / national agencies and partners.<br />
Broadly, the multimedia communication around the above issues will follow the following approach :<br />
The state and district health communication plans for different programmes / issues will be prepared by the<br />
<strong>State</strong> Health Society. The communication plan will have following components :<br />
· Identification of issues to be communicated - NRHM's objectives<br />
· Identification and planning regarding communication channels guided by the state communication<br />
strategy<br />
· Capacity building of service providers- IPC, skills to use material and issues<br />
· Distribution and dissemination plan of communication material<br />
· Monitoring and evaluation mechanisms<br />
SHSB will work in the development of communication plans and materials for various programmes covered<br />
under NRHM Part A, B and C of the S<strong>PIP</strong>.<br />
Inter Personal Communication, counseling by trained functionaries supported with various social<br />
mobilization and mass media activities will be built into communication plan for each programme under<br />
NRHM.<br />
5. Skill Building of Frontline Functionaries<br />
Inter Personal Communication being the core element of the communication package and the lead medium, it<br />
is imperative to build the skills of frontline functionaries who are in direct interface with the communities at<br />
household and / or facility level. SHSB will create a pool of trainers at <strong>State</strong>, District and Block levels on :<br />
· Use of Interpersonal Communication and counseling techniques to promote health seeking behaviors<br />
in the context of issues identified under RCH II.<br />
· Appropriate and effective use of communication tools and materials<br />
104
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
In order to build the skills of service providers around a number of issues, <strong>State</strong> Health Society will develop<br />
and use a training module based on Facts for Life (FFL) framework. A detailed training and monitoring plan<br />
using cascade approach and also SATCOM training technology (on pilot basis) will be developed and<br />
implemented.<br />
6. Institutional Strengthening of IEC Bureau<br />
In order to mainstream strategic communication in all health programmes, revival and strengthening of IEC<br />
Bureau as the nodal body for implementation of all health communication is necessary. <strong>State</strong> Health<br />
department will review the current status of the Bureau and prepare an action plan plug the gaps in terms of<br />
human resource as well as directives and operational guidelines. This will serve a long term objective of<br />
sustained communication interventions as against the campaign mode of communication activities.<br />
A well planned IEC/BCC strategy and implementation framework is being placed and<br />
District Level IEC plans is being prepared. This year our focus was to make programmes based on this. The<br />
basic constraint here was to reinforce the need to understand the importance of IEC/BCC planning for local<br />
specific and outcome based BCC programmes. The state lacks a rigorous planning unit that conceptualizes<br />
and strategizes the programmes and an implementing team that realizes these programmes to the expected<br />
levels. We are planning for adding this as part of this <strong>PIP</strong>.Currently, the key strategy adopted by the state is<br />
folk art based on Kalajathas, wall writings, printed posters and handouts, TV/Radio interventions etc, some<br />
innovative strategies were adopted. It has been found that the current state level centralisation of this needs to<br />
be shifted to local level strategies, for which a policy has been formulated. This year, we are also planning to<br />
have specific focus on IEC areas for each month.<br />
Objectives of Behaviour Change Communication:<br />
Empowering the family and individuals to take health related decisions based on information and analysis<br />
Motivating the community to play a proactive role in improving their health status<br />
Effective greater utilization of health services through an improved public understanding of health care<br />
Mainstreaming gender and equity and strengthening governance through BCC strategy<br />
Creating competencies and enabling environment to assist with the above objectives<br />
Key strategy and activities for Behavior Change Communication<br />
Developing IEC materials and designing campaigns for area specific and different age<br />
groups- by social, linguistic and ethnic characteristic<br />
Distributing BCC kit (flip chart, flash cards, resource book on local food,<br />
105
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
complimentary feeding decision chart, films etc) to the Mitanins and building their<br />
capacity through training for its proper and effective use.<br />
Key areas on RCH behavior<br />
The BCC/IEC cell will be set up at the directorate. To establish BCC/IEC cell will need<br />
to have necessary equipments like computers with adequate software back up fordesigning, printers, printing<br />
materials, stationeries and furniture etc. Strengthening of<br />
the BCC/IEC cell will be done by in sourcing technical experts (3 technical experts) of the subject like<br />
nutrition, communication, medical doctors, graphic artist and designersfor the effective designing of the<br />
communication strategies etc. The function of the BCC cell would be<br />
To design the behaviour matrix- communication strategies and media materials in order to ensure in-house<br />
production.<br />
The in-house materials production (films, radio programs, posters, kalajattha, etc) this will serve as<br />
reference materials on health and will also be used by other department for IEC.<br />
The cell has to make operational framework for BCC.<br />
It will work in coordination with the other relevant departments by incorporating the ideas and components<br />
relevant to the context of the subject.<br />
Intersectoral coordination for BCC on common intervention with W&CD, PHED, Education, Health,<br />
SCERT, Unicef, CGSACS Doordarshan etc<br />
94 Major emphasis would be given on awareness generation on behaviour change. The action planned for<br />
this is to use combination of mediums for the reach and penetration of the messages. Radio would be used as<br />
a strategy at the district level for the penetration of the messages and for the dissemination of the district<br />
specific messages<br />
Comprehensive approach shall be taken up to address the health related problems like imparting life skill<br />
education to the adolescent groups, distributing BCC kit to the ASHAs, using combinations of mediums for<br />
the dissemination of the messages .<br />
Advertising of different programmes of NRHM in different types of certificates issued by<br />
BDO/CO and Block Informatics Centre established by Rural Development Department, Govt. of Bihar<br />
Under the Rural Development Department, GoB in all the 533 blocks, Block Informatic Centres have been<br />
established whose implementation and maintenance has been given to an outsourced agency under PPP for 3<br />
years. Major work of these centres is generation of various certificates to be issued by CO/BDO and SDO.<br />
Various certificates to be issued are Caste certificate, Income Certificate, OBC certificate, Birth and Death<br />
certificate, LPC certificate, Character certificate, Residential proof certificate etc.<br />
Altogether in a day yearly 60,000 certificates are issued, that means 18.00 lakh in a month and about 2.00<br />
crore per annum. These certificates can be a very good medium of advertisement as the certificates are<br />
obtained by people belonging to different status and are preserved properly for a long period of time.<br />
The certificates shall have the certificates on the front side however back side will be blank. The concerned<br />
Department has also authorized the Outsourced agency to generate advertisements for printing on the back<br />
side of the certificate.<br />
106
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
The Proposal<br />
The SHS aims to utilize this opportunity to advertise NRHMs various programmes on these certificates<br />
through which information and benefits of the programmes can reach to nearly 1.5 to 2.00 crore families.<br />
These advertisements shall exist on these certificates for ever and can act as an effective medium for<br />
Governments advocacy.<br />
Budget Expense Estimate:<br />
Coloured advertisement per Certificate cost -Rs.1,50 p and for black and white advertisement Rs.1.00 p.<br />
For advertisements on approximate 2.00 crore certificates, anticipated expenditure would be Rs.3.00 crores.<br />
107
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
14. Procurement of Equipments/Instruments and Drugs/Supplies<br />
Details annexed<br />
Strengthening Life Saving Skills for Anesthesia (LSAS) Part A<br />
Procuring equipment for the Anesthesia departments in six medical colleges<br />
In Bihar state, LSAS training is being undertaken in all six Government Medical Colleges for the<br />
last two years. A total of 55 doctors have been trained in LSAS till now. All the six medical<br />
colleges in the state are imparting this training. Monitoring visits to all Medical Colleges has been<br />
undertaken by UNICEF Health Officer Dr O P Kansal, Dr Himanshu Bhushan from GoI and Dr A<br />
K Tiwari, Programme officer for Anesthesia trainings, in the last one year. An exposure visit was<br />
also organized to Gujarat comprising <strong>State</strong> Programme Officer, all Heads of the departments of<br />
Anesthesiology and Health officer, UNICEF in April, 2008.<br />
In the last one year, there have been many formal and informal discussions with the heads of the<br />
Anesthesia departments of all the medical colleges. With the technology update taking place all<br />
around, the anesthesia departments in the state need strengthening of the basic infrastructure. The<br />
departmental heads had submitted a proposal to this effect about a year ago. It is proposed to spend<br />
Rs. Nine crore (@Rs One and half crore for each of these colleges) to help them procure the<br />
equipment. This in terms will help the trainees of LSAS training grasp the skills as per the current<br />
technology. A simple indicative list of the equipment required is given in the table below.<br />
S No Equipment Requirement<br />
1 Anesthesia workstation For all colleges<br />
2 Boyles apparatus latest 3 sets for each<br />
model<br />
college<br />
3 Fibreoptic<br />
nasopharyngolarryngoscope<br />
One for each<br />
college<br />
4 Anesthesia emergency One for each<br />
resuscitation kit<br />
college<br />
5 Ethylene Oxide sterlizer One for each<br />
college<br />
It is worth mentioning that the funds to the state medical colleges would be released as per the need<br />
and therefore fresh proposals would be invited from them after the GoI approval.<br />
Additional Suggested Action Points:<br />
1. Third party review of Anesthesia trainings: It is requested to get a review, of the LSAS<br />
training process in Bihar, conducted by Anesthesiologists of National repute already<br />
associated with GoI. Based on the assessment, the <strong>State</strong> Health Society, Bihar can be<br />
requested to fill in the gaps.<br />
2. Reorientation of Anesthesia trainers: There are two to three Anesthesiologists in each<br />
medical college who were trained in LSAS training about two years ago. A reorientation of<br />
all these trainers, for two days in Patna by GoI identified trainers, can be helpful in adhering<br />
to the standard training protocols and thus improving the quality of the trainings. A tentative<br />
amount of Rs Five lakhs is being proposed for this.<br />
108
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
3. Identification of five district hospitals having good anesthesia facilities where the trainees<br />
may be deputed for 10 weeks during the total training period of 18 weeks.<br />
4. Continuous field monitoring: The <strong>State</strong> has an established Quality Assurance Cell. Quality<br />
check of LSAS trainings also form a part of this cell activity. A regular (once a month for<br />
each medical college) monitoring visit should be conducted.<br />
5. Immediate posting plans for the LSAS trained doctors in the designated FRUs should also<br />
follow.<br />
6. Infrastructure strengthening process at the FRU level to give requisite working<br />
environment to the LSAS trained doctor should also be completed.<br />
7. Voluntary application/nomination system for the future batches of LSAS trainings should<br />
be proactively encouraged by the state.<br />
109
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
16. Programme Management<br />
Programme management arrangements have been made at state, district and block level. The entire NRHM<br />
including RCH is governed by the highest body i.e. <strong>State</strong> Health Mission chaired by the Honble CM. The<br />
SHSB functions under the overall guidance of the <strong>State</strong> Health Mission.<br />
<strong>State</strong> Health Mission<br />
Composition<br />
· Chairperson : Chief Minister<br />
· Co-Chairperson : Minister of Health and Family Welfare, <strong>State</strong> Government<br />
· Convener : Principal Secretary/Secretary (Family Welfare)<br />
· Members :<br />
Ministers in charge of Departments relevant to NRHM such as AYUSH, Women and Child<br />
Development, Medical Education, Public Health Engineering, Water and Sanitation,<br />
Panchayati Raj, Rural Development, Social Welfare, Urban Development, Planning,<br />
Finance, etc.<br />
Nominated public representatives (5 to 10 members) such as MPs, MLAs, Chairmen, Zila<br />
Parishad, urban local bodies (women should be adequately represented)<br />
Official representatives: Chief Secretary/Development Commissioners and Principal<br />
Secretaries/Secretaries in-charge of relevant departments such as Women and Child<br />
Development, Public Health Engineering, Panchayati Raj, Rural Development, Tribal<br />
Welfare, Urban Development/Affairs, Finance, Planning and Representative, MoHFW, GoI,<br />
Director (Health Services)/Director (AYUSH).<br />
Nominated non-official members (5 to 8 members) such as health experts, representatives of<br />
medical associations, NGOs, etc<br />
Representatives of Development Partners.<br />
<strong>State</strong> Health Society<br />
Objectives of the Society<br />
To provide additional managerial and technical support to the Department of H &FW, Government<br />
of Bihar for implementation of National Rural Health Mission which includes RCH II, General<br />
Curative Care, National Disease Control Programme and AYUSH<br />
110
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Governing Body<br />
Governing Body has following members.<br />
(i.) Development Commissioner, Govt. of Bihar- Chairperson<br />
(ii.) Finance Commissioner, Govt. of Bihar- Deputy Chairperson<br />
(iii.) Secretary, Dept. of Health & Family Welfare, Govt. of Bihar- Chief Executive Officer<br />
(iv.) Secretary, Dept. of Medical Education and ISM, Govt. of Bihar- Member<br />
(v.) Secretary, Dept. of Planning- Member<br />
(vi.) Project Director, BSACS- Member<br />
(vii.) Director, ICDS, Bihar- Member<br />
(viii.) Executive Director, SHSB- Member Secretary<br />
Executive Committee<br />
Executive Committee consists of following members.<br />
(i.) Secretary, Dept. of Health & Family Welfare, Govt. of Bihar To preside .<br />
(ii.) Executive Director, SHSB- Member Secretary<br />
(iii.) Director in Chief, Health Services, Govt. of Bihar- Member<br />
(iv.) Joint Secretary/ Deputy Secretary, Dept. of H & FW, Govt. of Bihar- Member<br />
(v.) Additional Director, Dept. of H & FW, Govt. of Bihar- Member<br />
(vi.) Representative of UNICEF- Member<br />
(vii.) Representative of WHO- Member<br />
(viii.) Representative of European Commission- Member<br />
(ix.) Representative of Ministry of H & FW, GOI- Member<br />
(x.) Regional Director of H & FW, GOI- Member<br />
Project Appraisal Committee (PAC) comprises of<br />
(i.) Executive Director, SHSB<br />
(ii.) Director in Chief, Health Services, Govt. of Bihar<br />
(iii.) <strong>State</strong> Representative, UNICEF, Bihar<br />
111
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
(iv.) Regional Coordinator, WHO<br />
(v.) Regional Director, Regional Health Directorate, GOI<br />
(vi.) Programme Officer- SHSB- Tuberculosis<br />
(vii.) Programme Officer- SHSB- Kala Azar<br />
(viii.) Programme Officer- SHSB- Leprosy<br />
(ix.) Programme Officer- SHSB- Blindness<br />
(x.) Assistant Engineer-PWD, Bihar<br />
(xi.) Joint Secretary, Finance Department, Govt. of Bihar<br />
(xii.) A representative of Vigilance Department<br />
‣ A project Appraisal Committee (PAC) shall consider the district plans and other expenditure<br />
proposals.<br />
‣ All proposals will be submitted to the concerned authority having delegated powers provided for<br />
final approval. In case the designated authority does not agree with the recommendations of the<br />
PAC, she/he shall record the reasons for such disagreement and may include the proposal in the full<br />
meeting of the Governing Body which shall have the full powers to accept/ reject the<br />
recommendations of the PAC provided that the reasons for rejecting the PAC recommendations shall<br />
be recorded in the minutes of the GB.<br />
Financial powers of the bodies/office bearers<br />
Type of Expenditure<br />
Extent of powers<br />
A. Approval of District/city plans Full powers to the Governing Body, provided that<br />
the plan(s) have been endorsed by the Project<br />
Appraisal Committee (PAC).<br />
B. Allocations of funds Full powers to the Governing Body.<br />
C. Approving programme and campaign Full powers to the Governing Body.<br />
activities under NRHM<br />
D. Hiring of contractual staff, including sanction<br />
of compensation package<br />
For Staff of Category A &B of Organogram-Full<br />
powers to the Chairperson of the GB provided<br />
the contracts shall be for a period not exceeding<br />
11 months at a time.<br />
112
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
For Staff of Category C of Organogram- Full<br />
powers to the Executive Director subject to the<br />
compensation package approved by the GB,<br />
provided the contracts shall be for a period not<br />
exceeding 11 months at a time.<br />
E. Release of funds for implementation of plans<br />
Full powers to the ED.<br />
approved by GB/EC<br />
F. All related activities in pursuance of <strong>State</strong> /<br />
Full powers to the ED.<br />
District plan approved by GB, such as<br />
Advertisement charges, Advance to contractors,<br />
Repayment of earnest money/security deposit,<br />
Freight charges, demurrage, Furniture &<br />
fixtures(within Budget limit),stationery,<br />
conveyance, electricity & water charges,<br />
Insurance, legal charges, postage, telephone, Fax,<br />
Repair and maintenance of equipment, Hiring of<br />
taxis, Auditors, all trainings, payment of TA/DA<br />
/Honoraria to resource persons, workshops,<br />
training material, books, TA/DA to society staff,<br />
payment related to documentation etc.<br />
<strong>State</strong> Level (<strong>State</strong> Programme Management Unit):<br />
Following are the Support staff of <strong>State</strong> Programme Management Unit<br />
SL Designation No.<br />
Salary<br />
Pm<br />
Salary<br />
Pa<br />
10%<br />
Total<br />
(E+F)<br />
1 <strong>State</strong> Programme Manager 1 33000 396000 39600 435600<br />
2 Consultant NRHM 1 30000 360000 36000 396000<br />
3 Data Asstt. Cum System Analysis 1 25000 300000 30000 330000<br />
4 Consultant Cold Chain 1 25000 300000 30000 330000<br />
5 Consultant - Maternal Health 1 25000 300000 30000 330000<br />
6 Consultant-Child Health 1 25000 300000 30000 330000<br />
7 Media Expert 1 20000 240000 24000 264000<br />
8 Consultant Procurement and Logistics 1 25000 300000 30000 330000<br />
Consultant Accounts Manager(Salary<br />
9 Rs.15000/- Pension Rs.Rs.7495.00) 1 7505 90060 9006 99066<br />
10 Accountant 1 15000 180000 18000 198000<br />
113
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
11 Store Keeper 2 8000 192000 19200 211200<br />
12 Clerk cum Steno 1 11000 132000 13200 145200<br />
13 Data Assistant 6 9000 648000 64800 712800<br />
14 Computer Operator 1 8000 96000 9600 105600<br />
15 Accountant 1 15000 180000 18000 198000<br />
16 Executive Assistant 8 9000 864000 86400 950400<br />
17 Computer Operator-cum-Steno 10 8000 960000 96000 1056000<br />
Total 5838060 583806 6421866<br />
A 10% hike in salaries per year has been recommended in the <strong>PIP</strong> and is part of RCH II budget.<br />
The Overall picture of programme management functioning is as follows<br />
Governing Body<br />
Executive Committee<br />
Secretary Health & family welfare-cum- CEO SHSB<br />
Executive Director, SHSB<br />
<strong>State</strong> Management Unit<br />
38 District Health Societies<br />
Rogi Kalyan Samitis at the Hospitals till Block levels<br />
District Health Societies<br />
The society shall direct its resources towards performance of the following key tasks:-<br />
· To act as a nodal forum for all stake holders-line departments, PRI, NGO, to participate in<br />
planning, implementation and monitoring of the various Health & Family Welfare Programmes<br />
and projects in the district.<br />
· To receive, manage and account for the funds <strong>State</strong> level Societies in the Health Sector) and Govt.<br />
of India for Implementation of Centrally Sponsored Schemes in the Districts.<br />
· Strengthen the technical/management capacity of the District Health Administration through<br />
recruitment of individual/ institutional experts from the open market.<br />
114
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
· To facilitate preparation of integrated district health development plans.<br />
· To mobilize financial/non-financial resources for complementing /supplement the NRHM activity<br />
in the district.<br />
· To assist Hospital Management Society in the district.<br />
· To undertake such other activity for strengthening Health and Family Welfare Activities in the<br />
district as may be identified from time to time including mechanism for intra and inter sectoral<br />
convergence of inputs and structures.<br />
Governing body of DHS<br />
1. District Magistrate & Collector Chairperson<br />
2. District Development Commissioner (CEO Zilla Parishad) Vice Chairperson<br />
3. District Social Welfare Officer Member<br />
4. Executive Officer, Municiplity, Saharsa Member<br />
5. Addl. Chief Medical Officer Member<br />
6. District RCH Officer Member<br />
7. Deputy Superintendent of the District Hospital Member<br />
8. Civil Surgeon Member Secretary<br />
Executive Body of DHS<br />
1 Civil Surgeon of the District Chairperson<br />
2 Additional Chief Medical Officer Cum member Sec. DBCS, Member<br />
Saharsa.<br />
3 District RCH Officer, Member<br />
4 District Leprosy Officer, Member<br />
5 District T.B. Officer, Member<br />
6 District Malaria Officer, Member<br />
7 District Programme Manager (ICDS) Member<br />
8 Chief Executive Officers Nagar Nigam, Member<br />
9 Deputy Superintendent, Sadar Hospital Member Secretary<br />
10 Sec. IMA Member<br />
11 Sec. Indian Red Cross Society, Member<br />
115
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
District Programme Management Support unit Consist of Following Personnel:-<br />
1. District Programme Manager<br />
2. District Accounts Manager<br />
3. District Data Asstts<br />
Financial Management<br />
FUND FLOW MECHANISMS AT <strong>STATE</strong><br />
Presently the <strong>State</strong> Health Society is getting Grants-in-Aid from GoI through electronic transfer by crediting<br />
the A/c of SHS. These funds are transferred to District Health Society A/c as Untied funds as per their<br />
respective District Action Plans, which then get flowed to the CHCs, PHCs, district hospitals and RKS for<br />
smooth conduct of the activities of RCH- II.<br />
On the same lines of the GOI regarding transfer of funds, SHS is under the process of implementing the<br />
system of e-transfer of funds to the districts and blocks. This process is likely to be completed very soon.<br />
116
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
FUND FLOW<br />
MOHFW, NEW DELHI<br />
By E-Transfer<br />
<strong>STATE</strong> <strong>HEALTH</strong> <strong>SOCIETY</strong><br />
BLOCKS<br />
DISTRICT <strong>HEALTH</strong> <strong>SOCIETY</strong><br />
through A/c payee cheques<br />
PHC, CHC<br />
R.K.S<br />
NGOs<br />
OTHER<br />
AGENCIES<br />
OPERATION OF BANK ACCOUNTS<br />
· The Account of <strong>State</strong> Health Society is being operated as per the delegated powers.<br />
· The persons authorized as per the powers delegated to them are also operating the bank accounts of<br />
DHS.<br />
ACCOUNTING PROCEDURES FOLLOWED<br />
The <strong>State</strong> is following the Double Entry System of accounting on Cash Basis.<br />
For the sake of convenience in consolidation of accounts districts are also instructed to follow the same<br />
system.<br />
117
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
In addition to this for proper accounting and maintenance of books, a manual cum guidelines had been issued<br />
to the districts. Also the monthly auditor appointed at each district is reporting on the accounting procedures<br />
followed by the districts on a monthly basis, along with the deviations, if any.<br />
FINANCIAL MANAGEMENT AT <strong>STATE</strong><br />
The Financial Management group at state consists of the <strong>State</strong> Finance Consultant and state accounts officer.<br />
Similarly at districts also the DAM is looking after the financial matters<br />
FINANCIAL MONITORING<br />
The financial monitoring is being done through the understated mechanisms-<br />
1. Analysis of SOEs submitted by the districts and its comparison with audited expenditures on<br />
monthly basis and reconciliation of the same by the financial consultant.<br />
2. Training cum discussion meets with all the districts officials at regular intervals.<br />
3. AUDITS:<br />
a) Comprehensive audit (Annual) as per the Directions of GoI. The auditor for the F.Y 2007-08<br />
has been appointed and they have initiated the audit of DHSs accounts.<br />
b) Monthly Audit is being conducted and reports are submitted to state regularly which are then<br />
reviewed.<br />
c) Audit by CGA officials is also going on as on date.<br />
Appointment of CA at SHSB & C.A. Level<br />
Due to increase in funds flow & for maintenance of Accounts as per NRHM guidelines, all the DHS were<br />
directed to appoint C.A. at a monthly cost of Rs.20, 000/- P.M. Similarly; CA. at SHSB level is to be<br />
appointed soon.<br />
Budget:<br />
Activity @ Proposed Budget<br />
Audit of SHSB/DHS by CA for 2009-10 Rs. 6,00,000/-<br />
Appointment of CA at SHSB @25000/- PM x 12months 3,00,000/-<br />
CA at DHS level 20,000x38x12 91,20,000/-<br />
Total 1,00,20,000/-<br />
118
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Constitution of Internal Audit wing at SHSB:<br />
Internal Audit wing is proposed to be constituted in 2009-10 in which services of 6 retired officers form<br />
Recognised Audit & Accounts Services will be engaged, who will be well versed in Audit work.<br />
Budget:<br />
Activity @ Proposed Budget<br />
Last pay drawn Pension = Approx exp of 20,000x6x12 14,40,000/-<br />
Rs.20,000/-PM<br />
TA/DA for Audit 1000x6x30x12 21,60,000/-<br />
Training of SHSB/DAM/BHM) FM Group Head Quarter<br />
36,00,000<br />
level=6x1500x12=1,08,000/-<br />
DAM=38x1500x4=<br />
2,28,000/-<br />
BHM=538x1500x4=32,28,000/-<br />
Total 1,00,20,000/-<br />
119
CEO<br />
ED<br />
ED Cell<br />
Steno cum CO<br />
PA/DA-1<br />
Clerk cum-Steno E/H -<br />
2<br />
Computer Operator-1<br />
I/C Adm.<br />
Storekeeper<br />
Pharmacist<br />
PO T.B.<br />
PO<br />
Imm<br />
PO<br />
Fi<br />
PO N<br />
POK<br />
POBl<br />
.<br />
POL<br />
PM<br />
P&A<br />
IEC<br />
MCH<br />
CC<br />
DO & SA<br />
MF<br />
M A/C<br />
Tech.<br />
Wing<br />
<br />
<br />
<br />
ind<br />
nes<br />
s<br />
<br />
Steno cum CO<br />
CP<br />
DA-1<br />
CO-3<br />
Steno cum<br />
CO<br />
FO<br />
Accountant-<br />
3<br />
Astt. Eng.<br />
DA-2<br />
1P & A<br />
- Personnel & Administration<br />
2POBl<br />
- Programme Officer Blindness<br />
3PON<br />
- Programme Officer Nutrition<br />
4POK<br />
- Programme Officer Kala-Azar<br />
5PO Fi<br />
- Programme Officer Filaria<br />
6PO Imm<br />
- Programme Officer Immunization<br />
7MF<br />
- Manager Finance<br />
8MA/C<br />
- Manager Accounts<br />
9PM<br />
- Programme Manager<br />
1FO<br />
- Finance Officer<br />
1CO<br />
- Computer Operator<br />
1DO & SA - Data Officer & System Analyst<br />
1POL<br />
- Program Officer Leprosy<br />
1MCH<br />
- Maternal & Child Health<br />
1CC<br />
- Cold Chain<br />
1Asst. Eng - Assistant Engineer<br />
1CP<br />
- Computer Programmer<br />
1DA<br />
- Data Assistant<br />
1PA<br />
- Private Assistant<br />
Steno cum<br />
CO-1
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
17. Convergence and Coordination<br />
Coordination with other departments such as ICDS, PHED, Education and Panchayat Raj is important for<br />
tackling health issues. The involvement of representative of these departments help the health service<br />
providers in reducing the maternal mortality, Infant Mortality and increase the coverage of Family Planning<br />
Service and Adolescent Health Service. The state would take certain initiatives to ensure a synergistic effort<br />
from the community level to the state level which is defined in part E along with a detailed budget<br />
18. Role of <strong>State</strong>, District and Blocks<br />
The role of <strong>State</strong>, District and Block are well defined. The role of each one has been clearly indicated in the<br />
workplan (Annex 3 d) as per activity wise. The decentralization process has given more roles to Districts and<br />
Blocks to perform in executing the various programs. The <strong>State</strong> mainly looking after Monitoring, Policy<br />
decisions, Centralize capital purchase, technical support etc and help the district in execute the actions<br />
planned.<br />
19. Monitoring and Evaluation<br />
One of the major weaknesses of the RCH program in the Bihar is the absence of an effective Monitoring and<br />
Evaluation system that would provide accurate and reliable information to program managers and<br />
stakeholders and enable them to determine whether or not results are being achieved and thereby assist them<br />
in improving program performance. A triangulated process of Monitoring and Evaluation would enable cross<br />
checking and easy collection, entry, retrieval and analysis of data.<br />
Activities<br />
ü Strengthening and up gradation of monitoring and evaluation cell<br />
ü Mobility support<br />
ü Equipping and furnishing demographic cells<br />
ü Conducting survey and concurrent evaluation<br />
ü Formation of Databank<br />
ü Revised CNAA for all levels would be persuaded and guidelines for preparation district plans<br />
ü Web/internet based computer software for use at district and state level<br />
ü Reporting formats for providing requisite information<br />
121
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
ü Road map of each health centre for easy communication<br />
ü Triangulation of data<br />
Triangulation Process for Monitoring and Evaluation<br />
Computerized MIS<br />
Community Monitoring<br />
Focused Studies<br />
Monitoring<br />
Key progress<br />
indicators<br />
Evaluation<br />
Input Indicators<br />
· Staff<br />
position,<br />
· Training &<br />
orientation,<br />
· supplies,<br />
· frequency of<br />
immunization<br />
Output<br />
Indicators<br />
· Maternal<br />
Health<br />
Indicators<br />
· Child<br />
Health<br />
Indicators<br />
· Family<br />
Planning<br />
· Adolescent<br />
Key Finanacial<br />
Indicators<br />
· Percentage<br />
funds<br />
received by<br />
state<br />
according to<br />
schedule<br />
· Percentage<br />
funds<br />
disbursed to<br />
districts<br />
Key<br />
Development<br />
Indicators<br />
· MMR<br />
· IMR<br />
· NMR<br />
· TFR<br />
Key Development Indicators<br />
The key development indicators for measuring progress in reaching the overall project development<br />
objectives for the RCH programme in the state are as follows.<br />
· Maternal Mortality Rate<br />
122
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
· Infant Mortality Rate<br />
· Neonatal Mortality Rate<br />
· Total Fertility Rate<br />
Key progress indicators<br />
Key progress indicators enable the monitoring of delivery of project inputs and the achievement of project<br />
outputs.<br />
Table : Examples of Input Indicators<br />
Institutional<br />
Strengthening:<br />
Infrastructure<br />
Institutional<br />
Strengthening:<br />
Human Resource<br />
· No. of new · No. of health<br />
facilities<br />
personnel<br />
constructed appointed<br />
· No. of new · No. of health<br />
facilities<br />
personnel<br />
upgraded<br />
trained for<br />
· No. of essential capacity<br />
equipment<br />
building<br />
Programme<br />
HMIS<br />
Supervision<br />
management<br />
· No. of programme<br />
managers<br />
appointed at<br />
state/district levels<br />
· No. of programme<br />
managers trained at<br />
state / district<br />
levels<br />
· Number of<br />
operational<br />
equipment such<br />
as computers<br />
supplied to<br />
reinforce HMIS<br />
· Number of new<br />
formats<br />
developed<br />
· Percentage of<br />
work<br />
computerized<br />
supplied<br />
Key financial indicators<br />
Key financial indicators help assess the project's budgetary and financial health.<br />
· Percentage of funds received by state according to schedule<br />
· Percentage of funds disbursed to districts<br />
· Percentage of funds disbursed to districts according to schedule (within 15 days)<br />
Percentage of utilization of funds against allocation by state / districts<br />
The National Rural Health Mission has been launched with the aim to provide effective health care to rural<br />
population. The programme seeks to decentralize with adequate devolution of powers and delegation of<br />
responsibilities has to have an appropriate implementation mechanism that is accountable.<br />
In order to facilitate this process the NRHM has proposed a structure right from the village to the national<br />
levels with details on key functions and financial powers. To capacitate the effective delivery of the<br />
programme there is a need proper a proper HMIS system<br />
Regular monitoring, timely review of the NRHM activities should be carried out. The quality of MIES in<br />
<strong>State</strong> HQ and in districts is very poor. Reporting and recording of RCH formats (Plan and monthly<br />
123
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
reporting) are irregular, incomplete, inconsistent and few districts are not reporting at all. Formats are not<br />
filled up completely at the sub center level. There information is not properly reviewed at the PHC level. No<br />
feedback is provided upon that information.<br />
For overall management of the programme, there is a Mission Directorate and a <strong>State</strong> Programme<br />
Management Unit in the state. The Unit is responsible for overall monitoring and evaluation of the<br />
programme in the state and the districts. The data gathering is being facilitated by the state, District and PHC<br />
data Centres. The numerous formats being used have been reviewed and it is found that data needs to be<br />
compiled only as per RCH, NRHM programme and <strong>State</strong> needs. Hence the new MIES formats have been<br />
shared with all the health functionaries and it is expected that they shall be reporting in the new formats from<br />
the 3 rd quarter after brief orientation training.<br />
At district level, there is a District Health Society who will be responsible for the data dissemination from the<br />
sub-district level to the district level. Data Manager/HMIS expert at the <strong>State</strong> level and Data Assistant at the<br />
district level will be responsible for management of HMIS.<br />
As such, there will be a Monitoring Team constituted each at state and district level to monitor the<br />
implementation of the NRHM activities. The Team will comprise of representatives from the Mission<br />
Directorate and Programme Committee for various health programmes. The Team will also comprise of<br />
representatives from Govt. of India.<br />
There is Hospital Management Committee/ Rogi Kalyan Samity at all PHCs and CHCs. The PHC / CHC<br />
Health committee will monitor the performance of SC under their jurisdiction and will submit the report. The<br />
PHC/ CHC health committee will monitor and evaluate the SC performance .and performance will be<br />
submitted to the District, which will compile and sent it to the state.<br />
REPORTS REQUIRED FROM DHS<br />
· Monthly Fund flow statement<br />
· Form -9 (accurate and fully filled)<br />
· ASHA selection and training report<br />
· Mobile Medical unit (if working )<br />
· Janani Evam Baal Suraksha Yojana Reports (no. of institutional deliveries, Deliveries under<br />
JBSY,No. of Pvt Institutions accredited)<br />
· Immunization reports. Vaccine wise coverage<br />
· Training reports of the current trainings being given in the district or being under taken by district<br />
officials<br />
124
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
· 24 X 7 PHC working, Status of telephones working , No. of ambulance and their usage, monitoring<br />
of doctors and ANMs presence, No. of OPD patients, No. of IPD, No. of referrals, No. of deliveries<br />
being conducted<br />
· Rogi Kalyan Samitis formation and working , meetings of RKS<br />
· Sub centre untied funds, Joint A/c of ANM and Panchayat member (female), UCs of untied funds<br />
· Integration of AYUSH at PHC level<br />
· Availability of essential drugs, Vaccines, AD syringes in DH, SDH, PHC, SC<br />
· Contract Appointment of doctors, ANMs, Staff Nurses and other Staff<br />
· Health melas, No. of beneficiaries<br />
· Family planning services, male steris, female steris , IUD,<br />
· MNGO working (if present)<br />
· Other Special programmes specific to the district<br />
· Quarterly Finance Management Report<br />
The DPM along with the DAM (in financial matters) shall be responsible for compilation and timely<br />
reporting<br />
Table : HMIS Forms<br />
Form No. Information Filled by<br />
Form No.1 General information, no. of births, Cases of complicated ANM<br />
pregnancies and deliveries, sick newborns , RTI/STD cases, oral<br />
rehydration performance data [action plan by ANM or SC]<br />
Form No. 2 Deliveries, MTPs ,RTI/STD, Immunization, need assessment of PHC level<br />
individual ANMs [action plan for PHC]<br />
Form No. 3 Sterilization, ,immunization, services in obstetric care STI/RTI Sub division<br />
[action plan for FRU/Subdivision/DH]<br />
level<br />
Form No. 4 District action plan District<br />
Form No. 5 <strong>State</strong> action plan <strong>State</strong> level<br />
Form No. 6 Monthly report by ANM ANM<br />
Form No. 7 Monthly report by PHC PHC<br />
Form No. 8 Monthly report by FRU/Subdivision FRU<br />
Form No. 9 Monthly report by District District<br />
125
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Action plan Forms<br />
Form 5<br />
1. <strong>State</strong> Staff position,<br />
2. Training & orientation,<br />
3. supplies,<br />
Form 4<br />
District Action Plan<br />
Compilation of Action Plans submitted by all PHCs, FRUs, Sub-Divisional<br />
Hospitals at the District Hospitals and submitted to the <strong>State</strong><br />
Form 1<br />
HSC Action Plan<br />
Prepared by: ANM with<br />
the help of DFWO<br />
Submission: Once in a<br />
year, Feb-March<br />
Form 2<br />
PHC Action Plan<br />
Prepared by: PHC, LHVs<br />
& ANMs<br />
Submission: Once in a<br />
Year, Feb-March<br />
Form 3<br />
FRU/SDH Action Plan<br />
Prepared by: Sub<br />
Divisional Hospitals<br />
Submission: Once in a<br />
Year, Feb-March<br />
Reporting Forms<br />
Form-9<br />
Compiled at: District Level<br />
Responsibility: CS/ACMO<br />
Flow of form: District to <strong>State</strong><br />
Submission: 25th of each month<br />
Form-8<br />
Form-7<br />
Compiled at: FRU/SDH Level<br />
Responsibility: MOIC<br />
Flow of form: Hospital to District<br />
Submission: Monthly<br />
Compiled at: PHC Level<br />
Responsibility: MOIC<br />
Flow of form: PHC to District<br />
Submission: Monthly<br />
Form-6<br />
Compiled at: HSC Level<br />
Responsibility: ANM<br />
Flow of form: HSC to PHC<br />
Submission: Monthly<br />
126
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
20. Synergie with NRHM Additionalities<br />
The NRHM is an effort to bring about the architectural change to overall program management to enable<br />
rationalization of resources and simultaneously to augment then limited resources so that equity in health is<br />
ensured. The commonality of initiatives in the following areas would be complementing the similar efforts<br />
under NRHM;<br />
• Infrastructures for facility development,<br />
• Manpower recruitment,<br />
• Capacity building through training, program management, institutional strengthening, organizational<br />
development,<br />
• Communitization,<br />
• Promotional efforts for demand generation and<br />
• Improved monitoring & evaluation systems developed under RCH II<br />
• Public Private Partnership<br />
• Convergence & Coordination<br />
.<br />
The convergence approach which was mooted earlier now finds a clear policy initiative and procedural<br />
development by health and all health determinants sectors so that a joint effort is made in tandem from<br />
planning to impact evaluation / outcome to ensure investments in health reach the poor /<br />
unnerved/underserved/excluded segment of the population. These common efforts would also strengthen<br />
gender equity through adolescent and other initiatives of both RCH & NRHM to provide a safety net to<br />
young women and girl children.<br />
127
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
21. Sustainability<br />
The usage of government services in Bihar has certainly picked up with number of patients increasing<br />
manifolds due to free drugs and availability of doctors at PHC level. Similarly there has been an<br />
unprecedented increase in number of deliveries being conducted at government health facilities under Janani<br />
Baal Suraksha Yojana This can be largely attributed to huge influx of funds under NRHM. To hedge the<br />
growth from lack of funds and for its sustainability Government of Bihar has already applied user charges for<br />
pathology and radiology services. The ambulance user charges are being determined by Rogi Kalyan<br />
Samitis. The state already has paying wards in our medical colleges and GoB is contemplating having such<br />
wards in all district hospitals too.<br />
For sustainability of manpower incentives for specialist services and for postings in rural areas have been<br />
proposed in this Programme Implementation Plan. Government is working on Dynamic ACP and Cadre<br />
division of doctors for providing them better benefits.<br />
Private parties are also being encouraged to make investments in Health sector so that the sector doesnt<br />
become dependent on NRHM funds. However they would be urged to take up mapping of available facilities<br />
and also analysis of demand before investing and providing services so that any duplication may be avoided.<br />
Moreover GoB is also increasing its allocation to health sector. This year the state government proposed to<br />
establish Emergency Medical Service, Dialysis Unit, Telemedicine system under PPP initiative. The state<br />
also increasing the number of Adll PHCs to be outsource to the NGOs.<br />
128
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
22. Extra Inclusions in RCH<br />
IFA (Details Annexed)<br />
Maternal and perinatal death inquiry and Response:<br />
Maternal and perinatal death inquiry (MAPEDIR) is an operational tool that strengthens community<br />
participation in evidence-based planning. MAPEDIR aims to help healthcare providers and community<br />
members understand the<br />
avoidable factors that underlie maternal and perinatal deaths and to identify ways to prevent these deaths. The<br />
main objective of introducing MAPEDIR is to develop a framework for the assessment of maternal and<br />
perinatal deaths and implementation of effective, high impact strategic interventions through:<br />
1. Sensitizing communities to maternal and perinatal health issues, including the need for birth<br />
preparedness, complication readiness,<br />
2. Identifying maternal deaths and conducting community-based inquiries with close acquaintances of<br />
the women to find ways to prevent maternal deaths;<br />
3. Sharing the findings with communities, helping them interpret the data and develop appropriate<br />
interventions and advocate for improvements in health care-seeking; and<br />
4. Using the findings to advocate with policy makers for improvements in maternal health care.<br />
Maternal and perinatal death inquiry and Response:<br />
In the year 2007-2008, UNICEF has piloted the MAPEDIR in Vaishali District. GoB proposes to take will<br />
take it to scale to 2 more districts (Kishanganj and Jehanabad) in 2009-10 with UNICEF support as part of<br />
the next Annual NRHM <strong>State</strong> Plan.<br />
Major Activities<br />
Identification of Staff: Supervisors, Interviewers and Notifiers<br />
£ Identification and selection and training of the supervisors and interviewers (ANM and LHVs) will<br />
be conducted supported by UNICEF. Selection of Notifiers (ASHA workers)band their one day<br />
orientation will take place.<br />
Capacity Building of Staff: Supervisors, Interviewers and Notifiers<br />
£ Once the identification process is over, a four day training of the Interviewers and the supervisors<br />
will be conducted to educate them over the entire concept of MAPEDIR and the implementation<br />
process.This training will be conducted with UNICEF support.<br />
£ Once the training of supervisors is over, a one day orientation of the notifiers from the all the<br />
Panchayats of all the blocks will be organized to equip them, with the process of notification of<br />
deaths and reporting to the supervisors<br />
129
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
Notification of Cases<br />
£ This activity will be taken up by the notifiers once they undergo the orientation program and are<br />
placed in their respective Panchayat. The activity will consist of verifying the information shared by<br />
the informants, Filling-up the Notification Format and Contacting the Supervisors<br />
Interviews<br />
£ Interviews will be conducted by skilled and trained interviewers trained during the 5 day capacity<br />
building program. This activity takes place once the supervisor assigns the case to the interviewer.<br />
The interviewer will visit the household where the death took place and will interview the closest<br />
person who stood when the death took place. The recorded information in the prescribed format will<br />
be submitted to the supervisor who then will verify the recordings and promote it for entry and<br />
analysis.<br />
Data Entry and Analysis of information<br />
£ Data Entry and Analysis will take place only when the above processes of Notification, Interview<br />
and Verification are over. All entry will take place at the District level and analyzed at UNICEF<br />
level<br />
Community Sensitization Program<br />
£ At the monthly Mahila Mandal meetings sensitization of the community members functionaries will<br />
be done for generating awareness on the causes of maternal of death, precautionary measures and<br />
community initiatives. Other forums for the same will be explored.<br />
Orientation and Sensitization of Health Functionaries<br />
£ At the block and District Level one day orientation of the Health Functionaries will be carried out to<br />
develop a consensus on the process.<br />
Advocacy Meetings<br />
£ Finally, the analyzed data are to be utilized for advocacy and policy modification at the district and<br />
state level. These advocacy meetings will be very strategic in nature where decisions regarding<br />
effective service delivery and service effectiveness will be targeted.<br />
Costs incurred per Maternal death investigate/non maternal death notified<br />
Honorarium & Travel<br />
Informants 30 1 30<br />
Notifiers 70 1 70<br />
Interviewers 250 2 500<br />
Supervisors 250 1 250<br />
Total per maternal death investigated Rs. 850<br />
130
NRHM <strong>STATE</strong> PROGRAMME IMPLEMENTATION PLAN- 2008-09<br />
23. Work plan<br />
Annexure 3 d<br />
24. Budget<br />
Annex 3e and 3c<br />
131
PART- B<br />
NRHM Flexible Pool /<br />
NRHM Additiona lities<br />
2009-2010<br />
132
1. Decentralization<br />
For effective decentralization in principle as well as practice, health societies have been established at all levels<br />
of the healthcare delivery structure. Systematic involvement of various stakeholders at all levels through these<br />
societies has helped make healthcare delivery responsive to the needs of the people via participatory planning<br />
and removal of bottlenecks at implementation levels. <strong>State</strong> Health Society provides overall guidance and<br />
supervision for effective planning and implementation, and also coordinates activities across the board. The<br />
<strong>State</strong> Health Mission, the Governing Body and the Executive Committee meet at regular intervals and take<br />
decisions regarding all matters. District level activities are taken care of through the District Health Society.<br />
Rogi Kalyan Samitis at PHC, CHC, Sub Divisional Hospitals, District Hospitals and Medical Colleges have<br />
been set up. The formation of societies under NRHM has given a new direction to management and overall<br />
functioning of the health department towards the achievement of its goals.<br />
133
ASHA<br />
One of the key components of the National Rural Health Mission is to provide every village in the country with<br />
a trained female community health activist ASHA or Accredited Social Health Activist. Selected from the<br />
village itself and accountable to it, the ASHA is trained to work as an interface between the community and the<br />
public health system.<br />
Under NRHM, 87135 ASHAs (revised as per the decadal growth in 2008) are to be selected and trained in<br />
Bihar. The previous target was 74313 (as per 2001 census). The first orientation training of seven days has been<br />
completed for about 60,016 ASHAs. The 2nd, 3rd and 4th round /2, 3 & 4th module training is being done by<br />
PHED and its NGOs. The PHED had proposed a total cost of Rs.40.70 cr. which has now been reworked to<br />
Rs.27.15 Crores. A total no. of 76 <strong>State</strong> Level trainers/Master Trainers were trained till June 2008 and 393<br />
district level trainers/Block resource persons are being trained. The 5 th round/module of training is to be started<br />
just after the completion of 2 nd , 3 rd & 4 th round of training.<br />
A total number of 67506 ASHAs have been selected so far. Orientation training of seven days has been<br />
provided to 60016 till now. The ASHAs are given the copies of each module (Hindi version) and reading<br />
material in the form of flip charts for their better understanding and also dissemination of key health messages<br />
among villagers.<br />
Table 1: ASHA Status (Target, Selection and Training)<br />
Revised Selection Target (As Selected as Trained with<br />
Sl.<br />
District per 2.3 % per annum decadal on Module<br />
No.<br />
growth rate)<br />
01.01.09 1/Phase 1<br />
I II III IV V<br />
1 Araria 2376 2026 2026<br />
2 Arwal 773 652 652<br />
3 Aurangabad 2160 1646 1567<br />
4 Banka 1820 1532 1471<br />
5 Begusarai 2629 2091 1771<br />
6 Bhagalpur 2311 1936 1877<br />
7 Bhojpur 2264 1661 1637<br />
8 Buxar 1493 1086 945<br />
9 Champaran(E) 4326 2910 2130<br />
10 Champaran(W) 3206 2653 2177<br />
134
11 Darbhanga 3550 2357 2250<br />
12 Gaya 3514 2780 2240<br />
13 Gopalganj 2371 2015 1868<br />
14 Jamui 1520 1254 1254<br />
15 Jehanabad 871 769 769<br />
16 Kaimur 1462 1247 1247<br />
17 Katihar 2549 1779 711<br />
18 Khagaria 1412 1001 891<br />
19 Kishanganj 1368 1112 799<br />
20 Lakhisarai 802 581 557<br />
21 Madhepura 1711 1403 1403<br />
22 Madhubani 4046 3034 2751<br />
23 Munger 961 840 820<br />
24 Muzaffarpur 3984 3120 2544<br />
25 Nalanda 2365 2010 2010<br />
26 Nawada 1959 1531 1284<br />
27 Patna 3233 2571 1932<br />
28 Purnia 2723 2113 2000<br />
29 Rohtas 2490 1950 1935<br />
30 Saharsa 1622 765 676<br />
31 Samastipur 3835 3143 3004<br />
32 Saran 3459 2681 2329<br />
33 Sheikhpura 521 426 402<br />
34 Sheohar 580 99 82<br />
35 Sitamarhi 2965 2147 1665<br />
36 Siwan 3008 2538 2327<br />
37 Supaul 1928 1515 1492<br />
38 Vaishali 2969 2532 2521<br />
Total 87135 67506 60016<br />
ASHA is the first port of call for any health related demands of deprived sections of the population, especially<br />
women and children, who find it difficult to access health services and she will provide her service mainly<br />
under the following heads-<br />
135
Table 1: The compensation package of ASHA<br />
Sl. No. Programme & Relevant Task Amount of Compensation<br />
1.<br />
Janani & Bal Suraksha Yojana For Institutional @Rs. 200/-(Only Rs.Two hundred) Per<br />
Delivery and Full Immunization of the New Born Pregnant Woman<br />
2.<br />
Mobilizing all the children of the village for @ Rs. 150/-(Only Rs. One hundred<br />
Immunization<br />
fifty only) Per Month<br />
3. Providing DOTS under Tuberculosis Control Program Rs 250 per patient.<br />
4.<br />
For identifying Patient of Leprosy and accompanying @ Rs. 300/- (Only Rs. Three hundred)<br />
him/her to PHC<br />
Per Patient<br />
5. Training<br />
D.A. Per Day<br />
@ Rs. 100/- (Only Rs. One hundred)<br />
Per Day(During the Training)<br />
T.A. Per Training (To & Fro)<br />
@ Rs. 50/- (Only Rs. Fifty) Per<br />
Meeting<br />
6. To participate in ASHA Divas organized at PHC<br />
@ Rs. 75/- (Only Rs. Seventy Five) Per<br />
Meeting<br />
7. For motivating for Sterilization<br />
@ Rs. 150/- (Only Rs. One hundred<br />
Fifty) on Completion of Surgery<br />
8. For motivating client for vasectomy/ NSV<br />
@ Rs. 200/- (Only Rs. Two hundred)<br />
on Completion of Surgery<br />
9. For 6 no. home visits under HBNC and IMNCI<br />
@ Rs. 200/- (Only Rs. Two hundred)<br />
on Completion of the 6 th visit<br />
Programme Description<br />
1.11 At the <strong>State</strong> Level<br />
Personnel– The Project Manager and Deputy Project Manager at the <strong>State</strong> level have been appointed.<br />
Additional personnel including Statistical assistant, data assistant and office attendant have been provided for<br />
effective implementation and execution of different aspects of work.<br />
ASHA Mentoring Group- A Mentoring Group comprising of leading NGOs and well known experts on<br />
community health is under the process of formation, to provide guidance and advice on matter relating to<br />
selection, training and support for ASHA.<br />
Development of IEC and Monitoring Material – For effective documentation, information dissemination and<br />
reporting, ASHA Flip Chart, ASHA Activity Diary, ASHA Register, IEC Material, Monitoring and Reporting<br />
Formats and resource materials for meetings and for Behavior Change Communication will be ensured.<br />
136
Monitoring and Supervision and Operation Research and Documentation: This will ensure basic field<br />
level assessment, working towards the gap identified, analyzing and assessing the outcome and thus eventually<br />
working towards a holistic strategy development. This will include the following components:<br />
a. Periodic Surveys at District Level (once in three months)<br />
b. Operational and Action Research from <strong>State</strong> Level (every six months)<br />
c. Field Visits every month by the Consultants ASHA<br />
d. Monitoring of the Training being conducted<br />
e. Community monitoring<br />
ASHA Sammelan and exposure visit: ASHA Sammelan will act as a platform where ASHAs accompanied by<br />
Block Health Manager, Block Health Organizer, District Nodal Officer and Senior Nurse of one district/block<br />
meet the ASHAs of another district/block to share their experiences of work with District & Block Health<br />
Officials, Medical staffs and beneficiaries. This will help in networking, information sharing and build a kind of<br />
connectivity between the workers and the <strong>State</strong>.<br />
Workshop, Seminars and Consultative meetings: - This will involve experts on health from the national level<br />
along with members of ASHA Mentoring Group for analysis of the operation research and monitoring to work<br />
towards further strategy development.<br />
1.12. At the District Level<br />
Additional Personnel<br />
Community Mobilizer/ District Project Manager ASHA – She/He will be appointed in the capacity of<br />
Community Mobilizer and will act as a Nodal Officer at the district level for effective programme management,<br />
implementation and execution.<br />
Data Assistant: She/He will assist the community mobilizer and existing staff of the District PMU in all the<br />
ASHA related work.<br />
ASHA Help Desk: An ASHA help desk will be formed at the district level whose overall in-charge will be the<br />
community mobilizer. This will be expanded to the block level for strengthening of referral support system, to<br />
redress grievances of ASHAs, if any and to work as an information networking and management system.<br />
1.13. At the Block Level<br />
Block ASHA Manager/ Block Level Organizer– An Officer will be appointed as a block level organizer for<br />
effective programme management, implementation and execution and to act as a link and network between the<br />
ASHAs and the District and will be assisted by a facilitator 1 on every 20 ASHAs. The Facilitator will be the<br />
21 st ASHA worker. This will help in building up and developing the necessary skill required for a community<br />
health worker in a sustainable way.<br />
137
ASHA Help Desk: An ASHA Help Desk will be formed also at the block level. Overall in-charge of Block<br />
level ASHA Help Desk will be block level organizer and MOIC. This shall be in network with the District<br />
Level ASHA Help Desk. It will act as a network integrating the Village, Block and the District. It will help in<br />
strengthening referral support system, redress grievances of ASHAs, if any, and work as an information<br />
networking and management system.<br />
1.14. At the Village Level<br />
Community Monitoring and Community Need Assessment: Community-based Monitoring ensures that the<br />
services reach those for whom they are meant, for those residing in rural areas, especially the poor, women and<br />
children. Community Monitoring is also seen as an important aspect of promoting community led action in the<br />
field of health and to understand if the work is moving towards the decided purpose. Although, ASHA hails<br />
from the same village, she may not be having knowledge and information on the health status of the village<br />
population. For this purpose, she will be advised to visit every household and undertake a sample survey of the<br />
residents of the village to understand their health status. In this way she will come to know the villagers, the<br />
common diseases which are prevalent amongst the villagers, the number of pregnant women, the number of<br />
newborn, educational and socio-economic status of different categories of people, the health status of weaker<br />
sections especially scheduled castes/scheduled tribes etc. She will be provided with a simple format for<br />
conducting the surveys. The ASHA Activity Diary will also help her keep a record of the base level. In this she<br />
should be supported by the AWW and the Village Health & Sanitation Committee. Such a review will help to<br />
identify obstacles in the work, so that appropriate changes can be made to cross the obstacles by the team of the<br />
block level organizers.<br />
Networking with VHSC, PRI and SHGs – All ASHAs will be involved in this Village Health and Sanitation<br />
Committee of the Panchayat, as Members. ASHAs will coordinate with Gram Panchayat in developing the<br />
village health plan, along with the Block Level Organizer, Block Medical Officer and Block Facilitator. The<br />
untied funds placed with the Sub-Centre or the Panchayat will be used for this purpose. The SHGs, Womans<br />
Health Committees, Village Health and Sanitation Committees of the Gram Panchayat will be major sources of<br />
support to ASHA. The Panchayat members will ensure secure and congenial environment for enabling ASHAs<br />
to function effectively to achieve the desired goal.<br />
1.15. ASHA Training<br />
The second phase of ASHA training which includes the 2 nd , 3 rd and 4 th modules is being done by PHED and its<br />
NGOs. The <strong>State</strong> Level ToT has been completed and the district level training is going on. The District resource<br />
person will in turn train the ASHAs at the Block Level. Additionally against the revised ASHA target, the new<br />
incumbents shall have to be provided trainings on Module 1, 2,3 and 4.<br />
138
1.16. ASHA Drug Kit and it’s replenishment<br />
To ensure provision of ASHA Drug Kit to 12822 new ASHAs and replenishment as it is one of the key<br />
components of NRHM<br />
1.17. Emergency Services of ASHA<br />
Bihar has been experiencing regular floods which have created havocs in lives of lakhs of people both<br />
economically and psychologically. During the time of floods, health related problems become extremely acute.<br />
In such a situation the role of ASHA becomes extremely crucial. Thus ASHAs will be provided intensive<br />
training/capacity building preferably of three days and would then be deputed in 16 flood prone districts or<br />
similar natural disaster areas.<br />
1.18. Motivations for ASHA<br />
Provision of Two Sarees to ASHA – The provision of Sarees will ensure the following:-<br />
· The availability of Sarees will help in building up of better motivation of the ASHA workers.<br />
· Identification in any work helps in rooting identity for the worker and the work itself. The<br />
availability of Sarees will help in doing so.<br />
· Sarees will help in easy deliverance of work and make the worker more accessible by the<br />
community as it will help in easy identification of the ASHA worker.<br />
· It will help in boosting the morale of the ASHA worker and shall make the relationship stronger<br />
and would help in connecting the ASHA worker and the <strong>State</strong>.<br />
Provision of One Umbrella to ASHA– The provision of Umbrella will ensure the following:-<br />
· The availability of Umbrella will act as an aid to the ASHA worker in extreme weather conditions,<br />
which will facilitate the health facility/services in a smooth way<br />
· The availability of Umbrella will help her comply with her nature of work<br />
· It will help in building up of motivation of the ASHA worker, enhance her identity.<br />
· It will help in boosting the morale of the ASHA worker and making the relationship stronger and<br />
ensure connectivity between the ASHA worker and the District<br />
1.19. Capacity Building/Academic Support Programme:<br />
a) Enabling ASHA 10 th pass For upgradation of academic strength of ASHA, SHSB will provide examination<br />
fees for the 10 th examination of open schooling mode/Board/IGNOU to 1000 ASHAs in 1 st Phase. Fee for the<br />
same to be provided by SHSB.<br />
b) Training for Help Desk The person/officer involved in operationalising the ASHA help desk at District<br />
level and Block level will be trained.<br />
139
1.20. ASHA Divas<br />
ASHA Divas will be held per month. This will include the following componentsü<br />
Monthly Meetings for ASHA Divas of ASHAs, ANMs and AWWs shall provide the necessary<br />
platform to share the work experiences, identify the loop holes and work towards the same.<br />
ü Best ASHA worker and ANM worker felicitation as per their monthly performance at the<br />
ASHA Divas will provide motivation. The performance will be rated as per the ASHA Activity<br />
Diary.<br />
ü Provision of I-Card will be done to the newly selected ASHA workers.<br />
ü Replenishment of ASHA Drug Kit for at least the next two months. This will ensure treatment<br />
of common ailments and first level prompt care and referrals initiated based on symptoms of<br />
necessary cases. For this, effective access to basic drugs in every village should be ensured<br />
through ASHA Drug Kit.<br />
Key Dimension of ASHA Programme:-<br />
· The structural mechanism relating to a support system for ASHAs will ensure the facilitation of<br />
effective service delivery and a clear communication channel from the Block to the <strong>State</strong>. The Human<br />
resource in form of a strong network system will provide the necessary support for effective<br />
implementation and execution of the ASHA Programme.<br />
· Continued training and capacity building to the ASHAs will facilitate the service delivery and ensure<br />
community broad basing of the programme.<br />
· Inter-sectoral convergence among different health related institutions and individuals will ensure<br />
effective service delivery. The ASHA Help Desk will ensure an extensive and intensive communication<br />
and management system right up to the community level.<br />
· Empowering ASHA through various motivational methods including provision of Sarees and umbrella,<br />
best ASHA felicitation, performance based incentive, capacity building, training, documenting the work<br />
through ASHA activity diary and register, incentive to ASHA for mobilizing ANC and PNC Cases for<br />
check-up and ASHA help desk will assist and facilitate overall development of the worker.<br />
· Additionally, the ASHA being a facilitator at the Block Level will also go in a long way towards<br />
developing the necessary skills of a Community Health Worker, making the whole process sustainable<br />
and empowering the worker and the community itself.<br />
140
· A Community based monitoring system coupled with operational research and continued evaluation<br />
will help in field level analysis and seminars for consultation of the same will help in holistic strategy<br />
development.<br />
Budget:<br />
Sr. No. Particulars Tentative Budget<br />
(A) AT THE <strong>STATE</strong> LEVEL<br />
1 Personnel on contract<br />
1. Project Manager (MBA/PG in HRD) - Rs.25,000/- per<br />
5,40,000/-<br />
month x12 months = Rs.3,00,000<br />
2. Deputy Project Manager (Master in Social Works) <br />
Rs.20000/- per month x 12= Rs.2,40,000/-<br />
Total of (1)+(2)= Rs.5,40,000/-<br />
3 Development of IEC and monitoring materials (ASHA flip chart,<br />
2,61,40,500/-<br />
ASHA Activity Diary, ASHA Register, IEC material, reporting<br />
format, monitoring formats and resource materials for meetings) =<br />
300 x 87135 = 2,61,40,500/-<br />
4 Monitoring and supervision 2,00,000/-<br />
5 Operation research and documentation 2,00,000/-<br />
6 ASHA Sammelan and exposure visits @ Rs. 150/- per ASHA<br />
1,30,70,250/-<br />
(Rs.100/- Hon. + Rs.50/- TA/DA)= 150 x 87135 = 1,30,70,250/-<br />
7 Workshops, seminars and Meetings 2,00,000/-<br />
8 ASHA Mentoring Group Budget 2,00,000/-<br />
9 Contingency 1,00,000/-<br />
Total (A) 4,06,50,750/-<br />
(B) ASHA Support System at the District Level<br />
1 Strengthening of the District PMU for undertaking ASHA support<br />
system<br />
Additional Personnel<br />
(a) Community Mobilizer/District Project Manager-ASHA (Master<br />
in Social Work) Rs.20,000/- per month x 12 months =<br />
Rs.2,40,000/- who will report to District Nodal Officer<br />
21,60,000/-<br />
141
(b) Data Assistant (Graduate with Basic Computer knowledge) - to<br />
strengthen the District PMU to take additional work. He/She will<br />
assist the existing staff of District PMU in all the work related to<br />
NRHM including ASHA related work. Rs.8,000/- per month x12<br />
months = Rs. 96,000/-<br />
(c) TA/DA to be paid from District Health Society (Programme<br />
Management Cost) for monitoring visits and collection of<br />
information Telephone, fax, computer, stationeries etc to be used<br />
from District PMU (3000 x 12 x 38 = 13,68,000.00)<br />
(d) ASHA Help Desk at the district level (As In-charge Community<br />
Mobilizer) = 1000/- x 38 district x 12 months =4,56,000.00<br />
(C) ASHA Support System at the Block Level<br />
(A) Block ASHA Manager/An officer Block Level Organizer in<br />
all the blocks. (Rs. 12000 x 533 x 12 months = Rs. 7,67,52,000.00)<br />
(B) ASHA Help Desk at the Block Level (as in-charge Block Level<br />
Organizer and MOIC) = 500/- x 533 x 12= 31,98,000/-<br />
(D) ASHA Support System at Village Level<br />
Community Monitoring and Community need assessment<br />
1 (20 ASHA and block facilitator, PRIs, SHG, two beneficiaries and<br />
NGO representative.)(Rs.150/- x 2500 x 12) = 45,00,000/-<br />
(E) ASHA Trainings<br />
1 One day Orientation programme of <strong>State</strong> Level resource person =<br />
65,000/-<br />
2 12 days training of District Resource Team<br />
(38 district x Rs.2,35,000/-)= 89,30,000/-<br />
3 12 days training of ASHA at Block level (2489 batches x<br />
Rs.1,00,000/-) = 24,89,00,000/-<br />
7,99,50,000/-<br />
45,00,000/-<br />
8,68,95,000/-<br />
(Rs.17.15 crores was made<br />
available in 2008-09, of<br />
which approx. Rs.50.00<br />
142
4 Documentation and Development of IEC materials = 5,00,000/- lakhs has been spent.<br />
Therefore of the total<br />
requirement of Rs.<br />
25,83,95,000/- additional<br />
fund required for 2009-10<br />
is 13,82,92,850/- and the<br />
balance available amount in<br />
SHSB may be ratified for<br />
use in 2009-10)<br />
Total (B+C+D+E) 17,35,05,000/-<br />
(F) ASHA Drug Kit & Replenishment<br />
1 Drug Kit @ Rs. 600/- for 12822 ASHA<br />
7693200<br />
Replensihment of Drug Kit @ 74313 ASHAs x Rs.200/-<br />
1,48,62,600/-<br />
Total 2,25,55800<br />
(G) Emergency Services of ASHA<br />
Deputation/ engagement of ASHA in Flood and other natural<br />
1 calamities for flood prone district (20 days x Rs.100 per day x<br />
approx 3000 ASHA= 60,00,000.00) 66,00,000/-<br />
Capacity Building/Training of ASHA in Flood and other natural<br />
2 calamities for flood prone district ( 2 days x Rs. 100 per day x<br />
approx 3000 ASHA = 6,00,000.00)<br />
(H) Motivation of ASHA<br />
1 Provision of two Sarees to ASHAs (87135 ASHAxRs.600( two<br />
Sarees) =5,22,81,000/- 6,31,72,875/-<br />
2 Provision of one umbrella to ASHAs (87135 ASHAs x Rs.125/-)<br />
=1,08,91,875/-<br />
(I) Capacity Building/Academic Support Programme<br />
1 Approx. 1000 ASHAs in the <strong>State</strong> to be enrolled into 10 th grade or<br />
Bachelors Preparatory Programme through Open Schools or<br />
IGNOU. Fee for the same to be provided by SHSB. The amount<br />
10,00,000/-<br />
being requested is less, more shall be requested in case of god<br />
response to the proposal.<br />
@ Rs.1000 x 1000 students =10,00,000<br />
2 Training for ASHA Help Desk (1104 x 500/-)= 5,52,000/- Provisioned in IEC<br />
component of Part A<br />
Total (F+G+H+I) 10,47,28,675/-<br />
143
1<br />
(J) ASHA Divas<br />
TA/DA for ASHA Divas @ Rs.75 per ASHAs per month<br />
(Rs. 87135 x 75x12) = 7,84,21,500/-<br />
2 Best performance award to ASHAs at district level. @ Rs.2000 per<br />
block=<br />
3 ASHAs from each block @ Rs.1000 for 1 st , Rs.500 for 2 nd and<br />
Rs. 300 for 3 rd prize, Rs. 200 for Certificate printing and<br />
distribution = Rs. 2000 x 533) = 10,66,000/-<br />
(For this activity the administrative system/procedure shall be<br />
chalked out with support of Development Partners)<br />
3 Identity Card (Rs. 20 x 87135) = 17,42,700/-<br />
8,12,30,200/-<br />
Total (J) 8,12,30,200/-<br />
Grand Total( A+B+C+D+E+F+G+H+I+J) 38,87,14,625/-<br />
Forty nine crores Eighty six lakhs Thirty four thousand Eight hundred and Seventy five Rs. only.<br />
144
Total Budget under ASHA Scheme<br />
Sl Particulars Amount (Rs.)<br />
1 ASHA Support System at <strong>State</strong> Level 4,06,50,750/-<br />
2 ASHA Support System at District Level 21,60,000/-<br />
3 ASHA Support System at Block Level 7,99,50,000/-<br />
4 ASHA Support System at Village Level 45,00,000/-<br />
5 ASHA Trainings 8,68,95,000/-<br />
6 ASHA Drug Kit & Replenishment 2,25,55,800/-<br />
7 Emergency Services of ASHA 66,00,000/-<br />
8 Motivation of ASHA 6,31,72,875/-<br />
9 Capacity Building/Academic Support Programme 10,00,000/-<br />
10 ASHA Divas 8,12,30,200/-<br />
Total Budget for ASHA 38,87,14,625/-<br />
Work-plan for ASHA Program<br />
Activities 2009-10<br />
Q1 Q2 Q3 Q4<br />
Development for IEC and monitoring material<br />
(IEC material, reporting format, ASHA Flip Chart, ASHA Activity Diary,<br />
ASHA Register, monitoring formats and resource material for meetings)<br />
Monitoring and supervision<br />
Operation research and documentation<br />
ASHA sammelan and exposure visits<br />
Workshops, seminars and Meetings<br />
Trainings<br />
Emergency Services of ASHA<br />
Empowerment of ASHA<br />
Capacity Building<br />
ASHA Divas<br />
145
1.21 Untied Fund for Health Sub Centre, APHC and PHC<br />
The objective of the activity is to facilitate meeting urgent yet discrete activities that need relatively small sums<br />
of money at Health Sub Centers.<br />
The suggested areas where Untied Funds can be used mentioned below:<br />
Þ Cover minor modifications to sub center-curtains to ensure privacy, repair of taps, installation of bulbs,<br />
other minor repairs, which can be done at the local level;<br />
Þ Ad hoc payments for cleaning up sub center, especially after childbirth; transport of emergencies to<br />
appropriate referral centers;<br />
Þ Purchase of consumables such as bandages in sub center;<br />
Þ Purchase of bleaching powder and disinfectants for use in common areas of the village;<br />
Þ Labour supplies for environmental sanitation, such as clearing/ larvicidal measures for stagnant water<br />
Þ Payment/reward to ASHA for certain identified activities.<br />
Budget<br />
Budget Head<br />
Untied Fund<br />
Sub-Heads<br />
@<br />
Proposed Budget<br />
(in Crores)<br />
Untied fund for sub-centre Rs. 10,000 x 8858 no. 8,85,80,000<br />
Untied fund for APHCs 1243 APHC x 25,000 3, 10, 75,000<br />
Untied fund for PHCs 533 PHC x 25,000 133, 25, 000<br />
For meetings at HSC Rs. 2000 x 38 district 76000<br />
PHC level ANMs 533 PHCs x Rs.3000) 15,99,000<br />
Orientation on Guidelines<br />
for Untied Funds for HSC<br />
Quarterly review meeting Rs.1000 per meeting x 4<br />
1,52,000<br />
of the ANMs under the<br />
chairmanship of PHC<br />
Medical Officer to monitor<br />
the usage of the fund<br />
quarter x 38 districts<br />
Total 13,48,07,000<br />
146
1.22 Village Health and Sanitation Committee<br />
Government of Bihar has decided to merge Village Health and Sanitation Committee with “Lok Swasthya<br />
Pariwar Kalyan and Gramin Swaschata Samiti constituted by Department of Panchayat Raj in Bihar.<br />
Budget<br />
Budget Head<br />
Untied Fund for VHSC<br />
Sub-Heads<br />
@<br />
Proposed Budget<br />
(in Crores)<br />
Untied fund for VHSCs 45077 villages x 10,000 450770000<br />
(Fund of Rs.10.00 cr is<br />
available in SHSB, so the<br />
balance amount of<br />
Rs.35,07,70,000/- is<br />
Training of members of<br />
VHSC regarding<br />
functioning mechanism at<br />
the PHC level<br />
required)<br />
533 PHCs x Rs.2500 13,32,500<br />
Total 35,21,02,500/-<br />
1.23 Seed Money for Rogi Kalyan Samitis<br />
Aims and Objectives<br />
The objectives of the RKS is :<br />
» Upgrade and modernize the health services provided by the hospital and any associated outreach<br />
services<br />
» Supervise the implementation of National Health Programme at the hospital and other health<br />
institutions that may be placed under its administrative jurisdiction<br />
» Organize outreach services / health camps at facilities under the jurisdiction of the hospital<br />
» Monitor quality of hospital services; obtain regular feedback from the community and users of the<br />
hospital services<br />
» Generate resources locally through donations, user fees and other means<br />
Functions of the RKS<br />
To achieve the above objective, the Society utilizes its resources for undertaking the following activities/<br />
initiatives:<br />
» Acquire equipment, furniture, ambulance (through, donation, rent or any other means) for the hospital<br />
147
Budget<br />
» Expand the hospital building, in consultation with and subject to any guidelines that may be laid<br />
down by the GoBMake arrangements for the maintenance of hospital building (including residential<br />
buildings), vehicles and equipments available with the hospital<br />
» Improve boarding/lodging arrangements for the patients and their attendants<br />
» Enter into partnership arrangement with the private sector (including individuals) for the<br />
improvement of support services such as cleaning services, laundry services, diagnostic facilities and<br />
ambulatory services etc<br />
» Develop/lease out vacant land in the premises of the hospital for commercial purposes with a view to<br />
improve financial position of the Society<br />
» Encourage community participation in the maintenance and upkeep of the hospital<br />
» Promote measures for resource conservation through adoption of wards by institutions or individuals<br />
» Adopt sustainable and environmental friendly measures for the day-to-day management of the<br />
hospital, e.g. scientific hospital waste disposal system, solar lighting systems, solar refrigeration<br />
systems, water harvesting and water re-charging systems etc.<br />
Budget Head<br />
Rogi Kalyan Samiti<br />
Sub-Heads<br />
@<br />
Proposed Budget<br />
(in Crores)<br />
District Hospitals 27 hospitals X 5 lakhs 1.35<br />
Sub-divisional hospitals 23 hospitals X 5 lakhs 1.15<br />
Referral hospitals 70 hospitals x 1 lakhs 0.70<br />
PHCs 533 PHCs x 1 lakhs 5.33<br />
Sensitization workshop for<br />
RKS members (653 x 3<br />
members =1959) at the<br />
sub-divisional level (TA,<br />
Food, Resource materials,<br />
resource persons etc)<br />
Exposure visit of members<br />
of RKS of 10 nonperforming<br />
districts to<br />
districts where RKS are<br />
performing<br />
217 participants x 9<br />
divisions x Rs.1000=<br />
19,53,000<br />
@ 2 members/RKS x 10<br />
hospitals x 10 districts =200<br />
x Rs.2000=4,00,000<br />
Provisioned in IEC<br />
componet (Part A)<br />
Provisioned in IEC<br />
componet (Part A)<br />
Total 8,53,00,000/-<br />
148
Infrastructure Development<br />
2.1 Construction/Establishment of Health Sub Centre (HSC)<br />
NRHM aims to ensure HSC facility on the Govt. of India population norms of 1 per 5000 population in general<br />
areas and 1 per 3000 populations in tribal areas. As per 2001 Census, population of the Bihar <strong>State</strong> is<br />
approximately 8,29,98,509. Existing facility of HSCs are 8858 out of total requirement of 16623. To facilitate<br />
the above population the state requires 7765 HSCs additionaly to achieve the total target. It is proposed to create<br />
1553 HSCs every year for next five years.<br />
The revised estimate is @ 9.50 lakhs as per GoI norms. The <strong>State</strong> proposes to share 25% expenses in the<br />
construction of these HSCs and for land acquisition. The balance 75% the state has put under this <strong>PIP</strong> for<br />
financial support from NRHM. These Health Sub Centres shall either be constructed or shall be taken up on<br />
rental basis. The cost provided also includes cost of land acquisition if Govt. land is not available. Till such<br />
time construction is complete the state shall take buildings for these facilities on rental also.<br />
NRHM Action - Plan 2009-10<br />
Expected<br />
Details of Budget<br />
Proposed<br />
Proposed Physical Out<br />
Basis of Costing ( No. of Units X Unit Cost )<br />
Budget<br />
Activity Come<br />
2009-10<br />
Creation of<br />
Initiating<br />
Rs. 950.00<br />
Total cost @ Rs 9.50 lakh<br />
Contribution of<br />
Contribution<br />
HSC<br />
construction of<br />
Lakhs<br />
per unit<br />
GoI (75% of<br />
of GOB<br />
100 HSC.<br />
9.50 lakhs i.e<br />
(Rs.9.50-<br />
@7.125 lakhs<br />
7.125 =<br />
per unit )<br />
2.375 lakhs<br />
per unit)<br />
100 x 9.50= Rs. 950.00<br />
Rs. 712.5<br />
Rs.237.5<br />
Lakhs<br />
Lakhs<br />
Lakhs<br />
In the year 2008-09 funds for construction of 1985 HSCs were released to Building Constrution Department,<br />
which has initiated necessary actions. All though construction of 500 HSCs were proposed in 2008-09 and<br />
under NRHM GoI released Rs. 30 Crores. In the year 2009-10 it is proposed to construct buildings of next 100<br />
HSCs where land is available. For this an amount of Rs. 950.00 lakhs is required.<br />
For Construction work two agencies have been identified BCD and District Health Society, Bihar.<br />
149
2.2 CONSTRUCTION OF PHC<br />
NRHM aims to ensure PHCs on the Govt. of India population norm of 1 per 30000 populations in general areas<br />
and 1 per 20000 population in tribal/ remote areas. As per 2001 census, population of Bihar state is<br />
approximately 82958509. The existing facility of PHCs is 1243, whereas the total requirement is 2787 PHCs.<br />
There are 121 PHCs which do not have their own building. Therefore 1665 PHCs buildings require to be setup<br />
by 2010.<br />
Unit cost of construction and land acquisition is 53.15 lacs as per NRHM guidelines. Some of the facilities will<br />
be taken up on a rental basis. The total built-up area of the PHCs will be 63 hundred Sq feet, which will include<br />
1500 sq. ft. for PHC & 4800 sq. ft. for its residential quarters. These PHCs would either be constructed or shall<br />
be taken up on rental basis. The cost provided also includes cost of land acquisition if Govt. land is not available<br />
for construction. Till such time construction is complete the state shall take buildings for these facilities on<br />
rental also. In addition, it is proposed to construct residential quarters for the staff in 500 old APHCs<br />
(previously sanctioned) in an area of 3000 Sq. ft.<br />
Proposed Activity<br />
1. Construction of<br />
residential quarters<br />
of 200 old APHCs<br />
for Staff nurses<br />
NRHM Action - Plan 2009-10<br />
Expected Physical Out<br />
Come<br />
Construction to be done in an<br />
area of 3000 sq. ft. (1000 sq.<br />
ft. x 3 quarters) @ Rs. 30<br />
lakhs per APHCs.<br />
Funds to be released to the<br />
Construction Agency.<br />
Proposed Budget<br />
Rs. 6000.00 Lakhs.<br />
Details of Budget<br />
Basis of Costing<br />
( No. of Units X Unit<br />
Cost)<br />
2. Construction of<br />
building of 51<br />
APHCs where land<br />
is available<br />
Funds to be released to BCD.<br />
An amount of Rs. 2710.65<br />
lakhs is required for the<br />
construction. Against these<br />
Rs. 31 lakhs has already been<br />
released to BCD. Total fund<br />
required in 2009-10 will be<br />
Rs. 3,79,67,000 .00. The rest<br />
to be carried over in 2010-11.<br />
Rs. 3,79,67,000.00 Rs. 3,79,67,000.00<br />
Total – Rs. 63,79,67,000.00<br />
Say Rs. 6379.67 lakhs<br />
150
2.3 UPGRADATION OF COMMUNITY <strong>HEALTH</strong> CENTRE (CHC)<br />
NRHM aims to ensure CHCs on the Govt. of India population norm of 1 per 1.20 Lakhs populations. The Govt.<br />
of Bihar plans to upgrade all its PHCs and Referral Hospitals below the headquarter level to CHC as per IPHS<br />
standards. In the state of Bihar the total no of existing PHCs are 533 and the no of Referral Hospital is 70.<br />
Hence a total of 603 units are needed to be upgraded to CHC standard and converted to 30-bedded hospitals. It<br />
is proposed to upgrade 200 facilities every year. As per NRHM guideline the entire cost of construction would<br />
be borne by GOI.<br />
It is proposed to take up upgradation of 100 PHCs to CHCs in the year 2009-10 and the balance PHCs/Referral<br />
hospitals will be upgraded to CHCs in next year. The unit cost of construction and land acquisition will be<br />
around Rs. 40 lakhs. The upgradation of hospital buildings shall be taken up from funds provided by the <strong>State</strong><br />
Govt. The doctors and staff quarters shall be provided under the NRHM. In case adequate land is not available<br />
the fund can also be used for land acquisition. The doctors quarters would also be taken up on rental basis. The<br />
cost provided also includes cost of land acquisition if Govt. land is not available. The costs also include<br />
provision of equipment at these hospitals either as per IPHS standard or as required.<br />
Proposed<br />
Activity<br />
Creation and<br />
Up gradation<br />
of CHCs as<br />
per IPHS<br />
Standard<br />
.<br />
Up gradation of Community Health Centre As Per IPHS<br />
NRHM Action - Plan 2009-10<br />
Expected Physical Out Come<br />
Details of Budget<br />
Proposed<br />
Basis of Costing (No. Of<br />
Budget<br />
Units X Unit Cost)<br />
Preparation and Finalization of Maps. Rs.8040.00 lacs Unit cost @ Rs. 40 lacs<br />
Finalization of Construction Agency &<br />
(Contribution of GOI<br />
Initiating Renovation of CHCs.<br />
100%) @ Rs. 40 lakhs x<br />
Funds to be released for the construction<br />
100 = Rs. 4000.00 Lakhs<br />
agency.<br />
100 CHCs shall be taken up<br />
Quarters for Doctors and Staffs,<br />
for upgradation.<br />
for the Purchase of New Surgical<br />
Rs. 4000 lakhs has already<br />
instruments, Equipments, Furniture,<br />
been approved by the GoI in<br />
2008-09 and has been<br />
received and the amount<br />
shall be expended this year<br />
in 2009-10.<br />
151
2.4 Infrastructure and Service improvement as per IPHS in 48 (District and Sub-<br />
Divisional) Hospitals for Accreditation / ISO : 9000 certification of Health<br />
Facilities<br />
The state of Bihar has 25 District Hospitals & 23 Sub Division Hospital at present. Construction for 11 District<br />
Hospitals are under process and have been nearly completed. Most of these District hospitals are 100 to 200<br />
bedded. The state has already appointed one hospital consultancy firm to carryout the situation analysis of these<br />
District Hospitals and prepares a master plan in terms of Infrastructure, Equipment and Manpower for<br />
strengthening these hospitals as per IPHS.<br />
The state with the help of NHSRC is in the process of ISO accreditation/certification for its District Hospital at<br />
Bhojpur. This year Bihar would like to outsource this task through NHSRC or some competent agencies to take<br />
up its 23 DHs and 25 SDHs under ISO certification across the state for addressing quality issues.<br />
The state also intends to develop the hospitals at Rajvanshi Nagar, Rajendra Nagar, Gardiner Road,<br />
Gardanibagh and Guru Govind Singh Hospitals at Patna into super speciality hospitals.<br />
The preparation of Master Plan will be completed within six months after which the state will take up the<br />
strengthening work. The upgradation would include upgradation of Civil Infrastructure as well as provision of<br />
equipment. The cost provided also includes cost of land acquisition if Govt. land is not available. The costs also<br />
include provision of equipment at these hospital either as per IPHS standard or as required. The costs also<br />
include provision of equipment at these hospitals either as per IPHS standard or as required.<br />
Budget:<br />
Activity Amount ( In Rs )<br />
Strengthening/Up gradation of District Hospitals, Sub-Divisional 3,40,00,000/-<br />
Hospitals and Super-Specialty Hospitals as per IPHS Standard<br />
Accreditation/ISO certification for 48 (District Hospitals + SDH) 9,60,00,000/-<br />
x Rs.20.00 lakhs<br />
Total 13,00,00,000/-<br />
2.5 Upgradation of Infrastructure of ANM Training Schools<br />
In year 2008-09, a <strong>State</strong> coordination committee for the strengthening ANM and GNM schools has been<br />
activated under the chairmanship of the Additional Commissioner, Health. The Executive Director, SHSB,<br />
152
officers from the Directorate and SHSB and UNICEF are its members. The committee has chalked a<br />
comprehensive strategy for the rejuvenation of the ANM and GNM schools.<br />
Key decisions made till now include<br />
Streamlining the student intake in all ANM and GNM schools up to their full capacity<br />
Ensuring that the vacant faculty and staff positions in all the schools are filled through<br />
contractual appointments to undertake teaching assignment sas per INC norms<br />
Finalizing five ANM schools in PPP mode<br />
Formulation of the managing committee at respective ANM and GNM schools to look after the<br />
local management affairs<br />
Strengthening the hands of the principals of these institutes<br />
Reviewing the progress on a regular basis<br />
Initiatives have been taken in Operationalisation of 22 ANM schools in terms of -<br />
site assessment,<br />
basic renovation,<br />
provision of kitchen items, audiovisual equipments, lab equipments<br />
provision of study material,<br />
capacity building of faculty,<br />
standard curriculum development for the ANMs and GNMs<br />
Facilitation in accreditation from Nursing Council of India.<br />
It is proposed to upgrade the Infrastructure of 22 ANM and 6 GNM Training Schools. In addition, the state is<br />
willing to open up more ANM and GNM schools as per the GoIs letter in this regard. The approximate cost of<br />
up gradation of each ANM/GNM Training Schools is expected to be Rs 50 lakhs per Unit. It was proposed to<br />
upgrade the Infrastructure of 12 ANM Training Schools in 2008-09 <strong>PIP</strong> and a fund for the same to the tune of<br />
Rs.3.00 crores is available.<br />
Additional funds are requested for the remaining 9 ANM schools and 6 GNM schools. The state is preparing a<br />
separate proposal to upscale the standards of nursing education. Additionally under PPP 5 ANM schools are<br />
proposed to be operationalised.<br />
M.Sc/B.Sc. nursing faculty for nursing school to be taken from hindi speaking states like MP, Pondicherry, for<br />
which Govt of India shall be approached for coordinating the same.<br />
Budget<br />
S No Description App. cost Duration Total<br />
1 Upgradation of infrastructure of 12 Rs. 600 lakhs Rs. 6,00,00,000/-<br />
153
ANM Training School including<br />
provision of furniture & equipment<br />
2 Strengthening of Nursing cell in the<br />
GoB<br />
3 Hiring of additional faculty for all<br />
ANM and GNM schools<br />
(Above fund is already<br />
available from S<strong>PIP</strong><br />
2007-08, 08-09)<br />
@Rs 50 lakhs 50,00,000<br />
Rs 50.00 lakhs Every year 50,00,000<br />
Total 7,00,00,000/-<br />
2.6 Annual Maintenance Grant<br />
During the course of up-gradation in setting up of different units in the different health facilities of the state,<br />
maintenance will also be essentially required. It is proposed that all district hospitals and sub divisional hospital<br />
are provided @ Rs.5 lacs and Referrals/PHCs @ Rs.1 lakh. Fund for the same was approved in 2009-10.<br />
Budget<br />
Activities<br />
Disbursement of the Grant at the end of the meeting on the same day to the<br />
respective medical officers (district hospitals (23) and sub divisional hospital<br />
(25) @ Rs.5 lacs, Referrals/PHCs (55+533) @ Rs.1 lakh)<br />
Total purposed<br />
budget<br />
Rs.8,20,80,000<br />
Contractual Manpower<br />
3.1. Incentives, Contractual Salaries and Bonus<br />
As human resources are the most important resource steps shall be taken to motivate them through various<br />
benefits and incentives like Cellphone facility for all ANMs, MOICs, Programme Officers, CDPOs etc. and<br />
rural and specialist incentives. All the doctors posted in the rural area would get an additional incentive of<br />
Rs.3000.<br />
A provision for Rs.50,000/- per PHC per year will be given as incentive to the PHCs for better performing in<br />
services.<br />
All the doctors performing specialist duties including the MBBS doctors trained for specialized tasks e.g. Life<br />
saving Anesthesia skills etc. will get an incentive of Rs.4000.<br />
154
Budget:<br />
Sub-Heads<br />
Incentive for PHC doctors & staffs @<br />
Rs. 50,000 for better performance in<br />
implementing programmes<br />
Salaries for contractual Staff Nurses<br />
(2900 existing and 910 new)<br />
Contract Salaries for ANMs (around<br />
8000) in year 2009-10<br />
3500 ANM will be paid by NRHM<br />
(Rest 4500 ANM will be paid by<br />
Treasury Root)<br />
Mobile facility for all health<br />
functionaries<br />
@<br />
Rs. 50,000/ - per year for about 250<br />
PHCs<br />
Rs.7500 per month<br />
Rs.6000 per month (12 Months<br />
Consolidated Salaries for<br />
Contractual ANMs)<br />
District officials, PHC in charge,<br />
CDPOs and ANMs @ 500 per<br />
Proposed Budget<br />
(Rs. In lakhs)<br />
125.00<br />
3439.00<br />
2520.00<br />
month 600.00<br />
Total 6767.02<br />
3.2. Block Programme Management Unit<br />
The state has already established Block Programme Management Unit in all the 398 Block PHCs. This year the<br />
state will establish the next 135 Block Programme Management Unit. Each BPMU consist of One Block Health<br />
Manager and One Accountant.<br />
It has been observed that<br />
after the establishment of BPMUs the implementation of National Programmes has been managed efficiently<br />
and getting improved results.<br />
Budget<br />
A. Recurring Expenses of 533 BPMUs<br />
Sl Particulars Qty Rate (Rs.) Amount (Rs.)<br />
1 Salary of Block Health Manager 1 12000/- pm 1,44,000/-<br />
2 Salary of Block Accountant 1 8000/- pm 84,000/-<br />
3 Mobility and Office Expenses 1 25000/- pm 3,00,000/-<br />
Recurring Expenses Per BPMU per Year 5,28,000/-<br />
Recurring Expenses of 533 BPMUs per Year 28,14,24,000/-<br />
B. Establishment Expenses for 135 BPMUs<br />
155
Sl Particulars Qty Rate (Rs.) Amount (Rs.)<br />
1 Computer System with Printer 1 50,000/- 50,000/-<br />
2 Furniture 1 10,000/- 10,000/-<br />
Establishment Expenses Per BPMU per Year 60,000/-<br />
Establishment Expenses of 135 BPMUs 81,00,000/-<br />
Total Budget for 2009-10 for Block Programme Management Unit (A + B) = Rs. 28,95,24,000/-<br />
3.3. Additional Manpower for <strong>State</strong> Health Society, Bihar<br />
NRHM being a large programme covering various components, SHSB requires more manpower to run the<br />
programmes. The <strong>State</strong> Health Society requires additional manpower other than <strong>State</strong> Programme Management<br />
Support to manage all the Programmes under NRHM umbrella. This year state also proposes to put 2 nos.<br />
Executive Engineers and 1 Bio-Medical engineer under SHSB for monitoring the construction and equipment<br />
activity under NRHM.<br />
The details of Manpower as follows with Budget:<br />
Details of Staff<br />
Sl Post Salary (pm) Salary (pa)<br />
1 Accountant (RNTCP) 15000 180000<br />
2 Pharmacist (RNTCP) 11500 138000<br />
3 Data Assistant (RNTCP) 9000 108000<br />
4 Computer Operator (RNTCP) 8000 96000<br />
5 Accountant (NBCP) 15000 180000<br />
6 Computer Operator/Data Assistant (NBCP) 8000 96000<br />
7 Steno-cum-LDC (NBCP) 8000 96000<br />
8 Computer Programmer (NLEP) 15000 180000<br />
9 Data Officer (Malaria/Kalazar) 15000 180000<br />
10 Computer Operator (Malaria/Kalazar) 8000 96000<br />
11 Store Keeper (Malaria /Kalazar) 8000 96000<br />
12 Accountant (Filaria) 15000 180000<br />
13 Computer Operator (Filaria) 8000 96000<br />
Total Per Annum 1722000/-<br />
10% annual increment as approved by the Governing Body of<br />
SHSB, therefore the total required =<br />
Rs.18,94,200/-<br />
156
Details of Programme Officers<br />
For Government officials on deputation new salary slab as such is proposed-<br />
Sl. Name Salary Pm Salary (pa)<br />
1 Administrative Officer- SHSB 34143 409716<br />
2 Programme Office - TB 32983 395796<br />
3 Programme Officer-Kalazar/IDSP 38643 463716<br />
4 Programme Officer -Blindness 29882 358584<br />
5 Programme Officer- IDD/Filaria 35664 427968<br />
6 <strong>State</strong> Immunization Officer 42108 505296<br />
7 Programme Officer-Malaria 30751 369012<br />
8 Programme Officer - Leprosy 30000 360000<br />
Total Salary of ProgrammeOfficers 274174 32,90,088<br />
Details of Engineers<br />
Sl. Name Salary Pm Salary (pa)<br />
1 Executive Engineer - SHSB 2 no. 30000 x 2<br />
2 Bio-Medical Engineer SHSB 1 no. 25000 x 1 10,20,000<br />
Total Salary for Engineers 85000<br />
-<br />
Total Budget for Additional Manpower at SHSB = Rs. 62,04,288/-<br />
3.4. Additional Manpower under NRHM<br />
Being a big state, Bihar requires more manpower to provide services at various facility levels.<br />
Moreover the infrastructure development is happening at a snails pace. To expedite this, it is proposed to hire 1<br />
Assistant Engineer at each district and 1 Junior Engineer for every four (4) blocks) on contract<br />
Budget<br />
Sl. Name Salary Pm Salary (pa)<br />
1 Hiring of AE on contract<br />
Rs.22,000/- x<br />
38 districts x 9<br />
months 75,24,000<br />
2 Hiring of JE<br />
Rs.15,000 x 9<br />
months x 133<br />
blocks 1,79,55,000<br />
Total Salary 2,54,79,000/-<br />
157
PPP Initiatives in <strong>State</strong><br />
4.1 Emergency Medical Service /102 – Ambulance Service<br />
The Toll free number 102 was launched during 2006-07 and is running in all the six regional headquarters<br />
successfully. Under this scheme Ambulance for emergency transport is being provided in all the districts of<br />
Bihar. The empanelled ambulance & ambulance available in Govt. institutions are made available on receipt of<br />
calls from the beneficiaries.<br />
This service has been outsourced to a private agency for Operationalisation. The Telephone Charges for the free<br />
toll free number is paid to BSNL by SHSB. The amount required would be for payment of incoming calls<br />
received from the beneficiaries.<br />
In the year 2008-09 (figures till December 2008) 12131 requisitions have been successfully met by this service.<br />
Budget summary of 102 :<br />
Budget Head<br />
102 Emergency Service<br />
Sub-Heads<br />
@<br />
Proposed Budget<br />
(in Crores)<br />
Control Room (including office rent, Rs. 41,000.00 x 6 units = Rs,<br />
40,32,000.00<br />
salary of staff (24x7), stationary,<br />
2 outgoing telephones for compliance<br />
of 102 & for reporting to Headquarter)<br />
246000.00 x 12 months =Rs.<br />
29,52,000.00 + Per Control Room Rs.<br />
15,000.00 pm x 6 = 90,000.00 x 12<br />
months<br />
Total 40,32,000/-<br />
4.2. Doctor on Call & Samadhan: Dial 1911<br />
A scheme is operational in the state wherein patients can dial a number and call for doctors. For this a special<br />
toll free number of 1911 has been provided for w.e.f. 01.3.2008. The objective of the scheme is to give medical<br />
assistance to the patient at their home at any time as well as act as a Samadhan of Rogi Shikayat.<br />
Doctors and Specialists have been empanelled for this scheme. Pathology labs have also been attached to collect<br />
samples for tests from patients home.<br />
Budget summary of 1911:<br />
Budget Head<br />
1911 Doctor on Call service<br />
Sub-Heads<br />
Control room 3,500 per person (Two person) =<br />
7,000.00 per control room is being<br />
@<br />
Proposed Budget<br />
(in Crores)<br />
5,04,000.00<br />
158
Telephone bill<br />
Provision of Annual<br />
Maintenance of EPBAX<br />
paid to the outsourced agency. Rs.<br />
7,000.00 x 6 = Rs. 42,000 x 12<br />
months<br />
Each control room is being paid<br />
telephone bill (i) Doctors<br />
conferencing Rs. 1,500.00 x 12<br />
months = 18,000 x 6 control rooms =<br />
1,08,000.00 & (ii) Rogi Jan Shikayat<br />
Rs. 2,000.00 x 12 months = 24,000 x<br />
6 control room = Rs. 1,44,000.00.<br />
Rs. 10,000.00 per annum x 6 control<br />
room<br />
2,52,000<br />
60,000.00<br />
Total 8,16,000/-<br />
4.3. Additional PHC management by NGOs<br />
The state has started to outsource the management of Adll. PHCs to the NGOs. In 2008-09 the state has given 44<br />
Adll PHCs to the NGOs for management. The result was good and it has been observed that the NGOs are<br />
properly managing the PHCs. This year the state proposes to outsource another 56 Adll PHCs to the NGOs for<br />
management.<br />
Last year 44 PHCs were given @ Rs.75,500/- pm per Adll. PHC.<br />
This year the state proposes to provide Rs.1,00,000/- per APHC to additional APHCs.<br />
Budget<br />
Sl No Particulars Amount (Rs.)<br />
1 Recurring Cost for existing 44 Adll PHCs @ 75,500 x 12 3,98,64,000/-<br />
month<br />
2 Cost of New 56 Adll. PHCs @ Rs.75,500/- x 12 months 5,07,36,000/-<br />
(This fund shall be<br />
asked for subject to<br />
evaluation of the<br />
already running<br />
APHCs at pt. 1 above)<br />
Total 3,98,64,000/-<br />
159
4.4. American Association of Physicians of Indian Origin (AAPIO)<br />
AAPIO survey on Specific Disease:<br />
The Ministry of Overseas Affairs, Govt. of India and American Association of Physicians of Indian Origin<br />
(AAPIO) signed an MoU at the Pravasi Bharatiya Divas in Jan 2006 to conduct a study on 5 specific diseases.<br />
Thereafter a meeting of Core Committee was held in New Delhi in this regard.<br />
As a follow-up to the above activities this project was included in the Annual Plan of NRHM in 2008-09 and a<br />
provision of Rs.50 lakhs was made in the <strong>PIP</strong>. The sum of Rs.1.56 Crores for the project has already been<br />
approved.<br />
This year the <strong>State</strong> again proposes another installment of Rs.56 lakhs in the 2009-10 <strong>State</strong> <strong>PIP</strong>.<br />
4.5. <strong>State</strong> Health Resource Center<br />
<strong>State</strong> Health Resource Center has been established in <strong>State</strong> Health Society, Bihar with a two year contract<br />
starting from January 08. M/s HOSMAC has been awarded this work and the total budget cost has been<br />
divided into two parts-<br />
· Retainership Fee<br />
· Amount payable on completion of milestones<br />
A total of Rs. 2.00 crores was approved in previous years <strong>PIP</strong> and the balance amount available in SHSB of<br />
Rs.1,38,44,799/- shall be utilized in the FY 2009-10.<br />
4.6. Services of Hospital Waste Treatment and Disposal in all Government Health<br />
facilities up to PHC in Bihar (IMEP)<br />
Bio medical waste management has emerged as a critical and important function within the ambit of providing<br />
quality healthcare in the country. It is now considered an important issue of environment and occupational<br />
safety. As per the Bio-Medical Waste (Management & Handling) Rules, 1998, all the waste generated in the<br />
hospital has to be managed by the occupier in a proper scientific manner. The GoI has also issued the IMEP<br />
guidelines for SCs, PHCs and CHCs. The state has outsourced the Biomedical Waste Management system for<br />
all the Government hospitals.<br />
160
Strategy/Project Description<br />
<strong>State</strong> Health Society Bihar is implementing National Rural Health Mission (NRHM) to carry out necessary<br />
architectural correction in the basic health care delivery system. In order to provide quality services to the<br />
public, SHSB has sought Public Private Partnership in providing proper Hospital Waste Treatment and Disposal<br />
Services, in all Health facilities right from Medical Colleges to the PHCs.<br />
Services to be provided<br />
1. Provide Service of Hospital Waste Treatment and Disposal in all Medical Colleges, District Hospitals,<br />
Sub-Divisional Hospitals, Referral Hospitals and PHCs of the <strong>State</strong>.<br />
2. Install, Operate and maintain appropriate Common Biomedical Waste Treatment facility, as per the<br />
Biomedical Waste (Management & Handling) Rules, 1998 and subsequent amendments in it.<br />
3. Provide one day orientation training to all the health service providers.<br />
4. Maintain the above-mentioned arrangement for a period of minimum 10 years. The Common<br />
Biomedical Waste Treatment facilities are proposed to be established at various locations across the<br />
<strong>State</strong><br />
Setting up a Bio-Medical Waste Management System:<br />
1. The state has started a CWTF facility at Indira Gandhi Institute of Medical Sciences, Patna<br />
(autonomous institute). The facility has been approached for undertaking waste treatment for all PHCs<br />
to DHs in all the eight districts of Patna division.<br />
Status Registration of the health facilities with IGIMS and with Bihar <strong>State</strong> Pollution Control Board<br />
being ensured. Anticipated to be fully functional in all the eight districts by March 2009.<br />
2. As per the rules each CWTF should cater to all facilities in 100 Km radius, keeping this in mind, more<br />
CWTF are to be operationalised in each of the division except Patna (which already has such a facility).<br />
To implement the IMEP in a comprehensive systematic manner, Private Parties have been<br />
invited through National Open Tender. SHSB has already finalized two agencies for undertaking the<br />
BWM project that would set up CBWM Treatment facilities at various locations in the <strong>State</strong> and cater<br />
to all the PHCs to DHs to MCHs in all the Divisions except Patna.<br />
The agency shall ensure segregation and collection of waste, disinfection, treatment,<br />
transportation, handling and disposal of waste both within and outside the healthcare setting; also<br />
ensure use of protective devices and safety precautions. The objective being to ensure waste<br />
management, waste minimization and infection control.<br />
Trainings to be provided to health care workers and officers in Infection Management and<br />
Environment Plan implementation by the respective agencies. Payment is to be made on a per bed per<br />
day monthly basis to both IGIMS and the Private Agencies.<br />
Status - The project is in the finalization stage, agencies have been finalised and approval of the<br />
Governing Body of SHSB is awaited on the Contract to be signed with both the agencies<br />
161
and further approval of the Bihar <strong>State</strong> Pollution Control Board is awaited. GOI had approved an<br />
amount of Rs.10.00 crores for the project in <strong>PIP</strong> 2008-09.<br />
Budget<br />
Activities<br />
Dissemination and Sensitization workshops on IMEP Guidelines at<br />
divisional levels<br />
Training of in-house staff (ANM, Safai Karmacharis, clinical support staff)<br />
on recognizing, segregating and disposing of bio-medical wastes<br />
Operationalization of Biomedical Waste Management @ Rs. 0.08 lacs pm<br />
per PHC (533), Rs. 0.12 lacs per Referral Hospital and SDH (113) and Rs.<br />
0.30 lacs per DH (36) and Rs 0.45 lacs pm per Medical College (6)<br />
Total<br />
Total proposed budget<br />
(in Rs.)<br />
1,00,000/-<br />
10,00,000/-<br />
9,36,16,000/-<br />
9,47,16,000/-<br />
(The fund received<br />
for the activity in<br />
2008-09, may be<br />
approved for<br />
utilization in this FY<br />
of 2009-10)<br />
Work plan<br />
Activities<br />
Dissemination and Sensitization workshops on IMEP Guidelines at<br />
divisional level<br />
Training of in-house staff (ANM, Safai Karmacharis, clinical support<br />
staff) on recognizing, segregating and disposing of bio-medical<br />
wastes<br />
Operationalization of BMW at PHCs, SDH, Referral Hospitals, DHs<br />
and Medical Colleges<br />
2007-08<br />
Q1 Q2 Q3 Q4<br />
4.7. Dialysis Units in various Government Hospitals of Bihar<br />
It is proposed to set up & Operationalising Dialysis Units through Public Private Partnership (PPP) in 25<br />
Hospitals of Bihar. This would require operation, maintenance and reporting 24-hours 7 days a week Dialysis<br />
units in Hospitals.<br />
162
The <strong>State</strong> Government shall provide vacant space in the premises of the Hospital itself with additional space for<br />
washing and RO plant installation (incase it is not in-built). The space provided shall be approx. 750-1000 sq.ft.<br />
including RO plant. The agency has to provide everything from equipments & machine, logistics, consumables<br />
etc to suitable medical personnel to man these units. The agency has to also ensure the installation,<br />
maintenance, functioning with provision of technical manpower round the clock. No rates shall be charged from<br />
the patients.<br />
Tender bids have already been floated for the same and M/s Apollo Hospitals, Chennai have been finalized for<br />
undertaking the task. Government/SHSB shall pay a monthly rental to the agency, based on the monthly cost as<br />
projected by them in the financial bid.<br />
Status Negotiations are on with M/s Apollo on the costing for the Dialysis unit<br />
GOI had approved Rs.3.00 crores for the project in the last <strong>PIP</strong>.<br />
Budget<br />
Activities<br />
Project cost for one Dialysis unit with 8 Dialysis machines<br />
(covering suitable manpower, power, diesel, water, general medical<br />
indent & consumables, CMC, RO membrane changing, resin<br />
changing, pre-filter changing, activated carbon filter changing,<br />
sedimentation filter changing, insurance of equipments, building<br />
maintenance, administrative expense, contingency, depreciation on<br />
equipments etc)<br />
Total proposed budget<br />
Rs.50.00 lacs x 1 year x 6 units=<br />
Rs.3.00 Crores<br />
(The previously approved Rs.3.00 is<br />
available with the <strong>State</strong> which may be<br />
ratified for expenditure in 2009-10)<br />
4.8. Setting Up of Ultra-Modern Diagnostic Centers in Regional Diagnostic<br />
Centers (RDCs) and all Government Medical College Hospitals of Bihar<br />
<strong>State</strong> Health Society Bihar is implementing the National Rural Health Mission (NRHM) to improve the<br />
availability of and access to quality health care for people. Setting up of Ultra-Modern Diagnostic Centres<br />
through Public Private Partnership (PPP) in 9 Regional Diagnostic Centres (RDCs) and 6 Medical College<br />
Hospitals (MCHs) of Bihar has been initiated.<br />
Project Area Regional Diagnostic Centers in Ara, Gaya, Bhagalpur, Munger, Muzaffarpur, Motihari, Purnea,<br />
Saharsa and Chapra.<br />
Government Medical College Hospitals PMCH, NMCH, SKMCH, DMCH, ANMMCH, JLMNCH<br />
163
M/s Softline, New Delhi and M/s Doyen Diagnostics, Kolkata have been contracted to set up the Ultra-Modern<br />
Diagnostic Centers.<br />
Project Scope To operate, maintain and report 24-hours Ultra-Modern Diagnostic<br />
Centers in RDCs & MCHs and report the progress to the RDDs (who would be in-charge of<br />
monitoring the RDCs project) and the Superintendents (who would be in-charge of monitoring<br />
the MCH project) and the SHSB.<br />
Project Condition -<br />
The <strong>State</strong> Government has created the buildings for Regional Diagnostic Centers at all the towns<br />
mentioned in Project Area. In the case of MCHs, space shall be provided in the premises of the MCH<br />
itself at the discretion of the Superintendent of the concerned MCH.<br />
The agency has to provide everything from equipments & machine, logistics, consumables etc to<br />
personnel; the said RDC/MCH will only provide space for the Diagnostic Centre along with space for<br />
storage at a nominal monthly rent payable to the DHS of the concerned district (in the case of RDC) and<br />
the Rogi Kalyan Samiti of the concerned MCH (in the case of MCH) by the agency.<br />
The agency has to ensure the installation, maintenance, functioning with provision of expert technical<br />
manpower round the clock.<br />
Rates (to be charged from the users) shall be applicable as per AIIMS, New Delhi for the basic,<br />
standard and other specialized tests under each Diagnostic head.<br />
The project is on a revenue sharing model<br />
The project is for ten (10) years depending upon performance further extension will be considered.<br />
Facilities that will be provided in RDCs and MCHs areà Pathology- Bio-Chemistry, Radiology Digital x-ray,<br />
CT scan, MRI, ECG, Mammography.<br />
GOI had approved the project in the S<strong>PIP</strong> 2008-09.<br />
The state requires budget in this regard only for reimbursement to the Private Parties by the RKS of the concerned<br />
hospital for providing free services to BPL patients. All the remaining cost for setting up centers will be borne by<br />
the private providers.<br />
Budget<br />
Activities<br />
Total proposed budget<br />
Reimbursement cost to the Private Parties by the RKS of the Rs.200 x 1000 BPL patients x 12<br />
concerned hospital for providing free services to BPL patients<br />
months x 15 units=<br />
Rs.3.60 Crores<br />
164
4.9. Providing Telemedicine Services in Government Health Facilities<br />
SHSB has sought Public Private Partnership in providing Telemedicine Services in Government Hospitals of<br />
Bihar. Additionally the <strong>State</strong> is also in consultation with ISRO for providing technical support for the same<br />
either based on Gujarat or Orissa model. The project shall be initially piloted in two or three districts.<br />
Project Goal:<br />
The goal of this project is to establish a model for application of Telemedicine to address the issues of<br />
improving accessibility, more efficient use, ensure equitable distribution and enhancing the quality of available<br />
health services across the state.<br />
Project Objectives:<br />
The overall objective of the assignment is to provide a comprehensive model for Telemedicine in the state of<br />
Bihar.<br />
The specific objectives of the assignment are -<br />
· Establish and Provide Telemedicine Network for accessibility of healthcare service facilities in the<br />
<strong>State</strong> linking 2-3 District Hospitals to Patna Medical College Hospital (PMCH) of the <strong>State</strong>.<br />
· To reduce the cost of health services by providing specialized service through the network.<br />
· Upgrade the skills of existing Medical staff at the DHs and PMCH.<br />
· To ensure routine Management and Administration of the activities<br />
· To provide timely reports and information to the SHS, Bihar for audit and review<br />
· To ensure Maintenance, Servicing & Up-gradation of the Telemedicine Facility<br />
Project Timeframe- the Project is planned for a period of five years, and after that based on evaluation by the<br />
SHSB the project may be extended.<br />
Scope of Work<br />
The outsourced agency will provide complete technical support in terms of designing the telemedicine network<br />
for DH & PMCH, supply of hardware and software required, installation and operationalization and<br />
maintenance of telemedicine system including necessary training. The agency shall also facilitate defining and<br />
formalizing linkages between DHs and MCH and thus facilitate consultation through telemedicine.<br />
The detailed roles and responsibilities of the private partners to meet the aforesaid objectives are as follows:<br />
‣ Providing the necessary equipment and software for establishment of the above system.<br />
‣ Install, Operate and maintain appropriate Telemedicine facility.<br />
‣ Sufficient bandwidth to transfer Data<br />
‣ Real time videoconferencing with Patient<br />
‣ Transfer of diagnostic data on real time basis or/and Store & Forward basis, as the case may be<br />
through V-sat/Broadband/ISDN<br />
‣ The facility should enable transmission of patients medical records, including images, and provide<br />
a live two-way audio and video link between patient and specialist<br />
‣ Building the capacity at DH as well as associated PMCH to operate and use the system by<br />
providing training.<br />
‣ Technical manpower support to run the system to operationalise the project.<br />
‣ Continued technical back up for maintenance of the system.<br />
165
‣ Ensuring Quality Standards<br />
‣ Providing detailed reports of Telemedicine services as per the Proformas provided at the time of<br />
signing of the contract, or as issued by the SHS from time to time.<br />
The Telemedicine framework shall be at the secondary and tertiary levels:<br />
‣ Level 1 District Hospital<br />
‣ Level 2 PMCH<br />
Tele Medicine Equipment<br />
‣ The Software should be able to use any Digital Imaging and Communications in Medical (DICOM<br />
standard compliant) equipment.<br />
‣ Attachments for capturing and transferring DICOM standard images from various available medical<br />
devices, including X Rays; CT Scans; MRIs, and Ultrasound Images<br />
‣ Devices for creating high resolution virtual slides from various Pathological images and transferring<br />
them<br />
‣ The agency shall provide the following equipment at the DHs under this project:-<br />
1. ECG suitable for neonatal, pediatric and adult patients<br />
2. EMG suitable for neonatal, pediatric and adult patients<br />
3. Ultrasound scanner (should be able to do various diagnosis like cardiology, obstetrics &<br />
gynecology, radiology etc)<br />
4. Color Doppler ultrasound scanner<br />
5. Endoscope<br />
6. Digital Microscope<br />
7. Indirect Ophthalmoscope<br />
8. Funds Camera<br />
9. Multipara monitor (ECG, Temp, NIBP, SPO2, Heart rate) suitable for neonatal, paediatric and<br />
adult patients<br />
10. Electronic Stethoscope<br />
11. Pulmonory function test<br />
12. TMT machine<br />
13. ENT Audiometry<br />
14. Mammography<br />
15. Glucometer<br />
16. Fetal Heart Rate Monitor (for measuring the heart rate of foetus)<br />
17. EEG<br />
Note:<br />
1. All the above mentioned instruments would be able to connect to the computer (DICOM compatible)<br />
for obtaining digital data.<br />
2. The hardware/software so installed would also be able to send data generated from Digital X-Ray, CT<br />
scan and MRI mechanism, which may be installed by the Government.<br />
Ailments to be covered under the facility<br />
Software would be capable of handling and transferring any type of medical data which may be text, audio,<br />
video or image.<br />
The Medical areas which would be handled include:<br />
ü Cardiology<br />
ü Radiology<br />
ü Oncology<br />
ü Pathology<br />
ü Ophthalmology<br />
166
ü<br />
ü<br />
ü<br />
ü<br />
ü<br />
ü<br />
ü<br />
ü<br />
Nephrology/Diabetes<br />
Urology<br />
Neurology<br />
Psychiatric<br />
Dermatology<br />
Gynaecology<br />
Cosmetic Surgery<br />
Vector borne deceases<br />
The following Telemedicine software package modules would be used <br />
a). Electronic Medical Record (EMR)<br />
b). Tele-Cardiology<br />
c). Tele-Radiology<br />
d). Tele-pathology<br />
e). Tele-dermatology<br />
f). Tele-endoscopies<br />
g). Tele- Ophthalmology<br />
h) Video Conferencing<br />
Indicators for assessment of the utility of telemedicine system<br />
1. Number of Online Consultations<br />
a. Gross Number<br />
b. Timings<br />
i. Routine<br />
ii. Emergency<br />
c. As percentage of total seen<br />
d. How many physically sent<br />
e. How saved the need for transfer<br />
f. Whether any dramatic savings (e.g. Life /death matters) ensued<br />
2. Number of investigations<br />
a. On line Routine / Emergency investigations.<br />
b. Number and type of specialized investigations, waiting time and reporting time<br />
3. Follow up visits<br />
4. Number and type of procedures<br />
a. At PHCs<br />
b. At centers where staff is referred to.<br />
5. Training of Health and paramedical staff in telemedicine.<br />
Expected results:<br />
a. Number<br />
b. Level of skills and confidence.<br />
‣ Speed: Patients can be diagnosed and treated quickly, without the need for a potentially life-threatening<br />
journey to a larger hospital.<br />
‣ Service extended: Referral process strengthened and specialist advice available at PHC level.<br />
‣ Economical: In terms of cost of travel to a hospital for a second opinion and in service itself, once<br />
facility set up.<br />
‣ Improved quality of health services.<br />
167
‣ Institutionalize linkages between PHCs and hospitals through formal arrangements to provide instant<br />
consultation to PHCs and also honor referral cases from PHCs.<br />
‣ Builds trust: Patients with low level of education are often suspicious of visiting a city specialist. Teleconferencing<br />
offers frequent consultation with the specialist, building confidence and improving<br />
patients compliance to treatment, thus patient satisfaction will increase<br />
‣ Through linkages with specialists and hospital, PHCs will be able to cater to wider spectrum of<br />
needs/expectations.<br />
Budget<br />
Activities<br />
Operational cost for providing telemedicine<br />
facility in the state in this FY 2009-10<br />
Total proposed budget<br />
Rs.3.00 Crores<br />
Note : GOI had approved the project and budget in<br />
the previous <strong>PIP</strong> and ratification is solicited for the<br />
same for this FY<br />
Work plan<br />
Activities<br />
Floating of tender, Awarding of contract and finalization of<br />
interactions with ISRO<br />
Pre-Commissioning period<br />
Implementation of the project<br />
2007-08<br />
Q1 Q2 Q3 Q4<br />
4.10. Outsourcing of Pathology and Radiology Services from PHCs to DHs<br />
Under this scheme Pathology and Radiology services have been outsourced to different Private agencies. The<br />
agencies have and/or are in the process of setting up centers/diagnostic labs/collection centers at the<br />
hospitals/facilities. The state has fixed the rates on which the agency charges from the patient. The state has to<br />
only provide space at the hospitals to the agency for running the Pathology and Diagnostic Centre.<br />
However under the project service expansion has been done and Ultrasound facility has to be provided at<br />
various locations at DHs and SDHs. For the purpose of establishment of Central Reporting System (CRS) for<br />
X-ray and Ultrasound Units is being done at IGIMS, Patna. The purpose being CR system will connect all the<br />
Ultrasound and X-ray centers of IGEMS set up in Government Hospitals under this contract, with Teleradiology<br />
in a phased manner.<br />
168
The Agency shall provide all necessary hardware, software and manpower for establishing the network between<br />
IGIMS and each of its Radiology unit having X-Ray and Ultrasound facilities for running the Tele-Radiology<br />
service.<br />
SHSB has to provide space in coordination with DoH, GOB; radiologist to report on the ultrasound and x-ray<br />
images (preferably retired persons), telephone line with broad band connection and necessary power<br />
connections.<br />
The state requires budget in this regard only. All the remaining cost for setting up centers and providing<br />
services will be borne by the private providers.<br />
Budget<br />
Activities<br />
Total proposed budget<br />
Telephone line with broad band connection and necessary<br />
Rs.1,00,000 x 12 months =12,00,000<br />
power connections<br />
Sourcing of private radiologists to report on the ultrasound<br />
and x-ray images through the CRS at IGIMS incase of nonavailability<br />
of Government radiologists @Rs.25000 per<br />
25000 x 6 x 12= 18,00,000<br />
month for 6 radiologists<br />
Total 30,00,000/-<br />
4.11. Operationalising Mobile Medical Unit<br />
SHS, Bihar on behalf of the Department of Health, Government of Bihar, has invited Private Service Providers<br />
for providing Mobile Medical Units (each unit fitted with GPS- Global Positioning System) to provide primary<br />
health care facilities in the hard to reach rural areas of various districts of Bihar.<br />
Three agencies have been awarded the contract for operationalising mobile medical units in all the districts.<br />
Scope of Work<br />
Private Service Providers for providing mobile health care services in rural Bihar of curative, preventive and<br />
rehabilitative nature, to be provided by the service provider along with all deliverables like Mobile Clinic (each<br />
unit fitted with GPS- Global Positioning System), professional manpower, and other such services, to provide<br />
and supplement primary health care services for the far flung areas in the various districts of Bihar and to<br />
provide a visible face for the Mission.<br />
169
Project Objective<br />
To provide and supplement regular, accessible and quality primary health care services for the farthest areas in<br />
the districts of Bihar and to provide visible face for the mission and the Government, also establishing the<br />
concept of Healthy Living among the rural mass<br />
Project Scope<br />
The detailed roles and responsibilities of the private partners to meet the aforesaid objectives are as follows:<br />
‣ Providing the requisite vehicle and equipments and software for Operationalization of the MMU.<br />
‣ Install, Operate and maintain appropriate GPS facility.<br />
‣ Technical manpower support to run the MMU and provide the services<br />
‣ Continued technical back up for maintenance of the system.<br />
‣ Ensuring Quality Standards<br />
‣ Providing detailed reports and maintain database of information of MMU services as per the<br />
Proformas provided at the time of signing of the contract, or as issued by the SHS from time to<br />
time.<br />
Vehicle Type for MMU<br />
o<br />
o<br />
o<br />
o<br />
o<br />
Brand new GPS fitted, fully Air Conditioned TATA 709 chasis or equivalent vehicle of similar dimension<br />
from reputed manufacturers for MMU<br />
An accompanying vehicle of TATA Sumo or Mahindra Bolero or equivalent specification make vehicle<br />
for Carriage of Medical persons and also to be used as ambulance for transporting patients in case of<br />
emergency. The body of vehicle should be suitably modified to serve this dual purpose.<br />
Mobile Van should be designed keeping in mind the following criteria -ease of deployment, female<br />
privacy, community acceptance and cost.<br />
Web enabled MIS has to be ensured along with a Control room at Patna or Commissioner HQ.<br />
Temporary shed facility shall have to be ensured at the site for the patients in waiting.<br />
Manpower<br />
The manpower to be employed for the program is to be appointed by the Private agency as such-1 Doctor, 1<br />
Nurse, 1 Pharmacist (van supervisor),1 OT assistant , 1 X-ray technician, 1 ANM , 1 Driver (Qualification<br />
requirements annexed)<br />
Equipments to be provided in the MMU<br />
Medical Equipments -Semi Auto-Analyzer, Portable X ray unit, Portable ECG, Microscope, Screen, Stretcher,<br />
O.T Table with standard accessories, Stools, Dressing Trolley/Instrument trolley, Dressing drums, Oxygen<br />
Cylinder, Suction Machine., Ophthalmoscope, Refraction set, Horoscope, Mobile light or Ceiling light (OT<br />
Light),Centrifugal Machine, Hemoglobin meter, Glucometer, Autoclave, Incubator, Urine Analyzer, Vaccine<br />
carrier, Weighing machines-adult and infant, Stethoscope, BP Instrument, Kits like Suture removal kit,<br />
Pregnancy test kit, IUD insertion kit, Starter, Regent kit, HIV testing kit, General Instrument kit, First Aid kit,<br />
various, tests and surgery kits, Normal Ambulance appliances or accessories like foldable furniture, waste<br />
basket, linen, mattress, mackintosh sheets, fire extinguisher etc<br />
Silent DG set, Audio-Visual Equipment with projection system for IEC especially with, 40 LCD, P&A<br />
System, Cell phone<br />
Service Areas<br />
The Medical areas which would be handled include:<br />
1. Free General OPD/ Doctor Consult<br />
170
2. Free Drugs - Free dispensation and procurement of medicines as per the Essential Drug List prescribed<br />
by GoB for PHCs (Annexed) has to be ensured by the private agency<br />
3. Emergency Services during epidemics and Disasters<br />
4. Network and referral between PHC/CHC/Private clinics<br />
5. Generating health indicators and monitoring behavioral changes<br />
6. Gynec clinic<br />
7. Antenatal Clinics<br />
8. Post Natal Care<br />
9. Infants and Child Care including immunization with Vitamin A supplementation (support for the same<br />
to be provided by the Government)<br />
10. Diagnosis, Referral and Rehabilitation for Non-communicable diseases eg. Cardiac Diseases,<br />
Hypertension, Diabetes, etc<br />
11. Adolescent and Reproductive Health<br />
12. Other Services like Treatment of Minor Injuries and Burns, Aseptic Dressing, TT immunization,<br />
Treatment of Minor burns, Minor Suturing and removal referral etc<br />
13. Minor lab investigations<br />
14. Eye examination<br />
15. ENT examination<br />
16. HIV testing<br />
17. Promotion of contraceptive services including IUD insertion.<br />
18. Prophylaxis and treatment of Anemia with IFA Tablets.<br />
19. IEC and counseling along with preventive health screening and health awareness programs<br />
20. Service related to different public health programmes.<br />
21. Pathological services.<br />
22. Radiology Services X-ray and Ultra-sound<br />
23. Preventive Health Screening and Health awareness programs<br />
24. Medical camps will have to be conducted whenever emergency need be<br />
Commissioning Period- 2 months from the date of contract signing<br />
Budget<br />
Activities<br />
Total proposed budget (in Rs.)<br />
Projected cost for 1 MMU project at district level<br />
Rs.4.68 lakhs x38 units x 9 months<br />
=16,00,56,000/-<br />
Total 16,00,56,000/-<br />
4.14. Monitoring and Evaluation<br />
<strong>State</strong> Data Centre<br />
The <strong>State</strong> has One Data Centre which collects data from all PHCs, Sadar Hospitals & Sub. Div. Hospitals of all<br />
districts on a daily basis through land line phones and mobile phones. The collected data are stored and<br />
maintained in a computerised format and they are sent to respective programme officers according to their<br />
requirements. The collected data includes all the parameters required under RCH/NRHM for monitoring. The<br />
Data Centre has the following facilities:-<br />
171
(1) Computer Programmers- 2 (Two)<br />
(2) Supervisor- 2 (Two)<br />
(3) Computer Operators- 20 (Twenty)<br />
(4) Server with UPS - 1 (One)<br />
(5) Computers (including one server) with UPS - 22 (Twenty two)<br />
(6) Fax Machine with Auto Sending & Receiving Facility - 1 (One)<br />
(7) Laser Printers with Fax & Photo Copy Facility - 4 (Four)<br />
(8) Telephone connection (with Broadband connection) - 20 (Twenty)<br />
(9) Invertor - 1 (One)<br />
(10) Software - As Required<br />
(11) EPABX-Telephone Network System - 1 (One)<br />
(12) All necessary furnitures - As Required<br />
District & Block Data Centres<br />
The Data Centers at each and every hospital (PHC, Sadar Hospital, Sub-Divisional Hospital etc.) are being<br />
established through outsourcing. The main purpose of these Data Centers of Hospitals is to gather and maintain<br />
health related data under RCH/NRHM programme in their computer system and they upload the gathered health<br />
related data on the web-server of SHSB on daily basis. The Data Centers contain one computer with UPS, Laser<br />
printer, Phone connection, Internet connection, Computer operator, Misc. etc.The GPRS enabled mobile sets<br />
have been given to each and every data centers. The total no. of Data Centers to be established is 685 and the<br />
estimated cost is Rs. 7500/- per Data Centre per month.<br />
The District/Block Data Centres units would be as such:<br />
ü Primary Health Centre (PHC): 533<br />
ü Sub-Divisional Hospital (SCH): 43 (23+20 (new))<br />
ü District Hospital: 38 (25+13 (new))<br />
ü RDD: 09<br />
ü District Health Society: 38<br />
ü Medical Colleges & Hospitals: 24 (6 x 4)<br />
Total Data Centre: 685<br />
Budget<br />
Activities<br />
Total proposed budget (in Rs.)<br />
<strong>State</strong> Data Centre (monthly payment of the Data Centre is<br />
Rs. 175000/-, therefore, Rs.175000 x 12<br />
Rs.2100000/-<br />
District & Block Data Centres Rs. 7500/- x 12 x 685 Rs. 61650000/-<br />
Total 6,37,50,000/-<br />
172
4.15. Generic Drug Shop<br />
Under the PPP initiative Generic Drug Stores shall be set up at all MCHs, DHs and PHCs. The Private agency<br />
has to keep 188 types of drugs at the store. The state has provided only space for this purpose to the agency and<br />
the agency shares a % revenue share with the Government. The state has also fixed rates for the Generic Drug<br />
as per MRP.<br />
No additional cost is involved.<br />
4.16. Nutrition Rehabilitation Centres (NRCs) for Treatment of Severe and Acute<br />
Malnutrition (SAM)<br />
Child malnutrition extracts a heavy toll on both human and economic development, accounting for more than<br />
50 % of child deaths world wide. The consequences of malnutrition are serious leading to stunting, mental and<br />
physical retardation, weak immune defense and impaired development. More than one-third of worlds<br />
malnourished children live in India.<br />
In India, as revealed by the recent National Survey (NFHS-3, 2005-06), malnutrition burden in children under<br />
three years of age is 46 %. With the current population of India of 1100 million, it is expected that 2.6 million<br />
under-five would be suffering from severe and acute malnutrition which is the major killer of children under<br />
five years of age. It can be direct or indirect cause of child death by increasing the case fatality rate in children<br />
suffering from such common illnesses as diarrhea and pneumonia.<br />
The risk of death in these children is 5-20 times higher compared to well-nourished children. Severe and acute<br />
malnutrition is defined by a very low weight for height, below -3 z* scores of the median WHO growth<br />
standards, presence of visible severe wasting or bipedal Oedema, or mid-upper arm circumference (MUAC)<br />
of
MEASURES TO MANAGE MALNUTRITION:<br />
While mild and moderate forms of malnutrition in the absence of any minor or major illness among children can<br />
be addressed through Anganwadi centres, by supporting mothers to ensure service utilization and appropriate<br />
feeding and care practices at the household level; the treatment of children with severe and acute malnutrition<br />
calls for facility-based treatment by admitting children to a health facility or a therapeutic feeding centre. This is<br />
mainly because these children generally are seen to suffer from acute respiratory infections, diarrhea and<br />
pneumonia. A decision was thus taken to set up Nutrition Rehabilitation Centers which is a unit for the<br />
management of SAM children where they are kept under observation and provided with medical and nutritional<br />
care. In additional to curative care, special focus is given on timely, adequate and appropriate feeding to<br />
children. Efforts are also made to build the capacity of mothers through counseling to identify the nutrition and<br />
health problems in their child.<br />
Initial discussions with UNICEF on establishment of NRCs in the 2007 flood affected districts, resulted to be<br />
extremely productive. It was thought worthwhile to pilot NRCs for treatment of children suffering from severe<br />
forms of malnutrition in 2 flood affected districts with support from UNICEF for supervision and monitoring of<br />
activities, especially in the initial period of management of NRCs.<br />
Thus the NRCs were established in the districts of Muzaffarpur and East Champaran during August-September<br />
2007. The proposal includes the establishment cost and the running cost for the two piloted NRCs in the<br />
management of child malnutrition.<br />
Budget<br />
Activities<br />
Running cost of two NRCs for one month = 2,05,600/- x 2<br />
= 4,11,200/-, therefore for one year, 411200 x 12 months<br />
Total proposed budget (in Rs.)<br />
49,34,400<br />
Total 49,34,400/-<br />
4.17. Hospital Maintenance (Funded by <strong>State</strong> Govt)<br />
The state has outsourced the maintenance of Hospitals to private agencies. The amount require for this purpose<br />
is borne by the state government.<br />
The activities include<br />
· Maintenance of Hospital Premises.<br />
· Generator Facility.<br />
· Cleanliness of Hospitals.<br />
174
· Washing<br />
· Diet.<br />
4.18. Providing Ward Management Services in Government Hospitals<br />
It is proposed to provide Ward Management Services including Ward Boys for about 1900 health facilities in<br />
Bihar like the 100, 300 and 500 bedded District Hospitals, 100 bedded Sub-Divisional Hospitals, 30 bedded<br />
Referal and Primary Health Centres and 6 bedded Additional Primary Health Centers and also Govt. Medical<br />
College Hospitals.<br />
The task shall be done under PPP, wherein the agency shall be responsible for the following services-<br />
· Providing one ward boy for 10 or less than 10 beds and at the rate of one boy per additional 10 beds.<br />
· Ensuring 7x24 hours services of Ward Boys.<br />
· Shall provide one wheel chair for 10 beds or less and @ one wheel stretch for additional 20 beds.<br />
· Deploying all Ward Boys in uniform dress bearing a unique identification no. with name.<br />
· Assisting the nurses in the detoxification unit.<br />
· Attending to the personal hygiene of bed-ridden patients.<br />
· Escorting the patients to labs, other specialists & wards.<br />
· Monitoring the visitors and checking patients for possession of drugs.<br />
· Conducting physical exercises for the patients.<br />
· Assisting in detoxification of toilets and ward etc.<br />
· Daily replacement of used bed-sheets by clean bed-sheets with proper care.<br />
· Any other task related to ward management prescribed by the authority.<br />
Payment shall be made on a per bed per month for all the hospitals. In the FY 2009-10, it is to be piloted in 5<br />
District Hospitals therefore initially fund is required as such -<br />
Budget - @Rs.100/- x 2500 beds x 12 months=30.00 lakhs<br />
4.19. Provision for HR Consultancy services<br />
SHSB has invited offers from Human Resource Consultancy Services for assisting <strong>State</strong> Health<br />
Society in selection and recruitment of doctors, nurses, paramedical staffs and other managerial and<br />
clerical staff under guidance and direction of <strong>State</strong> Health Society, Bihar.<br />
Responsibilities of the Human Resources Consultant: The Consultant will be required to prepare<br />
panel of names for selection for the post as per reservation roster. Applications would be invited<br />
through open advertisements. Selection process may include open written test or interview or marks<br />
obtained or combination of these processes in the qualifying examination depending upon the no. of<br />
applicants and urgency. The mode of selection to be adopted will be the sole discretion of the <strong>State</strong><br />
Health Society.<br />
175
To achieve this objective, Human Resources Consultant shall be responsible for the following<br />
services:-<br />
· Will have to set up an office for this purpose.<br />
· Will be providing all office equipments and professional manpower for this purpose. SHSB shall<br />
provide only space.<br />
· All works like processing, data entry, scrutiny, selection, panel formation as per reservation roaster<br />
and recruitment etc.<br />
· Any other task related to Human Resources Consultancy Services prescribed by the authority.<br />
4.20 Advanced Life Saving Ambulances<br />
Budget – Rs.22,50,000/- per year<br />
SHSB is endeavoring to provide prompt quality pre hospital care to patients, trauma victims, pregnant women,<br />
for the purpose of which Emergency Network service is being piloted under PPP in Patna District.<br />
The objective is to save lives of Road Traffic Accidents, cardiac emergencies, fire victims and other emergency<br />
cases.<br />
Description<br />
There will be 5 Advance Life saving Ambulances (Trauma, Critical & Cardiac Care) & 5 Basic Life saving<br />
Ambulances which will run within Patna Municipal Corporation area and its sub urban areas. Every Ambulance<br />
shall be manned by a Driver, an Emergency Medical Technician and trained Helper to provide basic care during<br />
transportation of patients.). For each trip made by the Ambulance to anywhere within the limits of Patna<br />
Municipal Corporation and its sub-urban areas, a charge of Rs. 300/- shall be collected by the outsourced<br />
agency from the patients. The agency has to set up a Control Room in Patna which would operate for 24 hours<br />
in a minimum of 3000 sq. ft. area through dedicated toll free three digit telephone numbers (102). The agency<br />
has to provide 10 parallel lines with hunting facilities. The Control Room will receive emergency calls related<br />
to Medical Services and from Police and Fire Fighting Services to cater to Medical Emergencies. The agency<br />
shall provide GIS (Geographic Information System) maps, GPS (Global positioning systems) / AVLT<br />
(Automatic Vehicle Location Track) and all the other necessary hardware/software for Computer Telephonic<br />
Integration. The agency shall keep a record of the contact numbers and location of each of the 10 Ambulances,<br />
all Hospitals of city which can provide medical emergency, all the Police Stations, Police Control Room, Police<br />
Head-quarters and Fire Services in the city. The agency shall bear all expenses relating to hire of space, water,<br />
electricity charges, furniture, furnishing etc in running the Control Room. The Control Room shall also keep<br />
battery / generator backup facility so that services could be provided un-interrupted round the clock.<br />
Support activities- The agency has to also undertake the following-listing of Govt and private hospitals which<br />
can provide emergency services round the clock. Necessary training of hospital personnel to take up<br />
Emergency cases. Dissemination of the scheme and the toll free numbers for police, fire, health, education and<br />
general public so that this service can be utilized.<br />
Budget-<br />
Items<br />
Amount (Cost/month)<br />
Cost of Emergency service network in 989000.00 x 9= 8901000<br />
Patna (annual cost for running 10<br />
ambulances)<br />
Total 89,01,000<br />
IEC of the project, dissemination, 25 lakhs being provisioned in IEC, Training (Part<br />
monitoring and training<br />
A budget)<br />
176
7. Mobilisation and Management Support for Disaster Management<br />
In Bihar, the northern part is extremely flood prone. Due to the confluence of many rivers as well as its<br />
proximity to the hills of Nepal, the population living in about twenty two districts in Bihar suffers from floods<br />
every year. In the year 2007, the floods have been among the most devastating in decades. East Champaran,<br />
Darbhanga and Madhubani districts of Bihar, have been affected by floods most of the years and face floods<br />
almost every year, only the extent and the intensity vary. In 2007 however, over 24 million people in some<br />
8,500 villages in 22 districts in Bihar (including 2.5 million children below 5 years) were affected by floods. As<br />
per the department of disaster management, over 800 people lost their lives. The most affected districts are<br />
Muzaffarpur, Sitamarhi, East Champaran, Saharsa, Supaul, Madhubani, Darbhanga, Katihar, Samastipur,<br />
Sheohar, Khagaria, Madhepura, Araria, Begusarai, Gopalganj and West Champaran. There is a need to<br />
strengthen local capacities and develop the community potential to tackle the flood moving towards early<br />
recovery. There are essentially two types of the vulnerable affected in need of immediate assistance: a) those<br />
who are displaced; b) those who are in original locations but cut off.<br />
In year 2008, the floods were mainly due to the rivers, in Kosi region, changing their course, which was an<br />
outcome of a major breach in the eastern embankment of Kosi River in Kusha (Indo-Nepal) border in mid-<br />
August 2008. The Department of Disaster Management, Bihar has estimated that 2.95 million people across 979<br />
villages are facing the perils of present floods in the five districts-Araria, Supaul, Saharsa, Madhepura and<br />
Purnea. About 1.18 lakh are expected to be the vulnerable segment of pregnant and nursing women and about<br />
4.4 lakhs are likely to be children less than 5 years of age.<br />
Preparedness is the best response: Global and National experience in disaster situations indicates that<br />
immediate and appropriate response mitigates the agony of affected population. In flood related disaster, due to<br />
several factors, such as, the timing of flooding, the magnitude of floods, large number of people affected, scope<br />
of displacement, and low awareness among the affected on the health hazards, there has been an acute risk of<br />
outbreaks of water borne and vector borne diseases, such as gastroenteritis, malaria, dengue fever, leptospirosis<br />
and diarrhoea in the flood affected areas. Children under five, pregnant mothers, elderly and patients are at the<br />
highest risk of becoming victims to epidemics. Another factor which increases vulnerability is the socioeconomic<br />
profile of the affected. A large majority of them belong to socially marginalized communities who are<br />
poor as well. Providing clean potable water, protecting the area from epidemics, Safe delivery options for the<br />
pregnant mothers, rehydrating the diarrhea affected people of all age groups with ORS, immunizing children<br />
from 6 months-10 years in the affected area with measles vaccine, essential treatment for the sick etc are some<br />
of the absolute priorities for the health personnel during a disaster.<br />
177
To protect the health of the affected population based on the past experience, it is proposed to preposition<br />
certain important health response supplies during the current year at <strong>State</strong> level. These supplies can be sent to<br />
the affected populace at the earliest to provide relief. The calculations are being done assuming the affected<br />
population to be 20 million and based on last years initiatives and expenditure by the state-<br />
With the experiences of the last year the state would like to propose a revolving fund for the preparedness and<br />
relief for the flood affected people in the <strong>State</strong>:<br />
Budget:<br />
Activity Unit Rate Amount<br />
( In Rs )<br />
Setting up of <strong>State</strong> Health Disaster Management 1 58,750 x 12 7,05,000<br />
Cell in Health Department, GoB<br />
months<br />
Mobilizing medical teams from Non flooded 50 25900 ( a team 12,95,000<br />
districts for one week<br />
of two Doctors<br />
and two<br />
paramedics for<br />
7 days)<br />
Transportation ,Mobility & Monitoring state &<br />
Rs.5.00 lakhs<br />
8000000<br />
district level for 16 districts<br />
per district<br />
Total 1,00,00,000/-<br />
8. Health Management Information System<br />
(1) Web Server System<br />
The <strong>State</strong> Health Society has established one web-server with 512 kbps leased-line connection for on-line<br />
uploading and reporting of Health related data through web-server application of <strong>State</strong> Health Society, Bihar.<br />
The following system shall be introduced in parallel to the existing system of Data centers:<br />
1. Online uploading of Health related data directly from Data Centers of PHC/Hospitals.<br />
2. Compilation and reporting of Health related data through developed application software in very less<br />
time.<br />
3. The reports will be more accurate and consistent.<br />
4. The DM/CS/DHS can view the different reports of Health services of their own district in on-line<br />
mode, therefore proper action can be taken quickly.<br />
5. The officers/staff of state level can view the reports of Health services of all districts in online mode,<br />
therefore proper action can be taken promptly.<br />
178
6. According to requirement, any new report can be added and the information can be obtained from<br />
PHC/Hospitals in online mode quickly.<br />
7. More security and safety of Health related database.<br />
Therefore further up-gradation and maintenance of web-server are required in coming financial year like<br />
blade server (more storage capacity and very high speed processing), maintenance support of web-server<br />
etc.<br />
The website for all 38 districts are also required to be designed, created and maintained along with the<br />
renovation of website of <strong>State</strong> Health Society, Bihar.<br />
Budget<br />
S. No Items Amount (Rs.)<br />
1 Leased Line(512 KBPS) Rs. 287642/-<br />
2 Up gradation of Leased Line - (1MBPS) Rs. 200000/-<br />
3 Antivirus (No. of antivirus-3) Rs. 15000/-(Rs. 5000 x 3)<br />
4 Web-site: (Design, Creation, Maintenance, Registration, Rs. 500000/-<br />
Hosting of state and all 38 districts)<br />
5 Blade Server(One Blade) Rs.300000/-<br />
6 One Additional Blade Rs.135000/-<br />
7 Maintenance Rs. 50000/-<br />
8 Software development Rs. 500000/-<br />
Total Rs. 19,87,644/-<br />
(2) HMIS Reports<br />
As we know that NRHM aims to continuously improve and refine its strategies based on the inputs and<br />
feedback received from the <strong>State</strong> and from various review missions. One of our priorities is to build a robust<br />
Health Management Information System (HMIS) that is used for improving, planning and programme<br />
implementation at all levels. NRHM has introduced Revised HMIS formats and they are as follows:<br />
SN Form No. Form Name Used at Frequency<br />
1 NRHM/HSC/3/M<br />
Monthly format for SCs and<br />
Monthly (5 th of<br />
HSC<br />
equivalent facilities<br />
following month)<br />
2 NRHM/PSC/3/M<br />
Monthly format for PHCs and<br />
Monthly (5 th of<br />
PSC<br />
equivalent facilities<br />
following month)<br />
3 NRHM/CSC/3/M<br />
Monthly format for CHCs and<br />
Monthly (5 th of<br />
CSC<br />
equivalent facilities<br />
following month)<br />
4 NRHM/SDH/3/M<br />
Monthly format for SDH and<br />
Monthly (5 th of<br />
SDH<br />
equivalent hospitals<br />
following month)<br />
5 NRHM/DH/3/M<br />
Monthly format for DH and<br />
Monthly (5 th of<br />
DH<br />
equivalent hospitals<br />
following month)<br />
179
6 NRHM/DHQ/3/M Monthly format for District DHQ<br />
Monthly (10 th of<br />
following month)<br />
7 NRHM/DHQ/2/Q Quarterly format for District DHQ Quarterly (10 th )<br />
8 NRHM/DHQ/1/A Annual format for District DHQ Annual (5 th )<br />
9 NRHM/SG/2/Q Quarterly format for <strong>State</strong> HQ <strong>State</strong> HQ Quarterly (20 th )<br />
10 NRHM/SG/1/A Annual format for <strong>State</strong> HQ <strong>State</strong> HQ Annual (15 th April)<br />
11 NRHM/GOI/3/M Monthly Consolidated <strong>State</strong> HQ/DHQ<br />
Monthly (20 th of<br />
following month)<br />
12 NRHM/GOI/2/M Quarterly Consolidated <strong>State</strong> HQ/DHQ<br />
Quarterly (20 th of<br />
following month)<br />
13 NRHM/GOI/1/A Annual Consolidated <strong>State</strong> HQ/DHQ Annual (30 th April)<br />
It is required to implement the Revised HMIS formats up to sub-center level.<br />
(A) Printing of Formats<br />
Sl.No. Form No. No. of<br />
Pages/<br />
Format<br />
Total No. of Pages<br />
used at one Health<br />
Institution<br />
Total No.<br />
of Health<br />
Institution<br />
Total No. of<br />
Pages used at<br />
all<br />
Institution/Yr<br />
Details<br />
1 NRHM/HSC/3/M 4 48(12x4) 11964 574272 11964x48<br />
2 NRHM/PHC/3/M 6 72(12x6) 1905 137160 1905x72<br />
3 NRHM/CHC/3/M 7 84(12x7) 533 44772 533x84<br />
4 NRHM/SDH/3/M 7 84(12x7) 43 3612 43x84<br />
5 NRHM/DH/3/M 7 84(12x7) 38 3192 38x84<br />
6 NRHM/DHQ/3/M 1 12(12x1) 38 456 38x12<br />
7 NRHM/DHQ/2/Q 2 8(4x2) 38 304 38x8<br />
8 NRHM/DHQ/1/A 2 2(1x2) 38 76 38x2<br />
9 NRHM/SG/2/Q 1 4(4x1) 1 4 1x4<br />
10 NRHM/SG/1/A 3 3(1x3) 1 3 1x3<br />
11 NRHM/GoI/3/M 6 72(12x6) 38 2736 38x72<br />
12 NRHM/GoI/2/Q 2 8(4x2) 38 304 38x8<br />
13 NRHM/GoI/1/A 7 7(1x7) 38 266 38x7<br />
Total 767157<br />
Surplus No. of Forms (including wastage and others-10%) 76716<br />
Grand Total of Pages- 843873<br />
Total Printing Cost ( @ Rs. 1.00 per page) Rs. 843873/-<br />
B: Transportation of Formats<br />
No. of pages sent per district= 843873/38 =<br />
22207(approx.)<br />
Transportation Costs per district=Rs. 1000<br />
180
Total Transportation Cost for all 38 districts=38xRs.1000= Rs. 38000/-<br />
C: Training At Block Level (PHCs, District Hospitals, Sub-Divisional Hospitals)<br />
Training on Revised HMIS formats at District Level has been completed, so Training on Revised HMIS<br />
Formats at Block Level (i.e. PHC, District Hospital and Sub-Divisional Hospital levels) has to be performed.<br />
Therefore it is required to train the followings :-<br />
ü Deputy superintendent of District & Sub-Divisional Hospitals<br />
ü MOIC of PHCs<br />
ü BHM<br />
ü BAM<br />
The training has to be performed to improve the quality of data. So the master trainer of each and every district<br />
will train Deputy Superintendent, MOIC, BHM and BAM in their respective district.<br />
Hence Fund require for giving TA/DA to all trainees and for training materials, stationeries and other cost. The<br />
TA/DA given to trainees is Rs. 200/- per trainee (Only one time) and miscellaneous cost is Rs. 50/- per trainee<br />
(Only one time)<br />
Therefore budget calculation is as follows:-<br />
(a) Total no. of trainees = 1680<br />
The details are as follows:-<br />
SN Designation Number<br />
1 Deputy superintendent of District 38 (25+13 (new))<br />
Hospital<br />
2 Deputy superintendent of Sub- 43 (23+20 (new))<br />
Divisional Hospital<br />
3 MOIC of PHC 533<br />
4 BHM 533<br />
5 BAM 533<br />
Total 1680<br />
Budget<br />
S. No Items Amount (Rs.)<br />
1 Web Server System 19,87,644/-<br />
2 HMIS Reports<br />
A Printing of Formats<br />
8,81,873<br />
B Transportation of Formats<br />
C Training of Formats at Block level (TA/DA Cost = Rs. 200/- 4,20,000<br />
per trainee (only one time) x 1680= Rs. 336000/- + Misc. cost =<br />
Rs. 50/- per trainee (one time) 50 x 1680=84000/-)<br />
Total 32,89,517/-<br />
181
9. Strengthening of Cold Chain<br />
Effective cold chain maintenance is the key to ensuring proper availability and potency of vaccines at all levels.<br />
However the recently concluded Vaccine Management assessment (VMAT) in Bihar in 2008 and the National<br />
Cold chain assessment (July 2008) observed several deficiencies in cold chain storage and management in<br />
Bihar.<br />
With a steadily increasing immunization coverage for Routine Immunization, rise in demand for Immunization<br />
services throughout the state, the consumption of large quantities of vaccines in frequent Supplementary<br />
Immunization activities and the possibility of introduction of newer vaccines in the near future, it is necessary<br />
that the capacity of existing cold chain stores as well as the proper management of immunization related<br />
logistics be strengthened on a urgent basis.<br />
For this there is need for refurbishment of existing cold chain stores at all levels, particularly at the level of the<br />
larger state, 9 regional and 38 district stores. Often there is lack of storage space in the existing health stores<br />
leading to dumping of critical immunization related logistics like AD syringes, vaccine carriers and cold boxes<br />
in the open, exposing them to the vagaries of nature and sometimes leading to their damage. Renovation of<br />
existing stores would help in creating more organized dry space for both proper storage of material as well as<br />
proper loading, packing and unloading of Immunization related logistics. The state store in particular receives<br />
large quantities of materials and a separate ware house is needed to store immunization related logistics.<br />
Provision to hire storage space on arrival of large quantities of material should also exist. In all stores across the<br />
state there is also a need for proper electrification and wiring to ensure longevity of electrical cold chain<br />
equipment and for reducing their frequent breakdown.<br />
The lack of dedicated support manpower for immunization logistics management and for cold chain equipment<br />
repair at all levels was observed during the aforesaid cold chain assessments and it was recommended that At<br />
each of these facilities there should be a full time dedicated store manager. Where the load of operations is high<br />
(SVS and RVS) the store manager should have adequate support staff to help him. (VMAT Bihar 2008) The<br />
National cold chain assessment also recommended that a there should be a cold chain technician along with a<br />
cold chain handler at all district stores and a cold chain handler at all PHCs. Since provision of regular staff in<br />
these positions is not possible it is envisaged that contractual persons be hired for these activities.<br />
Budget<br />
9.1 Infrastructure Strengthening for Cold Chain<br />
Items Units Amount<br />
Refurbishment and integration of existing Warehouse facilities for R.I. as well<br />
as provision for hiring external storage space for (during Immunization<br />
Campaigns) Logistics at <strong>State</strong> HQ @Rs 15,00,000/-<br />
1 1500000<br />
182
Refurbishment of existing Cold chain room for district stores in all districts<br />
with proper electrification,Earthing for electrical cold chain equipment and<br />
shelves and dry space for non elecrtical cold chain equipment and logistics<br />
@Rs 7 Lakhs per district<br />
38 26600000<br />
Earthing and wiring of existing Cold chain rooms in all PHCs @Rs 10000/-<br />
per PHC<br />
533 5330000<br />
Total 572 3,34,30,000<br />
12. Mainstreaming AYUSH under NRHM<br />
The Indian systems of medicine have age old acceptance in the communities in India and in most places they<br />
form the first line of treatment in case of common ailments. Of these, Ayurveda is the most ancient medical<br />
system with an impressive record of safety and efficacy.<br />
Other components such as Yoga, Naturopathy are being practised by the young and old alike, to promote good<br />
health. Now days, practice of Yoga has become a part of every day life. It has aroused a world wide awakening<br />
among the people, which plays an important role in prevention and mitigation of diseases. Practice of Yoga<br />
prevents psychosomatic disorders and improves an individuals resistance and ability to endure stressful<br />
situation.<br />
Ayurveda, Yoga, Unani, Siddha and Homoeopathy (AYUSH) are rationally recognised systems of medicine<br />
and have been integrated into the national health delivery system. India enjoys the distinction of having the<br />
largest network of traditional health care, which are fully functional with a network of registered practitioners,<br />
research institutions and licensed pharmacies. The NRHM seeks to revitalize local health traditions and<br />
mainstream AYUSH (including manpower and drugs), to strengthen the Public Health System at all levels. It is<br />
decided that AYUSH medications shall be included in the drug kit of ASHA, The additional supply of generic<br />
drugs for common ailments at SC/PHC/CHC levels under the Mission shall also include AYUSH formulations.<br />
At the CHC level two rooms shall be provided for AYUSH practitioner and pharmacist under the Indian Public<br />
Health Standards (IPHS) model. At the same time, it has been decided to place or provision one Ayush doctor<br />
on contract at the APHCs for the purpose and to ensure complete coverage of the population.<br />
Activities<br />
Improving the availability of AYUSH treatment faculties and integrating it with the existing Health Care<br />
Service.<br />
Strategies<br />
‣ Integrate and mainstream ISM &H in health care delivery system including National Programmes.<br />
‣ Encourage and facilitate in setting up of Ayush wings-cum-specialty centres and ISM clinics.<br />
‣ Facilitate and Strengthen Quality Control Laboratory.<br />
183
‣ Strengthening the Drug Standardization and Research Activities on AYUSH.<br />
‣ Develop Advocacy for AYUSH.<br />
‣ Establish Sectoral linkages for AYUSH activities Delivery System<br />
1. Integration of AYUSH services in 1234 APHC with appointment of contractual AYUSH Doctors.<br />
2. Appointment of paramedics where AYUSH Doctors shall be posted.<br />
3. Strengthening of AYUSH Dispensaries with provision of storage equipments.<br />
5. Making provision for AYUSH Drugs at all levels.<br />
6. Establishment of specialized therapy centers/yush wings in District Head Quarter Hospitals & Medical<br />
Colleges.<br />
7. AYUSH doctors to be involved in all National Health Care programmes, especially in the priority areas<br />
like IMR, MMR, JSY, Control of Malaria, Filaria, and other communicable diseases etc.<br />
8. Training of AYUSH doctors in Primary Health Care and NDCP.<br />
9. All AYUSH institutions will be strengthened with necessary infrastructure like building, equipment,<br />
manpower etc.<br />
10. Yoga trainings were held in various District hospitls to provide Yogic therapy for specific diseases and<br />
also as a synergistic therapy to all other systems of treatment.<br />
Integration of AYUSH with ASHA<br />
1. Training module for ASHAs and ANMs has to be updated to incorporate information of AYUSH.<br />
2. Training & capacity building to be undertaken by the Director, SIHFW and necessary training material<br />
for the purpose to be modified and provided accordingly.<br />
3. Drug kit that will be provided to ASHA contains one AYUSH preparation in the form of iron<br />
supplement. But other drugs which are used in the treatment of common diseases control of<br />
communicable diseases as well as drugs promoting the maternal and child health as well as improving<br />
quality of life could be included subsequently.<br />
Drug Management<br />
1. Provision of supply drugs per AYUSH dispensary has been projected as per NRHM norm.<br />
3. Provision of medicines for District AYUSH wings and Specialty Therapy Centres is proposed to be<br />
operated in the <strong>State</strong>.<br />
Special Initiatives for Mainstreaming and Strengthening of Ayush<br />
(a)<br />
Ayush department in Bihar contain 3 units known as Ayurvedic Unani and Homeopathic.<br />
Government of Bihar running individual dispensary in rural area and a district level joint dispensary<br />
of each 3 units (Ayurvedic, Unani and Homeopathic).<br />
Following details of rural and district dispensary is given with their required fund far medicine,<br />
machines and miscellaneous expenditures.<br />
Sl. Dispensaries<br />
N<br />
o.<br />
1. District Joint<br />
Hospitals<br />
(i) Ayurvedic<br />
No. of<br />
dispensa<br />
ries<br />
Medicine<br />
184<br />
Machines &<br />
equipments<br />
For<br />
miscellaneous<br />
expenditure<br />
26 25,000x26=6,50,000 25,000x26=6,50,000 10,000x26=2,60,000<br />
(ii) Unani 26 25,000x26=6,50,000 2,50,00x26=6,50,000 10,000x26=2,60,000<br />
(iii) Homeopathic 26 25,000x26=6,50,000 25,000x26=6,50,000 10,000x26=2,60,000<br />
2. Rural Dispensaries<br />
(i) Ayurvedic<br />
69 25,000x69=17,25,000 25,000x69=17,25,000 5,000x25=3,45,000
(b)<br />
Sl.<br />
N<br />
o.<br />
(ii) Unani 30 25,000x30=7,50,000 25,000x30=7,50,000 5,000x30=1,50,000<br />
(iii) Homeopathic 29 25,000x29=7,25,000 25,000x29=7,25,000 5,000x29=1,45,000<br />
Total 206 51,50,000.00 51,50,000.00 14,20,000.00<br />
Ayush Units are also functioning in additional primary health centre in general health services. The<br />
details of the APHC (Ayush) and their required medicines, machine and equipments and other<br />
expenses are given as follows:-<br />
Dispensaries<br />
1. APHC(Ayus<br />
h)<br />
(i) Ayurvedic<br />
No. of<br />
dispensari<br />
es<br />
Medicine<br />
Machines &<br />
equipments<br />
For<br />
miscellaneous<br />
expenditure<br />
263 25,000x263=65,75,000 25,000x263=65,75,000 10,000x263=26,30,000<br />
(ii)Unani 77 25,000x77=19,25,000 25,000x77=19,25,000 10,000x77=7,70,000<br />
(iii)<br />
59 25,000x59=1,47,5000 25,000x59=1,47,5000 10,000x59=5,90,000<br />
Homeopathic<br />
Total 399 99,75,000.00 99,75,000.00 39,90,000.00<br />
(c) Ayush treatment facility is required to attach with Allopathic hospitals. For this purpose in each 15 Sadar<br />
Hospital is proposed to open Ayush system of treatment with OPD and IPD of 3 system of medicine,<br />
(Ayurvedic, Unani and Homeopathic).<br />
The following provision is given as follows:-<br />
(i) Contraction and Renovation- 10,00,000.00<br />
(ii) Machines and Equipments- 1,50,0000.00<br />
(iii) Medicine and Diet- 7,00,000.00<br />
(iv) Training of Paramedical staffs- 1,00,000.00<br />
(v) One time miscellaneous expenditure- 2,00,000.00<br />
Total 35,00,000.00<br />
Total required for 15 Sadar Hospitals and 3 units of each (Ayurvedic, Unani & Homeopathic)-<br />
35,00,000 x3 x16=16,80,00,000.00<br />
(d) Strengthening the Quality Control Laboratory<br />
The quantum of Ayurvedic and Homoeopathic medicines used / procured in both public and<br />
private health sectors is huge. There has been wide ranging concern about spurious, counterfeit and sub<br />
standard drugs. In order to prevent the spread of sub standard drugs and to ensure that the drugs<br />
manufactured or sold or distributed throughout the state are of standard quality, drug regulation and<br />
enforcement unit has to be established in the state. The drug regulatory mechanism to be strengthened<br />
at the state level to improve the quality of drugs used in AYUSH and ensure proper standardization.<br />
(e).<br />
Strengthening the Drug Standardisation and Research Activities on AYUSH Standardisation- As<br />
research is an important activity in the process of development of a drug used for preventive and<br />
curative purpose, it has been found that the major drawback in the development of AYUSH is lack of<br />
research and development activity on the drugs used for the System. It is estimated that there are<br />
10,000/- plant species found all over the world having medicinal properties. The following activities<br />
will be undertaken to strengthen the drug standardisation and research activities on AYUSH:<br />
1. It has been proposed to evaluate the chemical, pharmacological and clinical efficacy of the plant drugs.<br />
2. The phytochemical entities responsible for the therapeutic activity of the plant drugs used in AYUSH<br />
system will be evaluated through intensive R & D activity.<br />
185
3. The pharmacologically viable drugs will be screened clinically under WHO guideline to establish the<br />
therapeutic activity.<br />
4. Clinical trial on different diseases like Psoriasis, Liver disorders, Diabetics, Asthma will be conducted<br />
to establish the effect of various drugs used for such diseases.<br />
5. It has also been proposed to conduct literary research like translation of manuscripts and its<br />
publications.<br />
6. Re-vitalisation of the local health traditions and the knowledge of traditional drugs used by experienced<br />
local health traditioners will be gathered and documented.<br />
(f) .<br />
Strengthening of the <strong>State</strong> and District Management System of AYUSH<br />
1. It is proposed to create necessary Managerial post in the <strong>State</strong> and District level for effective<br />
supervision and implementation of different activities.<br />
2. Necessary vehicles with supporting manpower has also been proposed to strengthen the supervisory<br />
3. Joint monitoring visits to health centres to be undertaken by both AYUSH and Health Care Officials at<br />
the District levels/<strong>State</strong> level.<br />
BUDGET<br />
AYUSH - Part A Requirement of the funds from NRHM –<br />
1. Ayurvedic, Unani and Homeopathic dispensaries-<br />
(i) Provision of 1 Ayush doctor at each APHC on contract<br />
@ Rs.20,000/- x 1243 APHC x 9 months 22,37,40,000.00<br />
(ii) Salary of Paramedics 4,36,29,300.00<br />
@ 3900 x 1243 x 9 months<br />
(iii) Salary of Pharmacists 7,27,15,500.00<br />
@6500 x 1243 x 9 months<br />
2. Training of Ayush Doctors & Paramedical staffs w.r.t Ayush wing-4,15,00,000.00<br />
3. IEC 1,00,00,000.00<br />
Grand Total (A) 39,15,84,800.00<br />
AYUSH Part B<br />
I. Requirement of the funds from the Ayush Departments for Ayush Dispensaries<br />
1. For Ayush dispensaries & additional PHCs already existing<br />
(i) For Medicine- 1,51,25,000.00<br />
(ii) Machine and equipments- 1,51,25,000.00<br />
(iii) Other Miscellaneous- 48,10,000.00<br />
Sub-Total 3,50,60,000.00<br />
2.New Ayush OPD and IPD in 15 Sadar Hospital 13,65,00,000.00<br />
Total II – Rs. 171560000/-<br />
II. Requirement of the funds from the Ayush Departments to uplift Ayush Medical Education for<br />
Government Ayush Medical Colleges<br />
1. Government TIBI College & Hospital (Unani), Patna<br />
186
Rs. in Crores<br />
(i) Building construction- 6.40/-<br />
(ii) Machine and equipments- 1.00/-<br />
(iii)Quality Testing Lab- 1.00/-<br />
(iv) Pharmacy- 1.00/-<br />
(v) Herbal Gardian - .20/-<br />
(vi) Medicine and Diet- 0.050/-<br />
Sub-total 9.65/-<br />
2. Government RBTS Homeopathic Medical College, Muzaffarpur<br />
Rs. in Crores<br />
(i) Building construction- 0.35/-<br />
(ii) Machine and equipments- 0.20/-<br />
(iii)Quality Testing Lab- 1.00/-<br />
(iv) Pharmacy- 1.00/-<br />
(v) Medicine and Diet- 0.02/-<br />
Sub-total 2.57/-<br />
3. Government Ayurvedic College, Begusarai<br />
Rs. in Crores<br />
(i) Building construction- 3.00/-<br />
(ii) Machine and equipments- 1.00/-<br />
(iii) Medicine and Diet- 0.02/-<br />
Sub-total 4.02/-<br />
4. Government Ayurvedic College Hospital, Patna<br />
Rs. in Crores<br />
(i) Building construction- 2.668/-<br />
(ii) Machine and equipments- 9.70/-<br />
(iii)Renovation and Beutification- 1.634/-<br />
(iv) Medicine and Diet- 0.50/-<br />
Sub-total 14.502/-<br />
5. Government Ayurvedic College, Patna<br />
Rs. in Crores<br />
(i) Building construction- 3.00/-<br />
(ii) Machine and equipments- 6.75/-<br />
(iii) Quality Testing Lab- 0.80/-<br />
(iv) Herbal Gardan- 0.20/-<br />
(v) Animal House- 0.05/-<br />
Sub-total 10.80/-<br />
Total II – Rs.415420000<br />
Grant total required for teaching institutions and dispensaries (I + II)- 171560000 + 415420000<br />
= Rs.58,69,80,000/-<br />
187
Sl.<br />
No.<br />
Summary Budget of NRHM Part B<br />
Budget Head<br />
Modified<br />
Budget<br />
1 2 6<br />
1 Decentralization<br />
1.11 ASHA Support System at <strong>State</strong> Level 40650750<br />
1.12 ASHA Support System at District Level 2160000<br />
1.13 ASHA Support System at Block Level 79950000<br />
1.14 ASHA Support System at Village Level 4500000<br />
Available<br />
under<br />
2008-09<br />
1.15 ASHA Trainings 86895000 1715.00<br />
1.16 ASHA Drug Kit & Replenishment 22555800<br />
1.17 Emergency Services of ASHA 6600000<br />
1.18 Motivation of ASHA 63172875<br />
1.19 Capacity Building/Academic Support programme 1000000<br />
1.2 ASHA Divas 81230200<br />
Total ASHA 388714625<br />
1.21 Untied Fund for Health Sub Center, Additional Primary Health Center<br />
and Primary Health Center<br />
134807000<br />
%<br />
1.22 Village Health and Sanitation Committee 352102500 1000.00<br />
1.23 Rogi Kalyan Samiti 85300000<br />
Total Decentralization 960924125 22.06<br />
2 Infrastructure Strengthening<br />
2.1 Construction of HSCs (100 no. x Rs.9.50 lakhs) 95000000<br />
2.2 Construction of PHCs 637967000<br />
2.2a Construction of residential quarters of 200 old APHCs for staff nurses 600000000<br />
2.2b Construction of building of 51 APHCs where land is available 37967000<br />
2.3 Up gradation of CHCs as per IPHS standards (100 CHCs x Rs.40.00<br />
lakhs)<br />
188<br />
400000000 8040.00<br />
2.4 Infrastructure and service improvement as per IPHS in 20 (DH & 130000000<br />
SDH) hospitals for accreditation or ISO : 9000 certification<br />
2.5 Upgradation of ANM Training Schools 10000000 600.00<br />
2.6 Annual Maintenance Grant 82080000<br />
Total Infrastructure strengthening 1355047000 31.10<br />
3 Contractual Manpower<br />
3.1 Contractual Salaries, Incentives and Bonus (PHC doctors and staffs,<br />
contractual staff nurses, ANM ®, mobile services)<br />
676702000<br />
3.1a Incentive for PHC doctors & staffs @ Rs. 50,000 for better performance in 12500000<br />
implementing programmes (Rs. 50,000/ - per PHC per year)<br />
3.1b Salaries for contractual Staff Nurses (2900 existing and 910 new) (Rs.7500 343900000
per month)<br />
3.1c Contract Salaries for ANMsRs.6000 per month x 3500 (12 Months<br />
Consolidated Salaries for Contractual ANMs)<br />
252000000<br />
3.1d Mobile facility for all health functionaries (District officials, PHC in charge, 60000000<br />
CDPOs and ANMs @ 500 per month)<br />
3.2 Block Programme Management Unit 289524000<br />
3.3 Addl. Manpower for SHSB 6204288<br />
3.4 Addl. Manpower for NRHM 25479000<br />
Total Contractual Manpower 997909288 22.90<br />
4 PPP Initiatives<br />
4.1 102-Ambulance service 4032000<br />
4.2 1911- Doctor on Call & Samadhan 816000<br />
4.3 Addl. PHC management by NGOs 39864000<br />
4.4 American Association of Physicians of Indian Origin (AAPIO) 5600000<br />
4.5 SHRC (HOSMAC) 138.44<br />
4.6 Services of Hospital Waste Treatment and Disposal in all Government<br />
947.16<br />
Health facilities up to PHC in Bihar (IMEP)<br />
4.7 Dialysis unit in various Government Hospitals of Bihar 300.00<br />
4.8 Setting Up of Ultra-Modern Diagnostic Centers in Regional Diagnostic<br />
Centers (RDCs) and all Government Medical College Hospitals of<br />
Bihar<br />
36000000<br />
4.9 Providing Telemedicine Services in Government Health Facilities 300.00<br />
4. 10 Outsourcing of Pathology and Radiology Services from PHCs to DHs 3000000<br />
4.11 Operationalising MMU (38 units x Rs.4.68 lakhs x 9 months) 160056000<br />
4.14 Monitoring and Evaluation (<strong>State</strong>, District, Block Data Centre) 63750000<br />
4.15 Generic Drug Shop No<br />
Funds<br />
required<br />
4.16 Nutritional Rehabilitation Centre 4934400<br />
4.17 Hospital Maintenance<br />
4.18 Providing Ward Management Services in Government Hospitals 3000000<br />
4.19 Provision for HR Consultancy services 2250000<br />
4.2 Advanced Life Saving Ambulance (Rs.9,98,000/- x 9 months) 8901000<br />
Total PPP Initiatives 332203400 7.62<br />
5 Procurement of Supplies<br />
5.1 Delivery kits at the HSC/ANM/ASHA (no.200000 x Rs.25/-) 50,00,000<br />
5.2 SBA Drug kits with SBA-ANMs/Nurses etc (no.50000 x Rs.245/-) 12250000<br />
5.3 Availability of Sanitary Napkins at Govt. Health Facilities<br />
950000<br />
@25000/district/year<br />
5.4 Procurement of beds for PHCs to DHs 70286000<br />
Total Procurement of Supplies 83486000 1.92<br />
6 Procurement of Drugs<br />
6.1 Cost of IFA for Pregnant & Lactating mothers (Details annexed) 50153000<br />
6.2 Cost of IFA for (1-5) years children (Details annexed) 40923000<br />
189
6.3 Cost of IFA for adolescent girls (Details annexed) 63750000<br />
Total Procurement of Drugs 154826000 3.55<br />
7 Mobilisation & Management support for Disaster Management 10000000 0.23<br />
8 Health Management Information System 3289517 0.08<br />
9 Strengthening of Cold Chain (Infrastructure strengthening) 33430000 0.77<br />
Refurbishment of existing Warehouse for R.I. as well as provision for hiring<br />
external storage space for (during Immunization Campaigns) Logistics at<br />
<strong>State</strong> HQ @Rs 1500000/-<br />
Refurbishment of existing Cold chain room for district stores in all districts<br />
with proper electrification,Earthing for electrical cold chain equipment and<br />
shelves and dry space for non elecrtical cold chain equipment and logistics<br />
@Rs 7 Lakhs per district x 38 districts<br />
Earthing and wiring of existing Cold chain rooms in all PHCs @Rs 10000/-<br />
per PHC x 533 PHCs<br />
10 POL of Generators for cold chain @ Rs. 600 per day per WIC. Rs. 500 per<br />
day per district and Rs. 400 per day per PHC<br />
1500000<br />
26600000<br />
5330000<br />
30000000 0.69<br />
11 Preparation of Action Plan 4100000 0.09<br />
11.1 Preparation of District Health Action Plan (Rs.1 lakh per district x 38) 3800000<br />
11.2 Preparation of <strong>State</strong> Health Action Plan @ 3 lakhs 300000<br />
12 Mainstreaming Ayush under NRHM 391,584,800 8.99<br />
Total 4,356,800,130 100.00<br />
190
PART- C<br />
Routine Immunization<br />
2009-2010<br />
191
Progress of Routine Immunization in Bihar:<br />
The aim is to immunize all the children and pregnant mothers under Universal Immunization<br />
Programme, in order to reduce IMR, MMR and NMR through routine immunization of all<br />
children and mothers from six vaccine preventable disease in the state. The <strong>State</strong> of Bihar<br />
has shown excellent Progress over the Years as shown in the Graphs below.<br />
Evaluated % of Fully Immunized Child in Bihar<br />
*** Ongoing Immunization Survey being carried out by SHSB outsourced to FRDS(Formative Research & Development Services) in the 1st<br />
quarter of 2008 (completed in 10 randomly selected districts). In the next quarter another 10 districts are being taken.<br />
100<br />
90<br />
80<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
11 11.6<br />
NFHS 2 1998-<br />
99<br />
18.6<br />
32.8<br />
CES 2002 CES 2005 NFHS 3 2005-CES 2006-07DLHS,2008/09 Survey By<br />
06<br />
FRDS ***<br />
38<br />
42<br />
52<br />
Data source- NHFS & CES<br />
Average % of Annual Increase/Decrease in full Immunization from<br />
NFHS-II to NFHS –III<br />
(a comparison among some of the states along with Bihar)<br />
4<br />
3<br />
2.93 3.03<br />
2<br />
1<br />
1.31<br />
2.09<br />
0<br />
-1<br />
Andhra<br />
Pradesh<br />
Punjab<br />
Tamil<br />
Nadu<br />
-1.14<br />
Karnataka Kerala Rajasthan Assam West<br />
Bangal<br />
-0.71 -0.63<br />
Bihar<br />
-2<br />
-1.81 -1.71<br />
-3<br />
Data source –NFHS<br />
192
Antigenwise Reported % of Cumulative<br />
Coverage Bihar (Jan 07 Dec 07)<br />
Some of the initiatives for increasing Immunization-coverage is given below.<br />
‣ Micro-plans have been prepared for each District to ensure full coverage.<br />
‣ Vaccines & Auto-Disposable (AD) Syringes provided free of cost to all<br />
beneficiaries.<br />
‣ Alternate System of Vaccine Delivery has been put in place for delivery of<br />
Vaccines at Immunization sites (@ Rs 50/- per session site).<br />
‣ Support is being provided for POL to PHCs/Districts/WICs/WIFs for maintenance<br />
of Cold Chain on a daily basis.<br />
‣ Mobility support is given to all the Diistricts and all DIO`s for Supervision of R.I .in<br />
the field.<br />
‣ Alternate Vaccinators are hired @1400/- per month where ever there is a shortage in<br />
the Districts.<br />
‣ All the Electrical Cold-chain Equipment in the Field are Under Annual Maintenance<br />
Contract, which is out-sourced by the <strong>State</strong> Health Society.<br />
‣ Generator are also out-sourced in all the PHC for un-Interrupted Power Supply to all<br />
the PHCs /ILR Points.<br />
‣ Fund has been provided for the Construction of Safety-Pits in every Block-PHC for the<br />
safe disposal of AD-Syringes.<br />
‣ All the H.W. (ANM) is being trained based on the Health Workers Immunization<br />
Module in phases for Improving Immunization all across the <strong>State</strong>.<br />
‣ Special Post Flood catch up Immunization Campaign in the Five Most Flood Affected<br />
Districts of Bihar has been conducted following the massive floods.<br />
193
No. of R.I. Session Site Monitored<br />
45000<br />
40000<br />
35000<br />
30000<br />
25000<br />
20000<br />
15000<br />
10000<br />
5000<br />
0<br />
38304<br />
18579<br />
11031<br />
4891<br />
2005 2006 2007 2008<br />
Muskan…Ek Abhiyan<br />
It has been decided by the Government of Bihar to attain 100% immunization of infants and<br />
pregnant women, for which tracking of pregnant women and infants are being undertaken<br />
through MuskanEk Abhiyaan .<br />
Objective:<br />
‣ To achieve 100% immunization of Infants and Pregnant Women<br />
Muskan … Operational Strategy<br />
‣ Convergence with ICDS and Health for our-reach-service delivery.<br />
‣ For Routine Immunization Aaganwadi Centers are acting as the service<br />
delivery unit as well as Headquarters for AWWs and ASHAs<br />
‣ For 8 10 AWWs , ANM are designated as Team Leader<br />
194
Components:<br />
‣ Tracking of all Pregnant Women and Newborns.<br />
‣ House-to-house survey.<br />
‣ Registration of all Pregnant Women and Children from 0 2 yrs age group<br />
‣ Immunization sessions at Anganwadi Centers on each Friday.<br />
‣ Field Verification in the form of Supportive Supervision by both MO`s<br />
& CDPO`s are also planned under Muskan to Improve Immunization coverage<br />
in the Blocks<br />
‣ Due List register to Track and Identify Due Beneficiaries for every RI-Session.<br />
‣ Mahila Mandal Meetings in the AWC to improve Health & Nutrition, in the<br />
Village.<br />
Percentage of Sessions Held Vs Planned<br />
100<br />
90<br />
80<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
91 93 92 91<br />
2005 2006 2007 2008<br />
195
% Presence of ANM / AWW / ASHA at Session Sites<br />
100<br />
90<br />
80<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
91<br />
94<br />
96<br />
95<br />
62<br />
68<br />
82<br />
88<br />
54<br />
57<br />
52<br />
75<br />
0<br />
14<br />
55<br />
64<br />
ANM Presence<br />
Mobilizer<br />
Presence<br />
ICDS<br />
Presence<br />
ASHA<br />
Presence<br />
2005 2006 2007 2008<br />
* Note : Year 2005 - Aug’2005 to Dec’2005 (5 months) : N - 4891<br />
Year 2006 - Jan’2006 to Dec’2006 (12 months) : N - 11031<br />
Year 2007 - Jan’2007 to Dec’2007 (12 months) : N - 18579<br />
Year 2008 - Jan’2008 to Nov’2008 (11 months) : N - 38304<br />
Catch –up round for Immunization, Health and Nutrition improvement<br />
Of children and pregnant women<br />
In Flood Affected districts in Bihar Oct 2008<br />
Background and Objective.<br />
Following a breach in the river embankment at Kusha in Nepal On 18 th August 2008, river Kosi had<br />
changed its course and shifted over120 km eastwards. As a result, large areas of Supaul, Madhepura,<br />
Purnea, Saharsa and Araria in Bihar were inundated. For over two months normal activity was<br />
disrupted and access to many areas impossible. However, with waters slowly receding and with the<br />
advent of normalcy the Department of Health, Government of Bihar, launched a post flood health<br />
and nutrition Catch up Round from October 20 th -27 th , 2008, in the five flood-affected districts of<br />
Bihar. The round aimed at providing appropriate focused interventions for health and nutrition to<br />
vulnerable populations such as expecting mothers and children previously displaced or living in<br />
hitherto inaccessible areas and at catching-up and thereafter restoring routine health services like<br />
immunization throughout the flood-affected districts.<br />
Interventions:<br />
The interventions identified for delivery during the round were as follows:<br />
Intervention Role Age group<br />
Catch-up Routine Proven to decrease morbidity and mortality Pregnant women and children<br />
immunization through 6 vaccine preventable diseases. as per EPI schedule<br />
196
Catch–up<br />
Vitamin A doses<br />
De-worming<br />
tablets<br />
Low osmolarity<br />
ORS<br />
Zinc<br />
Proven to prevent diarrhea as well as used to<br />
prevent measles and its complications<br />
Effective against intestinal parasites<br />
Prevention and treatment of dehydration due<br />
to diarrhea<br />
Prevention of pneumonia and prevents as well<br />
as limits diarrhea incidence<br />
9 months to 5 years<br />
2 years to 5 years<br />
All children affected with<br />
diarrhea; 6 months to 5 years<br />
Along with ORS<br />
The Coverage achieved during the Catch-up round were 768754 vaccine doses for routine<br />
immunization, 1347604 vitamin A doses (91.8% of total 1479642 estimated eligible children),<br />
817197 tablets of Albendazole (65.75% of 1242858 estimated eligible children) and 53532 courses<br />
of Zinc and ORS for children with diarrhea.<br />
Primary vaccine coverage (coverage of infants with EPI vaccines schedule by 1 completed year) was<br />
targeted against the estimated population of infants and pregnant women eligible for vaccine doses in a<br />
two-month period (two months being the duration of disruption of routine immunization services due<br />
to floods) and the following percent coverage was achieved for various antigens.<br />
% Coverage Achieved during Catchup Round<br />
91.1<br />
70.6<br />
71.0<br />
71.0<br />
60.3<br />
65.8<br />
33.2<br />
22.1<br />
38.3<br />
38.6 36.7<br />
38.7 36.8<br />
25.6<br />
TT1<br />
TT2+B<br />
BCG<br />
OPV0<br />
OPV1<br />
OPV2<br />
OPV3<br />
DPT1<br />
DPT2<br />
DPT3<br />
Measles<br />
Fully<br />
Immunized<br />
Vitamin A*<br />
Deworming<br />
tablet*<br />
% S e s s i o n s h e l d o u t o f t h o s e p l a n n e d d u r i n g c a t c h - u p r o u n d<br />
9 5<br />
9 2<br />
9 9 9 7 9 5 9 6<br />
A r a r i a M a d h e p u r a P u r n e a S a h a r s a S u p a u l 5 f l o o d a f f e t c e d<br />
d i s t r i c t s<br />
Catch-up Round Antigen Wise % Coverage achieved<br />
(of 2 monthly estimated target) for Pregnant women & Children#<br />
197
District<br />
Pregnant<br />
women Infants (birth to 1 year) 9m-5y 6m-5y<br />
TT1<br />
TT2+<br />
B<br />
BCG<br />
OP<br />
V0<br />
OPV<br />
1<br />
OPV<br />
2<br />
OPV<br />
3<br />
DPT<br />
1<br />
DPT<br />
2<br />
DPT<br />
3<br />
Msls<br />
Full<br />
Imnzed<br />
Vit A*<br />
Deworm<br />
tablet*<br />
ARARIA 33.5 24.0 81.6 44.0 75.6 45.2 43.9 75.4 45.5 43.6 61.0 39.3 98.5 91.4<br />
MADHEPUR<br />
A<br />
29.8 14.6 66.0 39.4 57.4 28.2 29.3 57.3 28.1 29.1 57.8 29.2 83.4 70.3<br />
PURNEA 33.7 24.5 59.5 35.8 70.3 40.1 35.5 72.5 39.8 36.1 51.5 19.0 92.5 40.6<br />
SAHARSA 39.3 26.7 86.0 38.1 83.7 43.3 38.2 80.3 44.4 38.6 71.4 10.7 90.2 74.5<br />
SUPAUL 29.9 19.1 64.2 34.4 67.5 33.4 34.8 67.4 33.1 34.4 64.7 28.4 87.1 60.6<br />
Grand Total 33.2 22.1 70.6 38.3 71.0 38.6 36.7 71.0 38.7 36.8 60.3 25.6 91.1 65.8<br />
* Annual targets are taken for VitA and Deworming tablets as biannual supplementary dose was administered during Catch-up round<br />
Catch-up Round Coverage Report Antigen Wise#<br />
District ARARIA MADHEPURA PURNEA SAHARSA SUPAUL Grand Total<br />
Session Planned 1775 1122 2658 1468 1325 8348<br />
Session Held 1686 1035 2620 1446 1257 8044<br />
of TT1 5048 3223 6068 4195 3700 22234<br />
TT2 3345 1420 4142 2529 2322 13758<br />
TTB 270 154 268 322 40 1054<br />
BCG 11174 6482 9749 8350 7225 42980<br />
OPV 0 6027 3875 5856 3697 3865 23320<br />
OPV 1 12332 7055 12824 10550 8751 51512<br />
OPV 2 7339 3275 6980 5343 4162 27099<br />
OPV 3 7537 3507 6380 4861 4471 26756<br />
DPT 1 12257 7014 13098 9948 8755 51072<br />
DPT 2 7392 3286 6997 5364 4160 27199<br />
DPT 3 7546 3509 6461 4941 4431 26888<br />
Measles 11665 8806 9981 12916 13064 56432<br />
Fully Immunized 7887 2873 5303 1640 3300 21003<br />
Vitamin 'A' 320427 201623 388835 234736 201983 1347604<br />
Deworming 251244 141507 144313 163970 116163 817197<br />
ORS & Zinc 14894 7840 21243 6816 2739 53532<br />
# Provisional reports<br />
Future Plans<br />
In order to ensure full-immunization status of infants in the flood affected areas, it is necessary that<br />
coverage of subsequent doses of OPV and DPT (2 nd and 3 rd doses) also be achieved at a level similar<br />
to that of the first dose. Two more catch-up rounds with the vaccination component in these districts<br />
spaced 4-6 weeks apart would give opportunity to achieve this.<br />
Bundling of a number of interventions had led to greater acceptability of services by the beneficiaries,<br />
empowering of the village level service provider and closer monitoring by multiple stakeholders<br />
198
involved in the various program components followed in the catch-up strategy. This approach could be<br />
scaled up to cover a larger geographical area during regular sessions of Routine Immunization.<br />
199
Introduction<br />
Strategic Plan for<br />
Measles Mortality Reduction In Bihar 2009<br />
Vaccine preventable diseases still remain major causes of morbidity, disability and mortality,<br />
with an estimated 40000 deaths (Chart 1 below) occurring annually in the Bihar <strong>State</strong>. This<br />
document outlines measles control acceleration strategies that Governments and stakeholders in<br />
immunization in the Bihar <strong>State</strong> will implement from 2009 onwards.<br />
Chart 1: Estimated Measles Mortality by Indian <strong>State</strong> 2006<br />
(Source: Preliminary results from a workshop held at NPSU, New Delhi, May 2007)<br />
70,000<br />
60,000<br />
Measles Deaths<br />
50,000<br />
Measles Deaths<br />
40,000<br />
30,000<br />
20,000<br />
10,000<br />
-<br />
LAKSHADWEEP<br />
A&N ISLANDS<br />
D&N HAVELI<br />
PONDICHERRY<br />
GOA<br />
SIKKIM<br />
DAMAN & DIU<br />
HIMACHAL PRADESH<br />
CHANDIGARH<br />
MIZORAM<br />
KERALA<br />
DELHI<br />
TAMIL NADU<br />
ARUNACHAL PR.<br />
MANIPUR<br />
JAMMU & KASHMIR<br />
TRIPURA<br />
MEGHALAYA<br />
NAGALAND<br />
PUNJAB<br />
UTTARANCHAL<br />
HARYANA<br />
KARNATAKA<br />
CHHATTISGARH<br />
MAHARASHTRA<br />
GUJARAT<br />
ORISSA<br />
ANDHRA PRADESH<br />
WEST BENGAL<br />
ASSAM<br />
JHARKHAND<br />
MADHYA PRADESH<br />
RAJASTHAN<br />
<strong>BIHAR</strong><br />
UTTAR PRADESH<br />
<strong>State</strong> Health Society, Bihar- is proposing this strategic plan aimed at guiding measles mortality<br />
reduction in Bihar. As a resource mobilization tool, the plan summarizes the requirements for measles<br />
control including routine measles immunization, supplemental immunization activities and Measles<br />
surveillance, as well as the projected <strong>State</strong> Health Society, Bihar support needs. For the purpose of<br />
monitoring progress with implementation, a set of milestones is included.<br />
Measles related Morbidity and mortality in Bihar<br />
200
U5MR<br />
110<br />
100<br />
90<br />
80<br />
70<br />
60<br />
50<br />
40<br />
B<br />
i<br />
h<br />
a<br />
r<br />
Non-Measles Mortality Rate Measles Mortality Rate Target for Child Mortality<br />
Potential Contribution of Accelerated Measles Control to Achieving MDG4 in India, 2006<br />
Reduction of Measles associated mortality would be a key intervention for Bihar to achieve the 4 th<br />
Millennium development goal. About half of the goal would be achievable just by reducing the<br />
measles deaths in the state.<br />
Of all the states in India, Bihar is poised to benefit most from Measles SIA leading to Measles<br />
mortality reduction.<br />
Measles outbreaks in Bihar<br />
In the year 2008-2009 (till Jan), Fourteen measles outbreaks were investigated in Bihar and the<br />
following age distribution of cases was determined. There were 485 cases (Age distribution of 394<br />
cases available) and 26 deaths reported from these outbreaks (Case Fatality rate 5.36). One outbreak<br />
was confirmed with laboratory diagnosis and the remaining was through clinical examination.<br />
88 % of the cases were between one and nine completed years justifying the age bracket to be covered<br />
during measles catch-up round.<br />
201
S<br />
No<br />
Measles outbreaks in Bihar 2008-2009 (status till 30th Jan 2009)<br />
Age distribution<br />
Number<br />
Month of Number<br />
120-<br />
District<br />
of 0-11 12-59 60-119<br />
outbreak of cases<br />
deaths<br />
179<br />
months months months<br />
months<br />
>179<br />
months<br />
1 Champaran East March 13 0 1 5 3 4 0<br />
2 Patna April 7 0 0 6 1 0 0<br />
3 Patna April 33 0 2 7 9 6 0<br />
4* Patna April 23 0<br />
5 Supaul November 37 2 0 29 7 1 0<br />
6 Bhagalpur November 5 0 0 4 0 1 0<br />
7* Madhubani December 52 3<br />
8 Madhepura December 51 7 0 28 19 1 0<br />
9 Madhepura December 10 1 0 8 0 0 0<br />
10 Madhepura December 27 0 0 10 12 3 0<br />
11<br />
Champaran<br />
West<br />
December 33 5 0 20 13 0 0<br />
12 Darbangha December 136 5 0 65 52 11 8<br />
13 Vaishali January 23 1 4 10 8 1 0<br />
14 Champaran East January 35 2 1 21 8 5 0<br />
Bihar total 485 26 8 213 132 33 8<br />
1. <strong>BIHAR</strong> Strategic Action Plan for Measles Mortality reduction<br />
Strategies<br />
It is envisaged that the <strong>State</strong> Health Society, Bihar with the support of other partners realize the stated<br />
measles control goal and objective using the following strategies<br />
1. Strengthen routine immunization (EPI) to raise routine measles coverage to 80% and above.<br />
2. Establish measles surveillance<br />
3. Establish a measles laboratory network for the confirmation of cases/epidemics.<br />
4. Provide a second opportunity for measles vaccination<br />
a. Initially through a catch up supplementary mass campaigns for the children aged 9<br />
months to 9 completed years<br />
202
. Follow up SIAs every 3-5 years for successive birth cohorts and<br />
c. Introducing second dose of Measles vaccine in EPI schedule when the evaluated<br />
routine coverage of the first dose goes above 80% in all districts throughout the<br />
state.<br />
5. Improve the clinical management of measles cases through the IMNCI approach.<br />
Implementation Roles<br />
The Department of Health and <strong>State</strong> Health Society, Bihar will implement phased activities for<br />
measles control in the context of systems strengthening and development. This will require the<br />
collaboration of various stakeholders in the field of immunization.<br />
Role of Govt of India<br />
The primary responsibility for the realization of this plan lies with the Ministry of Health Govt of<br />
India. The key roles will include:<br />
· Adoption of the National strategies, and developing appropriate national plans related to<br />
Measles morbidity reduction.<br />
· Securing funds, vaccines and supplies for immunization and providing the same to the <strong>State</strong> of<br />
Bihar.<br />
· Developing modules for training and program communication for Measles Supplementary<br />
Immunization<br />
· Providing guidelines and support for surveillance of measles and setting up of Mealses<br />
laboratories.<br />
Role of partners<br />
The <strong>State</strong> Health Society Bihar will form a Measles Technical Advisory group, Bihar headed by the<br />
Executive Director and comprised of the <strong>State</strong> Program Officer Immunization and IDSP and<br />
representatives of the UNICEF, NPSP-WHO, IMA, IAP and NIPI. This task force will be the focal<br />
committee for day-to-day implementation of the plan. Besides implementing the plan, the task force<br />
will prepare guidelines for district activities, budget norms, reporting forms tally sheets, monitoring<br />
checklists for measles campaign and other control activities.<br />
UNICEF:<br />
Member of technical advisory group on Measles Mortality reduction<br />
Measles Surveillance<br />
· Support during the initial phase of sentinel surveillance<br />
· <strong>State</strong> level coordinator<br />
For the Supplementary Catch-up immunization campaign<br />
203
· Trainings and capacity building<br />
· Micro planning<br />
· Monitoring<br />
· Social Mobilization and IEC<br />
· Logistics and cold chain monitoring<br />
· Ensuring safe injection practices<br />
· Data compilation analysis<br />
· Post coverage surveys<br />
NPSP-WHO<br />
Member of technical advisory group on Measles Mortality reduction<br />
Role in surveillance<br />
· Support in outbreak based surveillance<br />
· Setting up laboratories for serological confirmation of Measles.<br />
Role in SIA catch-up<br />
· Trainings and capacity building<br />
· Micro planning<br />
· Monitoring of activity<br />
NIPI, IAP, IMA<br />
Members of Measles Technical Advisory group.<br />
Logistics and vaccine requirement for Measles SIA<br />
Logistics and vaccine requirement for Measles Mortality reduction activities<br />
Item Requirement details Requirement Units<br />
1 Measles vaccine 1 dose per child with 1.33 wastage factor with 100% coverage 35453109 doses<br />
2 Measles diluent 1 dose per child with 1.33 wastage factor with 100% coverage 35453109 doses<br />
3 0.5 ml AD syringe 1 Per child vaccinated with 10% wastage 38998419 syringes<br />
4 5 ml Disposal syringes 1 per 5 dose vial with 10% wastage 7799684 syringes<br />
5 Hubcutters 1 per team with 10% buffer 18700 hubcutters<br />
6 Mealses Eliza kits 100 per lab with 10% buffer 990 kits<br />
Timeline for activity<br />
Development of strategy and<br />
POA<br />
Adoption of strategy by TAG<br />
Mealses Bihar<br />
Initiation of vaccine<br />
procurement activities<br />
Measles campaign activity timeline<br />
2008 2009<br />
Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec<br />
204
Development of guidelines<br />
and forms etc.<br />
Review and planning for<br />
districts<br />
Planning workshop for<br />
districts (at region)<br />
Provision of Logistics and<br />
finance support<br />
District planning and<br />
preparation activities<br />
Campaign in districts<br />
Evaluation of campaign<br />
Measles surveillance<br />
Pulse Polio Programme (P.E. Progress in the <strong>State</strong>) <br />
In the last one and half years several initiatives have been taken by the Government of Bihar for<br />
eradication of Polio form the state. It has been observed that majority of P1 cases was restricted to the<br />
most inaccessible areas of Kosi river, covering 20 blocks and 10 districts. A Kosi Operational-Plan<br />
was developed for intensification of overal Polio.Eradication. Activities in these high risk Areas(both<br />
SIA & Surveillance), the salient features of the plan are :<br />
‣ Intensification of human resources in Kosi areas<br />
‣ New Geo political boundaries were formed respective of districts boundaries called grids<br />
for implementation of Kosi Operational Plan.<br />
‣ Intensified Monitoring of the Polio rounds by WHO, UNICEF and <strong>State</strong> Monitors.<br />
Bihar has shown excellent progress till 2008, as regards IEAG Observation for India is concerned.<br />
Among the three kind of Polio Virus, Bihar has eradicated P-2 Polio Virus since 1999, and the<br />
Endemic Transmission of P-1 cases, which is the most dreaded & Virulent of the three, has stopped<br />
circulating in Bihar since, June/08 with multiple mOPV-I SIA Rounds. Circulation of P-3 Cases has<br />
also declined in the <strong>State</strong> after completion of few effective SIA`s with mOPV III rounds in Bihar in<br />
2007/08. With the highest ever sensitivity of AFP-Surveillance in the <strong>State</strong>, Bihar is very close to the<br />
Goal of Polio Eradication in the Country.<br />
205
A. Baseline information<br />
S.No.<br />
Beneficiaries<br />
Target<br />
2008-09 2009-10<br />
1 Pregnant Women 3527925 3154129<br />
2 0 to 1yr infants 3207205 2980338<br />
3 1-2 yr 2178312<br />
4 2-5 yr 6930990<br />
5 5 yr 3366484<br />
6 10 yr 4554652<br />
7 16 yr 1980283<br />
S.No. Routine Immunization Sessions 2008-09 2009-10<br />
1 Session planned in Urban Areas 25668 43236<br />
2 Session planned in Rural Areas 1288920 1450032<br />
3 Total Sessions Planned 1314588 1493268<br />
4 No. of session with hired vaccinators* 17950<br />
5 No. of hired vaccinators* 4488<br />
* No. of sessions and vaccinators hired in 2008-09 and planned in for 2009-10<br />
B. Trend of IMR<br />
S.No. Year IMR of the <strong>State</strong>/UT<br />
1 2003 60<br />
2 2004 61<br />
3 2005 61<br />
4 2006 62<br />
5 2007 60<br />
206
C. District - Wise Coverage reports ( in Numbers)<br />
S.No.<br />
Name of<br />
District<br />
Yearly Target (2007-<br />
08)<br />
Infants<br />
Pregnant<br />
Women<br />
Yearly Target (2008-<br />
09)<br />
Infants<br />
Pregnant<br />
Women<br />
Measles<br />
TT2+Booster<br />
BCG<br />
2007-08 2008-09 2007-08 2008-09 2007-08 2008-09<br />
1 Araria 75850 83435 82154 90369 71426 55609 53438 47376 26677 12928<br />
2 Arwal 19217 21139 25472 28019 19565 5669 14789 9148 10529 6938<br />
3 Aurangabad 65134 71647 77520 85272 52364 35407 48171 38046 28221 22825<br />
4 Banka 58425 64268 62202 68422 46155 41364 38572 36155 26956 22651<br />
5 Begusarai 75853 83438 90589 99648 46940 86326 37747 94721 28142 43146<br />
6 Bhagalpur 83025 91328 93966 103363 70542 46374 69425 51503 51671 35857<br />
7 Bhojpur 71750 78925 86353 94988 53933 36959 45413 36403 33791 19553<br />
8 Buxor 46993 51692 54263 59689 33675 28643 26963 28907 17496 17018<br />
9<br />
Champaran<br />
(E) 117276 129004 152090 167299 70001 73579 60447 58879 30398 37633<br />
10<br />
Champaran<br />
(W) 101475 111623 117656 129422 77754 43653 79741 42504 31035 19026<br />
11 Darbhanga 83907 92298 127029 139732 87533 64465 63845 58303 36848 38408<br />
12 Gaya 112762 124038 133970 147367 151760 61691 130348 129237 39018 28515<br />
13 Gopalganj 73581 80939 83102 91412 54838 27312 48730 32190 33009 19888<br />
14 Jahanabad 32062 35268 54032 59435 28967 21503 24536 21313 16375 12971<br />
15 Jamui 49255 54181 35744 39318 48062 25995 49440 25278 43799 17070<br />
16 Kaimur 46873 51560 49667 54634 32271 22748 18911 23284 14322 20404<br />
17 Katihar 94855 104341 92389 101628 55404 37521 40871 40612 27264 22284<br />
18 Khagaria 53351 58686 49361 54297 50086 7397 44528 9891 23457 2780<br />
19 Kishanganj 59225 65148 50034 55037 35090 28746 20087 20871 17295 17239<br />
20 Lakhisarai 28210 31031 30977 34075 19125 14522 13162 13768 11360 7835<br />
21 Madhepura 53710 59081 58947 64842 49054 27609 46257 33712 21758 8452<br />
22 Madhubani 130872 143959 138056 151862 100567 72245 113280 72977 47531 46782<br />
23 Munger 39975 43973 43903 48293 33349 21498 28382 22333 21718 14118<br />
24 Muzaffarpur 130086 143095 144752 159227 103512 72154 92585 66242 65311 39724<br />
25 Nalanda 78829 86712 91569 100726 64187 33585 58584 31321 42918 18267<br />
26 Nawada 56888 62577 69960 76956 46188 23562 40682 22012 26618 16821<br />
27 Patna 145232 159755 182102 200312 78638 37002 65957 40147 49809 21395<br />
28 Purnia 87110 95821 98237 108061 86243 55908 62194 54418 41808 29232<br />
29 Rohtas 55022 60524 94679 104147 55552 35765 43020 38884 27413 21074<br />
30 Saharsa 56396 62036 58244 64068 45777 40598 36431 47480 22735 18717<br />
31 Samastipur 98400 108240 131976 145174 86296 50565 76510 62626 49677 32835<br />
32 Saran 120540 132594 125715 138287 89463 48408 71949 41714 54525 26130<br />
33 Sheikhpura 16796 18476 20304 22334 17344 13443 15333 13079 12207 8461<br />
34 Sheohar 11685 12854 19884 21872 12379 8009 8288 6741 5367 3193<br />
35 Sitamarhi 74005 81406 103229 113552 61276 50567 49249 51735 31339 27179<br />
36 Siwan 92250 101475 104735 115209 89098 48294 74734 58978 27177 14491<br />
37 Supaul 60846 66931 67471 74218 43812 24064 32206 28283 22471 15850<br />
38 Vaishali 100085 110094 104872 115359 86155 48126 69468 48643 46751 26351<br />
Total 2757806 3033592 3207205 3527925 2254381 1476885 1914273 1559714 1164796 814041<br />
207
S.N<br />
o.<br />
C. District - Wise Coverage reports ( in Numbers)<br />
Yearly<br />
Target<br />
(2007-08)<br />
Name of<br />
District<br />
Yearly<br />
Target<br />
(2008-09) OPV- 1 OPV -3<br />
DPT - 1 DPT -3<br />
Infants Infants 2007-08 2008-09 2007-08 2008-09 2007-08 2008-09 2007-08 2008-09<br />
1 Araria 75850 82154 59879 74065 59545 51039 71754 55904 62947 49000<br />
2 Arwal 19217 25472 14550 6155 24537 7732 19840 5176 16125 7101<br />
3 Aurangabad 65134 77520 54718 38166 59748 37157 55180 32933 56008 33270<br />
4 Banka 58425 62202 33293 28200 56833 26089 45935 24489 40969 23189<br />
5 Begusarai 75853 90589 37604 102068 57878 86499 46867 77730 36710 82272<br />
6 Bhagalpur 83025 93966 62763 46865 104013 43848 70735 40690 71323 36737<br />
7 Bhojpur 71750 86353 43680 33676 68999 27371 52223 30829 47746 26411<br />
8 Buxor 46993 54263 29459 31024 38683 27783 35845 22475 28417 20160<br />
9 Champaran (E) 117276 152090 64373 70184 62735 54274 75905 60587 62036 43997<br />
10 Champaran (W) 101475 117656 61242 44049 70240 39906 94102 32488 73716 31036<br />
11 Darbhanga 83907 127029 79661 58985 81172 51689 87601 51385 68768 45394<br />
12 Gaya 112762 133970 121371 132357 83802 120782 146805 103865 136817 111767<br />
13 Gopalganj 73581 83102 44496 28971 69954 27189 55801 22333 54359 22313<br />
14 Jahanabad 32062 54032 24612 17758 34451 16625 28402 13988 25152 12476<br />
15 Jamui 49255 35744 39570 25023 86350 23835 45336 18443 45512 18914<br />
16 Kaimur 46873 49667 20675 17329 31803 14952 29698 18132 20485 15988<br />
17 Katihar 94855 92389 52604 38036 58862 37465 56604 24719 44750 24470<br />
18 Khagaria 53351 49361 43962 5385 52575 6874 46225 4851 38936 5911<br />
19 Kishanganj 59225 50034 32484 27580 39978 20109 35215 23216 23142 16577<br />
20 Lakhisarai 28210 30977 20112 11895 23679 9502 20619 9270 16119 8473<br />
21 Madhepura 53710 58947 56024 31007 47220 22119 57863 31495 44020 21886<br />
22 Madhubani 130872 138056 76267 60326 106131 57643 93150 57141 75225 54793<br />
23 Munger 39975 43903 35504 21381 46483 15767 33777 16572 27595 15891<br />
24 Muzaffarpur 130086 144752 102314 80085 135174 67798 110341 59591 101213 53129<br />
25 Nalanda 78829 91569 51802 31432 89200 27695 65339 27309 61177 25419<br />
26 Nawada 56888 69960 39436 24967 56818 19624 45730 18589 44816 15896<br />
27 Patna 145232 182102 67150 33242 106010 32091 82834 30084 71447 29383<br />
28 Purnia 87110 98237 78157 56320 93199 48572 84139 47317 68317 40384<br />
29 Rohtas 55022 94679 50661 27362 59608 22090 55683 23149 47779 19912<br />
30 Saharsa 56396 58244 43989 44188 49546 31915 47684 69658 39628 30544<br />
31 Samastipur 98400 131976 84207 46018 111419 42649 100249 41324 80768 40646<br />
32 Saran 120540 125715 79048 48527 115303 37780 89646 42784 84162 40080<br />
33 Sheikhpura 16796 20304 18192 11430 24620 12763 18178 11362 16524 12645<br />
34 Sheohar 11685 19884 11236 6205 10850 4475 13278 6259 9212 4631<br />
35 Sitamarhi 74005 103229 53647 48770 70514 45445 63711 41876 53008 38648<br />
36 Siwan 92250 104735 121737 97860 58362 52905 122454 97860 71808 53004<br />
37 Supaul 60846 67471 41117 27285 52335 24409 43897 27471 33646 22366<br />
38 Vaishali 100085 104872 68343 41068 93229 35621 82176 34296 78170 30220<br />
Total 2757806 3207205 2019939 1575244 2491858 1332081 2330821 1357640 1978552 1184933<br />
208
S.N<br />
o.<br />
C. District - Wise Coverage reports ( in<br />
Numbers)<br />
Name of<br />
District<br />
Yearly<br />
Target<br />
(2007-08)<br />
Infants<br />
Yearly<br />
Target<br />
(2008-<br />
09)<br />
Infants<br />
Hep B- Birth Hep B-1 Hep B-3<br />
2007<br />
-08<br />
2008<br />
-09<br />
2007-<br />
08<br />
2008-<br />
09<br />
2007-<br />
08<br />
2008-<br />
09<br />
JE-routine<br />
(Wherever<br />
applicable<br />
2007<br />
-08<br />
2008-<br />
09<br />
Vit A- Ist Dose<br />
2007-08 2008-09<br />
1 Araria 75850 82154<br />
37985 30909<br />
2 Arwal 19217 25472 11342 7752<br />
3 Aurangabad 65134 77520 38293 31881<br />
4 Banka 58425 62202 16174 16923<br />
5 Begusarai 75853 90589 13181 51987<br />
6 Bhagalpur 83025 93966 50095 41790<br />
7 Bhojpur 71750 86353 31980 25849<br />
8 Buxor 46993 54263 12529 21475<br />
9 Champaran (E) 117276 152090 31507 38343<br />
10 Champaran (W) 101475 117656 37820 20901<br />
11 Darbhanga 83907 127029 29540 36335<br />
12 Gaya 112762 133970 94657 47870<br />
13 Gopalganj 73581 83102 33997 27698<br />
14 Jahanabad 32062 54032 11863 12937<br />
15 Jamui 49255 35744 26521 36879<br />
16 Kaimur 46873 49667 17332 17037<br />
17 Katihar 94855 92389 20849 19329<br />
18 Khagaria 53351 49361 22537 4604<br />
19 Kishanganj 59225 50034 14249 14962<br />
20 Lakhisarai 28210 30977 4708 7149<br />
21 Madhepura 53710 58947 24777 27396<br />
22 Madhubani 130872 138056 72472 63159<br />
23 Munger 39975 43903 14868 17487<br />
24 Muzaffarpur 130086 144752 58300 51145<br />
25 Nalanda 78829 91569 31565 19016<br />
26 Nawada 56888 69960 21076 14319<br />
27 Patna 145232 182102 41274 27527<br />
28 Purnia 87110 98237 37126 30051<br />
29 Rohtas 55022 94679 25145 33176<br />
30 Saharsa 56396 58244 22464 32437<br />
31 Samastipur 98400 131976 34012 33770<br />
32 Saran 120540 125715 60809 39062<br />
33 Sheikhpura 16796 20304 11124 10560<br />
34 Sheohar 11685 19884 4160 4358<br />
35 Sitamarhi 74005 103229 26174 31930<br />
36 Siwan 92250 104735 48292 27350<br />
37 Supaul 60846 67471 12838 13981<br />
38 Vaishali 100085 104872 50466 44826<br />
Total 2757806 3207205 1154101 1034160<br />
Not Applicable<br />
209
S.No.<br />
D. District - wise VPD reports in 2008-09 ( in numbers)<br />
Teta<br />
nus<br />
Dipthe Pertus N (oth<br />
Polio<br />
Name of District ria is Tetanus er) Measles -P1<br />
Cases<br />
Deaths<br />
Cases<br />
Deaths<br />
Cases<br />
Deaths<br />
Cases<br />
Deaths<br />
1 Araria 6<br />
2 Aurangabad 1<br />
3 Banka 0 1<br />
4 Begusarai 12<br />
5 Bhagalpur 5 6<br />
6 Champaran (E) 13 8<br />
7 Champaran (W) 33 5 3<br />
8 Darbhanga 136 5 23<br />
9 Gaya 1<br />
10 Jamui 1 2<br />
11 Katihar 5<br />
12 Khagaria 22<br />
13 Kishanganj 1<br />
14 Lakhisarai 1<br />
15 Madhepura 88 8 13<br />
16 Madhubani 52 3 0 10<br />
17 Munger 2<br />
18 Muzaffarpur 14<br />
19 Nalanda 7<br />
20 Nawada 5<br />
21 Patna 63 9<br />
22 Purnia 9<br />
23 Saharsa 1 15<br />
24 Samastipur 0 30<br />
25 Saran 1 2<br />
26 Sheikhpura 2<br />
27 Sitamarhi 7<br />
28 Siwan 2<br />
29 Supaul 37 2 4<br />
30 Vaishali 23 1 6<br />
Grand Total As on Jan 09 450 24 3 229<br />
Cases<br />
Deaths<br />
Cases<br />
Deaths<br />
Polio-<br />
P3<br />
Cases<br />
Deaths<br />
Cases<br />
AES<br />
Deaths<br />
210
VPDs<br />
No. of<br />
Outbreaks<br />
reported<br />
2007-<br />
08<br />
E. Total VPD outbreaks in <strong>State</strong>/UT<br />
No. of<br />
OutbreaksInvestigated<br />
2008-<br />
2007-<br />
# 2007-08 2008-09#<br />
09 08<br />
No. of cases<br />
in Outbreaks<br />
2008- 2007-<br />
09 # 08<br />
No. of<br />
Deaths in<br />
Outbreaks<br />
2008-<br />
09 #<br />
Measures<br />
Taken<br />
Remarks<br />
Diphtheria 34<br />
Pertusis 786<br />
Measles 12 11 741 23<br />
AES<br />
Outbreak<br />
response, Vit-A<br />
supplementation,<br />
treatment of<br />
cases<br />
# Report for 2008-09 till Dec '08<br />
F. District Wise - AEFI Surveillance<br />
S.No.<br />
Name of District<br />
AEFI Committee<br />
constituted<br />
( Y/N)<br />
Serious AEFI<br />
Cases<br />
( till Dec ' 08)<br />
AEFI Deaths<br />
(till Dec'08)<br />
No. of<br />
FIRs sent<br />
No. of<br />
PIRs sent<br />
No. of<br />
DIRs sent<br />
Remarks<br />
1 Araria Yes<br />
2 Arwal Yes<br />
3 Aurangabad Yes<br />
4 Banka Yes<br />
5 Begusarai Yes<br />
6 Bhagalpur Yes<br />
7 Bhojpur Yes<br />
8 Gaya Yes 1<br />
9 Gopalganj Yes<br />
10 Kaimur Yes<br />
11 Khagaria Yes<br />
12 Kishanganj Yes<br />
13 Lakhisarai Yes<br />
14 Madhubani Yes 3<br />
15 Munger Yes 2<br />
16 Nalanda Yes<br />
17 Nawada Yes<br />
18 Saharsa Yes<br />
19 Sheikhpura Yes<br />
20 Sitamarhi Yes<br />
21 Siwan Yes<br />
22 Vaishali Yes 1<br />
23 Darbhanga 1<br />
24 Samastipur 1<br />
25 Katihaar 1<br />
Total 10 10 2 1<br />
211
G. RIMS status<br />
S.No. Name of District<br />
RIMS Installed Computer<br />
RIMS uploaded*<br />
& Operational Assistant Apr'08 May'08 Jun'08 Jul'08 Aug'08 Sep'08 Oct'08 Nov'08 Dec'08<br />
1 Banka Yes Yes Yes No Yes Yes Yes Yes Yes Yes<br />
2 Bhagalpur Yes<br />
3 Bhojpur Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes<br />
4 Buxar Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes<br />
5 Champaran-W Yes<br />
6 Darbhanga Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes<br />
7 Gopalganj Yes Yes Yes<br />
8 Kaimur Yes Yes Yes Yes Yes Yes Yes Yes<br />
9 Kishanganj Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes<br />
10 Madhubani Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes<br />
11 Munger Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes<br />
12 Saharsa Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes<br />
13 Samastipur Yes<br />
14 Saran Yes<br />
15 Sheikhpura Yes<br />
16 Sheohar Yes<br />
17 Sitamarhi Yes<br />
18 Siwan Yes<br />
19 Supaul Yes<br />
<strong>STATE</strong> / UT ** Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes<br />
*Write Yes/No for the month the district has uploaded RIMS data of district<br />
**Write Yes /No for the month the <strong>State</strong>/UT has uploaded <strong>State</strong>/UT level data<br />
212
Item<br />
H. Vaccine , Cold Chain and Other logistics<br />
Requirement<br />
Stock<br />
( Functional)**<br />
2009-10 2010-11<br />
Cold Chain Equipments-<br />
WIC 10 9 4<br />
WIF 3 2 1<br />
ILR-140 L (Small) 772 355 50<br />
ILR-300 L (Large) 92 82 20<br />
DF-140 L (Small) 467 175 25<br />
DF-300 L (Large) 162 128 20<br />
Cold Boxes L 3914 1190 1000<br />
Cold Boxes S 1769 1050 800<br />
Vaccine Carriers 59127 22950 15000<br />
Ice Pack 68530 197500 100000<br />
Vaccine Van 46 Not Required<br />
Vaccine stock and requirement ( including 25% wastage and 25% buffer)<br />
TT 2169245 2386170<br />
BCG 2860780 3146858<br />
OPV 919353 1011288<br />
DPT* 2398384 2638222<br />
Measles 984374 1082811<br />
Hep B<br />
JE(Routine)<br />
Remarks<br />
Including 5 replacements<br />
& 4 New for 2009-10<br />
Replacement out of 1 and<br />
One new<br />
Syringes including wastage of 10% and 25% buffer<br />
0.1ml 396956 4070720 4681328<br />
0.5ml 2571222 33379913 38386900<br />
Reconstitutional<br />
Syringes<br />
126864 6931501 7971226<br />
New ANM recruitment in<br />
Hub Cutters<br />
Very few<br />
process & further<br />
15800 8000<br />
functional<br />
additional Hubcutter<br />
needed.<br />
** As on 31st Dec '08 * Note : DPT is to be given instead of DT at 5 yrs w.e.f. 2009 - 10<br />
213
District wise and Head wise allocation of budget for Routine Immunization activities in Year 2009-10<br />
SL No. Name of District P.W. ANM<br />
<strong>State</strong> Total<br />
Allotment for<br />
the year<br />
2009-10<br />
Number<br />
of<br />
Alternate<br />
immunis<br />
Vaccinator<br />
ation<br />
Site<br />
District Profile used for calculation of Budget<br />
AWC ASHA HSC APHC BPHC Reffral<br />
+ SDH<br />
District<br />
Hospital/<br />
Metarnit<br />
y<br />
Hospital<br />
WIC<br />
+<br />
WIF<br />
Slums<br />
Under<br />
served<br />
Areas<br />
1 Araria 81600 285 257 497 2125 2026 424 73 9 4 1 60 95<br />
2 Arwal 21941 128 128 558 653 64 26 5 0 0 0<br />
3 Aurangabad 78966 436 446 2004 1842 207 58 11 4 1 1 86 15<br />
4 Banka 63106 546 546 1609 1552 265 32 10 4 0 33 138<br />
5 Begusarai 92920 568 598 2308 2245 289 25 18 2 1 50 119<br />
6 Bhagalpur 97221 611 611 2215 1966 280 41 16 3 1 1 133 70<br />
7 Bhojpur 86372 650 665 2104 2049 355 27 14 4 1 83 400<br />
8 Buxar 54528 374 15 374 1403 1318 287 47 11 1 1 92 110<br />
9 Champaran - E 153031 921 921 3897 2686 315 46 20 3 1 1 71 225<br />
10 Champaran - W 110256 454 38 465 2980 2734 377 30 17 3 1 52 127<br />
11 Darbhanga 118172 440 440 3231 2357 261 36 18 2 0 1 162 117<br />
12 Gaya 136251 877 877 3334 2997 541 73 25 2 3 265 241<br />
13 Gopalganj 93400 281 281 2158 2022 186 23 14 4 1 42 15<br />
14 Jahanabad 36264 257 257 925 769 104 32 7 3 1 82 0<br />
15 Jamui 54467 354 354 1397 1296 212 22 9 4 1 68 350<br />
16 Katihar 107722 469 472 2215 2174 257 25 16 3 1 28 154<br />
17 Kaimur 47962 307 307 1286 1247 196 19 10 4 1 150 94<br />
18 Khagaria 51331 382 382 1276 1204 193 24 7 1 1 45 63<br />
19 Kishanganj 66857 144 36 149 1296 1027 136 9 7 3 1 75 32<br />
20 Lakhisarai 31713 205 205 802 581 126 19 6 2 0 71 61<br />
21 Madhepura 60096 107 383 107 1526 1459 386 39 13 1 1 46 150<br />
22 Madhubani 162344 450 127 450 3569 3034 430 57 18 5 1 52 64<br />
23 Munger 44272 306 306 1074 951 227 33 9 1 1 86 17<br />
24 Muzaffarpur 159262 892 50 892 3669 3398 751 121 14 2 1 1 254 50<br />
25 Nalanda 80504 650 650 2319 1980 467 68 20 4 1 96 40<br />
26 Nawada 71303 424 40 424 1810 1810 338 56 14 3 1 85 44<br />
27 Patna 192249 888 893 3937 2634 418 60 23 6 0 4 771 316<br />
28 Purnia 94684 535 120 535 2482 2263 511 74 14 3 1 2 50 220<br />
29 Rohtas 91939 526 526 2309 2160 308 94 19 4 1 141 165<br />
30 Saran 128215 600 77 600 3178 3178 508 69 20 3 1 1 45 50<br />
31 Samastipur 17542 777 777 3438 3143 354 45 20 4 1 48 374<br />
32 Saharsa 60505 225 225 1428 676 152 15 10 0 1 1 102 109<br />
33 Sheikhpura 21005 179 179 526 439 85 17 6 2 0 44 0<br />
34 Sheohar 18997 35 31 35 513 495 34 7 5 2 0 25 16<br />
35 Siwan 90359 597 607 2618 2618 439 55 19 3 1 0 49<br />
36 Sitamarhi 106514 326 426 2557 2529 213 36 13 1 1 16 94<br />
37 Supaul 67163 119 133 119 1744 1538 178 19 11 3 0 56 300<br />
38 Vaishali 103096 576 640 2672 2532 337 30 17 2 1 0 16<br />
39 RDD/<strong>State</strong><br />
<strong>State</strong> Total 3154129 16901 1307 17366 80492 71582 11211 1582 515 105 32 13 3565 4500<br />
214
Mobility Support<br />
Cold chain maintenance<br />
Mobility<br />
support to<br />
District Officials<br />
Rs. 50000 per<br />
district (38) .<br />
Mobility<br />
support for<br />
supervision at<br />
state level @<br />
Rs. 100000 per<br />
year.<br />
machine per<br />
year for 2200<br />
machine<br />
( DF+ILR) and 10<br />
WIC and 3 WIF<br />
@ Rs. 10000<br />
per year and<br />
maintenance of<br />
vaccine vans<br />
@Rs.25000 per<br />
van for 47 vans.<br />
* 22,00,000 for<br />
AMC given at<br />
<strong>State</strong> level to<br />
one agency for<br />
repair of<br />
existing ILR &<br />
DF has been<br />
deducted from<br />
Rs. 50,00,000<br />
alloted and the<br />
remaining<br />
28,00,000 is<br />
divided for<br />
WIC/WIF<br />
maintainance of<br />
Vaccine vans as<br />
per approved<br />
rates. the final<br />
remaining<br />
amount of<br />
1430000 could<br />
be utilised for<br />
Minor Repair<br />
for district and<br />
regional Cold<br />
chain stores<br />
among the<br />
districts. @ Rs<br />
1900000 100000 5000000<br />
WIC/WIF Vaccine Van Minor Repair<br />
50000 25000 25859<br />
50000 25000 15515<br />
50000 10000 50000 31031<br />
50000 25000 28445<br />
50000 25000 49132<br />
50000 10000 50000 43960<br />
50000 25000 38788<br />
50000 25000 31031<br />
50000 10000 50000 54304<br />
50000 25000 46546<br />
50000 10000 50000 49132<br />
50000 25000 67233<br />
50000 25000 38788<br />
50000 25000 20687<br />
50000 25000 25859<br />
50000 25000 43960<br />
50000 25000 28445<br />
50000 25000 20687<br />
50000 25000 20687<br />
50000 25000 18101<br />
50000 25000 36203<br />
50000 25000 49132<br />
50000 25000 25859<br />
50000 10000 50000 38788<br />
50000 25000 54304<br />
50000 25000 38788<br />
50000 40000 50000 62061<br />
50000 20000 50000 38788<br />
50000 25000 51718<br />
50000 10000 50000 54304<br />
50000 25000 54304<br />
50000 10000 50000 28445<br />
50000 25000 18101<br />
50000 25000 15515<br />
50000 25000 51718<br />
50000 25000 36203<br />
50000 25000 31031<br />
50000 25000 46546<br />
100000 65002 2200000<br />
1900000 100000 195002 1175000 3629998<br />
215
Focus on slum & underserved areas in<br />
urban areas:<br />
for 3565 slums and 14385<br />
underserved areas @ Rs. 350<br />
per month per slum for one<br />
session<br />
* Slums @10000 population (<br />
Each AWC in a slum has 1500<br />
population therefore 7 slums<br />
=10000 population<br />
Alternate vaccinators<br />
honorarium<br />
(details in separate sheet)<br />
Mobilization of children through<br />
ASHA or other mobilizers<br />
@ Rs. 150 per month per per<br />
worker for 80000 sessions per<br />
month for remaining 5<br />
months as the <strong>State</strong> has<br />
budget the same under<br />
Muskan in RCH <strong>PIP</strong> . The state<br />
has projected this for month<br />
incase the same is not<br />
extended beyond Oct.09<br />
Alternative vaccine delivery in hard to reach areas<br />
Alternative vaccine delivery in<br />
hard to reach areas in 4500<br />
session per month @ Rs. 100<br />
per session<br />
Alternative Vaccine Deliery in<br />
other areas @ Rs. 50 per<br />
session for session- 17000<br />
ANMs for 104 days.<br />
75390000 60000000 5400000 88400000<br />
651000 4478600 1519500 114000 2470400<br />
0 98000 489750 0 665600<br />
424200 145600 1381500 18000 2301200<br />
718200 376600 1164000 165600 2673600<br />
709800 295400 1683750 142800 2966800<br />
852600 322000 1474500 84000 3093200<br />
2028600 397600 1536750 480000 2978000<br />
848400 478800 988500 132000 1812800<br />
1243200 702800 2014500 270000 4519200<br />
751800 792400 2050500 152400 2265600<br />
1171800 259000 1767750 140400 2147600<br />
2125200 473200 2247750 289200 4271200<br />
239400 67200 1516500 18000 1443200<br />
344400 144200 576750 0 1336400<br />
1755600 198800 972000 420000 1420800<br />
764400 201600 1630500 184800 2269600<br />
1024800 233800 935250 112800 1483600<br />
453600 270200 903000 75600 1910800<br />
449400 630000 770250 38400 736400<br />
554400 103600 435750 73200 992800<br />
823200 6463800 1094250 180000 376400<br />
487200 2258200 2275500 76800 2263200<br />
432600 196000 713250 20400 1570800<br />
1276800 1269800 2548500 60000 4578400<br />
571200 347200 1485000 48000 3332000<br />
541800 984200 1357500 52800 2152000<br />
4565400 515200 1975500 379200 4264400<br />
1134000 2374400 1697250 264000 2518000<br />
1285200 336000 1620000 198000 2537200<br />
399000 1621200 2383500 60000 3060000<br />
1772400 449400 2357250 448800 3591600<br />
886200 70000 507000 130800 1039200<br />
184800 92400 329250 0 930800<br />
172200 530600 371250 19200 162800<br />
205800 565600 1963500 58800 3097600<br />
462000 177800 1896750 112800 2102400<br />
1495200 2304400 1153500 360000 258800<br />
67200 273000 1899000 19200 3308800<br />
4197892 6313500 3496800<br />
38070892 31498600 60000000 5400000 88400000<br />
216
Computer Assistants support Printing and dissemination Review meetings<br />
Computer Assistants support for<br />
<strong>State</strong> level @ Rs. 12000 per person<br />
per month for 2 persons<br />
Computer Assistants support for<br />
District level @ Rs. 8000 per person<br />
per month for one computer<br />
assistant in each 38 districts<br />
Printing and dissemination of<br />
Immunization cards, tally sheets,<br />
monitoring forms etc. @ Rs. 5<br />
beneficiaries for 3469542<br />
beneficiaries with 10% buffer.<br />
Support for Quarterly <strong>State</strong> level<br />
review meetings of district officer @<br />
Rs. 1250/-/participant/day (<br />
CMO/DIO/Dist Cold chain Officer) for<br />
30 participants per meeting.<br />
Quarterly review meetings exclusive<br />
for RI at district level with one Block<br />
Mos, CDPO, and other stake holders<br />
@ Rs. 100 per participants for 5<br />
participants per per PHCs 515<br />
Quarterly review meetings exclusive<br />
for RI at block level @ Rs. 50/- PP as<br />
honorarium for ASHAs and Rs. 25 per<br />
persons for meeting expenses for<br />
80000 ASHAs<br />
288000 3648000 17347710 570000 1030000 24000000<br />
96000 448800 18000 607800<br />
96000 120676 10000 195900<br />
96000 434313 22000 552600<br />
96000 347083 20000 465600<br />
96000 511060 36000 673500<br />
96000 534716 32000 589800<br />
96000 475046 28000 614700<br />
96000 299904 22000 395400<br />
96000 841671 40000 805800<br />
96000 606408 34000 820200<br />
96000 649946 36000 707100<br />
96000 749381 50000 899100<br />
96000 513700 28000 606600<br />
96000 199452 14000 230700<br />
96000 299569 18000 388800<br />
96000 592471 32000 652200<br />
96000 263791 20000 374100<br />
96000 282321 14000 361200<br />
96000 367714 14000 308100<br />
96000 174422 12000 174300<br />
96000 330528 26000 437700<br />
96000 892892 36000 910200<br />
96000 243496 18000 285300<br />
96000 875941 28000 1019400<br />
96000 442772 40000 594000<br />
96000 392167 28000 543000<br />
96000 1057370 46000 790200<br />
96000 520762 28000 678900<br />
96000 505665 38000 648000<br />
96000 705183 40000 953400<br />
96000 96481 40000 942900<br />
96000 332778 20000 202800<br />
96000 115528 12000 131700<br />
96000 104484 10000 148500<br />
96000 496975 38000 785400<br />
96000 585827 26000 758700<br />
96000 369397 22000 461400<br />
96000 567028 34000 759600<br />
288000 570000 2525400<br />
217
288000 3648000 17347718 570000 1030000 24000000<br />
218
Trainings (separate annexure attached with details)<br />
Microplanning<br />
District level orientation for 2<br />
days for ANMs MPHW, LHV<br />
Health Assistants Nurse, Mid<br />
wife Bees and other specialist<br />
as per traning norm of RCH<br />
for 9000 persons in 600<br />
batches<br />
three days training of Mos on<br />
RI for 5000 persons in a group<br />
of 30 person per batch.<br />
One day refresher training of<br />
distict Computer assistants on<br />
RIMS/HIMS and<br />
immunization formats for 40<br />
persons in two batch.<br />
One day cold chain handlers<br />
training for block level cold<br />
chain hadlers by <strong>State</strong> and<br />
district cold chain officers in<br />
28 batchs. For 542 cold chain<br />
handlers<br />
One day training of block<br />
level data handlers by DIOs<br />
and District cold chain officer<br />
for 542 person.<br />
To develop microplan at subcentre<br />
level @ Rs 100/- per<br />
sub - centre<br />
For consolidation of<br />
microplans at block level @<br />
Rs. 1000 per block/ PHC(515)<br />
and at district level @ Rs.<br />
2000 per district for38<br />
districts.<br />
2183000 11271800 62000 704825 704825 1700000 591000<br />
68400 12800 10150 28500 11000<br />
82700 8000 6750 12800 7000<br />
143600 15200 11850 43600 13000<br />
366500 14000 11000 54600 12000<br />
287500 23800 17800 56800 20000<br />
313400 21400 16100 61100 18000<br />
386000 18800 14400 65000 16000<br />
221400 15200 11850 37400 13000<br />
680200 26200 19500 92100 22000<br />
89100 22600 16950 45400 19000<br />
164300 23800 17800 44000 20000<br />
419700 32200 23750 87700 27000<br />
68400 18800 14400 28100 16000<br />
142300 10400 8450 25700 9000<br />
195400 12800 10150 35400 11000<br />
117700 21400 16100 46900 18000<br />
229100 14000 11000 30700 12000<br />
253800 10400 8450 38200 9000<br />
15200 10400 8450 14400 9000<br />
103400 9200 7600 20500 8000<br />
59300 17600 13550 10700 15000<br />
164300 23800 17800 45000 20000<br />
192800 12800 10150 30600 11000<br />
376900 18800 14400 89200 16000<br />
338000 26200 19500 65000 22000<br />
181200 18800 14400 42400 16000<br />
375600 29800 22050 88800 25000<br />
242100 18800 14400 53500 16000<br />
327600 25000 18650 52600 21000<br />
300400 26200 19500 60000 22000<br />
436500 26200 19500 77700 22000<br />
68400 14000 11000 22500 12000<br />
93000 9200 7600 17900 8000<br />
7400 8000 6750 3500 7000<br />
179900 25000 18650 59700 21000<br />
174700 17600 13550 32600 15000<br />
60600 15200 11850 11900 13000<br />
266700 22400 16950 57600 19000<br />
11271800 62000<br />
8193500 11271800 62000 696800 532750 1690100 591000<br />
219
220
POL for vaccine delivery Consumables Injection safety<br />
POL for vaccine delivery<br />
from <strong>State</strong> to district and<br />
from district to<br />
PHC/CHCs @ Rs. 100000<br />
per district for 38<br />
districts.<br />
Consumables for<br />
computer including<br />
provision for internet<br />
access for RIMs Rs. 400<br />
per month per district<br />
for 38districts.<br />
Red/Black plastic bags<br />
etc. @ Rs.<br />
2/bags/session for<br />
17000<br />
(@ Rs 2 per bag for 2<br />
bags a month per ANM<br />
Bleach / Hypochlorite<br />
solution @ Rs. 500 per<br />
PHC/CHC per year for<br />
515 PHC<br />
Twin bucket @ Rs. 400<br />
per PHC/CHC per year<br />
for 515 PHCs<br />
3800000 182400 1279500<br />
100000 4800 13680 4500 3600<br />
100000 4800 6144 2500 2000<br />
100000 4800 20928 5500 4400<br />
100000 4800 26208 5000 4000<br />
100000 4800 27264 9000 7200<br />
100000 4800 29328 8000 6400<br />
100000 4800 31200 7000 5600<br />
100000 4800 17952 5500 4400<br />
100000 4800 44208 10000 8000<br />
100000 4800 21792 8500 6800<br />
100000 4800 21120 9000 7200<br />
100000 4800 42096 12500 10000<br />
100000 4800 13488 7000 5600<br />
100000 4800 12336 3500 2800<br />
100000 4800 16992 4500 3600<br />
100000 4800 22512 8000 6400<br />
100000 4800 14736 5000 4000<br />
100000 4800 18336 3500 2800<br />
100000 4800 6912 3500 2800<br />
100000 4800 9840 3000 2400<br />
100000 4800 5136 6500 5200<br />
100000 4800 21600 9000 7200<br />
100000 4800 14688 4500 3600<br />
100000 4800 42816 7000 5600<br />
100000 4800 31200 10000 8000<br />
100000 4800 20352 7000 5600<br />
100000 4800 42624 11500 9200<br />
100000 4800 25680 7000 5600<br />
100000 4800 25248 9500 7600<br />
100000 4800 28800 10000 8000<br />
100000 4800 37296 10000 8000<br />
100000 4800 10800 5000 4000<br />
100000 4800 8592 3000 2400<br />
100000 4800 1680 2500 2000<br />
100000 4800 28656 9500 7600<br />
100000 4800 15648 6500 5200<br />
100000 4800 5712 5500 4400<br />
100000 4800 27648 8500 6800<br />
4752<br />
3800000 182400 816000 257500 206000<br />
221
<strong>State</strong> specific requirement.<br />
POL of Generators for<br />
cold chain @ Rs. 600<br />
per day per WIC. Rs.<br />
500 per day per district<br />
and Rs. 400 per day per<br />
PHC.<br />
Catch Up campaigns for<br />
flood prone areas @ Rs.<br />
4813386 per district for<br />
5 districts.<br />
Ticklers bags for RI card<br />
counter foil @ rs. 250<br />
per bags per AWC for<br />
91703 workers<br />
Taken Rs 170 per bag<br />
for 80492 AWC<br />
Measles Mortality<br />
Reduction @ Rs. 45000<br />
per district year year for<br />
19 districts.<br />
Pits construction<br />
TOTAL<br />
0 0 13755450 0 319308510<br />
361250 11123639<br />
94860 2093995<br />
340680 6220002<br />
273530 7001766<br />
392360 8185766<br />
376550 8187854<br />
357680 9754964<br />
238510 5849847<br />
662490 12366973<br />
506600 8532396<br />
549270 8096018<br />
566780 12669790<br />
366860 5285836<br />
157250 3514125<br />
237490 6302560<br />
376550 7280893<br />
218620 5291542<br />
216920 5128614<br />
220320 3901733<br />
136340 3114653<br />
259420 10436287<br />
606730 10440354<br />
182580 4244223<br />
623730 13200875<br />
394230 8104406<br />
307700 6979507<br />
669290 15269995<br />
421940 10379920<br />
392530 8375311<br />
540260 10602547<br />
584460 11250591<br />
242760 3918483<br />
89420 2329491<br />
87210 1936389<br />
445060 8334259<br />
434690 7149768<br />
296480 7156170<br />
454240 8130012<br />
71810 31166956<br />
13755450 319308510<br />
222
223
S.no. District Name<br />
ANM -<br />
C<br />
Total<br />
Training<br />
load<br />
Health Workers training on Routine Immunization - Consolidated Budget 2009-10<br />
Total No. of<br />
training<br />
Batches ( 25<br />
person per<br />
batch)<br />
No of<br />
trainers<br />
per<br />
batch<br />
Honorarium + TA<br />
to Participants<br />
@Rs 400 per<br />
participants<br />
224<br />
Honararium for<br />
trainers/faculty<br />
@600 per day (<br />
subject to atleast 2<br />
lectature per guest<br />
faculty per day) for<br />
2 days<br />
Working lunch &<br />
Refreshments Rs 200<br />
per participants +<br />
faculty per day for 2<br />
days<br />
Incidential Exp for<br />
Photocopy , Job<br />
aids, flip charts,<br />
T.V./LCD hiring etc<br />
@ 250 per<br />
participants per<br />
days for 2 days<br />
Grand Total<br />
1 Araria 48 48 2 3 19200 3600 21600 24000 68400<br />
2 Arwal 59 59 2 3 23600 3600 26000 29500 82700<br />
3 Aurangabad 104 104 4 3 41600 3600 46400 52000 143600<br />
4 Banka 269 269 11 3 107600 3600 120800 134500 366500<br />
5 Begusarai 211 211 8 3 84400 3600 94000 105500 287500<br />
6 Bhagalpur 230 230 9 3 92000 3600 102800 115000 313400<br />
7 Bhojpur 284 284 11 3 113600 3600 126800 142000 386000<br />
8 Buxar 162 162 6 3 64800 3600 72000 81000 221400<br />
9 Champaran - E 502 502 20 3 200800 3600 224800 251000 680200<br />
10 Champaran - W 63 63 3 3 25200 3600 28800 31500 89100<br />
11 Darbhanga 119 119 5 3 47600 3600 53600 59500 164300<br />
12 Gaya 309 309 12 3 123600 3600 138000 154500 419700<br />
13 Gopalganj 48 48 2 3 19200 3600 21600 24000 68400<br />
14 Jahanabad 103 103 4 3 41200 3600 46000 51500 142300<br />
15 Jamui 142 142 6 3 56800 3600 64000 71000 195400<br />
16 Katihar 85 85 3 3 34000 3600 37600 42500 117700<br />
17 Kaimur 167 167 7 3 66800 3600 75200 83500 229100<br />
18 Khagaria 186 186 7 3 74400 3600 82800 93000 253800<br />
19 Kishanganj 8 8 1 3 3200 3600 4400 4000 15200<br />
20 Lakhisarai 74 74 3 3 29600 3600 33200 37000 103400<br />
21 Madhepura 41 41 2 3 16400 3600 18800 20500 59300<br />
22 Madhubani 119 119 5 3 47600 3600 53600 59500 164300<br />
23 Munger 140 140 6 3 56000 3600 63200 70000 192800<br />
24 Muzaffarpur 277 277 11 3 110800 3600 124000 138500 376900<br />
25 Nalanda 248 248 10 3 99200 3600 111200 124000 338000<br />
26 Nawada 132 132 5 3 52800 3600 58800 66000 181200<br />
27 Patna 276 276 11 3 110400 3600 123600 138000 375600<br />
28 Purnia 177 177 7 3 70800 3600 79200 88500 242100<br />
29 Rohtas 240 240 10 3 96000 3600 108000 120000 327600<br />
30 Saran 220 220 9 3 88000 3600 98800 110000 300400<br />
31 Samastipur 321 321 13 3 128400 3600 144000 160500 436500<br />
32 Saharsa 48 48 2 3 19200 3600 21600 24000 68400<br />
33 Sheikhpura 66 66 3 3 26400 3600 30000 33000 93000<br />
34 Sheohar 2 2 1 3 800 3600 2000 1000 7400
35 Siwan 131 131 5 3 52400 3600 58400 65500 179900<br />
36 Sitamarhi 127 127 5 3 50800 3600 56800 63500 174700<br />
37 Supaul 42 42 2 3 16800 3600 19200 21000 60600<br />
38 Vaishali 195 195 8 3 78000 3600 87600 97500 266700<br />
Total 5975 5975 241 114 2390000 136800 2679200 2987500 8193500<br />
Rates for training as per GOI guideline vide letter no. D.O.No.A-11033/101/2007-Trg dated 20.10.08<br />
S.no. District Name No. of PHCs<br />
Cold Chain Handler training on Routine Immunization - Consolidated Budget 2009-10<br />
No. of Cold<br />
Chain<br />
Handler (2<br />
per PHC & 2<br />
per district)<br />
Total<br />
Training<br />
load<br />
Total No. of<br />
training<br />
Batches ( 25<br />
person per<br />
batch)<br />
225<br />
No of<br />
trainers<br />
per batch<br />
Honorarium + TA<br />
to Participants<br />
@Rs 400 per<br />
participants<br />
Honararium for<br />
trainers/faculty @600<br />
per day ( subject to<br />
atleast 2 lectature per<br />
guest faculty per day)<br />
for 1 days<br />
Working lunch &<br />
Refreshments<br />
Rs 200 per<br />
Grand Total<br />
participants +<br />
faculty per day<br />
for one day<br />
1 Araria 9 20 20 1 1 8000 600 4200 12800<br />
2 Arwal 5 12 12 1 1 4800 600 2600 8000<br />
3 Aurangabad 11 24 24 1 1 9600 600 5000 15200<br />
4 Banka 10 22 22 1 1 8800 600 4600 14000<br />
5 Begusarai 18 38 38 2 1 15200 600 8000 23800<br />
6 Bhagalpur 16 34 34 2 1 13600 600 7200 21400<br />
7 Bhojpur 14 30 30 1 1 12000 600 6200 18800<br />
8 Buxar 11 24 24 1 1 9600 600 5000 15200<br />
9 Champaran - E 20 42 42 2 1 16800 600 8800 26200<br />
10 Champaran - W 17 36 36 2 1 14400 600 7600 22600<br />
11 Darbhanga 18 38 38 2 1 15200 600 8000 23800<br />
12 Gaya 25 52 52 2 1 20800 600 10800 32200<br />
13 Gopalganj 14 30 30 1 1 12000 600 6200 18800<br />
14 Jahanabad 7 16 16 1 1 6400 600 3400 10400<br />
15 Jamui 9 20 20 1 1 8000 600 4200 12800<br />
16 Katihar 16 34 34 2 1 13600 600 7200 21400<br />
17 Kaimur 10 22 22 1 1 8800 600 4600 14000<br />
18 Khagaria 7 16 16 1 1 6400 600 3400 10400<br />
19 Kishanganj 7 16 16 1 1 6400 600 3400 10400<br />
20 Lakhisarai 6 14 14 1 1 5600 600 3000 9200<br />
21 Madhepura 13 28 28 1 1 11200 600 5800 17600<br />
22 Madhubani 18 38 38 2 1 15200 600 8000 23800
23 Munger 9 20 20 1 1 8000 600 4200 12800<br />
24 Muzaffarpur 14 30 30 1 1 12000 600 6200 18800<br />
25 Nalanda 20 42 42 2 1 16800 600 8800 26200<br />
26 Nawada 14 30 30 1 1 12000 600 6200 18800<br />
27 Patna 23 48 48 2 1 19200 600 10000 29800<br />
28 Purnia 14 30 30 1 1 12000 600 6200 18800<br />
29 Rohtas 19 40 40 2 1 16000 600 8400 25000<br />
30 Saran 20 42 42 2 1 16800 600 8800 26200<br />
31 Samastipur 20 42 42 2 1 16800 600 8800 26200<br />
32 Saharsa 10 22 22 1 1 8800 600 4600 14000<br />
33 Sheikhpura 6 14 14 1 1 5600 600 3000 9200<br />
34 Sheohar 5 12 12 1 1 4800 600 2600 8000<br />
35 Siwan 19 40 40 2 1 16000 600 8400 25000<br />
36 Sitamarhi 13 28 28 1 1 11200 600 5800 17600<br />
37 Supaul 11 24 24 1 1 9600 600 5000 15200<br />
38 Vaishali 17 36 36 1 1 14400 600 7400 22400<br />
Total 515 1106 1106 52 38 442400 22800 231600 696800<br />
Rates for training as per GOI guideline vide letter no. D.O.No.A-11033/101/2007-Trg dated 20.10.08<br />
UNICEF will provide one trainer and all training materials for participants<br />
S.no.<br />
District Name<br />
No. of<br />
PHCs<br />
Block level Data Handler training on Routine Immunization - Consolidated Budget 2009-10<br />
Honararium for<br />
Total No. of<br />
trainers/faculty<br />
Honorarium + TA<br />
Total training No of<br />
@600 per day (<br />
to Participants<br />
Training Batches ( 25 trainers<br />
subject to atleast 2<br />
@Rs 400 per<br />
load person per per batch<br />
lectature per guest<br />
participants<br />
batch)<br />
faculty per day) for<br />
1 days<br />
No. of Data<br />
Handler (1<br />
per PHC & 2<br />
per district)<br />
226<br />
Working lunch<br />
& Refreshments<br />
Rs 200 per<br />
participants +<br />
faculty per day<br />
for one day<br />
Incidential Exp for<br />
Photocopy , Job<br />
aids, flip charts,<br />
T.V./LCD hiring<br />
etc @ 250 per<br />
participants per<br />
days for one day<br />
Grand Total<br />
1 Araria 9 11 11 1 1 4400 600 2400 2750 10150<br />
2 Arwal 5 7 7 1 1 2800 600 1600 1750 6750<br />
3 Aurangabad 11 13 13 1 1 5200 600 2800 3250 11850<br />
4 Banka 10 12 12 1 1 4800 600 2600 3000 11000<br />
5 Begusarai 18 20 20 1 1 8000 600 4200 5000 17800<br />
6 Bhagalpur 16 18 18 1 1 7200 600 3800 4500 16100<br />
7 Bhojpur 14 16 16 1 1 6400 600 3400 4000 14400<br />
8 Buxar 11 13 13 1 1 5200 600 2800 3250 11850<br />
9 Champaran - E 20 22 22 1 1 8800 600 4600 5500 19500
10 Champaran - W 17 19 19 1 1 7600 600 4000 4750 16950<br />
11 Darbhanga 18 20 20 1 1 8000 600 4200 5000 17800<br />
12 Gaya 25 27 27 1 1 10800 600 5600 6750 23750<br />
13 Gopalganj 14 16 16 1 1 6400 600 3400 4000 14400<br />
14 Jahanabad 7 9 9 1 1 3600 600 2000 2250 8450<br />
15 Jamui 9 11 11 1 1 4400 600 2400 2750 10150<br />
16 Katihar 16 18 18 1 1 7200 600 3800 4500 16100<br />
17 Kaimur 10 12 12 1 1 4800 600 2600 3000 11000<br />
18 Khagaria 7 9 9 1 1 3600 600 2000 2250 8450<br />
19 Kishanganj 7 9 9 1 1 3600 600 2000 2250 8450<br />
20 Lakhisarai 6 8 8 1 1 3200 600 1800 2000 7600<br />
21 Madhepura 13 15 15 1 1 6000 600 3200 3750 13550<br />
22 Madhubani 18 20 20 1 1 8000 600 4200 5000 17800<br />
23 Munger 9 11 11 1 1 4400 600 2400 2750 10150<br />
24 Muzaffarpur 14 16 16 1 1 6400 600 3400 4000 14400<br />
25 Nalanda 20 22 22 1 1 8800 600 4600 5500 19500<br />
26 Nawada 14 16 16 1 1 6400 600 3400 4000 14400<br />
27 Patna 23 25 25 1 1 10000 600 5200 6250 22050<br />
28 Purnia 14 16 16 1 1 6400 600 3400 4000 14400<br />
29 Rohtas 19 21 21 1 1 8400 600 4400 5250 18650<br />
30 Saran 20 22 22 1 1 8800 600 4600 5500 19500<br />
31 Samastipur 20 22 22 1 1 8800 600 4600 5500 19500<br />
32 Saharsa 10 12 12 1 1 4800 600 2600 3000 11000<br />
33 Sheikhpura 6 8 8 1 1 3200 600 1800 2000 7600<br />
34 Sheohar 5 7 7 1 1 2800 600 1600 1750 6750<br />
35 Siwan 19 21 21 1 1 8400 600 4400 5250 18650<br />
36 Sitamarhi 13 15 15 1 1 6000 600 3200 3750 13550<br />
37 Supaul 11 13 13 1 1 5200 600 2800 3250 11850<br />
38 Vaishali 17 19 19 1 1 7600 600 4000 4750 16950<br />
Total 515 591 591 38 38 236400 22800 125800 147750 532750<br />
Rates for training as per GOI guideline vide letter no. D.O.No.A-11033/101/2007-Trg dated 20.10.08<br />
S.no. District Name PHC PHC x<br />
5<br />
Calculation for Alternate Vaccinator (requirement and Honorarium - 2009-10<br />
APHC HSCs Total<br />
ANM -<br />
R<br />
ANM -<br />
C<br />
227<br />
Total<br />
ANM<br />
Diff of<br />
Personnel<br />
Altern<br />
ate<br />
Vaccin<br />
ator<br />
require<br />
d<br />
Honararium<br />
for Alternate<br />
vaccinator @<br />
Rs 1400/- per<br />
month<br />
No. of<br />
Contractu<br />
al ANM<br />
One month<br />
Honararium for<br />
Break period for<br />
Contractual<br />
ANM @ Rs<br />
1400/- per ANM<br />
Grand Total<br />
1 Araria 9 45 73 424 542 170 115 285 257 257 4317600 115 161000 4478600
2 Arwal 5 25 26 64 115 58 70 128 -13 70 98000 98000<br />
3 Aurangabad 11 55 58 207 320 332 104 436 -116 104 145600 145600<br />
4 Banka 10 50 32 265 347 277 269 546 -199 269 376600 376600<br />
5 Begusarai 18 90 25 289 404 357 211 568 -164 211 295400 295400<br />
6 Bhagalpur 16 80 41 280 401 381 230 611 -210 230 322000 322000<br />
7 Bhojpur 14 70 27 355 452 366 284 650 -198 284 397600 397600<br />
8 Buxar 11 55 47 287 389 212 162 374 15 15 252000 162 226800 478800<br />
9 Champaran - E 20 100 46 315 461 419 502 921 -460 502 702800 702800<br />
10 Champaran - W 17 85 30 377 492 344 110 454 38 38 638400 110 154000 792400<br />
11 Darbhanga 18 90 36 261 387 255 185 440 -53 185 259000 259000<br />
12 Gaya 25 125 73 541 739 539 338 877 -138 338 473200 473200<br />
13 Gopalganj 14 70 23 186 279 233 48 281 -2 48 67200 67200<br />
14 Jahanabad 7 35 32 104 171 154 103 257 -86 103 144200 144200<br />
15 Jamui 9 45 22 212 279 212 142 354 -75 142 198800 198800<br />
16 Katihar 16 80 25 257 362 325 144 469 -107 144 201600 201600<br />
17 Kaimur 10 50 19 196 265 140 167 307 -42 167 233800 233800<br />
18 Khagaria 7 35 24 193 252 189 193 382 -130 193 270200 270200<br />
19 Kishanganj 7 35 9 136 180 126 18 144 36 36 604800 18 25200 630000<br />
20 Lakhisarai 6 30 19 126 175 131 74 205 -30 0 74 103600 103600<br />
21 Madhepura 13 65 39 386 490 86 21 107 383 383 6434400 21 29400 6463800<br />
22 Madhubani 18 90 57 430 577 361 89 450 127 127 2133600 89 124600 2258200<br />
23 Munger 9 45 33 227 305 166 140 306 -1 0 140 196000 196000<br />
24 Muzaffarpur 14 70 121 751 942 585 307 892 50 50 840000 307 429800 1269800<br />
25 Nalanda 20 100 68 467 635 402 248 650 -15 0 248 347200 347200<br />
26 Nawada 14 70 56 338 464 201 223 424 40 40 672000 223 312200 984200<br />
27 Patna 23 115 60 418 593 520 368 888 -295 0 368 515200 515200<br />
28 Purnia 14 70 74 511 655 279 256 535 120 120 2016000 256 358400 2374400<br />
29 Rohtas 19 95 94 308 497 286 240 526 -29 0 240 336000 336000<br />
30 Saran 20 100 69 508 677 366 234 600 77 77 1293600 234 327600 1621200<br />
31 Samastipur 20 100 45 354 499 456 321 777 -278 0 321 449400 449400<br />
32 Saharsa 10 50 15 152 217 175 50 225 -8 0 50 70000 70000<br />
33 Sheikhpura 6 30 17 85 132 113 66 179 -47 0 66 92400 92400<br />
34 Sheohar 5 25 7 34 66 28 7 35 31 31 520800 7 9800 530600<br />
35 Siwan 19 95 55 439 589 193 404 597 -8 0 404 565600 565600<br />
36 Sitamarhi 13 65 36 213 314 199 127 326 -12 0 127 177800 177800<br />
37 Supaul 11 55 19 178 252 69 50 119 133 133 2234400 50 70000 2304400<br />
228
38 Vaishali 17 85 30 337 452 381 195 576 -124 0 195 273000 273000<br />
Total 515 2575 1582 11211 15368 9916 6700 16901 -1533 1307 21957600 6815 9541000 31498600<br />
229
PART- D<br />
National Disease Control Programmes<br />
(NDCP)<br />
2009-2010<br />
230
IDSP (Integrated Disease Surveillance Program)<br />
Surveillance is essential for the early detection of emerging (new) or re-emerging<br />
(resurgent) infectious diseases. In the absence of surveillance, disease may spread<br />
unrecognised by those responsible for health care or public health agencies, because<br />
many individual health care workers would see sick people in small numbers. By the time<br />
the outbreak is recognized, it may be too late for intervention measures. Continuous<br />
monitoring is essential for detecting the early signals of outbreak of any epidemic of a<br />
new or resurgent disease. For disease surveillance to prevent emerging epidemics, the<br />
time taken for effective action should be short.<br />
Integrated Disease Surveillance Program (IDSP) is intended to be the backbone of public<br />
health delivery system in the state. It is expected to provide essential data to monitor<br />
progress of on- going disease control programs and help in optimizing the allocation of<br />
resources. It will be able to detect early warning signals of impending outbreaks and help<br />
initiate an effective and timely response. IDSP will also facilitate the study of disease<br />
patterns in the state and identify new emerging diseases. It will play a crucial role in<br />
obtaining political and public support for the health programs in the state.<br />
Profile of Bihar : Bihar is located in the North East of India. It has a land with a covered<br />
area of 94,163 Sq. Km. It is mainly divided into two regions known as North of Ganges,<br />
and south of Ganges regions. The <strong>State</strong> is geographically classified into 38 districts and 72<br />
Sub divisions and 533 blocks. The population of Bihar as per 2001 Census is 828.8 million<br />
with a urban population of 8681800 as the density population per Sq. Km. is 880 against<br />
national figure of 324. There are 32 towns with a population of 50,000 or more and having<br />
about 40,000 villages in the state. The present sex ratio is 919 females per 1000 males<br />
(India Figure 933). The total literacy rate is 46.4%. It is mainly a rural inhabited state. The<br />
percentage of rural population is 66.08% against the Indias population of 72.2%.<br />
Diseases conditions under the surveillance program<br />
(i) Regular Surveillance:<br />
Vector Borne Disease:<br />
Malaria & Kala-azar<br />
Water Borne Disease: Acute Diarrhoeal Disease (Cholera) &<br />
Typhoid<br />
Respiratory Diseases:<br />
Tuberculosis<br />
Vaccine Preventable Diseases: Measles<br />
Diseases under eradication: Polio<br />
Other Conditions:<br />
Road Traffic Accidents<br />
231
Table 2: Integrated<br />
IDSP (Integrated Disease Surveillance Program)<br />
S.N. Heads Units Unit Cost Total<br />
1 Infrastructure<br />
a <strong>State</strong> Surveillance Cell at DMS & DHS 1 1,500,000 1,500,000<br />
b District Level Laboratory 39 100,000 3,900,000<br />
c Manuals 1 500000 500,000<br />
2 Laboratory<br />
a Equipment 39 100000 3,900,000<br />
b Reagents and consumables 39 200000 7,800,000<br />
3 Communication<br />
a Telephone & Fax 39 10000 390,000<br />
4 Salary<br />
a Data Entry Operator 39 6000 234,000<br />
b Accounts Assistant 39 5000 195,000<br />
5 Social Mobilization 39 30000 1,170,000<br />
6 Training 39 100,000 3,900,000<br />
7<br />
Biological Waste Management, 5%<br />
overhead expenses 39 917,000<br />
GRAND TOTAL 24,406,000<br />
(24406000 – 11400000 = 13006000)<br />
An amount One Crore Forteen lakhs (Rs. 1,14,00,000/-) was released to to <strong>State</strong>. Hence<br />
balance fund requirment will be Rs. 1,30,06,000/- lakhs (One crore Thirty lakhs six<br />
thousands only).<br />
232
IDSP (Integrated Disease Surveillance Project)<br />
SL No Name of District District Level IDSP Fund <strong>State</strong> Level IDSP Fund<br />
1 2 3 4<br />
1 Araria 574513.00<br />
2 Arwal 574513.00<br />
3 Aurangabad 574513.00<br />
4 Banka 574513.00<br />
5 Begusarai 574513.00<br />
6 Bhagalpur 574513.00<br />
7 Bhojpur 574513.00<br />
8 Buxar 574513.00<br />
9 Darbhanga 574513.00<br />
10 East Champaran 574513.00<br />
11 Gaya 574513.00<br />
12 Gopalganj 574513.00<br />
13 Jamui 574513.00<br />
14 Jehanabad 574513.00<br />
15 Kaimur 574513.00<br />
16 Katihar 574513.00<br />
17 Khagaria 574513.00<br />
18 Kishanganj 574513.00<br />
19 Lakhisarai 574513.00<br />
20 Madhepura 574513.00<br />
2574513.00<br />
21 Madhubani 574513.00<br />
22 Munger 574513.00<br />
23 Muzaffarpur 574513.00<br />
24 Nalanda 574513.00<br />
25 Nawada 574513.00<br />
26 Patna 574513.00<br />
27 Purnia 574513.00<br />
28 Rohtas 574513.00<br />
29 Saharsa 574513.00<br />
30 Samastipur 574513.00<br />
31 Saran 574513.00<br />
32 Sheikhpura 574513.00<br />
33 Sheohar 574513.00<br />
34 Sitamarhi 574513.00<br />
35 Siwan 574513.00<br />
36 Supaul 574513.00<br />
37 Vaishali 574513.00<br />
38 West Champaran 574513.00<br />
39 Unit Cost <strong>State</strong> Level<br />
Total 21,831,494.00 2,574,513.00<br />
Note- (i) District Level IDSP fund 21831494.00<br />
(ii) <strong>State</strong> Level IDSP Fund 2574513.00<br />
Total 24406007.00<br />
(24406007 - 11400000 = 13006007)<br />
233
An amount One Crore Forteen lakhs (Rs. 1,14,00,000/-) was released to <strong>State</strong>. Hence, balance fund requirement will be Rs.<br />
1,30,06,007/- lakhs (One Crore Thrity lakhs Six thousands Seven only),<br />
234
Iodine Deficiency Disorder<br />
Addressing Iodine Deficiency Disorders in Bihar.<br />
Introduction:<br />
Iodine deficiency is a world wide public health problem. It is the major cause of brain damage loss<br />
of energy, learning disability, poor motivation, poor human resource development and child<br />
survival. Thus, it remains a major threat to the health and development of school children and<br />
pregnant women. Children with iodine deficiency have intelligence (I.Q) 13.5 points less than that<br />
of children from areas where there is no iron deficiency. The only solution to this is simple and<br />
affordable, which is consumption of iodised salt. IDD elimination Programme was launched in the<br />
late 1960s. By 1988 legislative measures were put in place to ban the sale of non-iodised salt in the<br />
entire state.<br />
During the United Nations General Assembly Special Session for Children (2002), India has<br />
committed to eliminate IDD by 2005. Although, in national policy commitments, India commits to<br />
eliminate IDD by 2010, there is an urgent need to accelerate the strategy in India, especially when a<br />
decreasing trend, 49% to 37% (1998-99 to 2002-03), has been seen in households consuming<br />
adequately iodised salt.<br />
Iodine Deficiency Disorders in Bihar:<br />
In Bihar the northern part of the state lies in the sub-Himalayan region in which the existence of<br />
severe to moderate iodine deficiency in this region is well established. A recent study was<br />
undertaken in Bihar with support from UNICEF for Government of Bihar, to track progress towards<br />
sustainable elimination of IDD from the state. The results of the study reveal that iodine deficiency<br />
continues to be a public health problem. A high proportion of population (31.5%) has very low<br />
urinary iodine excretion suggesting existence of severe iodine deficiency in many pockets. Only<br />
40.1% of the households consume adequately iodised salt.<br />
The findings of this study warrant instituting corrective measure on a war footing to ensure that the<br />
population of Bihar has access to adequately iodised salt and at least 80% of the households receive<br />
and use adequately iodised salt.<br />
Major Objectives:<br />
· Creating universal demand for iodised salt at consumption level<br />
· Strengthening the monitoring system at the production level<br />
Role of Each Department:<br />
Awareness generation among consumers is a corner stone of the strategy and all possible means to<br />
disseminate information about the benefits of consuming iodised salt and to trigger behaviour<br />
change among the population. This surely requires the contribution of stakeholders outside the<br />
Health Department. In this regard the ICDS with its extended network of AWCs is a strong link<br />
through which the vulnerable population groups in the community can be reached out<br />
235
The priority of Iodine Deficiency Disorders should also be shouldered by the Education department.<br />
Schools provide an excellent infrastructure for promotional activities to reach out to masses thru<br />
children. Teachers can be trained for encouraging students to influence their families in purchasing<br />
iodised salt highlighting the benefit of IQ difference in children with iodine deficiency. Thus, a<br />
series of activities could be organized for awareness creation among children, who in turn can be<br />
expected to serve as change agents for influencing their families.<br />
Health:<br />
Health is the nodal department, while ICDS and Education will be the collaborating<br />
Departments. These have been specified under the role of departments of ICDS and Higher<br />
Education. To begin with the district will form a co-ordination Committee to take decisions on<br />
priority actions and review the progress of work once every quarter.<br />
However, the <strong>State</strong> Health Department will ensure the following:<br />
- Formation of District Co-ordination Committee to prioritize actions and review progress<br />
quarterly.<br />
Functions of District Co-ordination Committee:<br />
1. To facilitate Orientation and Planning Meetings for awareness generation<br />
and to strengthen monitoring of salt quality<br />
2. To support organization and implementation of awareness campaigns<br />
through schools and AWCs to reach out to the communities.<br />
3. To monitor campaigns/activities under the 3 departments and prepare<br />
district reports<br />
4. To institute follow-up actions in blocks areas with low or no iodine salt<br />
sale and consumption.<br />
- Directives to be issued to medical colleges and district hospitals and super specialty<br />
hospitals, for using iodised salt in cooking meals for the patients.<br />
- Civil Surgeon to hold meetings of lab technician and Food Inspectors in his district.<br />
- <strong>State</strong> Nutrition cell to ensure the following to districts and districts to distribute to AWCS,<br />
through CDPOs and to Schools through BEOs.<br />
- Reporting format<br />
- Distribution of STKs<br />
- Distribution of IEC material<br />
- Financial Support.<br />
ICDS:<br />
- Same Letter signed by Civil Surgeon, DPO and DSE for co-ordination by the functionaries<br />
of three district departments to organize and conduct joint training of ANMs and AWWs.<br />
- Directives to be re-issued as a reminder for use of iodised salt in supplementary food<br />
AWCs.<br />
236
- DPOs/DWOs to plan and conduct the orientation of CDPOs and LS.<br />
- CDPOs/LS to organize and carryout block level training of AWWs and their ANM along<br />
with MOICs and BEO<br />
- MOIC/CDPO to ensure supply of ST Kits, IEC materials, cash assistance etc to AWCs<br />
- Prepare a monitoring plan and carry out monitoring of the planned activities jointly in the<br />
village or community by involving the leaders, youth or school children.<br />
- Every AWW to prepare an Activity Report including a report on monitoring of salt<br />
- MOIC and CDPO to conduct joint review meetings with ANMs and AWWs in her/his block<br />
on 25th of every month.<br />
- DPO/CSEO to hold meeting of BEOs on 28 th of every month and receive reports for all<br />
schools in his district by 28 th of every month.<br />
- These meetings also to be utilized for planning activities for the next month with time line<br />
budget and role specificity.<br />
- MOIC and CDPO to facilitate organizing of activities in villages/tolas, AWW to take the<br />
lead.<br />
- ANM and AWW to prepare a joint report of activities to CS and DWO /DPO.<br />
- A copy of the report will be given to DSM.<br />
- DSM will forward a copy to RSM.<br />
- CS will forward a copy to MIS Cell of <strong>State</strong> Nutrition Cell.<br />
- MIS Cell will share a district-wise compiled report with UNICEF.<br />
Education:<br />
- Directives from DEO using iodised salt only in MDM in schools.<br />
- District DEO to facilitate and complete training of BEOs on IDD/USI<br />
- BEO to conduct training of Nodal Teachers along with MOIC/CDPO at the Block<br />
- Support Nodal Teachers to prepare a plan of activities and budget for the schools.<br />
- Submit a copy of plan and the budget of schools to DEOs office.<br />
- All students in the school to be sensitized with the problem of IDD and the benefits of<br />
iodised salt.<br />
Sensitizing School Children on IDD/IS<br />
School teacher shall take a 30 minutes class, and would explain to children why iodine is important,<br />
causes of iodine deficiency disorder, and consequences of IDD with emphasis on physical and<br />
mental development. Explain that iodised salt helps bring back iodine to the body. Thus iodised salt<br />
is important, but both iodised and non-iodised salt is available. Give emphasis to the difference in<br />
the IQ points up to 13, in children with iodine deficiency thus affecting leaning and school<br />
performance which further reflects on workout put and productivity. Thus good health can be<br />
ensured only with daily consumption of iodised salt.<br />
237
Activities within the school:<br />
- Essay/Story competition -Poetry Writing<br />
- Exhibitions -Play/Skits<br />
- Slogan writing -Songs<br />
-All children participating, to get a certificate and the best child/ children to get a prize)<br />
Monitoring salt for iodine content in the class room:<br />
All children requested to bring few pinches of salt from their homes<br />
Teacher to supervise the testing of salt using the kit, by each child. Children would be<br />
classified into two groups.<br />
Group 1 will have children with salt samples tested with adequate iodine.<br />
Group II will have children with salt samples tested with no iodine or inadequate iodine.<br />
Counseling to Group I: Your salt is of good quality and would allow you to perform well<br />
in school if you continue consuming iodised salt as you are and pay attention to your<br />
studies in the school. Insist that your parents always buy iodised salt only.<br />
Counseling to GroupII. Your salt does not contain iodine. Your are being left out from<br />
its benefits. If this continues, you are likely to face some serious risks. Your growth can<br />
be retarded and at the same time your school performance would be negatively affected.<br />
This can happen to your brothers and sisters, as they are also consuming the same salt<br />
without iodine or less amount of iodine that is required by the body. When we have the<br />
same session repeated next month, your salt test should show blue colour which means<br />
you have convinced your parents to buy salt which is iodised.<br />
In general, the Teacher should say, we want to see all children in group I and none in the<br />
other group. So our class should have children all using iodised salt.<br />
- BEOs to ensure supply of ST Kits, IEC materials, cash assistance etc to schools<br />
- Prepare a monitoring plan and carry out monitoring of the planned activities in the school<br />
along with MOICs and CDPOs.<br />
- Head Masters to facilitate organizing of activities within and outside school, Nodal Teacher<br />
to take the lead.<br />
Activities outside the school:<br />
- Organize Salt monitoring for advocacy in the community<br />
- Each Nodal Teacher to choose 20 children living in different localities<br />
- Each student to visit 15-20 houses and shops around them for monitoring and advocacy.<br />
- Slogans to be used for Prabhat Pheri<br />
- Human Chain<br />
- Marathon/Bicycle Race<br />
- All children to get a certificate, and the best performer to get a prize.<br />
238
- Each nodal teacher to prepare report for her class.<br />
- Every school to prepare an Activity Report including a report on monitoring of salt<br />
- BEO to conduct review meetings with Head Masters/Nodal Teachers on 25 th and collect the<br />
report for all schools in his block 25 th of every month.<br />
- DEO to hold meeting of BEOs on 28 th of every month and receive reports for all schools in<br />
his district by 28 th of every month.<br />
- These meetings also to be utilized for planning activities for the next month with time line<br />
budget and role specificity.<br />
Monitoring and Reporting:<br />
The monitoring of the activities will be done by the block level officers of all three departments. A<br />
plan for monitoring will be ensured and will prepared during the planning meetings.<br />
Each AWC/ANM will prepare a report and forward it to MOIC, CDPO BDO. The schools will<br />
prepare the activity report and forward it to BEO and BDO. The MOICs will compile and send the<br />
report to CS while, the CDPO will compile and send the report to DPO/DWO with a copy to CS.<br />
The BEO will compile for all schools in the block and forward it to DEO with a copy to CS.<br />
Civil Surgeon Office will prepare a final compiled report for the district and forward it to <strong>State</strong><br />
Nutrition Cell, copy to Directorate ICDS and Education, Government of Bihar, Patna.<br />
<strong>State</strong> Nutrition Cell and UNICEF along with Directors of respective departments will hold review<br />
meetings to discuss progress and strengthen efforts in low consumptions areas.<br />
<strong>State</strong> Nutrition Cell with support from UNICEF will also facilitate <strong>State</strong> Task Force Meeting in end<br />
September to take stock of achievements and future course of actions.<br />
_______________________________________________<br />
239
Budget for Intensified IDD / USI Activities in 38 District of Bihar<br />
Sl No. Name of District No. of PHC<br />
Training @<br />
Rs.1000<br />
Awareness @<br />
Rs. 500<br />
Activities in<br />
School @ 1000<br />
Activates at<br />
AWC &<br />
Communities<br />
@ 500<br />
IEC Material<br />
@ Rs.435<br />
1 ARWAL 5 5000 2500 5000 2500 2176<br />
2 AURANGABAD 11 11000 5500 11000 5500 4786<br />
3 BANKA 10 10000 5000 10000 5000 4351<br />
4 BEGUSARAI 19 19000 9500 19000 9500 8267<br />
5 BHAGALPUR 12 12000 6000 12000 6000 5221<br />
6 BHOJPUR 13 13000 6500 13000 6500 5656<br />
7 BUXAR 7 7000 3500 7000 3500 3046<br />
8 DARBHANGA 18 18000 9000 18000 9000 7832<br />
9 EAST CHAMPARAN 21 21000 10500 21000 10500 9137<br />
10 GAYA 24 24000 12000 24000 12000 10443<br />
11 GOPALGANJ 14 14000 7000 14000 7000 6092<br />
12 JAHANABAD 8 8000 4000 8000 4000 3481<br />
13 JAMUI 11 11000 5500 11000 5500 4786<br />
14 KAIMUR 11 11000 5500 11000 5500 4786<br />
15 KATIHAR 17 17000 8500 17000 8500 7397<br />
16 KHAGARIA 8 8000 4000 8000 4000 3481<br />
17 KISHANGANJ 8 8000 4000 8000 4000 3481<br />
18 LAKHISARAI 6 6000 3000 6000 3000 2611<br />
19 MADHUBANI 19 19000 9500 19000 9500 8267<br />
20 MUNGER 12 12000 6000 12000 6000 5221<br />
21 MUZAFFARPUR 15 15000 7500 15000 7500 6527<br />
22 NALANDA 23 23000 11500 23000 11500 10008<br />
23 NAWADA 15 15000 7500 15000 7500 6527<br />
24 PATNA 28 28000 14000 28000 14000 12183<br />
240
25 ROHTAS 19 19000 9500 19000 9500 8267<br />
26 SAMASTIPUR 15 15000 7500 15000 7500 6527<br />
27 SARAN 16 16000 8000 16000 8000 6962<br />
28 SEOHAR 5 5000 2500 5000 2500 2176<br />
29 SHEIKHPURA 7 7000 3500 7000 3500 3046<br />
30 SITAMARHI 14 14000 7000 14000 7000 6092<br />
31 SIWAN 16 16000 8000 16000 8000 6962<br />
32 VAISHALI 16 16000 8000 16000 8000 6962<br />
33 WEST CHAMPARAN 17 17000 8500 17000 8500 7397<br />
34 Supaul 13 13000 6500 13000 6500 5656<br />
35 Saharsa 11 11000 5500 11000 5500 4786<br />
36 Purnia 15 15000 7500 15000 7500 6527<br />
37 Madhepura 15 15000 7500 15000 7500 6527<br />
38 Araria 10 10000 5000 10000 5000 4351<br />
Total 524 524000 262000 524000 262000 228000<br />
Particulars Rate Total Amount in<br />
Rs.<br />
Sl No.<br />
1 Training Rs. 1000 / PHC 524000<br />
2 Awareness Generation Rs. 500 / PHC 262000<br />
3 Activities in School Rs. 1000 / PHC 524000<br />
4 IEC Material Rs. 400 / PHC 228000<br />
5 Activities in AWC & Communities Rs. 500 262000<br />
Grand Total 1800000<br />
Total Eighteen Lakh.<br />
241
PROJECT IMPLEMENTATION PLAN<br />
FOR<br />
NATIONAL PROGRAMME FOR<br />
CONTROL OF BLINDNESS<br />
2009 – 2010<br />
243
PROJECT IMPLEMENTATION PLAN<br />
FOR<br />
NATIONAL PROGRAMME FOR<br />
CONTROL OF BLINDNESS<br />
2009 – 2010<br />
244
Introduction<br />
National Programme for Control of Blindness (NPCB) was launched in the<br />
year 1976 as a 100% centrally sponsored scheme with the goal of reducing<br />
the prevalence of blindness. The goal set for the terminal year of the 10th<br />
Plan is to reduce the prevalence of blindness to 0.8% by 2007 prevalence of<br />
Blindness is 1% (2006-07 Survey) and 0.3% of population by 2020.<br />
The four pronged strategy of the programme is:<br />
strengthening service delivery,<br />
developing human resources for eye care,<br />
promoting outreach activities and public awareness and<br />
developing institutional capacity.<br />
NATIONAL POLICY :<br />
One of the basic human right is ‘THE RIGHT TO SIGHT’ we<br />
have to ensure that no citizen goes blind needlessly, or bring<br />
blind does not remain so, if by reasonable skill and resources<br />
his sight can be prevented from deteriorating, of if already lost<br />
can be restored.<br />
245
National Programme for Control of Blindness<br />
(Financial Year 2009-2010)<br />
There are two main Programmes under National Programme<br />
for Control of Blindness:<br />
(1) Cataract Operation<br />
(2) School Eye Screenings Programme:<br />
Cataract Operation:- Cataract Operations are being done in<br />
district Hospitals against the target fixed by state. In addition<br />
in the NGOs governed hospitals under the monitoring of<br />
District Health Society- Blindness Division.<br />
The following table shows the last six year’s physical<br />
record of Cataract Operation:-<br />
Sl. No. Year Target Achievement Percentage<br />
1. 2003-04 140000 90405 64.58<br />
2. 2004-05 140000 102531 73.24<br />
3. 2005-06 140000 131860 94.19<br />
4. 2006-07 140000 129064 92.19<br />
5. 2007-08 140000 137685 98.35<br />
6. 2008-2009<br />
Till Feb,09<br />
150000 82106<br />
School Eye Screening Programme :- Teachers are being<br />
trained, to conduct eye screening of the school children and to<br />
advise for using proper spectacles by the needy children with<br />
defective eyes is one of the main activities of the Programme.<br />
In addition to this free distribution of spectacles among the<br />
families belonging to below Poverty Line (BPL) is also a major<br />
component of the activities.<br />
246
The following table shows the last four year’s physical<br />
record of SES :-<br />
Sl.<br />
No.<br />
Year<br />
No. of school children underwent<br />
Eye Screening<br />
1. 2005-06 2,97,278<br />
2. 2006-07 2,43,095<br />
3. 2007-08 284398<br />
4. 2008-2009<br />
up to June,08<br />
55387<br />
Review Meeting: - A Two days Review Meeting of Additional<br />
Chief Medical Officer who is also the District Programme Officer<br />
of National Programme for Control of Blindness is proposed in<br />
near feature in which representative of Govt. of India shall also<br />
be requested to attend.<br />
<strong>State</strong> Level Workshop:- Three days <strong>State</strong> Level Workshop of<br />
Eye specialist/Eye surgeon of district level is also proposed in<br />
which representative of Govt. of India shall also be invited to<br />
attend.<br />
Vision Centre:- In remote rural areas where there is no facility<br />
of eye care , Govt. of India has provision for setting up vision<br />
centre<br />
made available.<br />
by the NGOs where all facilities for eye care shall be<br />
Training :- Under the NPCB training to Medical Officer of PHC,<br />
PMOAs and Nurses shall be imparted. Medical Officers shall be<br />
trained for three days, PMOAs for five days and<br />
training to the Nurses as per Govt. of India guideline.<br />
28 days<br />
IEC:- In order to make aware the people about how to take care<br />
of their eyes to acquaint them where to report for eye check up<br />
247
in case of any vision problem through hand bill, pump let,<br />
poster, banner, cable net work, hoarding and Doordarshan etc.<br />
Causes of Blindness in Bihar <strong>State</strong> :<br />
Following is the table showing the causes of blindness<br />
according to their magnitude of importance in the overall<br />
situation of blindness problem.<br />
F Cataract<br />
F Refractive Errors<br />
F Corneal Blindness<br />
F Glaucoma<br />
F Surgical Complications<br />
F Posterior segment disorders<br />
F Others<br />
Emerging Causes of Blindness :<br />
F Diabetic retinopathy<br />
F Glaucoma<br />
F Childhood blindness<br />
248
Comparison of Prevalence of Blindness National Surveys<br />
Parameter<br />
Estd. Prevalence of<br />
Blindness<br />
(Visual Acuity
Plan of action and Budgetary requirements during 2009-2010<br />
Sl. No. Name of Activity Estimated Cost.<br />
(Rupees in<br />
Lakhs)<br />
1. Remuneration, other activities & contingencies (Annex-A) 15.00<br />
2. Grant-in-Aid other Components-) 473.75<br />
3. Cash Grant for Salaries & SOC 30.00<br />
TOTAL:- 518.75<br />
Budgetary requirement during 2009-2010<br />
Annexure-A<br />
Sl.No. Particulars Cost p.a.<br />
1. Review Meeting 80,000<br />
2. Flexi pool fund (for staff remuneration & other ) 10,80,000<br />
3. TA/DA for Staff 96,000<br />
4. POL/Vehicle Maintenance 72,000<br />
5. Stationary and Consumables 52,000<br />
6. <strong>State</strong> level Workshop 120,000<br />
Total 15,00,000<br />
Annexure-B<br />
Grant in Aid other components-<br />
1. Recurring GIA for Eye Donation 150,000<br />
2. Vision Centre ( 50 @ 25,000/- per vision centres ) 625,000<br />
3. Eye Bank 5,00,000<br />
4. Eye Donation Centre 1,00,000<br />
5. Training 5,00,000<br />
6. IEC ( Schedule A) 5,00,000<br />
7. GIA for free Cataract Operation for 38/ DHS-Blindness<br />
4,40,00,000<br />
Division<br />
8. GIA for School Eye Screening for 38 DHS- Blindness Division 10,00,000<br />
Total:- 4,73,75,000<br />
250
Schedule :- 1<br />
IEC CAMPAIGN: PROPOSED BUDGET FOR IEC ACTIVITES DURING 2009-2010<br />
Sl.No. IEC Materials Tentative Quantity Rate<br />
(approx)<br />
Estimated<br />
Cost (Rs.)<br />
1. Hand Bill (For Eye) 1 Lakh 0.25/- piece 25,000<br />
2. Hand Bill (For Children)1 Lakh 0.25/- piece 25,000<br />
3. Leaflet 50 thousand 0.50/- piece 25,000<br />
4. Poster 40 thousand 1.25/- piece 50,000<br />
5. Banner 1000 (Five thousand) (38 District 80/- piece 80,000<br />
& Head Quarter)<br />
6. Cable Head Quarter 3500/- 61,000<br />
7. Hoarding (38 District & Head Quarter 39 6000/- 2,34,000<br />
TOTAL 5,00,,000.00<br />
251
Sl.<br />
No.<br />
Plan of Action and Budgetary requirements during 2009-2010<br />
Recurring Grants in Aid to NGOs for performing free Cataract<br />
Operation and other Intra Ocular Surgeries.<br />
Name of Dist. Target Total fund allocated by<br />
GOI for Cataract Operation<br />
for 38 DHS-Blindness<br />
Division during 2009-2010<br />
(Rs. in lacs)<br />
Total fund allocated by GOI<br />
for School Screening<br />
Programme for 38 DHS-<br />
Blindness Division during<br />
2009-2010 (Rs. in lacs)<br />
Remarks<br />
Fund directly<br />
allocated by GOI<br />
for DHS<br />
1. Araria 2000 - Do -<br />
2. Arwal 500 - Do -<br />
3. Aurangabad 3000 - Do -<br />
4. Banka 1500 - Do -<br />
5. Begusarai 4000 - Do -<br />
6. Bhagalpur 6000 - Do -<br />
7. Bhojpur 6000 - Do -<br />
8. Buxar 3000 - Do -<br />
9. Darbhanga 6000 - Do -<br />
10. E.Champn. 2500 - Do -<br />
11. Gaya 23000 - Do -<br />
12. Gopalganj 2000 - Do -<br />
13. Jamui 1500 - Do -<br />
14. Jehanabad 2000 - Do -<br />
15. Kaimur 2000 - Do -<br />
16. Katihar 4000 - Do -<br />
17. Khagaria 1500 - Do -<br />
18. Kishanganj 2000 - Do -<br />
19. Lakhisarai 1000 - Do -<br />
20. Madhepura 1000 - Do -<br />
21. Madhubani 1500 - Do -<br />
22. Munger 2000 - Do -<br />
23. Muzaffarpur 11000 - Do -<br />
24. Nalanda 11000 - Do -<br />
25. Nawada 3000 - Do -<br />
26. Patna 22000 - Do -<br />
27. Purnia 4000 - Do -<br />
28. Rohtas 2000 - Do -<br />
29. Saharsa 2000 - Do -<br />
30. Samastipur 2000 - Do -<br />
31. Saran 3000 - Do -<br />
32. Sheikhpura 500 - Do -<br />
33. Sheohar 500 - Do -<br />
34. Sitamarhi 1000 - Do -<br />
35. Siwan 2500 - Do -<br />
36. Supaul 1000 - Do -<br />
37. Vaishali 3500 - Do -<br />
38. W.Chamn. 3000 - Do -<br />
Total 150000 -<br />
252
Recurring Grants in Aid to NGOs for performing free Cataract Operation and other Intra Ocular Surgeries.<br />
Sl.N Name of Target ICCE @500/- ECCE/IOL@ 750/- Phaco<br />
Total<br />
o. Dist.<br />
(20%)<br />
(80%)<br />
1. Araria 2000 200,000.00 1,200,000.00 - 1,400,000.00<br />
2. Arwal 500 50,000.00 300,000.00 - 350,000.00<br />
3. Aurangabad 3000 300,000.00 1,800,000.00 - 2,100,000.00<br />
4. Banka 1500 150,000.00 900,000.00 - 1,050,000.00<br />
5. Begusarai 4000 400,000.00 2,400,000.00 - 2,800,000.00<br />
6. Bhagalpur 6000 600,000.00 3,600,000.00 - 4,200,000.00<br />
7. Bhojpur 6000 600,000.00 3,600,000.00 - 4,200,000.00<br />
8. Buxar 3000 300,000.00 1,800,000.00 - 2,100,000.00<br />
9. Darbhanga 6000 600,000.00 3,600,000.00 - 4,200,000.00<br />
10. E.Champn. 2500 250,000.00 1,500,000.00 - 1,750,000.00<br />
11. Gaya 23000 2,300,000.00 13,800,000.00 - 16,100,000.00<br />
12. Gopalganj 2000 200,000.00 1,200,000.00 - 1,400,000.00<br />
13. Jamui 1500 150,000.00 900,000.00 - 1,050,000.00<br />
14. Jehanabad 2000 200,000.00 1,200,000.00 - 1,400,000.00<br />
15. Kaimur 2000 200,000.00 1,200,000.00 - 1,400,000.00<br />
16. Katihar 4000 400,000.00 2,400,000.00 - 2,800,000.00<br />
17. Khagaria 1500 150,000.00 900,000.00 - 1,050,000.00<br />
18. Kishanganj 2000 200,000.00 1,200,000.00 - 1,400,000.00<br />
19. Lakhisarai 1000 100,000.00 600,000.00 - 700,000.00<br />
20. Madhepura 1000 100,000.00 600,000.00 - 700,000.00<br />
21. Madhubani 1500 150,000.00 900,000.00 - 1,050,000.00<br />
22. Munger 2000 200,000.00 1,200,000.00 - 1,400,000.00<br />
23. Muzaffarpur 11000 1,100,000.00 6,600,000.00 - 7,700,000.00<br />
24. Nalanda 11000 1,100,000.00 6,600,000.00 - 7,700,000.00<br />
25. Nawada 3000 300,000.00 1,800,000.00 - 2,100,000.00<br />
26. Patna 22000 2,200,000.00 13,200,000.00 - 15,400,000.00<br />
27. Purnia 4000 400,000.00 2,400,000.00 - 2,800,000.00<br />
28. Rohtas 2000 200,000.00 1,200,000.00 - 1,400,000.00<br />
29. Saharsa 2000 200,000.00 1,200,000.00 - 1,400,000.00<br />
30. Samastipur 2000 200,000.00 1,200,000.00 - 1,400,000.00<br />
31. Saran 3000 300,000.00 1,800,000.00 - 2,100,000.00<br />
32. Sheikhpura 500 50,000.00 300,000.00 - 350,000.00<br />
33. Sheohar 500 50,000.00 300,000.00 - 350,000.00<br />
34. Sitamarhi 1000 100,000.00 600,000.00 - 700,000.00<br />
35. Siwan 2500 250,000.00 1,500,000.00 - 1,750,000.00<br />
36. Supaul 1000 100,000.00 600,000.00 - 700,000.00<br />
37. Vaishali 3500 350,000.00 2,100,000.00 - 2,450,000.00<br />
38. W.Chamn. 3000 300,000.00 1,800,000.00 - 2,100,000.00<br />
Total 150000 15,000,000.00 90,000,000.00 - 105,000,000.00<br />
253
(Details of GIA for strengthening /expansion of eye care units in NGOs sector, Eye bank,<br />
eye donation Centres, IEC ,Training etc. under NPCB during 2008-2009.<br />
Sl.no<br />
Grant in Aid for various<br />
schemes.<br />
Balance<br />
available<br />
as on<br />
1.4.2008<br />
Fund received<br />
from GOI<br />
during 2008-09<br />
fund utilised/<br />
disbursed<br />
Balance<br />
as on<br />
31.12.2008<br />
-<br />
1<br />
Cataract Operation (for DBCS)<br />
- 7,000,000.00 7,000,000.00 -<br />
2 School Eye Screening 28,000.00 1,000,000.00 - 1,028,000.00<br />
3 Eye Donation 100,000.00 250,000.00 - 350,000.00<br />
4 Vision Centre - 563,000.00 - 563,000.00<br />
5 Eye Banks - - -<br />
6 Eye Donation Centres 150,000.00 - - 150,000.00<br />
7 Training 222,736.00 250,000.00 - 472,736.00<br />
8 IEC Activities 184,631.00 450,000.00 - 634,631.00<br />
9 SBCS remuneration and other activities (108,620.35) 800,000.00 132,166.00 559,213.65<br />
10 Cash Grant - - -<br />
11 Non recurring GIA to NGOs - - -<br />
Total:- 576,746.65 10,313,000.00 7,132,166.00 3,757,580.65<br />
Note:- Grant in aid of central assistance received from GOI,MH& FW, New Delhi vide letter no. T.12012/11/2006-BC<br />
dated 18.3.2008 for implementation of the following various new scheme under NPCB during 2007-2008. Received in<br />
Financial year 2008-2009 through ECS dt. on 3.4.2008<br />
Name of Activities:<br />
254<br />
F/Y 2007-2008<br />
fund received on<br />
3.4.2008<br />
Fund<br />
received from<br />
GOI during<br />
F/Y 2008-<br />
2009<br />
Total fund received<br />
during<br />
the F/Y 2008-2009<br />
from<br />
GOI<br />
Cataract Operation (for DBCS)<br />
7000000 7000000<br />
School Eye Screening 500000 500000 1000000<br />
Recurring GIA for Eye donation 250000 0 250000<br />
Non recurring GIA for Vision Centre 563000 0 563000<br />
Training Activities 250000 0 250000<br />
IEC Activities 250000 200000 450000<br />
SBCS staff remuneration and other<br />
activities 500000 300000 800000<br />
Total: 2313000 8000000 10313000
Sl.No<br />
a)<br />
Details of GIA for Procurement of Ophthalmic Equipments under NPCB during 2008-2009<br />
Grant in Aid for<br />
various Schemes<br />
1 Procurement<br />
for Ophthalmic<br />
equipments (DBCS)<br />
2 Medical Colleges:_<br />
Balance<br />
available<br />
as on<br />
1.4.2008<br />
Budget<br />
Allocated<br />
GIA<br />
released by<br />
GOI<br />
Expenditure/<br />
Disbursed<br />
7,991,500.00 - - -<br />
Balance<br />
as on<br />
31.12.2008<br />
0<br />
7,991,500.00<br />
S.K. Medical<br />
College & Hospital,<br />
Muzaffarpur - 3,000,000.00 3,000,000.00 - 3,000,000.00<br />
Total:- 7,991,500.00 3,000,000.00 3,000,000.00 - 10,991,500.00<br />
255
Schedule :- 2<br />
Fund allocated to DHS as per <strong>PIP</strong> allocation during the financial year 2009-2010<br />
Sl.No. Name of<br />
District<br />
Year Target GIA for<br />
free cataract<br />
operation for<br />
38 DHS<br />
of Rs.<br />
4,40,00,000<br />
GIA for<br />
School Eye<br />
Screening<br />
for 38 DHS<br />
of Rs.<br />
10,00,000<br />
Fund allocated<br />
to DHS as per<br />
<strong>PIP</strong> allocation<br />
Total Rs.4,50,00,000<br />
1 Araria 2009-2010 2000 600,000.00<br />
2 Arwal 2009-2010 500 150,000.00<br />
3 Aurangabad 2009-2010 3000 900,000.00<br />
4 Banka 2009-2010 1500 450,000.00<br />
5 Begusarai 2009-2010 4000 1,200,000.00<br />
6 Bhagalpur 2009-2010 6000 1,800,000.00<br />
7 Bhojpur 2009-2010 6000 1,800,000.00<br />
8 Buxar 2009-2010 3000 900,000.00<br />
9 Darbhanga 2009-2010 6000 1,800,000.00<br />
10 E.Champn. 2009-2010 2500 750,000.00<br />
11 Gaya 2009-2010 25000 7,500,000.00<br />
12 Gopalganj 2009-2010 2000 600,000.00<br />
13 Jamui 2009-2010 1500 450,000.00<br />
14 Jehanabad 2009-2010 2000 600,000.00<br />
15 Kaimur 2009-2010 2000 600,000.00<br />
16 Katihar 2009-2010 4000 1,200,000.00<br />
17 Khagaria 2009-2010 1500 450,000.00<br />
18 Kishanganj 2009-2010 2000 600,000.00<br />
19 Lakhisarai 2009-2010 1000 300,000.00<br />
20 Madhepura 2009-2010 1000 300,000.00<br />
21 Madhubani 2009-2010 1000 300,000.00<br />
22 Munger 2009-2010 2000 600,000.00<br />
23 Muzaffarpur 2009-2010 11000 3,300,000.00<br />
24 Nalanda 2009-2010 11000 3,300,000.00<br />
25 Nawada 2009-2010 3000 900,000.00<br />
26 Patna 2009-2010 22000 6,600,000.00<br />
27 Purnia 2009-2010 4000 1,200,000.00<br />
28 Rohtas 2009-2010 2000 600,000.00<br />
29 Saharsa 2009-2010 2000 600,000.00<br />
30 Samastipur 2009-2010 2000 600,000.00<br />
31 Saran 2009-2010 3000 900,000.00<br />
32 Sheikhpura 2009-2010 500 150,000.00<br />
33 Sheohar 2009-2010 500 150,000.00<br />
34 Sitamarhi 2009-2010 1000 300,000.00<br />
35 Siwan 2009-2010 2500 750,000.00<br />
36 Supaul 2009-2010 1000 300,000.00<br />
37 Viashali 2009-2010 3000 900,000.00<br />
38 W.Chamn. 2009-2010 2000 600,000.00<br />
Total 150000 45,000,000.00<br />
( Rupees four Crore fifty lac(s) only.)<br />
256
Sl.<br />
No.<br />
Budget summary for Year 2009-2010<br />
Name of activities DHS (Blindnes )<br />
SHSB<br />
(Blindness)<br />
Remarks<br />
1<br />
2<br />
3<br />
4<br />
5<br />
6<br />
7<br />
8<br />
9<br />
10<br />
Remuneration,other<br />
activities & contingencies ( Annex.-A) - 1,500,000.00 SHSB,level<br />
Recurring GIA for Eye donation - 150,000.00<br />
Vision Centre - 625,000.00<br />
Eye Bank - 500,000.00<br />
Eye Donation Centre - 100,000.00<br />
Disbursement<br />
of fund to DHS<br />
after approval .<br />
Training 500,000.00 SHSB,level<br />
IEC 500,000.00 SHSB,level<br />
Fund<br />
GIA for Cataract Operation 44,000,000.00<br />
disbursement<br />
to DHS<br />
GIA for SES 1,000,000.00<br />
after approval .<br />
Cash grant for salaries & SOC 3,000,000.00 SHSB, level<br />
Total:- 45,000,000.00 6,875,000.00 51,875,000.00<br />
257
ACTION PLAN<br />
(2009 – 2010)<br />
National Leprosy Eradication<br />
Programme<br />
(NLEP) – <strong>BIHAR</strong><br />
258
Executive Summary:<br />
National Leprosy Eradication Programme<br />
(11 th five Year Plan 2007 – 2012)<br />
<strong>State</strong> Action Plan 2009 – 2010<br />
<strong>BIHAR</strong><br />
· Even though new case detection rate and prevalence rate are going<br />
down, yet new cases continue to come up in large numbers in<br />
state.<br />
· The promotion of self reporting is now crucial to case detection, as<br />
case finding campaigns become less and less cost effective. It is<br />
important to identify and remove barriers that may prevent new cases<br />
coming forward and a greater emphasis on the assessment of disability<br />
at diagnosis, so that those at particular can be recognized and<br />
managed appropriately.<br />
· Leprosy being a disease associated with poverty, it is presumed there<br />
are still hidden cases in the SC and among the underprivileged in<br />
other categories, in both rural and urban areas.<br />
· Under special initiatives, to promote self reporting, focus will be on<br />
wide dissemination of key messages of leprosy i.e. curable, early<br />
signs, no need to be feared and support, in the urban and rural areas.<br />
This will reduce stigma & discrimination against persons affected<br />
with leprosy. The key messages along with proactive involvement of<br />
the community will bring about health behavior at individual,<br />
household and community level.<br />
· The out come of strategy will be promote further integration with<br />
general health care system by providing operational and technical on<br />
the job training. The better equipped and motivated GHC system will<br />
provide quality leprosy services on all working days to the affected<br />
communities, following the principles of equity and social justice.<br />
259
Background:<br />
· National Leprosy Control Programme was started by Govt. of India in<br />
1955 based on Dapsone Monotherapy through units implementing<br />
survey, education and treatment activities. It was only in 1970s that a<br />
definite cure was identified in the form of Multi Drug Therapy. The<br />
MDT came into wide use from 1982, following the recommendation<br />
by WHO study Group, Geneva in October 1981. Government of India<br />
established a high power committee under chairmanship of Dr. M. S.<br />
Swaminathan in 1981 for dealing with the problem of leprosy. Based<br />
on its recommendations the National Leprosy Eradication Programme<br />
(NLEP) was launched in 1983 with objective to arrest the disease<br />
activities in all the known cases of leprosy.<br />
· In order to strengthen the process of eradication, the World Bank<br />
supported the project in two phases. The first phase was started in<br />
1993 94 and ended on 31st March 2000. The second phase started in<br />
year 2001 2002 and ended on 31 st December 2004. Now since 2005<br />
the project is being continued with GOI funds. The cost of<br />
infrastructure is borne by the state funds. Additional support is<br />
received from World Health Organisation and ILEP (International<br />
Federation of Anti-Leprosy Associations). Multi Drug Therapy<br />
(MDT) was supplied free of cost by Novartis through WHO.<br />
· In Bihar whole state was covered under MDT in November 1996.<br />
· In Bihar till date more than 15 lakhs patients treated with leprosy.<br />
· The PR reduced to 14.2/10000 populations in year 1999.<br />
· Integration of leprosy services in to general health care system started<br />
in 2000 01 and fully integrated in 2003 -04.<br />
· Five rounds of Modified Leprosy Elimination Campaigns (MLECs)<br />
and four rounds of Block Level Awareness campaigns have been<br />
already successfully conducted in the state during the period 1998 to<br />
2008. These activities resulted in detection of more than 4 lakh cases.<br />
260
MDT in Bihar:<br />
· MDT started in Bihar in phased manner.<br />
· In composite state of Bihar, first phase MDT was started in two<br />
districts in 1982 (Bhagalpur & Rohtas).<br />
· 13 more districts added in 1994.<br />
· MDT was launched in whole state in 1996 97.<br />
Current status:<br />
· From 1996 97 onwards when entire state was brought under MDT, a<br />
steady decline in PR was recorded. The PR of 17.3/10000 populations<br />
in 1996-97 declined to 1.04/10000 populations on 31 st March 2008.<br />
· Now state is at the verge of elimination considering PR 1.04/10000<br />
populations on March 2008.<br />
· 15 districts reached elimination and 23 districts have PR between 1 to<br />
2 as on 31 st March 2008.<br />
· At present the NLEP is fully integrated into General Health Care<br />
System from subcentre to District Hospitals/Medical Colleges.<br />
· District Nucleus is formed at 36 out of 38 districts to monitor and<br />
supervise the programme.<br />
· The IEC activities including Inter Personal Communication are<br />
continued and therefore stigma has significantly come down. At<br />
present most of leprosy affected deformed patients are living with<br />
their family and leprosy patients are coming at health institutions<br />
voluntarily.<br />
261
<strong>STATE</strong> PROFILE<br />
Bihar is the third largest populated state in the country. There are 38<br />
districts in the state. Bihar is divided in two geographical areas- North<br />
and south areas<br />
POPULATION (2001 census)*<br />
*Estimated Population as on March<br />
2008<br />
829988509<br />
98516843<br />
MALES 43243795<br />
FEMALES 39754714<br />
SEX RATIO (females/1000 males) 921<br />
DENSITY OF POPULATION (Persons/<br />
Square Km)<br />
880<br />
URBAN POPULATION % 10.47<br />
LITERACY RATE (census 2001) in % 47<br />
MALE LITERACY in % 59.7<br />
MALE LITERATE in numbers 20644376<br />
FEMALE LITERACY in % 33.1<br />
FEMALE LITERATE in numbers 10465201<br />
BIRTH RATE (PER 1000) 30.9<br />
DEATH RATE (PER 1000) 7.9<br />
District Hospital 24<br />
Sub- Divisional Hospital 23<br />
Referral Hospital 71<br />
Primary Health Centre (PHCs) 484<br />
Additional Primary Health Centre<br />
(APHCs)<br />
1243<br />
Health Sub-Centre 8858<br />
No. of Villages 45100<br />
262
Situational Analysis – As on September 2008/ Districts/Blocks/Urbans<br />
Indicators recommended by GOI for Monitoring & Supervision:<br />
The Government of India has recommended the following three indicators:-<br />
(I) Major indicators:<br />
(1) Annual New Case Detection Rate(ANCDR) per 100000 population<br />
(2) Treatment Completion Rate<br />
(3) Prevalence Rate<br />
(II) Additional Indicators:<br />
(1) Proportions of Grade I disability among new cases<br />
(2) Proportions of Grade II disability among new cases<br />
(3) Proportions of child cases among new cases<br />
(4) Proportions of female cases among new cases<br />
(5) Proportions of MB cases among new cases<br />
(III) Indicators for patient management and follow up:<br />
(1) The proportion of new cases correctly diagnosed<br />
(2) The proportion of treatment defaulters<br />
(3) Number of relapse reported during year<br />
(4) The proportion of patients who develop new or additional disabilities<br />
during MDT.<br />
263
Shift in focus from PR to ANCDR:<br />
Since 2008-09 a shift in focus from PR to ANCDR was introduced, as it is a<br />
better indicator for epidemiological analysis.<br />
Sl. No.<br />
District<br />
Active<br />
Balance<br />
case at the<br />
end of<br />
September<br />
2008<br />
PD<br />
Ratio<br />
Female<br />
(%)<br />
New Visible<br />
Deformity<br />
(%) Grade<br />
II<br />
Child % MB %<br />
PR/<br />
10,000<br />
NCDR per<br />
100,000<br />
1 Aurangabad 294 0.60 29.26 1.85 15.93 34.07 1.23 20.4<br />
2 Bhojpur 239 0.51 32.57 3.21 22.02 33.94 0.90 13.7<br />
3 Buxar 168 0.61 29.68 0.65 15.48 41.29 1.01 17.5<br />
4 Bhagalpur 396 0.89 34.84 3.97 15.86 38.53 1.37 12.2<br />
5 Banka 339 0.6 35.60 0.00 0.31 35.60 1.77 26.9<br />
6 Darbhanga 474 0.7 46.87 0.25 21.55 45.11 1.21 17.3<br />
7 Katihar 288 0.78 39.92 2.52 14.29 39.08 1.01 12.9<br />
8 Muzaffarpur 522 0.58 49.71 2.16 14.93 29.47 1.17 20.2<br />
9 Nawadah 378 0.56 42.12 2.99 17.66 32.88 1.76 23.3<br />
10 Patna 702 0.55 30.88 2.28 17.19 51.23 1.25 25.8<br />
11 Purnia 344 0.59 39.93 2.83 15.90 33.92 1.14 18.6<br />
12 Kishanganj 285 0.56 31.1 00 19.79 47.00 1.85 29.9<br />
13 Araria 466 0.64 33.49 1.19 17.10 23.28 1.84 29.2<br />
14 Rohtas 778 0.6 32.33 2.09 27.09 32.33 2.67 42.08<br />
15 Kaimur 425 0.41 30.00 0.00 15.48 45.81 2.78 26.2<br />
16 Siwan 520 0.47 43.43 3.43 18.79 25.66 1.61 22.3<br />
17 Sitamarhi 352 0.5 44.19 1.45 20.35 25.00 1.11 16.8<br />
18 Sheohar 101 0.70 29.09 0.00 12.73 40.00 1.65 20.3<br />
19 W.Champaran 371 0.6 24.24 3.33 19.39 33.33 1.03 17.2<br />
20 Begusarai 287 0.53 34.47 4.17 11.74 42.05 1.03 13.7<br />
21 E.Champaran 547 0.5 36.56 0.97 16.25 27.85 1.17 26.0<br />
22 Gaya 730 0.55 40.06 1.02 21.93 31.43 1.77 25.1<br />
23 Gopalganj 348 0.52 44.02 0.58 21.28 28.28 1.36 18.6<br />
24 Jehanabad 269 0.5 37.85 5.58 17.53 45.02 2.44 31.0<br />
25 Arwal 153 0.49 35.71 1.43 21.43 40.71 2.20 33.8<br />
26 Khagaria 120 0.78 33.33 0.00 7.78 45.56 0.79 10<br />
27 Madhubani 768 0.55 44.34 2.41 16.14 42.23 1.81 22.05<br />
28 Madhepura 226 0.56 45.86 3.01 11.28 48.12 1.25 17.2<br />
29 Munger 203 0.68 45.63 4.38 16.88 33.75 1.50 22.5<br />
264
30 Sheikhpura 88 0.61 36.90 00 14.29 47.62 1.41 21.6<br />
31 Jamui 175 0.66 31.29 0.00 12.93 41.50 1.05 18.9<br />
32 Lakhisarai 187 0.72 33.92 0.00 16.37 46.78 1.96 20.4<br />
33 Nalanda 474 0.6 39.60 0.66 21.24 38.72 1.68 26.2<br />
34 Saharsa 171 0.59 46.81 4.26 17.02 34.75 0.95 15.9<br />
35 Supaul 197 0.5 39.64 1.18 9.47 35.50 0.95 17.8<br />
36 Samastipur 433 0.61 36.90 4.79 14.08 39.44 1.07 15.7<br />
37 Saran 524 0.43 29.10 1.23 15.98 44.88 1.36 26.2<br />
38 Vaishali 422 0.68 39.72 1.99 8.28 49.34 1.31 17.2<br />
Total 13764 0.54 37.52 1.96 17.64 36.98 1.40 20.9<br />
ANCDR: (20.9/100000)<br />
ANCDR(quarterly) of 21 districts is > 20/100000 of population. These<br />
districts are Aurangabad, Banka, Muzaffarpur, Nawada, Patna, Kishanganj,<br />
Araria, Rohatas, Kaimur, Siwan, Seohar, East Champaran, Gaya, jahanabad,<br />
Arawal, Madhubani, Munger, Sheikhpura, Lakhisarai, Nalanda and Saran.<br />
Therefore overall ANCDR of state is also > 20/100000 population<br />
265
Treatment Completion Rate- (2007-08):<br />
S.N. Districts Treatment Completion Rate(%)<br />
Rural(%) Urban(%) Total(%)<br />
1. Patna 98.9 88.6 94.8<br />
2 Bhojpur 96.2 100 96.6<br />
3 Buxar 94.9 97.2 95.1<br />
4 Aurangabad 98.9 100 98.9<br />
5 Arawal 92.9 No urban 92.9<br />
6 Gaya 96.5 93.7 96.3<br />
7 Nalanda 97.3 98.7 97.4<br />
8 Nawada 94.3 00 94.2<br />
9 Rohtas 97.4 97.9 97.4<br />
10 Vaishali 87.2 47.3 83.5<br />
11 Bhagalpur 97.7 73.08 95.3<br />
12 Banka 95.6 92.7 95.5<br />
13 Khagaria 94.08 100 94.2<br />
14 Muzaffarpur 93.5 98.08 93.8<br />
15 Samastipur 91.07 90.7 91.05<br />
16 East Champaran 95.02 100 95.06<br />
17 Sitamarhi 94.9 92.9 94.9<br />
18 Seohar 87.2 00 87.2<br />
19 Gopalganj 94.5 100 94.7<br />
20 Saran 88.5 67.3 86.06<br />
21 Araria 98.3 100 98.4<br />
22 Saharsa 95.7 88.0 94.9<br />
23 Supaul 100 100 100<br />
24 West Champaran 93.8 100 94.03<br />
25 Siwan 93.2 91.7 93.6<br />
<strong>State</strong> 94.7 87.4 94.03<br />
· TCR -2007-08 of Bihar state is more than 90% but in urban areas of few<br />
districts TCR is less than 90% and these districts are Patna, Bhagalpur,<br />
Saran, Saharasa. TCR of urban Vaishali is very less 47.3%.<br />
266
SWOT analysis:<br />
After analysis following are strengths, weaknesses, opportunities and threats<br />
in state.<br />
Strengths:<br />
1. trained district nucleus<br />
2. Trained experienced & motivated staff<br />
3. Better awareness and reduced stigma<br />
4. Adequacy of MDT<br />
5. Adequacy of fund form GOI and ILEP<br />
6. Better comprehensive infrastructure from subcentre to<br />
Medical college<br />
7. Integration of leprosy services with GHCs staff<br />
8. Training materials are available<br />
9. Regular NLEP staff meetings and monitoring<br />
10. Good coordination <strong>State</strong> Health System, WHO &<br />
ILEP<br />
11. Enough people willing to work for the cause.<br />
Weakness:<br />
1. Large state with many districts<br />
2. Reduction in ILEP support<br />
3. No WHO zonal coordinators<br />
4. Complicated procedures for fund utilization for leprosy<br />
work at district level<br />
5. Inadequacy of fund for vehicle operation and<br />
complicated procedure for hiring of vehicle<br />
6. Less support from public opinion leaders<br />
7. Poor POD services<br />
8. Leprosy being last priority of health programme<br />
9. Inadequate funds for rehabilitation and mobility aids<br />
10. Inadequate coordination between staff<br />
11. Vehicles Using in other programmes by DM and Civil<br />
Surgeons<br />
12. Inadequate training of NGOs/local practitioners<br />
13. incomplete data of deformities<br />
14. Less effective counseling<br />
267
Opportunities:<br />
1. Integration with NRHM<br />
(a) Support from ASHA<br />
(b) Additional flexible funds<br />
(c) Better monitoring and supervision<br />
(d) Better infrastructure and man power<br />
2. Integration with GHS<br />
3. Involvement of Medical Colleges/Hospitals/NGOs<br />
4. Full utilization of dermatologists, physicians and<br />
orthopaedic surgeons for diagnosis and rehabilitation<br />
5. Support of ILEP/NGOs/WHO<br />
Threats:<br />
1. Complacency among staff and less political commitment<br />
2. Priority to other programmes<br />
3. Transfer of programme officers at state and district<br />
4. Public stigma<br />
5. No self dependence of sufferer<br />
<strong>State</strong> will use this SWOT analysis for making strategies and plans in NLEP.<br />
National Leprosy Eradication Programme<br />
(11 th five year plan 2007 – 2012)<br />
Objectives:<br />
· To further reduce the leprosy burden<br />
· Provision of high quality leprosy services for all persons affected by<br />
leprosy, through general health care system including referral services for<br />
complications and chronic care.<br />
· Enhanced Disability prevention and Medical Rehabilitation (DPMR)<br />
services for deformity in leprosy affected persons.<br />
· Enhanced advocacy in order to reduce stigma and stop discrimination<br />
against leprosy affected persons and their families.<br />
268
· Capacity building among health service personal in integrated setting<br />
both for rural and urban areas.<br />
· Strengthen the monitoring and supervision component of the surveillance<br />
system.<br />
Strategy:<br />
(1) Integrated Leprosy Services and Special initiatives.<br />
(2) Disability Prevention and Medical Rehabilitation (DPMR)<br />
(3) Information, Education and Communication<br />
(4) Training and capacity building.<br />
(5) Supervision, monitoring and review.<br />
(6) Infrastructure maintenance<br />
Activities as per objectives and strategy:<br />
1. Integrated Leprosy Services and Special initiatives –<br />
1.1 Integrated Leprosy Services through all Primary Health Care facilities<br />
will continue to be provided in the rural areas.<br />
1.2 All the urban areas will be covered under urban leprosy control<br />
programme integrating services from all the partners available in the<br />
areas, including private practitioners.<br />
1.3 Involvement of multipurpose health functionaries, ASHA in villages,<br />
and selected NGOs in urban areas are to be engaged for case follow up<br />
during treatment to ensure regular MDT collection and consumption, so<br />
that all the cases put under treatment gets cured in shortest possible time.<br />
1.4 Emphasis will be laid on providing best quality leprosy services through<br />
the GHC system. This means easy availability of services on all working<br />
days to all patients, correct diagnosis and adequate counseling to patients<br />
269
and family members, provide MDT to patients whenever approached,<br />
regular monitoring of patient during treatment. Treatment completion by<br />
all under treatment patients will be desired outcome of the programme.<br />
1.5 The system of referral of difficult cases to the district hospital for<br />
diagnosis and management, which has already been started, will eb<br />
further strengthened with capacity building of persons involved at PHC<br />
as well district Hospital level.<br />
1.6 The laboratory facilities at District Hospitals for smear examination to<br />
diagnose difficult cases will be strengthened.<br />
1.7 Desegregated data for female, schedule tribe and schedule caste patients<br />
are to be maintained.<br />
1.8 Regular monitoring and surveillance at state, District and Block level<br />
will be continued to locate weak areas, so that needed plan for corrective<br />
action can be taken in time.<br />
Services through ASHA:<br />
After sensitization of ASHA in Leprosy they will be involved to refer a<br />
suspected case of leprosy from their villages for diagnosis at PHC and after<br />
diagnosis to follow up the patients for completion of their treatment, ASHA<br />
will be entitled to receive incentive as below-<br />
(i) On confirmed diagnosis of cases brought by them Rs 100/-<br />
(ii) On completion of full course of treatment within specified<br />
time <br />
PB Leprosy case Rs. 200/-<br />
MB Leprosy case Rs. 400/-<br />
Number of new leprosy cases detected cases in 2007-08 19041<br />
45% MB cases 8568<br />
55% PB cases 10473<br />
(It is expected that 50% of new MB and new PB cases will be brought by<br />
ASHA.<br />
50% of PB new cases = 5236<br />
50% of new MB cases = 4284)<br />
270
Budget:<br />
For MB cases = Rs.500.00*4284 cases<br />
= Rs. 2142000.00<br />
For PB cases = Rs. 300.00*5236<br />
= Rs. 1570800.00<br />
Total Cost of services through ASHA = Rs.3712800.00<br />
Urban Leprosy Control :<br />
· Total number of town ships selected for ULCP 24<br />
· Total number of medium city(I) selected for ULCP 6<br />
· Budget Rs.75000/- for one town ship x 24 = 1800000/-<br />
Rs.150000/- for one medium city(I) x 6 = Rs.900000/-<br />
Total cost of Urban Leprosy Control = 2700000/-<br />
2. Disability Prevention and Medical Rehabilitation -<br />
More emphasis will be given on Disability prevention among new leprosy<br />
cases and RCS services for deformed persons due to leprosy.<br />
2.1 Prevention of Disability:<br />
· Health workers will suspect cases of leprosy reaction, relapse, insensitive<br />
hands and feet and refer to PHC for diagnosis. They will also empower<br />
patients with self care procedure for prevention of deformity.<br />
· All PHC Medical Officers will diagnose cases of reaction/neuritis,<br />
provide counseling and treat them. Severe reaction/neuritis cases will be<br />
referred to the District Hospital if not responded within two weeks of<br />
starting treatment.<br />
· Service and care for impairment such as ulcers, cracks and wounds,<br />
septic hand or feet etc. will be available from all the health facilities<br />
routinely. Complicated ulcer cases will be referred to District Hospital.<br />
271
· Microcellular Rubber (MCR) footwear are to be provided to all needy<br />
patients ( under treatment and RFT) by the District nucleus staff at the<br />
concerned health facility. An appropriate system of need assessment,<br />
procurement and supply will be maintained and improved.<br />
· PHC will provide follow up treatment to all patients referred back by the<br />
secondary and tertiary level units for reaction, complication or post<br />
surgery care.<br />
· Operational guidelines on DPMR for primary and secondary level have<br />
been distributed to all districts and PHCs.<br />
2.2 Medical Rehabilitation:<br />
· Enlisting of disability cases has been completed in 24 districts and in<br />
remaining 14 districts enlisting is under process.<br />
· In districts the patients fit for RCS are being referred to identified RCS<br />
units(Department of PMR at PMCH, Patna and DMCH Darbhanga).<br />
· An estimated 200 RCS will be done during this year. Budget for RCS<br />
support and patient welfare for 200 patients is kept.<br />
· In addition to this TLM Hospital Muzaffarpur will continue to do RCS<br />
with ILEP support.<br />
· It is planned to start RCS in Magadh Medical college, Gaya in this year<br />
Incentive to patients undergoing RCS:<br />
· Provision to patients undergoing RCS @ Rs. 5000.00 to offset wage loss<br />
to BPL families as recommended by GoI. It is proposed that the above<br />
provision may be applied for for surgical Nerve Decompression also.<br />
Further it is suggested that leprosy is a disease associated with poverty,<br />
the provision of Rs. 5000.00 to offset wage loss may be given to all<br />
leprosy patients undergoing RCS/Nerve decompression surgery.<br />
Incentive to Institutions:<br />
· Provision to support Government Medical Colleges/PMR centres in the<br />
form of Rs. 5000.00 per RCS case has been kept for procurement of<br />
supply and material and other ancillary expenditure.<br />
272
Need based supply of MCR footwear to the needy patients will continue<br />
during year through District Societies, NGOs and concerned institutions.As<br />
grade I patients with insensitive feet have been included under DPMR plan<br />
for MCR supply the number of foot wear requirement will increase.<br />
Budget:<br />
(1) Provision to compensate wage loss to BPL persons affected with<br />
leprosy undergoing Reconstructive/Nerve Decompression surgery <br />
around 200 persons are expected to be operated. The reimbursement<br />
of Rs. 5000.00 is sought to be provided for <br />
Incentive @ Rs.100.00 per person*2*20 days = Rs. 4000.00<br />
Transportation for 2 persons(4-5 times) = Rs. 1000.00<br />
Total (one RCS) = Rs. 5000.00<br />
For 100 RCS- 5000.00*100<br />
= Rs.500000.00<br />
(2) Provision of incentive to Govt. institutions-<br />
For 100 RCS 5000.00*100 = Rs. 500000.00<br />
(3) MCR foot wear- 2280 pairs of MCR foot wears @ Rs.250.00<br />
2280*Rs.250.00 = Rs. 1938000.00<br />
Total cost of DPMR = 3413000.00<br />
3. Information, Education & Communication:<br />
Introduction –<br />
Leprosy is an age old disease. As there was no known remedy for the disease<br />
in the earlier days, the viciousness of disease, disfigurement and disability<br />
caused by the disease resulting in making the affected persons heavily, led to<br />
a number of myths, misconceptions, apprehensions and inhibitions in the<br />
minds of people. This resulted in to developing such a high degree of stigma<br />
against the disease that the community wanted to avoid all contacts with<br />
such persons. The leprosy affected persons were forced to leave their home<br />
273
and live in segregated areas. This is the only disease where sufferer had to<br />
live in separate colonies, villages and in distant islands.<br />
At present the situation has changed to a greater extent. Now there is<br />
cure for leprosy and patient can live in their home during treatment. Because<br />
of early treatment deformities and disabilities have reduced. Many<br />
discriminatory laws have been repealed all over the world. Yet there is<br />
discrimination against the person affected by leprosy, which need to be<br />
removed from the public mind, so that these persons can lead normal life<br />
like any other human being.<br />
Determinants of stigma:<br />
Stigma is perpetuated by (1) Lack of knowledge (2) Attitude (3) Fear (4)<br />
Blame & shame<br />
Intervention strategies:<br />
Spreading awareness: Spread the demystifying messages and its<br />
interpretations, mainly regarding nature of disease, whether leprosy cases are<br />
untouchable, role of immunity in occurrence of leprosy, what is burnt case<br />
and so on. However, mere information and education, to all and sundry<br />
about the signs and symptoms of leprosy and its curability, shall not work. It<br />
is imperative to break the barrier between persons affected by leprosy and<br />
the rest of the society, by appealing to the peoples emotions and their ability<br />
to empathies with those they feared and shunned.<br />
With reducing number of leprosy cases in community, awareness about<br />
curability of disease, lessening number of deformity due to leprosy, stigma<br />
associated with the disease has become slightly less. The effective way to<br />
deal with this difficult challenge of stigma removal is to embark on intensive<br />
inter personal communication (IPC) with the target groups<br />
The strategy involves, coordinates and facilitated by (1) civil societies (2)<br />
social activists (3) Health service providers (4) Community/opinion leaders<br />
(5) Corporate sectors (6) Media (7) Institutions under NRHM such as ASHA<br />
and other health functionaries, Rogi Kalyan Samities and Village Health &<br />
Sanitation Committees, Health Melas at district and block level etc.<br />
An IEC campaign towards achieving Leprosy free India recommended by<br />
GOI will be followed on following concept <br />
274
· The effort to further reducing leprosy burden in the communities have to<br />
be prioritized so that visible deformity in newly detected cases is reduced<br />
to minimum.<br />
· Early reporting and complete treatment of leprosy cases prevent<br />
disability.<br />
· Quality of services provided to leprosy affected persons be at optimum<br />
level to reduce suffering and prevent consequences in all cases put on<br />
treatment.<br />
· Leprosy patients will not be stigmatized and discriminated and would<br />
lead to a socially and economically productive life.<br />
Budget and norms for IEC:<br />
Mass media-<br />
Electronic Media Rs.200000.00<br />
Print media Rs.100000.00<br />
Out door media-<br />
Rallies(including banners) @ Rs.5000/- per district.<br />
Budget Rs.5000.00 x 38 districts<br />
= 190000/-<br />
Rural Media:<br />
School quiz @ Rs.500/- for one quiz.<br />
In each block 5 school quiz will be conducted.<br />
Budget Rs.500.00 x 484 blocks x 5<br />
= Rs.1210000/-<br />
Sensitisation meeting with PRI members-Rs.4000/- per meeting at<br />
each block<br />
Rs.4000/. * 484 blocks<br />
= 1936000/.<br />
Total cost of IEC = Rs.3826000/-<br />
275
4. Training Plan(training and capacity building):<br />
4.1 Leprosy training to GHC staff(new entrants)<br />
To improve quality of leprosy diagnosis, complications management, DPMR<br />
and programme monitoring the key medical and paramedical staffs will be<br />
provided trainings.<br />
1400 newly appointed contractual MOs will be provided four days modular<br />
training on leprosy and NLEP(including DPMR).<br />
Budget <br />
Venue District head quarter training hall.<br />
Trainers(2trainers) TA/DA @ Rs.300/- per day for two days<br />
Rs.300.00 x 2 days x 2 trainers = Rs.1200/-<br />
TA for trainees @ Rs.80/- per day for 30 trainees for 2 days<br />
Rs.80.00 x 30 trainees x 2 days = Rs.4800/-<br />
DA for trainees @ Rs.80/- per day for 30 trainees for 2 days.<br />
Rs.80.00 x 30 trainees x 2 days = Rs.4800/-<br />
Working lunch & tea @ Rs.150/- for 35 persons for 2 days<br />
Rs150.00 x 2 days x 35 = Rs.10500/-<br />
Learning materials, stationary etc @ Rs.250/- per head for 30 trainees.<br />
Rs.250.00 x 30 = 7500/-<br />
Miscellaneous Rs.2500/- per batch.<br />
Total expenditure for 2 days training of new MOs for one batch<br />
= Rs.31300/-<br />
Total number of batches in all districts of Bihar 47<br />
Total Expenditure – Rs.31300.00 x 47 batches<br />
= Rs.1471100/-<br />
4.2 One days refresher training of PHC medical officers:<br />
Total number of regular MOs in position 2712<br />
Total number of batches 90(batches distributed districtwise)<br />
90 batches x Rs 27300.00<br />
Total expenditure =Rs. 2457000/-<br />
276
Consumables:<br />
· For SHS(leprosy) Rs.28000/- and for DHS(leprosy) Rs.14000/- per<br />
district will be provided.<br />
Office expenses:<br />
· For SHS(leprosy) Rs.38000/- and for DHS(leprosy) Rs.18000/- per<br />
district will be provided.<br />
Vehicle Operation & Hiring:<br />
· Vehicle operation/POL/Hiring for SHS(leprosy) Rs.85000/- for two<br />
vehicles and for DHS(leprosy) Rs.75000/- one vehicle for one district<br />
will be kept.<br />
Drugs, Materials & supplies:<br />
· For supportive medicine Rs.25000/- per district.<br />
· For laboratory reagents- Rs.12000/- per year per district.<br />
· For patient welfare Rs.6000/- per year per district.<br />
Printing:<br />
· Required numbers of DPMR registers, formats and other formats will be<br />
printed at state head quarter and supplied to districts.<br />
(<strong>State</strong> Officers and WHO/ILEP Coordinators will also monitor the supply<br />
of different logistics at each level)<br />
Professional Services:<br />
· Audit fees will be met by <strong>State</strong> Health & FW Society for centralized<br />
audit of 38 DLS & SLS head quarter for preparation of consolidation<br />
Audit Report.<br />
277
Contractual Services:<br />
· As per annexure 1<br />
NLEP Monitoring and Review:<br />
· Monitoring of:<br />
- NCDR,TCR,PR & other NLEP indicators<br />
- Regularity of treatment & timely RFT<br />
- Reports(MPR,MDT indents,Tour reports etc)<br />
- Implementation of DPMR trainings with support of ILEP, RCS &<br />
other referral & IEC activities.<br />
- On the job training on DPMR formats, modified SIS & MDT stock<br />
management up to subcentre level<br />
· DPMR/SIS/MDT management & monitoring of<br />
-MDT stock situation in patient month BCPs<br />
-MDT indenting<br />
-MDT supply<br />
-Availability of prednisolone at PHCs.<br />
· Review Meetings of DLOs and members of District nucleus four<br />
times in one year<br />
278
<strong>STATE</strong> <strong>HEALTH</strong> <strong>SOCIETY</strong> (Leprosy), <strong>BIHAR</strong><br />
Budget for Year 2009-2010<br />
Anexxure 1<br />
1<br />
Sl. No.<br />
1.1<br />
Category of Expenditure : Component & Sub<br />
Component wise<br />
Under SHS(Leprosy) NLEP contractual<br />
services(staff)<br />
40 Drivers for 38 districts & for <strong>State</strong> Leprosy Cell<br />
@Rs.4500/-PM<br />
DLS<br />
SHSB<br />
(Leprosy)<br />
2052000 108000.00<br />
Total of<br />
activities<br />
1.2 DEO at <strong>State</strong> Leprosy Cell @ Rs.8000/- 96000.00<br />
1.3<br />
Honorarium @ Rs.400/- PM for 38 DLS for account<br />
work of Leprosy<br />
182400<br />
1.6 Audit Fees @ Rs.6000/- x 39(38 DHS + 1 SHS -L) 228000.00 6000.00<br />
Total contratual services(1.1 to 1.6) 2462400.00 210000.00 2672400.00<br />
2 Office expences<br />
2.1<br />
2.2<br />
SHS(leprosy) for rent,telephone,electricity, P & T<br />
charges, miscellaneous-Rs.38000/- per year<br />
DLS(leprosy) for rent,telephone,electricity, P & T<br />
charges, miscellaneous-Rs.18000/- per district/ year<br />
684000.00<br />
38000.00<br />
Total - Office expences(2.1 to 2.2) 684000.00 38000.00 722000.00<br />
3 Consumables<br />
3.1<br />
3.2<br />
Consumables for DHS(leprosy) : Stationery etc.@ Rs.<br />
14000/- per dist/year<br />
Consumables for SHS(leprosy) : Stationery etc.@ Rs.<br />
28000/- per year<br />
532000.00<br />
28000.00<br />
Total - Consumables(3.1 to 3.2) 532000.00 28000.00 560000.00<br />
4 Vehicle operation/hiring & POL/ Maintenance<br />
4.1<br />
One vehicle for each DHS(leprosy)-Rs.75000.00 per<br />
vehicle/district<br />
2850000.00<br />
4.2 Two vehicles for SHS(Leprosy)-Rs.85000/- per vehicle 170000.00<br />
Total - Vehicle operation(4.1 to 4.2) 2850000.00 170000.00 3020000.00<br />
5 Drugs, materials & supplies<br />
5.1 Supportive medicines-Rs. 25000/-per district/year 950000.00<br />
279
5.2<br />
Laboratory reagents & equipments -Rs.12000/-per<br />
district/year<br />
456000.00<br />
5.3 Patient welfare-Rs.6000/- per district/year 228000.00<br />
5.4 Printing of forms/DPMR registers etc 600000.00<br />
Total - Drugs,materials & supplies(5.1 to 5.4) 1634000.00 600000.00 2234000.00<br />
6 IEC<br />
6.1 Mass media:<br />
6.11 Electronic media-Radio/Doordarshan 500000.00<br />
6.12 Print media-News papers 200000.00<br />
6.2 Out door media:<br />
6.21<br />
Sensitisation meeting with PRI members-Rs.4000/- per<br />
meeting at each block<br />
1936000.00<br />
6.3 Rural media:<br />
6.31<br />
6.32<br />
School quiz-Rs.500/-per quiz (10quiz per block for 484<br />
blocks))<br />
Health Mellas/Fairs-Rs.5000/- per Mela(one Health<br />
mela/district)<br />
2420000.00<br />
190000.00<br />
Total -IEC 4546000.00 700000.00 5246000.00<br />
7 Training<br />
7.1<br />
7.2<br />
7.3<br />
2 days modular training of new entrant MOs-Rs.27300/-<br />
per batch for 47 batches<br />
1 days reorientation training for 2700 Mos-Rs.13650/-<br />
per batch for 90 batches<br />
Training of ASHA(half day)-for 659 Batches (40 ASHA /<br />
Batch)<br />
1283100<br />
1228500.00<br />
2108800.00<br />
Total - Training(7.1 to 7.6) 4620400 0.00 4620400<br />
8<br />
Disability Prevention and Medical Rehabilitation<br />
(DPMR)<br />
8.1 MCR & other footwears-4560 pairs @ Rs.250/- per pair 1140000.00<br />
8.2 Aids & appliances-Rs.12500/- per district 475000<br />
8.3<br />
8.4<br />
Welfare allowance for RCS patients @ 5000/- per<br />
patient for 120 patients<br />
Incentive to institution for RCSRs.5000/ - per RCS for<br />
80 RCS<br />
600000.00<br />
400000.00<br />
280
Total - DPMR(8.1 to 8.4) 475000.00 2140000.00 2615000.00<br />
9<br />
9.1<br />
9.2<br />
Services through ASHA(performance based<br />
incentive to ASHA)<br />
For PB new cases-4840(PB cases) @ Rs.300/- per<br />
case<br />
For MB new cases-3872(MB cases) @ Rs.500/- per<br />
case<br />
1452000.00<br />
1936000.00<br />
Total - Services through ASHA(9.1 to 9.2) 3388000.00 3388000.00<br />
10 Urban Leprosy Control Programme:<br />
10.1 For 24 townships-Rs.75000/- per town 1800000.00<br />
10.2 For 6 medium I cities-Rs.150000/- per medium city 900000.00<br />
Total -Urban leprosy control(10.1 to 1 0.2) 2700000.00 2700000.00<br />
11<br />
Review meetings of DLOs four times in a year-<br />
Rs.30000/- per meeting<br />
120000.00 120000.00<br />
Grand Total 27897800.00<br />
(Rs. Two Crore sevety eight lac ninety seven thousands & eight hundred only)<br />
281
Fund Allocation to <strong>State</strong> Leprosy Cell 2009-2010<br />
Sl.<br />
Expenditure Under SHS (Leprosy) Component & Sub Component w ise<br />
No.<br />
Amount Rs.<br />
1 Two Driver's Remuneration for <strong>State</strong> Leprosy Cell @ Rs. 4500/- 108000.00<br />
2 DEO at <strong>State</strong> Leprosy Cell @ Rs. 8000/- 96000.00<br />
3 Audit Fee for <strong>State</strong> Leprosy Cell 6000<br />
4 Telephone, Fax, P &T charges , Miscellaneous @ Rs. 38000/- per year 38000<br />
5 Consumables : Stationery etc. @ Rs. 28000/- per year 28000<br />
6 Two vehicles for SHS (Leprosy) @Rs. 85000/- Per vehicle / year 170000<br />
7 Printing of Forms / DPMR registers et. 600000<br />
8 Electronic media-Radio / Doordarshan 500000<br />
9 Print media-News papers 200000<br />
10 MCR & other Footwears- 4560 pairs @ Rs.250/- per pair 1140000<br />
11 Review meeting of DLOs four times in a year @ Rs. 30000/- per meeting 120000<br />
Total 3006000<br />
282
Fund Allocation to District Health Society (Leprosy) 2009-2010<br />
Contractual services<br />
Sl.<br />
No.<br />
District<br />
Populatiom March 2008 (Est.)<br />
Number of Block PHC<br />
PD Ratio<br />
Number of ASHAs<br />
Driver's Remuneration @<br />
Rs. 4500/ - per month<br />
Honorarium for Accounts work<br />
of Leprosy @ Rs. 400/ - per month<br />
Audit Fee @ Rs. 6000/ -<br />
DLS(leprosy) for<br />
rent,telephone,electricity,<br />
P & T charges, miscellaneous -<br />
Rs.18000/- per district/ year<br />
Consumable Expenses (Stationery &<br />
etc.) @ Rs. 14000/ - per year<br />
Vehicle Operation / hirin g,<br />
POL & Maintenance<br />
@ Rs. 75000/ - per vehicle / district<br />
1 Aurangabad 2383268 11 1552 54000 4800 6000 18000 14000 75000<br />
2 Bhojpur 2654828 13 1621 54000 4800 6000 18000 14000 75000<br />
3 Buxar 1668275 8 1074 54000 4800 6000 18000 14000 75000<br />
4 Bhagalpur 2888900 13 1971 54000 4800 6000 18000 14000 75000<br />
5 Banka 1912332 10 1535 54000 4800 6000 18000 14000 75000<br />
6 Darbhanga 3905394 18 2890 54000 4800 6000 18000 14000 75000<br />
7 Katihar 2840403 13 1866 54000 4800 6000 18000 14000 75000<br />
8 Muzaffarpur 4450244 14 2848 54000 4800 6000 18000 14000 75000<br />
9 Nawada 2150838 14 1591 54000 4800 6000 18000 14000 75000<br />
10 Patna 5598533 23 2549 54000 4800 6000 18000 14000 75000<br />
11 Purnea 3020199 11 2263 54000 4800 6000 18000 14000 75000<br />
12 Kishanganj 1538234 7 1024 54000 4800 6000 18000 14000 75000<br />
13 Araria 2525757 9 2026 54000 4800 6000 18000 14000 75000<br />
14 Rohtas 2910808 19 2030 54000 4800 6000 18000 14000 75000<br />
15 Kaimur 1526956 10 1247 54000 4800 6000 18000 14000 75000<br />
16 Siwan 3219960 15 2538 54000 4800 6000 18000 14000 75000<br />
17 Sitamarhi 3173657 14 2221 54000 4800 6000 18000 14000 75000<br />
18 Sheohar 611327 3 464 54000 4800 6000 18000 14000 75000<br />
19 W.Champaran 3617222 18 2494 54000 4800 6000 18000 14000 75000<br />
20 Begusarai 2785077 18 2091 54000 4800 6000 18000 14000 75000<br />
21 E.Champaran 4675857 20 2756 54000 4800 6000 18000 14000 75000<br />
22 Gaya 4118776 22 2440 54000 4800 6000 18000 14000 75000<br />
23 Gopalganj 2554894 14 1846 54000 4800 6000 18000 14000 75000<br />
24 Jehanabad 1100835 7 743 54000 4800 6000 18000 14000 75000<br />
25 Arwal 695751 5 658 54000 4800 6000 18000 14000 75000<br />
26 Khagaria 1517568 7 967 54000 4800 6000 18000 14000 75000<br />
27 Madhubani 4244381 18 3034 54000 4800 6000 18000 14000 75000<br />
28 Madhepura 1812266 7 1459 54000 4800 6000 18000 14000 75000<br />
29 Munger 1349751 9 820 54000 4800 6000 18000 14000 75000<br />
30 Sheikhpura 624223 6 439 54000 4800 6000 18000 14000 75000<br />
31 Jamui 1661158 6 1270 54000 4800 6000 18000 14000 75000<br />
32 Lakhisarai 952343 4 568 54000 4800 6000 18000 14000 75000<br />
33 Nalanda 2815197 20 2017 54000 4800 6000 18000 14000 75000<br />
34 Saharsa 1790658 12 777 54000 4800 6000 18000 14000 75000<br />
35 Supaul 2074339 11 1533 54000 4800 6000 18000 14000 75000<br />
36 Samastipur 4057475 23 3214 54000 4800 6000 18000 14000 75000<br />
37 Saran 3864981 15 2825 54000 4800 6000 18000 14000 75000<br />
38 Vaishali 3224178 17 2532 54000 4800 6000 18000 14000 75000<br />
Total 98516843 484 0 67793 2052000 182400 228000 684000 532000 2850000<br />
283
Drugs, materials &<br />
supplies<br />
Training<br />
Sl.<br />
No.<br />
District<br />
Supportive medicines @ Rs. 25000/ -<br />
per year<br />
Laboratory reagents & equipments<br />
@ Rs. 12000/ - per year<br />
Patient welfare @ Rs. 6000/ - per<br />
year<br />
School quiz @ Rs. 500/- per quiz<br />
(10 quiz per Blocks)<br />
Sensitisation meetings with PRI<br />
members @ Rs. 4000/- per<br />
meeting at block level<br />
Health Melas / Fairs @ Rs.<br />
5000/- per mela (One Health<br />
Mela / District)<br />
Two days modular<br />
training of new<br />
entrant MOs @<br />
Rs.27300/- per<br />
batch for 47 batch<br />
No.of<br />
Batch<br />
Amount<br />
One day reorientation<br />
training of MOs @<br />
Rs. 13650/- batch<br />
for 90 batches<br />
No. of<br />
Batch<br />
Amount<br />
1 Aurangabad 25000 12000 6000 55000 44000 5000 1 27300 2 27300<br />
2 Bhojpur 25000 12000 6000 65000 52000 5000 2 54600 3 40950<br />
3 Buxar 25000 12000 6000 40000 32000 5000 1 27300 2 27300<br />
4 Bhagalpur 25000 12000 6000 65000 52000 5000 2 54600 3 40950<br />
5 Banka 25000 12000 6000 50000 40000 5000 1 27300 2 27300<br />
6 Darbhanga 25000 12000 6000 90000 72000 5000 2 54600 3 40950<br />
7 Katihar 25000 12000 6000 65000 52000 5000 1 27300 2 27300<br />
8 Muzaffarpur 25000 12000 6000 70000 56000 5000 2 54600 3 40950<br />
9 Nawada 25000 12000 6000 70000 56000 5000 1 27300 2 27300<br />
10 Patna 25000 12000 6000 115000 92000 5000 2 54600 7 95550<br />
11 Purnea 25000 12000 6000 55000 44000 5000 1 27300 2 27300<br />
12 Kishanganj 25000 12000 6000 35000 28000 5000 0 0 1 13650<br />
13 Araria 25000 12000 6000 45000 36000 5000 1 27300 2 27300<br />
14 Rohtas 25000 12000 6000 95000 76000 5000 1 27300 2 27300<br />
15 Kaimur 25000 12000 6000 50000 40000 5000 1 27300 1 13650<br />
16 Siwan 25000 12000 6000 75000 60000 5000 1 27300 2 27300<br />
17 Sitamarhi 25000 12000 6000 70000 56000 5000 1 27300 3 40950<br />
18 Sheohar 25000 12000 6000 15000 12000 5000 0 0 1 13650<br />
19 W.Champaran 25000 12000 6000 90000 72000 5000 1 27300 3 40950<br />
20 Begusarai 25000 12000 6000 90000 72000 5000 2 54600 2 27300<br />
21 E.Champaran 25000 12000 6000 100000 80000 5000 2 54600 4 54600<br />
22 Gaya 25000 12000 6000 110000 88000 5000 2 54600 3 40950<br />
23 Gopalganj 25000 12000 6000 70000 56000 5000 1 27300 2 27300<br />
24 Jehanabad 25000 12000 6000 35000 28000 5000 1 27300 2 27300<br />
25 Arwal 25000 12000 6000 25000 20000 5000 1 27300 1 13650<br />
26 Khagaria 25000 12000 6000 35000 28000 5000 1 27300 1 13650<br />
27 Madhubani 25000 12000 6000 90000 72000 5000 1 27300 3 40950<br />
28 Madhepura 25000 12000 6000 35000 28000 5000 1 27300 2 27300<br />
29 Munger 25000 12000 6000 45000 36000 5000 1 27300 2 27300<br />
30 Sheikhpura 25000 12000 6000 30000 24000 5000 1 27300 2 27300<br />
31 Jamui 25000 12000 6000 30000 24000 5000 1 27300 1 13650<br />
32 Lakhisarai 25000 12000 6000 20000 16000 5000 1 27300 1 13650<br />
33 Nalanda 25000 12000 6000 100000 80000 5000 2 54600 3 40950<br />
34 Saharsa 25000 12000 6000 60000 48000 5000 1 27300 2 27300<br />
35 Supaul 25000 12000 6000 55000 44000 5000 1 27300 2 27300<br />
36 Samastipur 25000 12000 6000 115000 92000 5000 2 54600 5 68250<br />
37 Saran 25000 12000 6000 75000 60000 5000 1 27300 3 40950<br />
38 Vaishali 25000 12000 6000 85000 68000 5000 2 54600 3 40950<br />
Total 950000 456000 228000 2420000 1936000 190000 47 1283100 90 1228500<br />
284
Sl. No.<br />
District<br />
Training<br />
Training of ASHA<br />
(half day) @ Rs.<br />
3200/- per Batch<br />
of 40<br />
No. of<br />
Batch<br />
Amount<br />
DPMR<br />
Aids & appliances<br />
@ Rs.12500/- per<br />
district<br />
Services through ASHA<br />
(performance based<br />
Incentive to ASHA, 10 PB<br />
& 8 MB / BLOCK / YEAR)<br />
Urban Leprosy Control<br />
Programme<br />
Number of RCS<br />
RCS<br />
Welfare allowance<br />
for RCS patients<br />
(Rs. 5000/- / RCS)<br />
Incentive to<br />
Institution for RCS<br />
(Rs. 5000/- / RCS)<br />
1 Aurangabad 20 64000 12500 77000 75000<br />
2 Bhojpur 15 48000 12500 91000 75000<br />
3 Buxar 10 32000 12500 56000 75000<br />
4 Bhagalpur 20 64000 12500 91000 150000<br />
5 Banka 15 48000 12500 70000 0<br />
6 Darbhanga 25 80000 12500 126000 150000 5 25000 25000<br />
7 Katihar 20 64000 12500 91000 75000<br />
8 Muzaffarpur 25 80000 12500 98000 150000 40 200000<br />
9 Nawada 15 48000 12500 98000 75000<br />
10 Patna 25 80000 12500 161000 150000 75 375000 375000<br />
11 Purnea 20 64000 12500 77000 150000<br />
12 Kishanganj 10 32000 12500 49000 75000<br />
13 Araria 25 80000 12500 63000 0<br />
14 Rohtas 20 64000 12500 133000 75000<br />
15 Kaimur 10 32000 12500 70000 0<br />
16 Siwan 25 80000 12500 105000 75000<br />
17 Sitamarhi 20 64000 12500 98000 75000<br />
18 Sheohar 15 48000 12500 21000 0<br />
19 W.Champaran 20 64000 12500 126000 75000<br />
20 Begusarai 15 48000 12500 126000 75000<br />
21 E.Champaran 25 80000 12500 140000 75000<br />
22 Gaya 25 80000 12500 154000 150000<br />
23 Gopalganj 15 48000 12500 98000 75000<br />
24 Jehanabad 10 32000 12500 49000 75000<br />
25 Arwal 10 32000 12500 35000 0<br />
26 Khagaria 10 32000 12500 49000 0<br />
27 Madhubani 25 80000 12500 126000 75000<br />
28 Madhepura 15 48000 12500 49000 75000<br />
29 Munger 10 32000 12500 63000 75000<br />
30 Sheikhpura 10 32000 12500 42000 0<br />
31 Jamui 10 32000 12500 42000 75000<br />
32 Lakhisarai 10 32000 12500 28000 0<br />
33 Nalanda 15 48000 12500 140000 75000<br />
34 Saharsa 15 48000 12500 84000 75000<br />
35 Supaul 14 44800 12500 77000 75000<br />
36 Samastipur 25 80000 12500 161000 75000<br />
37 Saran 25 80000 12500 105000 75000<br />
38 Vaishali 20 64000 12500 119000 75000<br />
Total 659 2108800 475000 3388000 2700000 120 600000 400000<br />
285
Activity Chart for Action Plan 2009-10 (Gantt Chart) Annexure - 2<br />
Sl.<br />
No.<br />
Activity<br />
Persons<br />
responsible<br />
Time<br />
Frame<br />
Jan 09 Feb 09 Mar 09 Apr 09 May 09 Jun 09 Jul 09 Aug 09 Sep 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10<br />
I<br />
Planning of Activities<br />
1.1<br />
Development of Action Plan for<br />
2009-10 and its submission to GOI<br />
after aproval of SHS, Bihar<br />
1.2 Approval of <strong>State</strong> Action Plan GOI<br />
1.3<br />
1.4<br />
<strong>State</strong> Leprosy<br />
Officer,<br />
WHO/ILEP<br />
Coordinators<br />
Development of budgetary and <strong>State</strong> Leprosy<br />
operational guidelines for each and Officer,<br />
every activity as per approved WHO/ILEP<br />
action plan<br />
Coordinators<br />
Briefing of CS and DLOs on Action<br />
Plan and development of detialed<br />
districtwise operational plan with<br />
specific time frame in the first<br />
review and planning meeting at<br />
<strong>State</strong> HQ<br />
<strong>State</strong> Leprosy<br />
Officer,<br />
WHO/ILEP<br />
Coordinators,<br />
CS and DLOs<br />
By 19th Jan.<br />
2009<br />
By 30th Jan.<br />
2009<br />
By 10th May<br />
2009<br />
By 15th May<br />
2009<br />
1.5<br />
Budgetary allocation for each<br />
district<br />
<strong>State</strong> Health<br />
Society & SLO<br />
By 20th May<br />
2009<br />
1.6<br />
Approval of District Action Plan and<br />
its budget in District Health Society<br />
CS and DLO<br />
By<br />
30th May<br />
2009<br />
Statrt activities as per the action<br />
plan and continue activities on<br />
routine<br />
Concern<br />
officers at<br />
<strong>State</strong>, Dist and<br />
PHC level<br />
1st June<br />
2009 to 31st<br />
March 2010<br />
II<br />
Prcurement Plan<br />
2.1 Purchase of logistics such as<br />
286
2.2<br />
2.3<br />
MCR Chappals (Through a <strong>State</strong><br />
level committee)<br />
Supportive Medicine<br />
e.g.Prednisolone<br />
2.4 Splint, Crutches, Lab reagents<br />
2.5 Printing of Formats<br />
III Training<br />
3.1<br />
3.2<br />
3.3<br />
3.4<br />
3.5<br />
4 day training for MOs a batch of<br />
30 MOs x 47 batches<br />
2 days reorientation training for<br />
Medical Officers at Distt./PHC a<br />
batch of 30 Mos x 90 batches<br />
Refreshal training for one day for<br />
Health<br />
Supervisors/LHV/Pharmacists a<br />
batch of 30 x 50 batches<br />
5 days training of lab technicians a<br />
batch of 15 LTs x 3 batches<br />
1 day training of 'A'Grade nurses in<br />
48 batches<br />
3.6 Half day training of 50000 ASHA<br />
<strong>State</strong> Leprosy<br />
Officer<br />
CS and DLO<br />
<strong>State</strong> Leprosy<br />
Officer<br />
<strong>State</strong> Leprosy<br />
Officer<br />
<strong>State</strong> Leprosy<br />
Officer,<br />
WHO/ILEP<br />
Coordinators,<br />
DLOs By<br />
making 5 <strong>State</strong><br />
level teams<br />
June/July<br />
2009<br />
May/June<br />
2009<br />
June/July<br />
2009<br />
By July<br />
2009<br />
Aug. 2009<br />
to Dec.<br />
2009<br />
Sept. 2009<br />
CS, DLO,<br />
to Dec.<br />
District Nucleus<br />
2009<br />
Sept. 2009<br />
CS, DLO,<br />
to Dec.<br />
District Nucleus<br />
2009<br />
ILEP<br />
<strong>State</strong> Leprosy<br />
Officer,<br />
WHO/ILEP<br />
Coordinators<br />
In October<br />
2009<br />
Aug. 2009<br />
to Dec.<br />
2009<br />
CS,DLO,District May 2009<br />
Nucleus & to Aug.<br />
BPHC staff 2009<br />
IV<br />
Disability Prevention and<br />
Medical Rehabilation (DPMR)<br />
287
4.4<br />
RCS - 200 operations at Dept of<br />
PMR, Patna Medical College,<br />
Patna and operations at<br />
Darbhanga Medical College,<br />
Darbhanga & TLM Muzaffarpur<br />
DLO<br />
Patna,DLO<br />
Darbhanga,<br />
April 2009<br />
DLO<br />
to March<br />
Muzaffarpur,<br />
2010<br />
District Nucleus<br />
and Medical<br />
Collages<br />
V<br />
Information, Education,<br />
Communication (IEC)<br />
5.1 Radio Spots/Doordarshan<br />
5.2<br />
Meeting (Political Advocacy, for<br />
MLA, MLC )<br />
5.3 Hoarding<br />
5.5 Posters<br />
5.6 Cable Spot<br />
5.7 Wall panting<br />
5.8 Rallies (including banners etc.)<br />
<strong>State</strong> Leprosy<br />
Officer<br />
<strong>State</strong> Leprosy<br />
Officer,<br />
WHO/ILEP<br />
Coordinators<br />
DLS - CS,<br />
DLO, District<br />
Nucleus<br />
DLS - CS,<br />
DLO, District<br />
Nucleus, PHC<br />
staff<br />
DLS - CS,<br />
DLO, District<br />
Nucleus<br />
DLS - CS,<br />
DLO, District<br />
Nucleus, PHC<br />
staff<br />
DLS - CS,<br />
DLO, District<br />
Nucleus, PHC<br />
staff<br />
June 2009<br />
to March<br />
2010<br />
During<br />
Winter<br />
session<br />
June 2009<br />
to Aug.<br />
2009<br />
June 2009<br />
to Aug.<br />
2009<br />
June 2009<br />
to March<br />
2010<br />
June 2009<br />
to Dec.<br />
2009<br />
Antileprosy<br />
Week<br />
288
5.9 Quiz<br />
5.10 Cinema slides<br />
5.12 Meeting with Zilla Parishad<br />
5.13<br />
Orientation camp for NGO and<br />
Mahila Mandals<br />
5.14 Press Advertisement<br />
5.16 Health Mellas/Fairs<br />
5.18 Monitoring & Supervision<br />
DLS - CS,<br />
DLO, District<br />
Nucleus, PHC<br />
staff<br />
DLS - CS,<br />
DLO, District<br />
Nucleus<br />
DLS - CS,<br />
DLO, District<br />
Nucleus, PHC<br />
staff<br />
DLS - CS,<br />
DLO, District<br />
Nucleus<br />
DLS - CS,<br />
DLO, District<br />
Nucleus, PHC<br />
staff<br />
DLS - CS,<br />
DLO, District<br />
Nucleus, PHC<br />
staff<br />
DLS - CS,<br />
DLO, District<br />
Nucleus, PHC<br />
staff<br />
In January<br />
2010<br />
June 2009<br />
to March<br />
2010<br />
Oct. 2009<br />
to Dec.<br />
2009<br />
Jan. 2009 to<br />
Febr. 2010<br />
Jan. 2010<br />
to Feb.<br />
2010<br />
June 2009<br />
to Sept.<br />
2009<br />
October 09<br />
to March<br />
2010<br />
VI<br />
Epidemiological Situation<br />
Analysis<br />
6.1<br />
Status of Implementation of Action<br />
Plan for 2009-10<br />
6.2 MDT Stock Situation Analysis<br />
A <strong>State</strong> NLEP Every<br />
Coordination month from<br />
Committee April 2009<br />
under the to March<br />
chairmanship of 2010<br />
289
6.3<br />
Districtwise analysis based on the<br />
field observations of DLOs,<br />
WHO/ILEP Coordinators and <strong>State</strong><br />
Officers involving 6 DLOs in a<br />
month on rotation<br />
6.4 Quality of Diagnosis<br />
Regularity of treatment and timely<br />
6.4.1<br />
RFT<br />
Quality of information and<br />
6.4.2<br />
implementation of SIS<br />
Availability of MDT stock and other<br />
6.4.3<br />
logistics<br />
Capacity of GHCS staff and<br />
6.4.4<br />
integration<br />
Implementation of Action Plan<br />
6.4.5<br />
2009-10 including DPMR<br />
Briefing of Executive Director, SHS<br />
on the minutes of <strong>State</strong> NLEP<br />
6.4.6 Coordination Meeting and sharing<br />
the same with Director in Chief,<br />
Secretary Health, DDGL, etc.<br />
Additional<br />
Director and<br />
<strong>State</strong> Leprosy<br />
Officer, Leprosy<br />
will<br />
continuously<br />
monitor the<br />
programme at<br />
each level and<br />
do analysis in<br />
<strong>State</strong> NLEP<br />
Coordination<br />
Meeting at<br />
<strong>State</strong> HQ<br />
Following will<br />
be the<br />
members of<br />
committee<br />
Additional<br />
Director Health<br />
Services,<strong>State</strong><br />
Leprosy Officer<br />
and Controlling<br />
Officer, Bihar<br />
<strong>State</strong><br />
Coordinator<br />
(WHO/GOI),<br />
NLEP, Bihar<br />
ILEP Members<br />
Representative<br />
from PMCH,<br />
Patna<br />
DLOs from<br />
identified<br />
districts on<br />
rotation<br />
Epidemiologist<br />
SSAU<br />
290
6.5 Reviews<br />
<strong>State</strong> NLEP<br />
Coordination<br />
Committee<br />
Every<br />
month from<br />
April 2009<br />
to March<br />
2010<br />
VII<br />
7.1<br />
7.2<br />
7.3<br />
7.4<br />
7.5<br />
A review meeting of all DLOs will<br />
be called at <strong>State</strong> HQ every quarter<br />
to review all the activities in detail.<br />
Zonal review meetings at each<br />
zone<br />
District will review NLEP in routine<br />
monthly meetings<br />
Block will review NLEP in routine<br />
weekly meetings<br />
DLOs and District Nucleus will<br />
participate in weekly PHC meeting<br />
on rotation and review NLEP at that<br />
level<br />
Please tick mark in the square<br />
when the activity is completed and<br />
mark a question mark when due<br />
date is passed<br />
Executive<br />
Director, SHS,<br />
Add. Director,<br />
<strong>State</strong> Leprosy<br />
Officer,<br />
WHO/ILEP<br />
Coordinators,<br />
<strong>State</strong> Leprosy<br />
Officer Add.<br />
Director,<br />
WHO/ILEP<br />
Coordinators,<br />
May,<br />
August,<br />
November,<br />
February in<br />
2009-2010<br />
Alternate<br />
month<br />
Every<br />
CS, DLO, month from<br />
District Nucleus Apr. 2009 to<br />
Mar. 2010<br />
I/C MO PHC<br />
Every week<br />
from Apr.<br />
2009 to<br />
Mar. 2010<br />
Every week<br />
DLO and<br />
from Apr.<br />
District Nucleus<br />
2009 to<br />
on rotation<br />
Mar. 2010<br />
291
293
Annual Plan for Programme Performance & Budget for the year<br />
1 st April 2009 to 31 st March 2010<br />
<strong>State</strong>: Bihar (GFATM)<br />
Objectives:<br />
3.1.To achieve and maintain a cure rate of at least 85% among newly detected infectious (new<br />
sputum smear positive) cases, and<br />
4.2. To achieve and maintain detection of at least 70% of such cases in the population<br />
Formatted: Bullets and Numbering<br />
This action plan and budget have been approved by the STCS.<br />
Signature of the STO__________<br />
Name Dr.N.M. Sharma<br />
_______<br />
Section-A – General Information about the <strong>State</strong><br />
1 <strong>State</strong> Population (in lakh) GFATM Districts 670.23<br />
2 Number of GFATM districts in the <strong>State</strong> 30<br />
3 Urban population 50.46<br />
4 Tribal population 8<br />
5 Hilly population 6<br />
6 Any other known groups of special population for specific interventions<br />
(e.g. nomadic, migrant, industrial workers, urban slums, etc.)<br />
(These population statistics may be obtained from Census data /<strong>State</strong> Statistical Dept/ District plans)<br />
No. of districts without DTC: 3<br />
No. of districts that submitted annual action plans, which have been consolidated in this state plan:<br />
30<br />
Organization of services in the state:<br />
S.<br />
No.<br />
Name of the<br />
District<br />
Projected<br />
Population<br />
(in Lakhs)<br />
Please indicate number<br />
of TUs of each type<br />
Govt NGO Public<br />
Sector*<br />
294<br />
Please indicate no. of DMCs of<br />
each type in the district<br />
NGO<br />
Private<br />
Sector^<br />
Araria 24.42 5 0 12 1 5<br />
Arwal 7 1 0 5 0 0<br />
Aurangabad 23.04 5 0 14 2 2<br />
Banka 18.49 3 1 11 1 3<br />
Begusarai 26.93 5 0 18 1 3<br />
Bhagalpur 27.94 5 0 21 1 3<br />
Bhojpur 25.67 5 0 21 0 3<br />
Buxar 16.13 3 0 14 0 1<br />
Darbhanga 37.77 7 0 20 1 4<br />
Gaya 39.83 8 0 28 1 3<br />
Gopalganj 24.70 5 0 20 0 2<br />
Jamui 16.06 4 1 15 0 2<br />
Jehanabad 10.37 2 0 8 0 1<br />
Kaimur 14.76 2 1 12 0 1
Khagaria 14.67 3 0 13 0 1<br />
Kisanganj 14.87 2 1 10 0 2<br />
Lakhisharai 9.21 2 0 6 0 1<br />
Madhepura 17.52 3 0 14 1 1<br />
Madhubani 41.04 8 0 23 1 2<br />
Nalanda 27.22 5 0 20 0 3<br />
Nawadah 20.80 4 0 15 0 2<br />
W.Champaran 34.98 6 1 20 0 3<br />
Rohtas 28.15 5 0 20 2 2<br />
Saharsa 17.31 4 0 11 0 3<br />
Saran 37.38 6 0 29 0 3<br />
Sheikhpura 6.03 1 0 4 0 0<br />
Sheohar 5.91 1 0 4 0<br />
Sitamarhi 30.69 6 0 26 0 3<br />
Siwan 31.14 6 0 20 0 3<br />
Supaul 20.06 4 0 11 0 2<br />
126 5 465 12 64<br />
*Public Sector includes Medical Colleges, Govt. health department, other Govt. department and PSUs i.e. as defined in PMR<br />
report<br />
^ Similarly, Private Sect or includes Private Medical College, Private Practitioners, Private Clinics/Nursing Homes and<br />
Corporate sector<br />
295
RNTCP performance indicators:<br />
Important: Please give the performance for the last 4 quarters i.e. Oct ___ to September _____<br />
Name of the<br />
District (also<br />
indicate if it is<br />
notified hilly or<br />
tribal district<br />
Total<br />
number of<br />
patients<br />
put on<br />
treatment<br />
*<br />
Annualised<br />
total case<br />
detection<br />
rate<br />
(per lakh<br />
pop.)<br />
No of new<br />
smear<br />
positive<br />
cases put<br />
on<br />
treatment<br />
*<br />
Annualised<br />
New smear<br />
positive case<br />
detection rate<br />
(per lakh<br />
pop)<br />
Cure rate for<br />
cases<br />
detected in<br />
the last 4<br />
correspondin<br />
g quarters<br />
Plan for the next year<br />
Annualized<br />
NSP case<br />
detection<br />
rate<br />
Araria<br />
Arwal<br />
Aurangabad<br />
Banka 1744 94.78 919 94.49 75 70 85<br />
Begusarai 3141 116.12 870 33.05 69.64 70 85<br />
Bhagalpur 3908 138.48 1396 51.07 85.8 70 85<br />
Bhojpur 1128 450 60 70 85<br />
Buxar 708 235 70 85<br />
Darbhanga 3015 82.37 1173 32.04 81.87 70 85<br />
Gaya 70 85<br />
Gopalganj 70 85<br />
Jamui 1172 64.04 506 30.4 58.6 70 85<br />
Jehanabad 1058 50.25 473 61.85 75.65 70 85<br />
Kaimur 70 85<br />
Khagaria 836 14.67 356 24.26 63.63 70 85<br />
Kisanganj 1233 41.4 715 65 79 70 85<br />
Lakhisharai 651 56 248 35 83 70 85<br />
Madhepura 998 61 551 45.33 87.33 70 85<br />
Madhubani 2135 53.67 1051 26.42 74.29 70 85<br />
Nalanda 1928 49.85 946 46.7 89.78 70 85<br />
Nawadah 1068 53.52 531 35.48 88.74 70 85<br />
W.Champaran 2269 64 1093 31 72 70 85<br />
Rohtas 1995 71.97 890 42.81 78.21 70 85<br />
Saharsa 70 85<br />
Saran 70 85<br />
Sheikhpura 505 110 76 70 85<br />
Sheohar 70 85<br />
Sitamarhi 2588 85.07 1234 40.96 58.66 70 85<br />
Siwan 2093 57 739 27 50 70 85<br />
Supaul 70 85<br />
Cure rate<br />
Total<br />
* Patients put on treatment under DOTS regimens only are to be included.<br />
296
Section B – List Priority areas at the <strong>State</strong> level for achieving the objectives planned:<br />
S.No. Priority areas Activity planned under each priority area<br />
1<br />
1 a)Filling up of all <strong>State</strong> and District level Contractual Staff .<br />
Human Resource 1 b) Filling up the posts of DTOs & MOTCs,<br />
2 a) Training of untrained DTOs & MO TCs at National & state<br />
level and also of STS, STLS , LTs<br />
2 Training 2 b) Training and Refresher trainings of MOs & Para Medical<br />
Staff<br />
2 c) Training of ASHA as DOT providers<br />
2 d)Training and retraining of All contractual staff of RNTCP<br />
3 IEC 3 a) Printing of IEC Materials for the <strong>State</strong><br />
3 b)Involvement of masses through generating awareness via the<br />
print and electronic Media.<br />
4 Involvement of other<br />
sectors/ NGOs/PP<br />
3 c) Sensitisation of local MLAs and PRI members, empowering<br />
the community by making them aware of the RNTCP facilities<br />
4 a) Sensitisation workshop for other sectors, NGOs and PPs.<br />
On the revised schemes<br />
5 Strengthening of IRL, Lab<br />
network and<br />
Implementation of EQA<br />
4 b) Increased involvement of Faith Based and community based<br />
organisations.<br />
4 c) Involving IMA in RNTCP in the <strong>State</strong><br />
5 a)Starting more DMCs especially in the APHCs with the help of<br />
NGOs<br />
6 Minimizing Initial<br />
Defaulters<br />
5 c)Visit of IRL to all the 38 districts with at least one OSE and<br />
One Panel Testing.<br />
6 a) Ensuring in all districts line listing of all sputum smear +ve<br />
patients diagnosed on regular basis<br />
6 b) Regular data exchange for feedback within district regarding<br />
referral for treatment.<br />
297
Priority Districts for Supervision and Monitoring by <strong>State</strong> during the next year<br />
Activity<br />
S No District Reason for inclusion in priority list<br />
1 Supaul Low case Detection<br />
2 Buxar Low case Detection<br />
3 Bhojpur Low case Detection<br />
4 Gaya Low case Detection<br />
5 Madhepura Low case Detection<br />
6 Kaimur Low case Detection<br />
7 Saran Low case Detection<br />
Section C – Consolidated Plan for Performance and Expenditure under each head,<br />
including estimates submitted by all districts, and the requirements at the <strong>State</strong> Level<br />
1. Civil Works<br />
No. required<br />
as per the<br />
norms in the<br />
state<br />
No.<br />
already<br />
upgraded/<br />
present in<br />
the state<br />
No. planned<br />
to be<br />
upgraded<br />
during next<br />
financial<br />
year<br />
Pl provide justification<br />
if an increase is planned<br />
in excess of norms (use<br />
separate sheet if<br />
required)<br />
Estimated Expenditure on<br />
the activity<br />
Quarter in which<br />
the planned<br />
activity expected<br />
to be completed<br />
(a) (b) (c) (d) (e) (f)<br />
STDC/<br />
IRL<br />
SDS<br />
DTCs 30 27 3 Upgradation of DTCs 3 rd Quarter<br />
2009<br />
TUs 130 114 13 Up gradation of TUs<br />
+<br />
Maintenance of TUs<br />
DMCs 650 513 74 Up gradation of<br />
DMcs +<br />
maintenance civil<br />
works of DMCs<br />
TOTAL Rs 4266000/-<br />
3 rd Quarter<br />
2009<br />
4 th Quarter<br />
2009<br />
298
2. Laboratory Materials<br />
Activity<br />
Purchase of Lab<br />
Materials by Districts<br />
Amount<br />
permissible as<br />
per the norms in<br />
the state<br />
Amount<br />
actually<br />
spent in the<br />
last 4<br />
quarters<br />
Procurement<br />
planned<br />
during the<br />
current<br />
financial year<br />
(in Rupees)<br />
Estimated<br />
Expenditure for<br />
the next<br />
financial year<br />
for which plan is<br />
being submitted<br />
(Rs.)<br />
(a) (b) (c) (d) (e)<br />
1,00,53,000 2240090 7800000 1,10,50,000<br />
Justification/<br />
Remarks for (d)<br />
Lab materials for EQA<br />
activity at STDC<br />
3. Honorarium<br />
Activity<br />
Honorarium for DOT<br />
providers (both tribal<br />
and non tribal<br />
districts)<br />
Honorarium for DOT<br />
providers of Cat IV<br />
patients<br />
Amount<br />
permissible as<br />
per the norms<br />
in the state<br />
Amount<br />
actually<br />
spent in<br />
the last 4<br />
quarters<br />
Expenditure<br />
(in Rs)<br />
planned for<br />
current<br />
financial<br />
year<br />
Estimated Expenditure<br />
for the next financial<br />
year for which plan is<br />
being submitted<br />
(Rs.)<br />
Justification/<br />
Remarks for<br />
(d)<br />
(a) (b) (c) (d) (e)<br />
18,76,000 332375 1540000 2,60,00,000/-<br />
Community volunteers in all<br />
the districts*<br />
No. presently involved in RNTCP<br />
1315 40,000<br />
Additional enrolment proposed for the next<br />
fin. Year<br />
* These community volunteers are other than salaried employees of Central/<strong>State</strong> government and<br />
are involved in provision of DOT e.g. Anganwadi workers, trained dais, village health guides,<br />
ASHA, other volunteers, etc.<br />
299
4. IEC/Publicity:<br />
Permissible budget for <strong>State</strong> and all Districts as per Norms: Rs. 50,26,500<br />
Estimated IEC budget for all Districts, as per action plans (please enclose consolidation summary): Rs.<br />
_________<br />
Estimated IEC activities and Budget at the <strong>State</strong> level (excluding districts) for the next financial year<br />
proposed as per action plan detailed below: Rs. _____________________<br />
Target<br />
Group/<br />
Objective<br />
Patients<br />
and<br />
General<br />
public /<br />
for<br />
awareness<br />
generation<br />
and social<br />
mobilizati<br />
on<br />
Activity<br />
(All activities to be<br />
planned as per local<br />
needs, catering to the<br />
target groups<br />
specified)<br />
Outdoors:<br />
- wall paintings<br />
- Hoardings<br />
- Tin plates<br />
- Banners<br />
- others<br />
Outreach activities:<br />
- Patient provider<br />
interaction<br />
meetings<br />
- Community<br />
meetings<br />
- Mike publicity<br />
- Others<br />
Activities Planned at <strong>State</strong> Level<br />
No. of<br />
activities<br />
held in<br />
last 4<br />
quarters<br />
No of activities proposed in the<br />
next financial year, quarterwise<br />
Apr-<br />
Jun<br />
July-<br />
Sep<br />
Oct-<br />
Dec<br />
Jan-<br />
Mar<br />
Total<br />
activitie<br />
s<br />
propose<br />
d<br />
during<br />
next fin.<br />
year<br />
Estima<br />
ted<br />
Cost<br />
per<br />
activit<br />
y unit<br />
Total<br />
expenditure<br />
for the<br />
activity<br />
during the<br />
next fin.<br />
Year<br />
20,00,000<br />
1200000<br />
Puppet shows/ street<br />
plays/etc.<br />
School activities<br />
Print publicity<br />
- Posters<br />
- Pamphlets<br />
- Others<br />
2,20,000<br />
Media activities on<br />
Cable/local channels<br />
Radio<br />
Any other activity<br />
Opinion<br />
leaders/<br />
NGOs for<br />
advocacy<br />
Sensitization<br />
meetings<br />
Media activities<br />
Power point<br />
Presentations / one to<br />
one interaction<br />
Information<br />
Booklets/ brochures<br />
300
Health<br />
Care<br />
providers<br />
public<br />
and<br />
private<br />
Any Other<br />
Activities<br />
proposed<br />
World TB Day<br />
activities<br />
Any other public<br />
event<br />
- CMEs<br />
- Interaction<br />
meetings<br />
- one to one<br />
interaction<br />
meetings<br />
- Information<br />
Booklets<br />
- Any other<br />
Communication<br />
Facilitators (each for<br />
5-6 districts)<br />
12,00000<br />
76700<br />
13,32000<br />
Total Budget 60,28,700/-<br />
Item<br />
5. Equipment Maintenance:<br />
Computer<br />
Photocopier<br />
Fax<br />
Binocular Microscopes<br />
No.<br />
actually<br />
present<br />
in the<br />
state<br />
Amount<br />
actually<br />
spent in<br />
the last 4<br />
quarters<br />
Amount Proposed<br />
for Maintenance<br />
during current<br />
financial yr.<br />
Estimated Expenditure for the<br />
next financial year for which<br />
plan is being submitted<br />
(Rs.)<br />
(a) (b) (c) (d) (e)<br />
30 140393 750000 22,00,000<br />
28<br />
27<br />
504 15,25,000<br />
(RNTCP)<br />
STDC/ IRL Equipment 11,00,000<br />
Any Other (pl. specify)<br />
TOTAL 4825000/-<br />
Justification/<br />
Remarks for (d)<br />
301
6. Training:<br />
Activity<br />
Training of DTOs (at<br />
National level)<br />
Training of MO-TCs<br />
Training of MOs (Govt +<br />
Non-Govt)<br />
Training of LTs of DMCs-<br />
Govt + Non Govt<br />
Training of MPWs<br />
Training of MPHS,<br />
pharmacists, nursing staff,<br />
BEO etc<br />
Training of Comm<br />
Volunteers<br />
Training of Pvt<br />
Practitioners<br />
Other trainings #<br />
No.<br />
in<br />
the<br />
state<br />
No.<br />
already<br />
trained<br />
in<br />
RNTCP<br />
No. planned to be trained in<br />
RNTCP during each quarter<br />
of next FY (c)<br />
Q1<br />
Q2 Q3 Q4<br />
Expenditure<br />
(in Rs)<br />
planned for<br />
current<br />
financial<br />
year<br />
Estimated<br />
Expenditure<br />
for the next<br />
financial<br />
year<br />
(Rs.)<br />
(a) (b) (d) (e) (f)<br />
4000 3000 1500 2500<br />
2000 4000 6000 1000<br />
500 1000 1500 200<br />
Justification/<br />
remarks<br />
Re- training of MOs 400 400 400 200<br />
Re- Training of LTs of<br />
50 25 55 25<br />
DMCs<br />
Re- Training of MPWs<br />
Re- Training of MPHS,<br />
500 600 800<br />
pharmacists, nursing staff,<br />
BEO<br />
Re- Training of CVs<br />
Re-training of Pvt<br />
Practitioners<br />
TB/HIV Training of MO-<br />
TCs and MOs<br />
TB/HIV Training of STLS,<br />
LTs , MPWs, MPHS,<br />
Nursing Staff, Community<br />
Volunteers etc<br />
TB/HIV Training of STS<br />
Provision for Update<br />
Training at Various Levels<br />
#<br />
Review Meetings at <strong>State</strong><br />
Level<br />
800 700 400 200<br />
Any Other Training Activity<br />
# Please specify TOTAL Rs.52,41,000/-<br />
302
7. Vehicle Maintenance:<br />
Type of Vehicle<br />
Number<br />
permissible<br />
as per the<br />
norms in the<br />
state<br />
Number<br />
actually<br />
present<br />
Amount spent<br />
on POL and<br />
Maintenance<br />
in the<br />
previous 4<br />
quarters<br />
303<br />
Expenditure<br />
(in Rs)<br />
planned for<br />
current<br />
financial<br />
year<br />
Estimated<br />
Expenditure for the<br />
next financial year<br />
for which plan is<br />
being submitted<br />
(Rs.)<br />
(a) (b) (c) (d) (e) (f)<br />
Four Wheelers<br />
Two Wheelers 131 113 1082209 3000000 41,71,000/-<br />
TOTAL 41,71,000/-<br />
Hiring of<br />
Four<br />
Wheeler<br />
8. Vehicle Hiring*:<br />
Number<br />
permissible as<br />
per the norms in<br />
the state<br />
Number actually<br />
requiring hired<br />
vehicles<br />
Amount<br />
spent in<br />
the prev. 4<br />
qtrs<br />
Expenditure (in<br />
Rs) planned for<br />
current financial<br />
year<br />
Estimated Expenditure<br />
for the next financial<br />
year for which plan is<br />
being submitted (Rs.)<br />
Justification/<br />
remarks<br />
Justification/<br />
remarks<br />
(a) (b) (c) (d) (e) (f)<br />
For STC/<br />
STDC 95,29,600/-<br />
For DTO 30 30 1132699 4800000<br />
For MO-<br />
TC<br />
TOTAL 95,29,600/-<br />
* Vehicle Hiring permissible only where RNTCP vehicles have not been provided<br />
9. NGO/ PP Support:<br />
Activity<br />
No. of<br />
currently<br />
involved<br />
in RNTCP<br />
in the<br />
state<br />
Additional<br />
enrolment<br />
planned for this<br />
year<br />
Amount spent<br />
in the<br />
previous 4<br />
quarters<br />
Expenditure (in<br />
Rs) planned for<br />
current financial<br />
year<br />
Estimated<br />
Expenditure for the<br />
next financial year<br />
(Rs.)<br />
(a) (b) (c) (d) (e) (f)<br />
NGOs involvement<br />
scheme 1 3 19 0 Rs.161000<br />
NGOs involvement<br />
scheme 2 5 76 0 Rs.454000<br />
NGOs involvement<br />
scheme 3 2 5 0 0<br />
NGOs involvement<br />
scheme 4 3 15 0 Rs.300000<br />
NGOs involvement<br />
scheme 5 1 5 0 Rs.425313<br />
NGOs involvement<br />
unsigned<br />
Private practitioners<br />
scheme 1 0 160 10 Rs.10000<br />
Private practitioners<br />
scheme 2 134 527 0 Rs.71000<br />
Private practitioners<br />
scheme 3A 0 59 0 0<br />
Private practitioners<br />
scheme 3B 0 250 0 0<br />
Prvt Pract. scheme<br />
4A 0 3017 0 Rs.10000<br />
Justification/<br />
remarks
Pvt Pract. Scheme 4B<br />
TOTAL Rs70,00,000/-<br />
NGO/ PP Support: (New schemes w.e.f. 01-10-2008)<br />
Activity<br />
No. of<br />
currently<br />
involved<br />
in RNTCP<br />
Additional<br />
enrolment<br />
planned for<br />
this year<br />
Amount<br />
spent in<br />
the<br />
previous<br />
4<br />
quarters<br />
ACSM Scheme: TB<br />
advocacy, communication,<br />
and social mobilization<br />
SC Scheme: Sputum<br />
Collection Centre/s<br />
Transport Scheme:<br />
Sputum Pick-Up and<br />
Transport Service<br />
DMC Scheme: Designated<br />
Microscopy Cum<br />
Treatment Centre (A & B)<br />
LT Scheme: Strengthening<br />
RNTCP diagnostic<br />
304<br />
Expenditure<br />
(in Rs)<br />
planned for<br />
current<br />
financial<br />
year<br />
Estimated<br />
Expenditure for<br />
the next financial<br />
year for which<br />
plan is being<br />
submitted<br />
(Rs.)<br />
Justification/<br />
remarks<br />
(a) (b) (c) (d) (e) (f)<br />
3 10 0 75000<br />
0 20 0 0<br />
services<br />
Culture and DST Scheme:<br />
Providing Quality Assured<br />
Culture and Drug<br />
Susceptibility Testing<br />
Services<br />
Adherence scheme:<br />
Promoting treatment<br />
adherence<br />
Slum Scheme: Improving<br />
TB control in Urban<br />
Slums<br />
Tuberculosis Unit Model 2 1 0 530000<br />
TB-HIV Scheme:<br />
Delivering TB-HIV<br />
interventions to high HIV<br />
Risk groups (HRGs)<br />
3 0 0<br />
TOTAL 20,78,000/-<br />
* orZeku esa NGO/PPP ds dk;Zjr cy ds vuqlkj 2768250-00 dh jkfk iz;kZIr gksxhA<br />
10. Miscellaneous:<br />
Activity* Amount<br />
permissible as<br />
e.g. TA/DA,<br />
per the norms in<br />
Stationary, the state<br />
etc<br />
Amount spent in<br />
the previous 4<br />
quarters<br />
Expenditure (in<br />
Rs) planned for<br />
current financial<br />
year<br />
Estimated<br />
Expenditure for<br />
the next<br />
financial year<br />
(Rs.)<br />
(a) (b) (c) (d) (e)<br />
10053000 908919 5200000 90,84,000<br />
Justification/ remarks
11. Contractual Services:<br />
TOTAL 90,84,000/-<br />
* Please mention the main activities proposed to be met out through this head<br />
Category of<br />
Staff<br />
No.<br />
permissible<br />
as per the<br />
norms in the<br />
state<br />
No.<br />
actually<br />
present<br />
in the<br />
state<br />
No. planned<br />
to be<br />
additionally<br />
hired during<br />
this year<br />
Amount spent<br />
in the previous<br />
4 quarters<br />
Expenditure (in<br />
Rs) planned for<br />
current fin. year<br />
(a) (b) (c) (d) (e)<br />
TB/HIV Coord.<br />
Urban TB Coord.<br />
MO-STCS<br />
<strong>State</strong> Accountant<br />
<strong>State</strong> IEC Officer<br />
Pharmacist<br />
Secretarial Asst<br />
MO-DTC 6 4 2 40431072 4800000<br />
STS 134 110<br />
STLS 134 113<br />
TBHV 49<br />
DEO 30 20 10<br />
Accountant – part 30 18 12<br />
time<br />
Contractual LT 290 182<br />
Driver<br />
Any other<br />
contractual post<br />
approved under<br />
RNTCP<br />
Estimated<br />
Expenditure for<br />
the next financial<br />
year<br />
(Rs.)<br />
TOTAL 4,57,47,500/-<br />
Justification<br />
/ remarks<br />
* orZeku esa Contractual Staff ds dk;Zjr cy ds vuqlkj 40336000-00 dh jkfk<br />
iz;kZIr gksxhA<br />
12. Printing:<br />
Activity<br />
Printing-<strong>State</strong><br />
level:*<br />
Amount<br />
permissible<br />
as per the<br />
norms in the<br />
state<br />
Amount<br />
spent in<br />
the<br />
previous 4<br />
quarters<br />
Expenditure (in<br />
Rs) planned for<br />
current<br />
financial year<br />
Estimated Expenditure for<br />
the next financial year for<br />
which plan is being<br />
submitted<br />
(Rs.)<br />
(a) (b) (c) (d) (e)<br />
10053000 93,02,000/-<br />
Justification/<br />
remarks<br />
305
Printing- Distt.<br />
Level:*<br />
* Please specify items to be printed in this column<br />
* foxr o"kZ esa gq, NikbZ dk;Z dks ns[krs gq, 1026500-00 dh jkfk iz;kZIr gksxhA<br />
13. Research and Studies (excluding OR in Medical Colleges): Rs. 6,00,000/-<br />
Any Operational Research projects planned (Yes/No) ______________________________________<br />
(If yes, enclose annexure providing details of the Topic of the Study, Investigators and Other details)<br />
Whether submitted for approval/ already approved? (Yes/No) _______________________________<br />
Estimated Total Budget ____________________________________________<br />
306
14. Medical Colleges<br />
Activity<br />
Contractual Staff:<br />
• MO-Medical College (Total<br />
approved in state 3<br />
• STLS in Medical Colleges (Total no<br />
in state 3 )<br />
• LT for Medical College (Total no in<br />
state 3 )<br />
• TBHV for Medical College (Total<br />
no in state 3)<br />
Amount<br />
permissible as<br />
per norms<br />
Estimated Expenditure<br />
for the next financial<br />
year(Rs.)<br />
(a) (b) (c)<br />
Rs.12,96,000/- Rs.12,96,000/-<br />
Justification/<br />
remarks<br />
Research and Studies:<br />
1,00,000/-<br />
• Thesis of PG Students<br />
• Operations Research*<br />
Travel Expenses for attending<br />
STF/ZTF/NTF meetings<br />
IEC: Meetings and CME planned 7,00,000/-<br />
Equipment Maintenance at Nodal Centres<br />
* Expenditure on OR can only be incurred after due approvals of STF/ STCS/ZTF/CTD (as applicable)<br />
15. Procurement of Vehicles:<br />
Equipment<br />
4-wheeler **<br />
2-wheeler<br />
No. actually<br />
present in<br />
the state<br />
No. planned<br />
for<br />
procurement<br />
this year (only<br />
if permissible<br />
as per norms)<br />
Estimated Expenditure for the<br />
next financial year for which<br />
plan is being submitted (Rs.)<br />
(a) (b) (c) (d)<br />
8,85,000/-<br />
Justification/<br />
remarks<br />
** Only if authorized in writing by the Central TB Division<br />
307
16. Procurement of Equipment:<br />
Equipment<br />
Office Equipment<br />
(Computer, modem,<br />
scanner, printer, UPS<br />
etc.)<br />
Any Other<br />
No. actually<br />
present in the<br />
state<br />
No. planned<br />
for this year<br />
(only as per<br />
norms)<br />
Estimated Expenditure<br />
for the next financial<br />
year for which plan is<br />
being submitted (Rs.)<br />
(a) (b) (c) (d)<br />
30 0<br />
22<br />
5 395000<br />
19<br />
11 165000<br />
560000<br />
Justification/ remarks<br />
308
Section D: Summary of proposed budget for the state –<br />
Category of Expenditure Budget estimate for the coming FY 2009<br />
- 2010<br />
(To be based on the planned activities and<br />
expenditure in Section C)<br />
1. Civil works 4266000<br />
2. Laboratory materials 11050000<br />
3. Honorarium 26000000<br />
4. IEC/ Publicity 6028700<br />
5. Equipment maintenance 4825000<br />
6. Training 5241000<br />
7. Vehicle maintenance 4171000<br />
8. Vehicle hiring 9529600<br />
9. NGO/PP support 9078000<br />
10. Miscellaneous 9084000<br />
11. Contractual services 45747500<br />
12. Printing 9302000<br />
13. Research and studies 600000<br />
14. Medical Colleges 2096000<br />
15. Procurement vehicles 885000<br />
16. Procurement equipment 560000<br />
14,84,63,800/-<br />
TOTAL<br />
** Only if authorized in writing by the Central TB Division<br />
309
Annual Plan for Programme Performance & Budget for the year<br />
1 st April 2009 to 31 st March 2010<br />
<strong>State</strong>: <strong>BIHAR</strong> (World Bank)<br />
Objectives:<br />
1.3. To achieve and maintain a cure rate of at least 85% among newly detected infectious (new sputum<br />
smear positive) cases, and<br />
2.4. To achieve and maintain detection of at least 70% of such cases in the population<br />
Formatted: Bullets and Numbering<br />
This action plan and budget have been approved by the STCS.<br />
Signature of the STO__________<br />
Name : Dr. N.M.Sharma<br />
_______<br />
Section-A – General Information about the <strong>State</strong><br />
1 <strong>State</strong> Population (in lakh) (World Bank Districts) 282.57<br />
2 Number of districts in the <strong>State</strong> (World Bank Districts) 8<br />
3 Urban population 36.16<br />
4 Tribal population 0.87<br />
5 Hilly population 0<br />
6 Any other known groups of special population for specific interventions<br />
(e.g. nomadic, migrant, industrial workers, urban slums, etc.)<br />
1.55<br />
(These population statistics may be obtained from Census data /<strong>State</strong> Statistical Dept/ District plans)<br />
No. of districts without DTC: None<br />
No. of districts that submitted annual action plans, which have been consolidated in this state plan: 8<br />
Organization of services in the state:<br />
S.<br />
No.<br />
Name of the<br />
District<br />
Projected<br />
Population (in<br />
Please indicate number of<br />
TUs of each type<br />
Please indicate no. of DMCs of<br />
each type in the district<br />
Lakhs) Govt NGO Public<br />
Sector*<br />
NGO Private<br />
Sector^<br />
1 Katihar 27.47 5 0 21 1 1<br />
2 Purnia 29.20 5 0 25 0 0<br />
3 Samstipur 39.24 7 1 20 0 0<br />
4 E. Champaran 45.22 8 0 42 8 2<br />
5 Muzaffarpur 43.04 7 0 16 0 0<br />
6 Patna 54.14 10 0 9 2 0<br />
7 Vaishali 31.18 5 0 23 0 3<br />
8 Munger 13.05 2 0 28 1 0<br />
Total 282.57 49 1 184 12 6<br />
*Public Sector includes Medical Colleges, Govt. health department, other Govt. department and PSUs i.e.<br />
as defined in PMR report<br />
310
^ Similarly, Private Sector includes Private Medical College, Private Practitioners, Private Clinics/Nursing<br />
Homes and Corporate sector<br />
RNTCP performance indicators:<br />
Important: Please give the performance for the last 4 quarters i.e. Oct 07 to September 08<br />
Section B – List Priority areas at the <strong>State</strong> level for achieving the objectives planned:<br />
Name of the District<br />
(also indicate if it is<br />
notified hilly or tribal<br />
district<br />
Total<br />
number of<br />
patients<br />
put on<br />
treatment*<br />
Annualised<br />
total case<br />
detection rate<br />
(per lakh<br />
pop.)<br />
No of new<br />
smear<br />
positive<br />
cases put<br />
on<br />
treatment *<br />
Annualised<br />
New smear<br />
positive case<br />
detection rate<br />
(per lakh<br />
pop)<br />
Cure rate<br />
for cases<br />
detected in<br />
the last 4<br />
correspondi<br />
ng quarters<br />
Plan for the next year<br />
Annualized<br />
NSP case<br />
detection<br />
rate<br />
Cure rate<br />
Katihar 2390 43.01 1395 68.3 78 70 85<br />
Purnia 3016 113.32 1447 54.14 82.2 70 85<br />
Samstipur 4132 53.52 1561 54.73 79.36 70 85<br />
E. Champaran 2731 62 1160 26 85 70 85<br />
Muzaffarpur 6173 6173 1992 53 87 70 85<br />
Patna 471 471 173 45.85 87.98 70 85<br />
Vaishali 3215 3215 892 29 56 70 85<br />
Munger 1460 1460 70 85<br />
Total<br />
* Patients put on treatment under DOTS regimens only are to be included.<br />
S.No. Priority areas Activity planned under each priority area<br />
1<br />
1 a)Filling up of all <strong>State</strong> and District level Contractual<br />
Human Resource<br />
Staff .<br />
311
1 b) Filling up the posts of DTOs & MOTCs,<br />
2 Training 2 a) Training of untrained DTOs & MO TCs at National<br />
& state level and also of STS, STLS , LTs<br />
2 b) Training and Refresher trainings of MOs & Para<br />
Medical Staff<br />
2 c) Training of ASHA as DOT providers<br />
2 d)Training and retraining of All contractual staff of<br />
RNTCP<br />
3 IEC 3 a) Printing of IEC Materials for the <strong>State</strong><br />
3 b)Involvement of masses through generating awareness<br />
via the print and electronic Media.<br />
4 Involvement of other sectors/<br />
NGOs/PP<br />
3 c) Sensitisation of local MLAs and PRI members,<br />
empowering the community by making them aware of<br />
the RNTCP facilities<br />
4 a) Sensitisation workshop for other sectors, NGOs and<br />
PPs.<br />
On the revised schemes<br />
4 b) Increased involvement of Faith Based and<br />
community based organisations.<br />
4 c) Involving IMA in RNTCP in the <strong>State</strong><br />
5 Strengthening of IRL, Lab network<br />
and Implementation of EQA<br />
5 a)Starting more DMCs especially in the APHCs with<br />
the help of NGOs<br />
5 b)Construction of IRL and initiation of DOTS Plus<br />
action plan.<br />
5 c)Visit of IRL to all the 38 districts with at least one<br />
OSE and One Panel Testing.<br />
6 Minimizing Initial Defaulters 6 a) Ensuring in all districts line listing of all sputum<br />
smear +ve patients diagnosed on regular basis<br />
6 b) Regular data exchange for feedback within district<br />
regarding referral for treatment.<br />
Priority Districts for Supervision and Monitoring by <strong>State</strong> during the next year<br />
S No District Reason for inclusion in priority list<br />
1 Vaishali No contractual Supervisory Staff in the District<br />
312
(STS/STLS)<br />
Section C – Consolidated Plan for Performance and Expenditure under each head, including<br />
estimates submitted by all districts, and the requirements at the <strong>State</strong> Level<br />
1. Civil Works<br />
Activity<br />
No.<br />
required<br />
as per<br />
the<br />
norms<br />
in the<br />
state<br />
No.<br />
already<br />
upgraded/<br />
present in<br />
the state<br />
No.<br />
planned<br />
to be<br />
upgraded<br />
during<br />
next<br />
financial<br />
year<br />
Pl provide<br />
justification if an<br />
increase is<br />
planned in excess<br />
of norms (use<br />
separate sheet if<br />
required)<br />
Estimated<br />
Expenditure on the<br />
activity<br />
Quarter in which the<br />
planned activity<br />
expected to be<br />
completed<br />
(a) (b) (c) (d) (e) (f)<br />
STDC/ 1 1 1 IRL civil work By 3 rd Quarter 2009.<br />
IRL<br />
SDS 1 1 1 Inadequate<br />
Storage space<br />
By 2 nd Quarter of<br />
2009<br />
DTCs 8 8 0 - - -<br />
TUs 56 50 6 Up gradation By 2 nd Quarter of<br />
2009<br />
DMCs 282 202 20 Up gradation By 2 nd Quarter of<br />
2009<br />
TOTAL 32,46,000<br />
313
2. Laboratory Materials<br />
Activity<br />
Amount<br />
permissible<br />
as per the<br />
norms in<br />
the state<br />
Purchase of Lab<br />
Materials by<br />
Districts<br />
Lab materials for<br />
EQA activity at<br />
STDC<br />
Amount<br />
actually<br />
spent in<br />
the last 4<br />
quarters<br />
Procurement<br />
planned<br />
during the<br />
current<br />
financial<br />
year (in<br />
Rupees)<br />
Estimated<br />
Expenditure for<br />
the next financial<br />
year for which<br />
plan is being<br />
submitted<br />
(Rs.)<br />
Justification/ Remarks<br />
for (d)<br />
(a) (b) (c) (d) (e)<br />
42,375,00 10,244,34 3213066 62,07,000/- Project increase in<br />
Case detection and<br />
also increase in cost of<br />
Lab Consumables<br />
3. Honorarium<br />
Activity<br />
Honorarium for<br />
DOT providers<br />
(both tribal and<br />
non tribal<br />
districts)<br />
Honorarium for<br />
DOT providers<br />
of Cat IV<br />
patients<br />
Amount<br />
permissible<br />
as per the<br />
norms in<br />
the state<br />
Amount<br />
actually<br />
spent in<br />
the last 4<br />
quarters<br />
Expenditure<br />
(in Rs)<br />
planned for<br />
current<br />
financial<br />
year<br />
Estimated Expenditure<br />
for the next financial<br />
year for which plan is<br />
being submitted<br />
(Rs.)<br />
Justification/<br />
Remarks for<br />
(d)<br />
(a) (b) (c) (d) (e)<br />
791000 139925 651075 60,00,000* Committed<br />
honoraria to<br />
DOT<br />
Providers<br />
Community<br />
volunteers in all the<br />
districts*<br />
No. presently involved in Additional enrolment proposed for the<br />
RNTCP<br />
next fin. year<br />
1243 10,000<br />
* These community volunteers are other than salaried employees of Central/<strong>State</strong> government and are<br />
involved in provision of DOT e.g. Anganwadi workers, trained dais, village health guides, ASHA, other<br />
volunteers, etc.<br />
* orZeku esa Dot Privder dk;Zjr cy ds vuqlkj 10-00 yk[k dh jkfk iz;kZIr gksxhA<br />
4. IEC/Publicity:<br />
Permissible budget for <strong>State</strong> and all Districts as per Norms: Rs.(10,00,000 + 21,187,50)<br />
314
Estimated IEC budget for all Districts, as per action plans (please enclose consolidation summary):<br />
Rs.23,00,000<br />
Estimated IEC activities and Budget at the <strong>State</strong> level (excluding districts) for the next financial year<br />
proposed as per action plan detailed below: Rs. 23,00,000<br />
Target<br />
Group/<br />
Objective<br />
Patients<br />
and<br />
General<br />
public /<br />
for<br />
awareness<br />
generation<br />
and social<br />
mobilizati<br />
on<br />
Activity<br />
(All activities to be<br />
planned as per local<br />
needs, catering to the<br />
target groups<br />
specified)<br />
Outdoors:<br />
- wall paintings<br />
- Hoardings<br />
- Tin plates<br />
- Banners<br />
- others<br />
Outreach activities:<br />
- Patient provider<br />
interaction<br />
meetings<br />
- Community<br />
meetings<br />
- Mike publicity<br />
- Others<br />
Activities Planned at <strong>State</strong> Level<br />
No. of<br />
activities<br />
held in<br />
last 4<br />
quarters<br />
No of activities proposed in the<br />
next financial year, quarterwise<br />
Apr-<br />
Jun<br />
July-<br />
Sep<br />
Oct-<br />
Dec<br />
Jan-<br />
Mar<br />
Total<br />
activitie<br />
s<br />
propose<br />
d<br />
during<br />
next fin.<br />
year<br />
Estima<br />
ted<br />
Cost<br />
per<br />
activit<br />
y unit<br />
Total<br />
expenditur<br />
e for the<br />
activity<br />
during the<br />
next fin.<br />
Year<br />
14,00,000<br />
Puppet shows/ street<br />
plays/etc.<br />
School activities 3,00,000<br />
Print publicity<br />
- Posters<br />
- Pamphlets<br />
- Others<br />
Media activities on<br />
Cable/local channels<br />
Radio<br />
Any other activity<br />
8,00,000<br />
12,00,000<br />
Opinion<br />
leaders/<br />
NGOs for<br />
advocacy<br />
Sensitization<br />
meetings<br />
Media activities 2,00,000<br />
Power point<br />
Presentations / one to<br />
one interaction<br />
Information<br />
2,00,000<br />
Booklets/ brochures<br />
World TB Day<br />
2,00,000<br />
activities<br />
315
Health<br />
Care<br />
providers<br />
public<br />
and<br />
private<br />
Any Other<br />
Activities<br />
proposed<br />
Any other public<br />
event<br />
- CMEs<br />
- Interaction<br />
meetings<br />
- one to one<br />
interaction<br />
meetings<br />
- Information<br />
Booklets<br />
- Any other<br />
Communication<br />
Facilitators (each for<br />
5-6 districts)<br />
2,65,000<br />
Total Budget 45,65,000<br />
Item<br />
5. Equipment Maintenance:<br />
Computer<br />
(maintenance includes AMC,<br />
software and hardware upgrades,<br />
Printer Cartridges and Internet<br />
expenses)<br />
No.<br />
actually<br />
present<br />
in the<br />
state<br />
Amount<br />
actually<br />
spent in<br />
the last 4<br />
quarters<br />
Amount<br />
Proposed for<br />
Maintenance<br />
during<br />
current<br />
financial yr.<br />
Estimated<br />
Expenditure for<br />
the next<br />
financial year<br />
for which plan<br />
is being<br />
submitted<br />
(Rs.)<br />
Justification/<br />
Remarks for (d)<br />
(a) (b) (c) (d) (e)<br />
8 81,808 58,000 3,40,000 Upgradation of<br />
Computers for<br />
Windows based<br />
Epicenter +AMC<br />
Binocular Microscopes (RNTCP) 220 0 1,12,500 4,80,000<br />
STDC/ IRL Equipment 95,000<br />
Any Other ( Fax & OHP )<br />
TOTAL 9,15,000<br />
6. Training:<br />
Activity<br />
Training of DTOs (at<br />
National level)<br />
Training of MO-TCs<br />
Training of MOs<br />
(Govt + Non-Govt)<br />
Training of LTs of<br />
DMCs- Govt + Non<br />
No.<br />
in<br />
the<br />
state<br />
No.<br />
already<br />
trained<br />
in<br />
RNTCP<br />
No. planned to be trained<br />
in RNTCP during each<br />
quarter of next FY (c)<br />
316<br />
Expenditure<br />
(in Rs)<br />
planned for<br />
current<br />
financial<br />
year<br />
Estimated<br />
Expenditure<br />
for the next<br />
financial<br />
year<br />
(Rs.)<br />
Q1 Q2 Q3 Q4<br />
(a) (b) (d) (e) (f)<br />
7 9 2 2<br />
15 15 15 15<br />
30 15 10 5<br />
Justification/<br />
remarks
Govt<br />
Training of MPWs<br />
Training of MPHS,<br />
pharmacists, nursing<br />
staff, BEO etc<br />
Training of Comm<br />
Volunteers<br />
Training of Pvt<br />
Practitioners<br />
Other trainings #<br />
Re- training of MOs<br />
Re- Training of LTs of<br />
DMCs<br />
Re- Training of<br />
MPWs<br />
Re- Training of<br />
MPHS, pharmacists,<br />
nursing staff, BEO<br />
Re- Training of CVs<br />
Re-training of Pvt<br />
Practitioners<br />
150 150 150 150<br />
1000 1500 2000 4000<br />
75 100 80 120<br />
TB/HIV Training of<br />
40 40 40 40<br />
MO-TCs and MOs<br />
TB/HIV Training of<br />
STLS, LTs , MPWs,<br />
MPHS, Nursing Staff,<br />
Community<br />
Volunteers etc<br />
TB/HIV Training of<br />
STS<br />
Provision for Update<br />
Training at Various<br />
Levels #<br />
Review Meetings at<br />
<strong>State</strong> Level 1 1 1 1<br />
Any Other Training<br />
Activity<br />
# Please specify TOTAL 28,60,000<br />
7. Vehicle Maintenance:<br />
Type of Vehicle Number<br />
permissible<br />
as per the<br />
norms in<br />
the state<br />
Number<br />
actually<br />
present<br />
Amount<br />
spent on<br />
POL and<br />
Maintenance<br />
in the<br />
previous 4<br />
quarters<br />
Expenditure<br />
(in Rs)<br />
planned for<br />
current<br />
financial<br />
year<br />
Estimated<br />
Expenditure for the<br />
next financial year<br />
for which plan is<br />
being submitted<br />
(Rs.)<br />
(a) (b) (c) (d) (e) (f)<br />
Four Wheelers 8 4 5,00,000<br />
Two Wheelers 56 49 2,53,026 9,71,974 17,77,000<br />
TOTAL 22,77,000<br />
Justification/<br />
remarks<br />
317
8. Vehicle Hiring*:<br />
Hiring of Number<br />
Four permissible<br />
Wheeler as per the<br />
norms in the<br />
state<br />
Number<br />
actually<br />
requiring<br />
hired<br />
vehicles<br />
Amount<br />
spent in<br />
the prev.<br />
4 qtrs<br />
Expenditure<br />
(in Rs)<br />
planned for<br />
current<br />
financial year<br />
Estimated<br />
Expenditure for the<br />
next financial year<br />
for which plan is<br />
being submitted (Rs.)<br />
(a) (b) (c) (d) (e) (f)<br />
For STC/ 1 1 0 0<br />
STDC<br />
For DTO 4 4 1,88,628 6,51,372<br />
For MO-<br />
TC<br />
Justification/<br />
remarks<br />
50 50 Proposed to<br />
increase the<br />
no. Of TUs<br />
TOTAL 45,06,000/-<br />
* Vehicle Hiring permissible only where RNTCP vehicles have not been provided<br />
9. NGO/ PP Support:<br />
Activity<br />
No. of<br />
currently<br />
involved<br />
in<br />
RNTCP<br />
in the<br />
state<br />
Additional<br />
enrolment<br />
planned<br />
for this<br />
year<br />
Amount<br />
spent in<br />
the<br />
previous<br />
4<br />
quarters<br />
Expenditure<br />
(in Rs)<br />
planned for<br />
current<br />
financial<br />
year<br />
Estimated<br />
Expenditure<br />
for the next<br />
financial year<br />
(Rs.)<br />
(a) (b) (c) (d) (e) (f)<br />
NGOs involvement scheme 1 0 4 0 75000 Rs.100000/-<br />
NGOs involvement scheme 2 9 11 0 205000 Rs.450000/-<br />
NGOs involvement scheme 3<br />
NGOs involvement scheme 4 1 18 0 300000 Rs.265000/-<br />
NGOs involvement scheme 5 0 1 0 0 Rs.480000/-<br />
NGOs involvement unsigned 32 0 0 600000 Rs.0/-<br />
Private practitioners scheme<br />
1 0 84 0 20000 Rs.81200/-<br />
Private practitioners scheme<br />
2 0 334 0 8000 Rs.160500/-<br />
Private practitioners scheme<br />
3A<br />
Private practitioners scheme<br />
3B<br />
Prvt Pract. scheme 4A<br />
Pvt Pract. Scheme 4B<br />
TOTAL 1,01,25,000/-<br />
NGO/ PP Support: (New schemes w.e.f. 01-10-2008)<br />
Justification/<br />
remarks<br />
Activity<br />
ACSM Scheme: TB<br />
advocacy,<br />
communication, and<br />
social mobilization<br />
No. of<br />
currently<br />
involved<br />
in<br />
RNTCP<br />
Additional<br />
enrolment<br />
planned<br />
for this<br />
year<br />
Amount<br />
spent in<br />
the<br />
previous<br />
4<br />
quarters<br />
318<br />
Expenditure<br />
(in Rs)<br />
planned for<br />
current<br />
financial<br />
year<br />
Estimated<br />
Expenditure for<br />
the next<br />
financial year<br />
for which plan is<br />
being submitted<br />
(Rs.)<br />
Justification/<br />
remarks<br />
(a) (b) (c) (d) (e) (f)
SC Scheme: Sputum<br />
Collection Centre/s<br />
Transport Scheme:<br />
Sputum Pick-Up and<br />
Transport Service<br />
DMC Scheme:<br />
Designated Microscopy<br />
Cum Treatment Centre<br />
(A & B)<br />
LT Scheme:<br />
Strengthening RNTCP<br />
diagnostic services<br />
Culture and DST<br />
Scheme: Providing<br />
Quality Assured<br />
Culture and Drug<br />
Susceptibility Testing<br />
Services<br />
Adherence scheme:<br />
Promoting treatment<br />
adherence<br />
Slum Scheme:<br />
Improving TB control<br />
in Urban Slums<br />
Tuberculosis Unit<br />
Model<br />
TB-HIV Scheme:<br />
Delivering TB-HIV<br />
interventions to high<br />
HIV Risk groups<br />
(HRGs)<br />
1 5 0 75,000<br />
15 0 0<br />
9 5 0 18,00,00<br />
1 0 0 2,65,000<br />
6 0 0<br />
TOTAL 79,11,000/-<br />
* orZeku esa NGO/PPP ds dk;Zjr cy ds vuqlkj 25-00 yk[k dh jkfk izkIr gksxhA<br />
10. Miscellaneous:<br />
Activity*<br />
e.g. TA/DA,<br />
Stationary, etc<br />
Amount<br />
permissib<br />
le as per<br />
the norms<br />
in the<br />
state<br />
Amount<br />
spent in<br />
the<br />
previous 4<br />
quarters<br />
Expenditure<br />
(in Rs)<br />
planned for<br />
current<br />
financial<br />
year<br />
Estimated<br />
Expenditure<br />
for the next<br />
financial year<br />
(Rs.)<br />
(a) (b) (c) (d) (e)<br />
<strong>State</strong> Level 7,00,000 7,00,000<br />
District Level 42,37,500 2,08,047 10,50,000 45,14,000<br />
Justification/ remarks<br />
TOTAL 52,14,000<br />
* Please mention the main activities proposed to be met out through this head<br />
319
11. Contractual Services:<br />
Category of Staff<br />
No.<br />
permissible<br />
as per the<br />
norms in the<br />
state<br />
No.<br />
actuall<br />
y<br />
present<br />
in the<br />
state<br />
No.<br />
planned to<br />
be<br />
additionall<br />
y hired<br />
during this<br />
year<br />
Amount<br />
spent in<br />
the<br />
previous<br />
4<br />
quarters<br />
Expendit<br />
ure (in<br />
Rs)<br />
planned<br />
for<br />
current<br />
fin. year<br />
(a) (b) (c) (d) (e)<br />
TB/HIV Coord. 1 0 0 0 0<br />
Urban TB Coord.<br />
MO-STCS 1 0 0 0 0<br />
<strong>State</strong> Accountant 2 0 0 0 0<br />
<strong>State</strong> IEC Officer 1 0 0 0 0<br />
Pharmacist 1 0 0 0 0<br />
Secretarial Asst 1 0 0 0 0<br />
MO-DTC<br />
STS 50 45 5<br />
STLS 50 43 7<br />
TBHV 30 2 28<br />
DEO Districts 8 6 2<br />
DEO <strong>State</strong> 2 0 2 0 0<br />
Accountant – part 8 4 8<br />
time<br />
Contractual LT 120 88 32<br />
Driver 8 5 3<br />
Any other<br />
contractual post<br />
approved under<br />
RNTCP<br />
Estimated<br />
Expenditure<br />
for the next<br />
financial<br />
year<br />
(Rs.)<br />
TOTAL 2,90,82,000/-<br />
Justificatio<br />
n/ remarks<br />
12. Printing:<br />
Activity<br />
Printing-<strong>State</strong> level:*<br />
(All<br />
Modules,Guidelines,For<br />
ms,registers,IEC<br />
materials)<br />
Printing- Distt. Level:*<br />
Amount<br />
permissible<br />
as per the<br />
norms in<br />
the state<br />
Amount<br />
spent in<br />
the<br />
previous<br />
4<br />
quarters<br />
Expenditure<br />
(in Rs)<br />
planned for<br />
current<br />
financial year<br />
Estimated Expenditure for<br />
the next financial year for<br />
which plan is being<br />
submitted<br />
(Rs.)<br />
Justification/<br />
remarks<br />
(a) (b) (c) (d) (e)<br />
4237500 777337 45,74,000/- No printing<br />
carried out in<br />
the new<br />
formats,No IEC<br />
material at<br />
state /district<br />
* Please specify items to be printed in this column<br />
* foxr o"kZ esa gq, NikbZ dk;Z dks ns[krs gq, 20-00 yk[k dh jkfk iz;kZIr gksxhA<br />
320
13. Research and Studies (excluding OR in Medical Colleges): Rs. 6,00,000/-<br />
Any Operational Research projects planned (Yes/No) ______________________________________<br />
(If yes, enclose annexure providing details of the Topic of the Study, Investigators and Other details)<br />
Whether submitted for approval/ already approved? (Yes/No) _______________________________<br />
Estimated Total Budget ____________________________________________<br />
14. Medical Colleges<br />
Activity<br />
Contractual Staff:<br />
• MO-Medical College<br />
• STLS in Medical Colleges<br />
• LT for Medical College<br />
• TBHV for Medical College<br />
Research and Studies:<br />
• Thesis of PG Students<br />
• Operations Research*<br />
Travel Expenses for attending<br />
STF/ZTF/NTF meetings<br />
IEC: Meetings and CME planned<br />
Equipment Maintenance at Nodal<br />
Centres<br />
Amount<br />
permissible as<br />
per norms<br />
Estimated Expenditure<br />
for the next financial<br />
year(Rs.)<br />
(a) (b) (c)<br />
3<br />
3<br />
3<br />
3<br />
Total:28,47,200/-<br />
Justification/<br />
remarks<br />
15. Procurement of Vehicles:<br />
Equipment<br />
No.<br />
actually<br />
present in<br />
the state<br />
No. planned for<br />
procurement this<br />
year (only if<br />
permissible as per<br />
norms)<br />
321<br />
Estimated<br />
Expenditure for the<br />
next financial year for<br />
which plan is being<br />
submitted (Rs.)<br />
Justification/<br />
remarks<br />
(a) (b) (c) (d)<br />
4-wheeler **<br />
2-wheeler 43 26<br />
13,00,000/-<br />
** Only if authorized in writing by the Central TB Division<br />
16. Procurement of Equipment:<br />
Equipment<br />
Office Equipment<br />
(Computer,<br />
Photocopier<br />
No. actually<br />
present in the<br />
state<br />
LCD projector 2<br />
No.<br />
planned<br />
for this<br />
year (only<br />
as per<br />
norms)<br />
Estimated<br />
Expenditure for the<br />
next financial year<br />
for which plan is<br />
being submitted (Rs.)<br />
(a) (b) (c) (d)<br />
3<br />
3 7,80,000/<br />
Justification/<br />
remarks
Section D: Summary of proposed budget for the state <br />
Category of Expenditure<br />
Budget estimate for the coming FY<br />
2009 - 2010<br />
(To be based on the planned activities<br />
and expenditure in Section C)<br />
1. Civil works 3246000<br />
2. Laboratory materials 6207000<br />
3. Honorarium 6000000<br />
4. IEC/ Publicity 4565000<br />
5. Equipment maintenance 915000<br />
6. Training 2860000<br />
7. Vehicle maintenance 2277000<br />
8. Vehicle hiring 4506000<br />
9. NGO/PP support 18036000<br />
10. Miscellaneous 5214000<br />
11. Contractual services 29082000<br />
12. Printing 4574000<br />
13. Research and studies 600000<br />
14. Medical Colleges 2847200<br />
15. Procurement vehicles 1300000<br />
16. Procurement equipment 780000<br />
TOTAL 9,30,09,200/-<br />
** Only if authorized in writing by the Central TB Division<br />
322
Printing Details<br />
Sr No<br />
1<br />
Items name<br />
TB Register<br />
Quantity (No of<br />
copies)<br />
No of pages for print<br />
including cover<br />
(back and front)<br />
334 200 + 2<br />
2<br />
Lab Register<br />
1696 200 + 2<br />
3 Treatment Card 258552 2<br />
4 Identity Card 129276 2<br />
5 Lab form for Sputum Examination 692550 1<br />
6 TB Transfer form 6464 1<br />
7 Referral for treatment form 12928 1<br />
8 CF TU qtrly report 2672 1<br />
9 SC TU qtrly report 2672 1<br />
10 RT TU qtrly report 2672 1<br />
11 PMR TU qtrly report 2672 4<br />
12 PHI monthly Report 24422 2<br />
13<br />
14<br />
15<br />
Supervisory Registers (triplicate paging no)<br />
Desk Referance<br />
RNTCP at a glance<br />
1272 7 + (80 x 3) = 247<br />
18468 1<br />
18468 26 + 2<br />
16<br />
EQA coding (blinding) register<br />
76 100 + 2<br />
17<br />
EQA - RBRC roaster for STLSs rechecking and<br />
umpire rechecking 38 100 + 2<br />
18<br />
EQA - Register for Quality control of prepared<br />
reagents 76 100 + 2<br />
19 EQA reporting format - annexure M (for TU) 15264 1<br />
20<br />
EQA reporting format - annexure M (for district)<br />
1170 1<br />
21<br />
EQA reporting format - annexure E (for district)<br />
1170 1<br />
22 EQA reporting format - annexure B 20352 1<br />
23 EQA reporting format - Annexure C 20352 1<br />
24 EQA reporting format - Annexure D 20352 1<br />
25 EQA reporting format - checklist for STLS 20352 7<br />
26 EQA reporting format - annexure F 380 1<br />
27 EQA - IRL visit to DTC - OSE 100 10<br />
28 District Issue voucher (DIV) 16032 1<br />
29<br />
District worksheet for Reporting Drug Requirement<br />
(WRDR) 16032 1<br />
30 TU report for Reconstitution of Drugs 1670 1<br />
31 Drug Stock Register 410 200 + 2<br />
32 Line list of VCTC 9120 1<br />
33 VCTC monthly report 912 1<br />
34 Health provider guide (Local language) 18468 1<br />
35<br />
PP module<br />
9234 76<br />
323
36<br />
Revised Strategy for monitoring and supervision<br />
281 74 + 2<br />
37<br />
EQA Module - RNTCP Laboratory Network<br />
guidelines for Quality Assurance of smear<br />
microscopy for diagnosing TB.B60 256 91 + 2<br />
38 Mycobacterial Culture Sensitivity forms 6464 1<br />
39 NGO Guidelines 334 40 + 2<br />
40 PP guidelines+B20 334 40 + 2<br />
41 District Drug Store Manual 410 89 + 2<br />
42<br />
Reconstitution Register<br />
38 200 + 2<br />
43 Additional Drug Request 380 1<br />
44<br />
Referral for treatment Register<br />
205 200 + 2<br />
45<br />
RNTCP Modules with Exercise book and answer<br />
book for training of MO (1-4 Module) 4617 190 + 2<br />
46<br />
RNTCP MO training Exercise (E1, E2, E3) and<br />
answer books (EA1-3) 167<br />
(13+2) + (19+2) +<br />
(22+2) + (32+2) = 94<br />
47<br />
RNTCP Modules for training of MO-TC (5-9<br />
Module) 167 254 + 2<br />
48<br />
RNTCP Modules for training of STS with<br />
Exercise book 167 (131+2) + (26+2)<br />
49 RNTCP Modules for training of STLS 167 120 + 2<br />
50 RNTCP Modules for training of LT 923 74 + 2<br />
51<br />
RNTCP Modules for training of Medical college<br />
faculty 1150<br />
52 RNTCP Modules for training of MPWs 18468 54 + 2<br />
53 Modules for training in TB-HIV of MO 668 97 + 2<br />
54 Modules for training in TB-HIV of STS & STLS 334 63 + 2<br />
55<br />
Modules for training in TB-HIV of VCTC<br />
counsellor 200 66 + 2<br />
56 District PMR report 760 6<br />
57<br />
Strategy document for the supervision and<br />
monitoring 281 85 + 2<br />
58<br />
Guidelines for quality assuarance of smear<br />
microscopy for diagnosing tuberculosis 334 91 + 2<br />
59 Technical & operational guidelines 923 150 + 2<br />
60 One page Display for DOT Provider 18468 1<br />
61 One page Display for DOT Provider pead PWB 18468 1<br />
62<br />
Financial Management Manual for state & district<br />
societies norms and basis of costing 190 83 + 2<br />
63 Pages for Training in pediatric PWBs (Hindi) 18468 3<br />
64 Pages for Training in pediatric PWBs (English) 3040 3<br />
65 Programme review checklist for DMs & CMOs 950 2<br />
66 Quarterly report - Medical College 96 3<br />
67<br />
IE - Form 1: Review of TU reports and TB<br />
registers & Worksheet for form 1 200 1<br />
68 IE - Form 1: Worksheet for form 1 500 1<br />
69 IE - Form 2: Data collection at the district level 200 3<br />
70 IE - Form 3: Data collection at the DMC level 500 1<br />
71 IE - Form 4: Data collection at the DOT Centre 1000 1<br />
324
72 IE - Form 5:Patients Interview 500 1<br />
73 IE - Form 6 :Triangulation 200 1<br />
74<br />
75<br />
76<br />
77<br />
IE - Form 8: Form for interview of non-NSP<br />
patients 200 1<br />
IE - Form 9: Form for observations at the TU Drug<br />
store 100 1<br />
IE - Form 11: for review of the Medical College<br />
during Internal Evaluation 25 1<br />
IE - Form 12: Check List For Financial<br />
Management 500 1<br />
78 Physical Verification Sheet (PVS) 430 1<br />
79 Adequacy of Drug Stocks (ADS) 430 1<br />
80 Expiry Age Analysis of Drug Stocks (EAADS) 430 1<br />
81 Training certificates 2770 1<br />
82 Enrolment certificate (NGOs & PPs) 462 1<br />
83 Certificate of appreciation 308 1<br />
84 Pamphlets 92340 1<br />
85 Posters (Sputum Microscopy) 4617 1<br />
86 Posters (diagnosis) 9234 1<br />
87 Posters (Treatment) 9234 1<br />
88 Posters (DOTS) 9234 1<br />
89<br />
Plastic digital printed boards for Approved DOT<br />
centers 9234 1<br />
90<br />
Plastic digital printed boards for designated Pvt<br />
Sputum Microscopy centre 114 1<br />
91 Table Flip type calendars 2770 24<br />
92 Flip charts 2884<br />
93 Banners for workshop 38 1<br />
94 Banners for training 38 1<br />
95 Digital printed banners DOTS 4617 1<br />
96 Digital printed banners diagnosis 4617 1<br />
97 Digital printed banners Treatment 4617 1<br />
98<br />
RNTCP diary<br />
4617 200<br />
99 Car bumper stickers Plastic coated 9234 1<br />
325
Bihar S<strong>PIP</strong> 2009-10<br />
Malaria<br />
Filaria<br />
Kalazar<br />
326
i=kad -KA/R-12/08 @<br />
izs"kd% &<br />
MkWñ vkjñ,uñ ik.Ms;]<br />
la;qä funs'kd&lg&jkT; dk;ZØe inkf/kdkjh]<br />
eysfj;k@dkyktkj] fcgkj] iVukA<br />
lsok esa]<br />
funs'kd]<br />
jk"Vªh; oSDVj tfur jksx fu;a=.k dk;ZØe]<br />
22] 'kkeukFk ekxZ] fnYyh & 54 iVuk] fnukad % ----------------------------------<br />
fo"k;% iqu% lkksf/kr dkyktkj fu;a=k.kkFkZ foÙkh; o"kZ 2009&10 la'kksf/kr ctV izkôyuA<br />
egk'k;]<br />
mi;qZä fo"k;d v/kksgLrk{kjh ia=kd KA/R-12/08-57 fnukad 07-02-09 }kjk Hksts x;s ctV<br />
izkDyu ij Hkkjr ljdkj }kjk mBk;s x;s fcUnqvks ds laca/k esa vko';d izo`f"V djrs gq, la'kksf/kr<br />
ctV izkDyu Hkstk tk jgk gSA ctV izkdyu esa dkyktkj ds 2010 Elemination y{; dh izkfIr gsrq<br />
fujks/kkRed] mipkjkRed] jkT; eq[;ky; lqn`
miyC/k gS rFkk 'ks"k 11 ftyksa esa vko';drk ls vf/kd MhñMhñVhñ miyC/k gSA orZeku foÙkh;<br />
o"kZ esa Hkkjr ljdkj }kjk 440 ehñVu MhñMhñVhñ vkiwfrZ dh tk jgh gS ftls mUgh ftyksa esa<br />
vkiwfrZ djus gsrq Hkkjr ljdkj ls vuqjks/k fd;k x;k gS] tgk¡ vko';drk ls de MhñMhñVhñ<br />
miyC/k gSA<br />
5- 31 dkyktkj izHkkfor ftyk ls fNM+dko midj.kksa ds laca/k esa tks lwpuk izkIr gqbZ mls layXu<br />
fooj.kh ,usDpj & III esa fn[kk;k x;k gSA fooj.kh ds voyksdu ls fofnr gksxk fd dk;Z;ksX;<br />
,oa ejEefr ;ksX; midj.kksa dks feykdj vko';drk ds vuqlkj midj.k miyC/k gSaA fQj Hkh<br />
dqN ftyksa esa ;fn midj.kksa dh deh gksxh rks oSls ftyas tgk¡ vko';drk ls T;knk midj.k<br />
miyC/k gS] fopyu }kjk fNM+dko midj.kksa dh vkiwfrZ dh tk,xhA ejEefr ;ksX; midj.kksa ds<br />
ejEefr gsrq jkf'k dk izko/kku ctV esa fd;k x;k gSA<br />
6- fNM+dko ij gksus okys O;; dk enokj fooj.k bl izdkj gS % &<br />
¼ I ½ Js"B {ks=kh; dk;ZdÙkkZ & 1782 ¼etnwjh @ Rs. 113 izfrfnu dh nj ls 60 fnu dk<br />
etnwjh½ & 1782 X 60 X 113 =Rs. 1,20,81,960<br />
{ks=kh; dk;ZdÙkkZ & 8910 ¼etnwjh @ Rs. 92 izfrfnu dh nj ls 60 fnu dk<br />
etnwjh½ & 8910 X 60 X 92 = Rs. 4,91,83,200<br />
dqy etnwjh Rs.<br />
&6]12]65]160<br />
¼ftykokj fooj.kh ifjf'k"V II LraHk & 13 -------- n`"VO;½<br />
tgkW rd Deligation of Power of Payment for spraying at district level dk iz'u gS<br />
rks fNM+dko gsrq ftyks dks jkf'k miyC/k djk;h tkrh gS mldk mi;ksx @ O;; ftyk<br />
dk;Zdze inkf/kdkjh }kjk gh fu;ekuqlkj fd;k tk;sxkA O;; esa ftyk LokLF; lfefr ds<br />
inkf/kdkjh dk vuqeksnu fy;k tk;sxkA<br />
fNM+dko esa dk;Z djusokys etnwj foxr o"kksZa esa Hkh fNM+dko fd;s gS] vr% fNM+dko<br />
etnwjksa dh fNM+dko dh rduhdh tkudkjh gS] fQj Hkh etnwjksa dks fNM+dko ds iwoZ<br />
,d fnu dk izf'k{k.k fn;k tkrk gSA lacaf/kr ftyksa ds ftyk dk;ZØe inkf/kdkjh<br />
fNM+dko ds iwoZ ,d fnu dk if'k{k.k lqfuf'pr djsaxsA bl esa izf'k{k.k dks fNM+dko<br />
vof/k ds ekuo fnol esa x.kuk fd;k tk,xkA<br />
¼II½ dk;kZy; O;; ,oa vkDlfedrk % &<br />
izR;sd fNM+dko ny esa fNM+dko dk;Z esa iz;ksx gksus okys vko';d lkekuksa ;Fkk xs: feêh]<br />
jftLVj] lknk dkxt] isu] Nék ds fy, diM+k] XyOl bR;kfn ds fufer izfr fNM+dko ny<br />
#i;s 150@& dk;kZy; O;; en es ,ao #i;s 150@& vkDlfedrk en esa jkf'k dk izko/kku<br />
fd;k x;k gSA ftyk dk;ZØe inkf/kdkjh] izR;sd fNM+dko ny dks mijksä lkexzh miyC/k<br />
djkuk lqfuf'pr djsaxsA bl en ls ftyk eq[;ky; esa iz;ksx gksusokys LVs'kujh Ø; dk Hkh<br />
izko/kku gS % &<br />
dk;kZy; O;; & fNMdko ny X 150 ¼1782X 150½ & 267300 #i;s<br />
vkDlfedrk &fNMdko ny X 150 & ¼1782X150½&#i;s 2]67]300@&<br />
dqy & #i;s 5]34]600@&<br />
¼ftykokj fooj.kh ifjf'k"V II LraHk & 14 ,oa 15 n`"VO;½<br />
¼III½ fNM+dko gsrq MhñMhñVhñ dh
ftyk eq[;ky; ls iz[k.M rd @ Rs. 1,000/-<br />
izfr izHkkfor iz[k.M dh nj ls ¼310 X 1]000½ & #i;s 3]10]000@&<br />
iz[k.M eq[;ky; ls LFky rd @ Rs. 500/-<br />
izfr izHkkfor iz[k.M dh nj ls ¼310 X 500½ & #i;s 1]55]000@&<br />
dqy &#i;s 4]65]000@&<br />
¼ftykokj fooj.kh ifjf'k"V II LraHk & 16 ,oa 17 n`"VO;½<br />
¼IV½ fNM+dko esa O;ogkj gksusokys fNM+dko midj.kksa ¼ejEefr ;ksX; midj.kksa ds½ ejEefr<br />
gsrq] fNM+dko ds nkSjku fNM+dko midj.kksa ds ejEefr ,oa LVhji iEi gsrq pqVdh oklj]<br />
xSyu lqrk bR;kfn ds fy, jkf'k dk izko/kku izfr fNM+dko ny #i;s 100@& ,oa<br />
uksty VhIl ds Ø; gsrq izfr izfr fNM+dko ny #i;s 400@&dh nj ls jkf'k dk<br />
izko/kku fd;k x;k gSA C;; C;ksjk bl izdkj gS % &<br />
¼d½ fNM+dko midj.kksa dh ejEefr ,oa oklj bR;kfn ds Ø; gsrq<br />
izfr fNM+dko ny #i;s 100@& 1782 X100 & Rs. 1]78]200@&<br />
¼[k½ uksty VhIl ds fy, izfr fNM+dko ny #i;s 400@&<br />
1782X400&Rs. 7]12]800@&<br />
dqy &Rs. 8]91]000@&<br />
¼ftykokj fooj.kh ifjf'k"V IV dkWye 5 rFkk 6 n`"VO;½<br />
ftyksa ls izkIr fNM+dko midj.kksa dh miyC/krk dk ftykokj fooj.k ifjf'k"V III esa<br />
n'kkZ;k x;k gSA fNM+dko ds vuqlkj mä ifjf'k"V III eas LVhji iEi] okYVh] xSyu<br />
estj] ikS.M Ekstj rFkk uksty VhIl dh vko';drk rFkk ftyksa eas miyC/k midj.kksa<br />
dk C;kSjk n'kkZ;h xbZ gSA fooj.kh ds voyksdu ls Li"V gksxk fd vf/kdka'kr% ftyksa esa<br />
vko';drk ls T;knk midj.k miyC/k gS ftu ftyksa esa ejEefr ds mijkar Hkh<br />
vko';drk ls de midj.k miyC/k gksaxs] mu ftyksa esa fopyu }kjk vU; ftysa ¼tgk¡<br />
vko';drk ls vf/kd midj.k gS½ ls fNM+dko midj.k miyC/k djk;k tk,xkA<br />
¼V½ i;Zos{k.k % & jkT; ds 31 dkyktkj izHkkfor ftyksa ds foxr ik¡p o"kksZ esa dkyktkj<br />
ls izHkkfor lHkh xzkeksa esa fNM+dko djk;k tkuk gSA fNM+dko ds lQy lapkyu ,oa<br />
xq.koÙkk iw.kZ fNM+dko dh n`f"V ls i;Zos{k.k ,oa ewY;kadu vko';d gSAi;Zos{k.k ftyk<br />
Lrj ,oa iz[k.M Lrj ds inkf/kdkjh ,oa deZpkjh }kjk fd;k tkrk gSA<br />
31 ftyksa esa ls 20 ftyksa esa ftyk eysfj;k inkf/kdkjh dk in l`ftr gS] 'ks"k<br />
11 ftysa esa in l`ftr ugha gSA bu ftyksa esa ek=k i;Zos{k.k dk nkf;Ro ftysa ds vij<br />
eq[; fpfdRlk inkf/kdkjh dks fn;k tk jgk gSA bl fufer ftyk Lrj ij vij eq[;<br />
fpfdRlk inkf/kdkjh@ftyk eysfj;k inkf/kdkjh dh xkM+h gsrq jkf'k miyC/k djkbZ tk<br />
jgh gSA e/ksiqjk rFkk [kxfM+;k ftys ds flfoy ltZu }kjk i;Zos{k.k dk;Z fd;k<br />
tk,xkA<br />
ifjf'k"V I ds LraHk 13 ds voyksdu ls Kkr gksxk fd dqN ftyksa esa izHkkfor<br />
xzkeksa dh la[;k vf/kd gS rks dqN ftyksa esa de gSA vr% i;Zos{k.k gsrq jkf'k izHkkfor<br />
xzkeksa dks vk/kkj eku dj fn;k tk jgk gSaA izR;sd inkf/kdkjh ,d fnu ¼Hkze.k ds fnu½<br />
esa de&ls&de 6 xzkeksa ds fNM+dko dk i;Zos{k.k lqfuf'pr djsaxsA<br />
ftu ftyksa esa xkM+h miyC/k gS] mu ftyksa esa jkf'k dk mi;ksx xkM+h esa mi;qä<br />
gksus okys bZa/ku ij fu;ekuqlkj fd;k tk,xkA ftu ftyksa esa xkM+h miyC/k ugha gS os<br />
ftys HkkMs+ ij xkM+h ¼jkT; Lokñ lfefr] fcgkj iVuk }kjk fu/kkZfjr nj ij½ ysdj<br />
i;Zos{k.k dk;Z djsaxsA<br />
iz[k.M Lrj ij i;Zos{k.k gsrq iz[k.M ds fpñinkñ izfr izHkkfor xzke dh nj ls<br />
jkf'k miyC/k djkbZ tk,xhA iz[k.M ds fpñinkñ Hkze.k dh frfFk dks de&ls&de 6<br />
xzke dk i;Zos{k.k lqfuf'pr djsaxsA bl fufer vko';drk ds rgr~ HkkM+s ij Hkh ogu<br />
fy;k tk ldrk gS] tSlk fd Åij mYys[k fd;k x;k gSA<br />
9 ftyksa ds vij eq[; fpñinkñ ,oa 2 ftys [kxfM+;k] e/ksiqjk ds flfoy ltZu &<br />
¼izHkkfor xzke X100½ 1783X 100 & 1]78]300@&<br />
20 ftyksa ds ftñ eñinkñ &<br />
329
¼izHkkfor xzke X100½ 9031X 100 & 9]03]100@&<br />
31 ftyksa ds iz[k.M fpñinkñ &<br />
¼izHkkfor xzke X 50½ 10814X50 & 5]40]700@&<br />
dqy &Rs. 16]22]100 @&<br />
iz[k.M Lrj dh jkf'k ftyk dk;ZØe inkf/kdkjh }kjk iz[k.M fpñinkñ dks miyC/k<br />
djkbZ tk,xhA ¼ftyk fooj.kh ifjf'k"V IV LraHk 8]9 ,oa 10 nz"VO;½<br />
¼VI½ i;Zos{kh inkf/kdkjh@deZpkjh dk nSfud HkÙkk % &<br />
ek=k MhñMhñVhñ fNM+dko esa layXu i;Zos{kh inkf/kdkjh ,oa deZpkjh dks nSfud HkÙkk<br />
¼fu;ekuqlkj½ fn;k tk,xkA bl fufer izfr dkyktkj izHkkfor iz[k.M ds fy, #i;s<br />
1]000@& dh nj ls jkf'k dk vkdyu fd;k x;k gSA pw¡fd iz[k.M ds ek= izHkkfor<br />
xzkeksa dk gh fNM+dko fd;k tk jgk gSA iwjs iz[k.M dk ughaA bls eísutj j[krs gq, gh<br />
jkf'k dk vkdyu fd;k x;k gSA izLrkfor jkf'k &izHkkfor izk- Lok- dsUnz dh la[;k<br />
X1]000 & 310X 1]000 & #i;s 3]10]000@&<br />
¼ftyk fooj.kh ifjf'k"V IV LraHk 11 nz"VO;½<br />
(VII) vkbZñbZñlhñ % & fNM+dko ds iwoZ tu lk/kkj.k esa fNM+dko ds Qk;ns fNM+dko ds frfFk<br />
dh tkudkjh dh n`f"V ls bl en esa izfr izHkkfor iz[k.M #i;s 1]000@& dh nj ls<br />
jkf'k dk izko/kku fd;k x;k gSA ftyk Lrjh; dk;ZØe inkf/kdkjh iksLVj]bR;kfn ds<br />
ek/;e ls izpkj&izlkj djk;saxsA bl en dh jkf'k iz[k.M fpñinkñ dks #i;s 500@&<br />
izfr iz[k.M dh nj ls miyC/k djkbZ tk,xhA iz[k.M fpñinkñ izHkkfor xzkeksa esa<br />
fNM+dko ds iwoZ
Øe<br />
lañ<br />
lHkh izos{kh inkf/kdkjh ,oa deZpkjh dks vko';d funsZ'k fn;k tk;sxkA jkT; Lrj ds<br />
izosZ{kh inkf/kdkjh }kjk ftyksa ds Hkze.k ds nkSjku bl ij dM+h fuxjkuh j[kh tk;sxhA<br />
lcaf/kr {ks=h; eysfj;k inkf/kdkjh ,oa ftyk dk;Zdze inkf/kdkjh dks fNM+dko dh<br />
'kr izfr'kr xq.koÙkk lqfuf'pr djkus dk nkf;Ro fn;k tk;sxkA<br />
Qjojh&ekpZ] 2009 esa dkyktkj MhñMhñVhñ fNM+dko gsrq izLrkfor ctV dk ljka'k % &<br />
Ekn jkf'k ftyk dk;ZØe inkñdks dkyktkj<br />
izHkkfor ftyksa ds fooj.kh<br />
vuqlkj<br />
1- etnwjh 6]12]65]160@& rFkSo<br />
2- ¼i½ dk;kZy; O;;<br />
2]67]300@& rFkSo<br />
¼ii½ vkDlfedrk O;;<br />
2]67]300@&<br />
3- MhñMhñVhñ
tgkW rd Hkkjr ljdkj QSeyh odZj dks izksRlkgu jkf'k nsus laca/kh izLrko<br />
nsus dk lq>ko gS] rks bl fufer vk'kk dk;ZdÙkk dks izksRlkgu jkf'k nsus dks<br />
izko/kku ctV esa fd;k x;k gSA blds vfrfjDr vU; Health activist }kjk<br />
dkyktkj ds lEHkkfor jksxh yk;s tkus ij jksxh dks dkyktkj jksx lEiq"V<br />
gksus ds mijkUr iq.kZ fpfdRlksijkUr izksRlkgu jkf'k fn;k tk;sxkA<br />
¼2½ {kfriwfrZ jkf'k % &<br />
dkyktkj ds vf/kdka'k jksxh xjhc oxZ ds gksrs gS] tks etnwjh dj viuk thou fuokZg<br />
djrs gSA ,sls yksx >qXxh&>ksiM+h esa lqnwj nsgrh bykdksa esa jgrs gS] tgk¡ ls bykt gsrq<br />
ljdkjh vLirkyksa eas vkus esa dfBukbZ ds vfrfjä bykt djkus ds fy, ljdkjh<br />
vLirky esa fpfdRlk ds nkSjku 20&30 fnuksa rd jguk iM+rk gSA ftlls mudk nSfud<br />
etnwjh ckf/kr gks tkrk gS vkSj mUgsa vkfFkZd ladV dh nksgjh ekj gks tkrh gSA nSfud<br />
etnwjh rks ugha feyrh] vyx ls bykt ij Hkh O;; gks tkrk gSaA ifj.kkeLo:I<br />
dkyktkj ds ,sls jksxh ljdkjh laLFkkuksa esa fpfdRlk vof/k ¼vf/kdre 30 fnu½ rd<br />
Je {kfriwfrZ jkf'k nh tk,xhA<br />
izLrkfor jkf'k & dkyktkj jksfx;ksa dh la[;k×fpfdRlk vof/k×{kfriwfrZ jkf'k<br />
¾33]000X30X50¾Rs. 4]95]00]000@& ¼ifjf'k"V V LraHk 6 nz"VO;½<br />
¼3½ iz[k.M vLirky es 'k';k dk foLrkj % &<br />
{ks=k Hkze.k ds nkSjku ,slk ik;k x;k gS fd izkñLokñ dsUnz ds vLrirkyksa esa 'k';k dh<br />
deh ds dkj.k dkyktkj ds ejhtksa dks tehu ij foLrj yxkdj bykt fd;k tkrk<br />
gS] tks fpfdRlk dh n`f"V ls mfpr ugha gSA dkyktkj jksx ds lHkh jksfx;ksa dks 'k';k<br />
miyC/k gks ldsa bl n`f"V ls izR;sd izkñLokñ dsUnz ds vLirkyksa esa vfrfjä nl 'k';k<br />
yxk;k tk;A fnukad 29&30 fnlEcj] 2008 dks vk;ksftr cSBd esa Hkh bl fcUnq ij<br />
lgefr cuh FkhA<br />
bl fufer ,d 'k';k ds fy, vuqekfur jkf'k 1]000@& #i;s izfr 'k';k ¼Bed with<br />
Mattress) dk izko/kku fd;k x;k gSA<br />
izLrkfor jkf'k & dkyktkj izHkkfor iz[k.Mksa dh la[;k×'k';k ×nj ¾<br />
310X10 X1]000 ¾Rs. 31]00]000@& ¼ifjf'k"V V LraHk 7 nz"VO;½<br />
¼4½ iosZ{k.k % &<br />
Dkyktkj ds fu;a=k.k esa iosZ{k.k ,d egRoiw.kZ fgLlk gSA ;fn iwjs o"kZ esa ftyk Lrj ,oa<br />
iz[k.M Lrj ls l{ke iosZ{k.k fd;k tk, rks dkyktkj ds fu;a=k.k dk y{; izkIr fd;k<br />
tk ldrk gSA iosZ{k.k ds rgr~ MhñMhñVhñ fNMdko] jksfx;ksa dk fpfdRlk] vuqJo.k]<br />
izfrosnuksa dk lle; izs"k.k bR;kfn vkrs gSA o"kZ esa nks pØ MhñMhñVhñ fNMdko vof/k<br />
vFkkZr~ 4 ekg ds iosZ{k.k dk ctV izko/kku vkbñvkjñ ,lñ ds rgr~ fd;k x;k gSA 'ks"k<br />
vkB ekg ds iosZ{k.k gsrq mipkjkRed dkjZokbZ esa izko/kku fd;k tkuk gSA<br />
iosZ{k.k dk nkf;Ro ftyk Lrj ij ftyk dk;ZØe inkf/kdkjh ,oa iz[k.M Lrj ij<br />
iz[k.M fpfdRlk inkf/kdkjh dk gSA jkT; ds 31 dkyktkj izHkkfor ftyksa eas ek=k 20<br />
ftysa esa gh ftyk eñinkf/kdkjh dk in l`ftr gS 'ks"k 11 ftyksa esa bUgha ftyk eysfj;k<br />
inkf/kdkjh ds v/khu vkrs gSA lQy iosZ{k.k dh n`f"V ls izR;sd ftyk esa ,d ftyk<br />
Lrjh; ios{k.kh inkf/kdkjh gksuk pkfg,A bl fufer 20 ftyksa ds iosZ{k.k dk nkf;Ro<br />
ftyk eysfj;k inkf/kdkjh dks] 9 ftyksa ds vij eq[; fpfdRlk inkf/kdkjh dks rFkk<br />
'ks"k nks ftysa ¼[kxfM+;k vkSj e/ksiqjk½ ds flfoy ltZu fn;k tk jgk gSA<br />
fNM+dko vof/k ¼pkj ekg½ esa iosZ{k.k ds fy, jkf'k dk izko/kku layXu ifjf'k"V IV esa<br />
fn;k x;k gSA 'ks"k vkB ekg ds fy, jkf'k dk izko/kku layXu ifjf'k"V V esa fd;k x;k<br />
gSA ifjf'k"V V ds LraHk 8 esa flfoy ltZu e/ksiqjk ,oa [kxfM+;k dks 3]000@& izfr<br />
ekg dh nj ls ifjf'k"V V ds LraHk 9 eas vij eq[; fpfdRlk inkf/kdkjh ¼vjfj;k]<br />
vjoy] ckadk] cDlj] tgkukckn] fd'kuxat] y[khljk;] f'kogj ,oa lqikSy½ dks #i;s<br />
10]000 @& #i;s izfr ekg dh nj ls rFkk 'ks"k 20 ftyksa ds ftyk eysfj;k<br />
inkf/kdkjh dks #i;s 10]000@& izfrekg dh nj ls jkf'k dk izko/kku fd;k x;k gSA<br />
332
eysfj;k ,oa dkyktkj ;kstuk ds lQy lapkyu esa ;kstuk esa dk;Zjr eysfj;k<br />
fujh{kdksa dh vge~ Hkwfedk gksrh gSA izR;sd ftysa eas inkLFkkfir eysfj;k fujh{kd ds nks<br />
;k rhu iz[k.Mksa ds dk;Z dk nkf;Ro gSA vr% iz[k.M Lrj ij iosZ{k.k gsrq eysfj;k<br />
fujh{kd dks eksVj lkbZfdy miyC/k djkus dk izko/kku fd;k tk jgk gSA jkT; ds<br />
dkyktkj izHkkfor 31 ftyksa esa 21 ftyk es eysfj;k inkf/kdkjh dk;kZy; vofLFkr gSA<br />
bu 21 ftyksa eysfj;k inkf/kdkjh dk;kZy; esa ls 18 ftyksa esa inLFkkfir eysfj;k<br />
fujh{kd izfr ftyk nks eksVj lkbZfdy rFkk 3 ftyk ¼lgjlk] iwf.kZ;k rFkk eqaxsj½ dks<br />
izfr ftyk 3 dh nj ls eksVjlkbZfdy nsus dk izLrko fn;k tk jgk gSA bl rjg dqy<br />
¼18×2+3×3½ ¾ 45 eksVj lkbZfdy ds Ø; dk izLrko gSA ,d eksVlkbZfdy dh dher<br />
50]000@ & #i;s j[kk x;k gSA<br />
eysfj;k fujh{kd dks eksVj lkbZfdy ij izfrekg 30 yhVj izfr eksVj lkbZfdy<br />
izfrekg dh nj ls nsus dk izLrko gSA ftlds fy, #i;s 50@& izfr yhVj dh nj ls<br />
jkf'k dk vkdyu ifjf'k"V V esa fd;k x;k gSA<br />
blds vfrfjDr i;Zos{k.k gsrq Hkkjr ljdkj }kjk izR;sd dkyktkj izHkkfor ftyks esa<br />
dkyktkj rdfudh ¼KTS½ dk 6 in l`ftr djus dk funs'k fn;k x;k gSA bl rjg<br />
31 dkyktkj izHkkfor ftyks esa 186 ¼KTS½ ds in ds l`tu ,oa fu;qfDr ifdz;kUrxZr<br />
gS ¼KTS½ dks izfrekg 10]000@& :i;s osru fn;k tk;sxkA ftlds fy, jkf'k dk<br />
izko/kku fd;k tk jgk gSA pwfd fo'o cSd }kjk ¼KTS½ dks dkyktkj dk;Zdze esa j[kk<br />
tk jgk gS vr% blij gksus okys O;; dk ogu fo'o cSd }kjk djus dk izko/kku gSA<br />
izLrkfor jkf'k bl izdkj gS % &<br />
¼a½ nks flfoy ltZu dks #i;s 3]000@&<br />
izfrekg dh nj ls vkB ekg ds fy, &<br />
¼b½<br />
¼c½<br />
¼d½<br />
¼e½<br />
¼3]000 ×2×8½ ¾ 48]000@&<br />
9 ftyksa ds vij eq[; fpfdRlk inkf/kdkjh<br />
dks #i;s 3]000@& izfrekg dhnj ls vkB<br />
ekg ds fy, ,oa 20 ftyksa dks ftyk<br />
eysfj;k inkf/kdkjh dks & 29 ×10]000×8 ¾ 23]20]000@&<br />
eysfj;k fujh{kd ds eksVj lkbZfdy Ø; gsrq<br />
izfr eksVjlkbZfdy #i;s<br />
50]000@& dh nj ls 45 ×50]000 ¾ 22]50]000@&<br />
eksVjlkbZfdy ds fy, isVªkWy [kjhn gsrq<br />
izfr eksVjlkbfdy izfrekg 30 yhVj #i;s 50@&izfryhVj<br />
45 ×30×50×12 ¾ 8]10]000@&<br />
186 dkyktkj rduhdh i;Zsos{kd dks<br />
:i;s 10]000@&izfrekg dh nj ls 12 ekg ds fy,<br />
186X10]000X12<br />
= 2]23]20]000@&<br />
dqy ;ksx<br />
= 2]77]48]000@&:i;s<br />
¼5½<br />
¼ifjf'k"V V LraHk 8] 9] 10 rFkk 11 nz"VO;½<br />
eksVj lkbZfdy ds Ø; ds mijkar ,d c"kZ ds lfoZfalax bR;kfn dh xkjaVh dEiuh }kjk<br />
nh tkrh gSA vr% o"kZ 2009&10 esa j[k&j[kko ds fy, jkf'k dk izko/kku ugha fd;k<br />
x;k gSA<br />
dkyktkj dh nok ,EQksVsjhlhe ohñ dk HkaMkj.k O;oLFkk % &<br />
dkyktkj jksfx;ksa ds fpfdRlk gsrq Hkkjr ljdkj }kjk ,lñ,lñthñ ,EQkVsjhlhu oh<br />
dh nok dh vkiwfrZ dh tkrh gSA ,EQkVsjhlhu nok dh ,d fu/kkZfjr rkiØe ¼2 ls 8 0<br />
C½ ij j[kk tk tkuk gS] vU;Fkk nok dh {kerk dsa Ðgkl gksus dh laHkkouk gSA<br />
fu/kkZfjr rkiØe ij nok HkaMkj.k ds fy, 'khr J`[kyk@'khrx`g gh mi;qä gSA<br />
333
ftu ftyksa esa 'khr J`[kyk miyC/k gS bu ftyksa ds flfoy ltZu nok dks 'khr J`[kyk<br />
esa j[ksaxsA ftu ftyksa esa 'khr J`[kyk miyC/k ugha gS mu ftyksa esa 'khr x`g ¼Cold<br />
Storage½ esa nok j[kus dk izLrko gSA bl fufer izR;sd ftys dks mä nok HkaMkj.k<br />
gsrq ¼'khr J`[kyk miyC/k ugaha jgus ij dksYM LVksjst HkkM+s ij ysus gsrq½ #i;s<br />
500@& izfrekg dh nj ls ,d o"kZ ds fy, jkf'k dk izko/kku fd;k x;k gSA jkT;<br />
Lrj ij ¼jkT; dk;ZØe inkf/kdkjh½ Hkh mä nok ds HkaMkj.k gsrq 'khr x`g dh<br />
vko';drk gS] ftlds fy, #i;s 1500@& izfr ekg dh nj ls jkf'k dk izko/kku<br />
fooj.kh V LraHk 12 esa esa fd;k x;k gSA<br />
izLrkfor jkf'k &<br />
¼1½ ftyk Lrj ij HkaMkj.k gsrq #i;s 500 @& izfrekg<br />
dh nj ls ,d o"kZ ds fy, 31 X 500X 12 ¾ #i;s 1]86]000@&<br />
¼II½ jkT; Lrj ij HkaMkj.k gsrq #i;s 1]500 @& izfrekg<br />
dh nj ls ,d o"kZ ds fy, 1]500X 12 ¾ #i;s 18]000@&<br />
¼ifjf'k"V V LraHk 12 nz"VO;½<br />
6- fpfdRlk dkMZ % &<br />
dkyktkj jksfx;ksa ds fpfdRlk ds Øe esa nh tkusokyh nok ds [kqjkd dk<br />
ys[kk&la/kkj.k ,oa fpfdRlk C;ksjk ds fy, fpfdRlk dkMZ dk mi;ksx fd;k tkuk<br />
vko';d gS orZeku esa fpfdRlk dkMZ dk mi;ksx ftyk Lrj ds vLirky ls ysdj<br />
iz[k.M Lrj ij ugha fd;k tk jgk gS] ftlds dkj.k rduhdh ewY;kadu eas dfBukbZ<br />
gksrh gSA 'kh"kZ Lrj ij Hkh fpfdRlk dkMZ la/kkj.k ugha fd;s tkus ij fpark trkbZ xbZ<br />
gSA<br />
vr% fpfdRlk dkMZ ds mi;ksx dh egÙkk dks ns[krs gq, izfr jksxh 2 izdkj ds dkMZ dh<br />
vko';drk gksxhA ,d dkMZ dh NikbZ eas vuqekfur #i;s 2-50 O;; gksxkA bl rjg<br />
,d ¼,d jksxh ds fy, nks dkMZ ds fglkc ls ½ izfr jksxh ij 5@& #i;s O;; gksxkA<br />
ifjf'k"V V LraHk 4 esa o"kZ 2009 ds laHkkfor jksfx;ksa dh la[;k ds vuqlkj LraHk 13<br />
esa ftykokj jkf'k dk vkdyu fd;k x;k gSA<br />
izLrkfor jkf'k & jksfx;ksa dh la[;k nj ¼33]00X 5½ ¾ #i;s 1]65]000@&<br />
¼ifjf'k"V V LraHk 13 nz"VO;½<br />
7- dkyktkj jksfx;ksa dk lwpuk la/kkj.k iath % &<br />
dkyktkj jksfx;ksa ds foLr`r lwpuk ds la/kkj.k ,oa {ks=kh; Je {kfriwfrZ Hkkx ds<br />
la/kkj.k gsrq izR;s dkyktkj izHkkfor iz[k.M esa nks jftLVj j[kus dk izko/kku fd;k<br />
x;k gS rkfd 'kh"kZ Lrj ds inkf/kdkjh }kjk Hkze.k ds nkSjku jksfx;ksa dh foLr`r lwpuk<br />
,oa nSfud Je {kfriwfrZ jkf'k dk ewY;kdau fd;k tk ldsaA bl fufer izR;sd dkyktkj<br />
izHkkfor ftys ds dkyktkj izHkkfor izk- Lok- dsUnz dks nks jftLVj ¼,d ftLrk dk½<br />
vuqekfur dher #i;s 50@& ¼nks jftLVj½ dh nj ls jkf'k dk vkdyu fd;k x;k<br />
gSA<br />
izLrkfor jkf'k & 31 ftyk ds dkyktkj izHkkfor izk- Lok- dsUnz dh la[;k × nj<br />
310X50 ¾ 15]500@&<br />
¼ifjf'k"V V LraHk 14 nz"VO;½<br />
8- MhñMhñVhñ dk Hk.Mkj.k % &<br />
MhñMhñVhñ fNM+dko ds fy, Hkkjr ljdkj }kjk ftyksa esa MhñMhñVhñ dh vkiwfrZ dh tkrh<br />
gSA ftyksa es MhñMhñVhñ ds Hk.Mkj.k dh leqfpr O;oLFkk ugha jgus ds dkj.k MhñMhñVhñ<br />
{kfrxzLr ¼/kwi ,oa ikuh ls½ gksus dh laHkkouk gSA leqfpr Hk.Mkj.k O;oLFkk dks eísutj<br />
j[krs gq, ;k rks Hk.Mkj] HkkM+s ij fy;k tk; ;k ftyksa ds miyC/k jkT; HkaMkj fuxe<br />
ds xksnke esa j[kk tk;A<br />
Pkw¡fd ftyksa dks HkkM+s ij HkaMkj ysus esa fu;ekuqlkj iz'kklfud Lohd`fr ysus es dkQh<br />
dfBukbZ gksrh gSA Qyr% tc rd HkaMkj.k dh O;oLFkk ugha gksrh gSA rc rd<br />
334
MhñMhñVhñ dks ;=&r= j[kuk iM+rk gSA bl fufer HkkM+s ij xksnke ysus vFkok jkT;<br />
HkaMkj fuxe ¼ftldk nj ljdkj }kjk vuqeksfnr gS½ ds xksnke esa HkaMkj.k gsrq izfr<br />
ftyk izfr ekg #i;s 5]000@& dh nj ls iwjs o"kZ ds fy, jkf'k dk izko?kku fd;k<br />
x;k gSA<br />
izLrkfor jkf'k & 31X 5000X 12 ¾ 18]60]000@&<br />
¼ifjf'k"V V LraHk 15 nz"VO;½<br />
9- dkyktkj [kkst Ik[kokjk& dfri; dkj.kks ls lHkh dkyktkj ds jksxh dk iÙkk ugh<br />
py ikrk gS ftlls dkyktkj mUewyu y{; izkIr ugh gks jgk gSA dkyktkj o"kZ<br />
fnlEcj esa 15 fnuks dk [kkst Ik[kokjk eukus dk izLrko gSA[kkst Ik[kokjk jkT; ds 31<br />
dkyktkj izHkkfor ftyks ds lHkh iz[k.Mks esa euk;k tk;sxkA<br />
[kkst i[kokjk ds egRrk dks vke tu ds tkudkjh gsrq [kkst Ik[kokjk ds iwoZ pkj fnu<br />
izpkj xkM+h lHkh iz[k.Mks esa Hkstdj izpkj izlkj fd;k tk;sxk blds vfrfjDr lHkh<br />
iz[k.Mks esa iksLVj] iEiysV] cSuj bR;kfn ds }kjk Hkh [kkst i[kokjk ds laca/k esa izpkj<br />
izlkj fd;k tk;sxkA bl fufer vko';d jkf'k dk izko/kku otV izkdDyu esa fd;k<br />
x;k gSA izpkj xkM+h gsrq :i;s 750@& izfr izk0Lok0dsUnz dh nj ls 4 fnuks ds fy,<br />
jkf'k dk izko/kku fd;k x;k gSAizkLrkfor jkf'k bl izdkj gS%&<br />
izpkj okgu gsrq 338 iz[k.Mks ds fy, :i;s 750@&<br />
izfr okgu dh nj ls 4 fnuksa ds fy,& ¼338X750X4½ & 10]14]000@&<br />
iksLVj] iEiysV cSuj gsrq izfr izk0Lok0 dsUnz :i;s 1000@&<br />
dh nj ls &¼338X1000½ & 3]38]000@&<br />
dqy<br />
& 13]52]000@&<br />
10- Arrest Cases of Kalazar & o"kZ 2010 rd dkyktkj Elemenation y{; dks izkIr<br />
djus ds fy, lHkh dkyktkj jksfx;ks dks iw.kZ mipkj fd;k tk;sxk rFkk izHkkfor {ks=ks<br />
esa fujks/kkRed dkjokbZ ds rgr o"kZ esa nks okj Mh0Mh0Vh0 fNM+dko djk;k tk;sxkA<br />
blds vfrfjDr [kkst Ik[kokjk ds }kjk dkyktkj jksfx;ks dh [kkst dj fpfdRlk dh<br />
tk;sxhA vk'kk dk;ZdÙkkZ dks dkyktkj ds lEHkkfor dks ljdkjh vLirky esa ykdj]<br />
dkyktkj ds jksx lEiq"V gksus ,oa iw.kZ fpfdRlk ds mijkUr izksRlkgu jkf'k nh tk;sxhA<br />
bl rjg dkyktkj dsl dks lekIr fd;k tk ldrk gSA<br />
11- izLrkfor jkf'k dk enokj fooj.k % &<br />
1- izksRlkgu jkf'k & 33]00]000@&ftyk dk;ZØe inkñ dks<br />
2- nSfud Je {kfriwfrZ jkf'k 4]95]00]000@& rFkSo<br />
3- iz[k.M vLirky ds 'k';k foLrkj 31]00]000@& rFkSo<br />
4- IkosZ{k.k 2]77]48]000@& rFkSo<br />
5- nok dk Hk.Mkj.k 1]86]000@& rFkSo<br />
18]000@& jkT; dk;ZØe inkñ dks<br />
6- fpfdRlk dkMZ 1]65]000@& ftyk dk;ZØe inkñ dks<br />
7- lwpuk la/kkj.k iath 15]500@& rFkSo<br />
8- MhñMhñVhñ dk HkaMkj.k 18]60]000@& rFkSo<br />
9- dkyktkj [kkst i[kokjk 13]52]000@&<br />
dqy ;ksx 8]72]44]500@&<br />
¼vkB djksM+ cgrj yk[k pkSvkfyl gtkj ik¡p lkS #i;s ek= ½<br />
¼ifjf'k"V V nz"VO;½<br />
335
(x) jkT; Lrjh; dEiksusUV<br />
(jkT; dk;Z e inkf/dkjh dk;kZy; ds fy,)<br />
1- jkT; LVh;jhx dfeVh %& dkyktkj ds liQy lapkyu dh n‘f"V ls le;≤ ij ’kh"kZ Lrjh;<br />
inkfŁkdkfj;ksa ds ijke’kZ dh vko’;drk gksrh gSA bl n‘f"V ls jkT; jkT; ij ,d <strong>State</strong> Stearing<br />
Committee ds xBu dh vko’;drk eg’kwl dh xbZ gS A bl dfeVh esa fodkl vk;qDr] LokLF;<br />
vk;qDr] funs’kd izeq[k Lok- lsok;s] jkT; dk;Zdze ink- rFkk Hkkjr ljdkj ds ’kh"k ink- Hkh ’kkfey<br />
jgsxs A<br />
le;≤ ij mDr xfBr dfeVh ds cSBd vk;kstu djus ,oa cSBd ds vk;kstu esa<br />
gksus okys O;; dh n‘f"V ls jkf’k dk izko/ku fd;k x;k A dfeVh dh cSBd o"kZ esa de ls de rhu<br />
ckj djkus dk izLrko gS A<br />
izLrkfor jkf’k & Rs. 30,000/-<br />
(Rs. 10,000 izfr cSBd × 3 )<br />
[ foij.kh VI dafMdk 1 nz"VO; ]<br />
2. czkaM ,sEcsLMj<br />
dkyktkj ds jksdFkke dh n‘f"V ls le;≤ ij ekuuh; iz/ku ea=kh @ eq[; ea=kh @ vU; x.kekU;<br />
usrk @ vfHkusrk }kjk izpkj dk;Z vko’;d izrhr gksrk gS A bl fufer jkf’k dk izLrko gS ftldks O;;<br />
izpkj dk;Z ij gksxk A<br />
izLrkfor jkf’k & Rs. 50,000/-<br />
[ fooj.k VI dafMdk&2 nz"VO; ]<br />
3. dEI;wVj<br />
jkT; dk;Z e ink- dk;kZy; esa dk;Z e laca/h dk;Z ds lqpk: :i ls fu"iknu dh n‘f"V ls ,d MsLd<br />
VkWi dEI;wVj (;w-ih-,l- ds lkFk) dh vko’;drk gS A bl fufer jkf’k izLrko gS A<br />
izLrkfor jkf’k & Rs. 50,000/-<br />
[ fooj.kh VI dafMdk&3 nz"VO; ]<br />
4. ySi VkWi<br />
jkT; Lrj ij vofLFkr jkT; dk;Z e ink- esa rhu ink- ;Fkk jkT; dk;Z e ink-] mi eq[; eysfj;k<br />
ink- ,oa lgk;d funs’kd dkyktkj inLFkkfir gS ftuds }kjk dk;Z e dk lapkyu fd;k tkrk gSA bu<br />
rhuksa inkfd/kjh dks l le; lHkh rjg dh lwpuk j[kus @ ’kh"kZ inkf/dkfj;ksa dks lwpuk miyC/<br />
djkus gsrq rhu ySi VkWi dh vko’;drk gS A ftlds fy, jkf’k dk izLrko gS A izfr ySi VkWi Rs.<br />
50,000/- dh nj ls ; dk izLrko izLrkfor jkf’k Rs. 50,000 × 3 -------Rs. 1,50,000/-<br />
[ fooj.kh VI dafMdk 4 nz"VO; ]<br />
5. eksckby iQksu<br />
dkyktkj dk;Z dh lqxerk ,oa deZpkjh ink- ds chp lh/k lEidZ dh n‘f"V ls eksckby iQksu ds ;<br />
dk djus dk izLrko gS A jkT; dk;Zdze ink- dk;kZy; esa dk;Zjr rhu ink-] rduhdh ’kk[kk esa pkj]<br />
LVksuks ,d iz/ku fyfid ,oa ys[kkiky ,d (dqy nl) eksckby iQksu ds ; dk izLrko gSA izfr<br />
eksckby Rs. 2000/- dh nj ls jkf’k dk izko/ku fd;k x;k gSA<br />
eksckby ds e ds mijkUr izfrekg dqiu ij gksus okys O;; ij izfr eksckby Rs. 337/- dh nj ls<br />
12 ekg ds jkf’k dk izLrko gSA<br />
336
izLrkfor jkf’k &<br />
nl eksckby ; ---------- 10 × 2000---------- Rs 20,000/-<br />
eksckby ij ekfld O;;------- 10 × 337 × 12 ------ Rs.40,440/-<br />
dqy Rs. 60,440/-<br />
[ fooj.kh VI, dafMdk & 5 ]<br />
6. ystj izhaVj<br />
jkT; eq[;ky; vofLFkr jkT; dk;Z e ink- dk;kZy; gsrq ystj izhaVj ftlds rgr iQksu] iQSDl] Ldsuj<br />
lfgr] ; dk izLrko gS A ftlds ; gsrq jkf’k dk izLrko gS A<br />
izLrkfor jkf’k---------------------- Rs. 25,000/-<br />
[ fooj.kh VI, dafMdk& 6 ]<br />
7. iQksVks dkWih e’khu<br />
jkT; eq[;ky; esa iQksVks dkWih e’khu miyC/ ugha gS A ;kstuk ds dk;Z lEiknu esa iQksVks dkWih djkuk<br />
iM+rk gS ftls LFkkuh; cktkj ls djk;k tkrk gS A bls [kpZ Hkh vf/d gksrk gS lkFk gh dfBukbZ Hkh A<br />
vr% dk;Z lqyHkrk dh n‘f"V ls jkT; eq[;ky; gsrq ,d iQksVks dkWih e’khu dh vko’;drk gS ftlij<br />
gksus okys O;; dk izko/ku ctV esa fn;k tk jgk gS A<br />
izLrkfor jkf’k------------------- Rs. 1,50,000/-<br />
8. jkT;Lrj ij cSBd vk;kstu<br />
dk;Z e ds lapkyu esa ftyk dk;Z e ink- ds lkFk leh{kkRed cSBd djuk vko’;d gksrk gS A<br />
cSBd esa dk;Z e ds laca/ esa ftykokj foLr‘r leh{kk dh tkrh gS rFkk dk;Z e ds lapkyu ds laca/<br />
esa vxzrj dkjZokbZ gsrq Hkh fn’kk funs’k r; fd;k tkrk gS A<br />
jkT; Lrj o"kZ esa de ls de rhu ckj cSBd vk;ksftr djus dk izLrko gS A izR;sd cSBd esa Rs.<br />
10,000/-O;; gksus dh laHkkouk gS A bl fufer jkf’k dk izko/ku ctV esa fd;k x;k gS A<br />
izLrkfor jkf’k -------------------- 3 × 10,000 --------------------- Rs. 30,000/-<br />
9. bUVjusV lqfo/k<br />
jkT; eq[;ky; es a vofLFkr dEI;wVj esa bUVjusV lqfo/k vko’;d gS A blds vfrfjDr dk;kZy; ds<br />
dEI;wVj ds j[k j[kko ij Hkh O;; gksxk A vr% bUVjusV lqfo/k ,oa dEI;wVj ds j[k j[kko ij gksus<br />
oyks O;; ds fy, ctV esa jkf’k dk izLrkfor fn;k tk jgk gS A<br />
izLrkfor jkf’k----------------------- Rs. 30,000/-<br />
10. iosZ{k.k<br />
ftyk Lrj ds dk;Z e ink- ds ios Z{k.k gsrq ctV [k.M ^d* esa vkbZ-vkj-,l- es a pkj ekg ds fy, rFkk<br />
ctV [k.M ^[k* esa vkB ekg ds fy, jkf’k izLrkfor gS A<br />
jkT; Lrj ij ds inkf/dkfj;ksa ds ios Z{k.k ij gksus okys O;; ds fy, vko’;d jkf’k dk izko/ku ctV<br />
esa fn;k tk jgk gS A jkT; Lrj ij jkT; dk;Z e ink- dk;kZy; esa inLFkkfir rhu ink- }kjk dk;Z e<br />
dk ios Z{k.k fd;k tkuk gS A jkT; eq[;ky; es a ek=k ,d xkM+h gS og Hkh pkyq gkyr esa ugha gS A vr%<br />
miyC/ xkM+h ds ejEerh ,oa HkkM+s ij xkM+h ysdj iosZ{k.k fd;k tk;xk A ftlds fufer izfr inkizfrekg<br />
fd Rs. 2500 dh nj ls jkf’k dk izLrko gS A<br />
izLrkfor jkf’k---------------------------- 3 × 2500 ×12 -------------------- Rs. 90,000/-<br />
xkM+h ejEerh gsrq------------------------------------------------------------------- Rs. 10, 000/-<br />
337
[ fooj.kh VI dsfMdk----------------- 10 nz"VO; ] dqy Rs. 1,00,000/-<br />
11. tsujsVj lqfo/k<br />
jkT; eq[;ky; esa fctyh ckf/r gksus ij dk;Z dk lEiknu can gks tkrk gSA bl fufer ,d tsujsVj<br />
; dk izLrko gS A tsujsVj ds ; ,oa izfrekg mlds fy, ba/u ij gksus okys O;; ds fy, ctV esa<br />
jkf’k dk izko/ku fd;k x;k gS A<br />
izLrkfor jkf’k--------------------------------------------------- Rs. 50, 000/-<br />
tsujsVj ds ba/u gsrq Rs. 4000/- izfr<br />
ekg dh nj ls (12 × 400) --------------------------- Rs. 48,000/-<br />
;ksx Rs. 98,000/-<br />
(fooj.kh VI ---- dafMdk 11 nz"VO;)<br />
12. izpkj&izlkj<br />
le;≤ ij dkyktkj ds laca/ esa tula/kj.k esa tudkjh nSfud lekpkj i=k] jsfM;ks] Vh-ohbR;kfn<br />
ds ekŁ;e ls nsuk vko’;d gS A lHkh ftyks ds dkyktkj izHkkfor xkoks esa fNM+dko dh frfFk<br />
dh lwpuk LFkkuh; yksdfiz; nSfud lekpkj Ik=kks esa nks fnu izdkf’kr fd;k tk;sxkA bl fufer ctV<br />
esa jkf’k dk izko/ku fd;k x;k gS A<br />
dqy izLrkfor jkf’k---------------------------------------------- Rs. 4,00,000/-<br />
(fooj.kh VI--- dafMdk& 13 nz"VO;)<br />
13. {ks=kh; eysfj;k dk;kZy; gsrq<br />
eysfj;k ;kstuk esa iwjs jkT; esa pkj {ks=kh; eysfj;k ink- dk dk;kZy; gSA {ks=kh; e- ink- }kjk vius<br />
{ks=kk/hu feyksa ds liQy iosZ{k.k dh n‘f"V ls HkkM+s ij xkM+h ysus gsrq jkf’k dk izLrko gS ftlds rgr<br />
izfr {ks- e- ink- 20]000@& dh nj ls jkf’k dh izko/ku fd;k tk jgk gS A<br />
blds vfrfjDr {ks=kh; eysfj;k dk;kZy; esa ,d&,d dEI;wVj ; dk Hkh izLrko gS ftlls lacaf/r<br />
{ks- e- ink- vius v/huLFk ftyksa dk v|ru fLFkfr dk O;ksjk j[ksxs rFkk izR;sd lIrkg fLFkfr ls<br />
jkT; eq[;ky; dks voxr djk;sxs A<br />
izLrkfor jkf’k &<br />
ios Z{k.k ------------------------- 20,000 × 4 ------------------ 80,000/-<br />
dEI;wVj ;----------------- 50,000 × 4 ------------------ 2,00,000/-<br />
dEI;wVj ds j[k j[kkc---- 5000 × 4 ------------------ 20,000/-<br />
dqy 3,00,000/-<br />
izLrkfor ctV dk enokj fooj.kh<br />
1- jkT; LVh;jhx dfeVh -------------------------- Rs. 30,000/- jkT; dk;Z ; ink- gsrq<br />
2- czkaM ,EosLMj ------------------------- Rs. 50,000/- ]]<br />
3- dEI;wVj ------------------------- Rs. 50,000/- ]]<br />
4- ySi VkWi ------------------------ Rs. 1,50,000/- ]]<br />
5- eksckby iQksu ------------------------ Rs. 60,440/- ]]<br />
6- ystj izhVj ------------------------ Rs. 25,000/- ]]<br />
7- iQksVks dkWih e’khu ------------------------ Rs. 1,50,000/- ]]<br />
338
8- cSBd (jkT; Lrjh;) ------------------------- Rs. 30,000/- ]]<br />
9- bUVjusV lqfo/k ------------------------- Rs. 30,000/- ]]<br />
10- iosZ{k.k ------------------------- Rs. 1,00,000/- ]]<br />
11- tsujsVj ------------------------- Rs. 98,000/- ]]<br />
12- izpkj&izlkj ------------------------- Rs. 4,00,000/- ]]<br />
13- {ks- e- ink- dk;Zy; gsrq ------------------------- Rs. 3,00,000/- ]]<br />
dqy;ksx Rs. 14,73,440/-<br />
(?k) izf’k{k.k & dkyktkj Elemination y{; 2010 dh izfIr dh n‘f"V ls jkT; ds lHkh Lrj ds LokLF;<br />
foHkkx esa inLFkkfir fp- inkf/dkfj;ksa] eysfj;k ;kstuk esa dk;Zjr lHkh Lrj ds ikjk esfMdy dfeZ;ksa<br />
dk izf’k{k.k vko’;d izrhr gksrk gS rkfd fujks/kRed ,oa mipkjkRed dkjZokbZ esa mudk lf ;<br />
lg;ksx fey lds A blds vfrfjDr LokLF; loxZ ds dqN vU; ikjk esfMdy dfeZ;ksa iapk;fr jkT;<br />
ds lnL;ksa ,oa cgqnsf’k; dk;Z kk (vk’kk) Hkh fujks/kRed ,oa mipkjkRed dkjZokbZ ds fy, izf’kf{kr<br />
djuk vko’;d izrhr gksrk gSA<br />
bl n‘f"V dks.k ls Hkkjr ljdkj }kjk fn;s x;s fn’kk funs’k ds vuqlkj izf’k{k.k dk;Z e dh :ijs[kk<br />
rS;kj dh xbZ gS] ftls layXu ifjf’k"V VII esa ns[kk tk ldrk gS A ifjf’k"V VII esa ftykokj eysfj;k<br />
;kstuk ljdkjh vLirky ds fpfdRldks ,oa vU; LokLF; lEoxZ ds ikjk esfMdy dfeZ;k iapk;rh<br />
jkT; ds lnL;ksa ds izf’k{k.k dk ctV izkdyu rS;kj fd;k x;k gS A izf’k{k.k izLrko foLr‘r fooj.k<br />
bl izdkj gS &<br />
1. eysfj;k ;kstuk ds eysfj;k fujh{kdksa dk izf’k{k.k<br />
jkT; ds 31 dk;kZy; izHkkfor ftyksa esa dqy 114 e- fu- dk;Zjr gS A Hkkjr ljdkj ds fn’kk funs’kd<br />
ds vuqlkj 20 izf’k{k.kkfFkZ dks ,d oS/ esa izf’k{k.k fn;k tk;xk A bl rjg dqy 6 cSp gksxs A<br />
izf’k{k.k vof/ 1 fnuksa dh gksxh A<br />
o"kZ esa nks ckj izf’k{k.k nsus dk izLrko gS A ,d cSp ds izf’k{k.k ij dqy O;; 69,500/- :- gksxkA<br />
bl rjg iwjs o"kZ esa 6 cSp dks nks okj izf’k{k.k ij dqy O;;<br />
2 × 6 × 69, 500/-------------- Rs. 8,34,000/-<br />
(ifjf’k"V VII LrEHk 4 nz"VO;)<br />
2. iz;ksx’kkyk izkosf/d<br />
eysfj;k ;kstukUrxZr 31 dkyktkj izHkkfor ftyksa esa dqy 47 iz;ksx’kkyk izkoSf/d dk;Zjr gS A 20<br />
izf’k{k.kFkksZ ds fglkc ls dqy 2 cSp dks 10 fnuksa dk izf’k{k.k fn;k tk;xk A ,d cSp ds izf’k{k.k<br />
ij dqy O;; 1,25,000/- gksxk A<br />
ifjf’k{k.k ij izLrkfor O;;------------ 2 × 1,25, 000@&------------ Rs. 2,50,000/-<br />
iz;ksx’kkyk izkosfNd dks Re Orientation izf’k{k.k Hkh fn;k tk;xk A ftlesa 2 cSp ds izf’k{k.kkFkksZ<br />
dks 5 fnuksa dk izf’k{k.k fn;k tkuk gS A ,d cSp ds izf’k{k.k ij 75,620/- O;; gksxk A<br />
Orientation dkslZ ij izLrkfor ;-------- 2 × 75, 620 ------------ Rs. 1,51,240/-<br />
iz;ksx’kkyk izkoSfNd ds izf’k{k.k ij dqy O;; ----------- Rs. 4,01,240/-<br />
(ifjf’k"V VII LrEHk 6] 7 nz"VO;)<br />
3. cqfu;knh Lok- fujh{kd ,oa fuxjkuh fujh{kd<br />
jkT; ds 31 dkyktkj izHkkfor ftyksa esa eysfj;k ;kstuk ds 118 cqfu;knh Lok- fujh{kd ,oa 18<br />
339
fuxjkuh fujh{kd dk;Zjr gS A bl rjg 136 izf’k{k.kFkhZ dks 27 izfr cSp vuqlkj 5 oSp esa izf’k{k.k<br />
fn;k tk;xkA ;g izf’k{k.k nks fnuksa dk gksxk A izf’k{k.k ij izfr oSp 30,000 :- O;; dk izLrkohr<br />
gS A<br />
izLrkfor jkf’k------------------- 5 × 30, 000 ----------- Rs. 1,50,000/-<br />
(ifjf’k"V VII LrEHk 11 n‘"VO;)<br />
4. Lok- dk;Zd kkZ dk izf’k{k.k<br />
jkT; ds eysfj;k ;kstukUrxZr 31 dkyktkj izHkkfor ftyksa esa dqy 103 cqfu;knh Lok- dk;Zd kkZ] 33<br />
fuxjkuh dk;Zd kkZ] 43 {ks=kh; dk;Zd kkZ rFkk 19 Js- {ks- dk;Zd kkZ dk;Zjr gSA bl rjg dqy 198<br />
dk;Zjr dks izf’kf{kr fd;k tkuk gS A 25 izf’k{k.kkFkhZ izfr oSp dh nj ls 8 oSp esa izf’k{k.k fn;k<br />
tk;xkA izf’k{k.k vof/ nks fnuksa dh gksxh A izf’k{k.k ij izfr oSp 30,000/- :- O;; gksxk A<br />
izLrkfor jkf’k & 30,000 × 8 Rs. 2,40,000/-<br />
(ifjf’k"V VII LrEHk 16 n"VO;)<br />
5. fpfdRlk ink- dk izf’k{k.k<br />
jkT; ds 31 dkyktkj izHkkfor ftyksa ds lHkh Lrj ds vLirkyksa esa dk;Zjr fpfdRlk inkf/dkfj;ksa ds<br />
izf’k{k.k dk izLrko gS A lHkh Lrj ds vLirkyksa esa inLFkkfir fpfdRlk inkf/dkfj;ksa dk ftysokj<br />
la[;k layXu ifjf’k"V VIII ds LrEHk 3 ls 8 esa n’kkZ;k x;k gS A lHkh Lrj ij inLFkkfir fp- inkdh<br />
dqy la[;k 502 gS A 25 izf’k{k.kkFkhZ izfr oSp ds vuqlkj 20 oSp esa izf’k{k.k dk izLrko gS A<br />
izf’k{k.k vof/ rhu fnuksa dh gksxh ,d oSp ds izf’k{k.k ij dqy 1,20,000/- :- O;; izLrkfor gS A<br />
fp- iznk- ds izf’k{k.k dqy izLrkfor O;; 20 × 1,20,000--------- Rs. 24,00,000/-<br />
(ifjf’k"V VIII LrEHk 9 n‘"VO;)<br />
6. iapk;rh jkT; ds lnL;ksa dk izf’k{k.k<br />
jkT; esa iapk;rh jkT; ds ykxw gks tkus ls blds lnL;ksa dks ljdkjh dk;Z ds ns[k&js[k dk nkf;Ro<br />
fn;k x;k A dkyktkj ds djhc 90 izfr’kr jksxh xzkeksa ls gh vkrs gSa vr% iapk;r Lrj ds lnL;ksa dks<br />
dkyktkj ds fujks/kRed ,oa mipkjkRed dkjZokbZ ls :&c&: voxr djkus dh n‘f"V ls izf’k{k.k dk<br />
izLrko fn;k tk jgk gS A layXu ifjf’k"V IX ds LrHk 3 ls 5 esa iapk;rh jkTk ds lnL;ksa dk ftysokj<br />
vkadM+k fn;k x;k gS ftUgs a izf’k{k.k dk izLrko gS A<br />
ifjf’k"V ds voyksdu ls fofnr gksxk fd iapk;rh jkt ds dqy 13860 lnL;ksa dks izf’k{k.k nsus dk<br />
izLrko gS A 50 lnL; izfr oSp dh nj ls dqy 277 oSp esa izf’k{k.k fn;k tk;xkA izfr oSp dks 1<br />
fnu dk izf’k{k.k fn;k tk;xk A ,d oSp ds izf’k{k.k ij 2000 :- O;; gksxk A<br />
izLrkfor O;;---------------- 277 × 2000 -------------------------------------- Rs. 5,54,000/-<br />
(ifjf’k"V IX LrEHk 6 nz"VO;)<br />
7. fNM+dko dkfeZ;ksa dk izf’k{k.k<br />
jkT; ds dkyktkj izHkkfor 31 ftyksa ds foxr ik¡p o"kksZ esa dkyktkj izHkkfor xzkeksa ds dqy 32-39<br />
feyh;u tula[;k dks vPNkfnr djus esa dqy 1782 Js"B {ks- dk;Zd kkZ rFkk 8910 {ks- dk;Zd kkZ<br />
layXu fd;s x;s A iwoZ esa fNM+dko ds ,d fnu iwoZ fNMdko dfeZ;ksa dks izf’kf{kr fd;k tkrk FkkA<br />
orZeku esa Hkkjr ljdkj }kjk fu/kZfjr uhfr ds rgr dqy (1782 $ 8910) 10692 fNM+dko dfeZ;ksa<br />
dks izf’k{k.k fn;k tkuk gSA<br />
rnuqlkj 50 fNM+dko dehZ izfr oSp dh nj ls dqy 214 oSp esa 1 fnu dk izf’k{k.k fn;k tk;xkA<br />
340
,d fnu ds izf’k{k.k esa ,d oSp ij dqy 2000@& :- O;; dk izLrkfor gS A<br />
dqy izLrkfor O;; ------------------- 214 × 2000 --------------------------- Rs. 4,28,000/-<br />
(ifjf’k"V X LrEHk 5 n‘"VO;)<br />
8. cgq sf’k; dk;Zd kkZ (vk’kk) dk izf’k{k.k<br />
dk;Z e ds lapkyu esa vk’kk dk;Zd kkZ dks Hkh ’kkfey fd;k x;k gS vr% dkyktkj ds mipkjkRed<br />
dkjZokbZ ds laca/ esa izf’k{kr fd;k tkuk gS A ifjf’k"V X ds LrEHk 6 esa ftykokj vk’kk dk;Zd kkZ dh<br />
la[;k n’kkZ;h xbZ gS A dqy 52]065 vk’kk dk;Zd kkZ dks 50 izf’k{k.kkFkhZ izfr oSp dh nj ls 1041<br />
cSp esa izf’k{k.k nsus dk izLrko gS A izfr oSp dks ,d fnu dk izf’k{k.k fn;k tk;xkA ftlij 2000@&<br />
:- (izfroSp) dh nj ls O;; gksxk A<br />
dqy izLrkfor O;; -------------- 1041 × 2000 ---------------------- Rs. 20,82,000/-<br />
(ifjf’k"V X LrHk 7 n‘"VO;)<br />
9. izf’k{k.k ij dqy O;; dk lkjka’k<br />
1- eysfj;k fujh{kd -------------------------- Rs. 8,34,000/-<br />
2- iz;ksx’kkyk izkoSf/d ------------------------- Rs. 4,01,240/-<br />
3- cq-Lok- fu- ,oa fu- fu- ------------------------- Rs. 1,50,000/-<br />
4- Lok- dk;Zd kkZ ------------------------ Rs. 2,40,000/-<br />
5- fp- ink- ------------------------ Rs. 24,00,000/-<br />
6- iapk;rh jkt ------------------------ Rs. 5,54,000-<br />
7- fNM+dko dehZ ------------------------ Rs. 4,28,000/-<br />
8- cgq sf’k; dk;Z kkZ (vk’kk) ------------------------- Rs. 20,82,000/-<br />
dqy Rs. 70,89,240/-<br />
;kstuk ctV dk lkjka’k<br />
[k.M d & fujks/kRed dkjZokbZ & Rs. 13,10,85,720=00<br />
[k.M [k & mipkjkRed dkjZokbZ & Rs. 8,72,44,500=00<br />
[k.M x & jkT; eq[;ky; dk lqn‘
izfrfyfi {ks=kh; funs’kd] Lok- ,oa i- d- foHkkx] Hkkjr ljdkj] bfUnjk Hkou] ikWpoka eafaty] csyh jksM]iVuk]<br />
dks vuqyXud lfgr lwpukFkZ ,oa vko’;d dkjZokbZ gsrq izf"kr A<br />
la;qDr funs’kd lg jkT; dk;Z e inkeysfj;k@dkyktkj<br />
fcgkj] iVuk<br />
342
Name of<br />
Districts<br />
<strong>State</strong> & District Wise Fund Allocation - Kala-Azar, Bihar 2009-2010<br />
One Round Amount<br />
From Annex. II From Annex. IV<br />
Total Amount For One<br />
Round<br />
343<br />
Two Round Amount<br />
Total Amount For Two<br />
Round Spray i.e (Anneex.II+<br />
Annex.IV)<br />
From Annex. V Total ( Column 6+7)<br />
1 2 3 4 5 6 7 8<br />
1 Araria 4,105,740.00 161,450.00 4,267,190.00 8,534,380.00 5,072,950.00 13,607,330.00<br />
2 Arwal 73,860.00 9,700.00 83,560.00 167,120.00 1,008,250.00 1,175,370.00<br />
3 Banka 36,180.00 2,800.00 38,980.00 77,960.00 1,016,150.00 1,094,110.00<br />
4 Begusarai 1,923,900.00 86,250.00 2,010,150.00 4,020,300.00 2,119,550.00 6,139,850.00<br />
5 Bhagalpur 287,940.00 27,300.00 315,240.00 630,480.00 1,289,100.00 1,919,580.00<br />
6 Bhojpur 429,660.00 42,000.00 471,660.00 943,320.00 1,136,650.00 2,079,970.00<br />
7 Buxar 214,080.00 13,400.00 227,480.00 454,960.00 1,066,400.00 1,521,360.00<br />
8 Darbhanga 3,072,840.00 140,250.00 3,213,090.00 6,426,180.00 3,686,450.00 10,112,630.00<br />
9 E.Champaran 5,023,920.00 234,550.00 5,258,470.00 10,516,940.00 4,493,000.00 15,009,940.00<br />
10 Gopalganj 1,332,840.00 78,150.00 1,410,990.00 2,821,980.00 3,068,500.00 5,890,480.00<br />
11 Jehanabad 76,860.00 16,400.00 93,260.00 186,520.00 1,052,400.00 1,238,920.00<br />
12 Katihar 2,177,160.00 148,450.00 2,325,610.00 4,651,220.00 2,298,150.00 6,949,370.00<br />
13 Khagaria 667,920.00 39,350.00 707,270.00 1,414,540.00 2,005,550.00 3,420,090.00<br />
14 Kishanganj 1,361,520.00 79,950.00 1,441,470.00 2,882,940.00 1,503,800.00 4,386,740.00<br />
15 Lakhisarai 211,080.00 11,350.00 222,430.00 444,860.00 1,050,350.00 1,495,210.00<br />
16 Madhepura 2,750,220.00 111,100.00 2,861,320.00 5,722,640.00 4,254,350.00 9,976,990.00<br />
17 Madhubani 2,662,680.00 128,900.00 2,791,580.00 5,583,160.00 2,952,400.00 8,535,560.00<br />
18 Munger 217,080.00 22,800.00 239,880.00 479,760.00 1,178,800.00 1,658,560.00<br />
19 Muzaffarpur 5,188,320.00 293,450.00 5,481,770.00 10,963,540.00 6,976,700.00 17,940,240.00<br />
20 Nalanda 606,060.00 44,150.00 650,210.00 1,300,420.00 1,321,050.00 2,621,470.00<br />
21 Patna 2,035,440.00 124,300.00 2,159,740.00 4,319,480.00 1,628,050.00 5,947,530.00<br />
22 Purnea 4,319,820.00 202,600.00 4,522,420.00 9,044,840.00 4,410,900.00 13,455,740.00<br />
23 Saharsa 2,646,180.00 108,850.00 2,755,030.00 5,510,060.00 5,044,850.00 10,554,910.00<br />
24 Samastipur 3,662,400.00 185,650.00 3,848,050.00 7,696,100.00 4,248,200.00 11,944,300.00<br />
25 Saran 2,762,220.00 159,050.00 2,921,270.00 5,842,540.00 3,941,250.00 9,783,790.00<br />
26 Sheohar 419,160.00 17,200.00 436,360.00 872,720.00 1,202,850.00 2,075,570.00<br />
27 Sitamarhi 3,452,820.00 140,450.00 3,593,270.00 7,186,540.00 2,721,650.00 9,908,190.00<br />
28 Siwan 2,830,080.00 144,850.00 2,974,930.00 5,949,860.00 2,647,200.00 8,597,060.00<br />
29 Supaul 1,577,100.00 81,250.00 1,658,350.00 3,316,700.00 1,168,800.00 4,485,500.00<br />
30 Vaishali 3,935,340.00 191,150.00 4,126,490.00 8,252,980.00 5,650,550.00 13,903,530.00<br />
31 W.Champaran 2,204,340.00 86,000.00 2,290,340.00 4,580,680.00 6,011,650.00 10,592,330.00
Total 62,264,760.00 3,133,100.00 65,397,860.00 130,795,720.00 87,226,500.00 218,022,220.00<br />
<strong>State</strong> Level Activity<br />
1 Training At <strong>State</strong> Level From Annex. VII,VIII,IX & X 7,089,240.00<br />
2 <strong>State</strong> Level Activity From Annex. VI 1,473,440.00<br />
3 SPO & ZMO Mobility During Spray Period 145000.00 x2 =290000.00 290,000.00<br />
4 Storage of Amphoteracin B.At <strong>State</strong> Level 18,000.00<br />
Grand Total Of Kala-Azar Programme ,<strong>BIHAR</strong> 226,892,900.00<br />
344
District Infrastructure of Kala-Azar Affected Districts<br />
Anexure - I<br />
Sl. No. Name of Districts<br />
PHC HSC Block Panchyat<br />
Total No. of<br />
Revenue<br />
Village<br />
Urban<br />
Ward<br />
345<br />
Total No. of Affected<br />
Population PHC HSC Panchyat Village Ward Population<br />
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15<br />
1 Araria 9 109 9 221 757 54 2,670,845 9 88 165 563 0 2,153,592<br />
2 Arwal 3 64 0 0 335 0 651,717 3 7 0 18 0 41,144<br />
3 Banka 10 0 11 185 1681 40 0 1 1 1 2 0 12,719<br />
4 Begusarai 11 288 18 257 1064 36 2,900,088 11 51 154 245 0 999,274<br />
5 Bhagalpur 11 280 17 242 1929 62 2,948,451 7 0 0 62 0 145,797<br />
6 Bhojpur 12 304 14 228 1457 100 2,292,652 9 64 0 120 0 210,106<br />
7 Buxar 7 167 11 142 993 60 1,458,493 4 16 0 16 0 104,052<br />
8 Darbhanga 14 306 19 306 1522 48 3,442,496 14 206 206 455 0 1,602,617<br />
9 E.Champaran 20 318 27 387 1716 20 46,78,325 20 268 302 817 0 2,620,283<br />
10 Gopalganj 10 186 14 234 1499 12 2,398,707 10 107 0 261 0 693,562<br />
11 Jehanabad 5 81 12 161 947 52 1,029,742 5 15 0 36 0 37,257<br />
12 Katihar 18 257 16 238 1737 45 2,687,203 18 192 0 543 0 1,134,049<br />
13 Khagaria 6 0 7 129 306 18 0 6 0 0 119 0 348,271<br />
14 Kishanganj 7 79 7 118 761 28 1,554,007 6 36 63 323 0 712,592<br />
15 Lakhisarai 4 102 7 80 496 18 895,678 2 19 19 29 18 101,437<br />
16 Madhepura 7 196 13 170 838 41 1,669,001 7 139 0 384 0 1,431,240<br />
17 Madhubani 18 430 21 399 1072 75 4,094,575 18 294 294 366 0 1,376,642<br />
18 Munger 6 134 9 101 837 104 1,349,751 6 33 30 52 0 97,035<br />
19 Muzaffarpur 14 527 16 387 1937 49 4,561,521 14 459 0 1273 0 2,703,171<br />
20 Nalanda 12 0 20 249 1183 122 0 11 0 0 91 0 315,421<br />
21 Patna 16 0 23 331 1455 72 4,062,216 16 244 0 422 0 1,060,285<br />
22 Purnea 14 151 14 237 1075 0 3,174,330 13 107 191 764 0 2,258,220<br />
23 Saharsa 7 152 10 164 435 43 1,802,298 7 130 0 379 0 1,381,124<br />
24 Samastipur 14 0 20 381 1250 61 3,860,729 14 331 329 701 0 1,904,426<br />
25 Saran 15 413 20 0 1813 0 3,551,306 15 0 0 597 0 1,437,022<br />
26 Sheohar 2 0 5 54 207 15 0 2 0 0 48 0 212,868<br />
27 Sitamarhi 13 0 17 273 846 79 3,009,938 13 186 212 433 38 1,807,046<br />
28 Siwan 15 351 16 293 1458 51 3,100,210 14 219 0 509 0 1,481,302<br />
29 Supaul 11 178 11 180 688 0 1,968,535 11 0 0 245 0 809,393<br />
30 Vaishali 11 339 16 292 1680 45 3,250,683 11 0 278 751 0 2,054,842<br />
31 W.Champaran 16 369 18 354 2220 121 3,495,552 13 140 123 190 0 1,147,023<br />
Total 338 5,781 438 6,793 36,194 1,471 67,880,724 310 3,352 2,367 10,814 56 32,393,812
Sl.<br />
No.<br />
Name of<br />
Districts<br />
Dist. Wise Sqad,DDT,Wages,Office Exp.,Contigency,Transportation of DDT For Kala Azar Spray One Round<br />
Total No. of Total No. of DDT 50% Status (In Meric<br />
Total No. of Affected<br />
Sqad (55 Workers<br />
Ton)<br />
Sqad /10<br />
Lakhs<br />
PHC Population SFW FW Require. Available Balance<br />
Population<br />
Require.<br />
SFW(Rs. 113/-<br />
Per SFW For<br />
60 Days)<br />
WAGES<br />
FW(Rs.92/-Per<br />
FW For 60<br />
Days)<br />
Total<br />
Office<br />
Expense<br />
s (@ Rs<br />
150/-Per<br />
Sqad<br />
Contigenc<br />
y (@ Rs.<br />
150/- Per<br />
Sqad<br />
Annexure -II<br />
Transportation of DDT<br />
PHC To<br />
Village(R<br />
Total<br />
s.500/-<br />
PHC)<br />
District To<br />
PHC(RS.<br />
1000/- Aff.<br />
PHC)<br />
Grand Total<br />
(13+14+15+<br />
18)<br />
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19<br />
1 Araria 9 2,153,592 118 118 590 80.76 46.99 33.77 800,040 3,256,800 4,056,840 17,700 17,700 9,000 4,500 13,500 4,105,740<br />
2 Arwal 3 41,144 2 2 10 1.54 0.29 1.25 13,560 55,200 68,760 300 300 3,000 1,500 4,500 73,860<br />
3 Banka 1 12,719 1 1 5 0.48 0.00 0.48 6,780 27,600 34,380 150 150 1,000 500 1,500 36,180<br />
4 Begusarai 11 999,274 55 55 275 37.47 29.76 7.71 372,900 1,518,000 1,890,900 8,250 8,250 11,000 5,500 16,500 1,923,900<br />
5 Bhagalpur 7 145,797 8 8 40 5.47 5.20 0.27 54,240 220,800 275,040 1,200 1,200 7,000 3,500 10,500 287,940<br />
6 Bhojpur 9 210,106 12 12 60 7.88 25.00 -17.12 81,360 331,200 412,560 1,800 1,800 9,000 4,500 13,500 429,660<br />
7 Buxar 4 104,052 6 6 30 3.90 5.00 -1.10 40,680 165,600 206,280 900 900 4,000 2,000 6,000 214,080<br />
8 Darbhanga 14 1,602,617 88 88 440 60.10 132.00 -71.90 596,640 2,428,800 3,025,440 13,200 13,200 14,000 7,000 21,000 3,072,840<br />
9 E.Champaran 20 2,620,283 144 144 720 98.26 85.70 12.56 976,320 3,974,400 4,950,720 21,600 21,600 20,000 10,000 30,000 5,023,920<br />
10 Gopalganj 10 693,562 38 38 190 26.01 0.00 26.01 257,640 1,048,800 1,306,440 5,700 5,700 10,000 5,000 15,000 1,332,840<br />
11 Jehanabad 5 37,257 2 2 10 1.40 0.02 1.38 13,560 55,200 68,760 300 300 5,000 2,500 7,500 76,860<br />
12 Katihar 18 1,134,049 62 62 310 42.53 19.00 23.53 420,360 1,711,200 2,131,560 9,300 9,300 18,000 9,000 27,000 2,177,160<br />
13 Khagaria 6 348,271 19 19 95 13.06 4.60 8.46 128,820 524,400 653,220 2,850 2,850 6,000 3,000 9,000 667,920<br />
14 Kishanganj 6 712,592 39 39 195 26.72 38.61 -11.89 264,420 1,076,400 1,340,820 5,850 5,850 6,000 3,000 9,000 1,361,520<br />
15 Lakhisarai 2 101,437 6 6 30 3.80 2.05 1.75 40,680 165,600 206,280 900 900 2,000 1,000 3,000 211,080<br />
16 Madhepura 7 1,431,240 79 79 395 53.67 0.50 53.17 535,620 2,180,400 2,716,020 11,850 11,850 7,000 3,500 10,500 2,750,220<br />
17 Madhubani 18 1,376,642 76 76 380 51.62 157.30 -105.68 515,280 2,097,600 2,612,880 11,400 11,400 18,000 9,000 27,000 2,662,680<br />
18 Munger 6 97,035 6 6 30 3.64 15.75 -12.11 40,680 165,600 206,280 900 900 6,000 3,000 9,000 217,080<br />
19 Muzaffarpur 14 2,703,171 149 149 745 101.37 62.94 38.43 1,010,220 4,112,400 5,122,620 22,350 22,350 14,000 7,000 21,000 5,188,320<br />
20 Nalanda 11 315,421 17 17 85 11.83 33.26 -21.43 115,260 469,200 584,460 2,550 2,550 11,000 5,500 16,500 606,060<br />
21 Patna 16 1,060,285 58 58 290 39.76 58.90 -19.14 393,240 1,600,800 1,994,040 8,700 8,700 16,000 8,000 24,000 2,035,440<br />
22 Purnea 13 2,258,220 124 124 620 84.68 132.29 -47.61 840,720 3,422,400 4,263,120 18,600 18,600 13,000 6,500 19,500 4,319,820<br />
23 Saharsa 7 1,381,124 76 76 380 51.79 30.00 21.79 515,280 2,097,600 2,612,880 11,400 11,400 7,000 3,500 10,500 2,646,180<br />
24 Samastipur 14 1,904,426 105 105 525 71.42 20.85 50.57 711,900 2,898,000 3,609,900 15,750 15,750 14,000 7,000 21,000 3,662,400<br />
25 Saran 15 1,437,022 79 79 395 53.89 20.33 33.56 535,620 2,180,400 2,716,020 11,850 11,850 15,000 7,500 22,500 2,762,220<br />
26 Sheohar 2 212,868 12 12 60 7.98 3.80 4.18 81,360 331,200 412,560 1,800 1,800 2,000 1,000 3,000 419,160<br />
27 Sitamarhi 13 1,807,046 99 99 495 67.76 35.93 31.84 671,220 2,732,400 3,403,620 14,850 14,850 13,000 6,500 19,500 3,452,820<br />
28 Siwan 14 1,481,302 81 81 405 55.55 16.40 39.15 549,180 2,235,600 2,784,780 12,150 12,150 14,000 7,000 21,000 2,830,080<br />
29 Supaul 11 809,393 45 45 225 30.35 21.50 8.85 305,100 1,242,000 1,547,100 6,750 6,750 11,000 5,500 16,500 1,577,100<br />
30 Vaishali 11 2,054,842 113 113 565 77.06 41.00 36.06 766,140 3,118,800 3,884,940 16,950 16,950 11,000 5,500 16,500 3,935,340<br />
31 W.Champaran 13 1,147,023 63 63 315 43.01 46.64 -3.63 427,140 1,738,800 2,165,940 9,450 9,450 13,000 6,500 19,500 2,204,340<br />
Total 310 32,393,812 1,782 1,782 8,910 1,215 1,092 123 12,081,960 49,183,200 61,265,160 267,300 267,300 310,000 155,000 465,000 62,264,760<br />
346
Sl.<br />
No.<br />
Name of<br />
Districts<br />
Total No.<br />
of Sqad<br />
(55 Sqad<br />
/10 Lakhs<br />
Population<br />
Dist. Wise Status of Spray Equipments pf Kala Azar DDT Spray<br />
Required<br />
Districwise Status of Spray Equipment of K..A D.D.T Spray<br />
Annex. III<br />
Stirrup Pump Bucket Gallan Measure Pound Measure Nosal Tip<br />
Available<br />
in Good<br />
Condition<br />
Repairable<br />
Balance<br />
Required<br />
Required<br />
Available<br />
in Good<br />
Condition<br />
Repairable<br />
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20<br />
1 Araria 118 236 237 80 -1 472 319 0 153 118 115 0 3 118 120 0 -2 590<br />
2 Arwal 2 4 0 0 4 8 0 0 8 2 0 0 2 2 0 0 2 10<br />
3 Banka 1 2 0 0 2 4 0 0 4 1 0 0 1 1 0 0 1 5<br />
4 Begusarai 55 110 258 0 -148 220 508 0 -288 55 107 0 -52 55 85 0 -30 275<br />
5 Bhagalpur 8 16 250 40 -234 32 400 9 -368 8 140 5 -132 8 140 0 -132 40<br />
6 Bhojpur 12 24 40 193 -16 48 450 50 -402 12 100 10 -88 12 100 10 -88 60<br />
7 Buxar 6 12 0 0 12 24 0 0 24 6 0 0 6 6 0 0 6 30<br />
8 Darbhanga 88 176 294 0 -118 352 279 0 73 88 127 0 -39 88 127 0 -39 440<br />
9 E.Champaran 144 288 286 177 2 576 507 138 69 144 197 23 -53 144 193 20 -49 720<br />
10 Gopalganj 38 76 234 20 -158 152 438 40 -286 38 97 20 -59 38 97 20 -59 190<br />
11 Jehanabad 2 4 234 20 -230 8 438 40 -430 2 97 20 -95 2 97 20 -95 10<br />
12 Katihar 62 124 180 104 -56 248 354 120 -106 62 142 0 -80 62 142 0 -80 310<br />
13 Khagaria 19 38 110 50 -72 76 200 116 -124 19 79 0 -60 19 79 0 -60 95<br />
14 Kishanganj 39 78 50 50 28 156 240 0 -84 39 56 0 -17 39 42 0 -3 195<br />
15 Lakhisarai 6 12 40 58 -28 24 150 46 -126 6 49 0 -43 6 49 0 -43 30<br />
16 Madhepura 79 158 252 0 -94 316 324 0 -8 79 81 0 -2 79 81 0 -2 395<br />
17 Madhubani 76 152 526 0 -374 304 820 0 -516 76 225 0 -149 76 225 0 -149 380<br />
18 Munger 6 12 140 0 -128 24 200 0 -176 6 40 0 -34 6 40 0 -34 30<br />
19 Muzaffarpur 149 298 375 0 -77 596 647 0 -51 149 186 0 -37 149 175 0 -26 745<br />
20 Nalanda 17 34 257 3 -223 68 502 10 -434 17 100 0 -83 17 130 0 -113 85<br />
21 Patna 58 116 293 130 -177 232 519 112 -287 58 193 20 -135 58 172 2 -114 290<br />
22 Purnea 124 248 190 80 58 496 413 50 83 124 130 0 -6 124 82 0 42 620<br />
23 Saharsa 76 152 150 20 2 304 350 20 -46 76 75 0 1 76 75 0 1 380<br />
24 Samastipur 105 210 224 0 -14 420 300 0 120 105 90 0 15 105 90 0 15 525<br />
25 Saran 79 158 135 101 23 316 425 135 -109 79 105 0 -26 79 105 0 -26 395<br />
26 Sheohar 12 24 0 0 24 48 0 0 48 12 0 0 12 12 0 0 12 60<br />
27 Sitamarhi 99 198 105 65 93 396 295 68 101 99 111 0 -12 99 117 0 -18 495<br />
28 Siwan 81 162 124 104 38 324 439 60 -115 81 178 5 -97 81 170 5 -89 405<br />
29 Supaul 45 90 0 0 90 180 0 0 180 45 0 0 45 45 0 0 45 225<br />
30 Vaishali 113 226 217 49 9 452 362 59 90 113 115 4 -2 113 102 0 11 565<br />
31 W.Champaran 63 126 280 105 -154 252 380 65 -128 63 120 7 -57 63 118 4 -55 315<br />
Total 1,782 3,564 5,481 1,449 -1,917 7,128 10,259 1,138 -3,131 1,782 3,055 114 -1,273 1,782 2,953 81 -1,171 8,910<br />
Balance<br />
Required<br />
Required<br />
Available<br />
in Good<br />
Condition<br />
Repairable<br />
Balance<br />
Required<br />
Required<br />
Available<br />
in Good<br />
Condition<br />
Repairable<br />
Balance<br />
Required<br />
Required<br />
347
Sl.<br />
No.<br />
Name of<br />
Districts<br />
<strong>State</strong>ment Showing The Expenditure ,Repair,Mobility, DA Supervision & IEC For Kala Azar Spray<br />
Total No. of<br />
Affected<br />
PHC<br />
Village<br />
Total No. of<br />
Sqad (55<br />
Sqad /10<br />
Lakhs<br />
Population<br />
Repair of Spray Equipments<br />
Including Nozal Tips<br />
Repai<br />
r(RS.1<br />
00/-<br />
Per<br />
Sqad)<br />
Purch<br />
ase(<br />
Per<br />
Sqad<br />
Rs.40<br />
0/)<br />
Total<br />
District<br />
MobilityFor<br />
ACMO Vehicle<br />
@ Rs.100 Per<br />
Affected Village<br />
District Mobility<br />
DMO Vehicle<br />
@ Rs.100 Per<br />
Affected<br />
Village<br />
Mobility<br />
For PHC<br />
MO.@<br />
RS.50 Per<br />
Aff. Vill.<br />
DA For<br />
Supervision @<br />
Rs. 1000 Per<br />
Affected PHC<br />
Annex. IV<br />
IEC @ Rs.<br />
1000/- Per<br />
Affected<br />
PHC per<br />
Round<br />
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15<br />
1 Araria 9 563 118 11800 47200 59000 56,300 0 28150 9000 9000 161,450<br />
2 Arwal 3 18 2 200 800 1000 1,800 0 900 3000 3000 9,700<br />
3 Banka 1 2 1 100 400 500 200 0 100 1000 1000 2,800<br />
4 Begusarai 11 245 55 5500 22000 27500 0 24,500 12250 11000 11000 86,250<br />
5 Bhagalpur 7 62 8 800 3200 4000 0 6,200 3100 7000 7000 27,300<br />
6 Bhojpur 9 120 12 1200 4800 6000 0 12,000 6000 9000 9000 42,000<br />
7 Buxar 4 16 6 600 2400 3000 1,600 0 800 4000 4000 13,400<br />
8 Darbhanga 14 455 88 8800 35200 44000 0 45,500 22750 14000 14000 140,250<br />
9 E.Champaran 20 817 144 14400 57600 72000 0 81,700 40850 20000 20000 234,550<br />
10 Gopalganj 10 261 38 3800 15200 19000 0 26,100 13050 10000 10000 78,150<br />
11 Jehanabad 5 36 2 200 800 1000 3,600 0 1800 5000 5000 16,400<br />
12 Katihar 18 543 62 6200 24800 31000 0 54,300 27150 18000 18000 148,450<br />
13 Khagaria 6 119 19 1900 7600 9500 11,900 0 5950 6000 6000 39,350<br />
14 Kishanganj 6 323 39 3900 15600 19500 32,300 0 16150 6000 6000 79,950<br />
15 Lakhisarai 2 29 6 600 2400 3000 2,900 0 1450 2000 2000 11,350<br />
16 Madhepura 7 384 79 7900 31600 39500 38,400 0 19200 7000 7000 111,100<br />
17 Madhubani 18 366 76 7600 30400 38000 0 36,600 18300 18000 18000 128,900<br />
18 Munger 6 52 6 600 2400 3000 0 5,200 2600 6000 6000 22,800<br />
19 Muzaffarpur 14 1273 149 14900 59600 74500 0 127,300 63650 14000 14000 293,450<br />
20 Nalanda 11 91 17 1700 6800 8500 0 9,100 4550 11000 11000 44,150<br />
21 Patna 16 422 58 5800 23200 29000 0 42,200 21100 16000 16000 124,300<br />
22 Purnea 13 764 124 12400 49600 62000 0 76,400 38200 13000 13000 202,600<br />
23 Saharsa 7 379 76 7600 30400 38000 0 37,900 18950 7000 7000 108,850<br />
24 Samastipur 14 701 105 10500 42000 52500 0 70,100 35050 14000 14000 185,650<br />
25 Saran 15 597 79 7900 31600 39500 0 59,700 29850 15000 15000 159,050<br />
26 Sheohar 2 48 12 1200 4800 6000 4,800 0 2400 2000 2000 17,200<br />
27 Sitamarhi 13 433 99 9900 39600 49500 0 43,300 21650 13000 13000 140,450<br />
28 Siwan 14 509 81 8100 32400 40500 0 50,900 25450 14000 14000 144,850<br />
29 Supaul 11 245 45 4500 18000 22500 24,500 0 12250 11000 11000 81,250<br />
30 Vaishali 11 751 113 11300 45200 56500 0 75,100 37550 11000 11000 191,150<br />
31 W.Champaran 13 190 63 6300 25200 31500 0 19,000 9500 13000 13000 86,000<br />
Total 310 10,814 1,782 178,200 712,800 891,000 178,300 903,100 540,700 310,000 310,000 3,133,100<br />
Total<br />
Remarks<br />
348
Sl. No.<br />
Name of<br />
Districts<br />
Total No. of PHC<br />
Total No. of Affected PHC<br />
Budget Provision For Qurative Measures of Kala Azar<br />
Mobility For Officers & MI,POL &<br />
Maintenance<br />
Mobili<br />
ty For<br />
CS<br />
Mobility Of<br />
Khaga<br />
MI<br />
riya &<br />
Mobility Purchage<br />
Madh<br />
For DMO Of 1<br />
epura<br />
For Motorcycle<br />
@ Rs.<br />
Max.RS<br />
Estimated ProjectedCase For 2009 -2010<br />
Incentive<br />
ASHA(Rs.<br />
100/-Per<br />
Projected<br />
Case For<br />
Complete<br />
Treatment)<br />
Loss Of<br />
Wages<br />
Rs.50/-For<br />
30 Days<br />
Per<br />
Projected<br />
Case<br />
During<br />
Treatment<br />
Period<br />
Strengthin<br />
g Of Bed<br />
(10 Beds<br />
Per<br />
Effected<br />
PHC @ Rs.<br />
1000/-Bed<br />
With<br />
Mattress)<br />
3000/-<br />
Per<br />
Month<br />
For 8<br />
Month<br />
s(<br />
Exclu<br />
ding<br />
Spray<br />
Period<br />
)<br />
10,000/-Per<br />
Month for<br />
8 Months (<br />
Excluding<br />
Spray<br />
Period)<br />
349<br />
Per District<br />
@ Rs.<br />
50,000/-Per<br />
Motorcycle<br />
(Except 2<br />
Motorcycle<br />
For<br />
Selected<br />
Districts)<br />
POL For<br />
Motorcy<br />
cle @30<br />
Litres<br />
Per<br />
Months<br />
@<br />
Rs.50/-<br />
For 12<br />
Months<br />
Storage Of Drugs<br />
Emphot<br />
eracin<br />
Storage<br />
In<br />
District<br />
Level @<br />
Rs. 500/-<br />
Per<br />
Month<br />
For 12<br />
Months<br />
Treatme<br />
nt Card<br />
@Rs.<br />
2.50 Per<br />
Treatme<br />
nt Card<br />
For 2<br />
Diff.Typ<br />
es of<br />
Each<br />
Card For<br />
Projecte<br />
d Case<br />
Register<br />
For Line<br />
Listing /<br />
Loss Of<br />
Wages<br />
Record<br />
@<br />
Rs.50/-<br />
For 2<br />
Register<br />
Per<br />
Eff.PHC<br />
Annex. V<br />
Hiring of<br />
Warehous<br />
e at Dist.<br />
Level for<br />
Storage of<br />
DDT @ Rs.<br />
5000/-Per<br />
Month For<br />
12 Months<br />
Kala Azar<br />
Forthnight<br />
Programm<br />
e<br />
(@Rs.4000<br />
/-Per PHC<br />
Monthly<br />
Emoulmen<br />
t of KTS 6<br />
KTS For<br />
31 Dist. @<br />
Rs.<br />
10,000/-<br />
Per Month<br />
For 12<br />
Months<br />
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20<br />
1 Araria 9 9 2,500 250,000 3,750,000 90,000 0 80,000 50,000 18,000 6,000 0 12,500 450 60,000 36,000 720,000 5,072,950<br />
2 Arwal 3 3 20 2,000 30,000 30,000 0 80,000 50,000 18,000 6,000 0 100 150 60,000 12,000 720,000 1,008,250<br />
3 Banka 10 1 20 2,000 30,000 10,000 0 80,000 50,000 18,000 6,000 0 100 50 60,000 40,000 720,000 1,016,150<br />
4 Begusarai 11 11 600 60,000 900,000 110,000 0 80,000 100,000 36,000 6,000 0 3,000 550 60,000 44,000 720,000 2,119,550<br />
5 Bhagalpur 11 7 150 15,000 225,000 70,000 0 80,000 50,000 18,000 6,000 0 750 350 60,000 44,000 720,000 1,289,100<br />
6 Bhojpur 12 9 40 4,000 60,000 90,000 0 80,000 50,000 18,000 6,000 0 200 450 60,000 48,000 720,000 1,136,650<br />
7 Buxar 7 4 40 4,000 60,000 40,000 0 80,000 50,000 18,000 6,000 0 200 200 60,000 28,000 720,000 1,066,400<br />
8 Darbhanga 14 14 1,550 155,000 2,325,000 140,000 0 80,000 100,000 36,000 6,000 0 7,750 700 60,000 56,000 720,000 3,686,450<br />
9 E.Champaran 20 20 2,000 200,000 3,000,000 200,000 0 80,000 100,000 36,000 6,000 0 10,000 1,000 60,000 80,000 720,000 4,493,000<br />
10 Gopalganj 10 10 1,200 120,000 1,800,000 100,000 0 80,000 100,000 36,000 6,000 0 6,000 500 60,000 40,000 720,000 3,068,500<br />
11 Jehanabad 5 5 30 3,000 45,000 50,000 0 80,000 50,000 18,000 6,000 0 150 250 60,000 20,000 720,000 1,052,400<br />
12 Katihar 18 18 650 65,000 975,000 180,000 0 80,000 100,000 36,000 6,000 0 3,250 900 60,000 72,000 720,000 2,298,150<br />
13 Khagaria 6 6 650 65,000 975,000 60,000 24,000 0 50,000 18,000 6,000 0 3,250 300 60,000 24,000 720,000 2,005,550<br />
14 Kishanganj 7 6 300 30,000 450,000 60,000 0 80,000 50,000 18,000 6,000 0 1,500 300 60,000 28,000 720,000 1,503,800<br />
15 Lakhisarai 4 2 50 5,000 75,000 20,000 0 80,000 50,000 18,000 6,000 0 250 100 60,000 16,000 720,000 1,050,350<br />
16 Madhepura 7 7 2,000 200,000 3,000,000 70,000 24,000 0 100,000 36,000 6,000 0 10,000 350 60,000 28,000 720,000 4,254,350<br />
17 Madhubani 18 18 1,100 110,000 1,650,000 180,000 0 80,000 50,000 18,000 6,000 0 5,500 900 60,000 72,000 720,000 2,952,400<br />
18 Munger 6 6 100 10,000 150,000 60,000 0 80,000 50,000 18,000 6,000 0 500 300 60,000 24,000 720,000 1,178,800<br />
Emphot<br />
eracin<br />
Storage<br />
In <strong>State</strong><br />
Level @<br />
Rs.<br />
1500/-<br />
Per<br />
Month<br />
For 12<br />
Months<br />
=Rs.<br />
18,000/-<br />
Grand<br />
Total
19 Muzaffarpur 14 14 3,600 360,000 5,400,000 140,000 0 80,000 100,000 36,000 6,000 0 18,000 700 60,000 56,000 720,000 6,976,700<br />
20 Nalanda 12 11 100 10,000 150,000 110,000 0 80,000 100,000 36,000 6,000 0 500 550 60,000 48,000 720,000 1,321,050<br />
21 Patna 16 16 250 25,000 375,000 160,000 0 80,000 100,000 36,000 6,000 0 1,250 800 60,000 64,000 720,000 1,628,050<br />
22 Purnea 14 13 2,050 205,000 3,075,000 130,000 0 80,000 50,000 18,000 6,000 0 10,250 650 60,000 56,000 720,000 4,410,900<br />
23 Saharsa 7 7 2,500 250,000 3,750,000 70,000 0 80,000 50,000 18,000 6,000 0 12,500 350 60,000 28,000 720,000 5,044,850<br />
24 Samastipur 14 14 1,900 190,000 2,850,000 140,000 0 80,000 100,000 36,000 6,000 0 9,500 700 60,000 56,000 720,000 4,248,200<br />
25 Saran 15 15 1,700 170,000 2,550,000 150,000 0 80,000 100,000 36,000 6,000 0 8,500 750 60,000 60,000 720,000 3,941,250<br />
26 Sheohar 2 2 150 15,000 225,000 20,000 0 80,000 50,000 18,000 6,000 0 750 100 60,000 8,000 720,000 1,202,850<br />
27 Sitamarhi 13 13 1,000 100,000 1,500,000 130,000 0 80,000 50,000 18,000 6,000 0 5,000 650 60,000 52,000 720,000 2,721,650<br />
28 Siwan 15 14 900 90,000 1,350,000 140,000 0 80,000 100,000 36,000 6,000 0 4,500 700 60,000 60,000 720,000 2,647,200<br />
29 Supaul 11 11 50 5,000 75,000 110,000 0 80,000 50,000 18,000 6,000 0 250 550 60,000 44,000 720,000 1,168,800<br />
30 Vaishali 11 11 2,800 280,000 4,200,000 110,000 0 80,000 100,000 36,000 6,000 0 14,000 550 60,000 44,000 720,000 5,650,550<br />
31 W.Champaran 16 13 3,000 300,000 4,500,000 130,000 0 80,000 100,000 36,000 6,000 0 15,000 650 60,000 64,000 720,000 6,011,650<br />
*** <strong>State</strong> Level 0 0 0 0 0 0 0 0 0 0 0 18000 0 0 0 0 0 18,000<br />
Total 338 310 33,000 3,300,000 49,500,000 3,100,000 48,000 2,320,000 2,250,000 810,000 186,000 18,000 165,000 15,500 1,860,000 1,352,000 22,320,000 87,244,500<br />
350
Annex- VI<br />
Sl.No. <strong>State</strong> Level Component Activity Financial Cost<br />
1 <strong>State</strong> Stearing Committee 30,000.00<br />
2 Brand Ambassador 50,000.00<br />
3 Computer Desktop One 50,000.00<br />
4 Laptop Three (One For SPO, One For Dy. CMO, One For AD Kala-Azar) 150,000.00<br />
5 Mobile Phone For Officer & Staff At <strong>State</strong> Level Office 60,440.00<br />
6 Laser Printer (Phone+Fax +Scanner included) 25,000.00<br />
7 Xerox Machine 150,000.00<br />
8 Meeting With Officers Of Dist. Level Alternate Month 30,000.00<br />
9 Strengthininh Of Computer & Internet Facility 30,000.00<br />
10 Supervision Of Dist. At <strong>State</strong> Level 100,000.00<br />
11 Strengthininh Of ZMO Office ( All Four ZMO) 300,000.00<br />
12 Generator with fuel 98,000.00<br />
13 IEC 400,000.00<br />
14 Total 1,473,440.00<br />
351
<strong>State</strong> - Bihar Kala -Azar Action Plan 2009-2010 , Training Part I Annexure --VII<br />
Sl. No. Name of Districts<br />
Training Of Malaria<br />
Inspector<br />
Total<br />
No. Of<br />
MI<br />
TRG Cost Of<br />
MI<br />
TwoRounds<br />
Total No.of Malaria Inspectors114 .Total Provision of Training of 114 MI . Provision<br />
of 20 Participant in each Batch =12 Batches (TwoRound) @0.695 Lakhs per Batch<br />
=8.34 Lakhs As Per NVBDCP Guideline. Two Round.<br />
Training (Induction & Re-Orientation) Of LT Training Of Health Supervisor Training Of Health Worker<br />
Total No.<br />
Of LT<br />
TRG Cost<br />
Of LT<br />
(Induction<br />
TRG)<br />
Total No.of 47 Lab Technecian .Total Provision of Induction Training of 47 Lab<br />
Technecian. Provision of 20 Participant in each Batch =2 Batches @1.25 Lakhs per<br />
Batch for 10 Days =2.5 Lakhs As Per NVBDCP Guideline .One Time<br />
TRG Cost Of<br />
LT (Re-<br />
Orientation<br />
TRG)<br />
TRG of all 47 Lab Technecian Induction .Total Provision of Induction Training of 47<br />
Lab Technecian. Provision of 20 Participant in each Batch =2 Batches<br />
@0.7562Lakhs per Batch for 5 Days =1.5124 Lakhs As Per NVBDCP Guideline .One<br />
Time<br />
Grand Total<br />
Induction &<br />
Reorientation<br />
TRG of all 47 Lab Technecian Induction & Re-Orientation Grand Total. As Per<br />
NVBDCP Guideline .One Time<br />
352<br />
Total No.<br />
Of BHI<br />
Total<br />
No. Of<br />
SI<br />
TRG Cost<br />
Of Health<br />
Supervisor<br />
Total No.of BHI =118 +SI 18 Total 136 .Total Provision of Training of 136 Health<br />
Supervisor . Provision of 25 Participant in each Batch =5 Batches For 2 Days @<br />
0.30 Lakhs per Batch =1.50 Lakhs As Per NVBDCP Guideline. One Round.<br />
Total<br />
No. Of<br />
BHW<br />
Total<br />
No. Of<br />
SW<br />
Total No.<br />
Of FW<br />
Total No.<br />
Of SFW<br />
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16<br />
1 Araria 0<br />
0<br />
0 0<br />
0 0 0 0<br />
2 Aurangabad 4 0 1 0 3 0 1 0<br />
3 Arwal 0 0 0 0 0 0 0 0<br />
4 Banka 0 0 0 0 0 0 0 0<br />
5 Begusarai 3 1 3 0 7 0 1 2<br />
6 Bhagalpur 2 1 11 1 6 0 1 2<br />
7 Bhojpur 5 1 8 0 1 0 4 2<br />
8 Buxar 0 0 0 0 0 0 0 0<br />
9 Darbhanga 4 0 4 2 4 2 4 0<br />
10 E.Champaran 7 2 12 1 5 5 1 2<br />
11 Gaya 4 8 8 0 7 0 3 1<br />
12 Gopalganj 2 2 0 0 0 0 3 1<br />
13 Jamui 0 0 0 0 0 0 0 0<br />
14 Jehanabad 0 0 0 0 0 0 0 0<br />
15 Kaimur 0 0 0 0 0 0 0 0<br />
16 Katihar 3 0 2 0 6 0 0 0<br />
17 Khagaria 0 0 0 0 0 0 0 0<br />
18 Kishanganj 0 0 0 0 0 0 0 0<br />
19 Lakhisarai 0 0 0 0 0 0 0 0<br />
20 Madhepura 0 0 0 0 0 0 0 0<br />
21 Madhubani 8 0 5 6 0 9 2 0<br />
22 Munger 5 3 4 3 11 5 2 0<br />
23 Muzaffarpur 4 1 7 0 3 0 3 0<br />
24 Nawada 2 2 1 1 0 1 2 0<br />
25 Nalanda 3 3 8 0 2 0 3 0<br />
26 Patna 10 11 11 0 9 0 5 2<br />
27 Purnea 9 0 6 1 7 0 3 0<br />
28 Rohtas 6 1 1 2 9 5 0 0<br />
29 Saharsa 6 3 6 0 3 0 0 0<br />
30 Samastipur 5 1 3 0 0 0 0 1<br />
31 Saran 6 1 6 0 4 0 0 1<br />
TRG Cost<br />
Of Health<br />
Worker<br />
Total No.of BHW =103 +SIW= 33 +FW=43 +SFW=19 Total 198 .Total Provision of<br />
Training of 198 Health Worker . Provision of 25 Participant in each Batch =8<br />
Batches For 2 Days @ 0.30 Lakhs per Batch =2.40 Lakhs As Per NVBDCP Guideline.<br />
One Round.
32 Sheikhpura 0 0 0 0 0 0 0 0<br />
33 Sheohar 0 0 0 0 0 0 0 0<br />
34 Sitamarhi 3 2 4 0 3 0 0 0<br />
35 Siwan 3 1 3 0 6 0 1 1<br />
36 Supaul 0 0 0 0 0 0 0 0<br />
37 Vaishali 5 1 4 0 5 0 3 2<br />
38 W.Champaran 5 0 0 1 2 6 1 2<br />
ZMO Office (All 4) 0 2 0 0 0 0 0 0<br />
Total 114 834,000 47 250,000 151,240 401,240 118 18 150,000 103 33 43 19 240,000<br />
353
Sl.<br />
Name of Districts<br />
No.<br />
Training of Medical Officer<br />
TRG OF MEDICAL OFFICERS<br />
Govt.Medical<br />
Referal<br />
Sub.<br />
Govt.Hospital<br />
Sadar Hospital<br />
College<br />
Hospital<br />
Hospital<br />
PHC<br />
TRG Cost of MO<br />
1 2 3 4 5 6 7 8 9<br />
1 Araria 0 0 3 0 1 9<br />
2 Aurangabad 0 0 3 1 0<br />
3 Arwal 0 0 0 0 0 3<br />
4 Banka 0 0 3 0 1 10<br />
5 Begusarai 0 0 2 1 0 11<br />
6 Bhagalpur 1 0 2 1 1 11<br />
7 Bhojpur 0 0 2 0 0 12<br />
8 Buxar 0 0 0 0 1 7<br />
9 Darbhanga 1 0 2 0 0 14<br />
10 E.Champaran 0 0 3 1 0 20<br />
11 Gaya 1 0 2 1 0<br />
12 Gopalganj 0 0 3 1 1 10<br />
13 Jamui 0 0 3 0 1<br />
14 Jehanabad 0 0 2 1 0 5<br />
15 Kaimur 0 0 2 0 1<br />
16 Katihar 0 0 3 1 0 18<br />
17 Khagaria 0 0 1 1 0 6<br />
18 Kishanganj 0 0 2 0 1 7<br />
19 Lakhisarai 0 0 1 0 1 4<br />
20 Madhepura 0 0 1 1 0 7<br />
21 Madhubani 0 0 2 1 1 18<br />
22 Munger 0 0 1 1 0 6<br />
23 Muzaffarpur 1 0 1 1 0 14<br />
24 Nawada 0 0 2 1 0<br />
25 Nalanda 0 0 3 1 1 12<br />
26 Patna 2 7 4 0 3 16<br />
27 Purnea 0 0 2 1 0 14<br />
28 Rohtas 0 0 1 1 1<br />
29 Saharsa 0 0 0 1 0 7<br />
354<br />
TRG of all Govt. Medical College Medical Officer @ 2 MO For 6 Med.Coll<br />
=12,Gont.Hospital @ 2 x 7= 14,Referal Hospital@1x7=70, Sadar Hospital @<br />
2x24 =48, Sub Divisional Hospital @ 1x22 =22, PHC @1x336=336 .Total<br />
Provision of Training of 502 Medical Officers.Provision of 25 particepents<br />
in each batch =20 Batch @ 1.2 Lakhs p er Batch for three days =24.0 Lakhs<br />
as per NVBDCP Guide line ,One Time<br />
Annexure VIII
30 Samastipur 0 0 1 1 3 14<br />
31 Saran 0 0 3 1 0 15<br />
32 Sheikhpura 0 0 1 0 1 0<br />
33 Sheohar 0 0 1 0 1 0<br />
34 Sitamarhi 0 0 1 1 0 13<br />
35 Siwan 0 0 2 1 0 15<br />
36 Supaul 0 0 1 0 1 11<br />
37 Vaishali 0 0 2 1 0 11<br />
38 W.Champaran 0 0 2 1 1 16<br />
ZMO Office (All 4) 0 0 0 0 0 0<br />
Total 6 7 70 24 22 336 2,400,000<br />
355
Training of PRI Members<br />
Sl. No. Name of Districts Advocasy Workshop & Training of PRI<br />
Annexure -IX<br />
Block<br />
Panchyat<br />
Zila Parishad Members( Per Dist.15<br />
Members)<br />
Total Cost Of PRI<br />
Members<br />
1 2 3 4 5 6<br />
1 Araria 9 221 15<br />
2 Aurangabad 0 0 0<br />
3 Arwal 0 0 15<br />
4 Banka 11 185 15<br />
5 Begusarai 18 257 15<br />
6 Bhagalpur 17 242 15<br />
7 Bhojpur 14 228 15<br />
8 Buxar 11 142 15<br />
9 Darbhanga 19 329 15<br />
10 E.Champaran 27 387 15<br />
11 Gaya 0 0 0<br />
12 Gopalganj 14 234 15<br />
13 Jamui 0 0 0<br />
14 Jehanabad 12 161 15<br />
15 Kaimur 0 0 0<br />
16 Katihar 16 238 15<br />
17 Khagaria 7 129 15<br />
18 Kishanganj 7 118 15<br />
19 Lakhisarai 7 80 15<br />
20 Madhepura 13 170 15<br />
21 Madhubani 21 399 15<br />
22 Munger 9 101 15<br />
23 Muzaffarpur 16 387 15<br />
24 Nawada 0 0 0<br />
25 Nalanda 20 249 15<br />
26 Patna 23 331 15<br />
27 Purnea 14 246 15<br />
28 Rohtas 0 0 0<br />
29 Saharsa 10 164 15<br />
30 Samastipur 20 381 15<br />
31 Saran 20 0 15<br />
32 Sheikhpura 0 0 0<br />
33 Sheohar 5 54 15<br />
34 Sitamarhi 17 273 15<br />
35 Siwan 16 293 15<br />
36 Supaul 11 180 15<br />
37 Vaishali 16 292 15<br />
38 W.Champaran 18 354 15<br />
ZMO Office (All 4) 0 0 0<br />
Total No.of Blocks =438 x15 BDC Members Per Blocks=6570 Persons +Total No. Of Panchyats =6825 = 6825 Mukhiya +31 Districts<br />
x15 Zila Parishad Members =465 Members= Total 13860 Members .Total Provision of Training of PRI Members 13860 . Provision of<br />
50 Participant in each Batch =277 Batches For 1 Days @ 0.02 Lakhs per Batch =5.54 Lakhs As Per NVBDCP Guideline. One Round .<br />
Total 438 6,825 465 554,000<br />
356
Training of Spray Worker & ASHA Annexure -X<br />
Sl. No.<br />
Name of<br />
Districts<br />
Training Of Spray Worker<br />
Training Of MPW (ASHA)<br />
Contractual<br />
Total<br />
No. Of<br />
SFW<br />
Total<br />
No. Of<br />
FW<br />
TRG Cost Of<br />
Spray Worker<br />
Total No. Of<br />
ASHA<br />
TRG Cost Of<br />
MPW (ASHA)<br />
1 2 3 4 5 6 7<br />
1 Araria 118 590<br />
2026<br />
2 Arwal 2 10 644<br />
3 Banka 1 5 1455<br />
4 Begusarai 55 275 2018<br />
5 Bhagalpur 8 40 1877<br />
6 Bhojpur 12 60 1621<br />
7 Buxar 6 30 1074<br />
8 Darbhanga 88 440 2890<br />
9 E.Champaran 144 720 2686<br />
10 Gopalganj 38 190 1868<br />
11 Jehanabad 2 10 769<br />
12 Katihar 62 310 1486<br />
13 Khagaria 19 95 967<br />
14 Kishanganj 39 195 648<br />
15 Lakhisarai 6 30 568<br />
16 Madhepura 79 395 1403<br />
17 Madhubani 76 380 2751<br />
18 Munger 6 30 820<br />
19 Muzaffarpur 149 745 2544<br />
20 Nalanda 17 85 2017<br />
21 Patna 58 290 2549<br />
22 Purnea 124 620 2002<br />
Total No.of Spray Worker FW=8910 +SFW=1782 Total 10692 .Total Provision<br />
of Training of 10692 Spray Worker . Provision of 50 Participant in each<br />
Batch =214 Batches For 1 Days @ 0.02 Lakhs per Bat ch =4.28 Lakhs As Per<br />
NVBDCP Guideline One Round.<br />
23 Saharsa 76 380 777<br />
24 Samastipur 105 525 3214<br />
25 Saran 79 395 2289<br />
26 Sheohar 12 60 426<br />
27 Sitamarhi 99 495 464<br />
28 Siwan 81 405 1665<br />
29 Supaul 45 225 2538<br />
30 Vaishali 113 565 1477<br />
Total No.of MPW(ASHA)Contractual 52065.Total Provision of Training of<br />
52065 MPW(ASHA)Contractual . Provision of 50 Participant in each Batch<br />
=1041 Batches For 1 Days @ 0.02 Lakhs per Batch =20.8 2 Lakhs As Per<br />
NVBDCP Guideline One Round.<br />
31 W.Champaran 63 315 2532<br />
Total 1,782 8,910 428,000 52,065 2,082,000<br />
357
i=kkad----------------------------------<br />
izs"kd]<br />
MkW- vkj-,u-ik.Ms;]<br />
la;qDr funs’kd lg jkt; dk;Z e inkeysfj;k@dkyktkj]<br />
fcgkj] iVuk<br />
lsok esa]<br />
funs’kd]<br />
jk"V“h; oSDVj tfur jksx fu;a=k.k dk;Z e<br />
22&’kkeukFk ekxZ] fnYyh&54<br />
iVuk] fnukad----------------<br />
fo"k; & iqu% la’kksf/r eysfj;k ds fu;a=k.kkFkZ fo kh; o"kZ 2009&10 dk ctV<br />
izkoDyu A<br />
egk’k;]<br />
mi;q ZDr fo"k; ds laca/ esa dguk gS fd jkT; ds 38 ftyks a esa ls ek=k 7 ftys ;Fkk<br />
eaaqxsj] teqbZ] uoknk] vkSjaxkckn] x;k] dSeqj rFkk jksgrkl eysfj;k ls xaHkhj jQi ls izHkkfor<br />
ftys gS aA bu ftyksa esa fujks/kRed dkjZokbZ ds rgr Mh-Mh-Vh- fNM+dko dk izLrko gSA<br />
mijksDr lkr eysfj;k izHkkfor ftyksa ds ftyk eysfj;k ink- ls miyc/ dk;Z<br />
;kstuk dh ekax dh xbZ Fkh A uoknk ftys dks NksM+dj vU; N% ftyksa ls fNM+dko dk;Z<br />
;kstuk izkIr ugha gqbZ A lEHkor% jkT; esa 7-01-09 ls py jgs vjktif=kr deZpkfj;ksa ds<br />
gM+rky ds dkj.k dk;Z ;kstuk vizkIr gSA ,slh fLFkfr esa ftysokj fNM+dko ds fy, yf{kr<br />
tual[;k bR;kfn nsuk laHko ugha gS] iyr% jkT; eq[;ky; Lrj ij miyC/ lwpuk ds<br />
vuqlkj ctV izLrko rS;kj fd;k x;k gS A<br />
fcgkj jkT; dh dqy vkcknh 10]00]00]000 gS ftles a eysfj;k izHkkfor lkr ftyksa<br />
dh dqy tula[;k 1]66]66]603 (vFkkZr~ 16-66 feyh;u gS) eysfj;k izHkkfor lkr ftyksa<br />
ds (1-925) feyh;u tula[;k dks fNM+dko ls vkPNkfnr djus dk izLrko gSA fooj.kh I<br />
esa 7 eysfj;k izHkkfor ftyksa dk ftysokj tula[;k bR;kfn dk fooj.k fn;k x;k gS A<br />
358
(d) fujks/kRed dkjZokbZ<br />
jkT; ds lkr eysfj;k izHkkfor ftyksa ds vuqekfur 2 feyh;u tul[a;k esa<br />
fNM+dko gsrq fNM+dko ny rFkk Mh-Mh-Vh- dk vko’;drk bl izdkj gS &<br />
fNM+dko o ny & ,d feyh;u tula[;k esa eysfj;k i…fr ls fNM+dko gsrq<br />
dqy 44 fNM+dko ny 75 fnuksa ds fy, izko/ku gS A izR;sd o"kZ 2 p fNM+dko djk;k<br />
tkuk gS A ;g fNM+dko ebZ ls flrEcj rd djkuk gS A bl rjg dqy &<br />
(a) fNM+dko ------------------- 44 × 2 ------------------- 88<br />
Js- {ks- dk;Zjr fNM+dko ny dh la[;k X 1---------- 88<br />
{ks- dk;Zjr dk;Zjr fNM+dko ny dh la[;k X 5--------- 440<br />
(b) Mh-Mh-Vh& ,d fefy;u tula[;k ds fy, 75 eh-Vu ,d p ds fy,<br />
dqy Mh-Mh-Vh- dh vko’;drk & 2 × 75 = 150 eh- Vu ,d p esa<br />
orZeku esa eysfj;k ;sktuk esa 15 eh- Vu Mh-Mh-Vh- miyC/ gS rFkk 210 eh- Vu Mh-Mh-Vh-<br />
Hkkjr ljdkj }kjk miyc/ djk;k tk jgk gS A bl rjg dqy 225 eh- Vu Mh-Mh-Vhmiyc/<br />
gS tks ,d p fNMdko ds fy, i;kZIr gS A<br />
1. Je ,oa fu;kstu foHkkx }kjk fNM+dko etnwjksa ds fy, la’kksf/r etnwjh nj [<br />
S.F.W. @ Rs. 113/- izfrfnu rFkk F.W. @ Rs. 92/- izfrfnu dh nj ls etnwjh dk vkdyu<br />
fd;k x;k gS A etnwjh en dk izLrkfor jkf’k bl izdkj gS &<br />
,d p vFkkZr~ 75 fnuksa ds fy,<br />
Js- {ks- dk;ZdrkZ dk etnwjh& 88 × 75 × 113 Rs. 7,45,800<br />
{ks- dk;ZdrkZ dk etnwjh & 440 × 75 × 92 Rs. 30,36,000<br />
dqy etnwjh Rs. 37,81,800<br />
2. Mh-Mh-Vh-
ftyksa esa Mh-Mh-Vh- ds HkaMkj.k dh leqfpr O;oLFkk ugha gS vr% Mh-Mh-Vh- dks jkT;<br />
Hk.Mkj fuxe ds xksnke ftl ftyksa esa jkT; HkaMkj ftyk dk xksnke ugha gS] ogk¡<br />
fu;ekuqlkj HkkM+ s ij xksnke ysus gsrq) izfr ftyk izfrekg Rs. 500/- dh nj ls HkaMkj.k<br />
’kqYd dk izko/ku fd;k x;k gS A<br />
izLrkfor jkf’k & 7 × 500 × 12 Rs. 42,000/-<br />
dqy Rs. 2,17,000/-<br />
3. dk;kZy; O;; & fNM+dko esas mi;ksx gksus okys xs: feV~Vh] NUuk ds fy, diM+k]<br />
jftLVj] lknk dkxt bR;kfn izR;sd fNM+dko ny dks miyC/ djk;k tkuk gS A ftlds<br />
fy, izfr fNM+dko ny Rs. 300/- dh nj ls jkf’k dk izko/ku fd;k x;k gSA ftyk<br />
eq[;ky; esa Hkh LVs’kujh bR;kfn ds fufer Rs. 2000/- izfr ftyk dks jkf’k dk izko/ku<br />
fd;k x;k gS A<br />
izLrkfor jkf’k & fNM+dko ny gsrq & fNM+dko ny × 300<br />
88 × 300 - Rs. 26,400/-<br />
ftyk eq[;ky; gsrq 7 × 2000 - Rs. 14,000/-<br />
dqy Rs. 40,400/-<br />
4. fNM+dko midj.kksa dh ejEerh rFkk vko’;d ikVZl dk ; &<br />
ftyk esa fNM+dko midj.kksa dh ejEerh ,oa LVhji iEi ds fy, oklj xSyu] lqrk]<br />
pqVdh oklj] ,oa vU; ikVZl ds fy, izfr fNM+dko ny Rs. 100/- rFkk uksty VhIl ds<br />
; gsrq izfr fNM+dko ny 400/- dh nj ls jkf’k dk izko/ku fd;k x;k gSA<br />
izLrkfor jkf’k & midj.kksa dh ejErh ,oa ikVZl ; ds fy,<br />
(fNM+dko ny × 100) 88 × 100 -Rs. 8,800/-<br />
uksty VhIl ; gsrq - 88 × 400- Rs. 35,200/-<br />
5. iQkWfxx& eysfj;k izHkkfor ftyksa esa eysfj;k egkekjh dh fLFkfr esa ekykfFk;ku dk<br />
iQkfxax djkuk vko’;d izrhr gksrk gS rkfd eysfj;k dk jksdFkke izHkkoh
ds iQkfxax dk ctV dk izko?kku fd;k x;k gSA izR;sd ftys esa nl yk[k izfr ftyk ds nj<br />
nj ls & 4 ftyk X 10 yk[k = 40 yk[k dk izLrko gSA<br />
6. i;Zos{k.k & Mh-Mh-Vh- fNM+dko ds liQy i;Zos{k.k ,oa xq.koDrk iw.kZ fNM+dko dh<br />
n‘f"V ls i;Zos{k.k fd;k tkuk gS A ftu ftyksa esa xkM+h miyC/ gS] mu ftyksa dks xkM+h ds<br />
fy, bZ/u] ejEerh (fu;ekuqlkj) ds fy, jkf’k rFkk ftu ftyksa esa xkM+h miyC/ ugha gS<br />
39 ftyksa dks jkT; Lok- lfefr }kjk vuqeksfnr nj ij ,d p fNM+dko ds fy, jkf’k<br />
dk izLrko gS A izR;sd ekg 20 fnu ds i;Zos{k.k ds dk;Z lEiknu djus gsrq ,d p ds<br />
fy, 50 fnuksa ds i;Zos{k.k gsrq jkf’k dk vkdyu fd;k x;k gS A<br />
izLrkfor jkf’k& 7 × 650 × 50 -Rs. 2,27,500/-<br />
eysfj;k ;kstuk esa 5 ekg ds fNM+dko vof/ esa i;Zos{k.k gsrq jkf’k fujks/kRed<br />
dkjZokbZ ls miyC/ djk;k tk jgk gS A ’ks"k 7 ekg ds i;Zos{k.k gsrq dkyktkj ;kstuk ls<br />
x;k ,oa eqxsaj ds ftyk eysfj;k ink- dks jkf’k miyc/ djk;k x;k gS A ’ks"k ikWp ftys<br />
;Fkk teqbZ ,oa dSeqj ds vij eq[; fpfdRlk inkf/dkjh dks] (ftyk eysfj;k inkf/dkjh<br />
dk in ;gkW Lohd‘r ugh gS) jksgrkl] uoknk] vkSjxkckn ftys ds ftyk eysfj;k<br />
inkf/dkjh] dqy ikWp ftyks dks 10 gtkj :i;k izfrekg dh nj ls lkr ekg ds fy;s<br />
dqy &<br />
5 ftyk X 10 gtkj :i;s x 7 ekg = 3]50]000 :i;s dk izko/ku j[kk x;k gSaA<br />
7- izpkj&izlkj & fNM+dko ds iwoZ fNM+dko ds laca/ esa turk dks tkudkjh fn;k<br />
tkrk gS rkfd os fNM+dko ds fy, l≤ rS;kj jgs A bl fufer iksLVj] iEiysV]
4- fNM+dko midj.k& Rs. 44, 000.00<br />
5- i;Zos{k.k & Rs. 2,27,500.00<br />
6- izpkj&izlkj & Rs. 1,05,000.00<br />
,d p fNM+dko ds fy, dqy izLrkfor jkf’k Rs. 44,15,700.00<br />
nks p fNM+dko ds fy, dqy izLrkfor jkf’k Rs. 88,31,400/-<br />
7. iQkfxax& Rs. 40,00,000/-<br />
8. ftyk eysfj;k dk;Zy; ds lkr ekg dk i;Zos{k.k&<br />
Rs. 3,50,000/-<br />
dqy 1,31,81,400/-<br />
(,d djksM- ,drhl yk[k ,dklh gtkj pkj lkS :i;s )<br />
([k) mipkjkRed dkjZokbZ &<br />
eysfj;k ds jksxh ds igpku ds fy, Toj fifM+r jksfx;ksa dk jDriV tkWp fd;k<br />
tkrk gSA jDriV dh deh ds dkj.k foxr o"kksZ esa jDriV laxzg y{; ds vuqlkj ugha<br />
gqvk] iQyr% eysfj;k jksfx;ksa dk lgh vkdM+k miyC/ ugha gks ik;k A bl fufer LykbM<br />
,oa fj,tsUV ; dk izLrko gSA<br />
1- Hkkjr ljdkj ls izkIr fn’kk funs’k ds vuqlkj dqy vkcknh dk 10» jDriV laxzg<br />
okf"kZd fd;k tkuk gS A fcgkj dh dqy vkcknh nl djksM+ (yxHkx) gS A vr% jDriV<br />
laxzg ,d djksM+ gksuk pkfg, A lkr eysfj;k izHkkfor ftyksa dk dqy tula[;k<br />
1]66]66]603 gS A<br />
ftyksa ls izkIr lwpukuqlkj foxr o"kksZ esa djhc 1]25]000 jDriV laxzg fd;k x;k<br />
gSA vr% orZeku esa 5 yk[k jDriV ; dk izLrko gS A ,d jDriV ds ; ds fy,<br />
Rs. 1/- O;; gksxk A<br />
dqy 5]00]000 jDriV ds ; ij dqy O;; & Rs. 5,00,000/-<br />
362
jDriV lxazg ds fy, fizfdax fufMy] :bZ] LizhV rFkk fj,tsUV dh vko’;drk<br />
gksxhA bl fufer 5]00]000 fizfdax fufMy dk ; dk izLrko gS A izfr fizfdax fufMy<br />
:- 1-50 dh nj ls dqy O;; :- 7]50]000@& dkVu] LizhV rFkk fj,tsUV ds ; ij :-<br />
4@& izfr LykbM dh nj ls O;; dk vkdyu fd;k x;k gS A vr% 5 yk[k LykbM ds<br />
fy, dkVu] LizhV rFkk fj,tsUV ij dqy 5,00,000 × 4 = 20,000,00/- O;; gksxk A bl rjg<br />
jDriV ; ,oa fj,tsUV bR;kfn ij dqy O;; & 5]00]000 $ 7]50]000 $ 20]00]000<br />
:- 32]50]000 O;; gksxk A<br />
2. i;Zos{k.k & i;Zos{k.k dh n‘f"V ls eysfj;k izHkkfor ftyksa ds eysfj;k fujh{kd dks<br />
izfr ftyk nks eksVj lkbZfdy ; dk izLrko gS rkfd i;Zos{k.k dk;Z lqpk: ,oa fu;fer<br />
fd;k tk ldsA ,d eksVj lkbfdy ds ; ij :- 50]000@& O;; gksxk A bl rjg 7<br />
ftyksa eysfj;k izHkkfor ftyksa esa ls ek=k uoknk] vkSjaxkckn] jksgrkl ftyksa dks izfr ftyk 2<br />
eksVj lkbfdy ds<br />
dkyktkj ;kstuk ls eksVjlkbfdy<br />
; dk izLrko gS ’ks"k 4 eysfj;k izHkkfor ftyksa x;k] eaqxsj dks<br />
inkf/dkjh ds vf/uLFk ftys s dkyktkj ls izHkkfor gS A<br />
; dk izLrko gS A eqaxsj ,oa x;k ftyk eysfj;k<br />
izLrkfor jkf’k & 3 × 2 × 50,000 - 3,00,000/-<br />
eksVjlkbfdy ds fy, ba/u gsrq izfr eksVj lkbfdy 30 yhVj izfr ekg dh nj ls<br />
12 ekg ds fy, jkf’k dk izko/ku fd;k tk jgk gSA (izfr yhVj isV“kWy :- 50@& dh nj<br />
ls)<br />
dqy izLrkfor jkf’k 6 × 30 × 50 × 12 - Rs. 1,08,000/-<br />
dqy Rs. 4,08,000/-<br />
3. eysfj;k ls cpko ds fy, osMusV &<br />
& dqy 7 ftyksa esa izHkkfor tula[;k & 20 yk[k<br />
& 5 O;fDr ds vk/kj ij 1 ifjokj dh<br />
x.kuk djus ij dqy ifjokj dh la[;k & 4 yk[k<br />
& ,d ifjokj esa 2 osMusV dk izko/ku<br />
j[kus ij dqy osMusV dh vko’;drk & 8 yk[k<br />
363
ysfdu dsoy ch-ih-,y- xHkZorh efgyk dks izkFkfedrk ds vk/kj ij osMusV<br />
miyC/ djk;k tk;xk A ;g Epidemic out Break okys ftyksa dks gh eqgS;k djkus dk<br />
izLrko gS A bl rjg dqy 1 yk[k osMusV dh vko’;drk dk vkdyu fd;k x;k gS] tks<br />
Hkkjr ljdkj }kjk miyC/ djk;k tk;xk A<br />
izLrko gS A<br />
&<br />
4. izf’k{k.k &<br />
osMusV dh vkiwfrZ es a
(?k)- Lok- dk;ZorkZ dk izf’k{k.k &<br />
lkr eysfj;k izHkkfor ftyksa esa dqy 30 cqfu;knh Lok- fujh{kd] 11 fuxjkuh dk;ZdrkZ] 8<br />
{ks=kh; dk;ZdrkZ rFkk 1 Js"B {ks=kh; dk;ZdrkZ gS A bl rjg dqy 50 dk;ZdrkZ dks izf’kf{kr<br />
fd;k tkuk gS A 25 izf’k{k.kkFkhZ izfr oSp dh nj ls nks oSp esa izf’k{k.k dk izLrko gS A<br />
izf’k{k.k vof/ 2 fnuksa dh gksxh A izf’k{k.k ij izfr oSp fd 30]000@& dh nj ls O;;<br />
dk izLrko gS A<br />
dqy izLrkfor jkf’k & 2 × 30,000 60,000/-<br />
bl rjg izf’k{k.k ij dqy O;; &<br />
(d) e- fu- ds izf’k{k.k & 1]39]000@&<br />
([k) iz;ksx’kkyk izkoSf/d & 200]620@&<br />
(x) cq- Lok- fu- ,oa fu- fujh{kd & 30]000@&<br />
(?k) Lok- dk;ZdrkZ & 60]000@&<br />
vuqyXaud lyaXu<br />
dqy & 4,29,620/-<br />
365
NAMMIS<br />
National Anti Malaria Management Information System (NAMMIS) ds rgr lHkh<br />
ftyksa dks Web based NAMMIS Software dk;Z e ls Internet ds ekŁ;e ls tksM+uk ,oa<br />
Report ladfyr fd;k tkuk gS A 2009-10 ds Action Plan ds rgr fuEuor ctV izLrko gS<br />
&<br />
1- lHkh ftyksa esa miyC/ djk, x, Computer esa CD/DVD Writer ugh yxk gSA vr% lHkh<br />
40 computer esa CD/DVD writer yxkus gsrq izfr CD/DVD writer 1500/- :- izfr dh nj<br />
ls dqy 40 dEI;wVj gsrq & 40 × 1500 Rs. = 60,000.00 dk izLrko gSA<br />
2- eq[;ky; esa yxs nks Computer System gsrq 2GB RAM, 250 GB Hard Disk dk izLrko<br />
gS A vHkh System esa 256 MB RAM ,oa 40 GB Hard Disk yxk gS tks eq[;ky; esa<br />
dk;Z dks ns[krs gq, de gS A blesa 2GB RAM dh dher vuqekfur 3000-00 :-<br />
gS rFkk vfrfjDr nks 250 GB Hard Disk dh vuqekfur dher 3500-00 :- gS] dk<br />
izLrko gS A dqy 6500@& :- dk izLrko gSA<br />
3- lHkh 40 dEI;wVj gsrq ikVZl lfgr AMC (Annual Maintence Cost) dk izLrko gSA blesa<br />
izfr dEI;wVj izfr o"kZ AMC dk vuqekfur ykxr yxHkx 6]000@& (N% gtkj :i;s<br />
ek=k) dh nj ls 40 × 6,000/- :- 2]40]000@& (nks yk[k pkyhl gtkj :i;s ek=k)<br />
yxus dh laHkkouk gS] izLrko gS A<br />
4- NAMIS dks dk;kZfUor djus gsrq lHkh 40 dEI;wVj esa Internet dh lqfo/k gsrq Broad<br />
Band/USB Broad Band yxkuk vfuok;Z gS A blds rgr Broad Band dk nj izfrekg<br />
vuqekfur :-800@& = 800 × 12 ekg 9]600@& okf"kZd ,oa Broad Band ds Installation<br />
charge yxHkx 4500@& :- izfr System yxkus dh laHkkouk gSA dqy vuqekfur ykxr &<br />
1]80]000 :-<br />
9600 + 1,80,000 = 1,89,600 = 00 yxus dh laHkkouk gS A<br />
5- lHkh ftyk eysfj;k dk;kZy; esa Basic Telephone dh lqfo/k iwoZ ls gh miyC/ gSA<br />
Internet dh lqfo/k gsrq Telephone dh ekfld fcy vuqekfur :i;k 500@& izfr<br />
ftyk dh nj ls 38 ftys gsrq 38 × 500 = 19,000.00 :i;s × 12 ekg 2]28]000-00<br />
366
:i;s ,oa jkT; Lrjh; eq[;ky; gsrq 1000 :i;s izfr ekg dh nj ls 12 ekg gsrq 12]<br />
000@& :i;s] dqy& 2]28]000 00<br />
12]000 00<br />
2,40,000 00 :- yxus dk ctVh; izLrko gSA<br />
6- lHkh ftyksa dks Comptuer ds Cartridage, CD/DVD, Xerox Paper, UPS ds cSV“h ,oa vU;<br />
vko’;d oLrqvksa dh [kpZ gsrq vuqekfur 5]000@& :i;s dh nj ls 38 ftyk ×<br />
5000.00 = 1,90,000.00 ,oa jkT; Lrjh; eq[;ky; ij 20]000-00<br />
dqy & 2]10]000-00 :- [kpZ gksus dh laHkkouk gS A<br />
7- NAMMIS dks dk;kZfUor djus gsrq lHkh ftys dks ftyk eysfj;k inkf/dkjh dqy<br />
la[;k&24] lHkh ftyksa ds ACMO = 14, 24 ftyksa ds dfeZ;ksa 48 ,oa vU; l{ke<br />
O;fDr dks izf’k{k.k fn;k tkuk t:jh gS A blesa dqy vuqekfur & 100 O;fDr;ksa dks<br />
izf’k{k.k fn;k tkuk gS A jkT; Lrj ls nks dfeZ;ksa dks Master Trainer ds :i esa<br />
NVBDCD }kjk izf’k{k.k fn;k tk pqdk gS A ;s TOT lHkh lacaf/r O;fDr;ksa dks<br />
izf’k{k.k] nsus gsrq izf’k{kq ,oa izf’k{kd dk ekuns; ,oa vU; vk/kjHkwr lqfo/kvksa gsrq<br />
10 O;fDr izfr cSp nks fnu dh nj ls 10 cSp (100 O;fDr;ksa gsrq) @ 25,000/- =<br />
dqy 2]50]000@&:- yxus dh laHkkouk gS A<br />
NAMMIS ds izf’k{k.k ds vykok lkjk [kpZ <strong>State</strong> Component Plan esa j[kk x;k gS<br />
dqy [kpZ dafMdk&<br />
1- 60]000-00<br />
2- 6]500-00<br />
3- 2]40]000-00<br />
4- 1]89]600-00<br />
5- 2]40]000-00<br />
6- 2]10]000-00<br />
7 2]50]000-00<br />
11]96]100-00<br />
367
l rjg ;kstuk dk dqy O;;<br />
1- fujks/kRed 1]31]81]400-00<br />
2- mipkjkRed 37]08]000-00<br />
3- izf’k{k.k 429]620-00<br />
4- ukfel gsrq 11]96]100-00<br />
1,85,15,120.00<br />
5. ,d yk[k csMusV @ 250 Rs./ izfr csMusV = 2]50]00]000@& :i;s<br />
dqy ctV dk izko?kku &<br />
4,35,15,120@&<br />
nks vuqyXaud layXu<br />
fo’oklHkktu<br />
la;qDr funs’kd lg jkT; dk;Z e inkeysfj;k@dkyktkj<br />
fcgkj] iVuk<br />
Kkikad---------------------------------@ iVuk fnukad-----------------------------<br />
izfrfyfi iz/ku lfpo] Lok- ,oa i- d- foHkkx] fcgkj iVuk] funs’kd izeq[k Lok- lsok;sa<br />
fcgkj] dk;Zikyd funs’kd] jkT; Lok- lfefr] iVuk dks vuqyXud lfgr lwpukFkZ ,oa<br />
vko’;d dkjZokbZ gsrq izf"kr A<br />
Kkikad---------------------------------@ iVuk fnukad-----------------------------<br />
la;qDr funs’kd lg jkT; dk;Z e inkeysfj;k@dkyktkj<br />
fcgkj] iVuk<br />
izfrfyfi {ks=kh; funs’kd] Lok- ,oa i- d- foHkkx] Hkkjr ljdkj] bfUnjk Hkou] ikWpoka<br />
eafaty] csyh jksM]iVuk] dks vuqyXud lfgr lwpukFkZ ,oa vko’;d dkjZokbZ gsrq izf"krA<br />
la;qDr funs’kd lg jkT; dk;Z e inkeysfj;k@dkyktkj<br />
fcgkj] iVuk<br />
368
Sl.<br />
No.<br />
Name of<br />
Districts<br />
Dist.Wise Malaria Affected Population , No. of Sqad,DDT Requirement ,Wages,Contegency,Equipment Repair,Mobility & Transportation of DDT of Malarial DDT Spray for 2009-2010<br />
Total No. of Malaria<br />
Affected<br />
PHC HSC Populatio<br />
n<br />
Total<br />
No. of<br />
Sqad<br />
(44<br />
Sqad<br />
/10<br />
Lakhs<br />
Popula<br />
tion<br />
Total No. of<br />
Workers<br />
SF<br />
W<br />
FW<br />
DDT 50%<br />
Status (In<br />
Meric Ton )<br />
Require.<br />
Available<br />
SFW(Rs.<br />
113/-Per<br />
SFW Per<br />
Day For<br />
75 Days)<br />
WAGES<br />
FW(Rs.92/-<br />
Per FW Per<br />
Day For 75<br />
Days)<br />
Total<br />
Office<br />
Expen<br />
ses (@<br />
Rs<br />
300/-<br />
Per<br />
Sqad<br />
EXPENDETURE FOR I ROUND<br />
Contigen<br />
cy At<br />
Dist.<br />
Level (@<br />
Rs. 2000/-<br />
Per Dist.<br />
Repair<br />
of<br />
Spray<br />
Equip<br />
ments<br />
Includi<br />
ng<br />
Nozal<br />
Tips @<br />
Rs.<br />
500/-<br />
Per<br />
Sqad<br />
District<br />
Mobility<br />
DMO<br />
Vehicle<br />
@<br />
Rs.650/-<br />
Per<br />
Affected<br />
Dist. For<br />
50 Days<br />
Transportation of<br />
DDT<br />
For @ Rs.<br />
25,000 /-<br />
Per Dist.<br />
Storage of<br />
DDT @<br />
RS. 500/-<br />
Per Month<br />
For 12<br />
Months<br />
IEC @<br />
Rs.15000/<br />
- Per Dist.<br />
Total<br />
(Column No.<br />
13 to 20)<br />
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 22<br />
1 Munger 1 26 154,135 8 8 40 12 10 67,800 276,000 343,800 2400 2000 4000 32500 25000 6000 15000 430,700 861400<br />
100<br />
000 0 1861400<br />
0<br />
2 Jamui 5 47 548,070 24 24 120 42 30 203,400 828,000 1,031,400 7200 2000 12000 32500 25000 6000 15000 1,131,100<br />
100<br />
700<br />
2262200 000<br />
00<br />
0<br />
3332200<br />
3 Nawada 2 11 106,942 5 5 25 5 50 42,375 172,500 214,875 1500 2000 2500 32500 25000 6000 15000 299,375 598750 0<br />
700<br />
00<br />
668750<br />
4 Rohtas 2 15 192,106 9 9 45 15 30 76,275 310,500 386,775 2700 2000 4500 32500 25000 6000 15000 474,475 948950<br />
5 Kaimur 2 12 153,035 7 7 35 12 30 59,325 241,500 300,825 2100 2000 3500 32500 25000 6000 15000 386,925 773850<br />
6 Aurangabad 1 3 630,194 28 28 140 48 40 237,300 966,000 1,203,300 8400 2000 14000 32500 25000 6000 15000 1,306,200 2612400 0<br />
700<br />
00<br />
2682400<br />
7 Gaya 5 12 140,000 7 7 35 11 20 59,325 241,500 300,825 2100 2000 3500 32500 25000 6000 15000 386,925 773850 0 0 773850<br />
Total 18 126 1,924,482 88 88 440 145 210 745,800 3,036,000 3,781,800 26,400 14,000 44,000 227,500 175,000 42,000 105,000 4,415,700<br />
EXPEN<br />
DETUR<br />
E FOR II<br />
ROUND<br />
8,831,40<br />
0<br />
FO<br />
GGI<br />
NG<br />
100<br />
000<br />
0<br />
100<br />
000<br />
0<br />
MO<br />
BAL<br />
ITY<br />
FOR<br />
SEV<br />
EN<br />
MO<br />
NTH<br />
700<br />
00<br />
700<br />
00<br />
GRAND<br />
TOTAL<br />
2018950<br />
1843850<br />
4,00<br />
350,<br />
0,00 13,181,400<br />
000<br />
0<br />
<strong>STATE</strong> LEVEL 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0<br />
Purchage of Blood Slide & Reagent 3,250,000<br />
1 Curarive Purchase of Motorcycle for Supervision 408,000<br />
Transportation & Purchase of Bednets 25,050,000<br />
MI 139,000<br />
2 Training<br />
LT 200,620<br />
BHI & SI 30,000<br />
Health Worker 60,000<br />
3 NAMMIS 1,196,100<br />
Grand Total Of Malaria Programme 43,515,120<br />
369
Dist.Wise Malaria Training of Malaria Inspector,Lab Technecian,health Supervisor & Health Worker for 2009-2010<br />
Annexure II<br />
Sl.<br />
No.<br />
Name of<br />
Districts<br />
Training Of Malaria<br />
Inspector<br />
Training (Induction & Re-Orientation) Of LT<br />
Training Of Health<br />
Supervisor<br />
Training Of Health Worker<br />
Total<br />
No. Of<br />
MI<br />
TRG Cost Of<br />
MI<br />
TwoRounds<br />
Total<br />
No. Of<br />
LT<br />
TRG Cost<br />
Of LT<br />
(Induction<br />
TRG)<br />
TRG Cost Of<br />
LT (Re-<br />
Orientation<br />
TRG)<br />
Grand Total<br />
Induction &<br />
Reorientation<br />
Total<br />
No. Of<br />
BHI<br />
Total<br />
No.<br />
Of SI<br />
TRG Cost Of<br />
Health<br />
Supervisor<br />
Total<br />
No.<br />
Of<br />
BHW<br />
Total<br />
No. Of<br />
SW<br />
Total<br />
No. Of<br />
FW<br />
Total<br />
No. Of<br />
SFW<br />
TRG Cost Of<br />
Health Worker<br />
1 2 OK OK OK OK OK OK OK<br />
1 Aurangabad 4<br />
Total No.of Malaria Inspectors 21 .Total<br />
Provision of Training of 21 MI . Provision of<br />
20 Participant in each Batch =1Batches<br />
(TwoRound) @0.695 Lakhs per Batch = 1.39<br />
Lakhs As Per NVBDCP Guideline. Two Round.<br />
0<br />
Total No.of 14 Lab Technecian .Total Provision<br />
of Induction Training of 14 Lab Technecian.<br />
Provision of 20 Participant in each Batch = 1<br />
Batches @1.25 Lakhs per Batch for 10 Days<br />
=1.25 Lakhs As Per NVBDCP Guideline .One<br />
Time<br />
TRG of all 14 Lab Technecian Induction .Total<br />
Provision of Induction Training of 14 Lab<br />
Technecian. Provision of 20 Participant in<br />
each Batch =1 Batches @0.7562La khs per<br />
Batch for 5 Days =0.7562 Lakhs As Per<br />
NVBDCP Guideline .One Time<br />
TRG of all 14 Lab Technecian Induction & Re -<br />
Orientation Grand Total. As Per NVBDCP<br />
Guideline .One Time<br />
1 0<br />
2 Gaya 4 8 8 0<br />
3 Jamui 0 0 0 0<br />
4 Kaimur 0 0 0 0<br />
5 Munger 5 3 4 3<br />
6 Nawada 2 2 1 1<br />
7 Rohtas 6 1 1 2<br />
Total 21 14 15 6<br />
Total No.of BHI =15 +SI 6 Total 21 .Total<br />
Provision of Training of 21 H ealth Supervisor<br />
. Provision of 25 Participant in each Batch =1<br />
Batches For 2 Days @ 0.30 Lakhs per Batch<br />
=0.30 Lakhs As Per NVBDCP Guideline. One<br />
Round.<br />
3 0 1 0<br />
7 0 3 1<br />
0 0 0 0<br />
0 0 0 0<br />
11 5 2 0<br />
0 1 2 0<br />
9 5 0 0<br />
30 11 8 1<br />
Total No.of BHW =30 +SW= 11 +FW= 8<br />
+SFW=1 Total 50 .Total Provision of Training<br />
of 50 Health Worker . Provision of 25<br />
Participant in each Batch =2 Batches For 2<br />
Days @ 0.30 Lakhs per Batch =0.60 Lakhs As<br />
Per NVBDCP Guideline. One Round.<br />
370
i=kkad----------------------------------<br />
izs"kd]<br />
MkW- vkj-,u-ik.Ms;]<br />
la;qDr funs’kd lg jkt; dk;Z e inkeysfj;k@dkyktkj]<br />
fcgkj] iVuk<br />
lsok esa]<br />
funs’kd]<br />
jk"V“h; oSDVj tfur jksx fu;a=k.k dk;Z e<br />
22&’kkeukFk ekxZ] fnYyh&54<br />
iVuk] fnukad----------------<br />
fo"k;& iqu% la’kksf/r Msaxq ,oa fpdquxhfu;k dh jksdFkke ds fy, fo kh; o"kZ<br />
2009-10 gsrw ctV izLrko A<br />
egk’k;]<br />
mi;q ZDr fo"k; Ms axq ,oa fpdquxhfu;k dh jksdFkku ,oa mipkjkRed mik; gsrw jkT;<br />
ds NMCH, iVuk dks Sentival Surveillance Hospital ds :i esa /;fur dk izLrko gS]<br />
Sentinel Site ds Laboratory Strengthening gsrq NVBDEP Guide Line ds vkyksd esa "One<br />
time financial grant Rs. 25.00 Lakhs will be provided to each ARLS (Apex Referral<br />
Laboratories) for the infrastructure development. In addition, recurring expenditure to the<br />
tune of Rs. 1.00 lakh to each ARL and Rs. 0.50 Lakh to each SHs (Approved by<br />
GO1/will be provided to meet the contingency expenditure of the Laboratory" dk izko/ku<br />
fd;k tk ldrk gS A fcgkj esa Msxq dk dsl o"kZ 2008&09 esa dsoy ,d ik;k x;k gS tks<br />
dSeqj ftys dk gSA Chikungunya dk dsl o"kZ 2008&09 esa Reported ugh gSA Hkfo"; esa<br />
Dengu & Chikungunya mipkjkRed ,oa fujks/kRed gsrq 10 yk[k :i;s dk ctVh;<br />
izko/ku gS A dqy Dengu & Chikungunya dk ctVh; izko/ku = 25.00 Laks + 1.00 Lakhs<br />
+ 0.50 Lakhs + 10.00 Lakh = 36.50 Lakh.<br />
fo’oklHkktu<br />
la;qDr funs’kd lg jkT; dk;Z e inkeysfj;k@dkyktkj<br />
fcgkj] iVuk<br />
372
Kkikad---------------------------------@ iVuk fnukad-----------------------------<br />
izfrfyfi iz/ku lfpo] Lok- ,oa i- d- foHkkx] fcgkj iVuk] funs’kd izeq[k Lok- lsok;sa<br />
fcgkj] dk;Zikyd funs’kd] jkT; Lok- lfefr] iVuk dks vuqyXud lfgr lwpukFkZ ,oa<br />
vko’;d dkjZokbZ gsrq izf"kr A<br />
Kkikad---------------------------------@ iVuk fnukad-----------------------------<br />
la;qDr funs’kd lg jkT; dk;Z e inkeysfj;k@dkyktkj<br />
fcgkj] iVuk<br />
izfrfyfi {ks=kh; funs’kd] Lok- ,oa i- d- foHkkx] Hkkjr ljdkj] bfUnjk Hkou] ikWpoka<br />
eafaty] csyh jksM]iVuk] dks vuqyXud lfgr lwpukFkZ ,oa vko’;d dkjZokbZ gsrq izf"krA<br />
la;qDr funs’kd lg jkT; dk;Z e inkeysfj;k@dkyktkj<br />
fcgkj] iVuk<br />
373
Dengu & Chikungunia Dist.Wise Plan 2009-2010<br />
Sl.No.<br />
Name of<br />
Dist.<br />
Curative &<br />
Presumptive<br />
Measures<br />
Fogging of JE @ Rs.<br />
10.00 Lakhs / Dist.<br />
Sentinal Survillance<br />
Hospital<br />
Grand Total<br />
1 HQ. 1000000 -- 0 0<br />
2 Patna 0 0 2650000 2650000<br />
Total 1000000 0 2650000 3650000<br />
Note-<br />
Amount for Curative & Presumptive Measures & Sentinal Survillance Hospital for PMCH<br />
Patna kept in <strong>State</strong> Level Office.<br />
374
i=kkad----------------------------------<br />
izs"kd]<br />
MkW- vkj-,u-ik.Ms;]<br />
la;qDr funs’kd lg jkt; dk;Z e inkeysfj;k@dkyktkj]<br />
fcgkj] iVuk<br />
lsok esa]<br />
funs’kd]<br />
jk"V“h; oSDVj tfur jksx fu;a=k.k dk;Z e<br />
22&’kkeukFk ekxZ] fnYyh&54<br />
iVuk] fnukad----------------<br />
fo"k; & iqu% la’kksf/r Japanese Encephalitis dh jksdFkke ds fy, fo kh; o"kZ<br />
2009-10 gsrw ctV izLrko A<br />
egk’k;]<br />
1- mijksDr fo"k;d foÙkh; o"kZ 2009&10 gsrq x;k] floku]eqtIQiqj ,oa if'pe pEikj.k ftys esa<br />
Vaccination izLrko gSA blds iwoZ 2007 eqtQjiqj esa yxHkx 41-00 yk[k dk ,oa csfr;k esa yxHkx<br />
48-00 yk[k #i;s dk ctVh; izko/kku FkkA bl foÙkh; o"kZ esa x;k gsrq 50-00 yk[k dk cTkVh; izko/kku<br />
j[kk x;k gSA<br />
dqy pkj ftys x 50 yk[k = 2 djksM- :i;s<br />
2- J.E ds fy, Sentinal Surveillance Hospital ds :Ik esa SKMCH es eqtQjiqj]<br />
ihŒ,eŒlhŒ,pŒ] iVuk ,oa ANMCH, x;k dks j[kk x;k gSA NVBDCP ds Guide ds<br />
vkyksd esa izfr Sentinal Surveillance Hospital gsrq 26-50 dk nj fu/kkZfjr gSA vr% dqy<br />
26.50 X 3 = 79.50 yk[k #i;s dk ctVh; izko/kku gSA<br />
3- Sentinel Site ds Laboratory Strengthening gsrq NVBDEP Guide Line ds<br />
vkyksd esa "One time financial grant Rs. 25.00 Lakhs will be provided to<br />
each ARLS (Apex Referral Laboratories) for the infrastructure development.<br />
In addition, recurring expenditure to the tune of Rs. 1.00 lakh to each ARL<br />
and Rs. 0.50 Lakh to each SHs (Approved by GO1/will be provided to meet<br />
the contingency expenditure of the Laboratory"<br />
4- J.E ds jksdFkke gsrq mÙkj izns'k ls lVs fcgkj ds ftys ;Fkk csfr;k] eksfrgkjh] eqtQjiqj] lhoku]<br />
xksikyaxt rFkk tsŒbZŒ ls izHkkfor vU; ftys ;Fkk&x;k] uoknk] vkSjaxkckn] tgkukckn ,oa vjoy<br />
esa QkWfxax dk izLrko gSA bu 10 ftyksa esa vuqekfur 10 yk[k #Πizfr ftyk dh nj ls 1 djksM-<br />
#i;s dk ctVh; izLrko j[kk x;k gSA<br />
JE dk dqy cTkV &<br />
375
(i) Vaccination - 200.00 yk[k<br />
(ii) Sentinal Surveillance Hospital - 79.50 yk[k<br />
(iii) Fogging - 100.00 yk[k<br />
379-50 yk[k<br />
fo’oklHkktu<br />
la;qDr funs’kd lg jkT; dk;Z e inkeysfj;k@dkyktkj<br />
fcgkj] iVuk<br />
Kkikad---------------------------------@ iVuk fnukad-----------------------------<br />
izfrfyfi iz/ku lfpo] Lok- ,oa i- d- foHkkx] fcgkj iVuk] funs’kd izeq[k Lok- lsok;sa<br />
fcgkj] dk;Zikyd funs’kd] jkT; Lok- lfefr] iVuk dks vuqyXud lfgr lwpukFkZ ,oa<br />
vko’;d dkjZokbZ gsrq izf"kr A<br />
Kkikad---------------------------------@ iVuk fnukad-----------------------------<br />
la;qDr funs’kd lg jkT; dk;Z e inkeysfj;k@dkyktkj<br />
fcgkj] iVuk<br />
izfrfyfi {ks=kh; funs’kd] Lok- ,oa i- d- foHkkx] Hkkjr ljdkj] bfUnjk Hkou] ikWpoka<br />
eafaty] csyh jksM]iVuk] dks vuqyXud lfgr lwpukFkZ ,oa vko’;d dkjZokbZ gsrq izf"krA<br />
la;qDr funs’kd lg jkT; dk;Z e inkeysfj;k@dkyktkj<br />
fcgkj] iVuk<br />
376
Sl.No.<br />
Name of Dist.<br />
JE Dist.Wise Plan 2009-2010<br />
Vaccination of JE @<br />
Rs. 50.00 Lakhs /<br />
Dist.<br />
Fogging of JE @ Rs.<br />
10.00 Lakhs / Dist.<br />
Sentinal Survillance<br />
Hospital<br />
Grand Total<br />
1 Gaya 5000000 1000000 2650000 8650000<br />
2 Siwan 5000000 1000000 0 6000000<br />
3 Muzaffarpur 5000000 1000000 2650000 8650000<br />
4 W.Champaran 5000000 1000000 0 6000000<br />
5 Nawada 0 1000000 0 1000000<br />
6 Aurangabad 0 1000000 0 1000000<br />
7 Jehanabad 0 1000000 0 1000000<br />
8 Arwal 0 1000000 0 1000000<br />
9 East Champaran 0 1000000 0 1000000<br />
10 Gopalganj 0 1000000 0 1000000<br />
11 Patna 0 0 2650000 2650000<br />
Total 20000000 10000000 7950000 37950000<br />
Note-<br />
Amount for Sentinal Survillance Hospital for ANMMCH,Gaya,SKMCH,Muzaffarpur,PMCH Patna kept<br />
in <strong>State</strong> Level Office.<br />
377
i=kkad----------------------------------<br />
izs"kd]<br />
MkW- vkj-,u-ik.Ms;]<br />
la;qDr funs’kd lg jkt; dk;Z e inkiQysfj;k]<br />
fcgkj] iVuk<br />
lsok esa]<br />
funs’kd]<br />
jk"V“h; oSDVj tfur jksx fu;a=k.k dk;Z e<br />
22&’kkeukFk ekxZ] fnYyh&54<br />
iVuk] fnukad----------------<br />
fo"k; & la’kksf/r iQysfj;k fnol eukus gsrq fof k; o"kZ 2009-10 gsrw ctV<br />
izkDdyu Hkstus ds laca/ esaA<br />
egk’k;]<br />
mi;qDr fo"k;d o"kZ 09&10 dk ctV izkDdyu (vkSicf/d) bl i=k ds lkFk<br />
layXu fd;k tk jgk gSA jkT; esa deZpkfj;ksa ds gM+rky ds dkj.k ftyksa ls iw.kZ vkWadM+k<br />
ugh izkIr gks ldk gSA iQyLo:Ik vkSicf/kd ctV izkDdyu Hkstk tk jgk gSA iw.kZ lwpuk<br />
izkIr gksus ds ckn ctV izkDdyu esa la’kks/u lHkao gSA o kZeku ctV izkDdyu<br />
6]52]83]000@& (N% djksM- ckou yk[k rsjklh gtkj :i;s) dk gSA<br />
izkDdyu dk fuekZ.k dk vko’;drk ,oa vk/kkj dk fuEu :Ik esa inokj vkadyu<br />
fd;k x;k gSA<br />
ctV izkDdyu dqy izkFkfed LokLF; dsUnzks 398 ,oa ftyk eq[;ky;ksas 38 esa jg<br />
jgs yxHkx 10 djksM+ tula[;k dks iQkbZysfj;k fu;a=.k dk;Zdze ds rgr vPNkfnr djus ds<br />
mn~ns’; ls rS;kj fd;k x;k gS] ftlds vUrxZr ,d fu/kZfjr frfFk dks mez ds fglkc ls<br />
fu/kZfjr ek=k esa Mh0 bZ0 lh0 f[kykus ds dk;Z e djk;k tk;sxk ,oa mDr fnol dks NqVs<br />
gq, tuekul dks vxys nks fnu rd ekSi&vi p pykus dk dk;Z e rS;kj fd;k x;k<br />
gSA ctV izkDdyu jkT; Lrj ,oa ftyk Lrj ij O;; gksus okyh jkf’k ds vk/kj ij rS;kj<br />
fd;k x;k gS A<br />
(d) jkT; Lrj<br />
378
(1) ftyk Lrjh; inkf/dkjh dk izf’k{k.k%& blds rgr dqy 1]52]000@& jkf’k dks<br />
vkadfyr fd;k x;k gS a A iQkbysfj;k fnol dks iw.kZ lqxerk ls lapkyu gsrq izR;sd<br />
ftyk ls ,d&,d inkf/kdkjh dks izf’kf{kr fd;s tkus dk dk;Z e gSA<br />
izf’k{k.k ,d fnolh; gksxk rFkk 19&19 dh la[;k esa izf’k{k.kkfFkZ;ksa dks izf’kf{kr<br />
fd;s tkus dk y{; j[kk x;k gS] tks izf’k{k.kksijkUr ftyk Lrjh; izf’k{k.k ds<br />
izf’k{kd dk dk;Z djsxsaA (ctV vkadyu dafMdk 6 nz"VO;)<br />
(2) izpkj izlkj%& jkT; Lrj ij izpkj izlkj gsrq 10]00]000@& :i;s vkadfyr fd;k<br />
x;k gS] ftlds rgr nwjn’kZu] jsfM;ksa] lekpkj i=k ds lans’k nsuk ,oa izpkj&izlkj<br />
lkexzh;ksa dk eqnz.k djkuk lfEefyr gSA (ctV vkadyu dafMdk 7 nz"VO;)<br />
(3) jkT; Lrj ij izf’k{k.k gsrq 60]000@& :i;sA<br />
(4) jkT; Lrj ij ikjkesfMdy LVkiQ dk izf’k{k.k 1]50]000@& :i;sA<br />
(5) ih0vks0,y0%& bl en esa 3]00]000@& :i;s dk vkadyu fd;k x;k gS] ftlds<br />
rgr jkt; eq[;ky; ls lHkh ftyksa ds fy;s Hksts tkus okys I;Zos{kh inkf/kdkjh ds<br />
Hkze.k gsrq ckgu dh lqfo/k miyC/ djkus ,oa bZ/u vkfn esa O;; fd;k tk;sxkA<br />
(ctV vkadyu dafMdk 14 ekad 1 nz"VO;)<br />
([k) ftyk Lrj ij O;; gksus okyh jkf’k dk vkadyu<br />
(6) ,d ftyk leUo; lfefr dh cSBd gsrq izfr ftyk 15]00]000=00 dh nj ls<br />
dqy 5]70]000 (ikWp yk[k lRrj gtkj :i;s) ek=k dk vkadyu fd;k x;k gSA<br />
bl jkf’k ls iQkbZysfj;k fnol ds liQy lapkyu gsrq fofHkUu foHkkxksa ds<br />
inkf/dkfj;ks a dh leUo; cSBd dk vk;kstu fd;k tk;sxkA(ctV vkadyu dafMdk<br />
8 nz"VO;)<br />
(7) izpkj izlkj en%& bl en esa ftyksa dh tula[;k ,oa izkFkfed LokLF; dsUnzks dh<br />
la[;k ds vk/kj ij ctV izkDdyu dafMdk 9 esa nZ’kk;h x;h gS rFkk bl en esa<br />
dqy 14]55]000@& :i;s vkadfyr dh x;h gSA lEcfU/kr ftyk bl en dh jkf’k<br />
ls cSuj @iksLVj ,oa vU; la’kk/uks ls iQkbZysfj;k fnol ds lEcU/ esa vke turk ds<br />
chp izpkj izlkj dk dk;Z djsxsaA<br />
(8) ftyk Lrjh; fpfdRlk inkf/dkfj;ks a dk izf’k{k.k%& bl en esa ctV izkDdyu<br />
dafMdk 10 esa dqy 22]05]000@& (ckbZl yk[k ikWap gtkj) :i;s dks vkadfyr<br />
379
fd;k x;k gSA jkT; Lrj ij izf’kf{kr fpfdRlk inkf/dkjh ftyk Lrj izkFkfed<br />
LokLF; dsUnzks ds fpfdRlk inkf/dkjh dks izf’kf{kr djsxsaA izf’k{k.k ,d fnolh;<br />
gksxkA<br />
(9) ikjkesfMdy dehZ dk izf’k{k.k% ctV izkDdyu dafMdk 11 esa ftyksa ds ikjk<br />
esfMdy LVkiQ dk izf’k{k.k iz[k.M Lrj ij dk;Zjr ikjk esfMdy LVkiQ dks mDr<br />
iz[k.M ds izf’kf{kr fpfdRlk inkf/dkjh }kjk izf’kf{kr fd;k tk;sxkA bl en esa<br />
mDr dafMdk esa ftyksa ds uke ds lkeus jkf’k dk vkadyu fd;k x;k gSA vkadfyr<br />
jkf’k 18]85]000@&:i;k gSA<br />
(10) ykbZu fyfLVax % ctV izkDdyu ds dafMdk 12 esa dqy 15]20]000@& (iUnzg yk[k<br />
chl gtkj) :i;s izkDdfyr gSA<br />
(11) ftyk Lrj ij isV“ksy ywcjhdsV gsrq en esa 11]98]000@&(X;kjg yk[k vuBkuos<br />
gtkj :i;s)A<br />
(12) jkf=k jDr iV laxzg% ctV izkDdyu ds dafMdk 13 esa dqy 5]74]546@& (ikWp<br />
yk[k pkSgrj gtkj ikWp lkS fN;kyhl) :i;s vkadfyr dh x;h gS A<br />
(13) nok forj.k d kkZ dk izf’k{k.k en% bl en esa dqy 2]62]410@& (nks yk[k oklB<br />
gtkj pkj lkS nl nok forj.k d kkZ dks 92-00 (ckuos) :i;s ds nj ls ,d fnu<br />
ds fy;s dqy 2]41]41]720@& (nks djksM+ ,drkyhl yk[k ,drkyhl gtkj lkr<br />
lkS chl ) :i;s ek=k izkDdfyr gSA<br />
(14) nok forj.k d kkZ ekuns; jkf’k% bl en esa ctV izkDdyu ds dafMdk 7 esa nks<br />
yk[k cklB gtkj pkj lkS nl nok forj.k d kkZ dks 92 :i;s dh nj ls ,d fnu<br />
ds fy, dqy 2]41]41]720@& (nks djksM+ ,drkyhl yk[k ,drkyhl gtkj lkr<br />
lkS chl) :i;s ek=k izkDdfyr gSA<br />
(15) nok i;Zos{kd dk izf’k{k.k jkf’k% bl en dk ctV izkDdyu ds dafMdk 5 esa<br />
26]239-00 (NCchl gtkj nks lkS mupkfyl lqijckbtj dks 113@& :i;s dh nj<br />
ls ,d fnu ds fy, dqy 2]96]5007@& (nks djksM- fN;kuos yk[k ikWp gtkj<br />
lkr) :i;s izkDdfyr gSA<br />
(16) lqijokbtj dk ekuns; jkf’k% bl en esa ctV izkDdyu ds dafMdk 9 esa 26]239@&<br />
(Nchl gtkj nks lkS mupkfyl dks 113@& :i;s dh nj ls ,d fnu ds fy, dqy<br />
380
2]96]5007@& (nks djksM- fN;kuos yk[k ikWp gtkj lkr :i;s) dk ctV<br />
izkDdfyr gSA<br />
fo’oklHkktu<br />
la;qDr funs’kd lg jkT; dk;Z e inkiQysfj;k<br />
fcgkj] iVuk<br />
Kkikad---------------------------------@ iVuk fnukad-----------------------------<br />
izfrfyfi iz/ku lfpo] Lok- ,oa i- d- foHkkx] fcgkj iVuk] funs’kd izeq[k Lok- lsok;sa<br />
fcgkj] dk;Zikyd funs’kd] jkT; Lok- lfefr] iVuk dks vuqyXud lfgr lwpukFkZ ,oa<br />
vko’;d dkjZokbZ gsrq izf"kr A<br />
Kkikad---------------------------------@ iVuk fnukad-----------------------------<br />
la;qDr funs’kd lg jkT; dk;Z e inkiQysfj;k<br />
fcgkj] iVuk<br />
izfrfyfi {ks=kh; funs’kd] Lok- ,oa i- d- foHkkx] Hkkjr ljdkj] bfUnjk Hkou] ikWpoka<br />
eafaty] csyh jksM]iVuk] dks vuqyXud lfgr lwpukFkZ ,oa vko’;d dkjZokbZ gsrq izf"krA<br />
la;qDr funs’kd lg jkT; dk;Z e inkiQysfj;k<br />
fcgkj] iVuk<br />
381
l0 fu0<br />
,e- Mh- ,- dk izLrkfor la’kksf?kr ctV izkDdyu fof k; o"kZ 2009&10<br />
jk"V“h; iQkbysfj;k fnol 2009&10 ds eukus gsrq fofHkUu enksa dk vyx&vyx rS;kj fd;k<br />
tk jgk gS] ftldk C;kSjk fuEu izdkj gSA<br />
Dzekad en dk uke izLrkfor jkf’k<br />
1. jkT; Lrj ij ftys ds fofdRlk ink0 dk izf’k{k.k gsrq 152000<br />
2. jkT; Lrj ij vkbZ0bZ0lh0 1000000<br />
3. jkT; Lrj ij izf’k{k.k 60000<br />
4. jkT; Lrj ij ikjkesfMdy LVkiQ dk izf’k{k.k 150000<br />
5. jkT; Lrj ij isV“ksy ,oa Y;wcfjdsV gsrq 3,00000<br />
6. ftyk Lrj ij leUo; lfefr dk cSBd nks fnuks dk 570000<br />
7. ftyk Lrj ij vkbZ0bZ0lh0 1455000<br />
8. ftyk Lrj ij fp0ink0 dk izf’k{k.k 2205000<br />
9. ftyk Lrj ij ikjkesfMdy LVkiQ dk izf’k{k.k 1885000<br />
10. ftyk Lrj ij ykbu fyLVhax gsrq 1520000<br />
11. ftyk Lrj ij isV“ksy Y;wcfjdsV gsrq 1198000<br />
12. jkf=k jDr iV laxzg 574546<br />
13. ftyk Lrj ij nok forjdks dk izf’k{k.k gsrq 24141720<br />
14. ftyk Lrj ij nok forjdks dk ekuns; jkf’k 24141720<br />
15. ftyk Lrj ij i;Zos{kdks dk izf’k{k.k jkf’k 2965007<br />
i;Zos{kdks dk ekuns; jkf’k 2965007<br />
Dqy 65,283,000<br />
la- fu- Lok0 lsok,a as lg<br />
jkT; dk;Zdze ink0 iQkbysfj;k<br />
fcgkj] iVukA<br />
382
<strong>State</strong>- Bihar NAME OF PROGRAMME , MASS DRUG ADMINISTRATION ,BUDGET FOR 2009-2010<br />
Sl.No.<br />
<strong>State</strong> &<br />
NameOf<br />
District<br />
No. Of<br />
PHC<br />
Dist. HQ<br />
Total<br />
(PHC<br />
Dist.HQ)<br />
Training<br />
Of Dist.<br />
Officer<br />
IEC ( <strong>State</strong><br />
Level)<br />
Dist.& Coordination<br />
Meeting(Two<br />
Meeting in<br />
each Dist.)<br />
IEC ( For<br />
Dist. HQ)<br />
Traing For MO<br />
Training For<br />
Para<br />
Medical<br />
Staff<br />
Line Listing<br />
Night<br />
Blood<br />
Survey<br />
POL Total (A) Remarks<br />
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16<br />
1 <strong>State</strong> Level 0 0 0 152,000 1,000,000 0 0 60,000 150,000 0 0 300,000 1,662,000<br />
2 Araria 9 1 10 0 0 15,000 35,000 55,000 40,000 35,000 16,698 28,000 224,698<br />
3 Aurangabad 11 1 12 0 0 15,000 40,000 55,000 45,000 35,000 16,698 33,000 239,698<br />
4 Arwal 3 1 4 0 0 15,000 30,000 20,000 25,000 20,000 16,698 13,000 139,698<br />
5 Banka 10 1 11 0 0 15,000 35,000 50,000 40,000 35,000 16,698 30,000 221,698<br />
6 Begusarai 11 1 12 0 0 15,000 35,000 50,000 40,000 35,000 16,698 33,000 224,698<br />
7 Bhagalpur 11 1 12 0 0 15,000 40,000 55,000 40,000 40,000 16,698 33,000 239,698<br />
8 Bhojpur 12 1 13 0 0 15,000 40,000 55,000 45,000 40,000 16,698 35,000 246,698<br />
9 Buxar 7 1 8 0 0 15,000 35,000 55,000 40,000 40,000 16,698 23,000 224,698<br />
10 Darbhanga 13 1 14 0 0 15,000 40,000 55,000 60,000 45,000 16,698 38,000 269,698<br />
11 E.Champaran 20 1 21 0 0 15,000 50,000 90,000 90,000 65,000 16,698 55,000 381,698<br />
12 Gaya 19 1 20 0 0 15,000 50,000 90,000 90,000 65,000 16,698 53,000 379,698<br />
13 Gopalganj 10 1 11 0 0 15,000 35,000 55,000 45,000 35,000 16,698 30,000 231,698<br />
14 Jamui 7 1 8 0 0 15,000 35,000 45,000 40,000 40,000 16,698 23,000 214,698<br />
15 Jehanabad 4 1 5 0 0 15,000 25,000 25,000 25,000 20,000 16,698 16,000 142,698<br />
16 Kaimur 9 1 10 0 0 15,000 35,000 45,000 40,000 30,000 16,698 28,000 209,698<br />
17 Katihar 11 1 12 0 0 15,000 40,000 55,000 40,000 40,000 16,698 33,000 239,698<br />
18 Khagaria 6 1 7 0 0 15,000 35,000 55,000 40,000 30,000 16,698 20,000 211,698<br />
19 Kishanganj 7 1 8 0 0 15,000 35,000 55,000 45,000 30,000 16,698 23,000 219,698<br />
20 Lakhisarai 4 1 5 0 0 15,000 25,000 25,000 25,000 20,000 16,698 15,000 141,698<br />
21 Madhepura 7 1 8 0 0 15,000 35,000 55,000 40,000 30,000 16,698 23,000 214,698<br />
22 Madhubani 19 1 20 0 0 15,000 50,000 90,000 90,000 60,000 16,698 53,000 374,698<br />
23 Munger 6 1 7 0 0 15,000 35,000 55,000 40,000 30,000 16,698 20,000 211,698<br />
24 Muzaffarpur 14 1 15 0 0 15,000 45,000 70,000 65,000 45,000 16,698 40,000 296,698<br />
25 Nawada 10 1 11 0 0 15,000 40,000 55,000 40,000 35,000 16,698 30,000 231,698<br />
26 Nalanda 12 1 13 0 0 15,000 40,000 65,000 40,000 45,000 16,698 35,000 256,698<br />
383
27 Patna 16 1 17 0 0 15,000 50,000 90,000 90,000 70,000 16,698 45,000 376,698<br />
28 Purnea 11 1 12 0 0 15,000 40,000 55,000 45,000 40,000 16,698 33,000 244,698<br />
29 Rohtas 13 1 14 0 0 15,000 40,000 55,000 60,000 45,000 16,698 38,000 269,698<br />
30 Saharsa 7 1 8 0 0 15,000 35,000 50,000 45,000 30,000 16,698 23,000 214,698<br />
31 Samastipur 14 1 15 0 0 15,000 45,000 70,000 60,000 50,000 16,698 40,000 296,698<br />
32 Saran 15 1 16 0 0 15,000 45,000 70,000 65,000 50,000 16,698 43,000 304,698<br />
33 Sheikhpura 3 1 4 0 0 15,000 30,000 25,000 25,000 20,000 16,698 13,000 144,698<br />
34 Sheohar 3 1 4 0 0 15,000 25,000 25,000 25,000 45,000 16,698 13,000 164,698<br />
35 Sitamarhi 13 1 14 0 0 15,000 40,000 55,000 65,000 50,000 16,698 38,000 279,698<br />
36 Siwan 15 1 16 0 0 15,000 40,000 70,000 55,000 30,000 16,698 43,000 269,698<br />
37 Supaul 9 1 10 0 0 15,000 35,000 55,000 45,000 40,000 16,698 28,000 234,698<br />
38 Vaishali 11 1 12 0 0 15,000 40,000 55,000 45,000 40,000 16,698 33,000 244,698<br />
39 W.Champaran 16 1 17 0 0 15,000 50,000 90,000 90,000 65,000 16,698 45,000 371,698<br />
Total 398 38 436 152,000 1,000,000 570,000 1,455,000 2,205,000 2,035,000 1,520,000 634,524 1,498,000 11,069,524<br />
384
<strong>State</strong>- Bihar NAME OF PROGRAMME , MASS DRUG ADMINISTRATION ,BUDGET FOR 2009-2010<br />
Sl.No.<br />
<strong>State</strong> &<br />
NameOf<br />
District<br />
No. Of<br />
House in<br />
Dist.<br />
No. of Drug<br />
Distri.in Dist<br />
No. of<br />
Supervisior<br />
Training Of<br />
Drug<br />
Distributer in<br />
Dist. (@ Rs.<br />
92 Each)<br />
Honararium Of<br />
Drug Distri.( @<br />
Rs. 92 Each)<br />
Training Of<br />
Supervisior<br />
(113 Each)<br />
Honararium of<br />
Supervision in<br />
Dist. @ Rs.<br />
113/- Each<br />
Toatl (B)<br />
Toatl (A)<br />
( From<br />
Previous<br />
Sheet)<br />
Grand Total<br />
( A+B)<br />
1 2 3 4 5 6 7 8 9 10 11 12<br />
1 <strong>State</strong> Level 0 0 0 0 0 0 0 0 1,662,000 1,662,000<br />
2 Araria 416,693 8,400 838 772,800 772,800 94,694 94,694 1,734,988 224,698 1,959,686<br />
3 Aurangabad 359,820 7,240 724 666,080 666,080 81,812 81,812 1,495,784 239,698 1,735,482<br />
4 Arwal 99,698 2,000 200 184,000 184,000 22,600 22,600 413,200 139,698 552,898<br />
5 Banka 271,286 5,450 545 501,400 501,400 61,585 61,585 1,125,970 221,698 1,347,668<br />
6 Begusarai 379,947 7,650 765 703,800 703,800 86,445 86,445 1,580,490 224,698 1,805,188<br />
7 Bhagalpur 424,352 8,510 851 782,920 782,920 96,163 96,163 1,758,166 239,698 1,997,864<br />
8 Bhojpur 347,780 7,000 700 644,000 644,000 79,100 79,100 1,446,200 246,698 1,692,898<br />
9 Buxar 213,834 4,300 430 395,600 395,600 48,590 48,590 888,380 224,698 1,113,078<br />
10 Darbhanga 508,044 10,200 1,020 938,400 938,400 115,260 115,260 2,107,320 269,698 2,377,018<br />
11 E.Champaran 538,386 10,750 1,075 989,000 989,000 121,475 121,475 2,220,950 381,698 2,602,648<br />
12 Gaya 563,963 11,300 1,130 1,039,600 1,039,600 127,690 127,690 2,334,580 379,698 2,714,278<br />
13 Gopalganj 345,846 6,930 693 637,560 637,560 78,309 78,309 1,431,738 231,698 1,663,436<br />
14 Jamui 215,571 4,320 432 397,440 397,440 48,816 48,816 892,512 214,698 1,107,210<br />
15 Jehanabad 124,264 2,500 250 230,000 230,000 28,250 28,250 516,500 142,698 659,198<br />
16 Kaimur 199,007 4,000 400 368,000 368,000 45,200 45,200 826,400 209,698 1,036,098<br />
17 Katihar 417,984 8,380 838 770,960 770,960 94,694 94,694 1,731,308 239,698 1,971,006<br />
18 Khagaria 274,709 5,520 552 507,840 507,840 62,376 62,376 1,140,432 211,698 1,352,130<br />
19 Kishanganj 217,089 4,360 436 401,120 401,120 49,268 49,268 900,776 219,698 1,120,474<br />
20 Lakhisarai 134,852 2,700 270 248,400 248,400 30,510 30,510 557,820 141,698 699,518<br />
21 Madhepura 255,280 5,320 532 489,440 489,440 60,116 60,116 1,099,112 214,698 1,313,810<br />
22 Madhubani 563,734 11,300 1,130 1,039,600 1,039,600 127,690 127,690 2,334,580 374,698 2,709,278<br />
23 Munger 187,522 3,750 375 345,000 345,000 42,375 42,375 774,750 211,698 986,448<br />
385
24 Muzaffarpur 573,302 11,500 1,150 1,058,000 1,058,000 129,950 129,950 2,375,900 296,698 2,672,598<br />
25 Nawada 288,581 5,800 580 533,600 533,600 65,540 65,540 1,198,280 231,698 1,429,978<br />
26 Nalanda 330,598 6,620 662 609,040 609,040 74,806 74,806 1,367,692 256,698 1,624,390<br />
27 Patna 679,619 13,600 1,360 1,251,200 1,251,200 153,680 153,680 2,809,760 376,698 3,186,458<br />
28 Purnea 456,118 9,140 914 840,880 840,880 103,282 103,282 1,888,324 244,698 2,133,022<br />
29 Rohtas 394,415 7,900 790 726,800 726,800 89,270 89,270 1,632,140 269,698 1,901,838<br />
30 Saharsa 226,070 4,540 454 417,680 417,680 51,302 51,302 937,964 214,698 1,152,662<br />
31 Samastipur 462,681 9,270 927 852,840 852,840 104,751 104,751 1,915,182 296,698 2,211,880<br />
32 Saran 467,382 9,350 935 860,200 860,200 105,655 105,655 1,931,710 304,698 2,236,408<br />
33 Sheikhpura 85,238 1,710 171 157,320 157,320 19,323 19,323 353,286 144,698 497,984<br />
34 Sheohar 35,956 1,720 172 158,240 158,240 19,436 19,436 355,352 164,698 520,050<br />
35 Sitamarhi 400,483 8,020 802 737,840 737,840 90,626 90,626 1,656,932 279,698 1,936,630<br />
36 Siwan 398,768 8,000 800 736,000 736,000 90,400 90,400 1,652,800 269,698 1,922,498<br />
37 Supaul 288,596 5,790 579 532,680 532,680 65,427 65,427 1,196,214 234,698 1,430,912<br />
38 Vaishali 415,794 8,320 832 765,440 765,440 94,016 94,016 1,718,912 244,698 1,963,610<br />
39 W.Champaran 488,581 9,250 925 851,000 851,000 104,525 104,525 1,911,050 371,698 2,282,748<br />
Total 13,051,843 262,410 26,239 24,141,720 24,141,720 2,965,007 2,965,007 54,213,454 11,069,524 65,282,978<br />
386
PART- E<br />
Intersectoral Convergence<br />
2009-2010<br />
388
Situational Analysis:<br />
Public health peripheral and extension services and its linkage with facility based services<br />
started less than a century in the country. The said services have developed many folds during<br />
the last sixty years initially on the recommendation of the Bhor Committee and subsequently on<br />
the basis of reviews and recommendations of several expert committees. It has achieved<br />
commendable results despite poor funding and lack of a uniform system of command. It is now<br />
increasingly understood larger fund allocation would increase the resources within the health<br />
administrative set up but to achieve the desired outcomes, sectors administering the<br />
determinants of health must work in tandem with common objectives. The NRHM rightly<br />
emphasized the need to develop a convergent system between the Department of Health and<br />
other sectors governing the areas of several health determinants. The NHRM also recognizes<br />
the need to develop ownership of partners / stakeholders in tackling local endemic issues to<br />
ensure better quality of life in all sections of the population. Considering the diversity and<br />
prevailing inequity amongst the people it is rightly considered that leadership must be provided<br />
at every level of governance to solve the health problems amongst the poor and the excluded.<br />
Governance at every level can only be provided by the Rural Local Self Governance and in the<br />
<strong>State</strong> of Bihar it is the three tiers Panchayat Raj Institution. The other sectors which directly<br />
administer the issues of health determinants are;<br />
· Department Social Welfare administers ICDS<br />
· Department of Education administers school and higher education,<br />
· Public Health Engineering Department and Panchayat administer supply of drinking<br />
water and environmental sanitation including solid waste management.<br />
NRHM also seeks partnership from Indian System of Medicine like Aurveda, Unani, Yoga, Sidda<br />
and Homeopathy now jointly named AUYSH. The NRHM also seeks involvement of Non<br />
Government Organizations (NGO) and For Profit Private Sector as partners in the public health<br />
services by developing local need specific Public Private Partnership schemes. It also visualizes<br />
the need to involve expert consultants and agencies in strengthening the Department of Health<br />
and development of a <strong>State</strong> Heath Resource Centre to provide Technical Support in carrying<br />
forward the Management of Change for efficient utilization of resources and effective delivery of<br />
health services.<br />
(a) Coordination with Panchayat /Village Council.<br />
The state is undergoing through the process in the decentralisation of Panchayati Raj System.<br />
Thus to strengthen and monitor the performance of the PHSC and PHC, this institution has<br />
been brought under the manifold of the Panchayat president and Zilla Panchayat members of<br />
the respective areas. Further the Panchayat presidents or the members are ex officio chairman<br />
of the Village Health Water and Sanitation committee, to have a direct involvement in the health<br />
issues of the community. Joint bank account of Panchayat president and ANM has been<br />
389
opened for PHSC untied fund. These processes paved the way for taking initiative in<br />
implementation in various health programmes under NRHM<br />
Department has good relationship with the Village Council and through coordination with the<br />
Village Council most of the health programmes are being implemented at the community level<br />
with satisfaction.<br />
(b) Coordination with ICDS<br />
The DPO is a member of the District Health Society & District Core Group (under NRHM) and<br />
thus the health department has been able to utilize his/her services for community mobilization<br />
at the grassroots level. Through coordinated effort of the ANM and the Anganwadi worker<br />
mothers and children are being mobilized for antenatal check up, institutional deliveries and<br />
immunisation. Now the coordination is to be extended to organize VHNDs (Village Health<br />
nutrition Days) at every AWC all over the district every month.<br />
Issues / Areas<br />
Support in School Health<br />
Programme<br />
Support in immunisation<br />
programme for provision<br />
of TT booster at the age<br />
of 10 years.<br />
Support in the adolescent<br />
health programme<br />
Areas of Convergent Action<br />
Due to shortage of manpower in the health department,<br />
plans to examine school children should be prepared<br />
jointly with the education department so that larger<br />
schools are covered first or priority should be set for<br />
village schools which have not been covered recently or<br />
threats/incidences of diseases/malnutrition are more.<br />
During the school health programme visits, the booster<br />
Tetanus Toxoid needs to be given to 10 year olds in the<br />
schools. This should be worked out with the Education<br />
department and visits planned accordingly.<br />
Problem villages to be identified in which ASRH services<br />
can be provided on priority basis.<br />
390
(c) Coordination with PRI<br />
Issues / Areas<br />
Drainage system in<br />
villages<br />
Garbage disposal in<br />
villages<br />
Emergency transportation<br />
services<br />
Convergent actions<br />
List of villages with major drainage problems to be shared<br />
by the Health and ICDS department with the Rural<br />
Development department for annual prioritization of<br />
resources<br />
The system of disposal of garbage (solid waste) needs to<br />
be set up and larger villages prioritized as per list<br />
submitted by ANMs and AWWs. The operational aspects<br />
need to be managed by the VHWSC as per guidelines.<br />
Standard Operation Procedure (SOPs) and operation of<br />
emergency transportation services in villages with<br />
support from the block are in process.<br />
(d) Coordination with AYUSH<br />
There are few practitioners of ISM that are in government employment. The service rules<br />
related to them are not well defined. However, practitioners of traditional systems are there.<br />
Before a strategy can be worked out as to how to mainstream or integrate this, a study need to<br />
be carried out to identify the points of common interest such as rational management of<br />
common diseases, communicable diseases control Programme and disease surveillance<br />
Outcome /Output:<br />
Effective coordination exists between health dept. and other line<br />
departments<br />
Objectively Verifiable Indicators (OVI):<br />
Increased participation of all the line departments with the health<br />
department<br />
1.1 – Strategy :<br />
· Constitute <strong>State</strong> level inter department standing committee to initiate policy review for<br />
convergence and develop implementation procedures<br />
· Constitute District level inter department committee under the Chairmanship of DM<br />
and involvement of the District Level PRI to ensure PHC level committees are<br />
constituted and implementing the directives of the <strong>State</strong> Level Standing Committee<br />
· SHRC and TSU can facilitate by providing Technical Assistance and Support<br />
Activities:<br />
1.1.1 Develop convergence platform at all levels with NRHM line<br />
departments by constituting the committees<br />
MoV<br />
Committees<br />
constituted<br />
391
1.1.2 Develop policy framework and procedural guidelines / manual<br />
Guidelines /<br />
manual<br />
1.1.3 Develop linkage with other departments like WCD, Urban & Rural<br />
Development, Education, Panchayat, Youth Affairs, etc at all Minutes of the<br />
levels by ensuring the committees are functioning as per meeting<br />
guidelines<br />
1.1.4 Involve civil society, partners, NGOs in district health society Membership list<br />
1.1.5 Establish convergent committee in all PHCs chaired by BDO<br />
Committees<br />
constituted<br />
1.1.6 PRI s to actively involve in health development activities Membership list<br />
Joint plans and<br />
1.1.7 Joint Action with the line departments at different levels<br />
monitoring and<br />
review documents<br />
1.1.8 Formation and effective functioning of Rogi Kalyan Samiti (RKS)<br />
at PHC level which will also function as convergence committee<br />
RKS constituted<br />
1.1.9 Joint Planning, monitoring, evaluation by ANM, AWW ASHA<br />
FNGO/NGO, VHWSC and PRI representatives in VHWSC<br />
meeting.<br />
1.1.10 Regular information sharing among converging departments and<br />
joint review of progress.<br />
1.1.11 Key officials of NRHM related departments at <strong>State</strong> level to be<br />
actively involved in monitoring at all levels<br />
1.1.12 Preparation of joint monitoring plan in consultation with all line<br />
departments<br />
1.1.13 Review and monitoring of activities jointly.<br />
Joint plan<br />
documents<br />
Minutes of meeting<br />
Joint monitoring<br />
and review<br />
documents<br />
Joint monitoring<br />
plan document<br />
Joint monitoring<br />
and review<br />
documents<br />
392
Programme wise convergence<br />
Strategies/Activities<br />
1. Maternal Health<br />
1.1 Organize VHNDs at each and every AWC once a month to deliver ANC<br />
services.<br />
1.1 Organize once in two months RCH camps in all PHC and District Hospital<br />
areas within the district.<br />
1.2 Involvement of community representative of Gram Sabha through<br />
VHWSCs & MSS for identifying & referring complicated cases to facilities<br />
1.3 Involvement of AWWs and PRIs to identify and track each pregnant<br />
woman and motivate them to avail ANC services. Regular updation of EC<br />
register and quarterly population survey of her coverage area.<br />
1.4 Collection of blood and urines samples of pregnant women and send it to<br />
PHC for examination and report back with in 24 hours<br />
1.5 ASHA, AWW and ANM to be involved in observed consumption of IFA<br />
tablets by moderately and severely anemic pregnant mothers through<br />
regular home visits and follow ups.<br />
1.6 Observed consumption of Iron Follifer Tabs by Girls students in schools<br />
MoV<br />
Consolidated report<br />
of the PHC &<br />
district hospital<br />
Consolidated report<br />
of PHC & district<br />
Supervision and<br />
monitoring reports<br />
Supervision and<br />
monitoring reports<br />
VHND Report<br />
Monitoring and<br />
supervision report<br />
of LHV/<br />
MO/DRCHO/PRI<br />
School Health<br />
Programme report<br />
1.7 De-worming of all pregnant and adolescents girls (Half Yearly) Programme report<br />
2. Child Health<br />
2.1 Organize VHNDs at each and every AWC once a month to deliver<br />
child health and nutrition services.<br />
2.2 Organize RCH camps once in two months in all PHCs<br />
2.3 Involvement of community representative of Gram Sabha through<br />
VHWSCs & MSS for identifying & referring malnourished cases to<br />
facilities<br />
2.4 Supervision & Monitoring on all VHNDs by PRI representatives<br />
2.5 Regular organization of VHNDs at every AWCs in co-ordination of<br />
ANMs, ASHAs and PRIs<br />
Consolidated report<br />
of the PHC &<br />
district hospital<br />
Consolidated report<br />
of PHC & district<br />
Supervision and<br />
monitoring reports<br />
Supervision and<br />
monitoring reports<br />
Programme report<br />
2.6 Estimation and registration of children under the age group of 0-5 yrs List of children<br />
2.7 Growth monitoring of each child during VHNDs, at PHSC & in other Supervision and<br />
393
facilities monitoring reports<br />
3. Family Planning<br />
of PRIs/Department<br />
3.1 Ensure distribution of OCPs, emergency pills, condoms and IUD<br />
insertion to eligible couple through ASHAs , AWCs and ANMs<br />
4. Adolescents Health<br />
4.1 To provide weekly dose of observed IFA and bi-annual dose of<br />
deworming to adolescents girls in school by teachers<br />
4.2 To provide weekly dose of observed IFA and bi-annual dose of<br />
deworming to adolescents girls in school by AWWs and ASHAs<br />
4.3 Training of school teachers, AWWs, ASHAs and female PRI<br />
representatives on following issues:<br />
· Hygiene and menstrual hygiene and genital cleanliness<br />
· Adolescents growth and development<br />
· Communicating with adolescents<br />
· Sexual and reproductive health concerns of boys and girls<br />
· Nutrition and anemia in adolescents<br />
· Contraception for adolescents<br />
· RTIs/STIs and HIV/AIDS in adolescents<br />
· Child bearing<br />
· Birth preparedness and parenting<br />
· Safe abortion<br />
4.4 Awareness development amongst adolescents girls by school teachers,<br />
AWWs, ASHAs and female PRI representatives on all issues mentioned<br />
above by community<br />
5. Immunization<br />
ASHA , AWW and ANM to conduct Home Visits to trace out the Unimmunized<br />
children and Drop outs<br />
Provision of Immunization during regular VHNDs organized at every<br />
AWCs<br />
Stock Register<br />
List of girls<br />
provided IFA %<br />
deworming<br />
List of girls<br />
provided IFA %<br />
deworming<br />
Report of training<br />
Report<br />
of<br />
counseling session<br />
List of children<br />
Performance report<br />
6. National Disease Control Programme<br />
IDSP<br />
Symptomatic identification of diseases covered under IDSP and refer to<br />
nearest health facility<br />
Report of cases<br />
394
Treatment all referral cases<br />
Performance report<br />
RNTCP<br />
Symptomatic detection of cases by ANMs, AWWs, ASHAs, PRIs and refer<br />
to nearest DOTS centre<br />
Awareness development at community level regarding signs and<br />
symptoms of reportable cases for early detection, isolation and seeking<br />
treatment through mass media,, IPS, & counseling<br />
Developing and dissemination of IEC material, including leaflets and<br />
posters to the community<br />
IPC through convergent approach<br />
report of cases<br />
Report of BCC<br />
activities<br />
Display and<br />
availability of BCC<br />
material<br />
Report of key<br />
functionaries<br />
Blindness<br />
Create awareness at the community level through effective mass media<br />
for screening camps to be organized by BCC activities<br />
Awareness development at community level regarding signs and<br />
symptoms of reportable diseases for early detection and seeking treatment.<br />
Developing and dissemination of IEC material, including leaflets and<br />
posters<br />
IPC through convergent approach<br />
Report of BCC<br />
activities<br />
Report of BCC<br />
activities<br />
Leaflets and<br />
posters in place<br />
Report of key<br />
functionaries<br />
Leprosy<br />
Involving ASHA, AWWs and PRIs to ensure accessible and uninterrupted<br />
MDT services available to all patients through flexible and patient friendly drug<br />
delivery system<br />
Clinic during<br />
conventional timing<br />
6.5 National Vector Borne Disease Control Programme<br />
6.5.1 Convergence with Panchayat/PHED for environmental sanitation and<br />
safe drinking water supply by detecting location with problems<br />
List of sites<br />
6.6 Water borne diseases<br />
6.6.1 Drainage system in villages<br />
List of villages with major drainage problems to be shared by the<br />
Health and ICDS department with the Rural Development department<br />
for annual prioritization of resources<br />
6.6.2 Garbage disposal in villages<br />
The system of disposal of garbage (solid waste) needs to be set up<br />
and larger villages prioritized as per list submitted by ANMs and<br />
AWWs. The operational aspects need to be managed by the VHWSC<br />
as per guidelines.<br />
List of villages<br />
List of villages and<br />
locations<br />
395
Work Plan<br />
Goal:<br />
Effective coordination exists between health dept. and other line departments<br />
Timeline<br />
2009-10 200 2011-<br />
Strategy / Activity<br />
10- 12<br />
Q1 Q2 Q3 Q4<br />
11<br />
Responsibilit<br />
y<br />
<strong>State</strong>/District<br />
Inter-sectoral Coordination<br />
Strategy: Refer to LFA above<br />
Activities:<br />
1.1.1 Develop convergence platform at all<br />
<strong>State</strong><br />
levels with NRHM line departments by<br />
constituting the committees<br />
1.1.2 Develop policy framework and procedural<br />
<strong>State</strong><br />
guidelines / manual<br />
1.1.3 Develop linkage with other departments<br />
like WCD, Urban & Rural Development,<br />
<strong>State</strong>/Distri<br />
ct<br />
Education, Panchayat, Youth Affairs, etc<br />
at all levels by ensuring the committees<br />
are functioning as per guidelines<br />
1.1.4 Involve civil society, partners, NGOs in<br />
District<br />
district health society<br />
1.1.5 Establish convergent committee in all<br />
District<br />
PHCs chaired by BDO<br />
1.1.6 PRIs to actively involve in health<br />
District<br />
development activities<br />
1.1.7 Joint Action with the line departments at<br />
different levels<br />
<strong>State</strong>/Distri<br />
ct<br />
1.1.8 Effective functioning of Rogi Kalyan Samiti<br />
District<br />
(RKS) at PHC level which will be also<br />
function as convergence committee<br />
1.1.9 Joint Planning, monitoring, evaluation by<br />
District<br />
ANM, AWW ASHA FNGO/NGO, VHWSC<br />
and PRI representatives in VHWSC<br />
meeting.<br />
1.1.10 Regular information sharing among<br />
<strong>State</strong>/Distri<br />
converging departments and joint review<br />
ct<br />
of progress.<br />
1.1.11 Key officials of NRHM related <strong>State</strong><br />
396
Strategy / Activity<br />
Timeline<br />
2009-10 200<br />
10-<br />
Q1 Q2 Q3 Q4<br />
11<br />
2011-<br />
12<br />
Responsibilit<br />
y<br />
<strong>State</strong>/District<br />
departments at <strong>State</strong> level to be actively<br />
involved in monitoring at all levels<br />
1.1.12 Preparation of joint monitoring plan in<br />
consultation with all line departments<br />
<strong>State</strong>/Distri<br />
ct<br />
1.1.13 Review and monitoring of activities jointly.<br />
<strong>State</strong>/Distri<br />
ct<br />
397
Budget:<br />
Activity Unit Rate Amount<br />
Joint Meeting at the 2 100000 2,00,000<br />
state level with<br />
various Deptt. like PR,<br />
ICDS etc<br />
Joint meeting at the 38 25000 9,50,000<br />
district level<br />
Joint monitoring from 6 20000 x 6 visits 120000<br />
state to districts to<br />
block/phc<br />
Joint meeting at the 60000 AWC Rs 100 pm X 12 7,20,00,000<br />
village level- Mahila<br />
mandal meetings<br />
months<br />
Incentive to AWW for 60000X200X12<br />
14,40,00,000<br />
social mobilization in<br />
Muskan Abhiyan<br />
months<br />
Total 21,72,70,000<br />
398
NRHM PART A : RCH II<br />
Sl. No. Budget Head Rs. lakhs %<br />
1 Maternal Health<br />
1.1 Operationalise facilities (dissemination,<br />
monitoring & quality) (details of infrastructure<br />
& human resources, training, IEC / BCC,<br />
equipment, Drug and supplies in relevant<br />
sections)<br />
14.50<br />
1.1.2 Operationalise Blood Storage units in FRU 469.68<br />
1.2 Referral Transport 0.00<br />
1.3 Integrated outreach RCH services 10.00<br />
1.4 Janani Evam Bal Suraksha Yojana/JBSY 22686.72<br />
Sub total 23180.90 47.80<br />
2 Child Health 4291.09 8.85<br />
3 Family Planning 7432.02 15.33<br />
4 Adolescent Reproductive and Sexual Health 49.05 0.10<br />
5 Urban RCH 134.33 0.28<br />
6 Vulnerable Groups 330.00 0.68<br />
7 Tribal Health 0.00 0.00<br />
8 Innovations 2077.30 4.28<br />
9 Strengthening of SIHFW 0.00 0.00<br />
10 Infrastructure and Human Resource 3783.76 7.80<br />
11 Institutional Strengthening 602.50 1.24<br />
12 Training 1122.32 2.31<br />
13 BCC/IEC (for NRHM Part A, B & C) 1140.89 2.35<br />
14 Procurement of Equipments/Instruments 3385.58 6.98<br />
15 Procurement of Drugs and Supplies 0.00 0.00<br />
16 Programme management 965.25 1.99<br />
TOTAL 48495.00 100.00<br />
399
PART- B<br />
Sl. No. Budget Head Modified Budget %<br />
1 2 6<br />
1 Decentralization<br />
1.11 ASHA Support System at <strong>State</strong> Level 27694500<br />
1.12 ASHA Support System at District Level 2160000<br />
1.13 ASHA Support System at Block Level 59950000<br />
1.14 ASHA Support System at Village Level 4500000<br />
1.15 ASHA Trainings 82421250<br />
1.16 ASHA Drug Kit & Replenishment 22555800<br />
1.17 Emergency Services of ASHA 2500000<br />
1.18 Motivation of ASHA 63172875<br />
1.19 Capacity Building/Academic Support programme 1000000<br />
1.2 ASHA Divas 81230200<br />
Total ASHA 347184625 7.97<br />
1.21 Untied Fund for Health Sub Center, Additional<br />
Primary Health Center and Primary Health Center<br />
134807000<br />
1.22 Village Health and Sanitation Committee 401332500<br />
1.23 Rogi Kalyan Samiti 85300000<br />
Total Decentralization 621439500 14.26<br />
2 Infrastructure Strengthening<br />
2.1 Construction of HSCs (100 no. x Rs.9.50 lakhs) 95000000<br />
2.2 Construction of PHCs 637967000<br />
2.2a Construction of residential quarters of 200 old<br />
APHCs for staff nurses<br />
2.2b Construction of building of 51 APHCs where land is<br />
available<br />
2.3 Up gradation of CHCs as per IPHS standards (100<br />
CHCs x Rs.40.00 lakhs)<br />
2.4 Infrastructure and service improvement as per IPHS<br />
in 20 (DH & SDH) hospitals for accreditation or ISO :<br />
9000 certification<br />
600000000<br />
37967000<br />
400000000<br />
100000000<br />
2.5 Upgradation of ANM Training Schools 70000000<br />
2.6 Annual Maintenance Grant 82080000<br />
Total Infrastructure strengthening 1385047000 31.79<br />
3 Contractual Manpower<br />
3.1 Contractual Salaries, Incentives and Bonus (PHC<br />
doctors and staffs, contractual staff nurses, ANM ®,<br />
mobile services)<br />
668400000<br />
3.1a Incentive for PHC doctors & staffs @ Rs. 50,000 for<br />
better performance in implementing programmes<br />
(Rs. 50,000/ - per PHC per year)<br />
12500000<br />
400
3.1b Salaries for contractual Staff Nurses (2900 existing<br />
and 910 new) (Rs.7500 per month)<br />
3.1c Contract Salaries for ANMsRs.6000 per month x<br />
3500 (12 Months Consolidated Salaries for<br />
Contractual ANMs)<br />
3.1d Mobile facility for all health functionaries (District<br />
officials, PHC in charge, CDPOs and ANMs @ 500<br />
per month)<br />
343900000<br />
252000000<br />
60000000<br />
3.2 Block Programme Management Unit 289524000<br />
3.3 Addl. Manpower for SHSB 6204288<br />
3.4 Addl. Manpower for NRHM 25479000<br />
Total Contractual Manpower 989607288 22.71<br />
4 PPP Initiatives<br />
4.1 102-Ambulance service 4032000<br />
4.2 1911- Doctor on Call & Samadhan 816000<br />
4.3 Addl. PHC management by NGOs 39864000<br />
4.4 American Association of Physicians of Indian Origin<br />
(AAPIO)<br />
5600000<br />
4.5 SHRC (HOSMAC) 13844000<br />
4.6 Services of Hospital Waste Treatment and Disposal<br />
in all Government Health facilities up to PHC in Bihar<br />
(IMEP)<br />
30000000<br />
4.7 Dialysis unit in various Government Hospitals of<br />
Bihar<br />
4.8 Setting Up of Ultra-Modern Diagnostic Centers in<br />
Regional Diagnostic Centers (RDCs) and all<br />
Government Medical College Hospitals of Bihar<br />
20000000<br />
36000000<br />
4.9 Providing Telemedicine Services in Government<br />
Health Facilities<br />
4. 10 Outsourcing of Pathology and Radiology Services<br />
from PHCs to DHs<br />
4.11 Operationalising MMU (38 units x Rs.4.68 lakhs x 9<br />
months)<br />
4.14 Monitoring and Evaluation (<strong>State</strong>, District, Block<br />
Data Centre)<br />
20000000<br />
3000000<br />
160056000<br />
63750000<br />
4.15 Generic Drug Shop<br />
4.16 Nutritional Rehabilitation Centre 4934400<br />
4.17 Hospital Maintenance<br />
4.18 Providing Ward Management Services in<br />
Government Hospitals<br />
3000000<br />
4.19 Provision for HR Consultancy services 2250000<br />
4.2 Advanced Life Saving Ambulance (Rs.9,98,000/- x 9<br />
8901000<br />
months)<br />
Total PPP Initiatives 416047400 9.55<br />
5 Procurement of Supplies<br />
401
5.1 Delivery kits at the HSC/ANM/ASHA (no.200000 x<br />
Rs.25/-)<br />
5.2 SBA Drug kits with SBA-ANMs/Nurses etc<br />
(no.25000 x Rs.245/-)<br />
5.3 Availability of Sanitary Napkins at Govt. Health<br />
Facilities @25000/district/year<br />
5000000<br />
6125000<br />
950000<br />
5.4 Procurement of beds for PHCs to DHs 40286000<br />
Total Procurement of Supplies 52361000 1.20<br />
6 Procurement of Drugs<br />
6.1 Cost of IFA for Pregnant & Lactating mothers<br />
(Details annexed)<br />
6.2 Cost of IFA for (1-5) years children (Details<br />
annexed)<br />
23944000<br />
40923000<br />
6.3 Cost of IFA for adolescent girls (Details annexed) 37541000<br />
Total Procurement of Drugs 102408000 2.35<br />
7 Mobilisation & Management support for Disaster<br />
Management<br />
10000000 0.23<br />
8 Health Management Information System 3289517 0.08<br />
9 Strengthening of Cold Chain (Infrastructure<br />
strengthening)<br />
Refurbishment of existing Warehouse for R.I. as well<br />
as provision for hiring external storage space for<br />
(during Immunization Campaigns) Logistics at <strong>State</strong><br />
HQ @Rs 1000000/-<br />
36131000 0.83<br />
1000000<br />
Refurbishment of existing Cold chain room for<br />
district stores in all districts with proper<br />
electrification,Earthing for electrical cold chain<br />
equipment and shelves and dry space for non<br />
elecrtical cold chain equipment and logistics @Rs 3<br />
Lakhs per district x 38 districts<br />
Earthing and wiring of existing Cold chain rooms in<br />
all PHCs @Rs 7000/- per PHC x 533 PHCs<br />
POL of Generators for cold chain @ Rs. 600 per day<br />
per WIC. Rs. 500 per day per district and Rs. 400<br />
per day per PHC<br />
11400000<br />
3731000<br />
20000000<br />
10 Preparation of Action Plan 1700000 0.04<br />
10.1 Preparation of District Health Action Plan (Rs.50<br />
thousand per district x 38)<br />
1600000<br />
10.2 Preparation of <strong>State</strong> Health Action Plan @ 1 lakhs 100000<br />
11 Mainstreaming Ayush under NRHM 391,584,800 8.99<br />
Total 4,356,800,130 100.00<br />
Rs. in Lakh 43568.00<br />
402
NRHM Part: C<br />
Sl Budget Head Total Budget<br />
(Rs. In lakhs)<br />
%<br />
1 Routine Immunization 3193.08 100.00<br />
Total 3193.08 100.00<br />
NRHM PART D – NATIONAL DISEASE CONTROL PROGRAMME<br />
Sl. No.<br />
Programme<br />
Budget 2009-10<br />
(Rs. In Lakhs)<br />
1 IDSP 130.06 1.82<br />
2 T.B. 2,414.73 33.85<br />
3 Leprosy 279.40 3.92<br />
4 Malaria 435.15 6.10<br />
5 Kalazar 2,268.92 31.81<br />
6 Dengu+Chikungunya 36.50 0.51<br />
7 Filaria 652.83 9.15<br />
8 Blindness 518.75 7.27<br />
9 IDD 18.00 0.25<br />
10 JE 379.50 5.32<br />
TOTAL 7,133.84 100.00<br />
%<br />
NRHM Part E : Intersectoral Convergence<br />
Sl. No.<br />
Programme<br />
Budget 2009-10<br />
(Rs. In Lakhs)<br />
%<br />
1 Intersectoral Convergence 2172.70 100<br />
403
SUMMARY of BUDGET<br />
PART<br />
HEAD<br />
BUDGET 2009-10<br />
(Rs. In lakhs)<br />
In Cr. %<br />
A RCH II 48495.00 484.95 37.89<br />
B NRHM Additionalities 43568.00 435.68 34.04<br />
C Immunization 3193.08 31.93 2.49<br />
D NDCP 7,133.84 71.34 5.57<br />
E Intersectoral Convergence 2172.70 21.72 1.70<br />
TOTAL 104562.62 1045.62 81.70<br />
PPI Operational Cost 76.97 6.01<br />
Infrastructure Maintenance<br />
(Treasury Fund) 157.22 12.28<br />
GRANT TOTAL 1279.81 100.00<br />
404