Monograph - College of Public Health - University of Georgia
Monograph - College of Public Health - University of Georgia
Monograph - College of Public Health - University of Georgia

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
1<br />
Careers in Aging<br />
The 23 rd Annual Southeastern Student<br />
Mentoring Conference in Gerontology and<br />
Geriatrics<br />
Keynote Addresses and Poster Abstracts<br />
Edited by Christina Barmon
2<br />
Careers in Aging<br />
The 23 rd Annual Southeastern Student<br />
Mentoring Conference in Gerontology and<br />
Geriatrics<br />
Keynote Addresses and Poster Abstracts<br />
Edited by Christina Barmon
3<br />
Copyright © 2013 by The <strong>University</strong> <strong>of</strong> <strong>Georgia</strong> Institute <strong>of</strong> Gerontology in the <strong>College</strong> <strong>of</strong><br />
<strong>Public</strong> <strong>Health</strong>. All rights reserved. No portion <strong>of</strong> this report, or the data that it contains, may be<br />
reproduced without the express written consent <strong>of</strong> the authors.<br />
Copies <strong>of</strong> this report may be obtained from The <strong>University</strong> <strong>of</strong> <strong>Georgia</strong> Institute <strong>of</strong> Gerontology,<br />
255 E. Hancock Ave., Athens, GA 30602. Our website is http://www.publichealth.uga.edu/geron.<br />
About the Cover: A conversation in the <strong>of</strong>fice. Stock photo credited to <strong>Georgia</strong> State <strong>University</strong>.<br />
Technical Report Number UGAIG-13-02.
iii<br />
Table <strong>of</strong> Contents<br />
Preface<br />
Elisabeth O. Burgess, Ph.D ………………………………………………………. iv<br />
Foreword<br />
Christina Barmon, MPH ………………………………………………………….. vi<br />
Co-sponsors ………………………………………………………………………………. viii<br />
Student Keynote Address I ……………………………………………………………… 1<br />
Identity and Career Development in Gerontology: A Student’s Perspective<br />
Brian Downer<br />
Student Keynote Address II ……………………………………………………………... 14<br />
Predictors <strong>of</strong> Electronic <strong>Health</strong> Record Use in Residential Care Facilities<br />
Amanda A. Holup<br />
The Anne & Everett Lee Scholarship Awards …………………………………………. 19<br />
Poster Presentation Abstracts …………………………………………………………… 21<br />
2012 Pictures ………………………………………………………………………………69
iv<br />
Preface<br />
The 23rd Annual Southeastern Mentoring Conference in<br />
Gerontology and Geriatrics met in Atlanta, <strong>Georgia</strong> on March 30-<br />
31. The Gerontology Institute at <strong>Georgia</strong> State <strong>University</strong> was<br />
proud to host this conference and welcome students and<br />
colleagues from across the southeast to Atlanta.<br />
This year’s conference theme, “Careers in Aging,”<br />
attracted one <strong>of</strong> the largest most diverse groups <strong>of</strong> student posters<br />
yet. The fields <strong>of</strong> gerontology and geriatrics are continuing to<br />
grow and students in our region are well poised to succeed in<br />
every discipline. A successful career requires numerous mentors<br />
and this year we highlighted the role <strong>of</strong> mentoring in career<br />
development. Dr. Peggye Dillworth-Anderson gave an insightful<br />
faculty keynote address on “Building a Career in Aging: The<br />
Importance <strong>of</strong> Mentoring & Collaboration.” In addition on<br />
Saturday lunch roundtables led by faculty provided students with the opportunity to explore<br />
issues <strong>of</strong> careers and career development from advocacy to research to job searches. In addition,<br />
award-winning veterans <strong>of</strong> the mentoring conference, Brian Downer and Amanda A. Holup,<br />
shared their wisdom with a new generation <strong>of</strong> students through the student keynote lectures.<br />
Both <strong>of</strong> these excellent papers are included in this monograph.<br />
This conference is unlike any other conference in gerontology and geriatrics. Students<br />
have the opportunity to present their work at a pr<strong>of</strong>essional conference where they can refine<br />
their presentations skills and learn from the expertise <strong>of</strong> an interdisciplinary team <strong>of</strong> faculty<br />
mentors. All conference sessions take place in one space, allowing students the opportunity to<br />
learn from each other and from the insightful commentary <strong>of</strong> faculty mentors. This experience is<br />
unique because the faculty members participating at this conference are committed to nurturing<br />
emerging scholars and engaging in dialogue about the aging research. Moreover, the best posters<br />
and presentations receive monetary awards. As always, this conference is made possible by the<br />
financial contributions <strong>of</strong> the sponsoring universities. The vision and dedication <strong>of</strong> the<br />
sponsoring faculty mentors and their institutional administrators make these annual conferences<br />
possible. The conference sponsors are: Armstrong Atlantic State <strong>University</strong>, Mercer <strong>University</strong>,<br />
<strong>Georgia</strong> State <strong>University</strong>, <strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, <strong>University</strong> <strong>of</strong> Alabama, <strong>University</strong> <strong>of</strong> Kentucky,<br />
and <strong>University</strong> <strong>of</strong> South Florida.<br />
Over the years, this conference has developed its own rituals and norms which reinforce<br />
the good nature <strong>of</strong> those involved and the belief that the best mentoring can also occur in<br />
informal settings and non-traditional ways. Whether it is tossing out school logo items as part <strong>of</strong><br />
drawings, leading stretching activities between sessions, or participating in friendly rivalries<br />
between sponsoring universities, mentoring conference faculty and veteran students keep things<br />
going with enthusiasm and a passion for this event. This year, undergraduate students<br />
contemplating graduate school, a doctoral student with years <strong>of</strong> experience, and numerous others<br />
received constructive feedback to assist them in reaching goals and polishing skills. I know that<br />
everyone found this to be an enriching experience. Furthermore, I want to extend a special thank<br />
you to the staff: GSU Gerontology staff, Quanda Miller and Christina Cummings, who managed<br />
local arrangements and UGA Gerontology faculty and staff, including Dr. Anne Glass, Dr.
v<br />
Kerstin Emerson, Anita Holmes and Jayne Clamp, who do amazing things to keep this<br />
conference going year after year. Finally, we were excited to welcome Dr. Toni P. Miles, the<br />
new Director <strong>of</strong> the Institute <strong>of</strong> Gerontology at the <strong>University</strong> <strong>of</strong> <strong>Georgia</strong> for her first Mentoring<br />
Conference. Dr. Miles brings new energy and leadership to this collaborative endeavor and we<br />
look forward to working with her in the coming years. Finally, I congratulate Christina Barmon<br />
for her outstanding leadership as editor <strong>of</strong> this volume. I know that she worked hard to produce a<br />
super monograph which accurately reflects the spirit <strong>of</strong> this conference.<br />
Elisabeth O. Burgess, Ph.D.<br />
Director, Gerontology Institute<br />
<strong>Georgia</strong> State <strong>University</strong>
vi<br />
Foreword<br />
The annual Southeastern Student Mentoring Conference in Gerontology and Geriatrics is<br />
a unique event in which students and faculty from nine participating schools come together to<br />
guide students in research and presenting. There is no other environment in which students have<br />
the opportunity to present in front <strong>of</strong> a large audience (scary!) that is truly supportive. We<br />
students, not only get a chance to present, many for the first time, but to get to know and learn<br />
from faculty and peers at neighboring schools that we might not have other opportunities to meet.<br />
This year the 23 rd annual conference was held in Atlanta and hosted by the Gerontology Institute<br />
at <strong>Georgia</strong> State <strong>University</strong>.<br />
Over the two days <strong>of</strong> the conference, 48 students presented their work both as posters and<br />
oral presentations. The resulting conference was the largest and most diverse event to date. This<br />
diversity was evident in the topics and disciplines <strong>of</strong> student papers which ranged from<br />
preventing age-related impairment and providing services and health care to older adults to<br />
improving quality <strong>of</strong> life for older adults in long-term care. Medical, doctoral, and masters-level<br />
students were joined by high achieving undergraduates who all presented exceptional papers.<br />
The result was vibrant discussions after each presentation and during the poster-viewing sessions.<br />
There were many changes to the conference this year. We welcomed Dr. Toni Miles as<br />
the new director <strong>of</strong> the Institute <strong>of</strong> Gerontology at <strong>University</strong> <strong>of</strong> <strong>Georgia</strong>. Dr. Miles brought<br />
enthusiasm and energy to this event and we look forward to her leadership for the student<br />
mentoring conference. Also new this year, in keeping with the purpose and the theme <strong>of</strong> the<br />
conference, were the “Careers in Aging” roundtables. For lunch on Saturday, we gathered at<br />
roundtables to participate in discussions led by experts in the topic. We chose from a wide<br />
variety <strong>of</strong> topics centered on careers in aging, including advocacy, academia, government,<br />
internships and volunteering, policy and legislation, the job search, and research. The<br />
roundtables were tailored to students at every stage from the undergraduate and graduate student<br />
looking for advice on internships to the advanced doctoral candidate preparing for the job market.<br />
At each roundtable, mentors and students participated in spirited discussions, which reinforced<br />
the collegial spirit <strong>of</strong> the conference.<br />
Each year, the conference welcomes veteran students to share research and experiences<br />
with the others in a student keynote address. The first student keynote speaker this year, last<br />
year’s first prize award recipient, was Brian Downer, a doctoral student in Gerontology at the<br />
<strong>University</strong> <strong>of</strong> Kentucky. Brian studies the interaction between genetics and behavior on cognitive<br />
functioning in later life. He shared his research and mentoring advice for finding and developing<br />
one’s identity in graduate school. His excellent presentation and paper uniquely integrates his<br />
research interests in behavioral risk factors for Alzheimer’s disease and how he has grown and<br />
developed as a graduate student. His insights are valuable for students at all stages <strong>of</strong> their career.<br />
Peggye Dilworth-Anderson gave the faculty keynote address. Dr. Dilworth-Anderson, a<br />
pr<strong>of</strong>essor in health policy and management and the co-director <strong>of</strong> the Institute on Aging at the<br />
<strong>University</strong> <strong>of</strong> North Carolina at Chapel Hill, shared her insights on mentoring. Through her many<br />
years <strong>of</strong> mentorship, she has learned that it is most important to know your students, their<br />
backgrounds, and their talents, as well as their weaknesses to know how to best guide them. She<br />
also emphasized the importance <strong>of</strong> having multiple mentors.
vii<br />
The second student keynote was given by Amanda A. Holup, who was last year’s second<br />
place award winner. Amanda is currently a doctoral student in the Aging Studies program at the<br />
<strong>University</strong> <strong>of</strong> South Florida. She shared her timely research in the determinants <strong>of</strong> electronic<br />
health records will be very important for the health and well-being <strong>of</strong> older adults in long-term<br />
care.<br />
Each year, the best presentations and posters are eligible for awards. Representatives<br />
from each <strong>of</strong> the sponsoring universities evaluate the student presentations and posters and<br />
present awards to the best presentations and posters. This year’s first place award winner was<br />
Michael Schuier from Mercer <strong>University</strong> for his presentation titled “Mini Mental Status Exam<br />
(MMSE): Differences Due to Scoring for Older Adults with Memory Problems.” The second<br />
place award went to Elizabeth Couser from the <strong>University</strong> <strong>of</strong> Kentucky for her presentation titled<br />
“Alzheimer’s Disease and the Visual System: Shifting the Focus to the Future Research.” We<br />
look forward to their keynote speeches next year.<br />
Every year, the hosting school edits a monograph <strong>of</strong> the event. This year I had the<br />
opportunity to edit the monograph and participate in and guide the peer review process. This was<br />
an invaluable educational opportunity. It is most definitely a collaborative effort. I would like to<br />
thank <strong>Georgia</strong> State Gerontology students, Renu Kumar, Erin Fisher, and Meagan Jain, for their<br />
excellent work and many hours reviewing the keynote speaker’s papers. I would also like to<br />
thank my advisor, Dr. Elisabeth Burgess from <strong>Georgia</strong> State, and Anne Glass, and the staff at the<br />
Institute <strong>of</strong> Gerontology at the <strong>University</strong> <strong>of</strong> <strong>Georgia</strong> for their guidance and assistance in<br />
producing this monograph.<br />
Christina Barmon MPH<br />
Ph.D. Student<br />
Gerontology Institute<br />
Department <strong>of</strong> Sociology<br />
<strong>Georgia</strong> State <strong>University</strong>
viii<br />
Co-Sponsors<br />
Co-Sponsors <strong>of</strong> the Twenty-third Annual Southeastern Student Mentoring Conference<br />
in Gerontology and Geriatrics<br />
Armstrong Atlantic State <strong>University</strong><br />
<strong>College</strong> <strong>of</strong> <strong>Health</strong> Pr<strong>of</strong>essions<br />
<strong>Health</strong> Sciences Department<br />
Savannah, GA 31419<br />
(912) 921-5480<br />
<strong>University</strong> <strong>of</strong> Alabama<br />
School <strong>of</strong> Psychology<br />
Center for Mental <strong>Health</strong> & Aging<br />
Tuscaloosa, AL 35487<br />
(205) 348-7518<br />
<strong>Georgia</strong> State <strong>University</strong><br />
Gerontology Institute<br />
Atlanta, GA 30303<br />
(404) 651-2692<br />
<strong>University</strong> <strong>of</strong> Kentucky<br />
Graduate Center for Gerontology<br />
Lexington, KY 40536<br />
(859) 257-1450<br />
Mercer <strong>University</strong><br />
Macon, GA 31207<br />
(800) MERCER-U<br />
<strong>University</strong> <strong>of</strong> South Florida<br />
School <strong>of</strong> Aging Studies<br />
Tampa, FL 33620<br />
(813) 974-2414<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong><br />
Institute <strong>of</strong> gerontology<br />
<strong>College</strong> <strong>of</strong> <strong>Public</strong> <strong>Health</strong><br />
Athens, GA 30602<br />
(706) 425-3222
1<br />
Student Keynote Address I<br />
Brian Downer entered the Ph.D. program in<br />
Gerontology at the <strong>University</strong> <strong>of</strong> Kentucky in the fall <strong>of</strong> 2010<br />
after receiving his B.S. in psychology and biology from<br />
Aquinas <strong>College</strong> in Grand Rapids Michigan. His research<br />
interests involve secondary data analysis examining the<br />
relationship between genetic traits, changes in health conditions<br />
across the lifespan, and late life cognitive functioning.<br />
Brian has presented his research at national and<br />
international meetings including the Gerontological Society <strong>of</strong><br />
America annual meeting and the Alzheimer’s Association<br />
International Conference. He has also co-authored several peer-reviewed reports and a<br />
manuscript.<br />
Brian’s ultimate goal is to earn a career in academia performing research, teaching and<br />
mentoring students at a research intensive university. It is his mission to reach this goal in<br />
order to contribute to the health and wellbeing <strong>of</strong> older adults, as well as to the development<br />
<strong>of</strong> future scientific investigators.<br />
In addition to being a student, Brian enjoys doing all forms <strong>of</strong> exercise and<br />
recreational activities including (but not limited to) biking, swimming, running and golfing.
2<br />
Identity and Career Development in Gerontology: A Student’s Perspective<br />
Brian Downer<br />
<strong>University</strong> <strong>of</strong> Kentucky Graduate Center for Gerontology<br />
The theme <strong>of</strong> the 23 rd Annual Student Mentoring Conference in Gerontology and<br />
Geriatrics is careers in aging. Before any <strong>of</strong> us choose our career, we first need to develop our<br />
identity as gerontologists. This is important because there are many factors that influence how<br />
people age and experience aging. These factors include physiological changes, diseases, housing<br />
and nutrition needs, end <strong>of</strong> life decision-making, and many others. Gerontologists cannot be<br />
experts in all <strong>of</strong> these areas. Therefore, we need to develop an identity that will allow us to excel<br />
in a specific area. In this paper I will share how choosing a graduate school, determining an area<br />
<strong>of</strong> expertise, and understanding what makes gerontology different from other disciplines have all<br />
contributed to my identity as a gerontologist. I will also share with you one <strong>of</strong> my own studies to<br />
demonstrate how my identity as a gerontologist is reflected in my research. All <strong>of</strong> us are going to<br />
have a different journey, but I hope that you will be able to take something away from my<br />
experiences and apply it to your own identity and career development.<br />
Selecting a Graduate School<br />
Students who attend the Student Mentoring Conference are all in different stages <strong>of</strong> their<br />
academic or pr<strong>of</strong>essional careers. There are undergraduate students who are interested in<br />
graduate school, but may be unsure if they want to attend a program that has a research or<br />
applied focus. Others may be earning their master’s degree and need to determine if their career<br />
goals will require them to have a PhD. This includes master’s students who have an applied<br />
degree but are interested in research or those with a research focused degree but want a career in<br />
an applied setting. There are also doctoral students who are preparing themselves for a career<br />
after graduate school. There may also be students who have pr<strong>of</strong>essional experience but have<br />
returned to school to earn an advanced degree. The type <strong>of</strong> graduate schools we apply to will be<br />
determined by whether we want a career in an applied or academic setting. Applied careers can<br />
include medicine, administration, or government, whereas academic careers can include teaching<br />
and performing research at a college or university. When I was choosing a graduate school, I<br />
knew I wanted to pursue a career in academia and research. I chose the <strong>University</strong> <strong>of</strong> Kentucky<br />
because the doctoral program in gerontology had the three qualities that I was looking for in a<br />
graduate program: an emphasis on student training and development, faculty passionate about<br />
aging research, and a multidisciplinary and interdisciplinary approach to Alzheimer’s disease<br />
research. While these qualities were important to me, other qualities to consider may include the<br />
location <strong>of</strong> the graduate school or availability <strong>of</strong> student funding. When choosing a graduate<br />
school, postdoctoral position, or your first career, it is important to make your decision based on<br />
the qualities that are the most important to you. This will allow you to be confident that you are<br />
making the decision that will give you the greatest likelihood for success.<br />
Determining Your Area <strong>of</strong> Expertise<br />
Gerontology is both multidisciplinary, with defined subfields such as biology <strong>of</strong> aging<br />
and sociology <strong>of</strong> aging (Shenk et al., 2001), and interdisciplinary, through the integration <strong>of</strong>
3<br />
methods, techniques and theories from multiple disciplines (Ferraro, 2007). Because gerontology<br />
is such a broad field, it is important to determine an area <strong>of</strong> expertise that you can develop over<br />
the course <strong>of</strong> your career. This can be a difficult process, but I will share with you the steps that<br />
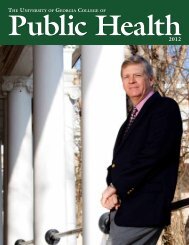
helped me determine my area <strong>of</strong> expertise. First, list the broad fields that can be included in<br />
gerontology (Figure 1a). The fields I have listed represent areas <strong>of</strong> research, but if you are not<br />
pursuing a career in research, then list careers that match your interests. Once you have created<br />
your list, the next step is to choose an area that you are interested in from that list. This will<br />
allow you to determine a field within gerontology that you want to pursue. Once you select a<br />
subfield within gerontology, the third step is to list the areas <strong>of</strong> study within that subfield and<br />
choose an area from this list. Continue with this selection process to determine your area <strong>of</strong><br />
expertise.<br />
I found this stepwise approach to be helpful in determining an area <strong>of</strong> research within<br />
gerontology that I wanted to specialize in. Prior to enrolling at the <strong>University</strong> <strong>of</strong> Kentucky, I<br />
knew I wanted to study disease prevention, specifically Alzheimer’s disease. Alzheimer’s<br />
disease prevention can be studied multiple ways, each with its own particular research settings,<br />
study designs, and objectives (Figure 1b). From these subfields, I selected research that would<br />
involve secondary analysis and association studies to examine factors that modify the risk for<br />
Alzheimer’s disease (Figure 1c). These risk factors can be environmental (e.g. mentally<br />
stimulating environment), behavioral (e.g. smoking, diet) or genetic (e.g. APOE, PSEN1). As I<br />
continued to read literature, I learned that health behaviors, environmental exposures, and<br />
genetic risk factors all contribute to Alzheimer’s disease and examining interactions between<br />
these exposures provides valuable insight into the etiology <strong>of</strong> the disease. Eventually, I narrowed<br />
my research interests to the study <strong>of</strong> gene-environment interactions in Alzheimer’s disease and<br />
Figure 1a Figure 1b Figure 1c<br />
cognitive decline.<br />
Determining an area <strong>of</strong> expertise takes time and patience and my particular research<br />
interests are a result <strong>of</strong> both personal and academic experiences. My interest in Alzheimer’s<br />
disease prevention is a result <strong>of</strong> growing up with all four <strong>of</strong> my grandparents in an<br />
intergenerational household. Three <strong>of</strong> my grandparents had passed away due to complications<br />
from Alzheimer’s disease by the time I had completed the first year <strong>of</strong> my undergraduate studies.<br />
Witnessing their cognitive decline and the effect it had on them and my family motivated me to
4<br />
learn about the psychological and biological changes that occur in the brain as the body ages. My<br />
academic experiences as a student, being involved in studies as a research assistant, and reading<br />
literature allowed me to refine my broad interest in Alzheimer’s disease prevention.<br />
Once you choose an area that you are interested in, it is important to allow for your<br />
interests within your area to evolve. This includes using methodologies, theories and technology<br />
from other areas <strong>of</strong> research that allow for advances in the field to be made. One way this can be<br />
accomplished is by keeping an open mind about the type <strong>of</strong> research that is being performed in<br />
other areas and being aware <strong>of</strong> what types <strong>of</strong> findings are being generated by other fields.<br />
What Makes Gerontology Different From Other Disciplines?<br />
Even though I worked hard to determine my own area <strong>of</strong> research within gerontology, I<br />
still struggled with my identity as a gerontologist. The biggest step forward in the development<br />
<strong>of</strong> my identity has come from understanding what makes gerontology different from other<br />
disciplines. For example, what separates me as a gerontologist studying gene-environment<br />
interactions from an epidemiologist or biostatistician? To answer this, let us examine the<br />
definition <strong>of</strong> gerontology. Gerontology is the study <strong>of</strong> aging, not just the study <strong>of</strong> the aged or <strong>of</strong><br />
older adults (Seccombe & Ishii-Kuntz, 1991). This distinction may seem trivial but it is<br />
important. Just because someone studies a disease, social problem, or other need that is prevalent<br />
among older adults, does not make that person a gerontologist; just as someone who uses<br />
statistics in their research does make them a statistician. I think it is important for gerontology<br />
students to remember that studying the process <strong>of</strong> aging does not need to be limited to only older<br />
adults because experiences from all stages <strong>of</strong> the life span are involved in the aging process.<br />
Adopting a life course approach to the study <strong>of</strong> older adults will allow for gerontologists to<br />
examine how the aging experience is influenced by biological and physiological changes, disease,<br />
public policies, end <strong>of</strong> life concerns, housing needs, and caregiving needs, just to name a few. As<br />
gerontologists, we are trained to incorporate the specific areas that make up the life course into<br />
our area <strong>of</strong> expertise.<br />
Relationship Between APOE-e4 Allele Status, Mean Alcohol Consumption Following<br />
Midlife and Cognitive Decline Among Older Adults<br />
I want to take this opportunity to share with you some <strong>of</strong> my own research. With the<br />
assistance <strong>of</strong> my coauthors Drs. David Fardo and Faika Zanjani, I am analyzing data from the<br />
Framingham Heart Study to examine the relationship between alcohol consumption and<br />
cognitive decline among older adults who have one or more APOE-e4 alleles. An allele is a<br />
specific form <strong>of</strong> a gene. The APOE gene has three alleles (e2, e3, e4), which result in six<br />
combinations or genotypes (e2/e2, e2/e3, e2/e4, e3/e3, e3/e4, e4/e4). Everyone has one <strong>of</strong> these<br />
six genotypes. People with one or more copies <strong>of</strong> the APOE-e4 allele are at an increased risk for<br />
Alzheimer’s disease (Corder et al., 1993), whereas those with one or more copies <strong>of</strong> the APOEe2<br />
allele are at a decreased risk (Corder et al., 1994). I am interested in this area <strong>of</strong> research<br />
because <strong>of</strong> my family’s history <strong>of</strong> Alzheimer’s disease, reading articles about the relationship<br />
between APOE and cognition, and by working with my advisor who studies alcohol consumption<br />
and cognition.<br />
The relationship between APOE-e4 and cognition is well understood. Examining if this<br />
relationship is modified by alcohol consumption can advance the understanding <strong>of</strong> causal
5<br />
biological pathways as well as provide evidence for the use <strong>of</strong> genetic and environmental risk<br />
factors in the identification <strong>of</strong> high-risk individuals for targeted interventions.<br />
Background<br />
The Framingham Heart Study (FHS) is a longitudinal study that began in 1948 with an<br />
original cohort <strong>of</strong> 5,209 men and women between the ages <strong>of</strong> 28 and 62 from Framingham,<br />
Massachusetts. The purpose <strong>of</strong> the FHS is to detect risk factors for cardiovascular disease, but<br />
the longitudinal design has made it a valuable resource for studying risk factors for Alzheimer’s<br />
disease and cognitive decline. The recruitment <strong>of</strong> participants for the Offspring cohort, who are<br />
the children <strong>of</strong> the Original Cohort, began in 1971 with 5,124 men and women between the ages<br />
<strong>of</strong> 5 and 70. A total <strong>of</strong> 3,021 participants between the ages <strong>of</strong> 40 and 93 attended the most recent<br />
clinical exam, which was completed in 2008. Additional cohorts have been created, which<br />
includes the Third Generation Cohort, who are the grandchildren <strong>of</strong> the Original Cohort, the<br />
Omni Cohort, the Second Generation Omni Cohort, and a New Offspring Spouse Cohort. For<br />
additional information on the FHS, please see Dawber et al. (1951) Feinleib et al. (1975),<br />
Massaro et al. (Massaro et al., 2004) and http://www.framinghamheartstudy.org/.<br />
Methods<br />
Measurements. The Offspring Cohort has undergone eight clinical examinations between<br />
1971 and 2008 and two neuropsychological examinations, which were completed in 2005 and<br />
2007. Participants received the Boston Naming Test, Wechsler Adult Intelligence Test, Wechsler<br />
Memory Scale, Halstead Reitan Neuropsychological Test Battery, and the Hooper Visual<br />
Organization during both <strong>of</strong> the neuropsychological examinations. I chose to use data from the<br />
Wechsler Memory Scale because it examines immediate and delayed recall <strong>of</strong> logical, paired<br />
associate, and visual memory. Each <strong>of</strong> these cognitive domains was analyzed independently.<br />
FHS investigators assessed alcohol consumption during clinical exams 1-7 (1971-2001)<br />
using three open-ended questions: (1) how many bottles, cans or glasses <strong>of</strong> beer do you<br />
consume per week; (2) how many glasses <strong>of</strong> wine do you consume per week; (3) how many<br />
cocktails (i.e. drinks containing liquor) do you consume per week? I calculated individual<br />
alcohol index scores for each clinical exam by adding the number <strong>of</strong> beers, cocktails, and glasses<br />
<strong>of</strong> wine together to determine the total number <strong>of</strong> alcoholic beverages consumed per week. I then<br />
calculated an average index score for each participant by dividing the total individual alcohol<br />
index scores by the number <strong>of</strong> clinical exams attended. I used this measure to group participants<br />
into the following classifications: (1) abstinent/light- less than one alcoholic beverage consumed<br />
per week; (2) moderate- between one and seven alcoholic beverages consumed per week; (3)<br />
heavy- more than seven alcoholic beverages consumed per week. These classifications are<br />
consistent with the recommendations <strong>of</strong> the National Institute for Alcohol Abuse and Alcoholism<br />
(NIAA).<br />
I dichotomized participants according to the presence <strong>of</strong> one or more APOE-e4 alleles.<br />
Participants with e2/e2, e2/e3, or e3/e3 genotype were defined as e4- and participants with e3/e4,<br />
e2/e4, or e4/e4 genotype were defined as e4+.<br />
Gender, age, education, smoking status, total cholesterol (TC), and number <strong>of</strong> years<br />
between neuropsychological exams were controlled for in all statistical models. The average<br />
time between neuropsychological exams was 6.13 years (SD 1.12, range 1.34-8.32). I
6<br />
dichotomized education, smoking, and total cholesterol as having obtained a college degree,<br />
being a current/former smoker or never smoked, and high TC (>200mg/dL) or normal/low TC<br />
(
7<br />
cognition among older adults with one or more APOE-e4 alleles. Heavy alcohol consumption<br />
was associated with fewer declines in logical, paired associate, and visual memory. However,<br />
these findings did not reach statistical significance.<br />
Discussion<br />
The presence <strong>of</strong> one or more APOE-e4 alleles was associated with greater decline in<br />
logical and paired associate memory. These findings are consistent with other studies that have<br />
found APOE-e4 to modify multiple cognitive domains (Wilson et al., 2002), including logical<br />
(Levy et al., 2004) and paired associate memory (Adamson et al., 2010). Mean alcohol<br />
consumption did not have a significant effect on the decline <strong>of</strong> immediate or delayed recall <strong>of</strong><br />
logical, paired-associate, or visual memory. Previous studies have found the association between<br />
alcohol consumption and cognition to follow a J or U shaped curve (Peters, Peters, Warner,<br />
Beckett, & Bulpitt, 2008), but some studies have found alcohol consumption not to be associated<br />
with cognitive function (Cervilla, Prince, & Mann, 2000; Launer, Feskens, Kalmijn, &<br />
Kromhout, 1996; Solfrizzi et al., 2007). We found that heavy alcohol consumption to be<br />
associated with less cognitive decline. This association was not statistically significant and can<br />
be attributed to several factors. The first is a survivor effect among heavy alcohol consumers<br />
(Anstey, Mack, & Cherbuin, 2009). Prolonged heavy alcohol consumption is associated with<br />
increased risks for cancer (Cho, Lee, Rimm, Fuchs, & Giovannucci, 2012) and stroke (Ikehara et<br />
al., 2008) among other causes <strong>of</strong> premature mortality. Because participants were required to be<br />
65 years <strong>of</strong> age or older upon receiving the first neuropsychological examination, heavy alcohol<br />
consumers who would have exhibited greater decline over time may not have remained in the<br />
FHS long enough to receive the second neuropsychological examination due to an increased risk<br />
for conditions associated with premature mortality. A second explanation is that alcoholics and<br />
heavy alcohol consumers are more likely than non-problem drinkers to under report or under<br />
estimate their alcohol consumption (Del Boca & Noll, 2000). If the number <strong>of</strong> alcoholic<br />
beverages consumed by “true” heavy alcohol consumers were under-reported, then these<br />
individuals may be categorized as moderate consumers, potentially leading for greater cognitive<br />
decline to be associated with lower alcohol consumption (Benedetti, Parent, & Siemiatycki,<br />
2009).<br />
APOE contributes to cognitive decline through pathological and vascular mechanisms.<br />
The concentration <strong>of</strong> cerebral β-amyloid <strong>of</strong> AD patients with one or more APOE-e4 alleles has<br />
been shown to be significantly greater than non-demented controls (Rebeck, Reiter, Strickland,<br />
& Hyman, 1993). This may be due to the e4 variant being less effective at binding to amyloid<br />
beta compared to APOE-e3 (Tokuda et al., 2000). The presence <strong>of</strong> one or more APOE-e4 alleles<br />
is a significant risk factor for heart disease (Nordlie, Wold, & Kloner, 2005) and high cholesterol<br />
(Heeren, Beisiegel, & Grewal, 2006), both <strong>of</strong> which have been shown to increase risk for<br />
cognitive decline and dementia. Conversely, alcohol consumption has been shown to be<br />
protective against such conditions (de Lorimer, 2000).<br />
A statistically significant interaction between genetic and environmental risk factors may<br />
suggest the existence <strong>of</strong> a biological pathway involving both risk factors. The findings from the<br />
current study do not support the presence <strong>of</strong> such a pathway, but significant gene-environment<br />
interactions between alcohol and APOE have been detected previously. Dufouil et al. (2000)<br />
found moderate alcohol consumption to be associated with a decreased risk for cognitive decline<br />
among individuals with no APOE-e4 alleles, whereas the opposite association was found among
those with one or more APOE-e4 alleles. In a second study (Carmelli, Swan, Reed, Schellenberg,<br />
& Christian, 1999), investigators determined that the protective effect <strong>of</strong> light to moderate<br />
alcohol consumption was greater among individuals with one or more APOE-e4 alleles.<br />
The lack <strong>of</strong> statistically significant findings for alcohol consumption or for an interaction<br />
between APOE-e4 and alcohol consumption may be due to the relatively small sample size<br />
compared to previous studies. Previous studies that have detected statistically significant<br />
associations between alcohol consumption and cognitive decline, as well as significant<br />
interactions between APOE-e4 and alcohol consumption have included sample sizes between<br />
1,400 (Anttila et al., 2004) to 1,800 (Elias, Elias, D'Agostino, Silbershatz, & Wolf, 1999)<br />
participants. Despite this limitation, the current study does include multiple strengths. First is the<br />
use <strong>of</strong> multiple measurements <strong>of</strong> alcohol consumption following midlife to longitudinally derive<br />
mean alcohol consumption. This method may help limit, but not fully prevent, the effect that<br />
dramatic changes in alcohol consumption over the life span has on cognitive functioning. Second,<br />
this study examined the relationship between APOE-e4, alcohol consumption, and cognitive<br />
decline in multiple domains. The brain is extremely heterogeneous and the effects <strong>of</strong><br />
environmental and genetic risk factors may act differently on various regions <strong>of</strong> the brain.<br />
Morphological changes to specific hemispheres in the brain have been associated with declines<br />
in logical (Bava et al., 2010), paired associate (Han et al., 2007), and visual (H<strong>of</strong>stetter,<br />
Achaibou, & Vuilleumier, 2012). This may explain why APOE-e4 had a significant effect on<br />
logical and paired associate memory, but not visual memory. Future research should examine the<br />
relationship between cognitive decline and changes in alcohol consumption following midlife<br />
and the effect that APOE genotypes may have on this relationship. Because alcohol consumption<br />
is a modifiable behavior, it is important to have a clear understanding on the relationship<br />
between alcohol consumption and cognition in order to provide appropriate recommendations on<br />
alcohol consumption across the life span.<br />
8
9<br />
Table 2.<br />
Descriptive characteristics <strong>of</strong> N=475 participants <strong>of</strong> the Offspring Cohort <strong>of</strong> the Framingham<br />
Heart Study.<br />
Variable<br />
Male(n=218) Female(n=257) P-Value<br />
Age during second cognitive exam (SD) 77.2 (4.1) 77.3 (4.2) 0.85<br />
Number <strong>of</strong> years between cognitive exams 6.1 (1.11) 6.2(1.12) 0.52<br />
(SD)<br />
Age during clinical exam 1 44.3 (4.3) 44.2 (4.4) 0.87<br />
Total cholesterol (%) 0.008<br />
High cholesterol 133 (61) 117 (45.5)<br />
Low cholesterol 85 (39) 140 (54.5)<br />
APOE status 0.14<br />
e4+ 51 (23.4) 46 (17.9)<br />
e4- 167 (76.6) 211 (32.1)<br />
Smoking Status
10<br />
Table 3.<br />
Time, Time x APOE and Time x Alcohol Consumption effects on cognitive change (p-values).<br />
Logical<br />
Paired Associate<br />
Immediate Delayed Immediate Delayed<br />
Time 0.0011
11<br />
Bava, S., Thayer, R., Jacobus, J., Ward, M., Jernigan, T. L., & Tapert, S. F. (2010). Longitudinal<br />
characterization <strong>of</strong> white matter maturation during adolescence. Brain Research, 1327,<br />
38-46.<br />
Benedetti, A., Parent, M. E., & Siemiatycki, J. (2009). Lifetime consumption <strong>of</strong> alcoholic<br />
beverages and risk <strong>of</strong> 13 types <strong>of</strong> cancer in men: Results from a case-control study in<br />
Montreal. Cancer Detection and Prevention, 32(5-6), 352-362.<br />
Carmelli, D., Swan, G. E., Reed, T., Schellenberg, G. D., & Christian, J. C. (1999). The effect <strong>of</strong><br />
apolipoprotein E epsilon4 in the relationships <strong>of</strong> smoking and drinking to cognitive<br />
function. Neuroepidemiology, 18(3), 125-133.<br />
Cervilla, J. A., Prince, M., & Mann, A. (2000). Smoking, drinking, and incident cognitive<br />
impairment: A cohort community based study included in the Gospel Oak project.<br />
Journal <strong>of</strong> Neurology, Neurosurgery, and Psychiatry, 68(5), 622-626.<br />
Cho, E., Lee, J. E., Rimm, E. B., Fuchs, C. S., & Giovannucci, E. L. (2012). Alcohol<br />
consumption and the risk <strong>of</strong> colon cancer by family history <strong>of</strong> colorectal cancer. The<br />
American Journal <strong>of</strong> Clinical Nutrition, 95(2), 413-419.<br />
Corder, E. H., Saunders, A. M., Risch, N. J., Strittmatter, W. J., Schmechel, D. E., Gaskell, P. C.,<br />
Jr., et al. (1994). Protective effect <strong>of</strong> apolipoprotein E type 2 allele for late onset<br />
Alzheimer disease. Nature Genetics, 7(2), 180-184.<br />
Corder, E. H., Saunders, A. M., Strittmatter, W. J., Schmechel, D. E., Gaskell, P. C., Small, G.<br />
W., et al. (1993). Gene dose <strong>of</strong> apolipoprotein E type 4 allele and the risk <strong>of</strong> Alzheimer's<br />
disease in late onset families. Science, 261(5123), 921-923.<br />
Dawber, T. R., Meadors, G. F., & Moore, F. E. (1951). Epidemiological approaches to heart<br />
disease: The Framingham Study. Americal Journal <strong>of</strong> <strong>Public</strong> <strong>Health</strong>, 41(3), 219-281.<br />
de Lorimer, A. A. (2000). Alcohol, wine, and health. American Journal <strong>of</strong> Surgery,<br />
180(5), 357-361.<br />
Del Boca, F. K., & Noll, J. A. (2000). Truth or consequences:Tthe validity <strong>of</strong> self-report data in<br />
health services research on addictions. Addiction, 95 Suppl 3, S347-360.<br />
Dufouil, C., Tzourio, C., Brayne, C., Berr, C., Amouyel, P., & Alperovitch, A. (2000). Influence<br />
<strong>of</strong> apolipoprotein E genotype on the risk <strong>of</strong> cognitive deterioration in moderate drinkers<br />
and smokers. Epidemiology, 11(3), 280-284.<br />
Elias, P. K., Elias, M. F., D'Agostino, R. B., Silbershatz, H., & Wolf, P. A. (1999). Alcohol<br />
consumption and cognitive performance in the Framingham Heart Study. American<br />
Journal <strong>of</strong> Epidemiology, 150(6), 580-589.
12<br />
Feinleib, M., Kannel, W. B., Garrison, R. J., McNamara, P. M., & Castelli, W. P. (1975). The<br />
Framingham Offspring Study. Design and preliminary data. Preventive Medicine, 4(4),<br />
518-525.<br />
Ferraro, K. F. (2007). Is gerontology interdisciplinary? The journals <strong>of</strong> gerontology. Series B,<br />
Psychological Sciences and Social Sciences, 62(1), S2.<br />
Han, S. D., Houston, W. S., Jak, A. J., Eyler, L. T., Nagel, B. J., Fleisher, A. S., et al. (2007).<br />
Verbal paired-associate learning by APOE genotype in non-demented older adults: fMRI<br />
evidence <strong>of</strong> a right hemispheric compensatory response. Neurobiology <strong>of</strong> Aging, 28(2),<br />
238-247.<br />
Heeren, J., Beisiegel, U., & Grewal, T. (2006). Apolipoprotein E recycling: Implications for<br />
dyslipidemia and atherosclerosis. Arteriosclerosis, Thrombosis, and Vascular Biology,<br />
26(3), 442-448.<br />
H<strong>of</strong>stetter, C., Achaibou, A., & Vuilleumier, P. (2012). Reactivation <strong>of</strong> visual cortex during<br />
memory retrieval: Content specificity and emotional modulation. NeuroImage, 60(3),<br />
1734-1745.<br />
Ikehara, S., Iso, H., Toyoshima, H., Date, C., Yamamoto, A., Kikuchi, S., et al. (2008). Alcohol<br />
consumption and mortality from stroke and coronary heart disease among Japanese men<br />
and women: The Japan collaborative cohort study. Stroke; a Journal <strong>of</strong> Cerebral<br />
Circulation, 39(11), 2936-2942.<br />
Launer, L. J., Feskens, E. J., Kalmijn, S., & Kromhout, D. (1996). Smoking, drinking, and<br />
thinking. The Zutphen Elderly Study. American Journal <strong>of</strong> Epidemiology, 143(3), 219-<br />
227.<br />
Levy, J. A., Bergeson, J., Putnam, K., Rosen, V., Cohen, R., Lalonde, F., et al. (2004). Contextspecific<br />
memory and apolipoprotein E (ApoE) epsilon 4: Cognitive evidence from the<br />
NIMH prospective study <strong>of</strong> risk for Alzheimer's disease. Journal <strong>of</strong> the International<br />
Neuropsychological Society : JINS, 10(3), 362-370.<br />
Massaro, J. M., D'Agostino, R. B., Sr., Sullivan, L. M., Beiser, A., DeCarli, C., Au, R., et al.<br />
(2004). Managing and analysing data from a large-scale study on Framingham Offspring<br />
relating brain structure to cognitive function. Statistics in Medicine, 23(2), 351-367.<br />
Nordlie, M. A., Wold, L. E., & Kloner, R. A. (2005). Genetic contributors toward increased risk<br />
for ischemic heart disease. Journal <strong>of</strong> Molecular and Cellular Cardiology, 39(4), 667-<br />
679.<br />
Peters, R., Peters, J., Warner, J., Beckett, N., & Bulpitt, C. (2008). Alcohol, dementia and<br />
cognitive decline in the elderly: A systematic review. Age and Aging, 37(5), 505-512.
13<br />
Rebeck, G. W., Reiter, J. S., Strickland, D. K., & Hyman, B. T. (1993). Apolipoprotein E in<br />
sporadic Alzheimer's disease: Allelic variation and receptor interactions. Neuron, 11(4),<br />
575-580.<br />
Seccombe, K., & Ishii-Kuntz, M. (1991). Perceptions <strong>of</strong> problems associated with aging:<br />
Comparisons among four older age cohorts. The Gerontologist, 31(4), 527-533.<br />
Shenk, D., Rowles, G. D., Peacock, J. R., Mitchell, J., Fisher, B. J., & Moore, K. S. (2001).<br />
Teaching research in gerontology: Toward a cumulative model. Educational Gerontology,<br />
27, 537-556.<br />
Solfrizzi, V., D'Introno, A., Colacicco, A. M., Capurso, C., Del Parigi, A., Baldassarre, G., et al.<br />
(2007). Alcohol consumption, mild cognitive impairment, and progression to dementia.<br />
Neurology, 68(21), 1790-1799.<br />
Tokuda, T., Calero, M., Matsubara, E., Vidal, R., Kumar, A., Permanne, B., et al. (2000).<br />
Lipidation <strong>of</strong> apolipoprotein E influences its is<strong>of</strong>orm-specific interaction with<br />
Alzheimer's amyloid beta peptides. The Biochemical Journal, 348 Pt 2, 359-365.<br />
Wilson, R. S., Schneider, J. A., Barnes, L. L., Beckett, L. A., Aggarwal, N. T., Cochran, E. J., et<br />
al. (2002). The apolipoprotein E epsilon 4 allele and decline in different cognitive<br />
systems during a 6-year period. Archives <strong>of</strong> Neurology, 59(7), 1154-1160.
14<br />
Student Keynote Address II<br />
Amanda A. Holup earned a B.S. in Biochemistry from<br />
Eckerd <strong>College</strong> and a Master’s degree in Bioethics and Medical<br />
Humanities from the <strong>University</strong> <strong>of</strong> South Florida. Currently,<br />
she is a third year doctoral student in the Aging Studies<br />
program at the <strong>University</strong> <strong>of</strong> South Florida. Her research<br />
experience and interests include health information technology,<br />
transitions across the long-term care continuum including<br />
community discharges from nursing homes, and bioethics.
15<br />
Facility Characteristics Associated with the Use <strong>of</strong><br />
Electronic <strong>Health</strong> Records in Residential Care Facilities<br />
Amanda A. Holup<br />
<strong>University</strong> <strong>of</strong> South Florida School <strong>of</strong> Aging Studies<br />
Characterized as the longitudinal collection <strong>of</strong> person-level and population-level<br />
electronic health information with provisions that support the delivery <strong>of</strong> healthcare, electronic<br />
health records (EHRs) have been credited as a safe and effective strategy for improving the<br />
safety <strong>of</strong> health care, eliminating administrative and operations inefficiencies, reducing costs,<br />
and encouraging greater patient engagement (Hedstrom, 2007; Kramer, Richard, Epstein, Winn,<br />
& May, 2009; Shekelle, Morton, & Keeler, 2006; Wald & Shojania, 2001). Because <strong>of</strong> the<br />
promise that EHRs have in facilitating efficient care, the federal government authorized<br />
Medicaid and Medicare incentive payments totaling $27 billion to acute care providers and<br />
hospitals to promote the adoption and meaningful use <strong>of</strong> EHRs. Unfortunately, long-term care<br />
(LTC) providers are currently ineligible for these incentives.<br />
Despite efforts to promote EHR adoption across the LTC spectrum, contextual data on<br />
EHR systems in settings outside <strong>of</strong> hospitals is lacking (Brandeis, Hogan, Murphy, & Murray,<br />
2007). Across the LTC continuum, studies examining EHR use in nursing homes suggest that<br />
larger, nonpr<strong>of</strong>it facilities that are members <strong>of</strong> a chain, have a longer tenure <strong>of</strong> the administrator,<br />
and provide a greater number <strong>of</strong> services to their residents and were more likely to use EHRs for<br />
clinical care and administrative domains (Chan, 2008; Resnick, Manard, Stone, & Alwan, 2009).<br />
Similarly, across home health and hospice agencies, nonpr<strong>of</strong>it or government providers,<br />
providers that were members <strong>of</strong> a chain, and those with a larger patient census, were more likely<br />
to use EHRs (Bercovitz, Sengupta, & Jamison, 2010). However, the ability to provide a<br />
comprehensive understanding <strong>of</strong> EHR utilization across the LTC spectrum has been hampered<br />
by the lack <strong>of</strong> information on residential care facilities (RCFs).<br />
In the past two decades, RCFs have emerged as a LTC alternative for older Americans.<br />
Nationally, these community-based living environments provide housing and can tailor personal<br />
care services to meet the changing needs <strong>of</strong> approximately one million elders (Golant, 2008).<br />
Although there is a great deal <strong>of</strong> heterogeneity in the types <strong>of</strong> services provided, the amount <strong>of</strong><br />
care <strong>of</strong>fered, and regulatory standards governing RCFs, these facilities have come to serve an<br />
increasingly disabled resident population (Spillman, K., & McGillard, 2002; Stevenson &<br />
Grabowski, 2010). However, since RCFs are not healthcare facilities, it is <strong>of</strong>ten a challenge to<br />
manage the care needs <strong>of</strong> residents, leaving them vulnerable to hospitalizations (Becker, Boaz,<br />
Andel, & DeMuth, 2011) and medications mismanagement (Sloane et al., 2004).Although EHR<br />
integration into RCFs may improve residents’ health outcomes, existing research on EHR use in<br />
RCFs is limited. Considering the potential significance <strong>of</strong> EHR integration across multiple care<br />
settings, this study addresses the current knowledge gap by examining the association between<br />
structural characteristics and the use <strong>of</strong> EHRs in RCFs.<br />
Method<br />
Source <strong>of</strong> the Data. Facility level data were drawn from the 2010 National Survey <strong>of</strong><br />
Residential Care Facilities (NSRCF), a nationally-representative, probability sample survey <strong>of</strong><br />
U.S residential care providers (Centers for Disease Control and Prevention, 2010). The RCFs
16<br />
included in the sample were licensed, registered, or otherwise regulated by the state; had 4 or<br />
more beds; at least one resident living in the facility providing personal care; 24 hour supervision<br />
and at least two meals a day to the residents. Facilities exclusively serving the mentally ill or<br />
developmentally disabled population were excluded. For the 2010 NSRCF, 3,605 RCFs were<br />
sampled and data were collected on 2,302 participating facilities.<br />
Measures<br />
Outcome Variable. The NSRCF defines an EHR as a computerized version <strong>of</strong> a resident’s<br />
health information that is used to manage his or her care (Centers for Disease Control and<br />
Prevention, 2010). A dichotomous variable representing whether or not a facility used an EHR<br />
was based on the question: “Other than for accounting or billing purposes, does this facility use<br />
Electronic <strong>Health</strong> Records?” Facilities endorsing the question were categorized as having EHR.<br />
Predictor Variables. Predictor variables included facility size, chain membership,<br />
ownership, Medicaid participation, occupancy, rural versus urban location, and staffing levels.<br />
The number <strong>of</strong> the licensed, registered, or certified residential care beds in each facility was used<br />
as a measure <strong>of</strong> facility size. A dichotomous variable to assess chain membership was defined as<br />
whether the facility was owned by a chain, group, or multi-facility system. Facility ownership<br />
was dichotomized as private, for pr<strong>of</strong>it and private, non-pr<strong>of</strong>it or government owned. Medicaid<br />
participation was affirmed based on whether the facility was certified or registered to participate<br />
in Medicaid. Occupancy rate was defined as the total number <strong>of</strong> residents divided by the total<br />
number <strong>of</strong> resident care beds in the facility and converted to a percentage. Staffing measures<br />
included direct care hours per patient day (HPPD) <strong>of</strong> registered nurses (RN), licensed practical<br />
nurses (LPN), and personal care aides (PCA). Rural verses urban facility location was<br />
determined based on the metropolitan statistical area (MSA). Resident demographics were<br />
described by the percentage <strong>of</strong> females and Caucasian residents residing in the facility.<br />
Statistical Analysis<br />
Exploratory analysis assessed specific domains <strong>of</strong> EHR use. Multinomial logistic<br />
regression was used to model the factors associated with EHR use in RCFs. Statistical<br />
significance was assessed with a two-tailed alpha <strong>of</strong> .05. The regression model was weighted by<br />
the appropriate sample weight to account for the complex, sampling design <strong>of</strong> the NSRCF. The<br />
regression model was estimated based on the SAS procedure SURERYLOGISTIC, which<br />
accounts for stratification, clustering, and unequal sample weighting within complex survey<br />
designs. All analyses were performed using SAS, Version 9.2<br />
Results<br />
Approximately 17% <strong>of</strong> RCFs (n=446) reported using an EHR with the most commonly<br />
reported functions being the ability to document resident demographics (38%) and the resident’s<br />
primary medical provider (37%). In contrast, EHR use for clinical care domains including<br />
recording drug interactions or contraindications (17%) and ordering or viewing diagnostic tests<br />
(4%) was less common.<br />
Logistic regression results indicated that chain membership, nonpr<strong>of</strong>it ownership, staffing,<br />
and participation in Medicaid were significantly associated with the use <strong>of</strong> an EHR in RCFs.
17<br />
Nonpr<strong>of</strong>it RCFs were 64% more likely to use an EHR (OR 1.642, 95% CI 1.218-2.215).<br />
Similarly, both chain membership and participation in Medicaid led to a roughly 40% increase in<br />
the likelihood <strong>of</strong> an RCF’s use <strong>of</strong> an EHR (OR 1.417, 95% CI 1.072-1.872 and OR 1.406. 95%<br />
CI 1.057-1.872, respectively). Facilities not providing care via LPNs were approximately 40%<br />
less likely to use an EHR (OR .599, 95% CI .413-.869). Several structural characteristics<br />
including size, MSA, occupancy rate, and resident case mix factors were not associated with the<br />
use this technology.<br />
Discussion<br />
Using data from the first nationally representative survey <strong>of</strong> RCFs, this study presents<br />
national estimates regarding the use <strong>of</strong> EHRs and the facility characteristics associated with the<br />
use <strong>of</strong> the technology. Our study revealed that ownership, chain membership, staffing levels, and<br />
Medicaid participation were significantly associated with EHR use suggesting that structural<br />
characteristics do play a role in influencing the adoption <strong>of</strong> EHRs in RCFs.<br />
With 17% <strong>of</strong> RCFs nationwide currently using EHRs, these findings provide benchmark<br />
evidence that the majority <strong>of</strong> RCFs are not using the technology. However, considerable<br />
variability exists within both EHR-users and nonusers across specific domains suggesting that<br />
EHR use may be implemented in stages with the use <strong>of</strong> this technology best modeled by a<br />
continuum <strong>of</strong> applicability instead <strong>of</strong> the current dichotomy. Moreover, there are many facilities<br />
nationwide that are considered non-users <strong>of</strong> the technology, but still opt to use specific EHR<br />
domains suggesting that clarification <strong>of</strong> the operational definition <strong>of</strong> an EHR system is needed.<br />
The study design, including its large sample, generalizability, and theoretical basis is a<br />
particular strength <strong>of</strong> the study. However, some limitations must be considered in interpreting the<br />
results. First, the NSRCF lacks questions regarding the duration <strong>of</strong> use the technology. Second,<br />
this study only examined the broad use <strong>of</strong> EHRs in RCFs and was unable to assess the impact<br />
that EHRs would have on resident outcomes. Future investigations are required to understand the<br />
impact that implementation and daily use <strong>of</strong> EHRs would have on resident outcomes.<br />
Although EHRs were originally developed for clinical care settings, the technology<br />
seems to hold promise across the LTC continuum. Considering the potential for EHRs to ease the<br />
transfer <strong>of</strong> information across multiple care settings, EHRs may serve as a valuable rebalancing<br />
tool as the industry moves toward more patient-centered care.<br />
References<br />
Becker, M., Boaz, T., Andel, R., & DeMuth, A. (2011). Predictors <strong>of</strong> avoidable hospitalizations<br />
among assisted living residents. Journal <strong>of</strong> the American Medical Directors Association.<br />
doi: 10.1016/j.jamda.2011.02.001<br />
Bercovitz, A., Sengupta, M., & Jamison, P. (2010). Electronic medical record adoption and use<br />
in home health and hospice (Vol. 45). Washington, D. C.: Centers for Disease Control<br />
and Prevention.<br />
Brandeis, G., Hogan, M., Murphy, M., & Murray, S. (2007). Electronic health record<br />
implementation in community nursing homes. Journal <strong>of</strong> the American Medical<br />
Directors Association, 8(1), 31-34. doi: 10.1016/j.jamda.2006.09.013
18<br />
Centers for Disease Control and Prevention. (2010). National survey <strong>of</strong> residental care facilities.<br />
Chan, S. (2008). Factors associated with the use <strong>of</strong> electronic information systems for drug<br />
dispensing and medication administration records in nursing homes. Journal <strong>of</strong> the<br />
American Medical Directors Association, 9(6), 414-421. doi:<br />
10.1016/j/jamda.2008.02.009<br />
Davis, J. A., Brannon, D., & Whitman, M. V. (2009). Organizational factors association with the<br />
use <strong>of</strong> information systems in nursing homes. <strong>Health</strong> Care Management Review, 34(2),<br />
141-151. doi: 10.1097/HMR.0b013e31819e912f<br />
Golant, S. M. (2008). The future <strong>of</strong> assisted living residences. A response to its uncertainity. In S.<br />
M. Golant & J. Hyde (Eds.), The assisited living residences. A vision for the future (pp. 3-<br />
45). Baltimore, MD: John Hopkins Press.<br />
Hedstrom, K. (2007). The values <strong>of</strong> IT in elderly care. Information Technology and People, 20,<br />
72-84.<br />
Kramer, A., Richard, A. A., Epstein, A., Winn, D., & May, K. (2009). Understanding the costs<br />
and benefits <strong>of</strong> health information technology in nursing homes and home health<br />
agencies: Case study findings. Washington, D. C.: Retrieved from<br />
http://aspe.hhs.gov/daltcp/reports/2009/HITcsf.htm.<br />
Resnick, H. E., Manard, B. B., Stone, R. I., & Alwan, M. (2009). Use <strong>of</strong> electronic information<br />
systems in nursing homes: United States, 2004. Journal <strong>of</strong> the American Medical<br />
Informatics Association, 16(2), 179-186. doi: 10.1197/jamia.M2955<br />
Shekelle, P., Morton, S. C., & Keeler, E. B. (2006). Costs and benefits <strong>of</strong> health information<br />
technology. Rockville, MD: Agency for <strong>Health</strong>care Research and Quality.<br />
Sloane, P. D., Gruber-Baldini, A. L., Zimmerman, S., Roth, M., Watson, L., Boustani, M., . . .<br />
Hebel, J. R. (2004). Medication undertreatment in assisted living settings. Archives <strong>of</strong><br />
Internal Medicine, 164(18), 2031-2037.<br />
Spillman, B., K., L., & McGillard, C. (2002). Trends in residental long-term care: Use <strong>of</strong><br />
nursing homes and assisted living and characteristics <strong>of</strong> facilities and residents.<br />
Washington, D. C.: Office <strong>of</strong> the Assistant Secretary for Planning and Evaluation.<br />
Stevenson, D. G., & Grabowski, D. C. (2010). Sizing up the market for assisted living. <strong>Health</strong><br />
Affairs, 29, 35-43 doi: 10.1377/hlthaff.2009.0527<br />
Wald, H., & Shojania, K. G. (2001). Making health care safer: A critical analysis <strong>of</strong> patient<br />
safety practices Rockville, MD: Agency for <strong>Health</strong>care Research and Quality.
19<br />
The Anne & Everett Lee Scholarship Awards<br />
Every year faculty judges from each <strong>of</strong> the participating schools choose the top three<br />
student presentations for awards <strong>of</strong> $200, $100, and $50. The presenters are judged based on<br />
the importance, the timeliness, the relevance <strong>of</strong> their topic, the soundness <strong>of</strong> approach, and the<br />
clarity <strong>of</strong> their presentations. In addition to the monetary awards, there are honorable<br />
mentions for the best individual presentation and poster as well as the best undergraduate.<br />
Since 2005, the awards have been given in the name <strong>of</strong> Drs. Everett S. and Anne Lee.<br />
Dr. Everett Lee was a pr<strong>of</strong>essor emeritus <strong>of</strong> sociology and served as the assistant director <strong>of</strong><br />
the Institute <strong>of</strong> Gerontology at the <strong>University</strong> <strong>of</strong> <strong>Georgia</strong>. Dr. Everett Lee was interested in the<br />
demographics <strong>of</strong> aging, and both <strong>of</strong> the Lees had research interests in migration. Dr. Anne<br />
Lee now provides funding for the awards.
20<br />
First Place Overall<br />
Michael Schuier<br />
Second Place Overall<br />
Elizabeth Couser<br />
Third Place Overall<br />
Chad Straight<br />
Best Presentation<br />
Hyunjin Noh<br />
Best Poster<br />
Ruth Robbins<br />
Best Undergraduate<br />
Jessica Lyles
21<br />
Poster Presentation Abstracts<br />
Holly Aversano<br />
hollyave@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, Institute <strong>of</strong> Gerontology<br />
Exploring the Role <strong>of</strong> Occupational Therapy in Promoting Patient Meaning-Making<br />
Self-efficacy and mastery over environmental demands have been shown to predict positive<br />
mental health. Those who feel autonomous are less likely to experience depressive symptoms or<br />
feel as though their lives are meaningless. However, individuals with functional disabilities (e.g.,<br />
physical, cognitive) are vulnerable to loss <strong>of</strong> self-efficacy and mastery, and are therefore at risk<br />
for poor mental health outcomes. Data suggest that impaired individuals may benefit from<br />
expressing meaning through occupation. By definition, occupational therapy promotes selfefficacy<br />
and environmental mastery for patients with functional loss. Yet, the role <strong>of</strong><br />
occupational therapy in promoting meaning-making in impaired older patients’ lives is unknown.<br />
The objective <strong>of</strong> this study therefore is to report preliminary data from in-depth interviews with<br />
occupational therapists and older patients’ receiving therapy with the goal <strong>of</strong> exploring meaningmaking<br />
through occupation and perceived environmental mastery. Both the role <strong>of</strong> occupational<br />
therapy in promoting meaning-making and barriers to achieving meaning-making through<br />
occupation will be described.
22<br />
Lauren Breland<br />
Elizabeth A. Di Napoli<br />
Rebecca S. Allen<br />
glbreland@gmail.com<br />
<strong>University</strong> <strong>of</strong> Alabama, Department <strong>of</strong> Psychology Center for Mental <strong>Health</strong> and Aging<br />
Staff Knowledge and Perceptions <strong>of</strong> Sexuality and Dementia among Older Adults in<br />
Long-Term Care<br />
As the geriatric population grows larger in the US, long-term nursing care becomes an extremely<br />
important facet <strong>of</strong> our nation’s health care system. In order to ensure that these older adults are<br />
enabled to safely express their autonomy in such settings, we must take a closer look at long term<br />
care practices that facilitate or inhibit personal choice. Sexuality has been deemed by<br />
psychologists and physicians to be a healthy outlet for natural desires and intimacies in all<br />
mature age groups. Some researchers even found that expression <strong>of</strong> sexuality in older adults<br />
improved their mental and physical state, and thereby lengthened their lifespans. Since older<br />
adult sexuality is popularly rejected by mainstream society, LTC staff might object or limit<br />
sexual expression in their residents. Negative attitude can become exacerbated when the older<br />
adults expressing sexual desires suffer from dementia or other cognitive impairments; sexual<br />
confusion and capacity to consent become important factors for recognizing what sexual<br />
behavior is healthy and safe for dementia patients. In any case, incapacitated residents deserve a<br />
chance to balance their autonomy and sexual fulfillment with safety issues surrounding<br />
diminished consent capacity. We examined LTC staff (N=58) opinions and attitudes about<br />
sexuality and dementia in long-term care. The 63-item questionnaire measured staff knowledge<br />
<strong>of</strong> dementia and sexuality, levels <strong>of</strong> religiosity, frequency <strong>of</strong> sexual behavior in residents, and<br />
staff attitudes towards these behaviors. Although we are still collecting data, preliminary<br />
analyses reveal associations between religiosity, dementia and sexuality knowledge, and LTC<br />
staff attitudes toward residents’ sexual expression.
23<br />
Kristen Condeelis<br />
Elizabeth Hahn, B.S.<br />
William Haley, Ph.D.<br />
kcondeelis@mail.usf.edu<br />
<strong>University</strong> <strong>of</strong> South Florida, School <strong>of</strong> Aging Studies<br />
Psychological Distress and Cognitive Functioning in Older Adults with Mild Cognitive<br />
Impairment<br />
Older adults with mild cognitive impairment (MCI) report depressive symptoms and other<br />
psychological distress, which may be associated with deficits in cognitive functioning. In<br />
addition, past research indicates that the level <strong>of</strong> depressive symptoms exhibited by older adults<br />
with MCI is positively correlated with the severity <strong>of</strong> their cognitive deficits, but it is unclear<br />
how this relationship in persons with MCI may differ from cognitively healthy older adults. This<br />
research project examined whether older adults with MCI reported poorer psychological wellbeing<br />
than cognitively healthy controls and whether poorer psychological well-being is<br />
correlated with level <strong>of</strong> global cognitive functioning. Psychological well-being was measured<br />
using the Perceived Stress Scale, Center for Epidemiologic Studies Depression Scale (CES-D),<br />
Life Satisfaction Scale, and average daily negative affect. Participants were on average 75 years<br />
old, and the sample consisted <strong>of</strong> 10 older adults with MCI (6 females and 4 males) and 17<br />
cognitively healthy older adult controls (14 females and 3 males). Approximately 74% <strong>of</strong><br />
participants were White. Results from this project indicate that having MCI was associated with<br />
greater depressive symptoms (p=.047) but did not differ on perceived stress or life satisfaction.<br />
The control participants had significantly higher global cognitive functioning. Higher global<br />
cognitive functioning was associated with lower life satisfaction but was not significantly<br />
associated with depressive symptoms or perceived stress. Persons with MCI experience<br />
depressive symptoms greater than that experienced in cognitively healthy older adults. Further<br />
research is needed to identify other potential areas <strong>of</strong> psychological distress in persons with MCI.
24<br />
Elizabeth Couser, BA, MSW<br />
elizabeth.couser@uky.edu<br />
<strong>University</strong> <strong>of</strong> Kentucky, Graduate Center for Gerontology<br />
Alzheimer’s Disease and the Visual System: Shifting the Focus to Future Research<br />
Introduction: Alzheimer’s disease has many avenues through which to conduct research. Studies<br />
have shown a relationship between the visual system (including structural changes in the retina,<br />
pupil, optic nerve) and Alzheimer’s. Some research has provided a follow up on these changes<br />
that may be able to assist in a more rapid diagnosis and subsequent treatment <strong>of</strong> Alzheimer’s.<br />
The purpose <strong>of</strong> the current review is to provide a summary <strong>of</strong> research concerning the<br />
relationship between Alzheimer’s and the visual system and to discuss valuable studies that have<br />
proceeded in the direction <strong>of</strong> diagnosis and treatment <strong>of</strong> AD through the visual system.<br />
Methods: A literature search was conducted in Medline. Search terms used were “Alzheimer’s,”<br />
“vision,” and “ocular biomarkers” The only inclusion criterion was the study had to discuss a<br />
relationship between Alzheimer’s disease on changes <strong>of</strong> the eye and/or visual system that may be<br />
indicative <strong>of</strong> AD. >100 articles met this requirement.<br />
Results: Reports <strong>of</strong> the exact changes in the eye and visual system were varied with no<br />
standardized methods to assess such changes. Studies reported changes in visual acuity, visual<br />
field, depth perception, color discrimination, and structural changes in the optic nerve, retina and<br />
pupil. A few recent studies examined the presence <strong>of</strong> amyloid β in the lens, aqueous humor and<br />
vitreous humor <strong>of</strong> the eye.<br />
Conclusion: Further research is required to compose a definitive list <strong>of</strong> changes that occur in the<br />
eye/visual system & to assist in the development <strong>of</strong> earlier non-invasive diagnoses and better<br />
treatments <strong>of</strong> AD.
25<br />
Brittany Taylor Cruce<br />
Lynn Snow<br />
Michelle Hilgeman<br />
Lindsey Jacobs<br />
Melissa Machac-Burleson<br />
Latrice Vinson<br />
Jenny Palmer<br />
Patricia Parmelee<br />
Rebecca Allen<br />
Dan Berlowitz<br />
Christine Hartmann<br />
btcruce@crimson.ua.edu<br />
<strong>University</strong> <strong>of</strong> Alabama, Center for Mental <strong>Health</strong> and Aging<br />
Development <strong>of</strong> the Resident-centered Assessment <strong>of</strong> Interactions with Staff and<br />
Engagement (RAISE): A Nursing Home Quality <strong>of</strong> Care Observational Tool<br />
Person-centered care has become a widespread nursing home (NH) care model, yet measuring<br />
successful implementation remains a challenge. We used an ethnographic approach to develop<br />
an assessment tool. We conducted over 60 hours <strong>of</strong> ethnographic observations on 4 NH units in<br />
one Veteran’s Affairs (VA) facility and 20 hours <strong>of</strong> interviews with staff and residents. Thematic<br />
analysis revealed quality and frequency <strong>of</strong> staff-resident interactions and resident engagement as<br />
aspects <strong>of</strong> person-centered care not captured by current quality assurance systems (e.g., MDS 3.0,<br />
annual inspections). We then developed the RAISE (Resident-centered Assessment <strong>of</strong><br />
Interactions with Staff and Engagement), a structured observational tool, to capture these<br />
identified constructs. We conducted 100 hours <strong>of</strong> observation using the tool in 8 NH units in 2<br />
VA facilities. Using an iterative approach informed by ethnographic notes and coding meetings,<br />
we identified a set <strong>of</strong> coding rules and administration processes that were as simultaneously<br />
efficient, non-reactive, and representative <strong>of</strong> CLC life as possible. Inter-rater reliabilities among<br />
a group <strong>of</strong> psychologist raters have been adequate (Cohen’s kappa = .75; averaged across RAISE<br />
variables and protocol types, n = 47 observations). We are now conducting further modifications<br />
and inter-rater reliability analyses to achieve adequate inter-rater reliability in a group <strong>of</strong> raters<br />
with wider variety in experience and representing multiple disciplines.
26<br />
Jason Dhabliwala, BS<br />
Lee Hyer, PhD<br />
Ciera V. Scott, MS<br />
Catherine Yeager, PhD<br />
dhabliwala.jason@mccg.org<br />
Mercer <strong>University</strong> School <strong>of</strong> Medicine & Family <strong>Health</strong> Center <strong>of</strong> Central <strong>Georgia</strong><br />
<strong>Georgia</strong> Neurosurgical Institute & Mercer <strong>University</strong> School <strong>of</strong> Medicine<br />
Mercer <strong>University</strong>, Clinical Mental <strong>Health</strong> Counseling Program & <strong>Georgia</strong> Neurosurgical Institute<br />
Eisenhower Army Medical Center, Department <strong>of</strong> Psychology<br />
Effects <strong>of</strong> a Holistic Memory Clinic for Older Adults<br />
Studies have shown that cognitive training for older adults is an asset to improving attention and<br />
working memory. Recent studies show promise that a more “holistic” and integrated approach<br />
are beneficial to less cognitively fit older adults. This analysis will examine whether the<br />
implementation <strong>of</strong> a 6-session, manualized memory training program can assist with improving<br />
function and overall well-being. Consented participants (N = 112) from the Central <strong>Georgia</strong><br />
community with Age Associated Memory Impairment (AAMI), Mild Cognitive Impairment<br />
(MCI), or mild dementia were asked to participate in memory training on cognitive habits, and<br />
attitudes, as well as function and adjustment. Compliance was also measured. We also had a<br />
Control group (N=30) who received no training. Finally, we classified participants by Risk<br />
Status—Low, Medium and High. Results showed that on the pre-measures the Memory Clinic<br />
group did not differ from the Control group. This pattern was also true <strong>of</strong> the post measures for<br />
the two groups. When the groups were separated by risk, however, the Low Risk Group was<br />
superior to the other groups, including Control, and continued to be superior in post measures on<br />
most cognitive assessments. Compliance also made a difference as those who complied<br />
performed better than those who did not. These tended to be Low and Medium Risk subjects.<br />
There were differences too on memory complaints and adjustment, again for the Low and<br />
Medium Risk Groups. Identifying high and low risk subjects was most helpful, resulting in clear<br />
differences between memory complaining subjects.
27<br />
Kristy Douglas, M.A.<br />
Christina S. McCrae, Ph.D<br />
Natalie D. Dautovich, Ph.D<br />
kdouglas@crimson.ua.edu<br />
<strong>University</strong> <strong>of</strong> Alabama, Psychology Department<br />
Age Differences and Variability in Pre-Sleep Arousal and Sleep Outcomes<br />
The purpose <strong>of</strong> this study was to examine age differences in mean values and variability in presleep<br />
arousal and sleep outcomes. Research has found age differences in sleep outcomes but no<br />
study has examined age differences in pre-sleep arousal, or the variability <strong>of</strong> pre-sleep arousal.<br />
Understanding these processes could inform research investigating the sleep-arousal relationship.<br />
50 younger and 50 older community-dwelling adults completed 14 consecutive daily diaries.<br />
Two arousal (Pre-Sleep Arousal Scale [PSAS] cognitive and somatic) and five sleep (sleep onset<br />
latency [SOL], wake after sleep onset [WASO], total sleep time [TST], sleep efficiency [SE],<br />
and sleep quality rating [SQR]) variables were analyzed using MANOVA’s. Intraindividual<br />
variability analyses were conducted to investigate age differences in variability. There was a<br />
significant difference between younger and older adults on sleep outcomes, F(4, 94)=7.88,<br />
p
28<br />
Katy L. Ford<br />
Ami N. Bryant,<br />
Giyeon Kim, Ph.D.<br />
klford@crimson.ua.edu<br />
<strong>University</strong> <strong>of</strong> Alabama, Psychology Department<br />
Age Differences in Satisfaction with and Perceived Benefit from Mental <strong>Health</strong> Services:<br />
Results from the Collaborative Psychiatric Epidemiology Surveys<br />
Although an extensive body <strong>of</strong> research reports older adults’ attitudes toward and underutilization<br />
<strong>of</strong> mental health services (MHS), relatively few studies have focused on age<br />
differences in mental health care among those utilizing MHS. This study examined variation by<br />
age in satisfaction with and perceived amount <strong>of</strong> benefit from MHS among those who had used<br />
MHS during the past year. Drawn from the Collaborative Psychiatric Epidemiology Surveys<br />
(2001-2003), 2,179 adults aged 18-87 were included in the multiple linear regression analyses.<br />
Results showed older age was positively associated with both MHS satisfaction (p
29<br />
Susannah L. Gordon, BS<br />
Kathryn N. Porter MS, RD, LD<br />
Kristen Brown, RD, LD<br />
Joan G. Fischer, PhD, RD, LD<br />
Gordon Jensen MD, PhD<br />
Mary Ann Johnson, PhD<br />
gordon21@uga.edu<br />
The <strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, Department <strong>of</strong> Foods and Nutrition<br />
Penn State <strong>University</strong>, Department <strong>of</strong> Nutritional Sciences<br />
Non-dietary Predictors and Consequences <strong>of</strong> Obesity in Older Adults in Congregate Meal<br />
Programs<br />
The purpose <strong>of</strong> this study is to explore non-dietary predictors and consequences <strong>of</strong> obesity in<br />
congregate meal participants in senior centers from Northeast <strong>Georgia</strong>’s Area Agency on Aging<br />
(AAA). Participants were recruited from the congregate meal program in senior centers <strong>of</strong><br />
Northeast <strong>Georgia</strong> (n = 97, mean age = 75 years, 78% female, 54% Caucasian, 46% African<br />
American). Height and weight were measured and obesity was defined as body mass index (BMI,<br />
kg/m 2 ) greater than 30 kg/m 2 (44% were obese). All measures were assessed using a<br />
questionnaire from the Geisinger Rural Aging Study. Compared to non-obese, the obese<br />
participants were greater than 15-percentage points more likely to have an unhealthy personal<br />
and family history <strong>of</strong> weight gain and/or obesity, watch more than 4 hours <strong>of</strong> television per day,<br />
use an assistive device, and utilize a clinic or physician’s <strong>of</strong>fice more than 4 times in twelve<br />
months. Although not always statistically significant (p = .0005 to .18), these data suggest<br />
several non-dietary factors that should be considered when addressing the problem <strong>of</strong> obesity in<br />
senior center participants.
30<br />
Brian Hentz<br />
brian.hentz@business.uconn.edu<br />
<strong>University</strong> <strong>of</strong> Connecticut, School <strong>of</strong> Business<br />
Cross-Generational Workplace Communication: Bridging the Divide in Age-Integrated<br />
Contexts<br />
Numerous scholars have brought attention to the coming aging revolution’s substantive impact<br />
on workplace dynamics (Beatty &Visser, 2004; Moseley & Dessinger, 2006), as well as<br />
suggested issues that should be integrated into universities’ business programs to prepare<br />
practitioners for an increasingly aging society (Brucker, 2004). Responding to these suggestions,<br />
I integrated a broad-based aging literacy framework into my undergraduate and graduate<br />
pr<strong>of</strong>essional communication courses to develop practitioners’ cultural competency. This<br />
framework allows learners not only to appreciate cross-generational dynamics more fully, but<br />
also to question their own assumptions about aging and critique the age-segregated life course in<br />
which they are embedded. My instructional framework for introducing topics on aging in these<br />
courses consists <strong>of</strong> 3 interconnected literacies: a representational literacy that encourages<br />
learners to examine the language and images they use to represent older adults; a perceptual<br />
literacy that challenges learners to questions myths and assumptions about aging; and a<br />
conceptual literacy that promotes an age-integrated model <strong>of</strong> the life course.<br />
I surveyed students following the aging literacy modules in my courses, and survey results<br />
indicate that students found discussions <strong>of</strong> aging not only relevant and timely, but personally<br />
rewarding. Nonetheless, more substantive efforts will be required to promulgate aging literacy<br />
across the business curriculum. Specifically, business school faculty will require pr<strong>of</strong>essional<br />
development to confidently integrate aging literacy into their courses. Also, stronger crossdisciplinary<br />
synergies between Schools <strong>of</strong> Business and Gerontology programs should be<br />
encouraged, for aging-specific materials, instructional cases, and other necessary resources will<br />
help facilitate robust learning.
31<br />
Aasha Hoogland, MA<br />
Faika Zanjani, PhD<br />
aasha.anderson@uky.edu<br />
<strong>University</strong> <strong>of</strong> Kentucky, Graduate Center for Gerontology<br />
Musical Memory in Individuals with Alzheimer’s Disease<br />
Introduction: Individuals with Alzheimer’s Disease (AD) face memory loss, personality changes,<br />
cognitive decline, and limited quality <strong>of</strong> life (QOL). Research on the role <strong>of</strong> music has indicated<br />
selective preservation <strong>of</strong> music memories in persons with AD, suggesting that music recognition<br />
might be present after other cognitive abilities have been lost. Music can induce an arousing<br />
response, and the therapeutic implications <strong>of</strong> retained musical memory in this population are<br />
immense as it could affect individuals’ QOL by providing enjoyment and relaxation, improving<br />
mood, and enhancing memory for novel experiences. The purpose <strong>of</strong> this review is to summarize<br />
the literature on musical memory in people with AD and examine implications for research.<br />
Methods: A literature review <strong>of</strong> articles addressing musical memory in people with AD was<br />
conducted through the PubMed (1989-2011) and PsycInfo databases (1991-2011).<br />
Results: Studies are conflicting with some showing evidence <strong>of</strong> preserved music memory in<br />
people with AD, and others indicating a complete loss <strong>of</strong> music memory. One explanation for the<br />
differences is that only certain types <strong>of</strong> memory are selectively preserved in individuals with AD.<br />
Some researchers have also indicated that an extensive musical background might facilitate<br />
preserved musical memory.<br />
Conclusion: Research is contradictory and suggests preservation <strong>of</strong> musical memory in select<br />
AD individuals, with a complete loss <strong>of</strong> musical memory in others. These findings indicate that<br />
further research is needed to elucidate the mixed pattern <strong>of</strong> results, and assess whether applied<br />
practices focusing on the utilization <strong>of</strong> musical memory can improve the QOL in individuals<br />
with AD.
32<br />
Francesca Iannaccone<br />
frani@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, <strong>College</strong> <strong>of</strong> <strong>Public</strong> <strong>Health</strong>, Department <strong>of</strong> <strong>Health</strong> Promotion and Behavior<br />
<strong>Public</strong> <strong>Health</strong> and Aging in Taiwan<br />
Issue/Problem: The population <strong>of</strong> older adults in both the United States and Taiwan is increasing<br />
rapidly. Currently, people aged 65 and older in Taiwan and the United States make up 10.9% and<br />
13.1% <strong>of</strong> the population respectively. The percentage <strong>of</strong> older adults in these countries is<br />
expected to continue to increase due to increased life expectancy and decreased birth rates. The<br />
aging experience in these countries is different in many ways. These countries have different<br />
health systems, attitudes towards aging, and programs <strong>of</strong>fered to older adults. Taiwan currently<br />
has a compulsory, single-payer healthcare system, while healthcare in the United States is largely<br />
privatized and is undergoing major changes. Attitudes towards older adults in Taiwan are<br />
strongly related to the concept <strong>of</strong> filial piety, while in the United States aging is associated with<br />
illness and decline. Research: The information presented was gathered during the <strong>University</strong> <strong>of</strong><br />
<strong>Georgia</strong>’s <strong>College</strong> <strong>of</strong> <strong>Public</strong> <strong>Health</strong> study abroad program, “<strong>Public</strong> <strong>Health</strong> and Aging,” during<br />
May <strong>of</strong> 2011 in Taiwan. This program consisted <strong>of</strong> field trips to facilities for older adults and<br />
lectures at Kaohsiung Medical <strong>University</strong>.<br />
Conclusion: Global population aging will have a great impact on all aspects <strong>of</strong> life. Taiwan<br />
addresses the needs <strong>of</strong> an aging population in unique ways. The study <strong>of</strong> older adults in Taiwan<br />
provides important information that can inform aging in the United States as this population<br />
continues to increase.
33<br />
Ashlynn Jackson<br />
ashlynnjackson@gmail.com<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, <strong>College</strong> <strong>of</strong> <strong>Public</strong> <strong>Health</strong>, Institute <strong>of</strong> Gerontology<br />
Advocacy Internship: <strong>Georgia</strong> Council on Aging<br />
An aging public policy issue in the state <strong>of</strong> <strong>Georgia</strong> is the Personal Needs Allowance (PNA),<br />
which nursing home residents on Medicaid receive each month. For years, aging advocates in the<br />
state have lobbied to increase the PNA amount that nursing home residents receive. In 1974, the<br />
Federal government set a minimum PNA <strong>of</strong> $25 and increased it to $30 in 1988. Although states<br />
have the option to increase this amount, <strong>Georgia</strong> remained at the $30 level for 18 years until the<br />
<strong>Georgia</strong> General Assembly raised the minimum to $50 in 2006. The current PNA amount has not<br />
been increased since 2006; therefore it does not keep up with the current costs <strong>of</strong> goods and<br />
services. While interning with the <strong>Georgia</strong> Council on Aging, I had the opportunity to gather<br />
research on PNA data in the state <strong>of</strong> <strong>Georgia</strong> and in other states. I developed a fact sheet to be<br />
used by advocates and volunteers to assist with presenting the issue to their local representatives<br />
and senators. The fact sheet is currently being used by <strong>Georgia</strong> Council on Aging lobbyists to<br />
educate General Assembly members about this policy issue and to recommend proposed<br />
legislation to increase the PNA in the state. My internship experience with the <strong>Georgia</strong> Council<br />
on Aging has given me insight into the public policy making process and the career <strong>of</strong> an aging<br />
advocate/lobbyist. I would like to share my experience with other gerontology students to raise<br />
their awareness <strong>of</strong> this career opportunity in aging.
34<br />
Meagan Jain<br />
Christina Sims Cummings<br />
mjain1@student.gsu.edu<br />
csims9@gsu.edu<br />
<strong>Georgia</strong> State <strong>University</strong>, Gerontology Institute<br />
Addressing Social Isolation in Older Adults: Adopt-A-Grandparent Program at GSU<br />
Several studies have investigated the relationship between social isolation and health outcomes<br />
among older adults. Victor, Scambler, and Bond (2009) posit that existing literature on social<br />
isolation and loneliness has mistakenly associated the two conditions as a normal part <strong>of</strong> aging.<br />
This can prove to be detrimental for older adults because they need social relationships similarly<br />
to all other age categories and may be more at risk for losing access to personal social networks.<br />
These companionate relationships indeed impact the well-being <strong>of</strong> the aging experience over the<br />
entire life course. In this paper we explore the purpose and implementation <strong>of</strong> the Adopt-a-<br />
Grandparent Program (AGP) at <strong>Georgia</strong> State <strong>University</strong>. The GSU-AGP was created to address<br />
the social disconnect that exist between the young and old, particularly for college-age students.<br />
By increasing the interaction among younger and older adults, we hope to reduce social isolation<br />
and loneliness among vulnerable seniors in the metro Atlanta area. Recruitment for participation<br />
in AGP is two-pronged: 1) we secured a relationship with A.G. Rhodes-Wesley Woods for<br />
access to institutionalized seniors; and 2) we solicited student volunteers from <strong>Georgia</strong> State that<br />
will serve as companions to selective grandparents. The students will be required to visit<br />
residents at the A.G. Rhodes facility for one hour every week. This program provides students<br />
the unique opportunity to build personal and reciprocal relationships with older adults in Metro<br />
Atlanta. This program has great implications for policy and practice.
35<br />
Aleta Johannaber<br />
Ann Pearman, Ph.D.<br />
ajohannaber1@student.gsu.edu<br />
<strong>Georgia</strong> State <strong>University</strong>, Gerontology Institute<br />
Primary Care and the Older Adult: A Review <strong>of</strong> the Literature<br />
In our society, a working relationship between patient and primary care physician (PCP) is not<br />
only highly valued by the patient but also appears to be an instrumental component <strong>of</strong> accurate<br />
diagnosis and successful treatment. When working with an older population, this relationship<br />
becomes even more valuable with the process <strong>of</strong> aging potentially bringing novel symptoms and<br />
disease such as cognitive decline, dementia, or stroke. While mild cognitive decline may present<br />
as expected primary aging, it is important for the PCP to maintain a cognizance <strong>of</strong> potential<br />
impairments in order to detect abnormal deterioration that can unnecessarily reduce quality <strong>of</strong><br />
life. The PCP is responsible for not only initiating discussion surrounding aging but also creating<br />
an environment conducive for the patients to dialogue about concerns they have with their health.<br />
This is <strong>of</strong>ten a challenging both because <strong>of</strong> the brevity <strong>of</strong> time a PCP <strong>of</strong>ten spends with patients<br />
during <strong>of</strong>fice visits and because <strong>of</strong> the cultural stigma towards older adults and aging in general.<br />
This presentation will discuss further the current research literature regarding patient care in the<br />
older population and the PCP’s impact on effective detection and treatment <strong>of</strong> cognitive decline.<br />
Preliminary results from a study about potential barriers to seeking help from one’s PCP will<br />
also be presented. Given that seeing one’s PCP is generally the first course <strong>of</strong> action for older<br />
adults with either mental or physical problems, understanding the potential barriers to quality<br />
care is an important step in improving service provision to older adults.
36<br />
Kristen Johnson<br />
Dr. Tom Price, MD<br />
Pat King, RN<br />
Sheryl Strasser, PhD<br />
Kjohn44@emory.edu<br />
Emory <strong>University</strong>, Division <strong>of</strong> Geriatrics<br />
Taskforce Against Mistreatment <strong>of</strong> Elders (TAME)<br />
Literature has shown elder abuse is a prevalent and misunderstood phenomenon occurring<br />
throughout the United States. Many publications address the topic, but there have been no<br />
consistent findings that can provide first responders with useful intervention systems that help<br />
identify and prevent the issue. The study intends to create an intervention program with easy,<br />
effective scoring tools for elder abuse dependent upon the commonalities <strong>of</strong> both victims and<br />
perpetrators. We have collected 98 cases from the Dekalb County court system (years: 2009,<br />
2010). To date, we have 41 cases have been reviewed through our carefully constructed case<br />
report form. We are using standardized methods <strong>of</strong> descriptive epidemiology to analyze our<br />
findings. Preliminary findings show victims were 48.8% female, averaged 71 years old,<br />
predominantly Caucasian (African American, 34.1; Caucasian, 51.2; Other, 2.4), and 29.3% had<br />
a shared living situation. Perpetrators were 73.2% male, averaged 46 years old, predominantly<br />
African American (African American, 53.7; Caucasian, 29.3; Other, 2.4), and 43.9% were<br />
children <strong>of</strong> the victim.
37<br />
Morgan Kiamy<br />
Grant Harris<br />
Patricia Parmelee<br />
Rebecca Allen<br />
mkkiamy@ua.edu<br />
<strong>University</strong> <strong>of</strong> Alabama, Department <strong>of</strong> Psychology, Center for Mental <strong>Health</strong> and Aging<br />
With or Without God: The stabilizing Effect <strong>of</strong> Religious Coping Style on Depression<br />
Symptoms in Chronically Ill Older Adults<br />
Older adults are at an increased risk for illnesses and poor health. The presence <strong>of</strong> a chronic<br />
illness brings with it multiple onerous alterations that <strong>of</strong>ten result in stress and other negative<br />
emotions. Some changes in older adults may provide resources for coping with disease and<br />
functional impairments that may affect people at this stage <strong>of</strong> life. The use <strong>of</strong> religious coping<br />
methods increase as one transitions from midlife to older adulthood. Hill’s (2010)<br />
Biopsychosocial Model <strong>of</strong> Religious Involvement suggests that religious involvement (e.g.,<br />
religious coping practices) moderates the association between stressful conditions (e.g., poor<br />
health) and mental health. The current study represents an examination <strong>of</strong> this aspect <strong>of</strong> the<br />
model. Participants included 45 non-demented older adults with advanced, chronic illness. This<br />
sample included approximately equal numbers <strong>of</strong> Caucasians and African Americans. Eight<br />
regression analyses were conducted to examine one’s religious coping style as a moderator <strong>of</strong> the<br />
effect <strong>of</strong> physical health on depression symptoms (i.e., CESD). The four religious coping styles<br />
used were differentiated by their level <strong>of</strong> involvement with God. Half <strong>of</strong> the models included an<br />
indicator <strong>of</strong> physical symptom number and half included physical symptom distress as an<br />
indicator <strong>of</strong> physical health. Race/ethnicity was a covariate in each model. Seven <strong>of</strong> the eight<br />
models included a significant interaction. Results indicate that religious coping moderates the<br />
effect <strong>of</strong> physical symptom number and burden on depression symptoms. Specifically, greater<br />
engagement with religious coping styles that include involvement with God stabilizes the effect<br />
<strong>of</strong> physical health on one’s depression symptoms.
38<br />
Junghyun Kim<br />
hpkjh@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, School <strong>of</strong> Social Work<br />
International Social Work for Older Asian Immigrants<br />
The proportion <strong>of</strong> Asian older adults in the older U.S. population is increasing and the rate <strong>of</strong> this<br />
increasing percentage will be much higher than that <strong>of</strong> non-Hispanic White older adults. There<br />
will be an increase in demands for social services to older Asian immigrants for social workers.<br />
The purpose <strong>of</strong> this study is to describe cultural issues <strong>of</strong> older Asian immigrants and existing<br />
programs related to international social work among the population through a literature review.<br />
A social worker’s awareness <strong>of</strong> cultural diversity is a key point for international pr<strong>of</strong>essional<br />
action. Older immigrants face the complicated process <strong>of</strong> adjustment to aging at the same time<br />
that they may experience <strong>of</strong> acculturative stress. The norm <strong>of</strong> filial piety which is rooted in Asian<br />
culture is a factor causing the acculturative stress among older Asian immigrants. The culture <strong>of</strong><br />
filial piety exists in the daily lives <strong>of</strong> Asian immigrants although it is not part <strong>of</strong> the American<br />
culture, causing gaps and conflicts. Although the form <strong>of</strong> filial duties has changed, filial piety<br />
from Confucianism is still an important value among Asians. Elderly Long Term Care Insurance<br />
(ELTCI) in Korea mirrors the current culture <strong>of</strong> filial piety in Asia. It is useful to identify the<br />
home delivered programs in the United States focusing on ethnic minority users for finding the<br />
way to enhancing the well-being <strong>of</strong> older Asian immigrants. When practitioners and policy<br />
makers have sensitivity to cultural diversity and try to understand older Asian immigrants’<br />
challenges, they can help immigrants adapt to current society and contribute to social integration.
39<br />
Cassandra Koehn<br />
ckoehn@mail.usf.edu<br />
<strong>University</strong> <strong>of</strong> South Florida, Aging Studies<br />
Quality <strong>of</strong> Life vs. Quantity: Care <strong>of</strong> End-Stage Nursing Home Residents with Dementia<br />
Recent research has called into question the necessity <strong>of</strong> curative medication, artificial hydration,<br />
and artificial nutrition as part <strong>of</strong> standard treatment for people with end-stage cognitive<br />
impairment. The difficulty <strong>of</strong> deciding on care is only amplified in nursing homes, where the fear<br />
<strong>of</strong> regulatory scrutiny does not always favor what makes the patient most comfortable. The aim<br />
<strong>of</strong> this literature review is to help determine the preferences and demographics <strong>of</strong> nursing home<br />
residents with end-stage dementia when it comes to the use <strong>of</strong> these life-sustaining methods. It<br />
also aims to review potential risks and benefits <strong>of</strong> these methods for these residents, as well as<br />
determine the level <strong>of</strong> discomfort that occurs when treatment is withdrawn. Information was<br />
gathered through literature search engines Academic Search Premier, AgeLine, LexisNexis<br />
Academic, Google Scholar, PsychINFO (Ovid), and MEDLINE (Ovid).<br />
Conclusion: Despite the extensive use <strong>of</strong> these life-prolonging measures in nursing homes, there<br />
appears to be many risks and side effects that may outweigh the benefits <strong>of</strong> treatment. Gaps in<br />
the literature include demographics <strong>of</strong> those most likely to undergo artificial hydration and<br />
studies on whether patients experience discomfort when curative medication is withdrawn. It is<br />
hoped that researchers will use the information compiled in this literature review to examine<br />
gaps in current studies and ascertain how better to serve this vulnerable section <strong>of</strong> the population.
40<br />
Renu Kumar<br />
rkumar9@student.gsu.edu<br />
<strong>Georgia</strong> State <strong>University</strong>, Gerontology Institute<br />
The Relationship <strong>of</strong> Marital Interaction and Memory in Older Adults<br />
Some loss in memory is considered a part <strong>of</strong> normal aging; however, there is a considerable<br />
heterogeneity in cognitive aging among older adults. Studies show that living arrangements,<br />
social interaction, social relationships and size <strong>of</strong> social network are among the predictors <strong>of</strong><br />
memory decline for older adults. Moreover, marriage has been associated with physiological<br />
health as well as psychological and social well-being. The purposed study will examine the<br />
relationship between the marital status and memory performance in older adults. I hypothesize<br />
that (1) being married will be positively related to memory <strong>of</strong> older adults; (2) participants with<br />
larger supportive social network will perform better on memory tests; and (3) that quality <strong>of</strong><br />
married life will be positively related to memory for married older adults. The study will survey<br />
two groups <strong>of</strong> 50 older adults – married people and non-married people (single, divorced, and<br />
widowed). The Mental Mini State Examination and Word List Recall will be used to measure<br />
memory (dependent variable). Independent variables will be measured with Marital Adjustment<br />
Test, Satisfaction with Life Scale, and Lubean Social Network Scale - 6. The t-test will be<br />
performed to calculate variance between the memory <strong>of</strong> married and non-married older adults<br />
and correlation will be performed to calculate the relationship between the quality <strong>of</strong> married life<br />
and memory <strong>of</strong> married older adults. Results from this study will provide a better understanding<br />
<strong>of</strong> the relationship between marital status and memory performance.
41<br />
Sung-Ae Kwon<br />
sak398@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, School <strong>of</strong> Social Work<br />
Attitude <strong>of</strong> Asians on Hospice Care<br />
With growing minority populations, cultural awareness and sensitivity toward such populations<br />
has become important in practice for all health pr<strong>of</strong>essionals. Particularly with respect to end-<strong>of</strong>life<br />
care, hospice care plays an important role in improving the quality <strong>of</strong> life <strong>of</strong> terminally ill<br />
patients and their families. However, Asians, African-Americans, and Latinos significantly<br />
underutilize hospice care as compared to non-Hispanic Whites. Efforts to enhance the quality <strong>of</strong><br />
end-<strong>of</strong>-life care for these minority groups would benefit from a culture-specific understanding <strong>of</strong><br />
how these populations view and understand hospice care. This study explores the attitudes <strong>of</strong><br />
Asians (N = 60) toward hospice care. Data were collected from Asian participants (Koreans,<br />
Japanese, Chinese, and Thais) by mail survey. Survey responses indicate that overall participants<br />
(83%) in this study show a neutral attitude toward hospice care; participants were more likely to<br />
have an agreement on hospice philosophy while disagreeing with the notion that hospice care is<br />
popular in their own cultures. 50 participants answered that they know hospice care only “little”<br />
or “not at all.” Participants who are young showed the lack <strong>of</strong> comfort with discussing the topic<br />
<strong>of</strong> death and dying, including the topic <strong>of</strong> hospice care. Overall, the findings highlight the<br />
importance <strong>of</strong> cultural considerations on the topic <strong>of</strong> death and dying and the need for more<br />
culture-specific approach.
42<br />
Anna Lee, MPH<br />
Lee Hyer, PhD<br />
Ciera V. Scott, MS<br />
lee_a@med.mercer.edu<br />
Mercer <strong>University</strong> School <strong>of</strong> Medicine<br />
<strong>Georgia</strong> Neurosurgical Institute & Mercer <strong>University</strong> School <strong>of</strong> Medicine<br />
Mercer <strong>University</strong>, Clinical Mental <strong>Health</strong> Counseling Program & <strong>Georgia</strong> Neurosurgical Institute<br />
Cogmed: A Cognitive Rehabilitation Intervention to Improve Working Memory in Older<br />
Adults<br />
Deficits in working memory are associated with age-related decline. We report on findings from<br />
a clinical trial that examined the effectiveness <strong>of</strong> Cogmed, a computerized program that trains<br />
working memory (WM). We assess this program against a sham control group in older adults.<br />
Older adults (N=68) living in the Central <strong>Georgia</strong> community who had memory impairment<br />
during initial screening (RBANS Delayed Memory Index), but had normal MMSEs, ADLs, and<br />
IADLs, were assessed. They met criteria for Mild Cognitive Impairment (MCI). Participants<br />
were randomized to either Cogmed or to the Sham cognitive program. A total <strong>of</strong> 25 sessions<br />
were completed over 5-7 weeks. Pre, post and post-post (12 weeks after intervention) measures<br />
were applied, involving cognitive, mood and function measures. Paired t-tests were conducted to<br />
find significant changes in outcomes between pre, post and post-post measures, as well as<br />
regression analyses on pre and post/post-post measures. In general, all subjects showed gains<br />
relative to the cognitive pre-measures. The Cogmed group showed statistically significant<br />
improvements in Digit Span Age, Span Board Age, Letter Number Sequencing Age, Story<br />
Memory, and Story Recall evaluations at post assessment. At post-post times, significant<br />
improvements were noted for Trails A, Trails B, Coding, Figure Memory, Figure Recall, Coding<br />
Age, and Matrix Reasoning Age. The Cogmed group also performed better on adjustment,<br />
satisfaction and affect relative to Sham. Results suggest that both the Cogmed group and Sham<br />
group enhance working memory in older adults with MCI. Cogmed especially appears to be<br />
effective for older adults.
43<br />
Jessica Lyles<br />
Kevin Waits, BS<br />
Ciera V. Scott, MS<br />
Lee Hyer, PhD<br />
jessica.l.lyles@live.mercer.edu<br />
Mercer <strong>University</strong>, Departments <strong>of</strong> Psychology & Biology<br />
Mercer <strong>University</strong> School <strong>of</strong> Medicine<br />
Mercer <strong>University</strong>, Clinical Mental <strong>Health</strong> Counseling Program & <strong>Georgia</strong> Neurosurgical Institute<br />
<strong>Georgia</strong> Neurosurgical Institute & Mercer <strong>University</strong> School <strong>of</strong> Medicine<br />
Value <strong>of</strong> Spinal Cord Stimulators for Older Adults: A Success Story<br />
The number <strong>of</strong> surgical interventions for chronic spinal pain is over 15 million. One procedure,<br />
spinal cord stimulation (SCS), is substantially less common than spinal surgery and is generally<br />
indicated after failed back surgery. Outcomes have generally failed to identify predictive<br />
variables <strong>of</strong> success in the SCS procedure, especially for older adults. We study core variables <strong>of</strong><br />
back pain patients, separated by intervention success and by age. Subjects (n=97) who present<br />
for the SCS procedure were evaluated using medical, psychiatric, personality, adjustment, and<br />
general demographic variables. We identified those that received the procedure (N= 39),<br />
targeting success, as well as age (Older and Younger, age 60 as our cut-<strong>of</strong>f). Patients were<br />
assessed prior to the procedure with the MBMD and with self-report scales, including depression<br />
(GDS-SF), anxiety (PSWQ), pain (BPI), and sleep (ESS). No differences were found in the premeasures.<br />
Using the MBMD symptom pr<strong>of</strong>ile, results showed that the Helped Group has less<br />
anxiety and depression and were less emotionally labile. As for personality, the Helped Group<br />
showed a Cooperative and Self-Assured style relative to the Non-Helped Group. The Non-<br />
Helped group was found to be more Oppositional. Regarding treatment variables, the Non-<br />
Helped Group had more Interventional Fragility than the Helped Group. Separated by age, the<br />
Older Group had a higher success rate than the Younger Group (54% vs. 36%). The MBMD<br />
pr<strong>of</strong>ile showed that the Older Group was more Self-Assured and had less Medication Abuse than<br />
the Younger Group. We discuss the importance <strong>of</strong> these personality and symptom variables.
44<br />
Gina M. McCaskill, MSW, MPA<br />
Kathleen A. Bolland, PhD<br />
gmmccaskill@crimson.ua.edu<br />
<strong>University</strong> <strong>of</strong> Alabama, School <strong>of</strong> Social Work<br />
A Review: Social Work Education and Aging Careers<br />
The growth <strong>of</strong> the older adult population in the United States means there is a concomitant<br />
growing need for geriatric social workers. Social work educators could play an important role in<br />
attracting undergraduate and graduate social work students into aging careers. The purpose <strong>of</strong><br />
this study was to identify the degree to which social work educators are developing and using<br />
evidenced-based approaches to the recruitment and retention <strong>of</strong> social work students into aging<br />
careers. A systematic review <strong>of</strong> peer-reviewed articles in the electronic database <strong>of</strong> the Journal<br />
<strong>of</strong> Social Work Education was conducted. Articles published from 1999 to 2011 were examined<br />
for topics related to the recruitment and retention <strong>of</strong> social work students into aging careers.<br />
Thirteen articles were found for the years under review. Nine <strong>of</strong> the thirteen articles met the<br />
review criteria. The majority <strong>of</strong> articles focused on developing aging-related social work<br />
graduate curricula and improving the field education experience in aging for graduate social<br />
work students. To a lesser degree, articles examined graduate and undergraduate social work<br />
students’ attitudes towards older adults and career interests in aging. The extant articles show<br />
promise for building knowledge in this area. The relatively small number <strong>of</strong> articles illustrates a<br />
need for further efforts to develop and disseminate evidenced-based approaches for recruiting<br />
social work students into careers in gerontology. A larger and more comprehensive review <strong>of</strong> the<br />
research literature for evidenced-based approaches is currently underway.
45<br />
Eve McClennen<br />
eveem@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, School <strong>of</strong> Social Work, Institute <strong>of</strong> Gerontology<br />
Social Work Perspectives on the Emory Alzheimer’s Disease Research Center<br />
The goal <strong>of</strong> the Emory Alzheimer’s Disease Research Center (ADRC) – one <strong>of</strong> 32 active centers<br />
in the nation supported by the National Institutes <strong>of</strong> <strong>Health</strong> – is “to bring scientists together to<br />
facilitate their research and help learn more about Alzheimer’s and related diseases [and also] to<br />
commit to the education <strong>of</strong> health care pr<strong>of</strong>essionals, persons with Alzheimer’s disease, their<br />
families, and our community to aid in understanding, diagnosis and treatment <strong>of</strong> these illnesses.”<br />
Perhaps almost as important as the psychoeducational groups and family sessions I undertook as<br />
a student intern – and not mentioned in the mission or ADRC website – was locating needed<br />
resources and forging key linkages to help people navigate the maze <strong>of</strong> dementia and learn how<br />
to best survive the present and plan for the future.<br />
By “shadowing” other social workers on the Wesley Woods campus, I gained a better<br />
understanding <strong>of</strong> social work roles and challenges. The social workers were interviewed about<br />
the need for geriatric social workers in settings similar to theirs; job satisfaction; and current and<br />
future challenges for social workers assisting geriatric patients and their families. The social<br />
workers interviewed are employed in the following areas: administration at Wesley Woods<br />
hospital, psychiatry (the Fuqua Center), the movement disorders unit, and the long-term acute<br />
care (LTAC).<br />
Conclusion: Social workers play an integral role in the work <strong>of</strong> interdisciplinary teams, bridging<br />
the gap between the overwhelming medical reality and tremendously difficult challenges<br />
involving quality <strong>of</strong> life, loss and death.
46<br />
Kishauna McDonald<br />
Lee Hyer, PhD<br />
Miranda Pratt, PhD<br />
Ciera V. Scott, MS<br />
kishauna.alexandra.mcdonald@live.mercer.edu<br />
Mercer <strong>University</strong>, Department <strong>of</strong> Psychology<br />
<strong>Georgia</strong> Neurosurgical Institute & Mercer <strong>University</strong> School <strong>of</strong> Medicine<br />
Mercer <strong>University</strong>, Clinical Mental <strong>Health</strong> Counseling Program & <strong>Georgia</strong> Neurosurgical Institute<br />
Pilot Data: The Relationships among Affect, Coping Behaviors, Personality, and Quality <strong>of</strong><br />
Life <strong>of</strong> Patients with Aneurysms<br />
Cerebral aneurysms, balloon-like bulges <strong>of</strong> cerebral arteries, are devastating problems in a<br />
person’s life. They <strong>of</strong>ten come without warning and can cause death or severe disabilities from a<br />
stroke. This can occur at all ages. Given the severe nature <strong>of</strong> aneurysms, patients struggle to<br />
come to terms with this malady. Neurosurgeons are constantly debating which <strong>of</strong> three treatment<br />
options are best for brain aneurysm patients. Importantly, little is known about the psychological<br />
variables that may influence QoL in brain aneurysm patients. Along with treatment factors, this<br />
study explores what additional variables that can predict outcomes in QoL. Study variables<br />
included background and medical variables, affect, coping, and personality, specifically<br />
conscientiousness. Brain aneurysm patients from a southeastern neurosurgical institute complete<br />
a questionnaire soon after learning about the aneurysm, with a follow-up period <strong>of</strong> 60 days,<br />
assessing anxiety and depression, coping behaviors, personality and quality <strong>of</strong> life.<br />
We present pilot data on ~20 subjects. T-tests, a 2x2 mixed model ANOVA, and a step-wise<br />
regression were/are being used to analyze the results. Preliminary data show that task oriented<br />
coping is a predictor <strong>of</strong> QoL, followed by degree <strong>of</strong> conscientiousness, and lastly anxiety and<br />
depression. Preliminary results suggest that style <strong>of</strong> coping provided important information that<br />
will help the neurosurgery team better able to address factors that may be contributing to the<br />
variability in QoL. Also, strategies and interventions that will help patients cope with and<br />
overcome their health problems are suggested. It is believed that this also may help influence<br />
patient satisfaction.
47<br />
Hyunjin Noh, MSW<br />
hyunjinnoh@wisc.edu<br />
<strong>University</strong> <strong>of</strong> Wisconsin-Madison, School <strong>of</strong> Social Work<br />
Terminally Ill Black Elders: Making the Choice to Receive Hospice Care<br />
The racial and ethnic inequality in receiving hospice care has been witnessed for decades in the<br />
United States. Researchers have explored the barriers to minorities’ accessing hospice care and<br />
their end-<strong>of</strong>-life healthcare preferences. Though knowledge from previous studies provides<br />
insight into why minority elders might not choose to use hospice care even when they have<br />
access to it, currently there appears to be no research that has explored why some minority elders<br />
do choose to receive such care. This study seeks to address this gap by interviewing terminally ill<br />
older minority hospice patients and gathering information regarding the following three research<br />
questions: why do terminally ill minority elders choose to use hospice care?; what structural<br />
barriers do they face when accessing hospice care, and how have they overcome them?; and what<br />
cultural preferences do they have in receiving hospice care and what is their experience in having<br />
their preferences respected? To gain such information, face-to-face interviews were conducted<br />
using a semi-structured survey with 31 older minority hospice patients in <strong>Georgia</strong>, the vast<br />
majority <strong>of</strong> whom were black. Participants’ responses were analyzed using the content analysis.<br />
Themes that emerged include the importance <strong>of</strong> open communication between healthcare<br />
providers and patients, the sources <strong>of</strong> correct/incorrect information, family support/non-support<br />
in choosing to use hospice care, the role <strong>of</strong> spirituality/religiosity in making the choice, and<br />
important values in receiving hospice care. The findings <strong>of</strong> this study will provide end-<strong>of</strong>-life<br />
care providers with insights for strategies to promote the hospice use by minority communities.
48<br />
Jonathan W. Rich<br />
Rodney L. Parks, Ph.D.<br />
jonrich@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, Office <strong>of</strong> the Registrar<br />
Back to School: Baby Boomers in the Classroom<br />
As members <strong>of</strong> the Baby Boom cohort begin to approach the age <strong>of</strong> retirement, they are<br />
increasingly returning to the classroom to pursue degrees for “encore careers.” Academic<br />
planners must pay careful attention to the specific concerns <strong>of</strong> Boomers to help ease their<br />
transition into a university setting after decades <strong>of</strong> absence. Following the tenets <strong>of</strong> qualitative<br />
phenomenology, this study aimed to understand the meaning <strong>of</strong> the experiences <strong>of</strong> seven students<br />
participating in a 62 and over reduced tuition program at a large, traditional Southeastern<br />
university. Two sets <strong>of</strong> semi-structured interviews were analyzed using open-coding and thick<br />
descriptions to identify major themes <strong>of</strong> participants’ experiences. Economic insecurity,<br />
preference for youthful college-town atmosphere, and commitment to lifelong learning were the<br />
principle motivations behind participants’ decision to return to school. Challenges relating to<br />
technology, generational differences, isolation from campus life, and interaction with traditional<br />
students were explored. A number <strong>of</strong> academic policy changes relating to admissions and<br />
registration are recommended to help institutions better serve the growing Baby Boomer<br />
population.
49<br />
Ruth Robbins<br />
Amy A. Overman, Ph.D.<br />
rrobbins2@elon.edu<br />
Psychology Department, Elon <strong>University</strong><br />
Neuroscience Program, Elon <strong>University</strong><br />
A Model Cognitive Training Intervention for Minority and Low SES Older Adults<br />
Integral to our culture is the belief that the mind and quality <strong>of</strong> life will deteriorate in adults as<br />
they age. However, recent research demonstrates that cognitive training and social interaction<br />
can help maintain or even improve older adults’ brain function and quality <strong>of</strong> life (Mahncke, et<br />
al., 2006; Carlson et al., 2009). This is particularly relevant to the growing elderly population in<br />
the United States and it is important to share this information about healthy aging with them.<br />
Unfortunately minority and lower socioeconomic status older adults are particularly underreached<br />
with regard to this type <strong>of</strong> information and are at higher risk for health problems<br />
(Paasche-Orlow et al., 2005). Therefore, through partnerships with community organizations, we<br />
implemented an innovative pilot 10-week cognitive training interventions with minority and/or<br />
lower socioeconomic status elderly adults. The interventions consisted <strong>of</strong> social interaction and<br />
cognitive training exercises that challenged attentional and memory functions for one hour each<br />
week over the span <strong>of</strong> 10 weeks. We measured participants’ (n=12) satisfaction with life and<br />
cognitive function with pre- and post-training neuropsychological assessments. Results showed a<br />
significant improvement on the Satisfaction with Life Scale ratings over the 10 week training<br />
period. This health intervention has the potential to improve quality <strong>of</strong> life and reduce disparities<br />
in cognitive health in old age.
50<br />
Navtej K. Sandhu<br />
Candace L. Kemp,Ph.D.<br />
Mary M. Ball, Ph.D.<br />
Molly M. Perkins, Ph.D.<br />
nsandhu1@student.gsu.edu<br />
<strong>Georgia</strong> State <strong>University</strong>, The Gerontology Institute<br />
Emory <strong>University</strong>, Division <strong>of</strong> Geriatric Medicine and Gerontology<br />
Co-resident Relationships in Assisted Living: Examining the Influence <strong>of</strong> Functional Status<br />
Social relationships can have considerable influence on physical and mental well-being,<br />
especially in later life when individuals are at greater risk <strong>of</strong> functional decline. A growing<br />
number <strong>of</strong> frail elders manage decline by relocating to assisted living (AL). AL research suggests<br />
that other residents are among the most available social contacts and that co-resident<br />
relationships can affect life satisfaction, quality <strong>of</strong> life, and well-being. Although functional<br />
status influences social relationships, research has yet to provide an in-depth understanding <strong>of</strong><br />
how cognitive and physical function affects co-resident relationships in AL. In this paper, we<br />
present an analysis <strong>of</strong> qualitative data collected over a one-year period through participant<br />
observation and formal and informal interviews with AL residents, administrators, and staff in<br />
two diverse settings and ask: 1) How does functional status influence co-resident relationships?;<br />
and 2) What factors shape its influence? Data suggest that hearing, speech, and cognitive<br />
impairment can be relationship barriers. However, more impaired residents’ need for help can<br />
promote contact and relationships with less impaired residents. Individual (e.g. relationship<br />
strategies, attitude) and facility (e.g., staff intervention) factors affect the influence functional<br />
status has on relationships. We conclude by discussing strategies for promoting more positive<br />
relationships among residents in AL.
51<br />
Elisabeth Lilian Pia Sattler, BSPharm<br />
Matthew Perri III, PhD, RPh<br />
Jung Sun Lee, PhD, RD<br />
lilian@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, <strong>College</strong> <strong>of</strong> Family and Consumer Sciences, Department <strong>of</strong> Foods and<br />
Nutrition<br />
Medication Adherence Measures derived from Administrative Pharmacy Claims Data in<br />
Older Americans: A Systematic Review<br />
Appropriate medication adherence is critical for the management <strong>of</strong> chronic conditions highly<br />
prevalent among older Americans. Administrative pharmacy claims data has gained importance<br />
to objectively derive medication adherence measures. Numerous measures have been developed,<br />
however little is known about the types <strong>of</strong> such measures used in older Americans. The objective<br />
<strong>of</strong> this study was to identify types <strong>of</strong> administrative pharmacy claims-derived medication<br />
adherence measures (APCAM) used in older Americans. A systematic search <strong>of</strong> the PUBMED<br />
database was conducted to identify studies using APCAM exclusively in older adults aged 60+<br />
years, and published in the U.S. between January 2000 and March 2011. Key search terms<br />
included twenty-nine currently available medication adherence measure names combined with<br />
other search criteria terms. Studies identified from the key word search were manually reviewed<br />
to select relevant articles. Nineteen studies were identified. They used APCAM based on two<br />
major concepts: medication availability and medication consistency. All studies used one<br />
medication availability concept-based measure (e.g. medication possession ratio). The majority<br />
<strong>of</strong> studies used a single medication availability measure (57.9%), and almost one third <strong>of</strong> studies<br />
used multiple measures based on both concepts. Not all APCAM based on the same concept used<br />
consistent names and algorithms. Even APCAM with the same name differed by various factors,<br />
including observation periods and number <strong>of</strong> medications considered. Although one concept <strong>of</strong><br />
medication adherence was predominantly used, there was no consistency among names and<br />
algorithms across different APCAM used in older Americans.
52<br />
Michael Schuier, BS<br />
Lee Hyer, PhD<br />
Ciera V. Scott, MS<br />
mschuier@me.com<br />
Mercer <strong>University</strong> School <strong>of</strong> Medicine, Marriage & Family Therapy Program<br />
<strong>Georgia</strong> Neurosurgical Institute & Mercer <strong>University</strong> School <strong>of</strong> Medicine<br />
Mercer <strong>University</strong>, Clinical Mental <strong>Health</strong> Counseling Program & <strong>Georgia</strong> Neurosurgical Institute<br />
Mini Mental Status Exam (MMSE): Differences due to Scoring for Older Adults with<br />
Memory Problems<br />
The Mini Mental Status Exam (MMSE) is a universally used mental status exam that has set a<br />
standard for briefly assessing mental capacities, especially for older adults. Although the exam<br />
<strong>of</strong>fers directions on the assessment, there are allowances for the examiner to <strong>of</strong>fer alternatives.<br />
Indeed, extant norms are based on differing instructions for the test administration. This study<br />
aims to view and assess the differences in patients who are given both tasks. We endeavor to<br />
determine the effects <strong>of</strong> educational level, gender, depression, physical functioning, and amount<br />
<strong>of</strong> medication prescribed on differences in scores on the Attention and Concentration subtests on<br />
the MMSE. The two options at issue are “Serial 7s” versus spelling the word “World” backwards.<br />
We do this in a group <strong>of</strong> patients who present for psychiatric problems, most commonly<br />
dementia. The sample included older adults (N=35) who were patients at the Family <strong>Health</strong><br />
Center <strong>of</strong> Central <strong>Georgia</strong> and the <strong>Georgia</strong> Neurosurgical Institute in Macon. A full cognitive<br />
assessment, including a MMSE, was given to all subjects. Preliminary results show that MMSE<br />
scores do differ in this age group with more patients successfully completing “World” than Serial<br />
7s. Many subjects actually would be categorized as demented on Serial 7’s and not so on<br />
“World.” Educational level was the highest predictor <strong>of</strong> variance, followed by living situation<br />
and level <strong>of</strong> mobility. Special consideration is given to the effect <strong>of</strong> depression on cognitive<br />
scores. We discuss the importance <strong>of</strong> consistency on the subtests on the MMSE.
53<br />
Chris Scoggins, BS<br />
Ciera V. Scott, MS<br />
Lee Hyer, PhD<br />
scoggins_chris@msn.com<br />
Mercer <strong>University</strong>, Master <strong>of</strong> <strong>Public</strong> <strong>Health</strong> Program<br />
Mercer <strong>University</strong>, Clinical Mental <strong>Health</strong> Counseling Program & <strong>Georgia</strong> Neurosurgical Institute<br />
<strong>Georgia</strong> Neurosurgical Institute & Mercer <strong>University</strong> School <strong>of</strong> Medicine<br />
The Millon Behavioral Medicine Diagnostic: Pr<strong>of</strong>iles <strong>of</strong> Dementia and Depression<br />
Dementia (or cognitive decline) either results in or causes changes in personality and treatment<br />
patterns as the person declines. From a sample <strong>of</strong> older adults with memory complaints who have<br />
varying problems <strong>of</strong> dementia, depression or both, we address two issues: (1) we provide a<br />
personality, stress moderator and treatment prognostic pr<strong>of</strong>ile <strong>of</strong> older adults with and without<br />
dementia; and (2) we consider the question <strong>of</strong> the added influence <strong>of</strong> depression related to these<br />
variables. For question 1, older subjects (N=112) were disaggregated by dementia and nondementia<br />
status; for question 2, the older adults (age>60; N=62) were further separated into those<br />
with a dementia, those who are depressed, and those with both dementia and depression. Patients<br />
were interviewed and self-report scales were given to all subjects. All patients had a caregiver.<br />
Cognitive and personality styles, treatment and stress markers, and Axis I variables, as well as<br />
background and adjustment, were measured. For dementia/non-dementia groups, results show<br />
that the dementia group was more detached, had more problems with depression and cognitive<br />
dysfunction, and showed less concerns about Informational Fragility. When the three groups<br />
were considered, the combined and dementia groups had the most problems, including more<br />
fixed personality features, more psychiatric problems, more stress moderators and more<br />
problematic treatment prognostics. We also show pr<strong>of</strong>iles <strong>of</strong> treatment prognostics and stress<br />
moderators <strong>of</strong> each personality type for a dementia, depression and dementia/depression. We<br />
highlight the importance <strong>of</strong> depression at later life either with or without a dementia.
54<br />
Ciera V. Scott, MS<br />
Lee Hyer, PhD<br />
ciera.v.scott@gmail.com<br />
Mercer <strong>University</strong>, Clinical Mental <strong>Health</strong> Counseling Program & <strong>Georgia</strong> Neurosurgical Institute<br />
<strong>Georgia</strong> Neurosurgical Institute & Mercer <strong>University</strong> School <strong>of</strong> Medicine<br />
Impact <strong>of</strong> Duloxetine in Perioperative Spine Patients: Pain, Depression, and Quality <strong>of</strong> Life<br />
<strong>of</strong> Injured Older Adults<br />
Since its inception in the early 2000s, Cymbalta (duloxetine Hcl) has been prescribed to treat<br />
Major Depressive Disorder (MDD), Generalized Anxiety Disorder (GAD), diabetic peripheral<br />
neuropathic pain, fibromyalgia, and most recently, chronic lower back pain. We assessed the<br />
utility <strong>of</strong> duloxetine in improving pain in back surgery patients sans clinical depression. Our<br />
subjects consisted <strong>of</strong> patients undergoing the following back surgeries at the <strong>Georgia</strong><br />
Neurosurgical Institute (GNI) in Macon, <strong>Georgia</strong>—lumbar micro discectomy, lumbar<br />
decompression and fusion, or anterior cervical decompression and fusion. Over 50% <strong>of</strong> our<br />
subjects were over the age <strong>of</strong> 55. The study followed a controlled, double-blind model with<br />
subjects randomized to either a duloxetine or placebo group. All study participants (N=98) were<br />
assessed for pain, physical functioning, adjustment, and mood markers using the following—the<br />
BPI-SF, BDI-II, CIBIC-Plus, SF-36, ADCS-ADL, SCL-90-R., Trails A and B, and Semantic<br />
Fluency and Digit Span from the RBANS. Subjects were assessed a total <strong>of</strong> three times—a week<br />
prior to surgery, four weeks post-surgery, and 12 weeks post-surgery. Presently, overall data<br />
supports Cymbalta as a pain management agent, especially in older adults (age>55). Patients in<br />
the drug group reported less pain and improved levels <strong>of</strong> functioning, emotional well-being, and<br />
quality <strong>of</strong> life in relation to their placebo counterparts. Older subjects reported significant levels<br />
<strong>of</strong> reduction in pain, opioid use, and depression/anxiety symptoms versus the younger group.<br />
Trends reinforce the positive effect <strong>of</strong> Cymbalta in postoperative spine patients. Further data<br />
(N=140) should allow for increased power for more refined results.
55<br />
Jennifer Shelton<br />
Lauren Brown<br />
Avani Shah, Ph. D.<br />
shelt013@crimson.ua.edu<br />
<strong>University</strong> <strong>of</strong> Alabama, School <strong>of</strong> Social Work<br />
Use <strong>of</strong> Self-Help Materials for Mood in Older Adults with Depressive Symptoms<br />
A large number <strong>of</strong> self-administered treatments and self-help materials are available for use and<br />
could serve as the first line <strong>of</strong> treatments in a stepped care treatment plan, particularly for the<br />
treatment <strong>of</strong> depressive symptoms. However, no recent studies have evaluated how common<br />
self-help use for depression is among older adults. This study evaluates the use <strong>of</strong> self-help<br />
materials for mood in community dwelling older adults and assesses if higher depression scores<br />
(Patient <strong>Health</strong> Questionnaire-9) are related to self-help usage. The sample consists <strong>of</strong> older<br />
adults (N = 100; M age = 73.23) who were recruited from senior nutrition centers and primary<br />
care clinics. Those age 55 or above with adequate self-reported reading ability were eligible to<br />
participate and were approached about participating in a 20 minute survey on depression<br />
screening. Participants completed counterbalanced self-administered survey packets, which<br />
included a depression screen, demographics form, and a yes/no question about their use <strong>of</strong> selfhelp<br />
materials for mood. To compensate for their time, participants were either entered into a<br />
drawing for $100 or provided $5 for participating. Older adults who had endorsed self-help<br />
usage for mood evidenced significantly higher scores on the PHQ-9 than those who did not<br />
(t(82) =-2.23;M =5.9 vs. M = 2.73). A table will be provided on the demographics characteristics<br />
<strong>of</strong> older adults who use self-administered mood materials.<br />
Conclusion: Older adults with more depressive symptoms seem to be more likely to seek the<br />
assistance <strong>of</strong> self-help materials to improve mood.
56<br />
Josh Skelton<br />
jskelt@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, <strong>College</strong> <strong>of</strong> <strong>Public</strong> <strong>Health</strong>, Department <strong>of</strong> <strong>Health</strong> Policy & Management<br />
Evaluation <strong>of</strong> the “We Honor Veterans” Program<br />
“We Honor Veterans” is a recent joint initiative by the National Hospice & Palliative Care<br />
Organization and Veterans Administration. The two organizations started this program in 2008<br />
to improve hospice care provided to veterans. A large portion <strong>of</strong> the older adult population is<br />
comprised <strong>of</strong> veterans and many <strong>of</strong> them suffer from illnesses that are different from non-veteran<br />
hospice patients. After receiving approval from the UGA Institutional Review Board for research<br />
with human subjects, I will be surveying the staff at a local hospice provider, who joined the<br />
program in 2011, to assess the effectiveness <strong>of</strong> the program thus far. I plan to analyze and<br />
evaluate the results and provide recommendations to the company on how to improve the care<br />
they provide to veterans and provide additional education if needed. The agency is also<br />
providing access to data from a patient survey and “military checklist,” as well as a family<br />
caregiver survey, with the names removed, which will provide me with information about<br />
demographics, diagnoses, and satisfaction with care. I will examine which health issues are most<br />
prevalent in this population. In addition, I plan to research the prevalence <strong>of</strong> health issues in<br />
veterans nationwide and compare them to non-veterans. This research will show the difference in<br />
prevalence rates and why additional training and education is needed when providing care to<br />
veteran hospice patients. Many veterans are unaware that the Veterans Administration covers<br />
hospice care, so it will also be important to inform veterans about their benefits.
57<br />
Elizabeth Sleeman<br />
Renu Kumar<br />
Aleta Johannaber<br />
Erin Fisher<br />
Ann Pearman, Ph.D.<br />
esleeman1@student.gsu.edu<br />
<strong>Georgia</strong> State <strong>University</strong>, Gerontology Institute<br />
Very Late Onset Schizophrenia-like Psychosis: A Review <strong>of</strong> the Literature<br />
Schizophrenia has long been thought <strong>of</strong> as a disease that has its onset solely in younger<br />
adulthood. However, very late onset schizophrenia-like disorder (VLOSP) is now recognized by<br />
the International Consensus on Late-Onset and Very-Late-Onset Schizophrenia Group. For a<br />
person to receive a diagnosis <strong>of</strong> VLOSP, the first psychotic incident has to occur after the age <strong>of</strong><br />
60. This presentation will focus on identifying the critical features <strong>of</strong> VLOSP that are important<br />
for clinicians, gerontologists, and others working with the elderly to recognize. While the<br />
symptoms <strong>of</strong> early onset schizophrenia and VLOSP are fairly similar. Patients with VLOSP<br />
<strong>of</strong>ten present with more hallucinations and delusions. This particular set <strong>of</strong> symptoms has<br />
significant overlap with the symptoms <strong>of</strong> several <strong>of</strong> the dementias, including Alzheimer’s disease,<br />
which makes differential diagnosis particularly challenging. However, it is critical to understand<br />
the differences in these diseases as the treatment strategies for dementia and VLOSP are quite<br />
dissimilar. Risk factors for VLOSP include social isolation, cognitive dysfunction, and sex<br />
(female). Persons with VLOSP are at particularly high risk for job loss and subsequent<br />
institutionalization if not given the proper treatment. Suggested treatments include very low dose<br />
atypical antipsychotics, supported employment rehabilitation, social and functional skills training,<br />
and other psychosocial therapies. Understanding the symptoms, risk factors, and treatments for<br />
schizophrenia with an onset in older adulthood is important for anyone working with older adults,<br />
particularly given the projected increase in mental health problems in the elderly in the next 20<br />
years.
58<br />
Chad R. Straight<br />
Christie L. Ward<br />
Bhibha M. Das<br />
Rudy J. Valentine<br />
John <strong>Georgia</strong>dis<br />
Ellen M. Evans<br />
chad1419@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, Department <strong>of</strong> Kinesiology<br />
Adiposity Impacts Physical Function More than Leg Lean Mass in Community-Dwelling<br />
Older Men and Women<br />
The interaction <strong>of</strong> body composition measures, strength and physical activity and the most<br />
salient outcome for lower-extremity physical function (LEPF) in older adults is an active area <strong>of</strong><br />
research due to the implications for physical disability. Therefore, to elucidate the relative<br />
importance <strong>of</strong> adiposity (%Fat), leg lean mass, muscle strength, muscle quality (MQ), and<br />
physical activity (PA) on LEPF, we assessed community-dwelling adults (n=231, 96 male;<br />
68.5±6.7 y) for body composition via dual energy X-ray absorptiometry, upper leg strength via<br />
isokinetic dynamometer (MVC), PA via pedometer, and LEPF via the timed up-and-go test<br />
(UPGO), 30-second chair stand test (CHR), and fast 7-m walk (WLK). MQ was calculated as<br />
MVC normalized for upper leg mineral-free lean mass (MFLM). No significant differences were<br />
observed between men and women in PA, MQ, or MFLM. As expected, men were 35% stronger<br />
than women (p
59<br />
Karlyn E. Vatthauer, B. S.<br />
Jason G. Craggs, Ph.D.<br />
Michael Marsiske, Ph.D.<br />
Joseph M. Dzierzewski, M. S.<br />
Christina S. McCrae, Ph. D.<br />
kvatthauer@phhp.ufl.edu<br />
<strong>University</strong> <strong>of</strong> Florida, Clinical and <strong>Health</strong> Psychology Department<br />
Increased Nightly Wake Time Predicts Increased Inconsistency in Executive Functioning<br />
Performance in Older Adults<br />
Complaints <strong>of</strong> reduced cognitive functioning are common among individuals with complaints <strong>of</strong><br />
insomnia. Such complaints appear to increase with age. However, the majority <strong>of</strong> sleep and<br />
cognitive functioning research is within younger adults populations. Previous studies <strong>of</strong> sleep<br />
and cognitive functioning in older adults have focused on typical cognitive functioning (using<br />
averages) and have ignored the (<strong>of</strong>ten considerable) amount <strong>of</strong> intraindividual variability in the<br />
data. Such an approach makes sense when the fluctuations observed represent noise or error.<br />
However, recent reports indicate that for cognitive functioning, intraindividual variability<br />
represents meaningful data as it is related to other important late life health concerns, including<br />
increased blood pressure and decreased positive affect. In some cases, studying intraindividual<br />
variability revealed unique relationships that were missed when the cognitive functioning data<br />
were averaged. The present study examined total wake time (TWT) and executive functioning<br />
(Symbol Digit Modalities Test, SDMT) variability in older adults. Sixty-four older adults<br />
(M=70.02 years, SD=7.59 years) were selected from the baseline screening for a study <strong>of</strong><br />
behavioral insomnia treatment. Participants completed sleep diaries and the SDMT for 14<br />
consecutive days upon waking. Multilevel modeling revealed that increased mean TWT<br />
predicted increased variability in SDMT scores (β=.018, t(64.76)=2.83, p=.006). These results<br />
suggest nightly wake time may negatively impact older adults’ executive functioning as<br />
increased nightly wake time predicted more inconsistent executive functioning performance.<br />
Future research investigating whether treatments (i.e., cognitive-behavioral treatment for<br />
insomnia) that decrease nightly wake times can also stabilize older adults’ executive functioning<br />
appears warranted.
60<br />
Latrice D. Vinson, M.A.<br />
Chao-Hui Huang, M.Ed.<br />
Ernest Wayde, M.A.<br />
Audrey Austin, MPH, M.A.<br />
Adriana Hyams, B.A.<br />
Susan Guin, MSN, CRNP<br />
Martha R. Crowther, Ph.D., MPH<br />
ldvinson@crimson.ua.edu<br />
<strong>University</strong> <strong>of</strong> Alabama, Department <strong>of</strong> Psychology<br />
Center for Mental <strong>Health</strong> & Aging<br />
<strong>University</strong> <strong>of</strong> Alabama , Department <strong>of</strong> Community and Rural Medicine<br />
Mobile <strong>Health</strong>care: An Interdisciplinary Approach to Provide Behavioral Care to Rural<br />
Elders<br />
The elderly population is increasing in rural communities, yet many rural elders have fewer<br />
resources and poorer mental and physical health than their urban counterparts. Rural elders are<br />
also at a higher risk for developing metabolic syndrome (MSX), a cluster <strong>of</strong> risk factors for<br />
cardiovascular disease, stroke, and mortality, which has been linked to depression and cognitive<br />
impairment. An interdisciplinary healthcare team provided behavioral and physical health<br />
screens to adults in four rural communities on a mobile health unit. The goal <strong>of</strong> the project was<br />
to support: a) community-based approaches directed to both enhance the training <strong>of</strong> scholars and<br />
contribute to the well-being <strong>of</strong> older, rural residents; b) interdisciplinary collaboration between<br />
Psychology, Rural Medicine, and Social Work; and c) the dissemination <strong>of</strong> promising practices<br />
in rural education and mental health promotion. A secondary data analysis assessed the risk<br />
factors for MSX among rural elders. The predominately African American sample included 384<br />
health screens <strong>of</strong> adults age 55 and older conducted on the mobile unit. The results <strong>of</strong> a two-way<br />
repeated measures ANOVA revealed significant differences in the average number <strong>of</strong> risk factors<br />
per site (Wilks’ Lamda = .75, F(3, 30) = 3.35, p = .03), suggesting there is an increased risk for<br />
MSX within rural communities where lower educational attainment, income, and socioeconomic<br />
status are more prevalent. Additionally, rural elders are at increased risk <strong>of</strong> developing MSX.<br />
Using innovative methods such as mobile healthcare delivery is crucial to providing quality<br />
healthcare and health education to an underserved population.
61<br />
Temitope Y. Walker<br />
Kathryn N. Porter<br />
Kristen L. Brown<br />
Jung Sun Lee<br />
Mary Ann Johnson<br />
taiyejorun@gmail.com<br />
The <strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, <strong>College</strong> <strong>of</strong> <strong>Public</strong> <strong>Health</strong>, Department <strong>of</strong> Foods and Nutrition<br />
Barriers to Food Stamp Participation among Older Adults<br />
The goal <strong>of</strong> this study is to identify potential barriers to the process <strong>of</strong> applying for the food<br />
stamp program that may hinder older adult participation among congregate meal participants.<br />
Therefore, a questionnaire was administered that included quantitative and qualitative measures<br />
to assess the barriers to food stamp participation. The questionnaire consisted <strong>of</strong> about 40<br />
questions administered in one session with older adults at senior centers in Northeast <strong>Georgia</strong>.<br />
The participants were categorized into 3 groups, those not interested in food stamps (n=58<br />
people), those who were currently using or had ever used food stamps (n=38 people), and those<br />
who wanted food stamps (n=14 people). This report examines the distinguishing characteristics<br />
<strong>of</strong> only those who wanted food stamps. Most, but not all, indicated they needed food stamps<br />
(79%) supporting other results that some manage to “get by” without food stamps (57%).<br />
Regarding applying, most did not know how to use the internet (79%) and half <strong>of</strong> the<br />
respondents could not complete a food stamp application online. Most respondents were not<br />
familiar with how to take medical deductions (86%) or determine household size (64%).<br />
Participants reported not knowing how to apply (50%), that the process required too much<br />
paperwork (35%), having no one to assist in the completion <strong>of</strong> the application (35%), and<br />
difficulty getting to the food stamp <strong>of</strong>fice (35%) as barriers. The results indicate that there are<br />
modifiable barriers that must be addressed to increase food stamp participation among eligible<br />
older adults.
62<br />
Natalya Watson<br />
Toni Miles, Ph.D.<br />
nwatson@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, <strong>College</strong> <strong>of</strong> <strong>Public</strong> <strong>Health</strong>, Institute <strong>of</strong> Gerontology<br />
Literature Review <strong>of</strong> Research on Interdependent <strong>Health</strong> and Collateral Effects <strong>of</strong> Mortality<br />
Issue: Individuals create social networks from the day they are born with those who surround<br />
them, and the interactions which happen within these networks effect the person’s wellbeing. For<br />
example, current research has demonstrated that when one loses a family member their health<br />
deteriorates, and these findings suggest that mortality is a risk. Therefore, we completed a<br />
literature search which investigated this concern. The results <strong>of</strong> the review suggest that death<br />
does influence the health <strong>of</strong> survivors. A study completed in Sweden demonstrated that<br />
following the death <strong>of</strong> a parent, adult children experience increasing risk <strong>of</strong> death during the ten<br />
years after the event. Furthermore, studies have shown that children who experience the death <strong>of</strong><br />
a parent have a greater risk for disease and illness. In addition, other studies have found that the<br />
death <strong>of</strong> a spouse also increases the risk <strong>of</strong> mortality in the surviving partner.<br />
Conclusion: There is a small but compelling body <strong>of</strong> research that documents the collateral<br />
effects <strong>of</strong> parental and spouse mortality on the health and well-being <strong>of</strong> surviving children and<br />
spouses.<br />
Next steps: In an aging society, many families experience the loss <strong>of</strong> an older relative each year.<br />
We are working to measure the public health impact <strong>of</strong> those deaths on the health <strong>of</strong> survivors.<br />
Our next steps are focused on measuring the extent <strong>of</strong> these collateral effects.
63<br />
Didier Wayoro<br />
dwayoro@brandeis.edu<br />
Brandeis <strong>University</strong>, Heller School for Social Policy and Management<br />
How Happy are You when You get Older? Evidence from South Africa<br />
In this study, we examined the determinants <strong>of</strong> happiness as people age in South Africa. Using<br />
the second wave <strong>of</strong> WHO Sage Data set (2007-2010) and an ordered logistic model we found a<br />
positive association between happiness (Subjective Well -Being) and income, health status and<br />
marriage. Moreover, our study revealed a hyperbolic relationship between happiness and age<br />
whereby happiness declines until it reaches a minimum around 44 years <strong>of</strong> age and increases to a<br />
maximum at around 78 years <strong>of</strong> age before declining again. Such heterogeneous age effects on<br />
happiness have important policy implications in terms <strong>of</strong> inequalities, welfare programs such as<br />
social security, health care expenditures and trade<strong>of</strong>f when it comes to the allocation <strong>of</strong><br />
government resources among different age groups in South Africa.
64<br />
Elizabeth Wilson<br />
lserieux@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, <strong>College</strong> <strong>of</strong> <strong>Public</strong> <strong>Health</strong>, Institute <strong>of</strong> Gerontology<br />
Attitudes about Aging among <strong>Health</strong>care Providers in Saint Lucia<br />
The issue addressed is that <strong>of</strong> aging in the developing country <strong>of</strong> Saint Lucia. According to the<br />
latest National Census figures, Saint Lucia’s population is approximately 161,557. The<br />
breakdown according to age is: 0-14 years: 22.8%, 15 – 64 years: 67.5%, 65 years and over:<br />
9.7%. The average life expectancy is 76.84 years and the growth rate is 0.389%. These figures<br />
clearly indicate that Saint Lucia will confront an increasingly older population and so the island<br />
needs to prepare for this phenomenon. This study specifically investigates attitudes about aging<br />
among health care providers in the north <strong>of</strong> the island. The information was gathered using a<br />
survey questionnaire. The questionnaires were given to healthcare providers in the island’s main<br />
public hospital, the island’s only private hospital, and two larger private clinics in the north <strong>of</strong><br />
the island. The questionnaires were completed anonymously and then returned to a collection<br />
box placed in each <strong>of</strong> the locations. The questionnaires were subsequently collected and the data<br />
therein reviewed. In addition to close ended questions, the questionnaires contained open ended<br />
questions to ascertain the level <strong>of</strong> training in the area <strong>of</strong> gerontology that exists among those<br />
health care providers. I also sought to ascertain the perceived need for training in this area. The<br />
response rate was 56% (n= 24). The findings were very consistent and indicated that the issue <strong>of</strong><br />
aging has not been given sufficient importance. The majority <strong>of</strong> the respondents had not received<br />
any training in this area, and the perceived need for such training was high. The study and poster<br />
present the existing situation in Saint Lucia, regarding attitudes to aging among healthcare<br />
providers. It will also use the responses <strong>of</strong> the interviewees to present ways in which the situation<br />
can be adequately addressed.
65<br />
Jun Yin<br />
Alan Mobley<br />
Francesca Iannaccone<br />
Jamie Samuels<br />
sly1314@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, Department <strong>of</strong> <strong>Health</strong> Promotion and Behavior<br />
Denny Tower Community Assessment and Rewards Program<br />
Applying the knowledge <strong>of</strong> the Community Based Participatory Research (CBPR) to conduct a<br />
needs assessment and developed an incentive program for the residents <strong>of</strong> Denney Tower (DT)<br />
in Athens, <strong>Georgia</strong>. It is a home to low-income older adults, many <strong>of</strong> whom have chronic<br />
diseases. By speaking with the residents on a number <strong>of</strong> different occasions we learned that lack<br />
<strong>of</strong> participation in events was a concern to the community. In order to work successfully with the<br />
community, a long-term partnership was built with the residents. We gained their trust by<br />
attending resident meetings and focus groups. We realized that material incentives might play an<br />
important role in getting residents involved in the project. Foods were served during each<br />
meeting. We expressed the necessity to have a collaborative project that would empower them to<br />
address the lack <strong>of</strong> participation in the community. In addition, we sought the residents’ feedback<br />
at all points during the process. Due to the fact that this is an ongoing project, no final conclusion<br />
has been made. However, we believe these activities provide instrumental and emotional types <strong>of</strong><br />
social support. In addition, an increased participation will lead to a greater sense <strong>of</strong> community at<br />
DT. Resident leaders were involved in the development <strong>of</strong> the program and will be the ones to<br />
carry out and maintain the program.
66<br />
Lin Yi-Yin<br />
yiyin@uga.edu<br />
<strong>University</strong> <strong>of</strong> <strong>Georgia</strong>, Adult education<br />
Intrinsic Motivations in Older Adult Learners: Taiwan Context<br />
Aging is expected to accelerate in Taiwan at a faster rate than any other country globally<br />
(Council for Economic Planning and Development, 2011). The Taiwan government in<br />
responding to this trend issued a white paper entitled, Toward an Aged Society: Policies on<br />
Education for Older Adults (Taiwan Ministry <strong>of</strong> Education, 2006) to widely promote learning<br />
activities for older adults. With the exploding grey population, there is a need to focus research<br />
on older adult learners. The purpose <strong>of</strong> this research was to investigate the motivations <strong>of</strong> older<br />
learners in Taiwan from the view point <strong>of</strong> intrinsic motivation with survey method. In total, 816<br />
Taiwanese older adults were investigated. The findings <strong>of</strong> this study are: (1) The intrinsic<br />
motivations <strong>of</strong> older adult learners are high; the most salient motivations for older adult learners<br />
were the desire for stimulation and generativity. (2) Institutional predictor variables are the most<br />
important predictors <strong>of</strong> intrinsic motivation <strong>of</strong> older adult learners. (3) Teacher support and peer<br />
support significantly enhance the intrinsic motivations <strong>of</strong> older adult learners.
67<br />
Karolina Zakoscielna, M.A.<br />
Patricia A. Parmelee , Ph.D.<br />
kzakoscielna@crimson.ua.edu<br />
<strong>University</strong> <strong>of</strong> Alabama, Department <strong>of</strong> Psychology and Center for Mental <strong>Health</strong> and Aging<br />
Pain Variability and its Predictors: Depression, Affect, Cognition, Functionality, and <strong>Health</strong><br />
A strong correlation has been found between pain and variables such as depression, affect,<br />
cognition, functionality, and health. Pain variability, however, has neither been concisely studied,<br />
nor has its relationship with the previously mentioned variables. The purpose <strong>of</strong> this secondary<br />
data analysis is to determine whether depression, affect, cognition, functional status, and health<br />
are predictors <strong>of</strong> day-to-day pain variability in older adults in long-term care settings. Drawn<br />
from the Philadelphia Geriatric Center database, 56 adults aged 68 years and older were included<br />
in the multiple linear regression analyses. Pain variability was measured over 30 days <strong>of</strong> selfreported<br />
pain levels. The Geriatric Depression Scale (GDS), Philadelphia Geriatric Center<br />
Positive and Negative Affect Rating Scale, Memory-Information-Concentration test, Physical<br />
Self-Maintenance Scale (PSMS), and perceived health were used as predictors. Results show a<br />
significantly positive association between total GDS score and pain variability (p
68<br />
Roberto B. Zamora<br />
Kenneth L. Lichstein<br />
Daniel J. Taylor<br />
Brant W. Riedel<br />
Andrew J. Bush<br />
rbzamora@crimson.ua.edu<br />
<strong>University</strong> <strong>of</strong> Alabama<br />
<strong>University</strong> <strong>of</strong> North Texas<br />
<strong>University</strong> <strong>of</strong> Memphis<br />
<strong>University</strong> <strong>of</strong> Tennessee, Memphis<br />
Consistency <strong>of</strong> Older Adults’ Sleep Diaries over Two Weeks<br />
Sleep diaries are used as an assessment procedure for insomnia research; however, sleep diaries<br />
may be used as a form <strong>of</strong> self-monitoring. The present study attempts to examine week<br />
differences in 2 weeks <strong>of</strong> sleep diaries in older adults (65+) with and without chronic insomnia to<br />
determine if the task <strong>of</strong> completing sleep diaries alters sleep efficiency (SE). 246 older adults,<br />
collected in a normative epidemiological study, were enrolled using random-digit dialing.<br />
Participant’s SE was collected for 14 days via 2 weeks <strong>of</strong> sleep diaries. A two–way mixed<br />
ANOVA was performed to analyze SE week differences between individuals with insomnia and<br />
normal sleepers. The mean SE for week 2 (M = 83.28) was significantly higher than week1 (M =<br />
82.43), F (1, 244) = 4.32, p = .04, ƞ 2 = .02. The mean SE <strong>of</strong> those with insomnia (M = 77.38) was<br />
significantly lower than those without insomnia (M = 88.33), F (1, 244) = 99.58, p < .001, ƞ 2<br />
= .29. A significant interaction between week difference and insomnia condition found that<br />
individuals with insomnia had an increase in mean SE from week 1 (M = 76.201) to week 2<br />
(78.55), whereas those who did not have insomnia had a decrease from week1 (M = 88.67) to<br />
week 2 (87.99), F (1, 244) = 13.96, p < .001, ƞ 2 = .05. The presence <strong>of</strong> sleep difference between<br />
the 2 weeks suggests that the task <strong>of</strong> completing sleep diaries can alter SE in older adults,<br />
especially for individuals with insomnia; however the effect is small. Future directions will<br />
examine the issue in a multi-level approach to optimally capture day to day variability.<br />
Research supported by National Institute on Aging grants AG12136 and AG14738
2012 Pictures<br />
70