

Diabetes in pregnancy: are we providing the best care ... - HQIP
Diabetes in pregnancy: are we providing the best care ... - HQIP
Diabetes in pregnancy: are we providing the best care ... - HQIP

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
A comparison of type 1 and type 2 diabetes<br />
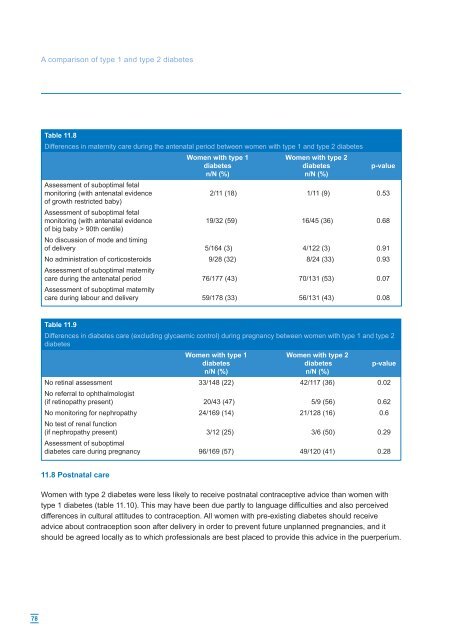
Table 11.8<br />
Differences <strong>in</strong> maternity c<strong>are</strong> dur<strong>in</strong>g <strong>the</strong> antenatal period bet<strong>we</strong>en women with type 1 and type 2 diabetes<br />
Women with type 1<br />
diabetes<br />
n/N (%)<br />
Women with type 2<br />
diabetes<br />
n/N (%)<br />
p-value<br />
Assessment of suboptimal fetal<br />
monitor<strong>in</strong>g (with antenatal evidence<br />
2/11 (18) 1/11 (9) 0.53<br />
of growth restricted baby)<br />
Assessment of suboptimal fetal<br />
monitor<strong>in</strong>g (with antenatal evidence<br />
19/32 (59) 16/45 (36) 0.68<br />
of big baby > 90th centile)<br />
No discussion of mode and tim<strong>in</strong>g<br />
of delivery 5/164 (3) 4/122 (3) 0.91<br />
No adm<strong>in</strong>istration of corticosteroids 9/28 (32) 8/24 (33) 0.93<br />
Assessment of suboptimal maternity<br />
c<strong>are</strong> dur<strong>in</strong>g <strong>the</strong> antenatal period 76/177 (43) 70/131 (53) 0.07<br />
Assessment of suboptimal maternity<br />
c<strong>are</strong> dur<strong>in</strong>g labour and delivery 59/178 (33) 56/131 (43) 0.08<br />
Table 11.9<br />
Differences <strong>in</strong> diabetes c<strong>are</strong> (exclud<strong>in</strong>g glycaemic control) dur<strong>in</strong>g <strong>pregnancy</strong> bet<strong>we</strong>en women with type 1 and type 2<br />
diabetes<br />
Women with type 1<br />
diabetes<br />
n/N (%)<br />
Women with type 2<br />
diabetes<br />
n/N (%)<br />
p-value<br />
No ret<strong>in</strong>al assessment 33/148 (22) 42/117 (36) 0.02<br />
No referral to ophthalmologist<br />
(if ret<strong>in</strong>opathy present) 20/43 (47) 5/9 (56) 0.62<br />
No monitor<strong>in</strong>g for nephropathy 24/169 (14) 21/128 (16) 0.6<br />
No test of renal function<br />
(if nephropathy present) 3/12 (25) 3/6 (50) 0.29<br />
Assessment of suboptimal<br />
diabetes c<strong>are</strong> dur<strong>in</strong>g <strong>pregnancy</strong> 96/169 (57) 49/120 (41) 0.28<br />
11.8 Postnatal c<strong>are</strong><br />
Women with type 2 diabetes <strong>we</strong>re less likely to receive postnatal contraceptive advice than women with<br />
type 1 diabetes (table 11.10). This may have been due partly to language diffi culties and also perceived<br />
differences <strong>in</strong> cultural attitudes to contraception. All women with pre-exist<strong>in</strong>g diabetes should receive<br />
advice about contraception soon after delivery <strong>in</strong> order to prevent future unplanned pregnancies, and it<br />
should be agreed locally as to which professionals <strong>are</strong> <strong>best</strong> placed to provide this advice <strong>in</strong> <strong>the</strong> puerperium.<br />
78














