Child Drowning
Child Drowning
Child Drowning

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
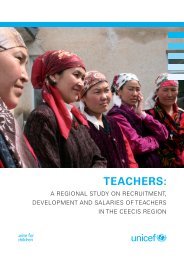
Figure 19: Resuscitation received by drowning children (aged 0-17 years)<br />
100%<br />
80%<br />
Trained resuscitation Traditional resuscitation No resuscitation Unknown<br />
60%<br />
40%<br />
20%<br />
0%<br />
Bangladesh Jiangxi, China Cambodia<br />
Source: Survey data from the countries included: Bangladesh Health and Injury Survey 2003, Cambodia Accident and Injury<br />
Survey 2006 and Jiangxi (China) Injury Survey 2005.<br />
On average, less than 10 per cent of drowning victims received resuscitation from a trained responder.<br />
This reflects both the lack of widespread resuscitation skills in the population and the fact that most<br />
drowning occurred in settings where resuscitation was not possible. The majority of drowning occurred<br />
among very young children who escaped supervision and drowned. Their caretakers were unaware of<br />
the drowning for lengthy periods of time and resuscitation was not an option. The majority of the<br />
drowning incidents among older children occurred when they were alone, or with a peer that lacked<br />
swimming, rescue or resuscitation skills.<br />
For every country studied, when traditional resuscitation was given, the methods used were ineffective<br />
and harmful, and may have contributed to the drowning fatality. These methods generally fell into three<br />
categories:<br />
1. Attempts to expel water from the drowned child’s body by physical force (e.g. whirling the child<br />
overhead, pressing or jumping on the child’s chest and stomach).<br />
2. Attempts to expel water from the drowning child by inciting vomiting or coughing (e.g. forcing<br />
rotten food or other noxious substances into the child’s mouth to induce vomiting, or inserting<br />
sticks or other objects into the child’s trachea to induce coughing), and:<br />
3. Attempts to expel water from the drowned child’s body through physical means that involved<br />
drying (e.g. covering the child in ashes or in mud, heating the child’s body over a warm fire).<br />
These practices were found across the different cultures in the surveys. They were widely cited by<br />
respondents, regardless of level of educational attainment or rural or urban location. As such, they<br />
represent broad social norms in response practices to drowning in children. To be effective, drowning<br />
interventions will need to take into account the deeply embedded nature of these behaviours and to<br />
design appropriate strategies to counteract them.<br />
The lessons learned from combating diarrhoeal diseases may be useful in this regard. Many of the early<br />
interventions focused on stopping deeply ingrained harmful behaviours, such as ceasing breastfeeding<br />
when the child had diarrhoea, or feeding the child solids in an attempt to decrease the diarrhoea.<br />
Changing these pervasive behaviours required extensive and long-term behavioural change<br />
interventions. Given the rural concentration and generally low educational attainment of mothers,<br />
45