Proton Beam Therapy - Outline Business Case (OBC) - Volume 2
Proton Beam Therapy - Outline Business Case (OBC) - Volume 2
Proton Beam Therapy - Outline Business Case (OBC) - Volume 2

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
UniversityCollegeLondonHospitals<br />
<br />
<strong>Proton</strong><strong>Beam</strong><strong>Therapy</strong><br />
<strong>Outline</strong><strong>Business</strong><strong>Case</strong><br />
<br />
<strong>Volume</strong>2of4:Appendices<br />
<br />
<br />
COMMERCIALINCONFIDENCE<br />
Version2 31 st May2013
Contents:<br />
APPENDIX 1A CIB AND MONITOR CHECKLIST........................................................... 3<br />
APPENDIX 2A: OVERVIEW OF PROTON BEAM THERAPY ........................................ 4<br />
APPENDIX 2B: UCLH SERVICE STRATEGY............................................................... 16<br />
APPENDIX 2C: EQUALITY IMPACT ASSESSMENT ................................................... 19<br />
APPENDIX 2D PROJECT RISK REGISTER ................................................................. 21<br />
APPENDIX 3A: UCLH AND THE CHRISTIE PBT THROUGHPUT MODELLING ........ 28<br />
APPENDIX 3B: PBT QUALITATIVE BENEFITS ANALYSIS........................................ 30<br />
APPENDIX 3C: ECONOMIC ASSESSMENT WITH QALY ANALYSIS ........................ 31<br />
APPENDIX 3D: BENEFITS REGISTER......................................................................... 36<br />
APPENDIX 3E: FINANCIAL APPRAISAL ..................................................................... 38<br />
APPENDIX 4A PROPOSED TARIFF ARRANGEMENTS ............................................. 68<br />
APPENDIX 4B: EQUIPMENT PROCUREMENT STRATEGY....................................... 71<br />
APPENDIX 4C: CONSTRUCTION PROCUREMENT STRATEGY ............................. 115<br />
APPENDIX 4D: CABINET OFFICE ICT SPEND CONTROL FORM (V2.18) .............. 127<br />
APPENDIX 4E: PBT MILESTONE TRACKER ............................................................ 134<br />
APPENDIX 6A: PROJECT RESOURCING SCHEDULE............................................. 135<br />
APPENDIX 6B: STAKEHOLDER MANAGEMENT PLAN........................................... 136<br />
APPENDIX 6C: LETTERS OF COMMISSIONER AND STAKEHOLDER SUPPORT. 141<br />
APPENDIX 6D: CONTINGENCY IN THE EVENT OF ACCELERATOR / PBT CENTRE<br />
FAILURE....................................................................................................................... 154<br />
APPENDIX 6E: RISK POTENTIAL ASSESSMENT ................................................- 156 -<br />
<br />
<br />
<br />
Page2
Appendix2A:Overviewof<strong>Proton</strong><strong>Beam</strong><strong>Therapy</strong><br />
DepartmentofHealth’soverseasprogramme<br />
1.1. Overall250patientshavebeenreferredintotheDH’soverseasprogrammesinceitsstarted<br />
in2008and160patientshavebeenreferredforprotontreatmentabroadincludingnearly<br />
100paediatriccases.50patientstravelledoverseasfortreatmentin2010/11atacostof<br />
£5m. For 2011/12, in the first 7 months, 42 patients from England had begun treatment<br />
overseas. The panel is currently carefully managing the programme, recognising that the<br />
overseascapacitytotreatpatientsislimited.Itwasplannedthat120patientswouldreceive<br />
treatment overseas in 2011/12 at a cost of £9m; however, the programme is currently<br />
estimating80patientsasUScostshaveincreasedtakingtheaveragecostthisyearto£110k<br />
perpatient(anincreaseontheplanningfigure).Forthesereasons(capacityandcost),the<br />
expert reference panel is being deliberately cautious in the cases it sends overseas for<br />
treatment.InOctober2010,thegovernmentannouncedanadditionalfundingoverthenext<br />
Spending Review period so that all high priority patients have access to this treatment<br />
benefitting400patientsperyearbytheendoftheSpendingReviewperiod.Estimatedspend<br />
onoverseasPBTtreatmentby2014/15is£30mperannum<br />
<br />
1.2. In 2011/12, the average cost per patient sent overseas is currently around £90k with the<br />
majoritybeingtreatedattheJacksonvillecentreinFlorida.CapacitytodeliverPBTfornon<br />
eyecancersinEuropeisstillverylimited.Difficultiesinintegratingothertreatmentsandthe<br />
quality of patient experience have led to France not being used currently 1 . There is a<br />
recognised need to increase capacity in Europe and existing services are under increasing<br />
pressuretotreattheirowncases<br />
<br />
Marketanalysis<br />
1.3. The only proton facility in the UK is a low energy facility at the Clatterbridge Centre for<br />
Oncology,Liverpool;thisissuitableforeyetumoursonly.Ittreatsaround100patientsayear<br />
with excellent outcomes and over 90% permanent control (effective local cure and saves<br />
enucleatingtheeye).<br />
<br />
1.4. Fromourmarketintelligence,therearecurrentlysixmanufacturersofferingPBTequipment<br />
solutions with only a few centres in operation or in development around the world. This<br />
implies that in general manufacturers have relatively sparse experience of equipping and<br />
installingcurrentoperationalcentres,butalsothatthetechnologyprocuredwillberelatively<br />
untestedinaclinicalenvironment.<br />
•<br />
<br />
• <br />
• <br />
• <br />
• <br />
<br />
1 OrsayisastandalonePhysicsresearchlabandtherewererestrictionsonthebeamusefor<br />
treatment. The lack of a clinical setting and language barriers also impacted on patient<br />
experience<br />
<br />
<br />
<br />
Page4
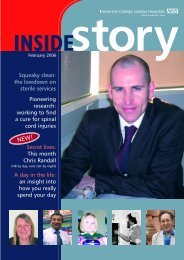
Fig.1LocationofhighenergyPBTfacilities<br />
Page7
PBTsystemsinothercountries<br />
1.6. Discussionswiththeprivatehealthcaremarketinthe haveestablishedthat<br />
thereislittleappetiteforcapitalinvestmentinaPBTfacilityorwillingnessonthepart<br />
of private healthcare insurers to pay for treatment. Private patients in the UK would<br />
thereforebeselffunders<br />
<br />
1.7. OtherEuropeanhealthsystemswhichhavesystemsofevaluatingthecosteffectiveness<br />
orrationingofcarehavedevelopedindicationlists.<br />
<br />
1.8. Facilities are currently under construction or planned in Austria, the Netherlands,<br />
Sweden,Germany,Italy,PolandandFrance.<br />
<br />
ManagingPBTTechnologyRisk<br />
PBT involves a highly technical solution with cutting edge technology that leads to complex<br />
design solutions. PBT remains a relatively novel healthcare treatment with only a handful of<br />
clinicalcentresintheworldandrelativelyfewmanufactures.Whenaddedtothehighcostofthe<br />
equipment and design and build costs, this emphasises the importance of getting the<br />
procurementoftheequipmentright.<br />
<br />
Wehaveapproachedtheissueoftechnologyselectioninsomedepth.Ourfocusthroughoutour<br />
wholeinvolvementwithPBThasbeenonbeingfullypreparedtoprovidetheserviceassoonas<br />
the Department of Health sees fit.This clearly involves not just thinking conceptually about<br />
issuessuchastechnologyselectionandfinancing,butformallyprogressingdifferentoptionsand<br />
reachingsomefirmconclusionsandpreferences.<br />
<br />
WiththerelativeimmaturityofthePBTmarket,andthelongleadintimefromprocurementtoa<br />
facilitybeingoperational,thechosentechnologysolutionisunlikelytohavebeenoperationalin<br />
manycentresifatall.Asaresult,wehaveputaparticularemphasisontechnologyselection.<br />
Unlikeinotherclinicalareas,technologyselectioninformsboththecapabilityofacentretotreat<br />
its patients, but also the process of testing the feasibility of a PBT centre fitting onto an<br />
organisation’sdesiredsite.Therearealsokeydecisionstomakeaboutemergingtechnologies<br />
andmodalities.<br />
<br />
Ourprocess,whichisoutlinedbelow,hasbeento:<br />
<br />
• Analysethebasicspecificationofrequiredfacility(i.e.numberoftreatmentandresearch<br />
rooms;highlevelspecificationofinroomequipment)<br />
• Analysetheoptimumtechnicalspecificationofasystemindetail<br />
• Submit our requirements to vendors and on the basis of their responses assess our<br />
‘preferredvendors’<br />
• BegindesigningaPBTfacility(upto1:200stage)onourchosensiteonthebasisofour<br />
‘preferredvendors’<br />
<br />
<strong>Proton</strong><strong>Beam</strong><strong>Therapy</strong>overview<br />
<br />
ThesetupofaPBTcentrehassimilaritiestoastandardphotonRadiotherapyfacility.However,<br />
thecurrentsolutionsinthemarketprimarilyofferseparateequipmentfortheacceleratorand<br />
<br />
<br />
<br />
Page8
treatmentroomwithbothoftheseatconsiderablesizeandcost.AlongsidethePBTequipment,<br />
aPBTfacilitywouldalsorequireimagingequipmentandsoftwareintheformofRadiotherapy<br />
Management Systems (including Treatment Planning Systems). Although both of these are<br />
standardforaRadiotherapyfacility,duetotherelativenoveltyofPBT,therearecurrentlyfew<br />
solutionsinthemarket.<br />
<br />
Marketanalysisontechnologyobsolescence<br />
<br />
UCLHhastheopportunitytobecomeoneoftherelativelyfewPBTfacilitiesaroundtheworld.As<br />
would be expected in a relatively immature, hightechnology market, we also have the<br />
opportunitytoinstalltechnologyatahigherspecificationthaninanyothercentreintheworld.<br />
But due to the long leadin time from procurement to an operational facility, the technical<br />
solution will be a balance between what is tested and can be delivered, and what will limit<br />
obsolescence risk. There are three scenarios that need to be considered on technological<br />
obsolescence.<br />
<br />
• Due to microlevel developments in PBT systems, the system we procure becomes<br />
outdated and does not represent the highest clinical quality system for UK patients.<br />
Thiswouldresultinpatients,orcommissioners,choosingothercentresoverUCLH<br />
• PBT is superseded by technological developments – either within the field of<br />
radiotherapy(i.e.heavyiontherapy),orbya“silverbullet”cureforcancer.Thiswould<br />
resultinalossofpatients,income,andtheviabilityofthewholeservice.<br />
• RefinementsintechnologyleadtoPBTbeingdeliveredinsmallerandcheaperways.<br />
Thiswouldresultinmorecentresenteringthemarket,andresultantpressureonboth<br />
ourpatientnumbersandperpatientincome.<br />
<br />
Wehaveanalysedallthreescenariosonthebasisof:<br />
<br />
• Theimpactoftherisk<br />
• Thelikelihoodoftheriskoccurring<br />
• Actionswecantaketomitigateagainsttherisk<br />
ThePBTsystemweprocurebecomesoutdated<br />
<br />
PBT technology is constantly developing. It is therefore imperative to ensure any system<br />
purchasedwillbecapableoftreatingpatientsnotjustinthenext35years,butinthenext1020<br />
and beyond.The impact of procuring an inadequate system would be severe.Competitors<br />
wouldbeabletosupplyaclinicallysuperiorsystem,andwe wouldlosepatientsandincome.<br />
Systemsaredevelopingrapidly,andthereareseveralsignificantinnovationsonthehorizonthat<br />
onedayallPBTcentreswillprovide(e.g.spotscanning).Thisriskcouldbemilitatedagainstby<br />
procuringasystemwhichmatchesthefollowingbroadspecifications.Thiswouldensurethatthe<br />
currentlyavailableequipmentwillnotbeobsoletein1015yearstime.<br />
<br />
• Sufficientpenetrationtotreatanywhereinthebody<br />
• Reliability–uptimebetterthan97%<br />
• Workload–sufficientcapacityforanticipateddemand<br />
• VersatilitySpotscanningandIMPT<br />
• Excellentimmobilizationandpositioning<br />
• Flexiblebeamentryoptions<br />
• Shortbeamontimeperfield<br />
• Fastchangefromonefieldtothenext<br />
<br />
<br />
<br />
Page9
• Fastchangefromonepatienttothenext<br />
• Lowneutroncontamination(importantespeciallyforchildren)<br />
• AvailabilityofaresearchroomforRadiobiologyandPhysics<br />
• StateoftheartInRoomImagingforpositionandtreatmentverification<br />
<br />
To further mitigate against obsolescence, current research and development requires the<br />
followingadditionalspecifications:<br />
<br />
• Sufficientpenetrationforprotonradiography<br />
• InroomInvivodosimetry<br />
• Abilitytoretrofitorreplaceequipmentwithnewerdevelopments<br />
<br />
TechnicalDevelopmentsduringlifetimeoffacility.<br />
<br />
Thetendershallincludetherequirementofaservicecontractthatguaranteestheavailability<br />
and implementation of all future hardware and software upgrades over the lifetime of the<br />
equipment.Replieswillneedtoincludespecificationsofthebuildingandlayoutrequirementsto<br />
ensurehardwarecanberetrofittedwhennecessary.<br />
<br />
In addition, and in parallel, research and development projects undertaken jointly with UCL<br />
Academic Departments will ensure that the capabilities of the proton therapy system and its<br />
associatedimagingandplanningtoolswillkeepabreastofthestateoftheartintheirfields.<br />
<br />
PBTissuperseded<br />
<br />
Bya“silverbullet”cureforcancer<br />
<br />
ThispossibilitywasalsoanalysedwithinthePhase3FinalInvestment<strong>Case</strong>, 2 andthescientific<br />
andclinicalbackdroptothediscussionremainsverymuchunchanged.Whilsttherearemany<br />
new modalities in development (such as gene therapy, immunological therapy, photodynamic<br />
therapy etc), none of these represent a cure for cancer.A reduction in demand for cancer<br />
treatmentisthereforehighlyunlikelyinthenearfuture.<br />
<br />
Byheavyiontherapy<br />
<br />
TheonlyformofradiotherapywhichcouldbeprovensuperiortoPBTisheavyiontherapy.It<br />
usesthesametechnologyasPBT,butonalargerscaletoaccelerateheavierparticles,suchas<br />
Helium and Carbon. They have similar physical deposition patterns, but different biological<br />
properties, which may prove advantageous for certain tumours. Further research needs to be<br />
undertaken to prove these advantages, as only three active facilities currently exist – two in<br />
JapanandoneinGermany.ThereareafewmoreinplanninginEuropeandAsia,butnonein<br />
planningintheUS. 3 <br />
<br />
TheimpacttoUCLHwouldbelow.Ifheavyionsareclinicallyprovenandsuchafacilityislocated<br />
nearLondon,therewouldcertainlybeareductionintheflowofPBTeligiblepatientstoUCLH.It<br />
isestimated,however,thatonlyaround1020%ofthosepatientswhobenefitfromPBTwould<br />
<br />
2<br />
CancerCentreFinalInvestment<strong>Case</strong>forPhase3(2008),p87<br />
3<br />
TheParticle<strong>Therapy</strong>CooperativeGroupwebsite(Accessed:14.03.2012)<br />
URL:http://ptcog.web.psi.ch/<br />
<br />
<br />
<br />
Page10
ebetter treatedwithheavyiontherapy.Significantly,thereislittleconfidence inheavyion<br />
therapybeingusedtotreatchildren, 4 whichwouldformalargeproportionofUCLH’scaseload. 5 <br />
Thelikelihoodofthishappeningwith510yearsisverylow.HeavyIonsarestillattheresearch<br />
stage because of their different radiobiology, whilst PBT is considered a stateoftheart<br />
modality.ThecostofheavyionfacilitiesisalsouptodoublethatofaPBTfacilities,meaning<br />
even when heavy ions are clinically proven (as they are likely to be), it will be exceptionally<br />
difficult for organisations to provide a service.There are few developments on the horizon<br />
suggestingheavyiontherapywillbecomecommerciallyviablewithinthenext1020years.The<br />
costinensuringnowthattheUCLHfacilitycouldbelaterupgradedtoHeavyIonsishigh.Larger<br />
accelerators,magnetsandgantrieswouldberequired(roughly170%to230%thefootprintand<br />
thecost).However,itislikelythatin10yearstime,technologywillhaveadvancedtothepoint<br />
thatnew(superconducting)magnetscouldberetrofittedintheoriginalfacilitytoprovidethe<br />
choiceofheavierions,ifdeemednecessary.Thereforethereislittletobegainedby‘future<br />
proofing’thefacilityagainstheavyiontherapydevelopment.<br />
<br />
SmallerandcheaperPBTsystemsaredeveloped<br />
<br />
The main technological developments around particle therapy are not those which make PBT<br />
redundantorsuperseded –theyarearoundmakingPBTsmallerandcheaper.Therearetwo<br />
relevant technologies which are currently under development but are more than 510 years<br />
awayfromclinicalavailability(evenlongerforcommercialavailability).<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
TheimpactofthesedevelopmentswouldbetomakePBTcheapertodeliver,whichwouldlower<br />
theoveralltariffprice.Itislikelythesetechnologies,orsimilarones,willbecomeavailableat<br />
somepoint.However,itishighlyunlikelythatthiswillbecomeavailableonthemarketfor1015<br />
years. By the time these technologies become available on the market, UCLH will have<br />
establisheditselfasaleadingPBTexpertintheUK.Wewillbeseenasacentreofexcellencefor<br />
patients,staffandcommissionersalike.Anysignificantimpactondemandisthereforelow.<br />
<br />
ThekeytechnologicalrisktoPBTisthereforenotobsolescence(thisishighlyunlikely),norfuture<br />
unreliability/unsuitability(thekeyspecificationsofafutureproofedsystemareclear).Rather,<br />
the key risk is around systems becoming smaller and cheaper in future. However, from our<br />
<br />
4<br />
AddressofStephanieCombs(UniversityofHeidelberg)totheParticle<strong>Therapy</strong>CooperativeGroupAnnualMeeting,2009.<br />
5<br />
DuetothepartnershipwithGOSH<br />
<br />
<br />
<br />
Page11
Appendix2B:UCLHServiceStrategy<br />
TheUCLHBoarddiscussedtruststrategyatitsawaydayon9 th November.<br />
SPBagreedthefollowingnextstepsatitsmeetinglaterthatmonthtobeginimplementationof<br />
theconclusionsoftheBoardawayday:<br />
• Produceashortsummarydocumentupdatingthetruststrategicplan<br />
• UpdatetheStrategicProgrammeBoardTermsofReference<br />
• DevelopanddiscussatSPBthestrategyforeachofthekeyprioritiesidentifiedby<br />
theBoard:<br />
o<br />
o<br />
o<br />
o<br />
o<br />
Neurosciences<br />
Cancer<br />
Women’sHealth<br />
Providerpartnerships<br />
Integratedcare<br />
• Developaforwardworkprogramme(byDecemberSPB)thatalignstheSPBagenda<br />
withkeydecisionscomingtotheBoardin2012<br />
Setoutbelowisadraftsummaryupdateofthetrust’sstrategicprioritiesfor2012.Theintention<br />
ofthisdocumentwouldbetouseitasthebasisforcommunicationmorewidelybothinsideand<br />
outsidethetrust.<br />
UCLHServiceStrategy–2012/13<br />
1.1. Background<br />
TheBoardreviewedthetruststrategicserviceprioritiesfor2012/13atitsawaydayin<br />
November.Thispapersummarisestheconclusions.<br />
TheBoardlastrevieweditsservicestrategyin2008.Sevenserviceareaswereidentifiedwith<br />
fourspecifiedascoreresearchspecialities.Theywere:neurosciences,cancer,cardiac,women’s<br />
health,dental,paediatricsandacuteservices.<br />
Threeyearsonwehavemadeconsiderableprogressagainstthestrategicprioritiesweidentified<br />
atthetimeforeachserviceincludingworkingwithUCLtosecurethebidforanew<br />
neurosciencesresearchcentre(SainsburyWelcome),successfullymovingwomen’shealthintoa<br />
newfacilityinPhase2in2008andcompletingthedevelopmentofanewCancercentreand<br />
cancerpartnershipwithMacmillan.<br />
Wehavedeliveredthesechangeswhilstcontinuingtomaintainandbuilduponourreputation<br />
forexcellentpatientcare,recognisedbyDrFosterin2009and2011.<br />
WehavecontinuedtogrowUCLHasanorganisationwiththeacquisitionoftheRoyalNational<br />
ThroatNoseandEarHospitalin2012whichwillformtheplatformforthefurtherdevelopment<br />
ofHead&NeckservicesatUCLH.<br />
Wehavealsocontinuedourfocusonresearchandacademicexcellence.UCLHwasafounding<br />
memberofUCLPin2009,theUKslargestandarguablyleadingAcademicHealthScienceCentre.<br />
In2011,togetherwithUCLwesuccessfullysecuredCBRCfundingof£100mtowardsourjoint<br />
clinicalandtranslationalresearchagenda.<br />
<br />
<br />
<br />
Page16
1.2 Thechallengeahead<br />
Lookingforwardhowever,wefaceachallengingenvironment:<br />
• WefacearealtermsflatNHSbudgetforpossiblyaslongasto2020(accordingtothe<br />
KingsFund)<br />
• WehavebetterfacilitiesthanthemajorityoftrustsinLondonbutcapacitywithin<br />
thebuildingisnowconstrained(e.g.A&E,maternity).Furthergrowthcouldrequirea<br />
stepchangeininvestmentoramajorchangeinworkingpractices<br />
• Commissionershavesignalledtheirintenttocontinuesupportingashiftofcareout<br />
of hospital into the community whilst centralising some specialist services to<br />
improvequality<br />
• Wehavefurtherworktodotodevelopourpartnershiprelationshipswiththelocal<br />
DGHandprimarycarecommunity<br />
• Theproviderlandscapearoundusischangingrapidlywithplansformergersinmost<br />
sectorsinLondon<br />
• Arrangementsforthecommissioningofmedicaleducationarechanging<br />
• BRC funding is now directed towards Experimental Medicine and we have been<br />
challengedtonarrowourareasoffocus.<br />
1.3 Ourvision<br />
TheBoardagreedourvisionremainsunchangedfrom2008;UCLHiscommittedtodelivering<br />
topqualitypatientcare,excellenteducationandworldclassresearch.<br />
Underpinningthiscorporatevisionisourcommitmenttocontinuetoprovidebothaserviceto<br />
ourlocalpopulationalongsidespecialistservicesforthepopulationofLondonandbeyond.<br />
1.4 Strategicdevelopmentpriorities<br />
TheBoardreviewedourcurrentservicesagainstarangeofcriteria.Theyincluded:<br />
• LinkwiththeBRCstrategyforthenext5years<br />
• Competitivepositionatalocal,Londonandnationallevel<br />
• Extenttowhichtheservicehascriticalmassandacomprehensiveoffer<br />
• Availabilityofcapacity<br />
TheBoardagreedthreestrategicservicedevelopmentprioritiesandfourareasofpartnershipto<br />
focusonintheyearahead.Theywere:<br />
Services<br />
• Neurosciences; where priorities include securing further neurooncology and<br />
neurosurgeryactivity<br />
,ensuringacademicandclinical<br />
priorities and strengths are aligned where possible, building on the successful<br />
Wolfsonbidtodevelopexperimentalneurologyandincreaserecruitmenttoclinical<br />
trials,anddevelopingplansfornewcapacityincludingworkingupa“QueensSq@”<br />
deliverymodel<br />
• Cancer;whereprioritiesincludesuccessfulcommissioningofthenewCancerCentre,<br />
delivering a step change in patient experience, securing <strong>Proton</strong> <strong>Beam</strong> <strong>Therapy</strong>,<br />
<br />
<br />
<br />
Page17
Partnerships<br />
supportingthedevelopmentoftheLondonCancerpartnershipandsupportingthe<br />
expansionofacademiccancertocompetenationally<br />
• Women’s health; where priorities include developing plans for expansion of<br />
maternity in line with women’s choice, and to further develop UCLH’s role as a<br />
network,Londonandnationalproviderofcomplexcareforwomenandneonates,<br />
andinadditionsupportingthecanceragendaingynaecologicalcancersandbreast<br />
cancersurgery.<br />
• DevelopthepartnershipwithBLTforthefuturejointprovisionofcardiacservices<br />
• DevelopanapproachtoIntegratedCarebasedoneffectivepartnershipswithlocal<br />
primaryandcommunitycareproviders<br />
• FurtherdevelopthepartnershipwithGOSHforcancercareforchildrenandyoung<br />
people,andtertiarypaediatricspecialties.<br />
• Considerwherethetrustcanworkwithlocalacutepartnerstodevelopservices<br />
• Work with UCL to align the trust and university strategies in order to successfully<br />
competeinanincreasinglyglobalmarketplace<br />
Inaddition,wehavealreadyhighlightedaboveontheinterrelationshipbetweenourstrategic<br />
servicedevelopmentprioritiesandlocalhospitalcommitment.<br />
Ourvisionofsuccessfuldevelopmentofspecialistservicesrequiresaplatformofexcellencein<br />
surgery,emergencymedicineandacutepaediatrics.Thismeansinvestingindevelopmentof<br />
surgeryparticularlyinareaswhichsupportourobjectivesandensuringthatnewcommissioner<br />
standardsforacuteservicequalityandsafetyaremet.<br />
1.5 Nextsteps<br />
TheExecutiveBoardandtheTrustBoardhaverequestedthatplansarenowdevelopedto<br />
achieveourobjectivesforeachprioritiesidentified.Thesewillbedevelopedanddiscussed<br />
duringthefirsthalfof2012.<br />
<br />
<br />
<br />
Page18
Appendix2C:EqualityImpactAssessment<br />
UCLH<strong>Proton</strong><strong>Beam</strong><strong>Therapy</strong>EqualityImpactAssessment<br />
Whatistheobjective(s)ofthisactivity?<br />
DevelopmentofNational<strong>Proton</strong><strong>Beam</strong><strong>Therapy</strong>ServiceonUCLHOdeon/Rosenheimsite<br />
Whowillbeaffectedbythisactivity?<br />
Patients,Carers,Staff<br />
Is there any evidence or potential that affected people might have different experiences or<br />
needsinrelationtothisactivity?<br />
AGEYes<br />
Basedonthecurrentindicationlist,around20%patientswillbechildren,andwithasignificant<br />
proportionrequiringGAs.<br />
The needs of this group of patients have been built into the PBT plans. UCLH has the largest<br />
paediatricandyoungadultcentreforradiotherapyintheUKandwithaclosepartnershipwith<br />
GreatOrmondStreetHospital.PBTwilltakeforwardthemodelalreadysuccessfullybeingused<br />
inUCLH’sRadiotherapyservice.<br />
<br />
DISABILITY–Yes<br />
Enablingdisabledpatients’fulluseofthePBTfacilityhasbeendevelopedintothedesigns.The<br />
facility will be built to legal requirements regarding disability access. Information will also be<br />
developed to enable access for all patients. Providing the appropriate transport and<br />
accommodationwillalsobebuiltintotheplans.<br />
TheDHcurrentlyreferpatientsabroadsoUCLHwillbeabletotapintotheresourcescurrently<br />
usedtounderstandthewiderrequirementsofdisabledgroups.<br />
<br />
SEXYes<br />
Theextendedworkingdaywillaffecttheshiftpatterns;somewillneedtoworkearlyshiftsand<br />
late shifts. This could adversely impact upon those with childcare responsibilities (which are<br />
more commonly females). The working day is a business requirement and there is a need to<br />
ensure there are sufficient staff to work unsocial shift patterns. The shift patterns can not be<br />
avoided, but the project will be working with HR to appropriately develop new employment<br />
contracts.<br />
<br />
RACEYes<br />
AsPBTisanationalservice,patientsfromavarietyofbackgroundswillbetreatedatUCLH.The<br />
PBT service will build on UCLH’s current approach to diversity and will use local translation<br />
serviceswhereappropriate.ThePBTteamwilllearnfromtheexistingDH<strong>Proton</strong><strong>Beam</strong><strong>Therapy</strong><br />
programmetoreferpatientstooverseascentres.<br />
<br />
<br />
<br />
Page19
RELIGIONORBELIEFNo<br />
StandardNHSpolicieswillapplytotreatmentsensuringnodiscrimination.<br />
<br />
SEXUALORIENTATIONNo<br />
<br />
GENDERREASSIGNMENTNo<br />
<br />
MARRIAGE,CIVILPARTNERHSIPNo<br />
<br />
PREGNANCY,MATERNITYNo<br />
<br />
Basedontheabove,isafullequalityimpactanalysisrequiredforthisactivity?<br />
No<br />
• The service will be delivered in a new centre. This will be designed to meet all<br />
equalityrequirementsassetoutinlaw.<br />
• Accesstotheservicewillnotberestrictedduetoage.Theservicewillbuildonthe<br />
currentmodelinRadiotherapy<br />
• Access to the service through insufficient communication will not occur as<br />
appropriate comms materials will be provided to disabled groups and to their<br />
referringcentres.<br />
• Access will not be restricted to through language issues as appropriate comms<br />
materialswillbeprovidedinnecessarylanguagesandtotheirreferringcentres.<br />
• The service is being coordinated by DH at the moment (as they refer patients<br />
abroad).Thereexperienceofcommunicatingtovariousgroupswillbeinvaluable.<br />
• The extended working hours will impact staff groups, and could adversely affect<br />
thosewithchildcareresponsibilities.Thiscannotbeavoidedasthereisabusiness<br />
needtoworkthelongerhours.<br />
<br />
<br />
<br />
Page20
Appendix3A:UCLHandtheChristiePBTthroughputmodelling<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
Page28
Page29
Appendix3B:PBTQualitativeBenefitsAnalysis<br />
<br />
<br />
<br />
<br />
Page30
Appendix3C:EconomicAssessmentwithQALYAnalysis<br />
The<strong>OBC</strong>NetPresentValueanalysisinTable14onpage63oftheUCLH<strong>OBC</strong>waspredicatedona<br />
40 year appraisal period. Notwithstanding this, the Trust has responded to the challenge of<br />
considering the proposal over a 20 year period. The following sections update the economic<br />
assessmentacross20years.<br />
Following the Green Book guidance, the Trust has updated the Economic Analysis of the PBT<br />
<strong>OBC</strong>. The Trust has included an assessment of QALY analysis within its presentation, which is<br />
derivedfromtheanalysispresentedintheDepartmentofHealthStrategic<strong>Outline</strong><strong>Case</strong>;thisis<br />
includedinAppendix3A.TheQALYassessmentpresentstheUCLHoptionsanalysiswithinthe<br />
QALYanalysisframeworkdevelopedforDepartmentofHealthStrategic<strong>Outline</strong><strong>Case</strong>.<br />
EconomicAppraisalupdate<br />
This economic assessment focuses on the economic impact of the UCLH PBT Service. The<br />
followingcostsandbenefitswereconsidered:<br />
Capitalcosts<br />
Revenuecosts<br />
Overseascosts<br />
Radiotherapy<br />
costs<br />
Opportunity<br />
costs<br />
Costofrisk<br />
ResidualValueof<br />
assets<br />
Building designs have been developed with our design team led by<br />
architects<br />
, and Construction costs have been<br />
providedbytheteam’scostadvisors, .<br />
Equipmentcostshavebeendevelopedfromthemarketsoundings.<br />
Contingencyat10%andOptimismBiasof14.3%hasbeenincludedin<br />
thecosts.<br />
Capitalisedprojectmanagementcostshavebeendeterminedinternally<br />
bydefiningthestaffingandsupportrequirementsoftheservice.<br />
Revenuecostshavebeendeterminedinternallybydefiningthestaffing<br />
and nonpay operational requirements of the service, including<br />
overheads.<br />
Costs of continuing to treat patients at overseas centres, source DH<br />
Strategic<strong>Outline</strong><strong>Case</strong>(SOC).<br />
Costsofcontinuingtotreatpatientswithradiotherapy,sourceSOC.<br />
Opportunitycoststypicallyrepresenttheassociateduseofthelandto<br />
development the centre. The Trust has plans to develop the site on<br />
whichtheproposedPBTfacilitywillbelocated.AssuchtheTrusthas<br />
no intention to dispose of the site and so it considers that the land<br />
thereforehasnodirectopportunitycostforthePBT<strong>OBC</strong><br />
Anumberofriskitemswerequantifiedincluding:<br />
Costchanges:Equipment,Construction,ProjectManagement,Staffing,<br />
VAT,andnonPay.<br />
Delay costs from procurement, design work, equipment delivery,<br />
construction, commissioning impact on both extending Project<br />
Management costs and reducing the number of patients treated<br />
thereforereducingthelevelofQALYs<br />
Theestimatevalueofthebuildingafter20yearsofoperation<br />
<br />
<br />
<br />
Page31
Developrelationshipswithcharitiesthathaveexistingassociationwithservicestobeprovidedin<br />
Phase4<br />
Philanthropy: raisedforPBT<br />
Research&innovationobjectives<br />
Technicalsolutionensuresfutureproofing<br />
100%PBTpatientsenrolledinclinicaltrials(DHpolicy)<br />
Partnerships<br />
ResolutionoffutureworkingarrangementswithinUCLPonLondonCancer<br />
EstablishmentofNational<strong>Proton</strong><strong>Beam</strong><strong>Therapy</strong>ServicewithDH,NCBandTheChristie<br />
Patientexperience<br />
ReviewpatientinformationserviceanddeterminewhatisrequiredtomakeserviceatUCLH<br />
thebestinthecountrywhenthePhase4opens<br />
<br />
Page37<br />
<br />
<br />
<br />
<br />
DHStrategic<strong>Outline</strong><strong>Case</strong><br />
(January2012)
Appendix3E:FinancialAppraisal<br />
PHASE4DEVELOPMENTOUTLINEBUSINESSCASE<br />
CONTENTSOFFINANCIALMODELLINGAPPENDIX<br />
Section Appendixdetail<br />
1 PBTFinancialmodel–keyassumptions<br />
2 Economic<strong>Case</strong><br />
Keyfinancialextracts<br />
3 Financial<strong>Case</strong><br />
Keyfinancialextracts–I&E,balancesheetandcashflow<br />
4 Commentaryon<strong>Proton</strong><strong>Beam</strong>Recurringandnonrecurringrevenuecosts<br />
5 Reconciliation of capital costs – Quantity Surveyor magnitude of cost to<br />
financialmodelcapitalcost<br />
6 OptimismBiasCalculation<br />
<br />
Page38
SECTION2–ECONOMICCASE–FINANCIALEXTRACT(REAL)<br />
<br />
<br />
Version4 Page45
Version4 Page46
Version4 Page47
SECTION3–FINANCIALCASEEXTRACTSI&E,BALANCESHEETNADCASHFLOW(NOMINAL)<br />
PROTONBEAMFINANCIALSTATEMENTS<br />
Version4 Page48
Version4 Page49
Version4 Page50
SECTION4Commentaryon<strong>Proton</strong><strong>Beam</strong>Recurringandnonrecurringrevenuecosts<br />
1 <strong>Proton</strong><strong>Beam</strong>RevenueCosts<br />
RecurringFacilityinfrastructurerunningcosts<br />
The revenue infrastructure costs for the new build have been estimated based on the size and configuration of the proposed facility with the recurring<br />
revenuecostsforthenewbuildoptionsbeingestimatedtakingaccountofthefollowing:<br />
• CapitalChargesandfundingmechanism<br />
• UtilitieswithseparatecalculationsforPBTelectricityconsumption<br />
• Rates(basedonPhase3)<br />
• HardandSoftFacilitiesManagement(basedonPhase3)<br />
• AllrevenuecostsincludenonrecoverableVAT<br />
The project team is mindful of the fact that cost estimates included with the Strategic Investment Framework for the Cancer Centre turned out to be<br />
substantiallyunderestimatedwhencomparedtoactualcoststhatarosepostopening.<br />
ComparisonshavebeenmadebetweentheestimatedrunningcostsforPhase4facilityascomparedtotheactualcostsofbothPhase3andPhase1and2.<br />
WherethishasidentifieddeficienciesinthePhase4runningcostestimatesthesehavebeenanalysedandwhereappropriatePhase4costadjustmentshave<br />
beenmade.<br />
Thetrustcurrentlyhasoutsourcedfacilitiesmanagement(FM)servicesacrossitssites,includingtherecentlyopenedcancercentre.Inthefirstinstanceitis<br />
feltthatthatthefacilitiesmanagementservicesinPhase4willagainbeprovidedbyanoutsourcedsolution.AccordinglyFMcostsestimatesforthePhase4<br />
facilityhavebeenbasedonthecurrentlyoutsourcedsolutionforboththetower/podiumandthecancercentre.<br />
The final cost consideration was the PBT utility costs which represent one of the key operating costs for the PBT facility. In order to provide a robust<br />
electricitycostestimatethetrustpreviouslyworkedwithaUSoperationfacility toidentifyamethodologyofderivingarobustutilitycosts<br />
estimate.Thiscostestimatewasvalidatedby in2010asbeingreasonableforPBTfacilityandsothecostshavebeenupdatedtocurrentutility<br />
costswithinthecurrentfinancialmodel.<br />
Accordinglytheprojectteamfeelsthatitnowhasrobustestimatesforthefacilitycostsidentifiedabove.<br />
Version4 Page51
• Directandindirectnonpaycosts<br />
• Corporateoverheads<br />
PBTstaffcosts<br />
Duringyearoneofoperation,thePBTfacilitywillbecommissionedattherateof1roomperquarter,resultinginthreeroomsbeingfullyoperationalbythe<br />
endofquarter3andwhereappropriatefourroomsbeingfullyoperationalbytheendofthefirstyear.Thiscommissionofrooms,coupledwithshortworking<br />
daysof8hourssubstantiallylimitspatientthroughputinyear1ofoperation.<br />
AsidentifiedundernonrecurringPBTcostsitwillbenecessarytorampupstaffinthefinalyearofconstructionsothatstaffareabletobefullytrainedas<br />
wellasbeinginvolvedwithtestingthePBTequipmentandestablishingtheclinicalpathway.<br />
BasedonexperiencefromtheUS,itisanticipatedthattypicallyitwillbetheendofyearthreebeforethesiteisfullyoperational,atwhichstageithasbeen<br />
projectedthatitwilloperateona16hourday5daysaweekbasis(8hoursperdayinyear1and11hoursperdayinyear2).Theopeninghoursofthefacility<br />
andtotalquantumofstaffcostshavebeencomparedwiththeChristie’sstaffingmodelandfoundtobewhollyconsistent.<br />
Equipmentmaintenance<br />
AsidentifiedinthecapitalcostsectionthePBTsolutionishighlycapitalintensivewithPBTequipmentandsupportdiagnostictechnologycostingintheregion<br />
of for a 3 room solution. Broadly speaking NHS experience is that in general maintenance of clinical equipment costs in the region of<br />
<br />
• Treatmentplanningsystem <br />
• Datamanagementsystem <br />
• Imagingsystems <br />
• CorePBTequipment <br />
Corporateoverheads<br />
TheprojectteamhasrecognisedthatthePBTproposalrepresentsasubstantialsteppedchangetothetrust’sactivity.Anestimateofclinicaladministrative<br />
resources has been included in the PBT staff cost estimate, including such roles as general manager, business manager and data management staff. In<br />
Version4 Page53
addition, the financial model includes a cost estimate of . to cover an increase in other indirect trust cost representing approximately 5.0% of<br />
projectedRealincomeofcirca .<br />
Otheroperatingcosts<br />
The exact scope of the PBT service has yet to be definitely agreed with DH. By way of example although such costs as patient transport and patient<br />
accommodationwillbeanimportantpartoftheoverallPBTpathway,thetrusthasconsistentlynotedthatitisunabletoincludeacostestimateofsuch<br />
activitiesunlessDHareabletoconfirmwhetherthiscostshouldbebornecentrally,locallyorbythePBTcentres.Thetrusthasclearlynotedanumberof<br />
exclusionsfromitsprojectedcostbasewhichwillbeincludedwithintheSIF.<br />
Notwithstandingthesespecificexclusions,thetrusthasmadespecificcostallowanceswithinthefinancialmodelforadministration,marketingandother<br />
nonpropertyrelatedcontractedoutservicesat orabout ofincome.<br />
ItisfeltthatthesecostestimatesshouldrepresentaprudentestimateofPBTcostsbasedonbothU.S.APBTandlocalradiotherapyexperience.<br />
<br />
Version4 Page54
Version4 Page56
OBForm1–SummaryofCapitalCosts.<br />
<br />
Version4 Page57
OBForm2SupplierAWorksCosts<br />
<br />
Version4 Page58
OBForm2SupplierBWorksCosts<br />
<br />
<br />
Version4 Page59
OBForm3SupplierAOnCosts<br />
<br />
<br />
Version4 Page60
OBForm3SupplierBOnCosts<br />
<br />
<br />
<br />
<br />
Version4 Page61
OBForm4SupplierAFeesandNonWorksCosts<br />
<br />
<br />
<br />
Version4 Page62
OBForm4SupplierBFeesandNonWorksCosts<br />
<br />
<br />
Version4 Page63
SECTION6OptimismBiasCalculation<br />
Version4 Page64
Programme opportunities in the PBT equipment procurement process<br />
Introduction<br />
The purpose of this paper is to outline the selected procurement process, the timescales, the level of<br />
commitment on the part of the Trusts to proceed, and provide recommendations for the appropriate timing of<br />
the procurement phases.<br />
The equipment procurement is on the critical path for the PBT project (See Annex A for current agreed<br />
programme milestones 7 ). As a result, any opportunities for time savings in the procurement process will lead<br />
to efficiencies in the overall programme with any delays similarly feeding into the overall programme. Under<br />
the current programme, the Expression of Interest phase with a Pre-Qualifying Questionnaire is launched at<br />
the end of January 2013 (Line 8). However, this is linked to full Government approval of the Trusts’ <strong>Outline</strong><br />
<strong>Business</strong> <strong>Case</strong>s (Line 7). It is estimated that there is a minimum of a two month period for this phase, which is<br />
prior to launching the tender phase with the Invitation to Participate in Dialogue (ITPD) (Line 9). This paper<br />
makes the following recommendations:<br />
Keep to the current programme and launch the Expression of Interest phase in early 2013<br />
Launch the tender phase at the point of full Government approval of the Trusts’ <strong>Outline</strong> <strong>Business</strong><br />
<strong>Case</strong>s (<strong>OBC</strong>)<br />
Procurement Route<br />
Due to the complexity of the equipment procurement, it has been determined that Competitive Dialogue (CD)<br />
is the most appropriate procurement route to ascertain the technical means of meeting the Trusts’<br />
requirements. As such, there are two main phases for the procurement:<br />
1. Expression of Interest (EoI) phase<br />
Process<br />
The Expression of Interest (EoI) phase is launched with the publication of three documents in the supplement<br />
to the Official Journal of the European Union (Line 8):<br />
<br />
<br />
<br />
<br />
A Contract Notice (CN). This will define the procurement route and the single lot procurement of PBT<br />
equipment and services for both Trusts. The Contract Notice will define the maximum and minimum<br />
number of Bidders to be taken through to CD.<br />
A Pre-Qualification Questionnaire (PQQ). This will define the range of data (financial, insurances,<br />
policies, previous relevant experience, case studies and testimonials) that Bidders need to make<br />
available as part of their expression of interest submissions.<br />
A Memorandum of Information (MoI). This document provides information on the background to the<br />
project, an overview of the procurement process, evaluation criteria and weightings, commercial<br />
principles and guidelines for the Bidders.<br />
Expressions of interest will be then be evaluated. Bidders who pass through the two pass/fail gateways<br />
covering eligibility and financial standing will then be considered in terms of their technical and professional<br />
ability. Marks will be awarded based on bidders’ experience, case studies and testimonials. At the end of this<br />
stage the Bidders will be ranked to determine who will be invited to tender for the equipment procurement and<br />
participate in the CD.<br />
Level of commitment<br />
<br />
7 N.B. The Programme Milestones tracks the key activities and does not provide the full details on<br />
the PBT equipment procurement and wider PBT programme. There is also a difference in<br />
terminology used<br />
Version4 Page87
Up to this point in the process, no future commitment – financial or otherwise – has been made by the Trusts.<br />
The process to this point merely seeks expressions of interest from Bidders who wish to be considered. The<br />
MoI referred to above will make it clear to Bidders that the Trusts will be under no obligation to pay for any<br />
costs incurred by Bidders or to award a contract as a result of the procurement process. This can be mirrored<br />
in the CN as well. If at this point, the project does not continue, whilst there will be a reputational impact on the<br />
Trusts, the only costs incurred by the Trusts will be in relation to the procurement and legal advice provided.<br />
There would be no further known Trust-related liabilities and none in relation to the DH.<br />
Time Period<br />
There is a minimum 30 day period from issue of CN, PQQ and MoI to receipt of expressions of interest and a<br />
further 30 days for the evaluation of expressions of interest. As such, this phase is currently programmed in<br />
for a minimum of a two month period.<br />
Recommendations<br />
To maintain the current programme requires the launch of the EoI phase at the end of January 2013. As the<br />
level of commitment to the Trusts is minimal, and does not involve a tender for solutions, the recommendation<br />
is the current programme is maintained. This could be linked to the approval of the Strategic Investment<br />
Framework to give all parties sufficient formal support for the overall PBT project.<br />
2. Tender phase<br />
Process<br />
The CD procurement route provides a high degree of flexibility in relation to how the dialogue is phased and<br />
the time period the dialogue is conducted within. An indicative timetable for the CD will be indicated in the MoI<br />
and the Trusts will reserve the right to adjust this timescale. The following process is based on the<br />
assumption that the CD will comprise two stages:<br />
Invitation to Participate in Dialogue (ITPD) (Line 9)<br />
The Invitation to Participate in Dialogue document will be issued to shortlisted Bidders at the commencement<br />
of the dialogue phase. It will set out the Trusts’ requirements, define how the dialogue will be conducted and<br />
confirm the number of down selection phases. It will also include the criteria and weightings for the rest of the<br />
process and the indicative timetable.<br />
1st stage dialogue<br />
In this first stage of the dialogue the focus will be on the technical solutions and some of the key commercial<br />
considerations. Prior to commencement of the 1:1 first stage dialogues there is the option of holding a Bidders<br />
open day to talk through the process.<br />
Invitation to submit outline solution (ISOS)<br />
At the end of the first stage dialogue Bidders will be invited to submit their outline design solutions. Bidders<br />
can be requested to include indicative costs at this point. These bids will be evaluated against the agreed<br />
criteria to down select to the Bidders taken through to the 2nd stage dialogue.<br />
2nd stage Dialogue (Line 10)<br />
In the second stage dialogue the focus will be on refining proposals and the development of commercial and<br />
contractual aspects. It needs to be remembered that all aspects of the contract have to be agreed<br />
substantially before the dialogue phase is concluded.<br />
Submission of final tenders<br />
When the Trusts consider that the competitive dialogue can be drawn to a close the Bidders will be asked to<br />
submit their final tenders. These final tender submissions will then be evaluated in accordance with the<br />
published procedure to determine the successful bidder.<br />
Version4 Page88
Evaluation, clarification and fine tuning<br />
There will then be a period of post-tender dialogue.<br />
Contract award notification and standstill period<br />
At the appropriate time Bidders will be notified of the contract award decision and it is at this point that the<br />
mandatory 10 day standstill period commences.<br />
Level of commitment<br />
The ITPD document issued to Bidders at the commencement of the CD phase will indicate that the Trusts will<br />
be under no obligation to pay for any costs incurred by Bidders or to award a contract as a result of the<br />
procurement process.<br />
Time Period<br />
The programme currently indicates that the period of competitive dialogue will be a minimum of 12 months.<br />
Recommendations.<br />
As the ITPD will issue the Trusts’ requirements and tender process, this requires formal approval of the<br />
project to proceed. As such, the recommendation is that the ITPD is linked to full Government approval of the<br />
Trusts’ <strong>OBC</strong>s.<br />
Version4 Page89
1. This paper outlines the requirements for external technical advisors for the procurement of PBT<br />
equipment.<br />
Background<br />
2. A range of external advisors will be required to ensure the <strong>Proton</strong> <strong>Beam</strong> <strong>Therapy</strong> (PBT) programme<br />
delivers the required outcomes:<br />
Financial<br />
Legal<br />
Procurement<br />
Design<br />
Technical<br />
Clinical<br />
Beyond the procurement stage the trusts would require further advice and support during the<br />
mobilisation and ramp-up stages which may include a comprehensive training package for clinicians,<br />
physics staff and radiographic staff. Depending on the supplier of the final equipment, the trusts may<br />
choose to select different technical advisors at the two different stages of the project (procurement<br />
and mobilisation).<br />
Recommendation<br />
3. We recommend that:<br />
the selection of the technical advisors for the trusts for the initial procurement stage be<br />
selected first,<br />
the appointment of the second set of advisors, for mobilisation and ramp up, is completed<br />
once the procurement stage is complete and the preferred proton equipment supplier(s) are<br />
known.<br />
The Steering Committee is asked to endorse the above recommendations.<br />
Procurement Stages<br />
4. The Christie and UCLH will be the first trusts in the UK to procure high energy PBT equipment. The<br />
procurement of proton therapy will be a complex process as:<br />
PBT equipment represents a significant amount of the considerable capital required for the<br />
development of the clinical service.<br />
PBT technology is progressing rapidly with several vendors bringing new products to market.<br />
PBT procurement decisions have often been challenged.<br />
There are four stakeholders DH, NHS Commissioners, UCLH and Christie involved in the<br />
process.<br />
5. It is important to ensure that the PBT equipment procurement results in the purchase of the correct<br />
equipment to deliver the proton therapy programme and importantly:<br />
<br />
<br />
<br />
is performed in compliance with EU procurement legislation;<br />
is conducted without bias to any particular manufacturer and<br />
is completed expediently to facilitate timely opening of the centres.<br />
Subject Areas for Advice<br />
6. The areas where a need for external advice has been identified are:<br />
<br />
Technical advice proton beam therapy – <strong>Proton</strong> treatments are significantly different to photon<br />
radiotherapy treatments that the Christie and UCLH are used to planning and delivering.<br />
Consequently the trusts lack knowledge about PBT treatments that will dictate requirements<br />
for proton therapy equipment. Technical advice from physicists accustomed to proton therapy<br />
equipment will strengthen the procurement team.<br />
Version4 Page91
Technical advice proton equipment – The progress of proton therapy technology means that<br />
the procurement process will need to evaluate technology that may not have been clinically<br />
implemented. This will require assessment of the development timeline for manufacturer’s<br />
equipment and analysis of the impact of changes to PBT equipment. There is considerable<br />
expertise from the particle physics accelerator community in designing and building proton<br />
accelerators and this expertise could assist in assessing potential developments tendered by<br />
PBT vendors.<br />
Contract Negotiation – During visits to PBT centres the importance of contract negotiation<br />
with proton beam manufacturers has been stressed by several centres. PBT requires an<br />
ongoing relationship with the equipment supplier and attaining the correct contractual<br />
framework to enable constructive working practices for the trusts and the equipment suppliers<br />
is essential.<br />
Type of advice, Commitment and Cost<br />
7. The procurement process is likely to take more than twelve months and the roles of those<br />
participating, internally and externally, need to be clearly defined. The key areas that have been<br />
identified for external advice are:<br />
<br />
<br />
<br />
<br />
Advising on detailed specification for PBT equipment.<br />
Advice on evaluation criteria for PBT equipment.<br />
Clarification of technical detail in the PBT tenders from manufacturers.<br />
Advice on scope and detail of contracts with PBT manufacturers.<br />
8. It should be noted that external advisors act in a purely advisory role and will not be involved in the<br />
evaluation of tender responses. Acting in an advisory role, rather than being involved in the primary<br />
evaluation, should reduce the liability of individuals, trusts and DH, should the process be challenged.<br />
As advisors they cannot be involved in the actual scoring of the tender responses again reducing the<br />
possibility of a challenge during the procurement stages. The evaluation of tender responses will be<br />
taken forward by the Trusts’ teams.<br />
9. The PBT Technical Advisory Group should be consulted at all the key steps of the procurement<br />
process and in particular should advise on (See #17 on group governance):<br />
<br />
<br />
<br />
<br />
Content for pre qualification questionnaires.<br />
The technical specification for proton therapy equipment.<br />
Returns from manufacturers at all stages in the procurement process.<br />
Discussions at contract stage with the two preferred bidders.<br />
10. The particular requirements will depend on the procurement process employed and should be<br />
mapped out as part of planning the PBT procurement.<br />
11. The Trust appointed technical advisors will be required to give advice at several points in the process<br />
and the time commitment has been estimated at 50hrs over the procurement process. An estimated<br />
market rate for specialist technical advice has been estimated at per hour but cost may vary.<br />
Travel for advisors will be kept to a minimum and importantly they will not be required to attend site<br />
visits with potential suppliers. So the cost of additional advisors will be in the order of split<br />
between the trusts.<br />
12. Given this estimated costs, market testing will be conducted whereby two quotations will be sought for<br />
each advisory role. The trusts will then decide on the most suitably-qualified person for each role<br />
including a value-for-money analysis.<br />
Selecting Advisors<br />
13. The trusts have established links with many potential advisors in the PBT community and the DH<br />
have commissioned advice from through the development of the proton<br />
beam programme. The route for procurement of further advice will need to be agreed by the trusts<br />
and the DH. Market testing may be of limited effect in an area with few specialized advisors and care<br />
Version4 Page92
would need to be taken that an open selection process did not disenfranchise important proton links<br />
nationally or internationally. It is important that the process will provide the required advice to the<br />
trusts and the DH.<br />
14. Through established links developed during the proton programme the trusts and DH have identified<br />
potential advisors who could provide advice in the required areas:<br />
Technical advice proton beam therapy - continues to serve as a<br />
member of the PBT Steering Committee, it is suggested that Professor Lomax is asked to<br />
chair the PBT Technical Advisory Group,<br />
Technical advice proton equipment - Both UCLH and The Christie have established links with<br />
proton accelerator scientists and have suggested advisors. UCLH have proposed <br />
and The Christie . It is envisaged that they will<br />
advise both Trusts as they bring different knowledge and skill-base to the Trusts. <br />
has extensive knowledge on accelerator design, beam optics and beam transport whilst<br />
offers expertise on beam diagnostics and dynamic beam simulations. They will be<br />
appointed individually through the separate trusts due to existing relationships<br />
Contract Negotiation – The Christie and UCLH have both recommended <br />
of who has experience of contract negotiation for a large and complex<br />
proton therapy project. The s econd proposed advisor to approached, for market<br />
testing purposes, would be Dr Al Smith, formerly of<br />
who has extensive<br />
Physics experience in one of the longest-running clinical centres.<br />
15. The Trusts shall draw up a joint contract between Trusts and the individual advisor, as opposed to<br />
their organisations. The length of this contract shall extend through the procurement process through<br />
to final signing of contracts with the preferred PBT supplier. This is expected to be approximately 30<br />
months.<br />
16. Contracts between the trusts and the advisors shall abide by terms and conditions as set out in the<br />
NHS Conditions of Contract for the Supply of Services (September 2010).<br />
Proposed Governance<br />
17. It is suggested that the advisors appointed form a trust advisory group (Technical Advisory Group)<br />
which<br />
will be invited to chair. The DH may also require technical advice to the<br />
wider programme and the trust advisory group would also be able to advise where appropriate should<br />
the DH wish to commission them.<br />
18. Members of the Technical Advisory Group would be expected to sign Non-disclosure Agreements<br />
(NDA) with both trusts which would also include the NDA agreements signed between trusts and<br />
suppliers.<br />
19. The commitment required for the role should be clear and it is important that the advisors see their<br />
role as advising the national programme as well as individual trusts and in particular contracts should<br />
be arranged through the trusts. Any conflicts of interest with particular manufacturers should be<br />
declared and any resultant restrictions to the scope of the advice given will be discussed with<br />
procurement and legal advisors.<br />
Non-Disclosure Agreements (NDA)<br />
20. Currently, The Christie and UCLH have signed three way non disclosure agreements with the<br />
suppliers. During the procurement process, information forwarded under these agreements will be<br />
disclosed to the advisory panel. Currently the three way NDA signed by The Christie and UCLH would<br />
not allow them to disclose information to the DH proton team. The procurement process must set<br />
suitable NDA arrangements to ensure a free flow of information between all parties participating and<br />
advising procurement.<br />
Trust requirements from the Technical Advisory Group to procurement completion<br />
Version4 Page93
21. Once appointed, the Trusts would call on the Technical Advisory Group for support and advice as<br />
follows:<br />
to hold an initial series of meetings with all interested parties at UCLH and Christie to be<br />
briefed on issues, requirements, priorities and methods of communication etc.<br />
to review technical specifications for upcoming procurements of technical equipment.<br />
the development of technical documentation for procurement equipment<br />
review and support the development of evaluation criteria for supplier tender responses<br />
to contribute towards the assessments tender responses<br />
to advise on the tender responses from equipment suppliers<br />
to contribute towards the working up of the competitive dialogue documents<br />
to provide advice on the Trusts’ evaluations of the tender responses following the Trusts’<br />
assessments<br />
assist in contract negotiation in technical advice on, but not exclusively:<br />
• Maintenance requirements<br />
• Deliverability and KPI<br />
To provide advice on build designs for functionality and radiation protection<br />
22. The technical advisors will not be expected to take part in the formal evaluation of the tender<br />
responses or the final selection of suppliers. This will remove any risk of challenge from suppliers on<br />
the basis of any bias towards suppliers familiar to advisors.<br />
will be able to bring<br />
valuable technical experience to the process, but they do not have any direct clinical experience,<br />
hence would not be well placed to evaluate against the requirements of the two Trusts. <br />
have relevant clinical experience but have pre-existing relationships with<br />
manufacturers that are likely to be involved in the procurement process.<br />
Trust requirements for advice for commissioning and ramp-up (Mobilisation Stage)<br />
23. Support from the Technical Advisory Group as described should see the Trusts through to the<br />
completion of the contractual stages of the procurement where the final chosen supplier(s) are<br />
selected. Beyond this stage, the Trusts would seek to commission further or new advisors to assist<br />
through the commissioning and ramp-up stages of the project. The advice and support during the<br />
mobilisation and ramp-up stages would include a comprehensive training package for clinicians,<br />
physics staff and radiographic staff. This role would be provided by an existing PBT centre with the<br />
choice of centre dependent on selection of the preferred proton equipment supplier(s) and include<br />
representatives from a clinical team experienced in delivering PBT to paediatric and complex adult<br />
indications to include Clinicians, Physicists, radiographers and facility administrators<br />
24. At this stage, the Trusts will draw up a joint contract between Trusts and the advisory team from the<br />
chosen clinical centre. The length of this contract shall extend through the acceptance and<br />
commissioning phase through to the initial ramp-up clinical stage. This is expected to be<br />
approximately 12-18 months.<br />
<br />
Version4 Page94
Annex D<br />
Document no 2<br />
Purpose<br />
REQUIREMENTS DOCUMENT<br />
Technical Advice to Support the Procurement of <strong>Proton</strong> <strong>Beam</strong> <strong>Therapy</strong> Delivery Systems<br />
UCL Hospitals NHS Foundation Trust and The Christie NHS Foundation Trust (the Trusts) seek<br />
expressions of interest to provide Medical Physics technical advice to both Trusts and Department<br />
of Health (DH) to support the procurement of <strong>Proton</strong> <strong>Beam</strong> <strong>Therapy</strong> delivery equipment for the UK<br />
National Service through to the completion of contracts with the chosen PBT supplier.<br />
Introduction<br />
The UK Department of Health has announced the development of two facilities to provide a National<br />
<strong>Proton</strong> <strong>Beam</strong> therapy (PBT) service. The two selected sites are University College London<br />
Hospitals NHS FT in London and The Christie NHS FT in Manchester.<br />
The Christie and UCLH will be the first Trusts in the UK to procure high energy PBT equipment.<br />
<strong>Proton</strong> treatments are significantly different to photon radiotherapy treatments that the Christie and<br />
UCLH are used to planning and delivering. Consequently the Trusts lack knowledge about PBT<br />
treatments that will dictate requirements for proton therapy equipment. Technical advice from<br />
physicists accustomed to proton therapy equipment and its clinical use will strengthen the<br />
procurement team.<br />
The procurement of proton therapy will be a complex process as:<br />
<br />
<br />
<br />
<br />
PBT equipment represents a significant amount of the considerable capital required for the<br />
development of the clinical service.<br />
PBT technology is progressing rapidly with several vendors bringing new products to market.<br />
PBT procurement decisions have often been challenged.<br />
There are four stakeholders DH, NHS Commissioners, UCLH and Christie involved in the<br />
process.<br />
It is important to ensure that the PBT equipment procurement results in the purchase of the correct<br />
equipment to deliver the proton therapy programme and importantly:<br />
<br />
<br />
<br />
is performed in compliance with EU procurement legislation;<br />
is conducted without bias to any particular manufacturer and<br />
is completed expediently to facilitate timely opening of the centres.<br />
The two Trusts are therefore seeking to procure Medical Physics technical advice to assist in the<br />
procurement and contractual stages of the project.<br />
Version4 Page95
Proposed Governance<br />
The DH has appointed<br />
as their technical advisor. The Trusts have also secured<br />
accelerator technology advisors in the persons of <br />
. It is proposed that all the technical advisors, including the one(s) appointed<br />
through this bid, form a Technical Advisory Group which<br />
will be invited to chair.<br />
The DH may also require technical advice to the wider programme and the Technical Advisory<br />
Group would also be able to advise where appropriate should the DH wish to commission them.<br />
The PBT Technical Advisory Group should be consulted at all the key steps of the procurement<br />
process and in particular should advise on:<br />
<br />
<br />
<br />
<br />
Content for pre-qualification questionnaires.<br />
The technical specification for proton therapy equipment.<br />
Returns from manufacturers at all stages in the procurement process.<br />
Discussions at contract stage with the two preferred bidders.<br />
Members of the Technical Advisory Group would be expected to sign Non-disclosure Agreements<br />
(NDA) with both Trusts which would also include the NDA agreements signed between Trusts and<br />
suppliers. Currently, The Christie and UCLH have signed three way non-disclosure agreements with<br />
the suppliers. During the procurement process, information forwarded under these agreements will<br />
be disclosed to the advisory panel. It is anticipated that appropriate NDA will be in place to allow the<br />
free-flow of information with the advisory group.<br />
The commitment required for the role should be clear and it is important that the advisors see their<br />
role as advising the national programme as well as individual Trusts and, in particular, contracts<br />
should be arranged through the Trusts. Any conflicts of interest with particular manufacturers should<br />
be declared and any resultant restrictions to the scope of the advice given will be discussed with<br />
procurement and legal advisors.<br />
Contracts between the Trusts and the advisors shall abide by terms and conditions as set out in the<br />
NHS Conditions of Contract for the Supply of Services (September 2010).<br />
Instructions to Potential Advisors<br />
Potential advisors are required to insert a narrative under each of the numbered points in the Trusts<br />
requirement from the Technical Advisory Group section of this document, in order to<br />
demonstrate their understanding of the requirement and to indicate the expertise and added value<br />
potential advisors can contribute towards it. The attached Offer Schedule (Document no. 5) must<br />
also be completed with man days and costs inserted against each numbered point in the brief. The<br />
attached Form of Offer (Document no. 4) and Assumptions Sheet (Document no. 6) must also be<br />
completed and returned.<br />
Note on Fees and Expenses<br />
It is hoped that several meetings can take place via teleconference and electronic communication<br />
but there may be a need for some face-to face meetings. Therefore, in applying for the advisory<br />
role, the applicant is required to provide proposed details of the number of meeting attendances<br />
they would expect to complete in the UK with total expenses indicated in the Offer Schedule<br />
(Document no. 5).<br />
Version4 Page96
Any potential advisors’ assumptions associated with their quotation must be detailed in the attached<br />
‘List of Assumptions’ document.<br />
Scoring of Tenders<br />
Tenders will be evaluated on the basis of the following award criteria and weightings:<br />
The narratives provided against requirements 1- 12 only of the ‘Trusts’ requirements from the<br />
Technical Advisory Group’ section of the Requirements Document (Document no. 2) will be marked<br />
out of 5 for a) understanding, b) added value. This allows for a total potential score of 10 for each of<br />
the 12 scored requirements.<br />
The 0 to 5 scoring methodology for the 12 scored requirements is as follows:<br />
<br />
<br />
0<br />
1<br />
2<br />
3<br />
4<br />
5<br />
Fails to provide evidence of their ability to meet requirements<br />
Evidences limited ability to meet some but not all of the requirements<br />
Evidences limited ability to meet all requirements<br />
Provides good evidence of the ability to meet all requirements<br />
Provides good evidence of the ability to meet all the requirements and<br />
exceeds them in some areas<br />
Provides good evidence of the ability to meet all the requirements and<br />
exceeds them in the majority of areas<br />
Total marks awarded for the 12 scored requirements will be multiplied by the quality weighting<br />
(100%) to arrive at a weighed score for the quality criteria.<br />
The total offer price will be divided by the weighted score for the quality criteria to arrive at a total<br />
score. The contract will be awarded to the potential provider with the lowest total score. The Trusts<br />
reserves the right not to award a contract against this Invitation to Tender.<br />
Type of Advice and Time Commitment<br />
The procurement process is likely to take from twelve to eighteen months, starting around October<br />
2012.The roles and commitments of those participating, internally and externally, need to be clearly<br />
defined.<br />
The technical advisors will not be expected to take part in the formal evaluation of the tender<br />
responses or the final selection of suppliers. This will remove any risk of challenge from suppliers<br />
on the basis of any bias towards suppliers familiar to advisors. As advisors they cannot be involved<br />
in the actual scoring of the tender responses, again reducing the possibility of a challenge during<br />
the procurement stages. The evaluation of tender responses will be taken forward by the Trusts’<br />
teams.<br />
Version4 Page97
Trusts requirements from the Technical Advisory Group<br />
Once appointed, the Trusts would call on the Technical Advisory Group for support and advice up to<br />
procurement conclusion as follows:<br />
1. to hold an initial series of meetings with all interested parties at UCLH and Christie to be<br />
briefed on issues, requirements, priorities and methods of communication etc.<br />
2. to review content for pre-qualification questionnaires<br />
3. to review technical specifications for proton therapy equipment.<br />
4. to support the development of technical documentation for procurement equipment<br />
5. to review and support the development of evaluation criteria for supplier tender responses<br />
6. to support review of returns from manufacturers at all stages in the procurement process<br />
7. to contribute towards the assessments tender responses<br />
8. to advise on the technical trustworthiness of tender responses from equipment suppliers<br />
9. to contribute towards the working up of the competitive dialogue documents<br />
10. to provide advice on the Trusts’ evaluations of the tender responses following the Trusts’<br />
assessments<br />
11. to assist in contract negotiation with the final two suppliers, with technical advice on, but not<br />
exclusively:<br />
a. Maintenance requirements<br />
b. Deliverability and KPI<br />
c. Delivery and installation priorities<br />
12. to provide advice on build designs for functionality and radiation protection<br />
13. A breakdown of proposed expenses should be supplied as part of the application with any<br />
assumptions clearly identified in the attached ‘List of Assumptions’ document.<br />
Version4 Page98
Annex E<br />
Procurementsupport/advicefor<strong>Proton</strong><strong>Beam</strong><strong>Therapy</strong>ProjectforUCLHospitalsNHSFoundationTrust<br />
andtheChristieNHSFoundationTrust<br />
Revisedbrief<br />
Thispapersetsoutthebriefforthejointlyappointedprotontherapyequipmentprocurementadvisorsfor<br />
UCLHandTheChristie.Theoriginalbriefhasbeenupdatedtoreflectdevelopmentsintheprogrammeata<br />
nationallevel,inparticulartheprovisionofpublicfundingandtheconfirmationoftwositesfordeliveryof<br />
the national service will require the current drafted procurement documentation to be refreshed.The<br />
timescalehasbeenextendedfollowingslippageinthenationalprogramme–theequipmentprocurementis<br />
expectedtobelaunchedfollowingagreementofthe<strong>Outline</strong><strong>Business</strong><strong>Case</strong>byHMTreasury(estimatedearly<br />
2013).Shouldtheprogrammeslipfurtherflexibilitywillberequiredtodeliverthebrief.Theinvolvementof<br />
the Department of Health, National Commissioning Board and Major Projects Authority create additional<br />
stakeholdersandexternalscrutiny.Finallyshouldtheprotontherapyprogrammenotbeapprovedtomove<br />
forwardtheactivitiesrequiredfrom<strong>OBC</strong>approvalwillnotberequired.<br />
<br />
Introduction<br />
UniversityCollegeLondonHospitalsNHSFoundationTrust(UCLH)andTheChristieNHSFoundationTrust<br />
(Christie)havebeenselectedbytheDepartmentofHealth(DH)asthetwocentrestoprovide<strong>Proton</strong><strong>Beam</strong><br />
<strong>Therapy</strong>(PBT)servicesinEnglandfromtheendof2017.UCLH,onbehalfofbothTrusts,isseekingsupport<br />
for the development and coordination of the equipment procurement.The equipment procurement is<br />
expected to commence immediately HM Treasury approval of the <strong>OBC</strong> is secured.Documentation is<br />
expectedtobedraftedinadvanceof<strong>OBC</strong>approvalinlinewithMajorProjectsAuthorityassuranceprocess.<br />
Theprocurementsupportrequiredisadedicated,flexibleresourceforthisperiodonan‘asrequired’basis.<br />
Whilst full time support is not necessary for the duration of the procurement it is envisaged that the<br />
resource will be required for several days per week in the precompetitive dialogue phase of the<br />
procurementandthatthiswillfluctuatethroughoutthevariousphasesofthecompetitivedialogueprocess.<br />
<br />
InstructionstoBidders<br />
Biddersarerequiredtoinsertanarrativeundereachofthenumberedpointsinthebriefforprocurement<br />
support to demonstrate their understanding of the requirement and to indicate the expertise and added<br />
valuebidderscancontributetowardsit.TheattachedOfferSchedulemustalsobecompletedwithmandays<br />
andcostsinsertedagainsteachnumberedpointinthebrief.<br />
Any bidders’ assumptions associated with their quotation must be detailed in the ‘List of Assumptions’<br />
document.<br />
Anybidders’questionsonthebriefitselfmustbesubmittedusingtheattached‘QuerySheet’.<br />
Fulldetails,includingskillsandabilities,ofthededicatedresource(s)whowillundertaketheservicesinthis<br />
briefaretobeprovidedineachbidders’response.<br />
<br />
Overviewforprocurementsupport/advice<br />
Version4 Page99
Tocoordinatetheproductionofthedocumentationincludingprocurementmethod(currentlyassumedto<br />
becompetitivedialogueprocess),ContractNotice,PreQualificationQuestionnaire(PQQ),Memorandumof<br />
Agreement(MoI)andcompetitivedialoguedocumentsincludingevaluationstrategy,criteriaandweightings<br />
andjustificationsasrequired.<br />
To coordinate the equipment procurement process from issuing contract notice to conclusion of<br />
challenges.<br />
To work closely with both trusts’ project teams and trusts’ appointed legal advisor to coordinate<br />
procurement advice to the trusts and all other advisors to the procurement process including financial,<br />
technicalandclinicalasrequired.<br />
<br />
Briefforprocurementsupport/advice<br />
1. Hold briefing meetings with all interested parties at UCLH and Christie to be updated on the project,<br />
issues, requirements, priorities, methods of communication etc. Reaffirm appropriate procurement<br />
approach.<br />
2.ToworkcloselywithTrusts’appointedlegaladvisortocoordinateprocurementadvicetotheTrustsand<br />
all other advisors to the procurement process including financial, technical and clinical as required to co<br />
ordinate the production of the documentation and procurement process including procurement method<br />
(currently assumed to be competitive dialogue process), and coordinate production of all procurement<br />
documentation including Contract Notice, PreQualification Questionnaire (PQQ), Memorandum of<br />
Agreement(MoI)andcompetitivedialoguedocumentsincludingevaluationstrategy,criteriaandweightings<br />
andjustificationsasrequired.<br />
3. Develop/Refresh Contract Notice for purchase of PBT equipment/services and seek legal sign off via<br />
Trusts’appointedlegaladvisorandagreementbybothTrusts.<br />
4. Develop/Refresh previously prepared procurement documents (using DoH or Trust standard PQQ<br />
templateasastartingpoint)forPBTequipmentandseeklegalsignoffandagreementbybothTrusts.<br />
5. Develop/Refresh Memorandum of Information (MoI) detailing high level requirements and the<br />
methodology for evaluation the PQQs) and seek legal sign off via Trusts’ appointed legal advisor and<br />
agreementbybothTrusts.<br />
6.SubmitContractNoticeforpublicationinEuropeanJournal.<br />
7. Coordinate and contribute towards assessment of PQQs by both Trusts and compile<br />
assessment/recommendationreport.<br />
8.Coordinateandcontributetowardstheworkingupofcompetitivedialoguedocuments(ordocuments<br />
relevanttotheprocurementprocessifcompetitivedialoguenolongerappropriate)andissuetoselected<br />
potentialproviders.<br />
9.Provideprocurementadvice,andseeklegaladviceviaTrusts’appointedlegaladvisorasrequired,onany<br />
relevant commercial aspects of the scheme during the course of the competitive dialogue with potential<br />
providers.<br />
10.Participateinbiddersopenday(ifheld).<br />
11. Coordinate and contribute towards the working up of offer documents, seek legal advise via Trusts’<br />
appointedlegaladvisorasrequired,signoffbybothTrustsandissuetoselectedpotentialproviders.<br />
Version4 Page100
12. Coordinate and contribute towards the evaluation of offers from potential providers seeking legal<br />
adviceviaTrusts’appointedlegaladvisorifrequired.<br />
13. Coordinate and contribute towards postoffer clarification dialogue with potential providers seeking<br />
legaladviceviaTrusts’appointedlegaladvisorifrequired.<br />
14.Coordinateandcompileassessment/recommendationreport.<br />
15.Issuecontractawardnotificationtopotentialproviders.<br />
16.Awardcontracttosuccessfulsupplieratendofstandstillperiod.<br />
17.Leadandcoordinatesupplierdebriefs.<br />
18.Compileperiodicandadhocreports(includingamonthlyupdate)andattendmeetingsasrequired.<br />
19.Coordinateandcontributetowardsresponsetoanylegalchallengespresented.<br />
<br />
Other<br />
20.TraveltoUCLHandtheChristieatManchesterwillberequired.Ahotdesk,PCandtelephonewillbe<br />
providedatbothlocationsasneeded.<br />
21.Liaisewithotherparallel/relatedprocurementsasrequired,forexamplebuild,externaladvisors(5days<br />
maximum)<br />
22.Toprovideprocurementsupport/advice(preworkandfollowup)toanyfurthersoftmarketsoundings<br />
thatareundertakeninadvanceoftheprocurementlaunch(2daysmaximum)<br />
23.ToworkwiththetruststoestablishadocumentmanagementapproachandITsolutiontofacilitatethe<br />
jointprocurement.<br />
24. To provide information where necessary for any supporting documentation required by other key<br />
stakeholderssuchastheDepartmentofHealthandNationalCommissioningBoard.(5daysmaximum)<br />
25. To work constructively to assure any external assurance/approval processes as required (for example<br />
GatewayReview).(5daysmaximum)<br />
<br />
Contractmanagement<br />
Thecurrentprocurementadvisorsareinvitedtosubmitarevisedproposaltomeetthespecificationsetout<br />
above.<br />
Version4 Page101
Annex F<br />
<br />
UCLH and Christie proton therapy equipment procurement technical meeting<br />
25 October 2012<br />
Present:<br />
Actions<br />
1 Procurement strategy<br />
Draft procurement strategy and identify<br />
gaps/circulate<br />
2 Joint procurement advisors<br />
<br />
by 12 Nov<br />
Reinstate procurement advisors by 12 Nov<br />
3 Joint financial and legal advisors<br />
Procure financial and legal advisors asap<br />
4 Joint external technical advisors<br />
Procure external technical advisors by 12 Nov<br />
5 Trust technical advisors<br />
Finalise paperwork for Hywel asap<br />
6<br />
PQQ<br />
6.1<br />
Review existing PQQ documentation.<br />
<br />
by w/c 12 Nov<br />
6.2<br />
Once procurement advisors appointed – meet with<br />
procurement advisors for briefing<br />
<br />
w/c 12 Nov (or<br />
19 Nov)<br />
6.3<br />
Procurement advisors to refresh PQQ<br />
documentation excluding technical specification.<br />
<br />
<br />
by 30/11/12<br />
7 Technical specification<br />
Version4 Page102
7.1<br />
Assign criteria in to categories for review and<br />
distribute.<br />
<br />
by 2 Nov<br />
7.2<br />
Sections to be reviewed as follows:<br />
Introduction and up to criteria 52<br />
Safety<br />
Throughput<br />
Dose distribution<br />
Imaging<br />
Sections to be reviewed and suggested changes<br />
made as follows:<br />
<br />
<br />
<br />
<br />
<br />
by 9 Nov<br />
<br />
<br />
<br />
<br />
<br />
<br />
Ensure specification is a question for the<br />
supplier i.e. produces an answer that can be<br />
evaluated.<br />
Remove any duplication/ensure consistency in<br />
statements.<br />
Identify if criteria are mandatory or scored and<br />
suggest types of responses/scores.<br />
Weightings.<br />
Ensure is supplier neutral.<br />
Degree of confidence.<br />
7.3<br />
Produce composite revised specification and<br />
circulate/discuss at second meeting to be held w/c<br />
12 Nov or w/c 19 Nov.<br />
Further iterations/revisions and discussions as<br />
required.<br />
<br />
Meeting date<br />
to be<br />
confirmed w/c<br />
12 Nov or w/c<br />
19 Nov<br />
8 Evaluation criteria and weightings<br />
Meeting of group with procurement advisors.<br />
Production of first draft evaluation criteria.<br />
Meeting of group and procurement advisors to<br />
work through draft.<br />
Further revisions and discussions as required.<br />
9 Further meetings<br />
Establish availability for further<br />
teleconference/meetings:<br />
<br />
<br />
<br />
w/c 12 Nov or<br />
19 Nov<br />
w/c 3 Dec<br />
Version4 Page103
w/c 12 Nov or w/c 19 Nov<br />
- Review revised technical specification<br />
- Brief procurement advisors on technical<br />
specification for 1 st draft evaluation criteria<br />
to be produced by procurement advisors<br />
- Brief procurement advisors on revised<br />
PQQ for procurement advisors to refresh<br />
PQQ documentation.<br />
w/c 3 Dec<br />
- Review first draft evaluation criteria<br />
- Develop weightings<br />
- Sign off refreshed PQQ<br />
Next meeting:<br />
Details to be confirmed – meeting/teleconference to be arranged for w/c 12 November or w/c 19<br />
November.<br />
Version4 Page104
Annex G<br />
University College London Hospitals NHS Foundation Trust (UCLH) and The Christie NHS<br />
Foundation Trust (The Christie)<br />
National <strong>Proton</strong> <strong>Therapy</strong> Service Programme<br />
Competitive Dialogue Procurement Law Issues and Conclusions<br />
1. Availability of the Competitive Dialogue Procedure<br />
On 31 March 2004 the European Parliament and the Council of Ministers adopted a new<br />
consolidated public/"classical" sector procurement Directive: Directive 2004/18/EC on the coordination<br />
of procedures for the award of public works contracts, public supply contracts and public<br />
services contracts (the "Consolidated Directive"). This Directive has been implemented in England,<br />
Wales and Northern Ireland by The Public Contracts Regulations 2006 (the "Regulations") which<br />
came into force on 31 January 2006.<br />
The Regulations specify the procedures to be followed by regulated procuring authorities<br />
("contracting authorities") in respect of the award of regulated public works, supply and services<br />
contracts. These procedures include those which are already well-established in public procurement<br />
practice: the open, restricted and negotiated procedures. A new contract award procedure was,<br />
however, also provided for: the competitive dialogue procedure.<br />
Key points to note:<br />
<br />
A contracting authority can always follow either an open or a restricted procedure as of right.<br />
The more flexible competitive dialogue and competitive negotiated procedures are only<br />
available, in contrast, where the relevant contracting authority could justify their use by<br />
satisfying particular conditions.<br />
The open and restricted procedures are, however, relatively inflexible and are, most<br />
significantly, subject to a prima facie prohibition on post-tender negotiations. Commercially<br />
this would often pose substantial difficulties for complex projects and may not always be<br />
conducive to producing the best value solution for a contracting authority.<br />
Whilst the (well-established) competitive negotiated procedure is still available under the<br />
procurement legislation, the risks of legal challenge in respect of use of this procedure are<br />
now significantly higher following introduction of the new competitive dialogue procedure.<br />
Version4 Page105
Both the EU Commission and the European Court of Justice are likely to take a very<br />
restrictive approach to the interpretation of the grounds for using the competitive negotiated<br />
procedure and the Commission is far more likely to take action than has historically been the<br />
case. In practical terms, this procedure should therefore now be avoided save in exceptional<br />
circumstances.<br />
<br />
Whilst the restricted procedure may be the technically safest procedure to use, and should<br />
therefore be used for relatively straightforward procurements, the competitive dialogue<br />
procedure will probably be the most suitable procedure for a contracting authority's complex<br />
procurements (where previously a competitive negotiated procedure would have been used)<br />
in view of the greater flexibility that it will afford.<br />
2. When may the Competitive Dialogue Procedure be Used?<br />
No automatic right of use<br />
The Regulations provide that a contracting authority shall use either the open or the restricted<br />
procedure in all circumstances except where it may use either the negotiated procedure or the<br />
competitive dialogue procedure on the basis of satisfying the particular conditions provided for the<br />
use of those procedures. Put another way, whilst a contracting authority can always use an open or<br />
a restricted procedure, and indeed is generally expected to do so, it may only use a negotiated or a<br />
competitive dialogue procedure when it can justify this on the basis of the particular conditions<br />
provided for the use of those procedures.<br />
Circumstances for using the competitive dialogue procedure<br />
As indicated above, a contracting authority has no automatic right to use the new competitive<br />
dialogue procedure. In order to do so, the authority will need to justify use of the procedure by<br />
satisfying the particular conditions provided for in regulation 18 of the UK Regulations which<br />
implements article 29 of the Consolidated Directive.<br />
Under the legislation, the competitive dialogue procedure may be used where:<br />
(i) a contracting authority wishes to award a "particularly complex contract"; and<br />
(ii) the authority considers that the open or restricted procedure will not allow the award of that<br />
contract.<br />
Version4 Page106
A "particularly complex contract" is specifically defined as being a contract in respect of which a<br />
contracting authority is not objectively able 8 to:<br />
(i) define the technical means 9 capable of satisfying its needs or objectives; or<br />
(ii) specify either the legal or financial make-up of a project or both.<br />
It is helpful to read this legal definition in the context of the first sentence of recital 31 of the<br />
Consolidated Directive which states that:<br />
"Contracting authorities which carry out particularly complex projects may, without this being<br />
due to any fault on their part, find it objectively impossible to define the means of satisfying<br />
their needs or of assessing what the market can offer in the way of technical solutions and/or<br />
financial/legal solutions."<br />
Recital 31 of the Consolidated Directive provides some limited guidance in respect of the type of<br />
projects that the EU legislature had in mind as being examples of appropriate cases for using the<br />
competitive dialogue procedure. The recital refers in particular to the implementation of:<br />
<br />
<br />
<br />
integrated transport infrastructure projects;<br />
large computer networks; and<br />
projects involving complex and structured financing, the financial and legal make-up of which<br />
cannot be defined in advance.<br />
The OGC, in its January 2006 Guidance on the Competitive Dialogue Procedure in the New<br />
Procurement Regulations appears to take a relatively wide approach to the interpretation of the<br />
requirements for technical, legal or financial complexity, although it does not analyse the conditions<br />
in any real detail.<br />
In respect of technical complexity, the OGC guidance makes the observation that "in many complex<br />
contracts, contracting authorities will seek to explore what the best solution might be to fit its needs".<br />
The guidance then concludes that "as a result, the contracting authority would not be able to define<br />
<br />
8 Regulation 18(1) and article 1(11)(c). Recital 31 of the Consolidated Directive, however, refers instead to contracting<br />
authorities finding it "objectively impossible" to define the matters referred to and this concept of "objective impossibility"<br />
(emphasis added) has been picked up by the EU Commission in its January 2006 Explanatory Note on the competitive<br />
dialogue (at section 2.1).<br />
9 Whether this is by reference to performance or functional requirements and/or by reference to technical specifications.<br />
Version4 Page107
the technical means of satisfying their needs at the outset and consequently the use of the<br />
competitive dialogue procedure is justified as technical complexity exists."<br />
The OGC guidance identifies the legal and financial complexity conditions as being particularly<br />
relevant to PPP/PFI projects, pointing out that for such contracts "it is often the case that the<br />
financial or legal make-up cannot be defined in advance, because issues such as risk allocation,<br />
how the project is going to be carried out and financed and who is going to be responsible for which<br />
services, will be the subject of discussions with the potential providers." The OGC considers that<br />
the competitive dialogue final text of the Consolidated Directive "fitted better with existing UK PFI<br />
practice" and that "the end result is a structured negotiated procedure, which is similar in many<br />
ways to the existing practice of letting PFI contracts."<br />
In its January 2006 Explanatory Note on the competitive dialogue, the Commission appears to have<br />
taken a relatively broad interpretation of the technical complexity condition. The Commission states<br />
that the most usual situation in which the condition will apply is where "the contracting authority<br />
would not be able to determine which of several possible solutions would be best suited to satisfying<br />
its needs." The example is given of a contracting authority wanting to create a connection between<br />
the shores of a river: it cannot determine whether the best solution would be a bridge or a tunnel,<br />
even though it would be able to establish the specifications for either possibility. The Commission's<br />
view is that the competitive dialogue would be justified in such a case on grounds of technical<br />
complexity.<br />
In respect of the legal or financial complexity condition, the Commission, like the OGC, states that<br />
this will frequently apply to PPPs. Although this will "very, very often" be the case, the Commission<br />
does point out that PPPs will not automatically be covered by the condition and that it is necessary<br />
to consider this on the merits of each procurement "even though that will most often be the case."<br />
3. Overview of the Structure of a Competitive Dialogue Procedure<br />
A competitive dialogue procedure can be structured in such a way as to reflect, to a very large<br />
degree, a previous "best practice" structured negotiated procedure. It offers a high degree of<br />
flexibility. That flexibility ends, however, at the point at which final bids are sought. Following<br />
submission of final bids, there is very little scope to make changes and certainly the practice of<br />
substantive preferred bidder negotiations which has been a feature of many negotiated procedures<br />
in the past would not be permissible under the rules.<br />
The procedure would begin by publication of a contract notice in the Official Journal of the European<br />
Union ("OJEU"). A deadline for expressions of interest is set in the OJEU notice which will normally<br />
be a minimum of 37 days from the date of despatch (as opposed to publication) of the notice. It<br />
Version4 Page108
may be possible to reduce this minimum period by up to 7 days if the notice is submitted on-line, on<br />
the Commission's website. It may also, however, be necessary to provide a longer period,<br />
depending on the circumstances of a particular procurement including, inter alia, its complexity and<br />
the volume of documentation involved.<br />
Interested parties will then undergo a qualification and selection stage – usually on the basis of<br />
information submitted in response to a Pre-qualification Questionnaire. At this stage, candidates<br />
will be assessed in respect of:<br />
<br />
<br />
<br />
Certain eligibility requirements – which may lead to either mandatory or discretionary<br />
exclusion;<br />
Their economic and financial standing; and<br />
Their technical or professional ability.<br />
Selected candidates (being a minimum of three) will then be invited to participate in a dialogue with<br />
the Authority during which all aspects of a proposed contract may be discussed. The Invitation to<br />
Participate in a Dialogue will, inter alia, set out the contract award criteria which will be taken into<br />
account in determining which offer is most economically advantageous. The relative weightings of<br />
the award criteria should be given.<br />
The purpose of the dialogue is to identify one or more solutions which are capable of meeting the<br />
Authority's requirements. The dialogue stage may be conducted in iterations during which the<br />
number of participants/solutions to be discussed is reduced.<br />
Once one or more solutions capable of satisfying the Authority's requirements has been identified,<br />
the Authority will declare the dialogue at an end and invite the submission of final bids. Following,<br />
perhaps, some very limited fine-tuning and confirmation of commitments, the Authority will reach its<br />
contract award decision. Before actually awarding the contract, it must send an Alcatel notification<br />
and relevant debrief information to all participants in the process and then provide for a minimum<br />
ten day mandatory standstill period. Within 48 days of contract award, a Contract Award Notice in<br />
prescribed form must be sent to the Office for Official Publications of the European Union.<br />
4. National <strong>Proton</strong> <strong>Therapy</strong> Service Programme Considerations<br />
The National <strong>Proton</strong> <strong>Therapy</strong> Service Programme procurement has a number of features that justify<br />
the use of the Competitive Dialogue procedure:<br />
Version4 Page109
Contracting authorities could be UCLH, The Christie or a new company formed as a special<br />
purpose vehicle. Additionally, there is a possibility that University Hospitals Birmingham NHS<br />
Foundation Trust may become a party to the procurement.<br />
Each of the potential contracting authorities wishes to retain the independence to contract<br />
with its own choice of supplier should it wish to do so, or to join forces with any of the other<br />
contracting authorities to place a joint contract with a supplier. This has necessitated dividing<br />
the procurement into Lots.<br />
The procurement seeks to secure complex equipment and services whose cost will run into<br />
the tens of millions of pounds, if not more.<br />
The scale of spend necessitates that numerous financial options need to be explored as a<br />
means of contracting, including renting, PFI, project financing and self financing.<br />
Both scanning and passive scattering based technology solutions could be used to satisfy<br />
the contracting authorities’ requirements, and the selection of the most appropriate method<br />
is a decision that requires analysis and discussion with suppliers before arriving at a<br />
conclusion.<br />
The procurement is therefore not straightforward, but complex. The contracting authorities are not<br />
objectively able to define the technical means capable of satisfying their needs and objectives at the<br />
outset and additionally they are not able to specify both the legal and financial make-up of the<br />
project. There are several possible solutions that could satisfy their joint needs. The procurement<br />
requires greater flexibility than that afforded by the open and restricted processes. The contracting<br />
authorities believe that it would simply not be possible to award a contract under the open or<br />
restricted procedures. For these reasons the competitive dialogue procedure will be followed.<br />
<br />
<br />
Version4 Page110
Annex H<br />
Joint <strong>Proton</strong> <strong>Therapy</strong> Equipment Procurement Group<br />
Terms of Reference<br />
1. Name Of Group: Joint <strong>Proton</strong> <strong>Therapy</strong> Equipment Procurement Group<br />
2. Accountable To:<br />
Technical and operational workstream, The Christie<br />
Phase 4 Programme Board, UCLH<br />
3. Aims And Purpose: To develop and manage the equipment procurement process, coordinating<br />
activities between The Christie and UCLH, making<br />
recommendations for approval within both trusts.<br />
4. Objectives And<br />
Responsibilities:<br />
Joint group<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
Develop robust equipment procurement strategy, documented<br />
and approved by:<br />
o Manchester <strong>Proton</strong> <strong>Therapy</strong> Programme Board<br />
o UCLH Phase 4 Programme Board<br />
Identify resources required for procurement<br />
Identify external advice required and potential costs<br />
Procure technical advisors, legal advisors, procurement<br />
advisors and other external advice where necessary<br />
Seek and co-ordinate advice from all advisors including<br />
procurement, legal and external technical advisors<br />
Agree procurement process, budget and timescales with<br />
Programme Manager(s) for UCLH and Christie<br />
Establish clearly defined rules of engagement with potential<br />
suppliers communicated and managed across all team<br />
members<br />
Make recommendations on strategy, documentation and<br />
equipment procurement outcome to Manchester <strong>Proton</strong><br />
<strong>Therapy</strong> Programme Board and UCLH Phase 4 Programme<br />
Board<br />
Ensure effective and proactive lines of accountability<br />
To co-ordinate input as required from key stakeholders and<br />
ensure effective communications as required<br />
Ensure timescales of process are coordinated with the wider<br />
programme<br />
Manage procurement of equipment to deliver on time and to<br />
budget<br />
Regularly report to Technical and Operational Workstream<br />
lead and UCLH Senior Responsible Officer<br />
Contribute to the development of UCLH and Christie FBCs as<br />
Version4 Page111
equired<br />
Develop and maintain a risk register throughout the duration of<br />
the programme<br />
Follow document management policy and instigate document<br />
management software as required to co-ordinate procurement<br />
5. Membership: Core Team Members<br />
<br />
<br />
<br />
<br />
Physics<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
Secretariat<br />
<br />
<br />
<br />
<br />
Wider team members<br />
Representatives from both trusts as required:<br />
Clinical<br />
Radiographer<br />
Engineer<br />
Capital planning<br />
Financial<br />
Advisors<br />
Version4 Page112
Joint procurement advisors<br />
Joint legal advisors<br />
The core team will be responsible for agreeing the procurement<br />
documentation including technical specification and evaluation,<br />
making recommendations to both Trusts’ steering groups on how the<br />
proceed.<br />
During the procurement of equipment phase the core team together<br />
with the wider team and advisors will undertake the procurement and<br />
make recommendations to both trusts boards on the outcome of the<br />
equipment procurement.<br />
6. Members’<br />
responsibilities<br />
1. Confidentiality<br />
All meeting material and supporting information, whether verbal or<br />
written, electronic or hard copy is deemed to be commercially<br />
sensitive and is shared on the basis of commercial in confidence.<br />
It is the responsibility of each member to ensure that information<br />
remains confidential. All non-Trust employee members will be<br />
required to sign a Non-Disclosure Agreement?<br />
2. Communicating within organisation<br />
It is the responsibility of each member to ensure that they<br />
communicate appropriate information within their organisation and<br />
represent views from within their organisation to the programme<br />
board.<br />
3. Decision taking<br />
It is expected that members will be authorised by their organisation<br />
to take decisions on behalf of their organisations within the<br />
boundaries of each organisation’s approval processes.<br />
4. Attendance<br />
Members are expected to attend meetings on a regular basis.<br />
Where this is not possible the programme board reserves the right<br />
to review the membership and seek alternative representation.<br />
Deputies may be sent with the agreement of the Joint Chair.<br />
7. Quorum To be quorate each meeting should have equal numbers of people<br />
represented from both trusts including at least one of the joint chairs.<br />
8. Frequency Of<br />
Meetings<br />
This will be determined by the schedule of work to develop the<br />
procurement strategy and documentation and then the requirements<br />
of the equipment procurement. To be not less than monthly in<br />
frequency.<br />
9. Governance and<br />
accountability<br />
The Joint Group will be accountable to the Technical and Operational<br />
Workstream (Christie) and Phase 4 Programme Board (UCLH). It will<br />
Version4 Page113
produce a monthly report covering progress, highlighting risks and<br />
issues.<br />
10. Escalation In the event of any material failure to agree escalation would first be to<br />
the SROs for UCLH and The Christie to reach mutual agreement. In<br />
the event that this was not possible it would be escalated to the Board<br />
of Directors of both trusts.<br />
11. Review Date<br />
The terms of reference for the Joint Group will be reviewed by each<br />
Trust’s Programme Board at <strong>OBC</strong>, FBC and at annual intervals in<br />
between.<br />
<br />
Version4 Page114
Appendix4C:ConstructionProcurementStrategy<br />
PBTConstructionProcurementStrategy<br />
Overviewandimplementationtimeline:<br />
ThePBTconstruction procurementstrategysetsoutthemain procurementroutesavailabletoUCLHand<br />
highlightstheprincipalconsiderationsassociatedwitheachofthesealternativesprocurementroutes.The<br />
strategypresentedherewassummarisedinthe<strong>Outline</strong><strong>Business</strong><strong>Case</strong>.<br />
The need to review the procurement route for the project has been driven mainly around the following<br />
considerations;<br />
• Theprojectdeliverytimelinetodeliveranoperationalbuilding(Q1–2018)<br />
• Levelofriskwhichcanbeacceptedortransferredadequately<br />
• Outturncostcertainty<br />
• Flexibility in terms of control of design interface by client & contractor design approvals<br />
necessary<br />
• Changewhichcanbeaccommodatedwithintheprojectorresultingcontract<br />
• Leveloftechnicalcompetencewithinthemarkettodelivertheproject<br />
• MeetingOJEUthresholdsandregulatoryrequirements<br />
<br />
All of the above have been considered in context of what can also be bought or transferred within the<br />
marketwithoutpayingsignificantpremium.<br />
UCLHasanorganisationhaveanextensivetrackrecord,experienceandresourcedteamofexpertswhoare<br />
capableofassessingandimplementingprocurementstrategies,mostrecentlyhavingsuccessfullycompleted<br />
thePhase3CancerCentreatanoutturncostapproaching£100m.<br />
Incontextofthisproject,thePBTteamhaveextensivelyexploredarangeofprocurementoptionsavailable<br />
alreadypriortowritingthistext.<br />
UCLH’sprocurementapproachhasbeendevelopedoverthepasttwoyearsinconjunctionwiththeChristie<br />
from bid submission. This has been done with the assistance of UCLH’s in house procurement team and<br />
appointedexternallegaladvisors, .<br />
<br />
.<br />
Inparticular,theconsiderationsoftheintendedprocurementstrategyhastakenintoconsideration:<br />
<br />
<br />
• Jointequipmentandbuildcontractsorasseparateprocurementworkstreams<br />
• Equipmentprocurementinisolation<br />
• Buildprocurementinisolation<br />
<br />
Version4 Page115
Design&Build<br />
formofcontract<br />
Thisprocurementroutewilldelivertheprojectby(Q1–2018)–Thisroute<br />
offersDesign&CostcertaintyandallowstheDesignProcesstoproceedin<br />
tandemwithboththeProcurementandConstructionProcess.It<br />
necessitatesanagreementupfrontofafixedpriceandaprogrammeand<br />
mayalsoinvolvethenovationornonnovationofsomeorallofthe<br />
presentdesignconsultantstotheMainContractor(fortheconstruction<br />
delivery).<br />
<br />
ToenablethefacilitytobeopenontimetheteamareproposingaDesign<br />
&Buildformofcontractwhereacontractorisselectedfromalistof3or4<br />
toproceedtopriceanddevelopthedesignfromthatpointtoapoint<br />
whereafixedpriceisagreedwhilstalsoseparateequipmentvendoris<br />
beingsought.Thefinalorderplacementismadewhenanequipment<br />
providersdetailsarefinalisedandcoordinatedwiththecontractor’s<br />
proposals.<br />
ManagedFormof<br />
contract<br />
Thisprocurementroutewilldelivertheprojectby(Q1–2018)–The<br />
managedformsofcontractinvolvesacontractorwhowillmanageand<br />
procureeachoftheindividualelementsofwork(workpackages),then<br />
placecontractswiththesesuppliersandtheemployertoexecutethe<br />
works,thecontractoralsothencoordinatestheirdeliveryonsite.<br />
<br />
<br />
Procure21+<br />
ProCure21isaframeworkwhichhasbeenorganisedbytheDHfor<br />
constructioncontractsthroughouttheNHS.Theframework,nowinits<br />
secondgeneration,isbasedoncollaborativeworkingthroughtheuseof<br />
theECCContract,OptionC.TheframeworkwasletinOctober2010andis<br />
duetorunfor6years.<br />
<br />
AstheframeworkhasalreadypassedthroughtheEUprocurement<br />
process,acontractorcanbeappointedwithoutnotificationintheOJEU.<br />
Becausetheframeworkisbasedonapreagreedpricingmechanism,no<br />
actualtenderprocessisrequired.Selectionismadefromtheframework<br />
Version4 Page119<br />
Single Point responsibility for<br />
the above and below ground<br />
(Constructionworks)<br />
Programme Certainty to<br />
deliver the building for<br />
requiredopening.<br />
Cost certainty to deliver the<br />
building once contract has<br />
beenawarded<br />
Retains a degree of control<br />
with client team through<br />
remaining design evaluation<br />
reviews with contractor(with<br />
or without novation of design<br />
team)<br />
<br />
MoretimefortheDesignTeam<br />
to refine the detail/coordinate<br />
andcompletethedesign.<br />
MoretimefortheDesignTeam<br />
toobtainEnduserinput,ifthe<br />
briefisemergingorunclear<br />
<br />
Easy and quick timescale to<br />
appointcontractor<br />
MoretimefortheDesignTeam<br />
to refine the detail/coordinate<br />
andcompletethedesign.<br />
MoretimefortheDesignTeam<br />
toobtainEnduserinput,ifthe<br />
briefisemergingorunclear
contractors,referredtoasPrincipalSupplyChainPartners(PSCPs),solely<br />
onthebasisofquality.<br />
Todothis,aschemeinformationpackisemailedtothePSCPs,inresponse<br />
towhichPSCPswhowishtobeconsideredsubmitanexpressionof<br />
interest.TheNHSclientselectsashortlistofPSCPsandinvitesthemtoan<br />
openday,followingwhichtheyattendaninterviewandaselectionis<br />
made.Thisprocesstakesthreetofourweeksalthough,insome<br />
circumstances,aPSCPcanbeappointedquickerthanthis.<br />
Theearlyappointmentofthecontractorhasbothprogrammebenefitsand<br />
enablesconstructioninputtothedesignprocess,thusinfluencing“build<br />
ability”.<br />
UnderProCure21+,theTrustandPSCPagreeaTargetPrice.Shouldthe<br />
projectcostlessthanthisfigure,thefirst5%ofthedifferenceissplit50/50<br />
betweentheTrustandPSCP.Anysavingbelowthislevelgoes100%tothe<br />
Trust.Shouldtheprojectcostmore,theclientTrustonlypaystheTarget<br />
Price.ForthisreasontheTargetPriceunderProcCure21+isnormally<br />
referredtoastheGuaranteedMaximumPrice(GMP).<br />
TheGMPisestablishedbasedonframeworkratesandaprocessofopen<br />
bookmarkettestingofworkspackages.<br />
ThisreportconsidersthatProCure21+isnotthemostappropriate<br />
frameworkforprocurementoftheworksduetothelimitednumberof<br />
Procure21members,lackofcompetitioncomparedtoopenmarket<br />
tenderingandhighoverheadandprofitcostswhichexistunderthis<br />
arrangement.<br />
IESEFramework<br />
TheImprovementandEfficiencySouthEast(IESE)frameworksupports<br />
councilsandpublicsectororganisationsinthesoutheastincludingLondon<br />
Authorities.Assuch,UCLHareeligibletoutilisetheframework.The<br />
frameworkwasoriginallyplacedinJuly2007.<br />
TheIESEframeworkisbasedontheprincipleofatwostagetender<br />
process.Otherthanareductionintimescales,amajoradvantageofthis<br />
approachistheearlyinvolvementofthecontractorwhocancontributehis<br />
constructionexpertisetothedesignprocess,thusinfluencing‘buildability’<br />
costandtimescales.AnadditionalbenefitofIESEisthatitisnotbasedona<br />
specificformofcontractenablingtheTrusttoselectasappropriate.<br />
<br />
Version4 Page120<br />
Easy and quick timescale to<br />
appointcontractor<br />
MoretimefortheDesignTeam<br />
to refine the detail/coordinate<br />
andcompletethedesign.<br />
MoretimefortheDesignTeam<br />
toobtainEnduserinput,ifthe<br />
briefisemergingorunclear<br />
Nosetordefinedcontractand
Competitive<br />
Dialogue<br />
Equipment<br />
Toappointacontractor,aprojectoutlinewouldbedevelopedbythe<br />
designteamandissuedtothetencontractorsbytheframeworkmanagers.<br />
Thecontractorsrespond,demonstratingtheirintentviaanexpressionof<br />
interest.Fromthesubmissions,theframeworkmanagersdrawupa<br />
shortlistofcontractors.<br />
Thenextstageoftheprocessinvolvesaminitenderwherebythe<br />
shortlistedcontractorsareinvitedtosubmittheirbidsonthebasisof<br />
informationdevelopedbythedesignteam.Ratesforprelims,overhead<br />
andprofitwereconfirmedwhenthecontractorswereappointedtothe<br />
frameworkwhichthecontractorsutilisewhenbuildingthepreliminaries<br />
costsforevaluationinminicompetition.<br />
Withintheminitendersubmissions,contractorsarerequired<br />
todemonstratetheirprojectspecificapproach,competenciesandkey<br />
initialcommercialinformation.Predominantlyevaluationandselectionofa<br />
contractorisonthebasisofqualityandvalueratherthanlowestprice,on<br />
70%quality30%commercialbasis.<br />
Followingtheminitenderthechosencontractorwouldbeappointedona<br />
preconstruction agreement to develop the design, depended on the<br />
procurementrouteandformofcontractandthenenterintoaprocessof<br />
open book market testing of works packages to arrive at a Target Price.<br />
Thisisthenfirmedupaftertheopenbooktenderstoafixedcontractoffer.<br />
On arrival at the target price, the Trust would appoint the contractor to<br />
deliver the project. If the project were aborted at this stage the Trust<br />
wouldbeliableforanycontractorcostsincurred<br />
Inarapidlyadvancingtechnologywebelieveitisextremelyimportantto<br />
understand what the equipment manufacturers can offer in terms of<br />
delivery against or exceeding our requirements and as such we have<br />
concluded the most appropriate procurement approach is to use<br />
competitivedialoguefortheequipmentonly.<br />
<br />
The following longlist of options for the procurement of PBT equipment<br />
hasbeenconsideredinarrivingatthisdecision:<br />
A single procurement with one lot procurement for purchase of<br />
equipmentfromonelotsuppliertoUCLHandtheChristie.<br />
Asingleprocurementwithtwoseparatelotstosupplyequipment<br />
forUCLHandtheChristie<br />
Asingleprocurementwiththreelotsasfollows:<br />
Version4 Page121<br />
<br />
thereforepotentiallyflexibleto<br />
contractterms<br />
Relatively easy and quick<br />
timescale to engage with<br />
market<br />
GivesmoretimefortheDesign<br />
Team to refine the detail /<br />
Coordinate and complete the<br />
design as a result of feedback<br />
on options and offers from<br />
market.<br />
MoretimefortheDesignTeam<br />
toobtainEnduserinput,ifthe<br />
brief is emerging or unclear,<br />
which the PBT element is as<br />
opposed to the infrastructure
SupplyofPBTtobothsites;<br />
SupplyofequipmenttoUCLHand<br />
SupplyofequipmenttoTheChristie.<br />
Completelyseparateprocurements.<br />
Thispaperconcludesthatonesupplierispreferabletotwosuppliersdueto<br />
thepotentialbenefitsofaconsistentsystemintwositesandthepotential<br />
discountsavingsofjointprocurement,althoughitshouldbenotedthatthe<br />
financialbenefitsarenotyetavailabletobeevidenced.TheTrustsandDH<br />
willundertakefurtherinvestigationstoascertainwhether:<br />
Anjointevaluationcriteriacanbedevelopedtomeettheneedsof<br />
bothsites;<br />
Equipment suppliers can deliver solutions that meet the<br />
restrictionsofeachsite;<br />
Themarketcandeliversuchasolutioninsimilartimescales;and<br />
It can be shown that this represents the optimum solution in<br />
termsof,forexample,valueformoney.<br />
Scopeofequipmentprocurement<br />
Theassumptionisthattheprocurementwillbefortheequipmentplusa<br />
maintenance service (currently expected to be for a minimum of five<br />
years).<br />
A managed service has been discounted as the service needs to be<br />
integratedintoeachFoundationTrustservicedeliverystrategy.<br />
Version4 Page122<br />
<br />
works which are fairly well<br />
defined.<br />
Nosetordefinedcontractand<br />
thereforepotentiallyflexibleto<br />
contract terms which the<br />
suppliers understand and can<br />
reduceriskpremiums
Thediagramillustratedbelowhighlightsthemajorityofdifferingtypesofprocurementroutesandresulting<br />
contractopportunitieswhichexisteachwithcompetingcharacteristicswithregardtodesignflexibility,<br />
programmecertainty,costandchange:<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
NOVATIONCONSIDERATIONS<br />
The Design & Build route does require that there are considerations and further discussions and<br />
agreementsheldwithregardtothepossiblenovationofthedesignteamtothemaincontractorandhow<br />
thisstrategybestfitstheclientaspirationsandrequirements.<br />
Ifthewholedesignteamisnovated(toworkfor)thecontractor,theclientusuallyhasconcernsthatany<br />
controlhehadoverthedesignteaminensuringthatqualitystandardsweremetduringtheconstruction<br />
phasewilldisappearwhenthecontractorbecomesthedesignteam’snewemployer.<br />
Thisconcerncanbeeasilyovercomebyintroducingintoanynovationagreementtherequirementofthe<br />
designertocompleteonaregularbasisareportfortheoriginalemployerthatconfirmsorotherwisethat<br />
in the opinion of the consultant the works are being designed or constructed in accordance with the<br />
specificationrequirements.Thishasbecomeknownasa“whistleblower”clause.<br />
There can also be concerns both from the design team and the main contractor that there may be an<br />
incompatibilitybetweentheirseparatestyles,whichmeansthatneitherpartyrelishestheopportunityto<br />
work with each other. The main contractor may have practices with which he has a preference to use<br />
aheadofthedesignteambeingproposed.Inthesecircumstancestherearenosetrulesbutwhathastobe<br />
consideredandproposedisascenariowhereallpartiestothecontractfeelcomfortable.<br />
Itisnormalpractiseitiscommonthatifaconsultantisnovatedthenthereisapreferencethattheybe<br />
novated as a team and that their novation agreements should contain the “whistle blower” clause as<br />
described above and if proposed would be a reasonable and workable solution. The contractual<br />
relationshipsarenormallyalteredbetweenthedesignteam/contractorandEmployeronceNovationhas<br />
occurred.<br />
CHANGECONTROL<br />
AsystemofChangeControlmustbemaintainedifcontractsareeffectivelymanagedsothatanydeviations<br />
tothebrieforcontractisunderstoodandsignedoffpriortoimplementation.ThePBTisnodifferentandit<br />
is envisaged that this protocol will continue throughout the duration of the project. The system will<br />
Version4 Page123
Construction works will not be included in the lot as it is considered important to reduce complexity to<br />
better manage the project specific cost and timescales risks under a Design & Build arrangement with<br />
advancedemployers’requirementsreflectingtheirdetailedrequirements,whichwilleffectivelyresultina<br />
highdegreeofprogramme,costandqualitybeingestablishedattheoutset.<br />
<br />
<br />
Version4 Page126
Appendix4D:CabinetOfficeICTSpendControlForm(v2.18)<br />
Cabinet Office ICT Spend Control Form (v2.18)<br />
<br />
ThepurposeofthisformistoprovideanoverviewofproposedICTexpendituretoaidapprovalthroughtheCabinet<br />
OfficeITControlProcess.Thisformshouldmakereferencestoandbesupplementedbyrelevantdepartmental<br />
documents(e.g.latestbusinesscases).<br />
<br />
ThisformshouldbereadinconjunctionwiththeCabinetOfficeControlGuidanceavailablehere<br />
<br />
Forallqueriesorfeedbackrelatingtothiscontrolpleasecontactyourdepartmentalleadforthecontrols,alternatively<br />
contacttheCabinetOfficeat:<br />
Unclassified:ictfutures@digital.cabinetoffice.gov.uk<br />
Restricted:ictspendapproval@cabinetoffice.gsi.gov.uk<br />
<br />
Earlyengagementbeforeanapprovalisrequiredwillalwaysimprovethechancesofasuccessfuloutcome.This<br />
formisintendedtobedevelopediterativelyfromearlyengagementwiththeCabinetOfficeuntilthefinalspend<br />
requestissubmitted.ItincludesquestionstosupportapprovalofothercontrolssuchasStrategicSuppliers.<br />
<br />
FormVersionNumber:<br />
V 0.0<br />
Organisational information<br />
Organisationname: UCLHNHSFoundationTrust<br />
Parentdepartment: N/A<br />
<br />
Organisationapprovals<br />
TrustBoardapprovalofthe<strong>Outline</strong><strong>Business</strong><strong>Case</strong>andFull<strong>Business</strong><strong>Case</strong><br />
DepartmentofHealthapprovalthe<strong>Outline</strong><strong>Business</strong><strong>Case</strong>andFull<strong>Business</strong><strong>Case</strong><br />
HMTreasuryapprovalofthe<strong>Outline</strong><strong>Business</strong><strong>Case</strong>andFull<strong>Business</strong><strong>Case</strong> <br />
Monitorthe<strong>Outline</strong><strong>Business</strong><strong>Case</strong>andFull<strong>Business</strong><strong>Case</strong><br />
Department information<br />
<strong>Business</strong>activity/Projectname: <br />
Referencenumber(ifknown): enterreference.<br />
SRO: entername.<br />
Mainpointofcontact: entername.<br />
Mobile/phone: enternumber.<br />
Email: enteremail.<br />
Version4 Page127
PBTwilldelivertheseobjectives:<br />
TheNationalRadiotherapyAdvisoryGroupReport,2007<br />
TheCancerReformStrategy,2007<br />
AframeworkforthedevelopmentofPBTserviceinEngland,2009<br />
ImprovingOutcomes:Astrategyforcancer,2011<br />
TheDHandNHSEnglandhaveworkedwithTheChristieandUCLHtodevelopaServiceandInvestmentFramework<br />
(SIF).ThisisacooperationagreementbetweentheTrusts,theSecretaryofStateforHealth,andNHSEnglandthat<br />
providesthegovernance,clinical,technical,commercial,procurementandfinancialstructureswithinwhichthe<br />
servicewillbedevelopeduptoapprovaloftheFBC.<br />
<br />
Isthisspendassociatedtoaproject/programmeincludedontheGovernmentMajorProjectPortfolio?Yes<br />
<br />
Whatstageistheproject/programmerelatedtothisrequestatinitslifecyclee.g.StartingGate,SOC,<strong>OBC</strong>,FBC<br />
TheNHSEnationalprogrammehasdevelopedaSOC,approvedbyDHCIB/HMT.<br />
Thisisan<strong>OBC</strong>forthedevelopmentofaservicebasedatUCLH.<br />
<br />
Highlevelspendbreakdownbystage(ifknown):Notknown<br />
<br />
Start<br />
date<br />
End<br />
date<br />
Stage<br />
Spendalready<br />
committed(£k)<br />
Spendsoughtfor<br />
approval(£k)<br />
Spendyettobe<br />
confirmed(£k)<br />
Predesign <br />
Design <br />
Build <br />
Test <br />
Implement <br />
Run <br />
Total <br />
Version4 Page130<br />
Totalspend<br />
forecast(£k)<br />
Requirements & Options:<br />
<br />
Pleaseexplainoptionsconsidered(includingdonothing).Thiswillinclude:<br />
Whataretheuseroutcomesthatthisinvestmentissupporting?<br />
Howdoesthistransfertheburdenfromthestatebyempoweringtheuser?<br />
Howdoesthisfitinwiththedepartment’soverallinformationandtechnicalarchitectureobjectivesanddesign?<br />
Ifreplacinglikeforlike,pleaseprovidecostpertransactioncomparisons<br />
<br />
ThealternativeoptionstodevelopingaPBTserviceare:<br />
Providesuboptimaltreatments(e.g.radiotherapy)topatients<br />
Treatalimitednumberofpatientsoverseas<br />
TheDHproducedaSOCwhichwasapprovedbyHMTreasuryon12Feb2012.Thisshowsthedevelopmentofa<br />
nationalPBTservicewillrepresentgoodvalueformoney.<br />
Procurement & commercial strategy:<br />
Itisunderstoodthatsomeofthisinformationmaynotbeknowatthecurrentactivitylifecycle,pleasecompletewhat<br />
isknown.<br />
<br />
Whatprocurementvehicleislikelytobeused(e.g.OJEU,Framework,existingsupplier)?<br />
TheprocurementvehiclefortheICTelementoftheprojecthasyettobedecided,thisisinlinewiththeprojectplan.<br />
TheICTequipmentsupplierscannotbeprocureduntiltheprotonbeamtherapyequipmentisselected;ourlatest<br />
programmeplanidentifiesthatthisisduetobecompletedinOctober2014.Thereforetoensurethatthemost
commerciallyappropriatevehicleisselectedprocurementshouldbedoneonatimelybasis.Detailedspecifications<br />
ofICTrequirementswillbeworkeduppost<strong>OBC</strong>approval,whichisplannedforJune2013.<br />
Thereareonlyalimitednumberofsuppliersforthetreatmentspecificsoftware,andthereforeOJEUislikelytobe<br />
theprocurementroute.However,ifthereareexistingframeworksinplaceitispossiblethatthesewillbeutilized<br />
wheretheyofferadvantagesoveranopenprocurementroute.ItislikelythatforgeneralICTaframeworkwillbe<br />
utilized<br />
<br />
PleaselistbelowtherelevantFrameworkspursuanttowhichrelevantsolutions/servicesarelikelytobeprocured.<br />
ForgeneralICTitislikelythattheGPSframeworkwillbeused<br />
<br />
LikelyprimaryITsupplier(s)(ifknown):<br />
Notknownatthisstage<br />
<br />
Whoistheexistingsupplier(ifapplicable):<br />
N/A.Thisisanewservice<br />
<br />
SOC<strong>OBC</strong>:howdoyouintendtoensurecompetitivetensionisbuiltintotheprocurementtoassistindetermining<br />
ValueforMoney?<br />
<br />
FBC:howwasrealcompetitivetensionbuiltintotheprocurementtoassistindeterminingvalueformoney?If<br />
competitivetensionwasnot,whynot?<br />
Allopportunitieswillbeexploredtodelivervalueformoney<br />
<br />
Howisthespendsplitbetweensuppliers?(Filltablebelowifknown):Notknown<br />
Supplier Spend(£m) Duration(months Activity<br />
<br />
<br />
Total <br />
<br />
Isthecontractopenbook,ifnotwhynot?<br />
<br />
Contractstructurenotknownatthisstage<br />
Whatisthepricingbasis?(fixedprice/fixedpriceincentive/costplusfixedfee/costplusincentivefee/T&Metc.)?<br />
<br />
Pricingstructurenotknownatthisstage<br />
Howhaveyoumanaged/doyouintendtomanagetheriskof,orexposureto,nondelivery,slippage,oroverspendby<br />
thesupplier?<br />
ProgrammeBoardestablishedtomanagecontractandprojectrisks<br />
Legaladvisorsappointedtoensurerisksappropriatelyapportionedincontactandanyongoingcontractualissues<br />
<br />
Pleaseprovideusthatratecardbeingused,andtheaveragedayrate(onshore/offshore):<br />
<br />
Notknownatthisstage<br />
HowdotheratescomparewithrateselsewhereintheDepartment?Pleaseprovideabreakdown.<br />
Version4 Page131
Notknownatthisstage<br />
WhatchecksandbenchmarkinghastheDepartmentdonetoconfirmthepriceiscompetitive?Pleaseprovidedetailed<br />
evidence.<br />
<br />
Notknownatthisstage<br />
Whatdiscounthasbeenappliedacrosslabour,software,andhardware?<br />
<br />
Notknownatthisstage<br />
Pleaseprovideuswithabreakdowninanylicensingcostsassociatedwiththisproject:<br />
<br />
Notknownatthisstage<br />
Pleaseprovideuswithabreakdowninanytransitioncostsassociatedwiththisproject:<br />
<br />
Notknownatthisstage.<br />
Canyoupleasefilloutthetablebelow:Notknownatthisstage<br />
<br />
Supplier<br />
Total<br />
spend<br />
(£m)<br />
Average<br />
Dayrate<br />
(£)<br />
Gross<br />
margin<br />
(%)<br />
Net<br />
margin<br />
(%)<br />
Discount<br />
applied<br />
Onshore/offshore<br />
Start<br />
date<br />
Labour <br />
Hardware <br />
Software <br />
Total <br />
Policyrelevance&ITStrategicandSIPAlignment<br />
ThissectionisakeycomponentofthisSpendControlFormasitwillenablethedepartmentandCabinetOffice<br />
determinethelevelofpolicyandSIPcompliance.<br />
Duration<br />
PleasecompletethissectionalongsidetheExcelSIPCompliancespreadsheet.Pleaseusethissectiontoaddcomments<br />
inrelationtothecompletedSIPcompliancespreadsheet.<br />
HowdoesthisspenddelivertheGovernmentICTPolicyobjectivesinaccordancewiththeStrategicImplementation<br />
Plan,specificallyobjectivesof:<br />
AlignmentofITwiththe<strong>Business</strong><br />
EconomicGrowth<br />
CreatingaCommonICTInfrastructure<br />
UsingICTtoDeliverChange<br />
<br />
N/A<br />
<br />
LinktoSIP:http://www.cabinetoffice.gov.uk/content/governmentictstrategystrategicimplementationplan<br />
Version4 Page132
StrategicImplementationPlanDepartmentalProjectCompliance<br />
EachsectionlistedbelowispartoftheCabinetOfficeITStrategicImplementationPlan.<br />
Pleaserateyourcompliancewiththesestrategicgoalsusingthedropdownboxes<br />
1. Alignment of IT with the <strong>Business</strong><br />
<strong>Business</strong> <strong>Case</strong><br />
Delivers Cashable<br />
Savings<br />
Delivers better public<br />
services<br />
Transparency Policy<br />
Not Relevant Not Relevant Compliant Not Relevant<br />
2. Economic Growth<br />
ASK ICT – Asset and<br />
Services<br />
Knowledgebase<br />
Demonstrates Open<br />
Source level playing<br />
field<br />
Procurement<br />
Open procurement<br />
process<br />
Complies with £100m<br />
ceiling<br />
Avoids commercial<br />
lock-in and retains<br />
competitive, open<br />
market<br />
Validation via<br />
independent<br />
benchmarking and<br />
market testing<br />
Contributes to<br />
growing the role of<br />
SMEs<br />
Focuses on<br />
capabilities rather<br />
than infrastructure<br />
acquisition<br />
Agile Capability<br />
Not Relevant Not Relevant Not Relevant Not Relevant Compliant Not Relevant Not Relevant Not Relevant Not Relevant Not Relevant Not Relevant<br />
3. Creating a Common ICT Infrastructure<br />
Open Standards<br />
Reference<br />
Architecture<br />
Open technical<br />
standards<br />
Cloud computing and<br />
applications store<br />
Public services<br />
network<br />
Data centre<br />
consolidation<br />
End-user device<br />
strategy<br />
Green ICT Information strategy<br />
Privacy, security and<br />
identity policy<br />
Risk management<br />
regime<br />
Not Relevant Not Relevant Not Relevant Not Relevant Not Relevant Not Relevant Not Relevant Not Relevant Not Relevant Not Relevant Not Relevant<br />
4. Using ICT to Deliver Change<br />
Channel Shift<br />
Open Application<br />
Programme<br />
Interfaces (APIs)<br />
Contributes to big<br />
society with open<br />
APIs and open data<br />
Online government<br />
consultation<br />
Social media<br />
Not Relevant Not Relevant Not Relevant Not Relevant Not Relevant<br />
End of Sheet<br />
Data Validation Below - Please leave<br />
Compliant<br />
SomeEvidence<br />
LittleEvidence<br />
NoEvidence<br />
NotRelevant<br />
AwatingInformation<br />
Version4 Page133
Appendix4E:PBTMilestoneTracker<br />
Version4 Page134
Communications,HR,Finance,etc.)<br />
UCLHStaff<br />
StaffUnionsandassociations<br />
Serviceuserspatients<br />
TheChristieNHSFoundationTrust<br />
EDH&RNTNEStaff<br />
LocalAuthority–CamdenCouncil<br />
Local Authority – Town Planning and<br />
BuildingControl<br />
EnvironmentAgency<br />
MetropolitanPolice<br />
TransportforLondon<br />
LocalResidents’Association<br />
Local<strong>Business</strong>es<br />
CharitiesandtheVoluntarySector<br />
Publicgeneral<br />
Commissioners<br />
GP’s<br />
UniversityCollegeLondon<br />
Other Universities and Academic<br />
Institutions<br />
Media–nationalandlocal<br />
LocalMP’s/Politicians<br />
PBTContractor/Operator<br />
DesignTeam<br />
Projectcontractors<br />
C<br />
C<br />
C<br />
A<br />
C<br />
C<br />
B<br />
B<br />
B<br />
B<br />
C<br />
C<br />
C<br />
C<br />
A<br />
D<br />
B<br />
B<br />
C<br />
B<br />
<br />
A<br />
A<br />
A<br />
<br />
Stakeholder analysis of the above individuals/groups will be undertaken to ascertain the<br />
following:<br />
• Whatinterestdotheyhaveintheproject?Isitpositiveornegative?<br />
Version4 Page137
UCLH<br />
<strong>Outline</strong><strong>Business</strong><strong>Case</strong><br />
STAKEHOLDERACTIONPLANWORKSHEET<br />
STAKEHOLDER<br />
NAME<br />
COMMUNICATIONS<br />
APPROACH 1 <br />
KEY INTERESTS &<br />
ISSUES<br />
CURRENT<br />
STATUS 2 <br />
DESIRED<br />
SUPPORT 3 <br />
DESIRED PROJECT<br />
ROLE(ifany)<br />
ACTIONS<br />
DESIRED (if<br />
any)<br />
MESSAGES<br />
NEEDED<br />
ACTIONS &<br />
COMMUNICATIONS<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
1 Manageclosely/Keepsatisfied/Keepinformed/Monitor<br />
2 Advocate/Supporter/Neutral/Critic/Blocker<br />
3 High / Medium / Low<br />
Version4 Page139
Itisrecognisedthatwithinoverallstakeholdergroupsthereare‘subgroups’,andthesesubgroupsmaywellhavedifferingprioritiesandinterests.Itisanticipated<br />
thattheactionplanscanbenuancedtoaccommodatethesedifferences.<br />
<br />
(A)KeyPlayers<br />
These are the most important Stakeholders – they have high power and high interest in UCLH and its activities. Such stakeholders need to be involved in all<br />
relevantdevelopmentsandcouldhaveaconsiderableinfluenceoverthefuture.<br />
<br />
(B)KeepSatisfied<br />
TherelationshipwithstakeholdersingroupBcanbedifficult.Inthisgrouparefoundnationalrepresentativeorlegislativebodies.Theybehavepassivelymostof<br />
thetime,butcanexertanenormous impactontheTrust. Itis thereforenecessarytoanalyzepotentialintentions andreactionsofthesegroupsinallmajor<br />
developmentsandtoinvolvethemaccordingtotheirinterests.<br />
<br />
(C)KeepInformed<br />
StakeholdersingroupChaveahighinterestintheorganisationanditsactions.However,theyhavelimitedmeanstoinfluence.Despitetheirlowerinfluence,such<br />
stakeholderscanbevaluablealliesinimportantdecisions.Therefore,itisadvisabletokeeptheminformedabouttheissuestheyareinterestedin.<br />
<br />
(D)MinimalEffort<br />
StakeholdersingroupDhavelittleinterestinUCLH,orthepowertoexertmuchimpact.Itis,therefore,appropriatetokeepthesegroupsinformed,butnotinvest<br />
toomucheffortintothem.<br />
<br />
StakeholderManagement<br />
<br />
The overall approach to Stakeholder Management needs to be structured and supported, This will include the identification of clear leads responsible for<br />
maintainingrelationships–andpersonalandteamobjectivestoreflectthis.<br />
<br />
Differentialstrategiesneedtobedeployedtotargetspecificrelationshipswithstakeholders,reflectingtheneedtopositivelymaintainsomerelationships,develop<br />
newrelationshipsand/orreorientorextendexistingones<br />
<br />
Aregularprogrammeofcommunications,ledbytheHeadofCommunications,whichwillraiseawareness,enhancethereputation,andimprovetheperceptionof<br />
UCLHanditsPhase4DevelopmentProgrammewillbeimplemented.<br />
<br />
<br />
<br />
Version4 Page140
<strong>Outline</strong><strong>Business</strong><strong>Case</strong><br />
<br />
<br />
Version4 Page153
<strong>Outline</strong><strong>Business</strong><strong>Case</strong><br />
Appendix6D:ContingencyintheeventofAccelerator/PBTCentreFailure<br />
<br />
Contingency in the event of Accelerator/PBT centre failure<br />
The purpose of this paper is to set out the contingency arrangements for patients under going PBT<br />
in the UK in the event that one of the national service’s two centres is unavailable.<br />
The paper considers the impact of whether site availability is planned (servicing) or unplanned<br />
(accelerator failure, power outage, gantry issues, planning system failures or other serious<br />
untoward incidents) and where in the treatment pathway the patient is. The paper also looks at the<br />
impact of compatibility of referral systems and technology solutions and their affect on contingency<br />
planning.<br />
1. Reduction in available capacity<br />
Scenarios<br />
Planned<br />
Downtime<br />
(Servicing)<br />
Contingency<br />
Modelling of this scenario can be done well in advance with a prioritised indication list<br />
for centre that will continue functioning, with liaison between centres well in advance of<br />
the proposed servicing schedule.<br />
No new patients accepted at facility to be serviced. This process needs to commence<br />
over a month prior to servicing, with the centre not being serviced also required to<br />
reduce the number of new starters – prioritising clinically those patients referred to their<br />
centre.<br />
Planned completion of treatments at the affected centre prior to servicing.<br />
Waiting list of patients to be sent to facility continuing treatment and new referrals added<br />
to that waiting list. Patients to be treated at continuing facility to be prioritised until<br />
capacity is reached (Clinical criteria to be established).<br />
Patients not prioritised for treatment at continuing facility to be triaged for<br />
commencement after servicing complete, some patients (given timescales) may require<br />
transfer to photon plans or referral abroad (clinical criteria to be established).<br />
Unplanned<br />
Downtime<br />
(New<br />
Patients)<br />
Mitigation plan as for planned downtime.<br />
Daily review of waiting lists required until confirmed date for reopening and<br />
patients/referrers kept informed.<br />
Unplanned<br />
Downtime<br />
(Patients<br />
on<br />
treatment)<br />
Patients on treatment at downed facility nearing completion of treatment to be changed<br />
to emergency photon plans until completion.<br />
Patients mid treatment converted to photon plans in the interim and prioritised for<br />
continuing <strong>Proton</strong> <strong>Beam</strong> treatment at functioning facility.<br />
Patients at start of treatment at downed facility starting treatment, clinical decision to be<br />
made to stop completely and restart as a new patient (criteria to be established), or<br />
Version4 Page154
<strong>Outline</strong><strong>Business</strong><strong>Case</strong><br />
conversion to a photon plan with the expectation of continuing treatment with protons at<br />
functioning facility (clinical criteria to be established).<br />
<br />
Issues of note when considering contingency for particular groups of patients are:<br />
The patients that would benefit the most from protons (i.e. the current indication list who we are<br />
currently sending abroad) would take priority in being transferred. However, even a small transfer<br />
time might mean some patients will require conversion to photons at the downed site as some<br />
tumours require treating in exceptionally short timescales (e.g. Medulloblastoma etc.).<br />
The duration of the repair of the beam would also affect how new referrals to the proton centre<br />
were dealt with. If the repairs were to be lengthy (?weeks) then we would have to prioritise referrals<br />
to the single working centre. For prolonged periods of downtime there is the potential for some<br />
clinical staff temporarily supporting the other centre in planning prioritised patients.<br />
2. Compatibility of referral systems and technology solutions<br />
The existence of two UK proton beam therapy facilities, regardless of technology solution, allows<br />
high priority patients (current indication list) to be prioritised within a national service and to access<br />
timely treatment in the UK.<br />
Any contingency will be limited by the capacity of the remaining centre and the logistics of<br />
transferring patients. To reduce the risk of untimely delays in transferring patients, the data<br />
systems must allow easy transfer of patient information (joint referral storage and waiting list<br />
systems), including patient records, imaging and proton plan (if available) for reference. Both<br />
centres using the same referral system will mitigate much of this.<br />
The timely transfer of patients is less sensitive to the type of technology, planning and<br />
immobilisation systems at each site. In the case of patients who do not have PBT plans at the<br />
downed facility or when servicing is scheduled, there would be no difference in timeliness to<br />
treatment whether there were different technologies or the same technology at both centres. For<br />
those patients with PBT plans or have started treatment, or where there is unexpected failure of<br />
service, the limiting factor to transfer will be the capacity at the functioning centre (which will need<br />
to wind down low priority new starters in any event). This will give sufficient time for those<br />
prioritised transferred patients to be planned at the functioning centre.<br />
<br />
<br />
Version4 Page155
<strong>Outline</strong><br />
<strong>Case</strong><br />
<strong>Business</strong><br />
Guidance for Completion of the RPA<br />
<br />
What is the RPA for?<br />
This version of the Risk Potential Assessment (RPA) is designed to provide a standard set<br />
of high-level criteria for assessing the strategic risk potential of programmes and projects,<br />
and of emerging policies and initiatives that are expected to be delivered through a<br />
programme or project in the future.<br />
The RPA is used to initiate a Starting Gate, a Project Assessment Review (PAR) or<br />
an OGC Gateway review, by helping to determine who should arrange and manage a<br />
review and decide on the make-up of the review team. This RPA replaces the earlier<br />
2009 RPA previously used only for OGC Gateway reviews.<br />
Once agreed the completed form should be sent to the Departmental Assurance<br />
Coordinator (DAC)910 for onward transmission to the Cabinet Office Major Projects<br />
Authority (MPA), where appropriate.<br />
This assessment is an indicator of risk potential and is not an exhaustive risk analysis<br />
model. However, it can be the starting point for a more exhaustive risk assessment. The<br />
RPA enables a conversation to be had about the risks and responsibilities for delivery of<br />
a programme or project, and its visibility, reporting and assurance in a wider portfolio<br />
management context. The RPA can also help to identify areas where specific skills sets,<br />
commensurate with the level of programme or project complexity, may be required.<br />
How to complete this RPA<br />
Assurance reviews are applicable to a wide range of change programmes and projects,<br />
including policy driven, business, property/construction, ICT enabled or<br />
procurement/acquisition-based change initiatives.<br />
The RPA should be completed as early in the life of a change initiative as possible, e.g.<br />
when policy is being formulated or to support the development of the Integrated<br />
Assurance and Approval Plan (IAAP). The RPA should subsequently be reviewed before<br />
its use to initiate all MPA assurance reviews.<br />
The RPA requires the Senior Policy Owner (SPO) or Senior Responsible Owner (SRO) or<br />
Project Executive, to consider the initiative from two perspectives: firstly through a<br />
strategic assessment of the Consequential Impact, should the programme or project fail<br />
to deliver its objectives or outcomes (see Table A); followed secondly, if appropriate, by<br />
an assessment of Complexity (see Table B).<br />
Each table is made up of a series of assessments, with the result indicated by<br />
marking X in the appropriate box between VERY LOW (VL) and VERY HIGH (VH).<br />
These assessments are made using the knowledge and judgement of the SPO/SRO and<br />
policy/programme/project team, and should be considered in the light of the strategic<br />
context for the initiative. Examples have been provided as a guide to what might be<br />
considered as VL or VH assessments. For each assessment a short explanatory note of<br />
the reasoning for each mark should be given (where appropriate) in the text box to<br />
provide an audit trail of the considerations.<br />
Table A – Consequential Impact Assessment<br />
Having considered each Strategic Impact Area an overall assessment is required to<br />
determine the Consequential Impact Assessment. This is based on the holistic<br />
assessment of all five areas in total; there is no formula or calculation involved. The<br />
overall assessment should be shown by an X in the final (pink) section of Table A.<br />
An explanatory note must be given in the text box provided to give the reasoning for the<br />
overall assessment.<br />
<br />
10<br />
This role was previously called the Departmental Gateway Coordinator (DGC) but with expansion in the range of assurance reviews<br />
available, the original role name is no longer accurate. In some organisations Departmental Gateway/Assurance Coordinator will be<br />
somebody’s job title; in others someone with a different job title will fulfil the DAC function.<br />
Version4 Page159
<strong>Outline</strong><br />
<strong>Case</strong><br />
<strong>Business</strong><br />
During policy development, when assurance may be provided through a Starting Gate or<br />
equivalent review, completion of only Table A is required. Only the Overall Consequential<br />
Impact Assessment mark should be entered in Box 14 on the cover sheet. If this<br />
assessment indicates that the impact is MEDIUM or above, the RPA should, after<br />
agreement of the SPO, be submitted to the DAC.<br />
For existing programmes/projects if, after completing Table A, the Overall<br />
Consequential Impact Assessment is considered to be VERY LOW, completion of Table<br />
B is optional and the completed RPA can be sent to the DAC, who will discuss with the<br />
programme/project what assurance activity might be most appropriate.<br />
<br />
Table B – Complexity Assessment<br />
If the Consequential Impact Assessment (Table A) is assessed as greater than VERY<br />
LOW, completion of the Complexity Assessment (Table B) is required. The approach for<br />
Table B largely follows the same format as for Table A, but for convenience is broken<br />
down into four Complexity Areas.<br />
Having assessed each factor in each of the four complexity areas, an assessment is then<br />
required to determine a summary assessment for each area. Again an X should be<br />
marked in the appropriate (yellow) score box for each complexity area and an explanation<br />
given in the notes box.<br />
At the end of Table B there is a (yellow) table headed Complexity Assessment Summary<br />
where the area summary assessment results should be recorded.<br />
Consideration should now be given to reaching an Overall Complexity Assessment for<br />
the initiative, based on the four area assessments. Again, there is no scoring or formula<br />
for determining this; it is the policy/programme/project team’s holistic assessment.<br />
The Overall Complexity Assessment is recorded in the final (green) section of the<br />
Complexity Assessment Summary with an X marked in the appropriate box. An<br />
explanatory note must be provided to support the overall complexity assessment for<br />
audit trail purposes.<br />
Finalising the Risk Potential Assessment<br />
As the environments in which programmes or projects operate will vary, there may be other<br />
aspects that might not be covered by the RPA which affect the impact and/or complexity<br />
assessments in this form. These additional aspects, if considered material to the overall<br />
impact and/or complexity assessments, should be reflected with explanatory notes in the<br />
overall assessments in Tables A and B respectively.<br />
Having completed the Consequential Impact Assessment (Table A) and the Complexity<br />
Assessment (Table B), the overall Risk Potential Assessment for the programme or<br />
project is determined by plotting the respective assessments on Table C.<br />
Using the overall results from the Consequential Impact and Complexity Assessments and<br />
the respective axis of Table C, mark an X in the appropriate cell where the two<br />
assessments intersect. This will then indicate what level of review may be required, as<br />
suitable for the Low, Medium or High Risk level of the initiative. The overall level of<br />
review (L/M/H) should then be noted in Box 14 on the cover sheet of the RPA.<br />
The SPO or SRO (as relevant) must agree the completed RPA, after which the completed<br />
RPA should then be sent to the DAC, who in turn will copy it on to the organisation’s<br />
Portfolio Manager (or an equivalent e.g. Head of Centre of Excellence), for validation.<br />
For all submissions the Portfolio Manager (or equivalent) should independently validate the<br />
RPA and be satisfied that it fairly reflects the initiative’s strategic profile within the<br />
organisation’s overall change portfolio. If the RPA is deemed by them to be inaccurate, a<br />
discussion with the SPO/SRO should be held to reach a consensus.<br />
Using the RPA for assurance purposes<br />
Version4 Page160
<strong>Outline</strong><br />
<strong>Case</strong><br />
<strong>Business</strong><br />
Once an RPA is agreed the DAC will instigate the assurance review process by arranging<br />
an Assessment Meeting. There are lead times between the Assessment Meeting and<br />
the review itself (see below Table C) which depend on a number of factors; your DAC can<br />
offer advice on those lead times.<br />
PLEASE NOTE: It may not be possible for the MPA to organise a review at shorter<br />
notice, based on limited availability of reviewers.<br />
The initial RPA assessment will normally be used throughout the life of the integrated<br />
assurance and approval process, even though the risk potential might decline as the<br />
programme/project progresses through the change lifecycle. Should the RPA marking<br />
increase, the higher assessment may take precedent. Departments, Agencies and<br />
NDPBs, in discussion with the MPA, should undertake periodic reviews of their portfolios<br />
to ensure a consistent and appropriate use of the RPA in setting risk levels, and hence<br />
the appropriate assurance regimes.<br />
The RPA will also be reviewed at each Assessment Meeting to ensure there have been no<br />
material changes since it was completed. Following the Assessment Meeting the<br />
constitution of the review team and duration of the review will be determined.<br />
<br />
For further information see contact details on last page.<br />
Version4 Page161