Authorization to Release Protected Health Information
Authorization to Release Protected Health Information
Authorization to Release Protected Health Information

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
1.<br />
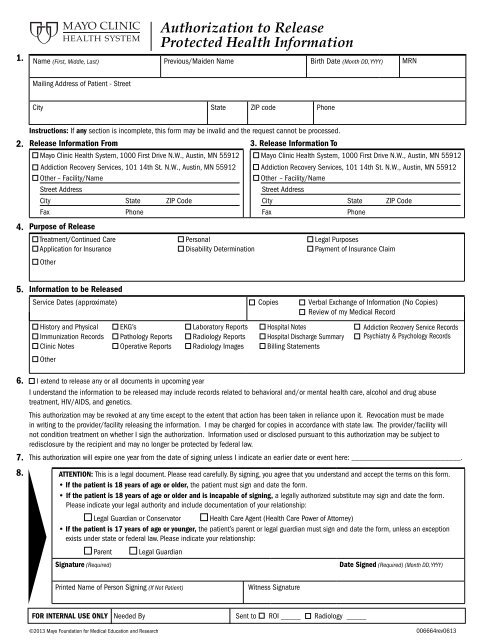
<strong>Authorization</strong> <strong>to</strong> <strong>Release</strong><br />
<strong>Protected</strong> <strong>Health</strong> <strong>Information</strong><br />
Name (First, Middle, Last) Previous/Maiden Name Birth Date (Month DD, YYYY) MRN<br />
Mailing Address of Patient - Street<br />
City State ZIP code Phone<br />
2.<br />
4.<br />
Instructions: If any section is incomplete, this form may be invalid and the request cannot be processed.<br />
<strong>Release</strong> <strong>Information</strong> From<br />
3. <strong>Release</strong> <strong>Information</strong> To<br />
Mayo Clinic <strong>Health</strong> System, 1000 First Drive N.W., Austin, MN 55912<br />
Addiction Recovery Services, 101 14th St. N.W., Austin, MN 55912<br />
Mayo Clinic <strong>Health</strong> System, 1000 First Drive N.W., Austin, MN 55912<br />
Addiction Recovery Services, 101 14th St. N.W., Austin, MN 55912<br />
Other – Facility/Name<br />
Other – Facility/Name<br />
Street Address<br />
Street Address<br />
City State ZIP Code<br />
City State ZIP Code<br />
Fax<br />
Phone<br />
Fax<br />
Phone<br />
Purpose of <strong>Release</strong><br />
Treatment/Continued Care Personal Legal Purposes<br />
Application for Insurance Disability Determination Payment of Insurance Claim<br />
Other<br />
5.<br />
6.<br />
7.<br />
8.<br />
<strong>Information</strong> <strong>to</strong> be <strong>Release</strong>d<br />
Service Dates (approximate) Copies Verbal Exchange of <strong>Information</strong> (No Copies)<br />
Review of my Medical Record<br />
His<strong>to</strong>ry and Physical EKG’s Labora<strong>to</strong>ry Reports<br />
Immunization Records Pathology Reports Radiology Reports<br />
Clinic Notes Operative Reports Radiology Images<br />
Other<br />
Hospital Notes<br />
Hospital Discharge Summary<br />
Billing Statements<br />
I extend <strong>to</strong> release any or all documents in upcoming year<br />
I understand the information <strong>to</strong> be released may include records related <strong>to</strong> behavioral and/or mental health care, alcohol and drug abuse<br />
treatment, HIV/AIDS, and genetics.<br />
This authorization may be revoked at any time except <strong>to</strong> the extent that action has been taken in reliance upon it. Revocation must be made<br />
in writing <strong>to</strong> the provider/facility releasing the information. I may be charged for copies in accordance with state law. The provider/facility will<br />
not condition treatment on whether I sign the authorization. <strong>Information</strong> used or disclosed pursuant <strong>to</strong> this authorization may be subject <strong>to</strong><br />
redisclosure by the recipient and may no longer be protected by federal law.<br />
This authorization will expire one year from the date of signing unless I indicate an earlier date or event here: ___________________________.<br />
ATTENTION: This is a legal document. Please read carefully. By signing, you agree that you understand and accept the terms on this form.<br />
• If the patient is 18 years of age or older, the patient must sign and date the form.<br />
• If the patient is 18 years of age or older and is incapable of signing, a legally authorized substitute may sign and date the form.<br />
Please indicate your legal authority and include documentation of your relationship:<br />
Legal Guardian or Conserva<strong>to</strong>r <strong>Health</strong> Care Agent (<strong>Health</strong> Care Power of At<strong>to</strong>rney)<br />
• If the patient is 17 years of age or younger, the patient’s parent or legal guardian must sign and date the form, unless an exception<br />
exists under state or federal law. Please indicate your relationship:<br />
Parent<br />
Signature (Required)<br />
Legal Guardian<br />
Addiction Recovery Service Records<br />
Psychiatry & Psychology Records<br />
Date Signed (Required) (Month DD, YYYY)<br />
Printed Name of Person Signing (If Not Patient)<br />
Witness Signature<br />
FOR INTERNAL USE ONLY Needed By Sent <strong>to</strong> ROI _____ Radiology _____<br />
©2013 Mayo Foundation for Medical Education and Research 006664rev0613
<strong>Release</strong> of <strong>Information</strong> Instructions<br />
Albert Lea and Austin<br />
Austin<br />
<strong>Authorization</strong> Completion Instructions<br />
To protect the privacy of our patients and <strong>to</strong> maintain the confidentiality of their personal health information, we must obtain a valid, complete,<br />
and legible authorization for release of medical records.<br />
1. Patient:<br />
• Name: Print the full, legal name of the patient<br />
• Previous/Maiden Name: Any previous legal names<br />
• Birth Date: Month, Day, and Year of birth<br />
• Mailing Address of Patient: Street, City, State, and Zip Code of Patient<br />
• Phone: Patient’s phone number<br />
2. <strong>Release</strong> <strong>Information</strong> From:<br />
• Check the sites listed where you have received care and who you want <strong>to</strong> allow <strong>to</strong> release your medical information.<br />
• If the provider authorized <strong>to</strong> release information is other than Mayo Clinic <strong>Health</strong> System – Austin, check the Other box and<br />
complete the Individual, Facility or Company Name of that person or Provider. Fill in their complete address. Include their phone<br />
number if known.<br />
3. <strong>Release</strong> <strong>Information</strong> To:<br />
• Print the name of the person or organization that is <strong>to</strong> receive the information, along with their complete address, city, state,<br />
and zip code. Please include their phone number if known.<br />
4. Purpose of <strong>Release</strong>:<br />
• Check the appropriate box that best explains the purpose of the request.<br />
• If the Other box is checked, please write the reason in the space provided.<br />
5. <strong>Information</strong> <strong>to</strong> be <strong>Release</strong>d:<br />
• Fill in the approximate dates of service if known.<br />
• Check the appropriate box if copies, a verbal exchange, or a review of the medical record is requested.<br />
• Check the box next <strong>to</strong> the types of information requested.<br />
• If the other box is checked, please write the needed information in the space provided.<br />
6. I extend <strong>to</strong> release any or all documents in the upcoming year:<br />
• Check this box <strong>to</strong> authorize medical information that is created after the date of signature on this form <strong>to</strong> be released. If this box<br />
is not checked, we are only able <strong>to</strong> release medical information that was created on or before the date this authorization was signed.<br />
7. Expiration Date:<br />
• This authorization will be valid for one year unless otherwise specified by a date written in this area. Do not write <strong>to</strong>day’s date<br />
as the expiration date or the request will not be able <strong>to</strong> be processed.<br />
8. Signature:<br />
• The patient or legal representative must sign and date the authorization.<br />
• Attach copies of documents outlining the representative’s legal right <strong>to</strong> sign on the patient’s behalf.<br />
If records are needed <strong>to</strong> be released from Mayo Clinic <strong>Health</strong> System – Austin, please return the completed authorization by one of the<br />
following methods:<br />
FAX | 507-434-1447 IN PERSON | <strong>Health</strong> <strong>Information</strong> Management/ MAIL | Mayo Clinic <strong>Health</strong> System<br />
<strong>Release</strong> of <strong>Information</strong><br />
Attention: <strong>Release</strong> of <strong>Information</strong><br />
1000 First Drive N.W.<br />
Austin, MN 55912<br />
If records are needed from a facility other than Mayo Clinic <strong>Health</strong> System – Albert Lea and Austin, the completed authorization should be forwarded<br />
directly <strong>to</strong> that facility. If assistance is needed with completing this form, contact the <strong>Health</strong> <strong>Information</strong> Management Department at 507-434-1132<br />
during the hours of 8 a.m. <strong>to</strong> 5 p.m., Monday through Friday.<br />
©2013 Mayo Foundation for Medical Education and Research 006664rev0513