Moderate Sedation Presentation - Mayo Clinic Health System
Moderate Sedation Presentation - Mayo Clinic Health System
Moderate Sedation Presentation - Mayo Clinic Health System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
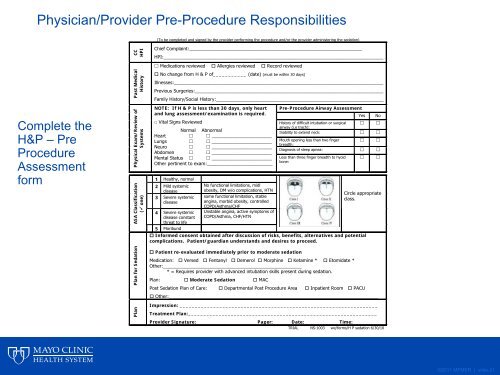
Physician/Provider Pre-Procedure Responsibilities<br />
(To be completed and signed by the provider performing the procedure and/or the provider administering the sedation)<br />
Complete the<br />
H&P – Pre<br />
Procedure<br />
Assessment<br />
form<br />
CC<br />
HPI<br />
Past Medical<br />
History<br />
Physical Exam/Review of<br />
<strong>System</strong>s<br />
ASA Classification<br />
( one)<br />
Chief Complaint:__________________________________________________________________<br />
HPI:____________________________________________________________________________________<br />
Medications reviewed Allergies reviewed Record reviewed<br />
No change from H & P of___________ (date) (must be within 30 days)<br />
Illnesses:________________________________________________________________________________<br />
Previous Surgeries:________________________________________________________________________<br />
Family History/Social History:________________________________________________________________<br />
NOTE: If H & P is less than 30 days, only heart Pre-Procedure Airway Assessment<br />
and lung assessment/examination is required.<br />
Yes No<br />
□ Vital Signs Reviewed<br />
History of difficult intubation or surgical <br />
airway (i.e trach):<br />
Normal Abnormal<br />
Inability to extend neck: <br />
Heart _______________________<br />
Lungs _______________________ Mouth opening less than two finger <br />
breadth:<br />
Neuro _______________________<br />
Diagnosis of sleep apnea: <br />
Abdomen _______________________<br />
Mental Status _______________________ Less than three finger breadth to hyoid <br />
bone:<br />
Other pertinent to exam:_________________________<br />
_____________________________________________<br />
1 <strong>Health</strong>y, normal<br />
2 Mild systemic<br />
disease<br />
3 Severe systemic<br />
disease<br />
4 Severe systemic<br />
disease constant<br />
threat to life<br />
5 Moribund<br />
No functional limitations, midl<br />
obesity, DM w/o complications, HTN<br />
some functional limitation, stable<br />
angina, morbid obesity, controlled<br />
COPD/Asthma/CHF<br />
Unstable angina, active symptoms of<br />
COPD/Asthma, CHF/HTN<br />
Circle appropriate<br />
class.<br />
Informed consent obtained after discussion of risks, benefits, alternatives and potential<br />
complications. Patient/guardian understands and desires to proceed.<br />
Plan for <strong>Sedation</strong><br />
Plan<br />
Patient re-evaluated immediately prior to moderate sedation<br />
Medication: Versed Fentanyl Demerol Morphine Ketamine * Etomidate *<br />
Other:_____________________________________________________<br />
* = Requires provider with advanced intubation skills present during sedation.<br />
Plan: <strong>Moderate</strong> <strong>Sedation</strong> MAC<br />
Post <strong>Sedation</strong> Plan of Care: Departmental Post Procedure Area Inpatient Room PACU<br />
Other:________________________________________________________________________________<br />
Impression: _________________________________________________________________<br />
Treatment Plan:______________________________________________________________<br />
Provider Signature:____________________Pager:______Date:___________ Time:________<br />
TRIAL NS-1003 we/forms/H P sedation 6/30/10<br />
©2011 MFMER | slide-21