Uterine Suspension - CooperSurgical
Uterine Suspension - CooperSurgical
Uterine Suspension - CooperSurgical

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Uterine</strong> suspension ---<br />
collision dyspareunia relief for<br />
women with a retroverted uterus<br />
BACKGROUND: Dyspareunia is a multi-faceted problem that can involve a number of factors and disease states. Women rarely<br />
report it on their own, but may discuss the issue upon direct inquiry. Evaluation of a patient responding affirmatively should involve a<br />
complete and careful sexual history and a comprehensive physical exam. It is important to identify the severity, character and location<br />
of pain during intercourse. This information can used to determine whether the patient is experiencing superficial or deep dyspareunia<br />
or both.<br />
In cases of deep dyspareunia, particular attention should be paid to uterine position during the pelvic exam. If the pain experienced during<br />
intercourse can be reproduced with a digital exam, the patient is a good candidate for uterine suspension. Some investigators have advocated<br />
a pessary trial prior to uterine suspension. However, others have noted that the trial is unnecessary and that pessary use can cause<br />
sexual dysfunction and further gynecological concerns. 1 <strong>Uterine</strong> suspension represents a long-term solution for women with dyspareunia<br />
secondary to a retroverted uterus.<br />
DOCUMENTATION: In a series of 75 women with a symptomatic retroverted uterus who underwent laparoscopic uterine suspension,<br />
Carter found that 84% (n=63) reported complete relief from dyspareunia with up to two-year follow-up. 2 Another 7% (n=5) reported<br />
mild pain and 4% (n=3) moderate pain. For all 75 patients, pain with intercourse decreased from 8.1 to 1.5 on a 10-point scale (0=no<br />
pain and 10=the worst pain the patient has ever experienced). Each patient was evaluated for degree of retroversion and was assessed<br />
by ultrasound to identify any uterine or ovarion abnormalities. Dyspareunia was reproduced by palpation of the retroverted uterus.<br />
Ostrzenski found that all patients (n=32) who underwent laparoscopic uterine suspension for symptomatic uterine retroversion reported<br />
complete relief from dyspareunia after at least 24 months follow-up. 3 Surgery was conducted in the context of a prospective randomized<br />
study.<br />
Batioglu performed laproscopic uterine suspension on 30 women with chronic pelvic pain unexplained by causes other than uterine<br />
retroversion. 4 Dyspareunia was resolved in 19 of 20 women who completed two-year follow-up. The one woman still experiencing<br />
dyspareunia had a retroverted uterus and refused a second suspension procedure.<br />
Gargiulo concluded that uterine suspension effectively relieves dyspareunia after conducting a prospective study of 50 women with<br />
symptomatic uterine retroversion and no other clinical findings to explain their symptoms. 5 At one year follow-up, 33 of the 40 women<br />
remaining in the study had an anteverted uterus, complete remission of pain and a markedly improved sex life.<br />
Other researchers have reached similar conclusions on the efficacy of uterine suspension for dyspareunia related to a retroverted uterus:<br />
Koh - 100% (n=22) of the women reported that “their sexual life had tremendously improved” at up to two-year follow-up. 6<br />
Serour - 89% (n=75) of women improved with follow-up of 6 to 30 months. 7<br />
Patterson - 76% (n=53) experienced complete relief of dyspareunia and 14% (n=10) had partial relief with a mean<br />
follow-up of 40.5 months. 8<br />
CONCLUSION: <strong>Uterine</strong> suspension provides effective long-term relief of deep dyspareunia due to a retroverted uterus.
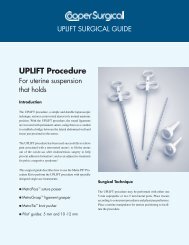
Perform fast, effective and reimbursed uterine<br />
repositioning with the UPLIFT procedure and<br />
the Metra PS ® kit.<br />
UPLIFT PROCEDURE:<br />
Shortens and strengthens the round ligaments<br />
Lifts the uterus out of the cul-de-sac to a neutral/slightly<br />
anteverted position<br />
Minimal procedure time averaging 12 minutes in a series<br />
of 75 women 9<br />
Reimbursed - for both physician and hospital fees<br />
MetraGrasp DuoGrasp<br />
<br />
METRA PS ®<br />
KIT:<br />
Specifically designed instruments to facilitate<br />
the UPLIFT procedure.<br />
MetraPass suture passer - Designed for passing suture<br />
through soft tissue<br />
MetraGrasp ligament grasper - An indentation allows<br />
atraumatic manipulation of the round ligaments<br />
MetraTie knot pusher - Helps insure appropriate suture tension<br />
Investa ®<br />
suture material - Lubricious, elastic and permanent<br />
for long-term stability<br />
Pilot ®<br />
suturing guides - (5 and 10/12 mm sizes) For quick and<br />
consistent full-thickness closure of all port sites<br />
REFERENCES:<br />
UPLIFT laparoscopic uterine repositioning procedure<br />
See product instructions for further information on product use.<br />
1<br />
Candy JW. Modified Gilliam <strong>Uterine</strong> <strong>Suspension</strong> Using Laproscopic Visualization. Obstet Gynecol 1976;47:242.<br />
2<br />
Carter JE. Carter-Thomason <strong>Uterine</strong> <strong>Suspension</strong> and Positioning by Ligament Investment, Fixation and Truncation. Journal of Reproductive Medicine<br />
1999;44(5):417-422.<br />
3<br />
Ostrzenski A. Laparoscopic Retroperitoneal Hysteropexy, A Randomized Trial. Journal of Reproductive Medicine 1998;43(4):361-366.<br />
4<br />
Batioglu S and Zeyneloglu HB. Laparoscopic Plication and <strong>Suspension</strong> of the Round Ligament for Chronic Pelvic Pain and Dyspareunia. Journal of the<br />
American Association of Gynecologic Laparoscopists 2000;7(4):547-551.<br />
5<br />
Gargiulo T, Leo L and Gomel V. Laparoscopic <strong>Uterine</strong> <strong>Suspension</strong> Using Three-Stitch Technique. Journal of the American Association of Gynecologic<br />
Laparoscopists 2000;7(2):233-235.<br />
6<br />
Koh LW, Tang FC and Huang MH. Preliminary Experience in Pelviscopic <strong>Uterine</strong> <strong>Suspension</strong> Using Webster-Baldy and Franke’s Method. Acta Obstetrica<br />
et Gynecologica Scandinavica 1996;75:575-578.<br />
7<br />
Serour GJ. Hefnawi O, Kandil O, Alaskani N, et al. Laparoscopic Ventrosuspension: A New Technique. International Journal of Gynaecological<br />
Obstetrics 1982;20:129-131.<br />
8<br />
Paterson MEL, Jordan JA and Logan-Edwards R. A Survey of 100 Patients Who Had Laproscopic Ventrosuspensons. British Journal of Obstetrics and<br />
Gynaecology 1978;85:468-471.<br />
9<br />
Carter JE.<br />
95 Corporate Drive, Trumbull, CT 06611 • 800.243.2974 or 203.601.5200 • Fax: 800.262.0105 • www.coopersurgical.com<br />
Form # 81404 06/08