Download - Smile Dental Journal
Download - Smile Dental Journal
Download - Smile Dental Journal

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> - June 2011 - Volume 6, Issue 2 - www.smiledentaljournal.com - Distributed free of charge<br />
Ankyloglossia<br />
in a Pseudo-Class III<br />
Malocclusion<br />
In-House<br />
Maxillofacial 3D<br />
Rapid Prototyping<br />
3D Innovations of<br />
Cranioplasty Plate<br />
Construction<br />
Celebrating<br />
5 th Anniversary<br />
“1 st <strong>Smile</strong> Symposium”<br />
Confusing<br />
Endodontic<br />
Cases<br />
Functional<br />
and Aesthetic<br />
Management of<br />
Worn Dentition<br />
with Direct<br />
Composite<br />
Restorations<br />
ISSN: 2072-473X
Time for a new breed<br />
of ergonomics<br />
S220TR HYBRID<br />
YOUR TALENT INSPIRES US<br />
STERN WEBER Via Bicocca, 14/C - 40026 Imola - (BO) Italy - Tel. 0542 653441 - Fax 0542 653601 - www.sternweber.com - sternweber@sternweber.com<br />
Ambidextrous as and when required, yet always multi-functional.<br />
The S220TR HYBRID is a simple yet effective concept that enhances<br />
ergonomics whatever your working style. Characterised by outstanding<br />
<br />
provides an ergonomic positioning potential in a class of its own.<br />
Right-handed to left-handed in seconds: complete operating freedom is now<br />
<br />
S SERIES , TR SERIES, TRC SERIES: OVER 20 STERN WEBER MODELS TO MEET YOUR EVERY NEED.
Sealed. Safe.<br />
* Most used Endo-Sealer in many countries, over 50 million fillings worldwide (data on file).<br />
** 6.2 ±1.4 MPa adhesion to root canal dentin (Gogos et al.)<br />
The No. 1 Endo-Sealer*<br />
Unique Dentine-Adhesion**<br />
Outstanding Dimensional Stability<br />
Over 10 years proven clinical success<br />
www.dentsplymea.com
Coming<br />
Soon<br />
Simplicity is the real innovation<br />
• Only one sterile NiTi instrument per root canal in most cases<br />
• Decreases the global shaping time by up to 40%*<br />
• Reciprocating technology respecting the root canal anatomy<br />
• Single use as new standard of care<br />
*data on file<br />
www.dentsplymea.com
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong><br />
June 2011<br />
Volume 6, Issue 2<br />
Quarterly Issued<br />
Distributed Free of Charge<br />
+962 7 96367954<br />
Amman, Jordan<br />
info@smile-mag.com<br />
sola@smiledentaljournal.com<br />
www.smiledentaljournal.com<br />
Director<br />
Dr. Ma’moon A. Salhab<br />
Director in Charge &<br />
Chief Editor<br />
Dr. Issa S. Bader<br />
Editorial Director<br />
Dr. Hassan A. Maghaireh<br />
Marketing Director<br />
Solange R. Sfeir<br />
Photography<br />
Solange R. Sfeir<br />
Art & Design<br />
Yazid M. Masa<br />
Published by MENA Co. for<br />
<strong>Dental</strong> Services<br />
Jordanian National Library<br />
Registration # 3954/2008/P<br />
ISSN 2072-473X<br />
Printed By:<br />
Ad-Dustour Commercial Printing Press<br />
Amman, Jordan<br />
Mission Statement<br />
Bridging the gap between advanced uptodate<br />
peer-reviewed dental literature and<br />
the dental practitioners enabling them to<br />
do their jobs better- is our ultimate target.<br />
Besides, <strong>Smile</strong> provides readers with<br />
information regarding the available dental<br />
products, armamentarium, news<br />
and proceedings of dental symposia,<br />
workshops and conferences.<br />
Disclaimer<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> makes every<br />
effort toreport clinical information and<br />
manufacturers’ product news accurately, but<br />
cannot assume responsibility for the validity<br />
of product claims or typographical errors.<br />
Opinions or interpretations expressed by the<br />
authors are their own and do not necessarily<br />
reflect nor hold <strong>Smile</strong> team responsible for<br />
the validity of the content.<br />
Editorial Review Board<br />
• Prof. Louis Hardan / Lebanon<br />
DDS, DEA, PhD, Restorative & Esthetic Dentistry<br />
• Dr. Maher Abdeljawad / Jordan<br />
BDS, MDentSci, Restorative Dentistry<br />
• Dr. Hani Abudiak / UK<br />
BDS, MFDS RCSFRCD, PhD Paediatric Dentistry<br />
• Dr. Eyas Abu-Hijleh / UAE<br />
DDS, PhD, Orthodontics & Dentofacial Orthopedics<br />
• Dr. Layla Abu-Naba’a / Jordan<br />
BDS, MFD, RCS, PhD, Prosthodontics<br />
• Dr. Ali Abu Nemeh / Jordan<br />
BDS, NDB, MSc, Endodontics<br />
• Dr. Hazem Al-Ahmad / Jordan<br />
BDS, MSc, FDSRCS, Maxillo-Facial Surgery<br />
• Dr. Muna Al-Ali / Australia<br />
BDS, MFDS<br />
• Dr. Suhail H. Al-Amad / UAE<br />
D.Clin.Dent (Melb), FRACDS-Oral Med, GradDip<br />
ForOdont (Melb), JMC-Oral Med<br />
• Dr. Zaid Al-Bitar / Jordan<br />
BDS, MSc, MOrth, RCS, Orthodontics<br />
• Dr. Wesam Aleid / UK<br />
BDS, MBBS, MRCSEd, FFDRCSI(OSOM), FRCS(OMFS)<br />
Oral, facial, and Head & Neck Surgeon<br />
• Dr. Raed Al-Jallad / Palestine<br />
BDS, MSc, FFDRCS, FDSRCS, Oral & Maxillofacial<br />
Surgery<br />
• Dr. Hani Al Kadi / KSA<br />
BDS, Dip ODONT, MDS, Endodontics<br />
• Dr. Mohammad Al-Rabab’ah / Jordan<br />
BDS, MFD RCSIre, MRD(Pros), RCSEd, JB(Cons) PhD<br />
• Dr. Hatem Al-Rashdan/ Jordan<br />
BDS, MSc, Jordanian Board of Maxillofacial Surgery<br />
• Dr. Majd Al-Saleh / Jordan<br />
BDS, DDS, MSc, Pediatric Dentistry<br />
• Dr. Ahmad Al-Tarawneh / Jordan<br />
DDS, M.Clin.Dent, Jordanian Board of Orthodontics<br />
• Dr. Hayder Al-Waeli / Jordan<br />
BDS, MSc, Jordanian Board of Periodontology<br />
• Dr. Muayad Assaf / Jordan<br />
BDS, MSc Endodontics<br />
• Dr. Manal Azzeh / Jordan<br />
BDS, MSc, Jordanian Board of Periodontology<br />
• Dr. Menah Barmawi / Jordan<br />
BDS, Jordanian Board of Maxillofacial Surgery<br />
• Dr. Bader Eddin Borgan / Jordan<br />
BDS, MDS, MOrth, RCSEd, Orthodontics<br />
• Dr. Edgard El Chaar / USA<br />
DDS, MS. Periodontology & Implantology<br />
• Dr. Lama Jarrah / Jordan<br />
BDS, MSc, Jordanian Board of Orthodontics<br />
• Dr. Ghada Karien / Jordan<br />
BDS, JDB, Pediatric Dentistry<br />
• Dr. Ahmad Kutkut / USA<br />
DDS, MS, Prosthodontics, USA<br />
• Dr. Yousef Sadik Marafie / Kuwait<br />
BDS, MSD, Prosthodontics<br />
• Dr. Hakam Mousa / Jordan<br />
BDS, MSD, Operative Dentistry<br />
• Dr. Jumana Sabbarini / Jordan<br />
BDS, MSc, Jordanian Board of Pediatric Dentistry<br />
• Dr. Samer Sunna / Jordan<br />
BDS, MSc, M.Orth, RCS, Orthodontics<br />
• Dr. Thamer Theeb / Jordan<br />
BDS, MSc, Prosthodontics<br />
• Dr. Leema Yaghmour / Jordan<br />
BDS, DUA, DUB, Pediatric & Community Dentistry<br />
International Advisory Board<br />
• Prof. Abdullah Al-Shammery / KSA<br />
BDS, MS Restorative Dentistry / Rector, Riyadh Colleges of<br />
Dentistry & Pharmacy<br />
• Prof. Magid Amin Ahmed / Egypt<br />
Oral & Maxillo-Facial Surgery / Vice President MSA University<br />
Dean, Faculty of Dentistry MSA University<br />
• Prof. Jamal Aqrabawi / Jordan<br />
DDS, DSc, DMD Endodontics / <strong>Dental</strong> Faculty, University of Jordan<br />
• Prof. Nabil Barakat / Lebanon<br />
DDS, MSc, FICD Maxillo-Facial Surgery / President of LAO & EMAO<br />
• Prof. Stephen Cohen / USA<br />
MA, DDS, FICD, FACD, Diplomate, American Board of Endodontics<br />
• Prof. Azmi Darwazeh / Jordan<br />
BDS, MSc, PhD Oral Pathology Oral Medicine / Former Dean,<br />
Faculty of Dentistry JUST / Examiner, Faculty of Dentistry RCS<br />
Ireland<br />
• Prof. Mohamed Sherine Elattar / Egypt<br />
BDS, MSc, PhD Prosthodontics / Dean, Faculty of Dentistry, Pharos<br />
University / President of AOIA<br />
• Prof. Dr. Marco Esposito / Italy<br />
DDS PHD, Editor of the Cochrane Oral Health Group<br />
Editor in Chief of the European <strong>Journal</strong> of Oral Implantology<br />
• Prof. Fouad Kadim / Jordan<br />
BDS, MSc, PhD Conservative Dentistry / Vice Dean, Faculty of<br />
Dentistry, University of Jordan<br />
• Prof. Howard Lieb / USA<br />
DMD General Dentistry & Management Sciences / College of<br />
Dentistry, New York University<br />
• Prof. Edward Lynch / UK<br />
PhD (Lon), MA, BDentSc, TCD, FDSRCS (Ed), FADFE, FDSRCS (Lon)<br />
Head of <strong>Dental</strong> Education and Research Warwick University<br />
• Prof. Lamis D. Rajab / Jordan<br />
DDS, PhD, Pediatric Dentistry / Former Dean, Faculty of Dentistry,<br />
University of Jordan<br />
• Prof. Issam Shaaban / Syria<br />
BDS, PhD, Maxillo-Facial Surgery / Former Dean, Faculty of<br />
Dentistry Damascus University / President of Syrian OMFS Society<br />
• Prof. Yousef Talic / KSA<br />
BDS, MSc, DASO, FICOI, FICD, Editor-in-Chief, Saudi <strong>Dental</strong><br />
<strong>Journal</strong> / Consultant in Prosthodontics & Implantology, College of<br />
Dentistry, King Saud University<br />
• Prof. Abbas Zaher / Egypt<br />
BDS, MS, PhD Orthodontics, Professor of Orthodontics / Vice-<br />
Dean, Alexandria University / Vice-President, World Federation of<br />
Orthodontists<br />
• Prof. Carina Mehanna Zogheib / Lebanon<br />
DDS, PhD Restorative and Esthetic Dentistry, FICD<br />
Head of Restorative and Esthetic Dentistry Department, Saint-<br />
Joseph University<br />
• Dr. Nadim Abou-Jaoude / Lebanon<br />
CES, DU, FICD Prosthodontics, Lecturer, Lebanese University /<br />
Clinical Associate, American University of Beirut<br />
• Dr. Hasanen H. Al-Khafagy / UAE<br />
BDS, MSc, PhD Conservative Dentistry, Ajman University of Science<br />
& Technology<br />
• Dr. Jaser Al-Ma’itah / Jordan<br />
BDS, MSc Oral Surgery, Head of <strong>Dental</strong> Department, Jordanian<br />
Royal Medical Services<br />
• Dr. Maher Almasri / UK<br />
DDS, MSc, PhD, FADFE, Director of Oral Surgery Courses, Bone<br />
Graft Modules Leader, Warwick University / President of the Syrian<br />
Section of IADR<br />
• Dr. Abdelsalam Elaskary / Egypt<br />
BDS, FICOI, President of ASOI<br />
• Dr. Yasin El-Husban / Jordan<br />
DDS, MSc Prosthodontics, Former Minister of Health<br />
Former Head of <strong>Dental</strong> Department & King Hussein Hospital<br />
• Dr. Zbys Fedorowicz<br />
Director, The Bahrain Branch of the UK Cochrane Centre<br />
• Dr. Wolfgang Richter / UK<br />
DDS, PhD, Restorative Dentistry, President of ESCD<br />
• Dr. Mohammad Sartawi / Jordan<br />
BSc, BDS, MSc, FFDRCSI (OSOM)<br />
Senior Consultant Maxillo-Facial Surgery
12<br />
Orthodontics<br />
Ankyloglossia in a Pseudo-Class III Malocclusion: A<br />
Case Report<br />
By Salwa Jeragh Alhaddad, Mohammed Alnoori, Manar Alnoori<br />
Maxillofacial<br />
18 In-House Maxillofacial 3D Rapid Prototyping<br />
By Wesam Aleid<br />
<strong>Dental</strong> Laboratory<br />
22 3D Innovations of Cranioplasty Plate Construction: a Case Report<br />
By Muhanad M. Hatamleh, Jason Watson<br />
Endodontics<br />
26<br />
Confusing Endodontic Cases: Case Series Report<br />
By Masahiro Yoneda, Nao Suzuki, Sonia M. Macedo, Hisashi Anan, Takao Hirofuji<br />
Restorative<br />
Functional and Aesthetic Management of Worn Dentition with<br />
Direct Composite Restorations: A Clinical Report<br />
32<br />
By Shihab A. Romeed, R. Malik, S.M. Dunne<br />
Debate in Focus<br />
08<br />
36<br />
42<br />
Research<br />
Summaries in<br />
Focus<br />
Maxillary Sinus<br />
Augmentation as a Risk<br />
Factor for Implant Failure<br />
The McGill and York<br />
Consensus Statements on<br />
Two- Implant Overdentures<br />
Interventions for Replacing<br />
Missing Teeth: <strong>Dental</strong><br />
Implants in Fresh Extraction<br />
Sockets (Immediate,<br />
Immediate-Delayed and<br />
Delayed Implants)<br />
46<br />
54<br />
66<br />
Ask the Experts<br />
Flash News<br />
Event Reviews<br />
2 Minutes With<br />
Affiliation & Distributors<br />
• Bahrain<br />
Bahrain <strong>Dental</strong> Society<br />
+973 17723767, bahds@batelco.com.bh<br />
• Egypt<br />
Alexandria Oral Implantology Association<br />
+203 5451277, www.aoiaegypt.com<br />
• Iran<br />
Shayan Simin Teb Co.<br />
+98 21 66380364/5, info@shayansiminteb.com<br />
Iranian General <strong>Dental</strong> Association<br />
+98 2188287794/5, info@igda.ir<br />
• Iraq<br />
Iraqi <strong>Dental</strong> Association<br />
+964 015379267, Info@iraqidental.org<br />
Kurdistan <strong>Dental</strong> Association<br />
+964 7504510315, dara_saeed@yahoo.com<br />
• Jordan<br />
Basamat Medical (Pharmadent)<br />
+962 6 5605395, www.basamat.com<br />
• Kuwait<br />
Kuwait <strong>Dental</strong> Association<br />
+965 5325094, www.kda.org.kw<br />
• Lebanon<br />
Lebanese <strong>Dental</strong> Association<br />
+961 1 611555, www.lda.org.lb<br />
Lebanese <strong>Dental</strong> Laboratory<br />
Association<br />
+961 5955 151, www.opdlb.com<br />
Richa <strong>Dental</strong> Store<br />
+961 5 452555, www.richadental.com<br />
• Oman<br />
Oman <strong>Dental</strong> Society<br />
+968 95769039, omandent@omantel.net.om<br />
• Qatar<br />
Qatar <strong>Dental</strong> Society<br />
+974 4393144, www.qatardentalsociety.org<br />
Ali Bin Ali Medical The i-partner<br />
+974 4867871 ext. 247, www.alibinali.com<br />
• Saudi Arabia<br />
Saudi <strong>Dental</strong> Society<br />
+966 1 4677743, www.sds.org.sa<br />
• Sudan<br />
Sudanese <strong>Dental</strong> Association<br />
+249 83 779769, sdaassnan@hotmail.com<br />
• Syria<br />
Najjar Trading Est.<br />
+963 (11) 2244140, najjest@scs-net.org<br />
• United Arab Emirates<br />
Noble Medical Equipment<br />
+971 4 8854544, imad.kafity@noblemedical.ae<br />
Dubai Medical Equipment L.L.C.<br />
+971 6 554 0206, www.mamut-dental.com<br />
Editorial Policy<br />
• Our objective is to publish a dental journal of consistent high quality and help to increase the exposure of literature written by dental professionals from our region at a global<br />
level.<br />
• Literature review, original research, clinical case reports, case series, short communication, randomized clinical trials, and book reviews are among our scope of published<br />
material, where the clinical aspect of dentistry is presented in a scientific way, starting each article with an abstract, backed up by references in accordance with the<br />
Vancouver citation style.<br />
• The journal encourages the submission of papers with a clinical approach, practical or management oriented, besides papers that bridge the gap between dental research<br />
and clinical application.<br />
• Received manuscripts are first revised by the editor to check if it is appropriate for publishing in <strong>Smile</strong> and that it complies with the author›s guidelines. The manuscript is then<br />
forwarded to two or more professional reviewers. Anonymity of both the author and reviewer is preserved (double blinded peer-review process).<br />
• Our editorial policy which controls the quality of articles and assures their accuracy, clarity, and smooth readability through high level enthusiast regional and<br />
international team of experts is our golden key for success.<br />
• Finally, we believe that a controlled content of advertisements could be informative and beneficial especially in dentistry, where the armamentarium and pharmaceuticals<br />
are a major and integral part of the dental science.
Happy 5 th Birthday to<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong><br />
This month, we are celebrating the 5th Birthday of <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> and it’s<br />
time to look back on the last five years of our journal. The plan for the last years was<br />
to bridge the gap between advanced up-to-date peer-reviewed dental literature and<br />
the dental practitioners enabling them to do their jobs better. I believe that we have<br />
achieved this goal; <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> already has more than 30.000 readers in more than 28 countries and has<br />
become the official publication of many <strong>Dental</strong> Societies and Congresses in the Middle East and North Africa<br />
region.<br />
As a new Editorial Director I am very pleased with this achievement and would like to congratulate and thank my<br />
predecessors, my colleagues in the International Advisory Board, the Editorial Review Board and <strong>Smile</strong> Directors<br />
for their efforts and achievements in promoting <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> in the last five years. I look forward to<br />
continuing this momentum.<br />
The next question is whether we are satisfied, and of course the answer is no. There is a bias in the publications,<br />
in the sense that the same group of authors have contributed to many articles in addition to the fact that some of<br />
the submitted manuscripts were of poor quality. The challenge now is to deliver a premium clinical & evidence<br />
based journal to bridge the gap in a very competitive field, providing sound science on which to base decisions for<br />
everyday clinical practice, and I would like to invite you to submit your manuscripts for the upcoming issues of<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong>. You can contribute in a variety of ways: write a clinical case report with an evidence based<br />
review, retrospective, prospective or any other clinical study conducted at your University, Hospital or Private<br />
office. You could also share your practice, clinical and or management tips and tell your colleagues what has (or<br />
hasn’t) worked for you in your practice by contributing to one of the newly introduced sections: Debate in Focus,<br />
Ask <strong>Smile</strong> Experts and Research Summaries in Focus in addition to the other new section you will find in this<br />
issue: Two minutes with a <strong>Smile</strong> guest.<br />
We wish to be open-minded and objective and to present reliable and balanced information. We shall aim for quality<br />
and not for numbers of published articles in order to publish articles with good, sound and up to date evidence in<br />
order to join the MEDLINE and other high quality databases as quickly as possible.<br />
Finally, we would like to welcome the new esteemed Editorial Team, Reviewers as well as Advisory, whom with<br />
their help, we plan to change things for the better.<br />
I wish you all a pleasant reading. In the mean time, should you have any comments or suggestions, please do not<br />
hesitate to email me at maghaireh@smiledentaljournal.com<br />
Dr. Hassan Maghaireh<br />
BDS, MFDS, MSc Implants (Manchester)<br />
Editorial Director<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong><br />
| 4 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 12 - 2011
Calendar of Events<br />
September 14 - 17<br />
FDI Annual World<br />
Congress<br />
Mexico City, Mexico<br />
www.fdiworldental.org<br />
September 21 - 24<br />
21 st BIDM & 7 th Arab<br />
German Implantology<br />
Meeting of DGZI<br />
Dbayeh, Lebanon<br />
www.lda.org.lb<br />
October 6 - 8<br />
International<br />
Expodental<br />
Rome, Italy<br />
www.exp odental.it<br />
October 12 - 15<br />
20 th EAO Annual<br />
Scientific Congress<br />
Athens, Greece<br />
www.eao-congress.com<br />
October 22 - 23<br />
<strong>Dental</strong> Istanbul 2011<br />
Istanbul, Turkey<br />
www.dentalistanbul.com<br />
October 25 - 28<br />
Egyptian <strong>Dental</strong><br />
Association (EDA)<br />
Congress<br />
Cairo, Egypt<br />
www.eda-egypt.org<br />
October 27 - 28<br />
3 rd <strong>Dental</strong>-Facial<br />
Cosmetic International<br />
Conference<br />
Dubai, UAE<br />
www.cappmea.com/aest<br />
hetic2011<br />
November 17 - 18<br />
1 st <strong>Smile</strong> Symposium<br />
Amman, Jordan<br />
www.smiledentaljournal.com<br />
November 22 - 24<br />
7 th International Sudanese <strong>Dental</strong><br />
Association Conference<br />
Khartoum, Sudan<br />
www.sdasudan.org<br />
November 27 - 30<br />
Greater New York<br />
<strong>Dental</strong> Meeting 2011<br />
New York, USA<br />
www.gnydm.com<br />
December 7 - 9<br />
3 rd Sharjah <strong>Dental</strong> College & 16 th<br />
EMA International <strong>Dental</strong><br />
Conference<br />
Sharjah, UAE<br />
www.sharjah.ac.ae<br />
For more events visit www.smiledentaljournal.com or our page on Facebook.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 5 |
<strong>Smile</strong> Message<br />
If You Want Something Done, Ask a Busy Person to Do It<br />
It is with great delight we welcome our new Editorial Director; Dr. Hassan Maghaireh<br />
whom I have known personally since he was an undergraduate student in the mid<br />
nineties. Dr. Maghaireh graduated from the University of Cairo in June 2000 after<br />
which he undertook a five year maxillofacial training in the United Kingdom Hospitals,<br />
he obtained his MFDS from the Royal College of Surgeons in Edinburgh in May<br />
2004 and was awarded his Clinical Masters Degree in <strong>Dental</strong> Implantology from<br />
the University of Manchester in July 2008, when he started working with Professor<br />
Marco Esposito at the Oral health group in Cochrane Collaboration, as well as a Clinical Mentor at the Association of <strong>Dental</strong><br />
Implantology in England. Hassan acts as a co-author for implant related systematic reviews as part of Prof. Marco Esposito’s<br />
research team and he is on the Editorial Board of the European <strong>Journal</strong> of Oral Implantology.<br />
Dr. Maghaireh is now a part time clinical teacher at the Department of Implant Dentistry at the Univeristy of Manchester, he also<br />
maintains a private implant referral practice in Leeds- England.<br />
Indexing of <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong><br />
As you might all be aware, it is not an easy task to attract high quality articles and we are well aware that many authors are<br />
concerned that the journal is not yet indexed in PubMed and has no impact factor. However, we are proud to say that <strong>Smile</strong><br />
<strong>Dental</strong> <strong>Journal</strong> has moved from a magazine aimed to bridging the gap between advanced up-to-date peer-reviewed dental<br />
literature and the readers, to a well recognized peer-reviewed and indexed scientific journal. <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> has been<br />
selected to be one of the sources of input of the Index Medicus for the WHO Eastern Mediterranean Region (IMEMR), Ulrich’s,<br />
DOAJ, Open J-Gate, Index Copernicus, Portal LivRe and The Electronic <strong>Journal</strong>s Library.<br />
Any scientific journal aims to be indexed by PubMed and this request can only be made after several issues with strong, evidence<br />
based and well conducted studies have been published at this journal. Therefore, our priority in the next two years is to improve<br />
the quality of our published articles in order to have <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> indexed in PubMed and Scopus as soon as possible. In<br />
the mean- time, we wish to grow and become the leading provider of evidence-based information for dentists in the Middle East<br />
and North Africa region.<br />
Publishing at <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong><br />
Our new editorial team has taken a clear decision to only accept well conducted clinical studies, clinical audits and rare case<br />
reports providing an up-to date, evidence based mini review is enclosed as part of that article. Priority in publishing will<br />
always be given to higher quality clinical studies rather than to the date of acceptance. We would like to invite all our readers;<br />
academics and clinicians to submit to <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> and in return we promise a quick and efficient reviewing process and<br />
publishing good quality articles in no time in addition to exposing your clinical work and yourself to more than 30.000 readers<br />
in more than 28 countries.<br />
1 st <strong>Smile</strong> <strong>Dental</strong> Symposium: “Implant Dentistry: Is Quicker Always Better?”<br />
Our mission at <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> has always been to bridge the gap between evidence based dentistry and clinical practice.<br />
For the last five years our focus was mainly on the hard and electronic copies of our journal as main tools to implement our<br />
mission and spread the message, but today, recognizing the importance of continual education as one of the tools in bridging<br />
the gap between the up to date evidence based literature and day to day clinical practice, we at <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> are<br />
delighted to invite you all to our 1 st <strong>Smile</strong> <strong>Dental</strong> Symposium which will be on Implant Dentistry. This clinical symposium which<br />
will be at the continual education centre in the University of Jordan in Amman, on 17 th November 2011, will be run by Professor<br />
Dr. Marco Esposito and our editorial director; Dr. Hassan Maghaireh and will be on the importance of timing of dental implants<br />
placement and loading. The up to date evidence on immediate implants, clinical scenarios and tips & hints will be presented and<br />
discussed at this one day symposium.<br />
Dr. Mamoon Salhab Tamimi<br />
Director<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong><br />
| 6 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 12 - 2011
1 st <strong>Smile</strong> <strong>Dental</strong><br />
Symposium<br />
First Announcement<br />
17 – 18 November 2011<br />
Amman – Jordan<br />
“<strong>Dental</strong> Implants<br />
Is Quicker Always Better?”<br />
Prof. Dr. MARCO ESPOSITO<br />
Editor of the Cochrane Oral Health<br />
Group, The University of Manchester, UK<br />
Assoc. Prof. in Biomaterials, Göteborg<br />
University, Sweden<br />
Editor-in-Chief of the European <strong>Journal</strong> of<br />
Oral Implantology (EJOI)<br />
Editor of the Rivista Italiana di Stomatologia,<br />
Italy<br />
Specialist Periodontists, UK<br />
Dr. HASSAN MAGHAIREH<br />
Clinical Teacher in Implant Dentistry,<br />
The University of Manchester, UK<br />
Editorial Director of <strong>Smile</strong> <strong>Dental</strong><br />
<strong>Journal</strong><br />
Editorial Board, European <strong>Journal</strong> of<br />
Oral Implantology<br />
Senior Clinical Mentor, Association of<br />
Implant Dentistry (ADI), UK<br />
Implant Private Practice, Leeds, UK<br />
Post Symposium Clinical Course<br />
Soft Tissue Management Around <strong>Dental</strong> Implants<br />
This course includes tutorials on basic and advanced<br />
soft tissue management and designed to provide<br />
clinicians with the knowledge, skill sets and confidence<br />
in raising and managing flaps for implant surgery.<br />
More info:<br />
www.smiledentaljournal.com<br />
symposium@smile-mag.com<br />
+962 795556333
Zirconia All-Ceramic Restorations:<br />
Do They Perform Well?<br />
Ahmad Jum’ah<br />
BDS(Hons), MSc/PhD (Clin) Student-First year<br />
Restorative Dentistry Department, Leeds <strong>Dental</strong> Institute, University of Leeds, UK<br />
dnaahj@leeds.ac.uk<br />
The extensive use of ceramics in industrial, medical and<br />
dental fields makes this period of time a good candidate<br />
to be named as the “Ceramic age” (Vagkopoulou et<br />
al. 2009). In dentistry, PFM (Porcelain Fused to Metal)<br />
restorations are among the most commonly prescribed and<br />
serviceable restorations with the longest and most traceable<br />
record of predictable performance. However, driven by<br />
the extraordinary increase of aesthetic demands, concerns<br />
about allergies and systemic effects of metal alloys, and<br />
adverse effects of destructive tooth preparation for PFM<br />
restorations, light has been shed on all-ceramic restorations<br />
and rigorous research and development in this field has<br />
been performed. The ambition of complete replacement<br />
of PFM restorations with all-ceramic counterparts was<br />
curbed by the brittleness and limited flexural strength of the<br />
latter especially in areas subjected to high occlusal forces.<br />
Development of high strength zirconia and alumina cores<br />
seems to be potentially effective to overcome this problem.<br />
Partially stabilized zirconia based ceramics have distinct<br />
mechanical and optical properties and exhibit a very<br />
high biological compatibility with the oral environment:<br />
consequently, huge amount of research has been<br />
directed toward this material. Thus, clinicians should<br />
be aware of the current evidence and literature about<br />
zirconia all-ceramic restorations and their clinical<br />
serviceability in order to communicate with patients on<br />
solid scientific bases, clearly describe pros and cons<br />
of such restorations, and deal with the material in the<br />
proper way to guarantee better longevity.<br />
As is the case with all new dental materials, clinicians<br />
should bear in mind that the evidence available about<br />
zirconia is largely based on in vitro studies that might be<br />
inapplicable to some clinical situations and the long term<br />
clinical trials are scarce. In general, clinical data about<br />
this material is of a short term and unfortunately, many<br />
contradictory findings are present. This article briefly<br />
envisages these findings, and attempts to establish a<br />
well-structured argument that will help the reader to<br />
get a broader image about the performance of these<br />
restorations in terms of their functional, aesthetic, and<br />
biological characteristics.<br />
Recently, zirconia or “Ceramic steel” has been used<br />
extensively in fabrication of extra-coronal restorations<br />
especially, crowns and FPDs (Fixed Partial Dentures).<br />
This is largely attributed to the excellent mechanical<br />
properties the material exhibits and increasing<br />
popularity of CAD/CAM technology. The evidence<br />
from experimental work by Guazzato et al. 2004<br />
indicates that the core of the all-ceramic crown dictates<br />
the fracture strength of the restoration. Thus, utilizing<br />
zirconia as substructure guarantees high success rate for<br />
such restorations. Clinical trials studying the performance<br />
of zirconia single crowns are few; most clinical trials<br />
examined the performance of multiunit restorations. In<br />
their 3-year clinical study, Beuer et al. 2010 reported<br />
that none of fifty single crowns failed at the end of the<br />
observation period. However, fractured lingual cusps of<br />
all-ceramic crowns used to restore mandibular molars is<br />
a frequent technical complication that has been reported<br />
by Raigrodski et al. 2006. Area-specific modification of<br />
the core design and thickness was suggested to increase<br />
support for the veneering porcelain. Silva et al. 2010<br />
found increased reliability of modified Y-TZP (Lava)<br />
crowns while such an improvement wasn’t demonstrated<br />
by Lorenzonis’ et al. study in the same year.<br />
In contrary to his findings regarding single crowns,<br />
Guazzato et al. 2004 stated that the strengthening<br />
action of the Y-TZP is outweighed by the weaker<br />
veneering porcelain in case of FPDs. This experimental<br />
finding has been substantiated by number of clinical<br />
studies that reported high incidence of chipping or<br />
complete delamination of veneering porcelain. Poor<br />
mechanical properties of the veneering porcelain and<br />
“a weak interface” between zirconia core and veneer<br />
are blamed for such complications. The former is a<br />
well-accepted justification for minor chipping especially<br />
when low fusing ceramics are used while some authors<br />
cast doubt that the weak interface even exists. Bond<br />
strength between zirconia core and veneering porcelain<br />
was found to be similar to the bond in metal ceramic<br />
samples used as controls (Al-Dohan et al. 2004). This<br />
in vitro finding was substantiated by Raigrodski et al.’s<br />
2006 clinical study who reported absence of adhesive<br />
failures at the interface after 3 years follow-up period.<br />
However, the amount of evidence demonstrating the<br />
role of -“a weak interface”- in zirconia FPDs seems to be<br />
convincing (Aboushelib et al. 2007).<br />
| 8 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
Clinical studies reported 73.9-100% survival rate of<br />
zirconia all-ceramic FPDs over 2-5 years observation<br />
periods. The most common complication (15% in 3<br />
studies) was veneer layer chipping or delamination<br />
(Sailer et al. 2007, Raigroski et al. 2006, and Vult von<br />
Steyern et al. 2005). Framework fracture was a far rarer<br />
complication and found to be as low as 0-2.2% in some<br />
studies (Sailer et al. 2006, 2007). The high complication<br />
rate in some studies may be worrying especially when<br />
compared to survival rate of PFM FPDs which is 94.4%<br />
for 5 years as estimated in the systematic review by Sailer<br />
et al. 2007. However, Denry and Kelly 2008 remarked<br />
that replacement of any restoration due to veneer layer<br />
crazing or chipping was not needed. The oscillation of<br />
complication and survival rates between different studies<br />
necessitates careful interpretation and paying attention<br />
to what is deemed to be failure. From a clinical point<br />
of view, the restoration is successful if it does not need<br />
further intervention or remaking, and it maintains health,<br />
function and aesthetics (Ahmad 2006).<br />
The amount of research tackling mechanical properties<br />
of zirconia dental ceramics far exceeds that investigating<br />
wear properties of this material. This is largely attributed<br />
to the fact that wear properties of veneered zirconia<br />
restorations are primarily dictated by those of the<br />
veneering porcelain and the clinical applications of<br />
unveneered zirconia are not so popular and limited to<br />
cases of lack of interocclusal clearance, compromised<br />
abutments and resin-bonded and inlay-retained zirconia<br />
FPDs. In 2010, two papers published on the wear of<br />
unveneered zirconia, one investigated the antagonistic<br />
tooth wear (wear of the tooth structure opposing to<br />
restoration) and found that unveneered zirconia is<br />
associated with a lower antagonistic tooth wear when<br />
compared to polished feldspathic porcelain (Jung et<br />
al.2010). The other study was by Albashaireh et al. who<br />
found that wear resistance of the zirconia ceramics is the<br />
highest when compared to others. These studies indicate<br />
that zirconia ceramics are compatible to opposing<br />
dentition and at the same time structurally stable. These<br />
results may be promising and encourage the use of<br />
unveneered zirconia especially in the era of improved<br />
shading techniques of zirconia frameworks; however<br />
the phenomenon of low temperature degradation –<br />
alternatively called aging- that causes slow material<br />
deterioration when exposed to wet environment is still<br />
troublesome and concerning.<br />
Bonding to zirconia poses a big challenge in some<br />
clinical situations as surface treatments used with glass or<br />
silica containing ceramics, e.g., hydrofluoric acid etching<br />
and silanization, have been found to be ineffective<br />
(Blatz et al. 2007). Use of adhesive cementation was<br />
found to have no effect on the performance of zirconia<br />
restorations, however it is still necessary when dealing<br />
with cases of compromised retention as in the case of<br />
short abutments or when using resin bonded zirconia<br />
FPDs (Komine et al. 2010). Lack of bonding also<br />
compromises the outcome of repairing delaminated<br />
veneering porcelain layer. in vitro studies investigated<br />
different surface treatments in attempts to overcome such<br />
problems, tribochemical silica coating (e.g. Rocatec ® and<br />
CoJet ® ), plasma spraying, pre-treatment with phosphate<br />
containing primers, airborne particles and etching with<br />
CO 2 laser were among those found to be effective.<br />
However, a recent report by Behr et al. 2011 found that<br />
silica coating and application of phosphate containing<br />
primers in addition to silanization was insufficient to<br />
attain a clinically acceptable bond strength which was<br />
predetermined as 10 MPa.<br />
Owing to their excellent optical properties, zirconia allceramic<br />
restorations are aesthetically appealing.<br />
Absence of the black line at the gingival margins is an<br />
important advantage of using white zirconia frameworks<br />
over PFM restorations. Translucency and opacity of<br />
zirconia frameworks vary between different systems.<br />
For example, a 0.5mm thick core made of In-Ceram<br />
Zirconia or Cercon is completely opaque, it is thus<br />
recommended to be used in cases when masking<br />
discoloured cores is necessary. On the other hand, Lava<br />
frameworks are considered to be semi-translucent and<br />
they are advantageous as they enhance the accurate<br />
reproduction and depth of the natural tooth shade.<br />
The introduction of coloured zirconia frameworks<br />
hypothetically enhances the overall colour matching,<br />
disputes the concerns about “too white frameworks”,<br />
negates the need for liner application -which was<br />
found to weaken core-veneer interface- and reduces<br />
the thickness of veneering layer. Aboushelib et al.<br />
2008 found that air-borne particle abrasion increased<br />
bond strength of the core-veneer interface when used<br />
with white zirconia framework in contrast to coloured<br />
ones. Furthermore, they stated that application of liner<br />
was found to enhance the bond in case of coloured<br />
frameworks yet, a high incidence of de-lamination<br />
was reported. Colored Cercon frameworks showed<br />
higher core-veneer bond strength than Lava despite the<br />
fact that their chemical composition was similar. They<br />
attributed this to the structural changes occurring as a<br />
result of different staining procedures. The significance<br />
of using coloured zirconia frameworks was assessed<br />
two years later by the same authors who concluded that<br />
this technique did not offer any direct advantage over<br />
the white zirconia frameworks layered with veneering<br />
porcelain. Finally, Jung et al. 2007 investigated soft<br />
tissue colour changes associated with veneered and<br />
unveneered zirconia. It was found that zirconia did not<br />
induce visible colour changes when thickness of mucosa<br />
was 2 and 3mm. Also, the colour change that occurred<br />
with 1.5mm thick mucosa was the least in case of<br />
zirconia when compared to titanium. This may indicate<br />
that gingival aesthetics are not affected when margins of<br />
zirconia restorations placed in a sub-gingival location.<br />
Results of in vitro and in vivo studies that proved high<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 9 |
iocompatibility of zirconia coupled with reduced<br />
bacterial and plaque colonization when compared to<br />
titanium encouraged the use of zirconia in implant and<br />
restorative dentistry as a material with periointegrative<br />
properties. Readers are referred to the excellent review<br />
by Hisbergues et al. 2008 for more information about<br />
the biocompatibility of zirconia and its applications in<br />
implant dentistry.<br />
Finally, there remain debatable questions to be asked<br />
when all-ceramic zirconia restorations are concerned.<br />
Firstly, if the tooth preparation guidelines are basically<br />
similar to PFM restorations and zirconia has no<br />
advantage over other types of all-ceramic restorations in<br />
cases of limited inter-occlusal space and para-functional<br />
habits, do we really get a benefit from substituting PFM<br />
restorations with zirconia in terms of conservation of<br />
tooth structure and dealing with difficult cases? Secondly,<br />
does the gain from excellent aesthetic, mechanical and<br />
biological properties outweigh the risk of restoration<br />
failure -mainly delamination- which was found to be very<br />
high in some studies? Thirdly, is there any guarantee<br />
that zirconia restorations will not massively fail in a<br />
manner analogous to zirconia heads used in total hip<br />
arthroplasty due to low temperature degradation?<br />
Answering these questions should be done through<br />
conducting long term clinical trials exploiting the results<br />
of in vitro research in hot topics like improving coreveneer<br />
interface utilizing different surface treatments and<br />
testing aging-free zirconia ceramics namely, zirconia<br />
toughened alumina and ceria-doped zirconia.<br />
Acknowledgment<br />
I would like to acknowledge with gratitude Dr. Brian<br />
Nattress for the clinical photographs, Professor David<br />
Wood for editing the paper and continuous support and<br />
Dr. Hassan Maghireh for his kindness and motivation.<br />
A clinical case of three-unit all-ceramic zirconia FPD over implants with an excellent aesthetic outcome. Zirconia abutments were used.<br />
Grasp and Safely Handle All Types of Crowns!<br />
Even on posterior teeth, placing a crown with Geko Tweezers ® is as easy as child's play.<br />
Autoclavable ultra-flexible silicone tips and Geko sticky paste (included in intro kit)<br />
guarantee perfect grip and time-savings when removing excess cement.<br />
This Intro kit contains:<br />
• 1 pair of Tweezers (autoclavable 135 °C/275 °F)<br />
• 20 silicone tips (autoclavable 135 °C/275 °F)<br />
• 1 syringe of sticky Geko paste<br />
| 10 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011<br />
www.wamkey.com
PowerPen<br />
International<br />
Dealers Welcome<br />
info@quicklase.com<br />
Cordless<br />
Soft Tissue<br />
Management<br />
Diode Laser<br />
Specifications:<br />
Dimensions length 195mm (with battery)<br />
Diameter 18 mm<br />
Weight < 200g, with battery attached<br />
Laser Diode Wavelength 810±10 nm<br />
Output Power 4w (Auto power)<br />
Operation Mode, continuous wave (CW)<br />
Fibre Tip Diameter 400 um / 200um<br />
Aiming Beam diode 650 nm, < 1mW output<br />
Battery Rechargeable 3.2 volt DC, 600mAh<br />
Laser specialist since 1992<br />
Can also be used with<br />
Whitening<br />
Systems<br />
UK & International<br />
+44 1227 780009<br />
PPEN2WQL240511RG
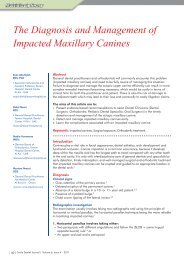
Ankyloglossia in a Pseudo-Class III<br />
Malocclusion: A Case Report<br />
Abstract<br />
This case report describes a 14 year old female patient, with pseudo-Class III incisor<br />
relationship on a mild Class III skeletal base with ankyloglossia. It highlights the<br />
relationship of an unfavorable soft tissue environment exerted by “tongue tie” and<br />
genetic factors proposed by the presence of family history in the development of a<br />
Class III malocclusion. Orthodontic treatment was provided on, a non-extraction basis<br />
to correct the Class III relationship. The patient was then referred for labial and lingual<br />
frenectomy using laser surgery to stabilize the achieved correction and facilitate the<br />
wear of orthodontic retainers by the patient. The first annual review carried out at the<br />
age of 17 years has revealed stable results.<br />
Keywords: Ankyloglossia, Pseudo Class III, Frenectomy.<br />
Salwa Jeragh Alhaddad<br />
BChD, MFDS RCSI, MSc<br />
Orthodontics, M’Orth<br />
RCSEng.<br />
Specialist Orthodontist at Ameri<br />
Hospital and Kuwait University<br />
Kuwait<br />
drjeragh@hotmail.com<br />
Mohammed Alnoori<br />
BDS, MS<br />
Senior Specialist Periodontist at<br />
Ameri Hospital<br />
Kuwait<br />
Manar Alnoori<br />
BDS, MFDS, MGD<br />
Ameri <strong>Dental</strong> Center<br />
Kuwait<br />
Introduction<br />
The etiology of malocclusions has been the subject of a long standing debate in the<br />
orthodontic literature. 1 The role of both genetic and soft tissue factors has been well<br />
established. Monozygotic twin studies suggested a complex interplay between the two<br />
factors. 2,3 Successful management of orthodontic patients is dependent on accurate<br />
identification of all etiological factors involved in the development of the malocclusion.<br />
With an estimated incidence of 4.8% 4 ankyloglossia is a congenital anomaly in which<br />
the mucous membrane under the tongue is too short, limiting the mobility of the<br />
tongue. The condition varies in the degree of its severity from mild mucous membrane<br />
bands to complete tethering of the tongue to the floor of the mouth. Patients with<br />
ankyloglossia frequently suffer from feeding, cleaning and swallowing difficulties, 5<br />
with the later being associated with anterior open bite due to a constant forced tongue<br />
thrust. 6<br />
Despite the lack of strong evidence, the constant forward tongue position has also been<br />
implicated, as a factor contributing to the establishment of a Class III malocclusion. 7<br />
Diagnosis and Aetiology<br />
A 14 year old female patient, with no relevant medical history, presented to our clinic<br />
with a chief complaint of upper midline diastema and inability to bite. Extraorally, the<br />
patient presented with a mild Class III skeletal pattern, slight maxillary hypoplasia,<br />
flattening of the malar base and increased lower anterior facial height.<br />
The family history revealed a genetic component towards Class III jaw relationship,<br />
with similar presenting features of the malocclusion evident in the patient’s father.<br />
The condition, however, was further complicated by the presence of ankyloglossia.<br />
Intraorally, she had a generally well aligned dentition with a 2mm maxillary midline<br />
diastema associated with a prominent labial frenum.<br />
In occlusion, the patient had a Class III incisal relation, with reverse overjet of 3mm<br />
following a displacement from an initial edge to edge incisal relation (centric relation to<br />
centric occlusion). The overbite was adequate with a 50% vertical overlap of the lower<br />
incisor. Canines and Molars were also in Class III relation. Ankyloglossia was evident,<br />
and the lower centre-line was displaced 2mm to the right of the patient’s mid-facial line<br />
due to mandibular shift on maximum intercuspal position.<br />
| 12 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
Pre Orthodontic intra-oral Views Pre Orthodontic Extra-oral Views<br />
A<br />
B C D<br />
E<br />
F<br />
G<br />
H I J<br />
(Picture 1) A: Initial facial view, B: Initial facial view with a smile, C: Initial 3-4 view, D: Initial lateral profile view, E: Initial<br />
incisal relation in centric relation, F: Initial incisal relation in centric occlusion, G: Initial right buccal segment in occlusion,<br />
H: Initial left buccal segment in occlusion, I: Initial occlusal view of the lower arch, J: Initial occlusal view of the upper arch.<br />
Cephalometric analysis confirmed a mild skeletal III<br />
pattern (ANB= -3 degrees), mild maxillary hypoplasia<br />
(Angle SNA=76 degrees), normal mandibular length,<br />
and dental compensation through retroclination of the<br />
lower labial segment (Angle LIMP=84 degrees) (Figure 1<br />
& Table 1).<br />
(Table 1)<br />
Measurement Value Norm Standard deviation<br />
SNA 77˚ 81˚ +/-2˚<br />
SNB 79˚ 79˚ +/-2˚<br />
ANB -2˚ 3˚ +/-1˚<br />
UIMP 109˚ 113˚ +/-6˚<br />
LIMP 84˚ 92˚ +/-6˚<br />
IIA 139˚ 135˚ +/-11˚<br />
MMPA 30˚ 24˚ +/-2˚<br />
SnMax 10˚ 8˚ +/-3˚<br />
LAFH 57% 55% +/-2%<br />
(Fig. 1) Patient’s lateral cephalogram tracing prior to<br />
orthodontic treatment.<br />
Rationale for Treatment<br />
Elimination of the forward mandibular posture was<br />
considered; to eliminate the risks of incisal attrition, root<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 13 |
esorption due to occlusal trauma, and reduce the stress<br />
on the tempomandibular joint as a result of repeated<br />
forward mandibular displacement.<br />
Correction of the lower centerline by eliminating<br />
the lateral mandibular displacement to the right on<br />
maximum intercuspal position, to enhance dental and<br />
facial aesthetics.<br />
Space closure within the maxillary arch was considered<br />
to give favorable aesthetics despite the added difficulty in<br />
Class III correction.<br />
Both patient and parents were informed, that patient’s<br />
co-operation in wearing Class III elastics played a key<br />
role in treatment success. Whilst the adverse effects of<br />
further forward mandibular growth were fully explained.<br />
Labial and lingual frenectomies using laser surgery were<br />
recommended to eliminate any potential role of these<br />
soft tissues in the etiology of the patient’s malocclusion,<br />
to help stabilize the orthodontic treatment outcome and<br />
to facilitate the wearing of retainers.<br />
Treatment<br />
The patient was treated on a non-extraction basis,<br />
keeping orthognathic surgery as a valid treatment option<br />
should future growth dictate it. Treatment objectives<br />
were, to close the spaces within the maxillary arch, and<br />
eliminate forward mandibular displacement.<br />
Upper and lower fixed appliances of MBT prescription,<br />
with a 0.022 inch bracket slot were bonded with the four<br />
first molars banded using Andrew’s prescription due to<br />
their characteristic lingual torque to maintain the molar<br />
relation.<br />
Treatment Results<br />
The patient completed the orthodontic treatment in 23<br />
months at the age of 16 years. Complete space closure<br />
with correction of the incisal relation were achieved<br />
enhancing the existing dentoalveolar compensation.<br />
The mandibular shift was eliminated successfully and<br />
the patient and parents were happy with the treatment<br />
outcome.<br />
Following debond, the patient was referred to undertake<br />
Post Orthodontic intra-oral Views Post Orthodontic Extra-oral Views<br />
A<br />
E<br />
H<br />
B C D<br />
F<br />
I<br />
G<br />
(Picture 2) A: Facial view, B: Facial<br />
smile, C: 3-4 view, D: Lateral profile<br />
view, E: Anterior view of the dentition in<br />
occlusion, F: Right view of the dentition<br />
in occlusion, G: Left view of the dentition<br />
in occlusion, H: Lower occlusal view, I:<br />
Upper occlusal view.<br />
| 14 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
laser frenectomy for the labial and lingual frenal<br />
attachments. Signs of healing were evident on the next<br />
day review and salt water mouth rinses in conjunction<br />
with routine tooth cleaning were advised.<br />
Upper and lower Begg style, wrap around retainers were<br />
A<br />
B<br />
(Picture 3) A: Anterior view one day post laser labial<br />
frenectomy, B: Lower occlusal view one day post laser<br />
lingual frenectomy.<br />
augmented with local anaesthesia for more severe<br />
cases as required. Laser surgery eliminates the need for<br />
general anaesthesia but it is essential that the patient<br />
is cooperative and remains motionless throughout the<br />
procedure. The procedure offers virtually no bleeding,<br />
with reduced reported pain and risk of infection.<br />
The “pseudo” nature of the Class III relationship in this<br />
case, may suggest a stronger influence of the soft tissue<br />
over the inherited genetics.<br />
However, it is very difficult to draw conclusions based<br />
on the presenting findings in isolation, regular reviews<br />
of future growth, as well as the stability of the achieved<br />
correction, are the only ways to determine the roles<br />
played by soft tissues and growth in the etiology of the<br />
malocclusion seen in this case.<br />
Cephalometric analysis at the first annual review at the<br />
age of 17 years, revealed a stable enhancement of the<br />
dental compensation presented initially at 14 years of<br />
age, with a 3 degrees increase in the upper incisor to<br />
maxillary plane angle (109 to 112 degrees, 8 degrees<br />
of retroclination of the lower labial segment with regard<br />
to the mandibular plane (84 to 76 degrees) and stable<br />
skeletal features and vertical proportions. (Figure 2 &<br />
Table 2).<br />
The stability observed in this case may suggest a<br />
potential relation between the unfavorable soft tissue<br />
“tongue tie” and the Class III malocclusion seen in this<br />
case.<br />
given to the patient emphasizing the importance of full<br />
time wear and the need for regular reviews until growth<br />
ceases. At the age of 17, the patient attended her first<br />
annual post-orthodontic treatment review with a stable<br />
treatment outcome.<br />
Discussion<br />
This case report highlights the role of both genetic<br />
influence proposed by the patient’s family history, as well<br />
as the role of unfavorable soft tissue environment exerted<br />
by ankyloglossia, in the development of a pseudo-Class<br />
III skeletal pattern in a 14 year old female patient.<br />
While accepting milder cases of ankyloglossia<br />
remains a common option, particularly if there was<br />
a lack of patient’s concern, surgical intervention<br />
may be considered in more severe cases. Different<br />
types of surgical procedures have been described<br />
in the literature. However, case selection remains<br />
the key to successful management. Surgical partial<br />
frenectomy, complete frenectomy, revision frenoplasty<br />
or electrocautery procedures have all been described. 8<br />
More recently, however, laser surgery has been used<br />
to relieve ankyloglossia. 9,10 Topical gel analgesia has<br />
been recommended for this procedure which may be<br />
(Fig. 2) Patient’s lateral cephalogram tracing after<br />
orthodontic treatment.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 15 |
(Table 2)<br />
Measurement Value Norm Standard deviation<br />
SNA 76˚ 81˚ -1˚<br />
SNB 79˚ 79˚ 0˚<br />
ANB -3˚ 2-4˚ -1˚<br />
UIMP 112˚ 113˚ +3˚<br />
LIMP 76˚ 92˚ -8˚<br />
IIA 142˚ 135˚ +3˚<br />
MMPA 30˚ 24˚ 0˚<br />
SnMax 10˚ 5-11˚ 0˚<br />
LAFH 57% 55% 0%<br />
Conclusion<br />
The coexistence of both genetic “family history”<br />
and soft tissue “tongue tie’’ factors and their<br />
association with the development of Pseudo Class<br />
III malocclusion has been highlighted in this case<br />
report. Special emphasis is placed on the need<br />
for accurate diagnosis, elimination of unfavorable<br />
features and regular reviews of future growth,<br />
as these are regarded as keys to successful<br />
management.<br />
References<br />
1. Subtelny JD. Malocclusions, orthodontic corrections<br />
and orofacial muscle adaptation. Angle Orthod.<br />
1970;40(3):170-201.<br />
2. Kawala B, Antoszewka J, Necka A. Genetic or environment?<br />
A twin-method study of malocclusions. World J Orthod.<br />
2007;8(4):405-10.<br />
3. Jena AK, Duggal R, Mathur VP, Parkash H. Class III<br />
malocclusion: Genetic or environment? A twin study. J Indian<br />
Soc Pedod Prev Dent. 2005;23(1):27-30.<br />
4. Messner AH, Anna H, Lalakea M, et al., Ankyloglossia:<br />
Incidence and associated feeding difficulties.<br />
Otolaryngology–Head and Neck Surgery. 2000;126:36-9.<br />
5. Messner AH and Lalakea ML, The effects of ankyloglossia on<br />
speech in children. Otolaryngology-Head and Neck Surgery.<br />
2002;127(6):539-45.<br />
6. Horton CE, Crawford HH, Adamson JE, et al. 1969,<br />
‘’Tongue-tie’’. The Cleft palate journal;6:8-23.<br />
7. ang SJ, Cha BK, Ngan P, Choi DS, Lee SK, Jang I.<br />
Relationship between the lingual frenulum and craniofacial<br />
morphology in adults. Am J Orthod Dentofacial Orthop.<br />
2011;139(4 Suppl):e361-7.<br />
8. Naimer S, Biton A, Vardy D et al., Office treatment<br />
of congenital ankyloglossia. Med Sci Monit.<br />
2003;9(10):CR432-5.<br />
9. Kotlow LA. Using the Erbium: Yag Laser to correct an<br />
abnormal lingual frenum attachment in newborns. The<br />
journal of the Academy of Laser Dentistry. 2004;12(3):22-3.<br />
10. Suter VG and Bornstein MM. Ankyloglossia: facts and myths<br />
in diagnosis and treatment. <strong>Journal</strong> of periodontology. 2009;<br />
80(8):1204-19.<br />
| 16 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
TM<br />
TREATMENT PROGRAM<br />
Finally, instant * sensitivity relief<br />
patients can take home.<br />
A breakthrough: Pro-Argin TM Technology<br />
The results are revolutionary<br />
BEFORE 1<br />
AFTER 1<br />
Instant relief achieved with direct application<br />
of toothpaste massaged on sensitive tooth for<br />
one minute and continued relief with subsequent<br />
twice-daily brushing 3<br />
In Vitro SEM photograph of untreated<br />
dentin surface.<br />
The tubules that lead to<br />
sensitivity are open<br />
In Vitro SEM photograph of dentin<br />
surface after application.<br />
The tubules are plugged<br />
for instant, lasting relief<br />
With Pro-Argin Technology, you can finally provide instant*<br />
and lasting relief from dentin hypersensitivity using the<br />
Colgate® Sensitive Pro-Relief Treatment Program:<br />
• In-office desensitizing paste<br />
• At-home everyday toothpaste<br />
Air blast sensitivity score<br />
3<br />
2<br />
1<br />
0<br />
Baseline<br />
60%<br />
Immediate<br />
70%<br />
improvement<br />
3-day<br />
Sensitivity relief<br />
When applied directly<br />
to the sensitive tooth<br />
with a fingertip and<br />
gently massaged for<br />
1 minute, Colgate ®<br />
Sensitive Pro-Relief<br />
Toothpaste provides<br />
instant sensitivity<br />
relief compared to the<br />
positive and negative<br />
controls. The relief was<br />
maintained after 3 days<br />
of twice-daily brushing.<br />
Pro-Argin Technology works through a natural process of<br />
dentin tubule occlusion that attracts arginine and calcium<br />
carbonate to the dentin surface to form a protective seal<br />
that provides instant relief. 2<br />
Colgate ® Sensitive Pro-Relief Toothpaste<br />
Positive control:<br />
Toothpaste with 2% potassium ion<br />
Negative control:<br />
Toothpaste with<br />
1450 ppm<br />
fluoride only<br />
* Instant relief is achieved with direct application of toothpaste massaged on<br />
sensitive tooth for 1 minute.<br />
Scientific works cited: 1. Petrou I et al. J Clin Dent. 2009;20(Spec Iss):23-31. 2. Cummins D et al. J Clin Dent. 2009;20(Spec Iss):1-9.<br />
3. Nathoo S et al. J Clin Dent. 2009;20(Spec Iss):123-130.<br />
Visit www.colgateprofessional.com to learn more<br />
about how instant relief from dentin hypersensitivity<br />
can impact your practice.<br />
YOUR PARTNER IN ORAL HEALTH
In-House Maxillofacial 3D Rapid<br />
Prototyping<br />
Abstract<br />
Three-Dimensional Imaging (3D) and rapid prototyped (RP) planning models have<br />
been reported many times in the past two decades. It has always been described as<br />
an excellent diagnostic tool. 1 The major limitations are the increased time needed 2<br />
especially in management of emergency cases 3,4 and increased costs. 4,5 Some of<br />
the technical and organisational issues encountered in the implementation of this<br />
technology in a modelling service have been addressed elsewhere. 6<br />
In this note I will describe the office based system, advantages, technique, and current<br />
applications.<br />
Wesam Aleid<br />
BDS, MBBS, MRCSEd<br />
(Surgery-in-General),<br />
FFDRCSI (OSOM), FRCSEd<br />
(OMFS)<br />
Oral, Maxillofacial, and Head<br />
& Neck Surgeon<br />
eidwisam@yahoo.com<br />
Keywords: Three-Dimensional Imaging, Prototyping, Trauma, Oncology, Facial<br />
Prosthesis.<br />
Satellite RP Bureaus are expensive to set up (high cost machinery and overheads).<br />
Making profit relies on wide service provision and high numbers. Office based<br />
systems are far less expensive, require smaller premises and use simpler technology.<br />
Technology choices are limited to 3D printers (Gypsum/Starch based) (Figure 1), Fusion<br />
deposition modelling (FDM - ABS plastic based) (Figure 2) or Thermojet- Wax based<br />
systems.<br />
The ZCorp 310 Plus is a 3D Gypsum based printer. It is relatively cheap, fast (4 hours<br />
for a full skull), easy to maintain, accurate (+- 0.1mm in Z plane, +-0.2mm in the X,<br />
Y planes), cost effective (£1cm3) with low waste, has small proportions and its output<br />
models can be made with different properties (hard, soft, flexible).<br />
Utilizing MIMICS Z software, the system can be used to identify different types of body<br />
tissues, by selecting predefined threshold setting (Figure 3). Being an office based<br />
systems the clinician have the control of the interface with the use of Computer Aided<br />
Design (CAD) for image manipulation.<br />
(Fig. 1) 3-D Printer (Gypsum based).<br />
(Fig. 2) FDM (ABS plastic based).<br />
| 18 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
Technique<br />
Data can be acquired using a laser surface scanner<br />
(Figure 4), a photographic surface scanner or a CT scan.<br />
CT is the preferred medium. The CT data (Dicom) then<br />
can be transferred on a CD, into an ordinary windowsoperated<br />
computer. The Dicom is then converted using<br />
MIMICS Z software (Materialize, Belgium) which allows a<br />
some image manipulation (Figure 3). Following selection<br />
of the required threshold setting image noise and<br />
artefacts can be reduced to define any required structure<br />
(Figure 5).<br />
(Fig. 5) Image noise and artefact reduction.<br />
The image is then exported to the ZCorp proprietary<br />
software (ZPrint V 7.6) and placed into the virtual build<br />
area of the printer. Multiple images can be placed into<br />
the build area to maximise its use. The print head expels<br />
a binding solution onto a powder surface. This moves<br />
down a layer and a new powder is distributed. This next<br />
layer is then built on the first, building a solid 3D model.<br />
The powder that is not used supports the built structure.<br />
The unused powder is vacuumed from around the model<br />
exposing its surface (Figure 6). The model is very porous<br />
and can be infiltrated with different solutions to create<br />
different properties.<br />
(Fig. 3) Software (tissue identification).<br />
(Fig. 6) 3-D Model Building.<br />
This technology can successfully be used for planning<br />
of trauma (Figure 7) and oncology cases, osteotomies,<br />
radiotherapy, burns (Figure 8), facial prosthetics, and<br />
deep buried implant design and manufacture (Figure 9). 7<br />
(Fig. 4) Laser surface scanner.<br />
In summary, rapid prototyping is not new but the use<br />
of in-house RP, has wide applications in maxillofacial<br />
surgery, and huge potential for service development.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 19 |
(Fig. 7) Complex Maxillofacial<br />
Trauma.<br />
(Fig. 8) Mask prepared<br />
using 3-d Prototyping<br />
for Burn Patient.<br />
(Fig. 9) Software interface in preperation of deeply burried<br />
skull implant.<br />
Acknowledgement<br />
Special thanks to Mr. J Watson for the provision of the<br />
excellent photographs and the superb technical work to<br />
produce these models.<br />
References<br />
1. Aleid W, Watson J, Sidebottom A, Hollows P. Development of<br />
in-house rapid manufacturing ofthree-dimensional models in<br />
maxillofacial surgery. Br J Oral Maxillofac Surg. 2010;48:479-81.<br />
2. Kernan T., Wimsatt A. Use of a Stereolithography Model for<br />
Accurate, Preoperative Adaptation of a Reconstruction Plate. J Oral<br />
Maxillofac Surg. 2000;58:349-51.<br />
3. Arvier JF, Barker TM, Yau YY, D’Urso PS, Atkinson RL, McDermant<br />
GR. Maxillofacial biomodelling. Br J Oral Maxillofac Surg.<br />
1994;32:276-83.<br />
4. Al-Sukhun J, Helenius M, Lindqvist C, Ashammakhi N, Törnwall<br />
J, Penttila H. Stereolithography and the use of pre-adapted or<br />
fabricated plates for accurate repair of maxillofacial defects.<br />
Corrected Proof, 30 November 2006 Br J Oral Maxillofac Surg<br />
DOI: 10.1016/j.bjoms.2006.10.016<br />
5. Cunningham L, Madsen M, Peterson G. Stereolithographic<br />
Modeling Technology Applied to Tumor Resection. J Oral<br />
Maxillofac Surg. 2005;63:873-8.<br />
6. Sugar A, Bibb R, Morris C, Parkhouse J. The development of a<br />
collaborative medical modelling service: organisational and technical<br />
considerations. Br J Oral Maxillofac Surg. 2004;42:323-30.<br />
7. Chandra A, Watson J, Rowson J.E, Holland J, Harris R A, Williams<br />
D J. (2005) Application of rapid manufacturing techniques in<br />
support of maxillofacial treatment; evidence of the requirements of<br />
clinical applications. <strong>Journal</strong> of Engineering and Manufacturing;<br />
ImechE Vol 219 Part B.<br />
| 20 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
3D Innovations of Cranioplasty Plate<br />
Construction: a Case Report<br />
Abstract<br />
Titanium cranioplasty is one of the well-established and widely used techniques<br />
in restoring skull defects for optimal protection to skull internal structures and reestablishing<br />
skull conformity. Nowadays, most centres utilise computer-assisted<br />
reconstruction for manufacture of titanium plates. In this paper we presented a method<br />
for making titanium cranioplasty plates using the 3D innovation through making a 3D<br />
model.<br />
It can be stated that computer assisted production titanium plate for repairing skull defects<br />
is hassle free to patient and prosthetists, efficient and reliable, accurate and reproducible<br />
method. Furthermore, the resultant prosthesis constructed is accurately fitting.<br />
Muhanad M. Hatamleh<br />
BSc, MPhil, MSc (Health<br />
Mgmt), MaxFac Dip, PhD<br />
Tutor, School of Dentistry,<br />
University of Manchester.<br />
Trainee, Maxillofacial<br />
Prosthetics and Technologies,<br />
Queen Medical Centre,<br />
Nottingham University Hospital<br />
Trust, Nottingham, UK<br />
muhanad.hatamleh@<br />
manchester.ac.uk<br />
Jason Watson<br />
BMed Sc, MIMPT<br />
Consultant, Maxillofacial<br />
Prosthetists and Healthcare<br />
Scientist, Maxillofacial Dep.,<br />
Queens Medical Centre<br />
Campus, Nottingham<br />
University Hospital Trust, UK<br />
jason.watson@nuh.nhs.uk<br />
Keywords: Titanium, Cranioplasty, Skull defects, Three-Dimensional Model.<br />
Introduction<br />
Maxillofacial prosthetics are defined as “ the art and science of anatomical, functional or<br />
cosmetic reconstruction by means of artificial substitutes of those regions in the maxilla,<br />
mandible, and face that are missing or defective because of surgical intervention,<br />
trauma, pathology, or developmental or congenital malformation”. 1 Facial defects often<br />
result in devastating cosmetic, functional and psychological consequences and continue<br />
to require difficult and challenging management procedures from maxillofacial surgeons<br />
and prosthodontics alike.<br />
Complete rehabilitation of patients with disfigurements (i.e. facial, skull) is achieved using<br />
a multidisciplinary team approach, involving both surgical and prosthetic personnel.<br />
The role of technology in facial prosthetics is vital in transforming the fabrication process<br />
of facial prosthetics. It spans wide uses including computerized shade selection, threedimensional<br />
digital photography, virtual surgical planning, surface scanning, and threedimensional<br />
imaging to obtain the wax pattern. 1<br />
Three-dimensional photography and surface scanning have been achieved using<br />
Phase measuring profilometry (PMP), CAD/CAM technology and laser scanning. 1-4 A<br />
cranioplasty is the term that relates to the procedure of repairing skull bone defect, 5<br />
to provide neural protection to the internal skull structures (including the brain) in an<br />
aesthetically desirable and functional way. Ideally, bone flap is removed during the<br />
operation and is stored for later insertion. However, in most cases a bone flap may not<br />
be available to repair, especially trauma defects caused by congenital abnormalities,<br />
comminuted or compound fractures, skull tumours, osteomyelitis or bone flap<br />
resorption. 6,7 Thus, many substitute materials proven to have high biocompatibility and<br />
clinical reliability, such as Poly Methyl Metha crylate (PMMA), titanium, and ceramics 6<br />
and it is still unclear of the optimum material. However, titanium plates offer an excellent<br />
choice for cranioplasty based on their strength, low infection rate, biocompatibility,<br />
handling characteristics and being suitable for postoperative imaging techniques. 6 There<br />
have been different methods documented in the literature to manufacture titanium plates<br />
including conventional impression techniques or computer assisted technique. 8-10<br />
| 22 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
Techniques of plate fabrication have often been<br />
difficult and inexact. Additionally, producing a cosmetic<br />
deformity, poorly shaped prostheses may be problematic<br />
to insert which subsequently cause scalp necrosis,<br />
perforation and infection. 7 Modern computer technology<br />
enables three-dimensional (3D) reconstruction of<br />
computer tomography (CT) images. Usually these 3D<br />
reconstructions are viewed as two dimensional (2D)<br />
images. Models produced by these CT scans are of<br />
high accuracy, details and reproducible. Furthermore,<br />
these models enable the operator for better visualisation<br />
of the defect in 3D orientation and thus better results<br />
are achieved when compared to conventional casts<br />
produced by traditional impression techniques. This<br />
paper aims to present a method of making titanium<br />
cranioplasty plate utilizing 3D innovations.<br />
Case History and Presentation<br />
Diagnosis: A 26 year old female teacher was originally<br />
admitted to Kings Mill Mansfield A&E department<br />
(Nottingham, UK) following a sudden onset occipital<br />
headache. A CT scan showed subarachnoid blood and<br />
was transferred to the neurosurgical unit at Queens<br />
Medical Centre (QMC, Nottingham, UK). She was found<br />
to have a large left deep cerebral Venous Malformation<br />
(VM) on CT angiogram. She underwent a partial<br />
embolisation of this VM complicated by intra-vetricular<br />
re-bleed. Her GCS (Glasgow Coma Score) were initially<br />
well being at 14-15 however, 7 days post procedure she<br />
developed dense right hemiparesis and became aphasic<br />
secondary to vasospasm. Her GCS dropped to 4. A CT<br />
showed large left-sided maturing infarct with global left<br />
hemispheric swelling and mild sub-falcine herniation.<br />
The same day she underwent a left decompressive<br />
cranioectomy. Later, she underwent tracheostomy and<br />
her GCS improved to 11.<br />
Her management plan included physiotherapy, speech<br />
and language therapy and occupational therapy prior<br />
to transfer to a rehabilitation unit. Follow up showed<br />
that she improved. On examination her face is moving<br />
symmetrically and she still has good sensation in her right<br />
arm and leg. Her left craniotomy wound has healed nicely.<br />
2. MCS extension files were converted to files with PR<br />
extension that makes them compatible (readable) with<br />
the Z print software (Z Corp 310 plus print system,<br />
Burlington, MA, USA). A 3D virtual model was produced<br />
giving us the potential for rotating and slicing. The CT<br />
scan files enabled us to customize the area of interest for<br />
printing as only the defect was sent for printing rather<br />
than printing the entire skull (Figure 1).<br />
3. The printer formed the 3D model by binding gypsum<br />
powder (ZB 140, Z Corp, USA) particles using clear<br />
binder solution (ZB 60, Z Corp, USA) and water in<br />
layering technique. Then the mould was sealed and<br />
made ready for waxing up.<br />
(Fig. 1) 3D CT scan Imported into MIMICS (A), modelling<br />
(B) and slicingpossibilities (C) and production of the working<br />
template (D) in Z PRINT Software.<br />
2. Titanium plate production: Steps are illustrated<br />
in figure 2. The defect was restored by waxing up<br />
to normal conformity, and then it was duplicated in<br />
crystal cal (Stone Type IV, British Gypsum, UK). An<br />
impression of the wax and surrounding area is taken<br />
using alginate (Hydrogum, Coltene, UK) which is backed<br />
with plaster (Sugical plaster, British Gypsum, UK). Then<br />
the impression was cast with vacuum mixed crystal cal<br />
gypsum. Using an indelible pencil a line outlining the<br />
defect margin was drawn, and another line was drawn<br />
Next steps of treatment are titanium cranioplasty<br />
manufacture and fitting and further treatment of her<br />
residual deep VM.<br />
Cranioplasty Manufacture<br />
1. Production of 3D model: A three dimensional (3D)<br />
CT of the defect has been conducted in order to produce<br />
a 3D model of the defect following these steps:<br />
1. CT scans are produced as DICOM digital format.<br />
These are then converted using MIMICS (Materialize,<br />
Belgium) into MCS extension files. These files were<br />
converted to STL (Standard Triangulation Language). This<br />
is an open format that is possible to be opened by most<br />
3D manufacture machines world wide.<br />
(Fig. 2) Steps followed in constructing the titanium plate.<br />
The 3D model produced (A&B), defect wax up (C), stone<br />
duplication (D), titanium plate swaging (E) and final<br />
titanium plate prior to sterilization (F).<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 23 |
5mm outside the defect line. These lines determine the<br />
periphery of the final titanium implant.<br />
The model is then invested in a large flask to produce<br />
the die, which was then separated with mould seal<br />
(Vertex, Bracon, UK) and topped with another crystal cal<br />
mix to produce the counter-die. Then a piece of titanium<br />
plate (0.5 mm, Titanium International, UK) is cut, larger<br />
than the defect and placed between the two halves of<br />
the flask, and the flask was closed slowly using hydro<br />
press to swage the plate to the desired shape. Then the<br />
flask was opened after couple of hours and the excess<br />
was cut. It was closed, and tightened and placed under<br />
bench press, and the opening/closing process was<br />
repeated couple of times (over 5 days period) till the<br />
implant has been swaged to the desired contour. The<br />
periphery rounded using rubber wheels, and holes (for<br />
screws fixing) were drilled. The implant was cleaned and<br />
sterilized (10w Steam at 132°C) prior to sending it to<br />
theatre.<br />
Discussion<br />
The need for precision-fitting titanium plates has<br />
prompted the development of several computeraided<br />
methods of cranioplasty plate manufacture.<br />
Defects have been modelled from CT scan data using<br />
SLA (Stereolithography), LOM (Laminated Object<br />
Manufacture), Thermojet Wax Printer, SLM (Selective<br />
Laser Melting), and FDM (Fused Deposition Modelling).<br />
On one hand, titanium cranioplasty plates manufactured<br />
using most of these methods have been reported to fit<br />
even the most complex defects, are easy to insert, and<br />
produce excellent cosmetic results. 7 Furthermore, 3D<br />
modelling and scanning technique have been related to<br />
storage saving in addition to reproducibility (meaning<br />
ability to cast as much models as needed without the<br />
need to take another impression) and being patient<br />
friendly.<br />
On the other hand, the main disadvantage of these<br />
computer-assisted techniques is capital. It is necessary<br />
to have access to a computer work station with a large<br />
memory capacity and running appropriate software that<br />
will render the CT data. The final cost of the titanium<br />
plate would be about £695 which is the sum of the<br />
cost of running the work station, royalties for using the<br />
software, maintenance contract annual, production<br />
of the model by a computer modelling technique and<br />
fabrication of the titanium prosthesis. For difficult and<br />
complex cases, the improvement in cosmetic results and<br />
the probable reduction in complication rates would justify<br />
the cost. However, it needs to be said that the expense<br />
and time involved in producing a plate may currently<br />
preclude the routine use of the computer techniques,<br />
but as equipment costs and production time diminish,<br />
this may become the standard allograft cranioplasty<br />
technique.<br />
A side form the technological aspect, titanium sheet is<br />
a commonly used material for cranioplasty. While it is<br />
a safe and highly biocompatible material, it can modify<br />
the presentation of post-operative complications, 11<br />
thus we are currently in the process of investigating the<br />
possible use of net shaped glass fibres that have been<br />
used in crown and bridge restoration in what is known<br />
as all-polymer fixed prostheses. They have shown similar<br />
or increased mechanical properties in comparison to<br />
conventional metal ceramic prostheses, indicating fibres<br />
as suitable substitutes for metal FPDs. 12 They are highly<br />
aesthetic and easy to manipulate and work with. We<br />
expect that this new technique in comparison to the<br />
conventional titanium-plate technique will save time,<br />
effort, materials and subsequently cost.<br />
Recommendations for future use of CT scans and<br />
measurements are to create an analogue without the<br />
cost and time required for an SLA model.<br />
Summary<br />
Computer assisted production of titanium plate for<br />
repairing skull defects is hassle free to patient and<br />
prosthetists, efficient and reliable, accurate and<br />
reproducible method. Furthermore, the resultant<br />
prosthesis constructed is accurately fitting.<br />
References<br />
1. Davis, B.K., The role of technology in facial prosthetics. Curr Opin<br />
Otolaryngol Head Neck Surg. 2010;18(4):332-40.<br />
2. Wu, G., et al., Computer-aided design and rapid manufacture of<br />
an orbital prosthesis. Int J Prosthodont. 2009;22(3):293-5.<br />
3. Ciocca, L. and R. Scotti, CAD-CAM generated ear cast by means<br />
of a laser scanner and rapid prototyping machine. J Prosthet Dent.<br />
2004;92(6):591-5.<br />
4. Feng, Z., et al., Computer-assisted technique for the design and<br />
manufacture of realistic facial prostheses. Br J Oral Maxillofac<br />
Surg. 48(2):105-9.<br />
5. Department of Neurosurgery, B., Havering and Redbridge<br />
Hospitals NHS Trust, Your Operation: Cranioplasty. http://www.<br />
bhrhospitals.nhs.uk/neuro/pdfs/neuropicranioplasty.pdf [Accessed<br />
December 2010], 2010.<br />
6. Cabraja, M., M. Klein, and T.N. Lehmann, Long-term results<br />
following titanium cranioplasty of large skull defects. Neurosurg<br />
Focus. 2009;26(6):E10.<br />
7. Stoodley, M., J. Abbott, and D. Simpson, Titanium cranioplasty<br />
using 3-D computer modelling of skull defects. <strong>Journal</strong> of Clinical<br />
Neuroscience. 1996;3(2):149-55.<br />
8. Bhargava, D., et al., Construction of titanium cranioplasty plate<br />
using craniectomy bone flap as template. Acta Neurochir (Wien).<br />
152(1):173-6.<br />
9. Bartlett, P., L.M. Carter, and J.L. Russell, The Leeds method for<br />
titanium cranioplasty construction. Br J Oral Maxillofac Surg.<br />
2009;47(3):238-40.<br />
10. Joffe, J.M., S.R. Nicoll, R. Richards, A.D. Linney, and M. Harris,<br />
Validation of computer-assisted manufacture of titanium plates for<br />
cranioplasty. Int J Oral Maxillofac Surg. 1999;28(4):309-13.<br />
11. Martin, M.P. and S. Olson, Post-operative complications with<br />
titanium mesh. J Clin Neurosci. 2009;16(8):1080-1.<br />
12. Unlu, N. and S. Belli, Three-year clinical evaluation of fiberreinforced<br />
composite fixed partial dentures using prefabricated<br />
pontics. <strong>Journal</strong> of Adhesive Dentistry. 2006;8(3):183-8.<br />
| 24 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
Confusing Endodontic Cases<br />
Case Series Report<br />
Abstract<br />
Here, we introduce some confusing endodontic cases, which we had experienced in<br />
our clinic. The first case had been misdiagnosed as a skin lesion and received extended<br />
skin treatment. The second case had been misdiagnosed as a periodontal lesion and<br />
received periodontal treatment by two former dentists. The third case exhibited oral<br />
malodor and the patient worried about his breath odor for a long period. These three<br />
cases have received endodontic treatment in our clinic, and the patients were free from<br />
their long-lasting problems. We also discuss other confusing cases with literature minireview.<br />
Keywords: Diagnosis, Endodontics, Skin Lesion, Periodontics.<br />
Masahiro Yoneda<br />
Section of General Dentistry,<br />
Department of General<br />
Dentistry, Fukuoka <strong>Dental</strong><br />
College, Fukuoka, Japan<br />
Yoneda@college.fdcnet.ac.jp<br />
Nao Suzuki<br />
Section of General Dentistry,<br />
Department of General<br />
Dentistry, Fukuoka <strong>Dental</strong><br />
College, Fukuoka, Japan<br />
Sonia M. Macedo<br />
Faculdade de Odontologia da<br />
Universidade de São Paulo<br />
São Paulo, Brazil<br />
Hisashi Anan<br />
Section of Operative<br />
Dentistry and Endodontology,<br />
Department of Odontology,<br />
Fukuoka <strong>Dental</strong> College<br />
Fukuoka, Japan<br />
Takao Hirofuji<br />
Section of General Dentistry,<br />
Department of General<br />
Dentistry, Fukuoka <strong>Dental</strong><br />
College, Fukuoka, Japan<br />
Introduction<br />
Making a diagnosis is one of the most important stages in dental treatment. We<br />
sometimes encounter endodontic cases in which making a straight forward diagnosis<br />
can be a real challenge. Furthermore, endodontic lesions sometimes manifest<br />
symptoms that are similar to those of other diseases. However, one of the difficult<br />
points in endodontic treatment is that the lesion cannot be seen from the outside, and<br />
unless we take a 3D radiograph, we need to speculate about what is happening in<br />
the bone. It is also dangerous for dentists to make a diagnosis with preconceptions.<br />
Here, we report endodontic cases that had been misdiagnosed as skin or periodontal<br />
diseases. Conversely, certain diseases, including malignant diseases, are sometimes<br />
misdiagnosed as endodontic lesions. We also present a literature review of these<br />
diseases that show similar manifestations to endodontic disease.<br />
Case Reports on Endodontic Lesion-derived Symptoms that had been<br />
Misdiagnosed<br />
Skin problem caused by an endodontic lesion<br />
A 22-year-old male patient visited the Fukuoka <strong>Dental</strong> College Hospital complaining<br />
of a prolonged fistula in the right lower cheek skin. 1 His former doctor treated the<br />
patient for 6 months. Repeated skin incisions and long-term antibiotic therapy were<br />
not effective and the doctor referred the patient to us. An external dental fistula with a<br />
diameter of about 10mm and continuous pus discharge was observed (Figure 1A). By<br />
X-ray findings and electric pulp examination, we diagnosed an external dental fistula<br />
caused by chronic purulent apical periodontitis of tooth 46 (Figure 1B). We performed<br />
an infected root canal treatment including anaerobic culture examination. The response<br />
to the root canal treatment was good. The size of the external dental fistula dramatically<br />
decreased and the skin lesion became dry at the third visit (Figure 2A). After confirming<br />
that intra-root canal bacteria were negative, the root canals were filled (Figure 2B).The<br />
external dental fistula completely closed after 2 months. Two and half years after the<br />
root canal filling, the patient came for tooth maintenance. The external dental fistula<br />
had not recurred (Figure 3A) and radiolucency in the periapical and furcation area had<br />
disappeared (Figure 3B).<br />
| 26 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
(Fig. 1A) Right facial view at the first visit. An external dental<br />
fistula with pus discharge is observed at the right cheek area.<br />
(Fig. 1B) <strong>Dental</strong> X-ray photograph at the first visit.<br />
Radiolucency at the apex and furcation area of tooth 46 is<br />
observed.<br />
(Fig. 2A) External dental fistula after the initiation of<br />
endodontic treatment. The pus discharge has stopped and<br />
the external dental fistula is dry.<br />
(Fig. 2B) <strong>Dental</strong> X-ray photograph at the root canal filling.<br />
(Fig. 3A) Right facial view at 2.5 years after the root canal<br />
filling. The external dental fistula has not recurred.<br />
(Fig. 3B) <strong>Dental</strong> X-ray photograph at 2.5 years after<br />
the root canal filling. The radiolucency at the apex and<br />
furcation area of tooth 46 has disappeared.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 27 |
Gingival swelling and furcation bone loss caused by<br />
an endodontic lesion<br />
A 59-year-old female attended our hospital with a<br />
chief complaint of mobility of tooth 46 and recurrent<br />
gingival swelling around the tooth (Figure 4A). She had<br />
previously received dental treatment from two dentists<br />
who performed gingival incisions, scaling and root<br />
planning, but her gingival condition did not improve. 2<br />
Her tooth 46 manifested the symptoms of typical<br />
periodontitis, such as gingival swelling, tooth mobility,<br />
pus discharge from the periodontal pocket and furcation<br />
bone loss (Figure 4B). The tooth responded to electric<br />
pulp examination but a gutta-percha point inserted from<br />
the fistula reached the mesial root apex. Consequently,<br />
we diagnosed a type I endoperiodontal lesion of<br />
tooth 46. Soon after root canal treatment, the gingival<br />
condition at tooth 46 improved without periodontal<br />
treatment (Figure 5A). After confirming the absence of<br />
bacteria, the root canals were filled (Figure 5B). After<br />
3 months, the furcation bone loss was on the way to<br />
recovery (data not shown). At 5 years after the root canal<br />
filling, the patient came for treatment of other caries. The<br />
gingival condition was good and the furcation bone loss<br />
had not recurred (Figure 6A, B).<br />
(Fig. 4A) Lateral view of the right teeth and gingiva at the first<br />
visit. Gingival swelling is observed around the margin of tooth<br />
46.<br />
(Fig. 4B) X-ray photograph of tooth 46 at the first visit.<br />
Bone resorption is observed at the furcation area, and the<br />
periodontium around the mesial root of tooth 46 is enlarged.<br />
(Fig. 5A) Lateral view of the right teeth and gingiva after<br />
initiation of endodontic treatment. Soon after initiation of<br />
the infected root canal treatment, the gingival swelling has<br />
disappeared.<br />
(Fig. 5B) X-ray photograph of tooth 46 after the root canal<br />
filling. Furcation bone loss remains at the root canal filling.<br />
(Fig. 6A) Lateral view of the right teeth and gingiva at 5<br />
years after the root canal filling. Gingival condition is good.<br />
(Fig. 6B) X-ray photograph of tooth 46 at 5 years after the<br />
root canal filling. There is no furcation bone loss.<br />
| 28 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
Oral malodor caused by an endodontic lesion<br />
A 72-year-old male patient visited our breath clinic<br />
complaining of strong breath odor. Former dentists had<br />
performed periodontal treatments including scaling and<br />
root planing, but his oral malodor did not decrease.<br />
third visit and restored with metal bridge (Figures 8A, B).<br />
We measured the breath odor and compared it with that<br />
at the initial visit. All of the malodor scores were found to<br />
have decreased (Figure 9) and the patient was satisfied<br />
with our treatment.<br />
(Fig. 7A) Occlusal view of upper jaw at the first visit. Severe<br />
inflammation was not observed, but there is an unfitted metal<br />
crown on tooth 16.<br />
(Fig. 7B) X-ray photograph of tooth 16 at the first visit. No<br />
periapical lesion is observed, but the root canals appear to<br />
be poorly treated.<br />
(Fig. 8A) Occlusal view of upper jaw at the time of bridge set.<br />
A bad odor was confirmed by halitosis measurements<br />
including an organoleptic test, a portable sulfide<br />
monitor and gas chromatography. 3 We performed an<br />
oral examination, but no remarkable problems such as<br />
gingival swelling, deep periodontal pockets, big caries or<br />
dry mouth, which may cause oral malodor production,<br />
were detected (Figure 7A). The patient also complained<br />
of an uneasy feeling in tooth 16. There was an<br />
improperly fitted restoration in tooth 16 and we sensed<br />
some malodor when compressed air was applied. An<br />
X-ray of the tooth did not reveal a periapical lesion, but<br />
the root canals appeared to be poorly treated (Figure<br />
7B). Immediately after removing the metal crown and<br />
core, a large amount of pus accompanied by malodor<br />
coming from the root canals. We diagnosed that part<br />
of the oral malodor was caused by a periapical lesion<br />
of tooth 16, and performed an infected root canal<br />
treatment. The condition of the root canals had improved<br />
at the second visit, and the root canals were filled at the<br />
(Fig. 8B) X-ray photograph of tooth 16 after the root canal filling.<br />
(Fig. 9) Comparison of the breath odor measurements<br />
before and after treatment. The results of organoleptic tests<br />
and the concentrations of three volatile sulfide gases are<br />
shown.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 29 |
Summary and Discussion<br />
Endodontic lesions usually manifest typical symptoms<br />
such as percussion pain, gingival swelling or a dental<br />
fistula around the root apex. X-ray photographs also<br />
indicate the causative teeth by radiolucency around the<br />
root apex. Consequently, dentists can usually identify<br />
endodontic lesions. However, the lesions sometimes<br />
spread to the skin in distant areas and are misdiagnosed<br />
as skin lesions. Patients with an external fistula<br />
sometimes visit a dermatologist. If they are properly<br />
diagnosed, they will be referred to a dentist and the<br />
lesion will soon be resolved. 4,5 However, diagnostic<br />
errors can result in multiple excisions, biopsies and<br />
ineffective long-term antibiotic therapy. 6,7 A case of<br />
odontogenic sinus simulating a basal cell carcinoma has<br />
been reported. 8 On the other hand, a case of extraoral<br />
sinus that was not caused by an endodontic lesion has<br />
also been reported. 9 Therefore, careful examination and<br />
close contact between dentists and dermatologists are<br />
strongly recommended. 10,11<br />
Endoperiodontal lesions are sometimes difficult to<br />
diagnose. Endoperiodontal lesions are sometimes<br />
misdiagnosed, and the importance of a differential<br />
diagnosis is noted. 12 There is a possibility that oral<br />
malodor can be caused by an endodontic lesion. These<br />
cases may be rare, but dentists need to consider such<br />
cases in the diagnosis of oral manifestations. We have<br />
also reported a case of oral malodor associated with<br />
internal root resorption. 13 The main causes of oral<br />
pathologic halitosis are periodontal disease and tongue<br />
coating, 14,15 and oral malodor caused by an endodontic<br />
lesion is rarely reported. However, careful examination<br />
is necessary if no apparent causes are found in the oral<br />
cavity of a patient with oral malodor.<br />
The main theme of this case series report is to introduce<br />
several symptoms caused by endodontic lesions.<br />
However, the opposite cases are sometimes reported,<br />
in which the manifestations of other diseases are<br />
very similar to those of endodontic lesions. Periapical<br />
cemental dysplasia is known to be similar to periapical<br />
granuloma. 16,17 To prevent misdiagnosis, application of<br />
electric pulp examination and confirmation of the dental<br />
history are recommended. Giant cementoblastoma<br />
can also be misdiagnosed as an endodontic lesion. 18<br />
Paradental cysts mimicking a radicular cyst 19 and a<br />
simple bone cyst 20 have been reported. Since there is<br />
a possibility that these cases can be misdiagnosed as<br />
endodontal lesions, detailed clinical and radiographic<br />
examinations are necessary. Other osseous diseases,<br />
such as ossifying fibroma, 21 focal cemento-osseous<br />
dysplasia 22 and Stafne’s bone cavity, 23 have also been<br />
reported. We need to be careful in the diagnosis of<br />
these diseases, because they sometimes manifest similar<br />
symptoms to those of a periapical lesion.<br />
There is also a possibility to misdiagnose malignant<br />
diseases as an endodontic lesion. In fact, a gingival<br />
squamous cell carcinoma mimicking a dentoalveolar<br />
abscess has been reported. 24 Some metastatic<br />
carcinomas manifesting as periapical lesions have<br />
also been reported as well as an oral-derived<br />
carcinoma. 25,26 An osteosarcoma 27 and a mesenchymal<br />
chondrosarcoma 28 resembling dental periapical lesions<br />
have also been reported. Some lymphomas were<br />
misdiagnosed as endodontic lesions and the proper<br />
treatments were delayed. 29 Although some cases may be<br />
difficult to diagnose, 30 we always need to consider the<br />
possibility of malignant diseases.<br />
In this way, making diagnosis is important in the<br />
treatment of endodontic cases and cases, which manifest<br />
endodontic-like symptoms.<br />
Acknowledgment<br />
This work was partly supported by a Grant-in-Aid for<br />
Scientific Research (No. 20592249) from the Japanese<br />
Ministry of Education, Science, Sports and Culture.<br />
References<br />
1. Yoneda M, Anan H, Motooka N, Hirofuji T, Matsumoto A, Isobe<br />
R, Kabashima H, Maeda K. Disappearance of an external dental<br />
fistula with an endodontic treatment of the causative tooth. Jap J<br />
Conserv Dent. 2003;46(2):143-8.<br />
2. Yoneda M, Motooka N, Naito T, Maeda K, Hirofuji T. Resolution<br />
of furcation bone loss after non-surgical root canal treatment:<br />
application of a peptidase-detection kit for treatment of type I<br />
endoperiodontal lesion. J Oral Sci. 2005;47(3):143-7.<br />
3. Yoneda M, Uchida H, Suzuki N, Mine M, Iwamoto T, Masuo<br />
Y, Naito T, Hatano Y, Hirofuji T. A case report of tooth wear<br />
associated with a patient’s inappropriate efforts to reduce oral<br />
malodor caused by endodontic lesion. Int J Dent. 2009, article ID<br />
727481, 5a, doi:1155/2009/727481.<br />
4. Tagami H, Yoshitake K. Chronic dental fistula on the nose. Acta<br />
Dermatol Venereol. 1977;57(4):365-71.<br />
5. Chidyllo SA. Intraoral examination inpyogenic facial lesions. Am<br />
Fam Phys. 1992;46(2):461-60.<br />
6. Marasco PV JR, Taylor RG, Marks RG, Argenta LC. Dentocutaneous<br />
fistula. Anals Plastic Surg. 1992;29(3):205-10.<br />
7. Steiner DR. A lesion of endodontic origin misdiagnose as a<br />
globulomaxillary cyst. J Endod. 1999;25(4):277-81.<br />
8. Cohen PR, Eliezri YD. Cutaneous odontogenic sinus simulating<br />
a basal cell carcinoma: case report and literature review. Plast<br />
Reconst Surg. 1990;86(1):123-7.<br />
9. Cohenca N, Karni S. Rotstein I. Extraoral sinus tract misdiagnosed<br />
as an endodontic lesion. J Endod. 2003;29(12):841-3.<br />
10. Held JL, Yunakov MJ, Barber RJ, Grossman ME. Cutaneous sinus<br />
of dental origin: a diagnosis requiring clinical and radoglogic<br />
correlation. Cutis. 1989;43(1):22-4.<br />
11. Yasui H, Yamaguchi M, Ichimiya M, Yoshikawa Y, Hamamoto<br />
Y, Muto M. A case of cutaneous odontogenic sinus. J Dermatol.<br />
2005;32(10):852-5.<br />
12. Benatti BB, Carvalho MD, Gomes BP, de Toledo S, Nociti Jr FH,<br />
Nogueira-Fiho Gda R. Importance of differential diagnosis<br />
in endodontic-periodontal lesions: case reports. Gen Dent.<br />
2003;51(3):246-8.<br />
13. Yoneda M, Naito T, Suzuki N, Yoshikane T, Hifofuji T. Oral malodor<br />
associated with internal resorption. J Oral Sci. 2006:48(2):89-92.<br />
14. Tonzetich J. Production and origin of oral malodor: a review of<br />
mechanisms and methods of analysis. J Periodotol. 1977;48(1):13-<br />
20.<br />
| 30 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
TOOLS TO KEEP SMILING<br />
15. Yaegaki K, Coil JM. Examination, classification, and<br />
treatment of halitosis; clinical perspectives. J Can Dent Assoc<br />
2000;66(5):257-61.<br />
16. Ward MR, Periapical cemental dysplasia: a case report. New<br />
Zeal Dent J. 1993;89(395):53-4.<br />
17. Smith S, Patel K, Hoskinson AE. Periapical cemental<br />
dysplasia: a case of misdiagnosis. Brit Dent J.<br />
1998;185(3)122–3.<br />
18. Puterman M, Fliss DM, Sidi J, Zirkin H. Giant<br />
cementoblastoma simulating a peridental infection. J<br />
Laryngol Otol.1988;102(3):264-6.<br />
19. Silva TA, Batista AC, Camarini ET, Lara VS, Consolaro A.<br />
Paradental cyst mimicking a raducular cyst on the adjacent<br />
tooth: case report and review of terminology. J Endod.<br />
2003;29(1):73-6.<br />
20. Fregnani ER, de Moraes Ramos FM, Nadalin MR, Silva-<br />
Sousa YT, Da Cruz Perez DE. Simple bone cyst: possible<br />
misdiagnosis in periapical pathology. Gen Dent.<br />
2007;55(2):129-31.<br />
21. De Moraes Ramos-Perez FM, Soares UN, ilva-Sousa YT, Da<br />
Cruz Perez DE. Ossifying fibroma misdiagnosed as chronic<br />
apical periodontitis. J Endod. 2010;36(3):546-8.<br />
22. Galgano C, Samson J, Kuffer R, Lombardi T. Focal cementoosseous<br />
dysplasia involving a mandibular lateral incisor. Int<br />
Endod J. 2003;46(12):907-11.<br />
23. Bornstein MMM, Wiest R, Balsiger R, Reichart PA. Anterior<br />
Stafne’s bone cavity mimicking a periapical lesion<br />
of endodontic origin: report of two cases. J Endod.<br />
2009;35(11):1598-602.<br />
24. Lee JJ, Cheng SJ, Lin SK, Chiang CP, Yu CH, Kok<br />
SH. Gingival squamous cell carcinoma mimicking<br />
a dentoalveolar abscess: report of a case. J Endod.<br />
2007;33(2):177-80.<br />
25. Khalili M, Mahboobi N, Shams J. Metastatic breast<br />
carcinoma initially diagnosed as pulpal/periapical disease: a<br />
case report. J Endod. 2010;36(5):922-5.<br />
26. Thompson IO, Phillips VM, Kalan M. Metastatic squamous<br />
carcinoma manifesting as a periapical lesion. J Dent Assoc<br />
South Africa. 1992;47(11):481-3.<br />
27. Soares RC, Soares AF, Souza LB, Santos AL, Pinto LP.<br />
Osteosarcoma of mandible initially resembling lesion of<br />
dental periapex: a case report. Brit J Otorhinolaryngol.<br />
2005;71(2):242-5.<br />
28. Bueno MR, De Carvalhosa AA, Castro PH, Pereira KC, Borges<br />
FT, Estrela C. Mesenchymal chondrosarcoma mimicking<br />
apical periodontitis. J Endod. 2008;34(11):1415-9.<br />
29. Graham RM, Thomson EF, Cousin GC, Kumar SN, Awasthi<br />
A. A case of faciel lymphoma mimicking dental infection.<br />
Dntal Update. 2009;36(4):244-6.<br />
30. Saund D, Kotecha S, Rout J, Dietrich T. Non-resolving<br />
periapical inflammation: a malignant deception. Int Endod J.<br />
2010;43(1):84-90.<br />
No less than ...<br />
...4 launches !<br />
Mechanical scouting sequence<br />
10/.02<br />
15/.02<br />
Desobturation made easy<br />
20/.02<br />
www.d-race.ch<br />
Discover the other novelties on<br />
www.fkg.ch<br />
• Crêt-du-Locle 4 • CH-2304 La Chaux-de-Fonds • Switzerland •<br />
• Tél.: +41 (0)32 924 22 44 • Fax: +41 (0)32 924 22 55 • info@fkg.ch • www.fkg.ch •<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 31 |
Functional and Aesthetic Management<br />
of Worn Dentition with Direct Composite<br />
Restorations: A Clinical Report<br />
Abstract<br />
The management of tooth surface loss (TSL) could be challenging in primary dental care<br />
settings. However the introduction of resin-based composite restorative materials have<br />
significantly changed our traditional mechanistic approach in favour of more toothtissues<br />
conservative treatments whilst improving both functional and aesthetic demands<br />
by patients. Direct bonding to remaining tooth tissues is more predictable than any time<br />
before, it has been clinically proven that the applications of direct composite restorations<br />
could be extended beyond building up a single tooth and become a viable option for full<br />
mouth rehabilitation. Economic factors are crucial elements in the success of our day to<br />
day dental treatments as there is more emphasis on implementing time and cost-effective<br />
and reversible treatments at low biological risks.<br />
Shihab A. Romeed<br />
PhD, MSc, MFDS, DDS<br />
Lecture and Honorary<br />
Specialist Registrar in<br />
Restorative Dentistry<br />
Kings College London <strong>Dental</strong><br />
Institute, Denmark Hill, UK<br />
shihab.romeed@kcl.ac.uk<br />
R. Malik<br />
BDS<br />
Graduate Dentist<br />
S.M. Dunne<br />
PhD, FDS, BDS<br />
Professor and Honorary<br />
Consultant in Restorative<br />
Dentistry<br />
Keywords: Tooth surface loss, Dahl concept.<br />
Introduction<br />
Tooth surface loss (TSL) can be defined as the loss of tooth substance in the absence<br />
of caries or trauma. TSL is becoming an increasingly common problem and presents<br />
increasing restorative management challenges. The adult dental health survey in 1998<br />
stated that 65% of adults in the UK had some form of toothwear. 1,2 TSL can arise due to<br />
erosion, attrition, abrasion and abfraction and often these occur in combination with each<br />
other, though one usually predominates. These terms are usually applied based on the<br />
presentation of the tooth wear and there are a number of aetiological factors that can lead<br />
to these types of tooth surface loss. 3<br />
Case description<br />
A 49 year-old male patient was referred by his general dental practitioner to King’s<br />
College London <strong>Dental</strong> Hospital in late 2009. The patient’s chief complaints were<br />
unsightly smile, tooth sensitivity and loss of efficient masticatory function. However,<br />
appearance was his main concern as it led to a lack of self esteem.<br />
The patient’s medical history was unremarkable. Social and diet history revealed daily<br />
consumption of two large glasses (250ml) of red and white wine along with significant<br />
amount of soft drinks and orange juice. He smokes 10 cigarettes a day. The impact of<br />
his excessive consumption of alcohol and acidic drinks was evident on all teeth in a form<br />
of cupped out surfaces which clearly represents severe erosion (Figure1). Bruxism was<br />
also identified as one of the main aetiological factors for the TSL in this case. The patient<br />
first noticed some changes in the size of his teeth approximately five years ago. However,<br />
his problems rapidly deteriorated which resulted in a progressive TSL especially on the<br />
anterior teeth. He had lost some of his posterior teeth namely 12, 13, 18, 19.<br />
Clinical Examination showed scalloping of the tongue borders, hyperkeratosis lines on<br />
the buccal mucosa, bilateral masseter hypertrophy, tooth attrition and antegonial notches<br />
which are all indicative signs of bruxism as another contributing factor for his generalised<br />
tooth surface loss. The patient had no symptoms of temporomandibular joint disorders<br />
(TMDs). Periodontal examination indicated generalised moderate chronic periodontitis<br />
and his dentition was moderately restored (Figure 2). Significant loss of occlusal vertical<br />
dimension (OVD) was very obvious in centric occlusion. Upper left lateral incisor was<br />
fractured at the gingival level and root treated long time ago. The history and clinical<br />
presentation indicated that tooth surface loss was a combination of erosion and attrition<br />
along with some element of abrasion (Figure 3).<br />
| 32 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
provided will ultimately fail therefore it is a crucial step in<br />
the management of wear.<br />
(Fig. 1) Generalised tooth surface loss in a form of cupped<br />
out surfaces on the buccal surfaces and attrition on the<br />
incisal edges.<br />
(Fig. 2) Generalised erosion and attrition on the lower<br />
teeth, corroded and ditched amalgam restorations on<br />
posterior teeth.<br />
(Fig. 3) Tooth no 7 was vital and underwent sever TSL. Tooth<br />
no 9 lost its post crown and root treated.<br />
Plaque control advice, smoking cessation and diet<br />
counselling, supra and sub-gingival debridement and<br />
root planning were performed as part of the treatment<br />
plan. Initially it was important to stabilise the patient’s<br />
periodontal condition as there is an increase risk of<br />
failure of restorative treatment in a mouth with active<br />
periodontal disease. An early analysis has revealed a<br />
significant reduction in plaque and bleeding scores. A<br />
programme to prevent further tooth surface loss was<br />
also simultaneously implemented which consisted of<br />
diet counselling and wearing a lower soft occlusal splint.<br />
The splint was provided to reduce forces generated<br />
during bruxism and prevent further loss of tooth<br />
substance caused by citrus fruits and soft drinks whilst<br />
the periodontal health was being stabilised. 4 Without<br />
prevention surface loss will continue and treatment<br />
The tooth surface loss was deemed to be pathological<br />
as the degree of wear exceeded the TSL level excepted<br />
at the patient’s age and subsequently function<br />
and appearance were compromised. 5 A decision<br />
was therefore made to restore the worn dentition<br />
conservatively with direct composite restorations with the<br />
goal of preserving and protecting the remaining tooth<br />
tissues and providing durable aesthetic restorations.<br />
Other advantages of using composite include; reduction<br />
of costs and treatment time, ease of repair as well as<br />
giving the clinician control over the aesthetics. 6,7<br />
It is well documented in the literature that indirect<br />
restorations confer higher strengths than direct<br />
restorations. Improvements in composite mechanical<br />
properties and bonding chemistry over the years,<br />
however, have made it possible to restore surfaces<br />
of worn teeth directly without recourse to indirect<br />
restorations, though this option remains viable if the<br />
need arises in the future. Hemmings et al., conducted<br />
a 30 month prospective clinical trial using direct<br />
composite restorations for the treatment of localised<br />
anterior toothwear. The group reviewed the progress<br />
of 225 restorations placed over a period of 5 months<br />
to six years in thirty-one patients. They found relatively<br />
low failure rates of the composites; failure was mainly<br />
due to generalised marginal failure and discolouration.<br />
They also confirmed that the median survival rate of the<br />
composites used to treat TSL was five years. 8,9<br />
Discussion<br />
Generally there are two types of techniques that can<br />
be employed in the direct build up of worn teeth; free<br />
hand technique and matrix-guided technique. These<br />
techniques can be used regardless of whether dentalalveolar<br />
compensation has occurred or not. However it is<br />
important to determine whether there is a freeway space<br />
loss because that will have implications on the available<br />
space for the amount of composite build-ups and on the<br />
anatomical form of the restorations i.e. the height/width<br />
proportion of the finished restorations 10 and whether the<br />
Dahl concept needs to be applied or not. 11<br />
1. Free-hand technique<br />
In this technique the worn teeth are built individually one<br />
by one. A silicone putty matrix is taken of the palatal/<br />
lingual surface of the articulated diagnostic wax up. This<br />
provides an intra-oral template which is used to determine<br />
the height of the restoration. The next step is to start<br />
building up composite on the palatal/lingual surface<br />
of the tooth against this template. Once the first initial<br />
opaque layer of composite is placed, the template can be<br />
removed and the next layer built. It is important to have<br />
good isolation and this can be achieved by rubber dam if<br />
there is enough tooth tissues left or cotton wool rolls and a<br />
saliva ejector. Mylar strips are used to obtain good contact<br />
points both mesially and distally. We found the use of PTFE<br />
tape (polytertafluoroethylene tape) which is usually used<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 33 |
in plumbing effective to prevent adhesion of composite<br />
to adjacent teeth. It is simply wrapped around adjacent<br />
teeth to provide effective isolation. Dentine followed by<br />
the enamel shade should be applied incrementally. Finally<br />
the restoration is finished to the required dimensions by<br />
the use of fine diamond and carbide burs, polishing discs<br />
and interproximal polishing strips (Sof-Lex, 3M ESPE, MN,<br />
USA). Occlusion should be checked with the aid of an<br />
articulating paper (8-12 microns thick) in protrusive and<br />
lateral excursive movements ensuring even contacts on<br />
anterior guidance and mutually-protected occlusion on<br />
either side, if possible, with no non-working side occlusal<br />
interferences.<br />
2. Matrix technique<br />
Vacuum-formed matrix is produced using a duplicate of<br />
the diagnostic wax-up articulated model in the retruded<br />
position or centric relation (CR) (Figure 4). Initially the<br />
matrix should be checked intra-orally for accuracy of fit.<br />
The teeth should be etched and bonded, matrix is then<br />
filled with composite; usually a layer1.5-2mm thick of<br />
composite is applied. 12 The matrix is then placed on the<br />
corresponding teeth and the composite is light-cured<br />
through its holding matrix. The procedure is repeated<br />
till the whole tooth is fully built up and the remaining<br />
restoration is then finished as described above for the<br />
free hand procedure.<br />
The technique chosen largely depends on the preference<br />
of the operator. Both confer certain advantages and<br />
disadvantages. The major advantage of the matrix<br />
technique is the formation of good anatomical form<br />
providing the anatomy of the diagnostic wax up is<br />
acceptable to the patient and clinician. However a<br />
commonly found problem is that adjacent teeth can<br />
become bonded together through this technique. The<br />
free hand technique prevents this, providing mylar strips<br />
have been used. However in the hands of inexperienced<br />
operators it can be difficult to obtain correct dimensions<br />
and anatomy of the tooth being restored. Though<br />
experienced clinicians may prefer having control of the<br />
dimensions and opt to use free-hand technique for that<br />
reason. It also provides the operator with ease in restoring<br />
the teeth using different shades but can be time consuming.<br />
(Fig. 4) Waxed-up study model at centric relation (retruded<br />
contact position).<br />
In our presented case both techniques were adopted in the<br />
posterior segments a suck-down matrix was used to restore<br />
the posterior teeth as most of the surface loss was located<br />
buccally and occlussally to a lesser extent. Anteriorly<br />
free-hand technique was adopted to have some control<br />
over shade and shape forming. Two-step etch-and-rinse<br />
bonding adhesive was employed using OptiBond Solo Plus<br />
(5 th generation) (Kerr, Orange, CA, USA). Dentine shade<br />
D3 and enamel shade E3 were layered using Dentsply<br />
Ceram.X Duo composite. Anterior teeth were built up<br />
first followed by posteriors. Upper left lateral incisor was<br />
restored with fibre post and direct full composite crown as<br />
illustrated in post-operative views Figures 5-8.<br />
Occlusion was reorganised rather than depending on<br />
a conformative approach as OVD was lost and several<br />
of the occluding surfaces were re-built. 13 Furthermore,<br />
stable contacts were lost due to the tooth surface loss<br />
and an attempt to produce restorations in centric<br />
occlusion would have increased the risk of interferences<br />
in lateral and protrusive movements, ultimately leading<br />
to failure of treatment. A face bow record was taken in<br />
order to allow correct mounting of the maxillary cast on<br />
the articulator so that all aspects of the occlusion could<br />
be analysed outside of the patient’s mouth and allow<br />
an articulated diagnostic wax up of both upper and<br />
lower arches to be produced accordingly. In addition the<br />
waxed-up models allow more accurate assessment of the<br />
restoration height and subsequently the increase in OVD,<br />
help identify any potential difficulties that may arise<br />
during treatment and to allow the patient to visualise the<br />
treatment outcome (Figure 4). 6<br />
As a result of tooth wear the patient’s OVD was reduced<br />
and the FWS increased. We benefited from the fact that<br />
there was no dental-alveolar compensation i.e. over<br />
eruption of teeth and no loss of the freeway space, hence<br />
the freeway space provided the space necessary for the<br />
placement of the anterior composite restorations. 14<br />
Further, some space was obtained from re-organising<br />
the occlusion into CR. If there was compensation present<br />
then space should have been created by following the<br />
principles of Dahl, 11 Dhal expalined that for worn anterior<br />
teeth space could be created where it had been lost by the<br />
use of a cobalt chrome appliance consisting of an anterior<br />
bite plane. The appliance would result in the separation<br />
of the posterior teeth which over a period of few weeks<br />
and maximum two months would allow overeruption of<br />
the posterior teeth back into occlusion and intrusion of the<br />
anterior teeth. Subsequently, the space created anteriorly<br />
could be used for placement of definitive restorations. It<br />
was then realised with time that the Dahl concept could<br />
be utilized without the provision of an active appliance<br />
by placing anterior restorations at an increased occlusal<br />
vertical dimension thus reducing the need for compliance<br />
with an appliance, simplifying treatment and shortening<br />
the time required for treatment. 6<br />
In our case The OVD was increased by 5mm. The patient<br />
adapted well to the increase with no associated signs or<br />
symptoms to suggest otherwise. It is desirable to have<br />
adequate anterior guidance including the upper canines,<br />
as posterior interferences between opposing teeth could<br />
result in production of potentially damaging lateral<br />
forces on these teeth during bruxism, leading to fracture<br />
| 34 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
(Fig. 5) Direct composite build-ups and recontouring of the<br />
upper anterior teeth.<br />
(Fig. 7) Direct composite build-ups and recontouring of the<br />
right upper and lower posterior teeth.<br />
(Fig. 8) Completed direct composite build-ups for the<br />
anterior and posterior teeth.<br />
(Fig. 6) Direct composite build-ups and recontouring of the<br />
lower anterior teeth.<br />
of restorations. 15 Occlusion was therefore assessed<br />
continually throughout treatment to ensure that there was<br />
even contact in the retruded contact position (CR) and<br />
that there were no posterior interferences and no nonworking<br />
side interferences. Most importantly no occlusal<br />
contact on upper lateral incisors during protrusive<br />
movement was planned to limit shear stresses on these<br />
fully built composite crowns especially the upper left<br />
lateral incisor whose ferrule was almost 1mm.<br />
Conclusions<br />
Tooth wear is a multifactorial dental problem which<br />
is classified as pathological if it exceeds the expected<br />
level at different age points. Planning treatment is<br />
extremely important. Factors such as occlusion should<br />
be thoroughly planned to ensure occlusal harmony and<br />
stability, which is paramount for the long term success<br />
and survival of the direct composite restorations. 11<br />
Treatment of worn teeth should be attempted using direct<br />
composite restorations first. This has the advantage<br />
of retaining and protecting remaining tooth structure.<br />
Reversibility of the procedure, ease of repair and<br />
reduced costs are added benefits. Advances in composite<br />
technology and the availability of data showing that<br />
these restorations have the ability to withstand functional<br />
and parafunctional forces which makes them ideal in<br />
treatment of tooth wear cases without recourse to the use<br />
of expensive, non-conservative indirect restorations.<br />
Acknowledgment<br />
This case report was part of a final-year undergraduate<br />
project for Mr. Raheel Malik at Kings College London<br />
<strong>Dental</strong> Institute. We would like to thank Dentsply, UK for<br />
donating all composite materials (Ceram.X Duo composite)<br />
which were exclusively used in managing this case.<br />
References<br />
1. Kidd EAM, Smith BGN, Watson TF. Pickard’s manual of operative<br />
dentistry. 8 th ed. Oxford Press. 2003;20-27.<br />
2. Kelly M, Steele JG, Nuttall N. Adult <strong>Dental</strong> Health Survey. Oral<br />
Health in the United Kingdom, London: ONS. 1998.<br />
3. Kelleher M, Bishop K. Tooth Surface Loss. BDJ Publications.<br />
2000;3-8.<br />
4. Solberg WK, Clark GT, Rugh JD. Nocturnal electromyographic<br />
evaluation of bruxism patients undergoing short-term splint<br />
therapy. J Oral Rehab. 1995;12:215-23.<br />
5. Capp NJ. Tooth Surface Loss. BDJ Publications. 2000;15-20.<br />
6. Robinson S, Nixon PJ, Matthew JG, Martin FWC. Techniques for<br />
restoring worn anterior teeth with direct composite resin. Dent<br />
Update. 2008;35:551-8.<br />
7. Allen PF. Use of tooth-coloured restorations in the management of<br />
toothwear. Dent Update. 2003;30:550-6.<br />
8. Hemmings KW, Darbar UR, Vaughan S. Toothwear treated with<br />
direct composite restorations at an increased vertical dimension:<br />
results at 30 months. J Prosthet Dent. 2000;83:287-93.<br />
9. Redman CD, Hemmings KW, Good JA. The survival and clinical<br />
performance of resin-based composite restorations used to treat<br />
localised anterior tooth wear. Br Dent J. 2003;194:566-72.<br />
10. Mizrahi B. A technique for simple and aesthetic treatment of<br />
anterior Toothwear. Dent Update. 2004;31:109-14.<br />
11. Dahl BL, Krogstad O, Karlsen K. An alternative treatment in cases<br />
with advanced localized attrition. J Oral Rehabil. 1975;2:209-14.<br />
12. Daoudi MF, Radford JR. Use of a matrix to form directly applied<br />
resin composite to restore worn anterior teeth. Dent Update.<br />
2001;28:512-4.<br />
13. Davies SJ, Gray RJM, Whitehead SA. A Clinical Guide To occlusion.<br />
BDJ Publications. 2002;37-46.<br />
14. Faigenblum M. Tooth Surface Loss. BDJ Publications. 2000;21-24.<br />
15. Davies S.J, Gray RJM. A Clinical Guide To occlusion. BDJ<br />
Publications. 2002;3-11.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 35 |
June’s Panel<br />
Mohammad Sartawi<br />
BSc, BDS, MSc (OMFS)<br />
London, FFDRCSI (OSOM)<br />
Dublin<br />
• Senior Consultant, Maxillo<br />
• Director, Jordan British<br />
Specialty Center for Oral<br />
& Maxillofacial Surgery<br />
& Implantology, Amman,<br />
Jordan<br />
• EX-Chairman/Scientific<br />
Committee of the JDA 02-04.<br />
• Member of International<br />
Advisory Board, <strong>Smile</strong> <strong>Dental</strong><br />
<strong>Journal</strong><br />
• Visiting Clinical Professor<br />
and External Examiner in<br />
Oral & Maxillofacial Surgery,<br />
Jerusalem University<br />
Hakam Mousa<br />
D.D.S., M.S.D., F.A.G. D.<br />
• Musa <strong>Dental</strong> Clinics,<br />
Amman, Jordan<br />
• Bachelors of <strong>Dental</strong> Surgery<br />
(B.D.S.), University of Jordan<br />
• Postgraduate Certificate in<br />
Operative Dentistry, Major<br />
in Operative Dentistry, Minor<br />
in <strong>Dental</strong> Materials, Indiana<br />
University, USA<br />
• Masters of Science in<br />
Dentistry (M.S.D.), Indiana<br />
University, USA<br />
Ashraf E Abu Karaky<br />
BDS MSc MFDSRCSEd<br />
FFDRCSI<br />
• Assistant Professor, Faculty<br />
of Dentistry the University of<br />
Jordan, Amman, Jordan<br />
• Consultant Oral and<br />
Maxillofacial Surgeon,<br />
Jordan University Hospital<br />
Yousef Sadik Marafie<br />
BDS, MSD, Prosthodontist<br />
• Advanced Education in<br />
General Dentistry Certificate,<br />
Baltimore College of <strong>Dental</strong><br />
Surgery, Maryland, USA<br />
• Certificate in Prosthodontics,<br />
Medical College of Georgia,<br />
USA<br />
• Master of Science in<br />
Prosthodontics, Boston<br />
University, USA<br />
• Clinical Instructor, Faculty of<br />
Dentistry, Kuwait University<br />
• Full Time Prosthodontist at<br />
Bayan <strong>Dental</strong> Center, Egaila,<br />
Kuwait<br />
A patient reported to my clinic<br />
with an ulcer on the side of his<br />
tongue. The ulcer is non-healing,<br />
expanding, with raised borders,<br />
firm and indurated. However,<br />
although it has been there for<br />
more than three weeks, it is<br />
painless and the base of the<br />
ulcer looks smooth. I have three<br />
questions please:<br />
1. What is the most likely<br />
diagnosis?<br />
2. What is the most common<br />
technique to confirm the<br />
diagnosis?<br />
3. What are the current therapeutic<br />
approaches for treatment?<br />
Dr. Soud Ammeri, Jeddah, Saudi<br />
Arabia<br />
Answer: Dr. Mohammad Sartawi<br />
1. The diagnosis is most likely to be<br />
Squamous cell carcinoma.<br />
2. Biopsy remains the most common<br />
and definitive technique for the<br />
diagnosis of a suspected oral<br />
cancer. Biopsy should be incisional<br />
rather than excisional so as not to<br />
obscure the extent of the tumor.<br />
3. Early detection and treatment<br />
really have a positive impact on<br />
outcome and prognosis. Tumor<br />
staging which provides a uniform<br />
system to describe the lesion and<br />
its projected clinical behavior. The<br />
staging of oral cancer involves<br />
three parameters: the size and<br />
extent of the tumor, the presence<br />
and extent of lymph node<br />
involvement, and the presence or<br />
absence of metastases. The system<br />
that was developed in 1942 is thus<br />
called the TNM system for tumor,<br />
nodes and metastases.<br />
The current therapeutic approaches<br />
for treatment of Squamous cell<br />
carcinoma are:<br />
• Definitive surgery with wide safety<br />
margins<br />
• Definitive radiation therapy<br />
• Surgery with planned postoperative<br />
radiation therapy<br />
• Definitive radiation with surgery<br />
only for salvage or recurrence<br />
• Palliation with chemotherapy or<br />
radiation therapy<br />
• Radiation therapy with concomitant<br />
chemotherapy<br />
Therefore, a thorough and<br />
aggressive routine clinical<br />
examination of the mouth by health<br />
care provider’s especially dental,<br />
oral and maxillofacial surgeons<br />
is crucial for early diagnosis and<br />
radical treatment of Squamous<br />
cell carcinoma aiming for better<br />
prognosis and cure.<br />
Some clinicians advocate the use<br />
of fibber based posts rather than<br />
the cast post and core group, is<br />
there any evidence supporting the<br />
use of the fibber based posts over<br />
the classical metal based posts?<br />
Dr. Rana Omar, Jeddah - Saudi Arabia<br />
Answer: Dr. Hakam Mousa<br />
The use of fiber post systems<br />
in recent years has increased<br />
in an attempt to replace metal<br />
prefabricated and/or cast post and<br />
core systems.<br />
First, what is a fiber post?<br />
It is made of specially - oriented<br />
reinforcement of continuous<br />
elongated fibers, a matrix of a<br />
| 36 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
proprietary epoxy resin and an<br />
interface: a bonding system between<br />
the matrix and the fiber.<br />
Some of The advantages of using<br />
fiber posts is in the aesthetic zone.<br />
Its white or translucent color, will<br />
help dentists to use more options for<br />
direct or indirect restorations since<br />
no metal shadowing could be seen.<br />
one other advantage is more<br />
favorable stress distribution along<br />
the long access of the root area,<br />
causing less risk of root fracture,<br />
this is due in part to elastic modulus<br />
(relative rigidity) that is close to<br />
dentin(e).<br />
Retrievability is another advantage of<br />
fiber post systems.<br />
The use of fiber posts, prefabricated<br />
metal posts, or cast post and core<br />
systems should be the dentist<br />
decision according to his or her<br />
experience and clinical case<br />
management.<br />
UL1 Root, prepared for a post crown<br />
Fiber post UL1<br />
Post and Core UL1<br />
UL1 post crown<br />
Hopefully some of these articles<br />
comparing fiber post and metal<br />
post systems will aid in making<br />
an informed decision relying on<br />
evidence based practices in selecting<br />
the type of post system(s) you wish to<br />
adopt in your practice.<br />
Ref: Naumann M, Sterzenbac GJ, Alexandra F,<br />
Dietrich T. Randomized controlled clinical pilot<br />
trial of titanium vs. glass fiber prefabricated<br />
posts: preliminary results after up to 3 years.<br />
Int J Prosthodont. 2007;20(5):499-503.<br />
- Goodacre CJ. Carbon fiber posts may have<br />
fewer failures than metal posts. Evid Based<br />
Dent Pract. 2010;10(1):32-4.<br />
- G. Bateman,1 D. N. J. Ricketts2 and P.<br />
Saunders3. Fibre-based post systems: a<br />
review British <strong>Dental</strong> <strong>Journal</strong>, Volume 195<br />
July122003W.<br />
I started placing and restoring<br />
dental implants in my private<br />
practice and i would like to know<br />
whether there is a strong evidence<br />
recommending antibiotics<br />
prophylaxis before and after<br />
implant surgery, and if so, what is<br />
the recommended regimen?<br />
Dr. Fadi Sukaria, Leeds - UK<br />
Answer: Dr. Ashraf Abu Karaky<br />
Despite the daily practice of dental<br />
implantology worldwide, and despite<br />
the importance of careful selection<br />
and prescribing of antibiotics, till<br />
present there is no consensus on<br />
the antibiotic protocols in dental<br />
implantology. Whereas some studies<br />
found no significant benefits from<br />
antibiotics prescribing in ordinary<br />
dental implants insertion, others<br />
recommend otherwise and prescribe<br />
antibiotics. Recently several systemic<br />
reviews has recommended the oral<br />
administration of 2gms amoxicillin<br />
one hour prior to implant insertion,<br />
this is thought to reduce the number<br />
of patient experiencing implant<br />
failure. Little is known about the<br />
efficacy of post-operative antibiotics<br />
and about its appropriate type, dose<br />
and duration. At Jordan University<br />
Hospital we conducted a study to<br />
compared three different antibiotic<br />
regimens for dental insertion<br />
(preoperative, postoperative, pre<br />
and post-operative), and we found<br />
no significant difference on implant<br />
survival rate between the three<br />
group. (Antibiotic prophylaxis and<br />
early dental implant failure: a quasirandom<br />
controlled clinical trial, EJOI<br />
2011). Based on the evidence found<br />
in the dental literature and based<br />
on the results we had from our study,<br />
I recommend a single preoperative<br />
oral dose of 2gms amoxicillin one<br />
hour before implant insertion with<br />
no postoperative antibiotics. And<br />
for patients allergic to penicillin, I<br />
recommend a single preoperative<br />
oral dose of 600mgs clindamycin<br />
one hour before implant insertion.<br />
Ref: Antibiotic prophylaxis and early dental<br />
implant failure: a quasi-random controlled<br />
clinical trial. Karaky AE, Sawair FA, Al-<br />
Karadsheh OA, Eimar HA, Algarugly SA,<br />
Baqain ZH.Eur J Oral Implantol. 2011<br />
Spring;4(1):31-8.<br />
Is it safe to adjust and prepare<br />
the implant abutment intra-orally,<br />
and if not, do you recommend<br />
any way to facilitate extra-oral<br />
abutment preparation?<br />
Dr. Ahmad Abdelazeez, Cairo - Egypt<br />
Answer: Dr. Yousef Marafie<br />
After osseointegration of dental<br />
implant(s), definitive abutment(s)<br />
and a final prosthetic superstructure<br />
must be fabricated. Some<br />
abutments could be custom made<br />
and prepared by the laboratory<br />
technician, alternatively the dentist<br />
might choose to use a ready made<br />
abutment and adjust it chair side to<br />
reduce cost and time of the implant<br />
treatment. In these case,the restoring<br />
dentist has the option of using a<br />
direct or indirect technique for the<br />
preparation of implant abutments.<br />
With the direct technique,<br />
excessive heat generation at the<br />
implant-bone interface may cause<br />
irreversible bone damage and loss<br />
of osseointegration as reposted<br />
by Gross et al. in the int J Oral<br />
Maxillofac Implants (1995).<br />
Therefore, extra oral abutment<br />
preparation is recommended to<br />
avoid peri-implant marginal bone<br />
loss and/or dental implant failure.<br />
Other advantages of extra oral<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 37 |
QUICK, EFFECTIVE and SAFE<br />
preparation are:<br />
1. Ease of preparing better margins<br />
and emergence profile<br />
2. Improved quality of dies to<br />
fabricate the prosthesis<br />
3. Subgingival margin preparation is<br />
made possible without risk of soft<br />
tissue trauma or postimpression<br />
shrinkage.<br />
However, extra oral abutment is<br />
often a challengeable task due to<br />
difficulty in holding and controlling<br />
the abutment while preparation.<br />
Londono and Marafie et al from<br />
Medical College of Georgia (USA)<br />
described in their case report in<br />
the J Prosthet Dent. 2009;102:54-<br />
5, an easy, quick, accessible, and<br />
economical way of fabricating<br />
an implant abutment holder for<br />
extraoral abutment preparation.<br />
Only 3 instruments for most cases<br />
R1 15/.06 R2 25/.04 R3 30/.04<br />
It can be used with any implant<br />
abutment using a corresponding<br />
implant replica that can be fit in to<br />
the active part of the tissue punch<br />
using a small amount of acrylic resin<br />
followed by preparing the abutment<br />
using high-speed handpiece and<br />
suitable burs.<br />
Implants replicas fitted into the<br />
tissue punch<br />
Endo treatment of teeth 47<br />
with the iRaCe R1, R2, R3.<br />
Curvatures have been fully respected.<br />
Abutments connected to the<br />
implant replicas<br />
Courtesy of Dr. Bertrand Khayat (France)<br />
Extra oral abutment preparation<br />
www.iRaCe.ch<br />
| 38 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
W&H sterilizers created<br />
for you!<br />
Lisa and Lina, two type-B sterilizers with one single aim:<br />
to meet your needs and adapt to your practice requirements through<br />
Lisa’s automatic traceability system and made-to-measure cycles,<br />
and the essentials of sterilization with Lina.<br />
wh.com<br />
Totally type B
Summarized & Presented by:<br />
Hassan Maghaireh<br />
BDS, MFDS, MSc Implants (Manchester)<br />
Clinical Teacher, Dept. of <strong>Dental</strong> Implants, University of Manchester<br />
bjdi.group@hotmail.com<br />
Maxillary Sinus Augmentation as a Risk Factor<br />
for Implant Failure<br />
McDermott N., Chuang S-K., Woo V., Dodson T.<br />
Int. <strong>Journal</strong> of Oral and Maxillofacial Implants, Vol. 21 No. 3, June 2006<br />
Maxillary sinus augmentation is commonly undertaken to enhance otherwise inadequate bone support for placement of dental<br />
implants in the posterior maxilla. Generally speaking it has been shown that bone grafting is not correlated with an increase<br />
in implant failure, however little specific data exists for sinus grafts alone. This study therefore set out to undertake a rigorous<br />
multivariate analysis of a retrospective cohort, adjusted for clustered, correlated observations, to determine if sinus grafts (SG)<br />
are an independent risk factor for implant failure.<br />
Materials and Methods<br />
All patients treated in one center over an 8-year period for the replacement of missing maxillary molars and premolars were<br />
included in the analysis. Patients were grouped according to whether they required pre-implant sinus grafting (SG group) or not<br />
(non-SG group). Patients who showed 4mm or less of alveolar bone below the floor of maxillary sinus, underwent sinus grafting<br />
which was carried out either via a modified Summer’s technique simultaneous with implant placement or via a Caldwell Luc<br />
approach with a lateral window and staged implant placement 4 to 8 months later. Grafts included both autogenous and nonautogenous<br />
materials.<br />
Implant failure was defined as implant removal as a result of perceptible mobility. Survival times were calculated from time<br />
of placement to time of implant removal or most recent follow-up. In addition to failure, information was collated on patient<br />
demographics, patient health status, anatomy, bone density, implant location, implant dimension, abutment dimension, angled<br />
versus non-angled abutments, fixed versus removable prosthesis, and use of antibiotics. These data were also analyzed with respect<br />
to risk for implant failure.<br />
Results<br />
Seven hundred and two patients were included in this retrospective cohort of which 677 had adequate records for analysis. Of<br />
these 318 patients received 762 implants in the posterior maxilla, with a mean follow-up of 22.5 months. The vast majority of<br />
patients were systemically healthy and there was a relatively equal number of males and females in the SG and non-SG groups.<br />
The mean age for both groups was circa 56years. Nine percent of patients in the SG group were smokers compared to 11.9% in<br />
the non-SG group. A greater number of molars were treated in the SG group, p < 0.001 where the bone density was described<br />
as less dense, p < 0.001. Implant dimensions were comparable in the two groups. There was no significant difference between<br />
the groups with a one year survival rate of 96.2% for the SG group and 92.6% for the non-SG group. The 5-year survival rates<br />
were 87.9% and 88.0% respectively.<br />
Discussion and Conclusions<br />
In the current study there was no significant difference in the implant survival rates at 5 years between implants in sinus grafts<br />
and those in native alveolar bone. The sinus graft was not identified as a risk factor for implant failure. However, considering<br />
potentially confounding variables, it was possible to identify implants in smokers, molar implants and implants placed in a<br />
simultaneous procedure with grafting as having a greater risk of failure.<br />
| 42 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
The McGill and York Consensus Statements on Two- Implant<br />
Overdentures<br />
J.M. Thomason, S.A.M. Kelly, A Bendkowski , J.S. Ellis<br />
Introduction<br />
The default position for treatment for the edentulous patient is complete conventional dentures (complete removable maxillary<br />
and mandibular dentures). However, such prostheses especially the mandibular denture, have well-documented problems such<br />
as lack of stability and retention which can cause them to move around in the mouth (Doundoulakis 2003). This can be affected<br />
by the height and shape of the mandibular ridge and in edentulous patients continued loss of alveolar bone and resorption of<br />
the mandibular ridge can occur over time, and cause previously stable dentures to become ill-fitting. It has been reported that<br />
more than 50% of those with mandibular complete dentures may have problems with stability and retention (Redford 1996).<br />
These factors cause a range of problems for patients ranging from minor discomfort and inconvenience to more significant<br />
impacts. Many patients experience pain when eating and chewing. Patients are often concerned about the denture moving<br />
when eating, speaking or laughing and report fears about the negative effect of dentures on social situations (Hyland 2009).<br />
Movement of the denture can lead to concerns about aesthetics and patients also report that because of difficulty eating foods<br />
that are difficult to bite or chew they have to adapt their food choices, especially when eating out and in social situations. In<br />
some cases, people avoid social situations completely.<br />
Implant-supported overdentures (ISOD’s) offer better stability and retention of the mandibular denture and better chewing<br />
function. Patients also report greater satisfaction with aesthetics because the denture is not visibly moving. Additionally, implants<br />
can help to prevent further resorption of the mandible. It has been reported that the long-term success rate of implants in the<br />
lower mandible is at least 95% (Doundoulakis 2003) and there are few serious complications.<br />
The McGill and York consensus statements on overdentures<br />
The McGill consensus statement on overdentures (The McGill consensus statement on overdentures. European <strong>Journal</strong> of<br />
Prosthodontics and Restorative Dentistry 2002) was published following a symposium held at McGill University in Montreal, Canada<br />
in 2002. A panel of relevant experts in the field stated that: The evidence currently available suggests that the restoration of the<br />
edentulous mandible with a conventional denture is no longer the most appropriate first choice prosthodontic treatment. There<br />
is now overwhelming evidence that a two-implant overdenture should become the first choice of treatment for the edentulous<br />
mandible.<br />
In 2009, a further consensus statement was released as a support and follow-up to the McGill consensus statement. This report was<br />
jointly created by members of the BSSPD (British Society for the Study of Prosthetic Dentistry) Council and the panel of presenters at<br />
the BSSPD conference in York, UK in April 2009 (Thomason JM, Feine J, Exley C, Moynihan P, Muller F, Naert I, et al. Mandibular<br />
two implant-supported overdentures as the first choice standard of care for edentulous patients-the York Consensus Statement. British<br />
<strong>Dental</strong> <strong>Journal</strong> 2009). This report also highlighted that since the McGill statement in 2002, uptake by dentists of implant technology<br />
for complete denture wearers has been slow.<br />
The York statement concluded that “a substantial body of evidence is now available demonstrating that patients” satisfaction and<br />
quality of life with implant-supported mandibular overdentures is significantly greater than for conventional dentures. Much of this<br />
data comes from randomised controlled trials.<br />
While it is accepted that the two-implant overdenture is not the gold standard of implant therapy it is the minimum standard that<br />
should be sufficient for most people, taking into account performance, patient satisfaction, cost and clinical time.<br />
This paper aims to present the current evidence and rationale to support the McGill and York consensus statements.<br />
Conclusions<br />
There is now overwhelming evidence to support the proposal that a two-implant overdenture should become the first choice<br />
of treatment for the edentulous mandible. The next task is to identify and overcome barriers for the delivery of this care for the<br />
benefit of edentulous patients.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 43 |
Interventions for Replacing Missing Teeth: <strong>Dental</strong> Implants in<br />
Fresh Extraction Sockets (Immediate, Immediate-Delayed and<br />
Delayed Implants)<br />
Marco Esposito, Maria Gabriella Grusovin, Ilias P Polyzos, Pietro Felice, Helen V Worthington<br />
The Cochrane Library June 2010, issue 10, 2010<br />
Background<br />
“Immediate” implants are placed in dental sockets just after tooth extraction. “Immediate-delayed” implants are those implants<br />
inserted after weeks up to about a couple of months to allow for soft tissue healing. “Delayed” implants are those placed<br />
thereafter in partially or completely healed bone. The potential advantages of immediate implants are that treatment time can<br />
be shortened and that bone volumes might be partially maintained thus possibly providing good aesthetic results. The potential<br />
disadvantages are an increased risk of infection and failures. After implant placement in post-extractive sites, gaps can be<br />
present between the implant and the bony walls. It is possible to fill these gaps and to augment bone simultaneously to implant<br />
placement. There are many techniques to achieve this but it is unclear when augmentation is needed and which could be the<br />
best augmentation technique.<br />
Objectives<br />
To evaluate success, complications, aesthetics and patient satisfaction between “immediate”, “immediate-delayed” and<br />
“delayed” implants. Also, to evaluate whether and when augmentation procedures are necessary and which is the most effective<br />
technique.<br />
Selection Criteria<br />
Randomised controlled trials (RCTs) comparing immediate, immediate-delayed, and delayed implants, or comparing various bone<br />
augmentation procedures around the inserted implants, reporting the outcome of the interventions to at least 1 year after functional<br />
loading.<br />
The authors used the following definitions:<br />
• Immediate implants: any implant placed in a fresh extraction socket just after tooth extraction.<br />
• Immediate-delayed implants: any implant placed in a extraction socket within 8 weeks after tooth extraction.<br />
• Delayed implants: any implants placed at least 2 months after tooth extraction.<br />
Fourteen eligible RCTs were identified but only seven trials could be included. Four RCTs evaluated implant placement timing. Two<br />
RCTs compared immediate versus delayed implants in 126 patients and found no statistically significant differences. One RCT<br />
compared immediate-delayed versus delayed implants in 46 patients.<br />
Main Results<br />
The following interventions were tested in this systematic review:<br />
1. Immediate versus delayed implants (2 trials):<br />
• One study (Lindeboom 2006) of parallel group design compared immediate versus delayed implants in periapical infected<br />
sites. Twenty-five patients were enrolled in each group and none dropped out. All patients were bone grafted at implant<br />
placement and subjected to a regenerative therapy with resorbable membranes. One year after placement, there were no<br />
statistically significant differences for prosthesis and implant failures, aesthetics assessed by a dentist: papilla height and the<br />
level of the perimplant marginal mucosa in relation to that of the adjacent teeth, and perimplant marginal bone level changes.<br />
• Another study (Block 2009) of parallel group design compared immediate versus delayed implants. Seventy-six patients were<br />
enrolled and 16 dropped. Two years after loading, four implants failed in the immediate group versus one in the delayed<br />
group and this was not statistically significant.<br />
2. Immediate-delayed versus delayed implant placement (1 trial):<br />
• (Schropp 2003) in their parallel group RCT compared immediate-delayed versus delayed implant placement up to 5 years<br />
after loading. Twenty-three patients were enrolled in each group. Three early implant failures occurred, two in the immediatedelayed<br />
group and one in the delayed group. Four postoperative minor complications occurred all in the immediate-delayed<br />
group: one fistula in relation to remnants of cement at the implant-abutment joint (after meticulous scaling the fistula<br />
disappeared but the patient suffered from a bad taste originating from the perimplant mucosa), two cases of temporarily<br />
sensibility disturbances which recovered within 1 month, and one minor postoperative bleeding. After 2 years there were<br />
no statistically significant differences for prosthesis and implant failures, complications, aesthetics assessed by the patient,<br />
the papilla height assessed by the dentist, and marginal bone level changes. However, there was statistically significantly<br />
higher patient satisfaction in the immediate-delayed group and an independent blinded assessor also judged the level of the<br />
perimplant marginal mucosa in relation to that of the adjacent teeth as more appropriate in the immediate-delayed group.<br />
3. Immediate versus immediate-delayed implant placement (1 trial):<br />
• One trial of parallel group design compared eight patients receiving nine single immediate postextractive implants with eight<br />
patients receiving nine immediate-delayed implants 8 weeks after extraction at maxillary anterior and premolar teeth (Palattella<br />
| 44 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
2008). Implants were restored within 48 hours with provisional acrylic crowns not in occlusal contact. Two years after implant<br />
placement there were no implant failures, complications, drop-outs, nor statistically significant differences for the level of the<br />
perimplant marginal mucosa in relation to the implant collar, and perimplant marginal bone level changes.<br />
4. Are augmentation procedures necessary? (1 trial)<br />
• One trial of parallel group design compared 14 patients receiving particulate autogenous bone harvested from the implant<br />
osteotomy site versus 12 patients who were not subjected to any augmentation procedure at immediate single implants placed<br />
in fresh extraction sockets at maxillary anterior and premolar sites (Chen 2005) up to 2 years post-loading. Two complications<br />
occurred in the group treated with autogenous bone: one abscess that determined the early failure of the implant and one<br />
wound dehiscence. In total two implants were lost in the autogenous bone group, whereas no complications or failures<br />
occurred in the non-augmented control group. Both treatments resulted in statistically significant bone gain, however no<br />
statistically significant differences were found among the two procedures. With respect to cost and treatment time, the<br />
difference between groups may not be clinically significant.<br />
5. Which is the most effective augmentation technique? (2 trials)<br />
• One trial of parallel group design (Chen 2005) compared 12 patients receiving non-resorbable barriers versus 11 patients<br />
receiving resorbable barriers versus 13 patients receiving resorbable barriers and particulate autogenous bone harvested from<br />
the implant osteotomy site at immediate single implants placed in fresh extraction sockets at maxillary anterior or premolar<br />
sites up to 2 years post-loading. No patients dropped out. Four complications occurred, two dehiscences occurred in the<br />
resorbable group whereas one abscess (successfully treated with systemic antibiotics) and one dehiscence occurred in the group<br />
treated with resorbable barriers and autogenous bone All treatments resulted in statistically significant bone gain, however no<br />
statistically significant differences were found between the three procedures.<br />
• Another trial compared 10 patients receiving Bio-Oss versus 10 patients receiving Bio-Oss plus a resorbable barrier at<br />
immediate single implants placed in fresh extraction sockets at maxillary anterior or premolar sites up to 3 years post-loading.<br />
These two groups were compared to a third control group of 10 patients who received no barrier and no graft After 3 years,<br />
three patients dropped out from the Bio-Oss group and five patients from the Bio-Oss plus barrier group. There were no<br />
prosthesis or implant failures. Two complications occurred in the Bio-Oss plus barrier group: one abscess developed during<br />
the healing period around one implant (the site was re-treated with the same procedure); another implant displayed a chronic<br />
inflammation of the perimplant tissues (perimplant mucositis) for the entire study period. No statistically significant differences<br />
in bone gain were found between the two procedures. With respect to treatment time, the differences among groups may not<br />
be clinically significant. The only difference in cost between the two procedures was the additional cost of the barrier.<br />
• The fact that five different augmentation procedures were tested in these two trials which were conducted by Chen et al. and<br />
included 56 patients, eliminated the already scarce possibility to find any possible statistically significant difference, therefore<br />
the findings were inconclusive.<br />
Discussion<br />
The meta-analyses of two trials (Lindeboom 2006; Block 2009) comparing immediate versus delayed implants found no<br />
statistically significant differences for prosthesis and implant failures, though trends clearly suggested that more implant failures<br />
occurred at immediate implants. No other meta-analysis could be done, nor other outcome was significant.<br />
One trial (Cornelini 2004) which showed some statistically significant difference but has to be excluded from this systematic<br />
review update, because it was decided to include only trials having a follow-up of at least 1 year after loading, worth<br />
mentioning. This trial, having a follow-up to abutment connection/implant loading, compared 10 patients with an immediate<br />
post-extractive implant covered by a resorbable barrier versus 10 patients treated with a resorbable barrier plus anorganic<br />
bovine bone (Bio-Oss) at implants placed in fresh extraction sockets. No failures, complications or drop-outs occurred. A<br />
statistically sig- nificant higher position of the soft tissue margins in relation to the implant shoulder was found at the buccal<br />
aspects of implants treated with barrier plus Bio-Oss.<br />
Authors’ Conclusions<br />
Implications for practice<br />
There is insufficient evidence to determine possible advantages or disadvantages of immediate, immediate-delayed or delayed<br />
implants, therefore these preliminary conclusions are based on few underpowered trials often judged to be at high risk of<br />
bias. There is a suggestion that immediate and immediate-delayed implants may be at higher risk of implant failures and<br />
complications than delayed implants; on the other hand the aesthetic outcome might be better when placing implants just<br />
after teeth extraction. There is not enough reliable evidence supporting or refuting the need for augmentation procedures at<br />
immediate implants placed in fresh extraction sockets or whether any of the augmentation techniques are superior to the others.<br />
Implications for research<br />
There is a definite need for randomized controlled trials evaluating the best timing for placing dental implants after teeth<br />
extractions. These trials must be powered to detect a difference for primary outcomes such as prosthesis/implant success<br />
and complications, should evaluate objective aesthetic outcomes assessed by blind outcome assessors and the patient’s own<br />
perception of aesthetics, and should be reported according to the Consolidated Standards of Reporting Trials (CONSORT)<br />
guidelines (www.consortstatement.org). We also need to understand when bone augmenta- tion procedures are needed and<br />
which are the most effective. Trials evaluating the efficacy of non/slow resorbable bone substitutes in alternative to autogenous<br />
bone should be prioritised.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011| 45 |
Lisa and Lina<br />
W&H Sterilizers Created for You!<br />
Lisa and Lina, two type-B sterilizers with one single aim:<br />
to meet your needs, through Lisa’s exclusive “made-tomeasure”<br />
type-B cycles and integrated automatic traceability<br />
system featuring a load release option, and with Lina, the<br />
new addition to the range, that has everything you would<br />
expect of a W&H sterilizer as well as the possibility to adapt<br />
to your practice requirements when needed.<br />
Lisa “fully automatic”<br />
W&H invents the “made-to-measure” cycle<br />
Lisa is designed for intensive use and therefore features new<br />
type-B cycles, that automatically reduce and optimize the<br />
whole sterilization cycle according to the number and type<br />
of instruments to be sterilized, and shorten drying thanks<br />
to the patented ECO-Dry system. Lisa therefore becomes a<br />
premium performing sterilizer for medium loads as there is<br />
no longer the need to wait until having a full load. The result<br />
is time savings of 15 to 25 minutes for these smaller loads<br />
and your valuable instruments are also less exposed to heat,<br />
increasing their lifespan.<br />
Lina: Simple but expandable<br />
As well as staying true to the W&H concept by offering<br />
exclusively type-B cycles and a short ECO-B cycle for your<br />
small loads, and by ensuring ease-of-use through its<br />
practical key-pad, the Lina sterilizer was also designed to<br />
evolve according to the requirements of your practice. When<br />
needed, it is therefore<br />
possible to add the<br />
optional Multiport which<br />
allows the saving of<br />
cycles on USB stick and<br />
the printing of bar-code<br />
labels via the LisaSafe<br />
printer.<br />
www.wh.com<br />
Hydrorise, the Innovation that<br />
Did Not Exist<br />
Nowadays, dentists can count on an innovative new<br />
impression material:<br />
Hydrorise, the first hyperhydrophilic A-silicone that is<br />
suitable for any kind of impression technique, in all clinical<br />
conditions.<br />
Hyperhydrophilic technology has been exclusively developed<br />
by Zhermack research, making hydrorise extremely flowable<br />
like water.<br />
With a contact angle less than 10° and thanks to the effects<br />
of the AMDA System (Advanced Moisture Displacement<br />
Action), Hydrorise is able to move fluids from the gingival<br />
sulcus and reproduce impression margins with maximised<br />
precision, like no other material on the market.<br />
The attention paid by researchers in the Zhermack<br />
impression materials development phase is focused on the<br />
company's aim to create clinically relevant products. An<br />
impression material must guarantee extremely accurate and<br />
reliable results, even in particularly difficult clinical situations.<br />
The perfect synergy between physical and mechanical<br />
properties found in Hydrorise ensures clinical success at each<br />
use, drastically improving the flowability of the silicone deep<br />
within the gingival sulcus.<br />
Hydrorise is available in different viscosities: putty - heavy<br />
body – regular body – light body – extra light body –<br />
monophase, all available both in normal set or fast set.<br />
BCS ® Basal Implants<br />
Basal implants are today the devices of first choice, when<br />
it comes to loading immediately, treating patients with<br />
compromisted health and smokers. BCS ® implants with<br />
proven long term success rates above 99% are offering<br />
all options for successful treatments both in the mandible<br />
and in the maxilla.<br />
BCS implants are resistant to peri-implant infections and<br />
safe to use even for the non experienced implantologist.<br />
Avaiable diameterts range from 3.5mm - 12mm, with<br />
lengths from 10mm to 38mm. BCS ® implants are<br />
suitable for placement into healed bone areas as<br />
well as for fresh extraction sockets or<br />
after losses of other implants. The<br />
implants may be combined<br />
with lateral basal<br />
implants (BOI)<br />
or any<br />
other brand<br />
of screw<br />
implants.<br />
www.implant.com<br />
www.zhermack.com<br />
| 46 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
Morita introduces a new Rotary outbreak:<br />
The Tri Auto Mini<br />
The high-performance Tri Auto mini endodontic motor excels with its extremely high level of<br />
flexibility. With its compact dimensions and low weight, it fits perfectly into the hand and opens<br />
up a new degree of freedom in treatment possibilities due to its rechargeable battery operation.<br />
The user can adjust file speed, torque values and various safety functions at the touch of a<br />
button and in this way increase safety for patients. And the various parameters for individual<br />
indications can be stored for even easier handling.<br />
In combination with the Root ZX mini apex locator, you have an endometric and treatment<br />
instrument of the very highest quality. Special display setting for left-handers<br />
Flexibility<br />
• Tri Auto mini is suitable for all standard NiTi files<br />
• Rotational handpiece (250°) for optimum visibility in all quadrants<br />
• Speed range from 50 - 1,000 rpm<br />
• Suitable for both right-handers and left-handers<br />
• Battery-operated (rechargeable) and cable-free<br />
Treatment Comfort<br />
• Easy-to-handle angle piece with extremely small<br />
head (9mm) for high patient comfort<br />
• Clear, energy-saving LC coloured display<br />
• Selectable signal tones<br />
• Variable file speeds<br />
• Variable torque values<br />
• 6 storage locations for treatment parameters<br />
www.morita.com<br />
WaveOne brings simplicity to Endodontics<br />
WaveOne, from DENTSPLY Maillefer, is the new endodontic system designed to provide simplicity and efficiency to the<br />
root canal shaping procedure.<br />
The WaveOne motor works in a reciprocating mode with a large rotating angle in the cutting direction provides high<br />
efficiency, whereas a smaller angle in the reverse direction allows the WaveOne file to safely progress along the canal<br />
path, respecting the root canal anatomy. The optimised angles also reduce the risk of a screwing effect and file breakage.<br />
Single file technique<br />
The reciprocating technique makes it possible to shape most root canals using only one single WaveOne Nickel-<br />
Titanium(NiTi) file. No time is wasted changing NiTi instruments during the root canal shaping procedure and the global<br />
shaping time is decreased by up to 40% versus a traditional continuous rotary technique, whilst still providing premium<br />
quality root canal treatments.<br />
The WaveOne file geometry was conceived specifically to benefit from the optimised preprogrammed<br />
reciprocating movement of the WaveOne motor. The proprietary DENTSPLY<br />
M-Wire Nickel-Titanium technology provides additional flexibility and greater resistance to cyclic<br />
fatigue, the leading cause of file separation.<br />
Single patient use<br />
DENTSPLY Maillefer advocates single patient use as a new standard of<br />
care, by proposing the WaveOne reciprocating NiTi files exclusively in<br />
presterilized blister packs and fitted with a non autoclavable handle. The<br />
advantages are:<br />
• Simplicity<br />
• No risk of cross contamination<br />
• Optimal cutting efficiency<br />
• Better control of file breakage<br />
www.dentsply.com<br />
| 48 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
Special Offer<br />
Buy 12 packs<br />
of a Zeta Hygiene product*<br />
and get 2 extra packs FREE<br />
for example:<br />
BUY<br />
12x<br />
FREE<br />
2x<br />
12x<br />
2x<br />
ZHERMACK STERILIZATION SOLUTIONS PROTECT YOURSELF AND YOUR PATIENTS<br />
*Zeta 5 Unit excluded<br />
The range of Zeta Hygiene products for<br />
sterilisation and disinfection allows the user to<br />
deal with all the hygienic–sanitary requirements<br />
of the dental surgery. Developed and tested<br />
according to the latest harmonised European<br />
disinfection standards.<br />
years<br />
ZHERMACK’S range of disinfection and<br />
sterilisation products satisfies all the needs of<br />
the modern dental surgery.<br />
Tel. +39 - 0425 597611 - Fax +39 - 0425 597645<br />
comm.expo@zhermack.com - www.zhermack.com
"Pentron Clinical" Launching Ceremony<br />
Organized by Prodent s.a.l.<br />
Pentron Clinical launching ceremony organized by Prodent s.a.l. counts as<br />
one of the most successful events of the year 2011.<br />
During the evening hours of the Day May 30, 2011 and under the Prodent’s<br />
Skies, more than 100 dentists visited Prodent to inspect the new restorative<br />
line of products.<br />
The President of the LDA, Dr. Ghassan Yared, Dean of the Lebanese<br />
University Prof. Mounir Doumit, Dean of the Arab university Prof. Essam<br />
Osman and Dr. Carina Mehanna Zoghaib representing the Saint-Joseph<br />
University were present to give a round of applause for this achievement.<br />
Dr. Gregori Kurtzman from Pentron Clinical, who has been selected annually<br />
since 2006 as one of the “TOP DENTAL” lecturers by Dentistry Today, was<br />
honored to be surrounded by the huge number of dentists and answered to<br />
their detailed and qualified questions.<br />
The soft music and the original exotic food were also a part of this friendly<br />
gathering which added pleasant and fun to this event.<br />
www.prodent-me.com<br />
Planmeca launches a full Digital Intraoral Scanning Solution:<br />
World’s first dental unit integrated intraoral scanner Planmeca PlanScan<br />
The new patient-friendly, high-performance process delivers complete clinical information about the patient anatomy by<br />
combining the surface data from Planmeca PlanScan intraoral scanner with Planmeca Promax 3D CBVT X-ray data and<br />
the 3D facial photo acquired from Planmeca Promax 3D ProFace. Unique 3D combination of these three cutting edge<br />
3-dimensional data enables more accurate treatment planning, procedures, and more satisfied patients.<br />
Making the treatment process faster and more accurate<br />
Planmeca PlanScan intraoral scanner allows the dentists to capture the complete intraoral situation directly and save it as a<br />
highly accurate 3D digital model. This model is instantly ready to use for design. Dentists can omit the taking of impressions<br />
and bypass related disadvantages such as inaccuracies, material costs, impression retakes and manual handling. Patient<br />
satisfaction soars – due to less chair time, reduced remakes, faster treatment completion, better fits and an overall improved<br />
chair-side experience. Planmeca PlanScan intraoral scanner is fully integrated to dental unit, which enhances ergonomics<br />
and all-digital workflow. Planmeca PlanScan is, however, also offered as Cart delivery when preferred.<br />
Planmeca PlanScan - Enabling labs to tighten relationships with dentists<br />
Labs can strengthen their professional ties with their dentist clients by offering new digital services that include receiving the<br />
dentist’s Planmeca PlanScan scanner data directly. They will be effectively helping dentists transition into digital impression<br />
taking while enabling them to enjoy the full range of indications and high<br />
quality results that come with professional dental technician expertise.<br />
The lab will also experience workflow benefits – more accurate case input<br />
and shorter turnaround times because restoration design work can start<br />
immediately without creation of a physical model.<br />
Digital Perfection – revolutionary integration of three 3D data<br />
The innovative combination of intraoral surface data, 3D X-ray data and<br />
facial soft tissue image delivers clear benefits for different specialists.<br />
Integrating surgical planning and prosthetic planning, the 3D digital model<br />
helps defining the ideal position of implant. Furthermore, the implant<br />
planning data can be used in crown design.<br />
The 3D X-ray data alone contains accurate information about the bone<br />
structure. Now with the combined data, periodontal tissues can be evaluated<br />
in relation to bone. For Orthodontic treatment no gypsum models are no<br />
longer necessary, and the treatment follow up can be done using radiation<br />
free Planmeca ProFace images.<br />
www.planmeca.com<br />
| 50 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
TOTAL SOLUTIONS FOR<br />
EXCELLENT TOTAL SOLUTIONS DENTISTRY FOR<br />
EXCELLENT DENTISTRY<br />
Hu-Friedy brings you a wide range of top quality instruments, efficient solutions for cleaning and<br />
sterilisation as well as a well-planned instrument management system to support your needs, your<br />
Hu-Friedy brings you a wide range patient’s of top health quality and instruments, staff’s safety. efficient solutions for cleaning and<br />
sterilisation as well as a well-planned instrument management system to support your needs, your<br />
Quality, choice and focus on the patient’s practitioner’s health needs and staff’s are the safety. pieces that only Hu-Friedy can bring<br />
together through world-class products and service.<br />
Quality, choice and focus on the practitioner’s needs are the pieces that only Hu-Friedy can bring<br />
together through world-class products and service.<br />
THIS IS MORE THAN<br />
A CASSETTE.<br />
THIS IT IS IS A MORE BUSINESS THAN<br />
A SOLUTION.<br />
CASSETTE.<br />
IT IS A BUSINESS<br />
Increase safety and productivity of your<br />
practice with Hu-Friedy’s Instrument<br />
SOLUTION.<br />
Management System (IMS). IMS allows you<br />
Increase to move safety instruments and productivity from cleaning of your through<br />
practice chairside with without Hu-Friedy’s touching, Instrument damaging or<br />
Management losing your System instruments. (IMS). IMS allows you<br />
to move instruments from cleaning through<br />
chairside without touching, damaging or<br />
losing your instruments.<br />
THE NEW STANDARD<br />
FOR PERFORMANCE IN<br />
NON-STICK THE NEW STANDARD COMPOSITE<br />
FOR PERFORMANCE INSTRUMENTS<br />
NON-STICK COMPOSITE<br />
INSTRUMENTS<br />
With the Hu-Friedy XTS product line, the<br />
processing of different composite materials has<br />
been completely revolutionised.<br />
The With result: the XTS Hu-Friedy instruments XTS with product a black line, aluminium the<br />
and processing titanium of nitrate different coating composite are especially materials hard, has smooth<br />
and scratch-resistant been completely - various revolutionised.<br />
composites can be<br />
The result: XTS instruments processed with a black better aluminium and more simply.<br />
and titanium nitrate coating are especially hard, smooth<br />
and scratch-resistant - various composites can be<br />
processed better and more simply.<br />
www.hu-friedy.eu<br />
www.hu-friedy.eu
<strong>Smile</strong>'s Content is Now Included in<br />
ALMANHAL Electronic Database<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> signed an agreement with<br />
ALMANHAL; an electronic publishing company established<br />
in 2009, which permits to include the content of <strong>Smile</strong><br />
in Al Manhal full-text searchable electronic database of<br />
scholarly, professional and peer-reviewed documents.<br />
As ALMANHAL is a Joint Venture between Wolters Kluwer,<br />
Ebrary, HRH Prince Bandar Bin Sultan and TechKnowledge,<br />
and it will utilize the distribution channels of its investor/<br />
partnerWolters Kluwer (Ovid) in order to make its <strong>Journal</strong>s<br />
available in universities, hospitals, governments and public<br />
libraries throughout the world.<br />
Mr. Basheer Alnasser; General Manager of ALMANHAL,<br />
stated that ALMANHAL aims to fulfill the increasing<br />
demand of the medical and academic institutions in the<br />
Arab world for the digital content originating from the<br />
Arab countries, thus providing search systems similar to<br />
those that are trusted by thousands of publishers around<br />
the world to publish their books and periodicals to more<br />
than 17 million user and more than 14000 institution in<br />
over 40 countries.<br />
Dr. Issa Bader; Founder and Chief Editor of <strong>Smile</strong>,<br />
declared that this agreement will enhance the exposure<br />
of <strong>Smile</strong>'s content all over the world and this would boost<br />
<strong>Smile</strong>'s impact factor and provides the authors who choose<br />
to publish their articles in <strong>Smile</strong> the opportunity to reach a<br />
greater number of readers and achieve more citation of<br />
their articles in the related published material worldwide.<br />
Neo AutoChip Maker<br />
Easy & Simple Auto Bone<br />
Collector<br />
Everyone knows auto graft bone is very good for<br />
bone formation, but there were limitations which<br />
the Quantity is limited and it is hard to get.<br />
Neo Autochip maker solves<br />
these problems.<br />
Easy and safe method to get 1cc<br />
autobone within 10 seconds.<br />
Features<br />
• Gathers bone while drilling<br />
• No bone loss<br />
• Reduce healing time<br />
• Control particle size<br />
• Gather fresh bone<br />
www.neobiotech.co.kr<br />
QuickLase Launches a New<br />
Dual Laser<br />
The NEW QuickLase 8w Dual wavelengths of 4w 810nm<br />
AND 4w 980nm at the same time. It is the ONLY laser<br />
on the market with ultimate coagulation and cutting, NO<br />
OTHER LASER LIKE IT with this technology. Its so powerful<br />
but controlled.<br />
In addition to the 8w Dual, the 3.5w is an entry level for<br />
most of soft tissue management such as gum re-contouring,<br />
with its touch screen technology, weighing under 1.6kg<br />
is small enough to fit into a briefcase and has audio<br />
confirmation and help screens for procedures as well built-in<br />
fibre optic housing making it easy to move from surgery<br />
to surgery. With<br />
far reaching<br />
applications from<br />
gingivectomy and<br />
crown lengthening<br />
to laser<br />
curettage and<br />
operculectomy,<br />
plus many<br />
more uses too<br />
numerous to<br />
mention.<br />
www.quicklase.com.<br />
Open your Doors to More Patients<br />
Become a LASER Dentist<br />
The New Cordless PowerPen Laser has been talked about by<br />
many dentists and compared to by its closest competitor:<br />
• Half the price of its competitor<br />
• Lightweight & easy to balance in one hand<br />
• Easy to operate<br />
• Cutting tips are easy to bend and have more uses before<br />
changing<br />
• Battery charges faster and lasts longer<br />
QuickLase have a range of soft tissue management<br />
lasers. Starting with the cordless PowerPen 2w 810nm,<br />
the 3.5w 810nm diode laser and the famous Dual 8w<br />
810nm+980nm for ultimate coagulation and ultimate<br />
cutting for the ultimate price.<br />
QuickLase lasers are made in the UK at Ramsgate, and<br />
supported direct by QuickLase. They are not made in China;<br />
they are made in the United Kingdom.<br />
www.quicklase.com<br />
| 52 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 2 - 2011
The MM . men...<br />
TALKING ABOUT<br />
A<br />
NEW!<br />
SEPARATION?<br />
3<br />
www.revo-s.com<br />
ENDO<br />
PLEASURE!<br />
The ideal all-in-one<br />
compatible with all NiTi<br />
systems on the market.<br />
JC.AUGÉ n www.jcauge.com<br />
®<br />
ENDOAce<br />
Endo motor with torque<br />
and speed control<br />
+ integrated apex<br />
locator<br />
= no more separation!<br />
Micro-Mega ®<br />
International Distribution<br />
mmid@micro-mega.com<br />
www.micro-mega.com<br />
®<br />
ENDOAce<br />
= NO m ORE<br />
<br />
Revo-S<br />
<br />
Revo-S<br />
Revolutionary NiTi files<br />
with asymmetrical<br />
cross section<br />
= less stress on the file,<br />
less risk of separation!<br />
SEPARATION<br />
Your Endo Specialist
6 - 7 April , 2011, Amman, Jordan<br />
7 th Jordanian Orthodontic Congress<br />
Prepared by Dr. Shadi Samawi<br />
Under the patronage of HE the Jordanian Minister of Health, the Jordanian Orthodontic Society (JOS) held its 7 th<br />
Jordanian Orthodontic Congress, at the Sheraton Hotel in Amman on the 6 th & 7 th of April 2011, under the main theme<br />
of “Early Orthodontic Treatment... An Ounce of Prevention”<br />
The congress’ memorial lecture was dedicated to the memory of the late Prof. Samir Bishara, one of the most influential<br />
figures in the world of Orthodontic research, and was presented by Guest speakers Prof. Abbas Zaher (Egypt) and Dr.<br />
Roy Sabri (Lebanon).<br />
In addition to the main scientific program<br />
spanning two full days - which included<br />
speakers from Jordan, Egypt, Palestine, Saudi<br />
Arabia, Syria, Lebanon & USA - among<br />
others, the conference’s scientific agenda<br />
also included two clinically-oriented pre- &<br />
post-congress courses by renowned guest<br />
speakers Professors Peter Ngan (West Virginia<br />
University - USA) and Bakr Rabie (University of<br />
Honk Kong). It also witnessed the introduction<br />
of the 7 th JOC’s first-ever Scientific Interactive<br />
Day which included various clinicallyrelevant<br />
table clinics, round table discussions<br />
and poster presentations covering major<br />
clinical orthodontic topics and state-ofthe-art<br />
technology currently trending in the<br />
profession.
Middle East<br />
Symposium<br />
7 - 8 Dec. 2011<br />
Jordan
9 - 11 April , 2011, Kuwait, Kuwait<br />
The 15 th Kuwait<br />
<strong>Dental</strong> Association<br />
International Scientific<br />
Conference<br />
“Invitation to a Practical<br />
World of Dentistry”<br />
Prepared by Dr. Yousef Sadik Marafie<br />
The Kuwait <strong>Dental</strong> Association has organized the<br />
15 th International Scientific Conference and their<br />
2 nd workshops at Radisson SAS Hotel Kuwait - Al<br />
Hashimi under the auspices of His Excellency the<br />
Minister of Health Dr. Hilal Al-Sayer.<br />
The <strong>Dental</strong> Association of Kuwaiti through this<br />
congress aimed to focus on 3-objective axes: local,<br />
Arab and international as follows:<br />
Local objectives:<br />
1. To raise the level of the dental profession in Kuwait<br />
for citizens to achieve the greatest health care.<br />
2. To contribute to the organization of practicing<br />
dentistry in the government sector and private<br />
companies, and overseeing the application of<br />
laws and health regulations and to ensure the<br />
submission of proposals developed for the benefit<br />
of citizens and the profession.<br />
Arab goals:<br />
1. To improve the health of the Arab people and to<br />
ensure better health services.<br />
2. To encourage cooperation and exchange of<br />
experience among dentists in the Arab world.<br />
3. Arabization of medical terminology in<br />
collaboration with trade associations and dentists<br />
in the Arab world.<br />
Global goals:<br />
The Association in cooperation with similar bodies in<br />
foreign countries and international organizations as<br />
well as the union of dentists aims to serve the global<br />
objectives of the association and its members.<br />
In addition to invaluable up-to-date clinical and<br />
scientific lectures and workshops, there was an<br />
exhibition organized by the congress committee in<br />
co-operation of leading international companies<br />
which aimed to present their latest equipment and<br />
dental technology. This of-course in addition to<br />
the very popular tourist entertainment program<br />
organized by the congress committee for the<br />
conference guests who were shown the traditional<br />
touristic and the modern commercial and leisure sites<br />
in the State of Kuwait.
DO YOU SUFFER FROM<br />
BLEEDING GUMS?<br />
BLEEDING GUMS CAN BE THE FIRST SIGN OF GUM DISEASE,<br />
WHICH IS THE NO. 1 CAUSE OF TOOTH LOSS.<br />
HELPS STOP BLEEDING GUMS<br />
A DAILY TOOTHPASTE WITH MINERAL SALTS AND 6 NATURAL HERB EXTRACTS
15 - 16 April , 2011, Erbil, Iraq<br />
1 st Iraqi <strong>Dental</strong> Reunion 2011<br />
CAPP, IDA and KDA Open the Doors of the<br />
<strong>Dental</strong> Market in Iraq<br />
The conference was vibrant with excitement the 1 st Iraqi <strong>Dental</strong> Reunion in 10 years reuniting old friends and colleagues<br />
from dental industry from across the region. 1 st Iraqi <strong>Dental</strong> Reunion 2011 was a great success, achieving record<br />
attendance and further establishing a reputation as the dental industry’s leading regional event. It took place at the<br />
Saad Palace, in a new and strikingly modern environment on 15 - 16 April, Erbil, Iraq. The conference was organized<br />
in the mutual cooperation of CAPP (Centre for Advanced Professional Practices), Iraqi <strong>Dental</strong> Association and Kurdistan<br />
<strong>Dental</strong> Association. Minister for Health, Dr. Taher Abdullah Hussein Hawrami opened the conference and expressed his<br />
pleasure to announce that this conference open the way for new business and scientific opportunities.<br />
Dr. Raffi M. Aljobory, President of Iraqi <strong>Dental</strong> Association and Dr. Shakhawan Qadir Khoshnaw, President of the <strong>Dental</strong><br />
Association Kurdistan greeted all participants with a warm welcome and expressed their thanks and appreciation to the<br />
sponsors and supporters of this conference.<br />
The event welcomed more than 1200 and 400 visitors including dentists and dental technicians form the government<br />
and private sector and students coming from all provinces of Iraq. Participants accumulate the latest opinions, trends<br />
and insights from industry thought leaders, shared experiences with colleagues, made new contacts and bound exciting<br />
relationships and exchange their ideas and knowledge.<br />
There was a significant presence of all Iraqi Colleges and Universities:<br />
Sulaimani, Al-Anbar University ( Mosul), Baghdad Al-Mustanserriyah, Isfahan, University of Medical Sciences and Health<br />
Services Faculty of Islamic Republic of Iran, Guilan University of Medical Sciences Islamic Republic of Iran, Qazvin<br />
University of Medical Sciences Islamic Republic of Iran, Medical College Site Sadr Teaching Hospital, Kufa City, Najaf<br />
Governorate, Iraq, Sulaimani, Iraq.<br />
The main conference schedule included four plenary sessions. The scientific program offered a wide variety of topics.<br />
16 different lectures with a variety of topics in addition to 8 workshops were held.<br />
A sophisticated exhibition accompanied the 1st Iraqi dental Reunion, featuring 22 dental companies from different<br />
countries - Germany, USA, UK, Brazil, Netherlands, Switzerland, and Turkey. 18 Distributor companies from Iraq,<br />
UAE, Lebanon, Turkey and Jordan represented 115 dental manufacturers. Participants circulated through the dynamic<br />
area throughout the conference, learning about the latest services and products, speaking with representatives from<br />
exhibiting companies and using the space as a central meeting and networking point.
12 - 13 May , 2011, Dubai, UAE<br />
5 th<br />
CAD/CAM<br />
& Computerized Dentistry International<br />
Conference<br />
To welcome its 5 th Anniversary this year, CAD/CAM & Computerized Dentistry Int’l<br />
Conference embarked on a brand new journey.<br />
The organizers, CAPP and Emirates <strong>Dental</strong> Society achieve for the 5 th time great record of<br />
attendance and established a reputation as the industry’s leading international conference.<br />
The Address Dubai Marina Hotel hosts 726 participants in the very elegant atmosphere.<br />
Technology is changing the world of dentistry. In an increasingly inter-linked global<br />
environment. New threats and challenges have created an urgent need for new responses.<br />
Nowhere is this more true than in the area of education and training where technology is<br />
bringing new advantages and opportunities.<br />
“A quick glance at the last IDS in Koln, Germany shows not only the extraordinary<br />
improvements to computerized technology, but the extraordinary improvements to this<br />
technology, but the vast number of manufacturers that are joining the market as well” Dr.<br />
M Silwadi.<br />
Bringing together leading experts and practitioners, the conference proved an excellent<br />
opportunity for networking and sharing experiences in the application of technology<br />
throughout the learning cycle - from primary and secondary education through to<br />
professional development and lifelong learning.
Planmeca Compact i Touch<br />
Intelligent digital dental unit<br />
Romexis<br />
PlanS<br />
ProFace<br />
• 3D<br />
ProMax<br />
•<br />
PlanScan<br />
P<br />
•<br />
Large integrated touch panel<br />
Simple and enjoyable to use<br />
Excellent ergonomy and workflow<br />
x 3D •<br />
D •<br />
CAD/CAM<br />
open for combination 3D Unique<br />
P<br />
ProFace<br />
More information<br />
www.planmeca.com<br />
Planmeca Oy<br />
Asentajankatu 6, 00880 Helsinki, Finland<br />
tel. +358 20 7795 500, fax +358 20 7795 555<br />
sales@planmeca.com<br />
1971 - 2011
REGISTRATION<br />
Sponsored by<br />
Fill in and send to CAPP by fax: +971 4 3686883<br />
or email: events@cappmea.com<br />
www.cappmea.com/aesthetic2011
AED 1.750/US $480<br />
Conference registration package<br />
Conference Pass + 2 Nights Byblos Hotel<br />
(2 days pass to the conference, certificate,<br />
lunch and coffee breaks for the conference,<br />
2 nights stay in Byblos Hotel “4 stars<br />
single/double room” inclusive of breakfast<br />
and transportation to the conference venue)<br />
AED 1.200/US $330<br />
Only Conference Registration<br />
(2 days pass to the conference, certificate,<br />
lunch and coffee breaks for the conference)<br />
*Book now limited spaces available<br />
Registration Sponsored by <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong><br />
Name:<br />
Speciality:<br />
Clinic:<br />
Country:<br />
City:<br />
P.O.Box:<br />
Tel:<br />
Fax:<br />
Mobile:<br />
METHOD OF PAYMENT<br />
Credit Card<br />
Visa MasterCard<br />
Email:<br />
AUTHORIZATION NOTE<br />
Please debit my credit card with an amount of AED<br />
Card Number:<br />
Expiry:<br />
Billing Adress:<br />
Name on Card:<br />
for the 3 rd <strong>Dental</strong> – Facial Cosmetic<br />
International Conference.<br />
The card holder will honor this transaction<br />
and not hold CAPP responsible if the credit<br />
card number has been compromised.<br />
Country/Emirate: Date: Signature:<br />
Bank Transfer:<br />
Account Name: CAPP FZ LLC.; KV,<br />
Dubai, U.A.E.; Account No:<br />
1011-178649-301; SWIFT Code:<br />
EBILAEAD; Bank Name: Emirates<br />
Bank; Al Karama Branch, U.A.E.<br />
Cheque payment on the<br />
name of CAPP
Lateral window technique is the formation of the access to the maxillary sinus through its lateral wall.<br />
The process using this tool is simpler and much comfortable than any other technique. Above all, this surgical kit<br />
provides ultimate solutions for cases of only having with a thin residual bone height which is difficult to approach with<br />
a crestal technique, membrane rupture by a sinus crestal approach or placing multiple implants.<br />
In addition, Sla reamers can be easily adapted for the case of formation of minimum flap size on the inferior wall.<br />
Interested in being a distributor for Neobiotech products in some Arab countries?<br />
Please contact us: +962 79622 3402<br />
nidalkhalil@eagleds.com
2 - 4 June , 2011, Beirut, Lebanon<br />
12 th Lebanese University <strong>Dental</strong> Congress<br />
The 12 th Lebanese University <strong>Dental</strong> Congress in Beirut was attended by more than 1200 dentists to hear about some of<br />
the up to date clinical techniques and scientific publications in dentistry. The objective of this three day congress was to<br />
focus on challenges encountered in dental daily practice, new treatment approaches, researches, latest techniques and<br />
biomaterials used in dentistry. To this extent, the scientific committee chaired by Ass Prof. Elie Azar Maalouf managed to<br />
attract high profile faculty of 22 national and 32 international speakers from more than twelve countries, who presented<br />
up to date clinical lectures on various dental specialties.<br />
Few of the many prominent speakers contributed at this successful event were Prof. Clarck Stanford, Dr. Edgard El Chaar<br />
and Dr. Daniel Perez from the United states, Prof. Tara Renton and Dr. Hassan Maghaireh from the United Kingdom<br />
and Dr. Gilles Chaumanet, Dr. Radhouane Dallel and Prof. Paul Pionchon from France, in addition to many other high<br />
profile speakers from Canada, Germany, Denmark, Austria, Egypt and of course Lebanon.<br />
In addition to oral presentations, the program included specialized pre-congress forums and workshops, young podium,<br />
live transmissions, posters and research sessions and oral presentations.<br />
A comprehensive exhibition ran alongside the congress programme, and this year the Lebanese university welcomed<br />
more than 60 different exhibitors. Attendees enjoyed meeting suppliers, picking up samples and learning about the new<br />
products and services being demonstrated at the event.
Two Minutes with<br />
Dr. Marco Esposito<br />
PROFILE<br />
Prof. Dr. Marco Esposito, DDS PHD<br />
• Editor of the Cochrane Oral Health Group<br />
• Associate Professor in Biomaterials with the Sahlgrenska<br />
Academy at Göteborg University- Sweden<br />
• Editor in Chief of the European <strong>Journal</strong> of Oral Implantology<br />
Marco graduated with honors in dentistry at the University of<br />
Pavia, Italy, in 1990 and was awarded a PhD in Biomaterials<br />
from the Göteborg University in 1999. He worked as Guest<br />
Researcher at NIOM (The Nordic Institute of <strong>Dental</strong> Materials),<br />
Haslum, Norway and is a specialist in Periodontics (UK). He<br />
also acted as the Director of the Postgraduate <strong>Dental</strong> Specialties<br />
courses in <strong>Dental</strong> Implantology, School of Dentistry, University<br />
of Manchester, UK between 2007 and 2011, but now he has<br />
decided to be a freelance researcher and devote his time<br />
entirely to evidence based research in dental implantology.<br />
He authored more than 90 scientific publications in<br />
international peer-reviewed journals. His main research interests<br />
are the assessment of the effectiveness of various therapeutic<br />
interventions with particular emphasis on dental implants.<br />
Marco is worldwide well-known lecturer and leading speaker<br />
and author on evidence based dental Implantogy. He will be<br />
lecturing at the European Association of Oral Implantology<br />
Congress in Athens in October 2011.<br />
We are delighted at <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> that Prof. Esposito is<br />
now on our international advisory board.<br />
Questions/Answers:<br />
Why did you choose to be researcher in implant dentistry?<br />
I started my research training in Sweden as a requirement for<br />
my clinical postgraduate training, I got stuck in it, then I started<br />
to enjoy it and now I see it as a mission.<br />
What are the best/worst aspects of your job?<br />
The nicest part of being a researcher is that it gives you the<br />
opportunity to understand how things work, and the worst part<br />
is the bureaucracy linked with initiating research.<br />
Where do you live?<br />
After 21 years abroad, now I live in a small village called<br />
Arcore near Milan in Italy, quite famous for the “bunga-bunga”<br />
activities.<br />
What do you drive?<br />
I seldom drive as I spend most of my time flying outside Italy<br />
What drives you?<br />
Curiosity<br />
What’s your favorite food?<br />
Buffalo mozzarella<br />
What’s your hobby?<br />
Military history as I enjoy collecting world war II uniforms from<br />
the North African region<br />
What’s your favorite film?<br />
I enjoy historical and comedy films<br />
Favorite holiday destination?<br />
As I spend most of my time outside Italy, I always look forward<br />
to visiting central and south Italy for holiday.<br />
What inspires you?<br />
The willingness to understand more<br />
What really annoys you?<br />
People trying to stop other people from achieving things<br />
What keeps you awake at night?<br />
I am a very good sleeper, but those situations in which I feel I<br />
have no control keeps me awake<br />
What makes you smile?<br />
The innocence of kids<br />
What is your best characteristic?<br />
Perseverance<br />
Worst fault?<br />
Sometimes I can be impulsive<br />
Can you describe yourself in three words?<br />
Analytical, objective and curious<br />
What do you do to relax?<br />
Visit historical places and talk with people with different<br />
backgrounds<br />
If you weren’t a dentist, what would you have liked to<br />
have been?<br />
An archeologist<br />
Do you read and recommend <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong><br />
regularly?<br />
I am delighted that my friend Dr. Hassan Maghaireh has been<br />
appointed as the Editorial Director, therefore i can recommend<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> as one of the leading evidence based<br />
dental journals in the Middle East area.<br />
What would be your motto in life?<br />
“Provando and riprovando” by Galileo which translates into<br />
“trying and trying again”<br />
| 68 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 1 - 2011
CMA<br />
®<br />
CORONAL • MEDIAN • APICAL<br />
Only one<br />
sequence<br />
for treatment<br />
and retreatment
DGZI Members:<br />
drtamimi@drtamimi.com
D.T. LIGHT-POST ® X-RO ®<br />
ILLUSION <br />
Translucent quartz fiber<br />
COLOR ON DEMAND FIBER POST<br />
The smartest post you could envision<br />
RADIOPAQUE +<br />
ANATOMICAL<br />
RELIABLE<br />
AESTHETIC<br />
EASY TO USE<br />
D.T. LIGHT-POST X-RO Radiopacity<br />
Courtesy of Dr Cheleux University of Toulouse<br />
X-RO ®<br />
u 50 % more radiopaque<br />
u 20 % stronger<br />
u 30 % more retentive
Supervised Clinical Training<br />
with an Integrated MSc<br />
Warwick Dentistry is one of the UK’s foremost providers<br />
of dental education.<br />
Our three year courses give you the opportunity to study for an MSc programme<br />
whilst gaining hands on supervised training in a leading clinical practice. You will<br />
be taught using the latest methods, equipment and techniques and will receive<br />
one-to-one mentoring for clinical cases. Your learning will emphasise delivering<br />
safe, predictable treatment for your patients.<br />
MSc Endodontics with Supervised <strong>Dental</strong> Clinical Training<br />
MSc Implant Dentistry with Supervised Oral Surgery Clinical Training<br />
MSc in Orthodontics with Supervised <strong>Dental</strong> Clinical Training<br />
MSc in Restorative Dentistry with Supervised <strong>Dental</strong> Clinical Training<br />
MSc in Oral Surgery with Supervised <strong>Dental</strong> Clinical Training*<br />
* subject to approval<br />
l Assessment: Portfolio of cases plus competency assessment<br />
l Duration: 3 years full time<br />
l Teaching: 30 hours per week<br />
W www.warwick.ac.uk/go/dentistry<br />
e dentists@warwick.ac.uk
Assurance<br />
Invest in reliability. Focus on the patient.<br />
Express your style. From the people<br />
who build the most dependable dental<br />
equipment in the world, A-dec 200<br />
provides you with a complete system to<br />
secure a successful future.<br />
Discover how you can gain assurance with<br />
A-dec 200. Contact your authorised<br />
A-dec dealer today.<br />
Discover A-dec 200. Contact your local dealer.<br />
A-dec Inc.<br />
2601 Crestview Drive, Newberg, Oregon 97132 USA<br />
www.a-dec.com
المؤتمر السعودي العالمي الرابع عشر لجامعة الملك سعود لطب الأسنان<br />
الثالث والعشرون للجمعية السعودية لطب الأسنان<br />
King Saud University 14th International <strong>Dental</strong> Conference<br />
the 23rd for the Saudi <strong>Dental</strong> Society<br />
مركز معارض الرياض الدولي<br />
خلال الفترة من ١٤-١٦ ربيع الأول ١٤٣٣ه - الموافق – ٦ ٨ فبراير ٢٠١٢م<br />
Venue Riyadh International Exhibition Center<br />
14 – 16 Rabi’ 1 1433H . 6 – 8 February 2012<br />
4677763 / 4677743 / 4677764 / 4677534<br />
www.sds.org.sa
Quality<br />
Quality and guarantee of<br />
effectiveness and trouble-free<br />
process of prosthetics is the main<br />
duty of Implasa Höchst company.<br />
Research & Development<br />
Is there a limit in development of<br />
dental practice? The answer to this<br />
question opens by itself, if we take a<br />
look to the way which the Implasa<br />
Höchst company passed for 10 years<br />
in the field of the newest technologies<br />
of the cure and prosthetics of teeth.<br />
Materials & Technologies<br />
The high-quality materials +<br />
constantly improving technologies =<br />
the guarantee of our quality and<br />
your success<br />
Production Cycle<br />
ImPlasa Höchst company specialists<br />
diligently control the quality of the<br />
released production at all the stages<br />
of technological process<br />
and production.<br />
Microscopy<br />
The surface of implants is prepared<br />
by unique technology of ImPlasa<br />
Höchst company, named<br />
ImPlapore, which allows to reach<br />
minimal traumatizing in the area of<br />
implant installation, and such way<br />
maximally eases the<br />
osseointegration process.<br />
The Sole Representative in the<br />
Middle East and Africa<br />
E: dr.munther@implasa.de<br />
Syria<br />
Kingdom Medical &<br />
<strong>Dental</strong> Instruments<br />
Tel: +963 21 5732052<br />
majedajami01@hotmail.com<br />
Lebanon<br />
Kingdom Medical &<br />
<strong>Dental</strong> Instruments<br />
Tel: +961 6 426462<br />
kingdom_est@hotmail.com<br />
Turkey<br />
ASYA DENTAL<br />
Tel: +902164957287<br />
gulcan_celebi@mynet.com
Quality<br />
Quality and guarantee of<br />
effectiveness and trouble-free<br />
process of prosthetics is the main<br />
duty of Implasa Höchst company.<br />
Research & Development<br />
Is there a limit in development of<br />
dental practice? The answer to this<br />
question opens by itself, if we take a<br />
look to the way which the Implasa<br />
Höchst company passed for 10 years<br />
in the field of the newest technologies<br />
of the cure and prosthetics of teeth.<br />
Materials & Technologies<br />
The high-quality materials +<br />
constantly improving technologies =<br />
the guarantee of our quality and<br />
your success<br />
Production Cycle<br />
ImPlasa Höchst company specialists<br />
diligently control the quality of the<br />
released production at all the stages<br />
of technological process<br />
and production.<br />
Microscopy<br />
The surface of implants is prepared<br />
by unique technology of ImPlasa<br />
Höchst company, named<br />
ImPlapore, which allows to reach<br />
minimal traumatizing in the area of<br />
implant installation, and such way<br />
maximally eases the<br />
osseointegration process.<br />
The Sole Representative in the<br />
Middle East and Africa<br />
E: dr.munther@implasa.de<br />
Syria<br />
Kingdom Medical &<br />
<strong>Dental</strong> Instruments<br />
Tel: +963 21 5732052<br />
majedajami01@hotmail.com<br />
Lebanon<br />
Kingdom Medical &<br />
<strong>Dental</strong> Instruments<br />
Tel: +961 6 426462<br />
kingdom_est@hotmail.com<br />
Turkey<br />
ASYA DENTAL<br />
Tel: +902164957287<br />
gulcan_celebi@mynet.com