Student Health Insurance Confirmation Form - St. George's University
Student Health Insurance Confirmation Form - St. George's University
Student Health Insurance Confirmation Form - St. George's University

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
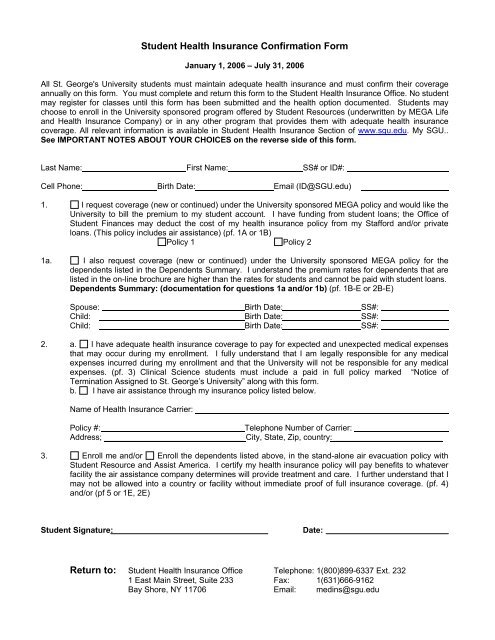
<strong><strong>St</strong>udent</strong> <strong>Health</strong> <strong>Insurance</strong> <strong>Confirmation</strong> <strong>Form</strong><br />
January 1, 2006 – July 31, 2006<br />
All <strong>St</strong>. <strong>George's</strong> <strong>University</strong> students must maintain adequate health insurance and must confirm their coverage<br />
annually on this form. You must complete and return this form to the <strong><strong>St</strong>udent</strong> <strong>Health</strong> <strong>Insurance</strong> Office. No student<br />
may register for classes until this form has been submitted and the health option documented. <strong><strong>St</strong>udent</strong>s may<br />
choose to enroll in the <strong>University</strong> sponsored program offered by <strong><strong>St</strong>udent</strong> Resources (underwritten by MEGA Life<br />
and <strong>Health</strong> <strong>Insurance</strong> Company) or in any other program that provides them with adequate health insurance<br />
coverage. All relevant information is available in <strong><strong>St</strong>udent</strong> <strong>Health</strong> <strong>Insurance</strong> Section of www.sgu.edu. My SGU..<br />
See IMPORTANT NOTES ABOUT YOUR CHOICES on the reverse side of this form.<br />
Last Name: First Name: SS# or ID#:<br />
Cell Phone: Birth Date: Email (ID@SGU.edu)<br />
1. I request coverage (new or continued) under the <strong>University</strong> sponsored MEGA policy and would like the<br />
<strong>University</strong> to bill the premium to my student account. I have funding from student loans; the Office of<br />
<strong><strong>St</strong>udent</strong> Finances may deduct the cost of my health insurance policy from my <strong>St</strong>afford and/or private<br />
loans. (This policy includes air assistance) (pf. 1A or 1B)<br />
Policy 1 Policy 2<br />
1a. I also request coverage (new or continued) under the <strong>University</strong> sponsored MEGA policy for the<br />
dependents listed in the Dependents Summary. I understand the premium rates for dependents that are<br />
listed in the on-line brochure are higher than the rates for students and cannot be paid with student loans.<br />
Dependents Summary: (documentation for questions 1a and/or 1b) (pf. 1B-E or 2B-E)<br />
Spouse: Birth Date: SS#:<br />
Child: Birth Date: SS#:<br />
Child: Birth Date: SS#:<br />
2. a. I have adequate health insurance coverage to pay for expected and unexpected medical expenses<br />
that may occur during my enrollment. I fully understand that I am legally responsible for any medical<br />
expenses incurred during my enrollment and that the <strong>University</strong> will not be responsible for any medical<br />
expenses. (pf. 3) Clinical Science students must include a paid in full policy marked “Notice of<br />
Termination Assigned to <strong>St</strong>. George’s <strong>University</strong>” along with this form.<br />
b. I have air assistance through my insurance policy listed below.<br />
Name of <strong>Health</strong> <strong>Insurance</strong> Carrier:<br />
Policy #:<br />
Telephone Number of Carrier:<br />
Address; _______________________________ City, <strong>St</strong>ate, Zip, country: ________________________<br />
3. Enroll me and/or Enroll the dependents listed above, in the stand-alone air evacuation policy with<br />
<strong><strong>St</strong>udent</strong> Resource and Assist America. I certify my health insurance policy will pay benefits to whatever<br />
facility the air assistance company determines will provide treatment and care. I further understand that I<br />
may not be allowed into a country or facility without immediate proof of full insurance coverage. (pf. 4)<br />
and/or (pf 5 or 1E, 2E)<br />
<strong><strong>St</strong>udent</strong> Signature:<br />
Date:<br />
Return to: <strong><strong>St</strong>udent</strong> <strong>Health</strong> <strong>Insurance</strong> Office Telephone: 1(800)899-6337 Ext. 232<br />
1 East Main <strong>St</strong>reet, Suite 233 Fax: 1(631)666-9162<br />
Bay Shore, NY 11706 Email: medins@sgu.edu
Important Notes About Your Choices<br />
1. Policy coverage is from August 1, 2005 to July 31, 2006, or January 1, 2006 to July 31, 2006 for<br />
those entering School in January 2006. The one-year pre-existing condition exclusion (any illness<br />
treated in the year prior to the first date of enrollment in the policy) should be taken into<br />
consideration if you are choosing the MEGA program for the first time unless you can provide<br />
HIPPA, proof of previous and continuous coverage.<br />
• The annual insurance premium is NON-REFUNDABLE unless you are not enrolled the first 31 days<br />
of the policy year. <strong><strong>St</strong>udent</strong>s who are not enrolled for the first 31 days will have the premium<br />
refunded and the policy cancelled without any further notice.<br />
• If you choose to enroll or continue your enrollment in the MEGA program, you will receive a bill for<br />
the annual premium on your SGU student accounts statement. January entering students will be<br />
billed for the seven month policy, (January-July), on their first term’s statement and will be required<br />
to reconfirm health insurance coverage the following August.<br />
• If your loan applications are complete and approved at the time payment is due you may, as with<br />
other <strong>University</strong> charges, defer payment until your loans are disbursed.<br />
• Eligible students may borrow the amount for health insurance from student loan programs by<br />
contacting their financial aid counselor and completing the necessary paperwork. However, you<br />
may not borrow or use your financial aid to pay for dependent policies. You will be asked to send a<br />
personal check to pay for dependent policies.<br />
. By checking box 2a you are certifying that you will maintain adequate health insurance throughout<br />
the year 8/1/05 to 7/31/06. Please consider that your current policy may not continue<br />
coverage after age 25. If you will turn the age of 25 during this year and your existing<br />
coverage will expire, you should enroll in the MEGA or some other program. You can only<br />
join the MEGA program in August or January. If you are studying on the islands of Grenada or<br />
<strong>St</strong>. Vincent you will need air evacuation coverage and must also check 2b or 3.<br />
• By checking 2b, you are certifying that your health insurance carrier will provide air evacuation<br />
benefits as well as health insurance benefits for your treatment and care. It is your responsibility<br />
to provide your family and the Director of <strong>University</strong> <strong>Health</strong> Services, Attn: Dr. V. Chellapilla<br />
in Grenada, the information about your health and air evacuation policy to use in an<br />
emergency situation. Please send a copy to our office to keep on file.<br />
• By checking 3, you are requesting the stand alone air assistance policy and also certifying that<br />
your health insurance will pay benefits at whatever facility you are taken to in an emergency. The<br />
$40.00 ($74.00 per family) charge for the stand-alone policy will be billed to your student account.<br />
Obviously it could put you in great harm should you arrive in a country and/or facility that would not<br />
accept you as a patient because they lacked proof of insurance. It is your responsibility to<br />
provide your family, the Director of <strong>University</strong> <strong>Health</strong> Services, ATTN: Dr. V. Chellapilla in<br />
Grenada, and our office with the information about your health insurance benefits should it<br />
become necessary to call the air ambulance on your behalf.<br />
2. Clinical Science Medical <strong><strong>St</strong>udent</strong>s who do not take the Mega policy (box 2), must include a copy of the<br />
paid in full policy marked “notice of Termination Assigned to <strong>St</strong>. George’s <strong>University</strong> along with this<br />
form. We will view you failure to do so by July 25th, 2005 as your notice to be enrolled instead in the<br />
Mega Policy Option 1. The cost of the policy will be applied to your student account. Please give the<br />
following address to your insurance company for notification of policy termination.<br />
<strong><strong>St</strong>udent</strong> <strong>Health</strong> <strong>Insurance</strong> Office, One East Main <strong>St</strong>reet, Suite 233, Bay Shore, NY 11706.<br />
See Dean Weitzman’s memo to clinical students regarding health insurance.