

sepsis and the kidney.pdf - SASSiT
sepsis and the kidney.pdf - SASSiT
sepsis and the kidney.pdf - SASSiT

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Crit Care Clin 21 (2005) 211 – 222<br />
Sepsis <strong>and</strong> <strong>the</strong> Kidney<br />
Jennifer Klenzak, MD, Jonathan Himmelfarb, MD*<br />
Division of Nephrology, Maine Medical Center, 22 Bramhall Street, Portl<strong>and</strong>, ME 04102, USA<br />
Acute renal failure (ARF) affects up to 20% of critically ill patients; <strong>sepsis</strong><br />
accounts for most ARF cases in <strong>the</strong>se patients. ARF occurs in 51% of patients<br />
with septic shock <strong>and</strong> positive blood cultures [1]. Approximately 700,000<br />
hospitalized patients develop <strong>sepsis</strong> each year in <strong>the</strong> United States, <strong>and</strong> <strong>the</strong>y<br />
account for 210,000 deaths. Between 5% <strong>and</strong> 51% of <strong>the</strong>se patients develop<br />
ARF, <strong>and</strong> <strong>the</strong> risk increases with positive blood cultures <strong>and</strong> worsening clinical<br />
signs of <strong>sepsis</strong>. The last 20 years have witnessed significant improvements<br />
in <strong>the</strong> care of critically ill patients, leading to improved outcomes in many<br />
diseases. Unfortunately, <strong>the</strong> septic patient with ARF has not benefited from<br />
technologic <strong>and</strong> <strong>the</strong>rapeutic advances to <strong>the</strong> same degree. Mortality remains<br />
unacceptably high for septic patients with ARF, hovering at 70%. The development<br />
of ARF in <strong>the</strong>se patients portends a poor outcome. It remains unclear,<br />
however, whe<strong>the</strong>r ARF plays a significant role in <strong>the</strong> subsequent development<br />
of multiple organ systems failure (MOSF), through its effects on metabolic<br />
homeostasis, or if ARF is merely a marker on <strong>the</strong> road to <strong>the</strong> loss of life.<br />
Patients who develop ARF in <strong>the</strong> setting of critical illness are more likely to<br />
die than dialysis-dependent patients admitted to <strong>the</strong> ICU, suggesting that <strong>the</strong><br />
outcome associated with <strong>the</strong> development of new renal dysfunction is based on<br />
<strong>the</strong> pathophysiology of <strong>sepsis</strong> <strong>and</strong> systemic dysregulation, ra<strong>the</strong>r than merely<br />
<strong>the</strong> renal dysfunction itself [2].<br />
* Corresponding author.<br />
E-mail address: himmej@mmc.org (J. Himmelfarb).<br />
0749-0704/05/$ – see front matter D 2005 Elsevier Inc. All rights reserved.<br />
doi:10.1016/j.ccc.2005.01.002<br />
criticalcare.<strong>the</strong>clinics.com
212<br />
klenzak & himmelfarb<br />
Pathophysiology<br />
Tubular epi<strong>the</strong>lium <strong>and</strong> acute tubular necrosis<br />
The clinical syndrome of ARF in <strong>the</strong> setting of critical illness, manifested by<br />
rising serum creatinine <strong>and</strong> decreasing urine output, results from injury to <strong>the</strong><br />
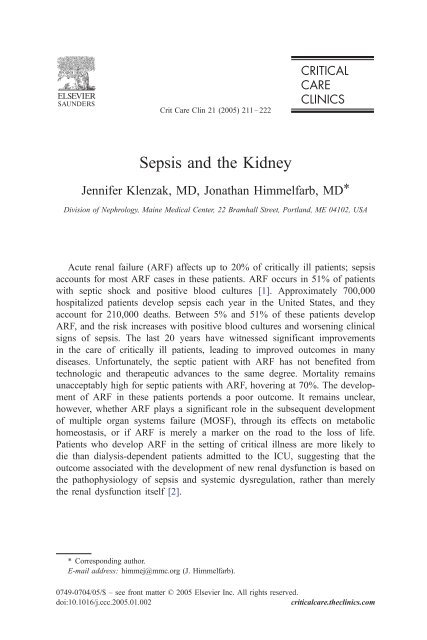
tubular epi<strong>the</strong>lial cells, or acute tubular necrosis (Fig. 1). Ischemic or toxic injury<br />
primarily affects this renal compartment, both because this area is most dependent<br />
on downstream blood flow, <strong>and</strong> <strong>the</strong>se cells are highly metabolically active,<br />
engaged in solute <strong>and</strong> water transport. The tubular epi<strong>the</strong>lial cells most vulnerable<br />
to ischemia line <strong>the</strong> S3 segment of <strong>the</strong> proximal tubule.<br />
Lethal injury to <strong>the</strong>se cells (necrosis or apoptosis) leads to loss of cell adhesion<br />
to <strong>the</strong> tubular basement membrane <strong>and</strong> subsequent shedding into <strong>the</strong> lumen. The<br />
denuded cells appear in <strong>the</strong> urine intact as tubular epi<strong>the</strong>lial cell casts, or <strong>the</strong>y<br />
may degrade leading to excretion of granular casts, both of which are typically<br />
found in <strong>the</strong> urine of patients with acute tubular necrosis. Such casts may cause<br />
micro-obstruction to urine flow. The damaged tubular basement membrane may<br />
fill with cast material, cellular debris, <strong>and</strong> Tamm-Horsfall protein. Sublethal<br />
injury results in loss of <strong>the</strong> brush border, which is <strong>the</strong> site of much energyconsuming<br />
metabolic activity.<br />
The mechanisms of injury to tubular epi<strong>the</strong>lial cells in <strong>sepsis</strong> are difficult to<br />
reproduce in <strong>the</strong> laboratory. Laboratory models of acute tubular necrosis have<br />
Pathophysiology of Ischemic Acute Renal Failure<br />
MICROVASCULAR<br />
Glomerular<br />
Medullary<br />
Vasoconstriction in response to:<br />
endo<strong>the</strong>lin, adenosine,<br />
angiotensin II, thromboxane A2,<br />
leukotrienes, sympa<strong>the</strong>tic nerve<br />
activity<br />
Vasodilation in response to:<br />
nitric oxide, PGE2, acetylcholine<br />
bradykinin<br />
Endo<strong>the</strong>lial <strong>and</strong> vascular smooth<br />
muscle cell structural damage<br />
Leukocyte-Endo<strong>the</strong>lial adhesion<br />
vascular obstruction, leukocyte<br />
activation, <strong>and</strong> inflammation<br />
O 2<br />
Inflammatory<br />
<strong>and</strong><br />
vasoactive<br />
mediators<br />
TUBULAR<br />
Cytoskeletal breakdown<br />
Loss of polarity<br />
Apoptosis <strong>and</strong> Necrosis<br />
Desquamation of viable<br />
<strong>and</strong> necrotic cells<br />
Tubular obstruction<br />
Backleak<br />
Fig. 1. Pathophysiology of ischemic acute renal failure. PGE2, prostagl<strong>and</strong>in E 2 .
<strong>sepsis</strong> <strong>and</strong> <strong>the</strong> <strong>kidney</strong> 213<br />
relied on ei<strong>the</strong>r ischemic or toxic injury to simulate ARF. More than ischemia or<br />
toxicity, however, is responsible for <strong>the</strong> cellular signaling to apoptosis in <strong>sepsis</strong>.<br />
In <strong>sepsis</strong> <strong>the</strong> loss of autoregulatory pathways, an imbalance between inflammation<br />
<strong>and</strong> anti-inflammatory cytokines, thrombosis <strong>and</strong> bleeding, vasodilation <strong>and</strong><br />
vasoconstriction, oxidation <strong>and</strong> reduction, catabolic <strong>and</strong> anabolic activity, <strong>and</strong><br />
dysregulation of enzyme activity all contribute to organ dysfunction through<br />
mechanisms not yet fully elucidated. It is in this pathologic milieu that <strong>kidney</strong><br />
function deteriorates in <strong>sepsis</strong>, which fur<strong>the</strong>r adds <strong>the</strong> stress of fluid <strong>and</strong><br />
electrolyte imbalance, waste clearance, <strong>and</strong> platelet dysfunction.<br />
Alterations in renal blood flow<br />
Intrarenal hemodynamic changes<br />
Systemic hypotension leads to autoregulation of local hemodynamics within<br />
<strong>the</strong> <strong>kidney</strong>. Afferent arteriolar vasoconstriction decreases capillary hydrostatic<br />
pressure <strong>and</strong> limits <strong>the</strong> perfusion of capillary beds. Impaired perfusion of capillary<br />
beds reduces filtration surface <strong>and</strong> leads to some reabsorption of interstitial<br />
fluid into <strong>the</strong> capillaries, as long as intravascular oncotic pressure remains constant<br />
or increases. Additionally, metabolic activity <strong>and</strong> waste products increase<br />
extracellular osmolality leading to fluid extravasation from cells. For <strong>the</strong>se<br />
reasons, intravascular <strong>and</strong> interstitial volume increase at <strong>the</strong> expense of intracellular<br />
volume.<br />
In <strong>the</strong> <strong>kidney</strong>, constriction of <strong>the</strong> afferent arterioles decreases glomerular<br />
perfusion. With less glomerular perfusion, less filtrate is generated. Micropuncture<br />
studies show that endotoxin decreases filtration rate <strong>and</strong> glomerular<br />
flow with increased renal arteriolar resistance [3]. This compensatory response<br />
may be somewhat protective in that it leads to less ATP-requiring work from <strong>the</strong><br />
highly metabolically active tubular epi<strong>the</strong>lial cells. Downstream of <strong>the</strong> glomerular<br />
capillary bed, decreased blood flow to <strong>the</strong> efferent arteriole reduces perfusion of<br />
<strong>the</strong> vasa recta. The vasa recta supply nutrients <strong>and</strong> oxygen, <strong>and</strong> serve as a conduit<br />
for <strong>the</strong> return of fluid <strong>and</strong> electrolytes to <strong>the</strong> systemic circulation from <strong>the</strong><br />
relatively hypoxic medulla. The S3 segment of <strong>the</strong> proximal tubule, or pars recta,<br />
is highly active <strong>and</strong> ATP-requiring. This segment is sensitive to alterations in<br />
blood flow because it depends on <strong>the</strong> deoxygenated blood of this microcirculation<br />
for its oxygen supply. For this reason, it is usually <strong>the</strong> first tubular<br />
segment to be injured from decreases in renal blood flow (RBF) or hypoxemia<br />
[4,5].<br />
Hypoxemia or decreased RBF is likely one of many mechanisms of renal<br />
injury in <strong>the</strong> setting of <strong>sepsis</strong>. It has also been suggested that renal ischemia<br />
related to decreased renal perfusion is not <strong>the</strong> main mechanism of ARF in <strong>sepsis</strong>.<br />
Animal models have shown increases in renal perfusion in <strong>the</strong> setting of<br />
hyperdynamic shock. ARF can occur in <strong>the</strong> setting of preserved or increased RBF
214<br />
klenzak & himmelfarb<br />
in <strong>the</strong> setting of hyperdynamic <strong>sepsis</strong>. Although <strong>the</strong> role of hypoperfusion needs<br />
elucidation in <strong>the</strong> setting of <strong>sepsis</strong>, <strong>the</strong>se studies certainly support <strong>the</strong> hypo<strong>the</strong>sis<br />
that mediators of cellular injury, ra<strong>the</strong>r than lack of blood, play a larger role in <strong>the</strong><br />
pathophysiology of ARF [6].<br />
Vasopressors <strong>and</strong> acute renal failure<br />
In <strong>the</strong> setting of hypodynamic septic shock, compensatory increases in<br />
systemic vascular resistance become disabled, leading to pressor desensitivity<br />
<strong>and</strong> refractory hypotension without local autoregulation of <strong>the</strong> vital organs.<br />
Clinical concerns regarding <strong>the</strong> use of vasopressor <strong>the</strong>rapies, which are known<br />
to induce vasoconstriction in <strong>the</strong> setting of ARF, are set aside by <strong>the</strong> supremacy<br />
of increasing systemic blood pressure to levels that continue to perfuse <strong>the</strong><br />
remainder of <strong>the</strong> vital organs. Norepinephrine infusion may, in fact, increase<br />
RBF. Several animal studies have demonstrated increases in RBF with <strong>the</strong> use of<br />
norepinephrine infusion [7–12]. Recent work by Di et al [13] demonstrated that<br />
norepinephrine infusion in septic sheep induced an increase in RBF, countering<br />
concern that vasoconstrictors worsen blood delivery to <strong>the</strong> renal parenchyma in<br />
<strong>the</strong> setting of vasodilatory shock.<br />
Nitric oxide synthase<br />
In contrast, in hyperdynamic shock RBF is preserved, with apparent<br />
redistribution of flow from cortex to medulla, maintaining oxygen delivery to<br />
<strong>the</strong> most vulnerable portions of <strong>the</strong> renal parenchyma, while also decreasing<br />
<strong>the</strong> work of <strong>the</strong> tubules. This redistribution of blood flow coincides with an increase<br />
in nitric oxide (NO) in <strong>the</strong> medulla [14]. Inducible NO synthase (iNOS)<br />
can be expressed locally, in glomerular mesangial cells <strong>and</strong> endo<strong>the</strong>lial cells,<br />
after stimulation with proinflammatory cytokines, including tumor necrosis factor<br />
(TNF) <strong>and</strong> interleukin (IL)-1, <strong>and</strong> endotoxin [15]. Nonselective or selective<br />
blockade of NOS decreases RBF while increasing mean arterial pressure. This<br />
suggests that iNOS plays a role in maintaining RBF in <strong>the</strong> setting of shock<br />
through its vasodilatory effects at <strong>the</strong> afferent arteriole. Despite increases in<br />
iNOS, renal vasoconstriction can be seen in <strong>the</strong> setting of systemic vasodilation.<br />
The mechanism of vasodilation by NO is dependent on <strong>the</strong> syn<strong>the</strong>sis of cyclic<br />
guanosine monophosphate by soluble guanylate cyclase. Studies of lipopolysaccharide<br />
(LPS) stimulation in mice leading to shock <strong>and</strong> ARF have demonstrated<br />
a decrease in cyclic guanosine monophosphate to basal levels at 24 hours,<br />
despite an early rise in <strong>and</strong> sustained iNOS levels, suggesting that desensitization<br />
of soluble guanylate cyclase results in loss of regulatory vasodilation in <strong>the</strong> <strong>kidney</strong><br />
[16]. NOS inhibition in animal models of endotoxemia results in glomerular<br />
thrombosis <strong>and</strong> declines in creatinine clearance. The glomerular thrombosis<br />
in <strong>the</strong> setting of NOS inhibition seems related to <strong>the</strong> antithrombotic qualities of
<strong>sepsis</strong> <strong>and</strong> <strong>the</strong> <strong>kidney</strong> 215<br />
NOS, by inhibiting leukocyte interactions with endo<strong>the</strong>lial cells <strong>and</strong> inhibiting<br />
platelet aggregation [17].<br />
Soluble <strong>and</strong> local mediators<br />
Endo<strong>the</strong>lins<br />
The production of endo<strong>the</strong>lins, which are potent vasoconstrictors, by endo<strong>the</strong>lial,<br />
mesangial <strong>and</strong> tubular cells is stimulated by proinflammatory cytokines,<br />
including TNF. The vasoconstrictors vasopressin <strong>and</strong> angiotensin II also<br />
stimulate endo<strong>the</strong>lin release. Endo<strong>the</strong>lins cause vigorous constriction of <strong>the</strong><br />
afferent <strong>and</strong> efferent arterioles, <strong>and</strong> mesangial cell contraction. The effects of<br />
endo<strong>the</strong>lin may be secondary to its induction of platelet-activating factor (PAF)<br />
syn<strong>the</strong>sis in <strong>the</strong> mesangium or thromboxane A 2 by <strong>the</strong> endo<strong>the</strong>lium. Additionally,<br />
endo<strong>the</strong>lin induces some vasodilators, counteracting its vasoconstricting effect,<br />
including prostacyclin, NO, <strong>and</strong> prostagl<strong>and</strong>in E 2 . Two endo<strong>the</strong>lin receptors are<br />
active in <strong>the</strong> renal parenchyma: <strong>the</strong> endo<strong>the</strong>lin-A receptor is found mainly in <strong>the</strong><br />
vascular compartment, <strong>and</strong> <strong>the</strong> endo<strong>the</strong>lin-B receptor is found mainly in <strong>the</strong><br />
tubular compartment. In an animal model of glycerol-mediated toxic renal injury,<br />
selective antagonism of <strong>the</strong> endo<strong>the</strong>lin-A receptor lessened <strong>the</strong> reduction in glomerular<br />
filtration rate [18]. Preliminary evidence suggested that <strong>the</strong> endo<strong>the</strong>lin-B<br />
receptor was integral to clearing endo<strong>the</strong>lin-1, <strong>and</strong> probably plays a beneficial<br />
role in ischemia. Studies of selective endo<strong>the</strong>lin-A receptor blockade <strong>and</strong><br />
nonselective endo<strong>the</strong>lin receptor blockade (both endo<strong>the</strong>lin-A receptor <strong>and</strong><br />
endo<strong>the</strong>lin-B receptor) demonstrated improved outcomes only for <strong>the</strong> selective<br />
blockade in a chronic ischemia animal model, fur<strong>the</strong>r supporting <strong>the</strong> beneficial<br />
effects of intact endo<strong>the</strong>lin-B receptor function [19].<br />
Tumor necrosis factor <strong>and</strong> interleukin-1<br />
Major mediators of cytokine-induced renal injury include TNF <strong>and</strong> IL-1, both<br />
of which promote fur<strong>the</strong>r cytokine release, induce vasoconstriction, neutrophil<br />
aggregation, production of reactive oxygen species, <strong>and</strong> induction of tissue<br />
factor <strong>and</strong> promotion of thrombosis [20]. When infused into animal models, TNF<br />
<strong>and</strong> IL-1 result in renal damage <strong>and</strong> decrease RBF <strong>and</strong> glomerular filtration rate<br />
[21]. TNF is produced <strong>and</strong> circulated systemically, whereas IL-1 is expressed in<br />
<strong>the</strong> glomerular endo<strong>the</strong>lial cells early in animal models of <strong>sepsis</strong>. These pleiotropic<br />
cytokines are capable of inducing mesangial <strong>and</strong> endo<strong>the</strong>lial production<br />
of PAF, endo<strong>the</strong>lin, adenosine, NO, <strong>and</strong> prostagl<strong>and</strong>in E 2 . The migration of<br />
activated neutrophils into <strong>the</strong> <strong>kidney</strong> in <strong>the</strong> setting of up-regulation of adhesion<br />
molecule expression by activated endo<strong>the</strong>lial cells leads to fur<strong>the</strong>r endo<strong>the</strong>lial<br />
damage <strong>and</strong> is likely a seminal event in <strong>the</strong> pathogenesis of ARF. Ischemic<br />
animal models of ARF demonstrate a protective effect of monoclonal antibodies<br />
to adhesion molecules [22].
216<br />
klenzak & himmelfarb<br />
Local soluble mediators<br />
Cellular <strong>and</strong> humoral cytokines are integral to organ dysfunction in <strong>sepsis</strong><br />
syndromes, with <strong>the</strong> <strong>kidney</strong> being especially vulnerable to cytokine-mediated<br />
injury. CD14 is expressed by mesangial cells <strong>and</strong> can be stimulated directly by<br />
LPS. The mesangial cells are capable of expressing multiple proinflammatory<br />
cytokines <strong>and</strong> chemokines, IL-1, IL-6, TNF, <strong>and</strong> PAF. Tubular cells are also<br />
capable of releasing proinflammatory cytokines after stimulation by LPS [23].<br />
Studies of isolated <strong>kidney</strong>s perfused ex vivo with LPS do not demonstrate<br />
a decrease in glomerular filtration rate despite increased mRNA expression for<br />
proinflammatory cytokines. In vivo experiments involving LPS stimulation<br />
demonstrate <strong>the</strong> expected renal dysfunction, however, suggesting that <strong>the</strong> ARF in<br />
this setting is caused by host factors outside <strong>the</strong> renal parenchyma [24,25].<br />
Specific mediators of vascular resistance <strong>and</strong> endo<strong>the</strong>lial injury whose expression<br />
is induced by LPS in vivo include PAF, endo<strong>the</strong>lin-1, <strong>and</strong> iNOS. Each of <strong>the</strong>se<br />
soluble proteins has been shown to decrease glomerular filtration rate <strong>and</strong> RBF,<br />
leading to decreased urine output. Animal studies using antagonists to each of<br />
<strong>the</strong>se soluble mediators have demonstrated amelioration of <strong>the</strong> renal injury<br />
[15,19,26].<br />
PAF is a vasoconstrictor that additionally is chemotactic for activated<br />
inflammatory cells, including neutrophils. It can be produced by glomerular<br />
cells <strong>and</strong> by circulating inflammatory cells, such as neutrophils <strong>and</strong> macrophages.<br />
Increases in PAF lead to a reduction in glomerular filtration rate. Blockade of<br />
PAF receptors lessens <strong>the</strong> deterioration of renal function in models of endotoxemia<br />
[26].<br />
Oxidative stress<br />
It has recently been demonstrated that <strong>the</strong>re are high levels of oxidative stress<br />
in patients with ARF in <strong>the</strong> setting of critical illness. These patients demonstrated<br />
diminished thiol content <strong>and</strong> increased carbonyl content in plasma proteins. The<br />
excess burden of protein oxidation is significantly greater in patients with ARF as<br />
compared with critically ill patients with preserved renal function or patients with<br />
dialysis-dependent chronic <strong>kidney</strong> disease. The levels of protein oxidation are<br />
improved by dialysis, but only transiently, <strong>and</strong> oxidized proteins continue to<br />
accumulate during <strong>the</strong> intradialytic period [27]. The oxidative burden in patients<br />
who have ARF in <strong>the</strong> setting of critical illness may be a target for potential<br />
<strong>the</strong>rapies to decrease <strong>the</strong>ir excess mortality.<br />
Endo<strong>the</strong>lium<br />
Endo<strong>the</strong>lial activation induced by circulating cytokines <strong>and</strong> activated complement<br />
is likely a key instigator in <strong>the</strong> evolution of <strong>sepsis</strong>-associated ARF.<br />
The changes induced in endo<strong>the</strong>lial function by this stimulation enhance <strong>the</strong>
inflammatory process by increasing <strong>the</strong> production of inflammatory mediators.<br />
Endo<strong>the</strong>lial activation is an early host response to circulating pathogens, <strong>and</strong><br />
likely is triggered by activated <strong>and</strong> adherent neutrophils <strong>and</strong> <strong>the</strong>ir degradation<br />
products. The release of cytokines from <strong>the</strong> activated endo<strong>the</strong>lium may be an<br />
early <strong>and</strong> aggressive defense. The dysfunctional endo<strong>the</strong>lium is more severely<br />
damaged <strong>and</strong> results in <strong>the</strong> leaky capillaries associated with <strong>sepsis</strong>. The process<br />
by which endo<strong>the</strong>lium evolves from activated <strong>and</strong> physiologic to damaged <strong>and</strong><br />
dysfunctional is relatively unknown <strong>and</strong> represents a key area for research <strong>and</strong> a<br />
potential target for <strong>the</strong>rapy.<br />
Coagulation cascade<br />
<strong>sepsis</strong> <strong>and</strong> <strong>the</strong> <strong>kidney</strong> 217<br />
The activation of coagulation <strong>and</strong> deposition of fibrin in <strong>the</strong> tissues is a welldefined<br />
component of <strong>the</strong> MOSF in <strong>sepsis</strong>. Increased expression of tissue factor<br />
in response to LPS <strong>and</strong> TNF stimulation of inflammatory <strong>and</strong> endo<strong>the</strong>lial cells<br />
may contribute to organ injury in <strong>sepsis</strong>, including renal injury. Tissue factor<br />
binds activated factor VII. This complex activates factor X, which cleaves<br />
prothrombin to thrombin, which in turn cleaves fibrinogen to fibrin. The activation<br />
of <strong>the</strong> coagulation cascade increases <strong>the</strong> tissue inflammatory response. Fibrin<br />
is often deposited in <strong>the</strong> intravascular space in animal models of <strong>sepsis</strong>, including<br />
<strong>the</strong> glomerular capillaries. For <strong>the</strong>se reasons, anticoagulant <strong>the</strong>rapies, or <strong>the</strong>rapies<br />
that interfere with initiation of coagulation, are of potential interest in ameliorating<br />
MOSF, including renal failure. In a primate model of <strong>sepsis</strong>, animals were<br />
treated with site-inactivated factor VIIa, which serves as a competitive inhibitor<br />
of tissue factor, to block <strong>the</strong> initiation of <strong>the</strong> coagulation cascade. The treated<br />
animals showed preserved renal function at 48 hours, less metabolic acidosis, <strong>and</strong><br />
better urine output. Histologic examination of <strong>the</strong> <strong>kidney</strong>s demonstrated less<br />
tubular injury, inflammatory cell infiltration, <strong>and</strong> fewer fibrin clots than in untreated<br />
animals [28]. Activated protein C improves outcomes in <strong>sepsis</strong>, <strong>and</strong> it is<br />
currently unclear whe<strong>the</strong>r it also attenuates <strong>sepsis</strong>-associated ARF [29].<br />
Management of <strong>sepsis</strong>-associated acute renal failure<br />
Renal replacement <strong>the</strong>rapy<br />
The introduction of hemodialysis for <strong>the</strong> treatment of severe ARF lowered <strong>the</strong><br />
mortality rate from greater than 90% to approximately 50%. The widespread<br />
availability of continuous renal replacement <strong>the</strong>rapies (CRRT) has led to a<br />
growing interest in its use for <strong>the</strong> possible removal of proinflammatory cytokines<br />
in <strong>sepsis</strong>, in addition to its use in volume <strong>and</strong> urea clearance. The use of CRRT<br />
is favored in patients with pressor-dependence because of its better hemodynamic<br />
tolerability than intermittent hemodialysis. Additionally, CRRT offers<br />
potentially improved adequacy through clearance of solute. After intermittent
218<br />
klenzak & himmelfarb<br />
hemodialysis, <strong>the</strong>re is a rebound effect on solutes that are intracellular or o<strong>the</strong>rwise<br />
sequestered. The continuous aspect of CRRT allows for a more physiologic<br />
<strong>and</strong> consistent clearance, without rebound effects. Delivered dose of RRT may<br />
have an impact on survival. In a study of three dose levels, indicated by differing<br />
filtration rates, a survival benefit was demonstrated for patients receiving<br />
<strong>the</strong> most ultrafiltration by continuous venovenous hemofiltration (CVVH).<br />
This study compared prescribed doses of 20, 35, <strong>and</strong> 45 mL/h/kg. The survival<br />
rates were 41%, 57%, <strong>and</strong> 58%, respectively. In this study, patients with <strong>sepsis</strong><br />
demonstrated more survival benefit than o<strong>the</strong>r critically ill patients with <strong>the</strong><br />
increase in dialysis dose from 35 to 45 mL/h/kg [30].<br />
This finding increased interest in using high-volume hemofiltration, or<br />
ultrafiltration beyond 3000 mL/h, in <strong>the</strong> treatment of <strong>sepsis</strong>-associated ARF.<br />
Animal models demonstrated survival <strong>and</strong> hemodynamic benefits for highvolume<br />
hemofiltration in endotoxemia. Fur<strong>the</strong>rmore, increases in ultrafiltration<br />
rate increase convective clearance, <strong>and</strong> increase clearance of middle molecules,<br />
which include most soluble mediators of <strong>sepsis</strong>. Controlled trials in patients have<br />
failed, however, to demonstrate a significant clearance of soluble cytokines in<br />
RRT. Specifically, a r<strong>and</strong>omized controlled trial of patients with <strong>sepsis</strong> <strong>and</strong><br />
preserved renal function allocated to ei<strong>the</strong>r CVVH at 2 L/h or no hemofiltration<br />
demonstrated no difference in circulating cytokines or anaphylatoxins. CVVH<br />
in this setting did not improve clinical indicators, such as oxygenation, or <strong>the</strong><br />
duration of pressor support [31]. Additionally, a study of patients with <strong>sepsis</strong>associated<br />
ARF undergoing CVVH demonstrated no changes in circulating IL-6<br />
or TNF levels. There was clearance of IL-6, demonstrated by its presence in <strong>the</strong><br />
ultrafiltrate, but <strong>the</strong> plasma levels remained stable [32].<br />
To pursue middle molecule clearance, high-permeability membranes were developed<br />
to provide better diffusive clearance for soluble mediators of inflammation<br />
through increased pore size. The inflammatory dysregulation in systemic<br />
inflammatory response syndrome is characterized by a decreased proliferative<br />
capacity <strong>and</strong> hyporesponsiveness of peripheral blood mononuclear cells. Studies<br />
of patients with <strong>sepsis</strong>-associated ARF have demonstrated an improvement in<br />
<strong>the</strong>se circulating cells’ ability to respond ex vivo to stimuli after treatment with<br />
high-flux CRRT. Studies comparing high-flux with conventional CRRT have<br />
demonstrated restoration of <strong>the</strong> normal responsiveness to stimulation with anti-<br />
CD3 antibodies or endotoxin [33,34]. Morgera et al [33] additionally incubated<br />
peripheral blood mononuclear cells from healthy volunteers with <strong>the</strong> ultrafiltrate<br />
of septic patients <strong>and</strong> demonstrated <strong>the</strong> hyporesponsiveness characteristic of<br />
MOSF. There is likely a circulating suppressor of monocyte function.<br />
Plasmapheresis <strong>and</strong> adsorption<br />
Concurrent with interest in high-dose CRRT, it was postulated that normal<br />
inflammatory <strong>and</strong> anti-inflammatory balance could be restored with <strong>the</strong> use of<br />
o<strong>the</strong>r blood purification techniques, including plasmapheresis or plasma exchange,<br />
or adsorption techniques, in addition to RRT. A pilot study of adjunctive
treatment of 25 patients with plasma exchange in <strong>the</strong> setting of <strong>sepsis</strong>-associated<br />
MOSF, including renal failure, demonstrated a survival of 80%, higher than is<br />
expected [35]. O<strong>the</strong>r studies have shown survival rates of 0% to 100%. A larger<br />
trial that included 106 patients r<strong>and</strong>omized to receive plasma exchange or<br />
conventional treatment showed a mortality rate of 33.3% in <strong>the</strong> treated group<br />
versus 53.8% in <strong>the</strong> control group (P = .04). This study only included 19 patients<br />
who developed MOSF, however, 13 of whom were r<strong>and</strong>omized to <strong>the</strong> control<br />
group [36]. Theoretically, not only <strong>the</strong> removal of <strong>the</strong> dysregulated cytokines <strong>and</strong><br />
anaphylatoxins, including endotoxin, TNF, IL-6, IL-10, <strong>and</strong> PAI, but also <strong>the</strong><br />
removal of cellular debris, lysosomal enzymes, proteases, activated complement,<br />
<strong>and</strong> coagulation components, could be beneficial. Additionally, in plasma exchange,<br />
<strong>the</strong> reconstitution with healthy plasma components may also help restore<br />
<strong>the</strong> normal balance between proinflammatory <strong>and</strong> anti-inflammatory cytokines.<br />
A more selective approach to <strong>the</strong> removal of harmful solutes in <strong>the</strong> plasma is<br />
<strong>the</strong> use of adsorbent technology. In this type of purification, <strong>the</strong> plasma is filtered<br />
through a column containing polymyxin B beads, which preferentially bind<br />
toxins <strong>and</strong> have been shown to decrease plasma levels of TNF. In a prospective<br />
pilot trial of 10 patients r<strong>and</strong>omized to ei<strong>the</strong>r 10 hours of plasma filtration<br />
adsorption with hemodialysis or continuous venovenous hemodiafiltration<br />
(CVVHDF), <strong>the</strong> investigators found that adsorption <strong>the</strong>rapy increased monocyte<br />
responsiveness, as measured by LPS stimulation [37].<br />
Bioartificial <strong>kidney</strong><br />
<strong>sepsis</strong> <strong>and</strong> <strong>the</strong> <strong>kidney</strong> 219<br />
A newer RRT being developed is <strong>the</strong> renal tubule-assist device. In animal<br />
models of septic shock, Fissell et al [38] demonstrated superior hemodynamics,<br />
cytokine profiles, <strong>and</strong> outcomes using <strong>the</strong> bioartificial <strong>kidney</strong>, which is<br />
hemofiltration in series with <strong>the</strong> renal tubule-assist device. The renal tubule-assist<br />
device is created by growing porcine renal tubular cells in confluent monolayers<br />
along <strong>the</strong> inner surface of <strong>the</strong> fibers in a st<strong>and</strong>ard hemofiltration cartridge. In<br />
<strong>the</strong>ory, replacement of dialytic clearance with metabolically active tubular cells<br />
may provide a more physiologic metabolic milieu, possibly attenuating <strong>the</strong><br />
course of MOSF. In an animal model of <strong>sepsis</strong>-associated ARF, which consisted<br />
of dogs with bilateral nephrectomies followed by intraperitoneal administration<br />
of Escherichia coli, <strong>the</strong> animals received ei<strong>the</strong>r renal tubule-assist device <strong>the</strong>rapy,<br />
or a sham renal tubule-assist device treatment (blood was hemofiltered, but<br />
without <strong>the</strong> tubular cell column). The renal tubule-assist device–treated dogs<br />
survived significantly longer <strong>and</strong> demonstrated improved hemodynamics. They<br />
had significantly higher TNF <strong>and</strong> IL-10 plasma levels, <strong>and</strong> better electrolyte<br />
homeostasis. The investigators also measured 1,25-(OH) 2 vitamin D 3 levels, <strong>and</strong><br />
found that <strong>the</strong> sham renal tubule-assist device–treated dogs continued to show<br />
decline in plasma levels, whereas <strong>the</strong> renal tubule-assist device–treated group<br />
stabilized to pretreatment levels, demonstrating this metabolic activity in <strong>the</strong> renal<br />
tubule-assist device column [38]. In ano<strong>the</strong>r experimental model, <strong>the</strong> dogs were<br />
nephrectomized, stabilized on CRRT with renal tubule-assist device or without
220<br />
klenzak & himmelfarb<br />
renal tubule-assist device, <strong>and</strong> <strong>the</strong>n infused with endotoxin. Again, IL-10 levels<br />
were higher in <strong>the</strong> renal tubule-assist device–treated group, as was mean arterial<br />
pressure. Survival data were not published [39]. To assess whe<strong>the</strong>r <strong>the</strong> renal<br />
tubule-assist device ameliorates <strong>the</strong> course of <strong>sepsis</strong> before renal failure, <strong>the</strong><br />
investigators assessed it in pigs administered E. coli intraperitoneally, which were<br />
immediately started on CVVHF with or without renal tubule-assist device. All of<br />
<strong>the</strong> animals developed ARF within hours. This study demonstrated a significant<br />
increase in survival time, associated with better systemic hemodynamic<br />
measurements <strong>and</strong> renal artery blood flow. IL-6 <strong>and</strong> interferon-g levels were<br />
lower in renal tubule-assist device–treated animals, but most cytokines measured<br />
did not demonstrate significant differences between renal tubule-assist device <strong>and</strong><br />
sham-treated animals [40].<br />
Summary<br />
When renal failure occurs, <strong>the</strong> systemic <strong>and</strong> local dysregulation of <strong>sepsis</strong> is<br />
compounded by loss of metabolic, fluid, <strong>and</strong> electrolyte homeostasis. The loss of<br />
renal function increases mortality, <strong>and</strong> those who do survive likely do so with <strong>the</strong><br />
return of renal function. The interplay between systemic host responses <strong>and</strong> local<br />
injury <strong>and</strong> activity in <strong>the</strong> <strong>kidney</strong> affects <strong>the</strong> vascular bed, <strong>the</strong> immune system, <strong>and</strong><br />
plays a role in <strong>the</strong> development of MOSF. Patients with end-stage renal disease<br />
<strong>and</strong> <strong>sepsis</strong> have a lower mortality rate than those who develop ARF in <strong>the</strong> setting<br />
of <strong>sepsis</strong>. Despite advances in RRT <strong>and</strong> critical care, mortality rates have<br />
remained fairly stable over <strong>the</strong> last two decades for <strong>sepsis</strong>-associated ARF. There<br />
is little conclusive evidence from human trials of great benefit from <strong>the</strong> myriad of<br />
original <strong>the</strong>rapies tested to date.<br />
For <strong>the</strong>se reasons, it is important to learn more about <strong>the</strong> human response to<br />
<strong>sepsis</strong> <strong>and</strong> ARF, <strong>and</strong> to clarify <strong>the</strong> differences between patients who develop renal<br />
failure <strong>and</strong> those who do not; <strong>and</strong> to clarify <strong>the</strong> differences between those who<br />
survive, <strong>and</strong> those who do not. It is <strong>the</strong>se variables, in <strong>the</strong> ICU, which may serve<br />
to aid in designing rational <strong>the</strong>rapies for <strong>the</strong> restoration of metabolic balance <strong>and</strong><br />
<strong>the</strong> return of renal function.<br />
References<br />
[1] Rangel-Frausto MS, Pittet D, Costigan M, et al. The natural history of <strong>the</strong> systemic inflammatory<br />
response syndrome (SIRS): a prospective study. JAMA 1995;273:117–23.<br />
[2] Clermont G, Acker CG, Angus DC, et al. Renal failure in <strong>the</strong> ICU: comparison of <strong>the</strong> impact<br />
of acute renal failure <strong>and</strong> end-stage renal disease on ICU outcomes. Kidney Int 2002;62:986–96.<br />
[3] Lugon JR, Boim MA, Ramos OL, et al. Renal function <strong>and</strong> glomerular hemodynamics in<br />
male endotoxemic rats. Kidney Int 1989;36:570–5.<br />
[4] Kashgarian M, Siegel NJ, Ries AL, et al. Hemodynamic aspects in development <strong>and</strong> recovery<br />
phases of experimental postischemic acute renal failure. Kidney Int Suppl 1976;6:S160–8.
<strong>sepsis</strong> <strong>and</strong> <strong>the</strong> <strong>kidney</strong> 221<br />
[5] Mason J, Torhorst J, Welsch J. Role of <strong>the</strong> medullary perfusion defect in <strong>the</strong> pathogenesis<br />
of ischemic renal failure. Kidney Int 1984;26:283–93.<br />
[6] Wan L, Bellomo R, Di GD, et al. The pathogenesis of septic acute renal failure. Curr Opin Crit<br />
Care 2003;9:496–502.<br />
[7] Schaer GL, Fink MP, Parrillo JE. Norepinephrine alone versus norepinephrine plus low-dose<br />
dopamine: enhanced renal blood flow with combination pressor <strong>the</strong>rapy. Crit Care Med 1985;<br />
13:492–6.<br />
[8] Anderson WP, Korner PI, Selig SE. Mechanisms involved in <strong>the</strong> renal responses to intravenous<br />
<strong>and</strong> renal artery infusions of noradrenaline in conscious dogs. J Physiol 1981;32:121–30.<br />
[9] Korner PI, Stokes GS, White SW, et al. Role of <strong>the</strong> autonomic nervous system in <strong>the</strong> renal<br />
vasoconstriction response to hemorrhage in <strong>the</strong> rabbit. Circ Res 1967;20:676–85.<br />
[10] Zhang H, Smail N, Cabral A, et al. Effects of norepinephrine on regional blood flow <strong>and</strong> oxygen<br />
extraction capabilities during endotoxic shock. Am J Respir Crit Care Med 1997;155:1965 –71.<br />
[11] Bersten AD, Rutten AJ. Renovascular interaction of epinephrine, dopamine, <strong>and</strong> intraperitoneal<br />
<strong>sepsis</strong>. Crit Care Med 1995;23:537– 44.<br />
[12] Bersten AD, Rutten AJ, Summersides G, et al. Epinephrine infusion in sheep: systemic <strong>and</strong> renal<br />
hemodynamic effects. Crit Care Med 1994;22:994–1001.<br />
[13] Di GD, Morimatsu H, May CN, et al. Intrarenal blood flow distribution in hyperdynamic<br />
septic shock: effect of norepinephrine. Crit Care Med 2003;31:2509–13.<br />
[14] Cohen RI, Hassell AM, Marzouk K, et al. Renal effects of nitric oxide in endotoxemia.<br />
Am J Respir Crit Care Med 2001;164(10 Pt 1):1890–5.<br />
[15] Spain DA, Wilson MA, Garrison RN. Nitric oxide synthase inhibition exacerbates <strong>sepsis</strong>induced<br />
renal hypoperfusion. Surgery 1994;116:322–30.<br />
[16] Knotek M, Esson M, Gengaro P, et al. Desensitization of soluble guanylate cyclase in renal<br />
cortex during endotoxemia in mice. J Am Soc Nephrol 2000;11:2133–7.<br />
[17] Zimmerman GA, Prescott SM, McIntyre TM. Endo<strong>the</strong>lial cell interactions with granulocytes:<br />
te<strong>the</strong>ring <strong>and</strong> signaling molecules. Immunol Today 1992;13:93 – 100.<br />
[18] Shimizu T, Kuroda T, Ikeda M, et al. Potential contribution of endo<strong>the</strong>lin to renal abnormalities<br />
in glycerol-induced acute renal failure in rats. J Pharmacol Exp Ther 1998;286:977–83.<br />
[19] Forbes JM, Hewitson TD, Becker GJ, et al. Simultaneous blockade of endo<strong>the</strong>lin A <strong>and</strong> B<br />
receptors in ischemic acute renal failure is detrimental to long-term <strong>kidney</strong> function. Kidney Int<br />
2001;59:1333– 41.<br />
[20] Thijs A, Thijs LG. Pathogenesis of renal failure in <strong>sepsis</strong>. Kidney Int Suppl 1998;66:S34–7.<br />
[21] Kohan DE. Role of endo<strong>the</strong>lin <strong>and</strong> tumour necrosis factor in <strong>the</strong> renal response to <strong>sepsis</strong>.<br />
Nephrol Dial Transplant 1994;9(Suppl 4):73–7.<br />
[22] Linas SL, Whittenburg D, Parsons PE, et al. Ischemia increases neutrophil retention <strong>and</strong> worsens<br />
acute renal failure: role of oxygen metabolites <strong>and</strong> ICAM 1. Kidney Int 1995;48:1584–91.<br />
[23] Camussi G, Ronco C, Montrucchio G, et al. Role of soluble mediators in <strong>sepsis</strong> <strong>and</strong> renal failure.<br />
Kidney Int Suppl 1998;66:S38– 42.<br />
[24] Xia Y, Feng L, Yoshimura T, et al. LPS-induced MCP-1, IL-1 beta, <strong>and</strong> TNF-alpha mRNA<br />
expression in isolated erythrocyte-perfused rat <strong>kidney</strong>. Am J Physiol 1993;264(5 Pt 2):F774–80.<br />
[25] Linas SL, Whittenburg D, Repine JE. Role of neutrophil derived oxidants <strong>and</strong> elastase in<br />
lipopolysaccharide-mediated renal injury. Kidney Int 1991;39:618–23.<br />
[26] Wang J, Dunn MJ. Platelet-activating factor mediates endotoxin-induced acute renal<br />
insufficiency in rats. Am J Physiol 1987;253(6 Pt 2):F1283–9.<br />
[27] Himmelfarb J, McMonagle E, Freedman S, et al. Oxidative stress is increased in critically ill<br />
patients with acute renal failure. J Am Soc Nephrol 2004;15:2449–56.<br />
[28] Carraway MS, Welty-Wolf KE, Miller DL, et al. Blockade of tissue factor: treatment for organ<br />
injury in established <strong>sepsis</strong>. Am J Respir Crit Care Med 2003;167:1200 – 9.<br />
[29] Bernard GR, Vincent JL, Laterre PF, et al. Efficacy <strong>and</strong> safety of recombinant human activated<br />
protein C for severe <strong>sepsis</strong>. N Engl J Med 2001;344:699–709.<br />
[30] Ronco C, Bellomo R, Homel P, et al. Effects of different doses in continuous veno-venous<br />
haemofiltration on outcomes of acute renal failure: a prospective r<strong>and</strong>omised trial. Lancet 2000;<br />
356:26–30.
222<br />
klenzak & himmelfarb<br />
[31] Cole L, Bellomo R, Hart G, et al. A phase II r<strong>and</strong>omized, controlled trial of continuous<br />
hemofiltration in <strong>sepsis</strong>. Crit Care Med 2002;30:100– 6.<br />
[32] Klouche K, Cavadore P, Portales P, et al. Continuous veno-venous hemofiltration improves<br />
hemodynamics in septic shock with acute renal failure without modifying TNF-alpha <strong>and</strong> IL-6<br />
plasma concentrations. J Nephrol 2002;15:150–7.<br />
[33] Morgera S, Haase M, Rocktaschel J, et al. High permeability haemofiltration improves peripheral<br />
blood mononuclear cell proliferation in septic patients with acute renal failure. Nephrol Dial<br />
Transplant 2003;18:2570–6.<br />
[34] Lonnemann G, Bechstein M, Linnenweber S, et al. Tumor necrosis factor-alpha during<br />
continuous high-flux hemodialysis in <strong>sepsis</strong> with acute renal failure. Kidney Int Suppl 1999;<br />
72:S84–7.<br />
[35] Stegmayr BG. Plasma exchange in patients with septic shock including acute renal failure.<br />
Blood Purif 1996;14:102–8.<br />
[36] Busund R, Koukline V, Utrobin U, et al. Plasmapheresis in severe <strong>sepsis</strong> <strong>and</strong> septic shock:<br />
a prospective, r<strong>and</strong>omised, controlled trial. Intensive Care Med 2002;28:1434–9.<br />
[37] Ronco C, Brendolan A, Lonnemann G, et al. A pilot study of coupled plasma filtration with<br />
adsorption in septic shock. Crit Care Med 2002;30:1250–5.<br />
[38] Fissell WH, Lou L, Abrishami S, et al. Bioartificial <strong>kidney</strong> ameliorates gram-negative bacteriainduced<br />
septic shock in uremic animals. J Am Soc Nephrol 2003;14:454–61.<br />
[39] Fissell WH, Dyke DB, Weitzel WF, et al. Bioartificial <strong>kidney</strong> alters cytokine response <strong>and</strong><br />
hemodynamics in endotoxin-challenged uremic animals. Blood Purif 2002;20:55– 60.<br />
[40] Humes HD, Buffington DA, Lou L, et al. Cell <strong>the</strong>rapy with a tissue-engineered <strong>kidney</strong> reduces<br />
<strong>the</strong> multiple-organ consequences of septic shock. Crit Care Med 2003;31:2421– 8.













