

Left-Sided Portal Hypertension - SASSiT
Left-Sided Portal Hypertension - SASSiT
Left-Sided Portal Hypertension - SASSiT

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Dig Dis Sci (2007) 52:1141–1149<br />
DOI 10.1007/s10620-006-9307-x<br />
REVIEW ARTICLE<br />
<strong>Left</strong>-<strong>Sided</strong> <strong>Portal</strong> <strong>Hypertension</strong><br />
Seyfettin Köklü · Şahin Çoban · Osman Yüksel ·<br />
Mehmet Arhan<br />
Received: 11 December 2005 / Accepted: 6 March 2006 / Published online: 24 March 2007<br />
C○ Springer Science+Business Media, Inc. 2007<br />
Abstract <strong>Left</strong>-sided portal hypertension is a rare clinical<br />
syndrome which may lead to bleeding from isolated gastric<br />
varices. Pancreatic disease is the most common etiology.<br />
<strong>Left</strong>-sided portal hypertension should be considered in the<br />
presence of gastrointestinal bleeding with normal liver function<br />
and unexplained splenomegaly. It may be difficult to<br />
diagnose this entity both endoscopically and radiologically.<br />
While splenectomy is the treatment of choice for cases complicated<br />
by variceal bleeding, there is no consensus on the<br />
treatment of asymptomatic patients. The prognosis of left-<br />
S. Köklü<br />
Department of Gastroenterology, Ankara Education and Research<br />
Hospital,<br />
Ankara, Turkey<br />
Ş. Çoban<br />
Department of Gastroenterology, Ankara University School of<br />
Medicine,<br />
Ankara, Turkey<br />
O. Yüksel<br />
Department of Gastroenterology, Ankara Numune Hospital,<br />
Ankara, Turkey<br />
M. Arhan<br />
Department of Gastroenterology, Ankara Oncology Hospital,<br />
Ankara, Turkey<br />
S. Köklü ()<br />
Karargahtepe mahallesi, Kumrulu sokak,<br />
18/1, 06300, Keçiören, Ankara, Turkey<br />
e-mail: gskoklu@yahoo.com<br />
sided portal hypertension mainly depends on the underlying<br />
etiology.<br />
Keywords <strong>Left</strong>-sided portal hypertension . Splenic vein .<br />
Thrombosis . Obstruction . Splenectomy . Gastrointestinal<br />
bleeding<br />
Incidence<br />
<strong>Left</strong>-sided portal hypertension (LSPH) is a localized form<br />
of portal hypertension that usually occurs as a result of isolated<br />
obstruction of the splenic vein [1, 2]. Obstruction of<br />
the proximal part of the portal vein together with the splenic<br />
vein may also be a rare complication in LSPH. The incidence<br />
of LSPH has increased over the past three decades<br />
due to increased awareness of the entity and advances in diagnostic<br />
approaches. Since most patients are asymptomatic<br />
and experience no complications, its exact incidence is unknown.<br />
However, it accounts for less than 5% of all patients<br />
with portal hypertension [3]. Diagnostic difficulties and lack<br />
of inclusion in the differential diagnosis may partly explain<br />
this low figure. Sutton et al. reviewed the English literature<br />
between 1900 and 1968 and reported 54 cases [4]. Madsen<br />
et al. reviewed the English literature from 1969 to 1984 and<br />
found 209 cases [3]. Since then, case reports and several case<br />
series have been added. To date, approximately 450 cases of<br />
LSPH have been reported in all. Most of the studies in the<br />
literature comprise a limited number of patients and are usually<br />
retrospective [3, 5–9]. In a prospective study performed<br />
by Bernades et al., 266 patients with chronic pancreatitis<br />
(one of the most common causes of LSPH) were screened<br />
with ultrasonography, and angiography or computed tomography<br />
was used to confirm venous obstruction [10]. In<br />
that study, the overall incidence of occlusion of one of the<br />
Springer
1142 Dig Dis Sci (2007) 52:1141–1149<br />
major splanchnic veins was 13%, with the splenic vein being<br />
occluded in 8% of patients, the portal vein in 4%, and the<br />
superior mesenteric vein in 1% [10].<br />
Synonyms<br />
LSPH has also been referred to as segmental [11], sinistral<br />
[7], regional [4], localized [12], compartmental [13], lineal<br />
[14], or splenoportal hypertension [15].<br />
Anatomy<br />
The splenic vein is a large and nontortuous vessel formed<br />
by five or six tributaries from the spleen. It lies inferior to<br />
the splenic artery and, after leaving the splenic hilus, runs<br />
behind the tail and the body of the pancreas. It is approximately<br />
0.5 cm in diameter and 12 cm long. The splenic vein<br />
crosses anterior to the left kidney, being separated from the<br />
left sympathetic trunk and crus by the left renal vessels and<br />
from the abdominal aorta by the superior mesenteric artery<br />
and left renal vein [16]. The tributaries of the splenic vein<br />
include the short gastric, left gastroepiploic, pancreatic, and<br />
inferior mesenteric veins. Behind the neck of the pancreas<br />
the splenic vein joins the superior mesenteric vein to form the<br />
portal vein. Since the splenic vein is contiguous with the<br />
pancreas throughout that organ’s entire length, pancreatic<br />
disorders contribute the main etiology, and any significant<br />
pancreatic pathology may be complicated with venous obstruction<br />
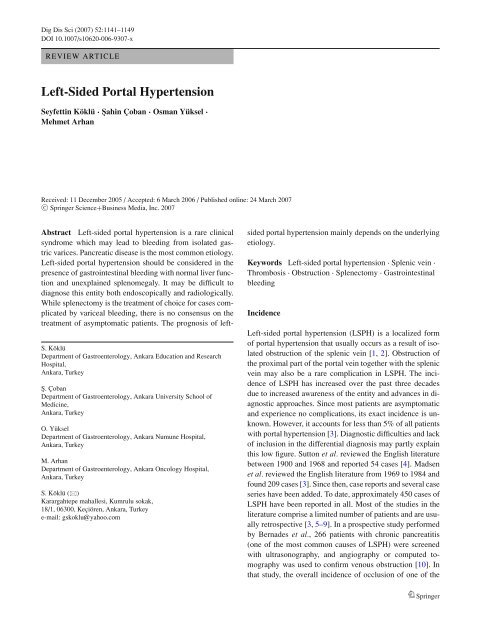
(Fig. 1). There is also close approximation between<br />
the splenic vein and the neighboring pancreatolienal lymph<br />
nodes. Therefore, even retroperitoneal diseases may contribute<br />
to splenic vein occlusion [17–21].<br />
Fig. 1 Illustration of splenic venous thrombosis and fundal varices.<br />
CV, coronary veins; GEV, gastroepiploic vein; PV, portal vein; SV,<br />
splenic vein; SMV, superior mesenteric vein<br />
Pathophysiology<br />
Blood flow through the splenic vein may be blocked secondary<br />
to either thrombosis formation or neighboring mass<br />
effect. Splenic vein occlusion results in venous hypertension<br />
in collateral pathways that carry splenic arterial blood to<br />
the superior mesenteric and portal veins including the short<br />
gastric, coronary, and gastroepiploic veins and the veins located<br />
in the upper half of the stomach. Following obstruction,<br />
splenic blood typically drains through the short gastric veins<br />
to the stomach. In the gastric wall veins of the fundus, blood<br />
flow and pressure increase and submucosal structures consequently<br />
dilate, producing gastric varices. Eventual decompression<br />
into the portal system occurs through the coronary<br />
and epiploic veins. The coronary vein drains to different parts<br />
of the portal system (directly to the portal vein, to the junction<br />
of the splenic and portal veins, and to the splenic vein).<br />
When the coronary vein drains distal to the obstruction in<br />
the splenic vein, esophageal varices may occur alone or in<br />
combination with gastric varices [2, 7, 22]. However, due to<br />
several anatomic variations, obstruction of the splenic vein<br />
may not always result in portal hypertension or formation of<br />
varices.<br />
Etiology<br />
The main cause of LSPH is splenic vein thrombosis (SVT).<br />
Rare causes of LSPH include compression of the splenic<br />
vein by other organs, edema, enlarged lymphadenopathies,<br />
and splenic artery aneurysm. There is a strong association<br />
between pancreatic disorders and SVT because of the splenic<br />
vein’s location. Because the splenic vein is posterior to the<br />
pancreas and in direct contact with it, any type of pancreatic<br />
disease is likely to involve the splenic vein [3, 8, 16].<br />
Acute and chronic pancreatitis and pancreas neoplasms are<br />
the most common causes of SVT [3, 8, 10, 16, 23–26]. In<br />
an early report in 1970, Sutton et al. found that 35% of their<br />
cases of isolated SVT were caused by tumors and only 17%<br />
by pancreatitis [4]. More recent reviews have found acute<br />
or chronic pancreatitis to be the probable cause of isolated<br />
SVT in the majority of cases [2]. In a study by Moosa et al.,<br />
pancreatitis—diagnosed with biopsy or operation—was the<br />
etiology in 87 (60%) of 144 cases, while pancreas malignancy<br />
was detected in only 13 (9%) of the patients [16].<br />
The reason for this difference may be due to increases in the<br />
incidence of pancreatitis and in diagnostic activities, as well<br />
as to improvements in diagnostic procedures [27].<br />
Single episodes of acute pancreatitis may lead to SVT,<br />
and the risk of SVT does not correlate with the severity of<br />
pancreatitis. Also, SVT may occur silently, as a complication<br />
of mild pancreatitis [7, 8].<br />
Springer
Dig Dis Sci (2007) 52:1141–1149 1143<br />
Table 1<br />
Etiologies of splenic vein obstruction<br />
1. Pancreatic diseases<br />
a. Pancreatitis<br />
Acute pancreatitis [3, 16, 23, 34]<br />
Chronic pancreatitis [3, 8, 10, 16, 23, 28]<br />
Familial pancreatitis [16, 29]<br />
Traumatic pancreatitis [13]<br />
b. Pancreas malignancies<br />
Adenocarcinoma [3, 5, 24]<br />
Islet cell carcinoma [30–32]<br />
Cystadenoma [5, 33]<br />
Pancreatic lymphoma [16]<br />
c. Other pancreatic causes<br />
Pancreatic pseudocysts [3, 5, 23, 26, 35]<br />
Pancreatic abscess [1]<br />
Pancreatic divisum [23]<br />
Pancreatic transplantation [16]<br />
Congenital cyst [36]<br />
Pancreatic pseudotumor [37]<br />
2. Nonpancreatic disorders<br />
a. Surgical procedures<br />
Umbilical vein catheterization [38]<br />
Partial gastrectomy [39]<br />
Distal splenorenal shunt [16]<br />
Splenectomy [2, 16]<br />
Selective venous catheterization [16]<br />
b. Metastatic carcinoma<br />
Lymphoma [3, 16]<br />
Oat cell carcinoma [5]<br />
Retroperitoneal liposarcoma [16]<br />
Renal cancer [3, 40]<br />
Gastric cancer [22]<br />
Colon cancer [3, 22]<br />
c. Miscellaneous<br />
Retroperitoneal fibrosis [12]<br />
Splenic artery aneurysms [16]<br />
Gastric ulcer [1]<br />
Hepatoportal sclerosis [22]<br />
Hereditary thrombocytemia [41]<br />
Myeloproliferative disorders [41]<br />
Protein S deficiency [22]<br />
Systemic lupus erythematosus [22]<br />
Renal abscess [17]<br />
Tuberculous adenitis [42]<br />
Retroperitoneal abscess [17, 21]<br />
Benign renal cysts [1]<br />
Various disorders other than pancreatic diseases can cause<br />
isolated SVT. However, they are rare and have a wide spectrum<br />
in terms of their mechanisms of splenic vein obstruction<br />
(Table 1) [1–5, 8, 10, 12, 13, 16, 17, 21–42].<br />
Presenting signs/symptoms<br />
The major clinical consequences of portal hypertension in<br />
general are the formation of gastroesophageal varices, ascites,<br />
and splenomegaly.<br />
Patients with portal hypertension frequently form varices<br />
[43]. When only a segment of the portal venous bed is obstructed,<br />
varices develop only in areas that decompress the<br />
corresponding segment. For example, segmental portal hypertension<br />
within the splenic vein (SVT) is associated with<br />
the formation of isolated gastric varices in the fundus of the<br />
stomach.<br />
Most commonly, LSPH is asymptomatic and is found<br />
incidentally on investigation. In symptomatic cases, the first<br />
clinical manifestation of LSPH is generally acute or chronic<br />
GI bleeding from ruptured esophageal or gastric varices,<br />
and rarely from colonic varices [44]. Usually the bleeding is<br />
serious. Patients may also present with chronic anemia due<br />
to portal hypertensive gastropathy. Gastrointestinal bleeding<br />
is the presenting symptom in 45% [16] to 72% [3] of patients<br />
with LSPH. The number of patients that bleed varies from<br />
series to series (Table 2) [5, 10, 16, 22, 44, 45]. Based on<br />
prospective studies, it appears that most patients with SVT do<br />
not bleed, suggesting that adequate low-pressure collateral<br />
flow develops without the formation of varices.<br />
Splenomegaly is a hallmark of long-standing portal hypertension<br />
and is frequently seen in patients with LSPH. The<br />
degree of splenomegaly in patients with presinusoidal portal<br />
hypertension including isolated SVT is often greater than<br />
in those with cirrhosis [46]. The mechanisms are not fully<br />
understood but are related to increased venous congestion<br />
and splenic arterial flow. Although up to 71% of patients<br />
have splenomegaly, few patients suffer from splenic pain<br />
and develop leukopenia or thrombocytopenia [3].<br />
Abdominal pain without bleeding can be caused in different<br />
patients by a variety of conditions, such as chronic<br />
pancreatitis, pseudocyst, carcinoma, and splenomegaly. It<br />
may be the presenting symptom in 25%–38% of patients<br />
[3, 16, 22].<br />
Patients with LSPH typically do not have significant ascites<br />
unless they develop acute dilutional hypoalbuminemia<br />
during fluid resuscitation for a variceal bleed or have associated<br />
cirrhosis. Therefore, development of ascites is a rare<br />
presenting manifestation in LSPH [47].<br />
Diagnosis<br />
The diagnosis of LSPH is based on clinical, biochemical, and<br />
radiological evaluation. Ultrasonography may show normal<br />
liver architecture. When the diagnosis is in doubt, a liver<br />
biopsy may be performed to rule out cirrhosis.<br />
Esophageal varices can be seen both radiologically and<br />
endoscopically. In contrast, gastric varices are often difficult<br />
to diagnose by either technique. On barium contrast studies,<br />
gastric varices appear as thick and tortuous mucosal folds,<br />
filling defects or distorted mucosal configurations anywhere<br />
along the greater curvature toward the cardia [48]. Although<br />
Springer
1144 Dig Dis Sci (2007) 52:1141–1149<br />
Table 2 The origin of acute<br />
gastrointestinal bleeding in<br />
patients with left-sided portal<br />
hypertension (LSPH)<br />
a For prospective studies.<br />
b Review of the literature.<br />
c Prospective studies.<br />
Number of Acute GI Mean<br />
patients with bleeding due Esophageal Gastric Combined follow-up<br />
Reference LSPH to varices varices varices varices time (mo) a<br />
78<br />
2<br />
2 20<br />
Moosa et al., 73 51 4 38 31<br />
1985 [16] b<br />
Warshaw 8 2 8<br />
et al., 1987<br />
[45]<br />
Bradley 11 2 6<br />
[44] c<br />
et al., 1987<br />
Evans et al., 12 10 10<br />
1990 [5]<br />
Bernades 22 1 100<br />
[10] c<br />
et al., 1992<br />
Sakorafas 34 6 12<br />
et al., 2000<br />
[7]<br />
Heider et al., 53 2 11 30<br />
2004 [23]<br />
Köklü et al., 24 6 21<br />
2005 [22] c<br />
most patients with gastric varices have thickened mucosal<br />
folds in the fundus of the stomach, the abnormality is rarely<br />
specific for the disorder [49]. These findings can be misinterpreted<br />
as gastric carcinoma, lymphoma, multiple polyps,<br />
or Menetrier’s disease [50, 51]. The reported accuracy of<br />
barium contrast studies in patients with proved gastric varices<br />
has ranged from 14% to 74% [52, 53]. Currently, bariumcontrast<br />
examinations are not frequently used because newer<br />
diagnostic techniques are preferred.<br />
Upper gastrointestinal endoscopy can be used to detect<br />
the presence of gastric varices. The endoscopic appearance<br />
of gastric varices varies from clear-cut variceal veins to irregularities<br />
or nodularities in the rugae [54]. If isolated gastric<br />
varices are seen on endoscopy, LSPH should be considered,<br />
and advanced diagnostic studies should be performed<br />
to clarify the diagnosis. As endoscopists have become more<br />
competent, the accuracy of visualizing gastric varices has<br />
increased. In an early series, less than half of the patients<br />
with gastric varices found on splenoportography were diagnosed<br />
correctly by endoscopy [49]. In a more recent study,<br />
gastric varices have been accurately diagnosed and localized<br />
in nearly 90% of cases [55]. A careful examination should<br />
be made to find gastric varices in every patient with gastrointestinal<br />
bleeding of obscure origin, particularly if it is<br />
accompanied by splenomegaly.<br />
Two techniques of angiography are available for diagnosing<br />
LSPH. Splenoportography was popularized by Leger<br />
in 1951 as a method to visualize the portal venous system,<br />
but that procedure is rarely used today because it is invasive<br />
and has potential morbidity, particularly in patients with portal<br />
hypertension [11]. Arteriography is the preferred method<br />
for diagnosis and is a safer and more controlled technique<br />
in patients with a prolonged prothrombin coagulation time<br />
and elevated portal or systemic pressures [56]. Angiography<br />
outlines the location of obstruction and the route of decompression.<br />
Catheterization of the celiac axis provides access to<br />
surrounding arterial structures, including abnormal hepatic<br />
and pancreatic neoplastic vasculature. Subsequently, venous<br />
phase studies can be performed [16]. The portal system is<br />
generally shown clearly; however, arterographic studies often<br />
fail to demonstrate collateral veins that can be seen on<br />
splenoportography [1].<br />
Venous phase angiography accurately shows both the location<br />
of the splenic vein obstruction and collateral flow.<br />
The diagnosis of SVT is confirmed on angiography when<br />
the splenic vein fails to opacify on the venous phase of the<br />
splenic artery injecton. Often venous collaterals in the splenic<br />
hilum and dilated gastroepiploic and short gastric veins are<br />
also seen [26].<br />
Intra-arterial digital substraction angiography (DSA) reliably<br />
shows the portal venous system, collateral circulation,<br />
shunt location and postoperative changes. The major advantage<br />
of intra-arterial DSA is the smaller amount of contrast<br />
medium injected, so that local and systemic side effects<br />
are rare [57]. Other well-known advantages of intra-arterial<br />
DSA are quicker execution, less injury to arteries offered<br />
by smaller-caliber catheters, and low cost. The major disadvantage<br />
of intra-arterial DSA is that the field size of the<br />
intensifier is limited to 6–9 in.<br />
Springer
Dig Dis Sci (2007) 52:1141–1149 1145<br />
Ultrasonography (US) is often used as a preliminary, noninvasive<br />
test for LSPH. US is the least invasive of all available<br />
tests. The accuracy of US in the diagnosis of SVT, versus in<br />
the diagnosis of portal vein thrombosis, may be limited by the<br />
size and location of the splenic vein [2]. Studies comparing<br />
US with angiography and arterial portography in evaluating<br />
portal vein patency have demonstrated US to be relatively<br />
accurate, with a sensitivity and specificity of 93% and 83%,<br />
respectively [58, 59]. However, US may be less accurate in<br />
assessing splenic vein patency because of the anatomic location<br />
of the splenic vein. In one study, by Alpern et al.,the<br />
direction of flow in the splenic vein was correctly determined<br />
in 9 of 16 patients undergoing duplex US. The study found<br />
that, in some patients with SVT, imaging of collateral vessels<br />
near the splenic hilum could be misinterpreted as the splenic<br />
vein, and that operator experience is paramount [59].<br />
Generally, Doppler ultrasonography is the first imaging<br />
technique used in patients with elevated portal pressure and<br />
is accurate in the assessment of the portal venous system [60,<br />
61]. Noninvasive and relatively inexpensive evaluation can<br />
be achieved with color Doppler US, which shows the portal<br />
vein and provides additional information about velocity<br />
and direction of flow. However, Doppler US is observerdependent<br />
and may be unsuccessful when the acoustic window<br />
is not available for evaluation of the whole portal venous<br />
system [60–62]. In addition, US does not show the overall<br />
anatomic structure that interests the clinician. Therefore, in<br />
patients who are potential candidates for surgery, a more<br />
exact diagnostic method that covers the whole portal venous<br />
system is required, such as magnetic resonance (MR)<br />
angiography [61].<br />
Recently, endoscopic ultrasound (EUS) has been used to<br />
assess the portal vasculature. This method appears to be a<br />
more accurate test than transabdominal US for evaluating<br />
patency of the splenic vein in some reports [63, 64]. As one<br />
of the most sensitive imaging methods for studying the pancreas,<br />
EUS has resulted in an improved ability to diagnose<br />
pancreatic mass lesions and to assess vascular involvement<br />
in pancreatic malignancies [63, 65]. EUS is superior to both<br />
US and computerized tomography (CT) in diagnosing small<br />
pancreatic lesions and assessing vascular invasion, with an<br />
accuracy of 94% and 87%, respectively [63, 65]. EUS is also<br />
useful in diagnosing chronic pancreatitis, with a sensitivity,<br />
specificity, and accuracy of 80%, 86%, and 84%, respectively<br />
[66]. It should be considered when other diagnostic methods<br />
have failed to confirm SVT as a cause of bleeding gastric or<br />
gastroesophageal varices [66]. It should also be considered<br />
in cases of SVT occurring without a history of chronic pancreatitis,<br />
so that pancreatic carcinoma can be investigated<br />
as a potential cause of SVT. Because SVT is generally associated<br />
with pancreatic pathology, EUS may be an ideal<br />
diagnostic method to evaluate the splenic vasculature and<br />
the pancreatic parenchyma. EUS has also been shown to be<br />
useful and highly sensitive in detecting paraesophageal and<br />
gastric varices [67–69, 90–92]. In a study comparing EUS<br />
and CT, the former was found to be more sensitive in detecting<br />
paraesophageal varices [67]. It has also been reported<br />
that EUS is more sensitive than conventional endoscopy in<br />
detecting gastric varices [70, 71].<br />
Contrast-enhanced CT portography can demonstrate the<br />
portal venous system in a short time [72–75]. However, it<br />
uses ionizing radiation and requires a large amount of iodinated<br />
contrast material. Unless multidetector CT is used,<br />
CT portography may also suffer from limited longitudinal<br />
coverage because usually CT provides only axial scan mode<br />
[76].<br />
Magnetic resonance imaging (MRI) is an increasingly<br />
valuable tool for the assessment of the portal venous system<br />
and splenic vasculature. MR angiography with gadopentetate<br />
dimeglumine has been shown to be a very promising noninvasive<br />
method for the assessment of the portal venous system<br />
[77–82]. MR angiography appears to be a more accurate diagnostic<br />
procedure than Doppler sonography and CT [60, 72,<br />
83, 84]. In one study, the splenic vein was not evaluated optimally<br />
due to gastrointestinal gas interfering with Doppler<br />
sonography in four patients; however, on MR portograms the<br />
splenic vein was shown to be normal in three patients and<br />
partially thrombosed in one [85]. Contrast-enhanced MR angiography<br />
has also been increasingly used in patients with<br />
portal hypertension for the diagnosis of patency or thrombosis<br />
of the portal venous system [85–87].<br />
It should be mentioned that thrombosis in the proximal<br />
splenic vein may not be shown even by the diagnostic techniques<br />
discussed here, and so sometimes it can be confirmed<br />
only intraoperatively [17, 26].<br />
Treatment<br />
LSPH is one of the rare curable syndromes causing portal<br />
hypertension [88]. To form a consensus on the treatment of<br />
patients with LSPH, the underlying diseases, the presence<br />
and severity of symptoms, and the general condition of the<br />
patients should be considered.<br />
Bleeding (variceal or nonvariceal) is the most common<br />
manifestation of LSPH [5]. Variceal bleeding may be severe<br />
and life-threatening and can originate from esophageal, gastric,<br />
or even colonic varices [27, 56, 89]. Management should<br />
be directed at the splenic side of the portal circulation because<br />
pressure is increased only on that side [5]. Proximal portal<br />
decompressive procedures (any sort of portosystemic shunt)<br />
are hazardous and do not address the disease process, since<br />
these patients have normal portal pressures and generally<br />
normal hepatic function [5]. Conservative therapy including<br />
balloon tamponade, sclerotherapy, vasoconstrictive therapy,<br />
and band ligation may be performed for bleeding control.<br />
Springer
1146 Dig Dis Sci (2007) 52:1141–1149<br />
Unfortunately, these treatment methods have often failed<br />
[1, 2, 5].<br />
Sclerotherapy is effective in patients with esophageal<br />
varices, but not in those with isolated varices in the fundus or<br />
gastric body [2, 90]. Recurrent bleeding occurs in more than<br />
half of patients who undergo endoscopic sclerosis of fundal<br />
varices [2]. However, current approaches in sclerotherapy<br />
have shown hopeful results. Some studies have demonstrated<br />
that endoscopic injection of cyanoacrylate is an effective and<br />
safe treatment for gastric variceal bleeding and obliteration<br />
of gastric varices, especially for the localized types [91–94].<br />
Compared with the other sclerotherapy agents, cyanoacrylate<br />
provides better hemostasis and is associated with less bleeding<br />
recurrence and mortality [93, 94]. However, this method<br />
may have life-threatening complications such as hemorrhage<br />
and peripheral embolic events (pulmonary embolism, cerebral<br />
infarction, or portal vein embolism). At present, the risk<br />
of peripheral embolic events limits its use in spite of currently<br />
available cyanoacrylate analogues [91, 95–97].<br />
A patient with active bleeding unresponsive to conservative<br />
management should be operated on quickly [1, 8].<br />
Splenectomy is the treatment of choice [98]. Removal of<br />
the spleen decreases the venous outflow through the collateral<br />
circulation and decompresses the associated varices to<br />
prevent further hemorrhage [16, 27]. In a large splenectomy<br />
series that included patients with isolated SVT, Moossa et al.<br />
reviewed the English literature between 1969 and 1984 and<br />
reported splenectomy in 79 of 144 cases [16]. Postoperative<br />
mortality was 8% and deaths were due to causes other than<br />
bleeding. None of the 73 patients had recurrent bleeding after<br />
splenectomy during the mean follow-up period of 11 months.<br />
In another study, reported by Evans et al., splenectomy was<br />
performed as a primary therapy in 10 patients. Hemorrhage<br />
was effectively controlled in all but one of these patients [5].<br />
Patients with LSPH and no history of bleeding are a problem<br />
in terms of the risk of future bleeding [8]. Recent studies<br />
have focused on investigations of optimal management<br />
for patients with asymptomatic SVT [23]. In a retrospective<br />
study of pancreatitis-induced splenic vein thrombosis, 53<br />
cases were followed up for a median period of 34 months;<br />
of these, 2 needed splenectomy due to variceal bleeding<br />
and 3 had hemorrhage due to nonvariceal sources. Because<br />
of the low incidence of gastric variceal hemorrhage [4%]<br />
and the absence of mortality related to variceal hemorrhage,<br />
the authors suggested that splenectomy not be performed<br />
routinely for these patients [23]. In a retrospective study<br />
done by Sakorafas et al., none of the eight patients with<br />
symptomatic LSPH who underwent splenectomy had recurrent<br />
gastrointestinal bleeding. Splenectomy was performed<br />
for three of the five asymptomatic patients with esophageal<br />
or gastric varices and none of those five patients had gastrointestinal<br />
hemorrhage during follow-up. Twelve of the 21<br />
asymptomatic patients without esophageal or gastric varices<br />
underwent splenectomy. None of those had bleeding; however,<br />
one of the remaining nine patients had bleeding during<br />
follow-up [7]. In our own experience, 6 of 24 patients with<br />
LSPH presented with gastrointestinal bleeding on admission.<br />
Urgent surgery was needed for only one patient who had a severe<br />
variceal hemorrhage. Other patients admitted with gastrointestinal<br />
bleeding did not need invasive treatment. None<br />
of our patients had recurrent bleeding during follow-up [22].<br />
Finally, there is not enough evidence supporting prophylactic<br />
splenectomy in the treatment of asymptomatic patients.<br />
Nonetheless, if abdominal surgery is performed for other<br />
purposes in a patient with known asymptomatic varices, a<br />
splenectomy may be preferred [2, 7].<br />
Transcatheter splenic artery embolization has been suggested<br />
by Jones and associates to produce a “nonsurgical<br />
splenectomy” [99]. It is performed by transcatheter deposition<br />
of gianturco coils, autologous clot, or absorbable gelatin<br />
sponge [6]. Embolization of the splenic artery by selective<br />
catheterization has been tried with varying success and<br />
has not become the preferred approach [27]. However, transcatheter<br />
embolization as a preoperative adjunct to splenectomy<br />
for hypersplenism has been advocated. Perhaps its role<br />
in LSPH should be as the planned first stage of a two-step<br />
therapeutic plan, embolization followed by splenectomy [5,<br />
6, 100]. Adams et al. showed that splenic artery occlusion<br />
during the splenectomy procedure diminished intraoperative<br />
blood loss [6]. However, splenectomy can be performed<br />
with an acceptable blood loss without splenic artery inflow<br />
control in many patients. Nevertheless, patients with LSPH<br />
who require operation for complications of chronic pancreatitis<br />
may benefit from preoperative placement of the splenic<br />
artery balloon catheter [5]. Splenic infarction and abscess<br />
formation may occur after the embolization procedure [99].<br />
Considering these issues, embolization without splenectomy<br />
should be restricted to patients for whom surgery would be<br />
highly risky [5, 16].<br />
Reconstruction of the splenic vein may be an alternative<br />
therapy in selected patients who have peripheral thrombosis<br />
of the splenic vein [101]. However, there are not enough data<br />
to evaluate the utility of that procedure.<br />
Prognosis<br />
The prognosis of LSPH mainly depends on the underlying<br />
disease. The occurrence or recurrence rate of gastrointestinal<br />
bleeding cannot be estimated. Since nearly half of the<br />
patients have an underlying malignancy, especially pancreas<br />
adenocarcinoma, most of those patients have a shorter life<br />
expectancy and the incidence of gastrointestinal bleeding<br />
is very low in that short period. In our recent prospective<br />
study, all but 1 of the 11 patients with malignancy complicated<br />
with LSPH died within a year, and 1 patient had a<br />
Springer
Dig Dis Sci (2007) 52:1141–1149 1147<br />
gastrointestinal hemorrhage before death [22]. None of the<br />
patients with nonmalignant disorders (three and eight patients<br />
with and without splenectomy, respectively) had bleeding<br />
during a mean period of 30 months. Similarly, in another<br />
prospective study none of the 23 patients with splenoportal<br />
vein thrombosis and LSPH (10 without splenectomy and 13<br />
with splenectomy) had digestive tract bleeding during the<br />
30-month follow-up period after diagnosis [10].<br />
Conclusion<br />
LSPH is a clinical syndrome that usually occurs as a result<br />
of isolated SVT, which in turn arises from various etiologies,<br />
mainly pancreatic diseases. LSPH should be considered in<br />
the presence of gastrointestinal bleeding with normal liver<br />
function tests and unexplained splenomegaly. It may be difficult<br />
to diagnose this entity both endoscopically and radiologically.<br />
However, noninvasive techniques including CT<br />
and MR angiography are making the diagnosis easier. Endoscopic<br />
ultrasonography is sensitive in determining isolated<br />
gastric varices and should be considered in highly suspect<br />
patients. Treatment should be directed to the underlying diseases,<br />
and while splenectomy is the treatment of choice for<br />
cases complicated by variceal bleeding, there is no consensus<br />
on the treatment of asymptomatic patients. Recurrent<br />
hemorrhage is not usual and the prognosis mainly depends<br />
on the underlying etiology.<br />
References<br />
1. Glynn MJ (1986) Isolated splenic vein thrombosis. Arch Surg<br />
121:723–725<br />
2. Weber SM, Rikkers LF (2003) Splenic vein thrombosis and<br />
gastrointestinal bleeding in chronic pancreatitis. World J Surg<br />
27:1271–1274<br />
3. Madsen MS, Petersen TH, Sommer H (1986) Segmental portal<br />
hypertension. Ann Surg 204:72–77<br />
4. Sutton JP, Yarborough DY, Richard JT (1970) Isolated splenic<br />
vein occlusion. Review of literature and report of an additional<br />
case. Arch Surg 100:623–626<br />
5. Evans GRD, Yellin AE, Weaver FA, et al. (1990) Sinistral (leftsided)<br />
portal hypertension. Am Surg 56:758–763<br />
6. Adams DB, Mauterer DJ, Vujic IJ, et al. (1990) Preoperative<br />
control of splenic artery inflow in patients with splenic venous<br />
occlusion. South Med J 83:1021–1024<br />
7. Sakorafas GH, Sarr MG, Farley DR, et al. (2000) The significance<br />
of sinistral portal hypertension complicating chronic pancreatitis.<br />
Am J Surg 179:129–133<br />
8. Little AG, Moossa AR (1981) Gastrointestinal hemorrhage from<br />
left-sided portal hypertension. An unappreciated complication of<br />
pancreatitis. Am J Surg 141:153–158<br />
9. Hwang TL, Jan YY, Jeng LB, et al. (1999) The different manifestation<br />
and outcome between pancreatitis and pancreatic malignancy<br />
with left-sided portal hypertension. Int Surg 84:209–212<br />
10. Bernades P, Baetz A, Levy P, et al. (1992) Splenic and portal<br />
venous obstruction in chronic pancreatitis: A prospective<br />
longitudinal study of a medical-surgical series of 266 patients.<br />
Dig Dis Sci 37:340–346<br />
11. Leger L, Lenriot JP, Lemigre G (1968) L’hypertension et la stase<br />
portales sgmentaires dans les pncreatites chronique: A propos de<br />
126 cas examines par spleno-portographie et spleno-manometrie.<br />
J Chir (Paris) 95:599–608<br />
12. Lavender S, Lloyd-Davis RW, Thomas ML (1970) Retroperitoneal<br />
fibrosis causing localized portal hypertension. Br Med J<br />
3:627–628<br />
13. Salam AA, Warren WD, Tyras DH (1973) Splenic vein thrombosis:<br />
A diagnosable and curable form of portal hypertension.<br />
Surgery 74:961–972<br />
14. Rösch W (1974) Isolated gastric varices: a hint of pancreatic<br />
disorders. Endoscopy 6:217–220<br />
15. Itzchak Y, Glickmann MG (1977) Splenic vein thrombosis in<br />
patients with a normal size spleen. Invest Radiol 12:158–163<br />
16. Moossa AR, Gadd MA (1985) Isolated splenic vein thrombosis.<br />
World J Surg 9:384–390<br />
17. KöklüS,Köksal A, Bayram G, et al. (2004) Isolated splenic vein<br />
thrombosis: An unusual cause and review of the literature. Can J<br />
Gastroenterol 19:837–838<br />
18. Salam AA, Warren WD (1974) Anatomic basis of the surgical<br />
treatment of portal hypertension. Surg Clin North Am 54:1247–<br />
1257<br />
19. Brooks DH (1975) Surgery of the spleen. Surg Clin North Am<br />
55:287–301<br />
20. Warshaw AL, McChesney T, Evans GW, et al. (1972) Intrasplenic<br />
dissection by pancreatic pseudocysts. N Engl J Med 287:72–75<br />
21. Nogueira Soriano JM, Diez GF, Pelaez DG, et al. (1991) Segmental<br />
portal hypertension due to a retroperitoneal abscess of<br />
tuberculous etiology. Rev Esp Enferm Dig 79:211–213<br />
22. Köklü S,Yüksel O, Arhan M, et al. (2005) Report of 24 leftsided<br />
portal hypertension cases: a single-center prospective cohort<br />
study. Dig Dis Sci 50:976–982<br />
23. Heider TR, Azeem S, Galanko JA, et al. (2004) The natural history<br />
of pancreatitis-induced splenic vein thrombosis. Ann Surg<br />
239:876–882<br />
24. Manenti A (1981) Splenic vein obstruction secondary to pancreatic<br />
carcinoma. Acta Chir Belg 80:245–248<br />
25. Keith RG, Mustard RA Jr, Saibil EA (1982) Gastric variceal<br />
bleeding due to occlusion of splenic vein in pancreatic disease.<br />
Can J Surg 25:301–304<br />
26. Illig KA, Spitzer RM, Oates TK (1997) Optimal diagnosis of<br />
splenic vein thrombosis. Am Surg 63:1005–1006<br />
27. Lankısch PG (1990) The spleen in inflammatory pancreatic disease.<br />
Gastroenterology 98:509–516<br />
28. Longstreth GF, Newcomer AD, Green PA (1971) Extrahepatic<br />
portal hypertension caused by chronic pancreatitis. Ann Intern<br />
Med 75:903–908<br />
29. McElroy R, Christiansen PA (1972) Hereditary pancreatitis in<br />
a kinship associated with portal vein thrombosis. Am J Med<br />
52:228–241<br />
30. Wolf JH, Long RJ, Miller FJ, et al. (1977) Pancreatic islet cell<br />
tumour presenting as bleeding gastric varices secondary to splenic<br />
vein occlusion. Am J Dig Dis 22:652–655<br />
31. Gallardo-Navarra V, Phillips E, Neyfeld P, et al. (1973) Segmental<br />
portal hypertension and islet cell adenoma of the pancreas. JAMA<br />
226:1466<br />
32. Bok EJ, Cho KJ, Williams DM, et al. (1984) Venous involvement<br />
in islet cell tumours of the pancreas. Am J Roentgenol 142:319–<br />
322<br />
33. Sheers R (1980) A pancreatic cystadenoma complicated by<br />
varices: Case report. Br J Surg 67:144–145<br />
34. Rogers C, Klatt EC (1989) Splenic vein thrombosis in patients<br />
with acute pancreatitis. Int J Pancreatol 5:117–121<br />
Springer
1148 Dig Dis Sci (2007) 52:1141–1149<br />
35. Negus D, Cotton P (1973) Splenic vein thrombosis with pancreatic<br />
pseudocyst. Proc Roy Soc Med 66:649–650<br />
36. Wolloch Y, Chaimoff C, Lubin E, et al. (1974) Splenic vein thrombosis,<br />
segmental portal hypertension and bleeding esophageal<br />
varices produced by a congenital pancreatic cyst. Israel J Med Sci<br />
10:670–673<br />
37. Harnar T, Johansen K, Haskey R, et al. (1982) <strong>Left</strong>-sided portal<br />
hypertension from pancreatic pseudotumor. Am J Gastroenterol<br />
77:639–641<br />
38. Vos LJM, Potocky V, Broker FHL, et al. (1974) Splenic vein<br />
thrombosis with oesophageal varices: A late complication of umbilical<br />
vein catheterization. Ann Surg 180:152–156<br />
39. Honda Y, Ueda M, Kyoi M, et al. (1978) An unusual case of<br />
portosystemic encephalopathy caused by splenic vein occlusion<br />
following gastrectomy. Am J Gastroenterol 69:590–593<br />
40. Koehler RE (1981) Splenic vein obstruction due to metastatic<br />
hypernephroma. Gastrointest Radiol 6:365–370<br />
41. Shaldon S, Sherlock S (1962) <strong>Portal</strong> hypertension in the myeloproliferative<br />
syndrome and the reticuloses. Am J Med 32:758–<br />
764<br />
42. Takeuchi H, Suzuki M, Unno M, et al. (2000) Splenic vein occlusion<br />
secondary to tuberculous lymphadenitis at the splenic hilum.<br />
Surg Today 30:383–385<br />
43. Alam H, Kim D, Provido H, et al. (1997) <strong>Portal</strong> venous thrombosis<br />
in the adult. Surgical implications in an era of dynamic imaging.<br />
Am Surg 63:681–684<br />
44. Bradley EL (1987) The natural history of splenic vein thrombosis<br />
due to chronic pancreatitis: indications for surgery. Int J<br />
Pancreatol 2:87–92<br />
45. Warshaw AL, Jin GL, Ottinger LW (1987) Recognition and clinical<br />
implication of mesenteric and portal vein obstruction in chrnic<br />
pancreatitis. Arch Surg 122:410–415<br />
46. Blendis LM, Banks DC, Ramboer C, et al. (1970) Spleen blood<br />
flow and splanchnic haemodynamics in blood dyscrasia and other<br />
splenomegalies. Clin Sci 38(1):73–84<br />
47. Witte CL, Chung YC, Witte MH, et al. (1969) Observations on<br />
the origin of ascites from experimental extrahepatic portal congestion.<br />
Ann Surg 170:1002–1015<br />
48. Marshall JP, Smith PD, Hoyumpa AM (1977) Gastric varices:<br />
problem in diagnosis. Am J Dig Dis 22:947–955<br />
49. Muhtehaler C, Gerlock AJ, Goncharenko V, et al. (1979) Gastric<br />
varices secondary to splenic vein occlusion: radiographic diagnosis<br />
and clinical significance. Radiology 132:593–598<br />
50. Rice RP, Thompson WM, Keloin FM, et al. (1977) Gastric varices<br />
without esophageal varices: an important pre-endoscopic diagnosis.<br />
JAMA 237:1976–1979<br />
51. Korr S, Wohl GT (1960) Clinical importance of gastric varices.<br />
N Engl J Med 263:665–669<br />
52. Gabrielson N (1971) Diagnosis of gastric varices by conventional<br />
roentgenography as compared with splenoportal phlebography.<br />
Acta Radiol Diagn 11:506–514<br />
53. Cho KJ, Martel W (1978) Recognition of splenic vein occlusion.<br />
Am J Roentgenol 131:439–443<br />
54. Okuda K, Yasumoto M, Goto A, et al. (1973) Endoscopic observations<br />
of gastric varices. Am J Gastroenterol 60:357–365<br />
55. Mathur SK, Dalvi An, Someshwar V, et al. (1990) Endoscopic<br />
and radiological appraisal af gastric varices. Br J Surg 77:432–<br />
435<br />
56. Yale CE, Crummy AB (1971) Splenic vein thrombosis and bleeding<br />
esophageal varices. JAMA 217:317–320<br />
57. Gattoni F, Baldini U, Pozzato C, et al. (1990) Pure and diluted<br />
contrast media in the visualization of the portal venous system<br />
using digital angiography. Radiol Med (Torino) 80:321–324<br />
58. Johansen K, Paun M (1990) ltrasonography of the portal vein.<br />
Surg Clin North Am 70:181–190<br />
59. Alpern MD, Rubin JM, Williams DM (1987) Porta hepatis: duplex<br />
Doppler US with angiographic correlation. Radiology 162:53–56<br />
60. Finn JP, Kane RA, Edelman LJ, et al. (1993) Imaging of the<br />
portal venous system in patients with cirrhosis: MR angiography<br />
vs. duplex Doppler sonography. Am J Roentgenol 161:989–994<br />
61. Naik KS, Ward J, Irving HC, et al. (1997) Comparison of dynamic<br />
contrast-enhanced MRI and Doppler ultrasound in the preoperative<br />
assessment of the portal venous system. Br J Radiol<br />
70:43–49<br />
62. Capasso P, Dondelinger RF (1998) Vascular disorders of the liver.<br />
In: Gazelle GS, Saini S, Mueller PR (eds) Hepatobiliary and<br />
pancreatic radiology: imaging and intervention. 1st ed. Thieme,<br />
New York, pp 294–334<br />
63. Wiersema MJ, Kochman ML, Cramer HM, et al. (1994)<br />
Endosonography-guided real-time fine needle aspiration biopsy.<br />
Gastrointest Endosc 40:700–707<br />
64. Lewis JD, Faigel DO, Morris JB, et al. (1998) Splenic vein thrombosis<br />
secondary to focal pancreatitis diagnosed by endoscopic<br />
sonography. J Clin Gastroenterol 26:54–56<br />
65. Rosch T (1994) Endoscopic ultrasonography in pancreatic cancer.<br />
Endoscopy 26:806–807<br />
66. Wiersema MJ, Hawes RH, Lehman GA, et al. (1993) Prospective<br />
evaluation of endoscopic ultrasonography and endoscopic<br />
retrograde cholangiopancreatography in patients with chronic abdominal<br />
pain of suspected pancreatic origin. Endoscopy 25:555–<br />
564<br />
67. Lo GH, Lai KH,Wang SJ, et al. (1997) Comparison of endoscopic<br />
ultrasound and computed tomogram in the evaluation of<br />
periesophageal varices. J Ultrasound Med 5:83–88<br />
68. Caletti GC, Brocchi E, Baraldini M, et al. (1990) Assessment of<br />
portal hypertension by endoscopic ultrasonography. Gastrointest<br />
Endosc 36:21–27<br />
69. Caletti GC, Brocchi E, Ferrari A, et al. (1992) Value of endoscopic<br />
ultrasonography in the management of portal hypertension. Endoscopy<br />
24:342–346<br />
70. Lo GH, Lai KH, Cheng JS, et al. (1999) Prevalence of paraesophageal<br />
varices and gastric varices in patients achieving variceal<br />
obliteration by banding ligation and by injection sclerotherapy.<br />
Gastrointest Endosc 49:428–436<br />
71. Boustiere C, Dumas O, Jouffre C, et al. (1993) Endoscopic ultrasonography<br />
classification of gastric varices in patients with cirrhosis.<br />
Comparison with endoscopic findings. J Hepatol 19:268–272<br />
72. Gollin G, Ward B, Meier GH, et al. (1994) Central splanchnic<br />
venous thrombosis: often unsuspected, usually uncomplicated. J<br />
Clin Gastroenterol 18:109–113<br />
73. Vogelzang RL, Gore RM, Anschuetz SL, et al. (1988) Thrombosis<br />
of the splanchnic veins: CT diagnosis. AJR Am J Roentgenol<br />
150:93–96<br />
74. Rahmouni A, Mathieu D, Mondher G, et al. (1992) Value of CT<br />
and sonography in the conservative management of acute splenoportal<br />
and superior mesenteric venous thrombosis. Gastrointest<br />
Radiol 17:135–140<br />
75. Mori H, McGrath FP, Malone DE, et al. (1992) The gastrocolic<br />
trunk and its tributaries: CT evaluation. Radiology 182:871–877<br />
76. Finn JP, Edelman RR, Jenkins RL, et al. (1991) Liver transplantation:<br />
MR angiography with surgical validation. Radiology<br />
179:265–269<br />
77. Prince MR (1994) Gadolinium-enhanced MR aortography. Radiology<br />
191:155–164<br />
78. Edelman RR, Zhao B, Liu C, et al. (1989) MR angiography and<br />
dynamic flow evaluation of the portal venous system. AJR Am J<br />
Roentgenol 153:755–760<br />
79. Ward J, Martinez D, Chalmers AG, et al. (1993) Rapid dynamic<br />
contrast-enhanced magnetic resonance imaging of the liver and<br />
portal vein. Br J Radiol 66:214–222<br />
Springer
Dig Dis Sci (2007) 52:1141–1149 1149<br />
80. Hughes LA, Hartnell GG, Finn JP, et al. (1996) Time-of-flight<br />
MR angiography of the portal venous system: value compared<br />
with other imaging procedures. Am J Roentgenol 166:375–378<br />
81. Nghiem HV, Freeny PC, Winter TC III, et al. (1994) Phasecontrast<br />
MR angiography of the portal venous system: preoperative<br />
findings in liver transplant recipients. Am J Roentgenol<br />
163:445–450<br />
82. Johnson C, Ehmann RL, Rakela J, et al. (1991) MR angiography<br />
in portal hypertension: detection of varices and imaging techniques.<br />
J Comput Assist Tomogr 15:578–584<br />
83. Taylor CR, McCauley TR (1992) Magnetic resonance imaging in<br />
the evaluation of the portal venous system. J Clin Gastroenterol<br />
14:268–273<br />
84. Levy HM, Newhause JH (1988) MR imaging of portal vein thrombosis.<br />
Am J Roentgenol 151:283–286<br />
85. Erden A, Erden I, Yağmurlu B, et al. (2003) <strong>Portal</strong> venous system.<br />
Evaluation with contrast-enhanced 3D MR portography. J Clin<br />
Imag 27:101–105<br />
86. Lin J, Zhou KR, Chen ZW, et al. (2003) 3D contrast-enhanced MR<br />
portography and direct X-ray portography: a correlation study.<br />
Eur Radiol 13:1277–1285<br />
87. Kreft B, Strunk H, Flacke S, et al. (2000) Detection of thrombosis<br />
in the portal venous system: comparison of contrast-enhanced MR<br />
angiography with intraarterial digital substraction angiography.<br />
Radiology 216:88–92<br />
88. Babb RR (1976) Splenic vein obstruction: a curable cause of<br />
variceal bleeding. Am J Dig Dis 21:512–513<br />
89. Burbige EJ, Tarder G, Garson S, et al. (1978) Colonic varices.<br />
A complication of pancreatitis with splenic vein thrombosis. Dig<br />
Dis 23:752–755<br />
90. Sarin SK (1997) Long-term follow-up of gastric variceal<br />
schlerotherapy: an eleven-year experience. Gastrointest Endosc<br />
46:8–14<br />
91. Rengstorff DS, Binmoeller KF (2004) A pilot study of 2-octyl<br />
cyanoacrylate injection for treatment of gastric varices in humans.<br />
Gastrointest Endosc 59:553–558<br />
92. Iwase H, Maeda O, Shimada M, et al. (2001) Endoscopic ablation<br />
with cyanoacrylate glue for isolated gastric variceal bleeding.<br />
Gastrointest Endosc 53:585–592<br />
93. Oho K, Iwao T, Sumino M, et al. (1995) Ethanolamine oleate<br />
versus butyl cyanoacrylate for bleeding gastric varices: a nonrandomized<br />
study. Endoscopy 27:349–354<br />
94. Sarin SK, Jain AK, Jain M, et al. (2002) A randomized controlled<br />
trial of cyanoacrylate versus alcohol injection in patient with<br />
isolated fundic varices. Am J Gastroenterol 97:10–15<br />
95. Roesch W, Rexroth G (1989) Pulmonary, cerabral and coronary<br />
emboli during bucrylate injection of bleeding fundic varices. Endoscopy<br />
30:89–90<br />
96. Shim CS, Cho YD, Kim JO, et al. (1996) A case of portal and<br />
splenic vein thrombosis after histoacryl injection therapy in gastric<br />
varices. Endoscopy 28:461<br />
97. Tan YM, Goh KL, Kamarulzaman A, et al. (2002) Multiple systemic<br />
embolism wiyh septicemia after gastric variceal obliteration<br />
with cyanoacrylate. Gastrointest Endosc 55:276–277<br />
98. Thavanathan J, Heughan C, Cummings TM (1992) Splenic vein<br />
thrombosis as a cause of variceal bleeding. Can J Surg 35:649–<br />
652<br />
99. Jones KB, deKoos PT (1984) Postembolization splenic abscess<br />
in a patient with pancreatitis and splenic vein thrombosis. South<br />
Med J 77:390–393<br />
100. Fujitani RM, Johs SM, Cobb SR, et al. (1988) Preoperarative<br />
splenic artery occlusion as an adjunct for high risk splenectomy.<br />
Am Surg 54:602–608<br />
101. Stein M, Link DP (1999) Symtomatic spleno-mesenteric-portal<br />
venous thrombosis: recanalization and reconstriction with endovascular<br />
stents. J Vasc Intervent Radiol 10:363–371<br />
Springer













