CT Protocols: (Brain, ENT, Spine, Vascular) - Department of Radiology
CT Protocols: (Brain, ENT, Spine, Vascular) - Department of Radiology CT Protocols: (Brain, ENT, Spine, Vascular) - Department of Radiology
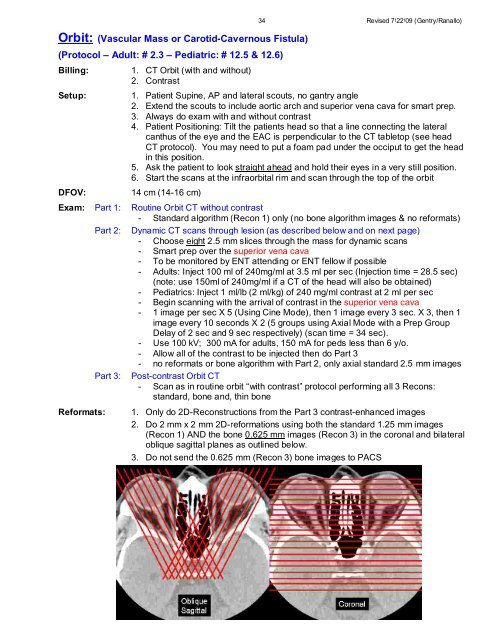
Orbit: (Vascular Mass or Carotid-Cavernous Fistula) (Protocol – Adult: # 2.3 – Pediatric: # 12.5 & 12.6) Billing: Setup: DFOV: Exam: Reformats: Part 1: Part 2: Part 3: 1. CT Orbit (with and without) 2. Contrast 34 Revised 7/22/09 (Gentry/Ranallo) 1. Patient Supine, AP and lateral scouts, no gantry angle 2. Extend the scouts to include aortic arch and superior vena cava for smart prep. 3. Always do exam with and without contrast 4. Patient Positioning: Tilt the patients head so that a line connecting the lateral canthus of the eye and the EAC is perpendicular to the CT tabletop (see head CT protocol). You may need to put a foam pad under the occiput to get the head in this position. 5. Ask the patient to look straight ahead and hold their eyes in a very still position. 6. Start the scans at the infraorbital rim and scan through the top of the orbit 14 cm (14-16 cm) Routine Orbit CT without contrast - Standard algorithm (Recon 1) only (no bone algorithm images & no reformats) Dynamic CT scans through lesion (as described below and on next page) - Choose eight 2.5 mm slices through the mass for dynamic scans - Smart prep over the superior vena cava - To be monitored by ENT attending or ENT fellow if possible - Adults: Inject 100 ml of 240mg/ml at 3.5 ml per sec (Injection time = 28.5 sec) (note: use 150ml of 240mg/ml if a CT of the head will also be obtained) - Pediatrics: Inject 1 ml/lb (2 ml/kg) of 240 mg/ml contrast at 2 ml per sec - Begin scanning with the arrival of contrast in the superior vena cava - 1 image per sec X 5 (Using Cine Mode), then 1 image every 3 sec. X 3, then 1 image every 10 seconds X 2 (5 groups using Axial Mode with a Prep Group Delay of 2 sec and 9 sec respectively) (scan time = 34 sec). - Use 100 kV; 300 mA for adults, 150 mA for peds less than 6 y/o. - Allow all of the contrast to be injected then do Part 3 - no reformats or bone algorithm with Part 2, only axial standard 2.5 mm images Post-contrast Orbit CT - Scan as in routine orbit “with contrast” protocol performing all 3 Recons: standard, bone and, thin bone 1. Only do 2D-Reconstructions from the Part 3 contrast-enhanced images 2. Do 2 mm x 2 mm 2D-reformations using both the standard 1.25 mm images (Recon 1) AND the bone 0.625 mm images (Recon 3) in the coronal and bilateral oblique sagittal planes as outlined below. 3. Do not send the 0.625 mm (Recon 3) bone images to PACS
35 Revised 7/22/09 (Gentry/Ranallo) Scan Factors for Part 2 only: (Adult and Pediatric) Smart Prep Prep Over Superior Vena Cava mA 40 (Adult) 20 (Peds) Monitoring Delay (sec) Monitoring ISD (sec) Enhancement Threshold Diagnostic Delay (sec) 10.0 2.0 50 3.0 Orbit: (Vascular Mass / Carotid-Cavernous Fistula) Adult and Pediatric Contrast (Part 2 Only) CT 1 CT 2 CT 3 CT 4 & ER CT East & RP CT Scanner GE LS Xtra GE LS 16 GE LS 16 Pro GE LS VCT 64 GE LS 8 Scan Type Cine then Axial Cine then Axial Cine then Axial Cine then Axial Cine then Axial Rotation Time (sec) 1.0 1.0 1.0 1.0 1.0 Detector Coverage (mm) 20 20 20 20 20 Slice Thickness (mm) 2.5 2.5 2.5 2.5 2.5 Scan FOV Head Head Head Head Head kV 100 100 100 100 100 mA Adults 380 300 300 300 300 mA Peds < 6 y/o 190 150 150 150 150 Recon 1: DFOV 18 18 18 18 18 Recon Type Standard Standard Standard Standard Standard WW/ WL 350/20 350/20 350/20 350/20 350/20
- Page 1 and 2: Name / MRN: ___________________ / _
- Page 3 and 4: Table of Contents (continued): 3 Re
- Page 5 and 6: 5 Revised 7/22/09 (Gentry/Ranallo)
- Page 7 and 8: 7 Revised 7/22/09 (Gentry/Ranallo)
- Page 9 and 10: 9 Revised 7/22/09 (Gentry/Ranallo)
- Page 11 and 12: Adult Head: (Axial Mode) (Protocol
- Page 13 and 14: 13 Revised 7/22/09 (Gentry/Ranallo)
- Page 15 and 16: 15 Revised 7/22/09 (Gentry/Ranallo)
- Page 17 and 18: 17 Revised 7/22/09 (Gentry/Ranallo)
- Page 19 and 20: 19 Revised 7/22/09 (Gentry/Ranallo)
- Page 21 and 22: 21 Revised 7/22/09 (Gentry/Ranallo)
- Page 23 and 24: 23 Revised 7/22/09 (Gentry/Ranallo)
- Page 25 and 26: 25 Revised 7/22/09 (Gentry/Ranallo)
- Page 27 and 28: 27 Revised 7/22/09 (Gentry/Ranallo)
- Page 29 and 30: 29 Revised 7/22/09 (Gentry/Ranallo)
- Page 31 and 32: 31 Revised 7/22/09 (Gentry/Ranallo)
- Page 33: 33 Revised 7/22/09 (Gentry/Ranallo)
- Page 37 and 38: 37 Revised 7/22/09 (Gentry/Ranallo)
- Page 39 and 40: 39 Revised 7/22/09 (Gentry/Ranallo)
- Page 41 and 42: 41 Revised 7/22/09 (Gentry/Ranallo)
- Page 43 and 44: 43 Revised 7/22/09 (Gentry/Ranallo)
- Page 45 and 46: 45 Revised 7/22/09 (Gentry/Ranallo)
- Page 47 and 48: 47 Revised 7/22/09 (Gentry/Ranallo)
- Page 49 and 50: 49 Revised 7/22/09 (Gentry/Ranallo)
- Page 51 and 52: 51 Revised 7/22/09 (Gentry/Ranallo)
- Page 53 and 54: Sinuses (Diagnostic): (Adult and Pe
- Page 55 and 56: 55 Revised 7/22/09 (Gentry/Ranallo)
- Page 57 and 58: 57 Revised 7/22/09 (Gentry/Ranallo)
- Page 59 and 60: 59 Revised 7/22/09 (Gentry/Ranallo)
- Page 61 and 62: 61 Revised 7/22/09 (Gentry/Ranallo)
- Page 63 and 64: 63 Revised 7/22/09 (Gentry/Ranallo)
- Page 65 and 66: 65 Revised 7/22/09 (Gentry/Ranallo)
- Page 67 and 68: 67 Revised 7/22/09 (Gentry/Ranallo)
- Page 69 and 70: 69 Revised 7/22/09 (Gentry/Ranallo)
- Page 71 and 72: 71 Revised 7/22/09 (Gentry/Ranallo)
- Page 73 and 74: 73 Revised 7/22/09 (Gentry/Ranallo)
- Page 75 and 76: 75 Revised 7/22/09 (Gentry/Ranallo)
- Page 77 and 78: 77 Revised 7/22/09 (Gentry/Ranallo)
- Page 79 and 80: 79 Revised 7/22/09 (Gentry/Ranallo)
- Page 81 and 82: 81 Revised 7/22/09 (Gentry/Ranallo)
- Page 83 and 84: 83 Revised 7/22/09 (Gentry/Ranallo)
Orbit: (<strong>Vascular</strong> Mass or Carotid-Cavernous Fistula)<br />
(Protocol – Adult: # 2.3 – Pediatric: # 12.5 & 12.6)<br />
Billing:<br />
Setup:<br />
DFOV:<br />
Exam:<br />
Reformats:<br />
Part 1:<br />
Part 2:<br />
Part 3:<br />
1. <strong>CT</strong> Orbit (with and without)<br />
2. Contrast<br />
34 Revised 7/22/09 (Gentry/Ranallo)<br />
1. Patient Supine, AP and lateral scouts, no gantry angle<br />
2. Extend the scouts to include aortic arch and superior vena cava for smart prep.<br />
3. Always do exam with and without contrast<br />
4. Patient Positioning: Tilt the patients head so that a line connecting the lateral<br />
canthus <strong>of</strong> the eye and the EAC is perpendicular to the <strong>CT</strong> tabletop (see head<br />
<strong>CT</strong> protocol). You may need to put a foam pad under the occiput to get the head<br />
in this position.<br />
5. Ask the patient to look straight ahead and hold their eyes in a very still position.<br />
6. Start the scans at the infraorbital rim and scan through the top <strong>of</strong> the orbit<br />
14 cm (14-16 cm)<br />
Routine Orbit <strong>CT</strong> without contrast<br />
- Standard algorithm (Recon 1) only (no bone algorithm images & no reformats)<br />
Dynamic <strong>CT</strong> scans through lesion (as described below and on next page)<br />
- Choose eight 2.5 mm slices through the mass for dynamic scans<br />
- Smart prep over the superior vena cava<br />
- To be monitored by <strong>ENT</strong> attending or <strong>ENT</strong> fellow if possible<br />
- Adults: Inject 100 ml <strong>of</strong> 240mg/ml at 3.5 ml per sec (Injection time = 28.5 sec)<br />
(note: use 150ml <strong>of</strong> 240mg/ml if a <strong>CT</strong> <strong>of</strong> the head will also be obtained)<br />
- Pediatrics: Inject 1 ml/lb (2 ml/kg) <strong>of</strong> 240 mg/ml contrast at 2 ml per sec<br />
- Begin scanning with the arrival <strong>of</strong> contrast in the superior vena cava<br />
- 1 image per sec X 5 (Using Cine Mode), then 1 image every 3 sec. X 3, then 1<br />
image every 10 seconds X 2 (5 groups using Axial Mode with a Prep Group<br />
Delay <strong>of</strong> 2 sec and 9 sec respectively) (scan time = 34 sec).<br />
- Use 100 kV; 300 mA for adults, 150 mA for peds less than 6 y/o.<br />
- Allow all <strong>of</strong> the contrast to be injected then do Part 3<br />
- no reformats or bone algorithm with Part 2, only axial standard 2.5 mm images<br />
Post-contrast Orbit <strong>CT</strong><br />
- Scan as in routine orbit “with contrast” protocol performing all 3 Recons:<br />
standard, bone and, thin bone<br />
1. Only do 2D-Reconstructions from the Part 3 contrast-enhanced images<br />
2. Do 2 mm x 2 mm 2D-reformations using both the standard 1.25 mm images<br />
(Recon 1) AND the bone 0.625 mm images (Recon 3) in the coronal and bilateral<br />
oblique sagittal planes as outlined below.<br />
3. Do not send the 0.625 mm (Recon 3) bone images to PACS


