Ankle and Foot 47 - Department of Radiology - University of ...
Ankle and Foot 47 - Department of Radiology - University of ...
Ankle and Foot 47 - Department of Radiology - University of ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
2304 VII Imaging <strong>of</strong> the Musculoskeletal System<br />
B<br />
C<br />
A<br />
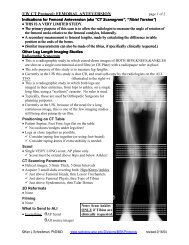
Figure <strong>47</strong>-107. Early Jones fracture in a 21-year-old college athlete. A, On the initial anteroposterior radiograph <strong>of</strong> the base <strong>of</strong> the fifth<br />
metatarsal there is a very subtle periosteal reaction (white arrow). There is a questionable lucency (open arrowheads) extending transversely<br />
through the lateral cortex. B, Far lateral sagittal inversion recovery (IR) image reveals bone marrow edema throughout the fifth metatarsal.<br />
C, Sagittal IR image through the asymptomatic fourth metatarsal for comparison revealed normal dark marrow signal. Because <strong>of</strong> the high<br />
propensity for Jones fractures to have delayed union or nonunion, elective internal fixation with a lag screw was performed the next day.<br />
D, Follow-up anteroposterior radiograph 2 weeks later reveals bone resorption (arrowheads) along the questionable lucency in A, part <strong>of</strong> the<br />
normal early healing response. Subsequent radiographs (not shown) demonstrated solid bony bridging 1 month later.<br />
D<br />
itive stress in athletes, or as in the case <strong>of</strong> Sir Robert Jones,<br />
“whilst dancing.” 25 The Jones fracture is well recognized to<br />
have a high rate <strong>of</strong> nonunion or delayed union because <strong>of</strong><br />
the relative hypovascularity <strong>of</strong> this portion <strong>of</strong> the fifth<br />
metatarsal, prompting orthopedic surgeons to recommend<br />
early screw fixation. MRI is useful in confirming the diagnosis<br />
when it is suspected in athletes with radiographically<br />
occult injuries (Fig. <strong>47</strong>-107).<br />
March Fracture. The march fracture is found most commonly<br />
in the mid- to distal diaphysis <strong>of</strong> the second metatarsal<br />
<strong>and</strong> less <strong>of</strong>ten in the third. Unlike the Jones fracture,<br />
which occurs in high-performance athletes, stress fractures<br />
in the second <strong>and</strong> third metatarsals occur in individuals<br />
who have previously led relatively sedentary lifestyles, then<br />
suddenly increase their level <strong>of</strong> activity. This fracture was<br />
first reported by Breithaupt in 1855, 11 when he described<br />
foot pain <strong>and</strong> swelling in military recruits in the Prussian<br />
army who were forced to go on long marches—hence the<br />
name “march fracture.” This was <strong>of</strong> course 40 years before<br />
Röntgen’s discovery <strong>of</strong> x-rays. The first radiographic reports<br />
<strong>of</strong> march fractures were in 1897.* Radiographically, the<br />
*In his 2006 academic dissertation for the <strong>University</strong> <strong>of</strong> Helsinki, Bone Stress<br />
Injuries <strong>of</strong> the <strong>Foot</strong> <strong>and</strong> <strong>Ankle</strong> (http://ethesis.helsinki.fi/julkaisut/laa/kliin/vk/<br />
sormaala/bonestre.pdf), Sormaala cites these two references:<br />
Schulte: Die sogenannte Fussgeschwulst. Arch Klin Chir 1897;55:872.<br />
Stechow: Fussödem und Röntgenstrahlen. Deutsche Militärärztliche Zeitschrift<br />
1897;26:465-<strong>47</strong>1.<br />
second <strong>and</strong> third metatarsals respond to stress by forming<br />
a periosteal reaction, although this may be imperceptible<br />
or subtle early on (Fig. <strong>47</strong>-108). Edema-sensitive MRI<br />
reveals abnormally bright marrow signal in the diaphysis<br />
as well as bright periosteal reaction outside the cortex.<br />
• Sesamoid Stress Fractures<br />
Sesamoid stress fractures are notoriously difficult to diagnosis<br />
radiographically. Perhaps because <strong>of</strong> their varying<br />
presence <strong>and</strong> appearance, radiologists tend to have a “blind<br />
spot” when it comes to the sesamoids. However, when<br />
looking at the sesamoids <strong>of</strong> the first metatarsophalangeal<br />
joint, there are some helpful statistics to keep in mind.<br />
Although the other sesamoid bones <strong>of</strong> the foot are present<br />
in less than 10% <strong>of</strong> people, the two sesamoids plantar to<br />
the head <strong>of</strong> the first metatarsal are present in 100% <strong>of</strong> the<br />
population. 16 Absence <strong>of</strong> either the medial (tibial) or lateral<br />
(fibular) sesamoids is always abnormal, <strong>and</strong> a destructive<br />
process should be considered (see Fig. <strong>47</strong>-92). And<br />
although a multipartite medial sesamoid bone is a common<br />
normal variant found in 13% to 30% <strong>of</strong> the population, a<br />
multipartite lateral sesamoid bone is an uncommon variant,<br />
found in only 1% <strong>of</strong> normal feet.<br />
When symptoms are referable to the lateral sesamoid<br />
<strong>and</strong> radiographs reveal it to be multipartite, this should be<br />
diagnosed as a fracture (Fig. <strong>47</strong>-109). Additional diagnostic<br />
imaging should not be required, although MRI or a nuclear<br />
Ch0<strong>47</strong>-A05375.indd 2304<br />
9/9/2008 5:36:04 PM