Ankle and Foot 47 - Department of Radiology - University of ...
Ankle and Foot 47 - Department of Radiology - University of ...
Ankle and Foot 47 - Department of Radiology - University of ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
2248 VII Imaging <strong>of</strong> the Musculoskeletal System<br />
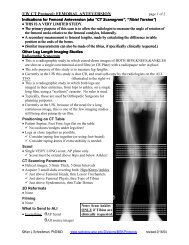
Figure <strong>47</strong>-53. Comparison <strong>of</strong> T2-weighted, fatsuppressed<br />
(A) <strong>and</strong> inversion recovery (B) MRIs in a<br />
35-year-old with plantar fasciitis. Both <strong>of</strong> these sagittal<br />
images <strong>of</strong> the calcaneus delineate the plantar<br />
aponeurosis (open arrowheads), as well as the edema<br />
in the adjacent heel fat pad (white arrowheads) <strong>and</strong> in<br />
the bone marrow at its origin (white arrow).<br />
A<br />
B<br />
Protocols<br />
Our ankle/foot MRI protocols call for acquiring images in<br />
three <strong>of</strong> the st<strong>and</strong>ard planes <strong>and</strong> typically take 45 to 60<br />
minutes. We start with straight sagittal images to survey the<br />
bones. For an ankle MRI, the FOV needs to include the<br />
distal tibia <strong>and</strong> fibula, all <strong>of</strong> the tarsal bones, <strong>and</strong> the bases<br />
<strong>of</strong> the metatarsals. For a foot MRI, the FOV needs to include<br />
all <strong>of</strong> the phalanges, all <strong>of</strong> the metatarsals, <strong>and</strong> the midfoot<br />
tarsal bones back to the Chopart joint. In cases in which<br />
the area <strong>of</strong> clinical concern is vague, the sagittal FOV can<br />
be enlarged to include the ankle <strong>and</strong> forefoot. When they<br />
are available, the radiologist should check these first sets<br />
<strong>of</strong> sagittal survey images, particularly the edema-sensitive<br />
sequence. If the radiologist observes edema in the talar<br />
dome, images can then be acquired in the mortise coronal<br />
<strong>and</strong> mortise sagittal planes (our OLT protocol). If there is<br />
edema elsewhere in the tarsal bones, oblique axial <strong>and</strong><br />
oblique coronal images are acquired (our tarsal stress fracture<br />
protocol). If the marrow edema is in a metatarsal, this<br />
is usually best demonstrated with short- <strong>and</strong> long-axis<br />
images (our metatarsal stress fracture protocol). If no bone<br />
marrow edema is found, we generally proceed with our<br />
tendon protocol (straight axial <strong>and</strong> oblique coronal) unless<br />
some other site is clinically requested.<br />
Sequences<br />
Because detecting abnormally edematous signal in the<br />
bones, tendons, <strong>and</strong> surrounding s<strong>of</strong>t tissues is the key to<br />
all musculoskeletal MRI, we run edema-sensitive sequences<br />
in all the planes we image. This can be either a fatsuppressed<br />
fast-spin echo T2-weighted sequence or an<br />
inversion recovery sequence. Although for the most part<br />
these two sequences are equivalent (Fig. <strong>47</strong>-53), we find<br />
that we get the best images when we use inversion recovery<br />
for the straight sagittal survey plane <strong>and</strong> T2-weighted<br />
sequences in all other planes.<br />
T1-weighted images, being inherently fat sensitive,<br />
well demonstrate the normal fat in yellow bone marrow<br />
as well as the subcutaneus fat <strong>and</strong> the deeper fat between<br />
muscles <strong>and</strong> tendons. We use T1 weighting in all imaging<br />
planes whenever the tendons are not the primary site <strong>of</strong><br />
interest.<br />
When the tendons are the site <strong>of</strong> clinical concern,<br />
we use proton-density–weighted images, along with T2-<br />
weighted sequences, in the straight axial <strong>and</strong> oblique<br />
coronal planes. The straight axial plane well images all 10<br />
<strong>of</strong> the ankle tendons in cross section at <strong>and</strong> above the level<br />
<strong>of</strong> the ankle joint. The oblique coronal plane well images<br />
the medial <strong>and</strong> lateral ankle tendons in cross section as<br />
they curve under the malleoli. Tears in the substance <strong>of</strong> the<br />
ankle tendons are usually best seen with proton-density–<br />
weighted images (Fig. <strong>47</strong>-54). However, because protondensity–weighted<br />
images are relatively insensitive for fluid,<br />
they should always be read side-by-side with edemasensitive<br />
images to look for abnormal amounts <strong>of</strong> fluid in<br />
the tendon sheaths, indicative <strong>of</strong> active tenosynovitis.<br />
• Use <strong>of</strong> Contrast<br />
Although the intravenous administration <strong>of</strong> a gadoliniumbased<br />
contrast agent (IVGd) is not needed for most<br />
musculoskeletal MRI, there are particular circumstances in<br />
which its use is invaluable.*<br />
Whenever possible, we use IVGd when there is a clinical<br />
concern for an inflammatory arthropathy or synovitis,<br />
such as in rheumatoid arthritis (Fig. <strong>47</strong>-55). The IVGd<br />
causes T1 signal enhancement <strong>of</strong> the hypervascularized<br />
inflammatory synovium (pannus) but not <strong>of</strong> the adjacent<br />
synovial fluid, a distinction that may not otherwise be seen<br />
on noncontrast T1-weighted or T2-weighted images.<br />
Likewise, we prefer to use IVGd whenever possible in<br />
cases <strong>of</strong> infection. IVGd can help distinguish an enhancing<br />
phlegmon from a nonenhancing pus pocket. Also, IVGd<br />
can distinguish cellulitis, which demonstrates contrast<br />
enhancement <strong>of</strong> the edematous skin, from “nonspecific<br />
edema from other causes” that does not enhance.<br />
*During the year leading up to the publication <strong>of</strong> this chapter, the U.S. Food<br />
<strong>and</strong> Drug Administration (FDA) has issued warnings describing the risk for nephrogenic<br />
systemic fibrosis (NSF) after exposure to gadolinium-containing contrast<br />
agents in patients with acute or chronic severe renal insufficiency. Information<br />
can be found at http://www.fda.gov/cder/drug/infopage/gcca. Before any contrast<br />
agent is administered to any patient, that patient should be screened in<br />
accordance to your institution’s policies.<br />
Ch0<strong>47</strong>-A05375.indd 2248<br />
9/9/2008 5:34:34 PM