Ankle and Foot 47 - Department of Radiology - University of ...
Ankle and Foot 47 - Department of Radiology - University of ...
Ankle and Foot 47 - Department of Radiology - University of ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>47</strong> <strong>Ankle</strong> <strong>and</strong> <strong>Foot</strong> 2223 <strong>47</strong><br />
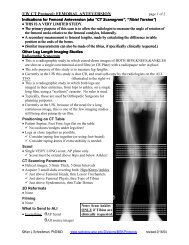
Figure <strong>47</strong>-22. A 57-year-old with<br />
an Achilles tendon that has healed<br />
with chronic scarring. Axial T1-<br />
weighted (A), axial T2-weighted<br />
(B), <strong>and</strong> sagittal T2-weighted (C)<br />
images reveal that the distal<br />
Achilles tendon is too round <strong>and</strong><br />
thick but contains no increased<br />
signal.<br />
A<br />
B<br />
C<br />
The flexor hallucis longus muscle is a posterior structure<br />
originating from the lower two thirds <strong>of</strong> the back <strong>of</strong><br />
the fibula. The musculotendinous junction extends distally<br />
to the level <strong>of</strong> the ankle joint, <strong>and</strong> the proximal end <strong>of</strong> the<br />
tendon passes through a groove along the posterior talus.<br />
Whereas the posterior tibial <strong>and</strong> flexor digitorum longus<br />
tendons pass under the medial malleolus, the flexor hallucis<br />
longus tendon passes under the sustentaculum tali.<br />
The flexor hallucis longus then crosses deep to the flexor<br />
digitorum longus, extends under the first metatarsal, <strong>and</strong><br />
passes between the two great toe sesamoids, to insert on<br />
the plantar base <strong>of</strong> the distal phalanx (see Fig. <strong>47</strong>-9D<br />
<strong>and</strong> E).<br />
A<br />
Medial<br />
malleolus<br />
B<br />
Injury<br />
Of the three medial ankle tendons, the posterior tibial is<br />
the most prone to tear, characteristically along the portion<br />
that curves around the medial malleolus. The posterior<br />
tibial tendon is relatively hypovascular in this region. 39<br />
This region <strong>of</strong> the tendon is also susceptible to mechanical<br />
wear as the tendon rubs against the medial malleolus (Fig.<br />
<strong>47</strong>-23). If the surrounding tendon sheath does not provide<br />
adequate lubrication, such as in stenosing tenosynovitis<br />
or rheumatoid pannus formation, this frictional wear<br />
increases. Perhaps because <strong>of</strong> these longitudinal frictional<br />
stresses, the posterior tibial tendon tends to tear with a<br />
longitudinal split, rather than the transverse rupture seen<br />
in Achilles tendon tears. When imaged in the axial plane,<br />
a longitudinal split in the posterior tibial tendon resembles<br />
two individual tendons. This longitudinally split posterior<br />
tibial tendon, when grouped with the flexor digitorum <strong>and</strong><br />
hallucis longus tendons, has been called the four-tendon<br />
sign (Fig. <strong>47</strong>-24).<br />
Tenosynovitis refers to inflammation between the<br />
tendon <strong>and</strong> the surrounding synovial sheath. This is <strong>of</strong>ten<br />
a chronic irritative process, more commonly affecting<br />
C D E<br />
Figure <strong>47</strong>-23. Illustration <strong>of</strong> posterior tibial tendon mechanical<br />
wear becoming a longitudinal tear. A, Medial view <strong>of</strong> the posterior<br />
tibial tendon (PT; red) as it wraps over the medial malleolus <strong>and</strong><br />
under the flexor digitorum longus tendon (FDL; blue). The PT is<br />
susceptible to mechanical wear as it rubs back <strong>and</strong> forth (as indicated<br />
by the double-headed black arrow) between the underlying medial<br />
malleolus (gray lightning bolts) <strong>and</strong> the overlying FDL (white lightning<br />
bolts). B, A more anterior view <strong>of</strong> a partially torn PT as it might appear<br />
if it were laid flat. The tendon is thickened <strong>and</strong> butterflied open, with<br />
the gray region representing abnormal internal signal. (The dashed<br />
line represents the location <strong>of</strong> cross sections C to E). C to E, MRI cross<br />
sections <strong>of</strong> the PT only (now shown as a black ellipse), taken in the<br />
axial or oblique coronal plane through the longitudinal tear as it<br />
develops. In C, there is a gray wedge <strong>of</strong> abnormally increased<br />
signal along the inner aspect <strong>of</strong> the flattened PT (black ellipse).<br />
In D, tendinopathy (gray wedges) now involves the outer <strong>and</strong> inner<br />
surfaces <strong>of</strong> the PT. In E, the wedges <strong>of</strong> tendinopathy have progressed<br />
to a longitudinal tear, giving the appearance in cross section that the<br />
PT is two tendons.<br />
Ch0<strong>47</strong>-A05375.indd 2223<br />
9/9/2008 5:33:49 PM