Neuroimaging Christopher Bever, MD, MBA (MODERATOR) Use of ...
Neuroimaging Christopher Bever, MD, MBA (MODERATOR) Use of ...
Neuroimaging Christopher Bever, MD, MBA (MODERATOR) Use of ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Neuroimaging</strong><br />
<strong>Christopher</strong> <strong>Bever</strong>, <strong>MD</strong>, <strong>MBA</strong> (<strong>MODERATOR</strong>)<br />
<strong>Use</strong> <strong>of</strong> MRI in Diagnosing and Monitoring MS<br />
Jack H. Simon, Portland, OR<br />
What MRI Taught Us about Neurodegeneration<br />
and MS<br />
Matilde Inglese, NewYork
MRI in the Diagnosis <strong>of</strong> Multiple<br />
Sclerosis<br />
and<br />
MRI For Monitoring Disease Activity<br />
Jack H. Simon<br />
Portland, Oregon
Disclaimer<br />
• The speaker has received research support<br />
from Biogen-Idec and Genentech, and has<br />
been a consultant and/or received honoraria<br />
for speaking from Biogen-Idec, Genentech,<br />
Serono, Teva, Genzyme. Recent research<br />
support is reviewed by the Portland VA<br />
Research Oversight committee.
Outline<br />
MS<br />
Diagnosis<br />
And Diagnostic<br />
Criteria<br />
Standardized<br />
Imaging<br />
Integrating New Techniques<br />
Following<br />
Sub-clinical<br />
Disease<br />
Is Treatment Effective ?<br />
Complications <strong>of</strong> Treatment
MRI in the Individual Patient<br />
(As Opposed to the Population)
MRI in MS Clinical Trials and Natural History Studies<br />
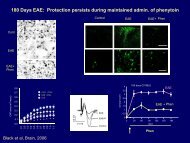
Interferon dosing<br />
Natural History Data<br />
From Li et al<br />
From Fisniku et al<br />
Question - The Relevance <strong>of</strong> Population Studies to<br />
the Individual ?
FROM SIMPLE TO COMPLEX<br />
T2-Lesions<br />
Gd-Enhancing Lesions<br />
T1-Black Holes<br />
Atrophy<br />
Magnetization Transfer<br />
Diffusion Tensor<br />
Myelin Water<br />
Functional MRI<br />
MR Spectroscopy<br />
•Long Experience, Validated - Secondary Measures in Trials<br />
•Increasing Relevance to Care <strong>of</strong> the Individual Patient
Lesion Overview
Gadolinium Enhancing Lesions<br />
Cell Trafficking<br />
Leaky<br />
Blood-Brain-Barrier<br />
Inflammation
Problem - MRI in Individual is a Snapshot in Time<br />
Jan Feb Mar Apr<br />
May Jun Jul Aug<br />
PD difference<br />
(Dec-Jan)<br />
Sep Oct Nov Dec<br />
Goodkin, Rooney, Sloan, Bacchetti, Gee, Vermathen, Abundo, Majumbdar, Nelson, Weiner Neurol. „98
T2 Lesions Non-Specific Pathology<br />
Including Edema, Demyelination<br />
Acute<br />
Weeks later
The T2 Footprint is Stable Over Time
Distribution--Periventricular >> Peripheral White<br />
MS-Mostly Periventricular- Minimial, Early<br />
Non-Specific<br />
Peripheral – other W<strong>MD</strong><br />
MS-Peripheral- Juxtacortical-Cortical
Brainstem/Cerebellum
T1 “Black Holes”<br />
A subset <strong>of</strong> T2 lesions with more damage<br />
Chronic T1- Black Holes- Lesions <strong>of</strong> more severe pathology<br />
Some Association with greater disability
Atrophy<br />
Strongest MRI - disability correlations but still only modest
Spinal Cord<br />
Proton/T2<br />
Proton density
Why MRI?<br />
• MS Is Largely<br />
Subclinical<br />
• That is--most current<br />
and new pathology is<br />
not known or detected<br />
by the patient or the<br />
clinician
Number Lesions<br />
Most <strong>of</strong> the Disease is Subclinical<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
Time <strong>of</strong> CIS<br />
0 6 12 18<br />
Time (months)
Baseline-CIS<br />
12 month<br />
18 month<br />
No Clinical Event over 5 years - Cognitive Deficits<br />
The Focal SubClinical Changes Are Relevant
MRI in Diagnostic Criteria
MRI Criteria for Diagnosis<br />
(& earlier diagnosis) <strong>of</strong> MS<br />
• Historical ( clinical) criteria for MS:<br />
– Dissemination in time and space<br />
• New Criteria<br />
– Quantitative (counts <strong>of</strong> specific T2 lesions) to<br />
document dissemination in space<br />
– MRI used as substitute (& strong) criteria for<br />
dissemination in time (second attack)
Accurate Prediction <strong>of</strong> Earliest MS<br />
1991-1995<br />
After First Clinical<br />
Event<br />
A positive MRI is a<br />
good predictor <strong>of</strong> a<br />
second clinically<br />
event which<br />
indicating MS
MRI Predictors <strong>of</strong> Second Clinical Event (MS)<br />
after a Clinically Isolated Syndrome<br />
N= 39 (max)<br />
From F. Bark<strong>of</strong>f
Bark<strong>of</strong>f<br />
Combined Criteria<br />
More Accurate Prediction <strong>of</strong> Second Clinical<br />
Event<br />
– 1 Enhancing or 9 T2<br />
– 1 Juxtacortical-Cortical<br />
– 3 Periventricular<br />
– 1 Infratentorial
Validation <strong>of</strong> Bark<strong>of</strong>f Criteria
McDonald Criteria<br />
Annals <strong>of</strong> Neurology 2001<br />
MRI Dissemination in<br />
Space<br />
3 <strong>of</strong> the 4 Bark<strong>of</strong>f Components<br />
1 Enhancing or 9 T2<br />
1 Juxtacortical-Cortical<br />
3 Periventricular<br />
1 Infratentorial<br />
+<br />
MRI Dissemination in<br />
Time<br />
Enhancing lesion<br />
or<br />
New T2 lesion
Classical Diagnosis <strong>of</strong> MS<br />
Clinically Isolated Syndrome<br />
Clinical Obvious<br />
Classic MS
Earlier Diagnosis <strong>of</strong> MS with MRI Event<br />
Clinically Isolated Syndrome<br />
MS<br />
Classic MS
MS (Diagnostic Criteria) After a CIS<br />
2005 - Polman et al<br />
revisions<br />
Spinal cord lesions can be<br />
utilized to substitute for<br />
brain lesions
The Criteria are Imperfect – Vigilance is Required<br />
PD<br />
T2<br />
December 1997 – CIS<br />
3 periventricular lesions-Doesn’t meet criteria
December 2002 - 5 year follow-up<br />
Strong evidence for ongoing demyelination despite not meeting formal criteria<br />
initially
Both criteria highly specific (>90%)<br />
Modified criteria more sensitive (77% v 46%)<br />
Modified criteria more accurate (86% v 73%)<br />
Swanton et al. JNNP 2005
Presentation ---Visual symptoms<br />
Infratentorial- none<br />
Enhancing or 9 T2-no<br />
Juxtacortical - not sure<br />
Periventricular - 3<br />
2003<br />
2004
2003<br />
Cortical Lesions only in retrospect<br />
2004 Improved Technique, Improved Diagnoses
Even Earlier Diagnosis?<br />
Radiologically Isolated<br />
Syndrome
Okuda et al. Neurology 2009;72:800
WiFi<br />
Worrisome Imaging Follow-up Indicated
<strong>Use</strong> <strong>of</strong> MRI to Follow Subclinical<br />
Disease
Lesion Counts<br />
Gadolinium–enhancing or T2<br />
Enhancing Lesions over 12 months<br />
Courtesy <strong>of</strong> Bill Rooney<br />
(Goodkin et al Neurology 98)<br />
Enhancing Lesions 6 months after a CIS<br />
Courtesy <strong>of</strong> Fred Barkh<strong>of</strong>
1<br />
4<br />
7<br />
10<br />
13<br />
16<br />
19<br />
22<br />
25<br />
28<br />
37<br />
40<br />
43<br />
46<br />
50<br />
Enhancing lesion number<br />
Untreated MS Patient<br />
16<br />
14<br />
12<br />
10<br />
8<br />
6<br />
4<br />
2<br />
0<br />
CEL<br />
month<br />
Courtesy <strong>of</strong> Nancy Richert – NIH
1<br />
6<br />
11<br />
16<br />
21<br />
26<br />
31<br />
36<br />
41<br />
46<br />
51<br />
56<br />
67<br />
74<br />
79<br />
84<br />
89<br />
94<br />
Enhancing lesion number<br />
T2LL (cc)<br />
Resumption <strong>of</strong> Disease Activity after IFN Discontinued<br />
(CEL and T2LL)<br />
30<br />
25<br />
IFN<br />
14<br />
12<br />
20<br />
10<br />
15<br />
10<br />
5<br />
0<br />
8<br />
6<br />
4<br />
2<br />
0<br />
CEL<br />
T2LL<br />
month<br />
Courtesy <strong>of</strong> Nancy Richert
<strong>Use</strong> <strong>of</strong> MRI to Determine<br />
Treatment Response<br />
Responders - Non-Responders<br />
Complications <strong>of</strong> Therapy
More specifically --- Can we<br />
monitor treatment response to<br />
disease modifying therapy by MRI<br />
in individual patients ?<br />
In Principle Any Disease Modifying Therapy
Evaluating the Therapeutic Response In<br />
The Individual Patient<br />
• Patient ---------Self-Report<br />
• Physician ------Global Impression<br />
• Other -----------More Objective Data<br />
– MS symptoms, relapses, disability<br />
– Biological Markers<br />
– MRI metrics<br />
Adapted from R. Rudick, Cleveland Clinic
Evidence-Based Studies to Define Treatment<br />
Failure<br />
Classification Parameters & Outcome Measure<br />
• Rudick et al (2004)<br />
• Rio et al (2008)<br />
• Durelli et al (2008)<br />
• Kinkel et al (2008)<br />
Gd/New T2 /Relapse<br />
Active Lesions (N,E,Gd+)<br />
Active MRI (and Nab)<br />
Gd+ and T2<br />
Outcome Measure – atrophy, disability, clinical event
Two year follow-up ; Outcome = Disability<br />
Active Lesions at One Year Post Therapy Predicted Disability
Durelli et al, 2008<br />
• Classification Parameter- Active Scan or NAb<br />
• Outcome Measure-One or more relapses or<br />
confirmed disease progression<br />
MRI Activity (any month) and Nab positive status<br />
71% sensitive, 86% specific, 50% PPV, 94% NPV
Treated Patients with 2 or more lesions at 6 months after treatment<br />
Are Non-Responders- Hazard Ratio 4.99 (p < 0.0001)<br />
R.P. Kinkel,1 P.W. O‟Connor,2 J. Simon,3 J. Carulli,4 M. del Carmen Castrillo,4 S. Goelz,4 R.<br />
Hyde,4 S. Lanker,4 A. Pace,4 A. Sandrock,4 and H. Zhang4<br />
*<br />
non-responder<br />
responder<br />
Kinkel et al, 2008
Odds Ratio 8.96 (p
New atypical weakness or seizure<br />
In a patient with established MS<br />
A<br />
B
2005
PML<br />
Concern is Detecting PML +MS<br />
•Limited mass effect<br />
•No enhancement<br />
•Follows cortical ribbon<br />
Charil, 2006
PML
Yousry et al. NEJM;2006 354:924-933
Who would biopsy?<br />
Feb 2006 Aug 2006<br />
Mar 2006<br />
From Tony Traboulsee, UBC
Standardized MRI<br />
For Improved Care<br />
Standardized Ordering<br />
Comparisons Possible<br />
Standard Terminology<br />
Optimal <strong>Use</strong> <strong>of</strong> MRI Metrics
Consortium MS Centers- Consensus Workshops<br />
– 2001 Vancouver Consensus workshop<br />
– 2003 Follow-up meeting<br />
• update the guidelines and protocol<br />
– 2008 Follow-up meeting<br />
• integration <strong>of</strong> advanced imaging ?<br />
• routine MRI follow-up ?<br />
Consider the CMSC Consensus Guidelines<br />
Simon et al. AJNR 27:455, 2006 - updated 2008 @<br />
www.mscare.org/cmsc/images/pdf/MRIprotocol2003.pdf<br />
taboulsee update???? MR Imaging in Diagnosing and Monitoring<br />
MS<br />
Don Paty
Standardized MRI Guidelines<br />
PD optional<br />
Recommended
Spinal Cord<br />
PD/T2<br />
PD/T2<br />
Sagittal < 3 mm<br />
Axial < 4 mm no gap<br />
No additional gadolinium required if spinal cord study<br />
immediately follows Gad-enhanced brain MRI
Update<br />
T. Traboulsee et al<br />
In 2009<br />
Mscare.org
New Issues in Standardized MRI<br />
(focal lesions)<br />
• Effect <strong>of</strong> Field strength – 3T and above<br />
• New Sequences –will the standards remain<br />
valid if these are 3D?<br />
• Cortical MS – how do incorporate new<br />
findings into clinical care?
Field Strength Matters<br />
Sicotte, 2003<br />
Wattjes, 2006<br />
Nielsen, 2006
Sicotte et al, 2003
We Expect 3D Acquisitions to<br />
become standard in future<br />
Axial Reformats<br />
Eur. Radiol. 2008
3D FLAIR - 1mm partitions<br />
3T MRI
3D FLAIR - 1mm partitions reconstructed to axial projection
Gray Matter Demyelination<br />
Double Inversion Recovery- DIR<br />
Images from six month follow-up; From Calabrese, Neuroimage, 2008<br />
Geurts, 2005, reported in Radiology a 500% advantage over T2; 150% over FLAIR
MRI Signal and Field Strength<br />
3T scanner should have twice SNR <strong>of</strong> 1.5T scanner<br />
7T should have ~4.7 times SNR <strong>of</strong> 1.5T.<br />
Modified from C.Rorden, www<br />
From: F. Fera et.al., J MRI 19:19-26 (2004)
Very High Field Imaging<br />
7T Human Scanner
7T MS MPRAGE 0.8 mm thick<br />
AIRC at OHSU, courtesy Bill Rooney
7 Tesla MRI - MS – T2*W Imaging<br />
Courtesy Bill Rooney, Oregon Health Sciences University-AIRC
MS, Fe Permeability Study<br />
OHSU 7T, Bill Rooney
A closer look <strong>of</strong> MS cortical grey at 7T<br />
3T (IR) SPGR<br />
Metcalf et al. Journal <strong>of</strong> <strong>Neuroimaging</strong> 2009
Summary- And Learning<br />
• Classical & new diagnostic criteria for MS diagnosis by<br />
MRI------From Populations to Individuals<br />
• MS is largely subclinical –What we don’t know can<br />
hurt us !<br />
• Monitoring therapy- better experimental criteria for<br />
non-responders<br />
• Standardized MS Exam<br />
• New considerations (3D, Field strength-Image Quality)
The End<br />
Thank You