Diseases of the salivary glands
Diseases of the salivary glands
Diseases of the salivary glands

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
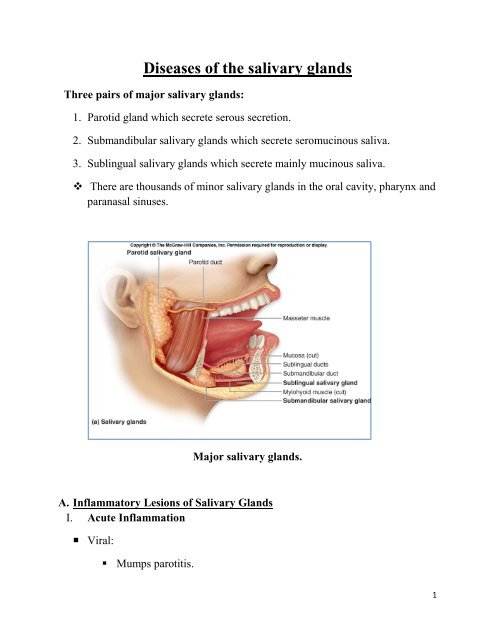
<strong>Diseases</strong> <strong>of</strong> <strong>the</strong> <strong>salivary</strong> <strong>glands</strong><br />
Three pairs <strong>of</strong> major <strong>salivary</strong> <strong>glands</strong>:<br />
1. Parotid gland which secrete serous secretion.<br />
2. Submandibular <strong>salivary</strong> <strong>glands</strong> which secrete seromucinous saliva.<br />
3. Sublingual <strong>salivary</strong> <strong>glands</strong> which secrete mainly mucinous saliva.<br />
There are thousands <strong>of</strong> minor <strong>salivary</strong> <strong>glands</strong> in <strong>the</strong> oral cavity, pharynx and<br />
paranasal sinuses.<br />
Major <strong>salivary</strong> <strong>glands</strong>.<br />
A. Inflammatory Lesions <strong>of</strong> Salivary Glands<br />
I. Acute Inflammation<br />
• Viral:<br />
• Mumps parotitis.<br />
1
• Bacterial<br />
• Acute suppurative parotitis<br />
Parotid abscess.<br />
Mumps.<br />
II.<br />
Chronic inflammation:<br />
• Chronic parotitis (Sialectasis): dilation <strong>of</strong> ductules <strong>of</strong> <strong>the</strong> parotid due to<br />
fibrosis <strong>of</strong> its proximal parts due to intercurrent inflammation (or stones).<br />
The gland is enlarged, s<strong>of</strong>t tender, usually bilaterally with attacks <strong>of</strong> acute<br />
exacerpations with high fever and pain.<br />
• Mikulicz’ syndrome: Enlargement <strong>of</strong> all <strong>the</strong> <strong>salivary</strong> <strong>glands</strong> (parotid,<br />
submandibular and sublinguals in addition to lachrymal gland. It is an<br />
autoimmune disease.<br />
• Sjögren’s syndrome: is similar to Mikilicz plus dryness <strong>of</strong> mouth and eye –<br />
xerostomia and xerophthalmia.<br />
B. Cysts <strong>of</strong> <strong>the</strong> <strong>salivary</strong> <strong>glands</strong><br />
Mucocele: It is a retention cyst which affect ei<strong>the</strong>r minor <strong>salivary</strong> <strong>glands</strong> (in <strong>the</strong><br />
oral cavity especially in <strong>the</strong> buccal mucosa) or in <strong>the</strong> major <strong>salivary</strong> <strong>glands</strong>.<br />
2
Rannula: A mucocele <strong>of</strong> <strong>the</strong> sublingual <strong>salivary</strong> gland, it presents as large tense<br />
bluish swelling in <strong>the</strong> floor <strong>of</strong> mouth which displaces <strong>the</strong> tongue.<br />
Mucocele<br />
Ranula<br />
C. Stones <strong>of</strong> <strong>the</strong> <strong>salivary</strong> <strong>glands</strong><br />
They are 30 times more common in submandibular <strong>glands</strong> than in parotids. Why?<br />
• Secretion <strong>of</strong> submandibular gland is more viscid.<br />
• The drainage is less dependent.<br />
• The opening <strong>of</strong> <strong>the</strong> submandibular duct is in <strong>the</strong> floor <strong>of</strong> <strong>the</strong> mouth, so food<br />
debris can precipitate in it.<br />
Clinical picture<br />
• The obstruction caused by <strong>the</strong> stone toge<strong>the</strong>r with <strong>the</strong> superadded infection<br />
leads to acute (or chronic) submandibular calculous sialadenitis.<br />
• This condition is manifested by pain and swelling <strong>of</strong> <strong>the</strong> gland on eating,<br />
swelling or seeing food. It may be associated with fever.<br />
• Clinically, <strong>the</strong> gland is felt bidigitally, <strong>the</strong> stone can be felt as well in <strong>the</strong><br />
floor <strong>of</strong> mouth.<br />
3
The submandibular stone lies in one <strong>of</strong> four positions;<br />
(1) meatal, (2) intraductal,(3) juxtaglandular, and (4) intraglandular.<br />
Treatment<br />
Anatomy <strong>of</strong> <strong>the</strong> submandibular gland.<br />
• meatal stone: only meatotomy and extraction.<br />
• intraductal stone: open <strong>the</strong> duct in <strong>the</strong> floor <strong>of</strong> mouth under local (nerve<br />
block) or general anaes<strong>the</strong>sia, extract <strong>the</strong> stone and do not close <strong>the</strong> incision.<br />
• juxtaglandular stone: do not try to extract <strong>the</strong> stone intra-orally to avoid<br />
injury to lingual nerve which hooks on <strong>the</strong> duct at this point, so excision <strong>of</strong><br />
<strong>the</strong> gland is mandatory.<br />
• intraglandular stone: The treatment is submandibular sialadenectomy.<br />
D. Tumours <strong>of</strong> <strong>salivary</strong> <strong>glands</strong><br />
The larger <strong>the</strong> gland, <strong>the</strong> more benign is <strong>the</strong> higher incidence<br />
Parotid <strong>glands</strong> 80% benign,<br />
Submandibular 60% benign,<br />
4
Minor <strong>salivary</strong> <strong>glands</strong> 50% malignant.<br />
Parotid is gland <strong>of</strong> tumor while submandibular is a gland <strong>of</strong> stones.<br />
Criteria <strong>of</strong> parotid gland swelling.<br />
• Elevation <strong>of</strong> ear lobule<br />
• Obliteration <strong>of</strong> furrow between <strong>the</strong> mandible and mastoid process.<br />
• Get prominent on clenching <strong>of</strong> teeth.<br />
• Less prominent on opening <strong>of</strong> <strong>the</strong> mouth.<br />
Benign tumors<br />
1. Pleomorphic adenoma<br />
Rule <strong>of</strong> 80%<br />
• 80% <strong>of</strong> tumors <strong>of</strong> <strong>salivary</strong> occurs in parotid<br />
• 80% <strong>of</strong> <strong>the</strong>m are benign<br />
• 80% <strong>of</strong> <strong>the</strong>m are pleomorphic adenoma<br />
Treatment:<br />
Superficial parotidectomy. If <strong>the</strong> tumour is in <strong>the</strong> deep lobe, we do total<br />
conservative parotidectomy.<br />
2. Warthin’s tumour. ( Adenolymphoma or Papillary cystadenoma<br />
lymphomatosum).<br />
• It occurs after 60 years <strong>of</strong> age, male to female = 4:1.<br />
• Only occurs in <strong>the</strong> parotid gland (15% <strong>of</strong> all parotid tumours).<br />
• Mostly in <strong>the</strong> tail <strong>of</strong> <strong>the</strong> parotid.<br />
• It is s<strong>of</strong>t or cystic.<br />
• It has high incidence <strong>of</strong> bilaterality and multiplicity.<br />
5
• Treatment: Superficial parotidectomy.<br />
Malignant <strong>salivary</strong> gland tumors.<br />
1. Acinic cell carcinoma<br />
It is a low grade tumour with very late lymph node and distant metastasis.<br />
Prognosis is good in comparison to o<strong>the</strong>r types.<br />
2. Mucoepidermoid carcinoma (2 types)<br />
Low grade malignancy type.<br />
High grade variant: with lymph nodes.<br />
3. Adenoid cystic carcinoma (cylinderoma)<br />
It is aggressive and has tendency to perineural spread even intracranially.<br />
4. Carcinoma ex pleomorphic adenoma (rare).<br />
Clinical picture <strong>of</strong> a malignant <strong>salivary</strong> tumors:<br />
• Pain.<br />
• Rapid rate <strong>of</strong> growth.<br />
• Consistency is mainly hard.<br />
• Facial nerve dysfunction or even paralysis.<br />
• Fixity to skin → Ulceration.<br />
• Fixity to deeper structures: muscles, bone.<br />
• Cervical lymph node metastasis.<br />
• Bone and lung metastasis.<br />
Investigations <strong>of</strong> a <strong>salivary</strong> gland mass<br />
• X-ray: Oblique view and intra-oral film for submandibular stone.<br />
6
• Ultrasonography.<br />
• CT.<br />
• MRI.<br />
• PET.<br />
• FNAC.<br />
• Sialography: Dye study is beneficial in diagnosing sialectasis.<br />
7