Neisseria gonorrhoeae - Pharos University in Alexandria
Neisseria gonorrhoeae - Pharos University in Alexandria
Neisseria gonorrhoeae - Pharos University in Alexandria

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Lecture 5 - Fall 2012-2013- (General Microbiology)<br />
MCR 311<br />
Gram -ve Diplococci<br />
Presented by:<br />
Prof. Dr. Mervat El Saygh<br />
Microbiology & Medical Immunology Dept,<br />
<strong>Pharos</strong> <strong>University</strong>
LEARNING OBJECTIVES<br />
• State the characteristics of the 2 types<br />
of <strong>Neisseria</strong><br />
23/10/2012
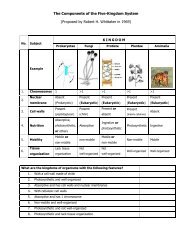
BACTERIA<br />
Staphylococci<br />
Streptococci<br />
Enterococci<br />
G+ cocci<br />
COCCI BACILLI SPIROCHETES<br />
Non spore-form<strong>in</strong>g<br />
G+ bacilli<br />
Spore form<strong>in</strong>g<br />
G+ bacilli<br />
Enterobacteriaceae<br />
Treponema<br />
Borrelia<br />
G- diplococci<br />
Pseudomonas/Vibrio<br />
Campylobacter<br />
Helicobacter<br />
Mycobacteria<br />
(TB/Leprae)<br />
Parvobacteriaceae<br />
23/10/2012
NEISSERIA<br />
• aerobic,<br />
• gram negative diplococci<br />
• require carbon dioxide for growth,<br />
• grow at 37°C,<br />
• grow best on media conta<strong>in</strong><strong>in</strong>g blood<br />
(blood agar and chocolate agar).<br />
• They are oxidase positive.<br />
23/10/2012
23/10/2012
<strong>Neisseria</strong> Men<strong>in</strong>gitidis
<strong>Neisseria</strong> Men<strong>in</strong>gitidis<br />
– causative agent of men<strong>in</strong>gococcal<br />
men<strong>in</strong>gitis <strong>in</strong> adults<br />
– spread by respiratory route.<br />
– is divided <strong>in</strong>to 13 serogroups accord<strong>in</strong>g to<br />
the capsular polysaccharide.<br />
– Serogroups A, B, C, Y, and W-135 are the<br />
most important.<br />
– Cl<strong>in</strong>ical picture: Rapid onset with<br />
headache, fever and neck stiffness<br />
23/10/2012
<strong>Neisseria</strong> Men<strong>in</strong>gitidis - Cl<strong>in</strong>ical<br />
Manifestations<br />
23/10/2012<br />
• Beg<strong>in</strong>s as mild pharyngitis with occasional slight fever.<br />
• Initial signs are fever, vomit<strong>in</strong>g, headache, and stiff<br />
neck.<br />
• A petechial eruption then develops that progress form<br />
erythematous macules to frank purpura; vasculitic<br />
purpura is the hallmark.<br />
• LPS of organisms causes <strong>in</strong>travascular coagulation,<br />
circulatory collapse, and shock.<br />
• Waterhouse-Friderichsen syndrome describes fulm<strong>in</strong>at<strong>in</strong>g<br />
men<strong>in</strong>gococcemia with hemorrhage, circulatory failure,<br />
and adrenal <strong>in</strong>sufficiency.
<strong>Neisseria</strong> Men<strong>in</strong>gitidis – Laboratory<br />
Diagnosis<br />
• Direct CSF exam<strong>in</strong>ation and Gram<br />
sta<strong>in</strong> reveals gram negative diplococci<br />
<strong>in</strong>tra and extra cellular<br />
• culture on blood agar or chocolate<br />
agar<br />
• oxidase positive<br />
23/10/2012
<strong>Neisseria</strong> Men<strong>in</strong>gitidis – Control<br />
Prevention<br />
• Provide penicill<strong>in</strong> prophylaxis for exposed young family<br />
children; if patient <strong>in</strong> day care sett<strong>in</strong>g with other young<br />
children, also give penicill<strong>in</strong>; no prophylaxis for older children<br />
or adults.<br />
• Give rifamp<strong>in</strong> to all family members and to patient to eradicate<br />
the carrier state (Penicill<strong>in</strong> will not eradicate carrier state).<br />
• Vacc<strong>in</strong>e is capsular polysaccharide from A and C serogroups<br />
(B serogroup polysaccharide is poorly immunogenic); biggest<br />
problem is vacc<strong>in</strong>e failure <strong>in</strong> target group aged 6 months to 2<br />
years where most <strong>in</strong>fections occur.<br />
23/10/2012
<strong>Neisseria</strong> Men<strong>in</strong>gitidis – Virulence<br />
Attributes<br />
• Capsular polysaccharide <strong>in</strong>hibits phagocytosis.<br />
• LPS causes extensive tissue necrosis, circulatory<br />
collapse, <strong>in</strong>travascular coagulation, and shock.<br />
• IgAase degrades IgA; probably important because<br />
these <strong>in</strong>fections beg<strong>in</strong> on mucosal membranes<br />
(streptococci, hemophilu, and neisseria have this<br />
enzyme).<br />
23/10/2012
N. men<strong>in</strong>gitidis<br />
(the “Men<strong>in</strong>gococcus")<br />
23/10/2012<br />
12
Capsule<br />
• capsule<br />
– <strong>in</strong>hibit phagocytosis<br />
• anti-capsular antibodies<br />
– stop <strong>in</strong>fection<br />
•antigenic variation<br />
– sero-groups<br />
23/10/2012<br />
• vacc<strong>in</strong>e<br />
–multiple sero-groups
<strong>Neisseria</strong> Gonorrhoeae
<strong>Neisseria</strong> Gonorrhea<br />
• Causative agent of gonorrhea (sexually<br />
transmitted disease).<br />
• It attacks the mucous membrane of the<br />
genito-ur<strong>in</strong>ary tract, eyes and the<br />
rectum produc<strong>in</strong>g acute suppuration,<br />
chronic <strong>in</strong>flammation and fibrosis.<br />
23/10/2012
<strong>Neisseria</strong> Gonorrhea<br />
• In male it causes gonococcal<br />
uretheritis<br />
• In female usually asymptomatic, found<br />
<strong>in</strong> the female cervix<br />
• Neonatal ophthalmia <strong>in</strong> those born to<br />
<strong>in</strong>fected mothers<br />
23/10/2012
<strong>Neisseria</strong> Gonorrhoeae<br />
Classification<br />
N. gonorrhea differentiated by auxotyp<strong>in</strong>g<br />
(nutritional requirements) or colonial morphology<br />
(types 1 and 2 are virulent, types 3, 4 and 5 are far<br />
less virulent).<br />
23/10/2012
NEISSERIA<br />
<strong>Neisseria</strong> 23/10/2012 <strong>gonorrhoeae</strong><br />
18
23/10/2012<br />
19
23/10/2012<br />
20
<strong>Neisseria</strong> Gonorrhoeae - Cl<strong>in</strong>ical<br />
Manifestations<br />
• Mucous membrane <strong>in</strong>fections that occur predom<strong>in</strong>antly <strong>in</strong><br />
anterior urogenital tract.<br />
• Asymptomatic <strong>in</strong>fection <strong>in</strong> 20% to 80% of females and 10% of<br />
males, these patients transmit the bacteria to consorts,<br />
result<strong>in</strong>g <strong>in</strong> symptomatic gonorrhea.<br />
• A number of different types of <strong>in</strong>fection:<br />
A- Urethirtis- thick, yellow, purulent exudates conta<strong>in</strong><strong>in</strong>g bacteria<br />
and numerous PMNs; pa<strong>in</strong>ful and frequent ur<strong>in</strong>ation; meatus may<br />
be erythematous.<br />
23/10/2012<br />
B- Complications of urethritis <strong>in</strong>clude epididymitis and prostatitis <strong>in</strong><br />
males and pelvic <strong>in</strong>flammatory disease <strong>in</strong> females; repeated<br />
<strong>in</strong>fections may cause scarr<strong>in</strong>g with subsequent sterility <strong>in</strong> both<br />
sexes.
<strong>Neisseria</strong> Gonorrhoeae - Cl<strong>in</strong>ical<br />
Manifestations (Cont’d)<br />
C- Rectal <strong>in</strong>fections- pa<strong>in</strong>ful defecation, discharge, constipation,<br />
pretties; prevalent <strong>in</strong> gay males.<br />
D- Pharyngitis- mild form mimics viral sore throat; severe form<br />
mimics streptococcal sore throat; purulent discharge.<br />
E- Dissem<strong>in</strong>ated <strong>in</strong>fection- bloodstream <strong>in</strong>vasion <strong>in</strong> which organisms<br />
<strong>in</strong>itially localize <strong>in</strong> sk<strong>in</strong> caus<strong>in</strong>g dermatitis (s<strong>in</strong>gle macular,<br />
popular, erythematous lesion); a few days later, organisms<br />
spread to the jo<strong>in</strong>t caus<strong>in</strong>g overt, pa<strong>in</strong>ful arthritis (hands, wrists,<br />
elbows, ankles).<br />
F- Infant eye <strong>in</strong>fection- ophthalmic neonatorum <strong>in</strong>volve sever,<br />
bilateral purulent through birth canal.<br />
23/10/2012
<strong>Neisseria</strong> Gonorrhoeae – Laboratory<br />
Diagnosis<br />
Cl<strong>in</strong>ical Specimens<br />
• On females, always do a genital and a rectal<br />
culture.<br />
• If us<strong>in</strong>g a speculum or endoscope, do not use a<br />
lubricant because it will kill organisms.<br />
• Organisms are labile, and specimens should be<br />
immediately.<br />
• If dissem<strong>in</strong>ated gonorrhea, culture blood and<br />
synovial fluid; culture of sk<strong>in</strong> lesion is rarely<br />
successful.<br />
23/10/2012
<strong>Neisseria</strong> Gonorrhoeae – Laboratory<br />
Diagnosis<br />
In acute <strong>in</strong>fection:<br />
• Direct smear of the discharge sta<strong>in</strong>ed<br />
by gram sta<strong>in</strong> revealed gram negative<br />
diplococci <strong>in</strong>tra and extracellular <strong>in</strong> pus<br />
cells.<br />
• cultured on chocolate agar.<br />
• Oxidase positive<br />
23/10/2012
<strong>Neisseria</strong> Gonorrhoeae – Laboratory<br />
Diagnosis<br />
In chronic <strong>in</strong>fection:<br />
• In male: morn<strong>in</strong>g drop<br />
• In female: endocervical swab<br />
• Culture on Thayer-Mart<strong>in</strong> agar<br />
(selective media)<br />
• Blood culture <strong>in</strong> dissem<strong>in</strong>ated cases<br />
23/10/2012
<strong>Neisseria</strong> Gonorrhoeae – Control<br />
Prevention<br />
• Treat partners because of contagious nature of<br />
gonorrhea.<br />
• To prevent newborn gonococcal conjunctivitis, use<br />
topical AgNo 3 or tetracycl<strong>in</strong>e; antibiotic is better because<br />
it will also kill Chlamydia trachomatis if present.<br />
• Use condom to prevent transmission.<br />
• Identify asymptomatic patients by cultur<strong>in</strong>g gonococci,<br />
23/10/2012<br />
and treat with penicill<strong>in</strong>.
<strong>Neisseria</strong> Gonorrhoeae – Virulence<br />
Attributes<br />
• IgAse that degrades IAg1; important because <strong>in</strong><br />
mucosal <strong>in</strong>fections, this antibody probably plays a<br />
key early role (IgAse also <strong>in</strong> hemphiuls and<br />
streptococcal organisms).<br />
• Plasmid that codes for penicill<strong>in</strong>ase production.<br />
• Pili are prote<strong>in</strong> surface appendages that mediate<br />
gonococcal attachment to mucosal epithelium.<br />
• Lipopolysacchride (LPS) damages mucosal cells.<br />
23/10/2012
<strong>Neisseria</strong> Gonorrhea<br />
In male it causes gonococcal uretheritis<br />
23/10/2012
Enterococci<br />
On blood agar they form colonies of variable hemolysis.<br />
They are heat resistant (40°C)<br />
They cause nosocomial <strong>in</strong>fections <strong>in</strong> hospitals.<br />
23/10/2012
MRSA<br />
are stra<strong>in</strong>s of staphylococci which are considered resistant<br />
to all beta lactam antibiotics <strong>in</strong>clud<strong>in</strong>g penicill<strong>in</strong>s<br />
23/10/2012
Streptococci<br />
Streptococci<br />
23/10/2012
Beta-hemolysis<br />
a clear zone of hemolysis on blood agar<br />
23/10/2012
<strong>Neisseria</strong><br />
gram negative diplococci<br />
require carbon dioxide for growth<br />
Oxidase positive<br />
23/10/2012
Coagulase negative<br />
staph<br />
Staphylococcus epidermidis and staphylococcus<br />
saprophyticus<br />
23/10/2012
<strong>Neisseria</strong> men<strong>in</strong>igitidis<br />
Causes men<strong>in</strong>gitis <strong>in</strong> adults<br />
23/10/2012
Enterotox<strong>in</strong><br />
A tox<strong>in</strong> that causes food poison<strong>in</strong>g<br />
23/10/2012
Thayer-Mart<strong>in</strong><br />
Selective media for neisseria<br />
23/10/2012
Viridans Streptococci<br />
cause subacute bacterial endocarditis of abnormal heart<br />
valves.<br />
23/10/2012
Thank You