Diagnostic and Therapeutic Endoscopy of Biliary Diseases
Diagnostic and Therapeutic Endoscopy of Biliary Diseases
Diagnostic and Therapeutic Endoscopy of Biliary Diseases

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
DISEASES OF THE BILIARY TRACT, SERIES #6<br />
Rad Agrawal, M.D., Series Editor<br />
<strong>Diagnostic</strong> <strong>and</strong> <strong>Therapeutic</strong><br />
<strong>Endoscopy</strong> <strong>of</strong> <strong>Biliary</strong> <strong>Diseases</strong><br />
by Yamini Subbiah, Shyam Thakkar, Elie Aoun<br />
The therapeutic approach to biliary diseases has undergone a paradigm shift over<br />
the past decade toward minimally invasive endoscopic interventions. This paper<br />
reviews the advances <strong>and</strong> different diagnostic <strong>and</strong> therapeutic endoscopic approaches<br />
to common biliary diseases including choledocholithiasis, benign <strong>and</strong> malignant biliary<br />
strictures <strong>and</strong> bile leaks.<br />
INTRODUCTION<br />
With the introduction <strong>of</strong> innovative endoscopic<br />
implements <strong>and</strong> options allowing for unprecedented<br />
access to the biliary tree, the therapeutic<br />
approach to biliary diseases has undergone a significant<br />
paradigm shift over the past decade toward minimally<br />
invasive endoscopic interventions. The days where biliary<br />
diseases were exclusively managed surgically are<br />
long gone, <strong>and</strong> much has changed since the first<br />
reported biliary sphincterotomies in 1974. The recent<br />
developments in peroral cholangioscopy <strong>and</strong> new<br />
modalities <strong>of</strong> anchoring high resolution nasogastric<br />
scopes in the bile duct <strong>of</strong>fer the opportunity <strong>of</strong> direct<br />
visualization <strong>of</strong> the bile duct lumen, which allows for<br />
not only better identification <strong>of</strong> the underlying disease<br />
process but also for targeting <strong>of</strong> biopsies <strong>and</strong> directed<br />
lithotripsy. Other modalities that add to the growing<br />
world <strong>of</strong> biliary luminal imaging include endoscopic<br />
ultrasound (EUS) <strong>and</strong> intraductal ultrasound, which<br />
enable the endoscopist to assess extrabiliary disorders.<br />
EUS-assisted fine needle aspiration (FNA) tissue sampling<br />
<strong>and</strong> immediate preliminary histopathologic analysis<br />
also assist in immediate decision making <strong>and</strong><br />
therapeutics. Other recent advances include cuttingedge<br />
molecular imaging technology that allows the<br />
endoscopist to differentiate between benign <strong>and</strong> malignant<br />
features, thus guiding decision making in real time.<br />
COMMON BILE DUCT STONES<br />
Over 98% <strong>of</strong> biliary disorders are linked to gallstones.<br />
Stones are found in the common bile duct (CBD) in up<br />
to 18% <strong>of</strong> patients with symptomatic cholelithiasis (1).<br />
The vast majority <strong>of</strong> gallstones are cholesterol-rich,<br />
form in the gallbladder <strong>and</strong> gain access to the CBD via<br />
the cystic duct. De novo CBD stone formation is also<br />
well described <strong>and</strong> is more common in patients <strong>of</strong><br />
Asian descent. These primary duct stones typically<br />
have a higher bilirubin <strong>and</strong> a lower cholesterol content<br />
<strong>and</strong> biliary stasis; further, bacterial infections have<br />
been implicated in their pathogenesis (2,3). CBD<br />
stones can lead to several complications including biliary<br />
colic, obstructive jaundice <strong>and</strong> cholangitis.<br />
<strong>Diagnostic</strong> Imaging Tests<br />
While a minority <strong>of</strong> patients with a straight-forward<br />
clinical presentation consistent with choledocholithiasis<br />
may immediately be treated with ERCP, the vast<br />
majority will benefit from diagnostic imaging studies<br />
to confirm the diagnosis. Performing a diagnostic<br />
ERCP with no prior imaging is not optimal due to the<br />
potential risks associated with the procedure. Current<br />
imaging modalities available for this purpose include<br />
transabdominal ultrasound, regular- <strong>and</strong> high-resolu-<br />
Yamini Subbiah, MD; Shyam Thakkar, MD; Elie Aoun,<br />
MD, MS, West Penn Allegheny Health System, Division<br />
<strong>of</strong> Gastroenterology, Hepatology <strong>and</strong> Nutrition,<br />
Pittsburgh, PA. (continued on page 32)<br />
30<br />
PRACTICAL GASTROENTEROLOGY • JULY 2011
<strong>Diagnostic</strong> <strong>and</strong> <strong>Therapeutic</strong> <strong>Endoscopy</strong> <strong>of</strong> <strong>Biliary</strong> <strong>Diseases</strong><br />
DISEASES OF THE BILIARY TRACT, SERIES #6<br />
(continued from page 30)<br />
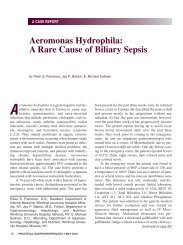
Figure 1. Endoscopic ultrasound showing stone in the<br />
common bile duct; B) Gallstone extraction during ERCP.<br />
tion computed tomography (CT) scans, magnetic resonance<br />
cholangiopancreatography (MRCP) <strong>and</strong> EUS.<br />
A transabdominal ultrasound remains the initial<br />
test <strong>of</strong> choice in suspected cases <strong>of</strong> choledocholithiasis<br />
because <strong>of</strong> its wide-spread availability <strong>and</strong> relatively<br />
lower costs. Dilated ducts seen on ultrasound are<br />
highly suggestive <strong>of</strong> biliary obstruction; however,<br />
normal caliber ducts do not exclude a CBD stone.<br />
Furthermore, differentiating between causes <strong>of</strong><br />
obstruction may also be difficult using this imaging<br />
modality. Even still, while the transabdominal ultrasound’s<br />
sensitivity in detecting choledocholithiasis is<br />
low (ranging between 25% <strong>and</strong> 58%), its specificity<br />
can be greater than 95% (4–6).<br />
MRCP has catapulted to the frontlines <strong>of</strong> diagnostic<br />
imaging <strong>and</strong> is typically the next test physicians<br />
perform following an indeterminate transabdominal<br />
ultrasound. Its sensitivity <strong>and</strong> specificity is 95% <strong>and</strong><br />
97%, respectively, in detecting the presence <strong>and</strong> level<br />
<strong>of</strong> biliary obstruction. However, its sensitivity in detecting<br />
stones is a function <strong>of</strong> stone size. While it ranges<br />
from 67%–100% for stones larger than 1 cm, it can be<br />
as low as 33%–71% in stones less than 6 mm (7–9).<br />
Conventional CT scans have relatively good accuracy<br />
(70%–94%) when it comes to identifying both the<br />
presence <strong>and</strong> the cause <strong>of</strong> biliary obstruction (10,11).<br />
A newer technique, the helical CT cholangiography<br />
(hCTC), is yet another diagnostic option <strong>and</strong> allows<br />
for three-dimensional reconstitution <strong>of</strong> images through<br />
the use <strong>of</strong> volumetric data after the administration <strong>of</strong><br />
both oral <strong>and</strong> intravenous (IV) contrast. It has proven<br />
to be beneficial in detecting CBD stones with a sensitivity<br />
<strong>of</strong> ~87% <strong>and</strong> a high specificity <strong>of</strong> 97%, accounting<br />
for an overall accuracy <strong>of</strong> 95% (12,13). However,<br />
hCTC remains underused due to its limited availability<br />
as compared with MRCP.<br />
Over the past few years, the use <strong>of</strong> EUS as a diagnostic<br />
imaging modality for CBD stones has gained<br />
significant momentum. While more invasive than the<br />
above methods, its associated risks <strong>and</strong> complications<br />
are lower than those with ERCP. The sensitivity <strong>and</strong><br />
specificity at detecting CBD stones are 95% <strong>and</strong> 98%,<br />
respectively, with a total accuracy <strong>of</strong> 96% (14,15).<br />
Furthermore, studies have shown that in cases with<br />
moderate or low clinical suspicion for choledocholithiasis,<br />
the use <strong>of</strong> EUS may prevent up to 30% <strong>of</strong> unnecessary<br />
ERCPs (16). Figure 1A illustrates an EUS<br />
showing a stone in the CBD.<br />
Endoscopic Therapy<br />
Prior to the introduction <strong>of</strong> ERCP with sphincterotomy<br />
in the 1970s, choledocholithiasis was mainly managed<br />
with surgical extraction <strong>and</strong> open bile duct exploration<br />
(17). Now, endoscopic techniques are first-line therapy<br />
for CBD stones.<br />
ERCP should be reserved for patients in whom a<br />
therapeutic intervention is likely to occur. Nevertheless,<br />
in certain rare situations where the diagnosis<br />
remains uncertain despite multiple imaging modalities,<br />
ERCP may be required. Once the diagnosis is suspected<br />
or established, stone extraction <strong>and</strong> ductal<br />
clearance become the therapeutic goals. Using a sideviewing<br />
scope which allows direct visualization <strong>and</strong><br />
easy access to the papilla, cannulation <strong>of</strong> the bile duct<br />
can be performed using a variety <strong>of</strong> available instruments<br />
including cannulas <strong>and</strong> sphincterotomes. In the<br />
h<strong>and</strong>s <strong>of</strong> an experienced endoscopist, cannulation success<br />
rates average ~95% (18). Once ductal access is<br />
established, contrast can be used to opacify <strong>and</strong> visualize<br />
the lumen. Typically stones are identified on the<br />
cholangiogram as filling defects around which the contrast<br />
flows. Opacification <strong>of</strong> the ducts also allows for<br />
measurement <strong>of</strong> the severity <strong>of</strong> the dilation proximal to<br />
the stone if any. Frey et al quote the accuracy <strong>of</strong> ERCP<br />
at detecting CBD stones to be at 96% (19).<br />
Once the stone is identified, the focus shifts to<br />
extracting it from the duct. Figure 1B shows gallstone<br />
extraction during ERCP. In the majority <strong>of</strong> cases, a biliary<br />
sphincterotomy is needed prior to stone removal.<br />
32<br />
PRACTICAL GASTROENTEROLOGY • JULY 2011
<strong>Diagnostic</strong> <strong>and</strong> <strong>Therapeutic</strong> <strong>Endoscopy</strong> <strong>of</strong> <strong>Biliary</strong> <strong>Diseases</strong><br />
DISEASES OF THE BILIARY TRACT, SERIES #6<br />
In certain cases where such a cut may be problematic,<br />
such as in patients on anticoagulation, the endoscopist<br />
may elect to balloon dilate the sphincter area. It should<br />
be noted though that there are reports <strong>of</strong> higher risks <strong>of</strong><br />
post-ERCP pancreatitis in cases where balloon dilation<br />
has been used (20). In cases where cannulation is difficult<br />
to achieve, a needle knife papillotome can be used<br />
in a technique known as “precutting” to establish direct<br />
access into the bile duct. Once access is achieved, a<br />
variety <strong>of</strong> instruments are available to attempt ductal<br />
clearance. Most stones up to 15 mm in size can be<br />
removed by sweeping the ducts with an extraction balloon,<br />
or alternatively by using a Dormia basket provided<br />
that a large enough sphincterotomy has been<br />
performed (21). In certain instances, though, the stone<br />
size may be too large to extract, <strong>and</strong> as such, alternative<br />
methods such as lithotripsy should be considered.<br />
Different lithotripsy modalities are available<br />
including mechanical, electrohydraulic, laser <strong>and</strong> extracorporeal<br />
shock wave (22,23). Mechanical lithotriptors<br />
are widely available. They consist <strong>of</strong> a basket with two<br />
sheaths: plastic <strong>and</strong> metal. Once the stone is caught in<br />
the basket wires, the metal sheath is advanced over the<br />
plastic sheath, <strong>and</strong> the stone is crushed into smaller<br />
pieces against the metal. Mechanical lithotripsy has<br />
high success rates but can be limited in the setting <strong>of</strong><br />
stone impaction (24). Most tertiary care centers have<br />
the capability <strong>of</strong> performing intraductal lithotripsy<br />
through the use <strong>of</strong> a SpyGlass ® choledochoscope<br />
(Boston Scientific Corp, Natick, MA, USA), which<br />
allows for direct visualization <strong>of</strong> the ductal lumen (25).<br />
Laser lithotripsy amplifies light energy to break up the<br />
stone, while the electrohydraulic method relies on<br />
shock waves produced by a power generator <strong>and</strong> transmitted<br />
through a bipolar electrode (22,26).<br />
Under certain circumstances, only partial ductal<br />
clearance is achieved, <strong>and</strong> a repeat ERCP is needed. In<br />
such situations, it is typical to insert a temporary biliary<br />
stent to secure ductal patency while the patient<br />
awaits the second procedure (27). In most cases, the<br />
ERCP can be performed on an outpatient basis <strong>and</strong><br />
does not require an overnight hospital stay unless early<br />
post-procedure complications are suspected.<br />
The readmission rates following biliary sphincterotomy<br />
<strong>and</strong> same day discharge are approximately 6%,<br />
with the majority <strong>of</strong> cases being readmitted for post-<br />
ERCP pancreatitis. Readmission is more likely to occur<br />
in patients who have one or more <strong>of</strong> the following risk<br />
factors: suspected sphincter <strong>of</strong> Oddi dysfunction, cirrhosis,<br />
difficult bile duct cannulation, precut sphincterotomy,<br />
or combined percutaneous-endoscopic procedure.<br />
The majority <strong>of</strong> complications requiring readmission<br />
occur within six hours following the procedure (28).<br />
PREVENTING RECURRENCE<br />
Recurrent CBD stones occur most frequently in patients<br />
with concurrent choledocholithiasis <strong>and</strong> cholelithiasis<br />
(29). A study <strong>of</strong> 371 patients who underwent an ERCP<br />
with sphincterotomy but who did not undergo subsequent<br />
cholecystectomy over a span <strong>of</strong> 7.7 years found a<br />
10% recurrence rate <strong>of</strong> choledocholithiasis (30). A<br />
smaller study <strong>of</strong> 120 patients who had undergone a biliary<br />
sphincterotomy for CBD stones <strong>and</strong> who were r<strong>and</strong>omized<br />
to laparoscopic cholecystectomy or a “wait<br />
<strong>and</strong> see” policy found that recurrent biliary events were<br />
observed more frequently over the next 2 years in the<br />
watchful waiting group as compared to the treated group<br />
(47% versus 2%, respectively) (31). It is therefore recommended<br />
that an elective cholecystectomy be performed<br />
as soon as possible following ductal clearance if<br />
the patient is deemed to be a surgical c<strong>and</strong>idate.<br />
BILIARY STRICTURES<br />
<strong>Biliary</strong> strictures can be benign or malignant. The general<br />
approach to treatment is based on the need to reestablish<br />
bile flow through the narrowed area in order<br />
to avoid complications including biliary stasis, jaundice<br />
<strong>and</strong> infections. A wide spectrum <strong>of</strong> clinical presentations<br />
has been described with biliary strictures<br />
ranging from asymptomatic patients with mild liver<br />
function test abnormalities to full blown obstructive<br />
jaundice, hyperbilirubinemia <strong>and</strong> recurrent episodes <strong>of</strong><br />
cholangitis. Many classifications have been generated<br />
for biliary strictures. However, the Bismuth classification<br />
is the most widely used. It subdivides strictures<br />
into five groups depending on the stricture location<br />
within the biliary tree (Table 1) (32).<br />
Differentiating between benign <strong>and</strong> malignant etiologies<br />
is <strong>of</strong> high clinical importance. A full discussion<br />
about the clinical indices <strong>of</strong> possible malignancy is<br />
beyond the scope <strong>of</strong> this review; however, certain ele-<br />
PRACTICAL GASTROENTEROLOGY • JULY 2011 33
<strong>Diagnostic</strong> <strong>and</strong> <strong>Therapeutic</strong> <strong>Endoscopy</strong> <strong>of</strong> <strong>Biliary</strong> <strong>Diseases</strong><br />
DISEASES OF THE BILIARY TRACT, SERIES #6<br />
Table 1.<br />
Bismuth Classification<br />
Stricture Type<br />
Benign strictures<br />
Type 1<br />
Type 2<br />
Type 3<br />
Type 4<br />
Type 5<br />
Malignant Strictures<br />
Type 1<br />
Type 2<br />
Type 3a<br />
Type 3b<br />
Type 4<br />
Description<br />
Low common bile duct stricture<br />
>2 cm distal to the bifurcation<br />
Mid common bile duct stricture<br />
2 cm distal to the bifurcation<br />
Mid common bile duct stricture<br />
<strong>Diagnostic</strong> <strong>and</strong> <strong>Therapeutic</strong> <strong>Endoscopy</strong> <strong>of</strong> <strong>Biliary</strong> <strong>Diseases</strong><br />
DISEASES OF THE BILIARY TRACT, SERIES #6<br />
(continued from page 34)<br />
cytology improves the brushing’s diagnostic accuracy<br />
(41). Targeted intraductal forceps biopsies through the<br />
use <strong>of</strong> a cholangioscope can improve the sensitivity to as<br />
high as 96% (42). The use <strong>of</strong> SpyGlass ® cholangioscopy<br />
results in a sensitivity <strong>of</strong> 71% <strong>and</strong> specificity <strong>of</strong> 100% in<br />
diagnosing malignancy in an indeterminate stricture<br />
(43). IDUS is a relatively newer technique which can<br />
better evaluate <strong>and</strong> distinguish between benign <strong>and</strong><br />
malignant lesions when coupled with ERCP, increasing<br />
the diagnostic accuracy to up to 90% (14).<br />
Image-enhanced cholangioscopy techniques<br />
include chromocholangioscopy, aut<strong>of</strong>luorescence imaging<br />
(AFI) <strong>and</strong> narrow b<strong>and</strong> imaging (NBI). These may<br />
further enhance the ability to detect malignancies in<br />
indeterminate lesions but have a limited availability <strong>and</strong><br />
require a high level <strong>of</strong> training (44). Confocal electromicroscopy<br />
has been recently introduced as an additional<br />
imaging modality. The miniprobe is used in<br />
conjunction with a cholangioscope, <strong>and</strong> it allows for the<br />
detection <strong>of</strong> specific vasculature patterns. The presence<br />
<strong>of</strong> irregular vessels predict a neoplastic process with an<br />
accuracy <strong>of</strong> 86%, a sensitivity <strong>of</strong> 83%, with a specificity<br />
<strong>of</strong> 88%. Further investigative studies are ongoing to better<br />
determine its future application (44–46).<br />
Managing Malignant Strictures<br />
Common etiologies <strong>of</strong> malignant biliary strictures<br />
include pancreatic carcinoma, ampullary carcinoma,<br />
cholangiocarcinoma, gallbladder cancer, hepatocellular<br />
carcinoma <strong>and</strong> metastatic lesions. Once a malignancy<br />
has been established, the focus switches to<br />
determine the extent <strong>of</strong> the disease <strong>and</strong> its resectability.<br />
Patients should be referred for surgical <strong>and</strong> oncologic<br />
evaluation. Immediate relief <strong>of</strong> the obstruction should<br />
be established if possible. The use <strong>of</strong> temporary plastic<br />
stents is favored in patients who may be surgical<br />
c<strong>and</strong>idates or in cases where the diagnosis is unclear.<br />
Self exp<strong>and</strong>ing metal stents (SEMS) are usually<br />
reserved for patients with unresectable disease <strong>and</strong> a<br />
life expectancy exceeding five to six months (47).<br />
Special Patient Populations: Chronic<br />
Pancreatitis, Primary Sclerosing<br />
Cholangitis <strong>and</strong> Liver Transplant Recipients<br />
Chronic pancreatitis related distal bile duct strictures<br />
deserve special attention as they account for up to 10%<br />
<strong>of</strong> all CBD strictures <strong>and</strong> carry a significant amount <strong>of</strong><br />
morbidity. Inflammation <strong>and</strong> fibrosis can make it difficult<br />
to establish adequate access during an ERCP, <strong>and</strong><br />
endoscopic management can therefore be limited. Studies<br />
suggest that the use <strong>of</strong> multiple stents may be superior<br />
to single stents in this patient population. In cases<br />
refractory to repeated stenting <strong>and</strong> endoscopic therapy,<br />
surgery may be required <strong>and</strong> is usually complicated<br />
because this patient population typically suffers from<br />
comorbid conditions <strong>and</strong> additional complications such<br />
as vascular thrombosis <strong>and</strong> liver involvement (43).<br />
In patients with primary sclerosing cholangitis<br />
(PSC), chronic inflammation leads to multiple fibrotic<br />
strictures <strong>of</strong> the entire biliary tree <strong>and</strong> eventually results<br />
in significant liver disease <strong>and</strong> cirrhosis (Figure 3).<br />
Medical therapy has not proven to be <strong>of</strong> benefit, <strong>and</strong> the<br />
use <strong>of</strong> ursodeoxycholic acid is no longer recommended.<br />
Liver transplantation is the only long-term option for<br />
Figure 2. Ischemic common bile duct stricture seen on<br />
cholangiogram with dilation <strong>of</strong> the proximal bile duct.<br />
Figure 3. Cholangiogram showing significant extrahepatic<br />
(thick arrow) <strong>and</strong> intrahepatic (thinner arrows) structuring<br />
consistent with primary sclerosing cholangitis.<br />
36<br />
PRACTICAL GASTROENTEROLOGY • JULY 2011
<strong>Diagnostic</strong> <strong>and</strong> <strong>Therapeutic</strong> <strong>Endoscopy</strong> <strong>of</strong> <strong>Biliary</strong> <strong>Diseases</strong><br />
DISEASES OF THE BILIARY TRACT, SERIES #6<br />
severe cases. Dominant extrahepatic strictures are common<br />
in PSC patients occurring in up to 50% <strong>of</strong> cases.<br />
They may lead to cholangitis, which in turn can worsen<br />
the extent <strong>of</strong> damage to the liver. Their presence is typically<br />
suspected clinically based on worsening jaundice<br />
<strong>and</strong> pruritis <strong>and</strong> increasing liver function test abnormalities.<br />
It is important to rule out a malignant process in<br />
these patients in view <strong>of</strong> the substantially increased risk<br />
<strong>of</strong> cholangiocarcinoma (8%-14% <strong>of</strong> patients) (48).<br />
Endoscopic therapy consists <strong>of</strong> dilation <strong>of</strong> the dominant<br />
stricture <strong>and</strong> extraction <strong>of</strong> any stones or sludge that may<br />
be lodged above the strictured area. Short-term stenting<br />
may be effective in a small number <strong>of</strong> patients. However<br />
stent occlusion remains a problem. Repeat dilations may<br />
be required in many cases. Stenting after balloon dilation<br />
may not have any additional benefit (49).<br />
Anastomotic strictures are common post orthotopic<br />
liver transplantation (OLT) with an incidence around<br />
5%–10%. These typically are short segment strictures<br />
<strong>and</strong> occur within one year <strong>of</strong> the transplant with early<br />
strictures resulting from technical complications <strong>of</strong> the<br />
surgery <strong>and</strong> later ones from vascular insufficiency <strong>and</strong><br />
fibrosis (50). Risk factors include tension at the anastomosis,<br />
caliber mismatch between donor <strong>and</strong> recipient<br />
ducts, <strong>and</strong> excessive use <strong>of</strong> electrocauterization for control<br />
<strong>of</strong> intra-operative bleeding (51). Endoscopic management<br />
with repeated dilation <strong>and</strong> stenting remains the<br />
treatment <strong>of</strong> choice. Newer data suggest that the use <strong>of</strong><br />
fully covered metal stents may be beneficial in these<br />
patients by spacing out the ERCPs needed <strong>and</strong> therefore<br />
decreasing costs <strong>and</strong> associated risks (52).<br />
BILE LEAKS<br />
Bile leaks occur mainly as a complication <strong>of</strong> biliary<br />
surgery, including laparoscopic cholecystectomy (up<br />
to 1.1% <strong>of</strong> cases) <strong>and</strong> cadaveric OLT. The leak can<br />
occur at the cystic duct stump or can involve the<br />
smaller ducts <strong>of</strong> Luschka. The presentation is typically<br />
acute within the first few days following surgery but<br />
may be delayed with a few cases presenting up to one<br />
month later. Imaging studies, such as an ultrasound or<br />
CT scan <strong>of</strong> the abdomen, are usually diagnostic, but<br />
the absence <strong>of</strong> a biloma on imaging does not exclude<br />
the diagnosis. Endoscopic cholangiography can establish<br />
the diagnosis in the vast majority <strong>of</strong> patients <strong>and</strong><br />
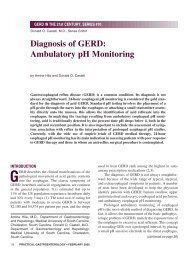
Figure 4. Cholangiogram showing extravasation <strong>of</strong> contrast<br />
diagnostic <strong>of</strong> a bile leak in a patient with recent cholecystectomy.<br />
can provide therapeutic means in the same setting (53).<br />
Figure 4 shows a cholangiogram illustrating a bile leak<br />
in a patient with a recent cholecystectomy.<br />
The therapeutic goal is to establish an area <strong>of</strong> lower<br />
resistance for the bile to flow through. This is usually<br />
achieved by the insertion <strong>of</strong> a short temporary biliary<br />
stent, therefore relieving the high transpapillary pressure<br />
gradient. A biliary sphincterotomy may be enough<br />
in certain milder cases. Response is typically measured<br />
by the clinical improvement <strong>and</strong> decreased outputs<br />
from percutaneous surgical drains. Stents are typically<br />
left in place for about four to six weeks. Bile leaks<br />
refractory to endoscopic treatment typically require<br />
surgical interventions to correct the defect (54).<br />
CONCLUSIONS<br />
In summary, much progress has been made over recent<br />
years in diagnosing <strong>and</strong> treating biliary tract disorders.<br />
Endoscopic therapy has become the predominant<br />
modality used in both the diagnosis <strong>and</strong> treatment <strong>of</strong><br />
these disorders. The future <strong>of</strong> therapeutic endoscopy<br />
promises to be quite interesting as it continues to<br />
evolve <strong>and</strong> <strong>of</strong>fer more innovative new techniques. n<br />
References<br />
1. Ko CW, Lee SP. Epidemiology <strong>and</strong> natural history <strong>of</strong> common bile duct<br />
stones <strong>and</strong> prediction <strong>of</strong> disease. Gastrointest Endosc 2002;56:165-169.<br />
2. Kaufman HS, Magnuson TH, Lillemoe KD, et al. The role <strong>of</strong> bacteria in<br />
gallbladder <strong>and</strong> common duct stone formation. Ann Surg 1989;209:584-<br />
591; discussion 591-592.<br />
3. Chung EJ, Kim MH, Lee SS, et al. Primary vs secondary common bile duct<br />
stones: apples <strong>and</strong> oranges. <strong>Endoscopy</strong> 2003;35:92; author reply 93.<br />
4. Sugiyama M, Atomi Y. Endoscopic ultrasonography for diagnosing choledocholithiasis:<br />
a prospective comparative study with ultrasonography <strong>and</strong><br />
computed tomography. Gastrointest Endosc 1997;45:143-146.<br />
PRACTICAL GASTROENTEROLOGY • JULY 2011 37
<strong>Diagnostic</strong> <strong>and</strong> <strong>Therapeutic</strong> <strong>Endoscopy</strong> <strong>of</strong> <strong>Biliary</strong> <strong>Diseases</strong><br />
DISEASES OF THE BILIARY TRACT, SERIES #6<br />
5. McKay AJ, Duncan JG, Lam P, et al. The role <strong>of</strong> grey scale ultrasonography<br />
in the investigation <strong>of</strong> jaundice. Br J Surg 1979;66:162-165.<br />
6. Deitch EA. The reliability <strong>and</strong> clinical limitations <strong>of</strong> sonographic scanning<br />
<strong>of</strong> the biliary ducts. Ann Surg 1981;194:167-170.<br />
7. Mendler MH, Bouillet P, Sautereau D, et al. Value <strong>of</strong> MR cholangiography<br />
in the diagnosis <strong>of</strong> obstructive diseases <strong>of</strong> the biliary tree: a study <strong>of</strong> 58<br />
cases. Am J Gastroenterol 1998;93:2482-2490.<br />
8. Sugiyama M, Atomi Y, Hachiya J. Magnetic resonance cholangiography<br />
using half-Fourier acquisition for diagnosing choledocholithiasis. Am J<br />
Gastroenterol 1998;93:1886-1890.<br />
9. Romagnuolo J, Bardou M, Rahme E, et al. Magnetic resonance cholangiopancreatography:<br />
a meta-analysis <strong>of</strong> test performance in suspected biliary<br />
disease. Ann Intern Med 2003;139:547-557.<br />
10. Kumar M, Prashad R, Kumar A, et al. Relative merits <strong>of</strong> ultrasonography,<br />
computed tomography <strong>and</strong> cholangiography in patients <strong>of</strong> surgical obstructive<br />
jaundice. Hepatogastroenterology 1998;45:2027-2032.<br />
11. Wyatt SH, Fishman EK. <strong>Biliary</strong> tract obstruction. The role <strong>of</strong> spiral CT in<br />
detection <strong>and</strong> definition <strong>of</strong> disease. Clin Imaging 1997;21:27-34.<br />
12. Soto JA, Alvarez O, Munera F, et al. Diagnosing bile duct stones:<br />
comparison <strong>of</strong> unenhanced helical CT, oral contrast-enhanced CT cholangiography,<br />
<strong>and</strong> MR cholangiography. AJR Am J Roentgenol 2000;175:<br />
1127-1134.<br />
13. Stockberger SM, Wass JL, Sherman S, et al. Intravenous cholangiography<br />
with helical CT: comparison with endoscopic retrograde cholangiography.<br />
Radiology 1994;192:675-680.<br />
14. Tse F, Barkun JS, Barkun AN. The elective evaluation <strong>of</strong> patients with<br />
suspected choledocholithiasis undergoing laparoscopic cholecystectomy.<br />
Gastrointest Endosc 2004;60:437-448.<br />
15. Chen CH, Tseng LJ, Yang CC, et al. The accuracy <strong>of</strong> endoscopic<br />
ultrasound, endoscopic retrograde cholangiopancreatography, computed<br />
tomography, <strong>and</strong> transabdominal ultrasound in the detection <strong>and</strong> staging <strong>of</strong><br />
primary ampullary tumors. Hepatogastroenterology 2001;48:1750-1753.<br />
16. Ang TL, Teo EK, Fock KM. Endosonography- vs. endoscopic retrograde<br />
cholangiopancreatography-based strategies in the evaluation <strong>of</strong> suspected<br />
common bile duct stones in patients with normal transabdominal imaging.<br />
Aliment Pharmacol Ther 2007;26:1163-1170.<br />
17. Hermann RE. The spectrum <strong>of</strong> biliary stone disease. Am J Surg<br />
1989;158:171-173.<br />
18. Joyce AM, Heiss FW. Endoscopic evaluation <strong>and</strong> therapies <strong>of</strong> biliary disorders.<br />
Surg Clin North Am 2008;88:1221-1240, viii.<br />
19. Frey CF, Burbige EJ, Meinke WB, et al. Endoscopic retrograde cholangiopancreatography.<br />
Am J Surg 1982;144:109-114.<br />
20. Baron TH, Harewood GC. Endoscopic balloon dilation <strong>of</strong> the biliary<br />
sphincter compared to endoscopic biliary sphincterotomy for removal <strong>of</strong><br />
common bile duct stones during ERCP: a metaanalysis <strong>of</strong> r<strong>and</strong>omized, controlled<br />
trials. Am J Gastroenterol 2004;99:1455-1460.<br />
21. Lauri A, Horton RC, Davidson BR, et al. Endoscopic extraction <strong>of</strong> bile duct<br />
stones: management related to stone size. Gut 1993;34:1718-1721.<br />
22. Siegel JH, Ben-Zvi JS, Pullano WE. Endoscopic electrohydraulic<br />
lithotripsy. Gastrointest Endosc 1990;36:134-136.<br />
23. Ponchon T, Martin X, Barkun A, et al. Extracorporeal lithotripsy<br />
<strong>of</strong> bile duct stones using ultrasonography for stone localization. Gastroenterology<br />
1990;98:726-732.<br />
24. Garg PK, T<strong>and</strong>on RK, Ahuja V, et al. Predictors <strong>of</strong> unsuccessful mechanical<br />
lithotripsy <strong>and</strong> endoscopic clearance <strong>of</strong> large bile duct stones. Gastrointest<br />
Endosc 2004;59:601-605.<br />
25. Chen YK, Pleskow DK. SpyGlass single-operator peroral cholangiopancreatoscopy<br />
system for the diagnosis <strong>and</strong> therapy <strong>of</strong> bile-duct disorders:<br />
a clinical feasibility study (with video). Gastrointest Endosc 2007;65:832-<br />
841.<br />
26. Neuhaus H. Endoscopic <strong>and</strong> percutaneous treatment <strong>of</strong> difficult bile duct<br />
stones. <strong>Endoscopy</strong> 2003;35:S31-S34.<br />
27. Horiuchi A, Nakayama Y, Kajiyama M, et al. <strong>Biliary</strong> stenting in the management<br />
<strong>of</strong> large or multiple common bile duct stones. Gastrointest<br />
Endosc71:1200-1203 e2.<br />
28. Freeman ML, Nelson DB, Sherman S, et al. Same-day discharge after endoscopic<br />
biliary sphincterotomy: observations from a prospective multicenter<br />
complication study. The Multicenter Endoscopic Sphincterotomy (MESH)<br />
Study Group. Gastrointest Endosc 1999;49:580-586.<br />
29. Wojtun S, Gil J, Gietka W, et al. Endoscopic sphincterotomy for choledocholithiasis:<br />
a prospective single-center study on the short-term <strong>and</strong> longterm<br />
treatment results in 483 patients. <strong>Endoscopy</strong> 1997;29:258-265.<br />
30. Saito M, Tsuyuguchi T, Yamaguchi T, et al. Long-term outcome <strong>of</strong> endoscopic<br />
papillotomy for choledocholithiasis with cholecystolithiasis. Gastrointest<br />
Endosc 2000;51:540-545.<br />
31. Boerma D, Rauws EA, Keulemans YC, et al. Wait-<strong>and</strong>-see policy or<br />
laparoscopic cholecystectomy after endoscopic sphincterotomy for bileduct<br />
stones: a r<strong>and</strong>omised trial. Lancet 2002;360:761-765.<br />
32. Bismuth H, Majno PE. <strong>Biliary</strong> strictures: classification based on the principles<br />
<strong>of</strong> surgical treatment. World J Surg 2001;25:1241-1244.<br />
33. Al-M<strong>of</strong>leh IA, Aljebreen AM, Al-Amri SM, et al. Biochemical <strong>and</strong> radiological<br />
predictors <strong>of</strong> malignant biliary strictures. World J Gastroenterol<br />
2004;10:1504-1507.<br />
34. Mann DV, Edwards R, Ho S, et al. Elevated tumour marker CA19-9: clinical<br />
interpretation <strong>and</strong> influence <strong>of</strong> obstructive jaundice. Eur J Surg Oncol<br />
2000;26:474-479.<br />
35. Krishnamurthy GT, Turner FE. Pharmacokinetics <strong>and</strong> clinical application<br />
<strong>of</strong> technetium 99m-labeled hepatobiliary agents. Semin Nucl Med<br />
1990;20:130-149.<br />
36. Prytz H, Keiding S, Bjornsson E, et al. Dynamic FDG-PET is useful for<br />
detection <strong>of</strong> cholangiocarcinoma in patients with PSC listed for liver transplantation.<br />
Hepatology 2006;44:1572-1580.<br />
37. DeWitt J, Misra VL, Leblanc JK, et al. EUS-guided FNA <strong>of</strong> proximal biliary<br />
strictures after negative ERCP brush cytology results. Gastrointest<br />
Endosc 2006;64:325-333.<br />
38. Saifuku Y, Yamagata M, Koike T, et al. Endoscopic ultrasonography can<br />
diagnose distal biliary strictures without a mass on computed tomography.<br />
World J Gastroenterol 16:237-244.<br />
39. Jailwala J, Fogel EL, Sherman S, et al. Triple-tissue sampling at ERCP in<br />
malignant biliary obstruction. Gastrointest Endosc 2000;51:383-390.<br />
40. Stewart CJ, Mills PR, Carter R, et al. Brush cytology in the assessment <strong>of</strong><br />
pancreatico-biliary strictures: a review <strong>of</strong> 406 cases. J Clin Pathol<br />
2001;54:449-455.<br />
41. Kipp BR, Stadheim LM, Halling SA, et al. A comparison <strong>of</strong> routine cytology<br />
<strong>and</strong> fluorescence in situ hybridization for the detection <strong>of</strong> malignant<br />
bile duct strictures. Am J Gastroenterol 2004;99:1675-1681.<br />
42. Seo DW, Lee SK, Yoo KS, et al. Cholangioscopic findings in bile duct<br />
tumors. Gastrointest Endosc 2000;52:630-634.<br />
43. Judah JR, Draganov PV. Endoscopic therapy <strong>of</strong> benign biliary strictures.<br />
World J Gastroenterol 2007;13:3531-3539.<br />
44. Terheggen G, Neuhaus H. New options <strong>of</strong> cholangioscopy. Gastroenterol<br />
Clin North Am 39:827-844.<br />
45. Meining A. Confocal endomicroscopy. Gastrointest Endosc Clin N Am<br />
2009;19:629-35.<br />
46. Wallace MB, Fockens P. Probe-based confocal laser endomicroscopy. Gastroenterology<br />
2009;136:1509-1513.<br />
47. Mad<strong>of</strong>f DC, Wallace MJ. Palliative treatment <strong>of</strong> unresectable bile duct cancer:<br />
which stent? which approach? Surg Oncol Clin N Am 2002;11:923-<br />
939.<br />
48. Tischendorf JJ, Geier A, Trautwein C. Current diagnosis <strong>and</strong> management<br />
<strong>of</strong> primary sclerosing cholangitis. Liver Transpl 2008;14:735-746.<br />
49. Kaya M, Petersen BT, Angulo P, et al. Balloon dilation compared to stenting<br />
<strong>of</strong> dominant strictures in primary sclerosing cholangitis. Am J Gastroenterol<br />
2001;96:1059-1066.<br />
50. Verdonk RC, Buis CI, Porte RJ, et al. Anastomotic biliary strictures after<br />
liver transplantation: causes <strong>and</strong> consequences. Liver Transpl 2006;12:726-<br />
735.<br />
51. Hisatsune H, Yazumi S, Egawa H, et al. Endoscopic management <strong>of</strong> biliary<br />
strictures after duct-to-duct biliary reconstruction in right-lobe living-donor<br />
liver transplantation. Transplantation 2003;76:810-815.<br />
52. Kim JH, Gwon DI, Ko GY, et al. Temporary Placement <strong>of</strong> Retrievable<br />
Fully Covered Metallic Stents versus Percutaneous Balloon Dilation in the<br />
Treatment <strong>of</strong> Benign <strong>Biliary</strong> Strictures. J Vasc Interv Radiol.<br />
53. Wu YV, Linehan DC. Bile duct injuries in the era <strong>of</strong> laparoscopic cholecystectomies.<br />
Surg Clin North Am 90:787-802.<br />
54. Zyromski NJ, Lillemoe KD. Current management <strong>of</strong> biliary leaks. Adv Surg<br />
2006;40:21-46.<br />
38<br />
PRACTICAL GASTROENTEROLOGY • JULY 2011