Requirement of Pre-Cataract Surgery Authorization - Philippine ...
Requirement of Pre-Cataract Surgery Authorization - Philippine ...
Requirement of Pre-Cataract Surgery Authorization - Philippine ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
' (AV/in/i/k- nfitic I'liilipjiiiicK/V<br />
I?"PHILIPPINE HEALTH INSURANCE CORPORATION&. ..\^<br />
^..,|;it-C'L-ii[ic Ruikhnii. 7tW Shav. Heiilvoml. Pas," Oily* * @''<br />
!:i|pHc.ilililine J4I-7-IJ4 v^-jij.l^-.nlih.-n^nli<br />
PhilHcullli Ciiciil.ii-<br />
N,. 0Sq s-nij<br />
- Jj,<br />
TO:ALL ACCREDITED HEALTH CAKE PROVIDERS. PH1LHEALTH<br />
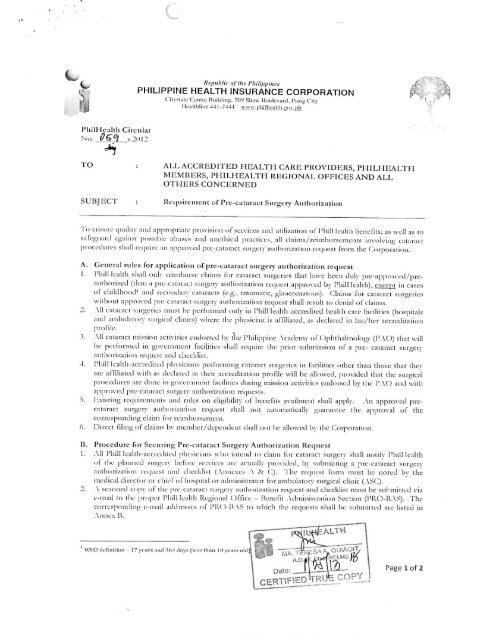
SUBJECT:Rei[iiiic-mciit <strong>of</strong> Ptc-c.unnict <strong>Surgery</strong> Aullioiizatiou<br />
MEMRERS, PI I1LHEALTH REGIONAL OFFICES AND ALL<br />
OTHERS CONCERNED<br />
1 o cnsuic qiulnv ;inJ approp, in le provision <strong>of</strong> sciviccs and ulilization r I'hill ij.--.ilt] @ benefits. n.s well as to<br />
safeguard iiji.iinsl pos-iblt- .iliiist-s and iim-llnc.i! praclicu-s, a!! claims, ccimbitj-funicnu involvmi; mlaracl<br />
A. GciK-ml luK:.^ loi ;i|iplit:;ilion <strong>of</strong> prc-c;il;uac[ surgciv aullioiiziiliini ict|uest<br />
1.rlilllk-allh sliiill cnly icimbm-si- claims I'm cataracl'snriic-i-n-s lhat have been duly pie-appi.,vcj/pi-eamliori/CLl<br />
rIhi-Li a pic-calai-acl suiyci-v -aullion/.alion icc|ncsl appiovcd b\ Pliill IcaltliK CNCcpl In cases<br />
<strong>of</strong> childhood' and scc.ndary canuacls ft-.g-., uaumalic, -laiiconialous). Clainii for calaracl sni-ciics<br />
M-ilhoul approved pu--c.u-.liM siiiiyiv anlhoMZalion ic^iicst shall ic-sult to denial <strong>of</strong> claims.<br />
2 Ml caiaiacl sui^eiic-s inusl be pcrfoimed only in Tlnll ieallh-accietlilL-d health care lacililies (hiisptL-.ils<br />
and ambulaloi-y sln^ical chnicsi -hc-ie the pilisician is alT.lialcd, .is dc-claicd in his 'her accicdltalion<br />
pi<strong>of</strong>lle<br />
3. All cararart mission activ nics endorsed by 11 it- <strong>Philippine</strong> Academv <strong>of</strong>f. )[-)hthalmolo;^- [^ACJJ that u ill<br />
Lie perUiimc-i.1 in e;o\ ernmcnl lacililies shall iee|niie the prior submission <strong>of</strong> a pie- cataracl suiyerv<br />
anlhori/alion leijuest and checklist.<br />
@I. I'hill lealth-accreeliled ph\sicians pcifoi miiiL'. calaiact surgeries in facilities other than those dial lliev<br />
are affiliated with as eleelaied in iheir accredilalion piollle will be allowed, provided that the smijjcal<br />
proceelures ale done in governmenl facilities dnrine, missi.)n activities endorsed by the PAO and with<br />
S. l-xistin.c; lequiiemenls and li.iles on eliBibllitv <strong>of</strong> benelils availnicnt shall apply. An appiovcd precalaracl<br />
snriiCiy aulhon/.aiion i-ecjuest shall not anlomalically L'.n.uanlee the ap[in.n-al <strong>of</strong> the<br />
corjespoiKlin.u el-ami foi reimbnrsemenl<br />
(i. Direct tiling <strong>of</strong> claims bv membci/dependent shall not be allowed by the Coipoiation.<br />
D. Piocceliue for Secunni; Pic-c-.itaiael Siifety Aullioiizalioii Rcqucsl<br />
1 All I'hill leallh-acciediled phvsieians ho intend lo elaun loi cataracl suigeri shall notify I'hill lealth<br />
<strong>of</strong> ihe planned smSni before services aie acuiallv |'rovided, bv submiltmi; a pre-cataiact surL-cry<br />
aulhoii/ation iee]uesl and checklist (Annexes \ & !.]. Ihe rei|iiesl bun must be noted liy the<br />
meelical clnccloi r,r chief <strong>of</strong> hospnal oi aelmtnistratoi for ambulatory smgical clinic ( \SCj.<br />
2.\ scanned cop\- <strong>of</strong> ihe pie-calaract surgery auihon/.auon ictjiiesl anel checklist must be sukmittcel via<br />
e-mail lo ihe propel I'hill leallh Regional (Mliee - Bencln Adminisli alion Section (PRO-BASj. The<br />
coiicspondmg e-mail addresses <strong>of</strong> PK( l-BAS lo which the requests shall be submitted are listed in<br />
\nne-. B.<br />
W1"@1?'-"@"-""-11"@W-:S<br />
F^t^ALTK 1<br />
fe^ouiAWy<br />
Dale:LL_"__\J'-'@<br />
CERTSFlEpJTB^CO?;;<br />
IlWJil2L- | Page 1 <strong>of</strong> 2
ll-<br />
3. Ml ncccs^.in inlonmium in the pi(--cni:ii;ia suryciy iHithru-izsitiun i.cquest ;md checklist must be<br />
Slli'jjIh The rUOs slmll nut process ic^ucsis with liicrnnplctc nifbimafioii ;ind will reiuin the<br />
k-cisiMii iIk-icoii xvilliin fn-L- (5) woikiiu.; d.iys fimn iLCCipt <strong>of</strong> llu- c
_ p.hjhnihli 2L>a-I<br />
Republic <strong>of</strong> the I'lliliptrinvs<br />
PHILIPPINE HEALTH INSURANCE CORPORATION<br />
Cinsuk- 011110 Lluikling. 7()
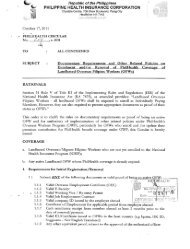
PRE-CATARACT SURGERY AUTHORIZATION REQUEST<br />
(Adult <strong>Cataract</strong>)<br />
Date <strong>of</strong> request:<br />
This is to request approval for my patient ___<br />
will undergo cataract operation at _______<br />
(name <strong>of</strong> patient)<br />
(age)<br />
and shall claim reimbursement from PhilHealth, under the terms and conditions as agreed for availment<br />
(name <strong>of</strong> hospital/ASC)<br />
<strong>of</strong> the <strong>Cataract</strong> Benefit Package.<br />
Requested by:<br />
Noted by:<br />
Name & Signature <strong>of</strong> Physician Medical Center Chief/Medical Dir. /<br />
A5C Administrator or any authorized personnel<br />
This Portion to be filled-out by PhilHealth<br />
?Approved*<br />
"Patient is eligible at the time <strong>of</strong> approval <strong>of</strong> pre-cataract surgery authorization.<br />
?Disapproved<br />
Reason:___^-<br />
Name and Signature <strong>of</strong> BAS Head<br />
Tracking number<br />
Date signed<br />
.TH<br />
|p-s<br />
CERT!<br />
Dnl:<br />
A]J2...<br />
s~&<br />
: copy
No.<br />
1<br />
2<br />
3<br />
4<br />
5<br />
6<br />
7<br />
S<br />
q<br />
10<br />
n<br />
12<br />
13<br />
14<br />
15<br />
16<br />
17<br />
18<br />
19<br />
20<br />
PRO1<br />
Region<br />
PROM<br />
PROIMA<br />
PROMIB<br />
PROIVA<br />
PROIVB<br />
PROV<br />
PROVI<br />
PROVII<br />
PROVIM<br />
PROIX<br />
PROX<br />
PROXI<br />
PROXII<br />
PROCAR<br />
PROCARAGA<br />
PROARMM<br />
PRONCR-North<br />
PRONCR-South<br />
PRONCR-Central<br />
EMAIL ADDRESSES FOR PRE-CATARACT SURGERY AUTHORIZATION<br />
c ainis.prrjl(S)philhealtlT.Rov.ph<br />
doknethinJyahoo.com<br />
c aims.pio3(n.'pliilhealth.EOv.ph<br />
benefil.pra3bjfflphilhealth.gov.ph<br />
c ainis.pirj4a(ipphithealthRov.gh<br />
c aims.pm4b(ffiphilhealth.ftovph<br />
hcmd.pro5(5)phi!heali:h.e;ov.ph<br />
pro&.hcclmd[tpginail.com<br />
^nns.pro7(aiphilheallh.Kov.|jh<br />
c ainis.pio8(5)philhealthcovph<br />
rossanapara^jjya(s1vahoo.com<br />
mmalcnto(S5philheaKh.ROv.ph;ba5.prolOiniphilhealth.gov.ph<br />
cubenmd2003(5>yahoo.com<br />
claims.prol2iSphilhealth.gov.ph<br />
claims.|iioca[(5>phi1health.gov.ph<br />
hcdmd.procaiaRaiaphilhealth.Eov.ph<br />
c aims.oioarmmiR'plnlhealthBov.oh:hcdmcf.i]ioarmm(cDohilheaUh.ROv.Dh<br />
c aims.promlat^philhealth.Rovjjh<br />
r aimspiolp@pliillisalth.ROvph<br />
c aims.procic(5>philhealtht;ov.i3h<br />
E-mailAddress<br />
m @ UiAOIT
yl<br />
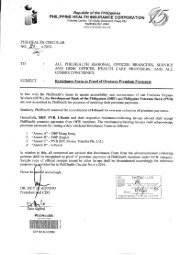
Annex C. Flowchart for pre-cataract surgery authorization request<br />
:oni|)li_.lerf Checklist and request for<br />
;ur[iciy,-Hilh.:.ri7,-i[ion to PHCI-DAS<br />
PR0-UA5.WI0WS<br />
Completeness<strong>of</strong><br />
Cl1Oib,lilV.."..Hi,,l<br />
CllXU<br />
nfoi 1,1110<br />
i,ifl<br />
Fni<br />
lir,<br />
IlL'Cl.llit.JP.1HCT1I<br />
1<br />
I@<br />
I rai O-EJASdotU<br />
I fa<br />
I Jls<br />
[z<br />
ir,. i<br />
o P>" \Sh<br />
i ll<br />
ll for<br />
>EJArj 5Ciiii5 Ihe doonner<br />
isliis/li^rinrlinlp<br />
.- _.-*<br />
F;qu&nALTH<br />
TRO-B^S<br />
adjudicHtoie<br />
I<br />
ithed.it.i.sc.iris<br />
'i f \ l" i on<br />
a..achCc