li1 - Philippine Health Insurance Corporation
li1 - Philippine Health Insurance Corporation li1 - Philippine Health Insurance Corporation
Name of Patient Write the complete name of the patient starting wirh last. Erst ::nd middle name. It should be separated by :i comma Extensions such as (but not limited to tine following) ]r., Sr., IJJ should be indicated after the Eisc Patient is the Member If patient is Llic member, check [he appiapime box and chen proceL'd to itc-m 9 Patient is a Dependent If pauent is a dependent (to be filled out if patient is dependent) Check the appropiuUe box if patient is :i child, spouse or parent of the member. Reminder If piiticnt is ky;d JeptndenL uf the member, the patient's name should appeal in the MDIt If not, attach applicable suppoiting documents as proof of dependency Certification of Member Signature over printed name of member The membei -affixes his/hci signature over printed name ceitih'ing tliat all information suppbed m Part I are true and cotrecr and granting consent 10 PhilHealth to use die supplied information for any legal purpose. In case die member is a niinoi 01 a survivor-child, a representative (legal guardian) will also counteisign using the membei representative portion. If die legal guaidian is not duly indicated in die JNIDR, a copy of u judicial oider shall be attached to die claim. Date signed The membei indicates the date when be/she signed die certificate following die prescribed format for date Signature overprinted name of member's representative ' An audiorized representative of die member may sign on lus/her btlv.ilf. Date signed The audiorized representaove of die pciueni; indicates the date when he/she signed on behalf of the patient following the prescribed form.it foi date. Relationship of the Representative to the member Check die appropriate box whether die representative of the member is Ins/her cliild (must be 1 S years old :md above), spouse, paienl and guardian/next nf kin Reason for signing on behalf of the member Indicate the reuson for signing on behalf ol" (.he membei such as: PI) Member is Abroad / Out-of-Towu; (2) Member is incapacitated and l'3) Other reasons F
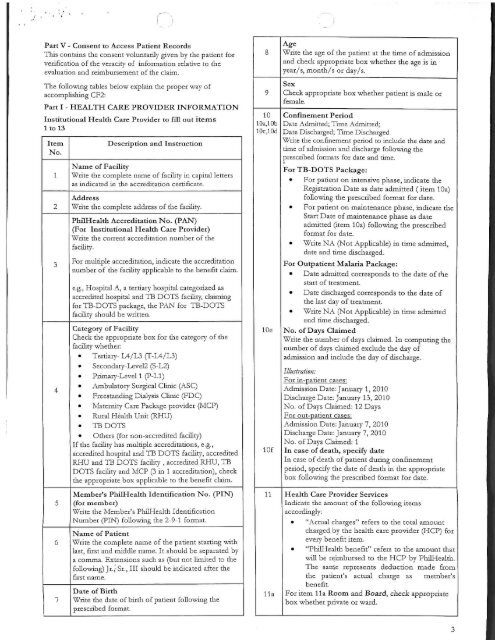
Part V - Consent to Access Patient Records Tins contains the consent voluntarily given by the patient lor verification of the veracity of information relative to the evaluation and reimbursement of the claim. The following tables below explain the proper way of accomplishing CF2: Part I - HEALTH CARE PROVIDER INFORMATION Institutional Health Care Provider to fill our items 1 to 13 No. 1 2 3 4 DescriptionandInstruction NameofFacility Writethecompletenameoffacilityincapitalletters asindicatedhidieaccreditationcertificate. Writediecompleteaddressofthefacility. e.g.,HospitalA,aternaryhospitalcategorizedas accreditedhospitalandTBDOTSfacility,claiming forTB-DOTSpackage,diePANforTB-DOTS facilityshouldbewritten. CategoryofFacility Checkdieappiopnateboxfordiecategoryofdie facilitywhether: @Tertiary-L4/L3fT-L4/L3) @Secondary-Level?(S-L2) @Pnniaiy-Level1fP-LlJ @AmbulatoiySurgicalClinic(ASC) @FreestandingDialysisClime(FDC) @MaternityCarePackageprovidei(MCP) @RuralHealthUnit(RHU) @TBDOTS @Otliers(fornon-accieditedfacility) Ifthefacilityhasmultipleaccreditations,e.g., accreditedhospitalandTBDOTSfacility,accredited RHUandTBDOTSfacility,accreditedRHU,TB DOTSfacilityandMCP(3miaccreditation),check theappropriateboxapplicabletodiebenefitclaim 10 Oa.lOh 0c,10d Age WiiLt; die ;ige of the patient at the time of admission and check appropriate box whether the age is in year/s, month/s or day/s "heck appropriate box whether patient is male or Confinement Period Date Admitted. Tune Admitted; Date Discharged. Time Discharged Write the confinement pei:iod to include the date and time of admission and discharge following the piescnbed formats lor date and time. ForTB-DOTS Package: @For patient on intensive phase, indicate die Registration Date as date admitted (item 10a) following die prescribed format for date. @For patient on maintenance phase, indicate die Start Date of maintenance phase as date admitted (item 10a) following the prescribed format far date. @Write NA (Not Applicable) in time admitted, date and time discharged. For Outpatient Malaria Package: @Date admitted corresponds to die date of the start of tieatment. @Date discharged corresponds to die date of the last day of treatment. @"Write NA ('Not Applicable) in time admitted and time discharged. No. of Days Claimed Write die number of days claimed. In computing the number of days claimed exclude the day of admission and include the day of discharge. Illniiration: For in-patient cases: Admission Date: January 1, 2010 Discharge Date: January 13, 2010 No of Days Claimed: 12 Days For Qut-pAllent cases: Admission Date: January 7, 2010 Discharge Date: January 7, 2010 No. of Days Churned. 1 In case of death, specify date In c:ise of death of patient during confinement penod, specirv the dnte of death in the appropriate box following die prescribed foimut for date 5 6 Member'sPhilHealthIdentificationNo.(PIN) (formember) WritetheMember'sPhilHealthIdentification Number(PIN)followingthe2-9-1form,it NameofPatient Writediecompletenameofthepatientstartingwith last,Cistandmiddlename.Itshouldbeseparatedby acomnu.Extensionssuchas(butnotlimitedtothe following)Jr.,Sr.,IIIshouldbeindicatedaftcidie firstname. "CC7ntethedate,ofbirthofpatientfollowingthe prescribedformat Health Care Provider Services Indicate die amount of the following items accordingly: @"Actual charges" refeis ro the total amount charged by the health caie provider (HCP) for every benefit item. @"PhilHenlth benefit" refers to the amount that will be reimbursed to the HCP by PhilHtaltli. The s.ime represents deduction made from die pa dent's actual chaige as member's benefit. For item lla Room and Board, check Appropriate box whether private or ward.
- Page 1 and 2: Republic of the Philippines PHILIPP
- Page 3 and 4: MCP[2 | iPhilHealth I Your Partner
- Page 5 and 6: @fc^ PhilHealtn MBramier Your Partn
- Page 7: GUIDELINES ON THE PROPER ACCOMPLISH
- Page 11 and 12: Note Check the box provided if offi
- Page 13: theictusonthefirstminute-andfive(5)
Part V - Consent to Access Patient Records<br />
Tins contains the consent voluntarily given by the patient lor<br />
verification of the veracity of information relative to the<br />
evaluation and reimbursement of the claim.<br />
The following tables below explain the proper way of<br />
accomplishing CF2:<br />
Part I - HEALTH CARE PROVIDER INFORMATION<br />
Institutional <strong>Health</strong> Care Provider to fill our items<br />
1 to 13<br />
No.<br />
1<br />
2<br />
3<br />
4<br />
DescriptionandInstruction<br />
NameofFacility<br />
Writethecompletenameoffacilityincapitalletters<br />
asindicatedhidieaccreditationcertificate.<br />
Writediecompleteaddressofthefacility.<br />
e.g.,HospitalA,aternaryhospitalcategorizedas<br />
accreditedhospitalandTBDOTSfacility,claiming<br />
forTB-DOTSpackage,diePANforTB-DOTS<br />
facilityshouldbewritten.<br />
CategoryofFacility<br />
Checkdieappiopnateboxfordiecategoryofdie<br />
facilitywhether:<br />
@Tertiary-L4/L3fT-L4/L3)<br />
@Secondary-Level?(S-L2)<br />
@Pnniaiy-Level1fP-LlJ<br />
@AmbulatoiySurgicalClinic(ASC)<br />
@FreestandingDialysisClime(FDC)<br />
@MaternityCarePackageprovidei(MCP)<br />
@Rural<strong>Health</strong>Unit(RHU)<br />
@TBDOTS<br />
@Otliers(fornon-accieditedfacility)<br />
Ifthefacilityhasmultipleaccreditations,e.g.,<br />
accreditedhospitalandTBDOTSfacility,accredited<br />
RHUandTBDOTSfacility,accreditedRHU,TB<br />
DOTSfacilityandMCP(3miaccreditation),check<br />
theappropriateboxapplicabletodiebenefitclaim<br />
10<br />
Oa.lOh<br />
0c,10d<br />
Age<br />
WiiLt; die ;ige of the patient at the time of admission<br />
and check appropriate box whether the age is in<br />
year/s, month/s or day/s<br />
"heck appropriate box whether patient is male or<br />
Confinement Period<br />
Date Admitted. Tune Admitted;<br />
Date Discharged. Time Discharged<br />
Write the confinement pei:iod to include the date and<br />
time of admission and discharge following the<br />
piescnbed formats lor date and time.<br />
ForTB-DOTS Package:<br />
@For patient on intensive phase, indicate die<br />
Registration Date as date admitted (item 10a)<br />
following die prescribed format for date.<br />
@For patient on maintenance phase, indicate die<br />
Start Date of maintenance phase as date<br />
admitted (item 10a) following the prescribed<br />
format far date.<br />
@Write NA (Not Applicable) in time admitted,<br />
date and time discharged.<br />
For Outpatient Malaria Package:<br />
@Date admitted corresponds to die date of the<br />
start of tieatment.<br />
@Date discharged corresponds to die date of<br />
the last day of treatment.<br />
@"Write NA ('Not Applicable) in time admitted<br />
and time discharged.<br />
No. of Days Claimed<br />
Write die number of days claimed. In computing the<br />
number of days claimed exclude the day of<br />
admission and include the day of discharge.<br />
Illniiration:<br />
For in-patient cases:<br />
Admission Date: January 1, 2010<br />
Discharge Date: January 13, 2010<br />
No of Days Claimed: 12 Days<br />
For Qut-pAllent cases:<br />
Admission Date: January 7, 2010<br />
Discharge Date: January 7, 2010<br />
No. of Days Churned. 1<br />
In case of death, specify date<br />
In c:ise of death of patient during confinement<br />
penod, specirv the dnte of death in the appropriate<br />
box following die prescribed foimut for date<br />
5<br />
6<br />
Member'sPhil<strong>Health</strong>IdentificationNo.(PIN)<br />
(formember)<br />
WritetheMember'sPhil<strong>Health</strong>Identification<br />
Number(PIN)followingthe2-9-1form,it<br />
NameofPatient<br />
Writediecompletenameofthepatientstartingwith<br />
last,Cistandmiddlename.Itshouldbeseparatedby<br />
acomnu.Extensionssuchas(butnotlimitedtothe<br />
following)Jr.,Sr.,IIIshouldbeindicatedaftcidie<br />
firstname.<br />
"CC7ntethedate,ofbirthofpatientfollowingthe<br />
prescribedformat<br />
<strong>Health</strong> Care Provider Services<br />
Indicate die amount of the following items<br />
accordingly:<br />
@"Actual charges" refeis ro the total amount<br />
charged by the health caie provider (HCP) for<br />
every benefit item.<br />
@"PhilHenlth benefit" refers to the amount that<br />
will be reimbursed to the HCP by PhilHtaltli.<br />
The s.ime represents deduction made from<br />
die pa dent's actual chaige as member's<br />
benefit.<br />
For item lla Room and Board, check Appropriate<br />
box whether private or ward.


