li1 - Philippine Health Insurance Corporation
li1 - Philippine Health Insurance Corporation
li1 - Philippine Health Insurance Corporation

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Republic of the <strong>Philippine</strong>s<br />
PHILIPPINE HEALTH INSURANCE CORPORATION<br />
Cilvslale Centre Building. 7(H> Shatv Blvd.. Pasig Cit\<br />
PHILHEALTH CIRCULAR<br />
N0./2. s.2010<br />
TO:ALLACC<br />
SUBJECT<br />
ALL ACCREDITED HEALTH CARE PROVIDERS<br />
(INSTITUTIONS AND PROFESSIONALS), ALL MEMBERS AND<br />
EMPLOYERS, ALL PHILHEALTH OFFICES AND ALL OTHERS<br />
CONCERNED<br />
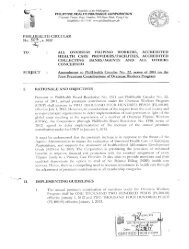
ENHANCED PHILHEALTH CLAIM FORMS<br />
For operational efficiency and to reduce administrative cost for both the <strong>Corporation</strong> and its partner<br />
stakeholders, the herein attached enhanced Pbil<strong>Health</strong> Claim Forms 1, 2 and 3 are issued. These<br />
forms shall be used for ail types of claims to include confinements, packages and out-patient<br />
services.<br />
For veriiication purposes, National Tuberculosis Program (NTP) card are still required for all TB-<br />
DOTS package claims. Providers are also advised to fill-out Part Tl of Claim Form 3 for Maternity<br />
Care Package (MCP) claims.<br />
In order to give ample time to prepare and consume old forms, these forms shall be used for all<br />
types of reimbursements effective admission date September 1. 2010.<br />
The new forms to include the guidelines on proper filling-out may be downloaded from the official<br />
Corporate website (wNvvv.philhcalrh.gov.ph)<br />
All issuances inconsistent hereof are hereby effectively repealed accordingly.<br />
For strict Gonipliiince.<br />
'
'Phil<strong>Health</strong><br />
;:::i"i:-"::iii \btir }*urtitt;-r in <strong>Health</strong>,_, . _<br />
L..-i:..i;:^{Claim Form)<br />
""@@'"revised February 2010<br />
IMPORTANT REMINDERS:<br />
PLEASE WRITE IN CAPITAL LETTERS AND CHECK THE APPROPRIATE BOXES.<br />
For local confinement, this form together with CF2 and other supporting documents should be filed within GO DAYS from dale of discharge.<br />
For confinement abroad, this form together with other supporting documents should be filed within 180 DAYS from date of discharge.<br />
Only one (I) original copy of this Form is required per claim application/availment.<br />
All information required in this form are necessary and claim forms with incomplete information shall not be processed.<br />
FALSE / INCORRECT INFORMATION OR MISREPRESENTATION SHALL BE SUBJECT TO CRIMINAL, CIVIL OR ADMINISTRATIVE LIABILITIES.<br />
1. Phil<strong>Health</strong> Identification No. (PIN):<br />
3. Name of Member<br />
PART I - MEMBER and PATIENT INFORMATION<br />
(Member/Representative to Fill out all items with the assistance of (he <strong>Health</strong> Care Provider)<br />
JI - I I I I I I I I I [-1I 2. Member Category:<br />
T' -'orm may be reproduced and is NOT FOR SALE<br />
CF1<br />
[^Employed| | Sponsored<br />
Drl,',"""@D0@<br />
Last NameFirst Name<br />
Middle Name(example Dela Cruz. Juan Jr., Sipag)r~||nd,viduallynufetime<br />
1@'paying'@'<br />
4. Mailing Address:<br />
5. Date of Birth:<br />
(House Number & Name of Street)<br />
t)(Barangay)(Month)(Day)(Year)<br />
(City/Municipality)<br />
6.Contact Information (if available):<br />
E-mail Address:<br />
(Province)<br />
Mobile No..<br />
7.Name of Patient-<br />
8 | | Patient is the Membei<br />
Qpatient is a Dependent<br />
Last Name<br />
Middle Name (example: Dela Cruz, Juan Jr., Sipag)<br />
I. CERTIFICATION OF MEMBER:f~' r"<br />
/ hereby certify that the herein information (ire true and correct and may be used for any legal purpose.<br />
Q ChildQ Parent<br />
j [spouse<br />
Signature Over Printed Name of Member<br />
Signature Over Printed Name of Member's Representative 10.Relationship of the Representative to the Member'<br />
I i I - LlJ - I i i i IDchili) [>arent<br />
Date Signed (rnonlh-day-year)Dale Signed (rnonlh-day-year) Dale Signed (rnonlh-day-year) Date Signed (rnonlh-day-yea,)QSpouse[^Guardian / tatof<br />
11 Reason for Signing on Behalf of the Member:<br />
{^Member is Abroad / Out-of-Town[^Member is IncapacitatedQother Reasons:<br />
PART II - EMPLOYER'S CERTIFICATION (for employed members only)<br />
LPhilHealtfi Employer No (PEN):[<br />
I I I I I 1 I 1-11 2. Contact No.:<br />
3. Business Name and Official Address:<br />
(Business Name of Employer)<br />
(Building Number and Street Name)<br />
{City / Municipality)(Province)(ZIP Code)<br />
4. CERTIFICATION OF EMPLOYER-<br />
This is to certify that all monthly premium contributions for and in behalf of the member, while employed in this company,<br />
including the applicable three (3) monthly premium contributions within the past six (6) months period prior to the first day oj this<br />
confinement, have been deducted/collected and remitted to Phil<strong>Health</strong>, and that the information supplied by the member or his/her<br />
representative on Part I are consistent with our available records.<br />
_ Signalure_OxejPr[nled_HamspfEmployery_AuJhoNzedRep;esenjajive Official Capacity/DesignationDate Signed [mqnth-clay-yeafl_<br />
(For Phil<strong>Health</strong> use only)!
MCP[2 |<br />
iPhil<strong>Health</strong><br />
I Your Partner hi Hvuith<br />
;:@@@.:@@ ::.@@(Claim Form)<br />
IMPORTANT REMINDERS:<br />
PLEASE WRITE IN CAPITAL LETTER5 AND CHECK THE APPROPRIATE BOXES<br />
For local confinement, mis form together with CF1 and other supporting document should be filed within GO DAYS from date of discharge<br />
FALSE / INCORRECT INFORMATION OR MISREPRESENTATION SHALL BE SUBJECT TO CRIMINAL, CIVIL OR ADMINISTRATIVE LIABILITIES<br />
PART I - PROVIDER INFORMATION (Institutional <strong>Health</strong> Care Provider to fill out items 1 to 13)<br />
This forn. ,,iay be reproduced and is NOT FOR SALE<br />
si" I I I I I I I I I I I I I<br />
(For PhilHe.lthu.* only)<br />
CF2<br />
3PhilHeallfi Accr-diialion No (PAN): I I I I I I I I I I-1. Calegoiy of Racilily<br />
{hi-tiluiion-IHealU. Car. Provider)Q -_u /L3 rj ASC g RH(J<br />
5PhHHeallh [dentificaticn No (PIHJ:|_LJ " I I I I I I I I I I " UQ S-L2 Q FDC Q TB DOTS<br />
@1. Calegoiy of Facility<br />
[] T-L-WL3 [] ASC[]RHU<br />
J ~ I1? S-L2Q FDC[3TB DOTS<br />
6MameofPaiieni@@@ ~7^7^_^7<br />
n p-li n mcp n ______<br />
Lasl NameFirsl NameMiddle Name (example Dela Cruz. Juan Jr.. Sipag}<br />
7 DateofBirih I t I ~ 1 i 1 ~ | i i i | 8 Age || Year/s [] Month/s [] Day/s [] 9. Sex [] Male [] Fern<br />
10. Confinement Period<br />
(monlh-day-ycar)<br />
a. Dale Admitted ! i I - |_|_J - | ii @ |b Time Admitted ]___J AM |j PMe Mo of Days Claimed ||<br />
.DaleAdi nilled Iil-lil-liii1<br />
bTimeAdmitted]___<br />
|AM<br />
(monlh-djy-year) (monlh-djy-year)<br />
c. Date Discharged [_jj - |_jj - | ,, , |d Time Discli^rgerJ-1| AM || PMf In c^Ge of Dealh, |_J - [_jj - |_j_<br />
.DateDis charged LJ-LJ-LllJ<br />
|AM<br />
(month-day-year) (mcnlh-day-year)specify date(nionlli-day-year)<br />
11.HeotlhCareProviderServices<br />
aRoomandBoardPrivate|IWardII<br />
ActualCharges<br />
Phil<strong>Health</strong>Benefit<br />
FarPliilHeatihUedOn^<br />
(Adjustments/Remarks)<br />
b.DrugsandMedicines(PartIIfordetails)<br />
cX-ray/Lab/SuppliesOthers(Par!IIIlorstalls)<br />
dOperatingRoomFee<br />
TOTAL<br />
eBenefitPackage<br />
12 Case Type' Qa Qb Qjc Qd13 ComplelelCD-10 Code/5<br />
"This is only applicable lor claims with fee for service paymenl mechanism<br />
(Professional <strong>Health</strong> Cat s to rill out items 14 to 16 )<br />
1'1AdmissionDiagnosis<br />
15CompleteFinalDiagnosis<br />
16 Professional fees I Charges<br />
a.NameofProfessional<br />
bPhilHeallhAccreditationMo<br />
cNumberofVisili/RVSCode<br />
clInclusiveDates(mmdj-m-y)<br />
o.ToIjIActual<br />
PFChargGs<br />
I.PhilHeallh<br />
Benefit<br />
bymembeii<br />
hSignature<br />
DateSigned<br />
Only<br />
1111l-lhi1<br />
1111l-l111111l-l1<br />
1,,,hil-l1<br />
1,1,1-1hi1
Generic/Brandname<br />
(dose/crip/syrup/injeclililo<br />
Wbv.Slin,'Jn\'}li;mcontcr.l)<br />
Qty<br />
UnitPrice<br />
Actual<br />
Charges<br />
Benefit<br />
TOTAL<br />
PARTIII-X-RAY,LABORATORIES,SUPPLIESANDOTHERS(useadditionalsheetifnecessary)<br />
Particulars<br />
Qty<br />
UnitPrice<br />
Actual<br />
Charges<br />
Phil<strong>Health</strong><br />
Benefit<br />
A.X-Ray(Imaging)<br />
B.Laboratories/Diagnostics<br />
CSuppliesandOthers<br />
? Official receipts for drugs and medicines / supplies purchased by member from external sources as well as laboratory procedures done outbide the<br />
hospital which are necessary for the confinement tie merit are attached are attached to this to this claim. claim.<br />
PART IV - CERTIFICATION OF INSTITUTIONAL HEALTH CARE PROVIDER<br />
I certify that sendees rendered were recorded in the patient's chart and hospital, records and that the herein information given are (rue and correct.<br />
TOTAL<br />
The foregoing items and charges are in compliance with the applicable laws, rules and regulations.<br />
Signature Signature Over Printed Over Name Printed of Authorized Name Representative of Authorized RepresentativeOfficial Capacity / DesignationDate Signed Official {month-day-year)<br />
Capacity/ Designation<br />
II _ II _ II<br />
PART V - CONSENT TO ACCESS PATIENT RECORD/S<br />
I hereby consent to the examination by Phil<strong>Health</strong> of the patient's medical records for the sole purpose of verifying the veracity of this claim<br />
I hereby hold Phil<strong>Health</strong> or any of its officers, employees and/or representatives free from any and all liabilities relative to the herein-mentioned<br />
consent which I have voluntarily and willingly given in connection with this claim for reimbursement before Phil<strong>Health</strong>.<br />
Signature Over Printed Name of Patient<br />
jJ - UJ - U^J<br />
Dale Signed (month-day-year)<br />
ignature Over Printed Name of Patient's Representative<br />
Date Signed (month-day-year)<br />
Reason for Signing on Behalf of the Patent<br />
Q Patient is IncapacitatedQ Other Reasons:<br />
Relationship of the Representative to the Patient<br />
j~| Spcuse r~] Child f~~j Parent r~j Guardian/
@fc^<br />
PhilHealtn<br />
MBramier Your Partner in in <strong>Health</strong> tieaun(Claim Form)<br />
*SPrevised February 2010<br />
IMPORTANT REMINDERS:<br />
THIS FORM SHOULO BE FILED TOGETHER WITH PHILHEALTH CLAIM FORMS 1 AMD 2 WITHIN GO CALENDAR DAYS FROM OATE OF DISCHARGE<br />
FOR LEVEL 1 FACILITY, THIS FORM SHALL BE REQUIRED FOR ALL BENEFIT CLf.lMS<br />
FOR LEVELS 2, 3 AND A FACILITIES, THIS FORM IS REQUIRED IN CASES OF I) EMERGENCY/TRANSFERRED 2) LESS THAN 24 HOURS ADMISSION 3) CASE TYPE 'D' DIAGNOSIS<br />
THIS FORM SHALL BE REQUIRED FOR ALL CLAIMS ON MATERNITY CARE PACKAGE.<br />
1 Phil<strong>Health</strong> Accreditation No (PAN) - Institutional <strong>Health</strong> Care Provider:I I 1 I I I I I I |<br />
PART I - PATIENT'S CLINICAL RECORD<br />
2. Name of Patient|7~Z. 1<br />
Thr Wrn may be reproduced and is NOT FOR SALE<br />
CF3<br />
Last Name,<br />
(example. Dela Cruz, Juan Jr, Sipag)<br />
4 Date Admitted<br />
Time Admitted. | |AM j |p<br />
5. Date Discharged'<br />
Time Discharged<br />
I AML|PM<br />
hh-mm<br />
6 Brief History of Present Illness / OB History<br />
7. Physical Examination ( Pertinent Findings per System )<br />
General Survey:<br />
Temperature1<br />
Abdomen<br />
HEENT<br />
Chest/Lungs<br />
GU(IE )<br />
Skin/Extremities<br />
CVS:<br />
NeuroExaminalion<br />
8. Course in the Wards (attach additional sheets if necessary).<br />
9 Perhnenl Laboratory and Diagnostic Findings ( CBC, Ufinalysis, Fecalysis, X-ray, Biopsy, etc )<br />
10 Disposition on Discharge: Q Improved\J Transferred\J HAMA\J Absconded Q Eipired
T<br />
-*RT II- MATERNITY CARE PACKAGE<br />
PRENATAL CONSULTATION<br />
1.Initial Prenatal Consultationi i I ~ I<br />
2.Clinical History and Physical Examination<br />
a.Vital Vital signs signs are are normalQc. normal[_ Menstrual History LMP |_j_| - | | | - j , , ,<br />
MonthDayYen<br />
Age of Menarche _<br />
3. Obstetric risk factors<br />
a Multiple pregnancy Qd Placenia pieviaQg Hislory of pie-eclampsia Q<br />
b Ovarian cyslj~~|13. Hislory c( 3 miscarriages Q]h Hislofy of eclampsia Q<br />
c. Myoma ulenr~jf History of stillbiifh|~~|i Premature conlraction f~<br />
g Hislory of pie-eclampsia Fl<br />
h Hislory of eclampsia Fl<br />
i Premature conlraction f~\<br />
4 Medical/Surgical risk factors<br />
bHearlDisease<br />
c.Diabeles<br />
?<br />
?<br />
d<br />
e.<br />
f.<br />
ThyroidDisorder<br />
Obesity<br />
Moderatetosevere<br />
?<br />
gEpilepsy<br />
hRenaldisease<br />
i.Bleedingdisorders<br />
?<br />
a<br />
k. Hislory of uterine myomectomy Fl<br />
5.AdmittingDiagnosis<br />
6.DeliveryPlan<br />
a. Orientation to MCP/Availment of Benefits<br />
? ?<br />
b. Expected date of delivery |_j_J - [ , | - [<br />
@Won HiDay<br />
7. Follow-up Prenatal Consultation<br />
a Prenatal Consultation No. | 2nd | | 3rd | | 4th [ | 5th | } Cth | [ 7ih | j 8ih | | 9ih | | 10th | | 11th j | 12th |<br />
b.Date of visit (mnvdn^ I I I I ! I I I<br />
c.AOG in weeks<br />
d.Weight & Vital signs.<br />
d1 Weight<br />
d.2 Cardiac Rale<br />
d 3 Respiratory Rats<br />
d.4 Blood Pressure<br />
d 5 Temperature<br />
?<br />
DELIVERY OUTCOME<br />
8. Date and Time of DeliveryDate [__j_J - |_jj - | , , , |Time ||flu ||ra<br />
AfnnffiDsyVesthh-nunIih-mm<br />
9 Maternal Outcome: Pregnancy Uterine,<br />
10. Birth Outcome:<br />
11.Scheduled Poslpartum follow-up consultation 1 week after delivery<br />
12.Date and Time of DischargeDate | , | - | , | - ] @ ,<br />
MonthDayYear<br />
POSTPARTUM CARE<br />
I I hi ! 1-1 I ! I 1<br />
MonlhDayyear<br />
Time ||am |U<br />
hh-iwnhh-ntm<br />
13.Perinea! wound careQ<br />
14.Signs of Maternal Postpartum ComplicationsQ<br />
15.Counselling and Education<br />
a. Breastfeeding and Nutrition[_]<br />
b Family Planning[_J<br />
16.Provided family planning service (o patient (as requested by paiieni)[J<br />
17.Referred to partner physician for Voluntary Surgical Sterilization (as requested by pi)Q<br />
18.Schedule the next postpartum follow-up\^\<br />
done<br />
19 CertificationofAttendingPhysician/Midwife'<br />
Icertifythat/heaboveinformationgiveninthisfan<br />
(art:trueandcorrect<br />
SignatureOverPrinledNameofAttendingPhysician/Midwife<br />
Dale Signed(Maul /Day/Year)
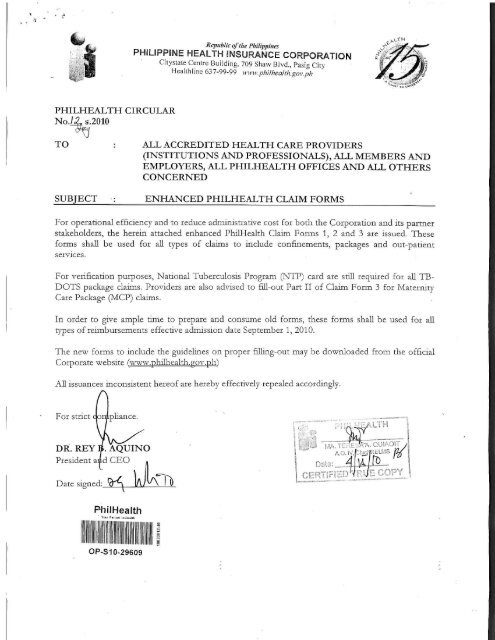
GUIDELINES ON THE PROPER<br />
ACCOMPLISHMENT OF REVISED PHILHEALTH<br />
CLAIM FORMS 1, 2, & 3<br />
I. General Guidelines applicable lo all Claim Forms:<br />
1.Claim Form 1 (CF1) -and Claim Foim 2 (CF2) shall be<br />
acecimpbshed and submitted for ALL claim applications<br />
except for confinement abiond.<br />
2.All CF shall be accomplished using capital letteis and by<br />
checking the appropriate boxes All items should be<br />
marked legibly by using ballpen or sign pen only.<br />
3.Names should be written starting with hist, first and<br />
middle name and should be separated by a comma.<br />
Extensions such as (but not limited to the following)<br />
jr., Sr., III should be indicated after die first name.<br />
Part II - Employer's Certification<br />
(for employed members' only)<br />
provides ihe basic information nbout the employer nnd<br />
contiiiii:; the ccrtiEcndon oi qualifying contributions and<br />
correctness of the informfition supplied by the member<br />
The tables below explain die proper way of accomplislirng<br />
CF1.<br />
Part I - Member and Patient Information (Member/<br />
Representative to fill out items 1 to 11)<br />
Item<br />
No.<br />
DescriptionandInstruction<br />
Illustration:<br />
DELA CRUZ, JUAN JR.,SIPAG<br />
Last nameFirst Name Middh Name<br />
4.All dates should be filled out following tins format<br />
MONTH-DAY-YEAR (MM-DD-YYYY).<br />
Illustration:<br />
July 27, 2010 should he written as 07/27/2030<br />
5 Time should be filled out using this format: HOUR<br />
MINUTE (HH:MM) following die 12-hour convention. It<br />
should be indicated in die appropriate box whether AM<br />
(morning) oi PM (afternoon and evening).<br />
I Has t ration:<br />
Nine fifteen in the morning should be written as 09:15 A A/<br />
6. PhilHeakh Identification No. (PTN) and PliilHeali.li<br />
Employer No (PEN) should be filled oul<br />
following die 2-c'-l format<br />
Wnstnitior.: 12-123456789-1<br />
7 PbiL<strong>Health</strong> Accreditation No (PAN) for institutions and<br />
professionals should be filled out following the presenbed<br />
formats<br />
Illustration jor@institutions.<br />
Hospitals -H12345678, ASC-A12345678, MCP-M12345,<br />
TBDOTS- T12345 and FDC- D12345<br />
Illustration for professionals: 1234-1254567-1<br />
8. For local confinement, supporting documents together<br />
with CF1 and CF2 should be filed with Phil<strong>Health</strong> witliin<br />
60 days horn date of discharge, e g.,1<br />
II. Specific Guidelines:<br />
@Member Data Record<br />
@MI5 (for individually paying members')<br />
@PliilHeallh ID (foi OF\V, Lifetime Member and<br />
Sponsoie.d Progrjm Ml-itiLvi)<br />
A. Chirm Form 1 (CF1)<br />
CFl is divided into two paits-<br />
Part I - Member and Patient Infoimatioii requnes<br />
rnfoiination about the membei and patient TO ascertain the<br />
identity of die member/patient/dependent for eligibility to<br />
Phil<strong>Health</strong> benefits<br />
1<br />
2<br />
3<br />
4<br />
5<br />
6<br />
ncasediePINisnotknown,thcmemberisad\nsed<br />
o<br />
Inquirefrom.myPliil<strong>Health</strong>office;or<br />
j.Seekinformationfromemployer(foremployed<br />
members)<br />
Checktheappropriateboxfordiecurrentmembership<br />
categorywhether:<br />
employed(goveinment/pnvate),IndividuallyPaying;<br />
Sponsored:OFW&Lifetime.<br />
Incasethenameisdifferentfromwhatisregistered<br />
withPhiL<strong>Health</strong>(perMDR}themembeiisadvisedto<br />
attachsupportingdocuments(birthcertificateor<br />
marriagecontiact;isapplicable)forupdaungofMDR.<br />
ft'hisistheaddresswheretheBenefitPaymentNoticepiPN]<br />
willbemailedto)<br />
Writethecompleteaddressofdiemember,indicating<br />
thehousenumber,nameofstreet,bamngay,<br />
municipalityorcity,provinceandzipcode.<br />
Writediedateofbirdiofmemberfollowingdie<br />
piescnbedLormutfordate.<br />
Writethemember'scontactinformationsuchasemail<br />
address,mobilenumberandkmdlinenumber,if<br />
available.
Name of Patient<br />
Write the complete name of the patient starting wirh<br />
last. Erst ::nd middle name. It should be separated by :i<br />
comma Extensions such as (but not limited to tine<br />
following) ]r., Sr., IJJ should be indicated after the Eisc<br />
Patient is the Member<br />
If patient is Llic member, check [he appiapime box and<br />
chen proceL'd to itc-m 9<br />
Patient is a Dependent<br />
If pauent is a dependent (to be filled out if patient is<br />
dependent)<br />
Check the appropiuUe box if patient is :i child, spouse or<br />
parent of the member.<br />
Reminder<br />
If piiticnt is ky;d JeptndenL uf the member, the patient's<br />
name should appeal in the MDIt If not, attach<br />
applicable suppoiting documents as proof of<br />
dependency<br />
Certification of Member<br />
Signature over printed name of member<br />
The membei -affixes his/hci signature over printed<br />
name ceitih'ing tliat all information suppbed m Part I<br />
are true and cotrecr and granting consent 10<br />
Phil<strong>Health</strong> to use die supplied information for any<br />
legal purpose.<br />
In case die member is a niinoi 01 a survivor-child, a<br />
representative (legal guardian) will also counteisign<br />
using the membei representative portion. If die legal<br />
guaidian is not duly indicated in die JNIDR, a copy of u<br />
judicial oider shall be attached to die claim.<br />
Date signed<br />
The membei indicates the date when be/she signed<br />
die certificate following die prescribed format for date<br />
Signature overprinted name of member's<br />
representative<br />
' An audiorized representative of die member may sign<br />
on lus/her btlv.ilf.<br />
Date signed<br />
The audiorized representaove of die pciueni; indicates<br />
the date when he/she signed on behalf of the patient<br />
following the prescribed form.it foi date.<br />
Relationship of the Representative to the member<br />
Check die appropriate box whether die representative<br />
of the member is Ins/her cliild (must be 1 S years old<br />
:md above), spouse, paienl and guardian/next nf kin<br />
Reason for signing on behalf of the member<br />
Indicate the reuson for signing on behalf ol" (.he<br />
membei such as: PI) Member is Abroad /<br />
Out-of-Towu; (2) Member is incapacitated and<br />
l'3) Other reasons F
Part V - Consent to Access Patient Records<br />
Tins contains the consent voluntarily given by the patient lor<br />
verification of the veracity of information relative to the<br />
evaluation and reimbursement of the claim.<br />
The following tables below explain the proper way of<br />
accomplishing CF2:<br />
Part I - HEALTH CARE PROVIDER INFORMATION<br />
Institutional <strong>Health</strong> Care Provider to fill our items<br />
1 to 13<br />
No.<br />
1<br />
2<br />
3<br />
4<br />
DescriptionandInstruction<br />
NameofFacility<br />
Writethecompletenameoffacilityincapitalletters<br />
asindicatedhidieaccreditationcertificate.<br />
Writediecompleteaddressofthefacility.<br />
e.g.,HospitalA,aternaryhospitalcategorizedas<br />
accreditedhospitalandTBDOTSfacility,claiming<br />
forTB-DOTSpackage,diePANforTB-DOTS<br />
facilityshouldbewritten.<br />
CategoryofFacility<br />
Checkdieappiopnateboxfordiecategoryofdie<br />
facilitywhether:<br />
@Tertiary-L4/L3fT-L4/L3)<br />
@Secondary-Level?(S-L2)<br />
@Pnniaiy-Level1fP-LlJ<br />
@AmbulatoiySurgicalClinic(ASC)<br />
@FreestandingDialysisClime(FDC)<br />
@MaternityCarePackageprovidei(MCP)<br />
@Rural<strong>Health</strong>Unit(RHU)<br />
@TBDOTS<br />
@Otliers(fornon-accieditedfacility)<br />
Ifthefacilityhasmultipleaccreditations,e.g.,<br />
accreditedhospitalandTBDOTSfacility,accredited<br />
RHUandTBDOTSfacility,accreditedRHU,TB<br />
DOTSfacilityandMCP(3miaccreditation),check<br />
theappropriateboxapplicabletodiebenefitclaim<br />
10<br />
Oa.lOh<br />
0c,10d<br />
Age<br />
WiiLt; die ;ige of the patient at the time of admission<br />
and check appropriate box whether the age is in<br />
year/s, month/s or day/s<br />
"heck appropriate box whether patient is male or<br />
Confinement Period<br />
Date Admitted. Tune Admitted;<br />
Date Discharged. Time Discharged<br />
Write the confinement pei:iod to include the date and<br />
time of admission and discharge following the<br />
piescnbed formats lor date and time.<br />
ForTB-DOTS Package:<br />
@For patient on intensive phase, indicate die<br />
Registration Date as date admitted (item 10a)<br />
following die prescribed format for date.<br />
@For patient on maintenance phase, indicate die<br />
Start Date of maintenance phase as date<br />
admitted (item 10a) following the prescribed<br />
format far date.<br />
@Write NA (Not Applicable) in time admitted,<br />
date and time discharged.<br />
For Outpatient Malaria Package:<br />
@Date admitted corresponds to die date of the<br />
start of tieatment.<br />
@Date discharged corresponds to die date of<br />
the last day of treatment.<br />
@"Write NA ('Not Applicable) in time admitted<br />
and time discharged.<br />
No. of Days Claimed<br />
Write die number of days claimed. In computing the<br />
number of days claimed exclude the day of<br />
admission and include the day of discharge.<br />
Illniiration:<br />
For in-patient cases:<br />
Admission Date: January 1, 2010<br />
Discharge Date: January 13, 2010<br />
No of Days Claimed: 12 Days<br />
For Qut-pAllent cases:<br />
Admission Date: January 7, 2010<br />
Discharge Date: January 7, 2010<br />
No. of Days Churned. 1<br />
In case of death, specify date<br />
In c:ise of death of patient during confinement<br />
penod, specirv the dnte of death in the appropriate<br />
box following die prescribed foimut for date<br />
5<br />
6<br />
Member'sPhil<strong>Health</strong>IdentificationNo.(PIN)<br />
(formember)<br />
WritetheMember'sPhil<strong>Health</strong>Identification<br />
Number(PIN)followingthe2-9-1form,it<br />
NameofPatient<br />
Writediecompletenameofthepatientstartingwith<br />
last,Cistandmiddlename.Itshouldbeseparatedby<br />
acomnu.Extensionssuchas(butnotlimitedtothe<br />
following)Jr.,Sr.,IIIshouldbeindicatedaftcidie<br />
firstname.<br />
"CC7ntethedate,ofbirthofpatientfollowingthe<br />
prescribedformat<br />
<strong>Health</strong> Care Provider Services<br />
Indicate die amount of the following items<br />
accordingly:<br />
@"Actual charges" refeis ro the total amount<br />
charged by the health caie provider (HCP) for<br />
every benefit item.<br />
@"PhilHenlth benefit" refers to the amount that<br />
will be reimbursed to the HCP by PhilHtaltli.<br />
The s.ime represents deduction made from<br />
die pa dent's actual chaige as member's<br />
benefit.<br />
For item lla Room and Board, check Appropriate<br />
box whether private or ward.
@Private - refers to a single occupancy room or<br />
with less than thi.ee beds per room divided by<br />
either a peimrmeni: or se nil-permanent<br />
partition.<br />
@Wmd - icfe-rs to a room with Uiiec 01 moic<br />
beds.<br />
For benefit packages not requiring ilcmiz,iuon PHIC<br />
benefit should be indicated in lie.<br />
Case Type<br />
Check the appropriate box of the coirccr illness case<br />
type whether A,B,C or D Tins is only applicable for<br />
claims with fce-for-service payment mechanism.<br />
Complete ICD-10 Codes<br />
Write die complete ICD 10 code/sof the p-.iuent's<br />
diagnosis. The fust code indicated should be the<br />
piimaiy illness. The succeeding codes shall represent<br />
co-morbidities.<br />
Professional <strong>Health</strong> Care Provider to fill out items 14 to 16<br />
16<br />
lfia,<br />
161)<br />
16c,<br />
16d<br />
Admission Diagnosis<br />
W'nte die admission diagnosis.<br />
Complete Final Diagnosis<br />
Write the complete final diagnosis of p;iuenfs<br />
illness/injuries including the mam diagnosis ;md<br />
other co-morbidities.<br />
Provide the following information, as applicable::<br />
u The cuologic agent ( e.g;, Escheiichia coli) in<br />
diagnosing infections,<br />
b For benign und malignant tumors, indicate the.<br />
site, moiphology and behavioui.<br />
c.In diagnosing injuries, provide the nature of<br />
die injury, and it possible, the place of<br />
occuncnce and die activity- of die one injured<br />
during die tune of the incident<br />
d.When diagnosing poisoning or advei.se<br />
reaction cases, specify die offending agent<br />
(e.g., drug, chemical).<br />
e.Specify if a condition is a late effect or<br />
sequelae of anodiei condition (e g , pubnonaiy<br />
Tibrosis sequelae of PTB).<br />
For mulaplc conditions, the main oi" primuLy condiuon<br />
must be the Gist diagnosis ihfit should be written<br />
e.g., Patient X is diagnosed with acucc pyelonephritis<br />
with concomitant hypertension and diabetes<br />
Complete Fin.il Diagnosis: acurc bacterial pi,-clonephriDb,<br />
hvpeiiension contioOed, diabetes mclliwr, cono-olled<br />
Professional Fees/Charges<br />
Name of Accredited Professional and<br />
Phil<strong>Health</strong> Accreditation No.<br />
Write the nnmc/s of pro regional health care<br />
provider/s who attended and provided services to die<br />
patient with corresponding PluIHealdi<br />
accieditation nmnber/s in the boxes provided.<br />
No. of Visits/ RVS Code and<br />
Inclusive Dates<br />
Indicate die following services rendered to the<br />
patient by die professional<br />
Medical C;ise -<br />
@Indiciite it daily visits with inclusive daiey<br />
@Indicate lrpreopcranve mpadeni consultation<br />
(CP Clearance) inclusive dates<br />
16f<br />
16g<br />
16h/l<br />
Surgical c.isc -<br />
@Indicate die appropriate RVS code rind date<br />
of opeiLition/procedure.<br />
@Anesthesia sendees - Indicate the type of<br />
anesthesia sendees given and date of service/<br />
procedure.<br />
Professional <strong>Health</strong> Care Services Indicate the<br />
amount of the following items accordingly:<br />
@"Total ..Actual Piofessional Fee Charges'1 refcis<br />
to the total amount of die professional fee<br />
chaigc-d by die health care professional to the<br />
patient before deduction of Phil<strong>Health</strong><br />
Benefit.<br />
@"Phil<strong>Health</strong> benefit1' refers to the amount that<br />
will be reimbursed to the professional by<br />
Phrl<strong>Health</strong>. The same represents deduction<br />
made from die patient's actual charge as<br />
member's benefit.<br />
@"Amount paid by member" refers to die<br />
payment made by die member after deduction<br />
of Phil<strong>Health</strong> benefit This represents die<br />
excess amount shouldered by die member. Tf<br />
full payment was made, indicate the amount<br />
equivalent to actual professional charges.<br />
Signature/Date Signed -<br />
@The professional who actually rendered die<br />
services shall sign in the box provided and<br />
indicate the date of signing following die<br />
pLCSdibed format for date.<br />
Part II - Drugs and Medicines<br />
List down dings and medicines used/consumed during<br />
confinement<br />
@Indicate the generic mime and the corresponding brand<br />
name ot die drug<br />
Illustration: amoxicillin (Amoxil);<br />
@Indicate coiresponding preparation (dose,cap/tab in<br />
mg; syrup/suspension in mg/ml; amp/vial in nag/ml);<br />
@Indicate total quantity used (piece, ampule, vial, etc);<br />
@Indicate the amount per unit;<br />
@"Actual charges" refers to the actual amount charged by<br />
die facil.it}' for ever)- item.<br />
@"Phil<strong>Health</strong> benefit" refers to the total amount of<br />
benefits foi all drug? and medicines<br />
@Indicate the total -amount of actual charges and<br />
Pliil<strong>Health</strong> Benefits for all drugs and medicines<br />
@Foi benefit packages not requiring iiemizanon, only die<br />
totnl amount of PHIC benefit should be indicated.<br />
Part III - X-ray, Laboratories, Supplies and Others<br />
Indicate all diagnostic procedures [imaging, laboratory tests,<br />
etc.) done and supplies and other items used during<br />
confinement<br />
@Indicate total number of procedures/items.<br />
@Indicate the amount per item;<br />
@'"Actual charges" refers to the total amount charged by<br />
die facility foi ever";' item or service rendered;<br />
@"Phil<strong>Health</strong> benefit" rcfeis 10 the total amount of<br />
"benefits foi x-ray, laboratories, supplies and others.<br />
@Indicate die total amount far columns Actual Chaiges<br />
and FhilHejilth Benefit
Note Check the box provided if official receipts foi<br />
drugs find medicines/supplies purchased by member from<br />
external sotuces us well as laboratory procedui.es done<br />
outside the hospital which are necessary for die<br />
confinement, are attached to tlie ckim.<br />
Part IV- Certification of Institutional <strong>Health</strong> Care<br />
Provider<br />
Signature over Printed Name of Authorized<br />
Representative<br />
The authorized representative shall write his/he: printed name<br />
and aftix his/her signature certifying th.\t the services rendered<br />
were recorded in the patient's chart and hospital records and the<br />
given information given are true and correct.<br />
Official capacity/Designation<br />
Write the official capacity/designation of the signatory<br />
Date signed<br />
Write die date of signing following the prescribed foimat<br />
for date.<br />
Part V - Consent to Access Patient Records<br />
Signature over Printed Name<br />
The patient shall write his/her name and affix his/hei<br />
signature signifying consent to PlnlHcnlth's verification of die<br />
veracity of die information contained in die claim.<br />
Date Signed<br />
Write the date of signing following the prescribed format for<br />
date.<br />
Part II Maternity Care Package<br />
Tins provides the inform a lion fib our die prenatal consultation,<br />
delivery outcome and postpaitum care of the patient.<br />
CF3 is not requiic-d in other Phil<strong>Health</strong> benefit packages such<br />
as Newborn Caie Package. Voluntary Surgical Contraception.<br />
Outpatient Malaria and TB-DOTS, regardless of facility level.<br />
The tables helow explain the propei wax of accomplishing<br />
CF3:<br />
Part I Patient's Clinical Record<br />
No.<br />
1<br />
2<br />
Description/Procedure<br />
Phil<strong>Health</strong>AccreditationNumber(PAN)<br />
Tinsreferstothecurrentaccreditationmirabeiof<br />
theinstitutionalhealthcareproviderassignedby<br />
PhilHcalth.<br />
Formultipleaccreditation,indicatetheaccreditation<br />
numberofthefacilityapplicabletothebenefit<br />
claim.<br />
WritePANfollowingtheprescribedformat.<br />
Vntediecompletenameofthepatientstartingwith<br />
ast,firstandmiddlename.Itshouldbeseparatedby<br />
comma.Extensionssuchas(butnotlimitedtothe<br />
ollownigj]r.,Si.,Hishouldbeindicatedafterthe<br />
firstname.<br />
Signature Over Printed Name of Patient's Representative<br />
The authorized represents!five of the patient may sign on<br />
behalf ot the patient.<br />
Date Signed<br />
Write die date of signing following the prescribed format for<br />
date.<br />
Relationship of the Representative to the Patient<br />
Write die relationship of die leprescntarive to the patient by<br />
checking the appropriate box whether spouse, child tor<br />
majority age, paient or guaidian/next ot kin.<br />
Reason for Signing on Behalf of the Patient<br />
Indicate the reason for signing on behalf of die patient<br />
whether patient is incapacitated or due to othei reasons<br />
(specify).<br />
C. Claim Form 3 (CF3) (To be filled out by accredited<br />
<strong>Health</strong> Care Provider)<br />
Tins cl.iim form will support the information supplied tn the<br />
Claim Foim 2 and shall be used in die evaluation of proper<br />
case type determination especially type D cases, emergency<br />
cases snd less than 2-1 hour admissions<br />
This ij. mandatory m:<br />
@Level 1 facilities,<br />
@Case type D;<br />
@Maternity Care Package,<br />
@" Emeigency/ Transferred cases, and<br />
@Less than 24-hour confinement<br />
Part I - Patient's Clinical Record<br />
This is die basis of PhilHcalth to ascertain die patient's clinical<br />
liistory, pertinent physical examination findings, laboratory &;<br />
diagnostic findings and disposition upon discharge.<br />
3<br />
4<br />
5<br />
(i<br />
7<br />
8.<br />
ndicatepatienL'schiefcomplaintforseeking<br />
consultationand/orreasonforadmission.<br />
followingtheprescribedformatfortime.<br />
Indicatethetimewhenthepatientwasdischarged<br />
followingtheprescribedformatfoitime.<br />
Indicatethechronologicaleventsofpresentillness<br />
includingallsignsandsymptoms,prompting<br />
consultationandsubsequentconfinementas<br />
describedbythepatient/guardian/informant.<br />
Indicatetheobjectivefindingsincludingpertinent<br />
negativefindingsperorgansystemelicitedduringdie<br />
conductofdiephysicalexamination.<br />
Indicatesignificantchanges/progressonthepatient's<br />
conditionduringconfinement.Mayaddadditional<br />
sheetsifnecessary<br />
Indicateallsignificantlaboratoryresultsand<br />
diagnosticfindings.
2)<br />
10<br />
D<br />
C<br />
w<br />
T<br />
spos<br />
eckt<br />
lethei<br />
,mstc<br />
tioi<br />
lea<br />
the<br />
@red<br />
onDischarge<br />
ipropnaccboxfoi<br />
pauenrwnsdischn<br />
HomeAgainstM<br />
(KAMA),AbscondedorExpired<br />
diedisposition<br />
rgedImproved,<br />
-dicalAdvice<br />
gEpilepsy<br />
hRenaldisease<br />
iBleedingdisorders<br />
1Historyofpreviouscaesanansection<br />
kHistoryofuterinemyomectomv<br />
Part II Maternity Cart Package (MCP)<br />
CF3 Part II shall be accomplished for MCP claims and<br />
must be submitted together with CF1 and CF2.<br />
5<br />
AdmittingDiagnosis<br />
Writetheadmittingdiagnosisofdiepatient<br />
Item<br />
No.<br />
Description/ Procedure<br />
PRENATAL<br />
Initial Prenatal Consultation<br />
Wine the- date of the initial prenatal consultation of<br />
tilt patient following die prescribed format fot dace.<br />
Clinical History and Physical Examination<br />
Vita) si^tis ate normal<br />
Check die box provided if die vital signs of the<br />
patient '.ire normal.<br />
(ib<br />
Writetheexpecteddaleofdeliveryfollowingthe<br />
prescribediormatfordate.<br />
Ascertain the present pregnancy is low risk-<br />
Check die box provided if present pregnancy is low<br />
nsk<br />
Menstrual History<br />
Indicate die dale of Last Menstrual Peiiod (LMP)<br />
following die prescribed format toi date and Age of<br />
Menarche.<br />
Obstetric History<br />
Write the Obstetric Seme of die patient by indicating<br />
die number of pregir.tncy./pregnancies (G) and the<br />
number of piegnancy/pregnancies Unit reached<br />
vi.ibilin' (P) The next four (4) blanks correspond to<br />
pregnancy outcome (Terr/i, Pralerm. .Abortion and<br />
Uvmg)<br />
lUitsirdtiQii A mother on hei duid pregnancy has had<br />
2 deliveries to m-o (2) Live, term offspring widi no<br />
hisiory of nboiiion.<br />
The obstetric score shall be<br />
7c<br />
7d<br />
Writedieweightandvitalsignssuchaycardi-aclate,<br />
respnaiorvrate,bloodpressureandtemperature<br />
conespondingtotheconsultation.<br />
DELIVERYOUTCOME<br />
Obstetric Risk Factors<br />
8<br />
WntediedateandtimeotdeliverytoUowmgdie<br />
ptesciibedformatfoidateandlime.<br />
Check die appropriate box it patient has any of the<br />
following obstetric risk factors:<br />
a.Multiple pmgn.incy<br />
b.Ovauiiui cyst<br />
c Myoma uixn<br />
d. Placenta pic via<br />
e Histoiy of 3 rmscamages<br />
1". Histoiy oi stiHbirLJi<br />
g. Mistoiy of pre-eclampsm<br />
h Histoiy of eclampsia<br />
1 Premature contraction<br />
9<br />
Wnlediematernaloutcomeasto.<br />
@ObstetricIndex-IndicatetheObstetricIndex<br />
eg.,G3P3(3003)<br />
@AOGbyLMP-IndicatetheAgeofGestation<br />
(AOG)mweeksbasedondieLastMenstrual<br />
Peiiod(LMP).<br />
@MannerofDelivery@Indicatediemannerof<br />
dekvery(NSD,assisted)<br />
@Presentation-Indicatethepresentationofdie<br />
fetus(cephalic,lueech,compound)<br />
Medical/ Surgical Risk Factors<br />
Check the appropriate box if p:iUcj.K has<br />
following mtdicdt/sui-giciil us!: faciors.<br />
a.Hypertension<br />
b.Heine Disease<br />
c.Diabetes<br />
d.Thyroid disorder<br />
e Obesitjf<br />
Moderate- to Severe Asthma<br />
of die<br />
10<br />
BirthOutcome<br />
WntethebhthoutcomeoitheIcaisasto<br />
@FetalOutcome@Indicatewhetlieithefetus<br />
isalive("live")ornotsuchas"fetaldeath"or<br />
"sullbudi".<br />
@Sex@Indicateihcsexoithefetuswnctlier<br />
femaleormale<br />
@Birthweight-Indicatethebirdiweightof<br />
feiuiingrams
theictusonthefirstminute-andfive(5)<br />
minutesthereafterasroAppealand.-.Pulse,<br />
Gnmace,ActivityandRespiration.<br />
11<br />
ScheduledPostpartumfollow-upcoiisultarion<br />
1weeknfterdelivery<br />
Writetliescheduledpostp.imimandnewborncare<br />
follow-upconsultationfollowingdieprescribed<br />
formatfordate.<br />
12<br />
Writethedateandtime,whenpauenrwnsdischarged<br />
followingtheprescribedformatsfor.dateandtime.<br />
POSTPARTUMCARE<br />
13<br />
14<br />
15<br />
15a,15b<br />
Perinealwoundcare<br />
Checktheboxprovidedifperinea!woundeaiewas<br />
done.Writesignificantfindings,ifany,indiemnai'ks.<br />
Checktheboxforanvsignofmaternalpostpartum<br />
complicationsWutesignificantEndings,ifany.iji<br />
tlieicm.irks.<br />
BreastfeedingandNutrition;FamilyPlanning<br />
Checktheboxitcounsellingandeducationwas<br />
piovidedtotliepatientonBreastfeedingand<br />
NutritionandFamilyPlanningUseremarksportion,<br />
ifany-<br />
16<br />
17<br />
Checktheboxiffamilyplanningservicewas<br />
providedtothepatientasrequested.Useremarks<br />
portion,ifany.<br />
ReferredtopartnerphysicianforVoluntary<br />
SurgicalSterilization(asrequestedbypatient)<br />
Checkdieboxifpatientwasreterredtopartner<br />
physicianforvoluntarysurgicalsterilizationas<br />
requested.Useremarksportion,ifany.<br />
IS<br />
Checktheboxifpatientwasscheduledforthenext<br />
postpartumfollow-upUseremarksportion,ifany.<br />
19<br />
Writethedateofsigningfollowingtheprescribed<br />
foimatfordate.