Pathogenesis of malignant ascites in ovarian cancer ... - doiSerbia
Pathogenesis of malignant ascites in ovarian cancer ... - doiSerbia
Pathogenesis of malignant ascites in ovarian cancer ... - doiSerbia

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Stanojeviæ Z. et al.<br />
at the <strong>in</strong>itial lymphatics. The necessary osmotic force can be created by active<br />
transendothelial transport <strong>of</strong> album<strong>in</strong> (20).<br />
CHARACTERISTICS OF MALIGNANT ASCITES<br />
Malignant <strong>ascites</strong> is characterized by positive cytology <strong>of</strong> <strong>malignant</strong> cells, large number <strong>of</strong><br />
white blood cells and a higher lactate dehydrogenase level (14, 21). Interest<strong>in</strong>gly, the ma<strong>in</strong><br />
ascitic fluid prote<strong>in</strong>-levels are high <strong>in</strong> patients with peritonitis carc<strong>in</strong>omatosa, as are <strong>ascites</strong><br />
album<strong>in</strong> concentrations (21).<br />
The data show <strong>in</strong>traperitoneal prote<strong>in</strong> and album<strong>in</strong> accumulation <strong>in</strong> <strong>malignant</strong> <strong>ascites</strong>. What<br />
are the reasons for impaired dra<strong>in</strong>age or <strong>in</strong>creased production?<br />
Fluid accumulation occurs if lymphatic dra<strong>in</strong>age <strong>of</strong> peritoneal cavity is compromised or if<br />
net filtration is <strong>in</strong>creased, overwhelm<strong>in</strong>g the lymphatic capacity. In <strong>malignant</strong> <strong>ascites</strong>, fluid<br />
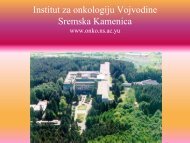
accumulation is the result <strong>of</strong> filtration m<strong>in</strong>us dra<strong>in</strong>age (Figure 2).<br />
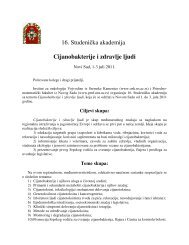
Figure 1. Schematic presentation <strong>of</strong> peritoneal <strong>in</strong>terstitium 1. Interstitial space, 2. Mesothelial cells,<br />
3. Fibrocyte, 4. Proteoglycans, 5. Collagen fibers, 6. Endothelial cell, 7. Basal lam<strong>in</strong>a<br />
Endothelial cells present the first barrier follow<strong>in</strong>g the route from the <strong>in</strong>travascular to the<br />
<strong>in</strong>traperitoneal space. Those cells have an extraperitoneal glycocalyx with fixed anionic<br />
charges, which is difficult to pass for album<strong>in</strong>. Album<strong>in</strong>s, as anionic macromolecules, considerably<br />
contribute to plasma oncotic pressure (16). Peritoneal endothelial cells are l<strong>in</strong>ked<br />
with tight junctions, so transendothelial transport is through the <strong>in</strong>tracellular pores (17).<br />
Endothelial basement membrane separates endothelial cells from the <strong>in</strong>terstitial space.<br />
Proteoglycans present <strong>in</strong> the basement membrane constitute a negative charge reticulum,<br />
which aga<strong>in</strong> is a selective barrier for anionic prote<strong>in</strong>s. The <strong>in</strong>terstitial space consists <strong>of</strong><br />
loose connective tissue composed <strong>of</strong> fibroblasts, collagen, hyaluronic acid, and negatively<br />
charged macromolecules. Hyaluronic acid b<strong>in</strong>ds a considerable amount <strong>of</strong> water. The <strong>in</strong>terstitial<br />
space acts as a filter and reduces or blocks diffusion <strong>of</strong> macromolecules. The submesothelial<br />
basement membrane is a cont<strong>in</strong>uous layer at the <strong>in</strong>terstitial site <strong>of</strong> the mesothelial<br />
cells. Negatively charged glycosam<strong>in</strong>oglycans are also present at this site. Mesothelial<br />
cells present the last barrier to be passed. The mesothelium consists <strong>of</strong> a monolayer <strong>of</strong> flat<br />
cells with a total estimated surface <strong>of</strong> approximately two square meters. Mesothelial cells<br />
are functionally similar to endothelial cells. They have glycocalyx conta<strong>in</strong><strong>in</strong>g anionic<br />
charges and transcellular channels for macromolecular transport. In summary, the presence<br />
<strong>of</strong> tight junctions between the endothelial cells <strong>in</strong> the peritoneal capillaries and the<br />
presence <strong>of</strong> negatively charged macromolecules at several extracellular sites produce an<br />
effective barrier aga<strong>in</strong>st leakage <strong>of</strong> negatively charged molecules such as album<strong>in</strong> from<br />
plasma to the peritoneal cavity. Those anatomic structures prevent excessive fluid-filtration<br />
from the capillaries to the peritoneum. The peritoneal lymphatic system collects fluid, prote<strong>in</strong>s,<br />
other macromolecules and cells and returns them to systemic circulation. The lymphatic<br />
capillary net is organized as a plexus along the submesothelial surface and dra<strong>in</strong>s to<br />
lymph vessels. Those have smooth muscle cells and are <strong>in</strong>nervated. Contractions <strong>of</strong> lymph<br />
vessels are generated by myogenic stimuli, and are <strong>in</strong>fluenced at least by activation <strong>of</strong> a-<br />
adrenovasoactive peptides. The anatomic features <strong>of</strong> peritoneal lymphatic system are the<br />
so-called stomata. The stomata serve for open communications between the abdom<strong>in</strong>al<br />
cavity and the submesothelial diaphragmatic lymphatics. They play a major role <strong>in</strong> peritoneal<br />
lymphatic dra<strong>in</strong>age, s<strong>in</strong>ce most <strong>in</strong>traperitoneal fluid is absorbed at this site (16).<br />
What are the mechanisms <strong>in</strong>volved <strong>in</strong> lymph formation? Those mechanisms are still<br />
unclear. A hydraulic pressure theory was proposed <strong>in</strong> the early 1930's <strong>of</strong> the last century<br />
(18). Normally, the <strong>in</strong>terstitial pressure is negative, thus an <strong>in</strong>crease <strong>in</strong> <strong>in</strong>traabdom<strong>in</strong>al pressure<br />
leads to <strong>in</strong>creased lymph production (19). Another hypothesis has focused on osmotic<br />
forces as a dom<strong>in</strong>ant factor. This theory postulates a prote<strong>in</strong> concentrat<strong>in</strong>g mechanisms<br />
Figure 2. Proposed pathogenesis <strong>of</strong> <strong>malignant</strong> <strong>ascites</strong>. * VEGF - vascular endothelial growth factor;<br />
b-FGF - basic-fibroblastic growth factor; TGFa and b - transform<strong>in</strong>g growth factor a and b; IL-8<br />
- <strong>in</strong>terleuk<strong>in</strong>-8; ** Starl<strong>in</strong>gÕs low <strong>of</strong> capillary hemodynamics: LpS[(Pcap -Pif) - s (pcap - pif)],<br />
***Changes <strong>in</strong> the balance between the capillary and <strong>in</strong>terstitial oncotic forces(pcap- pif)<br />
There is evidence <strong>of</strong> impaired lymphatic dra<strong>in</strong>age <strong>in</strong> peritonitis carc<strong>in</strong>omatosa, especially<br />
alterations <strong>in</strong> diaphragmatic and retrosternal lymph vessels (22). Decreased lymphatic<br />
dra<strong>in</strong>age is a contribut<strong>in</strong>g factor <strong>in</strong> the pathogenesis <strong>of</strong> <strong>malignant</strong> <strong>ascites</strong> (23). In addition<br />
to impaired lymphatic dra<strong>in</strong>age, there is evidence <strong>of</strong> six-to sixteen-fold <strong>in</strong>creased fluid production<br />
(9). Accord<strong>in</strong>g to the Starl<strong>in</strong>g's law <strong>of</strong> capillary hemodynamics, exchange <strong>of</strong> fluid<br />
between the plasma and the <strong>in</strong>terstitium is determ<strong>in</strong>ed by the hydraulic and oncotic pressure<br />
<strong>in</strong> each compartment (24).<br />
Net filtration = LpS (d hydraulic pressure - d oncotic pressure) = LpS [(P cap -P if ) - s (p cap<br />
- p if )]; Lp - unit permeability or porosity <strong>of</strong> the capillary wall; S - surface area available for<br />
filtration; P cap and P if - capillary and <strong>in</strong>terstitial fluid hydraulic pressures; p cap and p if - capillary<br />
and <strong>in</strong>terstitial fluid oncotic pressures; s - reflection coefficient <strong>of</strong> prote<strong>in</strong>s across the<br />
capillary wall with values rang<strong>in</strong>g from 0, if completely permeable, to 1 if completely impermeable<br />
(24).<br />
www.onk.ns.ac.yu/Archive August 10, 2004<br />
116