Download - Oemus Media AG
Download - Oemus Media AG
Download - Oemus Media AG

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
DENTAL TRIBUNE<br />
The World’s Dental Newspaper India Edition<br />
PUBLISHED IN INDIA www.dental-tribune.com VOL. 2 NO. 2<br />
News in brief<br />
Genes control early tooth<br />
development<br />
Several genes affect tooth<br />
development in the first year of<br />
life, according to the study conducted<br />
at the Imperial College<br />
London, the University of Bristol,<br />
& the University of Oulu<br />
in Finland. The research found<br />
that the babies’ teeth with<br />
certain genetic variants tend to<br />
appear later & that these children<br />
have a lower number of<br />
teeth by the age of one. In addition,<br />
those children whose teeth<br />
develop later have a 35 percent<br />
increased likelihood of requiring<br />
orthodontic treatment.<br />
Some of the genes identified<br />
have been linked, in previous<br />
studies, with the development<br />
of the skull, jaws, ears, fingers,<br />
toes, and heart. The discovery<br />
may lead to innovations in the<br />
early treatment and prevention<br />
of congenital dental and occlusion<br />
problem.<br />
Daniel Zimmermann<br />
DTI<br />
Trends & Applications<br />
Does dentine hypersensitivity<br />
affect oral<br />
health-related quality<br />
of life?<br />
4Page 4<br />
LEIPZIG, Germany: Clinical<br />
tests from the Department of<br />
Molecular Biology at the University<br />
of Salzburg in Austria have<br />
confirmed that dental treatment<br />
with Prozone, a next-generation<br />
ozone generator by Austrian<br />
manufacturer W&H, is highly<br />
effective against bacteria strains<br />
that are responsible for orodental<br />
infections and the development<br />
of dental caries. In the<br />
control study conducted in<br />
2009, samples of Streptococcus<br />
mutans and Escherichia coli<br />
were gassed immediately and<br />
after 1.5 hours with ozone for<br />
24 seconds and several times.<br />
The results demonstrated<br />
that treatments with 24 seconds<br />
ozone had visible effects on the<br />
treated area. In all tests immediate<br />
treatment was more effective<br />
than treatment after 1.5 hours.<br />
When the duration of the treatment<br />
was increased, the areas<br />
which contain no bacteria or<br />
4Page 12<br />
have a low bacterial count also<br />
increase.<br />
W&H’s ozone generator has<br />
been available to dentists worldwide<br />
since 2008. Despite it’s<br />
sterilizable ergonomically handpiece,<br />
it features preset predefined<br />
treatment times which<br />
make it easy to manage, the<br />
company states. Prozone is suitable<br />
for a wide range of dental<br />
applications including cavity<br />
and surgical disinfection as well<br />
as periodontal and endodontic<br />
Technology<br />
CAD/CAM-fixed<br />
prosthesis<br />
4Page 22<br />
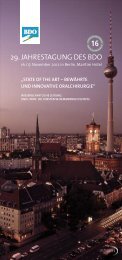
Prozone confirms effectiveness of ozone<br />
dental therapy<br />
These pictures shows agar plates with bacterial strain Escherichia coli. The left plate was treated with Prozone for 24 seconds<br />
and shows areas that are visibly bacteria-free. (DTI/Photo courtesy of Salzburg University, Austria)<br />
treatment. Treatment with<br />
ozone, a reactive three-oxygen<br />
molecule also found in earth’s<br />
atmosphere, is a relatively new<br />
concept in dentistry. Earlier<br />
studies indicate that it only takes<br />
a few seconds of therapy to kill<br />
99 percent of bacteria making<br />
it a thousand times more powerful<br />
than other bacteria killing<br />
agents. The new study shows that<br />
in order to reach the total potential,<br />
treatment has to be performed<br />
immediately. Delayed<br />
treatment also results in reduced<br />
bacteria count but the visible<br />
effects are less significant.<br />
Devices utilizing ozone technology<br />
such as Prozone expose<br />
filtered air to a highly electrical<br />
voltage which is directly applied<br />
to the treatment area where<br />
it destroys bacteria and viruses<br />
through oxidation. DT<br />
Highest quality made in Germany<br />
All our products convince by<br />
excellent physical properties<br />
easy handling<br />
perfect aesthetical results<br />
more information:<br />
www.promedica.de<br />
New:<br />
Bleach Shade!<br />
Glass ionomer filling cement<br />
- stable and abrasion resistant<br />
- excellent durable esthetics<br />
Interview<br />
“Evolution of miniimplants”<br />
Nano-Ceram-<br />
Technology<br />
Glass ionomer luting cement<br />
– very low film thickness<br />
– perfect occlusal accuracy<br />
PROMEDICA Dental Material GmbH<br />
Tel. + 49 43 21 / 5 4173 · Fax + 49 43 21 / 519 08<br />
Internet: http://www.promedica. · eMail: info@promedica.de<br />
de<br />
Light-curing micro-hybrid composite<br />
– excellent handling facilities<br />
– universal for all filling classes<br />
- also available as flowable version<br />
- with good flow and wetting capability<br />
Light-curing nano-ceram composite<br />
– highly esthetic an d biocompatible<br />
– universal for all cavity classes<br />
– comfortable handling, easy modellation<br />
– also available as flow version
2<br />
News DeNtal tribuNe | april-June, 2010<br />
News in brief<br />
No more dental colleges<br />
in the country<br />
The Dental Council of India<br />
(DCI) has decided not to sanction<br />
new dental colleges, anywhere<br />
in the country for the<br />
next five years, to regulate<br />
dental education and the dental<br />
profession. This announcement<br />
was made by DCI chief Dr<br />
Anil Kohli, who was in Mangalore<br />
to attend the silver jubilee<br />
celebration of A B Shetty Memorial<br />
Institute of Dental Sciences.<br />
“It is imperative to maintain<br />
quality in every sphere of life,”<br />
Dr Kohli said. “The field of medical<br />
sciences assumes far greater<br />
importance than ever before<br />
in this age of change,” he said,<br />
adding that “preserving quality<br />
of education is of paramount<br />
importance.” “Rather than<br />
sanctioning new dental colleges,<br />
DCI will focus its energy<br />
on ensuring that quality dental<br />
education is imparted to students<br />
in existing dental colleges<br />
in India,” he added.<br />
Indigenous implants will<br />
be a lot cheaper<br />
A report, published in The<br />
Times of India says that<br />
the Maulana Azad Institute<br />
of Dental Sciences (MAIDS),<br />
under the New Millennium<br />
Indian Technology Leadership<br />
Initiative by the Ministry of<br />
Science and Technology, has<br />
successfully developed a new<br />
indigenous dental implant,<br />
which will cost between Rs<br />
2,000 and 3000.<br />
Dr Mahesh Verma, principal<br />
investigator of the project, said<br />
that a team of doctors, from<br />
MAIDS, conceptualized & designed<br />
the outline for the implant<br />
which has been fabricated by<br />
IIT Delhi engineers. “Five<br />
human trials of the indigenous<br />
implant, fabricated in India,<br />
have been successfully completed,”<br />
he added. The micro<br />
CT analysis, to assess the percentage<br />
and quality of osseointegration<br />
of implant in the trial,<br />
conducted on rabbits was done<br />
at Trivandrum-based research<br />
institute have also shown<br />
positive results.<br />
The dental implants, imported<br />
from countries like US and<br />
Israel, cost up to Rs 20,000.<br />
The indigenous implants are<br />
expec-ted to provide a cheaper<br />
solution to wider loser implants<br />
in India.<br />
Nano-Bio-Chip detects oral cancer<br />
Photo courtesy of Textbook of Oral Pathlogy by Harsh Mohan.<br />
Isha Goel<br />
DT India<br />
New Delhi, India: A team of<br />
scientists at the Bio Science<br />
Research Collaborative, at Rice<br />
University, in Houston, US, has<br />
developed a nano-bio-chip (NBC)<br />
sensor technique that analyzes<br />
specimens from brush biopsies<br />
of lesions to detect oral cancer.<br />
The nano-bio-chip integrates<br />
multiple laboratory processes into<br />
Claudia Salwiczek<br />
DTI<br />
ERLANGEN/LEIPZIG, Germany:<br />
The brain is not able to<br />
discriminate between a painful<br />
upper tooth and a painful lower<br />
tooth, researchers found. The results<br />
of a new imaging study,<br />
which will be published in the<br />
journal Pain, may help devise<br />
better treatments for acute tooth<br />
pain, such as cavities or infections,<br />
and more chronic conditions<br />
like phantom pain of a tooth<br />
after it has been removed.<br />
The researchers led by Prof<br />
Clemens Forster of the University<br />
of Erlangen-Nuremberg in<br />
Germany analysed the brain activity<br />
in healthy volunteers as<br />
they experienced tooth pain. By<br />
delivering short electrical pulses<br />
to either the upper left or the<br />
lower left canine tooth, a painful<br />
sensation similar to that felt<br />
when biting into an ice cube was<br />
triggered. To see how the brain<br />
responds to pain emanating from<br />
different teeth, the researchers<br />
used functional magnetic resonance<br />
imaging (fMRI) to monitor<br />
changes in activity when the<br />
upper or the lower tooth was<br />
stimulated.<br />
“At the beginning, we expected<br />
a good difference, but that<br />
was not the case,” Forster stated.<br />
a single microfluidic platform:<br />
cell separation/capture on the<br />
membrane filter, biomarker<br />
immunolabeling and cytochemical<br />
staining, and fluorescent<br />
imaging and analysis. According<br />
to this pilot study, published in<br />
the Journal Cancer Prevention<br />
Research, the researchers compared<br />
results of traditional diagnostic<br />
test, and those obtained<br />
with the NBC, to find that the<br />
Many brain regions responded<br />
to top and bottom tooth pain—<br />
carried by signals from two<br />
distinct branches of a fibre<br />
called the trigeminal nerve—in<br />
the same way. The maxillary<br />
branch (V2) carries pain signals<br />
from the upper jaw, and the<br />
mandibular branch (V3) carries<br />
pain signals from the lower jaw.<br />
The researchers found that<br />
regions in the cerebral cortex,<br />
including the somatosensory<br />
cortex, the insular cortex and<br />
the cingulate cortex, all behaved<br />
similarly for both toothaches.<br />
These brain regions are known<br />
to play important roles in the pain<br />
projection system, yet none<br />
showed major differences between<br />
the two toothaches. “The<br />
activation was more or less the<br />
DENTAL TRIBUNE<br />
The World’s Dent al Newspaper India Ed ition<br />
Published by Jaypee Brothers Medical Publishers (P) Ltd., India<br />
© 2010, Dental Tribune International GmbH. All rights reserved.<br />
Dental Tribune India makes every effort to report clinical<br />
information and manufacturer’s product news accurately,<br />
but cannot assume responsibility for the validity of product<br />
claims, or for typographical errors. The publishers also do<br />
not assume responsibility for product names or claims, or<br />
statements made by advertisers. Opinions expressed by<br />
authors are their own and may not reflect those of Dental<br />
Tribune International.<br />
diagnostic NBC had comparable<br />
success rate with 97 percent<br />
sensitivity in detecting oral cancer,<br />
and 93 percent specificity<br />
in detecting which patients<br />
had malignant or premalignant<br />
lesions. The device will undergo<br />
a more extensive clinical trial<br />
involving 500 patients in Houston,<br />
San Antonio, and the<br />
U.K., which could lead to an<br />
application for FDA approval<br />
in two to five years.<br />
Oral cancer is among the<br />
ten most common cancers<br />
worldwide with a high mortality<br />
rate. According to a WHO<br />
survey report, India has the<br />
highest number of oral cancer<br />
cases in the world, out of which<br />
90 percent were due to tobacco<br />
related diseases, leading to<br />
2,200 deaths each day. The 5-<br />
year survival rate of 50 percent,<br />
among patients with oral cancer,<br />
has remained unchanged for<br />
Brain unable to localise tooth pain<br />
same,” Forster said, although, he<br />
added, “their experiments might<br />
have missed subtle differences<br />
that could account for why some<br />
tooth pain can be localised.”<br />
Because the same regions<br />
were active in both toothaches,<br />
International Imprint<br />
Publisher<br />
Torsten <strong>Oemus</strong><br />
t.oemus@dental-tribune.com<br />
Chairman DT India<br />
Jitendar P. Vij<br />
jaypee@jaypeebrothers.com<br />
Director<br />
P. N. Venkatraman<br />
venkatraman@jaypeebrothers.com<br />
Chief Editor<br />
Dr. Naren Aggarwal<br />
naren.aggarwal@jaypeebrothers.com<br />
the past 50 years as most cases<br />
are diagnosed in the advanced<br />
stages.<br />
This minimally invasive<br />
procedure requires just a little<br />
brush of the lesion with a toothbrush-like<br />
instrument instead<br />
of an invasive, painful biopsy,<br />
and can deliver results with<br />
in 15 mins. “One of the key<br />
discoveries in this paper is to<br />
show that the miniaturized,<br />
noninvasive approach produces<br />
about the same result as the<br />
pathologists do," study leader<br />
John McDevitt said in a<br />
statement.<br />
The Rice University has<br />
received a US $2 million grant<br />
from the National Institute for<br />
Dental & Craniofacial Research<br />
Division of the National Institutes<br />
of Health for their work. DT<br />
the brain—and the person—<br />
couldn’t tell where the pain was<br />
coming from. “Dentists should<br />
be aware that patients aren’t always<br />
able to locate the pain”,<br />
Forster says. “There are physiological<br />
and anatomical reasons<br />
for that.” DT<br />
Editor<br />
Dr. Isha Goel<br />
isha.goel@jaypeebrothers.com<br />
Editorial Consultants<br />
Dr. Gurkeerat Singh<br />
Dr. Amit Garg<br />
Dental Tribune India<br />
Published by :Jaypee Brothers Medical<br />
Publishers (P) Ltd.<br />
4838/24, Ansari Road, Daryaganj,<br />
New Delhi 110002, India<br />
Phone: +91 11 43574357<br />
e-mail:jaypee@jaypeebrothers.com<br />
Website: www.jaypeebrothers.com<br />
BDZ/0909/04
DeNtal tribuNe | april-June, 2010 News & Opinion 3<br />
IDEM confirms role as major APAC meeting<br />
Organiser announces plans for 2012/More variety in the scientific programme<br />
Daniel Zimmermann<br />
DTI<br />
SINGAPORE/LEIPZIG, Germany:<br />
With final participation numbers<br />
having been announced, the<br />
International Dental Exhibition<br />
and Meeting (IDEM) confirmed<br />
its position as a major dental<br />
meeting for the Asia Pacific<br />
region. An improved scientific<br />
programme & a higher number<br />
of exhibitors again drew more<br />
than 6,000 dental professionals<br />
to Singapore. Exhibitors and<br />
the organiser said that they<br />
were satisfied with the number<br />
and type of visitors this year.<br />
IDEM, which is organised<br />
by Koelnmesse Singapore Ltd,<br />
is held biannually in cooperation<br />
with the Singapore Dental Association<br />
and the FDI World Dental<br />
Federation.<br />
This year’s scientific programme<br />
focused on implantology<br />
and aesthetics— two of the most<br />
successful sectors in the Asia<br />
Pacific dental market. Although<br />
sales figures were significantly<br />
affected by the global financial<br />
crisis in 2008/09, growth rates<br />
are expected to pick up once<br />
the economy begins to recover,<br />
a May 2009 industry report<br />
stated. According to the same<br />
report, sales figures of dental<br />
implants in the Asia Pacific<br />
region experienced doubledigit<br />
growth rates back in 2008.<br />
Implantology was a significant<br />
part of this year’s trade<br />
Dentists crucial for<br />
detecting mouth<br />
breathing symptoms<br />
Singapore’s Health Minister Khaw Boon Wan (third from left) pays a visit to IDEM 2010. (DTI/Photo courtesy of Koelnmesse)<br />
exhibition, which saw increased<br />
numbers of dental surgical<br />
equipment and bone-grafting<br />
tools to aid dental implant<br />
procedures on display. Besides<br />
classical equipment like instruments,<br />
units or fillings, digital<br />
dentistry specialists also presented<br />
3-D imaging systems<br />
that aim to streamline communication<br />
between dentists and<br />
laboratories, and thus improve<br />
long-term treatment outcomes.<br />
For the first time, manufacturers<br />
from the republics of<br />
Slovenia & Colombia showcased<br />
their portfolio in Singapore. The<br />
British Dental Trade Association<br />
hosted their first national pavilion<br />
at the show alongside trade<br />
participations from Australia,<br />
Taiwan, Singapore, Korea,<br />
France and Switzerland. The<br />
US and German dental industry<br />
were the most well represented,<br />
with more than 20 companies<br />
representing all sectors in<br />
dentistry.<br />
Michael Dreyer, Vice-President<br />
Asia Pacific of Koelnmesse<br />
Pte Ltd, told Dental Tribune<br />
Asia Pacific that despite organisational<br />
changes and the economic<br />
turndown, IDEM 2010<br />
was in line with IDEM 2008.<br />
He said that his company will<br />
aim to improve the meeting<br />
further in order to make it<br />
available to further professional<br />
groups like dental assistants.<br />
Singapore Dental Association<br />
President Dr Lewis Lee said that<br />
the decision to hold pre-congress<br />
courses and master classes this<br />
year was well received by most<br />
congress attendees. He announced<br />
plans to broaden the scientific<br />
programme in 2012, incorporating<br />
more topics like dental<br />
materials, orthodontics or oral<br />
medicine. A larger number of<br />
hands on workshop will be<br />
offered as well, he added.<br />
DT page 6<br />
Daniel Zimmermann<br />
DTI<br />
NEW YORK, USA/LEIPZIG,<br />
Germany: Medical and dental<br />
problems associated with mouth<br />
breathing often go unnoticed by<br />
health professionals, a new<br />
study from the US suggests. The<br />
habit, which is caused by abnormalities<br />
of the upper respiratory<br />
tract, usually occurs in spring<br />
when many people suffer from<br />
pollen and seasonal allergies.<br />
Dentist are advised to regularly<br />
check for mouth breathing symptoms<br />
and swollen tonsils especially<br />
in children as young as<br />
5 years of age, the author<br />
recommends.<br />
If untreated, mouth breathing<br />
can cause a wide range of<br />
medical issues such as poor<br />
oxygen concentration in the<br />
blood, high blood pressure or<br />
sleep apnoea. In addition, it has<br />
been found to be responsible for<br />
abnormal facial growth primarily<br />
in the upper and lower jaw<br />
shape of children, leading to<br />
Long Face Syndrome, gummy<br />
smiles or other malocclusions.<br />
Moreover, poor sleeping habits<br />
that result from the condition<br />
can adversely affect growth and<br />
academic performance.<br />
Dentists may be the first to<br />
identify the symptoms of mouth<br />
breathing, as they typically<br />
request that their patients return<br />
every six months, which means<br />
that some people see their dentist<br />
more frequently than they see<br />
their physician.<br />
Treatment for mouth breathing<br />
can be beneficial for children’s<br />
medical and social conditions<br />
if caught early. Swollen<br />
tonsils and adenoids can be<br />
surgically removed by an earnose-throat<br />
specialist & dentists<br />
can use expansion appliances<br />
to help widen the sinuses and<br />
open nasal airway passages<br />
if the face and mouth are<br />
narrow. DT
4<br />
trends & applications DeNtal tribuNe | april-June, 2010<br />
Does dentine hypersensitivity affect oral<br />
health-related qualty of life?<br />
Dr Katrin Bekes<br />
Germany<br />
Dentine hypersensitivity is an<br />
oral complaint frequently reported<br />
in clinical dental practice.<br />
While many individuals do not<br />
seek treatment to desensitise<br />
their teeth because they do not<br />
perceive dentine hypersensitivity<br />
to be a severe oral health<br />
problem, a substantial number of<br />
patients experience discomfort<br />
to the extent that it interferes<br />
with their eating, drinking, oral<br />
hygiene habits and sometimes<br />
even breathing. These symptom<br />
often have a considerably adverse<br />
impact on their daily quality<br />
of life (QoL). This article reviews<br />
the impairments of oral health<br />
related quality of life in patients<br />
seeking care for dentine hypersensitivity.<br />
Traditionally, dentists have<br />
been trained to recognise & treat<br />
oral diseases & to describe them<br />
by using dental indices. Dental<br />
indices provide a quantitative<br />
method for measuring, scoring,<br />
and analysing dental conditions<br />
in individuals and groups. They<br />
describe the status of individuals<br />
or groups with respect to<br />
the condition being measured.<br />
How ever, important as these<br />
objective measures are, they<br />
only reflect the end-point of the<br />
disease processes. They give no<br />
indication of the impact of the<br />
disease process, es pecially oral<br />
disorder, on function or psychosocial<br />
well being, and only provide<br />
little insight into the impact<br />
on daily living and QoL.<br />
Therefore, QoL research in<br />
medicine & dentistry has attracted<br />
increasing attention over<br />
the past years. QoL is defined<br />
as an individual’s perception<br />
of his or her position in life, in<br />
the context of the culture and<br />
value systems in which he or<br />
she lives and in relation to his or<br />
her expectations, goals and concerns.<br />
QoL has multiple dimensions<br />
(such as cultural factors,<br />
social integration, socioeconomic<br />
status, quality of environment<br />
and personal autonomy).<br />
One dimension of QoL is health.<br />
The real impact of health and<br />
disease on QoL is known as<br />
health related quality of life<br />
(HRQoL). Oral health related<br />
quality of life (OHRQoL) is that<br />
part of HRQoL that focuses<br />
on oral health and orofacial<br />
concerns (Fig. 1). The concept<br />
of OHRQoL facilitates studying<br />
the impact of a disease on a<br />
person’s total oral health because<br />
it can be used across<br />
conditions. It describes the way<br />
in which oral health affects a<br />
person’s ability to function, his or<br />
her psychological status, social<br />
factors and pain or discomfort.<br />
How to measure OHRQoL<br />
OHRQoL is a multidimensional<br />
construct that cannot be observed<br />
directly. It needs to be visualised<br />
by means of suitable indicators.<br />
In order to comprehend<br />
a construct like this, target persons,<br />
that is patients, have to be<br />
asked pertinent questions. For<br />
example, some questions focus<br />
Fig. 1. OHRQoL is one dimension of quality of life.<br />
on function, some are concerned<br />
with pain and discomfort, and<br />
others evaluate self-image and<br />
social interaction. The Oral<br />
Health Impact Profile (OHIP)<br />
is amongst the most widely used<br />
instrument in studies evaluating<br />
OHRQoL. It attempts to measure<br />
both the frequency and severity<br />
of oral problems on functional &<br />
psychosocial well being. This<br />
tool was developed by Slade and<br />
Spencer in Australia in 1994.<br />
The OHIP is a 49-item measure,<br />
with statements grouped<br />
into seven theoretical domains,<br />
namely functional limitation,<br />
pain, psychological discomfort,<br />
physical disability, psychological<br />
disability, social disability and<br />
handicap. Examples of some<br />
OHIP questions are:<br />
• Have you had trouble pronouncing<br />
words because of<br />
problems with your teeth,<br />
mouth or dentures?<br />
• Have you found it uncomfortable<br />
to eat any foods because<br />
of problems with your teeth,<br />
mouth or dentures?<br />
• Have you felt that your sense<br />
of taste has worsened because<br />
of problems with your<br />
teeth, mouth or dentures?<br />
For each of the 49 OHIP questions,<br />
subjects are asked how<br />
frequently they have experienced<br />
the oral problem. Responses<br />
are according to a Likert-type<br />
scale: 0 = never, 1 = hardly ever,<br />
2 = occasionally, 3 = fairly often,<br />
and 4 = very often.<br />
A summary score of between<br />
0 & 196 results from the 49 questions,<br />
with 5 scoring steps each,<br />
which provides a good impression<br />
of the extent to which OHR<br />
QoL is affected. A score of 0<br />
indicates the absence of any oral<br />
health related problem. Higher<br />
scores represent an OHRQoL<br />
that is more impaired. The<br />
most extensive impairment of<br />
the OHRQoL is expressed by a<br />
score of 196. This is termed the<br />
problem index and demonstrates<br />
that all oral problems are<br />
frequently encountered. A table<br />
of standard values representative<br />
of different populations is<br />
provided, according to which the<br />
patient’s score can be compared<br />
and evaluated.<br />
Fig. 3. Differences in OHRQoL measured with the OHIP questionnaire in patients<br />
with dentine hypersensitivity and in a general population sample.<br />
To be able to assess levels of<br />
OHRQoL in non-English speaking<br />
populations, cross-culturally<br />
adapted translations of the original<br />
English-language version of<br />
the OHIP into Chinese, Dutch,<br />
Hungarian, Italian, Japanese,<br />
Portuguese, Spanish & Swedish<br />
has been achieved in several<br />
countries. The demand for an<br />
internationally comparable German<br />
tool led to the devel opment<br />
of a German version of the OHIP<br />
(OHIP-G), which determines the<br />
OHRQoL of German speaking<br />
persons. OHIP-G includes the 49<br />
items of the English original, as<br />
well as four additional items that<br />
were regarded as important for<br />
the German population specifically.<br />
OHIP-G can be applied to<br />
patients of 16 years and older.<br />
Fig. 2. Hypersensitive cervical dentine surfaces.<br />
OHRQoL in patients<br />
seeking care for dentine<br />
hypersensitivity<br />
Dentine hypersensitivity is a<br />
common oral complaint that is<br />
frequently reported in dental<br />
practice. It is characterised by<br />
a short and sharp pain arising<br />
from exposed dentine and occurring<br />
in the presence of thermal,<br />
chemical, tactile or osmotic<br />
stimuli (Fig. 2). From the relatively<br />
few studies that investigate<br />
the prevalence of dentine<br />
hypersensitivity, it can be concluded<br />
that it is a frequent condition.<br />
Studies have reported a<br />
prevalence of dentine hypersensitivity<br />
in the adult dentate population<br />
ranging from 4 to 57 percent.<br />
However, figures as high<br />
as 60 to 98 per cent have been<br />
reported in patients with periodontitis.<br />
While many individuals<br />
do not seek treatment to<br />
desensitise their teeth because<br />
they do not perceive dentine<br />
hypersensitivity to be a severe<br />
oral health problem, 10 to 25<br />
per cent of patients experience<br />
discomfort to the extent that<br />
it interferes with their eating,<br />
drinking (hot & cold beverages),<br />
oral hygiene habits and sometimes<br />
even breathing. The degree<br />
of discomfort depends on<br />
individual pain perception, pain<br />
tolerance, and emotional and<br />
physical factors. These symptoms<br />
are highly relevant from<br />
the patient’s point of view and<br />
often have a considerably adverse<br />
effect on daily QoL.<br />
A study was conducted at<br />
the Martin Luther University,<br />
Halle-Wittenberg, Germany to<br />
describe and evaluate OHR QoL<br />
in patients with dentine hypersensitivity.<br />
Data was collected<br />
through a questionnaire as part<br />
of a larger study targeting several<br />
areas of oral health beyond<br />
hypersensitive teeth, such as oral<br />
hygiene, prevention efforts, and<br />
oral behaviours and habits.<br />
There were 724 patients<br />
(mean age: 42.8 ± 13.0 years)<br />
who participated in the study,<br />
presenting at 161 German dental<br />
offices because of hypersensitive<br />
teeth and reacting positively<br />
to an air stimulus applied by the<br />
dentist. Patients with removable<br />
partial dentures & patients with<br />
missing answers in the OHIP<br />
questionnaire were excluded.<br />
After these exclusions, 656<br />
patients remained in the study<br />
for analysis. These patients were<br />
compared with 1,541 subjects<br />
without removable partial dentures<br />
from a national, general<br />
German population sample<br />
(mean age: 37.7 ± 13.4 years).<br />
OHRQoL was assessed using<br />
OHIP-G. The patients completed<br />
the OHIP-G questionnaire<br />
in the dental office.<br />
Fig. 4. OHRQoL in patients with dentine hypersensitivity and in a general population<br />
grouped by gender.
6<br />
trends & applications DeNtal tribuNe | april-June, 2010<br />
The OHIP-G summary score<br />
characterised the OHRQoL construct<br />
as a whole. The OHIP-G<br />
summary score of patients with<br />
hypersensitive teeth was 34.5<br />
(± 22.6), while the general<br />
population sample had a score<br />
of 12.2 (± 18.4). The 22.3 difference<br />
was statistically significant.<br />
The general population<br />
subjects had an OHIP-G median<br />
score of 5, while the patient<br />
group had an OHIP-G median<br />
score of 30 (Fig. 3). Ten percent<br />
of the subjects with the highest<br />
OHI P-G summary scores had<br />
scores of 36 (general population)<br />
and 66 (patients).<br />
Differences according to<br />
gender were minimal. Although<br />
the difference between gender<br />
of a mean 2.8 points was statistically<br />
significant (p < 0.01),<br />
it was regarded as negligibl.<br />
Amongst the patient group,<br />
women reported more problems<br />
with the con dition of<br />
dentine hypersen sitivity than<br />
men, which is in contrast to the<br />
general pop ulation, in which<br />
men had higher OHIP scores<br />
than women (Fig. 4).<br />
Conclusions<br />
QoL has been established as<br />
an important outcome for evaluating<br />
the impact of a disease<br />
and for assessing the efficacy<br />
of treatment. The impact of<br />
oral disorders and interventions<br />
on patients’ perceived oral<br />
health status and OHRQoL is<br />
increasingly recognised as an<br />
important component of health.<br />
Dentine hypersensitivity is a<br />
frequent problem that can be<br />
observed in adults of all ages.<br />
In this study, patients with<br />
sensitive teeth reported substantial<br />
OHR QoL impairment,<br />
which may have an influence<br />
on whether or how patients<br />
should be treated. The extent<br />
of this effect is comparable to<br />
that of other oral diseases and<br />
conditions, such as temporomandibular<br />
disorders. The<br />
present investigation is the first<br />
study that evaluates the impact<br />
of this condition using a widely<br />
used patient-centred outcome<br />
measure to characterise the<br />
broader influence of this<br />
condition on patients’ perceived<br />
oral health. DT<br />
About the author<br />
Dr Katrin Bekes is Assistant<br />
Medical Director at the Department<br />
of Operative Dentistry and<br />
Periodontology, University School<br />
of Dental Medicine, Martin Luther<br />
University Halle-wittenberg, Halle<br />
/Saale Germany. She can be contacted<br />
at katrin.bekes@medizin.<br />
uni-halle.de.<br />
DT page 3<br />
Delegates that joined the<br />
first precongress sessions on<br />
Thursday morning confirmed<br />
that the programme was a large<br />
improvement to the offerings<br />
in 2008. Most of the people interviewed<br />
said that because of<br />
these changes they were able to<br />
attend most of the sessions held<br />
during the course of the meeting.<br />
“I think the congress was pretty<br />
well organised and there was<br />
less overlapping which made<br />
it easier to get into more sessions,”<br />
said one dentist from<br />
Singapore.<br />
According to Mr Dreyer, preparations<br />
for the next edition of<br />
IDEM in 2012 have already<br />
begun and the first speakers<br />
have been announced. Amongst<br />
others, there will be sessions on<br />
the management of endodontic<br />
disasters, the biological effects<br />
of current restorative materials<br />
on the pulp-dentine complex<br />
and current concepts on posts<br />
and cores.<br />
The next meeting is scheduled<br />
to be held 20–22 April 2012. DT
DeNtal tribuNe | april-June, 2010 Case report 7<br />
A case report: Unusual anatomy of maxillary second molar<br />
Dr P D Joshi<br />
India<br />
Introduction<br />
The main objectives of an<br />
endodontic treatment are the<br />
elimination of microorganism<br />
from the root canal system<br />
and prevention of subsequent<br />
reinfection of the system. 1 Inability<br />
to find and properly treat<br />
the canal may cause failure. 2<br />
This case report presents<br />
an unusual maxillary right<br />
second molar with four roots<br />
(mesiobuccal, distobuccal, mesiopalatal,<br />
and distopalatal). The<br />
unusual morphology of roots of<br />
the maxillary second molar<br />
may be a challenge in diagnosis<br />
and treatment execution. 3-5<br />
Diamond, in his textbook<br />
on dental anatomy, has shown<br />
two cases of maxillary first<br />
molars with two distinct palatal<br />
roots. 6<br />
Sabala, et al, in a radiographic<br />
survey, found that the most<br />
common aberration of maxillary<br />
molars involved the fusion of<br />
22 percent of the facial roots<br />
of second molars. 7 They discovered<br />
that aberrations occurred<br />
in less than 1 percent of the<br />
cases and that of 90 percent<br />
of such aberrations were bilateral.<br />
Libfeld and Rostein also<br />
examined 1200 teeth radiographically,<br />
and reported that<br />
four rooted maxillary second<br />
molars occurred in 0.416% of<br />
cases. 8 The four roots in maxillary<br />
molar is more frequent in<br />
second molars, the conclusion<br />
made by Christie, et al. 9<br />
This case report illustrates<br />
the importance of knowledge<br />
about unusual variations in<br />
morphology of root and canal,<br />
proper acess opening, gaining<br />
straight line access, proper<br />
cleaning and shaping of canals,<br />
and obturation.<br />
Case report<br />
A 34-year-old female reported<br />
to the clinic with the chief complaint<br />
of pain in relation to upper<br />
left back tooth region since two<br />
days, and pain usually occur<br />
after stimulation with hot and<br />
cold liquids. The patient gave the<br />
history of pain getting worse on<br />
lying down, and waking up<br />
with pain in the middle of the<br />
night. The clinical examination<br />
showed a large carious lesion<br />
on the buccal surface of the<br />
maxillary left second molar<br />
(#27). Vitality test with cold<br />
stimulant revealed severe, rapid,<br />
and long-lasting pain from<br />
maxillary left second molar.<br />
Pre-operative periapical radiograph<br />
revealed a large carious<br />
lesion on buccal surface of #27<br />
involving the pulp (Fig. 1). Based<br />
on clinical and radiographical<br />
evidence, it was diagnosed as<br />
irreversible pulpitis.<br />
The careful observation of<br />
periapical radiograph shows that<br />
the second molar has unusual<br />
root morphology, i.e., it has four<br />
separate roots. The unusual two<br />
separated palatal roots are long<br />
and diverging like horns.<br />
The non-surgical endodontic<br />
therapy was planned for tooth<br />
#27. The treatment was started<br />
with administration of local<br />
anesthesia using 2% lignocaine<br />
with 1:200000 adrenaline. Caries<br />
was removed, and then the<br />
missing buccal surface of the<br />
tooth was build up using glass<br />
ionomer cement fuji type II, to<br />
facilitate the isolation of tooth<br />
using Rubber Dam (Hygienic<br />
Corp., USA).<br />
A usual triangular access<br />
cavity (Fig. 2) was modified<br />
to square-shaped (rhomboidal)<br />
(Fig. 3) using cavity access set (by<br />
Dentsply Mail-lefer, Ballagues),<br />
and was further refined with tip<br />
#2 of Start X ultrasonic kit (by<br />
Dentsply Maillefer, Ballagues)<br />
(Fig. 4). After access opening,<br />
the four orifices were explored,<br />
namely mesiobuccal (MB), distobuccal<br />
(DB), mesiopalatal (MP),<br />
and distopalatal (DP). Two distinct<br />
palatal orifices related to<br />
two separate palatal roots were<br />
identified.<br />
The extensive search with<br />
Ultrasonic tip #2 of Start X<br />
was carried out for second<br />
MB, but could not be located.<br />
They were further straightlined<br />
with X-Gates of cavity access<br />
set (by Dentsply Maillefer, Ballagues)<br />
(Fig. 5 & 6). The working<br />
length (WL) was determined<br />
using Root ZX electronic apex<br />
locator (EAL), (by Dentaport ZX,<br />
J. Morita, Japan).<br />
Files were placed in the<br />
canals (Fig. 7) according to WL<br />
determined by EAL, and then<br />
one more periapical radiograph<br />
was taken to confirm the WL<br />
(Fig. 8).<br />
The cleaning and shaping<br />
of canals were carried out with<br />
rotary NiTi Protaper instruments<br />
series (by Dentsply Maillefer,<br />
Ballagues), according to<br />
the manufacturer’s instructions.<br />
The final instrumentation was<br />
carried out with sizes S1 to F3<br />
of NiTi Protoper instruments<br />
(Fig. 9). For irrigation, 3%<br />
sodium hypochlorite was used<br />
during instrumentation and as<br />
well as after completion of<br />
the preparation. Conefit was<br />
carried out with non-standardized<br />
gutta-percha of medium<br />
size (Sure-endo, Korea)<br />
with the help of gutta-percha<br />
gauge (Dentsply Maillefer,<br />
Ballagues) (Fig. 10 & 11).<br />
Now, the canals were dried<br />
using paperpoints of size F3 (by<br />
Dentsply Maillefer, Balla-gues)<br />
and then obturated with selected<br />
cone, using down pack with system<br />
B and back pack with obtura<br />
II device (Fig. 12). A periapical<br />
radiograph (Fig. 13) was taken<br />
to confirm the quality of obturation.<br />
Permanent restoration was<br />
done on the next appointment.<br />
Discussion<br />
Incidence of four rooted maxillary<br />
second molar is very rare.<br />
Etienne Deveaux 10 presented<br />
a case report in Vol. 25, No. 8,<br />
JOE Aug. 1999, and Peter M<br />
Di Fiore 11 presented first molar<br />
in Vol. 25, No. 10, JOE Oct. 1999.<br />
Hartwell and Bellizi 12 reported<br />
that 9.6% of maxillary molars,<br />
they examined, had four canals,<br />
but had not mentioned about<br />
any case with four roots.<br />
Christie, et al, 9 have proposed<br />
a classification system for four<br />
rooted maxillary second molar<br />
abnormalities.<br />
Fig. 1: Pre-operative radiograph Fig. 2: Triangular access opening Fig. 3: Modified (Rhomboidal) access opening Fig. 4: Ultrasonic Tip<br />
Fig. 5: X-Gates being used for straight lining of access Fig. 6: Access after orifice enlargement Fig. 7: Files in position for WL Fig. 8: WL radiograph<br />
Fig. 9: WL radiograph for buccal canals Fig. 10: Shaping with Protaper Instruments Fig. 11: Conefit Fig. 12: Conefit Radiograph
8<br />
Case report DeNtal tribuNe | april-June, 2010<br />
Type I with long tortuous divergent<br />
separate palatal roots<br />
Type II with short blunt and<br />
parallel roots<br />
Type III those with three<br />
convergent roots and distinctly<br />
divergent fourth distobuccal<br />
root.<br />
The tooth treated in this<br />
case appears to be of Type I<br />
variety according to the<br />
Christie’s classification. According<br />
to literature, it occurs bilaterally,<br />
but in this patient it<br />
was unilateral.<br />
References<br />
1. De Deus QD. Endodontia,<br />
5th ed. Medsi: Rio de Janerio.<br />
1992.<br />
2. Zeigler PE, Serene TP. Failures<br />
in therapy. In: Cohen S, Burns<br />
RC, eds. Pathways of the pulp.<br />
4th ed. St Louis: CV Mosby 1987:<br />
723-753.<br />
3. Thompson BH. Endodontic<br />
therapy of an unusual maxillary<br />
second molar. J Endodontics<br />
1988; 14: 143-146.<br />
4. Fahid A, Taintor JF. Maxillary<br />
second molar with three buccal<br />
roots. J Endodontics 1988; 14:<br />
181-183.<br />
5. Malagnino V, Gallottni L, Passariello<br />
P. Some unusual clinical<br />
cases on root anatomy of<br />
permanent maxillary molars.<br />
J Endodontics 1997; 23: 127-<br />
128.<br />
6. Diamond M. Dental anatomy<br />
including anatomy of the head<br />
and neck. New York: MacMillan<br />
1952: 203-205.<br />
7. Sabala CL, Benenati FW, Neas<br />
BR. Bilateral root or root canal<br />
aberrations in a dental school<br />
patient population. J Endodontics<br />
1994; 20: 38-42.<br />
8. Libfeld H, Rotstein I. Incidence<br />
of four-rooted maxillary second<br />
molars: literature review and<br />
radiographic survey of 1, 200<br />
teeth. J Endodontics 1989; 15:<br />
129-131.<br />
9. Christie WH, Peikoff MD, Fogel<br />
HM. Maxillary molars with<br />
two palatal roots: a retrospec-<br />
Fig. 13: Post-obturation view<br />
EMS-SWISSQUALITY.COM<br />
AIR-FLOW KILLS<br />
BIOFILM<br />
THE NEW AIR-FLOW HANDY PERIO GETS RID OF THE ENEMY –<br />
WITH GENTLE ACTION AND UTMOST PRECISION<br />
Three horizontal nozzle apertures for<br />
the air-powder mixture, a separate<br />
vertical water nozzle aperture for rinsing:<br />
what used to be off limits is now<br />
easily reachable, through gentle action<br />
and without any risk of emphysema.<br />
And since the Air-Flow Powder Perio<br />
is particularly fine, the tooth surface<br />
is not damaged.<br />
Fig. 14: Post-obturation radiograph<br />
Fig. 15: Radiograph of contralateral side<br />
tive clinical study. J Endodontics<br />
1991; 17: 80-84.<br />
10. Etienne Deveaux: Maxillary<br />
second Molar with Two Palatal<br />
Roots; Vol. 25, No. 8, JOE. 1999<br />
Aug.<br />
11. Peter M.Di. Fiore: A Four-<br />
Rooted Quadrangular Maxillary<br />
Molar Vol. 25, No. 10,<br />
JOE. 1999 Oct.<br />
12. Hartwell G, Bellizzi R. Clinical<br />
investigation of in vivo endodontically<br />
treated mandibular &<br />
maxillary molars. J Endodontics<br />
1982; 8: 555-557. DT<br />
About the author<br />
DEEP DOWN, between tooth and gingiva,<br />
billions of bacteria managed to<br />
proliferate under the cover of malicious<br />
biofilm – until now.<br />
Grain size ~ 25 µm<br />
Together with the Original Air-Flow<br />
Powder Perio, the new Air-Flow<br />
handy Perio with its unique Perio-<br />
Flow nozzle tracks down biofilm, even<br />
in the deepest periodontal pockets.<br />
With its new Air-Flow handy Perio,<br />
Air-Flow has assigned its latest family<br />
member to combat –<br />
right on target for<br />
subgingival prophylaxis<br />
in your<br />
practice.<br />
For more information ><br />
welcome@ems-ch.com<br />
Dr P D Joshi graduated in dentistry<br />
from Nair Dental College, Mumbai<br />
in 1980, and has specialized in<br />
conservative dentistry & endodontics.<br />
He has a private practice<br />
specializing in endodontics in<br />
Mumbai. In addition, he has taken<br />
specialized training in microscopic<br />
endodontics from the University of<br />
Pennsylvania, USA, and in implant<br />
dentistry from Germany. He is an<br />
instructor in the department of<br />
micro-dentistry at Government<br />
Dental College, Mumbai. He lectures<br />
& demonstrates extensively<br />
in India and abroad on endodontics<br />
and micro-dentistry. He can be<br />
contacted at drjoshi01@gmail.com.
DeNtal tribuNe | april-June, 2010 Clinical 9<br />
Treating a peri-radicular abscess<br />
Dentist Nicolai Orsteen presents a clinical case study looking at the treatment of a maxillary left lateral front tooth<br />
The patient is a 24-year old white<br />
Northern European male. His<br />
chief complaint was pain from<br />
the maxillary left lateral front<br />
tooth, with periodic swelling of<br />
the left anterior palatal.<br />
The patient’s dental history<br />
indicated previous problems in<br />
this region, documenting an<br />
emergency appointment in<br />
March 2007 due to pain and<br />
swelling from tooth 22. He was<br />
prescribed a seven-day course of<br />
Penicillin V tablets (660mg<br />
qds*4) for acute apical periodontitis<br />
tooth 22. Following this<br />
appointment, the patient was<br />
Table 1: Clinical findings<br />
referred for examination and<br />
treatment of tooth 22.<br />
Diagnosis<br />
The extra-oral examination on<br />
30 January 2008 was within<br />
normal limits, shown in Figures<br />
2 and 3.<br />
However, as is visible in Table<br />
one, the intra-oral examination<br />
revealed gingival bleeding on<br />
prodding, no sinus tract and<br />
fluctuant swelling of the palate<br />
mucosa in the area of teeth 21,<br />
22 and 23. The periodontal<br />
pockets however, were within<br />
normal limits.<br />
21 22 23<br />
Sensitivity to Cold Yes No Yes<br />
Percussion No Yes No<br />
Palpation No Yes No<br />
Mobility No No No<br />
Probing Depth (mm) 2 2 2<br />
Restoration NoneComposite (Pal) None<br />
Further radiographic investigation in April 2008 revealed that the patient was suffering from a<br />
discontinuation of the lamina dura on tooth 22, as well as a large circumscribed apical radiolucency<br />
(Ø 15mm). The radiographic findings in the coronal part of the root were diagnosed as<br />
dens-in-dente (see Figure 4).<br />
Following the investigations,<br />
the diagnosis showed that a periradicular<br />
abscess was related to<br />
non-vital tooth 22. The problems<br />
associated with the diagnosis<br />
were a wide root canal, and an<br />
open apex with large apical<br />
lesion.<br />
The structured treatment<br />
plan involved conventional root<br />
canal treatment, and to be assess<br />
for surgery after six months.<br />
The treatment plan<br />
Treatment commenced on 3<br />
April 2008. Following an initial<br />
clinical examination, the tooth<br />
was diagnosed with & apical<br />
abscess (no sinus present). Access<br />
was gained under a rubber<br />
dam and the canal was filled<br />
with exudate.<br />
The root canal length was<br />
determined both by apex locator<br />
(RootZX) and a periapical radiograph.<br />
The root canal disinfection<br />
was completed mechanically<br />
using Hedstroms files<br />
(size 90/20 mm/incisal edge).<br />
Particular care was taken<br />
during irrigation due to the<br />
open apex, & ultrasonics were<br />
used for the further cleaning<br />
of the canal. A formula of one<br />
per cent NaOCl, two per cent<br />
CHX and 17 per cent EDTA were<br />
used for chemical root canal<br />
disinfection. The canal was<br />
dressed with Ca(OH)2 and IRM<br />
was applied as a temporary<br />
filling.<br />
Five days after the completion<br />
of the treatment, the patient<br />
sought an emergency consultation<br />
because of severe pain and<br />
swelling from tooth 22. He was<br />
prescribed an eight-day course<br />
of clindamycin (500 mg x 3*3)<br />
to ease the discomfort.<br />
Following the surgery, on<br />
May 29, tooth 22 was asymptomatic<br />
and swill sensitive to percussion.<br />
The temporary filling<br />
was removed and the root canal<br />
disinfected again with Irrisafe,<br />
as well as a formula of one<br />
percen NaOCl, two per cent<br />
CHX and 17 per cent EDTA.<br />
A long-term intra- canal dressing<br />
with Ca(OH)2 was placed, and<br />
IRM was applied as a temporary<br />
filling.<br />
Preparing for root<br />
treatment<br />
The patient missed the following<br />
three appointments, but returned<br />
on October 14. On this<br />
date the tooth was still sensitive<br />
to percussion and palpation. As<br />
there were no real signs of improvement,<br />
it was decided that<br />
the tooth should be root filled &<br />
an appointment for apical surgery<br />
was made. To ease discomfort,<br />
the root canal was filled<br />
with an 8mm length of white<br />
MTA, & a wet cotton pellet was<br />
placed over the MTA. On top of<br />
the cotton pellet, a temporary<br />
filling with IRM was placed.<br />
Fig. 1: Frontal view<br />
Fig. 2: Frontal view Fig. 3: Occlusal view Fig. 4: Pre-operatve periapical radiograph<br />
Fig. 5: Working lenght radiograph Fig. 6: MTA in the canal Fig. 7: MTA in the canal Fig. 8: MTA, wet cotton pellet and IRM Fig. 9: White MTA in the canal<br />
Fig. 10: Elevation of surgical flap Fig. 11: Granulation osteotomy<br />
Fig. 12: Granulation tissue removed & root-end resection performed Fig. 13: Flap sutured with 6-0 silk sutures
10<br />
Clinical DeNtal tribuNe | april-June, 2010<br />
Fig. 14: Suturing at the junction between the mesial<br />
vertical releasing incision and the horizontal<br />
marginal incision<br />
Fig. 15: Wound healing before removal of sutures<br />
Fig. 16: Wound healing at the junction between the<br />
mesial verical releasing incision and the horizontal<br />
marginal incision before removal of sutures<br />
Fig. 17: Wound healing after removal of sutures<br />
Fig. 18: Occlusal view after removal of sutures Fig. 19: Composite filling on the palatal aspect of tooth 22 Fig. 20: Post-operative view Fig. 21: Post-operative periapical<br />
radiographs<br />
The re-operative procedure<br />
a root-end resection of about<br />
tablets (qds 660 mg *4) for seven<br />
lined cystic wall with intense<br />
About the author<br />
was carried out on November<br />
three millimeters of the root.<br />
days was also given.<br />
chronic to acute inflammation,<br />
6. A marginal incision from<br />
The root end was inspected<br />
The sutures were removed<br />
consistent with a radicular cyst.<br />
the mesial aspect of tooth 21<br />
and to the distal aspect of tooth<br />
23 was made, followed by<br />
through the operating microscope,<br />
& no fracture was found.<br />
on November 13, and there was<br />
evidence of good soft tissue<br />
healing. The patient experi-<br />
Result<br />
Prognosis<br />
5mm vertical releasing incisions<br />
The adaptation of the white<br />
enced no discomfort from the<br />
The patient’s long-term prog-<br />
at the mesial aspect of tooth<br />
MTA to the root canal was judged<br />
surgical site.<br />
nosis is uncertain, due to the<br />
21, and a length of 10mm at the<br />
as good and the operation site<br />
thin root canal walls and risk<br />
distal aspect of tooth 23. The<br />
was inspected and rinsed with<br />
The temporary filling and<br />
of fracture.<br />
mucoperiostal flap was elevated<br />
(see Figure 10), and a pathological<br />
fenestration of the cortical<br />
buccal bone was evident, approximately<br />
3mm from the marginal<br />
bone crest between teeth<br />
22 & 23. An osteotomy was performed<br />
after which the lesion<br />
was treated by curettage. A biopsy<br />
of the lesion was taken.<br />
The palatal cortical bone also<br />
had a pathological perforation,<br />
sterile saline, before being<br />
sutured with five 6-0 silk sutures.<br />
The patient was informed<br />
about the prognosis of the<br />
tooth and given post-operative<br />
instructions. Six 400mg Ibuprofen<br />
tablets were dispensed, and<br />
the patient was instructed to<br />
take one every four hours in<br />
the first day following surgery.<br />
A prescription of Penicillin V<br />
cotton pellet were removed<br />
during the post-treatment restoration<br />
procedure, and replaced<br />
by a composite restoration<br />
(35 per cent phosphoric acid,<br />
Adper, Scotchbond, Filtek Flow<br />
(A3) in the apical part, Filtek<br />
Supreme (A3D and A2B) in the<br />
coronal part). Teeth 21 and<br />
23 maintained vitality. The histological<br />
report of the lesion<br />
showed a partial epithelium<br />
Follow-up<br />
On November 13 for a twelvemonth<br />
post-surgery appointment,<br />
the patient was still asymptomatic.<br />
Teeth 21 and 23<br />
were sensitive to ice-test, and<br />
there were no periodontal probing<br />
depths over four millimetres<br />
around tooth 22.<br />
The radiograph showed<br />
evidence of healing. DT<br />
Dr Nicolai Orsteen graduated<br />
from the University of Oslo in January<br />
2002, completing his specialist<br />
training in endodontics in June<br />
2009. He then worked in general<br />
practice in Oslo from February 2002<br />
was also a secretary on the regional<br />
dental board in Norway from 2004<br />
to 2006. From August 2008, Nicolai<br />
worked at a specialist practice in<br />
Oslo before joining the specialist<br />
team at Endocare Richmond and<br />
Harley Street. For more information<br />
please call 020 7224 0999 email<br />
reception@endocare.co.uk or visit<br />
www.endocare.co.uk .
12<br />
interview DeNtal tribuNe | april-June, 2010<br />
“Evolution of mini-implants”<br />
Interview with Dr Oliver Hennedige, Singapore<br />
Dr Oliver Hennedige is the<br />
Secretary General of Asia Pacific<br />
Dental Federation (APDF) and<br />
is Executive Director, International<br />
College of Continuing<br />
Dental Education (ICCDE). He<br />
runs a very successful group<br />
dental practice in Singapore,<br />
and lectures and demonstrates<br />
extensively on mini dental<br />
implants. DT India editor, Isha<br />
Goel, had a chance to speak with<br />
Dr Oliver during a workshop,<br />
organized by APDF, ICCDE, and<br />
Indian Dental Association (IDA)<br />
recently in New Delhi, India.<br />
Isha Goel: The dental implants<br />
have been the most influential<br />
change in dentistry and you recently<br />
shared your views about<br />
evolution of mini-implants in a<br />
workshop organized by Asia<br />
Pacific Dental Federation, ICCDE,<br />
and IDA recently in New Delhi,<br />
India. Can you give our readers<br />
an overview of the rationale<br />
for use of mini-implants?<br />
Dr Oliver: Mini dental implants<br />
evolved because of the drawbacks<br />
and failures of the larger<br />
diameter conventional implants.<br />
Conventional implants, while<br />
being promoted as the panacea<br />
for missing teeth, have a high<br />
failure rate as these would require<br />
an invasive procedure,<br />
a very skillful operator, a lot of<br />
understanding, and the use of<br />
a complex range of specialized<br />
and specific instruments. The<br />
complexity has resulted in strict<br />
protocols that hoped to minimize<br />
failures.<br />
While conventional dental<br />
implants are successful in the<br />
hands of an experienced and<br />
competent operator, it generally<br />
failed in the hands of those with<br />
less experience. It took time, and<br />
usually a lot of failures on the<br />
way before a dentist or specialist<br />
became adept in placing conventional<br />
implants.<br />
About 24 years ago, an accomplished<br />
implantologist, Dr Victor<br />
Sendax of America, decided to<br />
question the protocol and rationale<br />
in placing large diameter<br />
implants. He developed the<br />
small diameter implants with a<br />
straightforward protocol, which,<br />
in most instances require no<br />
surgery, and with an initial entry<br />
point with only a pilot drill, he<br />
proposed a self-tapping (screwing)<br />
procedure, which not only<br />
delivered the implant into the<br />
bone but also firmly secured it<br />
into its place. It was minimally<br />
invasive, incredibly less traumatic,<br />
and painless. It allowed<br />
the operator to stabilize dentures<br />
and securely fix crowns and<br />
bridges. Today, it is widely used<br />
worldwide and will, in my view,<br />
replace conventional implants.<br />
There are very few instances<br />
indeed and mini-implants, once<br />
it is understood, will become<br />
standard practice. In fact, there<br />
is an exponential growth of<br />
mini-implants in America and<br />
worldwide, because of simplicity,<br />
extremely high success rate,<br />
and above all patients talk about<br />
the straightforward procedures<br />
and good aesthetic results.<br />
Mini-implants growth is<br />
phenomenal and will be a procedure,<br />
which every dentist of<br />
the present and future generation<br />
will need to know. Its growth<br />
will be driven by patients’<br />
demand.<br />
How do mini-implants osseointegrate<br />
and what is your<br />
experience on their long-term<br />
stability?<br />
The probability of osseointegrating<br />
of mini-implant is much<br />
greater, as it does not utilize<br />
osteotomy (in simple terms,<br />
cutting out large chunks of bone<br />
in order to introduce the conventional<br />
implants). Without the<br />
trauma of this procedure, which<br />
may generate excessive heat,<br />
may ultimately result in bone<br />
necrosis & failure of the conventional<br />
implants, mini-implants<br />
utilize a self-tapping procedure,<br />
which allow, intimate and firm<br />
contact of mini-implant to bone,<br />
once it is introduced.<br />
With the specific design like<br />
a typical screw and surface<br />
coating osseointegration takes<br />
place, I must caution not all<br />
mini-implants and conventional<br />
implants are the same. They<br />
are not generic products, and<br />
you have to choose your miniimplant<br />
carefully, i.e., the company<br />
that produces it.<br />
in immediately extracted socket.<br />
What I do, is measure the length<br />
of the extracted root, choose<br />
a mini-implant at least 2-3 mm<br />
longer than the lenght of the<br />
root, and utilize the same procedure<br />
of the initial use of a pilot<br />
drill, I introduce the miniimplants<br />
into the socket. It is<br />
growth wherever these are<br />
introduced.<br />
What are the advantages and<br />
disadvantages of mini-implants<br />
over conventional implants, and<br />
are there limits for their use?<br />
Really, the advantages of miniimplants<br />
I utilize Mini Drive-Lock,<br />
(MDL), coming from the United<br />
firm and I always pack a bone<br />
augmentation material into the are phenomenal. You<br />
can even use in medically<br />
States of America. It has really socket and stitch tight the opening.<br />
compromised patients with<br />
good properties which allow<br />
easy placement and long-term<br />
stability, especially for crowns<br />
and bridges. The Food and<br />
If the opening is large,<br />
e.g., molar extraction, I place a<br />
membrane over the socket, so as<br />
to prevent washing out of the<br />
controlled diabetes, heart condition,<br />
and for those who are suffering<br />
from Alzheimer where there<br />
is very poor control of jaw<br />
Drug Administration from bone augmentation material. movement, stabilized dentures<br />
Dr Oliver, Dr Anil Kholi, Dr Jeffrey Tsang, and Dr Paramjit Singh (from left to right) during the workshop in New Delhi, India.<br />
America, which is very stringent<br />
in its protocol, has accepted<br />
MDL for long-term use in the<br />
mouth.<br />
I allow initial healing for<br />
about 3-4 weeks and then proceed<br />
to do the prosthetic aspect.<br />
I’ve met with very good results.<br />
I use Perioglas from the USA<br />
My experience having placed for best results.<br />
more than 3000 units, is that<br />
mini-implants not only work,<br />
patients love them and these<br />
are an excellent practice builder.<br />
I can safely say that I enjoy at<br />
least a 95 percent success<br />
rate. I see my patients regularly<br />
for all dental procedures on a<br />
6 monthly recall and miniimplants<br />
An observant selection, appropriate<br />
treatment plan, precise<br />
surgery, and proper design of<br />
prosthesis are essential for optimal<br />
outcome. How will you<br />
grade the success rate of miniimplants<br />
in comparison with<br />
conventional implants?<br />
placed in more than<br />
seven years ago (that is when Frankly speaking, there is<br />
I embarked on mini-implants)<br />
are still functioning well. It<br />
is truly an advancement that<br />
the dental profession cannot<br />
ignore.<br />
really no comparison. Miniimplants<br />
were actually developed<br />
because of the drawbacks<br />
and failures of conventional<br />
dental implants. They are affordable<br />
and are really revolutionizing<br />
Canmini-implants also be placed<br />
in the socket immediately after<br />
the tooth extraction like we do<br />
with the regular implants?<br />
the use of dental implants.<br />
As I predicted, seven years ago<br />
in an article, it will bring about<br />
a paradigm shift in the use of<br />
dental implants. Mini-implants<br />
In my practice and in my lectures,<br />
I teach the use of mini-implants<br />
are so successful that these<br />
are experiencing exponential<br />
with mini-implants or fixed<br />
crowns and bridges have been<br />
a gift to them.<br />
Very old and frail patients<br />
with badly resorbed jaws need<br />
not undergo invasive procedures<br />
of bone build-up. They<br />
can be really benefited with the<br />
use of mini-implants. I’ve placed<br />
mini-implants in such patients<br />
in their late seventies and<br />
eighties. Some of my patients<br />
are still eating well and living<br />
quality lives right into their<br />
nineties.<br />
I believe mini-implants will<br />
continue to evolve and a whole<br />
range of uses will come into<br />
existence, as they are minimally<br />
invasive, easy to use, operator<br />
friendly, patient friendly, and<br />
will be really a boon to patient<br />
care. Mini-implants are affordable<br />
and cost a fraction of<br />
conventional implants.<br />
Dr Oliver thank you very much<br />
for the interview.<br />
DT
Issue 2<br />
March 2010<br />
Proper Technique Helps Prevent Potential Oral Problems<br />
Brushing off<br />
Dentin Hyper<br />
the health of the<br />
dentition, may actually<br />
be a significan t factor in<br />
undermining the tooth<br />
structure and, in<br />
consequence, oral<br />
health, itself.<br />
Vigorous and<br />
horizontally directed<br />
strokes particularly on<br />
the gum area can wear a<br />
v-shaped abrasion on the neck of the tooth. This will<br />
render a large number of dentinal tubules exposed<br />
and open to the oral environment and the fluids<br />
inside vulnerable to rapid pressure changes which in<br />
turn elicit nerve response perceived as a painful<br />
sensation by the patient.<br />
Behavioral modification coupled with the use of<br />
“tissue friendly” soft toothbrush and gentle<br />
toothpaste may significantly prevent the<br />
unnecessary exposure of dentinal tubules. Using<br />
soft-bristled tooth brush, the patient may direct<br />
the tufts at a 45-degree angle around the gum<br />
area and apply deliberate but gentle sweeping<br />
strokes along the tooth surface towards the<br />
incisal or cuspal surfaces. The gum area should<br />
also be covered in the gentle brushing to aid in<br />
Dentinal hypersensitivity is described clinically as a<br />
short, sharp pain due to exposed dentinal tubules<br />
responding to a variety of external stimuli which<br />
includes thermal, osmotic, mechanical, evaporative,<br />
and tactile stimuli.<br />
Common treatment modalities usually involve<br />
prevention of the occurrence of nerve stimulation by<br />
either occluding the dentinal tubules or altering the<br />
nerve stimulation process. Reduction or elimination<br />
of risk factors, which include appropriate behavioral<br />
conditioning among others, is also an integral<br />
component of managing dentinal hypersensitivity.<br />
The exposure of dentinal tubules is generally<br />
attributed to the loss of tooth substance, both<br />
enamel and cementum. One of the factors<br />
contributing to the surface loss is poor tooth<br />
brushing technique. If done injudiciously,<br />
toothbrushing, the very activity designed to protect<br />
Opening of the dentinal tubules<br />
( Scanning Electron Microscope)<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
the top five oral problems which may compel an individual to seek dental care.<br />
YOUR PARTNER IN ORAL HEALTH<br />
<br />
Issue 2<br />
<br />
Issue 2<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
March 2010<br />
Issue 2<br />
<br />
March 2010<br />
Issue 2<br />
Brushing off<br />
<br />
Brushing off<br />
<br />
Brushing off<br />
<br />
Brushing off<br />
<br />
Brushing off<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
Dentin Hyper<br />
Brushing off<br />
<br />
Dentin Hyper<br />
Brushing off<br />
<br />
Dentin Hyper<br />
Brushing off<br />
<br />
Dentin Hyper<br />
Brushing off<br />
<br />
Dentin Hyper<br />
Brushing off<br />
<br />
Dentin Hyper<br />
<br />
Dentin Hyper<br />
<br />
Dentin Hyper<br />
<br />
Dentin Hyper<br />
<br />
Dentin Hyper<br />
<br />
Dentin Hyper<br />
<br />
<br />
<br />
<br />
Dentin Hyper<br />
Proper Technique Helps Prevent Potential Oral Problems<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
<br />
Dentin Hyper<br />
Proper Technique Helps Prevent Potential Oral Problems<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
<br />
Dentin Hyper<br />
Proper Technique Helps Prevent Potential Oral Problems<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
<br />
Dentin Hyper<br />
Proper Technique Helps Prevent Potential Oral Problems<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
<br />
Dentin Hyper<br />
Proper Technique Helps Prevent Potential Oral Problems<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
<br />
Dentin Hyper<br />
Proper Technique Helps Prevent Potential Oral Problems<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
<br />
Dentin Hyper<br />
<br />
Dentin Hyper<br />
<br />
Dentin Hyper<br />
<br />
Dentin Hyper<br />
<br />
Dentin Hyper<br />
<br />
<br />
<br />
<br />
includes thermal, osmotic, mechanical, evaporative,<br />
responding to a variety of external stimuli which<br />
short, sharp pain due to exposed dentinal tubules<br />
Dentinal hypersensitivity is described clinically as a<br />
the top five oral problems which may compel an individual to seek dental care.<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
<br />
includes thermal, osmotic, mechanical, evaporative,<br />
responding to a variety of external stimuli which<br />
short, sharp pain due to exposed dentinal tubules<br />
Dentinal hypersensitivity is described clinically as a<br />
the top five oral problems which may compel an individual to seek dental care.<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
<br />
includes thermal, osmotic, mechanical, evaporative,<br />
responding to a variety of external stimuli which<br />
short, sharp pain due to exposed dentinal tubules<br />
Dentinal hypersensitivity is described clinically as a<br />
undermining the tooth<br />
be a significan t factor in<br />
dentition, may actually<br />
the health of the<br />
the top five oral problems which may compel an individual to seek dental care.<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
<br />
undermining the tooth<br />
be a significan t factor in<br />
dentition, may actually<br />
the health of the<br />
the top five oral problems which may compel an individual to seek dental care.<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
<br />
undermining the tooth<br />
be a significan t factor in<br />
dentition, may actually<br />
the top five oral problems which may compel an individual to seek dental care.<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
<br />
the top five oral problems which may compel an individual to seek dental care.<br />
There is a growing professional awareness that dentinal hypersensitivity is one of<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
conditioning among others, is also an integral<br />
of risk factors, which include appropriate behavioral<br />
nerve stimulation process. Reduction or elimination<br />
either occluding the dentinal tubules or altering the<br />
prevention of the occurrence of nerve stimulation by<br />
Common treatment modalities usually involve<br />
and tactile stimuli.<br />
<br />
conditioning among others, is also an integral<br />
of risk factors, which include appropriate behavioral<br />
nerve stimulation process. Reduction or elimination<br />
either occluding the dentinal tubules or altering the<br />
prevention of the occurrence of nerve stimulation by<br />
Common treatment modalities usually involve<br />
and tactile stimuli.<br />
<br />
conditioning among others, is also an integral<br />
of risk factors, which include appropriate behavioral<br />
nerve stimulation process. Reduction or elimination<br />
either occluding the dentinal tubules or altering the<br />
prevention of the occurrence of nerve stimulation by<br />
Common treatment modalities usually involve<br />
includes thermal, osmotic, mechanical, evaporative,<br />
the gum area can wear a<br />
strokes particularly on<br />
horizontally directed<br />
Vigorous and<br />
health, itself.<br />
consequence, oral<br />
structure and, in<br />
<br />
the gum area can wear a<br />
strokes particularly on<br />
horizontally directed<br />
Vigorous and<br />
health, itself.<br />
consequence, oral<br />
structure and, in<br />
undermining the tooth<br />
<br />
the gum area can wear a<br />
strokes particularly on<br />
horizontally directed<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
brushing technique. If done injudiciously,<br />
contributing to the surface loss is poor tooth<br />
enamel and cementum. One of the factors<br />
attributed to the loss of tooth substance, both<br />
The exposure of dentinal tubules is generally<br />
component of managing dentinal hypersensitivity.<br />
conditioning among others, is also an integral<br />
<br />
brushing technique. If done injudiciously,<br />
contributing to the surface loss is poor tooth<br />
enamel and cementum. One of the factors<br />
attributed to the loss of tooth substance, both<br />
The exposure of dentinal tubules is generally<br />
component of managing dentinal hypersensitivity.<br />
conditioning among others, is also an integral<br />
<br />
brushing technique. If done injudiciously,<br />
contributing to the surface loss is poor tooth<br />
enamel and cementum. One of the factors<br />
attributed to the loss of tooth substance, both<br />
The exposure of dentinal tubules is generally<br />
component of managing dentinal hypersensitivity.<br />
conditioning among others, is also an integral<br />
sensation by the patient.<br />
turn elicit nerve response perceived as a painful<br />
inside vulnerable to rapid pressure changes which in<br />
and open to the oral environment and the fluids<br />
render a large number of dentinal tubules exposed<br />
v-shaped abrasion on the neck of the tooth. This will<br />
the gum area can wear a<br />
<br />
sensation by the patient.<br />
turn elicit nerve response perceived as a painful<br />
inside vulnerable to rapid pressure changes which in<br />
and open to the oral environment and the fluids<br />
render a large number of dentinal tubules exposed<br />
v-shaped abrasion on the neck of the tooth. This will<br />
the gum area can wear a<br />
<br />
sensation by the patient.<br />
turn elicit nerve response perceived as a painful<br />
inside vulnerable to rapid pressure changes which in<br />
and open to the oral environment and the fluids<br />
render a large number of dentinal tubules exposed<br />
v-shaped abrasion on the neck of the tooth. This will<br />
the gum area can wear a<br />
<br />
turn elicit nerve response perceived as a painful<br />
inside vulnerable to rapid pressure changes which in<br />
and open to the oral environment and the fluids<br />
render a large number of dentinal tubules exposed<br />
v-shaped abrasion on the neck of the tooth. This will<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
toothbrushing, the very activity designed to protect<br />
<br />
toothbrushing, the very activity designed to protect<br />
<br />
toothbrushing, the very activity designed to protect<br />
area and apply deliberate but gentle sweeping<br />
the tufts at a 45-degree angle around the gum<br />
soft-bristled tooth brush, the patient may direct<br />
unnecessary exposure of dentinal tubules.<br />
toothpaste may significantly prevent the<br />
“tissue friendly” soft toothbrush and gentle<br />
Behavioral modification coupled with the use of<br />
<br />
area and apply deliberate but gentle sweeping<br />
the tufts at a 45-degree angle around the gum<br />
soft-bristled tooth brush, the patient may direct<br />
unnecessary exposure of dentinal tubules.<br />
toothpaste may significantly prevent the<br />
“tissue friendly” soft toothbrush and gentle<br />
Behavioral modification coupled with the use of<br />
<br />
area and apply deliberate but gentle sweeping<br />
the tufts at a 45-degree angle around the gum<br />
soft-bristled tooth brush, the patient may direct<br />
unnecessary exposure of dentinal tubules.<br />
toothpaste may significantly prevent the<br />
“tissue friendly” soft toothbrush and gentle<br />
Behavioral modification coupled with the use of<br />
<br />
area and apply deliberate but gentle sweeping<br />
the tufts at a 45-degree angle around the gum<br />
soft-bristled tooth brush, the patient may direct<br />
unnecessary exposure of dentinal tubules. Using<br />
toothpaste may significantly prevent the<br />
“tissue friendly” soft toothbrush and gentle<br />
Behavioral modification coupled with the use of<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
also be covered in the gentle brushing to aid in<br />
incisal or cuspal surfaces.<br />
strokes along the tooth surface towards the<br />
<br />
also be covered in the gentle brushing to aid in<br />
incisal or cuspal surfaces.<br />
strokes along the tooth surface towards the<br />
area and apply deliberate but gentle sweeping<br />
<br />
also be covered in the gentle brushing to aid in<br />
The gum area should<br />
incisal or cuspal surfaces.<br />
strokes along the tooth surface towards the<br />
area and apply deliberate but gentle sweeping<br />
<br />
also be covered in the gentle brushing to aid in<br />
The gum area should<br />
strokes along the tooth surface towards the<br />
area and apply deliberate but gentle sweeping<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
YOUR<br />
<br />
<br />
<br />
IN<br />
<br />
<br />
<br />
R IN OR<br />
ER<br />
ARTNE<br />
YOUR PA<br />
<br />
H<br />
<br />
<br />
<br />
<br />
ALTH<br />
AL HEA<br />
N ORA<br />
<br />
H
THE DENTAL PROFESSION & PATIENT<br />
PARTNERSHIP<br />
ORAL CARE LINK<br />
OATE COLGATE PROFESSIONAL INFORMATION CENTER<br />
sensitivity<br />
Dr. Arturo De Leon<br />
Dean of Fatima College of Dentistry<br />
Philippines<br />
enhancing tissue stimulation and blood circulation<br />
for a more improved health of the gingiva.<br />
Brushing the teeth correctly, at least<br />
twice a day, with fluoride-containing<br />
toothpaste may help provide the<br />
individual with an acid-resistant<br />
protective layer.<br />
And in case of the<br />
onset of symptoms of dentinal<br />
hypersensitivity, one may find relief by<br />
using hypersensitivity relieving paste. In search of<br />
such appropriate relief, scientific advancements are<br />
directed towards the use of natural existing<br />
ingredients and more natural ways of relieving<br />
dentin hypersensitivity (e.g. sealing or occluding the<br />
dentinal tubules with calcium and phosphate -rich<br />
materials). As reported a more recent<br />
technological breakthrough paved the way<br />
towards the development of a toothpaste which<br />
is clinically proven to provide immediate and<br />
lasting relief from dentin hypersensitivity with<br />
the use of a naturally occurring amino acid found<br />
in saliva.<br />
A two-minute brushing is said to be sufficient to<br />
clean the different surfaces of the dentition. It is just<br />
like enjoying your favorite music while doing<br />
something after savoring your favorite dish or meal.<br />
Undoubtedly, it is also like brushing off a potential<br />
problem like dentinal hypersensitivity while enjoying<br />
an after-meal personal hygiene activity towards a<br />
healthy smile.<br />
Cuspal<br />
Colgate® 360°® Sensitive toothbrush<br />
www.colgateprofessional.com<br />
ww.<br />
ofes<br />
si<br />
onal.<br />
.com<br />
<br />
<br />
w<br />
i m
DeNtal tribuNe | april-June, 2010 Product Spotlight 17<br />
Saddle stool in dentistry<br />
Veli-Jussi Jalkanen, specialist in sitting ergonomics discusses a healthy and comfortable way to sit<br />
Dental Events<br />
2010<br />
While some dental professionals<br />
have insufficient knowledge to<br />
be able to recognise or manage<br />
sitting disorders, others realise<br />
that back pain and shoulder<br />
tension have a lot to do with<br />
sitting. Poor circulation in the<br />
lower extremities; shortage of<br />
oxygen; hip, knee and shoulder<br />
joint problems; sitting fatigue,<br />
and genital health problems<br />
are some examples of the ailments<br />
that belong to the large<br />
group of SDs (Sitting Disorders).<br />
All people working in dentistry<br />
are affected by these disorders<br />
whether they are aware of them<br />
or not. Many of those who are<br />
aware of SDs would usually like<br />
to improve the situation and look<br />
for a more healthy, productive<br />
and comfortable way to work.<br />
Healthy posture for long<br />
term sitting:<br />
1. Good, relaxed posture, balanced<br />
and without harmful<br />
supports<br />
2. Thighs 90° apart and pointing<br />
down enough to keep the<br />
upper body in balance<br />
3. Close to 135° angles in hips<br />
and knees<br />
4. Weight on the sitting bones,<br />
not the muscles<br />
5. No pressure on the genitals<br />
and under the hip (especially<br />
for men)<br />
This ideal position can be<br />
obtained with a saddle stool.<br />
Sitting on a saddle stool<br />
is based…<br />
…on the sitting bones that are<br />
located under the hip. They<br />
keep the buttocks and thighs<br />
from being pressed against the<br />
seat if they have a firm support.<br />
Thighs point down at a 45<br />
degree angle, tilting the pelvis<br />
to a near neutral position, as<br />
when standing. This allows the<br />
lower back and upper body to<br />
find a relaxed, natural posture<br />
without the need for a backrest.<br />
Feet rest on the floor on both<br />
sides of the body as if you were<br />
riding a horse. This way it is easy<br />
to operate pedals with your feet -<br />
they must be placed on the side.<br />
General benefits from a<br />
saddle stool in dentistry<br />
• Good, natural and relaxed<br />
posture which also keeps improving<br />
for years<br />
• Less shoulder area tension by<br />
allowing lower positioning of<br />
the patient<br />
• Relieving or eliminating<br />
lower back pain (oftentimes<br />
it disappears in a week)<br />
• Preventing fatigue & improving<br />
productivity through<br />
deeper breathing<br />
• Preventing shoulder, hip and<br />
knee joint problems, angles<br />
are more natural<br />
• Easier movements and good<br />
working positions<br />
• Improved circulation in lower<br />
extremities prevents varicose<br />
veins + cellulite built up<br />
• Easy visibility into the mouth<br />
by leaning forward with a<br />
straight back<br />
• Working at a close distance<br />
(also the assistant) with legs<br />
under the hoisted chair<br />
• Easy rolling & turning makes<br />
picking materials fast and<br />
effortless<br />
A divided seat is helpful…<br />
… because the free space allows<br />
proper pelvis/hip position without<br />
pressure or discomfort in<br />
the soft tissues on the pubic bone.<br />
For men (who have the pubic<br />
bone much further back than<br />
women) a divided seat is a safer<br />
solution in the long run. Pressure<br />
on the pudendal nerve & tissues<br />
on the pubic bone can lead to<br />
erectile dysfunction. Loose, light<br />
and stretching trousers are highly<br />
recommended for men when<br />
sitting on any seats. With women,<br />
an additional advantage is the<br />
decreased growth of bacteria<br />
as a result of better ventilation,<br />
lower humidity and temperature<br />
in the genital area. This has a<br />
positive effect on the Footoperated<br />
height control (accessory)<br />
keeps the gloves clean & is very<br />
helpful in maintaining the welfare<br />
of your body and accuracy<br />
of your work while you change<br />
positions and sitting height in the<br />
middle of a long procedure.<br />
Shoulder joint problems…<br />
…often come from elevated<br />
shoulder positions, which stress<br />
the joints. A riding-like sitting<br />
position allows lower positioning<br />
of the patient, which allows you<br />
to relax your shoulders.<br />
Sitting down & standing<br />
up…<br />
…is easy because on a saddle<br />
stool you are half way up already.<br />
Sitting down could not be any<br />
more fluent since the backrest is<br />
never in the way. You just lift your<br />
leg over the seat from the back<br />
and sit down. This kind of mounting<br />
puts you instantly into the<br />
right kind of relaxed sitting<br />
position with good posture.<br />
Data entering…<br />
…is more fluent and time-saving<br />
when you can roll back and forth<br />
fast and easily with your saddle<br />
chair. The movements you do<br />
while using the chair keep your<br />
muscles active and improve your<br />
metabolism.<br />
The Scandinavian<br />
working concept…<br />
…is shown in the pictures. Oftentimes,<br />
both the dentist and the<br />
assistant utilise a saddle stool.<br />
Good posture, easy visibility into<br />
the patient’s mouth, efficient and<br />
free movement can all become<br />
reality. The saddle stool allows<br />
close proximity to the patient,<br />
leaving more room for the legs<br />
under the patient. This method of<br />
working dramatically decreases<br />
problems for both the dentist and<br />
the assistant, and is becoming the<br />
most common way to sit and<br />
work for dentist in Scandinavia.<br />
Adapting to a saddle<br />
chair takes some effort…<br />
…because almost everything<br />
changes. The body needs time to<br />
adjust. Learning to use the saddle<br />
chair takes a few days and the<br />
“saddle soreness” in the buttocks<br />
and inner thighs as well as<br />
fatigue of the back muscles last<br />
two-14 days.<br />
It is worth it, but…<br />
…nothing comes for free. Financially,<br />
the change is cheap. But<br />
most importantly, you need<br />
to learn about sitting physiology<br />
to be motivated to make the<br />
change, alter your working<br />
movements and positions and<br />
tolerate temporary discomfort.<br />
As a return you may achieve a<br />
healthier body, better posture,<br />
higher productivity (more<br />
patients with the same energy),<br />
improved quality of work and<br />
more satisfying years at work. DT<br />
SINODENTAL<br />
Where: Beijing (China National<br />
Convention Center)<br />
Date: 09-12 June 2010<br />
Web site: www.sinodent.com.cn<br />
1 st HONG KONG INTERNATIONAL<br />
DENTAL EXPO<br />
Where: Hong Kong<br />
Hong Kong Dental Association<br />
Date: 18-20 June 2010<br />
Web site: www.hkideas.org<br />
35 th Annual Meeting of American<br />
Academy of Esthetic Dentistry<br />
Where: Chicago, USA<br />
Date: 03-08 August 2010<br />
Web site: www.estheticacademy.org<br />
ICOI World Congress<br />
Where: Hamburg, Germany<br />
Date: 26-28 August 2010<br />
Web site: www.icoi.org<br />
FDI WORLD DENTAL CONGRESS<br />
Where: Salvador de Bahia, Brazil<br />
Date: 02-05 September 2010<br />
Web site: www.fdiworldental.org<br />
IDEM INDIA, 2010<br />
Where: Mumbai, India<br />
Date: 09-11 September 2010<br />
Web site: www.idem-india.com<br />
DENTAL EXPO<br />
Where: Moscow<br />
Dental Expo Ltd.<br />
Date: 20-23 September 2010<br />
Web site: www.dental-expo.com<br />
International Expo Dental<br />
Where: Rome, Italy<br />
Date: 07-09 October 2010<br />
Web site: www.expodental.it<br />
ADA Annual Session<br />
American Dental Association<br />
Where: Orlando, United States<br />
Date: 09-12 October 2010<br />
Web site: www.ada.org<br />
BDTA Dental Showcase<br />
Where: Excel, London<br />
Date: 14-16 October 2010<br />
Web site: www.bdta.org.uk<br />
World Dental Show<br />
Where: Mumbai, India<br />
Date: 29-31 October 2010<br />
Web site: www.wds.org.in<br />
Dentech China 2010<br />
Where: Shanghai, China<br />
Date: 02-05 November 2010<br />
Web site: www.dentech.com.cn<br />
54 th AMIC Dental Expo<br />
Where: Mexico City, Mexico<br />
Date: 03-07 November 2010<br />
Web site: www.amicdental.com.mx<br />
FAMDENT SHOW 2010<br />
Where: Hyderabad, India<br />
Date: 26-28 November 2010<br />
Email: famdentresponse@gmail.com<br />
The Great New York Dental Meeting<br />
Where: New York, USA<br />
Date: 26 Nov-01 Dec 2010<br />
Web site: www.gnydm.com DT
18<br />
trends DeNtal tribuNe | april-June, 2010<br />
Current concepts in gutta-percha removal for re-treatment<br />
Two-part series by Dr Roheet Khatavkar & Dr Vivek Hegde—Part I<br />
Common reasons for an endo-<br />
3. Combination of paper points<br />
are available usually in amber-<br />
remnants. 3,4 Paper points can<br />
the gutta-percha by frictional<br />
dontic failure include missed<br />
and gutta-percha solvent<br />
colored bottles.<br />
also be used for retrieving sludge<br />
heat and facilitates its removal<br />
canals, ledge formation, perfo-<br />
4. Rotary instruments<br />
of soft-ened gutta-percha for-<br />
from the root canal by its H-file<br />
rations, separated instruments,<br />
a. Gates Glidden drill/Peeso<br />
Chloroform has been proven<br />
med on the reaction of solvent<br />
like flute design. These stainless<br />
inadequately filled canals, coro-<br />
reamer<br />
to be most successful in plastic-<br />
with gutta-percha.<br />
steel drills are more effective<br />
nal leakage, and error in post<br />
b. GPX gutta-percha remover<br />
izing gutta-percha points, and<br />
in the coronal and middle –third<br />
placement.<br />
c. NiTi rotary instruments<br />
thus facilitating its removal from<br />
The ‘wicking technique’ is<br />
portion of the root canals. These<br />
5. Specialized rotary instruments<br />
root canals during retreatment.<br />
used, i.e., flushing the root canal<br />
drills are available in various<br />
For a successful orthograde<br />
designed for retreatment<br />
The reported adverse effects<br />
with solvent followed by drying<br />
sizes, ranging from ISO 25–50,<br />
retreatment, the removal of the<br />
a. ProTaper Universal retreat-<br />
on the health, from exposure to<br />
it with paper points, which helps<br />
and more recently introduced<br />
endodontic filling material, such<br />
ment instruments<br />
chloroform, have necessitated<br />
in removing the softened gutta-<br />
NiTi GPX removers that can be<br />
as gutta-percha, is essential to<br />
b. Mtwo retreatment files<br />
the use of a less hazardous<br />
percha along with paper points.<br />
used in curved canals as well<br />
allow access to the canals for<br />
c. R-Endo retreatment files<br />
solvent replacing chloroform. 1, 2<br />
This technique is very useful in<br />
(Fig. 3).<br />
a successful debridement and<br />
re-obturation of the root canal<br />
6. Heat transfer devices<br />
a. Heat carrier tips<br />
The use of solvent softens<br />
narrow canals or the canals with<br />
a greater degree of curvature.<br />
C. NiTi Rotary Instruments<br />
system. This article deals with<br />
the removal of gutta-percha<br />
b. Ultrasonic tips<br />
7. Soft tissue laser.<br />
the gutta-percha, and then softened<br />
gutta-percha can be easily<br />
4. Rotary Instruments<br />
The use of NiTi Rotary instruments<br />
have the advantage of<br />
based obturating material, as<br />
an essential step in a successful<br />
1. K-files or H-files<br />
removed from the canals by<br />
placing the file into the canals<br />
A. Gates Glidden Drill and Peeso<br />
Reamer<br />
removing gutta-percha as well<br />
as shaping the root canals in an<br />
endodontic retreatment.<br />
K-files or H-files are the basic<br />
and applying firm pressure<br />
The use of Gates Glidden drill<br />
under-prepared tooth, simulta-<br />
instruments in an endodontist’s<br />
against the canal walls.<br />
or Peeso reamer (Figs 2a & b)<br />
neously. The number of studies<br />
The first step in planning for<br />
armamentarium, which can be<br />
is a well-known technique to<br />
carried out for comparing the<br />
a tooth requiring retreatment<br />
used to engage the mass of gutta-<br />
Micro-debriders and openers<br />
remove gutta-percha from the<br />
gutta-percha removal efficacy<br />
is – ‘Coronal disassembly’. This<br />
percha, and by applying an<br />
(Dentsply Maillefer) are small<br />
coronal and middle portion of<br />
of rotary with the hand instru-<br />
involves removal of the coronal<br />
outward firm-pressure mass can<br />
files having 90-degree bend at<br />
the root canal. 5 The non-flexible<br />
mentation, have shown both<br />
restoration including full cover-<br />
be removed. This technique,<br />
the working end and an attac-<br />
head and lateral cutting design<br />
techniques to be almost equally<br />
age restoration, core build-up<br />
however, allows for a gross<br />
hed handle (Fig. 1). It may also<br />
of these instruments do not<br />
effective. 6 It has been advocated<br />
material, and post placed into<br />
removal of gutta-percha espe-<br />
be used to substitute standard<br />
allow instrumentation in the<br />
that the use of rotary devices in<br />
the canal. After gaining access<br />
cially from large canals, which<br />
K-files and H-files.<br />
curved portion of the root canal.<br />
endodontic retreatment should<br />
into the pulp chamber, it is a<br />
prerequisite for the clinician to<br />
inspect the chamber floor for<br />
any missed canals, which can<br />
also be a cause of failure.<br />
are poorly compacted allowing<br />
files to bypass the obturating<br />
material and ‘bite’ into the mass.<br />
2. Gutta-percha Solvents<br />
3. Combination of Paper<br />
Points and Gutta-percha<br />
Solvents:<br />
Most of the literature shows that<br />
Therefore, the additional use<br />
of hand instrument is often<br />
necessary. Due to their stiffness<br />
and predisposition to fracture,<br />
they are safer in the straight<br />
be followed by hand instrumentation<br />
to achieve optimal<br />
cleanliness of root canal walls.<br />
The rotary instruments reach<br />
the whole working length easily,<br />
Techniques for Guttapercha<br />
Removal<br />
The clinician can use various<br />
A wide array of chemicals are<br />
available today as gutta-percha<br />
solvents, such as eucalyptus oil,<br />
turpentine, chloroform, xylol,<br />
gutta-percha filling material<br />
cannot be removed completely<br />
from the root canals. In such<br />
cases, a solvent is flushed into<br />
portions of the canal of anterior<br />
and posterior teeth.<br />
B. GPX Gutta-percha Remover<br />
plasticize gutta-percha through<br />
frictional heat, & remove guttapercha<br />
quickly. Later, hand<br />
instruments can refine and com-<br />
options for the removal of<br />
methylene chloride, orange-<br />
the root canals upto the level<br />
The GPX gutta-percha remover<br />
plete the removal. 6 These instru-<br />
obturating material:<br />
wood oil, methyl chloroform,<br />
of pulp chamber, in an effort<br />
(Prestige Dental) is a specially<br />
ments are recommended to be<br />
1. K-files or H-files<br />
endosolv E, endosolv R, and<br />
to maximize the interaction of<br />
designed file used in a slow-<br />
used at rotational speed of three-<br />
2. Gutta-percha solvent<br />
tetrahydrofuran. These solvents<br />
the solvent and gutta-percha<br />
speed handpiece. It plasticizes<br />
four times more than that of the<br />
rotational speed which is recom-<br />
A<br />
B<br />
mended for routine cleaning<br />
and shaping procedures. The<br />
rotary instruments also have<br />
increased chances of fracture<br />
in case they are forced through<br />
the mass of gutta-percha.<br />
DT<br />
Fig.1: Micro-debriders and Micro-openers from Dentsply Maiellefer<br />
Fig. 2a: Gates Glidden drills nos. 1-6 can be identified by the head-design and<br />
rings on the latch-type attachment<br />
Fig. 2b: Peeso reamers nos. 1-6 can be identified by the longer length of flutes<br />
on the head-design and the rings on latch-type attachment<br />
Editorial note: The references<br />
will be published with part II<br />
of this article in the next edition<br />
of Dental Tribune India.<br />
GPX TM · Stainless Steel Niti GPX TM · Nickel Titanium<br />
About the authors<br />
Packaging unit 6 6 6 6 6 6 Packaging unit 6 6 6 6 6 6<br />
Color code Color code <br />
Size DØ 1/100 mm 025 030 035 040 045 050 Size DØ 1/100 mm 025 030 035 040 045 050<br />
L=21 270..... 2001 2002 2003 2004 2005 2006 L=21 270..... 1901 1902 1903 1904 1905 1906<br />
Assortment 2000<br />
Assortment 1900<br />
CPX TM features a spiraled vent through which gutta-percha is extruded as it is plasterized<br />
from frictional heat.<br />
A latch-type nickel titanium alloy instrument for use on low speed hand pieces. CPX TM<br />
features a spiraled vent through which gutta-percha is extruded as it is plasterized from<br />
frictional heat.<br />
Fig. 3: GPX Stainless Steel & NiTi instruments available for removal of gutta-percha in straight and curved canals respectively<br />
Dr Roheet Khatavkar is a postgraduate<br />
student in the department<br />
of conservative dentistry<br />
and endodontics at M A Rangoonwala<br />
Dental College, Pune, India.<br />
Dr Roheet can be contacted at<br />
drkhatavkar @gmail.com.<br />
Dr Vivek Hegde is professor and<br />
head of the department of conservative<br />
dentistry and endodontics at<br />
M A Rangoonwala Dental College,<br />
Pune, India. He can be contacted<br />
at drvivekhegde@rediffmail.com.
DeNtal tribuNe | april-June, 2010 Clinical 19<br />
Case report: Interdisciplinary full mouth rehabilitation<br />
By Dr Ratnadeep Patil, Dr Kripa Shetty, and Dr Kavita Mahesh, India<br />
Introduction<br />
The success of functional and<br />
esthetic restorations in a case<br />
requiring full mouth rehabilitation<br />
is often dependant on<br />
our understanding of interdisciplinary<br />
concepts. With every<br />
patient being unique and representing<br />
a special blend of age,<br />
personality characteristics as<br />
well as expectations, our knowledge<br />
of interdisciplinary concepts<br />
can open a whole range<br />
of treatment options and outcomes.<br />
1 Today, every dental<br />
practitioner must have a thorough<br />
knowledge of the roles<br />
of these disciplines in producing<br />
an esthetic makeover, with the<br />
most conservative and biologically-sound<br />
interdisciplinary<br />
treatment plan. 2,3<br />
Case Report<br />
A 57-year-old female patient<br />
reported with the complaint of<br />
mobile teeth, spacing in anterior<br />
dentition, missing bridge, and<br />
desire to restore her smile.<br />
During clinical examination,<br />
it was noted that the patient<br />
had deep periodontal pockets,<br />
missing teeth, mobile and migrated<br />
teeth. Diagnostic periapical<br />
radiograph revealed horizontal<br />
bone loss and missing<br />
teeth. Based on the clinical<br />
and radiographical evidence,<br />
it was diagnosed that the patient<br />
was suffering from generalized<br />
moderate periodontitis with<br />
trauma from occlusion. The<br />
treatment plan was made keeping<br />
in mind the end-result,<br />
harmonious with biological<br />
and functional aspects. The<br />
treatment plan involved:<br />
- Periodontal therapy involving<br />
subgingival curettage.<br />
- Extraction of hopeless teeth.<br />
- Crowns and bridges on<br />
remaining teeth, along with<br />
implant-supported prosthesis<br />
for missing teeth. Rehabilitation<br />
of occlusion is the<br />
crucial phase to ensure longterm<br />
oral health.<br />
- Intentional root canal treatment<br />
was performed for<br />
remaining teeth in order<br />
to alleviate post-periodontal<br />
therapy hypersensitivity.<br />
- Maintenance and recall.<br />
Material options were given<br />
to the patient and a metal<br />
ceramic prosthesis was chosen.<br />
Treatment Sequencing<br />
Treatment was carried out in<br />
the mandibular arch followed<br />
by the maxillary arch in the<br />
following phases:<br />
Phase 1<br />
Subgingival curettage of the<br />
lower arch along with the<br />
extraction of lower right (LR)<br />
1 and 2, and lower left (LL)<br />
1, 2, and 7, followed by placement<br />
of immediate extraction<br />
implants (Xive/Frialit by Friadent,<br />
GmBH) on LR 6(4.5 x 13),<br />
2(3.4 x13) and LL 2(3.4 x 13),<br />
7(5.5 x 8) was done. Prefabricated<br />
provisional acrylic fixed<br />
prostheses were given in the<br />
same sitting resting on the<br />
remaining natural teeth. Occlusal<br />
adjustments were made<br />
to achieve proper function,<br />
comfort, and esthetics.<br />
After a week, subgingival<br />
curettage of the upper arch<br />
along with extraction of upper<br />
right (UR) 1, 2, 4, 5, and 6, and<br />
Upper left (UL) 1, 2, 4, and 6<br />
followed by immediate extraction<br />
implants (Xive/Frialit by<br />
Friadent, GmBH) on UR 2<br />
(3.4 x 11), 4(3.8 x 13), 5(3.8 x 11),<br />
6(4.5 x 9.5); UL 1(3.8 x 11),<br />
2(3.4 x 11), 4(3.8 x 13), 6(4.5<br />
x 8) was done. Prefabricated<br />
provisional acrylic fixed prostheses<br />
were given after bite<br />
adjustment. During the following<br />
visit, intentional root canal<br />
treatment was performed in<br />
LR 3, 4, 5, 7, and LL 3, 4, 5, 6<br />
teeth.<br />
Phase 2<br />
The loading of abutment in the<br />
upper and lower arch implants<br />
was performed six months after<br />
the stage 1 surgery. UL 3 was,<br />
also extracted due to persisting<br />
mobility, hence, poor long-term<br />
prognosis. Intentional root canal<br />
treatment was performed in UR<br />
3, 7 and UL 5, 7 to improve<br />
their prognosis and prepared<br />
to receive crowns.<br />
After a week, final impressions<br />
were made using rubber<br />
base impression material, and<br />
working casts were prepared<br />
to make abutments. The working<br />
casts were then mounted<br />
on a non-arcon, semi-adjustable<br />
articulator using facebow<br />
records. The centric relation<br />
and vertical dimension were<br />
also transferred to the articulator<br />
from the patient, using<br />
polyvinyl siloxane putty bite.<br />
During metal trial, fit of the<br />
castings and occlusal clearance<br />
were checked. A Bisque trial<br />
was, done to confirm fit, shade<br />
and occlusal parameters.<br />
Later, the final metal ceramic<br />
prosthesis was constructed. The<br />
final prosthesis, after all occlusal<br />
adjustment, was cemented<br />
using Glass Ionomer Cement.<br />
Recall appointments were given<br />
for cleaning and maintenance<br />
of the prostheses at every 6<br />
months.<br />
Restorative and Occlusal<br />
Consideraions<br />
The final occlusion given to<br />
the patient was Class II with<br />
anterior guidance, which<br />
1a 1b 1c 1d<br />
Figs. 1a-d: Pre-operative intra oral view<br />
1e 1f 2a<br />
Fig. 1e: Pre-operative smile Fig. 1f : Pre-operative OPG Fig. 2a: Maxillary occlusal view after final preparation<br />
2b 2c 3a<br />
Fig. 2b: Mandibular occlusal view after final preparation Fig. 2c: Post-loading OPG Fig. 3a:Post-operative intraoral view<br />
3b 3c 3d 3e<br />
Figs. 3b-d: Post-operative intraoral view<br />
Fig. 3e: Post-operative smile
20<br />
Clinical DeNtal tribuNe | april-June, 2010<br />
3f<br />
Discussion<br />
Dental problems are often<br />
multi-factorial, and may not be<br />
satisfactorily resolved by the<br />
restorative treatment alone. 5<br />
Fig. 3f: Post-operative OPG<br />
Fig. 4: Anterior excursive view<br />
allowed direct axial forces and<br />
had minimized off axial forces<br />
on the implant. Disclusion in<br />
excursive movements was given<br />
attention. Since, upper left canine<br />
was missing and was replaced<br />
with an implant supported<br />
bridge, a group functions was<br />
advisable, 4 whereas on the right<br />
side, canine-guided occlusion<br />
was given, since natural canines<br />
were present.<br />
FDI Annual World Dental Congress<br />
2-5 September 2010<br />
Salvador da Bahia, Brazil<br />
Creating the perfect smile<br />
along with health is a challenging<br />
procedure that requires<br />
a multidisciplinary approach,<br />
and meticulous treatment planning.<br />
Emphasis was given on<br />
occlusal adjustments in both<br />
temporary and final restoration,<br />
since occlusal rehabilitation<br />
is the key to long-term<br />
success of the restorations<br />
and the oral health.<br />
References<br />
1. Spear F, Kokich V, Mathews D.<br />
Interdisciplinary management<br />
of anterior dental esthetics.<br />
JADA 2006, Vol.137; 160-170.<br />
2. F. Dennis. Complete artificial<br />
dentition supported by endosseous<br />
implants: a case report<br />
of total in-office treatment.<br />
JOI 91-97.<br />
3. R Patil. Textbook of Esthetic<br />
Dentistry: An Artists Science.<br />
4. I Ahmad. Anterior dental esthetics:<br />
A gingival perspective.<br />
British Dental Journal 2005;<br />
199: 195–202. doi: 10.1038/<br />
sj. bdj.4812611.<br />
5. I Ahmad. Geometric considerations<br />
in anterior dental<br />
esthetics: Restorative principles.<br />
PPAD 1998; 10(7):<br />
813-22. DT<br />
About the authors<br />
Dr Ratnadeep Patil has maintained<br />
a successful private practice<br />
specializing in aesthetic and<br />
implant dentistry in Mumbai,<br />
since 1988. He is a diplomate of<br />
the International College of Oral<br />
Implantologists and is an active<br />
member of International Association<br />
of Dental Research. He has<br />
authored a clinical textbook<br />
on aesthetic dentistry (Esthetic<br />
Dentistry: An Artist’s Science)<br />
and been actively involved in<br />
conducting continuing dental<br />
education programmes.<br />
Dr Kripa Shetty has graduated<br />
from A B Shetty Dental College.<br />
She is an associate dental surgeon<br />
at Smile Care®, with special focus<br />
on restorative & esthetic dentistry.<br />
She is an active member in<br />
research and publication division<br />
of Smile Care®.<br />
congress@fdiworldental.org<br />
www.fdiworldental.org<br />
Dr Kavita Mahesh has been in<br />
clinical practice since she graduated<br />
from the Government Dental<br />
College and Hospital, Mumbai<br />
in 2002. She completed her postgraduate<br />
certificate in implant<br />
dentistry at New York. She is actively<br />
involved in clinical research<br />
and continuing dental education<br />
programs with the Smile Care®<br />
team.
FDI explores preventive dentistry at 2010 AEEDC Dubai<br />
FDI World Dental Federation introduces the Global Caries Initiative to the Gulf Region as part of a global consultation process<br />
Representatives from FDI World<br />
Dental Federation, including Dr<br />
Roberto Vianna, FDI President,<br />
were recently in Dubai for the<br />
2010 UAE International Dental<br />
Conference and Arab Dental<br />
Exhibition (AEEDC Dubai),<br />
where they participated in the<br />
AEEDC Conference Program,<br />
the Gulf Cooperation Council<br />
Preventive Dentistry Conference<br />
and the 7 th Annual Arab<br />
Asian Scientific Dental Alliance,<br />
introducing the FDI Global<br />
FDI World Dental Federation<br />
is participating in an official<br />
review of the WHO Patient Safety<br />
Curriculum Guide, together<br />
with the Organization for Safety<br />
and Asepsis Procedures (OSAP),<br />
International Federation of<br />
Dental Educators and Associations<br />
(IFDEA), and other leading<br />
global medical profession<br />
associations.<br />
Patient safety is an emerging<br />
discipline, aiming to reduce<br />
harm to patient caused by health<br />
care and to identify opportunities<br />
for improving patient out comes.<br />
According to the WHO Research<br />
Priority Setting Working Group<br />
on Patient Safety, tens of millions<br />
of patients worldwide suffer<br />
disabling injuries or death due to<br />
Caries Initiative to key opinion<br />
leaders of the Gulf Region.<br />
The Global Caries Initiative<br />
(GCI) was first conceived during<br />
the Rio Caries Conference in July<br />
2009, where conference attendees—including<br />
leading experts<br />
in epidemiology, cariology, dental<br />
education, prevention and<br />
change management conceded<br />
there is a need to establish a<br />
broad alliance of key influencers<br />
and decision-makers to effect<br />
fundamental change across<br />
health systems and in individual<br />
behaviour in order to eradicate<br />
caries worldwide by 2020.<br />
Departing from this objective,<br />
FDI World Dental Federation<br />
embarked upon a global<br />
consultation process to assess<br />
the potential challenges and impact<br />
of introducing a preventive<br />
model to existing systems for<br />
caries management. The most<br />
recent seminar took place at<br />
unsafe medical care every year.<br />
the 2010 AEEDC Conference<br />
Program: Dr Julian Fisher, FDI<br />
Asso ciate Director of Education<br />
and Scientific Affairs, described<br />
the context of GCI in a presentation<br />
entitled, “The Global Caries<br />
Initiative: A Profession-Led Callto-Action”<br />
and Dr Nigel Pitts, of<br />
the University of Dundee (Scotland),<br />
presented his research<br />
related to “A New Approach to<br />
Caries Classification, Detection<br />
and Assessment: The Experiences<br />
of ICDAS”, which addresses<br />
an underlying theme identified<br />
early in the GCI consultation<br />
process; that is, the need for<br />
the profession to establish a<br />
common language for caries.<br />
Dr Pitts has been working with<br />
FDI World Dental Federation to<br />
explore an international caries<br />
classification system within the<br />
context of GCI.<br />
Dr Roberto Vianna reinforced<br />
the FDI World Dental Federation<br />
commitment to oral health in<br />
FDI teams up with OSAP to improve<br />
global patient safety standards<br />
The multi-professional WHO<br />
Patient Safety Curriculum Guide<br />
was first published in 2009 to<br />
provide medical schools with<br />
guidelines for teaching patient<br />
safety, and has since been downloaded<br />
by more than 1000 institutions<br />
in 100 countries. In growing<br />
recognition of the harms<br />
caused by health care, the WHO<br />
initiated a review of the Guide<br />
and invited FDI World Dental<br />
Federation to participate as a<br />
primary partner in the project,<br />
together with the International<br />
Council of Midwives and other<br />
members of the World Health<br />
Professions Alliance (WHPA);<br />
International Council of Nurses,<br />
International Pharmaceutical<br />
Federation and World Medical<br />
Association. Professors Takashi<br />
Inoue and Nermin Yamalik, of<br />
the FDI Education Committee,<br />
will be contributing to the review.<br />
Details are expected to be<br />
finalised during a consensus<br />
meeting at the 2010 OSAP Annual<br />
Symposium in June. FDI<br />
an address to attendees of the<br />
Gulf Cooperation Council Preventive<br />
Dentistry Conference,<br />
paying a special thank you to<br />
Professor Abdullah Al Shammery,<br />
Dean of Riyadh Colleges<br />
of Dentistry and Pharmacy and<br />
AEEDC International Scientific<br />
Advisory Board Member. Dr Vianna<br />
said, that FDI World Dental<br />
Federation “is delighted to<br />
participate in this Conference<br />
and looks forward to working<br />
together with the Gulf Cooperation<br />
Council and FDI member<br />
The annual FDI Corporate Partners<br />
meeting took place at the<br />
end of February during the 145 th<br />
Chicago Dental Society Mid-<br />
Winter Meeting. FDI President<br />
Dr Roberto Vianna opened the<br />
meeting, welcoming & thanking<br />
FDI Corporate Partners for their<br />
un wavering support, particularly<br />
in view of the economic challenges<br />
still affecting businesses<br />
worldwide. Joining the FDI President<br />
at the meeting were FDI<br />
President-Elect, Dr Orlando Monteiro<br />
da Silva; Councillor, Dr<br />
Kathryn Kell; Executive Director,<br />
Dr David Alexander; and other<br />
full-time FDI professional staff<br />
from the Finance, Communications<br />
and Congress departments.<br />
Dr David Alexander presented<br />
a detailed report of ongoing<br />
FDI activities & achievements in<br />
2009, including the introduction of<br />
a new FDI website, preparations<br />
for the 2010 Annual World Dental<br />
Congress in Salvador da Bahia,<br />
Brazil, future congress venues,<br />
progress on the Global Caries Initiative<br />
and a summary of internal<br />
process improvements across the<br />
organisation. Dr Alexander reminded<br />
participants of the critical<br />
associations to further prevention<br />
at the national level.” FDI<br />
Dr Julian Fisher, FDI Education and<br />
Scientific Affairs Manager<br />
FDI Corporate Partners<br />
meeting in Chicago<br />
importance of partnership between<br />
FDI World Dental Federation<br />
and the dental industry, encouraging<br />
an “open dialogue, which<br />
strengthens our relationship and<br />
brings mutual benefits to both<br />
parties.” The presentations portion<br />
of the meeting included a<br />
financial review by Jerome Estignard,<br />
FDI Director of Finance &<br />
Operations, who summarised the<br />
2009 year-end results and budget<br />
forecasts for 2010 and beyond.<br />
The annual FDI Corporate<br />
Partners meeting is held in the<br />
first quarter of each year, alternating<br />
venues between the Chicago<br />
Dental Society Mid-winter Meeting<br />
and the International Dental<br />
Show in Cologne, Germany. FDI<br />
About the publisher<br />
Publisher<br />
FDI World Dental Federation<br />
Tour de Cointrin, Avenue Louis Casai 84,<br />
Case Postale 3<br />
1216 Cointrin – Genève, Switzerland<br />
Phone: +41 22 560 81 50<br />
Fax: +41 22 560 81 40<br />
E-mail: media@fdiworldental.org<br />
Web site: www.fdiworldental.org<br />
FDI Communications Manager<br />
Aimée DuBrûle<br />
FDI Worldental Communiqué is published by<br />
the FDI World Dental Federation. The newsletter<br />
and all articles and illustrations therein are<br />
protected by copyright. Any utilisation with out<br />
prior consent from the editor or publisher is<br />
inadmissible and liable to prosecution.
THE<br />
Mumbai, December-2009, V<br />
22<br />
technology DeNtal tribuNe | april-June, 2010<br />
Complete maxillary implant prosthodontic rehabilitation<br />
with a CAD/CAM-fixed prosthesis<br />
By Neo Tee-Khin, Ansgar C. Cheng, Helena Lee and Ben Lim, Specialist Dental Group, Singapore<br />
Endosseous implant treatment<br />
has been widely reported as a<br />
highly predictable treatment<br />
modality with a low percentage<br />
of clinical complications. Prudent<br />
clinical judgement and<br />
careful consideration of the<br />
risks and benefits of various<br />
treatment options are essential<br />
for the treatment planning and<br />
long-term success of prosthodontic<br />
treatment. 1<br />
Traditional implant prostheses<br />
are commonly fabricated<br />
using acrylic resin teeth supported<br />
by a metal framework.<br />
Significant space is designed at<br />
the tissue surface of the prosthesis<br />
to enhance oral hygiene<br />
maintenance.<br />
However, application of this<br />
prosthetic design in the maxillary<br />
arch is occa-sionally esthe-<br />
World Dental Show<br />
29 - 31 October 2010, Mumbai<br />
More than 30000 dental professionals<br />
expected in 2010<br />
tically inadequate and speech<br />
may be compromised.<br />
Conventional porcelain-fused-to-metal<br />
restorations require<br />
the placement of labial restoration<br />
margins below the free<br />
gingival margin in order to mask<br />
the hue and value transition between<br />
the sub-gingival implant<br />
sub-structures and the supragingival<br />
crown restorations.<br />
From a periodontal point of<br />
view, sub-gingival placement of<br />
restoration margins is related<br />
to adverse periodontal tissue<br />
response. 2–5 As a result, restoration<br />
margins are best placed<br />
coronally from the free gingival<br />
margin. 4,5<br />
More than 500 Booths<br />
<strong>Media</strong> Partners<br />
Be in the Forefront<br />
of Dental<br />
Exhibition<br />
in India<br />
10 Highly specialized courses<br />
Largest Exhibition in Asia in 2009<br />
<br />
Scientific Conference ence in association with<br />
University of California, San Francisco<br />
World<br />
Dental<br />
Show<br />
Mumbai<br />
Approved By<br />
Indian<br />
Trade Promotion Organisation<br />
Ministry of Health & Family Welfare<br />
Ministry of Home Affairs<br />
fairs<br />
Ministry of External Affairs<br />
fairs<br />
Approved By<br />
Porcelain-fused-to-metal restorations<br />
are commonly used<br />
in the posterior teeth because<br />
of their well-documented longterm<br />
clinical track record. 6–13<br />
CAD/CAM ceramic-based materials<br />
are prescribed nowadays,<br />
owing to their demonstrated<br />
promising physical properties<br />
14,15<br />
and clinical longevity. 16<br />
This article describes the<br />
clinical application of highstrength<br />
zirconium oxide restorations<br />
in the prosthodontic<br />
management of an edentulous<br />
maxilla with a failing implant<br />
prosthesis.<br />
Clinical report<br />
A 62-year-old female with an<br />
implant-supported maxillary<br />
prosthesis was evaluated at the<br />
Specialist Dental Group in Singapore.<br />
She presented clinically<br />
with a maxillary fixed complete<br />
denture supported by six endosseous<br />
implants (Nobel Replace,<br />
Tapered Groovy, Nobel Biocare).<br />
The National Voice of the Dental Profession<br />
Affiliate Members<br />
World Dental Federation<br />
<br />
Commonwealth Dental association International<br />
Association Society for Research on<br />
of Dental Research<br />
Nicotine & Tobacco<br />
Organiser<br />
Indian Dental<br />
Association<br />
Terrace, 2 nd<br />
Bombay Mutual<br />
Floor,<br />
534 Sandhurst Bridge, Opera House,<br />
Mumbai - 400 007<br />
Tel : +91 (22) 43434545, 23671515,<br />
+91 (22) 23696655<br />
Fax: (22) 23685613<br />
Email : info@wds.org.in<br />
Website :<br />
www.ida.org.in<br />
www.wds.org.in<br />
Venue - MMRDA, Opp. Citi Bank, Bandra - Kurla Complex Bandra ( E ) Mumbai 400051, Maharashtra<br />
The prosthesis had acrylic<br />
resin teeth supported by a gold<br />
alloy metal framework. The<br />
implant at the patient’s maxillary<br />
right canine area was exposed.<br />
The patient reported no symptoms<br />
(Fig. 1). An occlusal examination<br />
revealed a stable maximal<br />
intercuspation position<br />
with insignificant centric relation<br />
to maximal inter-cuspation<br />
slide at the teeth level. A canineguided<br />
occlusal scheme was<br />
noted. No parafunc-tional habits
DeNtal tribuNe | april-June, 2010 technology 23<br />
Fig. 1: Pre-treatment intra-oral frontal view: A large space was<br />
noted between the intaglio surface of the prosthesis and the<br />
maxillary tissue, and there was significant tissue resorption on<br />
the labial surface of the implant over the maxillary right canine<br />
area. The patient was asymptomatic.<br />
Fig. 2: Full-thickness flap revealed the advanced bone loss on the<br />
labial surface of the implant. In spite of the tissue damage, this<br />
implant was clinically firm.<br />
Fig. 3: Maxillary prosthesis before the application of tooth-colored<br />
porcelain; excessive crown length was noted at this stage.<br />
Fig. 4: Completed maxillary prosthesis with gingival-colored<br />
porcelain applied to provide adequate<br />
lip support; excessive crown height was reduced.<br />
Fig. 5: Anterior view showing the CAD/CAM--<br />
fabricated full-ceramic implant abutments at the<br />
approximated vertical dimension of occlusion.<br />
Fig. 6: Occlusal view of the maxillary arch before insertion<br />
of the maxillary prosthesis; favorable anterior-posterior<br />
spread allowed the replacement of<br />
posterior teeth with distal cantilevering.<br />
Fig. 7: Completed maxillary implant-supported<br />
prosthesis; note the placement of the supra-gingival<br />
margins.<br />
were reported. Sub-optimal<br />
maxillary lip support was noted.<br />
A significant amount of dead<br />
space was identified between<br />
the intaglio surface of the prosthesis<br />
& the maxillary soft tissue.<br />
Upon removal of the maxillary<br />
prosthesis, all the maxillary<br />
implants were found to be osseoin-tegrated.<br />
The patient desired<br />
to correct the failing implant,<br />
restore lip support, masticatory<br />
function and facial esthetics.<br />
The overall treatment planincluded<br />
removal of the implant<br />
at the maxillary right canine<br />
area, replacement of a new<br />
implant at the maxillary right<br />
canine region and fabrication<br />
of a full-arch, zirconium oxidebased<br />
ceramic restoration in<br />
the maxilla.<br />
Under local anaesthesia, the<br />
implant at the maxillary right<br />
canine area was removed surgically<br />
(Fig. 2) and a new 13 mm<br />
long regular platform implant<br />
was placed (NobelReplace, Tapered<br />
Groovy). The new implant<br />
was submerged and primary<br />
wound closure achieved. The<br />
existing prosthesis was reinserted<br />
during the healing period to<br />
serve as a provisional prosthesis.<br />
Once osseointegration was<br />
achieved a few months later, the<br />
new implant was exposed and<br />
the maxilla was ready for prosthodontic<br />
rehabilitation after a<br />
few weeks of soft-tissue healing.<br />
Six implant-level impression<br />
copings (NobelReplace) were<br />
placed onto the maxillary implants.<br />
High-viscosity vinyl polysiloxane<br />
material (Aquasil Ultra<br />
Heavy, DENTSPLY DeTrey) was<br />
carefully injected around all<br />
the impression copings. A stock<br />
tray loaded with putty material<br />
(Aquasil Putty, DENTSPLY De<br />
Trey) was seated over the<br />
entire maxillary arch to make<br />
the definitive impression.<br />
A jaw-relation record at the<br />
treatment vertical dimension<br />
was made with a vinyl polysiloxane<br />
material (Regisil PB,<br />
DENTSPLY DeTrey).<br />
The maxillary and mandibular<br />
definitive casts were<br />
mounted arbitrarily in the<br />
center of a semi-adjustable<br />
articulator (Hanau Wide-vue,<br />
Teledyne Waterpik) using average<br />
settings. 17,18<br />
The custom zirconium oxide<br />
abutments with gold-alloy fitting<br />
surface (Procera, Nobel Biocare)<br />
were CAD/CAM fabricated<br />
according to the prosthesis<br />
design.<br />
The development of the<br />
planned definitive maxillary<br />
restoration was carried out<br />
using a CAD/CAM process. The<br />
maxillary definitive cast with the<br />
custom full-ceramic abutments<br />
were scanned (Zeno Scan, Wieland<br />
Dental+Technik), and the<br />
prosthesis framework was designed<br />
using a software program<br />
(D700, 3Shape).<br />
The framework was milled in<br />
zirconium-base-material (Zeno<br />
Zr Bridge, Wieland Dental +<br />
Technik) with a milling machine<br />
(Zeno 4030 M1, Wieland Dental+<br />
Technik). The prosthesis framework<br />
was sintered according<br />
to the manufacturer’s recommendations.<br />
Subsequently, overlaying low<br />
-fusing, tooth-colored porcelain<br />
material (IPS e.max, Ivoclar<br />
Vivadent) was manually applied<br />
onto the exterior to create proper<br />
anatomic form (Fig. 3).<br />
Low-fusing, gingival-colored<br />
porcelain material (IPS e.max)<br />
was applied to create proper<br />
lip support (Fig. 4).<br />
During the delivery clinical<br />
session, the old prosthesis was<br />
removed and the new custom<br />
abutments were torqued to 32<br />
Ncm (Fig. 5).<br />
The new prosthesis was tried<br />
in to verify color, occlusion, lip<br />
support, teeth form and comfort.<br />
Upon confirmation of the<br />
patient’s acceptance, the implant<br />
abutments were sealed in guttapercha<br />
(Fig. 6) and the prosthesis<br />
was cemented in resinmodified<br />
glass-ionomer luting<br />
agent (RelyX Unicem, 3M ESPE).<br />
The patient was evaluated 2<br />
weeks postoperatively. Anterior<br />
guided occlusal schemes were<br />
verified intra-orally before andafter<br />
prosthesis cementation<br />
(Fig. 7). The patient reported<br />
no discomfort and she had<br />
been functioning well with the<br />
new resto-rations. No abnormal<br />
clinical signs were noted.<br />
Discussion<br />
Osseointegration is a welldocumented<br />
and predictable<br />
clinical treatment option. On<br />
the other hand, management<br />
of implant-failure is also a<br />
clinical reality.<br />
In this clinical report, the<br />
failure of one implant at a<br />
crucial location indicated the<br />
need for re-fabrication of the<br />
entire implant prosthesis.<br />
As the patient desired a high<br />
level of esthetics, full-ceramic<br />
restorations were selected. By<br />
prescribing tooth-colored ceramic<br />
abutments & full-ceramic<br />
restorations, prosthesis margins<br />
were made at the gingival level<br />
and gingival retraction procedures<br />
were eliminated during<br />
impression and prosthesis<br />
insertion.<br />
Full-arch prosthodontic rehabilitation<br />
using fixed prostheses<br />
usually requires longerterm<br />
provisional restoration in<br />
order to facilitate a predictable<br />
treatment outcome.<br />
In this patient, the existing<br />
maxillary prosthesis served as<br />
a long-term provisional restoration<br />
for verifying her adaptability,<br />
& multiple professional<br />
clinical adjustments of provisional<br />
restorations were not<br />
required.<br />
This treatment sequence<br />
increased the margin of safety<br />
in the execution of the definitive<br />
full-ceramic restoration.<br />
Intra-oral verification of the<br />
new treatment occlusal scheme<br />
and detailed in situ clinical<br />
adjustment of the restorations<br />
on the day of prostheses insertion<br />
still formed the essential<br />
foundation for proper treatment<br />
execution.<br />
In any major prosthodontic<br />
treatment, the patient should<br />
be informed of the potential<br />
financial and time implications<br />
should the need for refabrication<br />
of the restorations arise.<br />
Conclusion<br />
The functional management of<br />
an edentulous maxilla using a<br />
full-ceramic implant-supported<br />
maxillary prosthesis has beenreported.<br />
New CAD/CAM-based<br />
restorative materials were used<br />
in treating this case.<br />
The use of high-strength<br />
full-ceramic restorations enhances<br />
overall esthetic predictability<br />
and long-term functional<br />
outcome.<br />
A complete list of references<br />
is available from the publisher. DT<br />
About the author<br />
Dr. Ansgar C. Cheng is a prosthodontist<br />
with Specialist Dental<br />
Group, Mount Elizabeth Hospital,<br />
Singapore, and an adjunct<br />
associate professor at the National<br />
University of Singapore.<br />
Dr. Ansgar C. Cheng<br />
3 Mount Elizabeth #08-10<br />
Singapore 228510<br />
Republic of Singapore<br />
E-mail: drcheng@specialist<br />
dentalgroup.com
24<br />
Case report DeNtal tribuNe | april-June, 2010<br />
Epulis gravidarum mimicking a neoplasm<br />
A case report by Dr Deepak Chopra, Dr Mayur Kaushik, Dr Deepak Kochar, and Dr Sidharath Malik, India<br />
Introduction<br />
aled granulation tissue with<br />
Pregnancy is a delicate condi-<br />
non-neoplastic proliferation of<br />
tion, involving complex physi-<br />
endothelial cells, suggestive of<br />
cal and physiological changes. 1<br />
epulis gravidarum.<br />
Modification of metabolism,<br />
immunology, and high level of<br />
Case Description<br />
hormones make it possible for<br />
A 26-year-old female was refer-<br />
fetus to grow & develop, ending<br />
red with the chief complaint of an<br />
up with labor. Variations of these<br />
extensive gingival enlargement<br />
hormones cause some changes<br />
on the lower right anterior tooth<br />
on skin and oral mucosa. 2<br />
region. The lesion was of negligi-<br />
The changes progress due to<br />
ble size when the patient first<br />
increased level of sex hormones<br />
in blood and saliva. These hor-<br />
noticed it three weeks ago, but<br />
had grown rapidly over the past<br />
Fig. 1: Pre-operative view<br />
Fig. 2: Excised lesion<br />
mones are thought to be the<br />
twenty days to attain the present<br />
reasons for occurrence of infla-<br />
size. The patient’s medical<br />
mmatory process and the epulis<br />
history revealed that she was<br />
gravidarum. 3<br />
at five months of gestation with<br />
no systemic disease.<br />
The progesterone & estrogen<br />
receptors are situated in basal<br />
Clinical examination reve-<br />
and spinous stratum of the ep-<br />
aled an isolated exophytic,<br />
ithelium, and in the connective<br />
pedunclated lesion on the man-<br />
tissue. That is why those cells<br />
dibular right buccal side bet-<br />
are influenced by a high level of<br />
ween the interdental gingival of<br />
pregnancy hormones. 4<br />
Proges-<br />
lateral incisor and canine. It<br />
terone dilates blood vessels,<br />
makes them more permeable,<br />
measured approximately 2.5<br />
cm in diameter with some areas<br />
Fig. 3: Sutured with 6-0 silk sutures<br />
Fig. 4: Post-operative view<br />
and increases proliferation of<br />
capillary vessels. Estrogen regulates<br />
the proliferation, differentiation,<br />
and keratinization of<br />
the gingival tissue. These hormones<br />
increase gingival bleed-<br />
of erythema. The lesion was<br />
rough and firm in consistency<br />
on palpation that bled minimally<br />
(Fig. 1). The swelling also interfered<br />
with eating and speech.<br />
On examination, patient’s oral<br />
in that the lesion is not pus<br />
producing as “pyogenic” implies.<br />
It is however, a tumor of granulation<br />
tissue, as granuloma<br />
implies. 1 It has been called an<br />
epulis, because it is located<br />
sarcoma, kaposi’s sarcoma and<br />
non-hodgkins lymphoma. 10<br />
Conclusion<br />
Epulis gravidarum represents<br />
an important differential diag-<br />
7. Ababneh K, Khateeb T. Aggressive<br />
pregnancy tumor mimicking<br />
a malignant neoplasm:<br />
a case report. J Contemp Dent<br />
Pract. 2009 Nov 1; 10(6): E072-8.<br />
8. Angelopoulos AP. Pyogenic<br />
granuloma of the oral cavity:<br />
ing, cause gingival growth, and<br />
lead to deepening of periodontal<br />
pockets as well. 5<br />
Epulis gravidarum is a quite<br />
rare gingival disorder occurring<br />
hygiene was found good.<br />
Excisional biopsy of the<br />
swelling with a wide margin<br />
was performed (Figs. 2 & 3). The<br />
histopathological examination<br />
more frequently in the gingiva.<br />
Some other terms used are<br />
“granuloma telangiectaticum”<br />
and “pregnancy tumor”. The<br />
term “hemangiomatous granuloma”<br />
was suggested by An-<br />
nosis of oral masses and can<br />
behave in a very aggressive<br />
fashion, mimicking a malignant<br />
tumor. Excised specimens<br />
should be sent for histopathological<br />
reports to exclude malig-<br />
Statistical analysis and its clinical<br />
feature. J Oral Surg. 1971;<br />
29, 84-9.<br />
9. Daley TD, Nartey NO, Wysocki<br />
GP. Pregnancy tumor: an analysis.<br />
Oral Surg Oral Med Oral<br />
Pathol. 1991; 72(2): 196-99.<br />
in 1.8 to 5% of pregnant women,<br />
and it affects more commonly<br />
the anterior region of the upper<br />
jaw. 6 It is a smooth or lobulated<br />
exophytic lesion and manifests<br />
as a pink, red, or purple erythematous<br />
papule with pedunculated<br />
or sessile base. 1 It usually<br />
revealed young granulation<br />
tissue with non-neoplastic proliferation<br />
of endothelial cells<br />
and the enlargement of blood<br />
capillaries. Infiltration of acute<br />
and chronic inflammatory cells<br />
in a collagenous matrix was also<br />
present. Surface of the lesion<br />
gelopoulos to accurately reflect<br />
the characteristic histopathologic<br />
picture (hemangioma-like)<br />
and the inflammatory nature<br />
(granuloma) of the lesion. 8<br />
Clinically it presents as a<br />
lesion that is pedunculated or<br />
nancy. It is acceptable practice<br />
to excise aggressive variants<br />
of this lesion during pregnancy<br />
to avoid distressing side effects.<br />
References<br />
1. Jafarzadeh H, Sanatkhani M,<br />
Mohtasham N. Oral pyogenic<br />
granuloma: a review. J Oral<br />
10. Czerninski R et al. Comparison<br />
of clinical and histological diagnosis<br />
in lesions of oral mucosa.<br />
Oral Surg Oral Med Oral Pathol<br />
Oral Radiol Endond. 2007; 103<br />
(4): e20. DT<br />
arises in the 2 nd trimester, grows<br />
gradually over a few months<br />
time, and it also tends to bleed.<br />
After delivery of the child, it may<br />
regress and disappear entirely. 7<br />
The purpose of this article is<br />
to describe a gingival swelling<br />
in a five months pregnant 26-<br />
year-old woman, which grew<br />
very rapidly unlike for this kind<br />
of tumor mimicking a malignant<br />
neoplasm.<br />
The lesion was not painful<br />
and grew very rapidly over a<br />
three week period. The histopathological<br />
examination reve-<br />
showed hyperplastic parakeratinised<br />
stratified squamous epithelium<br />
with areas of atrophy<br />
and ulcer. These findings were<br />
consistent with a histopathological<br />
diagnosis of epulis<br />
gravidarum.<br />
After three weeks of postoperative<br />
followup, clinical<br />
appearance of normal gingiva<br />
was present at the site of the<br />
lesion (Fig. 4).<br />
Discussion<br />
Epulis gravidarum is also known<br />
as “Pyogenic granuloma”. The<br />
term is somewhat a misnomer<br />
broad based, highly vascularized,<br />
smooth, edematous, hemorrhagic,<br />
soft, red with glossy<br />
surface and hardened when it<br />
had been longstanding. It could<br />
be a single or multiple well<br />
localized outgrowth, painless<br />
or with dull pain. It usually<br />
is not bigger than 2 cm in the<br />
diameter. 9<br />
Differential diagnosis includes<br />
peripheral giant cell granuloma,<br />
epulis, peripheral ossifying<br />
fibroma, metastatic cancer,<br />
hemangioma, conventional granulation<br />
tissue, hyperplastic<br />
gingival inflammation, angio-<br />
Sci. 2006; 48: 167-75.<br />
2. Erickson CV, Matus NR. Skin<br />
disorders of pregnancy. Am<br />
Fam Physic. 1994; 3: 602-10.<br />
3. Laine MA. Effect of pregnancy<br />
on periodontal and dental<br />
health. Acta Odontol Scand.<br />
2002; 60: 257-64.<br />
4. Zeeman GG, Veth O, Dennison<br />
D. Focus on primary care on<br />
periodontal disease. Implications<br />
on women’s care. Obst<br />
Gynecol Survey. 2001; 56: 43-9.<br />
5. Henry F, et al. Blood vessel<br />
changes during pregnancy: a<br />
review. Am J Clin Dermatol.<br />
2006; 7: 65-9.<br />
6. Paradowska A, Slawecki K,<br />
Chojak EG. Pregnancy tumor:<br />
review of literature. Dent Med<br />
Probl. 2008; 45(1): 51-4.<br />
About the authors<br />
Dr Deepak Chopra is a reader in<br />
the department of periodontology<br />
at Inderprastha Dental College<br />
at Ghaziabad, India. He can be<br />
contacted at deepakchopra2010<br />
@gmail.com.<br />
Dr Mayur Kaushik is a reader in<br />
the department of periodontology<br />
at Subharati Dental College at<br />
Meerut, India.<br />
Dr Deepak Kochar is an assistant<br />
professor in the department of<br />
periodontology at Inderprastha<br />
Dental College at Ghaziabad,<br />
India.<br />
Dr Sidharath Malik is an assistant<br />
professor in the department of<br />
periodontology at Inderprastha<br />
Dental College at Ghaziabad,<br />
India.
DeNtal tribuNe | april-June, 2010 trends & applications 25<br />
Miniscrews—a focal point in practice<br />
Six-part series by Dr Björn Ludwig, Dr Bettina Glasl, Dr Thomas Lietz, & Prof. Jörg A. Lisson—Part IV<br />
Figs. 1a–c: Figs. 1a–d: The uprighting of a second molar with simultaneous reshaping of the dental arch. The problem is clearly visible in the X-ray. The uprighting spring is fixed to a miniscrew (a, b). Status<br />
after five months without reactivation of the arch section (c, d).<br />
Clinical examples (2)<br />
Repositioning individual teeth<br />
The uprighting of molars<br />
The straightening of mesially<br />
tipped (2 nd ) molars in a full dentition<br />
represents a therapeutic<br />
challenge. The treatment is further<br />
complicated if the tooth is<br />
not only tipped but also partly<br />
impacted. The presence of a nonerupted<br />
third molar does not<br />
simplify the process (Fig. 1a).<br />
When planning the required<br />
appliance, it is important to consider<br />
whether it is necessary,<br />
for example, to reshape the<br />
entire dental arch (Figs. 1a–d)<br />
or just upright the tipped tooth.<br />
If miniscrews with bracket<br />
heads are used, it is possible to<br />
employ a special NiTi uprighting<br />
spring (such as the Memory<br />
Titanol spring, FORESTADENT).<br />
A standard multi-bracket appliance<br />
can be used to reshape<br />
the dental arch. At the same time,<br />
a second force element can be<br />
applied with the aid of a miniscrew<br />
and an uprighting spring<br />
(Figs. 1b–d). This avoids the loss<br />
of anchorage that inevitably<br />
occurs when only an uprighting<br />
spring is fixed to the multibracket<br />
appliance (Fig. 2). The<br />
straightening of an individual<br />
tooth may become necessary<br />
for periodontological, prosthetic<br />
or orthodontic reasons. This is a<br />
very simple procedure if a miniscrew<br />
and uprighting spring<br />
are used, and the appliance remains<br />
invisible to the observer.<br />
The tooth need only be fitted<br />
with an appropriate attachment<br />
system that makes it possible to<br />
fix this to the uprighting spring.<br />
Depending on how the spring is<br />
Figs. 3a–c: The alignment of a displaced canine using a miniscrew. After the canines have been exposed, they are attached to a bracket by means of a miniscrew<br />
(a). After removal of the screw, the dental arch can be reshaped using a conventional technique (b, c).<br />
Fig. 2: The uprighting spring fixed to the main arch not only affects the molars, but<br />
also causes displacement of the premolars (loss of anchorage). (Photo: Prof.<br />
Dominguez, São Paulo, Brasil).<br />
nents tend to move towards each<br />
other. In the worst-case scenario,<br />
only the group providing<br />
anchorage is displaced from its<br />
original position. This can occur<br />
if there is ankylosis of the retinated<br />
tooth, something that is<br />
difficult to evaluate during initial<br />
examination. If an attempt is<br />
made to move an ankylosed<br />
canine towards insufficient dental<br />
anchorage, the result will be<br />
Figs. 4a–e: Obtaining additional transverse space by means of ‘hybrid RPE’. The initial diagnosis is an asymmetrical narrow jaw with insufficient space for tooth 13 (a). After fixture of the brackets,<br />
two mini screws (OrthoEasy) were inserted during the same session (b). The hybrid RPE appliance was attached to the miniscrews and molar bands using laboratory abutments (FORESTADENT; c). The<br />
diastema shows the effect of the appliance after ten days’ use (d). Status after transverse expansion and concurrent reshaping of the dental arch (e).<br />
Fig. 5: The hybrid RPE appliance with adjuvant anterior hooks for the attachment<br />
of a Delaire mask.<br />
set, it is even possible to achieve<br />
intrusion/extrusion of the tooth.<br />
This form of treatment is in expensive<br />
for the patient and the<br />
orthodontist will find it highly<br />
effective.<br />
Alignment of retinated<br />
teeth<br />
The alignment of retained or<br />
displaced teeth, particularly in<br />
the case of canines, is one of<br />
the most common forms of surgical<br />
intervention in the field of<br />
orthodontic techniques. Numerous<br />
appliances are available—<br />
rubber bands, springs, orthodontic<br />
chains—that are effective<br />
to a greater or lesser extent.<br />
All these mechanisms have<br />
the same underlying problem:<br />
the neighbouring teeth must be<br />
used—directly or indirectly—to<br />
provide an anchorage, so that<br />
the required traction forces can<br />
be applied. Ideally, the neighbouring<br />
teeth will offer the<br />
greater resistance so that only<br />
the retained tooth moves. Realistically,<br />
however, both compo-<br />
the worst-case scenario. This<br />
can lead to an open bite in the<br />
region of the anterior teeth and<br />
premolars. Miniscrews provide<br />
the definitive form of anchorage<br />
for the alignment of displaced<br />
teeth (Figs. 3a–c). If sufficient<br />
space is available, brackets will<br />
not be needed in the initial phase<br />
of treatment.<br />
Skeletal adjustments<br />
Palatine suture expansion<br />
Rapid palatal expansion (RPE) is<br />
one of the most effective and
26<br />
trends & applications DeNtal tribuNe | april-June, 2010<br />
Figs. 6a–d: Bilateral cross-bite in a seven-year-old boy (a). X-ray of the hybrid RPE appliance in situ (b). Status after ten days’ use: cross-bite has disappeared and vertical bite has remained stable (c, d).<br />
Figs. 7a–d: Anchorage of the canine using a miniscrew avoids protrusion of the anterior teeth when using a fixed Class II correction appliance (here: Williams appliance, FORESTADENT).<br />
Figs. 8a & b: The miniscrew stabilises the position of the molars to which the Kinzinger FMA is attached. This counteracts any protrusion of the premolars and<br />
an terior teeth (a). Class I dental status on completion of treatment (b).<br />
stable methods of acquiring<br />
more transverse space in the<br />
upper jaw. The targeted screw<br />
rate should be in the range of<br />
Fig. 9: The use of miniscrews to attach intermaxillary rubber traction bands<br />
means that no other attachments to the teeth are necessary.<br />
0.2 to 0.6 mm/day. As a rule,<br />
the appliance is fixed by means<br />
of bands to the molars & premolars.<br />
The desired transverse<br />
width can generally be achieved<br />
within 10 to 20 days. There<br />
after, a three-month stabilisation<br />
phase should be observed, in<br />
order to allow ossification of<br />
the ruptured pa latine suture.<br />
The standard anchorage technique<br />
with den tal support<br />
only has several disadvantages.<br />
The most significant is the risk<br />
of tipping the anchor teeth.<br />
Many appliances have been<br />
described that distribute the<br />
force over more than one tooth.<br />
A further problem is apparent<br />
here: as it is necessary to leave<br />
the appliance in place for a<br />
longer period after the active<br />
phase, it is only possible to<br />
commence further corrective<br />
treatment for teeth in the anterior<br />
region. It is possible to<br />
overcome these problems by<br />
using the ‘hybrid RPE’ (Figs.<br />
4–6). Bands are employed as<br />
usual in the molar region.<br />
In the anterior region, the RPE<br />
appliance is fixed using two<br />
miniscrews. These should<br />
be placed on a notional transverse<br />
line connecting the canine/<br />
premolar contact points paramedially.<br />
Distraction is achieved<br />
using the same method as in<br />
standard techniques. There are<br />
several advantages to hybrid<br />
RPE. Preparation of the apparatus<br />
is much simpler and<br />
cheaper, whilst the dental arch,<br />
including the premolars, is<br />
accessible for additional tooth<br />
correction measures.<br />
Class II corrections<br />
In the case of patients with<br />
Class II malocclusion who have<br />
completed or are near com -<br />
pleting their growth phase,<br />
simple techniques for the forward<br />
po sitioning of the lower<br />
jaw are usually ineffective.<br />
Following a thorough initial<br />
exami nation and diagnosis,<br />
there are three possible therapeutic<br />
approaches: camouflage,<br />
fixed Cass II correctional appliances<br />
(Herbst splint, Sabbagh<br />
Uni versal Spring, FMA, Jasper<br />
Jumper etc.) or orthognathic<br />
surgery. The patient must be<br />
informed of the advantages<br />
and dis ad vantages of each<br />
approach. All fixed Class II<br />
Figs. 10a–d: Missing tooth 12 is to be replaced by an implant-based crown. The initial phase of treatment involves widening the gap (a). The head of the vertically inserted OrthoEasy screw (b) is used to<br />
anchor a provisional crown (including bracket), which serves to widen the gap further (c).
DeNtal tribuNe | april-June, 2010 trends & applications 27<br />
correctional appliances—irrespective<br />
of whether these use<br />
the Herbst splint or canted<br />
plane principle—have the same<br />
problem and the same undesirable<br />
side effects. There is a<br />
risk of protrusion of the lower<br />
frontal teeth and/or distalisation<br />
of the upper molars. By means<br />
of passive stabilisation with<br />
the aid of two miniscrews<br />
(Figs. 7 and 8), these effects<br />
can be readily avoided.<br />
the dental ridge (Fig. 10b).<br />
There should be at least<br />
1 mm of bone to the mesial<br />
and distal sides of the mini -<br />
screw. The hole for the insertion<br />
of a miniscrew (1.6 mm) should<br />
thus be at least 2.6 mm. A provisional<br />
crown can then be<br />
mount ed onto the head of the<br />
mini screw. If necessary, a<br />
bracket can be fixed to this<br />
crown (Fig. 10c).<br />
Outlook<br />
The clinical use of mini screws<br />
supports a wide range of tasks.<br />
Dental repositioning that was<br />
previously deemed impossible<br />
becomes achievable, whilst<br />
possible repositioning techniques<br />
are improved and supported.<br />
In order to achieve<br />
this, miniscrews alone are not<br />
sufficient; an appropriate range<br />
of equipment is also necessary.<br />
Several suppliers of miniscrews<br />
offer, in addition to<br />
screws and insertion tools, a<br />
number of devices that facilitate<br />
the use of miniscrews. The<br />
fifth part of this series will<br />
focus on the wide range of<br />
useful auxiliaries that are<br />
available.<br />
DT<br />
About the author<br />
Dr. Björn Ludwig<br />
Am Bahnhof 54<br />
56841 Traben-Trarbach,<br />
Germany<br />
Tel.: +49 65 41 81 83 81<br />
Fax: +49 65 41 81 83 94<br />
E-mail: bludwig@<br />
kieferorthopaedie-mosel.de<br />
Editorial Note: The next edition<br />
of Dental Tribune India will<br />
feature part V of this article.<br />
Orthognathic surgery<br />
After surgical intervention<br />
to relocate or reposition the<br />
jaw (for orthodontic or traumatological<br />
reasons), it is important<br />
to maintain a stable correlation<br />
between bone fragments<br />
and the jaw in the postoperative<br />
phase. This promotes healing<br />
and prevents relapse. The<br />
occlusion appliance is fixed<br />
intraorally, using intermaxilliary<br />
elastic or wire ligatures,<br />
depending on the situation.<br />
It is essential to use the appropriate<br />
fixing options, whether<br />
this is a splint (Schuchardt<br />
splint) or a multi-bracket appliance.<br />
Where these are really<br />
only needed in one jaw or jaw<br />
section, the question arises<br />
of whether, in the era of<br />
the miniscrew, it is necessary<br />
to involve the other jaw in<br />
the stabilisation of the surgical<br />
effect. If miniscrews are used<br />
in the opposing jaw (Fig. 9),<br />
the same effect is achieved—<br />
but with considerably less<br />
restriction from the point<br />
of view of the patient.<br />
Pre-prosthetics<br />
It is the aim of pre-prosthetic<br />
orthodontics to position the<br />
teeth optimally for the subsequent<br />
prosthesis. This can<br />
include intrusion, uprighting,<br />
and the opening or closing<br />
of gaps, amongst other techniques.<br />
As this series and many<br />
other publications have already<br />
shown, miniscrews are particularly<br />
useful in this context.<br />
Mini screws can also be used<br />
as anchoring elements for<br />
a provisional prosthesis. Where<br />
teeth are missing (particularly<br />
the second canines, Fig. 10a)<br />
and the growth phase is not<br />
yet completed, the fitting<br />
of an intermediate prosthesis<br />
is problematic. As an alternative,<br />
particularly where additional<br />
anchorage is required,<br />
miniscrews can be used. A<br />
longer screw (8 or 10 mm) can<br />
be inserted in the centre of