January/February 2009 - Ontario College of Pharmacists
January/February 2009 - Ontario College of Pharmacists
January/February 2009 - Ontario College of Pharmacists

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
focus on error prevention<br />
Pediatric dosages<br />
Ian Stewart, R.Ph., B.Sc.Phm<br />
Toronto Community Pharmacist<br />
When checking prescriptions, pharmacists must consider<br />
the appropriateness <strong>of</strong> the dosage being prescribed.<br />
This can only be done if the pharmacist<br />
is aware <strong>of</strong>, or considers the indication for use or purpose <strong>of</strong> the<br />
medication being prescribed. For example, when codeine is<br />
prescribed for the treatment <strong>of</strong> acute pain, the reccommended<br />
adult dosage is 15 to 60 mg orally every four to six hours. 1 However,<br />
when used as a cough suppressant, the recommended<br />
dosage is 5 to 20 mg orally every four to eight hours.2 Yet, the<br />
indication for use or purpose <strong>of</strong> the medication is not usually<br />
included on prescriptions. This missing piece <strong>of</strong> information is<br />
<strong>of</strong>ten a contributing factor to medication errors.<br />
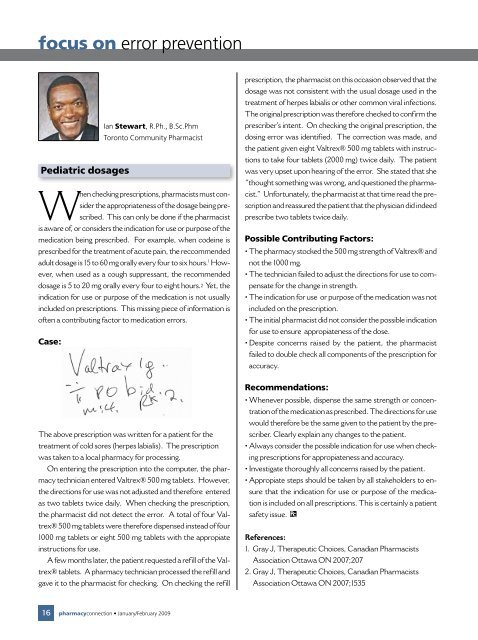
Case:<br />
prescription, the pharmacist on this occasion observed that the<br />
dosage was not consistent with the usual dosage used in the<br />
treatment <strong>of</strong> herpes labialis or other common viral infections.<br />
The original prescription was therefore checked to confirm the<br />
prescriber’s intent. On checking the original prescription, the<br />
dosing error was identified. The correction was made, and<br />
the patient given eight Valtrex® 500 mg tablets with instructions<br />
to take four tablets (2000 mg) twice daily. The patient<br />
was very upset upon hearing <strong>of</strong> the error. She stated that she<br />
“thought something was wrong, and questioned the pharmacist.”<br />
Unfortunately, the pharmacist at that time read the prescription<br />
and reassured the patient that the physician did indeed<br />
prescribe two tablets twice daily.<br />
Possible Contributing Factors:<br />
• The pharmacy stocked the 500 mg strength <strong>of</strong> Valtrex® and<br />
not the 1000 mg.<br />
• The technician failed to adjust the directions for use to compensate<br />
for the change in strength.<br />
• The indication for use or purpose <strong>of</strong> the medication was not<br />
included on the prescription.<br />
• The initial pharmacist did not consider the possible indication<br />
for use to ensure appropiateness <strong>of</strong> the dose.<br />
• Despite concerns raised by the patient, the pharmacist<br />
failed to double check all components <strong>of</strong> the prescription for<br />
accuracy.<br />
The above prescription was written for a patient for the<br />
treatment <strong>of</strong> cold sores (herpes labialis). The prescription<br />
was taken to a local pharmacy for processing.<br />
On entering the prescription into the computer, the pharmacy<br />
technician entered Valtrex® 500 mg tablets. However,<br />
the directions for use was not adjusted and therefore entered<br />
as two tablets twice daily. When checking the prescription,<br />
the pharmacist did not detect the error. A total <strong>of</strong> four Valtrex®<br />
500 mg tablets were therefore dispensed instead <strong>of</strong> four<br />
1000 mg tablets or eight 500 mg tablets with the appropiate<br />
instructions for use.<br />
A few months later, the patient requested a refill <strong>of</strong> the Valtrex®<br />
tablets. A pharmacy technician processed the refill and<br />
gave it to the pharmacist for checking. On checking the refill<br />
Recommendations:<br />
• Whenever possible, dispense the same strength or concentration<br />
<strong>of</strong> the medication as prescribed. The directions for use<br />
would therefore be the same given to the patient by the prescriber.<br />
Clearly explain any changes to the patient.<br />
• Always consider the possible indication for use when checking<br />
prescriptions for appropiateness and accuracy.<br />
• Investigate thoroughly all concerns raised by the patient.<br />
• Appropiate steps should be taken by all stakeholders to ensure<br />
that the indication for use or purpose <strong>of</strong> the medication<br />
is included on all prescriptions. This is certainly a patient<br />
safety issue.<br />
References:<br />
1. Gray J, Therapeutic Choices, Canadian <strong>Pharmacists</strong><br />
Association Ottawa ON 2007;207<br />
2. Gray J, Therapeutic Choices, Canadian <strong>Pharmacists</strong><br />
Association Ottawa ON 2007;1535<br />
16 pharmacyconnection • <strong>January</strong>/<strong>February</strong> <strong>2009</strong>