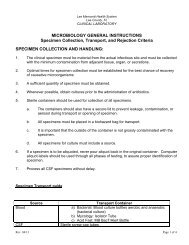
Intracranial Branch Atheromatous Disease (iBAD)
Intracranial Branch Atheromatous Disease (iBAD)
Intracranial Branch Atheromatous Disease (iBAD)

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Intracranial</strong> <strong>Branch</strong><br />
<strong>Atheromatous</strong> <strong>Disease</strong> (<strong>iBAD</strong>)<br />
Ross L Levine MD, FAHA, FAAN<br />
Spring 2012
Case<br />
78 yo man<br />
Onset of slurred speech, increasing<br />
dysphagia, and R-sided weakness<br />
about 7 days PTA<br />
Initially refused to come to the ED<br />
but because of progressive worsening<br />
and an inability to walk was<br />
eventually convinced to be evaluated
PMHx<br />
Prior R capsular stroke<br />
HBP<br />
DM<br />
CAD<br />
Dyslipidemia<br />
Former smoker and heavy drinker
Exam<br />
No bruits<br />
BP, HR okay<br />
Fairly sleepy but when aroused had<br />
severe, mixed dysarthria (spastic-plusscanning)<br />
Bifacial diplegia, brisk jaw jerk<br />
R > L UMN signs
Case<br />
57 yo man awoke with severe<br />
R-sided weakness and dysarthria<br />
Initial BP of 233/126<br />
On exam<br />
R F/UE/LE flaccid weakness<br />
Flaccid dysarthria
PMHx<br />
Untreated HBP<br />
Untreated dyslipidemia<br />
Smoking<br />
Depression
Neurology 1989;39:1246-1250
Pathology of <strong>iBAD</strong><br />
Three proposed disease states<br />
Luminal plaques<br />
Obstructing a branch artery<br />
Functional plaques<br />
Extending into a branch artery<br />
Microatheroma<br />
Forming within the orifice of a branch<br />
artery
In the final narrowing of a branch artery<br />
<br />
<br />
<br />
Micro-dissection<br />
Hemorrhage into a plaque<br />
Platelet and platelet-fibrin plugs<br />
The infarct resulting from occlusion of<br />
the mouth of a branch artery<br />
<br />
<br />
Can extend to the basal surface<br />
Forms an ‘island’ of ischemic tissue within<br />
the parenchyma
Clinical Issues that Suggest the<br />
Likelihood of <strong>iBAD</strong><br />
<strong>Branch</strong> disease is inferred clinically<br />
when<br />
The infarcts are small and deep<br />
Confined to the territory of 1 or a few<br />
penetrating arteries<br />
The infarct abuts the basal surface<br />
The pace and tempo of the ischemia<br />
TIAs or gradual or stepwise progression of<br />
SSx suggests intrinsic ‘thrombotic’ disease<br />
rather than occult embolism
<strong>Branch</strong> disease inferred clinically<br />
when<br />
Vascular diagnostic studies<br />
Show no important large vessel athero<br />
Show no cardiogenic source of embolism<br />
There is no past or present<br />
HBP<br />
Evidence of end-organ effects of HBP<br />
such as retinopathy or LVH
Specific Arteries and Syndromes<br />
Lenticulostriate branches<br />
<br />
<br />
Series of curving vessels that originate from<br />
the mainstem MCA or its upper division<br />
Features favoring branch disease<br />
Not hypertensive<br />
Often diabetic, non-white<br />
Often with infarcts that are larger than the<br />
expected infarct with a single lenticulostriate<br />
occlusion<br />
Do not have MCA disease or proximal embolic<br />
source
Thalamogeniculate branches<br />
Usually there is a ‘fan’ of<br />
thalamogeniculate arteries arising from<br />
the PCA<br />
Features favoring branch disease<br />
Diabetic, dyslipidemic<br />
Normal angiography<br />
Contralateral sensory stroke of F/UE/LE<br />
and ataxia or chorea in the same limbs
Anterior choroidal artery<br />
<br />
<br />
<br />
<br />
<strong>Branch</strong>es directly from the ICA at the siphon<br />
Larger than the previous infarcts<br />
Prevalent in DM, non-whites<br />
Clinical picture<br />
Many w/o SSx<br />
Many w/ isolated hemiparesis, hemianopia, or<br />
combined hemiparetic/hemisensory/hemianopic<br />
SSx contralateral to the infarct<br />
NEG angios, no proximal embolic source
Huebner’s artery<br />
Usually there are 2 and sometimes 4<br />
or more parallel recurrent arteries<br />
arising from the proximal ACA<br />
Supplies anterior basal ganglia and<br />
basal frontal areas<br />
Occlusion of 1 or more<br />
Infarction in the caudate<br />
Sometimes also in capsule, putamen
Huebner’s-cont-<br />
Clinical picture<br />
Dysarthria<br />
Slight or moderate hemi-motor dysfunction<br />
Abulia, agitation, neglect, or dysphasia<br />
Features<br />
MOST are hypertensive and/or diabetic<br />
NO severe ACA occlusive disease
Thalamoperforating artery branches<br />
Polar artery (tuberothalamic)<br />
From PComm<br />
Supplies anteromedial, anterolateral<br />
thalamus<br />
Infarctions result in abulia, minor motor<br />
changes, facial asymmetries, subtle<br />
dysphasia or left visual neglect<br />
OFTEN<br />
<br />
Basilar plaquing and no proximal embolic<br />
source
Thalamic-subthalamic artery<br />
Arises from proximal PCA<br />
Supplies medial thalamus with R and L<br />
arteries or both off a common trunk<br />
Unilateral infarction<br />
Amnestic, upgaze palsy<br />
Bilateral infarction<br />
Decreased LOC, hypersomnolence
Thalamic-subthalamic a.-cont-<br />
OFTEN<br />
Basilar plaquing<br />
No proximal embolic source<br />
IF an embolic source and ‘top of the BA<br />
syndrome’, then the occipital and temporal<br />
lobes are infarcted to some degree as well
Paramedian and short circumferential<br />
basilar artery branches<br />
Pontine paramedian branches<br />
ONLY proven branch disease to date<br />
Pure motor hemiplegia<br />
Or motor deficits w/ ataxia and dysarthria<br />
And occasionally diplopia and paresthesias
Dx of <strong>Branch</strong> <strong>Atheromatous</strong><br />
<strong>Disease</strong><br />
By exclusion of alternative<br />
possibilities<br />
And by recognizing a presentation<br />
that might fit into the syndromes so<br />
described
Doubters Often Argue<br />
Since hypertensive patients are also<br />
predisposed to accelerated athero<br />
and thus branch disease<br />
<strong>Branch</strong> disease and lipohyalinosis cannot<br />
easily be distinguished in HBP-patients<br />
<strong>Branch</strong> disease cannot be easily be<br />
separated from occlusion of branches<br />
by emboli arising in irregular proximal<br />
large artery plaques
Does the Treatment Differ?<br />
Need to Rx HBP, if it is present,<br />
anyway<br />
If proximal and non-stenotic large<br />
vessels are present,<br />
statins/antiplatelet agents<br />
Once we are able to DEFINE branch<br />
atheromatous disease clinically and<br />
CONFIRM the Dx technologically, we<br />
can then decide BETTER therapies
Neurology 2012;78:888-896
Analyzed 201 consecutive pts w acute<br />
MCA infarcts but with no demonstrable<br />
carotid or cardiac embolism source<br />
BOD (n=46)<br />
<br />
Subcortical infarcts w MCA stenosis<br />
Non-BOD (n=52)<br />
<br />
Infarcts beyond the subcortical area<br />
w MCA stenosis<br />
SAD (n=103)
HBP and current smoking were more<br />
prevalent in the non-BOD group<br />
The relevant MCA had more severe<br />
and focal stenosis in the non-BOD<br />
than in the BOD group<br />
76.9% vs 28.3%<br />
Non-relevant stenosis was more<br />
prevalent in the BOD than in the<br />
SAD group