CAHSEE Class Registration Form - Julian Charter School
CAHSEE Class Registration Form - Julian Charter School
CAHSEE Class Registration Form - Julian Charter School

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
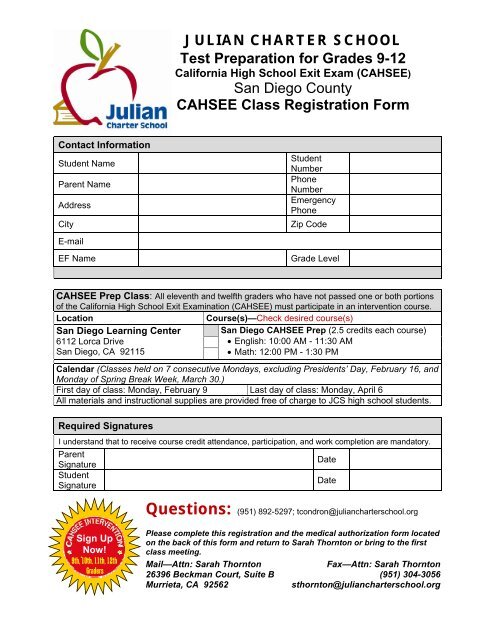
JULIAN CHARTER SCHOOL<br />
Test Preparation for Grades 9-12<br />
California High <strong>School</strong> Exit Exam (<strong>CAHSEE</strong>)<br />
San Diego County<br />
<strong>CAHSEE</strong> <strong>Class</strong> <strong>Registration</strong> <strong>Form</strong><br />
Contact Information<br />
Student Name<br />
Parent Name<br />
Address<br />
City<br />
Student<br />
Number<br />
Phone<br />
Number<br />
Emergency<br />
Phone<br />
Zip Code<br />
E-mail<br />
EF Name<br />
Grade Level<br />
<strong>CAHSEE</strong> Prep <strong>Class</strong>: All eleventh and twelfth graders who have not passed one or both portions<br />
of the California High <strong>School</strong> Exit Examination (<strong>CAHSEE</strong>) must participate in an intervention course.<br />
Location<br />
Course(s)—Check desired course(s)<br />
San Diego Learning Center<br />
6112 Lorca Drive<br />
San Diego, CA 92115<br />
San Diego <strong>CAHSEE</strong> Prep (2.5 credits each course)<br />
• English: 10:00 AM - 11:30 AM<br />
• Math: 12:00 PM - 1:30 PM<br />
Calendar (<strong>Class</strong>es held on 7 consecutive Mondays, excluding Presidents’ Day, February 16, and<br />
Monday of Spring Break Week, March 30.)<br />
First day of class: Monday, February 9 Last day of class: Monday, April 6<br />
All materials and instructional supplies are provided free of charge to JCS high school students.<br />
Required Signatures<br />
I understand that to receive course credit attendance, participation, and work completion are mandatory.<br />
Parent<br />
Signature<br />
Student<br />
Signature<br />
Date<br />
Date<br />
Questions: (951) 892-5297; tcondron@juliancharterschool.org<br />
Sign Up<br />
Now!<br />
9th, 10th, 11th, 12th<br />
Graders<br />
Please complete this registration and the medical authorization form located<br />
on the back of this form and return to Sarah Thornton or bring to the first<br />
class meeting.<br />
Mail—Attn: Sarah Thornton<br />
Fax—Attn: Sarah Thornton<br />
26396 Beckman Court, Suite B (951) 304-3056<br />
Murrieta, CA 92562<br />
sthornton@juliancharterschool.org
JCS Learning Center Medical<br />
Authorization <strong>Form</strong><br />
Required Parent Authorization for Student in Site<br />
<strong>Class</strong>es Sponsored by <strong>Julian</strong> <strong>Charter</strong> <strong>School</strong><br />
Authorization must be filled out by parent/legal guardian.<br />
Student Name _____________________________________________________ Grade _____________________<br />
Emergency Contact Information (During Hours of Event/<strong>Class</strong>):<br />
Parent/Guardian Name __________________________________________________________________________<br />
Home Phone _________________________ Work Phone _________________ Cell Phone _________________<br />
List name of alternative person that has permission to pick up your child in the event you can’t be reached.<br />
Name _______________________________ Relationship to Student _____________ Phone _______________<br />
Health of Student:<br />
q Check here if there are no special medical problems for the staff to be aware of and/or medications to administer<br />
during the course of this class.<br />
q Check here if your son or daughter has a special medical problem that the staff needs to be aware of in the event<br />
of an emergency. (This includes special diet, allergies, info. on blood transfusions, etc.) Please describe below:<br />
__________________________________________________________________________________________________________________<br />
q My child has medication that may need to be administered during school.<br />
Name of medication: ________________________________________________________________________<br />
(All prescriptions, except those which must be kept on the student’s person for emergency use, must be kept and<br />
distributed by the staff. Bring the medication to the front office with a physician’s written instructions for<br />
dispensing at first class meeting.)<br />
Consent to Treat: (One of the Two Choices Must Be Initialed) **ex. – MA for Mary Anderson: 1. X MA<br />
INDICATE YOUR CHOICE OF ACTION IN THE EVENT OF ACCIDENT OR EMERGENCY.<br />
1) X_____ In the event of an accident or emergency, I do hereby authorize a representative of the school to make such arrangements as<br />
he/she considers necessary for my child to receive medical/hospital care, including necessary transportation. I further<br />
authorize the physician named below to undertake whatever x-ray examination, anesthetic, medical, surgical treatment and<br />
hospital care considered necessary for my child as he/she considers necessary. In the event that said Physician is not<br />
available, I authorize such care and treatment to be performed by a licensed physician or surgeon. I FULLY UNDERSTAND<br />
THAT I WILL BE RESPONSIBLE FOR ALL COSTS INCURRED BY EMERGENCYTREATMENT SERVICES, INCLUDING<br />
AMBULANCE OR EMERGENCY TRANSPORTATION.<br />
Physician’s Name _________________________________ Phone ______________________________________<br />
Medical Insurance or HMO __________________________ Policy # _____________________________________<br />
2) X _____I do not choose the above statement and desire the following action to be taken. List below.<br />
_____________________________________________________________________________________________<br />
Ed. Code Sec. 35330 states that “All persons making the field trip or excursion shall be deemed to have waived all claims against the school, district or the State<br />
of California for injury, accident, illness, or death occurring or by reason of the field trip or excursion. All parents or guardians of pupils taking out of state field<br />
trips or excursions shall sign a statement waving such claims. My signature on this form shall constitute an informed and knowing waiver as required by law.<br />
Signature of Parent/Guardian __________________________<br />
Date ___________________ DL10/07