MAKETA 6/1 po
MAKETA 6/1 po
MAKETA 6/1 po

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
ISSN 1335-8421 Acta Med Mart 2006, 6(1)<br />
ACTA MEDICA<br />
MARTINIANA<br />
Journal for Biomedical Sciences,<br />
Clinical Medicine and Nursing<br />
Contents<br />
3<br />
Organization of the capillary network of subpapillary plexus<br />
in healthy human skin<br />
Desanka Výbohová, Katarína Adamicová, Yvetta Mellová, Gabriela Hešková, Lenka Kunertová,<br />
Magdaléna Marčeková, Milan Mello<br />
8<br />
Nibrin and its role in molecular mechanisms of the human<br />
Nijmegen Breakage Syndrome (NBS)<br />
Ján Lehotský, Ján Melter, Katarína Melterová, Marian Patrik, Vladimír Pohanka<br />
16<br />
Comparison of two methods for evaluation of the heart rate control in obese children<br />
Ingrid Tonhajzerova, Michal Javorka, Zuzana Trunkvalterova, Oľga Chroma, Zuzana Lazarova,<br />
Jana Javorkova, Kamil Javorka<br />
22<br />
Effects of Vasoactive Drugs on Cochlear Blood Flow After Transient Cochlear Ischemia<br />
Krzysztof F. Morawski, Grazyna Lisowska, Kazimierz Niemczyk<br />
28<br />
Is the hygienic disinfection of hands with waterless alcohol disinfectant currently<br />
the best way of hand-hygiene?<br />
Mária Štefkovičová, Henrieta Hudečková, Tibor Baška, Štefan Straka<br />
Published by the Jessenius Faculty of Medicine in Martin,<br />
Comenius University in Bratislava, Slovakia
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
E d i t o r - i n - C h i e f :<br />
Javorka, K., Martin, Slovakia<br />
I n t e r n a t i o n a l E d i t o r i a l B o a r d :<br />
Belej, K., Martin, Slovakia<br />
Buchanec, J., Martin, Slovakia<br />
Honzíková, N., Brno, Czech Republic<br />
Kliment, J., Martin, Slovakia<br />
Lehotský, J., Martin, Slovakia<br />
Lichnovský, V., Olomouc, Czech Republic<br />
Mareš, J., Praha, Czech Republic<br />
Plank, L., Martin, Slovakia<br />
Stránsky, A., Martin, Slovakia<br />
Tatár, M., Martin, Slovakia<br />
Żwirska-Korczala, K., Zabrze-Katowice, Poland<br />
E d i t o r i a l O f f i c e :<br />
Acta Medica Martiniana<br />
Jessenius Faculty of Medicine, Comenius University<br />
(Dept. of Physiology)<br />
Malá Hora 4<br />
037 54 Martin<br />
Slovakia<br />
Instructions for authors: http:|www.jfmed.uniba.sk (Acta Medica Martiniana)<br />
T l a č :<br />
P+M Turany<br />
© Jessenius Faculty of Medicine, Comenius University, Martin, Slovakia, 2006
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 3<br />
ORGANIZATION OF THE CAPILLARY NETWORK OF SUBPAPILLARY<br />
PLEXUS IN HEALTHY HUMAN SKIN<br />
DESANKA VÝBOHOVÁ 1 , KATARÍNA ADAMICOVÁ 2 , YVETTA MELLOVÁ 1 , GABRIELA HEŠKOVÁ 1 ,<br />
LENKA KUNERTOVÁ 1 , MAGDALÉNA MARČEKOVÁ 1 , MILAN MELLO 1<br />
1<br />
Department of Anatomy, Comenius University, Jessenius Faculty of Medicine, Martin,<br />
2<br />
Department of Pathology, Comenius University, Jessenius Faculty of Medicine, Martin<br />
A b s t r a c t<br />
Skin microcirculation is organized in two plexuses – superficial subpapillary and deep reticular plexus. The objective<br />
of this study was the observation of the capillary network of subpapillary plexus. The arrangement of subepidermal<br />
capillary loops in papillary line in various body regions, the shape, height of the capillary loops and interpersonal differences<br />
were studied in parallel and perpendicular (to the skin surface) sections. The organization of subpapillary capillary<br />
network was compared on the basis of two parameters: intercapillary distance and a number of adjacent capillary<br />
loops. The obtained values of these parameters didn’t reveal statistically significant differences. According to these<br />
results authors have suggested that mutual capillary loops arrangement in the papillary part of the dermis is identical<br />
in all observed regions and there are no significant interpersonal differences in this organization. The shape of the capillary<br />
loop showed a variability as for the height and course. Higher capillary loops, wavy course of the capillary loop and<br />
wide - rounded capillary loops were more often observed in regions with higher capillary density – in facial region. The<br />
obtained results were discussed with another studies dealing with the arrangement of the skin microcirculation.<br />
K e y w o r d s :<br />
skin, microcirculation, subpapillary plexus, capillary loop, organization<br />
INTRODUCTION<br />
The skin is supplied by two plexuses – deep reticular plexus and superficial subpapillary<br />
plexus. Both plexuses are situated within the dermis. The blood supply for the skin is coming<br />
from deeper vessels crossing the superficial fascia like septocutaneous, fasciocutaneous and<br />
musculocutaneous perforators. Their branches form deep-reticular plexus, which is connected<br />
by vertically oriented vessels with the superficial–subpapillary plexus (1, 2).<br />
Superficial subpapillary plexus is 1- 1.5 mm below the skin surface in the papillary part of<br />
the dermis. It consists of terminal arteriols, capillaries and <strong>po</strong>stcapillary venules. Terminal arteriols<br />
are 17 - 26 μm wide in diameter. Their wall consits of the endothelium, homogenous basal<br />
membrane, elastic fibres and smooth muscle cells. They function as a praecapillary sphicter and<br />
vasomotoric pacemaker (3, 4, 5). Capillaries form subepidermal capillary loops. Each dermal<br />
papilla has its own capillary loop. There are around 40 capillary loops per mm 2 (6). Each capillary<br />
loop has ascending limb (arterial part of the capillary loop), the apex of the loop (transitional<br />
zone) and descending limb (venous part of the capillary loop). Skin capillaries are continuous<br />
capillaries, formed by the endothelial cells, basal membrane and pericapillary cells – pericytes<br />
(3,4). Postcapillary venulles of subpapillary plexus consist of the endothelium, multilaminated<br />
basal membrane, collagen fibres and a layer of pericytes. Segment of <strong>po</strong>stcapillary venulles is<br />
physiologically the most reactive segment of the skin microcirculation and also the most affected<br />
segment by the pathological processes (3, 4).<br />
Deep reticular plexus lies in the borderline between the dermis and hy<strong>po</strong>dermis, cca 4 mm<br />
below the skin surface. The ultrastructure of this plexus is different from the superficial one (4).<br />
The aim of the work is the observation of the mutual arrangement of the skin microcirculation<br />
- especially capillary loops of the subpapillary plexus in healthy human skin.<br />
Address for corres<strong>po</strong>ndence:<br />
MUDr. Desanka Výbohová, Department of Anatomy, Malá Hora Str. N. 4, 037 54 Martin, Slovak Republic<br />
Phone: ++ 421434131427, e-mail: vybohova@jfmed.uniba.sk
4<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
METHODS<br />
Skin biopsy specimens (32) of healthy skin were taken from two human cadavers (43 and 45<br />
years old). Biopsies were excised from 6 designated to<strong>po</strong>graphic regions of the human body: facial<br />
region, thoracic region, abdominal region, back region, brachial and femoral region. Specimens<br />
were fixed in formalin, and embedded into the parraffin blocks. Serial parallel and vertical (to the<br />
surface of the skin) sections were made. Paraffin sections were stained by hematoxyline eosine and<br />
CD34 immunohistochemical stainning (M 7165 CD34 Class clone QBE end 10 DAKO Cytomation)<br />
– for the detection of the capillary endothelium. The shape and <strong>po</strong>sition of the capillary loops of the<br />
superficial subpapillary plexus were studied. The comparison of the architecture of the capillary<br />
network taken from various body regions, and a mutual comparison between two human cadavers<br />
were done. Parallel sections tightly above the papillary line were exactly compared. Two parameters<br />
– intercapillary distance and a number of adjecent capillary loops were established for the comparison.<br />
The microscopic views (microscope - Nikon EPI-FL3 13414 Japan) in constant magnification<br />
(x200) were photographed by the digital camera system (Olympus Camedia system 4.0<br />
megapixel). Digital pictures were processed into binary maps using Vision Assistant version 7.0.<br />
Delaunay triangulation of the <strong>po</strong>ints - marking the axes of the capillary loops was made for the best<br />
determination of assigned parameters. The intercapillary distance was determined as a distance<br />
between two adjacent axises of the capillary loops. These parameters were measured between all<br />
neighbouring capillary loops in Delaunay triangulation made in binary maps of parallel sections.<br />
Sections in the same levels (near the papillary line) were measured and compared. Measurement<br />
tools of Adobe Photoshop version 7.0 were used for the determination of the distance parameters.<br />
The intercapillary distance was measured in units. Units were specified in Adobe Photoshop preferences.<br />
All obtained values of intercapillary distances and a number of adjacent capillaries were<br />
comparable. Statistical analysis of both parameters, obtained of all designated body regions from<br />
the cadavers, was performed by t–test in Microsoft Excel.<br />
RESULTS<br />
Geometrical arrangement of the subepidermal capillary loops of subpapillary plexus in the<br />
papillary part of the dermis was studied in various levels (from the top of the papilla to the level<br />
of the papillary line). In all levels the mutual arrangement of the capillary loops was similar. Parallel<br />
sections, tightly above the papillary line, were exactly compared. Two parameters – intercapillary<br />
distance and a number of adjecent capillary loops were used for comparison of the<br />
mutual arrangement of subpapillary network. Average values of both parameters were determinated<br />
in various body regions of two cadavers (Table 1).<br />
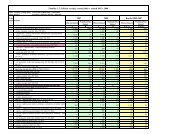
Table1. Average values of intercapillary distances<br />
Person A<br />
Person B<br />
Body<br />
region<br />
Intercapillary<br />
distance (units)<br />
average<br />
sd<br />
Intercapillary<br />
distance (units)<br />
average<br />
sd<br />
t<br />
(A vs B)<br />
Facial<br />
162.91<br />
28.36<br />
153.64<br />
29.36<br />
0.482 - NS<br />
back<br />
167.58<br />
18.42<br />
160.95<br />
22.27<br />
0.478 - NS<br />
abdominal<br />
165.78<br />
33.10<br />
166.33<br />
22.17<br />
0.857 - NS<br />
thoracic<br />
170.14<br />
24.18<br />
175.34<br />
33.46<br />
0.696 - NS<br />
brachial<br />
150.54<br />
25.44<br />
169.86<br />
24.03<br />
0.979 - NS<br />
femoral<br />
175.72<br />
25.80<br />
165.00<br />
20.98<br />
0.322 – NS<br />
T- test did not confirm statistically significant regional and interpersonal differences.
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 5<br />
It is evident that the differences between average values of intercapillary distances in various<br />
body regions are not statistically significant. Table 1 shows that the interpersonal differences of<br />
the intercapillary distances are not statistically significant either. Another studied parameter was<br />
the number of the nearest adjacent capillary loops to which the intercapillary distances were<br />
measured in Delaunay triangulation. Table 2 shows average values of a number of adjacent capillary<br />
loops to the observed capillary. It can be seen that there is no statistically significant difference<br />
between these values – either interpersonal or regional.<br />
Our results lead us to sup<strong>po</strong>se that the mutual horizontal arrangement of the capillary loops<br />
of subpapillary plexus in the papillary dermis within the observed regions of the skin is identical.<br />
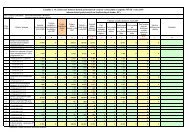
Table 2. Average values of number of adjacent capillary loops<br />
Person A<br />
Person B<br />
Body<br />
region<br />
Number of<br />
adjacent capillaries<br />
average<br />
sd<br />
Intercapillary<br />
distance (units)<br />
average<br />
sd<br />
t<br />
(A vs B)<br />
Facial<br />
5.63<br />
0.52<br />
5.25<br />
0.89<br />
0.323 - NS<br />
back<br />
5.43<br />
0.79<br />
5.63<br />
0.52<br />
0.586 – NS<br />
abdominal<br />
5.43<br />
0.74<br />
5.37<br />
0.52<br />
0.899 – NS<br />
thoracic<br />
5.43<br />
0.98<br />
5.33<br />
0.52<br />
0.827 – NS<br />
brachial<br />
5.14<br />
0.69<br />
5.25<br />
1.04<br />
0.816 – NS<br />
femoral<br />
5.33<br />
1.03<br />
5.57<br />
0.52<br />
0.626 – NS<br />
T - test did not confirm statistically significant regional and interpersonal differences.<br />
Our samples showed variability as for the shape and height of the capillary loop within the<br />
papilla. Sections showed significantly higher capillary density in facial regions in comparison to<br />
the other body regions. Higher capillary loops, wavy course and wide-rounded capillary loops<br />
were more often observed in regions with higher capillary density – especially in facial region. We<br />
have assumed higher capillary loops ( in aspect to the dermal papilla) on the basis of the occurrence<br />
of capillary lumens in more superficial parallel sections according to the top of the papilla.<br />
Wavy course of the capillary loop was demonstrated under the occurrence of a lot of capillary<br />
lumens and cross–sections in horizontal sections and it is known that only a single capillary loop<br />
is in each dermal papillae - that’s why the wavy course can be sup<strong>po</strong>sed. Wide-rounded capillary<br />
loops we sup<strong>po</strong>sed under more distant sections of capillary lumens (ascending and<br />
descendig limb of the capillary loop) visible in horizontal sections.<br />
DISCUSSION<br />
Skin microcirculation is res<strong>po</strong>nsible for supplying the skin with the nutrients and oxygen<br />
and for the regulation of body temperature. Because of its thermoregulatory function, the<br />
rate of blood flow through the skin is one of the most variable in the body and it is approximately<br />
10 times higher that is required for nutritional sup<strong>po</strong>rt. Skin microcirculation also<br />
participate in wound healing and in the pathogenesis in some skin diseases. Respecting of<br />
the particularities of the skin microcirculation is necessary in reconstructive surgery - in flap<br />
reconstruction.<br />
Although both dermal plexus - subpapillary and reticular, even their vertical arrangement<br />
and ultrastructure are well known, there are another parameters, also like horizontal geometrical<br />
properties of the capillary network, which need to be explored. We have aimed our observation<br />
to capillary network of subpapillary plexus in thin skin. On the basis of our results we have
6<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
Fig. 1: Parallel section of abdominal skin in the papillary<br />
part of the dermis. Sections of dermal papillae and surrounding<br />
epidermis with distinguishable red–brown crosssections<br />
of the capillary loops within the papillae. Immunohistochemical<br />
staining (CD34), magnification x 200.<br />
Fig. 2: Binary map ( made by Vision Assistant version<br />
7.0 ) of the parallel section of the abdominal skin (magnification<br />
x 200). Sections of capillary loops with marked<br />
intercapillary distances in Delaunay triangulation, d =<br />
intercapillary distance.<br />
Fig. 3: Binary map ( made by Vision Assistant version 7.0 )<br />
of the parallel section of the skin from thoracic region (magnification<br />
x 200). Sections of capillary loops with marked<br />
intercapillary distances in Delaunay triangulation.<br />
Fig. 4: Binary map (made by Vision Assistant version<br />
7.0 ) of the parallel section of facial skin (magnification x<br />
200). Sections of capillary loops with marked intercapillary<br />
distances in Delaunay triangulation.<br />
sup<strong>po</strong>sed that mutual horizontal arrangement of subepidermal capillary loops in subpapillary<br />
plexus is identical in all body regions in the thin skin and there are no evident interpersonal differences<br />
in this organization. Grunt et al. (6) in his scanning electron microscopic study of vascular<br />
bed in retroauricular skin also have shown no interindividual differences. Geometrical network<br />
analysis, performed by Santhilier et al. on the scalp, was a videocapillaroscopic study based on<br />
proximity parameters. They have inferred that capillary network is uniform and homogenous (7,8).
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 7<br />
What’s different - is the shape of the capillary loops within the dermal papillae. Similar sup<strong>po</strong>sition<br />
of various shape of capillary loop within the papilla is described by Miniati et al. (9). He<br />
studied capillary network using videocapillaroscopy on healthy subjects. In most body areas only<br />
summit of the capillary loop could be seen. In the facial region (forehead, cheek, chin) line and<br />
network forms appeared, which were interpreted like parallel course of the capillary loop (9). In<br />
our opinion and on the basis of our observation wavy and wide-rounded capillary loops seem to<br />
have parts with parallel course resulting in line forms visible in capillaroscopic views. Hern and<br />
Mortimer have reviewed various shapes of capillary loops. They described the presence of more<br />
shapes even in one region, mostly in facial regions (10).<br />
The height of the capillary loop can vary. It can be changed also during some pathological<br />
changes. For example in psoriasis the capillary loops are extremly high and tortuous. They reach<br />
nearly the top of the papillae (11,12). On the other hand decreased, capillary loops of the superficial<br />
plexus compare to healthy skin were described in systemic sclerosis (13).<br />
Just these features of the capillary loop–shape and height, can influence the capillary density,<br />
because only one capillary loop enters into the each dermal papilla. Samples in our study showed<br />
higher capillary density in facial regions compare to the others. Head and neck region are regions<br />
with highest capillary density as for the thin skin in Pasyk’s study too (14). Psoriasis is characterized<br />
by extremly high and tortuous capillary loops in lesional skin. It results in increased endothelial<br />
mass and significantly higher capillary density compare to the healthy skin (12, 13, 15).<br />
Detailed knowledge of the cutaneous microcirculation in the healthy skin is im<strong>po</strong>rtant not<br />
only for our basic morphological understanding but also because the microcirculation and its<br />
changes play a predominant role in some skin diseases.<br />
REFERENCES<br />
1. Čihák R. Kůže a kožní orgány. In: Čihák R. Anatomie 3. Praha: Grada Publishing; 1997. p. 559 – 574.<br />
2. Dylevský I. Kožní systém – integumentum commune. In: Dylevský I, Druga R, Mrázková O. Funkční anatomie člověka.<br />
Praha: Grada Publishing; 2000. p. 633 – 640.<br />
3. Braverman IM. The cutaneous microcirculation. J Invest Dermatol Sym<strong>po</strong>sium Proceedings 2000; 5: 3-9.<br />
4. Braverman IM. Ultrastructure and organisation of the cutaneous microvasculature in normal and pathological<br />
stages. J Invest Dermatol 1989; 93: 2S-9S.<br />
5. Braverman IM, Sibley J. Ultrastructural and 3–dimensional analysis of the contractile cells of the cutaneous<br />
microvasculature. J Invest Dermatol 1990; 95: 90-96.<br />
6. Grunt T, Lametschwandtner A, Staindl O. Angioarchitecture of the retroauricular skin in humans. HNO 1982; 30:<br />
420-425.<br />
7. Santhilier JM, Degouy A, Gharbi T, Pieralli C, Humbert P. Geometrical network analysis. Skin Res Technol 2003; 9:<br />
312-320.<br />
8. Sainthilier JM, Gharbi T, Muret P, Humbert P. Skin capillary network recognition and analysis by means of neural<br />
algorithms. Skin Res Technol 2005; 11: 9-16.<br />
9. Miniati B, Macchi C, Molino Lova R, Catini C, Gulisano M, Contini M, Conti AA, Gensini GF. Descriptive and morphometric<br />
anatomy of the architectural framework of microcirculation: a videocapillaroscopy study on healthy adult<br />
subjects. Ital J Anat Embryol 2001; 106: 233-238.<br />
10. Hern S, Mortimer PS. Visualization of dermal blood vessels – capillaroscopy. Clin Exp Dermatol 1999; 24: 473-478.<br />
11. Hern S, Allen MH, Sousa AR. Immunohistochemical evaluation of psoriatic plaques following selective photothermolysis<br />
of the superficial capillaries. Br J Dermatol 2001; 145: 45-54.<br />
12. Mordovstev VN, Albanova VI. Morphology of skin microvasculature in psoriasis. Am J Dermatopathol 1989; 11: 33-42.<br />
13. SauermannK, Gambichler T, Jaspers S, Radenhausen M, Rapp S, Reich S, Altmayer P, Clemann S, Teichmann S,<br />
Ennen J, Hoffmann K. Histometric data obtained by in vivo confocal laser scanning microscopy in patients with systemic<br />
sclerosis. BMC Dermatol 2002; 2: 2-8.<br />
14. Pasyk KA, Thomas SV, Hasset CA, Cherry GW, Faller R. Regional differences in capillary density of the normal human<br />
dermis. Plast Reconstr Surg 1989; 83: 939-945.<br />
15. Barton SP, Abdullah MS, Marks R. Quantification of microvascular changes in the skin in patients with psoriasis.<br />
Br J Dermatol 1992; 126: 569-574.<br />
Received: March, 7, 2006<br />
Accepted:May, 5, 2006<br />
Acknowledgements:<br />
This work was sup<strong>po</strong>rted by Comenius University – grant No UK/257/2006.
8<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
NIBRIN AND ITS ROLE IN MOLECULAR MECHANISMS OF THE HUMAN<br />
NIJMEGEN BREAKAGE SYNDROME (NBS)<br />
JÁN LEHOTSKÝ 1 , JÁN MELTER 2 , KATARÍNA MELTEROVÁ 2 , MARIAN PATRIK 2 ,<br />
VLADIMÍR POHANKA 2<br />
1<br />
Department of Medical Biochemistry, Jessenius Faculty of Medicine, Comenius University, Martin, 2 Šrobár’s Institute<br />
of Children Tuberculosis and Respiratory Diseases, Dolný Smokovec, and Clinic of Children and Adolescents, Jessenius<br />
Faculty of Medicine, Comenius University and Martin Faculty Hospital, Martin, Slovak Republic<br />
A b s t r a c t<br />
Backgrounds and aims: Nijmegen breakage syndrome (NBS) is an autosomal recessive chromosomal instability<br />
disorder with hypersensitivity to ionizing radiation. The clinical phenotype is characterized by congenital microcephaly,<br />
mild dysmorphic facial appearance, growth retardation, immunodeficiency, and a highly increased risk for lymphoreticular<br />
malignancy.<br />
Pathomechanism of disease process and experimental data: The gene causing the disease, NBS1- nibrin, is res<strong>po</strong>nsible<br />
for double strand DNA breaks repair. This review describes the pro<strong>po</strong>sed pathomechanism of NBS syndrome<br />
with emphasis on the role of NBS1 gene mutation in disease process. The data sup<strong>po</strong>rt the view that most of the Slovak<br />
NBS patients are homozygous for the Slavic mutation 657del5 of NBS1 gene.<br />
Conclusions: Advantages of early routine genetic analysis of NBS1 gene, together with combination of microcephaly<br />
diagnostis and preventive care can lead to significant improvement of patient’s life span expectancy.<br />
K e y w o r d s : Double strand DNA breaks, NBS1, nibrin, Nijmegen Breakage Syndrome<br />
INTRODUCTION<br />
In 1981 was by Dutch scientists first described the autosomal recessive genetically inherited<br />
disease, characterized by specific cellular alterations as res<strong>po</strong>nse to damage (breaks) in chromosomal<br />
double strand DNA (1). The disease which develops in early childhood was given by the<br />
name of the town where scientists worked - the Nijmegen breakage syndrome (NBS). Double<br />
strand breaks (DSBs) are one of the most serious influences to cellular homeostasis. Fortunatelly,<br />
human cells are endowed with mechanisms which are able to repair double strand<br />
breaks (DSB repair). However, if for unknow reason, the breaks are being unrepaired, the disorder<br />
might lead to aberrant reorganization of genomic DNA and might eventually follow to cellular<br />
death or cancerogenesis. These type of breaks are activated during the life of every cell of our<br />
body as a result of several external noxious stimuli, such as ionizing radiation, but also as<br />
results of endogenous processes linked with cellular and chromosomal division, such as DNA<br />
replication, meiotic and the so called V(D)J gene recombination.<br />
Nijmegen breakage syndrome is a typical example of the disease which is characterized by the<br />
defects in double strand DNA breaks (DSB) repair mechanism. The disease is clinically expressed<br />
in the early childhood in the form of immunodeficiency, recurrent infections of respiratory system,<br />
microcephaly, high risk of malignancies and growth retardation (2). The diseased cells are<br />
hypersensitive to ionised radiation on the cellular level. The hypersensitivity is expressed by<br />
chromosomal instability and immunodefectivity on both the cellular and humoral level (3).<br />
Defects of repair mechanisms of damaged cellular DNA in humans<br />
The process of multiple cellular division is biologically linked with several events with impact<br />
on both the cell itself and the whole organism. The process of cell division starts in the first minutes<br />
of prenatal development by combination of oval and spermal genetic material, it follows by<br />
division of fertilized egg and in the majority of human cells, the cell division persists over the<br />
whole life and ends by the death of cell or organisms. The DNA molecule as a carrier of genetic<br />
Address for corres<strong>po</strong>ndence:<br />
Prof. Dr. Jan Lehotsky, DrSc., Department of Medical Biochemistry,<br />
Jessenius Faculty of Medicine, Malá Hora Str. N. 4, 037 54 Martin, Slovak Republic<br />
Phone: 421-43-4131565, Fax: 421-43-4136770, e-mail: Lehotsky@jfmed.uniba.sk
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 9<br />
information is present in nuclear chromosomes and in mitochondria in the form of double helix<br />
of two complementary <strong>po</strong>lynucleotide chains. Defects (breaks) in DNA molecule in the form of<br />
double strand breaks- DBS are the most serious cellular events with impact on biological life of<br />
the cell. Our organism is fortunately equipped with several mechanisms res<strong>po</strong>nsible for repair of<br />
these defects (4). DNA breaks occur accidentally as a result of exogenous radiation or s<strong>po</strong>ntaneously<br />
as a side products of endogenous DNA replication, meiotic recombination and homologous<br />
recombination or non-homologous (V(D)J recombination of genes for immunoglobulines.<br />
Although in most cases the process of DNA repair has no immediate influence on cell viability,<br />
the presence of non-lethal defect and its repair might eventually lead to several pathological consequences.<br />
The most serious are:<br />
i) retardation of cell cycle due to the active function of repair mechanisms,<br />
ii) increased dis<strong>po</strong>sition to cancerogenesis,<br />
iii) various neonatal defects,<br />
iv) precocious aging and,<br />
v) severe shortening of the life expectance.<br />
Repair of damaged DNA requires a cascade of events which can be summarized as follows:<br />
i) recognition of the site of damage<br />
ii) its removal or splice<br />
iii) re-synthesis of new DNA<br />
iv) ligation of new DNA with non damaged DNA.<br />
As it has been already proved, more than 130 genes or their proteinous products are present<br />
in humans which are essential parts of the repair mechanisms. Likewise, the defect or total<br />
absence of these genes remarkably increase the percentage of mutated DNA (5). As a consequence,<br />
DBS similarly to other variations of DNA damages eventually leads to inhibition of replication<br />
and transcription of DNA and accidentally to the loss of heterozygozity.<br />
Several enzymes catalyze ligation of newly formed free DNA <strong>po</strong>lynucleotide chain ends within<br />
the DNA repair process. Of the known genes which encode for reparatory enzymes, several<br />
play role as protectant against nucleolytic attack of damaged DNA, on the other hand, several<br />
genes are also triggers for the diseased process (Tab. 1).<br />
Table 1. Examples of human diseases linked with disturbances of Double Strand DNA repair (5,9,16).<br />
Name<br />
MSH2-non<strong>po</strong>ly<strong>po</strong>us colorectal tumor<br />
MSH2<br />
Xeroderma pigmentosum<br />
(XP) group A–G<br />
Ataxia – teleangiectasia (AT)<br />
Breast cancer type 2<br />
BRCA-2<br />
Werner’s syndrome<br />
Bloom’s syndrome<br />
Fanconi anemia, group A–G<br />
Phenotype<br />
Intestinal cancer<br />
Skin cancer, cellular sensitivity to UV,<br />
neurological abnormalities<br />
leukemia, lymphoma, cellular sensitivity<br />
to gamma radiation, genomic<br />
instability<br />
Breast and ovarian cancer<br />
Progeria, multinodal cancer, genomic<br />
instability<br />
multinodal cancer<br />
Congenital abnormalities, leukemia,<br />
genomic instability<br />
Disturbed gene/ process<br />
Repair of uncorrect DNA base<br />
Nucleotide excission repair<br />
ATM protein, protein kinase activated<br />
with DSB<br />
Homologous recombination repair<br />
3 -exonuclease and DNA helicase<br />
DNA helicase<br />
Repair of DNA cross-link
10<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
In principle, the cells use two mechanisms for DSB repair (Fig.1):<br />
i) non-homologous end joining - NHEJ recombination<br />
ii) homologous recombination - HR<br />
Fig. 1. Schematic illustration of the homologous and non-homologous joining after repair of DNA breaks (4,5,9).<br />
NHEJ recombination requires recognition at least several base pairs of damaged DNA by two<br />
proteins Ku70 a Ku80. In addition, these proteins act as enzymes which can ligate both 3’ and<br />
5’ free DNA <strong>po</strong>lynucleotide ends. Other enzymes, such as DNA dependent protein kinase, additional<br />
protein XRCC4 and DNA ligase 4 are res<strong>po</strong>nsible for attachment of missing nucleotide<br />
pairs on damaged DNA. However, as shown experimentaly on cells derived from NBS patients,<br />
this type of DNA repair in not morbidly disturbed has not been proved as a part of NBS<br />
etiopathogenesis (5).<br />
Consequently, for proper function homologous recombination (HR repair) requires several<br />
proteins including protein called as NBS1. Mutation of NBS1 leads to initiation of several events,<br />
such as production of aberrant recombination intermediates, supression of inter-chromosomal<br />
translocation and complex cellular changes which are expressed clinically as Nijmegen breakage<br />
syndrome (NBS) (6).<br />
Nijmegen breakage syndrome (NBS)<br />
Nijmegen breakage syndrome (NBS) is a human recessive disease described in 1981 for the<br />
first time (1). In the register of genetic diseases, it can also be found under the alternative names<br />
such as BBS- Berlin Breakage Syndrome, Seeman’s syndrome, Ataxia teleangiectasia variant<br />
No. 1, for futher details see web site: www.genetests.org. Due to its similar clinical and cellular<br />
manifestations to Ataxia teleangiectasia (AT), the syndrome was at the beginning thought as clinical<br />
variant of AT. The breakthrough for the understanding of NBS pathomechanism was isolation<br />
of gene called NBS1 in 1998 (7). As was shown, mutation of this particular gene leads to the<br />
diseased state and molecularly, it is involved in the mechanism of DSB repair and regulation of<br />
check-<strong>po</strong>ints of cell cycle. Thus, NBS syndrome, like other similar inherited human diseases of<br />
this type such as Bloom’s syndrome, Fanconi anemia and Ataxia teleangiectasia, belongs commonly<br />
to the diseases characterized with defects in repair mechanism of double strand DNA<br />
breaks (7) (Tab.1).<br />
Clinical manifestations<br />
Clinically, the NBS is manifested in early childhood by growth retardation, facial dysmorphia<br />
such as typical bird-like face, characterized by a receding forehead, a prominent mid face with
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 11<br />
a long nose and a long philtrum and receding mandible. A progressive microcephalia with a mild<br />
deficiency of congnitive abilities is linked with a retarded psychomotoric development, occasionally<br />
also with hyperactivity, however linked always with very good interpersonal relations. Ovarian<br />
dysgenesis is probably caused by the increased level of gonadotropins. The most typical are<br />
very frequent infections of respiratory and urinary tracts. The prominent defects of cellular alterations<br />
are immunodeficiency, chromosomal instability, radiation hypersensitivity and exceptional<br />
incidence of malignancies in childhood and early adolescent age. Of these the most common<br />
are lymphomas, the majority of which is B cell type, leukemia, medulloblastoma, rhabdomyosarkoma<br />
etc. Of other signs, very common are the irregular skin pigmentation manifested<br />
once as hyperpigmented, or hy<strong>po</strong>pigmented s<strong>po</strong>ts, the congentital malformation such as<br />
hydrocephalus, the occipital cysts etc. (1,2). Immunodeficiency in cellular and humoral part is<br />
the constant laboratory finding in NBS patients. Agammaglobulinemia is found in about 35 %<br />
patients, frequent is also IgA deficiency in about 20 % patients. Although the total level of IgG is<br />
normal in most of the patients, very frequent is IgG2 and IgG4deficiency. The defects in cellular<br />
immunity reduce percentages of total CD3+ a CD4+ lymphocytes, although the count of CD8+<br />
lymphocytes is not influenced. Likewise, the cytokines production is depressed and the res<strong>po</strong>nse<br />
of T cell to phytohemagglutinin is markedly depressed (1, 2, 8).<br />
Karyotypes of the patients are basically normal. However, cytogenetic chromosomal abberations<br />
such as translocations, reorganizations, can be found in <strong>po</strong>sitivive individuals after<br />
phytohemagglutinin (PHA) stimulation of T cells. Chromosomal breaks (reorganizations) are<br />
indicated on chromosome 7 and 14, in sites of genes for immunoglobulins and receptors for<br />
T cells. Chromosomal abberations include inv (7) (p13q35), t(7,14) (p13, q11), t (7,14)<br />
(q35,q11), t (7,7) (p13,q35), T (14,14) p(11,q32) (9). Chromosomal analysis indicates for s<strong>po</strong>ntaneous<br />
chromosomal instability of chromatid type and hypersensitivity to ionised radiation.<br />
The radiation, which in normal cells blocks DNA synthesis, in cells from NBS patients initiates<br />
selective radio-resistant DNA synthesis (RDS). This feature due to abberant regulation<br />
of cell cycle is very similar to cells with Ataxia teleangiectasia (AT). However, clinical patterns<br />
are partially different. NBS patients do not express elevated level of α- fetoprotein, absent are<br />
cerebellar ataxia or teleangiectasia, on the other hand, both the microcephalia and the<br />
growth retardation are present. A new modification of AT has been proved in late 1990s called<br />
AT like disorder-ATLD (10) (Tab.2).<br />
Table 2. Comparison of clinical symptoms and cellular properties of AT, NBS and ATLD (5,9,16,17,18).<br />
Clinical symptoms<br />
AT<br />
NBS<br />
ATLD<br />
Telangiectasia<br />
+<br />
-<br />
-<br />
Cerebellar ataxia<br />
+<br />
-<br />
+<br />
Increased fetoprotein<br />
+<br />
-<br />
+<br />
Microcephalia<br />
-<br />
+<br />
-<br />
Bird like face<br />
-<br />
+<br />
-<br />
Immunodeficiency<br />
+<br />
+<br />
-<br />
Malignities<br />
+<br />
++<br />
Non-described<br />
Cellular properties<br />
Radiation sensitivity<br />
+<br />
+<br />
+<br />
Chromos. instability<br />
+<br />
+<br />
+<br />
RDS<br />
+<br />
+<br />
+<br />
Defective gene<br />
11q23<br />
8q21.3<br />
11q21<br />
Defective protein<br />
ATM<br />
NBS1<br />
MRE11
12<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
Gene res<strong>po</strong>nsible for NBS was mapped by complementation assay to chromosome 8q21-24<br />
and independently by linkage analysis to chromosome 8q 21.3. The gene has been later isolated,<br />
and it was shown to be of 50 kilobases in size with 16 exones. Gene is expressed (transcribed)<br />
to two kinds of mRNAs, one with size of 2.6 and second with size of 4.8 kbases, distinct only by<br />
<strong>po</strong>lyadenylation sites. Both mRNA types <strong>po</strong>ssess simple open reading frame, which give protein<br />
with 754 amino acids and molecular weight of 85 kDa after succesfull proteosynthesis. Gene is<br />
ubiquitously expressed in all tissues, particularly high amount can be found in testis, thymus,<br />
and other tissues with high proliferative activity such as liver, lungs, kidneys, gut, etc. (5).<br />
In healthy individuals the NBS gene shows several <strong>po</strong>lymorphisms. Fortunately, these allelic<br />
variants do not show any remarkable phenotypic pathologies (11) (Tab. 3).<br />
Table 3. Normal allelic variants described till now on NBS1 gene (5,9,16).<br />
Polymorphism<br />
102 G/A<br />
553 G/C<br />
1197 T/C<br />
2016 A/G<br />
Nucleotide alteration<br />
G/A to 102<br />
G>C to 553<br />
T>C to 1197<br />
A>G to 2016<br />
Exon<br />
2<br />
5<br />
10<br />
13<br />
Thus, as has been shown before, the gene product – protein called NBS 1- NIBRIN (or 95),<br />
(M r<br />
=85 kDa) takes part in the mechanism of DSB repair by homologous recombination (HR). The<br />
whole repair process is initiated immediately after the event of DNA break by recognition of the<br />
break site. After the recognition of deranged locus on DNA molecule, newly formed 3’end of single<br />
DNA strand attacks intact homologous chromosomes. This process is catalyzed by the action<br />
of protein RAD. As a result of catalysis, the recombinant homologous structures called Holiday<br />
structures of recombination are formed. Repair of DNA breaks is accomplished after definitive<br />
new DNA synthesis. Contrary to non-homologous repair, the homologous recombination repair<br />
mechanism requires at least several hundreds of base pairs on DNA molecule.<br />
Protein nibrin shows only small similarities to other known proteins. The only little homology<br />
can be found with yeasts N- terminal site of DNA repair protein Xrs2. The Xrs2 protein is subunit<br />
of multiprotein complex of two large proteins called MRE11 and RAD50. It is interesting that<br />
in mammals protein nibrin is also part of this complex and thus it represents the human homologue<br />
of yeast DNA repair protein (5). Protein MRE11 manifests both the endonuclease catalytic<br />
activity for single strand DNA and the activity of 3’ 5’-exonuclease for double strand DNA. Protein<br />
RAD50 is ATP-dependent DNA-binding protein with to<strong>po</strong>isomerase catalytic function. As has<br />
been shown by several experiments, the role of NBS1 is to maintain physical and functional<br />
attachment of both MRE11 and RAD50 proteins in cell nucleus and thus to form complex of<br />
MRE11/RAD50/NBS1 with the function of nuclease activity. This activity is necessary for the<br />
repair of damaged double strand DNA. Two domains, one called FHA (Fork head associated) and<br />
the second called BRCT (Breast cancer carboxy terminal), can be recognized on N- terminal part<br />
of nibrin molecule (Fig. 2).<br />
Fig. 2. Structural domains of protein NBS1- nibrin and their biological functions (6, 5).
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 13<br />
These domains are always present as highly conservative in proteins with repair function and/or<br />
proteins res<strong>po</strong>nsible for cell cycle regulation. Domain res<strong>po</strong>nsible for the interaction with MRE11<br />
protein is localized on C- terminus of NBS1 protein. The bond between NBS1 and MRE11 is essential<br />
for recruitment of MRE11 into the nucleus and concomitant physical and functional attachment<br />
of MRE11 and RAD50. In addition, the nibrin molecule contains selective SQ sequences, whose serines<br />
(Ser –278 and Ser –343), can be selectively phosphorylated by ataxia teleangiectasia kinase<br />
(ATM- kinase) on res<strong>po</strong>nse of DNA damage. This cellular event has a great influence on activation of<br />
control <strong>po</strong>int of S phase of cell cycle and thus it has a direct influence on cellular division. It is now<br />
known that ATM gene is a part of pathomechanism of both the chronic lymphocytic leukemia of<br />
B cells and prolymphocytic leukemia of T cells, where it act as tumour supressor gene. Although the<br />
NBS1 gene is also tumour supressor gene and in NBS patients is lymphoma of B cell very frequent,<br />
it has not yet been proved that NBS1 gene plays a remarkable role in carcinogenesis of s<strong>po</strong>radic lymphomas<br />
(13). Distincly, quite frequent missense mutations of NBS1 gene can be detected in children<br />
patients with acute lymphoblastic leukemia (ALL), which suggests that NBS1 gene can be thought<br />
as risk factor in the pathogenesis of this disease (14). As we has noticed before, NBS is ethiologically<br />
similar to ataxia teleangiectasia. Already mutated ATM gene or its kinase (ATM kinase) signalize<br />
presence of double strand DNA breaks by expression of enzyme activity which phosphorylates several<br />
proteins res<strong>po</strong>nsible for DNA repair but also for initiation of cell cycle arrest or cell a<strong>po</strong>ptosis.<br />
Unstressed cells or cells without DNA breaks have an ATM kinase in a dormant – dimeric state in<br />
the nucleus. When DNA breaks occur, chromatine structure locally disrupts. This event activates<br />
intermolecular modification and disaggregation of ATM dimer to monomers by its autophosphorylation<br />
on Ser 1981. ATM monomer migrates and recognizes the site of double strand DNA break and<br />
triggers phophorylation of several nuclear proteins. One of the most prominent is histone H2AX,<br />
which is phosphorylated on its C- terminal serine. What is im<strong>po</strong>rtant for NBS disease is that protein<br />
NBS1-nibrin is directly bound to phosphorylated histone H2AX by interaction with specific region on<br />
its molecule called FHA/BRCT. This forms a recognition site which enables DNA repair. Similarly,<br />
other proteins which <strong>po</strong>ssess BRCT region, such as protein of breast cancer-BRCA1 can be bound<br />
to histone H2AX by similar mechanism (5, 15). Complex NBS1-MRE11-RAD50 thus acts as a sensor<br />
of double strand DNA breaks for activation of ATM and its delivery to the break site. Besides histone,<br />
kinase phosphorylates also other cellular targets such as proteins p53 and Chk2, which eventually<br />
activate two separated processes:<br />
i) by histone phosphorylation is initiated repair of DNA breaks by homologous recombination<br />
ii) by p53 or Chk2 phosphorylation is regulated control <strong>po</strong>int of intra S phase and G2 phase of<br />
cell cycle (Fig. 3).<br />
Fig.3 Functional scheme of NBS1 protein- nibrin in human cells (5,15).
14<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
As has been recently shown on mice with activated NBS1 gene, this gene plays an im<strong>po</strong>rtant<br />
role also in prevention of neurological defects which can be frequently seen on human patients<br />
such as ataxia or cerebellar defects (16).<br />
All up to now identified disease - caused alleles of NBS1 gene have been shown to be a null<br />
alleles. In one of the best described group of NBS patients, more than 90% were homozygotic and<br />
had common deletion of 5 base pairs (657delACAAA) on exon No.6 of NBS1 gene and were of<br />
Slavic origin ( 14). Several other mutations have also been shown in another nations which were<br />
heterozygotic but with a secondary mutation on 657del5 (Tab. 4). It is interesting that cells from<br />
patients grown in cultures expressed an aberrant mRNAs from all mutated genes. However, due<br />
to very hard detection of protein nibrin by Western blot analysis, it is not clear if this protein is<br />
produced in a truncated form and thus undetectable or if it is completely lost from patient cells.<br />
Table 4. Pathologic allelic variants of NBS1 gene (5,9,16,17,18).<br />
Mutation<br />
657del5<br />
681del7<br />
698del4<br />
835del4<br />
842insT<br />
900del25<br />
976C>T<br />
1089C>A<br />
1142delC<br />
Nucleotide alteration<br />
657-661delACAAA<br />
681-682delT<br />
698-701delAACA<br />
835-838delCAGA<br />
842insT<br />
900-924del25<br />
C>T na 976<br />
C>A na 1089<br />
1142-1143delC<br />
Exon<br />
6<br />
6<br />
6<br />
7<br />
7<br />
8<br />
8<br />
9<br />
10<br />
Consequence<br />
shift<br />
Shift<br />
Shift<br />
Shift<br />
Shift<br />
Shift<br />
Q326X<br />
Y363X<br />
Shift<br />
Origin<br />
Slavic<br />
Russian<br />
English<br />
Italian<br />
Mexican<br />
African<br />
Dutch<br />
?<br />
Canadian<br />
Clinical observations<br />
Varon et al. (11) have found 25 heterozygotes of Slavic mutation on the sample of 4416 newborns<br />
from Poland, Czech Republic and Ukraine, e.i. the ratio of 1/177 with regional differences<br />
from 1:90 to 1:314. Seemanová et al. (17) in 1969-1992 have detected 24 homozygotes in Czechoslovakia.<br />
The detected mutation frequency from 5.2 million of Czechoslovak newborns was<br />
lower ( 1:271000) than it was expected in that time. One of the suggested explanations of the<br />
lower prevalence was underdiagnosis in subisolates. However, in spite of <strong>po</strong>ssible lower effectivity<br />
of detection in previous period, results of 2996 diagnosed newborn blood samples in 2002-<br />
2003 in Slovakia have detected only 3 heterozygotes (657del5), which represents the frequency<br />
of 1:199. In total, only 14 pacients with NBS from 11 families have been diagnosed from all newborns<br />
in Slovakia in 1969-2002. Of those 14 patients, 7 are NBS gene homozygotes. In Czech<br />
Republic, 8 NBS newborn patients (including 2 fetuses) have been detected in the same period,<br />
which in comparison to Slovakia (1:118180) represents the frequency of 1: 262500. In the study<br />
conducted in cooperation with the Šrobar Institute for Children Tuberculosis and Respiratory<br />
Diseases in Dolny Smokovec and Jessenius Faculty of Medicine Martin, the total of 1184 blood<br />
samples have been examined for DNA Slavic mutation in regions Turiec, Orava, Spiš in Slovakia<br />
(19). Of 724 newborns, 6 have been found heterozygotic to Slavic mutation and in 427 oncologic<br />
patients, no Slavic mutation has been detected. The relative high incidence of Slavic mutation<br />
(657del5) has been expected from previous studies which corres<strong>po</strong>nds to mutation frequency in<br />
other Slavonic countries. As a rule, all homozygotic patients suffered malignancies and immunodeficiencies,<br />
heterozygots are well-compensated by physiological allele.
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 15<br />
REFERENCES<br />
1. Weemaes CM, Hustinx TW, Scheres JM, van Munster PJ, Bakkeren JA, Taalman RD.: A new chromosomal instability<br />
disorder: the Nijmegen breakage syndrome. Acta Paediatr Scand. 1981; 70(4): 557-564.<br />
2. Seemanova E, Passarge E, Beneskova D, Houstek J, Kasal P, Sevcikova M.: Familial microcephaly with normal intelligence,<br />
immunodeficiency, and risk for lymphoreticular malignancies: a new autosomal recessive disorder. Am<br />
J Med Genet. 1985; 20(4):639-648.<br />
3. Conley ME, Spinner NB, Emanuel BS, Nowell PC, Nichols WW.: A chromosomal breakage syndrome with profound<br />
immunodeficiency. Blood. 1986; 67(5):1251-1256.<br />
4. Ferguson DO, Alt FW.: DNA double strand break repair and chromosomal translocation: lessons from animal models.<br />
Oncogene. 2001; 20(40):5572-5579.<br />
5. Matsuura S, Kobayashi J, Tauchi H, Komatsu K.: Nijmegen breakage syndrome and DNA double strand break repair<br />
by NBS1 complex. Adv Biophys. 2004; 38: 65-80.<br />
6. Carney JP, Maser RS, Olivares H, Davis EM, Le Beau M, Yates JR 3rd, Hays L, Morgan WF, Petrini JH.: The<br />
hMre11/hRad50 protein complex and Nijmegen breakage syndrome: linkage of double-strand break repair to the cellular<br />
DNA damage res<strong>po</strong>nse. Cell. 1998; 93(3):477-486<br />
7. Varon R, Vissinga C, Platzer M, Cerosaletti KM, Chrzanowska KH, Saar K, Beckmann G, Seemanova E, Cooper PR,<br />
Nowak NJ, Stumm M, Weemaes CM, Gatti RA, Wilson RK, Digweed M, Rosenthal A, Sperling K, Concannon P, Reis<br />
A.: Nibrin, a novel DNA double-strand break repair protein, is mutated in Nijmegen breakage syndrome. Cell. 1998;<br />
93(3):467-476<br />
8. Chrzanowska KH, Kleijer WJ, Krajewska-Walasek M, Bialecka M, Gutkowska A,<br />
Goryluk-Kozakiewicz B, Michalkiewicz J, Stachowski J, Gregorek H, Lyson-Wojciechowska G, et al.: Eleven Polish<br />
patients with microcephaly, immunodeficiency, and chromosomal instability: the Nijmegen breakage syndrome. Am<br />
J Med Genet. 1995; 57(3):462-471.<br />
9. Shiloh Y. Ataxia-telangiectasia and the Nijmegen breakage syndrome: related disorders but genes apart. Annu Rev<br />
Genet. 1997; 31:635-662.<br />
10. Stewart GS, Maser RS, Stankovic T, Bressan DA, Kaplan MI, Jaspers NG, Raams A,<br />
Byrd PJ, Petrini JH, Taylor AM.: The DNA double-strand break repair gene hMRE11 is mutated in individuals with<br />
an ataxia-telangiectasia-like disorder. Cell. 1999; 99(6):577-87.<br />
11. Varon R, Seemanova E, Chrzanowska K, Hnateyko O, Piekutowska-Abramczuk D,<br />
Krajewska-Walasek M, Sykut-Cegielska J, Sperling K, Reis A. Clinical ascertainment of Nijmegen breakage syndrome<br />
(NBS) and prevalence of the major mutation, 657del5, in three Slav <strong>po</strong>pulations. Eur J Hum Genet. 2000; 8(11):900-<br />
902.<br />
12. Resnick IB, Kondratenko I, Togoev O, Vasserman N, Shagina I, Evgrafov O, Tverskaya S, Cerosaletti KM, Gatti RA,<br />
Concannon P.: Nijmegen breakage syndrome: clinical characteristics and mutation analysis in eight unrelated Russian<br />
families. J Pediatr. 2002; 140(3):355-361.<br />
13. Cerosaletti KM, Morrison VA, Sabath DE, Willerford DM, Concannon P.: Mutations and molecular variants of the<br />
NBS1 gene in non-Hodgkin lymphoma. Genes Chromosomes Cancer. 2002 ;35(3):282-286<br />
14. Varon R, Reis A, Henze G, von Einsiedel HG, Sperling K, Seeger K.: Mutations in the Nijmegen Breakage Syndrome<br />
gene (NBS1) in childhood acute lymphoblastic leukemia (ALL). Cancer Res. 2001; 61(9):3570-3572.<br />
15. Lee JH, Paull TT.: ATM Activation by DNA Double-Strand Breaks Through the Mre11-Rad50-Nbs1 Complex. Science.<br />
2005; 308(5721):551-554.<br />
16. Frappart PO, Tong WM, Demuth I, Radovanovic I, Herceg Z, Aguzzi A, Digweed M, Wang ZQ.: An essential function<br />
for NBS1 in the prevention of ataxia and cerebellar defects. Nature Med. 2000; 11(6):538-544.<br />
17. Seemanova E, Pohanka V, Seeman P, Mišovicova N, Behunova J, Kvasnicova M, Dlholucky S, Valachova A, Cisarik<br />
F, Veghova E, Varon R, Sperling K.: Nijmegen breakage syndrome in Slovakia. Čas Lek Česk. 2004;143(8):538-541<br />
18. Lehotsky J, Melter J, Melterova K, Patrik P, Pohanka V. Inherited syndrome of chromosomal instability in Slovak<br />
<strong>po</strong>pulation and its influence on oncologic and immunologic diseases. Grant APVT No. 20-008202, 2005; Final re<strong>po</strong>rt,<br />
Martin.<br />
Received: December, 8, 2005<br />
Accepted: May, 4, 2006<br />
Acknowledgements:<br />
This work was sup<strong>po</strong>rted by grants APVT No. 20-008202 – „Inherited syndrome of chromosomal instability in Slovak<br />
<strong>po</strong>pulation and its influence on oncologic and immunologic diseases“ and VEGA No. 3380/06.
16<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
COMPARISON OF TWO METHODS FOR EVALUATION OF THE HEART<br />
RATE CONTROL IN OBESE CHILDREN<br />
1<br />
INGRID TONHAJZEROVA, 1 MICHAL JAVORKA, 1 ZUZANA TRUNKVALTEROVA,<br />
2<br />
OĽGA CHROMA, 1 ZUZANA LAZAROVA, 2 JANA JAVORKOVA, 1 KAMIL JAVORKA<br />
1<br />
Department of Physiology and 2 Clinic of Children and Adolescents, Jessenius Medical Faculty, Comenius University<br />
and University Hospital, Martin, Slovak Republic<br />
A b s t r a c t<br />
The aim of our pilot study was to compare the sensitivity of two methods – cardiovascular tests and heart rate variability<br />
(HRV) analysis – and to find the differences in the autonomic nervous system (ANS) activity regulating cardiovascular<br />
system between obese and nonobese group.<br />
Method: Twenty subjects were examined - 10 obese and 10 nonobese adolescents at the age of 12-18 years. The cardiovascular<br />
reactivity was examined using tests (deep breathing-DB, orthostatic test-OT, Valsalva manoeuvre-VM). The<br />
HRV was analyzed from 10-minute period of the rest in very low, low and high frequency bands.<br />
Results: Obese children have significantly higher body mass index, waist-hip ratio and percentage fat compared to<br />
controls. Cardiovascular tests: Obese subjects have significantly higher mean heart rate 0before DB and OT tests compared<br />
to controls. No significant differences were found in either cardiovascular test parameters. HRV analysis: Obese<br />
children have significantly decreased mean R-R interval compared to controls. Parameters - pNN50, rMSSD, logHF – were<br />
significantly lower in obese compared to nonobese group.<br />
Conclusion: We confirmed the decrease of parasympathetic activity (lower parameters of HRV analysis) and relative<br />
sympathetic dominance (higher mean heart rate before DB and OT) in obese children. The heart rate variability analysis<br />
was a more sensitive indicator of autonomic dysfunction than conventional cardiovascular tests.<br />
K e y w o r d s : obesity, autonomic nervous system, cardiovascular tests, heart rate variability, children and adolescents<br />
INTRODUCTION<br />
Obesity is an excess of the adi<strong>po</strong>se tissue accumulation and it is an im<strong>po</strong>rtant risk factor for<br />
developing chronic diseases. Although childhood obesity brings a number of additional problems<br />
- hyperinsulinaemia, <strong>po</strong>or glucose tolerance and a raised risk of type 2 diabetes, hypertension,<br />
sleep apnoea, social exclusion and depression - the greatest health problems will be seen in the<br />
next generation of adults (7, 8, 15, 17 and others).<br />
A regulatory system for maintenance of the constant energy storage likely involves complex interactions<br />
among humoral, neural, metabolic and psychological factors, and it has been suggested that<br />
the autonomic nervous system (ANS) may be central in the coordination of this system (2).<br />
Because both sympathetic and parasympathetic nervous system seem to be involved in<br />
modulating energy homeostasis, investigating the interactions between these two branches of the<br />
ANS may provide a new understanding of human obesity mechanisms (16).<br />
Cardiac function is extremely sensitive to autonomic regulatory inputs and it is therefore an<br />
attractive candidate for the evaluation of the ANS status (9). The Ewing battery of the cardiovascular<br />
tests and the heart rate variability (HRV) analysis are usually used for the cardiac autonomic<br />
neuropathy diagnosis because of their advantages – they are non-invasive, well-accepted<br />
and precise methods. Application of new mathematical tools based on nonlinear dynamics to<br />
HRV analysis provides supplementary information about systems involved in cardiovascular<br />
parameters changes (13, 14).<br />
The aim of the pilot study was to compare the sensitivity of two methods – cardiovascular<br />
tests and heart rate variability analysis – and to ascertain the differences of the heart rate<br />
chronotropic control between obese and nonobese children and adolescents.<br />
Address for corres<strong>po</strong>ndence:<br />
Ingrid Tonhajzerova, MD, PhD,Department of Physiology,<br />
Jessenius Medical Faculty, Comenius University, Mala Hora 4, 037 54 Martin Slovak Republic<br />
Phone/fax:++421-43-4131426, e-mail: tonhajzerova@jfmed.uniba.sk
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 17<br />
METHODS<br />
We examined 10 obese children and adolescents (7 girls, 3 boys) at the age of 12-18 years<br />
(mean age±SEM: 16.0±0.7 y.). Obesity was defined using reference cut-off <strong>po</strong>ints for overweight<br />
and obesity between 2-18 years (4) which are recommended by the International Obesity Task<br />
Force 2004 (15). The control group consisted of 10 healthy, gender and age matched subjects<br />
(mean age±SEM: 15.4±0.6 y.). All subjects – non-smokers - had no evidence of hypertension, cardiovascular<br />
and endocrinologic diseases, diabetes mellitus or other diseases. Children and adolescents<br />
were examined in a quiet room with standard temperature (23 o C) and minimal arousal<br />
stimuli from 8.30 to 12.00 a.m. Cardiovascular tests - in sequence: deep breathing → orthostasis<br />
→ Valsalva manoeuvre - were performed using Varia Cardio TF4 (Sima Media, Olomouc,<br />
Czech Republic). After 10 min of the rest, the subject has remained in supine <strong>po</strong>sition on the bed<br />
for next 50 min of the continual ECG recording through thoracic belt for HRV analysis.<br />
All subjects and their parents were carefully instructed about the study protocol and they<br />
gave written informed consent to participate in the study prior to examination. Subjects were<br />
instructed not to use substances influencing cardiovascular system (caffeine, alcohol) 24 h prior<br />
to examination.<br />
The study was approved by the Ethics Committee of Jessenius Medical Faculty, Comenius<br />
University.<br />
Cardiovascular tests:<br />
Deep breathing test (DB): The subject lying in a supine <strong>po</strong>sition was instructed to<br />
breathe deeply (maximally) four times in twenty seconds. Evaluated parameters: I-E – difference<br />
of the average maximal and minimal HR during deep inspirations and expirations from<br />
4 cycles, I/E - ratio of these values, CV R-R<br />
– coefficient of variation = (SD/MV)x100. Orthostatic<br />
test (OT): Active change of the body <strong>po</strong>sition was performed from the supine to standing<br />
up <strong>po</strong>sition (in 5 seconds) followed by 30 seconds lasting orthostasis. Evaluated parameters:<br />
30:15 – ratio of the length 30 th to 15 th R-R interval, RRmax/RRmin – ratio of the maximal and<br />
minimal length R-R 0interval, Brake index (BI) – (A-B)/Cx100 (A – the longest R-R interval, B<br />
– the shortest R-R interval during the first 30 seconds after standing, C – mean value of the<br />
R-R intervals before orthostasis), HRmax/HRrest – ratio of maximal heart rate during<br />
orthostasis and mean heart rate before orthostasis.<br />
Valsalva manoeuvre (VM): The subject was asked to perform Valsalva manoeuvre (an<br />
expiratory effort to mouthpiece connected to a tonometer and maintaining a pressure of 40<br />
mmHg for 15 seconds in sitting <strong>po</strong>sition). R-R intervals were recorded during the manoeuvre<br />
and for 25 seconds following release. Evaluated parameters: VR (Valsalva ratio) – ratio of the<br />
maximal HR to minimal HR, HRmax – maximal heart rate during the 1 st – 25 th second after<br />
the beginning of the expiratory effort, HRmin – minimal heart rate during the 15 th – 40 th second<br />
after reaching of the HRmax and their ratios and differences (HRmax/HRrest, HRmax-<br />
HRrest, HRmin/HRrest). Mean heart rate (HRrest) was evaluated before all tests at the rest.<br />
The analysis of heart rate variability<br />
R-R intervals were analyzed from ECG recording between the 20 th - 30 th minute of the rest.<br />
The analog output of ECG device CHIRASTAR 60 (Chirana, Slovak Republic) was transferred into<br />
PC by analog-digital conversion at sampling frequency of 500 Hz by PCL 711 data aquisition card<br />
(Advantech Co., Taiwan). R waves were detected using peak detection algorithm and the beat-tobeat<br />
R-R interval length was measured.<br />
The parameters of time domain analysis were evaluated: the mean R-R interval, standard<br />
deviation of normal R-R intervals (SDNN), the square root of the mean squared difference of the<br />
successive R-R intervals (rMSSD) and the pro<strong>po</strong>rtion of the interval differences of successive R-<br />
R intervals > 50 ms (pNN50). rMSSD and pNN50 reflect mainly parasympathetic (vagal) activity<br />
(23). Spectral analysis (fast Fourier transform) was performed on resampled (2 Hz, cubic spline)<br />
and consecutive 256 s of the R-R interval time series. The spectral <strong>po</strong>wers in frequency domain<br />
were quantified by integrating the areas under the <strong>po</strong>wer spectral density curves for the following<br />
bands: the very low frequency band (0.0156-0.04 Hz) – is much less defined; the thermoreg-
18<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
ulation, vasomotoric tone, renin-angiotensin-aldosterone system etc. are presumed physiological<br />
mechanisms, the low frequency band (0.04-0.15 Hz) – it is expressed by sympathetic and<br />
parasympathetic activity and reflecting baroreflex sensitivity (0.1 Hz), the high frequency band<br />
(0.15-0.5 Hz) is associated with parasympathetic activity (respiratory sinus arrhythmia), the total<br />
<strong>po</strong>wer (0.0156-0.5 Hz) – the sum of all spectral com<strong>po</strong>nents reflecting overall heart rate variability<br />
(1, 10, 23 and others).<br />
Anthro<strong>po</strong>metric measurements - weight, height (body mass index), circumference of waist<br />
and hip (waist-hip ratio) and percentage fat by the method based on Bioelectrical Impedance<br />
Analysis (OMRON BF 302, Japan) - were performed after the cardiovascular tests and HRV<br />
examination.<br />
Statistical analysis:<br />
All the used data are expressed as mean ± SEM. The non-Gaussian distribution of the variables<br />
was ascertained using Lilliefors test. Mann-Whitney U-test was used for statistical analysis<br />
of the parameters with non-Gaussian distribution and Student’s unpaired t-test was performed<br />
to assess statistical differences in variables with normal distribution.<br />
Because basal spectral absolute values differ greatly among individuals, the spectral <strong>po</strong>wers<br />
were then logarithmically transformed for statistical testing and Student’s unpaired t-test was<br />
used for between groups comparisons (obese vs. nonobese). The p< 0.05 was considered as significant.<br />
RESULTS<br />
Anthro<strong>po</strong>metric measurements<br />
Obese children have significantly higher body mass index (p=0.001), waist-hip ratio (p=0.011)<br />
and percentage fat (p=0.001) compared to healthy controls (Table 1).<br />
Table 1. Anthro<strong>po</strong>metric characteristics of the obese and nonobese children and adolescents.Values are expressed as<br />
mean ± SEM, significant difference is accepted p
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 19<br />
Fig. 1 Mean values of the pNN50 in obese and control<br />
group<br />
Fig. 2 Mean values of the rMSSD in obese and control<br />
group<br />
Fig. 3 Mean values of the log<br />
HF<strong>po</strong>wer in obese and control<br />
group<br />
DISCUSSION<br />
Obesity can be associated with alterations in vagosympathetic activity, the evidence of which<br />
has been described in adult humans (9, 3, 16). In most studies, the evaluation of individual com<strong>po</strong>nents<br />
of the ANS in obesity is characterized by the findings of decreased parasympathetic<br />
activity, whereas the conclusions related to sympathetic part are controversial.<br />
In obese adult people; the most studies confirmed decreased parasympathetic activity using<br />
heart rate variability analysis (25, 20). The 10% increase in body weight above initial weight<br />
resulted in the decline of the parasympathetic activity (9). On the other hand, Colak et al. (3)<br />
found normal parasympathetic activity with hy<strong>po</strong>functional sympathetic branch of the ANS<br />
using cardiovascular tests. Contrary, other authors found hyperactivity in sympathetic branch<br />
by the evaluation of blood pressure changes during handgrip test (25) or by the means of the<br />
microneurography of the muscle sympathetic nerve activity (MSNA) (6).<br />
The number of the studies concerning the relationship of the autonomic nervous system and<br />
childhood obesity is limited. Already in childhood low levels of the parasympathetic activity are<br />
associated with cardiac dysregulation in several diseases – diabetes mellitus, hypertension (11,<br />
12, 19). Nagai et al. (18) discovered lower parasympathetic and sympathetic activity using heart<br />
rate variability analysis in 42 obese children. Other studies ascertained higher sympathetic<br />
activity in obese adolescents by means of the spectral analysis of the HRV (22). Only a few studies<br />
used the cardiovascular tests for the evaluation of the heart rate reactivity in obese children.<br />
Yakinci et al. (24) referred to the dysfunction in parasympathetic activity – hy<strong>po</strong>activity in deep<br />
breathing test and hyperactivity in Valsalva manoeuvre test – in obese children at the age of 7-<br />
13 years. Despite this study we found no significant differences in heart rate res<strong>po</strong>nses to cardiovascular<br />
tests.
20<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
The mechanism underlying these changes of parasympathetic and sympathetic activities in<br />
obesity is unknown. The hy<strong>po</strong>thalamus is a regulatory centre of the „feeding and satiety“ and of<br />
the autonomic nervous system too. Therefore, the abnormalities at cellular level (determined also<br />
by genetic factors) in these centers might cause both obesity and the autonomic nervous system<br />
dysfunction (24). In the explanation of autonomic nervous system changes during obesity we<br />
have to take into consideration the metabolic consequences of the obesity (hyperinsulinemia,<br />
decreased insulin sensitivity, dyslipidemia etc.) which may be involved in the pathogenesis of<br />
impaired cardiac autonomic nerve function (21, 5).<br />
The main aim of our pilot study was to compare the sensitivity of two methods for the evaluation<br />
of the heart rate control – the cardiovascular tests and the method of heart rate variability<br />
analysis. We found no significant difference in cardiovascular tests parameters except higher<br />
resting mean heart rate before deep breathing and orthostatic tests. Parameters of the time and<br />
frequency heart rate variability analysis (mean R-R interval, rMSSD, pNN50, logHF <strong>po</strong>wer) were<br />
decreased in obese group compared to controls. The method of the heart rate variability analysis<br />
was a more sensitive indicator of the autonomic dysfunction than conventional cardiovascular<br />
tests in obese children and adolescents.<br />
REFERENCES<br />
1. Akselrod S, Gordon D, Ubel FA. Power spectrum analysis of heart fluctuation: A quantitative probe of beat-to-beat<br />
cardiovascular control. Science 1981; 213: 220-222.<br />
2. Bray GA. Autonomic and endocrine factors in the regulation of energy balance. Fed Proc 1986; 45: 1404-1410.<br />
3. Colak R, Donder E, Karaoglu A, Ayhan O, Yalniz M. Obesity and the activity of the autonomic nervous system. Turk<br />
J Med Sci 2000; 30: 173-176.<br />
4. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide:<br />
international survey. BMJ 2000; 320: 1240-1243.<br />
5. Emdin M, Gastaldelli A, Muscelli E, Macerata A, Natali A, Camastra S, Ferrannini E. Hyperinsulinemia and autonomic<br />
nervous system dysfunction in obesity. Circulation 2001; 103: 513-519.<br />
6. Grassi G, Seravalle G, Cattaneo BM, Bolla GB, Lanfranchi A, Colombo M, Giannattasio C, Brunani A, Cavagnini F,<br />
Mancia G. Sympathetic activation in obese normotensive subjects. Hypertension 1995; 25: 560-563.<br />
7. Gunnell DJ, Frankel SJ, Nanchahal K, Peters TJ, Smith GD. Childhood obesity and adult cardiovascular mortality:<br />
a 57-y follow-up study based on the Boyd Orr cohort1-3. Am J Clin Nutr 1998; 67: 1111-1118.<br />
8. Hainer V, Kunešová M, Bendlová B. Úloha genetických faktorů v etiopatogenezi obezity. Postgrad Med 2002; 4: 399-<br />
403.<br />
9. Hirsch J, Leibel RL, Mackintosh R, Aguirre A. Heart rate variability as a measure of autonomic function during<br />
weight change in humans. Am J Physiol 1991; 261 (Regulatory Integrative Comp. Physiol. 30): R1418-R1423.<br />
10. Honzíková N. Spectral analysis of circulatory rhythms. Masarykova univerzita, Brno 1992 ; 125 s.<br />
11. Javorka K, Javorková J, Petrášková M, Tonhajzerová I, Buchanec J, Chromá O. Heart rate variability and cardiovascular<br />
tests in young patients with diabetes mellitus type l. J Pediatr Endocrin Metab 1999; 12 (3): 423-431.<br />
12. Javorka K, Buchanec J, Javorková J, Buchancová J. Heart rate variability and physical fitness in children and adolescents<br />
with diabetes mellitus type 1. Int J Adolesc Med Health 2001; 13 (4): 297-309.<br />
13. Javorka M. Approximate entropy – parameter kvantifikujúci komplexitu regulácie. Čs Fysiol 2002; 51 (1): 21-27.<br />
14. Javorka M, Javorková J, Tonhajzerová I, Calkovska A, Javorka K. Heart rate variability in young patients with diabetes<br />
mellitus and healthy subjects explored by Poincaré and sequence plots. Clin Physiol Funct Imaging 2005; 25<br />
(2): 119-127.<br />
15. Lobstein T, Baur L, Uauy R for the IASO International Obesity TaskForce: Obesity in children and young people: a<br />
crisis in public health. Obes Rev 2004; 5: 4-85.<br />
16. Matsumoto T, Miyawaki C, Ue H, Kanda T, Yoshitake Y, Moritani T. Comparison of thermogenic sympathetic<br />
res<strong>po</strong>nse to food intake between obese and non-obese young women. Obes Res 2001; 9 (2): 78-85.<br />
17. McLennan J. Obesity in children. Tackling a growing problem. Aust Family Phys 2004; 33 (1/2): 33-36.<br />
18. Nagai N, Matsumoto T, Kita H, Moritani T. Autonomic nervous system activity and the state and development of obesity<br />
in Japanese school children. Obes Res 2003; 11 (1): 25-32.<br />
19. Olosová A, Javorka K, Zibolen M, Tonhajzerová I, Javorková J, Buchanec J, Petrášková M. Spektrálna analýza variability<br />
frekvencie srdca u juvenilných hypertonikov. Českoslov Pediatr 1999; 54 (7): 340-343.<br />
20. Piccirillo G, Vetta F, Viola E, Santagada E, Ronzoni S, Cacciafesta M, Marigliano V. Heart rate and blood pressure<br />
variability in obese normotensive subjects. Int J Obes 1998 ; 22: 741-750.<br />
21. Richter WO, Geiß HC, Aleksic S, Schwandt P. Cardiac autonomic nerve function and insulin sensitivity in obese subjects.<br />
Int J Obes 1996; 20: 966-969.<br />
22. Riva P, Martini G, Rabbia F, Milan A, Paglieri C, Chiandussi L, Veglio F. Obesity and autonomic function in adolescence.<br />
Clin Exp Hypertens 2001; 23 (1&2): 57-67.
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 21<br />
23. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology.<br />
Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Circulation 1996;<br />
93: 1043-1065.<br />
24. Yakinci C, Mungen B, Karabiber H, Tayfun M, Evereklioglu C. Autonomic nervous system functions in obese children.<br />
Brain Dev 2000; 22: 151-153.<br />
25. Zahorska-Markiewicz B, Kuagowska E, Kucio C, Klin M. Heart rate<br />
variability in obesity. Int J Obes 1993; 17: 21-23.<br />
Acknowledgements:<br />
This study was sup<strong>po</strong>rted by the Grant VEGA No. 1/2305/05 and the Comenius University Grant No. UK/49/2005.
22<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
EFFECTS OF VASOACTIVE DRUGS ON COCHLEAR BLOOD FLOW AFTER<br />
TRANSIENT COCHLEAR ISCHEMIA<br />
KRZYSZTOF F. MORAWSKI 1 , GRAZYNA LISOWSKA 2 , KAZIMIERZ NIEMCZYK 1 .<br />
1<br />
Department of Otolaryngology, Medical University of Warsaw, 2 Department of Otolaryngology, Medical University of<br />
Silesia, Zabrze, Poland<br />
A b s t r a c t<br />
Objectives: The aim of this study was to evaluate the pattern of cochlear blood flow (CBF) during transitional ischemia<br />
of the cochlea in non-pretreated ears and in ears pretreated by papaverine, sodium nitroprusside (SN) and mannitol.<br />
Methods: Young rabbits were used for this study. Reversible ischemic episodes within the cochlea were induced by<br />
directly compressing the internal auditory artery (IAA). Cochlear blood flow (CBF), cochlear blood volume (CBVol), and<br />
cochlear blood velocity (CBVel) were measured using a Laser-Doppler (LD) probe <strong>po</strong>sitioned at the round window (RW)<br />
niche. In test ears, prior to the IAA compressions, saline (control), mannitol, or SN were administered topically at the RW<br />
for 20-30 minutes while papaverine was delivered directly to the IAA and cochleovestibular nerve complex. Each ear<br />
underwent 1-, 3-, and 5-min IAA compressions.<br />
Results: In all ears, it was observed that a rapid reduction ranging from 50 to 75% of baseline in CBF, CBVol, and<br />
CBVel followed each IAA compression. In all cases an overshoot reaching 10% to 120% over baseline (BL) value after 30<br />
to 90 sec IAA releasing was observed. CBVel appeared to contribute most to the overshoot observed in CBF. Overshoots<br />
were greater for all three measures with longer duration of IAA compressions. In the pretreated ears all drugs changed<br />
the CBF, CBVol, and CBVel what would be the matter of consider of this presentation.<br />
Conclusions: Duration of IAA compression was found to be an im<strong>po</strong>rtant factor influencing the recovery pattern and<br />
overshoot of CBF, CBVol, and CBVel. Vasodilatants significantly changed the overshoot seen after release of the IAA compression.<br />
K e y w o r d s : cochlear blood flow, cochlear ischemia, vasoactive drugs<br />
INTRODUCTION<br />
Laser-Doppler (LD) measurements of cochlear blood flow (CBF) is one of the methods objectively<br />
reflecting the status of cochlear circulation, specifically useful when cochlear ischemia<br />
/reperfusion episodes are recorded. The LaserFlo BPM gives three outputs: volume (CBVol), velocity<br />
(CBVel), and flow - CBF. The volume parameter is defined as the mean number of Doppler<br />
events per photon. The velocity parameter is defined as the mean Doppler frequency, expressed<br />
in kHz (1). The flow parameter is the scaled product of the volume and velocity parameters, with<br />
scaling factor being equal to 60:<br />
Flow = m × f × 60 = ml x min -1 x 100g -1<br />
m – calculated blood volume<br />
f – mean Doppler frequency<br />
Monitoring of the cochlear status during reversible ischemic episodes using CBF and its contributors,<br />
i.e. cochlear blood velocity (CBVel) and cochlear blood volume (CBVol), is one of the<br />
aims of this study. Besides, different recovery models of the cochlear blood circulation following<br />
release of the internal auditory artery (IAA) blockage were described and discussed.<br />
METHODS<br />
Equipment<br />
To measure CBF, a commercial device (Vasamedics, LaserFlo BPM), with a wavelength of 780 nm<br />
and an optical <strong>po</strong>wer of 2 mW at the probe tip was used. A rigid needle sensor probe directed the<br />
Address for corres<strong>po</strong>ndence:<br />
Krzysztof Morawski, M.D., Ph.D.Department of Otolaryngology,<br />
Medical University of Warsaw, Banacha 1a Street, 02-097 Warsaw, Poland<br />
E-mail: hno@<strong>po</strong>czta.onet.pl
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 23<br />
laser beam. The sample rate for recording the CBF data was 2 <strong>po</strong>ints/s, with the on-line display<br />
consisting of a running average that was computed over a 10 s interval. The data were collected,<br />
transferred off-line, and analyzed using a commercially available spreadsheet (Microsoft Excel 2000;<br />
Microsoft Corp., Redmond, WA). The numerical values are normalized to baseline levels, however,<br />
because no meaningful absolute values could be obtained. Therefore, the baseline CBF measures<br />
were normalized to 100% and changes expressed as percent values greater or less that 100%.<br />
Subjects<br />
The protocol for the care and use of these rabbits was approved by the Institution’s Animal<br />
Care and Use Committee. Thirty three albino rabbits (3 – 6 months old), weighting between 2.5<br />
and 4 kg, were used for this study (Papaverine – 6 animals; Nipride - 6 animals; Mannitol – 5 animals;<br />
saline as a control – 11 animals). The animals were anesthetized routinely with an intramuscular<br />
injection of ketamine hydrochloride (50mg/kg) mixed with xylazine hydrochloride<br />
(10mg/kg). The anesthetized animals were placed on a feedback- controlled hearing blanket set<br />
to maintain a core body temperature of 38 o C within a standard double-walled, walk-in, sound<br />
treated chamber (Industrial Acoustics Corp., Bronx, N.Y.). After otoscopic examination to confirm<br />
normal ears, a head stabilization device was placed according to a standard procedure previously<br />
described. A level of surgical anesthesia was maintained by administration of supplemental<br />
doses of ketamine/xylazine as needed according to the evoking of an eye-blink or pain reflex.<br />
Experimental Procedures<br />
The subsequent surgical steps have been previously described by a protocol developed in this<br />
laboratory. The first surgical step used a retro-auricular approach to ex<strong>po</strong>se the cochlea and round<br />
window (RW) for placement of the laser-Doppler probe to measure CBF. Then, the middle ear was<br />
entered through the auditory bulla. After ex<strong>po</strong>sing the area with a curette, a drill fitted with a diamond<br />
burr was used to enter the middle ear between the bulla’s thick and thin <strong>po</strong>sterior walls. The<br />
cochlea was further ex<strong>po</strong>sed using either the diamond burr or rongeurs until the RW was clearly<br />
visualized (2-7). After ex<strong>po</strong>sure of the middle ear, the cerebello<strong>po</strong>ntine angle was ex<strong>po</strong>sed via a suboccipital<br />
<strong>po</strong>sterior craniotomy explained in a pre-published study. In brief, a <strong>po</strong>sterior mid-line incision<br />
was made inferior to the occipital process. Using rongeurs to remove parts of the <strong>po</strong>sterior calvarium,<br />
the cerebellum and brainstem were visualized through the operating microscope (2-8).<br />
After ex<strong>po</strong>sing this area, the laser-Doppler probe was placed into the RW niche on the side to be<br />
tested via the opening created by the previously described surgery. The probe was adjusted using<br />
a micro-manipulator so that an optimal level of CBF was detected.<br />
Papaverine Procedure<br />
The first ear in each of the first four animals to be investigated was tested with the administration<br />
of papaverine. After placing the laser-Doppler probe, PapaverineR (American Regent Laboratories,<br />
Shirley, NY) at a concentration of 30 mg/mL was applied to a piece of GelfoamR. With<br />
the use of the operating microscope, the <strong>po</strong>rus of the IAC was identified. The GelfoamR treated<br />
with papaverine was then placed on the eighth nerve complex for 20 minutes as it entered the<br />
IAC. Then, a glass microprobe was used to compress the ex<strong>po</strong>sed eighth nerve complex. The<br />
compression was maintained for 3 minutes and then released. The contralateral ear was then<br />
tested in a similar manner, using Gelfoam treated with saline instead of papaverine.<br />
Mannitol Procedure<br />
One ear in five animals to be investigated was tested after the administration of 25%-MannitolR<br />
(American Pharmaceutical Partners, Los Angeles, CA). Using insulin-syringe the RW niche<br />
was filled with mannitol at a concentration of 250 mg/mL. After 30 min, using a small suction<br />
canule, mannitol was evacuated gently. Just after RW cleaning, the LD probe was placed on the<br />
edge of the RW niche. Then, the <strong>po</strong>rus of the internal auditory canal (IAC) and the eighth nerve<br />
complex were identified. A glass microprobe was used to compress the ex<strong>po</strong>sed eighth nerve<br />
complex. The compressions were maintained for 5-min and then released. CBF were recorded
24<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
from the onset of ischemia through 40-min after release of the compression. The IAA compressions<br />
were repeated twice for a total of three 5-min compressions per ear. Five control ears were<br />
tested using saline instead of mannitol.<br />
Sodium Nitroprusside Procedure<br />
One ear in six animals to be investigated was tested after the administration of NiprideR<br />
(Roche, F) - sodium nitroprusside of 3% concentration. Nipride was administered topically using<br />
the same procedure as that for mannitol but the IAA compression lasted 3 min. Six control ears<br />
were tested with the same procedure using saline applied topically at the RW.<br />
RESULTS<br />
Saline – Control Ears<br />
Following IAA compression, LD measurements decreased rapidly and remained stable at low<br />
background levels between 10 and 25 sec. After release, CBF recovered rapidly to baseline levels<br />
within several seconds for 1-, 3-, and 5 min IAA compression and then, proceeded to exceed the<br />
baseline (i.e., overshoot) reaching a maximum approximately 40-45 sec after release for 1- and<br />
3 min IAA compression while for 5 min IAA compression a maximum was reached 87 sec after<br />
release. The maximum CBF mean value reached 218% of the pre-compression baseline levels<br />
after 5 min IAA compression, while for 1- and 3 min these values were similar and mean values<br />
were equal to 123% (Fig. 1). The comparison between CBF overshoot mean values showed that<br />
after 5 min IAA compression this value was significantly higher than after 1- and 3 min IAA compression.<br />
LD measures stabilized back down to baseline within 10-11 min following release of<br />
IAA compression after 5 min and 3 min IAA compression, although the pattern of the decrease<br />
for both cases was different. Recovery pattern after the release for 1 min IAA compression was<br />
somewhat different stabilizing around 10% above BL.<br />
Fig.1 The mean values of CBF presented as normalized data for 1-, 3-, and 5-min IAA compression recorded in control<br />
ears. ♦- IAA compression; ♦ IAA release.
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 25<br />
Saline – Papaverine – Nipride<br />
In all cases following 3 min IAA compression, LD measurements decreased rapidly and<br />
remained stable at low background levels very quickly (Fig. 2). After release, CBF recovered<br />
rapidly to baseline levels within several seconds for saline, papaverine, and Nipride, and<br />
then, proceeded to exceed the baseline reaching a maximum approximately 40-45 sec after<br />
release for saline- and papaverine ears. CBF recovery pattern for Nipride ears reached maximum<br />
value after 178 sec after release and no overshoot was observed. The maximum CBF<br />
mean value reached 148% of the pre-compression baseline levels in ears treated by papaverine<br />
while for saline 123%, and for nipride ears 112%. The comparison between CBF maximum<br />
overshoot mean values showed that after 3 min IAA compression the overshoot value<br />
in papaverine ears was significantly higher than in Nipride group (p
26<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
Fig. 3. The mean values of CBF presented as normalized data for three subsequent 5-min IAA compressions treated by<br />
mannitol.<br />
DISCUSSION<br />
Data from the present study show <strong>po</strong>st blockage CBF recovery patterns with their typical<br />
overshoots, although only for CBF. Duration of the IAA compression influences on the pattern of<br />
recovery. Basically, after 1-, and 3 min compression CBF patterns are rather similar, while after<br />
5 min compression amount of the overshoot exceeded 200% for CBF. The presence of overshoots<br />
after <strong>po</strong>st blockage is in relation to IAA wall tension, an amount of blood accumulated in IAA,<br />
and status of vessels in the cochlea. The largest overshoot occurring after 5 min compression is<br />
connected with a large amount of blood in artery reservoir in front to the compression of the IAA<br />
and the pressing of the systematic blood pressure on it. These two factors may explain why,<br />
according to earlier studies, CBVel is more flexible and characterized by overshoot, while CBVol<br />
is relatively stabile (5). Additionally, this results may suggest that the wall tension of the vessels<br />
within the cochlea is sufficient to adjust to systematic blood pressure and flow of a larger amount<br />
of blood through the cochlear vascular bed (9-11).<br />
The CBF recovery pattern in ears treated by papaverine and sodium nitroprusside are different.<br />
The greatest overshoot in papaverine treated ears after 3 min IAA compression may be the<br />
result of increasing the artery blood reservoir volume with simultaneously preserved correct vessel<br />
tension in the cochlea. Totally different administration of sodium nitroprusside - through the<br />
round window membrane – also may explain different pattern of <strong>po</strong>st blockage recovery of CBF,<br />
and other parameters- CBVel, CBVol- as the authors presented in earlier studies (5). The reduced<br />
vessel wall tension in the cochlea treated by sodium nitroprusside directly contributes to reduction<br />
of the CBVel since the same amount of blood as in the saline treated ears has to go through<br />
a larger cochlear vascular bed. In contrast to that, in papaverine ears, the cochlear vascular bed<br />
remains on the same level, while artery blood reservoir volume in front to the IAA compression<br />
is enlarged. In this way, after release of the IAA compression, enlarged amount of the blood has<br />
to go through the cochlear vascular bed directly, being the reason of CBVel overshoot with rela-
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 27<br />
tively stable CBVol (5-7). Such drugs administered topically at the RW (sodium nitroprusside) or<br />
topically on the eight nerve structure (papaverine) and in this way respectively enlarging blood<br />
vessel reservoir in the cochlea or in front to IAA compression may show and explain mechanism<br />
of dynamic changes observed in the cochlea, and then, in the future, will make easier the understanding<br />
of various cochlear blood supply pathologies (3, 12, 13, 14).<br />
Ears treated by mannitol or saline compressed three times for 5 min also showed overshoots.<br />
In general, after subsequent 5 min compressions the <strong>po</strong>st blockage overshoots were reduced<br />
after the second and third compression. And in all these cases CBVel was the main contributor<br />
to this phenomenon. The subsequent mechanical IAA compressions probably damaged somewhat<br />
or changed the properties of the IAA reducing its tension, and in this way reducing the CBF<br />
overshoot (4, 15, 16).<br />
REFERENCES<br />
1. Rendell M, Bergman T, O’Donnell G, Drobny E, Borgos J, Bonner RF. Microvascular blood flow, volume, and velocity<br />
measured by laser Doppler techniques in IDDM. Diabetes 1989; 38(7):819-24.<br />
2. Mom T, Telischi FF, Martin GK, Lonsbury-Martin BL. Measuring the cochlear blood flow and distortion-product otoacoustic<br />
emissions during reversible cochlear ischemia: a rabbit model. Hear Res 1999; 133:40-52.<br />
3. Morawski K, Telischi FF, Merchant F, Namyslowski G, Lisowska G, Lonsbury-Martin BL. Preventing internal auditory<br />
artery vasospasm using topical papaverine: an animal study. Otol Neurotol 2003; 24: 918-26.<br />
4. Morawski K, Telischi F, Merchant F, Abiy LA, Lisowska G, Namyslowski G. The Role of Mannitol in Reducing Post-<br />
Ischemic Changes in Distortion-Production Otoacoustic Emissions (DPOAEs): A Rabbit Model. Laryngoscope 2003;<br />
113(9): 1616-22.<br />
5. Morawski K, Telischi F, Abiy L, Yavuz E, Marchant F, Ozdamar O, Manns F. Effects of Vasoactive Drugs on Cochlear<br />
Blood Flow After Transient Cochlear Ischemia. Abstract Book of the 26th Annual MidWinter Research Meeting, Daytona<br />
Beach, Florida, USA February 22-27, 2003, Vol.26, p.251, Abstract No 992.<br />
6. Morawski K, Telischi F, Namyslowski G, Lisowska G, Abiy L, Yavuz E. Different Patterns of Internal Auditory Artery<br />
Vasospasm Evaluated Using Laser-Doppler Probe: A Rabbit Model. XVIII Biennial Sym<strong>po</strong>sium IERASG Puerto de la<br />
Cruz – Tenerife – Canary Islands, Spain 8-12 June, 2003. Abstract Book, P-171.<br />
7. Morawski K, Telischi F, Niemczyk K, Lisowska G, Merchant F. Assessment of Sodium Nitroprusside administered<br />
topically at the round window niche in preventing vasospasm of the cochlear vasculature and its effect on cochlear<br />
activity. An animal model. Abstract Book of 12th International Sym<strong>po</strong>sium on Audiological Medicine, Lyon, France,<br />
6-9 March 2005, p.16<br />
8. Widick MP, Telischi FF, Lonsbury-Martin BL, Stagner BB. Early effects of cerebello<strong>po</strong>ntine angle compression on rabbit<br />
distortion-product otoacoustic emissions: A model for monitoring cochlear function during acoustic neuroma surgery.<br />
Otolaryngol Head Neck Surg 1994; 111:407-416.<br />
9. Greenberg S, Curro FA, Tanaka TP. Regulation of vascular smooth muscle of the microcirculation. In: NA Mortillaro<br />
(Ed), The Physiology and Pharmacology of the Microcirculation, Vol 1 Harcourt Brace Jovanovich, New York 1983.<br />
10. Carlisle L, Aberdeen J, Forge A, Burnstock G. Neural basis for regulation of cochlear blood flow: peptidergic and<br />
adrenergic innervation of the spilar modiolar artery of the guinea pig. Hear Res 1990; 43:107-113.<br />
11. Miller JM, Ren TY, Nuttal AL. Studies of inner ear blood flow in animals and human beings. Otolaryngol Head Neck<br />
Surg 1995; 112: 101-113.<br />
12. Ohlsen KA, Didier A, Baldwin D, Miller JM, Nuttall AL, Hultcrantz E. Cochlear blood flow in res<strong>po</strong>nse to dilating<br />
agents. Hear Res 1992; 58: 19-25.<br />
13. Kassell NF, Helm GH, Simmons N, Phillips CD, Cail WS. Treatment of cerebral vasospasm with intra-arterial<br />
papaverine. J Neurosurg 1992; 77:848-852.<br />
14. Nakashima T, Nuttall AL, Miller JM. Effects of vasodilating agents on cochlear blood flow in mice. Hear Res 1994;<br />
80: 241-246.<br />
15. Quirk WS, Dengerink HA, Bademian MJ, Wright JW. Mannitol and dextran increase cochlear blood flow in normotensive<br />
and s<strong>po</strong>ntaneously hypertensive rats. Acta Otolaryngol 1990;109(5-6): 383-8.<br />
16. Baldwin DL, Ohlsen KA, Miller JM, Nuttall AL. Cochlear blood flow and microvascular resistance changes in res<strong>po</strong>nse<br />
to hypertonic glycerol, urea, and mannitol infusions. Ann Otol Rhinol Laryngol 1992;101(2 Pt 1):168-75.<br />
Received: February, 2, 2006<br />
Accepted: April, 3, 2006
28<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
IS THE HYGIENIC DISINFECTION OF HANDS WITH WATERLESS ALCOHOL<br />
DISINFECTANT CURRENTLY THE BEST WAY OF HAND-HYGIENE?<br />
MÁRIA ŠTEFKOVIČOVÁ 1 , HENRIETA HUDEČKOVÁ 2 , TIBOR BAŠKA 2 , ŠTEFAN STRAKA 2<br />
1<br />
Regional Office of Public Health, Trenčín, Slovakia, 2 Institute of Public Health, Comenius University,<br />
Jessenius Faculty of Medicine, Martin, Slovak Republic<br />
A b s t r a c t<br />
Introduction: The effects of the two officially approved procedures of hand disinfection – hygienic hand washing<br />
using disinfectant soap (HHW), and hand disinfection by waterless alcohol disinfectant (HHD), on transient hand microflora<br />
of artificially contaminated hands were tested.<br />
Methods: The study involved 20 volunteers, female assistants of hygiene and hospital nurses. For artificial contamination<br />
the testing strains of Staphylococcus aureus and Pseudomonas aeruginosa, within the range 10 7 CFU/ml -1<br />
were used. For quantitative testing of residual bacteria on the hands after HHW and HHD, the fingerprint contact method<br />
on solid culture medium was used (AHEM, Annex No. 7, State Health Institute, Prague, 1992).<br />
Results: Both methods have been proved effective in reducing transient hand microflora. The reduction after HHW<br />
was in average 35-49.5 CFU/petri dish, after HHD the reduction was more pronounced – 0.3-1.0 CFU/petri dish.<br />
Discussion and conclusions: Hygienic hand disinfection with waterless alcohol disinfectant was proved to be effective<br />
and can be recommended for routine use in nursing process in cases where hands are not visibly soiled and the<br />
reduction of hand microflora is desired.<br />
K e y w o r d s : hand hygiene, hospital infections, prevention of preventing transmission of infection<br />
INTRODUCTION<br />
Hand washing is considered as the cheapest and simplest way of preventing transmission of<br />
infection. However, compliance with hand hygiene (HH) is currently in some hospitals rather low.<br />
Several countries have adopted the HH guidelines in hospital setting. Hand washing, according<br />
to these rules, would be performed by less than 50% of nurses, and even less physicians (9,10).<br />
Thus the reduction of incidence of hospital infections transmitted by hands is hampered. Moreover,<br />
negligence in this field promotes colonization of hands of health workers with pathogens<br />
and their spread to their own families and their respective communities. In context of the current<br />
increase of resistance of pathogenic microorganisms <strong>po</strong>ses an im<strong>po</strong>rtant problem (2,4,9).<br />
New knowledge needs gradually a new terminology. Hand washing with common soap is<br />
called “common hand washing” (CHW). For hand washing using disinfectant soap the term<br />
“hygienic hand washing” (HHW) is used. In recent years more and more emphasised is the high<br />
efficacy of the waterless hand disinfection called technically as “hygienic hand disinfection”<br />
(HHD) based on rubbing hands with certain amount waterless alcohol disinfectants. HHD acts<br />
vary rapidly in a course of 20-30 seconds, it does not remove lipids from the skin, contains softening<br />
agents which provide care of the skin. This form of disinfection is significantly better<br />
accepted by health workers than HHW. The aim of HHW and HHD is to eliminate the transient<br />
microflora of hands and of HHW also in visibly soiled hands (4,5,11,12,13).<br />
CHW removes lipids from hands, dries and causes irritations to persons with habitually dry<br />
skin. Washing out the layers of protective lipids opens deeper layers of the skin for pathogenic<br />
microorganisms and chemical substances thus creating conditions for allergisation (3,6). On the<br />
other hand, we evidence an enormous increase of antibiotic resistance of many hospital<br />
pathogens, the world-wide spread of MRSA (methicillin-resistant Staphylococcus aureus) and<br />
VRE (vancomycine-resistant enterococci), more and more frequent are hospital diarrhoeas<br />
caused by Clostridium difficile. Recently emerges also the problems of liquidation of bacterial<br />
s<strong>po</strong>res of hands of health workers in case of bioterrorism.<br />
Address for corres<strong>po</strong>ndence:<br />
Mária Štefkovičová,MD, MPH. Regional Office of Public Health, Nemocničná 4, 911 01 Trenčín, Slovak Republic<br />
Phone: 032/6509521, e-mail:stefkovicova@ruvztn.sk
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 29<br />
Currently, when we are at the threshold of epidemic of allergies, we feel the need to reassess<br />
the existing procedures, to develop new ones, excepting the need of quick and large scale effect<br />
at the low rate of irritation and allergisation. This is one of the main ways to he safety of patients<br />
and health workers in modern hospitals. Implication of these measures in practice is mostly<br />
slow, complicated and long-term. Education in this field should be sustained and associated<br />
with practical training of hand disinfection.<br />
Aware of the above facts, we tried to verify the literary data that, if hands are not visibly soiled,<br />
the best way is to use the waterless alcohol disinfectants without the preceding hand washing.<br />
As the basic reasons here are considered the higher velocity of the effect, shorter ex<strong>po</strong>sure time<br />
to the disinfectant, reduction of irritation effect and elimination of work with <strong>po</strong>orly dried hands.<br />
Moist hands can transfer microorganisms much easier than dry ones.<br />
METHODS<br />
Our study involved 20 volunteers, female hygiene assistants and hospital nurses, participating<br />
in education of health workers and patients on safety precautions against hospital infections.<br />
These performed the CHW and then dried their hands using the dis<strong>po</strong>sable paper towel. Then<br />
fingerprints of their right hand fingers were made on blood agar. Subsequently 0.05 ml of the 16-<br />
hour suspension of Staphylococcus aureus culture of the density of 10 7 CFU/ml (CFU – colonyforming<br />
units) was applied to their hands and left to dry. After drying another control fingerprint<br />
was made. The half of the volunteers used HHD (hand hygiene disinfection) with waterless disinfectant<br />
(3 ml/30 sec.), and the other half washed the hands with disinfectant soap containing<br />
0.05% chlorhexidine (3 ml/2 min.) (hygienic hand washing - HHW). After drying their hands<br />
another fingerprint as made. Standard methods and standard trains of Staphyloccus aureus<br />
were used (1). Culture was made in thermostat in 37°C/24h. The same collection was performed<br />
with a collection strain of Pseudomonas aeruginosa (1). The effect of HHD on transient microflora<br />
and resident microflora were tested.<br />
RESULTS<br />
CHW did not result in total elimination of microflora from the hands of volunteers. We found<br />
on them averagely 78.8 – 151.2 CFU/petri dish. Both methods of hygienic disinfection of hands<br />
showed excellent results on the flora used for artificial contamination of hands. Both methods<br />
reduced also resident microflora of hands, however HHW less profoundly. HHD using hand-rub<br />
with waterless alcohol disinfectant resulted in rapid reduction of hand microflora, averagely<br />
down to 0.3-1.0 CFU, while HHW reduced it only averagely to 35.0-49.5 CFU. The most im<strong>po</strong>rtant<br />
results are shown in Tab. and Fig 1.<br />
Table 1 Evaluation of the effects of HHD and HHW<br />
Contaminating agent<br />
Average number of CFU/petri dish<br />
After<br />
After HHD<br />
After<br />
After HHW<br />
contamination<br />
(n=10)*<br />
contamination<br />
(n=10)**<br />
(n=10)<br />
> 300<br />
(n=10)<br />
Staphylococcus<br />
aureus<br />
0,3<br />
> 300<br />
35<br />
Pseudomonas<br />
aeruginosa<br />
> 300<br />
1<br />
> 300<br />
49.5<br />
* HHD – 3 ml of alcohol containing disinfectant rubbed in hands until complete eva<strong>po</strong>ration<br />
** HHW – hand washing with disinfectant soap – 3 ml/1 minute
30<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
300<br />
Average number of CFU<br />
250<br />
200<br />
150<br />
100<br />
50<br />
0<br />
After<br />
After HHD After HHD<br />
After<br />
contamination<br />
Staphylococcus<br />
aureus<br />
contamination<br />
Pseudomonas<br />
aeruginosa<br />
After HHW<br />
After<br />
After<br />
After HHW<br />
contamination<br />
Staphylococcus<br />
aureus<br />
contamination<br />
Pseudomonas<br />
aeruginosa<br />
Fig.1 Evaluation of the effects of HHD and HHW<br />
DISCUSSION<br />
Adequately accomplished hand disinfection decreases the amount of transient flora (mostly<br />
of pathogenic microorganisms on the hands of health workers. It can be assumed, that paralelly<br />
the incidence of hospital infections is decreased. CDC (Centers for Diseases Control and<br />
Prevention, Atlanta, USA) and other professional organisations recommend hand disinfection as<br />
the key tool of their reduction. However, averagely only about 40% of health workers perform it<br />
in their patient care adequately.<br />
Most of guidelines dealing with hand hygiene in their effort to eliminate their irritative and<br />
allergising effect on the skin recommend disinfection of hands with alcohol disinfectants (HHD).<br />
The original traditional disinfection of hands uses disinfectants in mixture with detergents and<br />
water (HHW). The effects of both methods were tested in several studies using different ways and<br />
with different results (4,5,11,13).<br />
The essence of our trial was to compare the effects of both methods (HHW and HHD) used in<br />
routine nursing care, after artificial contamination of hands of the volunteers. We observed good<br />
results in both methods, however, our study proved that HHD is superior to HHW. Reduction of<br />
CFU in HHD was averagely by one logarithmic progression then in hygienic hand washing. Our<br />
results are consistent with results of several studies using artificial contamination with various<br />
microorganisms (including MRSA, VRE, Acinetobacter baumannii) and they confirmed that HHD<br />
is more effective than HHW or CHW (4,5,11,13).<br />
Main factors of low compliance of high quality of washing and disinfection of hands in healthcare<br />
practice divided Pittet (9,10) into three main groups: general, personal and psychological.<br />
To the general risk factors affecting compliance with the recommended rules of the hand<br />
hygiene (HH) in health workers belong: professional level – physicians comply with HH principles<br />
less than nurses, males less than females, and the least of all the workers of intensive care units.<br />
Since their permanent work in risk reduces their alertness. The recommended principles are less<br />
followed during work days than during weekends. If the health workers are wearing gloves, they<br />
feel more safe and transmit infections often because they do not change the gloves. In risk wards<br />
with high demands of frequent hand washing (HW) personnel feels that the recommendations
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1 31<br />
cannot be physically implemented, and thus they neglect HW even more.<br />
To personal reasons affecting compliance of health workers with the recommended rules of the<br />
HW belong first of all the feeling of dryness and irritation of the skin, lack or difficult to reach wash<br />
basins, lack of soaps and paper hand towels, time pressure, lack of personnel, congested wards,<br />
and situations when patients need urgent help. The personnel may feel that frequently repeated<br />
hand washing disturbs communication and worsens patient-health worker relations. An im<strong>po</strong>rtant<br />
factor is also lack of protocol, rules, guidelines, for HH procedures, absenting <strong>po</strong>sitive examples<br />
from the colleagues and superiors, and general scepticism in this field. Even if guidelines are at<br />
hand, many health workers do not agree with them, mainly because of the lack of information<br />
about he scientific background and on the impact of HH on the transmission of infection.<br />
Psychological reasons, emotional barriers of HH non-compliance: health workers are not<br />
adequately motivated, model examples are missing, and they feel that HH is not the priority of<br />
the hospital ward. Generally, they consider it less im<strong>po</strong>rtant since in most hospitals they are no<br />
sanctions for breaching the rules of HH.<br />
Most im<strong>po</strong>rtant places belong to cognitive factors. Opinions, feelings and attitudes of health<br />
workers are similarly im<strong>po</strong>rtant as the knowledge on technique of HH or access to the tools. Then<br />
there comes the question of motivation, existence of <strong>po</strong>sitive or negative examples, and social<br />
pressure from the side of management, patients, and general public (8,10).<br />
Lack of knowledge and adequate educational programs are main stumbling blocks of higher<br />
motivation of health workers in implementing high-quality hygiene. From that follows, that if<br />
success has to be expected in implementing of appropriate procedures in HH we should use<br />
modern approaches, but also up-to-date education in those problems, involving not only common<br />
lecturing but also practical demonstration and training.<br />
On the basis of our knowledge and experiences we are inclined to adapt to the recommendations<br />
of CDC and several European countries on preferential use of HHD with waterless alcohol<br />
disinfectants and for HW the use of HHW (4,5,10,13).<br />
CHW using common soap and water is necessary to carry out at the entry to the ward and<br />
when leaving it, and in all cases of visibly soiled hands. During nursing process hands can be<br />
often optically clean but they are invisibly contaminated with pathogenic microorganisms from<br />
the environment. Therefore, prior to all invasive interventions, after handling biological material,<br />
and before any handling of immunocompromised patients pathogenic microorganisms that can<br />
be present on the skin of hands, should be killed (the so-called transient microflora of the skin).<br />
This is the case for using HHD. In case that the hands during nursing process are visibly soiled<br />
with biological or other material, and microbial contamination is assumed, HHW using disinfectant<br />
soap and warm tap water should be used.<br />
Beside education aimed to promote compliance of health workers with HH, the material supply<br />
of the necessary means for washing and disinfection of hands should be improved but mainly<br />
in multimode project of education in this field with adequate motivation and practical training<br />
should be implemented.<br />
CONCLUSIONS<br />
Our study has proved the published thesis that disinfection of hands using waterless alcohol<br />
disinfectants could be more effective than the traditional disinfection of hands with disinfection<br />
soap and water. It takes shorter time, the alcohol acts more promptly and the skin irritation<br />
occurs less frequently. This can be also the necessary motivation to better compliance of health<br />
workers with hand hygiene.<br />
We have confirmed the simple and instructional way of education in which the volunteers<br />
trained the adequate HHD and the same time the effect of CHW and HHW using the fingerprint<br />
method. They are now ready to apply their experiences in their work and nursing process and<br />
also in governmental health inspection in prevention of hospital infections and nosocomial infections<br />
other health facilities.
32<br />
A C T A M E D I C A M A R T I N I A N A 2 0 0 6 6/1<br />
REFERENCES<br />
1. AHEM, příloha č.7/1992. Vybrané mikrobiologické metody <strong>po</strong>užívané při prevenci a výskytu nemocničních nákaz.<br />
SZÚ Praha. 1992; s.49-52.<br />
2. Boyce JM: It is time for action: improving hand hygiene in hospitals. Ann Intern Med 1999;130:153–5.<br />
3. Boyce JM, Kelliher S, Vallande N: Skin irritation and dryness associated with two hand-hygiene regimens: soap-andwater<br />
handwashing versus hand antisepsis with an alcoholic hand gel. Infect Control Hosp Epidemiol<br />
2000;21:442–8.<br />
4. Boyce JM, Pittet D: Guideline for hand hygiene in healthcare settings: recommendations of the Healthcare Infection<br />
Control Practices Advisory Committee and HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Infect Control<br />
Hosp Epidemiol 2002;23(suppl):S3-S40.<br />
5. Girou E, Loyeau S, Legrand P, Oppein F, Brun-Buisson Ch: Efficacy of handrubbing with alcohol based solution versus<br />
standard handwashing with antiseptic soap: randomised clinical trial. BMJ 2002;325(7360):362.<br />
6. Hrubiško M: Alergológia Martin: Osveta; 2003,519s.<br />
7. Kampf G, Loffler H: Dermatological aspects of a succesful introduction and continuation of alkohol-based hand rubs<br />
for hygienic hand disinfection. J Hosp Infect. 2003;55(1):1-7.<br />
8. Kelčíková S: Význam kvalitnej profesionálnej prípravy sestier v problematike hygieny rúk. Nozokomiálne nákazy<br />
2003;4:36-44.<br />
9. Pittet D, Simon A, Hugonnet S, Pessoa-Silva CL, Sauvan V, Perneger TV: Hand hygiene among physicians: performance,<br />
beliefs and perceptions. Ann Intern Med. 2004;141(1):1-8.<br />
10. Pittet D: Improving Adherence to Hand Hygiene Practice: A multidisciplinary Approach. Emerg Inf Dis 2001;7(2):234-<br />
240.<br />
11. Rotter M: Arguments for alkoholic hand disinfection. J Hosp Infect. 2001;48 Suppl A:S4-8.<br />
12. Rutala W.A: APIC guideline for selection and use of disinfectants. Am J Infect Control 1996;24:313-42.<br />
13. Sickbert-Bennett EE, Weber DJ, Gergen-Teague MF, Sobsey MD, Samsa GP, Rutala WA: Comparative efficacy of<br />
hand hygiene agents in the reduction of bacteria and viruses. Am J Infect Control. 2005 Mar;33(2):67-77.<br />
Received: October, 29, 2005<br />
Accepted: March, 27, 2006