Urinary Incontinence in the Elderly Population
Urinary Incontinence in the Elderly Population
Urinary Incontinence in the Elderly Population

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Ur<strong>in</strong>ary</strong> <strong>Incont<strong>in</strong>ence</strong><br />
<strong>the</strong> <strong>Elderly</strong> <strong>Population</strong><br />
Dannyl S. CHurx,r, M.D., KsvIr C. Fl-n,rnnc, M.D., Manv P. BvnNs, M.D., JoNnru,tN M. EvnNs, M.D.,<br />
,lxt KaRnN L. ANnnews, M.D.<br />
. Ob.iective: To describe <strong>the</strong> causes, evaluation, and<br />
management of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence <strong>in</strong> <strong>the</strong> elderly<br />
population.<br />
. Design: We reviewed pert<strong>in</strong>ent articles <strong>in</strong> <strong>the</strong><br />
medical literature and summarized <strong>the</strong> types of <strong>in</strong>cont<strong>in</strong>ence<br />
and contribut<strong>in</strong>g factors.<br />
o Results: <strong>Ur<strong>in</strong>ary</strong> <strong>in</strong>cont<strong>in</strong>ence is common <strong>in</strong> elderly<br />
patients and often has a major role <strong>in</strong> determ<strong>in</strong><strong>in</strong>g<br />
whe<strong>the</strong>r a person can rema<strong>in</strong> <strong>in</strong>dependent <strong>in</strong> <strong>the</strong><br />
cornmunit-y or requires nurs<strong>in</strong>g home placement. <strong>Ur<strong>in</strong>ary</strong><br />
<strong>in</strong>cont<strong>in</strong>ence is not a s<strong>in</strong>gle entity but ra<strong>the</strong>r<br />
several different conditions, each with specific symptoms,<br />
f<strong>in</strong>d<strong>in</strong>gs on exam<strong>in</strong>ation, and recommended<br />
treatment. Thus, accurate classification is important<br />
for appropriate management. Because of <strong>the</strong> com-<br />
plexity of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence, many physicians are<br />
uncomfortable with undertak<strong>in</strong>g assessment and<br />
treatment. Hence, many patients are not asked about<br />
<strong>in</strong>cont<strong>in</strong>ence, and <strong>the</strong> condition rema<strong>in</strong>s untreated<br />
and often considered a natural consequence of <strong>the</strong><br />
ag<strong>in</strong>g process. <strong>Ur<strong>in</strong>ary</strong> <strong>in</strong>cont<strong>in</strong>ence can be treated<br />
and ei<strong>the</strong>r cured or alleviated with treatment.<br />
c Conclusion: <strong>Elderly</strong> patients should be asked<br />
about symptoms of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence because appropriate<br />
assessment and treatment can usually provide<br />
relief.<br />
(Mayo Cl<strong>in</strong> Proc 1996; 7I:93-I0l)<br />
BPH = benign prostalic hyperplasia; UI = ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence<br />
t<br />
I<br />
II<br />
t<br />
<strong>Ur<strong>in</strong>ary</strong> <strong>in</strong>cont<strong>in</strong>ence (UI) is a common but poorly understood<br />
problem <strong>in</strong> <strong>the</strong> elderly population.r An estimated l57o breakdown or pressure sores. The social consequences <strong>in</strong>-<br />
Ul can result <strong>in</strong> sk<strong>in</strong> irritation and can contribute to sk<strong>in</strong><br />
of community-dwell<strong>in</strong>g elderly persons and 50Vo of <strong>in</strong>stitutionalized<br />
elderly persons have severe ur<strong>in</strong>ary <strong>in</strong>conti-<br />
leave <strong>the</strong>ir homes.r" Absorbent undergarments may reduce<br />
clude guilt and isolation; some elderly persons are afraid to<br />
nence.2.s As <strong>the</strong> degree of functional dependence <strong>in</strong>creases, this fear but are expensive and can delay evaluatton.<br />
<strong>the</strong> frequency of <strong>in</strong>cont<strong>in</strong>ence <strong>in</strong>c-reases<br />
well. The prevalence<br />
of <strong>in</strong>cont<strong>in</strong>ence may be appreciably underestimatedtures and evaluation of UI and discuss management issues.<br />
In this article, we will review <strong>the</strong> pathophysiologic fea-<br />
because physicians rarely ask patients about <strong>the</strong> problem, Older adults need to be assured that, for most patients, diagnosis<br />
and treatment options are <strong>in</strong>cxpensive. non<strong>in</strong>vasivc.<br />
and patients seldom <strong>in</strong>itiate discussions about <strong>in</strong>cont<strong>in</strong>ence<br />
with <strong>the</strong>ir physician.6 Older patients may assume that UI is a and successful.<br />
normal consequence of ag<strong>in</strong>g. Some patients may be embarrassed<br />
by <strong>the</strong>ir <strong>in</strong>cont<strong>in</strong>ence or may fear <strong>in</strong>vasive test<strong>in</strong>g and URINARY ANATOMIC AND<br />
thus avoid evaluation.<br />
PHYSIOLOGIC FEATURES<br />
UI cornmonly results <strong>in</strong> medical, social. and economic For a better understand<strong>in</strong>g of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence <strong>in</strong> elderly<br />
consequences.Ts <strong>Incont<strong>in</strong>ence</strong> is a common reason for <strong>in</strong>stifutionalization<br />
among elderly persons. The care of <strong>in</strong>contiologic<br />
changes that result from ag<strong>in</strong>g." The ur<strong>in</strong>ary bladder<br />
persons, one needs to appreciate <strong>the</strong> anatomic and phys<strong>in</strong>ent<br />
nurs<strong>in</strong>g home residents is considerably more expensive is a musculareservoir with two functions. When <strong>the</strong> muscular<br />
wall (detrusor) relaxes. ur<strong>in</strong>e stora,ee results: when it<br />
than of cont<strong>in</strong>ent residents and necessitates more nurs<strong>in</strong>g<br />
time and tiequent l<strong>in</strong>en and cloth<strong>in</strong>g changes.e<br />
contracts, micturition occurs. The wall of <strong>the</strong> bladder is<br />
composed of <strong>in</strong>terlac<strong>in</strong>g bundles of smooth muscle, which<br />
allows <strong>the</strong> detrusor to expand and contract and <strong>the</strong>reby facilitate<br />
both ur<strong>in</strong>e storage and empty<strong>in</strong>g.<br />
Frotn <strong>the</strong> Section of Geriatrics (D.S.C.. K.C.F.. J.M.E.). Department of<br />
Obstetrics trics and Gyncco logy t M. P.E. ;. and Department of Phys ical Medic <strong>in</strong>e<br />
Sensory stretch receptors located with<strong>in</strong> <strong>the</strong> bladder wall<br />
and Rehabrlitarion<br />
Rehatl (K.t-.A.). MavoCl<strong>in</strong>ic Rochester. Rochester. M<strong>in</strong>nesota.<br />
help to assess <strong>the</strong> degree of bladder fullness. This <strong>in</strong>forma-<br />
Individual<br />
repr<strong>in</strong>ts of this arlicle are nor available. The entire Symposium<br />
on<br />
ln Ceriatri.r Oeriatr<br />
tion is transrnitted up <strong>the</strong> sp<strong>in</strong>al cord through <strong>the</strong> sp<strong>in</strong>othalamic<br />
tracts to <strong>the</strong> central nervous system. The<br />
will be availablc for purchase as a bound booklet from <strong>the</strong><br />
Proceeditltu,<br />
Proceed<strong>in</strong><br />
c,,.u[i,"^ ofi:i.c ar a lor., drre<br />
bra<strong>in</strong><br />
Moyo MoYo ctiu Cti, P rtt 1996..7 I :9-1- I 0I<br />
@ 1996 Maltt Foundattort for ltledit'al Eclttcrttiott attd Reseurrh
I<br />
94 URINARY INCONTINENCE IN ELDERLY PERSONS Mayo Cl<strong>in</strong> Proc, January 1996' Vol 7l<br />
sends <strong>in</strong>hibitory signals when detrusor relaxation is desired<br />
and excitatory signals when detrusor conffaction is desired.<br />
This <strong>in</strong>formation from <strong>the</strong> bra<strong>in</strong> is transmitted down <strong>the</strong><br />
sp<strong>in</strong>al cord to <strong>the</strong> ur<strong>in</strong>ary bladder through <strong>the</strong> dorsal columns<br />
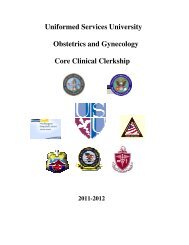
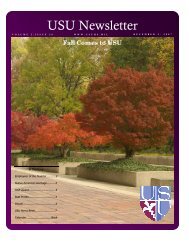
and corticosp<strong>in</strong>al tracts. The bladder has somatic, parasympa<strong>the</strong>tic,<br />
and sympa<strong>the</strong>lic <strong>in</strong>nervation (Fig. 1).<br />
The pudendal nerve is <strong>the</strong> somatic component of bladder<br />
<strong>in</strong>nervation and <strong>in</strong>nervates <strong>the</strong> external sph<strong>in</strong>cter. When<br />
stimulated, it produces contraction of <strong>the</strong> extemal urethral<br />
sph<strong>in</strong>cter. The extemal sph<strong>in</strong>cter has an <strong>in</strong>frequent role <strong>in</strong><br />
ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g cont<strong>in</strong>ence because it is able to rema<strong>in</strong> tightly<br />
contracted for only a brief period. This sph<strong>in</strong>cter normally<br />
contracts dur<strong>in</strong>g transient <strong>in</strong>creases <strong>in</strong> <strong>in</strong>tra-abdom<strong>in</strong>al pressure,<br />
such as occur with cough<strong>in</strong>g, sneez<strong>in</strong>g, and laugh<strong>in</strong>g'<br />
The parasympa<strong>the</strong>tic nerve fibers arise from <strong>the</strong> second<br />
through <strong>the</strong> fourth segments of <strong>the</strong> sacral sp<strong>in</strong>al cord and<br />
<strong>in</strong>nervate <strong>the</strong> detrusor muscle. Stimulation occurs when<br />
micturition is desired. When stimulated, <strong>the</strong> detrusor contracts;<br />
<strong>the</strong> result is <strong>in</strong>creased <strong>in</strong>travesicular pressure.<br />
The <strong>in</strong>temal ur<strong>in</strong>ary sph<strong>in</strong>cter is <strong>in</strong>nervated by <strong>the</strong> sympa<strong>the</strong>tic<br />
nervous system. These nerves orig<strong>in</strong>ate from <strong>the</strong><br />
lower thoracic and upper lumbar segments of <strong>the</strong> sp<strong>in</strong>al cord-<br />
When <strong>the</strong>se nerves are stimulated, <strong>the</strong> <strong>in</strong>temal sph<strong>in</strong>cter<br />
relaxes.<br />
The physiologic details of micturition are complex; however,<br />
a basic understand<strong>in</strong>g is necessary to appreciate <strong>the</strong><br />
causes and treatment of <strong>in</strong>cont<strong>in</strong>ehce.r2 As ur<strong>in</strong>e fills <strong>the</strong><br />
bladder through <strong>the</strong> ureters, <strong>the</strong> detrusor stretches and allows<br />
<strong>the</strong> bladder to expand. As <strong>the</strong> bladder fills, stretch receptors<br />
with<strong>in</strong> <strong>the</strong> bladder wall are stimulated, and <strong>the</strong> bra<strong>in</strong> is given<br />
<strong>in</strong>formation about <strong>the</strong> amount of ur<strong>in</strong>e with<strong>in</strong> <strong>the</strong> bladder.<br />
Approximately 300 mL of ur<strong>in</strong>e must be <strong>in</strong> <strong>the</strong> bladder<br />
before <strong>the</strong> <strong>in</strong>travesical pressure <strong>in</strong>creases enough for <strong>the</strong><br />
bra<strong>in</strong> to recognize a sense of bladder fullness. With low<br />
bladder volumes, <strong>the</strong> sympa<strong>the</strong>tic nervous system is stimulated<br />
and <strong>the</strong> parasympa<strong>the</strong>tic system is <strong>in</strong>hibited; thus, <strong>the</strong><br />
<strong>in</strong>temal sph<strong>in</strong>cter contracts and <strong>the</strong> detrusor relaxes. When<br />
<strong>the</strong> bladder is full and micturition is desired, <strong>the</strong> <strong>in</strong>hibitory<br />
signals from <strong>the</strong> bra<strong>in</strong> are replaced by impulses that stimulate<br />
<strong>the</strong> parasympa<strong>the</strong>tic system (and result <strong>in</strong> detrusor contraction)<br />
and that <strong>in</strong>hibit <strong>the</strong> sympa<strong>the</strong>tic system (and cause<br />
<strong>in</strong>temal sph<strong>in</strong>cter relaxation). The <strong>in</strong>travesical pressure <strong>the</strong>n<br />
<strong>in</strong>creases to a po<strong>in</strong>t at which it exceeds <strong>the</strong> resistance with<strong>in</strong><br />
<strong>the</strong> urethra. and ur<strong>in</strong>e flows out of <strong>the</strong> bladder.<br />
Once <strong>the</strong> bladder has emptied, <strong>the</strong> bra<strong>in</strong> aga<strong>in</strong> sends<br />
impulses that result <strong>in</strong> parasympa<strong>the</strong>tic <strong>in</strong>hibition and sympa<strong>the</strong>tic<br />
stimulation; hence, detrusor relaxation and <strong>in</strong>temal<br />
sph<strong>in</strong>cter contraction occur. The ur<strong>in</strong>ary bladder is aga<strong>in</strong><br />
ready to be filled with ur<strong>in</strong>e.<br />
CAUSES OF INCONTINENCE<br />
Although <strong>the</strong> anatomic and physiologic changes <strong>in</strong> <strong>the</strong> ur<strong>in</strong>ary<br />
tract that result from normal ag<strong>in</strong>g do not cause UI, <strong>the</strong>y<br />
do create a situation that allows <strong>in</strong>cont<strong>in</strong>ence to occur more<br />
o oo<br />
o<br />
C)<br />
o<br />
Sympa<strong>the</strong>tic<br />
nerves<br />
ParasymPa<strong>the</strong>tic<br />
nervgs<br />
Chol<strong>in</strong>ergic<br />
receptors<br />
Beta-adrenergic<br />
receptors<br />
Detrusor<br />
muscle<br />
Alpha-adrenergic<br />
receptors<br />
Somatic (pudendal) nerve<br />
External sph<strong>in</strong>cter<br />
Fig. 1. Diagram show<strong>in</strong>g <strong>in</strong>nervation of ur<strong>in</strong>ary bladder.
Mayo Cl<strong>in</strong> Proc,.lanuary 1996' Vol 7l URINARY INCONTINENCE IN ELDERLY PERSONS 95<br />
:<br />
I<br />
i<br />
I<br />
L-<br />
easily. Advanc<strong>in</strong>g age is associated with decreased size of veal anatomic abnormalities (for example, uter<strong>in</strong>e prolapse<br />
<strong>the</strong> ur<strong>in</strong>ary bladder and decreased bladder volume: <strong>the</strong>refore, or fecal impaction) or evidence of neurologic disease. The<br />
more frequent bladder empty<strong>in</strong>g (ur<strong>in</strong>ary frequency) is common<br />
<strong>in</strong> <strong>the</strong> geriatric population. Many elderly persons expe-<br />
with BPH. Many patients will describe both obstructive<br />
cl<strong>in</strong>ician should carefully assess <strong>the</strong> symptoms of patients<br />
rience early detrusor contractions, even at low bladder volumes,<br />
and have difficulty suppress<strong>in</strong>g such contracrions. der empty<strong>in</strong>g) from <strong>the</strong> enlarged prostate and <strong>the</strong> irritative<br />
symptoms (such as weak ur<strong>in</strong>ary stream or <strong>in</strong>complete blad,<br />
The outcome is a sense of urgency to empty <strong>the</strong> bladder. symptoms (urgency or frequency) from <strong>the</strong> detrusor<br />
In addition to <strong>the</strong>se changes of normal ag<strong>in</strong>g. many disease<br />
states commonly experienced by elderly persons can structive symptoms, it often has no effect on reliev<strong>in</strong>g <strong>the</strong><br />
overactivity. Although surgical treatment alleviates <strong>the</strong> ob-<br />
contribute to <strong>the</strong> problem of UI. <strong>Ur<strong>in</strong>ary</strong> tract <strong>in</strong>fections, irritative symptoms.<br />
prostatism, immobility. pelvic floor dysfunction, and fecal Overflow <strong>Incont<strong>in</strong>ence</strong>.-Overflow <strong>in</strong>cont<strong>in</strong>ence is less<br />
impactions are typical examples. Although age-related common than detrusor overactivity; it is estimated to occur<br />
changes can contribute to <strong>in</strong>cont<strong>in</strong>ence and <strong>the</strong>lefore need to <strong>in</strong> 7 to ll7o of <strong>in</strong>cont<strong>in</strong>ent elderly parients. Patients with<br />
be considered <strong>in</strong> <strong>the</strong> evaluation, one must never assume that overflow <strong>in</strong>cont<strong>in</strong>ence commonly have symptoms of substantially<br />
reduced ur<strong>in</strong>ary stream, <strong>in</strong>complete or unsuccess-<br />
UI <strong>in</strong> an elderly patient is due to ag<strong>in</strong>g alone. For appropriate<br />
assessment, classification by history, exam<strong>in</strong>ation, and results<br />
of test<strong>in</strong>g is important.<br />
bl<strong>in</strong>g. Overflow <strong>in</strong>cont<strong>in</strong>ence is generally due to a bladder<br />
ful void<strong>in</strong>g, and fiequent or even cont<strong>in</strong>uous ur<strong>in</strong>ary drib-<br />
with contractile dysfunction (hypotonic or atonic bladder) or<br />
TYPES OF INCONTINENCE<br />
obstructed ur<strong>in</strong>ary outflow. In ei<strong>the</strong>r case, large bladder<br />
Established UI can usually be divided <strong>in</strong>to one of fbur volumes result <strong>in</strong> an <strong>in</strong>travesicular pressure that exceeds <strong>the</strong><br />
types-detrusor oreractivi4, (urge <strong>in</strong>cor.rt<strong>in</strong>ence), ot'etJlou, <strong>in</strong>traurethral resistance and ultimately <strong>in</strong> symptoms of ur<strong>in</strong>ary<br />
dribbl<strong>in</strong>g.<br />
<strong>in</strong>contitte rtce. stress itl(otlt<strong>in</strong>ence (outleL <strong>in</strong>competence), or<br />
functional <strong>in</strong>cont<strong>in</strong>enc'e. Patients with <strong>the</strong>se disorders often Overflow <strong>in</strong>cont<strong>in</strong>ence secondary to an atonic bladder is<br />
have classic histories or typical physical f<strong>in</strong>d<strong>in</strong>gs. Unfortunately,<br />
elderly patients may have more rhan one type of UI; bladder <strong>in</strong>strumentation, or with <strong>the</strong> use of various medica-<br />
often transient after general or regional anes<strong>the</strong>sia. after<br />
accord<strong>in</strong>gly, <strong>the</strong> history and physical f<strong>in</strong>d<strong>in</strong>gs may be difficult<br />
to <strong>in</strong>terpret.<br />
der can be caused by disease of <strong>the</strong> peripheral nervgr-1ot<br />
tions such as narcotics. Contractile dysfunction of <strong>the</strong> blad-<br />
D etr u s o r O v e ractiv ity (U rg e I nc o nti ne nc e ).-Detrusor example, diabetic peripheral neuropathy---or sacral nerve<br />
overactivity is a common cause of UI <strong>in</strong> <strong>the</strong> elderly populatton,<br />
occurr<strong>in</strong>g <strong>in</strong> 40 to 70Vc of cases. This type of <strong>in</strong>contiable<br />
to an enlarged prostate from BPH. It may also be caused<br />
roots. Bladder outlet obstruction <strong>in</strong> men is usually attributnence<br />
is also known as detrusor <strong>in</strong>stability, detrusor by pelvic neoplasm or fecal impaction. Physical examrnation<br />
often reveals a distended bladder, and measurement of<br />
hyperreflexia, or un<strong>in</strong>hibited bladder. Patients with derrusor<br />
overactivity have early, forceful detrusor contractions, well ur<strong>in</strong>e volume after void<strong>in</strong>g reveals an <strong>in</strong>creased residual<br />
before <strong>the</strong> bladder is full. This situation creales a state of volume. Patients also have low ur<strong>in</strong>ary flow rates on urodynamic<br />
tests.<br />
ur<strong>in</strong>ary urgency and frequency. Patients with detrusor<br />
overactivity tend to lose small to lnoderate volumes of ur<strong>in</strong>e. Stress <strong>Incont<strong>in</strong>ence</strong> (Outlet Incompetence).-<strong>Ur<strong>in</strong>ary</strong><br />
If <strong>the</strong> detrusor contraction is strong enough to overcome <strong>the</strong> stress <strong>in</strong>cont<strong>in</strong>ence, also known as outlet <strong>in</strong>competence, is<br />
urethral resistance, <strong>in</strong>conl<strong>in</strong>ence occurs.<br />
common <strong>in</strong> women. Patients describe losses of small volumes<br />
of ur<strong>in</strong>e with activities that transiently <strong>in</strong>crease <strong>the</strong><br />
Detrusor overactivity can be found <strong>in</strong> conditions ofdefective<br />
centlal nervous system <strong>in</strong>hibition or <strong>in</strong>creased afferent <strong>in</strong>tra-abdom<strong>in</strong>al pressure (such as cough<strong>in</strong>g, sneez<strong>in</strong>g, runn<strong>in</strong>g,<br />
or laugh<strong>in</strong>g). Loss of ur<strong>in</strong>e can result from a reduced<br />
sensory stimulation fronr <strong>the</strong> bladder. Examples of disorders<br />
that impair <strong>the</strong> ability of <strong>the</strong> central nervous system to send tone of <strong>the</strong> <strong>in</strong>ternal and <strong>the</strong> extemal ur<strong>in</strong>ary sph<strong>in</strong>cter. Although<br />
this type of <strong>in</strong>cont<strong>in</strong>ence can occur <strong>in</strong> men, it is<br />
<strong>in</strong>hibitory signals are strokes, masses (tumor, aneurysm,<br />
hemorrhage), demyel<strong>in</strong>at<strong>in</strong>g disease (multiple sclerosis), usually limited to those who have had <strong>in</strong>temal sph<strong>in</strong>cter<br />
and Park<strong>in</strong>son's disease. Increased afferent stimulation from damage from urologic procedures.<br />
<strong>the</strong> bladder can result from lower ur<strong>in</strong>ary tract <strong>in</strong>fections.<br />
atrophic urethritis, fecal impaction, uter<strong>in</strong>e prolapse, or benign<br />
prostaric hyperplasia (BPH).<br />
The diagnosis of detrusor overacriviry is primarily based<br />
on <strong>the</strong> history. Patients have no pathognomonic f<strong>in</strong>d<strong>in</strong>gs on<br />
physical exam<strong>in</strong>ation, although a careful pelvic and rectal<br />
exam<strong>in</strong>ation and neurologic screen<strong>in</strong>g can occasionally re-<br />
In women, <strong>the</strong> cause of ur<strong>in</strong>ary stress <strong>in</strong>cont<strong>in</strong>ence is<br />
usually pelvic relaxation as a result of childbirth and <strong>the</strong><br />
ag<strong>in</strong>g process. These changes become more pronounced<br />
after menopause, when estrogen deficiency allows atrophy<br />
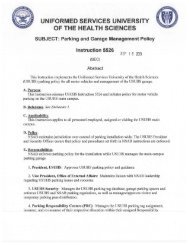
of <strong>the</strong> genitour<strong>in</strong>ary tissues. Pelvic relaxation, <strong>in</strong>clud<strong>in</strong>g<br />
uter<strong>in</strong>e prolapse and cystocele. allows descent of <strong>the</strong> normal<br />
urethrovesical angle (Fig. 2). This anatomic distortion al-<br />
:<br />
i;<br />
i.l
URINARY INCONTINENCE IN ELDERLY PERSONS<br />
Fig. 2. Dagrams depict<strong>in</strong>g posterior urethrovesical angle. A, Normal relationship. B, With pelvic relaxation (from ag<strong>in</strong>g, childbirth' a<br />
o<strong>the</strong>r factors), angle is <strong>in</strong>creased.<br />
lows <strong>the</strong> urethral sph<strong>in</strong>cter to be more vulnerable to <strong>in</strong>creased<br />
<strong>in</strong>travesical pressure from any activity that results <strong>in</strong> ei<strong>the</strong>r as a result of ur<strong>in</strong>e production (diuretics) or by dire<br />
some medications can affect ur<strong>in</strong>ary cont<strong>in</strong>ence (Table l<br />
<strong>in</strong>creased <strong>in</strong>tra-abdom<strong>in</strong>al pressirre. Loss of ur<strong>in</strong>e <strong>the</strong>n results.<br />
O<strong>the</strong>r less common causes <strong>in</strong>clude cauda equ<strong>in</strong>a le-<br />
sph<strong>in</strong>cter (sympa<strong>the</strong>tic agonists or antagonists).1r<br />
effects on <strong>the</strong> detrusor muscle (antichol<strong>in</strong>ergics) or <strong>in</strong>terr<br />
sions or peripheral neuropathy, Physical exam<strong>in</strong>ation may<br />
reveal evidence of pelvic relaxation, such as cystocele, EVALUATION OF INCONTINENCE<br />
rectocele, or uter<strong>in</strong>e prolapse. Loss of ur<strong>in</strong>e can usually be Assessment of <strong>the</strong> patient with established UI <strong>in</strong>volves elir<br />
demonstrated by hav<strong>in</strong>g <strong>the</strong> patient cough while <strong>in</strong> <strong>the</strong> sup<strong>in</strong>e<br />
position.<br />
physical exam<strong>in</strong>ation. Occasionally, various simple labor<br />
tation of a thorough medical history and performance ol<br />
F unc tio nal I n c ont<strong>in</strong> e n c e.-Patients with functional <strong>in</strong>cont<strong>in</strong>ence<br />
are those who would o<strong>the</strong>rwise be cont<strong>in</strong>ent but, urodynamic studies, are sometimes needed to determ<strong>in</strong>e t<br />
tory tests are necessary. More elaborate tests, <strong>in</strong>cludi<br />
because ofphysical or cognitive problems or use ofvarious type of <strong>in</strong>cont<strong>in</strong>ence that is present.<br />
medications, are unable to reach <strong>the</strong> toilet facilities <strong>in</strong> time. History.-The history is <strong>the</strong> most irnportant part of t<br />
This result may be ascribed to decreased mobility due to evaluation of UI. Patients should be asked how frequen<br />
severe arthritis, weakness (from strokes or decondition<strong>in</strong>g), <strong>in</strong>cont<strong>in</strong>ence is a problem and how much ur<strong>in</strong>e is lost w<br />
contractures, or <strong>the</strong> use of physical restra<strong>in</strong>ts. Functional each episode of <strong>in</strong>cont<strong>in</strong>ence. Small volumes of ur<strong>in</strong>e i<br />
<strong>in</strong>cont<strong>in</strong>ence may also be caused by medications, impaired lost <strong>in</strong> overflow <strong>in</strong>cont<strong>in</strong>ence and outlet <strong>in</strong>cornpetenr<br />
cognition (for example, from delirium or dementia), or excessive<br />
distance of <strong>the</strong> patient from <strong>the</strong> toilet facilities. Pa-<br />
Patients should be asked what activities produce an episo<br />
whereas moderate volumes are lost <strong>in</strong> detrusor overactivi<br />
tients with peripheral edema from any cause often have fluid of <strong>in</strong>cont<strong>in</strong>ence. Precipitat<strong>in</strong>g factors such as cough<strong>in</strong>g<br />
shifts at night from recumbency, result<strong>in</strong>g <strong>in</strong> nocturia. This sneez<strong>in</strong>g are highly suggestive of outlet <strong>in</strong>competence, I<br />
situation can exacerbate UI of any cause or can contribute to <strong>the</strong>se activities may also trigger premature detrusor contri<br />
its development when present <strong>in</strong> comb<strong>in</strong>ation with cognitive tions. Patients should be questioned about whe<strong>the</strong>r and<br />
impairment, immobility, or <strong>the</strong> effect of various medications.<br />
Generally, patients with functional <strong>in</strong>cont<strong>in</strong>ence have specifically, whe<strong>the</strong>r any degree of social isolation has<br />
what degree <strong>the</strong>ir <strong>in</strong>cont<strong>in</strong>ence limits <strong>the</strong>ir lifestyle ar<br />
normally function<strong>in</strong>g ur<strong>in</strong>ary systems, and <strong>the</strong> <strong>in</strong>cont<strong>in</strong>ence sulted because of <strong>the</strong> <strong>in</strong>cont<strong>in</strong>ence. O<strong>the</strong>r important qu'<br />
is a result of some external factor. Consequently, no typical tions <strong>in</strong>clude whe<strong>the</strong>r <strong>the</strong>y use protective absorbent und<br />
f<strong>in</strong>d<strong>in</strong>gs will be noted on physical exam<strong>in</strong>ation. F<strong>in</strong>ally, garments or pads, and how frequently <strong>the</strong>y need to char
Mayo Cl<strong>in</strong> Proc, .January 1996' Vol 7l<br />
URINARY INCONTINENCE IN ELDERLY PERSONS 9'7<br />
Tatrlc l.-Medications That Can Affect Cont<strong>in</strong>ence also be done to disclose any neurolo-lic deficiency. pl'ostate<br />
abnormalities, t-ecal irr.rpaction, or pelvic pathologic condition.<br />
Pelvic exanriliafion may be useful lor detection of<br />
T1,pe Lrl drug<br />
Potential action<br />
Drureltc s<br />
Cause brisk fillirtg of bladder cystocele. uter<strong>in</strong>e prolapse. rcctocele. of atrophic urogenital<br />
Antichol<strong>in</strong>ergics Impair detrusor contraction<br />
tissues. Intenral sph<strong>in</strong>cter weakness can be assessed by<br />
Sedative or h1'Pnotics Cause confusiotr<br />
Narcotic s<br />
Impair detrusor contf action hav<strong>in</strong>g <strong>the</strong> patient cough whilc ly<strong>in</strong>g sup<strong>in</strong>e otl <strong>the</strong> exatnilrrrtion<br />
table. Leakage of ur<strong>in</strong>c <strong>in</strong> this posititln is suggestive of<br />
g-Adreut-rg ic agonists Increase tone of <strong>in</strong>tental sph<strong>in</strong>cter<br />
g-Adrenerg tc antagonlsts Decrease tone of <strong>in</strong>temal sph<strong>in</strong>cter outlet <strong>in</strong>competence. A thorough neurolo-Eic e xarn<strong>in</strong>atiott tc'r<br />
Calcrunr chlrtnel Lrlockers Decrease rlett usol' conlraction assess fcrr evidcnce of central nervous systeln. spitrltl. tlr<br />
peripheral nerve disease should also be per'lbrmed.<br />
<strong>the</strong>ir clo<strong>the</strong>s because of lcakage of ul'<strong>in</strong>e. The nurnber of Laboratory Te.sl.r.-selected laboratory tests may be of<br />
episodes of nocturia should be recorded, as well as whe<strong>the</strong>r use <strong>in</strong> <strong>the</strong> evalualion of UI. Results ol urir.ralysis may<br />
noctumal i nctlt-tt<strong>in</strong>ence occurs.<br />
suggest <strong>in</strong>fection. <strong>in</strong>flarnmatiorr. or a malignant lesion. A<br />
Syrnpir>nrs of ur<strong>in</strong>ary urgency should sugges<strong>the</strong> presence<br />
of dr-trusor overactivlty. Increased ur<strong>in</strong>ary frequency is evicience ol'<strong>in</strong>fection or if <strong>the</strong> liistory suggests <strong>the</strong> possibility<br />
ur<strong>in</strong>e culture should be obta<strong>in</strong>cd if <strong>the</strong> ur<strong>in</strong>alysis shows<br />
often no(ed irr patients with overflclw <strong>in</strong>cont<strong>in</strong>ence and of ur<strong>in</strong>ary tract <strong>in</strong>f'ection. Although acute ul'illary tract <strong>in</strong>lections<br />
can producc <strong>in</strong>cont<strong>in</strong>ence, no firrn evidence <strong>in</strong>dicates<br />
detrusor oleractivity. Patietlts who describe dil'ficulty <strong>in</strong>itiat<strong>in</strong>g<br />
ur<strong>in</strong>lt ion. stra<strong>in</strong><strong>in</strong>g to void, or a decreased force of <strong>the</strong>ir that long-stand<strong>in</strong>g. asyrlptolnatic bacteriulia is associated<br />
ur<strong>in</strong>ary strL-ant may have a bladder outlet obstruction. The with <strong>in</strong>cont<strong>in</strong>encc ()r tllJl treatlnent ol' usyntplt)nlatic<br />
frequencl' and scverity of loss of' ur<strong>in</strong>e can be lrlolc accurately<br />
docuntcnted by hav<strong>in</strong>g tlre patient complete a weekly should <strong>in</strong>clude a me asure of renal function, stlch as a serum<br />
bacteriuria will alleviate ittcont<strong>in</strong>ence.rs<br />
'7 Blood tests<br />
diary ol krg. ir-r which lhe alnounts and types of lluids consumed.<br />
<strong>the</strong> liequency and volunles of void<strong>in</strong>gs, and <strong>the</strong> rnusclc mass. however, <strong>the</strong>sc measures can substantially un-<br />
creat<strong>in</strong><strong>in</strong>e or blootl urea nitrogcn. Becausc clf rcduced<br />
frequenc-r- nnd cst<strong>in</strong>ratcd voluntes of <strong>in</strong>conl<strong>in</strong>ent episodes are dercslimate <strong>the</strong> actual renal fut.tctiorr <strong>in</strong> elder'ly patients. If<br />
recordecl. C)l'ten withirr only a week or two, a pattem of <strong>the</strong> <strong>the</strong> history suggests a polyuric condition, serum calcium and<br />
type of L)l enrerges.<br />
glucose values should also be dctenn<strong>in</strong>cd. A s<strong>in</strong>rple test that<br />
The duration that thc <strong>in</strong>cont<strong>in</strong>ence has been present and can yield useful <strong>in</strong>tbrmation is a postvoid<strong>in</strong>g ur<strong>in</strong>ary tt'act<br />
<strong>the</strong> progression of symptoms nray provide some clues about ca<strong>the</strong>terization to record thc resiclual volunre. A ur<strong>in</strong>e volume<br />
that cxceeds 50 mL may <strong>in</strong>dicate ur<strong>in</strong>ary obstruetion or<br />
<strong>the</strong> likelihootl clf reversibility. The patient's functiona|a and<br />
cognitive slatus should be dctermirled. Severe constipation, a hypotonic bladder.<br />
diarrhea, or l'ecal iucont<strong>in</strong>ence nlay suggest neurologic or IJrodynamic Testittg.-The specific cause of Ul <strong>in</strong> a<br />
autonomic dysfunctiotr or a fecal impaction.<br />
patient can usuallv be established without tornial urodynamic<br />
test<strong>in</strong>g. Although urodynamic studies are fre-<br />
The past rnedical history should also be reviewed. The<br />
presence crl diabetes mellitus (especially with known neuropathy),<br />
BPH. neurologic disease. recun'ent ur<strong>in</strong>ary tract <strong>in</strong>formation exists about specific <strong>in</strong>dications for test<strong>in</strong>g'<br />
quently performed irr <strong>the</strong> evaluation of <strong>in</strong>cont<strong>in</strong>ence. little<br />
<strong>in</strong>fections. pr-lv ic disease. and postmenopausal gen itour<strong>in</strong>ary Urodynamic testittg lnust bc performed by tra<strong>in</strong>cd personnel<br />
atrophy mar., pr'giisplvse or contribute to <strong>in</strong>cont<strong>in</strong>ence. Prior <strong>in</strong> order to providc valid. reproducible results. Never<strong>the</strong>less'<br />
pelvic or iil.rdonr<strong>in</strong>al operations or radiation treatment should some elderly persons with UI will have nornlal urodynanric<br />
be documente
L]RINAR}' INC-']NTINENCE IN ELDERLY PERSONS<br />
Nlavo Cl<strong>in</strong> Proc. .lanuarr i.r'!n.<br />
-<br />
Vol 7l<br />
-<br />
E<br />
Ei<br />
t :<br />
dynamic studies. cystontetry is probably thc rntlst tlselul ln<br />
<strong>the</strong> assessment of <strong>the</strong> patient witl'r cletrusor overactivity.<br />
Trbic l. Indications for l-rrologic Consultation <strong>in</strong> 1'.rxign15<br />
With Ur<strong>in</strong>arr <strong>Incont<strong>in</strong>ence</strong><br />
Such patients will cien.ronstrate detrusor cotitractions and<br />
characteristic pressure <strong>in</strong>creases well before <strong>the</strong> bladder is<br />
filled. Multichannel urodynanric test<strong>in</strong>-s allows s<strong>in</strong>rLrltaneous<br />
measurenrents of <strong>in</strong>travesical, <strong>in</strong>tra-abdom<strong>in</strong>al. and<br />
urethral pressrtres dur<strong>in</strong>g rest<strong>in</strong>g, provocativL- nlaneuvcrs,<br />
and void<strong>in</strong>g and can dist<strong>in</strong>-euish among various typc's of<br />
Diagnosis is unclear (for cxample. nore than one 1)[r! ;l<strong>in</strong>cont<strong>in</strong>ence<br />
is descnbed)'i<br />
Overfl ow ir.rcont<strong>in</strong>ence is documentcd<br />
Paticnt does not re sponci to treatment<br />
Gross or nticroscopic helnaturia is prese nt<br />
F<strong>in</strong>d<strong>in</strong>gs on prostatc exam<strong>in</strong>ation suggest I nlalignant lrsion<br />
<strong>in</strong>cont<strong>in</strong>ence.<br />
*[lrodynarnic test<strong>in</strong>s ntay be necessarl'.<br />
<strong>Ur<strong>in</strong>ary</strong> Flow Measurement.-Occasionally. a lnellsurenrent<br />
of ur<strong>in</strong>ary flow is used lbr detect<strong>in</strong>g a urirlary<br />
obstruction. The flow pattern will be abnormal <strong>in</strong> patients<br />
with a poorly contract<strong>in</strong>g bladder. Bclth mean ancl peak<br />
ur<strong>in</strong>ary flows are nteasured. A mean ur<strong>in</strong>ary flow can easily<br />
be determ<strong>in</strong>ed without elaboratequipment s<strong>in</strong>rply by measur<strong>in</strong>g<br />
<strong>the</strong> volume of voided ur<strong>in</strong>e and clivid<strong>in</strong>g by <strong>the</strong> time of<br />
ur<strong>in</strong>ation. A norrnal ur<strong>in</strong>ary tlow rate should be at Ieast l()<br />
Detrusor ()veractivity.-Paticnts with detrusor overactivity<br />
often rcspond to behavioral <strong>the</strong>rapy corrsist<strong>in</strong>g of<br />
bladclerctra<strong>in</strong><strong>in</strong>g. if <strong>the</strong>y are mcltivated to clo stl lrnd are<br />
co-snitivcly <strong>in</strong>tact.rr:t FoL example, such patients lircr <strong>in</strong>structecl<br />
<strong>in</strong> a scheclule for <strong>in</strong>take of tlLricls. void<strong>in</strong>g technitlues.<br />
ancl scheduled voicl<strong>in</strong>g. lnstitr-rtionalized patic i rts can<br />
mL/s.<br />
also bcrrel-it from bchavioral tra<strong>in</strong><strong>in</strong>g by us<strong>in</strong>g scht:ciuled<br />
Llrethral Pressure Profile.-The urethral pressure lro- toilet<strong>in</strong>g or prompted void<strong>in</strong>g.rt r" Such methotls are<br />
['ilc nrcasures <strong>the</strong> pressure rvith<strong>in</strong> <strong>the</strong> urethra ancl its tunctional<br />
care-tiver-clepenclent and require a nurs<strong>in</strong>g staf't'detlie rited to<br />
len-gth. This profilc <strong>in</strong>dicatcs whe<strong>the</strong>r <strong>the</strong> resistlirtcc<br />
suf f icient to prevent leakage of ur<strong>in</strong>e tiorl <strong>the</strong> ur<strong>in</strong>ary blad-<br />
cler. This test may be usefulor cvaluation of'ur<strong>in</strong>arY stress<br />
lncontlnence.<br />
thc nranagenrent of patients with <strong>in</strong>cont<strong>in</strong>ence.<br />
Delmsor overaclivity also responds to vatrious pliarmaceLrtical<br />
agents (Table 3). Acetylchol<strong>in</strong>e is <strong>the</strong> neur()transrnitter<br />
that mecliates detrusor contraction. Therelbrc. antichol<strong>in</strong>ergic<br />
nreclications are often used to suppress <strong>the</strong>se<br />
Imag<strong>in</strong>g Studies.-lmag<strong>in</strong>g studies for urodytranlic<br />
analyses <strong>in</strong>clude two racliologic tests-<strong>in</strong>travenous carly contriictions. Cotrrnronly ttsecl agents <strong>in</strong>clutlo oxybutl'n<strong>in</strong><br />
chloride. flavoxate hycirochloride. and imipr,rm<strong>in</strong>e<br />
pyelography and voidirrg c1'stourethrography. Intravenotts<br />
pyelography is occasionally useful it' structulal abnornrali- hyclrochloride.sr'rr When <strong>the</strong>rapy with tl.rese drugs is rnitiatecl.<br />
Iies are suspccted.r') Void<strong>in</strong>g cystourethrography may detcct<br />
hladcler cliverticula, pelvic tloor relaxation, bladder tlutlet<br />
<strong>in</strong>conrpetence, ur<strong>in</strong>ary retlux, or outlet obstruction.<br />
<strong>the</strong> dosage shoirld be low and gradually <strong>in</strong>ct'eascd to<br />
<strong>the</strong>rapeutic level to m<strong>in</strong>imizc adverse et't.ects. surch as dry<br />
mouth, clry eyes. constipation, confusion. orthc)stiltic hypotension,<br />
and tachycardia. Although not approved spccifi-<br />
Imag<strong>in</strong>g of <strong>the</strong> genitour<strong>in</strong>ary tract by ultrasonography<br />
niay be clone to measure residual blaclder volltmc whcn<br />
ca<strong>the</strong>terization cannot be pertbrmed or to assess tor <strong>the</strong><br />
cally tbr r-rse <strong>in</strong> <strong>in</strong>cont<strong>in</strong>ence, calcium channcl blockcrs have<br />
been shorvn to be useful <strong>in</strong> <strong>the</strong> treattnent of detrusor<br />
presence of hyclronephrosis <strong>in</strong> patients with high rcsiclual overactivity because of <strong>the</strong>ir direct eff'ect on smooth muscle<br />
ur<strong>in</strong>e volumes.rl rr<br />
rclaxation.t5 Special care must be taken whcn <strong>the</strong>sc medications<br />
Urologic Evaluation.-Most cases of <strong>in</strong>cortt<strong>in</strong>enccltn<br />
be el'f'ectively evaluated by thc primary-care physician. For<br />
certa<strong>in</strong> patients, however. a urologist, gynecologist. or<br />
physratrist should be consulted (Table 2). Assessment by a<br />
gy nceolorist with ln <strong>in</strong>tcrcst or trairt<strong>in</strong>g <strong>in</strong> <strong>in</strong>cont<strong>in</strong>cnec mi.iv<br />
are used-especially <strong>in</strong> patients rvho may have urrnary<br />
outflow obstruction-because <strong>the</strong>se drugs can precipitate<br />
ur<strong>in</strong>ary retention. In patients with a ur<strong>in</strong>ary tract <strong>in</strong>f.ection oI<br />
symptoms of outflow obstruction. a postvoid<strong>in</strong>g restdual<br />
ur<strong>in</strong>e volume should be determ<strong>in</strong>ed as part of <strong>the</strong> evaluittion.<br />
be useful <strong>in</strong> women with prior bladder suspensiotr 1lt'tlceclures.<br />
pelvic floor relaxation (for example, cystocele, have <strong>in</strong>adequate <strong>in</strong>temal sph<strong>in</strong>cter tone ancl urethral resis-<br />
Stress I ncont<strong>in</strong>ence.-Patients with stress lnconttnence<br />
rectocele, or uter<strong>in</strong>e prolapse), or pelvic filasses. ln sot.ne<br />
rcgions, physiatrists have specialized <strong>in</strong> <strong>the</strong> evaluation and<br />
l'able 3.-Nledications Usei'ul for Treat<strong>in</strong>g<br />
lreatment of Ul. especially tn those patients with functional<br />
I)etrusor Overactivit-y or Stress <strong>Incont<strong>in</strong>ence</strong><br />
()r cL)gnitive limitations.<br />
Drug<br />
Dosage<br />
TREATMENT OF INCONTINENCE<br />
Most cases of UI can be eff'ectively treated and <strong>the</strong> symptoms<br />
alleviirted. providecl <strong>the</strong> type of <strong>in</strong>cont<strong>in</strong>ence prescnt i\<br />
determ<strong>in</strong>ed.<br />
Oryhutyn<strong>in</strong> chloriclc<br />
Flavorate hydrochloride<br />
Imiprarr <strong>in</strong>e hydrochloride<br />
Propan<strong>the</strong>l<strong>in</strong>e bromicle<br />
5 rng 3-.1 timcs/day<br />
100-200 mg 3-.1 tirnes/dai<br />
25-5t)mg 2 3 times/day<br />
7.5- l5 mg -l-:l times/da)
Mayo Cl<strong>in</strong> Proc, January 1996, Vol 7l URINARY INCONTINENCE IN ELDERLY PERSONS 99<br />
tance to prevent loss of ur<strong>in</strong>e when bladder pressure transiently<br />
<strong>in</strong>creases. The goal <strong>in</strong> nonsurgical treatment is to prazos<strong>in</strong> hydrochloride, terazos<strong>in</strong> hydrochloride, or dox-<br />
surgical candidates. a-Adrenergic antagonists such as<br />
<strong>in</strong>crease <strong>in</strong>ternal sph<strong>in</strong>cter tone.<br />
azos<strong>in</strong> mesylate reduce <strong>in</strong>temal sph<strong>in</strong>cter tone and can improve<br />
<strong>the</strong> flow of ur<strong>in</strong>e. These agents must be used cau-<br />
Pelvic floor exercises (for example, Kegel exercises or<br />
vag<strong>in</strong>al cones) can be effective <strong>in</strong> motivated patients.r6r8tiously <strong>in</strong> elderly patients because of <strong>the</strong>ir propensity to<br />
These exercises streng<strong>the</strong>n both <strong>the</strong> periurethral and <strong>the</strong> cause orthostatic hypotension. Doses should be low <strong>in</strong>itially<br />
pelvic floor muscles. They are easy to perform but must be and gradually <strong>in</strong>creased as tolerated. F<strong>in</strong>asteride may decrease<br />
<strong>the</strong> size of <strong>the</strong> prostate gland <strong>in</strong> some men such that<br />
done frequently throughout <strong>the</strong> day and cont<strong>in</strong>ued for longrerm<br />
effect. Patients can identify <strong>the</strong> pelvic floor muscles by ur<strong>in</strong>ary flow will improve, although no immediate effect<br />
attempt<strong>in</strong>g <strong>in</strong>terruption of void<strong>in</strong>g or by digital palpation should be anticipated. Its efficacy <strong>in</strong> <strong>the</strong> treatment of UI is<br />
dur<strong>in</strong>g contraction. Most proponents recommend l0 to 20 unclear.<br />
pelvic floor contractions for 10 seconds each, 3 times a day. Patients with overflow <strong>in</strong>cont<strong>in</strong>ence result<strong>in</strong>g from a hypotonic<br />
or atonic bladder can benefit from medications with<br />
Beneficial effects may not be noted until <strong>the</strong>se exercises<br />
have been done for 6 to 8 weeks. Reported improvement or chol<strong>in</strong>ergic agonist activity, such as bethanechol; however,<br />
cure rates have been as high asJJo/o. These results compare little evidence suggests that long-term success can be expected.<br />
For optimal effect, bethanechol should be adrn<strong>in</strong>is-<br />
favorably to treatment with medications. Cont<strong>in</strong>ued benefit<br />
after improvement with pelvic floor streng<strong>the</strong>n<strong>in</strong>g depends tered 20 m<strong>in</strong>utes before void<strong>in</strong>g is attempted. Postoperative<br />
on <strong>the</strong> patient's motivation and ability to cont<strong>in</strong>ue practic<strong>in</strong>g patients are <strong>the</strong> most likely to benefit from short-term use of<br />
<strong>the</strong> pelvic floor exercises.<br />
this medication. Patients with overflow <strong>in</strong>cont<strong>in</strong>ence can<br />
cr-Adrenergic agonists such as phenylpropanolam<strong>in</strong>e also be <strong>in</strong>structed <strong>in</strong> assistive void<strong>in</strong>g techniques (for example,<br />
abdom<strong>in</strong>al stra<strong>in</strong> or Cred6 maneuver).<br />
hydrochloride and pseudoephedr<strong>in</strong>e <strong>in</strong>crease <strong>the</strong> <strong>in</strong>ternal<br />
sph<strong>in</strong>cter tone and bladder outflow resistance.3e Intermittent<br />
use of <strong>the</strong>se medications (for example, for planned acaged<br />
with <strong>in</strong>termittent self-ca<strong>the</strong>terization or <strong>in</strong>dwell<strong>in</strong>g<br />
Patients with overflow <strong>in</strong>cont<strong>in</strong>ence may also be mantivities)<br />
can be beneficial. These drugs should be used bladder ca<strong>the</strong>terization.a6 ln patients who have new-onset<br />
cautiously <strong>in</strong> patients with hypertension or a history of cardiac<br />
arrhythmias.<br />
is occasionally noted after <strong>in</strong>dwell<strong>in</strong>g ca<strong>the</strong>terization <strong>in</strong> <strong>the</strong><br />
<strong>in</strong>cont<strong>in</strong>ence from a transient hypotonic or atonic bladder, as<br />
Estrogen replacement <strong>the</strong>rapy can be helpful <strong>in</strong> improv<strong>in</strong>g<br />
periurethral and vag<strong>in</strong>al tissue thickness and quality.a0al until <strong>the</strong> bladder tone returns. Initially, a ca<strong>the</strong>ter should be<br />
hospital, <strong>in</strong>termittent bladder ca<strong>the</strong>terization should be used<br />
Topical, oral, or transdermal preparations of estrogen are all <strong>in</strong>serted every 4 to 6 hours after a prompted or attempted<br />
effective . Topical homonal <strong>the</strong>rapy is generally adequate void <strong>in</strong> order to keep <strong>the</strong> bladder volumes less than 400 mL.<br />
unless o<strong>the</strong>r systemic effects are desired.<br />
Subsequently, <strong>the</strong> frequency of ca<strong>the</strong>terization should be<br />
Several surgical procedures may also prove helpful for based on <strong>the</strong> residual ur<strong>in</strong>e volumes. As <strong>the</strong> residual volume<br />
stress <strong>in</strong>cont<strong>in</strong>ence attributable to pelvic relaxation or <strong>in</strong>ternal<br />
sph<strong>in</strong>cter <strong>in</strong>sufficiency.a2{3 In women. correction of also decrease.<br />
of ur<strong>in</strong>e decreases, <strong>the</strong> frequency of ca<strong>the</strong>terizationshould<br />
pelvic relaxation and reestablishment of <strong>the</strong> normal urethrovesical<br />
angle can improve ur<strong>in</strong>ary retention. The placement long-term management of patients with overflow <strong>in</strong>conti-<br />
Intermittent self-ca<strong>the</strong>terization may also be used for<br />
of an artificial sph<strong>in</strong>cter, usually as a last resort, may also be nence who are cognitively <strong>in</strong>tact and have adequate manual<br />
beneficial <strong>in</strong> female patients or <strong>in</strong> men <strong>in</strong> whom complete dexterity.lT Most of <strong>the</strong>se patients can be taught safe selfca<strong>the</strong>terization<br />
techniques with clean ca<strong>the</strong>ters (sterility is<br />
sph<strong>in</strong>cter <strong>in</strong>sufficiency has developed.{{5 Local collagen<br />
<strong>in</strong>jections have also been used recently <strong>in</strong> selected patients to unnecessary). In <strong>the</strong> management of nurs<strong>in</strong>g home residents<br />
help alleviate ur<strong>in</strong>ary stress <strong>in</strong>cont<strong>in</strong>ence.<br />
with long-term UI, <strong>in</strong>termittent ca<strong>the</strong>terization by <strong>the</strong> nurs<strong>in</strong>g<br />
staff is usually prohibitively expensive (because of asso-<br />
Overflov' <strong>Incont<strong>in</strong>ence</strong>.-Patients with overflow <strong>in</strong>cont<strong>in</strong>ence<br />
have difficulty empty<strong>in</strong>g <strong>the</strong>ir bladder; <strong>the</strong>refore, ciated nurs<strong>in</strong>g and supply costs).<br />
<strong>the</strong> goal of treatment is to improve bladder dra<strong>in</strong>age. Occasionally,<br />
ne$, onset of overflow <strong>in</strong>cont<strong>in</strong>ence is precipitated cated for patients who are unable to empty <strong>the</strong>ir bladder and<br />
Long-term, <strong>in</strong>dwell<strong>in</strong>g ur<strong>in</strong>ary ca<strong>the</strong>terization is <strong>in</strong>di-<br />
by a neu' mc'tiication. anes<strong>the</strong>sia, or surgical procedure. have not responded to o<strong>the</strong>r treatment measures. Selected<br />
These patients often benefit from bladder dra<strong>in</strong>age fbr a few groups of patients such as <strong>the</strong> tem<strong>in</strong>ally ill or those for<br />
days, after n,hich normal bladder function resumes. Incont<strong>in</strong>ent<br />
personr. u'ith long-stand<strong>in</strong>g obstruction to ur<strong>in</strong>ary outfortable<br />
may also benefit from <strong>in</strong>dwell<strong>in</strong>g ca<strong>the</strong>terizalion.<br />
whom frequent ca<strong>the</strong>terizations would be difficult or uncomflow<br />
and orc.r'flow <strong>in</strong>cont<strong>in</strong>ence should be considered for Extemal (condom) ca<strong>the</strong>ters for male patients can also be<br />
surgtcal coneetion unless bladder atony is evident. Pharmacologic<br />
age:rrs .lte also available fbr patients who are not leakage, and sk<strong>in</strong> <strong>in</strong>itation or<br />
helpful, aithough <strong>the</strong>ir use may be limited by improper fit,<br />
breakdolr'rt.
lOO URINARY INCONTINENCE IN* ELDERLY PERSONS Mayo Cl<strong>in</strong> Pruc. ,lanuar.r 19q6, Vol ?l<br />
*<br />
I<br />
il<br />
F unctional I ncont<strong>in</strong>e nce.-Treatment of functional <strong>in</strong>cont<strong>in</strong>ence<br />
depends on <strong>the</strong> successful management of causment<br />
and appropriate treatment, <strong>the</strong> majority do not seek<br />
most patients with <strong>in</strong>cont<strong>in</strong>ence would benefit fiom assessative<br />
or contribut<strong>in</strong>g conditions. Mobility can be improved medical evaluation. Several different types of <strong>in</strong>cont<strong>in</strong>ence<br />
by reliev<strong>in</strong>g pa<strong>in</strong> and provid<strong>in</strong>g equipment for patients suffer<strong>in</strong>g<br />
from arthritis, contractures, decondition<strong>in</strong>g, and neu-<br />
evaluation. Only rarely are elaborate tests necessary. With a<br />
exist, and <strong>the</strong> history is usually <strong>the</strong> most important part of ths<br />
rologic impairments. Environmental modifications (for example,<br />
improv<strong>in</strong>g <strong>the</strong> light<strong>in</strong>g, us<strong>in</strong>g a bedside commode, or surgical trealments. most Patients can experience substantial<br />
comb<strong>in</strong>ation of behavioral, pharmacologic, and occasionally<br />
reduc<strong>in</strong>g <strong>the</strong> distance to <strong>the</strong> toilet) can be useful <strong>in</strong> selected improvement or cure of <strong>the</strong>ir symptoms of <strong>in</strong>cont<strong>in</strong>ence.<br />
patlents.<br />
Most cases of UI can be evaluated and treated by <strong>the</strong> primary-care<br />
physician, although a specialist should be con-<br />
UI associated with delirium usually resolves with treatment<br />
of <strong>the</strong> underly<strong>in</strong>g cause of <strong>the</strong> confusional state. Management<br />
of peripheral edema may decrease nocturia and its<br />
sulted for selected Patients.<br />
contribution to UI. Patients with dementia may benefit from<br />
prompted void<strong>in</strong>g, scheduled voids, and attention to behavioral<br />
signals that <strong>in</strong>dicate a desire to void. Adjustment of po-<br />
REFERENCES<br />
l Elv<strong>in</strong>g LB, Foldspang A, Lam GW, Mommsen S Descriptive<br />
epidemiology of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence <strong>in</strong> 3,100 women<br />
tentially offend<strong>in</strong>g medications (cessation or dose reduction)<br />
should be considered. In patients who abuse alcohol or <strong>in</strong> age 30-59. Scand J Urol Nephrol Suppl 1989: 125:31-43<br />
patients with UI exacerbated by "safe" levels of alcohol use, 2. Diokno AC, Brock BM, Brown MB, Herzog AR- Prevalence<br />
of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence and o<strong>the</strong>r urological symptoms <strong>in</strong> <strong>the</strong><br />
cessation of <strong>in</strong>gestion of any alcohol should be considered.<br />
non<strong>in</strong>stitutionalized elderly. J Urol 19861136:1022-1025<br />
Absorbent undergarments are often used by <strong>in</strong>cont<strong>in</strong>ent<br />
3. Resnick NM. Yalla SV. Laur<strong>in</strong>o E. The pathophysiology of<br />
patients.aE Several types are available' some disposable and ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence among <strong>in</strong>stitutionalized elderly persons'<br />
o<strong>the</strong>rs reusable. Although <strong>the</strong>se products can help elderly N Engl J Med 1989; 320:l'7<br />
patients rega<strong>in</strong> freedom lost as a result of UI' <strong>the</strong>y may cause 4. Thomas TM. Plymat KR, Blann<strong>in</strong> J, Meade TW- Prevalence<br />
many patients to forego medical evaluation and merely accept<br />
<strong>the</strong> <strong>in</strong>cont<strong>in</strong>ence as ano<strong>the</strong>r age-related <strong>in</strong>convenience.ae<br />
of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence. BMJ l9tt0; 281:1243-1245<br />
5. Ouslander JG, Palmer MH, Rovner BW' German PS. <strong>Ur<strong>in</strong>ary</strong><br />
<strong>in</strong>cont<strong>in</strong>ence <strong>in</strong> nurs<strong>in</strong>g homes: <strong>in</strong>cidence, remission<br />
Absorbent undergarments are expensive and may cause sk<strong>in</strong> and associated iactors. J Am Geriatr Soc 199314l:1083-<br />
irritation and breakdown with long-terrn use'<br />
r 089<br />
6. Jeter KF. Wagner DB. <strong>Incont<strong>in</strong>ence</strong> <strong>in</strong> <strong>the</strong> American home: a<br />
survey of36,500 people. J Am Geriatr Soc 1990; 38:379-<br />
INCONTINENCE IN LONG.TERM-CARE<br />
383<br />
SETTINGS<br />
7. Hu TW. Impact of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence on health-care costs.<br />
At least 507o of nurs<strong>in</strong>g home residents have a major problem<br />
with UI. Many of <strong>the</strong>se residents can benefit from Wyman JF. Hark<strong>in</strong>s SW, Choi SC, Taylor JR. Fantl JA.<br />
J Am Geriatr Soc 1990; 38:292-295<br />
behavioral <strong>the</strong>rapy, such as scheduled toilet<strong>in</strong>g, habit tra<strong>in</strong><strong>in</strong>g,<br />
and prompted void<strong>in</strong>g. Because of <strong>the</strong> high frequency of<br />
Psychosocial impact of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence <strong>in</strong> women.<br />
Obstet Gynecol 1987; 70:378-381<br />
9. McCormick KA, Scheve AAS, Leahy E' Nurs<strong>in</strong>g management<br />
of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence <strong>in</strong> geriatric <strong>in</strong>patients. Nurs<br />
cognitive impairment attributable to dementia' a considerable<br />
percentage of nurs<strong>in</strong>g home residents will not benefit Cl<strong>in</strong> North Am 1988 Mar 23:231-264<br />
from various types ofbehavioral <strong>the</strong>rapy. Federal guidel<strong>in</strong>es l0 Wyman JF, Hark<strong>in</strong>s SW, Fantl JA. Psychosocial impact of<br />
suggesthat nurs<strong>in</strong>g home residents with UI should undergo ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence <strong>in</strong> <strong>the</strong> community-dwell<strong>in</strong>g population.<br />
evaluation of <strong>in</strong>cont<strong>in</strong>ence and an attempt at treatment when J Am Ceriatr Soc 1990; 38:2it2-288<br />
l l<br />
Williams ME, Pannilt FC lll <strong>Ur<strong>in</strong>ary</strong> <strong>in</strong>cont<strong>in</strong>ence <strong>in</strong> <strong>the</strong><br />
I l .<br />
feasible.so Therefore, identify<strong>in</strong>g those patients who have<br />
elderly: physiology, pathophysiology, diagnosis, and treatment.<br />
Ann Intern Med 1982;91:895-90'7<br />
potential to respond to <strong>the</strong>rapeutic <strong>in</strong>terventions becomes<br />
important. Evidence now suggests that nurs<strong>in</strong>g home residents<br />
who are likely to benefit from behavioral <strong>the</strong>rapy for ag<strong>in</strong>g patient. Adv Intem Med 1989; 34: I 65- I 90<br />
12. Ouslander JG, Bruskewitz R. Disorders of micturition <strong>in</strong> <strong>the</strong><br />
IJ<br />
Ul can be easily identified. Incont<strong>in</strong>ent nurs<strong>in</strong>g home residents<br />
who respond to a simple, non<strong>in</strong>vasive assessment con-<br />
Resnick NM. <strong>Ur<strong>in</strong>ary</strong> <strong>in</strong>cont<strong>in</strong>ence <strong>in</strong> older adults. Hosp<br />
Pract 1992Oct.27:139-142; 147; l-50; 157r l601 164-166;<br />
178:180-l8l:184<br />
sist<strong>in</strong>g of a 3-day trial of prompted void<strong>in</strong>g have potential to T4 Williams ME, Gaylord SA. Role oi functional assessment rn<br />
show long-term benefit <strong>in</strong> control of <strong>the</strong>ir UI with use of <strong>the</strong> evaluation of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence. J Am Geriatr Soc<br />
1990;38:296'299<br />
prompted void<strong>in</strong>g.5l<br />
15 Boscia JA, Kabasa WD, Abrutyn E, Levison ME, Kaplan<br />
CONCLUSION<br />
UI is a common condition <strong>in</strong> <strong>the</strong> elderly population, both <strong>in</strong><br />
<strong>the</strong> community and <strong>in</strong> long-term-care sett<strong>in</strong>gs. Although<br />
AM, Kaye D. Lack of association between bacteriuria and<br />
symptoms <strong>in</strong> <strong>the</strong> elderly. Am J Med 1986; 8l:979-982<br />
16. Ouslander JG. Asymptomatic bacteriuria and <strong>in</strong>cont<strong>in</strong>ence<br />
0etterl. J Am Geriatr Soc 1989; 37:197-198<br />
1il<br />
E $<br />
\i<br />
*
ilIayo Cl<strong>in</strong> Proc, January 1996' Vol 7l<br />
URINARY INCONTINENCE IN ELDERLY PERSONS 101<br />
)<br />
yi<br />
I<br />
I<br />
.l<br />
t:.<br />
i,<br />
lr<br />
f;i<br />
li<br />
il ,<br />
i<br />
if<br />
I'.<br />
it<br />
ir ,i<br />
I<br />
H<br />
Ouslander JG, Schapira M, Schnelle JF, Uman G, F<strong>in</strong>gold S' 34. Moore KH, Hay DM, Imrie AE, Watson A, Goldste<strong>in</strong> M.<br />
Tuico E, et al. Does eradicat<strong>in</strong>g bacteriuria affect <strong>the</strong> severlty Oxybutyn<strong>in</strong> hydrochloride (3 mg) <strong>in</strong> <strong>the</strong> treatment of women<br />
of chronic ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence <strong>in</strong> nurs<strong>in</strong>g home residents? with idiopathic detrusor <strong>in</strong>stability. Br J Urol 1990;'66:479-<br />
Ann Intern Med 1995; 122:'749-754<br />
4ti5<br />
Diokno AC, Normolle DP, Brown MB, Herzog AR' We<strong>in</strong> AJ. Pharmacologic treatment of <strong>in</strong>cont<strong>in</strong>ence. J Am<br />
18.<br />
35.<br />
Urodynarnic tests fbr female geriatric ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence' Geriatr Soc 1990; 38:317-325<br />
Urology 1990; 36:431-439<br />
36. Bums PA, Marecki MA, Dittmar SS, Bullough B. Kegel's<br />
Diokno AC. Diagnostic categories of <strong>in</strong>cont<strong>in</strong>ence and <strong>the</strong> exercises with biofeedback <strong>the</strong>rapy for treatment of stress<br />
t9.<br />
role of urodynamic test<strong>in</strong>g. J Am Gcriatr Soc 1990: 38:300- <strong>in</strong>cont<strong>in</strong>ence. Nurse Pract 1985; l0:28; 33'34:' 46<br />
305<br />
37 Bums PA, Pranikoff K, Nochajski T, Desotelle P, Harwood<br />
Kurnar R, Schreiber MH. The chang<strong>in</strong>g <strong>in</strong>dications for excretory<br />
urography. JAMA 1985; 254:403-4O5<br />
cises and biofeedback. J Am Geriatr Soc 1990; 38:341-<br />
MK. Treatment of stress <strong>in</strong>cont<strong>in</strong>ence with pelvic floor exer-<br />
20.<br />
21 Courtney SP, Wightman JA. The value of ultrasound scann<strong>in</strong>g<br />
of <strong>the</strong> upper ur<strong>in</strong>ary tract <strong>in</strong> patients with bladder outlet 38. Ferguson KL, McKey PL, Bishop KR, Kloen P, Verheul JB'<br />
344<br />
obstruction. Br J Urol 1991; 68:169-171<br />
Dougherty MC. Stress ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence: effect of pelvic<br />
Haylen BT. Residual ur<strong>in</strong>e volumes <strong>in</strong> a normal female muscle exercise. Obstet Cynecol 1990,75:67 l-6'75<br />
22.<br />
population: application of transvag<strong>in</strong>al ultrasound. Br J Urol 39. Collste L, L<strong>in</strong>dskog M. Phenylpropanolam<strong>in</strong>e<br />
treatment of<br />
1989:64:347-349<br />
female stress ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence: double-bl<strong>in</strong>d placebo<br />
Webb JA. Ultrasonography <strong>in</strong> <strong>the</strong> diagnosis of renal obstruction.<br />
BMJ 1990; 301:944-946<br />
40 Cardozo L. Role of estrogens <strong>in</strong> <strong>the</strong> treatment of female<br />
controlled study <strong>in</strong> 24 patients. Urology 1987; 30:398-403<br />
23<br />
Burton JR, Pearce KL, Burgio KL, Engel BT, Whitehead ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence. J Am Geriatr Soc 1990; 38:326'328<br />
24<br />
WE. Behavioral tra<strong>in</strong><strong>in</strong>g for ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence <strong>in</strong> elderly 4l Hilton P, Tweddell AL, Mayne C. Oral and <strong>in</strong>travag<strong>in</strong>al<br />
ambulatory patients. J Am Geriatr Soc 1988; 36:693-698 estrogens alone and <strong>in</strong> comb<strong>in</strong>ation with alpha-adrenergic<br />
Fnntl JA, Wyman JF, Hark<strong>in</strong>s SW, Hadley EC. Bladder stimulation <strong>in</strong> genu<strong>in</strong>e stress <strong>in</strong>cont<strong>in</strong>ence. Int Urogynecol J<br />
l)<br />
tra<strong>in</strong><strong>in</strong>g <strong>in</strong> <strong>the</strong> management of lower ur<strong>in</strong>ary tract dysfunction 1990; l:80-86<br />
AA<br />
<strong>in</strong> women: a review. J Am Geriatr Soc 1990; 38:329-332 Beck RP, McCormick S, Nordstrom L' The fascia lata sl<strong>in</strong>g<br />
26. Fantl JA, Wyman JF, McClish DK, Hark<strong>in</strong>s SW, Elswick procedure lbr treat<strong>in</strong>g reculTent genu<strong>in</strong>e stress <strong>in</strong>cont<strong>in</strong>ence<br />
RK, Taylor JR, et al. Efficacy of bladder tra<strong>in</strong><strong>in</strong>g <strong>in</strong> older of ur<strong>in</strong>e. ObstetGynecol 1988; 72:699'703<br />
women with ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence. JAMA 1991; 265:609- +3. Raz S. Modified bladder neck suspension for female stress<br />
6r3<br />
<strong>in</strong>cont<strong>in</strong>ence. Urology l98l; l7:82-85<br />
2'1 . Hadley EC. Bladder tra<strong>in</strong><strong>in</strong>g and related <strong>the</strong>rapies for ur<strong>in</strong>ary 44 Diokno AC, Hollander JB, Alderson TP. Artificial unnary<br />
ircont<strong>in</strong>ence <strong>in</strong> older people. JAMA 1986; 256:372-379 sph<strong>in</strong>cter for recurrent female ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence: <strong>in</strong>dications<br />
andresults. J Urol 1987; 138:778-780<br />
28. Burgio LD. Engel BT, Hawk<strong>in</strong>s A, McCormick K, Scheve A,<br />
Jones LT. A staff management system for ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g improvements<br />
<strong>in</strong> cont<strong>in</strong>ence with elderly nurs<strong>in</strong>g home rest-<br />
after prostatectomy with <strong>the</strong> artificial ur<strong>in</strong>ary sph<strong>in</strong>cter' J<br />
45. Marks JL, Light JK. Management of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence<br />
dents. J Appl Behav Anal 1990; 23:111-l l8<br />
Urol 1989; 142:302-304<br />
29. Engel BT, Burgio LD, McCormick KA, Hawk<strong>in</strong>s AM, 46. Warren JW. Ur<strong>in</strong>e-collection devices for use <strong>in</strong> adults with<br />
Scheve AA. Leahy E. Behavioral treatment of <strong>in</strong>cont<strong>in</strong>ence ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence. J Am Geriatr Soc 1990; 38364-367<br />
<strong>in</strong> <strong>the</strong> long-terrn care sett<strong>in</strong>g. J Am Geriatr Soc 1990; 47, Lapides J, Diokno AC, Silber SJ, Lowe BS' Clean, <strong>in</strong>termittent<br />
self-ca<strong>the</strong>terization <strong>in</strong> <strong>the</strong> treatment of ur<strong>in</strong>ary tract<br />
38:361 -363<br />
dis-<br />
30. Schnelle JF. Treatment of ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence <strong>in</strong> nurs<strong>in</strong>g<br />
home patients by prompted void<strong>in</strong>g. J Am Geriatr Soc 1990;<br />
38:356-360<br />
31. Castleden CM, Duff<strong>in</strong> HM, Gulati RS. Double-bl<strong>in</strong>d study of<br />
imipram<strong>in</strong>e and placebo for <strong>in</strong>cont<strong>in</strong>ence due to bladder <strong>in</strong>stability.<br />
Age Age<strong>in</strong>g 1986; l5:299-303<br />
32. Chapple CR, Parkhouse H, Gardener C, Milroy EJ. Doublebl<strong>in</strong>d,<br />
placebo-controlled, cross-over study of flavoxate <strong>in</strong> <strong>the</strong><br />
featment of idiopathic detrusor <strong>in</strong>stability. Br J Urol 1990;<br />
66-.49t-494<br />
33. Gilja I, Radej M, Kovacic M, Parazajder J. Conservative<br />
treatment of female stress <strong>in</strong>cont<strong>in</strong>ence with imipram<strong>in</strong>e. J<br />
Urol 1984:132:909-911<br />
48<br />
49<br />
ease. J Urol 1972' 107:458-461<br />
Br<strong>in</strong>k CA. Absorbent pads, garments, and management strategies.<br />
J Am Geriatr Soc 1990; 38:368-373<br />
Starer P, Libow LS. Obscur<strong>in</strong>g ur<strong>in</strong>ary <strong>in</strong>cont<strong>in</strong>ence: diaper<strong>in</strong>g<br />
of <strong>the</strong> elderly. J Am Geriatr Soc 1985; 33:842-846<br />
50. Agency for Health Care Policy Research. <strong>Ur<strong>in</strong>ary</strong> <strong>Incont<strong>in</strong>ence</strong><br />
<strong>in</strong> Adults. Cl<strong>in</strong>ical Practice Guidel<strong>in</strong>e, No' 2'<br />
Rockville (MD): Agency for Health Care Policy Research,<br />
1992Mat (Publication No. AHCPR 92-0038)<br />
51. Ouslander JG, Schnelle JF, Uman G, F<strong>in</strong>gold S, Nigam JG'<br />
Tuico E, et al. Predictors of successful prompted void<strong>in</strong>g<br />
among <strong>in</strong>cont<strong>in</strong>ent nurs<strong>in</strong>g home residents' JAMA 1995;<br />
273:1366-1370<br />
End of Symposium onGeriatrics,<br />
Part Vll.<br />
Part Vlll will apPear <strong>in</strong><strong>the</strong> February issue.