QUALITY OF LIFE - National Cancer Centre Singapore
QUALITY OF LIFE - National Cancer Centre Singapore
QUALITY OF LIFE - National Cancer Centre Singapore

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Issue No. 18 • MICA (P) 061/10/2010<br />
AN NCCS BI-MONTHLY PUBLICATION<br />
September / October 2011<br />
...HELPING READERS TO ACHIEVE GOOD HEALTH<br />
Salubris is a Latin word which means healthy, in good condition (body) and wholesome.<br />
A PR<strong>OF</strong>ESSIONAL AND<br />
PERSONAL PERSPECTIVE ON<br />
<strong>QUALITY</strong> <strong>OF</strong> <strong>LIFE</strong>
PAGE A2<br />
In Focus<br />
SALUBRIS<br />
September / October 2011<br />
<strong>QUALITY</strong> <strong>OF</strong> <strong>LIFE</strong> –<br />
A PERSONAL AND<br />
PR<strong>OF</strong>ESSIONAL PERSPECTIVE<br />
PAGE A3<br />
In Focus<br />
SALUBRIS<br />
September / October 2011<br />
We often use “quality of life” to explain medical decision-making, especially at the end<br />
of life. The more medical technology progresses, the more we realise that it is not just<br />
the length, but the quality of survival, that matters.<br />
That said, there are patients with severe disease who report a reasonable quality of life. One<br />
explanation is that quality of life is the discrepancy between our expectations of life and our<br />
experience of it. Patients who have low expectations or who have become accustomed to<br />
their reduced level of function may regard their quality of life as good. On the other end of the<br />
spectrum, patients with good function and high expectations may rate a minor disability as a<br />
severe reduction in quality of life (the “disability paradox”).<br />
Once, a patient’s<br />
relatives complained to<br />
me: “The other doctor is<br />
so heartless – I told him<br />
I did not want to give up<br />
on my mother yet and<br />
he told me, but she has<br />
no quality of life… how<br />
would he know? He is<br />
not my mother.”<br />
Hence the importance of patient peersupport<br />
groups in many chronic disease<br />
conditions: meeting someone else<br />
(amputee, arthritis, alcoholism, etc)<br />
with similar experiences (or with worse<br />
disability but coping well) puts your own<br />
expectations in context.<br />
All these factors make it difficult to<br />
measure quality of life: people have<br />
different personalities and expectations at<br />
the beginning of their illness, people may<br />
be at different phases of their illness when<br />
their quality of life is measured, and their<br />
expectations may change over time (the<br />
“response shift”).<br />
My mother used to support people who<br />
facilitated euthanasia, like the late<br />
“Dr Death”. As soon as it became<br />
available in <strong>Singapore</strong>, she signed an<br />
advanced medical directive. When friends<br />
or relatives passed away, she consoled<br />
herself: “they are happier now and no<br />
longer suffering”.<br />
Last year she was diagnosed with a<br />
progressive terminal illness. She began to<br />
talk about euthanasia for herself and how she<br />
wanted to end things while “the going was<br />
good and she was still able to get going”.<br />
She weakened slowly over the months.<br />
She talked less about euthanasia, at least<br />
with regard to her own situation. Her<br />
attitude, however, appeared unchanged –<br />
in many of her hospitalisation episodes,<br />
she would point to someone else in<br />
the same ward and say out loud: “she<br />
shouldn’t be kept alive – she’s suffering”.<br />
(Much to our horror and embarrassment,<br />
she often said this within earshot of the<br />
family of whoever she was pointing to.)<br />
We noticed that her spirits<br />
improved considerably<br />
when she started to attend<br />
a hospice daycare centre.<br />
One day she told me she<br />
felt a bit like a fraud – all<br />
the other patients appeared<br />
to be much weaker than<br />
she was. I realised that one<br />
of the reasons she enjoyed<br />
the sessions (in addition<br />
to the company, the care<br />
and the activities) was that<br />
being with other ill patients<br />
who took their disease and<br />
their prognosis in stride<br />
made her own suffering<br />
pale in comparison.<br />
Given how subjective quality of life is,<br />
why do doctors still look for the “perfect”<br />
measuring tool, especially in chronic<br />
disease and end-of-life situations?<br />
In clinical practice, quality of life tools<br />
can help identify and prioritise complex<br />
problems the patient is facing. It can help<br />
communication when the patient has<br />
multiple symptoms, screen for hidden<br />
problems, and assist in shared clinical<br />
decision making.<br />
More commonly, it helps monitor<br />
response to treatment. In cancer, for<br />
example, where some of the treatments<br />
have side effects that affect patients’<br />
function, but can prolong the number of<br />
days, quality of life measures are used.<br />
As a research tool, quality of life measures<br />
can compare two different treatments<br />
for the same disease or symptom where<br />
outcome measures are not clear. A<br />
simplified example would be: comparing<br />
one treatment which prolongs life by 2<br />
months but has severe side effects, with<br />
another treatment that prolongs life by 1<br />
month with minor side effects.<br />
What happens when the patient cannot<br />
communicate their wishes? In such<br />
situations, we often expect their partners<br />
or close family to act as their proxies<br />
– people who know what the patient<br />
would want in a similar situation and<br />
who would act in their best interests.<br />
How much is the agreement between<br />
the patient and their partner, or between<br />
the patient and their healthcare worker?<br />
– Studies have shown fairly good<br />
agreements (almost half were identical or<br />
close ratings, and less than 20% showed<br />
profound discrepancies).<br />
But is that enough? Unfortunately, as in<br />
the story mentioned in the beginning<br />
of the article, not everyone accepts this<br />
assumption. We can ask as many people<br />
as we can what they would wish in the<br />
same situation, but they are not that<br />
person. Even if you are that person, things<br />
may change over time.<br />
My mother’s disease continued to<br />
progress. A few times, she was admitted<br />
to the intensive care unit. Each time, she<br />
would initially refuse intubation, and we<br />
would talk her into accepting it.<br />
She recovered well each time – somehow<br />
proving that we (her “proxies”) had been<br />
right to “persuade” her into accepting<br />
life-support measures.<br />
I left for a brief period of training in<br />
Australia when her disease looked stable.<br />
She was suffering from a bad bout of<br />
oral thrush infection when I left, and our<br />
farewell dinner was quite disappointing<br />
– her favourite curry dish “only tasted of<br />
pain” and she stared at the food on the<br />
table mumbling “what a waste…”.<br />
When peach season arrived in Australia,<br />
I lamented to myself that I could not bring<br />
the peaches back home for my mum, who<br />
loves peaches.<br />
Midway through my training, I received<br />
a phonecall. My mother was in intensive<br />
care again. I booked my flight back. On<br />
the way out of the house, I grabbed a bag<br />
of peaches from the kitchen.<br />
I stayed in <strong>Singapore</strong> long enough to<br />
see my mother out of intensive care and<br />
extubated. She devoured the peaches.<br />
I took her out on home leave while in<br />
hospital, back to her favourite restaurant.<br />
Her oral thrush infection had been treated<br />
and she wolfed down her food.<br />
Her memory is fading, and she now needs<br />
to be in a wheelchair when she goes out.<br />
She used to be imperiously impatient and<br />
pride herself in being the fastest to do<br />
anything – one of her favourite phrases was<br />
“time and tide and Irene wait for no man,<br />
woman or child”. Now, whenever we tell<br />
her it is time to do something – go out with<br />
us, take a shower, change her clothes… she<br />
would refuse to let us help her (not even<br />
with the simplest task of getting dressed),<br />
scold us for not giving her time to think,<br />
then stop and stare around her, looking for<br />
something she would never find.<br />
I don’t know what she would have thought<br />
of herself last year, had she seen herself now.<br />
Yet, she has stopped talking about ending<br />
her life, and seems to be enjoying it.<br />
By Dr Wong Ting Hway<br />
Associate Consultant,<br />
Department of General Surgery, SGH
PAGE A4<br />
In Other Words STEPPING UP ON SERVICE –<br />
SALUBRIS<br />
September / October 2011<br />
THE NCCS WAY<br />
GYNAECOLOGICAL CANCERS:<br />
TREATMENT AND SCREENING I<br />
PAGE B1<br />
Looking Forward<br />
SALUBRIS<br />
September / October 2011<br />
Disney comes to NCCS<br />
as the centre takes a<br />
great leap forward to<br />
improve its delivery to<br />
patients by adopting<br />
their service culture.<br />
VERONICA LEE reports.<br />
Gynaecological <strong>Cancer</strong>s broadly refers to<br />
cancers of the cervix, uterus and ovaries; less<br />
commonly also includes cancers of the vulva,<br />
vagina and fallopian tube. This article will<br />
focus on the three commonest gynaecological<br />
cancers, namely cancers of the uterus, ovaries<br />
and cervix, which are the 4th, 5th, and 6th<br />
commonest female cancers in <strong>Singapore</strong>.<br />
What initially started as an attempt<br />
to understand the importance of<br />
service quality for a clinician has<br />
now been spun off into a whole corporate<br />
culture shift in NCCS.<br />
An innocuous three-day seminar on<br />
“Disney’s Key to Excellence” saw among<br />
its participants our Senior Consultant,<br />
Dr Terence Tan, from the Department of<br />
Radiation Oncology at NCCS. Together with<br />
two other colleagues, they learnt about the<br />
Disney Approach to Business Excellence<br />
and Service Excellence. It was not only very<br />
interesting and engaging, but it inspired him<br />
to ask: why not at NCCS?<br />
“This was a programme which has been<br />
very well thought out, is established and<br />
known to produce good and consistent<br />
results. We came away feeling that it may<br />
be just what we needed to help bring<br />
service quality in NCCS to a new and<br />
higher level,” he said.<br />
He immediately got down to work, crafting<br />
NCCS’s common purpose. It was a big<br />
hurdle as there was no universal agreement<br />
on what the common purpose ought<br />
to be. A retreat was held for the senior<br />
management. It didn’t end there.<br />
Hours of deliberation followed thereafter.<br />
Finally the common purpose was written<br />
up: “We offer our patients hope by<br />
providing the best care, by having the best<br />
people and by doing the best research”.<br />
Next came the task of getting the staff<br />
to embrace the new quality standard in<br />
this order: Safety, Courtesy, Show and<br />
Efficiency. Knowledge and practice of<br />
safety is important for staff although they<br />
may not be directly involved in caring of<br />
patients. Safety must always come first,<br />
without any compromise.<br />
“Everyone who attended the programme<br />
could see how well it worked for Disney.<br />
Applying it to our various work scenarios,<br />
we could see that it applied equally<br />
well. Indeed, using appropriate examples<br />
in the subsequent phases of Disney<br />
implementation in NCCS, it was obvious<br />
that all staff understood and appreciated<br />
the applicability of the new service quality<br />
standard,” explained Dr Tan.<br />
The staffs responded enthusiastically.<br />
Attendance at a service quality event<br />
was overwhelming. It demonstrated a<br />
commitment to embrace a new culture –<br />
to provide better service to patients.<br />
“This is very heartening as it indicates our<br />
staff’s desire to learn more about how they<br />
can improve the way they can provide care<br />
to their patients,” added Dr Tan.<br />
Driven by the heartening response, what<br />
lies ahead is to take advantage of the current<br />
interest and momentum to ensure that the<br />
service standards and expected behaviours<br />
are universally adopted and practiced.<br />
“NCCS Cares”, a programme to<br />
continuously train and remind staff about<br />
the importance of putting the standards into<br />
practice, was rolled out with the launch of<br />
the NCCS Cares logo. It depicts a heart with<br />
two arms in a warm embrace, symbolising<br />
the spirit of caring. All NCCS patients can<br />
expect to receive “HOPE” with the “Best<br />
Experience”. NCCS is proud to be the first<br />
healthcare institution in the Singhealth<br />
cluster to implement such a programme.<br />
Dr Tan said that support from staff in<br />
supervisory roles is crucial. “We are<br />
counting on all HODs, managers,<br />
supervisors and all others in positions of<br />
influence to not only model the desired<br />
behaviours themselves, but also to motivate<br />
all others to exhibit the behaviours that will<br />
give patients the best experience.”<br />
CANCER <strong>OF</strong> THE CERVIX<br />
This is currently the 6th commonest female cancer in <strong>Singapore</strong>, with an incidence rate<br />
of 11.5 per 100, 000 per year. In KK Gynaecological <strong>Cancer</strong> <strong>Centre</strong>, we see an average<br />
of 140 to 150 new cases per year. The peak age groups affected are women in the 40s<br />
and 50s.One of the main advantages of TomoTherapy is that verification of CT images are<br />
acquired before each treatment. With daily CT imaging, the correctness of positioning<br />
can be verified for each treatment. This is particularly useful when treating a tumour site<br />
that can be influenced by day to day anatomical changes. For example, rectum or bladder<br />
distension can change the position of prostate gland tumours.<br />
In recent years, the underlying cause of cervical cancer has been uncovered. It is attributed<br />
to a sexually transmitted virus called the Human Papilloma Virus (HPV). This virus is said to<br />
account for 99.7% of all cervical cancers. There are two subgroups of HPV virus: low risk<br />
subtypes e.g. HPV type 6 and 11 and high risk subtypes e.g. HPV type 16 and 18. HPV virus<br />
is very prevalent in the community.<br />
Most sexually active women will<br />
have been exposed to this virus.<br />
Majority of the virus infection<br />
resolves spontaneously. It is only the<br />
persistence of the infection by the<br />
high risk subtypes that may result in<br />
cervical cancers years later. Hence,<br />
cervical cancer is a very rare outcome<br />
of a very common infection.<br />
People who are immunocompromised<br />
e.g. HIV patients, renal transplant<br />
patients, patients with autoimmune<br />
diseases on immunosuppression<br />
therapy, are more likely to have<br />
persistent infection.<br />
Other risk factors that predispose women<br />
with persistent infection with high risk<br />
subtypes include: women with multiple<br />
sexual partners, smokers and early age at<br />
first intercourse.<br />
Persistent infection with<br />
high risk HPV virus does<br />
not lead to cervical cancers<br />
overnight. The cells of the<br />
cervix initially undergo some<br />
changes first. These changes<br />
occur months to years before<br />
cancer develop and are<br />
known as precancer changes<br />
of the cervix, aka Cervical<br />
Intraepithelia Neoplasia<br />
(CIN). At this stage, there<br />
are no symptoms and signs.<br />
Precancer changes of<br />
the cervix can only be<br />
detected on routine Pap<br />
smears. It is only when<br />
precancer changes are<br />
undetected and untreated<br />
that cervical cancer<br />
eventually develops.<br />
Continued on page B2.
PAGE B2<br />
Looking Forward<br />
SALUBRIS<br />
September / October 2011<br />
GYNAECOLOGICAL CANCERS:<br />
TREATMENT AND SCREENING I<br />
COPING WITH<br />
UTERINE (WOMB) CANCER<br />
PAGE B3<br />
Tender Care<br />
SALUBRIS<br />
September / October 2011<br />
Continued from page B1.<br />
The uterus, or womb, is an important female reproductive<br />
organ. The uterus is the pelvic organ that holds the baby during<br />
pregnancy. <strong>Cancer</strong> of the womb (or uterine cancer) usually occurs<br />
after menopause and it is now the 4th most common cancer<br />
among women in <strong>Singapore</strong>. There are about 300 cases diagnosed<br />
annually according to the <strong>Singapore</strong> <strong>Cancer</strong> Registry 2005-2009.<br />
THE COMMON SYMPTOMS<br />
<strong>OF</strong> CERVICAL CANCERS<br />
ARE:<br />
• Bleeding after intercourse<br />
• Bleeding in between menses<br />
• Blood stained or foul smelling<br />
vaginal discharge<br />
• Bleeding after menopause<br />
• Pain is often a late sign of<br />
cervical cancer<br />
Cervical cancer presents as a growth on<br />
the cervix and a biopsy will be taken by the<br />
doctor to confirm the presence of cancerous<br />
cells. Once the cancer is confirmed, the<br />
patient will be referred to a gynaecologic<br />
oncologist for further management,<br />
which entails further investigations to<br />
determine the extent/spread of the cancer.<br />
This often entails imaging studies e.g.<br />
CT scan, MRI and a procedure called<br />
examination under anaesthesia.<br />
For early cancers, the choice of treatment is between surgery and radiotherapy. The choice<br />
will largely be dependent on factors e.g. age, surgical feasibility etc, which the oncologist<br />
will advice accordingly depending on the individual patient. For advanced disease, the<br />
treatment will be radiation concurrent with chemotherapy or chemotherapy.<br />
FIVE-YEAR OUTLOOK<br />
(SURVIVAL) IS<br />
DEPENDENT ON STAGE:<br />
• Stage 1 80-90%<br />
• Stage 2 50-70%<br />
• Stage 3 20-40%<br />
• Stage 4 10-20%<br />
The good news is that cervical cancer can be prevented. Concurrently, one can prevent<br />
cervical cancer by HPV vaccination (primary prevention) and Pap smear (secondary<br />
prevention). There are 2 vaccines available now: Cervarix and Gardasil. The latter covers<br />
subtypes 16 and 18 i.e. the high risk subtypes that account for 70% of cervical cancers,<br />
the latter besides covering subtypes 16 and 18 also covers low risk subtypes 6 and 11 that<br />
causes genital warts. The vaccines are indicated for girls aged 9 to 26. Cervarix is available<br />
at all polyclinics and is medisave deductible. Pap smear screening is recommended for all<br />
sexually active women aged 25 to 65 at least once every three years. The Pap smear test<br />
is a screening test for cervical cancer. It aims to detect precancer changes on the cervix<br />
which can easily be treated so that cancer development can be prevented. It is a simple<br />
and affordable test available at all polyclinics, GPs and Gynaecology Clinics.<br />
As this is a cancer that affects mainly<br />
women after menopause (75% of<br />
cases), the most common presenting<br />
symptom is postmenopausal bleeding (vaginal<br />
bleeding after menopause). However, in<br />
women who are still menstruating, it may<br />
present with heavy irregular periods or<br />
intermenstrual bleeding. There are several<br />
known risk factors for this cancer including:<br />
increasing age, late menopause, obesity, family<br />
history of breast or womb cancer, personal<br />
history of breast cancer, polycystic ovary<br />
syndrome and estrogen only hormone therapy.<br />
Treatment for womb cancer varies depending<br />
on overall health and how advanced the<br />
cancer is. Fortunately, most cancers of the<br />
womb occur at an early stage and surgery<br />
alone is curative. However, some patients<br />
will require further treatment after surgery<br />
if there is evidence of the cancer spreading.<br />
This includes radiotherapy, chemotherapy or<br />
hormonal therapy.<br />
The stage of the cancer will determine<br />
the type of treatment. The cancer is<br />
referred to as early if it remains confined<br />
to the region of the cervix. It is referred to<br />
as advanced if it has spread beyond the<br />
confines of the cervix to the surrounding<br />
organs or distant organs.<br />
By Dr Chia Yin Nin<br />
MBBS(S’pore), MRCOG(UK), FAMS(S’pore), DGO(RANZCOG), GDipHCML(SMU)<br />
Certified Gynaecologic Oncologist<br />
Head & Consultant , Gynaecological <strong>Cancer</strong> Unit, KK Women’s and Children’s Hospital<br />
Adjunct Assistant Professor, Duke’s Medical School, <strong>Singapore</strong><br />
Visiting Consultant, <strong>National</strong> <strong>Cancer</strong> <strong>Centre</strong> <strong>Singapore</strong><br />
Uterine cancer can be particularly difficult<br />
to cope with, physically and emotionally.<br />
Uterine cancer can be particularly difficult<br />
to cope with, physically and emotionally. If<br />
you have cancer, you may often feel tired. It is<br />
important to learn ways to manage symptoms<br />
of cancer and the side effects from cancer<br />
treatment, and to maintain good nutrition and<br />
overall well-being.<br />
Continued on page B4.
PAGE B4<br />
Tender Care<br />
SALUBRIS<br />
September / October 2011<br />
COPING WITH<br />
UTERINE (WOMB) CANCER<br />
妇 科 癌 症 : 治 疗 与 筛 检 1<br />
PAGE B5<br />
往 前 看<br />
SALUBRIS<br />
September / October 2011<br />
Continued from page B3.<br />
BE ACTIVE IF YOU CAN<br />
Most people feel, eat and sleep better<br />
when they exercise. Choose an exercise<br />
or sport that you enjoy. Even walking for<br />
a short time each day or a short ride on<br />
a bike / exercise bike can significantly<br />
boost your energy.<br />
DO FEWER THINGS<br />
Do the activities that are most important<br />
to you first. There will be times when you<br />
feel high in energy, but there will be low<br />
periods as well. Ask family and friends for<br />
help. They can make meals, drive you to<br />
the doctor, or help in other ways. Know<br />
your limits and avoid filling your day with<br />
too many activities.<br />
PLAN A WORK SCHEDULE<br />
THAT IS RIGHT FOR YOU<br />
Some people feel well enough to work,<br />
while others need to slow down. Take<br />
medical leave if needed and consider<br />
asking your boss if you can work part-time<br />
or from home.<br />
PLAN TIME TO REST<br />
You will need more rest during treatment<br />
especially following radiation therapy.<br />
Sleep at least eight hours each night and<br />
take short naps during the day (not more<br />
than an hour at a time). Studies have<br />
shown that relaxation techniques are<br />
essential to help reduce treatment-related<br />
side effects and improve emotional<br />
adjustment for patients undergoing<br />
non-surgical cancer treatment (Lubert et<br />
al, 2001). Engage in activities that help<br />
you to relax. Listening to music, watching<br />
your favourite TV show or reading helps<br />
to achieve relaxation.<br />
MANAGING SIDE EFFECTS<br />
<strong>OF</strong> CHEMOTHERAPY<br />
Chemotherapy side effects can be<br />
unpleasant. Knowing the side<br />
effects in advance can help you<br />
cope better during treatment.<br />
It is important to remember that most<br />
of the side effects of chemotherapy<br />
are short-term and will gradually<br />
disappear once the treatment is<br />
completed. Before you start your<br />
treatment, your doctor will discuss<br />
with you about the side effects of the<br />
treatment that you are having.<br />
MANAGING SIDE EFFECTS<br />
<strong>OF</strong> RADIATION THERAPY<br />
Treatment such as radiation therapy<br />
to the pelvis can lead to dryness, itch<br />
or burning sensation in the vagina,<br />
causing discomfort during sexual<br />
intercourse. There are gels or creams<br />
that help to alleviate these effects.<br />
Scarring from the treatment can<br />
narrow the vagina. A device called a<br />
dilator can help stretch the narrowed<br />
vagina. Side effects such as bowel<br />
changes, bladder and skin irritation<br />
may occur as well. Before you receive<br />
radiation treatment, you will be seen<br />
by a Radiation Oncologist (a doctor<br />
specialised in this type of treatment)<br />
who will assess your condition and<br />
explain to you about the treatment<br />
and its side effects. Talk to your doctor<br />
or nurse to get personalised advice<br />
tailored to your needs.<br />
MANAGE PAIN<br />
Having cancer does not mean that<br />
you will have pain. But if you do,<br />
you can manage most of your pain<br />
with medicine and other treatments.<br />
<strong>Cancer</strong> pain can range from mild to<br />
very severe. Some days it may be<br />
worse than others. It can be caused<br />
by the cancer itself, the treatment,<br />
or both. You may also have pain that<br />
has nothing to do with your cancer.<br />
Headaches and muscle strains are<br />
common for some people. Work with<br />
your doctors, nurses, and others to find<br />
the best way to control your pain, and<br />
check with your doctor before taking<br />
over-the-counter medications.<br />
SEXUALITY<br />
Many women have a sense of loss<br />
following a hysterectomy, feeling less<br />
feminine as a result. If you have not<br />
yet reached menopause, you have to<br />
come to terms with losing fertility.<br />
Side effects of radiation therapy,<br />
such as fatigue or pain can lower<br />
your sexual desire. If this applies<br />
to you, you are not alone. At times,<br />
losing interest in sex stops you from<br />
making an effort to enjoy all physical<br />
contact with your partner. If you<br />
feel nervous about starting your sex<br />
life again, give yourself time and<br />
more importantly, talk things over<br />
with your partner. Together you may<br />
work out what is best for you both.<br />
For most people, things improve<br />
with time. Keep in mind that you<br />
can always initiate a discussion with<br />
your doctor or nurse on matters<br />
concerning sexual relationship. If<br />
you prefer, you can request to be<br />
referred to professionals or specialists<br />
for support. There are also support<br />
groups composed of other women<br />
in similar life situations who meet<br />
regularly and share their experiences.<br />
REFERENCES<br />
C.H. Yarbro, M.H. Frogge & M.<br />
Goodman (1999).<strong>Cancer</strong> Symptom<br />
Management. (2nd Ed). Boston: Jones<br />
and Bartlett Publishers<br />
Luebbert, K., Dahmeb, B & Hasenbring, M.<br />
(2001). The effectiveness of relaxation<br />
training in reducing treatment-related<br />
symptoms and improving emotional<br />
adjustment in acute non-surgical<br />
cancer treatment: A meta-analytical<br />
review. Psycho-Oncology.10: 490-502.<br />
www.gyncancer.com/uterus.html<br />
www.cancer.gov/cancertopics/coping/<br />
physicaleffects#Fatigue<br />
By Jenna Teo<br />
Senior Nurse Manager, CEIS<br />
妇 科 癌 症 一 般 指 的 是 子 宫 颈 癌 、 子 宫<br />
癌 和 卵 巢 癌 ; 较 少 见 的 还 包 括 外 阴 癌 、<br />
阴 道 癌 和 输 卵 管 癌 。 本 文 将 着 重 介 绍<br />
三 大 常 见 妇 科 癌 症 — 子 宫 癌 、 卵 巢 癌<br />
和 子 宫 颈 癌 , 它 们 分 别 是 新 加 坡 女 性<br />
第 四 、 第 五 和 第 七 大 常 见 癌 症 。<br />
子 宫 颈 癌<br />
目 前 , 子 宫 颈 癌 是 新 加 坡 第 七 大 常 见 妇 科 癌 症 。 每 年 的 发 病 率 是 每 10 万 人 中 , 就 有<br />
11.5 人 患 病 。 在 竹 脚 妇 科 癌 症 中 心 , 每 年 平 均 有 140 至 150 起 新 病 例 。 女 性 发 病 高<br />
峰 年 龄 段 是 在 40 岁 至 50 岁 。<br />
近 年 来 , 研 究 人 员 已 找 出 罹 患 子 宫 颈 癌 的 根 本 原 因 。 它 是 由 一 种 称 为 “ 人 类 乳 头 状 瘤<br />
病 毒 ”( 简 称 HPV) 的 性 传 播 病 毒 所 引 起 的 。 在 所 有 子 宫 颈 癌 病 例 中 , 有 99.7% 是<br />
由 这 种 病 毒 所 引 起 的 。HPV 病 毒 可 分 成 两 大 类 : 低 危 亚 型 如 第 6 型 和 第 11 型 HPV<br />
病 毒 , 以 及 高 危 亚 型 , 如 第 16 型 和 第 18 型 HPV 病 毒 。HPV 病 毒 感 染 在 社 区 非 常 普<br />
遍 。 大 多 数 性 生 活 活 跃 的 女 性<br />
已 感 染 这 种 病 毒 。 在 多 数 情 况<br />
下 , 病 毒 感 染 会 自 发 清 除 。 只<br />
有 持 续 感 染 高 危 亚 型 病 毒 , 才<br />
会 在 几 年 后 患 上 子 宫 颈 癌 。 换<br />
言 之 , 子 宫 颈 癌 其 实 是 由 一 种<br />
常 见 病 毒 感 染 而 引 起 的 罕 见 后<br />
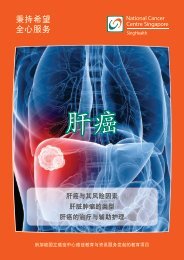
( 卵 巢 )<br />
果 。 免 疫 系 统 削 弱 者 如 爱 之 病<br />
( 输 卵 管 )<br />
( 子 宫 )<br />
患 者 、 肾 脏 移 植 病 人 , 以 及 接<br />
受 免 疫 抑 制 疗 法 的 自 身 免 疫 性<br />
( 肿 瘤 )<br />
疾 病 患 者 , 都 比 较 有 可 能 出 现<br />
( 子 宫 颈 )<br />
持 续 感 染 。 其 他 导 致 持 续 感 染<br />
( 阴 道 )<br />
高 危 亚 型 病 毒 的 女 性 较 容 易<br />
患 病 的 风 险 因 素 包 括 : 有 多 个<br />
性 伴 侣 、 吸 烟 , 以 及 年 龄 很 小<br />
就 发 生 第 一 次 性 交 。<br />
持 续 感 染 高 危 亚 型 HPV<br />
病 毒 , 并 不 会 使 子 宫 颈 癌<br />
在 一 夕 之 间 形 成 。 子 宫 颈<br />
细 胞 会 先 经 历 一 些 变 化 。<br />
这 些 变 化 经 过 几 个 月 甚 至<br />
几 年 的 时 间 , 才 会 形 成 癌<br />
症 , 这 种 情 况 叫 做 “ 子 宫 颈<br />
癌 前 病 变 ” 或 “ 宫 颈 上 皮<br />
内 瘤 样 病 变 ”(Cervical<br />
Intraepithelia<br />
Neoplasia, 简 称 CIN)。<br />
这 个 阶 段 并 没 有 任 何 症 状<br />
或 征 兆 。 子 宫 颈 癌 前 病 变<br />
只 能 通 过 例 常 的 子 宫 颈 抹<br />
片 检 查 检 测 出 来 。 只 有 当 癌<br />
前 病 变 未 被 检 测 和 治 疗 时 ,<br />
子 宫 颈 癌 才 会 形 成 。
PAGE B6<br />
往 前 看<br />
妇 科 癌 症 : 治 疗 与 筛 检 1<br />
应 对 子 宫 癌<br />
PAGE B7<br />
温 柔 呵 护<br />
SALUBRIS<br />
September / October 2011<br />
SALUBRIS<br />
September / October 2011<br />
( 正 常 ) ( 癌 症 )<br />
( 低 度 ) ( 高 度 )<br />
( 正 面 图 )<br />
( 癌 细 胞 )<br />
( 子 宫 颈 )<br />
( 阴 道 壁 )<br />
( 盆 腔 检 查 时 , 通 过 扩 张 器 观 看 的 子 宫 颈 )<br />
子 宫 是 女 性 的 重 要 生 殖 器 官 。 妇 女 怀 孕 时 , 子 宫 是 孕 育 胎 儿 的 盆<br />
腔 器 官 。 子 宫 癌 一 般 发 生 在 更 年 期 后 , 目 前 是 新 加 坡 妇 女 第 四 大<br />
最 常 见 癌 症 。 根 据 新 加 坡 癌 症 注 册 局 2005 年 至 2009 年 间 的 数<br />
据 , 每 年 有 大 约 300 起 确 诊 病 例 。<br />
由 于 这 种 癌 症 主 要 影 响 更 年 期 后 的 妇 女 ( 占 75% 的 病 例 ), 因 此<br />
最 常 见 的 症 状 是 停 经 后 出 血 ( 即 更 年 期 后 阴 道 出 血 )。 那 些 还 没<br />
停 经 的 妇 女 , 则 会 出 现 月 经 量 过 多 且 经 期 不 规 律 , 或 是 月 经 间 期<br />
出 血 的 症 状 。 这 种 癌 症 的 一 些 已 知 风 险 因 素 包 括 : 年 龄 增 长 、 更<br />
年 期 较 迟 、 肥 胖 、 家 族 成 员 曾 患 有 乳 癌 或 子 宫 癌 、 自 己 曾 患 有 乳<br />
癌 、 多 囊 卵 巢 综 合 症 , 以 及 接 受 雌 激 素 治 疗 。<br />
子 宫 癌 的 治 疗 , 须 视 病 患 的 健 康 情<br />
况 和 病 情 发 展 而 定 。 幸 好 , 多 数 的<br />
子 宫 癌 发 生 在 初 期 , 只 需 动 手 术 即<br />
可 治 愈 。 不 过 , 如 果 癌 细 胞 有 扩 散<br />
的 迹 象 , 病 患 就 必 须 在 手 术 后 接 受<br />
进 一 步 的 治 疗 , 包 括 放 射 治 疗 、 化<br />
疗 或 荷 尔 蒙 疗 法 。<br />
子 宫 癌 使 人 在 生 理 和 心 理 上 都 特 别<br />
难 以 应 付 。 癌 症 患 者 经 常 会 觉 得 疲<br />
惫 。 你 必 须 学 习 如 何 应 对 癌 症 症 状<br />
和 癌 症 治 疗 的 副 作 用 , 以 及 维 持 均<br />
衡 饮 食 和 整 体 健 康 。<br />
子 宫 颈 癌 的 常 见 症 状<br />
包 括 :<br />
• 性 交 后 出 血<br />
• 月 经 间 期 出 血<br />
• 阴 道 分 泌 物 有 血 迹 或 异 味<br />
• 停 经 后 出 血<br />
• 疼 痛 通 常 是 子 宫 颈 癌 的 后 期<br />
征 兆<br />
子 宫 颈 癌 以 肿 瘤 的 形 式 生 长 在 子 宫 颈 ,<br />
医 生 会 对 肿 瘤 进 行 活 组 织 抽 样 检 查 ,<br />
以 确 认 癌 细 胞 的 存 在 。 一 旦 确 认 病 人<br />
患 上 癌 症 , 病 人 将 被 转 介 给 一 名 妇 科<br />
肿 瘤 医 生 作 进 一 步 检 验 , 以 确 认 癌 症<br />
的 范 围 / 扩 散 程 度 。 这 往 往 包 括 一 些 影<br />
像 侦 查 , 如 电 脑 断 层 扫 描 (CT scan)<br />
、 磁 共 振 成 像 扫 描 (MRI), 以 及 一 种<br />
在 麻 醉 下 进 行 的 检 验 。<br />
治 疗 的 类 型 将 取 决 于 癌 症 的 阶 段 。 如<br />
果 癌 细 胞 只 局 限 在 子 宫 颈 部 位 , 癌 症<br />
仍 处 于 初 期 ; 如 果 癌 细 胞 已 扩 散 到 子<br />
宫 颈 外 邻 近 或 较 远 的 器 官 , 癌 症 就 处<br />
于 晚 期 。 初 期 癌 症 病 患 可 选 择 动 手 术<br />
或 进 行 放 射 治 疗 。<br />
这 主 要 是 根 据 年 龄 、 手 术 可 行 性 等 因 素 而 定 , 妇 科 肿 瘤 医 生 将 根 据 个 别 病 患 的 情 况<br />
给 予 建 议 。 至 于 晚 期 癌 症 病 患 的 治 疗 方 法 , 则 采 用 放 射 治 疗 加 化 疗 , 或 是 化 疗 。<br />
“5 年 存 活 率 ”<br />
是 根 据 癌 症 的 阶 段 而 定 :<br />
• 第 1 阶 段 80-90%<br />
• 第 2 阶 段 50-70%<br />
• 第 3 阶 段 20-40%<br />
• 第 4 阶 段 10-20%<br />
值 得 庆 幸 的 是 , 子 宫 颈 癌 是 可 以 预 防 的 。 人 们 可 以 同 时 通 过 HPV 疫 苗 注 射 ( 第 一<br />
级 预 防 ) 与 子 宫 颈 抹 片 检 查 ( 第 二 级 预 防 ) 来 预 防 子 宫 颈 癌 。 目 前 , 市 面 上 有 两 种 疫<br />
苗 : 卉 研 康 (Cervarix) 和 加 德 西 (Gardasil)。 后 者 可 预 防 第 16 型 和 第 18 型 亚 型<br />
病 毒 , 即 导 致 70% 子 宫 颈 癌 病 例 的 高 危 亚 型 病 毒 ; 后 者 除 了 可 预 防 第 16 型 和 第 18<br />
型 亚 型 病 毒 外 , 也 可 预 防 导 致 生 殖 器 疣 的 第 6 型 和 第 11 型 低 危 亚 型 病 毒 。 这 些 疫 苗<br />
适 合 年 龄 介 于 9 岁 至 26 岁 的 女 性 注 射 。 其 中 , 卉 研 康 在 所 有 综 合 诊 疗 所 都 有 提 供 ,<br />
而 且 可 动 用 保 健 储 蓄 支 付 费 用 。 所 有 年 龄 介 于 25 岁 至 65 岁 、 性 生 活 活 跃 的 女 性 , 每<br />
三 年 应 进 行 至 少 一 次 子 宫 颈 抹 片 检 查 。 子 宫 颈 抹 片 检 查 是 检 验 子 宫 颈 癌 的 方 法 。 它<br />
志 在 于 检 验 出 易 于 治 疗 的 子 宫 颈 癌 前 病 变 , 以 避 免 癌 症 的 生 长 。 这 是 一 项 简 单 且 负<br />
担 得 起 的 检 查 , 在 所 有 综 合 诊 疗 所 、 家 庭 诊 所 和 妇 科 诊 所 都 有 提 供 。<br />
以 上 文 章 由 谢 燕 妮 医 生 提 供<br />
MBBS( 新 加 坡 ),MRCOG( 英 国 ),FAMS( 新 加 坡 ),<br />
DGO( 皇 家 澳 大 利 亚 和 新 西 兰 学 院 妇 产 科 ),<br />
GDipHCML( 新 加 坡 管 理 大 学 )<br />
妇 科 肿 瘤 注 册 医 生<br />
竹 脚 妇 幼 医 院 妇 科 癌 症 部 门 主 任 兼 顾 问<br />
新 加 坡 杜 克 — 国 大 医 学 研 究 院 兼 职 助 理 教 授<br />
新 加 坡 国 立 癌 症 中 心 客 座 顾 问<br />
尽 可 能 保 持 活 跃 生 活<br />
多 数 人 在 运 动 后 , 心 情 、 食 欲 和 睡 眠 都 会 比 较<br />
好 。 选 择 一 项 你 喜 欢 的 运 动 或 体 育 项 目 。 即<br />
使 每 天 只 是 短 暂 步 行 , 或 是 骑 脚 车 / 运 动 脚 车 ,<br />
也 能 大 大 提 高 你 的 体 力 。<br />
不 要 操 劳 过 度<br />
先 处 理 那 些 你 认 为 最 重 要 的 事 情 。 有 时 候 , 你<br />
会 觉 得 精 力 充 沛 ; 有 时 , 你 又 会 觉 得 精 神 不 振 。<br />
你 可 以 向 家 人 和 朋 友 寻 求 协 助 。 他 们 可 以 帮 你<br />
准 备 膳 食 、 载 送 你 去 看 医 生 , 或 是 通 过 其 他 方<br />
式 协 助 你 。 凡 事 量 力 而 为 , 不 要 在 一 天 内 进 行<br />
太 多 活 动 。<br />
安 排 适 合 你 的 工 作 计 划<br />
有 些 人 觉 得 自 己 的 身 体 状 况 足 以 应 付 工 作 ,<br />
有 些 人 则 须 放 慢 脚 步 。 需 要 的 话 , 你 可 以 请<br />
病 假 , 以 及 考 虑 向 雇 主 要 求 转 为 兼 职 或 在<br />
家 办 公 。<br />
安 排 时 间 休 息<br />
治 疗 期 间 , 你 需 要 多 休 息 , 尤 其 是 接 受 放 射 治<br />
疗 后 。 每 晚 要 睡 至 少 8 个 小 时 , 白 天 则 可 以 小<br />
睡 片 刻 ( 每 次 不 超 过 1 小 时 )。 研 究 显 示 , 放 松<br />
技 巧 不 但 有 助 减 轻 跟 治 疗 相 关 的 副 作 用 , 也 能<br />
让 那 些 接 受 非 手 术 治 疗 的 癌 症 病 患 调 整 情 绪<br />
(Lubert et al, 2001)。 多 进 行 一 些 能 够 帮 助<br />
你 放 松 心 情 的 活 动 。 无 论 是 听 音 乐 、 观 看 喜 爱<br />
的 电 视 节 目 或 阅 读 , 都 有 助 于 松 懈 身 心 。<br />
子 宫 癌 使 人 在 生 理 和 心 理 上<br />
都 特 别 难 以 应 付 。<br />
应 付 化 疗 的 副 作 用<br />
化 疗 的 副 作 用 可 能 会 引 起 不 适 。 事 先 了 解 化 疗 的<br />
副 作 用 , 可 帮 助 你 更 好 地 应 付 疗 程 。 须 知 的 重 点<br />
是 : 化 疗 的 副 作 用 大 多 数 是 暂 时 性 的 , 疗 程 一 旦<br />
结 束 , 副 作 用 也 会 跟 着 逐 渐 消 失 。 在 你 开 始 接 受<br />
化 疗 前 , 医 生 将 跟 你 解 释 有 关 疗 程 的 副 作 用 。<br />
应 付 放 射 治 疗 的 副 作 用<br />
一 些 治 疗 , 例 如 在 骨 盆 部 位 进 行 放 射 治 疗 , 可 能<br />
导 致 阴 道 干 燥 、 痕 痒 或 有 灼 痛 感 , 使 你 在 性 交 时<br />
感 到 不 适 。 涂 抹 凝 胶 或 药 膏 , 可 缓 解 这 些 副 作<br />
用 。 此 外 , 治 疗 后 留 下 的 疤 痕 , 可 能 会 使 阴 道 狭<br />
小 。 使 用 一 种 叫 做 “ 扩 张 肌 ” 的 装 置 , 有 助 撑 大<br />
狭 小 的 阴 道 。 你 也 可 能 会 出 现 其 他 副 作 用 , 例 如<br />
排 便 习 惯 改 变 、 膀 胱 和 皮 肤 的 不 适 。 在 你 接 受 放<br />
射 治 疗 前 , 一 名 放 射 肿 瘤 科 医 生 将 评 估 你 的 病<br />
情 , 并 解 释 有 关 治 疗 的 程 序 及 其 副 作 用 。 你 可 向<br />
医 生 或 护 士 咨 询 。 他 们 将 根 据 你 的 需 要 , 提 供 适<br />
合 你 的 个 人 建 议 。<br />
应 付 疼 痛<br />
癌 症 患 者 并 不 一 定 会 感 到 疼 痛 。 不 过 , 如 果 你 有<br />
疼 痛 的 话 , 你 可 通 过 药 物 和 其 他 治 疗 来 缓 解 大<br />
部 分 的 疼 痛 。 癌 症 引 起 的 疼 痛 可 以 是 轻 微 的 , 也<br />
可 以 非 常 严 重 ; 有 时 会 比 平 常 来 得 更 痛 。 疼 痛 可<br />
能 由 癌 症 或 治 疗 引 起 , 或 两 者 皆 有 。 你 也 可 能 会<br />
有 与 癌 症 无 关 的 疼 痛 。 有 些 人 会 经 常 头 痛 和 肌<br />
肉 酸 痛 。 请 向 你 的 医 生 、 护 士 和 其 他 人 咨 询 控 制<br />
疼 痛 的 最 佳 方 法 , 并 且 在 服 用 非 处 方 药 之 前 , 向<br />
你 的 医 生 查 问 清 楚 。<br />
性 欲<br />
许 多 妇 女 在 进 行 子 宫 切 除 术 后 感 到 失 落 , 觉 得<br />
自 己 缺 少 了 女 性 特 质 。 如 果 你 还 没 有 进 入 更 年 期 ,<br />
你 就 必 须 接 受 无 法 生 育 的 事 实 。 放 射 治 疗 的 副<br />
作 用 , 例 如 疲 劳 或 疼 痛 , 也 可 能 会 降 低 你 的 性 欲 。<br />
如 果 你 有 上 述 情 况 , 你 绝 对 不 是 独 立 个 案 。<br />
有 时 候 , 失 去 性 欲 会 使 你 无 法 享 受 跟 伴 侣 之 间 的<br />
亲 密 接 触 。 如 果 你 对 重 新 展 开 性 生 活 感 到 惶 恐<br />
不 安 , 就 给 自 己 多 一 些 时 间 。 更 重 要 的 是 , 跟 伴<br />
侣 一 起 讨 论 , 共 同 找 出 对 彼 此 最 好 的 解 决 方 法 。<br />
对 多 数 人 而 言 , 情 况 会 随 着 时 间 的 流 逝 而 好 转 。<br />
切 记 , 你 随 时 都 可 以 主 动 向 医 生 或 护 士 咨 询 关<br />
于 性 关 系 的 问 题 。 如 果 你 愿 意 , 也 可 以 要 求 转 介<br />
到 专 家 或 专 科 医 生 , 向 他 们 求 助 。 本 地 也 有 一 些<br />
由 其 他 面 对 同 样 经 历 的 妇 女 所 组 成 的 互 助 小 组 ,<br />
她 们 会 定 期 见 面 , 分 享 经 验 。<br />
参 考 资 料<br />
C.H. Yarbro、M.H. Frogge 和 M. Goodman<br />
(1999 年 ),《 癌 症 症 状 管 理 》( 第 二 版 ),<br />
Boston: Jones and Bartlett Publishers<br />
Luebbert, K.、Dahmeb, B 和 Hasenbring,<br />
M.(2001 年 ), 回 顾 分 析 : 放 松 疗 法 在 纾 缓<br />
跟 治 疗 有 关 症 状 和 改 善 急 性 非 手 术 癌 症 治<br />
疗 的 情 绪 方 面 的 有 效 性 ,《 心 理 肿 瘤 学 》,<br />
10: 490-502。<br />
www.gyncancer.com/uterus.html<br />
www.cancer.gov/cancertopics/coping/<br />
physicaleffects#Fatigue<br />
张 業 苓<br />
高 级 护 理 经 理<br />
癌 症 教 育 与 资 讯 服 务
PAGE B8<br />
Outreach<br />
SALUBRIS<br />
September / October 2011<br />
UPCOMING PUBLIC EDUCATION<br />
ACTIVITIES / PROGRAMMES<br />
LAYING THE TRACKS<br />
FOR DUKE-NUS’ FUTURE<br />
CLINICIAN SCIENTISTS<br />
PAGE A5<br />
People<br />
SALUBRIS<br />
September / October 2011<br />
Event Name Date, Time, Venue Registration Details<br />
NCCS TEAM LENDS EXPERTISE IN CURRICULUM DEVELOPMENT<br />
Breast <strong>Cancer</strong><br />
Awareness Month<br />
English Public Forum –<br />
KEEP ABREAST FOR HEALTH<br />
TOPICS:<br />
a. Early Detection & Screening<br />
b. Common Breast Problems & Diagnosis<br />
c. Treatment Options<br />
15 October 2011, Saturday<br />
9.30am to 1.30pm<br />
Auditorium, Level 4<br />
<strong>National</strong> <strong>Cancer</strong> <strong>Centre</strong> <strong>Singapore</strong><br />
Admission fee: $5<br />
To register, please call: 6225 5655 or register<br />
online: www.nccs.com.sg (click events).<br />
The challenge for a group of NCCS doctors and scientist was daunting. On their<br />
shoulders rest the responsibility to draw up the curriculum and conduct the training for<br />
the pioneering group of clinician scientists.<br />
Undaunted, they gave their best shot, juggling between their clinics at NCCS and the<br />
Duke-NUS Medical School. Their efforts paid off when the first batch of 24 medical<br />
students graduated in July this year amid much fanfare.<br />
<strong>Cancer</strong>Wise Workshop –<br />
Coping with <strong>Cancer</strong><br />
TOPICS:<br />
a. Understanding your reactions and<br />
feelings towards the cancer<br />
b. Coping and adjustment to life after<br />
cancer treatment (Part 1)<br />
c. Coping and adjustment to life after<br />
cancer treatment (Part 2)<br />
d. Coping strategies<br />
22 October 2011, Saturday<br />
Session will be conducted in English.<br />
1pm<br />
– Registration<br />
1.30pm to 4pm – Workshop<br />
Function Room, Level 4<br />
<strong>National</strong> <strong>Cancer</strong> <strong>Centre</strong> <strong>Singapore</strong><br />
Admission fee: $5<br />
To register, please call: 6225 5655 or register<br />
online: www.nccs.com.sg (click events).<br />
The work of the pioneers from NCCS did not go unnoticed. They were among<br />
those named in the Faculty Awards 2011, namely, Prof Kon Oi Lian and<br />
Prof Koong Heng Nung for the Pioneer Award and Outstanding Educator<br />
Award; and A/Prof Patrick Tan and A/Prof Ha Tam Cam for the Pioneer Award.<br />
Indeed the challenges of drawing up a good curriculum were multiple-pronged<br />
as Prof Kon reflected on her task. She had worked with A/Prof Patrick Tan in<br />
developing the course on “Molecules and Cells”. They had to take into account<br />
the student’s expectations, some of whom had thought that the programme was a<br />
replication of the one in Duke University in the US.<br />
Then there was the added challenge to set up a local faculty staff with the relevant<br />
knowledge and willingness to be content experts in specialised topics.<br />
Public Forum on Pain<br />
& Palliative Care<br />
TOPICS:<br />
a. <strong>Cancer</strong> Pain: Myths and Reality<br />
b. What is Palliative Care and how can<br />
it help?<br />
c. Palliative Care services in <strong>Singapore</strong><br />
19 November 2011, Saturday<br />
Session will be conducted in both<br />
English & Chinese<br />
9.00am to 3pm<br />
The URA <strong>Centre</strong><br />
Function Hall (Level 5)<br />
Maxwell Road<br />
<strong>Singapore</strong> 069118<br />
Admission fee: $5<br />
To register, please call: 6225 5655 or register<br />
online: www.nccs.com.sg (click events).<br />
For A/Prof Tan, the tight timeline was his challenge. Fresh from attending a course<br />
on Team-Based Learning at Wright State University, he found himself having to put<br />
to good use his newly acquired skills.<br />
An added difficulty was the need to make it tightly aligned to the module at Duke<br />
University and to get the approval of the local faculty.<br />
”We were keenly aware that many key<br />
Duke-NUS stakeholders would be observing<br />
the performance of the students in the course.<br />
We needed toensure that the course was<br />
executed smoothly and without hiccups.”<br />
A/Prof Patrick Tan<br />
A/PR<strong>OF</strong> PATRICK TAN<br />
Continued on page A6.
PAGE A6<br />
People<br />
SALUBRIS<br />
September / October 2011<br />
LAYING THE TRACKS<br />
FOR DUKE-NUS’ FUTURE<br />
CLINICIAN SCIENTISTS<br />
PAGE A7<br />
People<br />
SALUBRIS<br />
September / October 2011<br />
Continued from page B3.<br />
The local faculty developed a curriculum that supplemented the<br />
video lectures and programme provided by Duke University. For<br />
the students, they benefited from learning from a one-of-a-kind<br />
programme where they could acquire knowledge from the<br />
What needs to be addressed now is how the curriculum can continue<br />
to be engaging for the next batch of students. Both professors already<br />
have some new learning strategies in mind. Their priority is to put<br />
together materials that maximise the students’ learning.<br />
best of two worlds – a leading medical college and a leading<br />
medical institution.<br />
“The Duke-NUS students are working hard to master two<br />
courses, albeit complementary, simultaneously. They became<br />
highly motivated and driven for success.”<br />
“The students can learn how to prioritise their preparation for<br />
class sessions with clearer direction from the faculty. It may<br />
help that they understand the rational framework for each topic<br />
before the inundation of facts and factoids. Reading materials<br />
can also be more appropriately selected and realistically scaled<br />
to the preparation time that students have.”<br />
Prof Kon Oi Lian<br />
Prof Koong Heng Nung<br />
The Team-Based Learning approach was strongly advocated throughout the course<br />
developed by Prof Kon and A/Prof Tan. It requires the students to be divided into<br />
teams of six to eight students. They take their assignments as a team and grades<br />
were assigned on individual and team performance.<br />
To ensure the programme’s effectiveness, the faculty had to produce preparatory<br />
and class room materials that were well designed and of high standards. To<br />
supplement and complement the US and <strong>Singapore</strong> content, it introduced short<br />
test questions and proof of application.<br />
A/Prof Tan believes that the new curriculum should also be about helping the<br />
students focus on what is really important and to make them feel the pulse of<br />
research. “One important work-in-progress we have lies in getting the faculty<br />
members to list the key learning objectives of each team-based learning session<br />
and striking a balance between pet topics of faculty members and key general<br />
concepts. We should also get students to be excited about research, and let<br />
them witness how discoveries, translated from bench to bedside, can radically<br />
transform and improve clinical practice. If we can achieve this, then I am sure<br />
we have succeeded.”<br />
According to Prof Kon, the approach not only benefitted the students<br />
but also the faculty.<br />
“It relieved the faculty from doing all the work during lectures,<br />
placing the responsibility of learning squarely on the students and<br />
offering great potential for developing deep learning. Students were<br />
able to acquire collegial skills of working in teams and to develop<br />
firm friendships.”<br />
Another innovation is the availability of all lectures on<br />
hard-drives before the commencement of the course.<br />
This way the students can prepare for their classes ahead<br />
of time and spend class time working on their assignments.<br />
Added Prof Kon, “We all learned a good deal of what it took to make learning<br />
interesting, stimulating and enduring.”<br />
PR<strong>OF</strong> KON OI LIAN<br />
Despite the high demands on the students, they<br />
graduated with flying colours.<br />
Prof Kon said that the curriculum has been<br />
helpful in getting the students to achieve<br />
success. “My impression is that although the<br />
students continually find the curriculum and<br />
learning methods rather challenging, they do<br />
enjoy learning in teams, acquiring confidence<br />
to explain their answers and pursuing areas of<br />
doubt to clear resolution.”<br />
The commitment shown by our clinicians and scientists in their quest<br />
for a better curriculum has also made an impression on the current<br />
batch of students such as Mr Christopher Ross Schlieve of Class<br />
2013. Motivated by Prof Koong, who was conferred the Pioneer and<br />
Outstanding Educator Awards. Mr Schlieve decided to enroll into the<br />
surgical clerkship elective and has not looked back since.<br />
He said ”Prof Koong is constantly thinking of new and unique ways to engage us<br />
as learners. He has devised a multitude of learning tools that has maximised our<br />
learning within the clerkship.”<br />
His colleague, Ms Fatima Usmani could not agree more. “Prof Koong’s<br />
commitment to our learning made itself evident repeatedly during our surgical<br />
clerkship as he taught me and my colleagues to extract valuable conceptual<br />
lessons from seemingly mundane clinical experience. By glancing at our answers,<br />
addressing our approaches and giving us constructive feedback, he effectively<br />
created an environment in which we were able to question, reflect, learn from one<br />
another, and address our own weaknesses.”<br />
PR<strong>OF</strong> KOONG HENG NUNG<br />
To date, 16 NCCS staff members are<br />
holding teaching positions at the<br />
medical school. NCCS Director Prof Soo<br />
Khee Chee leads the team as the Duke-<br />
NUS Vice Dean of Clinical and Faculty<br />
Affairs. In shouldering this added<br />
responsibility they are paving the way<br />
for NCCS to attain its goal of becoming<br />
a global leading cancer centre in patient<br />
care and research, as well as education.<br />
By Veronica Lee
PAGE A8<br />
Community<br />
SALUBRIS<br />
September / October 2011<br />
BE IT THROUGH CORPORATE<br />
OR INDIVIDUAL GIVING,<br />
IT CAN BE YOUR WAY <strong>OF</strong> <strong>LIFE</strong><br />
CANCER CARE FOR THE NEEDY<br />
CANCER RESEARCH FOR BETTER CARE & HOPE FOR CURE<br />
Editorial Advisors<br />
Dr Kon Oi Lian<br />
Prof Soo Khee Chee<br />
Executive Editors<br />
Ms Charissa Eng<br />
Ms Veronica Lee<br />
Mr Sunny Wee<br />
Contributing Editor<br />
Dr Wong Nan Soon<br />
Members, Editorial Board<br />
Mr Mark Ko<br />
Ms Sharon Leow<br />
Dr Shiva Sarraf-Yazdi<br />
Ms Jenna Teo<br />
Medical Editor<br />
Dr Richard Yeo<br />
Members, Medical Editorial Board<br />
Ms Lita Chew<br />
Dr Mohd Farid<br />
Dr Melissa Teo<br />
Dr Teo Tze Hern<br />
Dr Deborah Watkinson<br />
is produced with you<br />
SALUBRIS in mind. If there are other<br />
topics related to cancer that you would like to read about<br />
or if you would like to provide some feedback on the<br />
articles covered, please email to salubris@nccs.com.sg.<br />
NATIONAL CANCER CENTRE SINGAPORE<br />
Reg No 199801562Z<br />
11 Hospital Drive <strong>Singapore</strong> 169610<br />
Tel: (65) 6436 8000 Fax: (65) 6225 6283<br />
www.nccs.com.sg