

Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC
Invasive breast carcinoma - IARC

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
aged women (average age of presentation<br />
is 40-50 years) around 15-20 years<br />
older than for FAs.<br />
In Asian countries, PTs occur at a younger<br />
age (average 25-30 years) {487}.<br />
Malignant PTs develop on average 2-5<br />
years later than benign PTs. Among<br />
Latino whites, especially those born in<br />
Central and South America, malignant<br />
phyllodes is more frequent {254}.<br />
Isolated examples of PTs in men have<br />
been recorded {1424a,2023}.<br />
Aetiology<br />
P Ts are thought to be derived fro m<br />
intralobular or periductal stroma. They<br />
may develop de novo or from FAs. It is<br />
possible, in rare cases, to demonstrate<br />
the presence of a pre-existing FA adjacent<br />
to a PT.<br />
Clinical features<br />
Usually, patients present with a unilateral,<br />
firm, painless <strong>breast</strong> mass, not attached<br />
to the skin. Very large tumours (>10 cm)<br />
may stretch the skin with striking distension<br />
of superficial veins, but ulceration is<br />
very rare. Due to mammographic screening,<br />
2-3 cm tumours are becoming more<br />
common, but the average size remains<br />
around 4-5 cm {775,2425}. Bloody nipple<br />
discharge caused by spontaneous<br />
i n f a rction of the tumour has been<br />
described in adolescent girls {1781,<br />
2833}. Multifocal or bilateral lesions are<br />
rare {1932}.<br />
Imaging reveals a rounded, usually<br />
sharply defined, mass containing clefts<br />
or cysts and sometimes coarse calcifications.<br />
Macroscopy<br />
P Ts form a well circumscribed firm ,<br />
bulging mass. Because of their often<br />
clearly defined margins, they are often<br />
shelled out surgically.<br />
The cut surface is tan or pink to grey and<br />
may be mucoid. The characteristic<br />
whorled pattern with curved clefts<br />
resembling leaf buds is best seen in<br />
large lesions, but smaller lesions may<br />
have an homogeneous appearance.<br />
Haemorrhage or necrosis may be present<br />
in large lesions.<br />
Histopathology<br />
PTs typically exhibit an enhanced intracanalicular<br />
growth pattern with leaf-like<br />
p rojections into dilated lumens. The<br />
epithelial component consists of luminal<br />
A<br />
B<br />
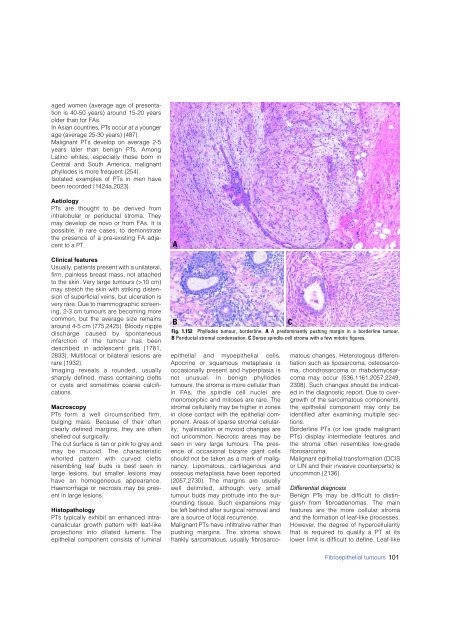
Fig. 1.152 Phyllodes tumour, borderline. A A predominantly pushing margin in a borderline tumour.<br />
B Periductal stromal condensation. C Dense spindle-cell stroma with a few mitotic figures.<br />
C<br />
epithelial and myoepithelial cells.<br />
Apocrine or squamous metaplasia is<br />
occasionally present and hyperplasia is<br />
not unusual. In benign phyllodes<br />
tumours, the stroma is more cellular than<br />
in FAs, the spindle cell nuclei are<br />
monomorphic and mitoses are rare. The<br />
stromal cellularity may be higher in zones<br />
in close contact with the epithelial component.<br />
Areas of sparse stromal cellularity,<br />
hyalinisation or myxoid changes are<br />
not uncommon. Necrotic areas may be<br />
seen in very large tumours. The presence<br />
of occasional bizarre giant cells<br />
should not be taken as a mark of malignancy.<br />
Lipomatous, cartilagenous and<br />
osseous metaplasia have been reported<br />
{2057,2730}. The margins are usually<br />
well delimited, although very small<br />
tumour buds may protrude into the surrounding<br />
tissue. Such expansions may<br />
be left behind after surgical removal and<br />
are a source of local recurrence.<br />
Malignant PTs have infiltrative rather than<br />
pushing margins. The stroma shows<br />
frankly sarcomatous, usually fibrosarcomatous<br />
changes. Heterologous differentiation<br />
such as liposarcoma, osteosarcoma,<br />
chondrosarcoma or rhabdomyosarcoma<br />
may occur {536,1161,2057,2249,<br />
2308}. Such changes should be indicated<br />
in the diagnostic report. Due to overgrowth<br />
of the sarcomatous components,<br />
the epithelial component may only be<br />
identified after examining multiple sections.<br />
Borderline PTs (or low grade malignant<br />
PTs) display intermediate features and<br />
the stroma often resembles low-grade<br />
fibrosarcoma.<br />
Malignant epithelial transformation (DCIS<br />
or LIN and their invasive counterparts) is<br />
uncommon {2136}.<br />
Differential diagnosis<br />
Benign PTs may be difficult to distinguish<br />
from fibroadenomas. The main<br />
f e a t u res are the more cellular stro m a<br />
and the formation of leaf-like pro c e s s e s .<br />
H o w e v e r, the degree of hyperc e l l u l a r i t y<br />
that is re q u i red to qualify a PT at its<br />
lower limit is difficult to define. Leaf-like<br />
Fibroepithelial tumours 101













