Differential Diagnosis of Dementias - Alzheimer's Association
Differential Diagnosis of Dementias - Alzheimer's Association
Differential Diagnosis of Dementias - Alzheimer's Association

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Differential</strong> <strong>Diagnosis</strong> <strong>of</strong> <strong>Dementias</strong><br />
George T. Grossberg, MD<br />
Samuel W. Fordyce Distinguished Pr<strong>of</strong>essor<br />
Director, Geriatric Psychiatry<br />
Department <strong>of</strong> Neurology & Psychiatry<br />
St Louis University School <strong>of</strong> Medicine
Disclosures<br />
• None for this presentation<br />
2
<strong>Differential</strong> <strong>Diagnosis</strong> <strong>of</strong> <strong>Dementias</strong><br />
Presentation Overview<br />
• Clinical evaluation for dementia<br />
• Cognitive assessment tools<br />
• Pr<strong>of</strong>iles <strong>of</strong> common dementias<br />
• Imaging the different dementias<br />
• Neuropsychiatric symptoms in dementias<br />
3
Common Types <strong>of</strong> Neurodegenerative<br />
Dementia 1<br />
• Alzheimer’s dementia (AD)<br />
• Parkinson’s disease dementia (PDD)<br />
• Dementia with Lewy bodies (DLB)<br />
• Vascular dementia (VaD)<br />
• Frontotemporal dementia (FTD)<br />
Lewy Body<br />
Dementia<br />
Spectrum 2<br />
• Mixed (multiple pathologies/etiologies) dementia<br />
1. American Psychiatric <strong>Association</strong>. Diagnostic and Statistical Manual <strong>of</strong> Mental Disorders. Fourth Edition. Text Revision. (DSM-IV-TR ® .) Washington, DC: American<br />
Psychiatric <strong>Association</strong>; 2000.<br />
2. Lewy Body Dementia <strong>Association</strong>, Inc. 2010. Caregiver Burden in Lewy Body <strong>Dementias</strong>: Challenges in Obtaining <strong>Diagnosis</strong> and Providing Daily Care. Atlanta, GA:<br />
Lewy Body Dementia <strong>Association</strong>; 2010.<br />
4
The Typical Dementia Scenario<br />
• Patients may not seek medical care for symptoms<br />
• Lack <strong>of</strong> insight common<br />
• Patient denies problem, family/friends express<br />
concerns<br />
• Caregivers may gradually compensate and cover<br />
up symptoms for the patient, "masking" the true<br />
magnitude <strong>of</strong> the deficits<br />
• Delayed diagnosis until moderate stage<br />
Agronin ME. Alzheimer disease and other dementias : a practical guide. 2nd ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008.<br />
5
Core features <strong>of</strong> degenerative dementia<br />
• Deficits in cognitive domains that may include<br />
memory<br />
• Usually progressive deterioration<br />
• Cognitive impairment interferes with social or<br />
occupational function<br />
• Not attributable to another disorder<br />
American Psychiatric <strong>Association</strong>. Diagnostic and Statistical Manual <strong>of</strong> Mental Disorders. Fourth Edition. Text Revision. (DSM-IV-TR ® .) Washington, DC:<br />
American Psychiatric <strong>Association</strong>; 2000.<br />
6
Clinical Evaluation for Dementia 1<br />
History<br />
Physical,<br />
Neurologic,<br />
Mental Status<br />
Examinations<br />
• Obtain medical and psychiatric history, along<br />
with current symptoms<br />
• Include collateral source such as family or<br />
other informant<br />
• Identify neurologic deficits<br />
• Conduct general screen for cognitive<br />
impairment<br />
Laboratory,<br />
Psychiatric, and<br />
Neuropsych Tests<br />
• Identify reversible causes <strong>of</strong> cognitive<br />
impairment<br />
• Build on mental status examination, and<br />
provide clearer picture <strong>of</strong> pattern and degree<br />
<strong>of</strong> cognitive impairment<br />
Agronin ME. Alzheimer disease and other dementias : a practical guide. 2nd ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008.<br />
7
The “Dementia Workup”<br />
• Detailed history from patient & reliable informant<br />
• Head to toe physical & neurological examination<br />
• Bloodwork(if not done recently)-<br />
CMP;CBC;TSH;B12/Folate; ?vit<br />
D;?CRP;?Homocysteine<br />
• RPR, HIV testing(if indicated)<br />
• Plain CT/MRI(one time);?FDG-PET;?amyloid-<br />
PET<br />
• UA;CXRY(if indicated);EKG<br />
• EEG,LP- not part <strong>of</strong> routine workup<br />
8
Delirium is a Reversible Cause <strong>of</strong> Cognitive<br />
Impairment<br />
Dehydration<br />
Electrolyte/Endocrine disorder<br />
Lack <strong>of</strong> oxygen<br />
Injury/Impaction<br />
Rule out psychiatric disorder<br />
Infection<br />
Urinary retention/Unfamiliar environment<br />
Medications<br />
Desai AK, Grossberg GT. Psychiatric consultation in long-term care : a guide for health care pr<strong>of</strong>essionals. Baltimore: Johns Hopkins University Press; 2010.<br />
9
Delirium, Dementia, and Depression 1,2<br />
Delirium Dementia Depression<br />
Onset Sudden Insidious Recent or recurrent<br />
Duration<br />
Minutes to<br />
days<br />
Months to years<br />
Weeks to months<br />
Progression<br />
Reversible –<br />
resolves with<br />
treatment<br />
Irreversible<br />
Reversible, relapses<br />
common<br />
Consciousness Fluctuating Generally alert<br />
Generally alert,<br />
possibly withdrawn<br />
History <strong>of</strong><br />
depression<br />
Usually<br />
negative<br />
Usually negative<br />
Usually positive<br />
Visuospatial Preserved Often abnormal Preserved<br />
Mood – Sadness/<br />
Guilt/Worthlessness<br />
Absent Usually absent Usually Present<br />
1. Cefalu C, Grossberg GT. Leawood, KS: American Academy <strong>of</strong> Family Physicians; 2001. 2. American Psychiatric <strong>Association</strong>. DSM-IV-TR ® .<br />
Washington, DC: American Psychiatric <strong>Association</strong>; 2000.<br />
10
Examples <strong>of</strong> Cognitive Assessment Tools<br />
for the Office Setting<br />
• Mini-Mental State Examination (MMSE) 1<br />
• AD8 informant interview 2<br />
• Mini-Cog assessment 3<br />
• Montreal Cognitive Assessment (MoCA) 4<br />
• St Louis University Mental Status (SLUMS)<br />
Examination 5<br />
Note. These are assessment tools, and are not fully diagnostic <strong>of</strong> dementia.<br />
1. Folstein MF et al. J Psychiatr Res. 1975;12:189-198. 2. Galvin JE et al. Neurology. 2005;65:559-564. 3. Borson S et al. Int J Geriatr Psychiatry.<br />
2000;15:1021-1027. 4. Nasreddine ZS et al. J Am Geriatr Soc. 2005;53:695-699. 5. Tariq SH et al. Am J Geriatr Psychiatry. 2006;14:900-910.<br />
11
Mini-Mental State Examination (MMSE)<br />
• Brief, structured mental status<br />
examination for global cognitive<br />
function 1<br />
• Typical deterioration <strong>of</strong> 3–4 points<br />
per year in a person with AD 2<br />
• Sensitivity and specificity vary in<br />
different patient populations 3<br />
• May be necessary to account for<br />
differences due to age, education,<br />
and ethnicity/race 3<br />
• Does not specifically test episodic<br />
memory 1<br />
• Copyright issues 3<br />
Score range, 0–30 1,3<br />
≥28<br />
Unimpaired*<br />
20–27 Mild AD<br />
10–19 Moderate AD<br />
The Informant Interview: The AD8<br />
• Informant-based questionnaire<br />
– Can be administered at home or<br />
in waiting room<br />
– Yes/No format<br />
• Detects change in individuals compared<br />
with previous level<br />
<strong>of</strong> function<br />
– No need for baseline assessment<br />
– Patients serve as their own control<br />
– Minimally affected by age, gender,<br />
race, and education<br />
• Brief (
Rapid Screen for<br />
Cognitive Impairment: Mini-Cog<br />
• Rapid screen for cognitive<br />
impairment<br />
Mini-Cog<br />
– 5 minutes to administer<br />
• 3-word registration<br />
• Simple clock-drawing test<br />
• 3-item recall<br />
• Not influenced by education<br />
level or language<br />
Recall 0 Recall 1-2 Recall 3<br />
Demented<br />
Nondemented<br />
• Sensitivity, 99%<br />
• Specificity, 93%<br />
Abnormal Clock<br />
Demented<br />
Normal Clock<br />
Nondemented<br />
Adapted from Borson S et al. Int J Geriatr Psychiatry. 2000;15:1021-1027; with permission.<br />
Borson S et al. Int J Geriatr Psychiatry. 2000;15:1021-1027.<br />
14
Montreal Cognitive Assessment (MoCA)<br />
• Brief (10-min) cognitive<br />
screening test sensitive to<br />
domains involved in AD 1<br />
• Demonstrated utility in PDD 2<br />
• Includes measures in<br />
executive function 1<br />
• Established utility in a multiple<br />
settings 1,2<br />
• Test free for nonpr<strong>of</strong>it use:<br />
http://www.mocatest.org/<br />
Image: The Montreal Cognitive Assessment. December 17, 2009. http://www.mocatest.org/. Accessed December 17, 2009; with permission.<br />
1. Nasreddine ZS et al. J Am Geriatr Soc. 2005;53:695-699. 2. Hoops S, Nazem S, Siderowf AD, et al. Nov 24 2009;73(21):1738-1745.<br />
15
Saint Louis University Mental Status<br />
Examination<br />
• Designed to improve screening for mild<br />
neurocognitive disorder (MNCD)<br />
• 11-item, clinician-scored scale<br />
High School<br />
Education<br />
Less Than High<br />
School Education<br />
Normal 27–30 25–30<br />
MNCD 21–26 20–24<br />
Dementia 1–20 1–19<br />
• Study <strong>of</strong> SLUMS vs MMSE (N = 705)<br />
– DSM-IV-TR ® criteria used to diagnose MNCD<br />
or dementia<br />
– Patients assessed by MMSE and SLUMS<br />
– Sensitivity and specificity<br />
• Dementia: similar for MMSE and SLUMS<br />
• MNCD: SLUMS appears superior to MMSE<br />
Tariq SH et al. Am J Geriatr Psychiatry. 2006;14:900-910.<br />
16
Rapid Brief Cognitive Screens:<br />
Pros and Cons<br />
Screening Test Pros Cons<br />
MMSE 1,2<br />
Widely used, validated, reliable<br />
Adjustments for age, education, and<br />
race may be necessary<br />
Copyright issues<br />
AD8 informant<br />
interview 3<br />
Mini-Cog<br />
assessment 4<br />
MoCA 5,6<br />
SLUMS<br />
examination 7<br />
Reliable, sensitive, specific, rapidly administered<br />
Superior to MMSE in prediction <strong>of</strong> dementia<br />
status, rapidly administered, produces a visible<br />
performance indicator<br />
Useful in patients with scores >25 on MMSE,<br />
strong executive function component<br />
Potentially superior to MMSE for early detection <strong>of</strong><br />
cognitive impairment<br />
Knowledgeable informants may not be<br />
readily available<br />
Clock-drawing test scoring is vulnerable<br />
to varying interpretations<br />
Conclusions regarding validity in PDD<br />
restricted to specialty clinic setting<br />
Research needed to confirm applicability<br />
beyond initial study group<br />
Note: insufficient information is available to determine whether any one screening tool is superior to another. Positive<br />
screening results should be followed by complete neurologic and medical examinations.<br />
1. Folstein MF et al. J Psychiatr Res. 1975;12:189-198. 2. Weiner MF, Garrett MD, Bret ME. Neuropsychiatric Assessment and <strong>Diagnosis</strong>. In: Weiner<br />
MF, Lipton AM, eds. Textbook <strong>of</strong> Alzheimer disease and other dementias. Washington, DC: American Psychiatric Pub.; 2009. 3. Galvin JE et al.<br />
Neurology. 2005;65:559-564. 4. Borson S et al. Int J Geriatr Psychiatry. 2000;15:1021-1027. 5. Nasreddine ZS et al. J Am Geriatr Soc. 2005;53:695-<br />
699. 6. Zadik<strong>of</strong>f C et al. Mov Disord. 2008;23:297-299. 7. Tariq SH et al. Am J Geriatr Psychiatry. 2006;14:900-910.<br />
17
Pr<strong>of</strong>iles <strong>of</strong> <strong>Dementias</strong>
Core<br />
Clinical<br />
Alzheimer’s Dementia<br />
• Multiple cognitive deficits, consisting <strong>of</strong><br />
memory impairment and ≥1 1<br />
– Aphasia<br />
– Apraxia<br />
– Agnosia<br />
– Executive function<br />
• Each deficit causes significant impairment<br />
in social or occupational functioning 1<br />
Language<br />
Praxis<br />
Gnosis<br />
• Difficulty learning and remembering<br />
new information 2<br />
• Repetitiveness, anomia 2<br />
• Poor orientation to time 2<br />
AD largely<br />
involves<br />
temporalparietal<br />
deficits 3<br />
1. American Psychiatric <strong>Association</strong>. Diagnostic and Statistical Manual <strong>of</strong> Mental Disorders. Fourth Edition. Text Revision. (DSM-IV-TR ® .) Washington, DC: American<br />
Psychiatric <strong>Association</strong>; 2000. 2. Geldmacher D. Alzheimer’s Disease. In: Weiner MF, Lipton AM, eds. Textbook <strong>of</strong> Alzheimer disease and other dementias. 1st ed.<br />
Washington, DC: American Psychiatric Pub.; 2009. 3. Tarawneh R, Galvin JE. Dementia with Lewy Bodies and other Synucleinopathies. In: Weiner MF, Lipton AM,<br />
eds. Textbook <strong>of</strong> Alzheimer disease and other dementias. 1st ed. Washington, DC: American Psychiatric Pub.; 2009.<br />
19
Core<br />
Clinical<br />
Parkinson’s Disease Dementia<br />
• Develops in the context <strong>of</strong> established PD (>2<br />
years) 1<br />
• Cognitive and motor slowing with significant<br />
impairments in: 1,2<br />
– Executive function<br />
– Memory retrieval<br />
• A decline from premorbid levels, with deficits<br />
sufficient to impair function 1,2<br />
• Slowing <strong>of</strong> cognitive processes/processing<br />
speed 2<br />
• Fluctuating attention deficits 2<br />
PDD affects the<br />
basal ganglia<br />
first, and<br />
disrupts<br />
ascending<br />
subcortical<br />
circuits 3<br />
• Difficulties with abstraction and visuospatial<br />
skills 2<br />
1. American Psychiatric <strong>Association</strong>. Diagnostic and Statistical Manual <strong>of</strong> Mental Disorders. Fourth Edition. Text Revision. (DSM-IV-TR ® .) Washington, DC: American Psychiatric<br />
<strong>Association</strong>; 2000. Emre M, Aarsland D, Brown R, et al. Mov Disord. Sep 15 2007;22(12):1689-1707; quiz 1837. 3. Tarawneh R, Galvin JE. Dementia with Lewy Bodies and 20<br />
other Synucleinopathies. In: Weiner MF, Lipton AM, eds. Textbook <strong>of</strong> Alzheimer disease and other dementias. 1st ed. Washington, DC: American Psychiatric Pub.; 2009.
Core<br />
Clinical<br />
Dementia with Lewy Bodies<br />
• Fluctuating cognition with pronounced<br />
variations in attention and alertness 1<br />
• Recurrent detailed visual hallucinations,<br />
• Spontaneous features <strong>of</strong> parkinsonism 1<br />
• Suggestive features 1<br />
• REM sleep behavior disorder<br />
• Severe neuroleptic sensitivity<br />
• Impairment in attention, visual perception<br />
and visual construction 1<br />
• Memory is relatively spared early on, but<br />
deficit evident with progression 1<br />
• Cognitive and motor symptoms <strong>of</strong>ten copresent<br />
DLB has basal<br />
ganglia,<br />
transitional,<br />
cortical forms 2<br />
1. McKeith IG, et al. Neurology. 2005;65:1863-1872. 2. Tarawneh R, Galvin JE. Dementia with Lewy Bodies and other Synucleinopathies. In: Weiner MF,<br />
Lipton AM, eds. Textbook <strong>of</strong> Alzheimer disease and other dementias. 1st ed. Washington, DC: American Psychiatric Pub.; 2009.<br />
21
Core<br />
Clinical<br />
Vascular Dementia<br />
• Decline in cognitive function from a<br />
prior baseline and a deficit in<br />
performance in ≥2 1<br />
– Executive/attention<br />
– Memory (may not always be impaired) 2<br />
– Language<br />
– Visuospatial function<br />
• Evidence <strong>of</strong> cerebrovascular<br />
disease via neuroimaing 1,3,4<br />
• Focal neurological signs that<br />
may relate to vascular lesion<br />
location 1,3,4<br />
• Cognitive deficits may occur in<br />
a stepwise fashion 1,3,4<br />
1. Gorelick PB, Scuteri A, Black SE, et al. Stroke. Sep 2011;42(9):2672-2713. 2. Szoeke CE, Campbell S, Chiu E. Vascular Cognitive Disorder. In: Weiner MF,<br />
Lipton AM, eds. Textbook <strong>of</strong> Alzheimer disease and other dementias. Washington, DC: American Psychiatric Pub.; 2009. 3. American Psychiatric <strong>Association</strong>.<br />
Diagnostic and Statistical Manual <strong>of</strong> Mental Disorders. Fourth Edition. Text Revision. (DSM-IV-TR ® .) Washington, DC: American Psychiatric <strong>Association</strong>; 2000.<br />
22<br />
4. Roman GC, Tatemichi TK, Erkinjuntti T, et al. Neurology. Feb 1993;43(2):250-260.
Frontotemporal Dementia<br />
• FTD may be classified into various subtypes 1,2<br />
– Primary progressive aphasia (PPA)<br />
• Progressive nonfluent aphasia<br />
• Logopenic variant<br />
• Semantic dementia (SD)<br />
– Behavioral Variant (bvFTD)<br />
• PPA primarily affects language early, whereas<br />
bvFTD may be classified as an early behavioral<br />
disorder 1<br />
• FTD variants may overlap later in the disease<br />
course 1,2<br />
1. Lipton AM, Boxer A. Frontotemporal Dementia. In: Weiner MF, Lipton AM, eds. Textbook <strong>of</strong> Alzheimer disease and other dementias. Washington, DC:<br />
American Psychiatric Pub.; 2009.2. Gorno-Tempini ML, Hillis AE, Weintraub S, et al. Neurology. Mar 15 2011;76(11):1006-1014.<br />
23
Core<br />
Clinical<br />
Behavioral Variant <strong>of</strong> Frontal Temporal<br />
Dementia<br />
• Progressive deterioration <strong>of</strong> behavior<br />
and/or cognition with ≥ 3 early: 1<br />
– Behavioral disinhibition<br />
– Apathy<br />
– Loss <strong>of</strong> sympathy/empathy<br />
– Perseverative, stereotyped or<br />
compulsive behavior<br />
– Hyperorality<br />
– Executive deficits with relative<br />
sparing <strong>of</strong> memory and visuospatial<br />
function<br />
• Frontal and/or anterior temporal<br />
atrophy on MRI or CT 1<br />
• Tactless and impulsive behavior 2,3<br />
1. Rascovsky K, Hodges JR, Knopman D, et al. Brain. Sep 2011;134(Pt 9):2456-2477. 2. Neary D, Snowden JS, Gustafson L, et al. Neurology. Dec 1998;51(6):1546-1554. 3.<br />
McKhann GM, Albert MS, Grossman M, et al. Arch Neurol. Nov 2001;58(11):1803-1809.<br />
24
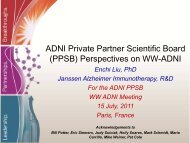
Imaging in the <strong>Diagnosis</strong><br />
• Left - AD shows prominent sulci in tempo-parietal areas, typically<br />
accompanied by ventricle enlargement<br />
• Middle- VaD most <strong>of</strong>ten shows cerebrovascular lesions on T2-weighted MRI<br />
• Right - FTD shows prominent sulci in frontotemporal areas with relative<br />
parietal and occipital sparing<br />
25
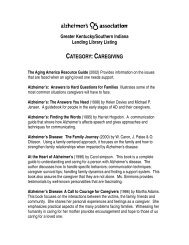
Imaging: AD vs DLB<br />
AD<br />
Hippocampal<br />
atrophy<br />
DLB<br />
• AD can show marked hippocampal atrophy<br />
• In DLB, the hippocampus may be relatively spared<br />
Tarawneh R, Galvin JE. Dementia with Lewy Bodies and other Synucleinopathies. In: Weiner MF, Lipton AM, eds. Textbook <strong>of</strong> Alzheimer disease and other<br />
dementias. 1st ed. Washington, DC: American Psychiatric Pub.; 2009.<br />
26
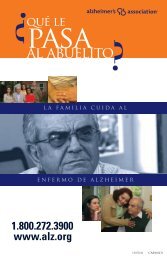
Neuropsychiatric Symptoms in <strong>Dementias</strong><br />
NPI Item AD PDD DLB VaD FTD<br />
Delusions ● ● ●● ● -<br />
Hallucinations - ●●● ●● ● -<br />
Agitation ●● ●● ●●● ●●● ●●●<br />
Depression ●● ●●● ●●● ●● ●●●<br />
Anxiety ●● ●●● ●●● ●● ●<br />
Apathy ●●● ●●● ●●●● ●●● ●●●●<br />
Disinhibition - - ● ● ●●●●<br />
Irritability ●● ● ●●● ●● ●●●<br />
Sleep ● ● ●●● ●● ●●<br />
- 0-14% ● 15-29% ●● 30-44% ●●● 45-59% ●●●●<br />
≥ 60%<br />
27
Pathologic Pr<strong>of</strong>iles <strong>of</strong> <strong>Dementias</strong><br />
Pathologic Signs AD PDD DLB VaD bvFTD<br />
Neuritic plaques ●●● ● ●● - -<br />
NFTs ●●● ● ●● - -<br />
Cortical Lewy bodies ● ● ●● - -<br />
Subcortical Lewy bodies ● ●●● ●●● - -<br />
Ischemic damage ●● - - ●●● -<br />
Tau or TDP-43 inclusions - - - - ●●●<br />
Biochemical Deficit AD PDD DLB VD FTD<br />
Cholinergic ●●● ●●●● ●●● -/● -<br />
Dopaminergic ● ●●● ●●● - -<br />
- Generally absent ● Infrequent ●● Typical ●●● Hallmark Feature ●●●● Severe Deficit<br />
1. Stahl SM. Stahl's essential psychopharmacology: neuroscientific basis and practical applications. 3rd ed, Fully rev. and expanded. ed. Cambridge ; New York: Cambridge<br />
University Press; 2008. 2. Geldmacher D. Alzheimer’s Disease. Textbook <strong>of</strong> Alzheimer disease and other dementias. 1st ed. Weiner MF, Lipton AM, eds. Washington, DC:<br />
American Psychiatric Pub.; 2009. 3. Tarawneh R, Galvin JE. Dementia with Lewy Bodies and other Synucleinopathies. Textbook <strong>of</strong> Alzheimer disease and other dementias. 1st<br />
ed. Weiner MF, Lipton AM, eds. Washington, DC: American Psychiatric Pub.; 2009. 4. Bird TD, Miller BL. Alzheimer’s disease and other dementias. Harrison’s Principles <strong>of</strong><br />
Internal Medicine. 16th ed. Kasper DL, Braunwald E, Fauci, AS, et al., eds. New York, NY: McGraw-Hill; 2005. 5. Szoeke CE, Campbell S, Chiu E et al, Vascular Cognitive<br />
Disorder. Textbook <strong>of</strong> Alzheimer disease and other dementias. 1st ed. Weiner MF, Lipton AM, eds. Washington, DC: American Psychiatric Pub.; 2009. 6. Rascovsky K, Hodges<br />
JR, Knopman D, et al. Sensitivity <strong>of</strong> revised diagnostic criteria for the behavioural variant <strong>of</strong> frontotemporal dementia. Brain. Sep 2011;134(Pt 9):2456-2477. 7. Bohnen NI, Kaufer<br />
DI, Ivanco LS, et al. Cortical cholinergic function is more severely affected in Parkinsonian dementia than in Alzheimer disease: an in vivo positron emission tomographic study. 28<br />
Arch Neurol. 2003;60:1745-1748.
Current FDA-Approved Therapies<br />
AD<br />
PDD<br />
Number <strong>of</strong> Acetylcholinesterase Inhibitors 1 4 1<br />
Number <strong>of</strong> NMDA Antagonists 1<br />
1 0<br />
• AD symptoms correlate with disruption <strong>of</strong> cholinergic circuits 2<br />
• PDD is characterized by a larger cholinergic deficit than AD 3<br />
• There are no FDA-approved medications <strong>of</strong> any class to treat<br />
DLB, VaD, or FTD<br />
1. Fortinash KM, Holoday-Worret PA. Psychiatric Mental Health Nursing. 3rd ed. St. Louis, MO: Mosby; 2004. 2. Boyd M Psychiatric Nursing: Contemporary<br />
Practice. 4th ed. Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008. 3. Reisberg B et al. N Engl J Med. 2003;348(14):1333-1341.<br />
29
The Importance <strong>of</strong> Making an Early<br />
<strong>Diagnosis</strong><br />
• Identify and treat reversible causes<br />
• Help explain presence <strong>of</strong> troublesome behaviors<br />
• Allow the patient to make critical life decisions<br />
• Identify and treat psychiatric symptoms<br />
• Maximize patient safety<br />
• To provide treatment<br />
• Allow caregiver early access to support and<br />
community resources<br />
Agronin ME. Alzheimer disease and other dementias : a practical guide. 2nd ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008.<br />
30
Caregiver Challenges in Different Types <strong>of</strong> <strong>Dementias</strong><br />
• AD – typically older onset, with frequent comorbidities<br />
• PDD – prominent motor symptoms leading to<br />
falls<br />
• DLB – frequent and sometimes severe<br />
neuropsychiatric symptoms<br />
• VaD – depression and continuing risk factors for<br />
stroke<br />
• FTD - younger onset, predominant behavioral<br />
and language symptoms<br />
31
Summary<br />
• <strong>Diagnosis</strong> <strong>of</strong> dementia begins with recognizing<br />
cognitive impairment (CI) in the patient<br />
– Cognitive assessment tools can be valuable<br />
• Reversible causes <strong>of</strong> CI should be ruled out via<br />
the dementia workup<br />
– Delirium must be ruled out, or if present, treated<br />
accordingly<br />
• Key clinical features <strong>of</strong> each dementia can aid<br />
the clinician in arriving at the specific diagnosis<br />
• Making the specific diagnosis early is critical for<br />
the patient and caregiver<br />
32