How to conduct a rapid nutrition assessment - Health Systems Trust
How to conduct a rapid nutrition assessment - Health Systems Trust
How to conduct a rapid nutrition assessment - Health Systems Trust

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
HOW TO CONDUCT A RAPID<br />
NUTRITION SITUATION<br />
ASSESSMENT<br />
A Guide for <strong>Health</strong> Districts<br />
and Sub-Districts<br />
in South Africa
HOW TO CONDUCT<br />
A RAPID NUTRITION<br />
SITUATION ASSESSMENT<br />
A guide for <strong>Health</strong> Districts<br />
and Sub-Districts in South Africa<br />
Developed by:<br />
Public <strong>Health</strong> Programme (University of the Western Cape)<br />
Initiative for Sub-District Support (<strong>Health</strong> <strong>Systems</strong> <strong>Trust</strong>)<br />
Eastern Cape Department of <strong>Health</strong>
Written by: Mickey Chopra & David McCoy<br />
With Assistance from: David Sanders & Ellen Piwoz<br />
Cover design by the Academy for Education Development<br />
Pho<strong>to</strong> Credits: UNICEF and HST<br />
Acknowledgements<br />
This product is one of the outputs of an initiative spearheaded by ISDS and PHP in<br />
partnership with the Mount Frere <strong>Health</strong> District and the Eastern Cape Department of <strong>Health</strong>.<br />
It is part of a series of training guides and resource materials that are being put <strong>to</strong>gether by the<br />
University of the Western Cape, the <strong>Health</strong> <strong>Systems</strong> <strong>Trust</strong>, Sustainable Approaches <strong>to</strong> Nutrition<br />
in Africa and the Academy for Educational Development. We would like <strong>to</strong> thank Thandi<br />
Puoane, Lesley Bamford, Susan Strasser, Jon Rohde, Wendy Hall and Rina Swart who have all<br />
assisted through discussions and debates.<br />
This Publication is<br />
ALSO available on the Internet<br />
www.hst.org.za<br />
Commissioned and Published by <strong>Health</strong> <strong>Systems</strong> <strong>Trust</strong><br />
<strong>Health</strong> <strong>Systems</strong> <strong>Trust</strong> Tel: (031) 307 2954<br />
401 Maritime House Fax: (031) 304 0775<br />
Salmon Grove<br />
Email: hst@healthlink.org.za<br />
Vic<strong>to</strong>ria Embankment<br />
Web: http://www.hst.org.za<br />
Durban 4001<br />
ISBN: 1-919839-09-7<br />
August 2000<br />
The publication of this document was funded by a grant provided by the Henry J.<br />
Kaiser Family Foundation and the European Union (through the National<br />
Department of <strong>Health</strong>)<br />
Designed and printed by The Press Gang, Durban - Tel: (031) 307 3240
Foreword<br />
It is with pleasure that I welcome the publication of this guide for health<br />
and <strong>nutrition</strong> workers in South Africa. Conducting a district-wide or sub-district<br />
<strong>assessment</strong> of mal<strong>nutrition</strong> <strong>to</strong>gether with the resources available <strong>to</strong> remedy the<br />
situation must be one of the first steps for any district or sub-district health team<br />
in South Africa.<br />
This guide also emphasises the importance of team-work, inter-sec<strong>to</strong>ral<br />
collaboration and local ownership in <strong>conduct</strong>ing a Nutrition Situation Assessment.<br />
I hope you will enjoy using this guide, and that it will contribute <strong>to</strong>wards a<br />
more effective response <strong>to</strong> the problems of mal<strong>nutrition</strong>.<br />
Nobahle Ndabula<br />
Deputy Direc<strong>to</strong>r: Nutrition<br />
Eastern Cape Department of <strong>Health</strong>.
Preface<br />
Designing and implementing comprehensive <strong>nutrition</strong> programmes within districts is<br />
one of the most important challenges facing district teams in South Africa. The first activity in<br />
this process is the collection of relevant information upon which <strong>to</strong> base planning decisions.<br />
The purpose of this guide is <strong>to</strong> provide health district <strong>nutrition</strong> workers with the steps<br />
and information necessary <strong>to</strong> complete a participa<strong>to</strong>ry NSA within the framework of the<br />
district health system. It will go through a framework and give examples of where and how<br />
information can be collected.<br />
This guide is meant for health district PHC workers who are motivated <strong>to</strong> implement an<br />
integrated <strong>nutrition</strong> programme. The key members of a district health team responsible for<br />
managing and <strong>conduct</strong>ing a NSA include:<br />
❖ INP Coordina<strong>to</strong>r<br />
❖ MCH Coordina<strong>to</strong>r<br />
❖ Environmental <strong>Health</strong> Coordina<strong>to</strong>r<br />
❖ Clinic Supervisors<br />
❖ Senior School <strong>Health</strong> Nurse<br />
❖ Senior <strong>Health</strong> Promotion Officer<br />
❖ District <strong>Health</strong> Information Officer<br />
❖ Doc<strong>to</strong>r/ Nurse in charge of paediatric ward.<br />
The guide is based mostly upon experiences of doing a similar exercise with <strong>nutrition</strong><br />
teams in two poor health districts: Hlabisa in KwaZulu-Natal and Mount Frere in the Eastern<br />
Cape. It is broken up in<strong>to</strong> the following sections:<br />
Section 1:<br />
Section 2:<br />
Section 3:<br />
The background <strong>to</strong>, and reasons for, performing a NSA.<br />
The steps that need <strong>to</strong> be completed in performing a NSA.<br />
The type of information that needs <strong>to</strong> be collected and suggestions about<br />
how this can be done.
CONTENTS<br />
Section 1: Introduction......................................................................................... 1<br />
1.1 The Integrated Nutrition Programme.......................................................... 1<br />
1.2 Why do a Nutrition Situation Assessment?................................................... 3<br />
Section 2: Steps in Conducting a Nutrition Situation Assessment 4<br />
Step 1: Identifying a district <strong>nutrition</strong> team ............................................................ 4<br />
Step 2: Build a common vision for the district health <strong>nutrition</strong> team ....................... 6<br />
Step 3: Establish the framework for the NSA ........................................................... 6<br />
Step 4: Identify what information is already available and what information<br />
is still required ............................................................................................. 8<br />
Step 5: Designing the <strong>to</strong>ols and methods for Information Collection ....................... 9<br />
Step 6: Collect the information ............................................................................. 10<br />
Step 7: Analyse information and write a report...................................................... 10<br />
Step 8: Disseminate the Information...................................................................... 10<br />
Section 3:<br />
Information for Conducting a Nutrition Situation<br />
Assessment...................................................................................... 11<br />
LEVEL 1 ................................................................................................................ 11<br />
1.1 The Geography and Mapping of the <strong>Health</strong> District ....................... 11<br />
1.2 The Community Composition (Demography) of the<br />
<strong>Health</strong> District................................................................................ 12<br />
1.3 Socio-Economic Profile.................................................................. 12<br />
1.4 Community Resources / Structures ................................................ 13<br />
LEVEL 2 ................................................................................................................ 13<br />
2.1 Household Food Security ............................................................... 13<br />
2.2 The Physical Environment .............................................................. 15<br />
2.3 Care ............................................................................................... 16<br />
LEVEL 3 ................................................................................................................ 17<br />
3.1 Nutrition Services .......................................................................... 17<br />
3.2 <strong>Health</strong> and Illness Profile ................................................................ 21
LEVEL 4 ................................................................................................................ 22<br />
4.1 Nutrition Status.............................................................................. 22<br />
FURTHER READING ............................................................................................. 23<br />
Appendix 1:<br />
Sample Observation Checklist for Assessing Growth<br />
Moni<strong>to</strong>ring and Promotion ............................................................................ 25<br />
Appendix 2:<br />
Sample Checklist for Assessing Common Infant Feeding<br />
Practices in the Community ......................................................................... 26<br />
Appendix 3:<br />
Example of a scoring system for targeting individual<br />
schools within a district or sub-district ................................................. 27
Section 1:<br />
Introduction<br />
1.1 The Integrated Nutrition Programme<br />
In South Africa more than 2 million children suffer from mal<strong>nutrition</strong>. It is an underlying<br />
cause in more than one in three of all childhood deaths in sub-Saharan Africa. It is also associated<br />
with reduced academic performance, physical outputs and earning capacity. Mal<strong>nutrition</strong><br />
therefore affects all sec<strong>to</strong>rs – health, education, welfare, agriculture and labour. Mal<strong>nutrition</strong> is<br />
an important reason why so many of the poor are caught up in the vicious cycle of poverty and<br />
poor health.<br />
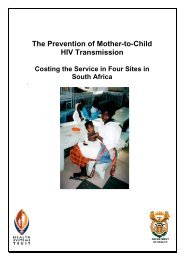
Mal<strong>nutrition</strong> is not just the result of a lack of food or ill health but the sum of many<br />
different causes. This can be shown by the framework of causes of mal<strong>nutrition</strong> drawn up by<br />
UNICEF (figure 1). Whilst mal<strong>nutrition</strong> usually presents <strong>to</strong> the health sec<strong>to</strong>r, many different<br />
sec<strong>to</strong>rs need <strong>to</strong> be involved <strong>to</strong> prevent mal<strong>nutrition</strong>.<br />
Traditionally <strong>nutrition</strong> interventions in South Africa have been vertical and food based.<br />
The main emphasis has been on giving food handouts accompanied by standard <strong>nutrition</strong><br />
messages, which are often inappropriate or irrelevant. The deficiencies of these programmes<br />
have been recognised in the new national Integrated Nutrition Programme (INP).<br />
The INP has outlined a comprehensive approach <strong>to</strong> address the underlying socioeconomic,<br />
environmental, educational and health related causes of under<strong>nutrition</strong>. The major<br />
aim of the INP is <strong>to</strong> shift from a reliance on feeding programmes <strong>to</strong> providing more<br />
comprehensive community and facility based <strong>nutrition</strong> interventions.<br />
The INP also proposes an interactive and participa<strong>to</strong>ry process of problem <strong>assessment</strong><br />
and analysis, followed by action, <strong>to</strong> be adopted at all levels. The INP is divided in<strong>to</strong> three broad<br />
areas of activity:<br />
❖ A health facility-based <strong>nutrition</strong> programme, incorporating the Protein Energy<br />
Mal<strong>nutrition</strong> (PEM) Scheme, <strong>nutrition</strong> education, growth moni<strong>to</strong>ring and promotion,<br />
the management of infectious diseases (including parasite control and diarrhoeal disease)<br />
and the in-patient management of severe mal<strong>nutrition</strong>.<br />
❖ A community-based <strong>nutrition</strong> programme (CBNP), which includes the Primary<br />
School Nutrition Programme (PSNP). It aims <strong>to</strong> strengthen household food security,<br />
improve knowledge and behaviour about <strong>nutrition</strong>, support the care of women and<br />
children, and promote a healthy environment, especially access <strong>to</strong> clean water and<br />
effective sanitation.<br />
❖ A <strong>nutrition</strong> promotion programme, which focuses on improving communication,<br />
advocacy and appropriate legislation in support of good <strong>nutrition</strong>.<br />
1
Figure 1: The UNICEF conceptual framework<br />
Mal<strong>nutrition</strong><br />
Manifestations<br />
Inadequate<br />
dietary intake<br />
Disease<br />
Immediate<br />
causes<br />
Insufficient<br />
Household<br />
Food Security<br />
Inadequate<br />
Maternal and Child<br />
Care<br />
Insufficient <strong>Health</strong><br />
Services & Unhealthy<br />
Environment<br />
Underlying<br />
causes<br />
Inadequate Education<br />
Resources & Control<br />
Human, Economic & Organisational<br />
Political and Ideological Superstructure<br />
Basic<br />
causes<br />
Economic Structure<br />
Potential Resources<br />
2
1.2 Why do a Nutrition Situation Assessment?<br />
Performing a <strong>nutrition</strong> situation <strong>assessment</strong> (NSA) is an important first step in<br />
implementing the INP. It serves <strong>to</strong>:<br />
❖ be the first step in the triple A cycle (Assessment, Analysis and Action) of the INP.<br />
❖ be an advocacy <strong>to</strong>ol, by persuading policy makers and funders of the problem of<br />
mal<strong>nutrition</strong> and the validity of your implementation plans.<br />
❖ assist in the future moni<strong>to</strong>ring and evaluation of the INP.<br />
❖ assist in the development of a district health system (a NSA would fit in<strong>to</strong> a broader<br />
district health situation <strong>assessment</strong>).<br />
❖ pull <strong>to</strong>gether the different members of the district health team <strong>to</strong> work <strong>to</strong>wards a<br />
common plan of INP implementation.<br />
❖ bring <strong>to</strong>gether a multi-sec<strong>to</strong>ral team and increase their appreciation of the need for<br />
all sec<strong>to</strong>rs <strong>to</strong> fight mal<strong>nutrition</strong> (especially the Departments of Education, Welfare,<br />
Agriculture and Water Affairs).<br />
Furthermore, <strong>conduct</strong>ing a NSA in a participa<strong>to</strong>ry manner can:<br />
❖ be an educational process for both the district <strong>nutrition</strong> team and the community as<br />
they come <strong>to</strong> realise the causes of mal<strong>nutrition</strong> and set about combating them; and<br />
❖ promote the participation of different community groups (in particular, women, poor<br />
people, young people) and thereby contribute <strong>to</strong> community empowerment.<br />
3
Section 2: Steps in Conducting a<br />
Nutrition Situation Assessment<br />
The steps for <strong>conduct</strong>ing a NSA are outlined below:<br />
1. Identifying a district <strong>nutrition</strong> team<br />
2. Build a common vision for the district health <strong>nutrition</strong> team.<br />
3. Establish the framework for the NSA<br />
4. Identify what information is already available and what information is still required<br />
5. Designing the <strong>to</strong>ols and methods for information collection<br />
6. Collect the information<br />
7. Analyse information and write a report<br />
8. Disseminate the report.<br />
Step 1:<br />
Identifying a district <strong>nutrition</strong> team<br />
Because mal<strong>nutrition</strong> has many causes, the solution <strong>to</strong> <strong>nutrition</strong> problems involves different<br />
people, programmes and institutions. This makes the process of “teambuilding” <strong>to</strong> be of crucial<br />
importance – it is worth the investment in time <strong>to</strong> get people, programmes, departments and<br />
organisations <strong>to</strong> understand and trust each other. <strong>How</strong>ever this is not easy and it is important<br />
not <strong>to</strong> wait until you have full participation from everybody before starting. Quite<br />
often as other sec<strong>to</strong>rs see you asking relevant questions and engaging with communities, they<br />
will want <strong>to</strong> join in.<br />
To start this process, an inven<strong>to</strong>ry of the organisation and institutions that are working<br />
locally or supporting local activities related <strong>to</strong> child health, <strong>nutrition</strong> and welfare should be<br />
drawn up. These can include government departments such as Education, <strong>Health</strong> and Agriculture,<br />
as well as NGOs involved in development work. Box 1 illustrates an exercise, which can be<br />
used <strong>to</strong> identify the important role-players in a district.<br />
4
Box 1: Identifying Key Role Players<br />
At the first meeting of the district <strong>nutrition</strong> team, a map of the district was shown <strong>to</strong><br />
everybody present. They were asked <strong>to</strong> point out where they were based and what<br />
child health, <strong>nutrition</strong> and welfare activities they were involved in within the district.<br />
The team then discussed other role players in the district who were not at the meeting,<br />
and ended up by developing the following table:<br />
Role-players Location Nutrition related Activities<br />
<strong>Health</strong> Sec<strong>to</strong>r<br />
Nutrition Co- Mary Theresa Hospital PEM Scheme, Creche Feeding, PSNP<br />
ordina<strong>to</strong>r<br />
PSNP co-ordina<strong>to</strong>r Based in Mt. Frere Providing school meals, school <strong>nutrition</strong><br />
education and school gardens<br />
Maternal & Child Mary Theresa Growth Moni<strong>to</strong>ring and Promotion,<br />
<strong>Health</strong> Coordina<strong>to</strong>r Hospital<br />
Nutrition education, PEM scheme,<br />
Immunisation services<br />
EHOs Sipetu Hospital Hygiene education and <strong>to</strong>ilet building<br />
projects in numerous communities<br />
<strong>Health</strong> Promotion Mary Theresa Hospital General health education campaigns in<br />
Coordina<strong>to</strong>r<br />
the district<br />
Clinics<br />
Hospitals<br />
Growth Moni<strong>to</strong>ring and Promotion,<br />
Nutrition education, PEM scheme,<br />
Immunisation services<br />
Growth Moni<strong>to</strong>ring and Promotion,<br />
Nutrition education, PEM scheme,<br />
Immunisation services, Management of<br />
severe illness such as severe malnurtition<br />
and diarrhoea<br />
Other Sec<strong>to</strong>rs<br />
Education Circuit Mt. Frere PSNP; The 4 A’s programme<br />
Office<br />
Agriculture In all parts of the Community garden and poultry<br />
Extension Officers district. projects; 4 A’s School Programme<br />
Welfare Mt. Frere and Sipetu Income generating projects; grants<br />
NGOs Isinamva Income generating projects, community<br />
health worker project<br />
Mvula <strong>Trust</strong><br />
Water and sanith~ion projects in all parts<br />
of the district<br />
5
Step 2:<br />
Build a common vision for the district<br />
health <strong>nutrition</strong> team<br />
All the relevant local people and institutions should then be invited <strong>to</strong> a meeting or<br />
workshop where the problem of under<strong>nutrition</strong>, the importance of a multi-sec<strong>to</strong>ral and<br />
participa<strong>to</strong>ry approach <strong>to</strong> tackling the problem can be discussed and agreed. The meeting<br />
should aim <strong>to</strong> set up and strengthen a <strong>nutrition</strong> task team whose first task is <strong>to</strong> <strong>conduct</strong> a<br />
participa<strong>to</strong>ry NSA for the district. Box 2 shows the aims of such an initial meeting in Mount<br />
Frere.<br />
Box 2: Aims of First Nutrition Workshop, in Mount Frere<br />
1. To introduce the various role players working in Mount Frere and Region E <strong>to</strong> each<br />
other and <strong>to</strong> share what they are doing<br />
2. To share the results of national and local surveys showing the prevalence and<br />
impact of mal<strong>nutrition</strong> in the region.<br />
3. To perform a mapping exercise of the district in order <strong>to</strong> share information about<br />
<strong>nutrition</strong> related activities and projects in the district<br />
4. To develop a common understanding of the causes of mal<strong>nutrition</strong>.,<br />
5. To motivate for the need for multi-sec<strong>to</strong>ral collaboration<br />
6. To form a regional and district integrated <strong>nutrition</strong> team which can perform a NSA<br />
and then a “health district” based INP.<br />
If it is not possible <strong>to</strong> organise a workshop or meeting then visiting key individuals such<br />
as the agricultural officer, education officer and other maternal and child health workers <strong>to</strong><br />
explain what you are going <strong>to</strong> do and how they might be involved can be a way of getting cooperation<br />
/ collaboration.<br />
Step 3:<br />
Establish the framework for the NSA<br />
After setting up a health district <strong>nutrition</strong> team, it is necessary <strong>to</strong> outline the NSA<br />
framework. A useful exercise is <strong>to</strong> ask the team what information they would require if they<br />
were requested by a district manager <strong>to</strong> recommend a <strong>nutrition</strong> intervention.<br />
In the Mount Frere district, for example, the team came up with the following headings:<br />
❖ The geography of the district<br />
❖ The community composition (demographic details) of the district<br />
❖ The socio-economic profile of the district<br />
❖ The health status of the population<br />
❖ The <strong>nutrition</strong> status of the population.<br />
❖ The environmental health indica<strong>to</strong>rs<br />
6
❖ Important child care practices<br />
❖ Household Food Security<br />
After further discussion it was also decided <strong>to</strong> add the following:<br />
❖ The quality and coverage of existing child, <strong>nutrition</strong> and welfare services and<br />
programmes, as they relate <strong>to</strong> <strong>nutrition</strong><br />
❖ The resources available in the district <strong>to</strong> tackle under<strong>nutrition</strong><br />
Drawing up the framework in this way helps <strong>to</strong> get the team <strong>to</strong> think about all the<br />
information that is required. The team can also now plan for the collection of data. It is therefore<br />
important that all members of the team understand each part of the framework. This manual<br />
provides a framework which can be adapted <strong>to</strong> fit the circumstances of a health district, but<br />
which is suggested as a model framework <strong>to</strong> allow comparisons between different districts.<br />
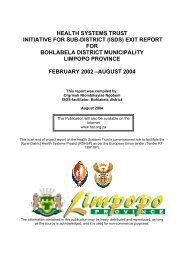
To make it easier <strong>to</strong> see what information needs <strong>to</strong> be collected, the framework can be<br />
rearranged in<strong>to</strong> an information pyramid as shown in figure 2.<br />
Figure 2: Information Framework<br />
Nutrition<br />
Status<br />
Nutrition<br />
Services<br />
<strong>Health</strong><br />
&<br />
Illness<br />
Profile<br />
Physical<br />
Environment<br />
Care<br />
Household<br />
Food<br />
Security<br />
Physical<br />
Geography<br />
Socio-<br />
Economic<br />
Profile<br />
Community<br />
Resources/<br />
Structures<br />
Community<br />
Composition<br />
Demography<br />
The bot<strong>to</strong>m level of the pyramid represents a foundation of information about community<br />
composition, socio-economic fac<strong>to</strong>rs, geography and existing resources and structures. It is<br />
important for <strong>nutrition</strong> planners <strong>to</strong> know about the community with which they are working<br />
and some of community resources available for <strong>nutrition</strong> interventions. It can assist in deciding<br />
what parts of the district need <strong>to</strong> be targeted first and whether there are very different groups<br />
of people within the district.<br />
7
The next level aims <strong>to</strong> establish the importance of the underlying causes of under<strong>nutrition</strong>:<br />
child caring practices, the environmental context and distribution of food at the household<br />
level.<br />
The third level concerns information on ill health and <strong>nutrition</strong>, and establishes the<br />
existence, coverage, accessibility and quality of <strong>nutrition</strong> and <strong>nutrition</strong>- related services. Finally,<br />
at the <strong>to</strong>p of the pyramid is some general information about relevant national and provincial<br />
health and <strong>nutrition</strong> policies.<br />
Step 4:<br />
Identify what information is already<br />
available and what information is still<br />
required<br />
The information pyramid can also be used <strong>to</strong> help decide what data is missing and still<br />
needs <strong>to</strong> be collected. The main team members can be asked <strong>to</strong> write down the pieces of<br />
information needed for each part of the pyramid (e.g. clean water, water availability, low birth<br />
weight rate, quality of growth moni<strong>to</strong>ring) and then identify which parts of this information<br />
are already available.<br />
Remember that the main reason for doing a NSA is <strong>to</strong> assist in making<br />
decisions about appropriate <strong>nutrition</strong> interventions. The NSA is not designed <strong>to</strong> collect<br />
all information about <strong>nutrition</strong>, but about relevant information that can be used <strong>to</strong> improve the<br />
quality of planning and implementation.<br />
In addition, it must be practical <strong>to</strong> collect this information. Large community surveys are<br />
expensive and time-consuming exercises, the results of which may not have much bearing on<br />
the planning of interventions. Where possible information which has already been collected,<br />
either by government services or by other organisations, should be identified and collected.<br />
Possible sources of information include:<br />
❖ The National Census<br />
❖ The National Demographic Household Survey and other surveys that have already<br />
been undertaken.<br />
❖ Government department records (e.g. water, agriculture, housing etc.)<br />
❖ Reports of studies done by local universities, research organisations or NGOs<br />
❖ Department of <strong>Health</strong> accounts showing budgetary expenditures<br />
After this exercise it will be easy <strong>to</strong> see what information is still required. The team must<br />
then decide about what information it will have <strong>to</strong> actively collect for itself. Remember that<br />
only information which is needed <strong>to</strong> help prioritise and plan <strong>nutrition</strong> interventions should be<br />
collected and that it might not be possible <strong>to</strong> collect all the information within the given<br />
timeframe.<br />
8
Step 5:<br />
Designing the <strong>to</strong>ols and methods for<br />
Information Collection<br />
Once the required information has been identified, plans must be drawn up <strong>to</strong> collect<br />
this information. There are a number of different methods which can be used <strong>to</strong> collect this<br />
information, some of which are described below:<br />
Key Informant Interviews<br />
Information about certain aspects of <strong>nutrition</strong> can often be derived by talking <strong>to</strong> a few<br />
key people who have insight and knowledge about that particular aspect of <strong>nutrition</strong>.<br />
Such people whose knowledge and understanding can be used <strong>to</strong> inform planning<br />
are termed “key informants”, and include the following three groups of people:<br />
❖<br />
❖<br />
❖<br />
People who work within the community and have a professional understanding of<br />
the issues: for example, school teachers, clinic nurses and social workers.<br />
People who are recognised as community leaders and seen <strong>to</strong> represent (a section<br />
of) the community: for example, councillors, church leaders, old women in the<br />
community<br />
People who are important within informal networks and often play a central role in<br />
local communications: for example, shop-owners, old women in the community,<br />
income generation project leaders.<br />
Observations<br />
Some information can only be obtained by actually seeing what is happening with<br />
your own eyes. For example, the actual way in which babies are weighed and growth<br />
moni<strong>to</strong>red. As a member of the NSA team, you may want <strong>to</strong> find out about the hygiene<br />
conditions in which mothers prepare food for children by visiting local homes, and<br />
observing other aspects of child health care at the same time. Generally it is a good<br />
idea <strong>to</strong> draw up a checklist of the different things <strong>to</strong> specifically look out for.<br />
Exit interviews with carers<br />
Exit interviews are interviews of patients or health care users <strong>conduct</strong>ed just after they<br />
have used a health service, and is usually designed <strong>to</strong> assess the quality of care provided<br />
from the user’s perspective. For example, the provision and standard of GMP and EPI<br />
services can be assessed by exit interview.<br />
Record review<br />
Ward registers, clinic registers, the actual case records of in-patients or even the patient–<br />
held Road-<strong>to</strong>-<strong>Health</strong> cards of children can all be used in various ways <strong>to</strong> collect<br />
information <strong>to</strong> assess various aspects of quality of care.<br />
Routine information<br />
The routine health information system can be used <strong>to</strong> collect a lot of useful information<br />
that is relevant <strong>to</strong> <strong>nutrition</strong>. For example, what proportion of the child catchment<br />
population are immunised? What proportion of babies are low birthweight?<br />
9
Step 6:<br />
Collect the information<br />
After the <strong>to</strong>ols have been developed and pre-tested you are ready <strong>to</strong> collect the information.<br />
Tasks must be clearly delegated <strong>to</strong> appropriate people with a clear timeframe for their completion.<br />
It is important for someone <strong>to</strong> take responsibility for moni<strong>to</strong>ring the process <strong>to</strong> ensure<br />
that the data is being collected as planned.<br />
Step 7:<br />
Analyse information and write a report<br />
The findings of the NSA should be presented as clearly and concisely as possible. The<br />
way in which information is presented is very important 1 . This should be done in the form of<br />
a report which will form the basis for planning and evaluating the required <strong>nutrition</strong><br />
interventions. The report should allow the “district <strong>nutrition</strong> team” <strong>to</strong>:<br />
❖ Identify priority <strong>nutrition</strong> problems, and their causes<br />
❖ Review the quality and coverage of existing <strong>nutrition</strong> activities in maternal and child<br />
health services<br />
❖ Review the quality and coverage of existing INP activities in the district<br />
❖ Identify community and public service resources for combating <strong>nutrition</strong> problems<br />
in the district<br />
❖ Define target groups, set <strong>nutrition</strong> objectives and identify strategies<br />
❖ Identify indica<strong>to</strong>rs for moni<strong>to</strong>ring progress with the <strong>nutrition</strong> programme<br />
If this is a follow up NSA then important areas of progress or deterioration over the past<br />
year in the district should be identified and reasons for these changes highlighted.<br />
Step 8:<br />
Disseminate the Information<br />
Once the report is finalised, it is important <strong>to</strong> disseminate it and make it available <strong>to</strong> key<br />
people. There are many other ways of disseminating the findings of the NSA:<br />
❖ Make short and easy-<strong>to</strong>-read policy and programme briefs on key findings and<br />
recommendations;<br />
❖ Make oral presentations <strong>to</strong> key decision-makers, managers, health workers, community<br />
organisations<br />
❖ Organise a dissemination workshop for decision-makers, managers, health workers,<br />
community organisations<br />
❖ Write press releases for the local media, including local and / or community media<br />
stations<br />
The wider the dissemination the more chance there is of the NSA leading <strong>to</strong> meaningful<br />
discussion and actions.<br />
10<br />
1 The training manual: ‘Integrating Nutrition in<strong>to</strong> Development Programmes’ has a whole section on<br />
these basic skills.
Section 3: Information for Conducting<br />
a Nutrition Situation Assessment<br />
This section reviews in greater detail the type of information required for the NSA, the<br />
sources of information and how <strong>to</strong> collect it. It is structured according <strong>to</strong> the information<br />
pyramid discussed in Section 2. Not all the blocks in the information pyramid are equally<br />
important, and this manual emphasises the important information within those blocks.<br />
LEVEL 1<br />
1.1 The Geography and Mapping of the <strong>Health</strong> District<br />
A simple map which outlines the boundaries of the health district, the major roads and<br />
rivers, clinics and mobile points, the hospital, the offices for education, agriculture and welfare<br />
and the major settlements is a very useful start. The map can be further improved with information<br />
about the location of the district relative <strong>to</strong> the nearest <strong>to</strong>wns as well as the physical attributes<br />
of the district (i.e. rural, hilly, state of the roads etc.).<br />
Develop the map in consultation with different sec<strong>to</strong>rs as they will have maps with<br />
different sorts of information available. For instance, the Department of Education should have<br />
a map of the schools in the district. By bringing the different sources of information <strong>to</strong>gether<br />
the team can build up a comprehensive picture of the activities and resources in a district.<br />
Finally, for specific local communities, community mapping exercises can be a quick and<br />
accurate means <strong>to</strong> get information about the structure of the community (see box 3). This sort<br />
of exercise can be done in conjunction with local clinics which can use these exercises <strong>to</strong> help<br />
define their catchment population, or mapping can be done with community groups that may<br />
be involved in district projects. The manual ‘Mapping for Primary <strong>Health</strong> Care’ from Management<br />
for Sciences for <strong>Health</strong> has a number of examples of performing mapping exercises.<br />
Box 3: Mapping exercise in Hlabisa<br />
After initial meetings with community leaders it was decided <strong>to</strong> hold a community<br />
meeting at the local school. To begin the meeting the facilita<strong>to</strong>rs asked the community<br />
<strong>to</strong> draw a map. There were thirty participants of whom about twenty were women.<br />
They readily <strong>to</strong>ok up the challenge of drawing a map on the ground using different<br />
colour powders <strong>to</strong> symbolise the roads and rivers, and s<strong>to</strong>nes <strong>to</strong> mark the various<br />
kraals. They were asked <strong>to</strong> mark important landmarks in the community. In this way<br />
the team gained useful insights in<strong>to</strong> what the community perceived as important<br />
structures. With little intervention from the facilita<strong>to</strong>rs they completed their map after<br />
about an hour. This was then checked by the elderly men and women who had not<br />
participated as fully during the exercise; they picked up a few points which the others<br />
had missed. The facilita<strong>to</strong>rs were then able <strong>to</strong> complete a <strong>rapid</strong> demographic survey<br />
of the community by asking for information about who lived in the various households<br />
located on the community map.<br />
11
1.2 The Community Composition (Demography) of the<br />
<strong>Health</strong> District<br />
The ratio of male <strong>to</strong> female children and the age distribution of the population (especially<br />
proportion of children under 5) are important pieces of information. <strong>How</strong>ever, accurate<br />
information on the demographic structure of the local population can be difficult <strong>to</strong> get. The<br />
recent census data and the local welfare office should be able <strong>to</strong> provide some statistics for the<br />
magisterial districts.<br />
If household surveys have been completed in parts of the district either for health, welfare,<br />
education or agriculture, you can use this as a source of information.<br />
1.3 Socio-Economic Profile<br />
A general description of the socio-economic profile of the health district will help <strong>to</strong><br />
contextualise the plans for an INP. But getting good quality data can be difficult so it is<br />
recommended that you speak <strong>to</strong> key informants in the district. Important issues <strong>to</strong> discuss with<br />
informants would be:<br />
❖ Where are the poorest communities in the district?<br />
❖ What are the main sources of income for families in the district?<br />
❖ What are the main sources of income for women in the district?<br />
❖ <strong>How</strong> widespread and successful are income generating projects?<br />
❖ Are there seasonal fac<strong>to</strong>rs for income generation?<br />
Box 4 outlines an exercise which can assist you in answering some of these questions:<br />
Box 4: Investigating different sources of income in Hlabisa<br />
After completing a community map and a walk through the village the facilita<strong>to</strong>r<br />
explained why it was useful <strong>to</strong> understand the different sources of income in the<br />
community. He then drew a house on the ground. Participants were asked <strong>to</strong> shout<br />
out the different sources of income coming in<strong>to</strong> their household. These were drawn<br />
and written on pieces of card and distributed around the drawing. The participants<br />
were then given one bean each and instructed <strong>to</strong> place it on the most important<br />
source of income in their household. The men were given different coloured beans<br />
from the women. Most women and men placed their bean on farming. They stated<br />
that even if pensions or remittances sometimes contributed larger amounts they were<br />
quite often irregular and farming was something they could rely upon. The sale of<br />
vegetables grown in the community gardens was also important for some women,<br />
whereas nearly half the men put down part-time jobs as an important source of income.<br />
This could include working on other peoples farms, putting up fencing and building<br />
kraals. They also mentioned that sometimes they get paid in kind with food rather<br />
than money in some of these jobs.<br />
12
1.4 Community Resources / Structures<br />
Because an important component of the INP is the development of community-based<br />
interventions, with community involvement and participation, it is important <strong>to</strong> have a good<br />
idea of the community structures and resources that exist. Some important resources include<br />
informal creches, Church Groups, Community Based Organisations, local GPs etc. Box 5 shows<br />
an exercise which can help <strong>to</strong> get this information.<br />
Box 5: Finding out about community resources<br />
During a community meeting a member of the district INP team asked a group of<br />
women and men <strong>to</strong> write down all the organisations that they belonged <strong>to</strong>o or were<br />
active in the area on pieces of paper which had been cut in<strong>to</strong> circles. Once they<br />
completed this she then asked them <strong>to</strong> discuss the importance of each of the<br />
organisations <strong>to</strong> the community. They were requested <strong>to</strong> write the name of the village<br />
on a piece of paper and place all the most important organisations next <strong>to</strong> the village<br />
name. The next important organisations were then placed a little further back. This<br />
continued until they had built a picture which allowed the team <strong>to</strong> see which<br />
organisations were present in the area and which ones the community regarded as<br />
most important.<br />
LEVEL 2<br />
2.1 Household Food Security<br />
A household is food secure when it has adequate access <strong>to</strong> the food (in terms of quality, quantity,<br />
safety and acceptability), needed for a healthy life for all its members and when it is not at undue risk of<br />
losing such access.<br />
In South Africa, not all households have food security and not all members within a<br />
family have equal access <strong>to</strong> that food.<br />
Households may not have food security either because they lack physical access <strong>to</strong> food<br />
and/or they lack the economic resources <strong>to</strong> buy food and/or because households are unable <strong>to</strong><br />
use the food available <strong>to</strong> them safely and appropriately. To assess household food security we<br />
need <strong>to</strong> find out about the availability, access and use of food by households. Table 2 provides<br />
a framework for collecting this information.<br />
13
Table 2: Assessment of Household Food Security<br />
Information needed Source of Method for<br />
information collection<br />
Food availability and access Community mem- Key informant<br />
<strong>How</strong> do households obtain their food? bers/ Agricultural interviews/<br />
What do they produce? officers Participa<strong>to</strong>ry<br />
What do they purchase? Other sources?<br />
appraisal<br />
Has this situation changed in the last<br />
few years? <strong>How</strong>? Why?<br />
Production for Household Consumption Community mem- Key informant<br />
What foods are produced by the house- bers/ Agricultural interviews/<br />
hold? <strong>How</strong> many months do staples last? Officers Participa<strong>to</strong>ry<br />
During which months do they eat the<br />
appraisal<br />
other foods? Do they grow energy-rich<br />
foods?<br />
What are the periods of food scarcity?<br />
For which foods?<br />
What efforts do people make <strong>to</strong> overcome<br />
these?<br />
Food Purchasing Community mem- Key informant<br />
<strong>How</strong> much of the household income is bers interviews/<br />
spent on food?<br />
Participa<strong>to</strong>ry<br />
What are the foods purchased? Which are<br />
appraisal<br />
considered as essential?<br />
Which as luxury? Why?<br />
<strong>How</strong> have purchasing habits changed in<br />
recent years? Why?<br />
Food Use Community mem- Key informant<br />
<strong>How</strong> many meals do the different house- bers interviews/<br />
holds members eat a day? In which season?<br />
Participa<strong>to</strong>ry<br />
Any snacks in between? Do children eat<br />
appraisal<br />
differently? <strong>How</strong> often do they prepare<br />
meals for young children?<br />
<strong>How</strong> do eating patterns change in times<br />
of scarcity?<br />
<strong>How</strong> is food obtained in such cases?<br />
If the household had more resources<br />
what foods would they like <strong>to</strong> more or<br />
more often? What foods are considered<br />
especially good or <strong>to</strong> be avoided in<br />
certain circumstances?<br />
What was the normal diet for children<br />
20 years ago? If it has changed,<br />
how and why?<br />
14
Answers <strong>to</strong> questions such as: “Who is at risk of poor household food security? What is<br />
the nature of the problem? Its severity? Its frequency and periodicity?” will inform the<br />
development of appropriate interventions which can help <strong>to</strong> target households and improve<br />
the availability of food at a household level.<br />
2.2 The Physical Environment<br />
Important causes of mal<strong>nutrition</strong> include illnesses such as diarrhoeal disease and worm<br />
infections, which are often caused by a poor living environment. An INP needs <strong>to</strong> be able <strong>to</strong><br />
moni<strong>to</strong>r and respond <strong>to</strong> a number of key environmental health indica<strong>to</strong>rs.<br />
Environmental health officers quite often collect information from local communities<br />
about the water supply and its quality, the number of <strong>to</strong>ilets, waste disposal facilities etc.<br />
Environmental health officers are also trained <strong>to</strong> perform observations <strong>to</strong> assess the environment<br />
of a community, and the <strong>nutrition</strong> team can draw upon this expertise. Requesting communities<br />
<strong>to</strong> indicate on the community maps the position of water sources, the quality of the water and<br />
the number of households with <strong>to</strong>ilets is also a way of assessing the environmental situation.<br />
This method also has the advantage of being able <strong>to</strong> lead in<strong>to</strong> a community discussion on issues<br />
concerning the environment. Table 3 outlines some of the information that may be important.<br />
Table 3: Physical Environment<br />
Information needed Source of Information Method for collection<br />
% with clean water supply Department of Water Literature review<br />
at home and Forestry Local survey<br />
% with communal taps Local surveys Key informant interviews<br />
% with no clean water supply<br />
% spend more than 30 mins<br />
<strong>to</strong> get <strong>to</strong> water supply<br />
% with <strong>to</strong>ilets in households Department of Water Literature review<br />
% with access <strong>to</strong> <strong>to</strong>ilets and Forestry Local survey<br />
Local surveys<br />
Key informant interviews<br />
% with waste disposal Department of Water Literature review<br />
facilities and Forestry Local survey<br />
Local surveys<br />
Key informant interviews<br />
% with adequate home water Department of Water Literature review<br />
s<strong>to</strong>rage facilities and Forestry Key informant interviews<br />
Local surveys<br />
% households with clean Observations Key informant interviews<br />
yards<br />
Observations<br />
% villages with no unburied<br />
faeces<br />
% taps with proper drainage<br />
15
2.3 Care<br />
Food and health services are necessary but not sufficient conditions for good <strong>nutrition</strong>.<br />
The third underlying determinant is care. Care refers <strong>to</strong> the practices of those who give care <strong>to</strong><br />
children, translating the available food and health resources in<strong>to</strong> a child’s survival, growth and<br />
development. Because it is women who are usually responsible for providing child care, the<br />
care provided <strong>to</strong> women is also important.<br />
Even when poverty causes food insecurity and there is limited health care, enhanced<br />
child care and affection can optimise the use of existing resources <strong>to</strong> promote good health and<br />
<strong>nutrition</strong> for women and children. Breastfeeeding is an example of a practice that provides<br />
food, health and care simultaneously.<br />
Through assessing the common child care beliefs and practices the <strong>nutrition</strong> team should<br />
be able <strong>to</strong> determine the need for certain health promotion and <strong>nutrition</strong> education services.<br />
Table 4 outlines some of the information that may be of importance.<br />
Table 4: Assessment of Care Practices<br />
Information needed Source of Method for<br />
information collection<br />
Breastfeeding and complementary feeding<br />
Proportion of children exclusively breastfed Carers of children Clinic surveys at<br />
at 3 months<br />
3 rd immunisation<br />
Proportion of children breastfed on demand Carers of children Clinic surveys at<br />
3 rd immunisation<br />
Average age when a)liquids b) milk and<br />
c)semi-solids are introduced<br />
Community mem- Key informant<br />
bers<br />
interviews<br />
What types of foods are they given, and Community mem- Key informant<br />
how are they prepared and fed <strong>to</strong> children bers/<strong>Health</strong> interviews<br />
under 2? <strong>How</strong> many times a day?<br />
personnel<br />
At what age is breastfeeding discontinued?<br />
Are any high energy foods given (e.g. peanut<br />
butter, oil, margarine etc.)?<br />
Community mem- Key informant<br />
bers<br />
interviews<br />
Community mem- Key informant<br />
bers<br />
interviews<br />
Psycho-social stimulation<br />
Do adults supervise when eating and actively<br />
encourage the children <strong>to</strong> eat? <strong>How</strong>? Carers of children Clinic surveys at<br />
3 rd immunisation<br />
16
Table 4: Assessment of Care Practices (continued)<br />
Information needed Source of Method for<br />
information collection<br />
Hygiene practices<br />
Are resources available in the community <strong>to</strong><br />
practice adequate hygiene?<br />
Community mem- Key informant<br />
bers<br />
interviews/<br />
Observations<br />
Are hygiene practices adequate in the Community Key informant<br />
household and community? members/<strong>Health</strong> interviews/<br />
personnel Observations<br />
Care for women<br />
What is the degree of control of decision Community Key informant<br />
making and finance of women in the members interviews<br />
household?<br />
Are girls valued just as much as boys? Community Key informant<br />
members interviews<br />
Are there any special cus<strong>to</strong>ms regarding Community Key informant<br />
the care and diet of pregnant and lactating members/<strong>Health</strong> interviews<br />
mothers?<br />
personnel<br />
LEVEL 3<br />
3.1 Nutrition Services<br />
The availability of effective and efficient health services can play a significant role in<br />
improving <strong>nutrition</strong> and reducing the impact of under<strong>nutrition</strong>. An attempt should be made <strong>to</strong><br />
assess maternal and child health services (MCH) in the district.<br />
For instance, good growth moni<strong>to</strong>ring and promotion (GMP) by health workers can<br />
prevent much under<strong>nutrition</strong>; similarly the proper care of severely malnourished children in<br />
the paediatric ward can significantly reduce the mortality of these children.<br />
The following are a list of priority MCH services that should ideally be assessed as part<br />
of any NSA:<br />
17
Primary level (clinic/CHC’s/ Hospital OPD)<br />
❖ GMP<br />
❖ Management of diarrhoeal disease<br />
❖ Vitamin A / Iron supplementation<br />
❖ Promotion of Breastfeeding<br />
❖ Ante-natal services<br />
❖ Immunisation service<br />
❖ Nutrition education<br />
Hospital<br />
❖ In-patient management of severe mal<strong>nutrition</strong> and diarrhoeal disease<br />
❖ Nutrition Education<br />
❖ Promotion of Breastfeeding.<br />
In Mount Frere the district <strong>nutrition</strong> team drew up a checklist of health service activities<br />
they thought were important in performing growth moni<strong>to</strong>ring and promotion. They then<br />
went <strong>to</strong> a number of clinics and hospitals in the district <strong>to</strong> perform observations and interviews<br />
using these checklists. They found a number of shortcomings in the performance of GMP.<br />
Their results have helped with designing a training programme <strong>to</strong> improve GMP in the district.<br />
At Hlabisa district hospital the paediatric team kept a simple record of the outcome of<br />
children admitted with severe mal<strong>nutrition</strong>. They then reviewed the management of these<br />
children. Through changing a few simple things they were able <strong>to</strong> achieve a five fold reduction<br />
in mortality.<br />
Other services which should be assessed include breastfeeding, immunisation and<br />
management of the sick child.<br />
Assessment of Services<br />
To help a team think about what needs <strong>to</strong> be measured <strong>to</strong> assess <strong>nutrition</strong> services we<br />
need <strong>to</strong> be sure that the correct things are available and in place (INPUTS) and that these are<br />
combined <strong>to</strong>gether (PROCESS), <strong>to</strong> produce a service (OUTPUTS) which will have an impact<br />
(OUTCOME). For example, <strong>to</strong> assess the quality of GMP the following table could be drawn<br />
up:<br />
18
Table 5: Assessing quality of GMP<br />
Information needed Source of Method for<br />
information collection<br />
Inputs<br />
Adequate number of trained staff<br />
Availability of drugs/food supplements<br />
Functioning scales<br />
Processes<br />
Timely and courteous service<br />
Correct weighing and plotting<br />
Appropriate counselling<br />
Correct treatments<br />
Growth moni<strong>to</strong>ring sessions<br />
Outputs<br />
Improved knowledge of mother about growth<br />
of her child<br />
Increased number of children correctly<br />
weighed and plotted<br />
Increased client satisfaction<br />
<strong>Health</strong> Staff/Clinic Key informant<br />
interviews/<br />
Observation<br />
Growth moni<strong>to</strong>ring Exit interviews<br />
clients<br />
Growth moni<strong>to</strong>ring Exit interviews<br />
clients<br />
Outcome<br />
Reduced mortality Provincial Records/ Literature and<br />
Reduced levels of mal<strong>nutrition</strong> Hospital and routine statistics<br />
Increased levels of immunisation coverage clinic records review<br />
Assessment of Nutrition Programmes<br />
South Africa is investing a lot of resources in <strong>nutrition</strong> programmes. Some of these, such<br />
as the PEM scheme are run by the Department of <strong>Health</strong>; some such as the Primary School<br />
Nutrition Programme (PSNP) are run in collaboration with other sec<strong>to</strong>rs (Education); and<br />
others, such as community garden projects are run in sec<strong>to</strong>rs outside of health (Agriculture). It<br />
is important <strong>to</strong> assess the efficiency and effectiveness of these programmes. The following is a<br />
suggested checklist of what <strong>to</strong> check for when assessing <strong>nutrition</strong> programmes in your district.<br />
Goals<br />
❖ Whether the programme has clear goals, measurable targets, and whether they are<br />
well unders<strong>to</strong>od;<br />
❖ Whether progress has been made <strong>to</strong>wards these targets in the previous 12 months or<br />
so, and if not, why;<br />
19
Activities<br />
❖ The current set of activities and services;<br />
❖ Whether the quality of the service is adequate;<br />
❖ Whether priority groups (i.e. pregnant and lactating women, young children) are<br />
being reached effectively;<br />
❖ Whether moni<strong>to</strong>ring, evaluation and supervision are adequate and if not, what needs<br />
<strong>to</strong> be done <strong>to</strong> improve it;<br />
❖ <strong>How</strong> the activities relate <strong>to</strong> other services provided in the district.<br />
Resources<br />
❖ The personnel available <strong>to</strong> work in the programme;<br />
❖ Whether supplies and transport are sufficient;<br />
❖ Whether resources (human, organisational, technical and financial) are adequate <strong>to</strong><br />
reach the programme objectives;<br />
Once again this information can be collected using a variety of methods. Box 6 shows an<br />
example from Mount Frere.<br />
Box 6: Assessment of PSNP in Mount Frere<br />
The Mount Frere <strong>nutrition</strong> team decided <strong>to</strong> assess the PSNP in the district. Because<br />
one member of the team was the district education officer, collecting information on<br />
the aims and objectives, the resources available and the coverage of the programme<br />
was relatively easy. The team interviewed key personnel such as the circuit education<br />
manager, a school principal and a contrac<strong>to</strong>r about their knowledge and understanding<br />
of these aims and objectives. Other members of the team drew up an observation<br />
checklist which included such things as the quality of the food, the children’s enjoyment<br />
of the food and the disruption it caused <strong>to</strong> the class. They then <strong>conduct</strong>ed interviews<br />
with a couple of the teachers, the school principals and members of the school<br />
committee asking about their opinions of the programme and any suggestions they<br />
might have for improvements.<br />
They found that the food was quite often stale and not much liked by the children. In<br />
addition, they found that the teachers and community were also dissatisfied since<br />
large amounts of money went <strong>to</strong> the large bakery in a distant <strong>to</strong>wn and the lunch was<br />
not reproducible at home. As a result of the <strong>assessment</strong> it was decided <strong>to</strong> explore the<br />
possibility of providing a locally produced lunch. This would then be linked <strong>to</strong> a school<br />
<strong>nutrition</strong> education programme and the school garden projects being supported by<br />
the Agriculture department.<br />
20
Here are some questions that you could ask about the PSNP programme:<br />
❖ What is the basic organisational structure and management of the PSNP?<br />
❖ What schools are targeted and what is the coverage?<br />
❖ <strong>How</strong> is the food supplied and prepared?<br />
❖ What is the community and NGO involvement?<br />
❖ What are the links <strong>to</strong> other interventions?<br />
❖ What are the outcomes/benefits of the programme?<br />
❖ What are the plans for the future?<br />
Appendix 3 gives an example of a scoring system that can be used <strong>to</strong> target the most<br />
needy schools.<br />
3.2 <strong>Health</strong> and Illness Profile<br />
Illnesses such as diarrhoea, measles, pneumonia, and HIV are important causes of<br />
under<strong>nutrition</strong> in children. Women who suffer from illnesses during pregnancy or during child<br />
care are also more likely <strong>to</strong> have undernourished children. Therefore, information on the<br />
frequency and prevalence of common childhood illnesses and women’s health is important.<br />
Table 6: Assessment of <strong>Health</strong> and Illness<br />
Information needed Source of Method for<br />
information collection<br />
<strong>Health</strong> Status<br />
Maternal mortality<br />
Infant mortality rate and Under 5 mortality<br />
rate<br />
Ante-natal HIV prevalence<br />
Prevalence of maternal anaemia<br />
National/Provincial Literature review<br />
Statistics<br />
Childhood Illnesses<br />
Prevalence of diarrhoea Hospital/Clinic Register/Record<br />
Prevalence of pneumonia Statistics Review<br />
Prevalence of severe mal<strong>nutrition</strong><br />
Prevalence of children with worm infestations<br />
In rural areas, especially, there can be a great deal of seasonal fluctuation in the incidence<br />
of some illnesses; for example, diarrhoea is quite often much worse during the rainy season.<br />
This can have an important bearing on the timing of interventions (e.g. increase our efforts of<br />
giving <strong>nutrition</strong> messages about feeding during diarrhoea during the rainy season).<br />
Clinic and hospital records can provide very useful information about the incidence of<br />
different illnesses. Once again this can be checked by asking community members of their<br />
opinions about the prevalence and seasonality of different illnesses.<br />
21
LEVEL 4<br />
4.1 Nutrition Status<br />
There are several indica<strong>to</strong>rs of <strong>nutrition</strong> status: weight-for-age, height-for-age, weightfor-height,<br />
low birthweight, prevalence of anaemia.<br />
Once again it is advisable for the team <strong>to</strong> use different sources for this information. If the<br />
clinics and mobile points are reaching most of the community and they have a good data<br />
collection system then clinic and hospital data on the number of children underweight for age,<br />
incidence of low birthweight and prevalence of anaemia in pregnant women can be very<br />
useful.<br />
Unfortunately in many districts this information is not very reliable. There have been a<br />
number of very good national <strong>nutrition</strong>al surveys in the last few years which are readily available.<br />
The South African Vitamin A Consultative Group study, for instance, measured the vitamin A<br />
and iron levels and the weights and heights of young children all over the country. The <strong>Health</strong><br />
<strong>Systems</strong> <strong>Trust</strong> has a publication entitled “The Nutritional Status of South Africans: A Review<br />
of the Literature from 1975-1996” which summarises the results from most of these national<br />
surveys and is available from the HST offices. In addition it is worth trying <strong>to</strong> find out whether<br />
there have been any local surveys done by universities or the Medical Research Council.<br />
Once again interviewing key informants, such as senior nurses, clinic workers, community<br />
health workers, about the prevalence of severe mal<strong>nutrition</strong> and changes over the recent past<br />
can lead <strong>to</strong> valuable information about the extent and severity of the problem.<br />
Table 7: Assessment of Nutrition Status<br />
Information needed Source of Method for<br />
information collection<br />
1. What % of young children are National/Provincial Literature Review<br />
underweight?<br />
Statistics<br />
2. What % of young children are stunted Surveys from<br />
(low height-for-age)<br />
Medical Research<br />
3. What % of young children are wasted Council, Univer-<br />
(low weight for height)<br />
sities etc.<br />
4. What % of young children have<br />
vitamin A deficiency?<br />
5. What % of newborns weigh less than Hospital/Clinic Record/Case<br />
2,500g? Records Review<br />
6. Are there some areas in the district which<br />
have rates of low birth weight than others?<br />
7. Are these <strong>nutrition</strong> problems improving Community Key Informant<br />
or getting worse? members/health interviews<br />
8. What geographical areas, communities or workers<br />
ethnic groups are more likely <strong>to</strong> have<br />
<strong>nutrition</strong>al problems?<br />
22
FURTHER READING<br />
McCoy D, Bamford L. 1998. <strong>How</strong> <strong>to</strong> <strong>conduct</strong> a <strong>rapid</strong> situation analysis: A guide<br />
for health districts in South Africa. (<strong>Health</strong> <strong>Systems</strong> <strong>Trust</strong>.)<br />
Bennett J, Rohde J. 1999. Mapping for primary health care. (Management Sciences<br />
for <strong>Health</strong>.)<br />
Chopra M, Sanders D, et al. 1999. Kwik Skwiz #22 Improving growth moni<strong>to</strong>ring<br />
and promotion in PHC clinics: Lessons from Mount Frere health district.<br />
(University of the Western Cape and <strong>Health</strong> <strong>Systems</strong> <strong>Trust</strong>.)<br />
Chopra M, Sanders D, Puoane T et al. 1999. Integrated Nutrition Programme<br />
Planning: A training guide for district <strong>nutrition</strong> managers. (University of the<br />
Western Cape and <strong>Health</strong> <strong>Systems</strong> <strong>Trust</strong>.)<br />
McCoy D, Sai<strong>to</strong>witz R, Saasa M et al. 1996. Evaluation of the Primary School<br />
Nutrition Programme. (<strong>Health</strong> <strong>Systems</strong> <strong>Trust</strong>.)<br />
Strasser S, Puoane T et al. 1999. Kwik Skwiz # 16: The WHO ten steps – The way<br />
forward for improved care of severe mal<strong>nutrition</strong>. (<strong>Health</strong> <strong>Systems</strong> <strong>Trust</strong>)<br />
Vorster H, Oosthuizen W et al. The <strong>nutrition</strong>al status of South Africans: A review<br />
of the literature.<br />
23
APPENDIX 1: SAMPLE OBSERVATION<br />
CHECKLIST FOR ASSESSING GROWTH<br />
MONITORING AND PROMOTION<br />
SITE: ..................................................................................<br />
DATE OF ASSESSMENT: ..................................................<br />
CATEGORY OF WORKER: ............................................<br />
INITIALS OF ASSESSOR:.................................................<br />
PRACTICE YES NO<br />
Did the service provider:<br />
1. Greet the mother?<br />
2. Ask the mother the purpose of the visit?<br />
3. Ask the mother <strong>to</strong> remove the child’s clothing?<br />
4. Set the scale <strong>to</strong> 0?<br />
5. Ask the mother <strong>to</strong> put the child on the scale?<br />
6. Correctly read scale?<br />
7. Tell the mother whether her child has gained, lost weight<br />
or stayed the same since last weighing?<br />
8. Ask if the child has any health problems since last weighing?<br />
9. Explain the importance of gaining weight for health?<br />
10. Tell mother when <strong>to</strong> take child for next weighing?<br />
11. Make recommendations regarding child feeding and<br />
care?<br />
12. Stress importance of using locally available energy<br />
dense foods with examples?<br />
12. Explain about exclusive of breastfeeding and good<br />
weaning practices?<br />
13. Explain how <strong>to</strong> feed children during illness?<br />
14. Explain the purpose of growth moni<strong>to</strong>ring?<br />
15. Ask mother if she has any questions?<br />
16. Explain where <strong>to</strong> go for growth moni<strong>to</strong>ring services?<br />
Adapted from N. Ndabula A pro<strong>to</strong>col <strong>to</strong> evaluate the quality of community based growth moni<strong>to</strong>ring and<br />
promotion in the Eastern Cape Masters in Public <strong>Health</strong> University of the Western Cape<br />
25
APPENDIX 2: SAMPLE CHECKLIST FOR<br />
ASSESSING COMMON INFANT FEEDING<br />
PRACTICES IN THE COMMUNITY<br />
Age Estimated Common reasons for s<strong>to</strong>pping Foods (other than Frequency Common feeding<br />
Group breastfeed breastfeeding before 2 years (or breastfmilk) commonly and amount problems; reasons<br />
ing rate supplementation before 4 months) given fed<br />
2 months S<strong>to</strong>pping:<br />
up <strong>to</strong> 4<br />
months Supplementation:<br />
4 months<br />
<strong>to</strong> 6<br />
months<br />
6 months<br />
<strong>to</strong> 12<br />
months<br />
12 months<br />
<strong>to</strong> 2 years<br />
Remember <strong>to</strong> note sources of information.<br />
Taken from: Pro<strong>to</strong>col for adapting feeding recommendations. IMCI initiative WHO/UNICEF 1999<br />
26
APPENDIX 3: EXAMPLE OF A SCORING<br />
SYSTEM FOR TARGETING<br />
INDIVIDUAL SCHOOLS WITHIN A<br />
DISTRICT OR SUB-DISTRICT<br />
Score<br />
Criteria 0 1 2 3<br />
Proportion of school entrants who are stunted < 5% 5 - 10% 11 - 15% > 15%<br />
State of school (electricity) Grid Alternative None -<br />
Electricity source of<br />
electricity<br />
State of school (water supply) Fully Less than 5 One well/ No source<br />
serviced taps for pump in of water on<br />
entire school school<br />
school grounds grounds<br />
Number of children per classroom - 20-10 41-60 >60 or 3 - 6 km > 6 km<br />
Sanitation and <strong>to</strong>ilets One flush One flush Adequate Inadequate<br />
<strong>to</strong>ilet per <strong>to</strong>ilet per VIP sanitation<br />
100 children 100 children latrines<br />
or less or more<br />
School drop-out rate between sub-A and Grade 8 10% >20%<br />
27