The Tensilon Test: A Case Report - Gundersen Health System
The Tensilon Test: A Case Report - Gundersen Health System
The Tensilon Test: A Case Report - Gundersen Health System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Author:<br />
Balaji Vishwanat, MD<br />
Physician Emeritus,<br />
Department of Neurology<br />
<strong>Gundersen</strong> Lutheran <strong>Health</strong> <strong>System</strong><br />
La Crosse, Wisconsin<br />
Address for correspondence:<br />
David Hartman, PhD,<br />
BC-ANCDS(A)<br />
Mail Stop EB3-002<br />
<strong>Gundersen</strong> Lutheran <strong>Health</strong> <strong>System</strong><br />
1900 South Avenue<br />
La Crosse, WI 54601<br />
Telephone: (608) 775-9000<br />
Fax: (608) 775-6358<br />
email: dehartma@gundluth.org<br />
<strong>The</strong> <strong>Tensilon</strong> <strong>Test</strong>: A <strong>Case</strong> <strong>Report</strong><br />
Abstract<br />
A patient presented with symptoms and signs consistent with a diagnosis of myasthenia<br />
gravis (MG), a neuromuscular junction disorder. Herein, findings from the patient’s physical<br />
examination and results of the edrophonium chloride (<strong>Tensilon</strong>) test administered to confirm<br />
the MG diagnosis are reported. <strong>The</strong> symptoms and underlying pathophysiology of MG are<br />
described. Finally the array of tests that can be used to aid in a diagnosis of MG are reviewed.<br />
A<br />
68-year-old man presented with a 2-month history of<br />
weakness of his jaw, drooping of his left upper eyelid, and<br />
double vision. All his symptoms were intermittent in nature. His<br />
jaw tired after he had chewed 3 or 4 mouthfuls and would recover<br />
after resting for a couple of minutes. <strong>The</strong> left upper eyelid would<br />
be fine in the morning but would start drooping by noon and stay<br />
that way the rest of the day. <strong>The</strong> double vision was also prominent<br />
toward the end of the day. He had experienced no difficulty<br />
swallowing or breathing. He had experienced no weakness of his<br />
neck muscles. His extremities were perfectly strong. Medical history<br />
was significant for rheumatic fever in childhood leading to aortic<br />
stenosis. He required aortic valve replacement and 2 revisions.<br />
Complete review of systems was unremarkable. <strong>The</strong> patient was<br />
taking no prescription medications.<br />
Findings from a general physical examination were<br />
unremarkable. A very definite ptosis was present on the left. <strong>The</strong><br />
patient had binocular diplopia on right and left lateral gaze. Jaw<br />
muscles were normal but easily fatigued. Mild bilateral lower motor<br />
neuron facial weakness was evident. Limb musculature strength<br />
was normal. Deep tendon reflexes were normal and the plantar<br />
responses flexor. <strong>The</strong>re were no sensory deficits.<br />
An edrophonium chloride (<strong>Tensilon</strong>) test was performed<br />
(Figures 1 and 2).<br />
(1) What is the likely diagnosis?<br />
(2) What does the <strong>Tensilon</strong> test show?<br />
(3) How would you manage this patient?<br />
junction by antibodies to the postsynaptic acetylcholine receptors<br />
(AChR). Normal quanta of acetylcholine are released at the<br />
nerve terminal, but the response is reduced, leading to weakness.<br />
In contrast, the defect in Lambert-Eaton syndrome lies in the<br />
presynaptic nerve terminals due to antibodies directed toward<br />
calcium channels and the release of insufficient quanta of<br />
acetylcholine. 1 Cobra venom and bungarotoxin produce blockage<br />
of neuromuscular transmission by prolonged nondepolarization of<br />
the neuromuscular junction. Botulinum toxin causes blockage of<br />
acetylcholine release from nerve terminals.<br />
In MG, the extraocular, facial, jaw, bulbar, neck, and shoulder<br />
girdle muscles are affected, most commonly in that order. <strong>The</strong><br />
extremity and respiratory muscles are also often involved. <strong>The</strong><br />
muscle weakness typically fluctuates, being minimal in the<br />
DISCUSSION<br />
This gentleman presented with classical symptoms and signs<br />
of myasthenia gravis (MG). MG is the prototypic neuromuscular<br />
junction disorder. Other entities in this spectrum are Lambert-<br />
Eaton myasthenic syndrome, botulism, congenital MG, familial<br />
infantile MG, and envenomation by cobra or alpha-bungarotoxin.<br />
A transitory form of MG affects 10% to 20% of the newborns<br />
whose mothers have autoimmune MG.<br />
<strong>The</strong> underlying pathophysiology in MG is distortion and<br />
simplification of the end-plate membrane in the neuromuscular<br />
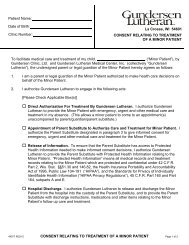
Figure 1. Ptosis of the left upper<br />
and right lower lid is evident.<br />
Figure 2. Following injection of<br />
the edrophonium chloride, the<br />
ptosis is resolved. <strong>The</strong> frontal<br />
and nasolabial creases are more<br />
prominent due to improved tone<br />
in the facial muscles.<br />
<strong>Gundersen</strong> Lutheran Medical Journal • Volume 5, Number 1, July 2008 19
morning and getting more noticeable toward the end of the day.<br />
Since MG is an autoimmune disease, patients tend to have an<br />
increased incidence of other disorders, such as rheumatoid arthritis,<br />
Hashimoto thyroiditis, and pernicious anemia.<br />
<strong>The</strong> <strong>Tensilon</strong> test can be very useful in the bedside diagnosis<br />
of MG. Ideally the test should be done in a double-blind fashion<br />
to improve objectivity. Edrophonium chloride is a short-acting<br />
cholinesterase inhibitor and will rapidly improve neuromuscular<br />
deficits due to MG. Ten mg of the drug in 1- cc doses are<br />
administered intravenously over about a minute. It is important<br />
that readily observable deficits are present so that any improvement<br />
that occurs is appreciated. <strong>The</strong> effect lasts about 5 minutes. <strong>The</strong><br />
usual side effects are lacrymation, sweating, abdominal cramps,<br />
bradycardia, and occasionally hypotension, all resolving within<br />
5 minutes. <strong>The</strong> author dilutes 1 cc of the drug with 1 cc of the<br />
patient’s blood and administers a 2-mg test dose. If there are no<br />
adverse effects, the remainder of the drug is given over the next<br />
minute. Electrocardiographic monitoring is not necessary.<br />
Another rapid and easy test for MG involves applying ice to<br />
the ptotic eyelid for a few minutes. Cooling maintains the sodium<br />
channels open for a longer period, thus enhancing the action<br />
potentials at the neuromuscular junction. This is the underlying<br />
principle that aggravates the symptoms of myotonia. <strong>The</strong> converse<br />
of this is also the reason for aggravation of symptoms in multiple<br />
sclerosis when the body temperature rises above normal.<br />
Laboratory tests can aid in diagnosis. Antibodies against AChR<br />
are found in most patients with MG. Antistriational antibodies are<br />
also found in patients who have thymic hyperplasia or thymoma.<br />
<strong>The</strong> antibody titers, however, do not correlate with the severity of<br />
the clinical illness.<br />
A small subset of patients with MG do not have AChR<br />
antibodies but may have antibodies to muscle-specific tyrosine<br />
kinase (MuSK). <strong>The</strong>se patients tend to have more prominent<br />
bulbar and respiratory muscle involvement and do not respond<br />
well to cholinesterase inhibitors. 2<br />
Since there is high incidence of thymic hyperplasia and of<br />
benign or malignant thymoma in patients with autoimmune MG,<br />
a computed tomographic (CT) scan of the chest should be obtained<br />
on all patients. Our patient’s CT scan revealed a thymoma.<br />
Repetitive nerve stimulation studies and single-fiber<br />
electromyography can also aid in diagnosis of MG.<br />
<strong>The</strong> immediate treatment of MG consists of an oral<br />
anticholinesterase-inhibiting drug such as pyridostigmine<br />
bromide. 3 <strong>The</strong> use of immunosuppressive drugs such as<br />
corticosteroids, azathioprine, cyclophosphamide, cyclosporin,<br />
mycophenolate mofetil, and rituximab may be necessary in some<br />
patients. Myasthenic crises usually respond well to plasmapheresis<br />
or intravenous immunoglobulin therapy. Thymectomy is<br />
indicated for thymoma and should be considered in all patients<br />
not responding to conventional medical therapies.<br />
Drugs known to cause neuromuscular blockage should be<br />
avoided. Other drugs that have a potential for aggravating the<br />
symptoms of MG include quinine, quinidine, procainamide,<br />
aminoglycosides, beta blockers, and calcium channel blockers.<br />
Induction of autoimmune MG by D-penicillamine 4 and statins 5<br />
is well documented.<br />
REFERENCES<br />
1. O’Neill JH, Murray NM, Newsom-Davis J. <strong>The</strong> Lambert-Eaton myasthenic<br />
syndrome. A review of 50 cases. Brain. 1988;111(Pt 3):577-596.<br />
2. Sanders DB, El-Salem K, Massey JM, McConville J, Vincent A. Clinical aspects of<br />
MuSK antibody positive seronegative MG. Neurology. 2003;60(12):1978-1980.<br />
3. Keesey JC. Clinical evaluation and management of myasthenia gravis. Muscle<br />
Nerve. 2004;29(4):484-505.<br />
4. Albers JW, Hodach RJ, Kimmel DW, Treacy WL. Penicillamine-associated<br />
myasthenia gravis. Neurology. 1980;30(11):1246-1249.<br />
5. Purvin V, Kawasaki A, Smith KH, Kesler A. Statin-associated myasthenia gravis:<br />
report of 4 cases and review of the literature. Medicine. 2006;85(2):82-85.<br />
Pelican<br />
Photograph by David E. Hartman, PhD<br />
<strong>Gundersen</strong> Lutheran<br />
20 <strong>Gundersen</strong> Lutheran Medical Journal • Volume 5, Number 1, July 2008