BadgerCare Plus & Medicaid SSI Provider Manual - Group Health ...
BadgerCare Plus & Medicaid SSI Provider Manual - Group Health ...
BadgerCare Plus & Medicaid SSI Provider Manual - Group Health ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Therapy Request Form<br />
Please indicate the type of therapy you are requesting (For speech therapy, please use specific form):<br />
Physical Occupational Pulmonary Cardiac<br />
Patient’s Name:<br />
DOB: ________________ ID#_____________________<br />
Ordering Physician:<br />
Clinic: ________________________________________<br />
Therapy <strong>Provider</strong>:<br />
Name/Specialty/Clinic<br />
Phone #: ___________________________<br />
Tax ID: _______________ Fax#:___________________<br />
Diagnosis: ICD-9: Date of Initial Eval:<br />
Is this a Worker’s Comp or accident case? Yes No<br />
Dates of service requested: __________________________________________________________<br />
Number of visits requested: __________________________________________________________<br />
PLEASE SEND EVALUATION FOR FIRST REQUEST ONLY.<br />
ADDITIONAL REQUESTS WILL NEED ONLY THE MOST RECENT VISIT NOTE.<br />
<strong>Provider</strong> Contact Name Phone # Date<br />
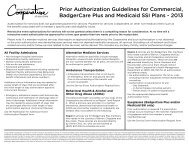
Prior authorization is not required for the initial evaluation and next five visits (first six visits) per calendar year. If<br />
additional visits are needed, authorization is required prior to the seventh visit. Services must be prescribed<br />
and monitored by a Primary Care Physician or Specialty Physician to be considered a covered benefit.<br />
Revised: 3/15/12 <strong>Health</strong> Management Fax: (715) 552-7202<br />
GHC11040