1.Tuberous xanthoma
1.Tuberous xanthoma
1.Tuberous xanthoma

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Go Back to the Top<br />
To Order, Visit the Purchasing Page for Details<br />
C. Xanthomas<br />
Definition<br />
Lipid-laden foamy histiocytes aggregate on the skin or mucous<br />
membranes to form yellowish lesions. This condition usually<br />
accompanies a systemic abnormality of lipid metabolism; however,<br />
lipid abnormality is not found in all cases. Xanthoma is divided<br />
by clinical features into several subtypes described below.<br />
Pathology<br />
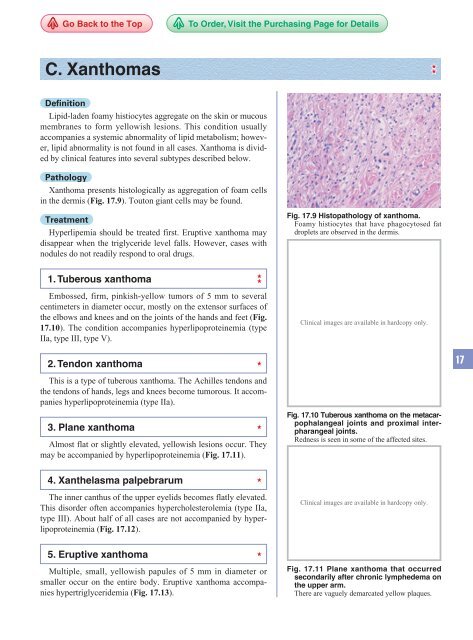
Xanthoma presents histologically as aggregation of foam cells<br />
in the dermis (Fig. 17.9). Touton giant cells may be found.<br />
Treatment<br />
Hyperlipemia should be treated first. Eruptive <strong>xanthoma</strong> may<br />
disappear when the triglyceride level falls. However, cases with<br />
nodules do not readily respond to oral drugs.<br />
Fig. 17.9 Histopathology of <strong>xanthoma</strong>.<br />
Foamy histiocytes that have phagocytosed fat<br />
droplets are observed in the dermis.<br />
1. Tuberous <strong>xanthoma</strong><br />
Embossed, firm, pinkish-yellow tumors of 5 mm to several<br />
centimeters in diameter occur, mostly on the extensor surfaces of<br />
the elbows and knees and on the joints of the hands and feet (Fig.<br />
17.10). The condition accompanies hyperlipoproteinemia (type<br />
IIa, type III, type V).<br />
Clinical images are available in hardcopy only.<br />
2. Tendon <strong>xanthoma</strong><br />
17<br />
This is a type of tuberous <strong>xanthoma</strong>. The Achilles tendons and<br />
the tendons of hands, legs and knees become tumorous. It accompanies<br />
hyperlipoproteinemia (type IIa).<br />
3. Plane <strong>xanthoma</strong><br />
Almost flat or slightly elevated, yellowish lesions occur. They<br />
may be accompanied by hyperlipoproteinemia (Fig. 17.11).<br />
Fig. 17.10 Tuberous <strong>xanthoma</strong> on the metacarpophalangeal<br />
joints and proximal interpharangeal<br />
joints.<br />
Redness is seen in some of the affected sites.<br />
4. Xanthelasma palpebrarum<br />
The inner canthus of the upper eyelids becomes flatly elevated.<br />
This disorder often accompanies hypercholesterolemia (type IIa,<br />
type III). About half of all cases are not accompanied by hyperlipoproteinemia<br />
(Fig. 17.12).<br />
Clinical images are available in hardcopy only.<br />
5. Eruptive <strong>xanthoma</strong><br />
Multiple, small, yellowish papules of 5 mm in diameter or<br />
smaller occur on the entire body. Eruptive <strong>xanthoma</strong> accompanies<br />
hypertriglyceridemia (Fig. 17.13).<br />
Fig. 17.11 Plane <strong>xanthoma</strong> that occurred<br />
secondarily after chronic lymphedema on<br />
the upper arm.<br />
There are vaguely demarcated yellow plaques.
278 17 Metabolic Disorders<br />
Clinical images are available in hardcopy only.<br />
Clinical images are available in hardcopy only.<br />
Fig. 17.12 Xanthelasma palpebrarum.<br />
Flatly elevated yellow plaques occur on the inner canthus of the upper<br />
and lower eyelids, accompanied by mild infiltration.<br />
Fig. 17.13 Eruptive <strong>xanthoma</strong>.<br />
D. Electrolytic disorders<br />
1. Acrodermatitis enteropathica<br />
Synonym: Zinc deficiency syndrome<br />
17<br />
Clinical images are available in hardcopy only.<br />
Clinical images are available in hardcopy only.<br />
Clinical images are available in hardcopy only.<br />
Fig. 17.14 Acrodermatitis enteropathica.<br />
<br />
<br />
<br />
Outline<br />
This is a zinc deficiency whose main symptoms are dermatitis,<br />
alopecia and diarrhea.<br />
The main types are a congenital type (autosomal recessively<br />
inherited) and an acquired type that is caused by<br />
administration of parenteral central venous nutrition or<br />
excision of the digestive tract.<br />
Erythema and erosion form on the distal portions of the<br />
extremities, and on the genitalia and orifices (the periphery<br />
of the eyes and mouth, nares, and auditory meatus),<br />
presenting clinical features similar to psoriasis, seborrheic<br />
dermatitis and cutaneous candidiasis.<br />
Clinical features<br />
Dermatitis tends to occur on sites that have mechanical pressure,<br />
such as the distal portions of the extremities, the genitalia,<br />
and the facial orifices (the periphery of the eyes and mouth, nares,<br />
and auditory meatus; Fig. 17.14). Acrodermatitis enteropathica<br />
begins with papules, small blisters, or erythema accompanied by<br />
pustules, and progresses to erosion and crusts. Annular scaling is<br />
clinically observed, resembling psoriasis, impetigo, seborrheic<br />
dermatitis and cutaneous candidiasis. Nail deformity and perionychia<br />
occur.<br />
Alopecia occurs in almost all cases, appearing on the occipital<br />
and temporal region of the head first and then spreading to the<br />
entire scalp and eyebrows. Diarrhea and vomiting recur.<br />
Pathogenesis<br />
The congenital type of acrodermatitis enteropathica is autosomal<br />
recessively inherited. It is caused by a mutation in the<br />
Go Back to the Top<br />
To Order, Visit the Purchasing Page for Details