Building on progress - where next for organ donation policy in ... - BMA
Building on progress - where next for organ donation policy in ... - BMA
Building on progress - where next for organ donation policy in ... - BMA

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> Progress:<br />
Where <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the UK?<br />
British Medical Associati<strong>on</strong><br />
February 2012
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
C<strong>on</strong>tents<br />
1. Introducti<strong>on</strong> ....................................................................................................................3<br />
The <strong>BMA</strong>’s <strong>in</strong>terest <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> ...............................................................................3<br />
Organ D<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the 21st Century .................................................................................3<br />
What has happened s<strong>in</strong>ce the last report?.........................................................................4<br />
Why are we publish<strong>in</strong>g this report? ...................................................................................5<br />
2. D<strong>on</strong>ati<strong>on</strong> rates and trends.............................................................................................6<br />
Types of d<strong>on</strong>ati<strong>on</strong>..............................................................................................................7<br />
The transplant wait<strong>in</strong>g list .................................................................................................8<br />
The NHS Organ D<strong>on</strong>or Register .........................................................................................8<br />
What is reas<strong>on</strong>able to expect <strong>in</strong> the UK? .........................................................................10<br />
3. The current legislative framework..............................................................................11<br />
C<strong>on</strong>sent <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> after death..........................................................................11<br />
D<strong>on</strong>ati<strong>on</strong> after circulatory death (DCD)............................................................................12<br />
Liv<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> .....................................................................................................13<br />
Mental capacity legislati<strong>on</strong> ..............................................................................................13<br />
EU Organs Directive.........................................................................................................14<br />
4. Develop<strong>in</strong>g the <strong>in</strong>frastructure.....................................................................................15<br />
The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce ........................................................................................15<br />
Cl<strong>in</strong>ical leads, specialist nurses and d<strong>on</strong>ati<strong>on</strong> committees ................................................17<br />
D<strong>on</strong>or identificati<strong>on</strong> and referral......................................................................................20<br />
Nati<strong>on</strong>al Organ Retrieval Service ......................................................................................21<br />
The <strong>organ</strong> allocati<strong>on</strong> and offer<strong>in</strong>g system ........................................................................22<br />
The potential d<strong>on</strong>or audit................................................................................................22<br />
Cl<strong>in</strong>ical, legal and ethical guidance..................................................................................25<br />
What more can or should be d<strong>on</strong>e? ................................................................................31<br />
Organ d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the NHS .............................................................................................34<br />
5. Increas<strong>in</strong>g the number of d<strong>on</strong>ors................................................................................36<br />
Expand<strong>in</strong>g the pool of potential d<strong>on</strong>ors...........................................................................36<br />
Ensur<strong>in</strong>g <strong>in</strong>dividuals’ wishes are known ...........................................................................41<br />
Mandated choice.............................................................................................................44<br />
Opt-out with safeguards..................................................................................................46<br />
Reciprocity.......................................................................................................................52<br />
A regulated market .........................................................................................................56<br />
Payment of funeral expenses ...........................................................................................60<br />
6. The way <strong>for</strong>ward <strong>for</strong> <strong>policy</strong>.........................................................................................66<br />
What can we learn from Spa<strong>in</strong>? ......................................................................................66<br />
Where <strong>next</strong> <strong>for</strong> public <strong>policy</strong>?..........................................................................................68<br />
7. Summary of key po<strong>in</strong>ts................................................................................................69<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 1
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
Medical Ethics Committee<br />
A publicati<strong>on</strong> from the <strong>BMA</strong>’s Medical Ethics Committee (MEC) whose membership <strong>for</strong> 2011/12 was:<br />
Dr Anth<strong>on</strong>y Calland*, Chairman General practice (retired), Gwent<br />
Dr J S Bamrah<br />
Psychiatry, Manchester<br />
Dr Mary Church<br />
General practice, Glasgow<br />
Dr John Chisholm* (Deputy)<br />
General practice, Bromley<br />
Professor Bobbie Farsides<br />
Medical law and ethics, Bright<strong>on</strong><br />
Professor Ilora F<strong>in</strong>lay*<br />
Palliative medic<strong>in</strong>e, Cardiff<br />
Claire Foster<br />
Medical ethics, L<strong>on</strong>d<strong>on</strong><br />
Professor Rob<strong>in</strong> Gill*<br />
Theology, Canterbury<br />
Professor Raanan Gill<strong>on</strong>*<br />
General practice (retired) and medical ethics, L<strong>on</strong>d<strong>on</strong><br />
Dr Zoe Greaves<br />
Junior doctor, Cleveland<br />
Dr Evan Harris*<br />
Former MP and hospital doctor, Ox<strong>for</strong>d<br />
Professor Emily Jacks<strong>on</strong><br />
Medical law and ethics, L<strong>on</strong>d<strong>on</strong><br />
Dr Surendra Kumar<br />
General practice, Widnes<br />
Professor Graeme Laurie<br />
Medical law, Ed<strong>in</strong>burgh<br />
Dr Lewis Morris<strong>on</strong><br />
General and geriatric medic<strong>in</strong>e, Lothian<br />
Dr A<strong>in</strong>sley News<strong>on</strong><br />
Biomedical ethics, Bristol<br />
Professor Julian Savulescu<br />
Practical ethics, Ox<strong>for</strong>d<br />
Dr Peter Tiplady (Deputy)<br />
Public health, Carlisle<br />
Dr Frank Wells<br />
Pharmaceutical physician (retired), Ipswich<br />
Dr M E Jan Wise<br />
Psychiatry, L<strong>on</strong>d<strong>on</strong><br />
<strong>BMA</strong> Chief Officers (ex officio)<br />
Professor David Haslam<br />
President<br />
Dr Steve Hajioff<br />
Chairman of the Representative Body<br />
Dr Hamish Meldrum<br />
Chairman of Council<br />
Dr Andrew Dearden<br />
Treasurer<br />
* Formed a sub-group <strong>on</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> to discuss this report<br />
Head of Professi<strong>on</strong>al Activities<br />
Report written by<br />
Professor Vivienne Nathans<strong>on</strong><br />
Ver<strong>on</strong>ica English<br />
In<strong>for</strong>mati<strong>on</strong> about this and other subjects covered by the Medical Ethics Committee may<br />
be obta<strong>in</strong>ed from the <strong>BMA</strong>’s website at: www.bma.org.uk/ethics or by c<strong>on</strong>tact<strong>in</strong>g the<br />
Medical Ethics Department at: British Medical Associati<strong>on</strong>, <strong>BMA</strong> House, Tavistock Square,<br />
L<strong>on</strong>d<strong>on</strong> WC1H 9JP. Tel: 020 7383 6286, Email: ethics@bma.org.uk<br />
Acknowledgements<br />
The <strong>BMA</strong> would like to thank the many <strong>in</strong>dividuals and <strong>organ</strong>isati<strong>on</strong>s who provided advice and<br />
<strong>in</strong><strong>for</strong>mati<strong>on</strong> dur<strong>in</strong>g the preparati<strong>on</strong> of this paper and those who commented <strong>on</strong> an earlier draft.<br />
2<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
1 Introducti<strong>on</strong><br />
The <strong>BMA</strong>’s <strong>in</strong>terest <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong><br />
The British Medical Associati<strong>on</strong> is <strong>in</strong>terested <strong>in</strong> all issues affect<strong>in</strong>g doctors and patients and has<br />
campaigned <strong>for</strong> improvements <strong>in</strong> a range of public health measures. Organ transplantati<strong>on</strong> is an<br />
area that has seen amaz<strong>in</strong>g medical achievements but has not yet reached its full life-sav<strong>in</strong>g and<br />
life-trans<strong>for</strong>m<strong>in</strong>g potential. As doctors it is difficult to see our patients dy<strong>in</strong>g and suffer<strong>in</strong>g when<br />
their lives could be saved or dramatically improved by a transplant. It is even more difficult when<br />
we know that lives are be<strong>in</strong>g lost unnecessarily because of poor <strong>organ</strong>isati<strong>on</strong>, lack of fund<strong>in</strong>g or<br />
because people who are will<strong>in</strong>g to d<strong>on</strong>ate <strong>organ</strong>s after their death simply never get around to<br />
mak<strong>in</strong>g their views known, result<strong>in</strong>g <strong>in</strong> relatives mak<strong>in</strong>g a decisi<strong>on</strong> without know<strong>in</strong>g the <strong>in</strong>dividual<br />
was will<strong>in</strong>g to d<strong>on</strong>ate. For this reas<strong>on</strong> the <strong>BMA</strong> began <strong>in</strong> the 1990s to look at ways <strong>in</strong> which the<br />
<strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> system could be improved to reduce the number of avoidable deaths, <strong>in</strong>crease<br />
the number of lives that could be trans<strong>for</strong>med by a transplant and make maximum use of the<br />
high level of altruism <strong>in</strong> UK society.<br />
This report focuses <strong>on</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. It is important to recognise, however, that another equally<br />
important and complementary way of reduc<strong>in</strong>g the number of unnecessary deaths is to focus <strong>on</strong><br />
public health measures to reduce the <strong>in</strong>cidence of chr<strong>on</strong>ic diseases that lead to the need <strong>for</strong> an<br />
<strong>organ</strong> transplant. The <strong>in</strong>creas<strong>in</strong>g <strong>in</strong>cidence of obesity and diabetes <strong>in</strong> our society, <strong>for</strong> example,<br />
which can be partly attributed to changes <strong>in</strong> our diet and our sedentary lifestyle, is a major public<br />
health issue that needs to be addressed as a matter of urgency. Public health measures and early<br />
<strong>in</strong>terventi<strong>on</strong>s to reduce demand <strong>for</strong> d<strong>on</strong>ated <strong>organ</strong>s and practical steps to improve the <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> system are both important; this report focuses <strong>on</strong> the latter.<br />
Organ D<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the 21st Century<br />
The <strong>BMA</strong>’s Medical Ethics Committee has discussed <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>on</strong> many occasi<strong>on</strong>s and,<br />
<strong>in</strong> 1999, the <strong>BMA</strong>’s Annual Representatives Meet<strong>in</strong>g adopted a <strong>policy</strong> call<strong>in</strong>g <strong>on</strong> the <strong>BMA</strong> to<br />
campaign <strong>for</strong> an opt-out system <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Follow<strong>in</strong>g this <strong>policy</strong> decisi<strong>on</strong> the <strong>BMA</strong><br />
published a report <strong>in</strong> 2000, Organ D<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the 21st Century – Time <strong>for</strong> a C<strong>on</strong>solidated<br />
Approach. This emphasised that shift<strong>in</strong>g to an opt-out system with safeguards would not make<br />
sufficient difference <strong>on</strong> its own but that this needed to be accompanied by a radical review of<br />
the <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> system with new legislati<strong>on</strong> and major changes to the <strong>in</strong>frastructure. Whilst<br />
undertak<strong>in</strong>g the work <strong>for</strong> this report it became apparent that a number of other <strong>organ</strong>isati<strong>on</strong>s<br />
were also call<strong>in</strong>g <strong>for</strong> changes to the <strong>in</strong>frastructure, but <strong>on</strong> an <strong>in</strong>dividual basis with little<br />
co-operati<strong>on</strong> or co-ord<strong>in</strong>ati<strong>on</strong>. The <strong>BMA</strong> there<strong>for</strong>e established the Transplant Partnership, a<br />
coaliti<strong>on</strong> of 18 professi<strong>on</strong>al and patient groups all committed to improv<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> rates<br />
<strong>in</strong> the UK. The Transplant Partnership undertook awareness-rais<strong>in</strong>g work with politicians and the<br />
public and liaised very effectively with the then leaders of UK Transplant and the <strong>policy</strong> team at<br />
the Department of Health. The Partnership lobbied <strong>on</strong> changes <strong>in</strong> legislati<strong>on</strong> and <strong>for</strong> practical<br />
improvements. The <strong>BMA</strong> also c<strong>on</strong>t<strong>in</strong>ued to encourage and facilitate debate about an opt-out<br />
system with safeguards, as <strong>on</strong>e part of this broader strategy.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 3
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
What has happened s<strong>in</strong>ce the last report?<br />
There have been dramatic improvements <strong>in</strong> the <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> system s<strong>in</strong>ce the <strong>BMA</strong>’s last report<br />
<strong>on</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> was published <strong>in</strong> 2000.<br />
• New legislati<strong>on</strong> has been passed throughout the UK provid<strong>in</strong>g a clear legal framework with<strong>in</strong><br />
which <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> can flourish. Legal uncerta<strong>in</strong>ties around c<strong>on</strong>sent and n<strong>on</strong>-heartbeat<strong>in</strong>g<br />
d<strong>on</strong>ati<strong>on</strong> (now referred to as d<strong>on</strong>ati<strong>on</strong> after circulatory death), have been clarified and a new<br />
legal system has been established <strong>for</strong> liv<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> provid<strong>in</strong>g a more rati<strong>on</strong>al and<br />
streaml<strong>in</strong>ed approach (see secti<strong>on</strong> 3).<br />
• A thorough and comprehensive review of the <strong>in</strong>frastructure with<strong>in</strong> which <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> takes<br />
place has been undertaken by an Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (see secti<strong>on</strong> 4) established by the<br />
last Government. It believed that many of the problems were caused by the lack of a structured<br />
and systematic approach to <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. The Task<strong>for</strong>ce looked at the system as a whole<br />
identify<strong>in</strong>g strengths and weaknesses with a view to design<strong>in</strong>g a nati<strong>on</strong>al system based <strong>on</strong> best<br />
practice around the country. The Task<strong>for</strong>ce also looked at <strong>in</strong>ternati<strong>on</strong>al models, such as those <strong>in</strong><br />
Spa<strong>in</strong> and the USA to see what, if any, less<strong>on</strong>s could be learned.<br />
• The Task<strong>for</strong>ce came up with 14 wide-rang<strong>in</strong>g and far-reach<strong>in</strong>g recommendati<strong>on</strong>s which, it<br />
believed, could <strong>in</strong>crease d<strong>on</strong>ati<strong>on</strong> rates by 50% by 2013 (an <strong>in</strong>crease of 405 deceased d<strong>on</strong>ors<br />
by 2012/13 compared with the 2007/08 basel<strong>in</strong>e of 809). It was adamant, however, that if the<br />
re<strong>for</strong>m was to be successful it would require clear political commitment, f<strong>in</strong>ancial <strong>in</strong>vestment<br />
and a will<strong>in</strong>gness to change established practice.<br />
• The Government and the Devolved Health Adm<strong>in</strong>istrati<strong>on</strong>s accepted all of the recommendati<strong>on</strong>s<br />
and provided the full fund<strong>in</strong>g requested. An Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce Programme Delivery<br />
Board was established and Mr Chris Rudge, <strong>for</strong>merly Medical Director of UK Transplant, was<br />
appo<strong>in</strong>ted as the first Nati<strong>on</strong>al Cl<strong>in</strong>ical Director <strong>for</strong> Transplantati<strong>on</strong> to manage and oversee<br />
implementati<strong>on</strong> of the recommendati<strong>on</strong>s <strong>on</strong> a day-to-day basis.<br />
• The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce undertook a review of the impact of <strong>in</strong>troduc<strong>in</strong>g an opt-out<br />
system <strong>in</strong> the UK. After a thorough review it decided aga<strong>in</strong>st recommend<strong>in</strong>g such a shift at that<br />
time, <strong>for</strong> various reas<strong>on</strong>s <strong>in</strong>clud<strong>in</strong>g the belief that the recommendati<strong>on</strong>s it had already made<br />
could make such a shift unnecessary. It recommended that the issue should be reviewed aga<strong>in</strong><br />
<strong>in</strong> the future if necessary.<br />
4<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
Why are we publish<strong>in</strong>g this report?<br />
The <strong>BMA</strong> has three ma<strong>in</strong> aims <strong>in</strong> produc<strong>in</strong>g this report.<br />
1. To acknowledge and celebrate the significant improvements that have been achieved and<br />
the c<strong>on</strong>siderable amount of work that has g<strong>on</strong>e <strong>in</strong>to this<br />
2. To highlight the fact that, despite these achievements, people are still dy<strong>in</strong>g unnecessarily<br />
because of a lack of <strong>organ</strong>s and<br />
3. To encourage health professi<strong>on</strong>als, <strong>policy</strong>-makers and the public to c<strong>on</strong>sider what more<br />
can and should be d<strong>on</strong>e.<br />
Four years after the publicati<strong>on</strong> of the Task<strong>for</strong>ce Report, we have seen significant improvements<br />
<strong>in</strong> the <strong>in</strong>frastructure and <strong>in</strong>creased d<strong>on</strong>or rates. As the implementati<strong>on</strong> programme reaches fruiti<strong>on</strong><br />
and the new systems and arrangements are becom<strong>in</strong>g settled, we need to decide, as a society,<br />
what the <strong>next</strong> steps should be. Now that we have a well-<strong>organ</strong>ised, well-funded, comprehensive<br />
<strong>in</strong>frastructure <strong>in</strong> place, is that enough? Can we say we have d<strong>on</strong>e all we can? Or, should we now<br />
look to go further and build <strong>on</strong> this <strong>progress</strong> by shift<strong>in</strong>g our attenti<strong>on</strong> to new ways of <strong>in</strong>creas<strong>in</strong>g<br />
the number of d<strong>on</strong>ors and the number of lives saved?<br />
We are at a cross-roads <strong>in</strong> terms of public <strong>policy</strong> <strong>on</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Should we stop now?<br />
Or should we cautiously move <strong>for</strong>ward? Nobody wants to underm<strong>in</strong>e what has already been<br />
achieved, but nor do we want to stop too so<strong>on</strong>, be<strong>for</strong>e every reas<strong>on</strong>able avenue has been<br />
properly explored. The <strong>in</strong><strong>for</strong>mati<strong>on</strong> provided <strong>in</strong> this report is aimed at encourag<strong>in</strong>g debate<br />
about these important questi<strong>on</strong>s.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 5
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
2 D<strong>on</strong>ati<strong>on</strong> rates and trends<br />
For more than a decade significant attenti<strong>on</strong> has been given to address<strong>in</strong>g the large and <strong>in</strong>creas<strong>in</strong>g<br />
gap between the number of <strong>organ</strong>s available <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> and the number of people requir<strong>in</strong>g a<br />
transplant. For many years the wait<strong>in</strong>g list <strong>in</strong>creased while the number of d<strong>on</strong>ors rema<strong>in</strong>ed fairly<br />
static. S<strong>in</strong>ce 2008, when the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce Report was published (see secti<strong>on</strong> 4),<br />
there has been major <strong>in</strong>vestment, re<strong>organ</strong>isati<strong>on</strong> and change. The latest published data (2010/11)<br />
show that over the last three years, d<strong>on</strong>ati<strong>on</strong> rates from deceased d<strong>on</strong>ors have improved by 25%<br />
(compared with 2007/08). 1 More recent data provided by NHS Blood and Transplant (NHS BT) show<br />
that the total <strong>in</strong>crease is projected to rise to 34% by April 2012 (based <strong>on</strong> d<strong>on</strong>ors up to 8 January<br />
2012). 2 Much, although not all, of this <strong>in</strong>crease is likely to be a result of the implementati<strong>on</strong> of the<br />
Task<strong>for</strong>ce’s recommendati<strong>on</strong>s although it is difficult to accurately judge the impact of specific<br />
changes. The Task<strong>for</strong>ce was c<strong>on</strong>fident that, with the changes it proposed, d<strong>on</strong>ati<strong>on</strong> rates could<br />
<strong>in</strong>crease by 50% with<strong>in</strong> five years 3 – an <strong>in</strong>crease of 405 d<strong>on</strong>ors by 2013.<br />
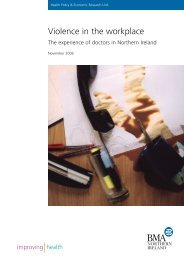
Number of deceased d<strong>on</strong>ors and transplants <strong>in</strong> the UK, 1 April 2001-31 March 2011,<br />
and patients <strong>on</strong> the active transplant lists at 31 March<br />
8000<br />
7655<br />
7877<br />
7997<br />
7800<br />
7219<br />
7000<br />
6698<br />
6000<br />
5604 5654 5673<br />
6142<br />
D<strong>on</strong>ors<br />
5000<br />
Transplants<br />
Transplants list<br />
Number<br />
4000<br />
3000<br />
2000<br />
2247<br />
2388<br />
2396<br />
2241<br />
2195<br />
2385<br />
2381<br />
2552<br />
2645<br />
2695<br />
1000<br />
745<br />
777<br />
770<br />
751<br />
764<br />
793<br />
809<br />
899<br />
959<br />
1010<br />
0<br />
2001-2002 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 2007-2008 2008-2009 2009-2010 2010-2011<br />
Year<br />
Source: Transplant activity <strong>in</strong> the UK, 2010-2011, NHS Blood and Transplant<br />
Graph reproduced with k<strong>in</strong>d permissi<strong>on</strong> of NHS Blood and Transplant.<br />
Transplant rates have also improved but not to the same extent as d<strong>on</strong>ati<strong>on</strong> rates. A significant<br />
reas<strong>on</strong> <strong>for</strong> this disparity is that fewer <strong>organ</strong>s can be obta<strong>in</strong>ed from d<strong>on</strong>ors follow<strong>in</strong>g circulatory<br />
death (DCD) who made up the majority of the <strong>in</strong>crease <strong>in</strong> d<strong>on</strong>ors. NHS BT also acknowledges that<br />
a shift <strong>in</strong> the profile of d<strong>on</strong>ors has affected transplantati<strong>on</strong> rates. With d<strong>on</strong>ors of higher age (30%<br />
were aged 60 or more <strong>in</strong> 2010/11 compared with 16% <strong>in</strong> 2001/02) and body mass <strong>in</strong>dex (20%<br />
were cl<strong>in</strong>ically obese compared with 12% <strong>in</strong> 2001/02 4 ), the number and quality of <strong>organ</strong>s retrieved<br />
6<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
are reduced and so the growth <strong>in</strong> transplantati<strong>on</strong> is proporti<strong>on</strong>ately lower than the growth <strong>in</strong> the<br />
number of d<strong>on</strong>ors. 5 (The use of ‘higher risk d<strong>on</strong>ors’ is discussed <strong>in</strong> secti<strong>on</strong> 5.)<br />
Types of d<strong>on</strong>ati<strong>on</strong><br />
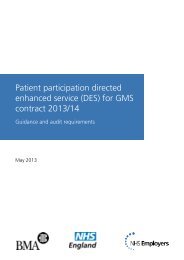
The graph below shows the way <strong>in</strong> which the type of d<strong>on</strong>or has changed over the last decade.<br />
In 2001/02 the vast majority of d<strong>on</strong>ors (62%) were people who were <strong>on</strong> a ventilator and had been<br />
declared dead follow<strong>in</strong>g bra<strong>in</strong> stem test<strong>in</strong>g (DBD d<strong>on</strong>ors). Only 42 (4%) were patients <strong>in</strong> whom<br />
treatment had been withdrawn and death diagnosed by cardiorespiratory failure (DCD d<strong>on</strong>ors –<br />
see secti<strong>on</strong> 3) and 34% were liv<strong>in</strong>g d<strong>on</strong>ors. By 2010/11 the positi<strong>on</strong> had changed completely with<br />
the majority be<strong>in</strong>g liv<strong>in</strong>g d<strong>on</strong>ors (51%) and DCD d<strong>on</strong>ors mak<strong>in</strong>g up 18% of the total number of<br />
d<strong>on</strong>ors and 37% of deceased d<strong>on</strong>ors.<br />
Number of deceased and liv<strong>in</strong>g d<strong>on</strong>ors <strong>in</strong> the UK, 1 April 2001-31 March 2011<br />
1100<br />
1000<br />
DBD d<strong>on</strong>ors<br />
DCD d<strong>on</strong>ors<br />
961<br />
1062<br />
1045<br />
900<br />
Liv<strong>in</strong>g d<strong>on</strong>ars<br />
858<br />
800<br />
Number<br />
700<br />
600<br />
500<br />
703<br />
716<br />
697<br />
472<br />
664<br />
485<br />
637<br />
599<br />
634<br />
702<br />
609<br />
611<br />
624<br />
637<br />
400<br />
300<br />
386<br />
397<br />
288<br />
335<br />
373<br />
200<br />
100<br />
0<br />
200<br />
159<br />
127<br />
87<br />
61<br />
73<br />
42<br />
2001-2002 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 2007-2008 2008-2009 2009-2010 2010-2011<br />
Year<br />
Source: Transplant activity <strong>in</strong> the UK, 2010-2011, NHS Blood and Transplant<br />
Graph reproduced with k<strong>in</strong>d permissi<strong>on</strong> of NHS Blood and Transplant.<br />
There are a number of reas<strong>on</strong>s <strong>for</strong> this change. Much of the <strong>in</strong>crease <strong>in</strong> liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> has<br />
resulted from a change <strong>in</strong> culture with<strong>in</strong> the transplant community which has facilitated expansi<strong>on</strong><br />
and promoted awareness of the opti<strong>on</strong> of liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong>. This has been aided by legislative<br />
changes which led, <strong>in</strong> 2006, to the <strong>in</strong>troducti<strong>on</strong> of a new, streaml<strong>in</strong>ed approval process <strong>for</strong> liv<strong>in</strong>g<br />
d<strong>on</strong>ati<strong>on</strong> and to paired and pooled d<strong>on</strong>ati<strong>on</strong>s (39 <strong>in</strong> 2010/11) and altruistic d<strong>on</strong>ati<strong>on</strong> to strangers<br />
(28 <strong>in</strong> 2010/11) 6 be<strong>in</strong>g allowed <strong>for</strong> the first time (see secti<strong>on</strong> 3). The <strong>in</strong>crease <strong>in</strong> DCD d<strong>on</strong>ors can<br />
also be attributed, <strong>in</strong> part at least, to chang<strong>in</strong>g views and practice with<strong>in</strong> the transplant community<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 7
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
and legislati<strong>on</strong> which clarified the law <strong>on</strong> DCD d<strong>on</strong>ors, 7 prompt<strong>in</strong>g significant <strong>in</strong>vestment <strong>in</strong> DCD<br />
programmes around the country. This shift <strong>in</strong> the type of d<strong>on</strong>or can also be seen as the result of<br />
a deliberate attempt to promote and facilitate liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> and d<strong>on</strong>ati<strong>on</strong> follow<strong>in</strong>g circulatory<br />
death <strong>in</strong> recogniti<strong>on</strong> of the fact that the number of potential DBD d<strong>on</strong>ors was decl<strong>in</strong><strong>in</strong>g and would<br />
be unable to meet demand. It has been recognised that more patients are surviv<strong>in</strong>g their <strong>in</strong>juries,<br />
and also that because of improved diagnostic equipment and test<strong>in</strong>g, it becomes clear at an earlier<br />
stage that recovery is not possible and so some patients are not be<strong>in</strong>g transferred to an <strong>in</strong>tensive<br />
care unit (ICU).<br />
Whilst the potential d<strong>on</strong>or audit (see secti<strong>on</strong> 4) <strong>in</strong>dicates some areas of practice that can be<br />
improved to <strong>in</strong>crease the number of DBD d<strong>on</strong>ors, any resultant <strong>in</strong>crease will never be sufficient<br />
to meet demand. As a result of c<strong>on</strong>siderable ef<strong>for</strong>ts, however, the number of d<strong>on</strong>ors follow<strong>in</strong>g<br />
circulatory death has <strong>in</strong>creased by 135% s<strong>in</strong>ce 2006/07 (see graph above). The <strong>BMA</strong> has always<br />
supported the use of DCD d<strong>on</strong>ors both as a way of <strong>in</strong>creas<strong>in</strong>g the d<strong>on</strong>ati<strong>on</strong> rate and also as a way<br />
of facilitat<strong>in</strong>g the wishes of those who want to d<strong>on</strong>ate but do not die <strong>in</strong> circumstances <strong>in</strong> which<br />
DBD is an opti<strong>on</strong>.<br />
The transplant wait<strong>in</strong>g list<br />
At the end of March 2011, there were 7,800 people <strong>on</strong> the UK’s active wait<strong>in</strong>g list <strong>for</strong> a transplant<br />
and a further 2,783 were temporarily suspended from the list because they were unfit or otherwise<br />
unavailable <strong>for</strong> a transplant. 8 Although still high, 2010/11 saw the first drop <strong>in</strong> the number <strong>on</strong> the<br />
wait<strong>in</strong>g list (by 197 patients) <strong>for</strong> more than a decade. Whilst this is encourag<strong>in</strong>g, NHS BT po<strong>in</strong>ts<br />
out that this is unlikely to reflect a true reducti<strong>on</strong> <strong>in</strong> demand <strong>for</strong> transplantati<strong>on</strong> s<strong>in</strong>ce if there<br />
were an unlimited supply of <strong>organ</strong>s, many more people would go <strong>on</strong>to the wait<strong>in</strong>g list. 9 Similarly,<br />
although the data show 511 deaths of people <strong>on</strong> the wait<strong>in</strong>g list <strong>in</strong> 2010/11, 10 the true number<br />
of people who died because of the shortage of <strong>organ</strong>s is likely to be much higher. The figure of<br />
1,000 deaths – or three deaths per day – is usually quoted. 11<br />
The NHS Organ D<strong>on</strong>or Register<br />
The NHS Organ D<strong>on</strong>or Register (ODR) was orig<strong>in</strong>ally established to measure the effectiveness of<br />
awareness-rais<strong>in</strong>g campaigns and has gradually, over a period of time, taken <strong>on</strong> the important<br />
operati<strong>on</strong>al role it currently fulfils – a role it was never designed to undertake. Follow<strong>in</strong>g an<br />
<strong>in</strong>dependent review <strong>in</strong>to its operati<strong>on</strong> <strong>in</strong> 2010, 12 a number of changes have been implemented –<br />
and more are planned – to ensure the register is both robust and fit <strong>for</strong> its current purpose. The<br />
quality of the data held <strong>on</strong> the ODR has subsequently been <strong>in</strong>dependently reviewed and found<br />
to be ‘of a reas<strong>on</strong>able level <strong>in</strong> comparis<strong>on</strong> to other companies’. 13<br />
Over the last few years significant ef<strong>for</strong>t has been put <strong>in</strong>to <strong>in</strong>creas<strong>in</strong>g the number of people <strong>on</strong> the<br />
ODR. By January 2012, more than 18.5 milli<strong>on</strong> people had signed up, 14 compared with 8.3 milli<strong>on</strong><br />
when the <strong>BMA</strong>’s first report was published <strong>in</strong> 2000. This represents 29% of the UK populati<strong>on</strong><br />
who have <strong>for</strong>mally registered their wish to d<strong>on</strong>ate. This is encourag<strong>in</strong>g, but there is still a significant<br />
gap between this figure and the 70-90% who say, when questi<strong>on</strong>ed, that they support <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong>. Ef<strong>for</strong>ts are c<strong>on</strong>t<strong>in</strong>u<strong>in</strong>g to <strong>in</strong>crease the number of people <strong>on</strong> the ODR (see secti<strong>on</strong> 5).<br />
8<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
The <strong>BMA</strong> supports these ef<strong>for</strong>ts, believ<strong>in</strong>g that anyth<strong>in</strong>g that encourages <strong>in</strong>dividuals to th<strong>in</strong>k<br />
about, discuss and make known their views about d<strong>on</strong>ati<strong>on</strong> is to be welcomed. Whilst there is not<br />
a direct correlati<strong>on</strong> between the number <strong>on</strong> the ODR and d<strong>on</strong>ati<strong>on</strong> rates (because it is often not<br />
those who sign up who die) the more people who jo<strong>in</strong> the register, the more likely it is that when<br />
people die their wishes will be known. In 2010/11, <strong>for</strong> example, 33% of deceased <strong>organ</strong> d<strong>on</strong>ors<br />
were registered <strong>on</strong> the ODR 15 compared with <strong>on</strong>ly 19% <strong>in</strong> 2001/02. Nevertheless, this percentage<br />
<strong>in</strong>crease is lower than the <strong>in</strong>crease <strong>in</strong> the number of people <strong>on</strong> the register, support<strong>in</strong>g the idea<br />
that those who die and go <strong>on</strong> to d<strong>on</strong>ate are proporti<strong>on</strong>ately under-represented <strong>on</strong> the register.<br />
Sign<strong>in</strong>g up to the ODR provides the legal c<strong>on</strong>sent (authorisati<strong>on</strong> <strong>in</strong> Scotland) required to proceed<br />
with d<strong>on</strong>ati<strong>on</strong>. Where the <strong>in</strong>dividual’s wishes are known, the approach to relatives is usually easier<br />
and <strong>in</strong> the majority of cases families are keen to fulfil their relatives’ wishes. The potential d<strong>on</strong>or<br />
audit shows that the rate of family objecti<strong>on</strong> varies c<strong>on</strong>siderably accord<strong>in</strong>g to whether the potential<br />
d<strong>on</strong>or is <strong>on</strong> the ODR. It is unusual <strong>for</strong> families of potential DBD d<strong>on</strong>ors to object to d<strong>on</strong>ati<strong>on</strong> if<br />
they know that is what the deceased wanted. Nevertheless, although they do not have a legal<br />
right of veto, <strong>where</strong>, despite encouragement, there is str<strong>on</strong>g and susta<strong>in</strong>ed oppositi<strong>on</strong> from the<br />
family, d<strong>on</strong>ati<strong>on</strong> is unlikely to proceed (see secti<strong>on</strong> 3). The message must, there<strong>for</strong>e, go out to<br />
those who wish to d<strong>on</strong>ate that it is essential that they <strong>in</strong><strong>for</strong>m their relatives of their wish to<br />
d<strong>on</strong>ate and that any disagreement is resolved be<strong>for</strong>e the situati<strong>on</strong> arises.<br />
What is it reas<strong>on</strong>able to expect <strong>in</strong> the UK?<br />
The UK does not fare well <strong>in</strong> <strong>in</strong>ternati<strong>on</strong>al comparis<strong>on</strong>s of d<strong>on</strong>ati<strong>on</strong> rates and, despite recent<br />
improvements, rema<strong>in</strong>s towards the lower end of European <strong>organ</strong> d<strong>on</strong>or rates.<br />
35<br />
Deceased d<strong>on</strong>ors (per milli<strong>on</strong> populati<strong>on</strong>) 2010<br />
30<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
Spa<strong>in</strong><br />
Croatia<br />
Portugal<br />
France<br />
Austria<br />
Italy<br />
Norway<br />
Slovenia<br />
Belguim<br />
Czech Republic<br />
Est<strong>on</strong>ia<br />
F<strong>in</strong>land<br />
Slovakia<br />
UK<br />
Hungary<br />
Germany<br />
Latvia<br />
Netherlands<br />
Poland<br />
Denmark<br />
Sweden<br />
Switzerland<br />
Ireland<br />
Lithuania<br />
Source: Produced us<strong>in</strong>g data published by the Council of Europe. 16<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 9
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
There are a very large number of variables that <strong>in</strong>fluence <strong>organ</strong> d<strong>on</strong>or rates, some of which are<br />
more amenable to change than others. These <strong>in</strong>clude the level of wealth, religious beliefs, legislati<strong>on</strong>,<br />
social norms, educati<strong>on</strong>, medical <strong>in</strong>frastructure, number of <strong>in</strong>tensive care beds and the number of<br />
deaths follow<strong>in</strong>g road traffic accidents and cerebro-vascular diseases. The fact that <strong>on</strong>e factor<br />
seems to be favourable to <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> <strong>on</strong>e country does not mean that it could or should be<br />
adopted <strong>in</strong> another. Countries with a high number of deaths follow<strong>in</strong>g road traffic accidents, <strong>for</strong><br />
example, may have a higher number of d<strong>on</strong>ors, but that is not someth<strong>in</strong>g the UK would want to<br />
emulate. As a society we should be will<strong>in</strong>g to look at other countries to see what can be learned<br />
but also to ma<strong>in</strong>ta<strong>in</strong> a UK focus. The d<strong>on</strong>ati<strong>on</strong> rate would, almost certa<strong>in</strong>ly, be higher if the UK<br />
had many more <strong>in</strong>tensive care beds and we should c<strong>on</strong>t<strong>in</strong>ue to <strong>in</strong>vestigate areas, such as this,<br />
<strong>where</strong> further <strong>in</strong>vestment would be beneficial. We also need to focus <strong>on</strong> the true potential <strong>for</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK at the current time, through the potential d<strong>on</strong>or audit (see secti<strong>on</strong> 4) which<br />
has recently been improved and expanded. As l<strong>on</strong>g as this shows that there are a significant<br />
number of potential d<strong>on</strong>ors who are not d<strong>on</strong>at<strong>in</strong>g, we must c<strong>on</strong>t<strong>in</strong>ue to strive <strong>for</strong> improvements.<br />
10<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
3 The current legislative framework<br />
Organ d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the United K<strong>in</strong>gdom is governed by the Human Tissue Act 2004 and the<br />
Human Tissue (Scotland) Act 2006. It is a crim<strong>in</strong>al offence to use <strong>organ</strong>s <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> without<br />
appropriate c<strong>on</strong>sent (referred to as authorisati<strong>on</strong> <strong>in</strong> Scotland), to give or receive any reward <strong>in</strong><br />
exchange <strong>for</strong> <strong>organ</strong>s <strong>for</strong> transplantati<strong>on</strong> or to transplant <strong>organ</strong>s from a liv<strong>in</strong>g d<strong>on</strong>or without the<br />
necessary prior approval. In additi<strong>on</strong>, the 2004 Act established the Human Tissue Authority (HTA)<br />
to regulate certa<strong>in</strong> activities and to oversee the implementati<strong>on</strong> of the legislati<strong>on</strong> <strong>in</strong> England, Wales<br />
and Northern Ireland. The HTA also regulates liv<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> throughout the UK. Detailed<br />
<strong>in</strong><strong>for</strong>mati<strong>on</strong> <strong>on</strong> the provisi<strong>on</strong>s of the human tissue legislati<strong>on</strong> is available <strong>in</strong> separate guidance from<br />
the <strong>BMA</strong>. 17 More detailed guidance <strong>for</strong> those <strong>in</strong> England, Wales and Northern Ireland can also<br />
be found <strong>in</strong> the HTA’s Code of Practice <strong>on</strong> transplantati<strong>on</strong>. 18<br />
The Human Tissue Authority was <strong>on</strong>e of a large number of <strong>organ</strong>isati<strong>on</strong>s <strong>in</strong>cluded <strong>in</strong> the Public<br />
Bodies Act 2011. The Act established a mechanism through which the Government could transfer<br />
the functi<strong>on</strong>s of public bodies to other <strong>organ</strong>isati<strong>on</strong>s. At the time of writ<strong>in</strong>g the Government’s<br />
stated <strong>in</strong>tenti<strong>on</strong> was to transfer most of the functi<strong>on</strong>s of the HTA to the Care Quality Commissi<strong>on</strong><br />
and to abolish the HTA by 2015. Up-to-date <strong>in</strong><strong>for</strong>mati<strong>on</strong> can be obta<strong>in</strong>ed from the <strong>BMA</strong>’s website.<br />
C<strong>on</strong>sent <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> after death<br />
In the <strong>BMA</strong>’s previous report, there was a lot of criticism of the Human Tissue Act 1961 which<br />
regulated <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> at the time. The 2004 and 2006 Acts addressed these c<strong>on</strong>cerns and<br />
clearly set out the legal requirements around c<strong>on</strong>sent (authorisati<strong>on</strong> <strong>in</strong> Scotland) <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> after<br />
death. D<strong>on</strong>ati<strong>on</strong> may not proceed without the explicit c<strong>on</strong>sent (authorisati<strong>on</strong>) of either the d<strong>on</strong>or,<br />
given dur<strong>in</strong>g his or her lifetime (usually by sign<strong>in</strong>g up to the Organ D<strong>on</strong>or Register), or some<strong>on</strong>e<br />
else legally empowered to give it. In the absence of explicit c<strong>on</strong>sent from the <strong>in</strong>dividual, c<strong>on</strong>sent<br />
or authorisati<strong>on</strong> may be given by some<strong>on</strong>e nom<strong>in</strong>ated by the deceased (<strong>in</strong> England, Wales and<br />
Northern Ireland), some<strong>on</strong>e with parental resp<strong>on</strong>sibility <strong>for</strong> a child who has died or other family<br />
members accord<strong>in</strong>g to a specified hierarchy. 19 In Scotland, the legislati<strong>on</strong> explicitly states that third<br />
parties cannot give authorisati<strong>on</strong> if they know the <strong>in</strong>dividual was unwill<strong>in</strong>g <strong>for</strong> any part of the body<br />
to be used <strong>for</strong> that purpose. If it may be necessary <strong>for</strong> a cor<strong>on</strong>er, or procurator fiscal <strong>in</strong> Scotland,<br />
to order the carry<strong>in</strong>g out of a post-mortem exam<strong>in</strong>ati<strong>on</strong>, <strong>organ</strong>s or tissues may be removed <strong>on</strong>ly<br />
with the specific agreement of those authorities. Guidance <strong>for</strong> cor<strong>on</strong>ers is discussed <strong>in</strong> secti<strong>on</strong> 4.<br />
Under the new legislati<strong>on</strong> the <strong>in</strong>dividual’s own wishes take precedence and, legally, the relatives’<br />
wishes cannot override those of the deceased. The legislati<strong>on</strong> is, however, enabl<strong>in</strong>g. It permits but<br />
does not require d<strong>on</strong>ati<strong>on</strong> to proceed. Whilst the Human Tissue Authority advises that families<br />
should be ‘encouraged’ to respect the views of their loved <strong>on</strong>es, 20 <strong>in</strong> practice <strong>in</strong> 2010/11, 6% of<br />
families refused d<strong>on</strong>ati<strong>on</strong> despite the <strong>in</strong>dividual hav<strong>in</strong>g authorised d<strong>on</strong>ati<strong>on</strong> dur<strong>in</strong>g his or her<br />
lifetime. 21 There are mixed views about the acceptability of this practice. In a survey of the general<br />
public, 56% said it was never acceptable <strong>for</strong> the family to override the known wishes of the<br />
<strong>in</strong>dividual to d<strong>on</strong>ate <strong>organ</strong>s after death. 22 The <strong>BMA</strong> takes a more pragmatic approach, recognis<strong>in</strong>g<br />
that the health care team also has a duty of care to the bereaved relatives. Insist<strong>in</strong>g <strong>on</strong> d<strong>on</strong>ati<strong>on</strong><br />
<strong>in</strong> the face of their str<strong>on</strong>g and susta<strong>in</strong>ed oppositi<strong>on</strong> is likely to add to their distress as well as,<br />
potentially, generat<strong>in</strong>g public hostility towards <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. It is also questi<strong>on</strong>able whether all<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 11
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
<strong>in</strong>dividuals who sign up to the ODR would want their wishes followed if to do so would cause very<br />
significant additi<strong>on</strong>al distress to their families. For many families it is important to spend time with<br />
their loved <strong>on</strong>e after death has been diagnosed. This can present difficulties, <strong>in</strong> terms of tim<strong>in</strong>g,<br />
if the <strong>in</strong>dividual wanted to d<strong>on</strong>ate <strong>organ</strong>s. This dilemma should be discussed <strong>in</strong> advance with the<br />
family and <strong>where</strong>ver possible arrangements should be made <strong>for</strong> this wish to be facilitated whilst<br />
still allow<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> to proceed. Where it is not possible to achieve both of these aims, a<br />
decisi<strong>on</strong> will need to be made, based <strong>on</strong> the <strong>in</strong>dividual circumstances and after discussi<strong>on</strong> with<br />
the family. In some circumstances – <strong>where</strong> it is evident that severe distress would be caused to<br />
the relatives – not proceed<strong>in</strong>g with d<strong>on</strong>ati<strong>on</strong> will be the right opti<strong>on</strong>. Individuals who have clear<br />
views about what they want to happen to their body after death, and do not want their relatives<br />
to override their wishes, should ensure that <strong>in</strong> additi<strong>on</strong> to <strong>for</strong>mally record<strong>in</strong>g their c<strong>on</strong>sent they<br />
have also discussed the issue with their relatives dur<strong>in</strong>g their lifetime.<br />
D<strong>on</strong>ati<strong>on</strong> after circulatory death (DCD)<br />
There are two different types of deceased d<strong>on</strong>ati<strong>on</strong>: d<strong>on</strong>ati<strong>on</strong> follow<strong>in</strong>g bra<strong>in</strong> stem death (DBD)<br />
and d<strong>on</strong>ati<strong>on</strong> after circulatory death (<strong>for</strong>merly referred to as ‘n<strong>on</strong>-heartbeat<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong>’ or<br />
‘d<strong>on</strong>ati<strong>on</strong> after cardiac death’). There is also an important dist<strong>in</strong>cti<strong>on</strong> with<strong>in</strong> d<strong>on</strong>ati<strong>on</strong> after<br />
circulatory death between ‘c<strong>on</strong>trolled DCD’ (also referred to as Maastricht category III) <strong>where</strong> death<br />
follows the planned withdrawal of life-susta<strong>in</strong><strong>in</strong>g treatment, and ‘unc<strong>on</strong>trolled DCD’ (Maastricht<br />
category I/II) <strong>where</strong> death is sudden and unexpected. The c<strong>on</strong>tributi<strong>on</strong> of each of these types of<br />
d<strong>on</strong>ati<strong>on</strong> to the total number of d<strong>on</strong>ors <strong>in</strong> the UK has shifted over time. Orig<strong>in</strong>ally when d<strong>on</strong>ati<strong>on</strong><br />
began <strong>in</strong> the 1950s all d<strong>on</strong>ati<strong>on</strong> was unc<strong>on</strong>trolled DCD. Once guidel<strong>in</strong>es were established <strong>for</strong><br />
diagnos<strong>in</strong>g death us<strong>in</strong>g bra<strong>in</strong> stem tests, DBD became the most comm<strong>on</strong> <strong>for</strong>m of d<strong>on</strong>ati<strong>on</strong> with a<br />
small amount of unc<strong>on</strong>trolled DCD. By around 2005, unc<strong>on</strong>trolled DCD d<strong>on</strong>or numbers had fallen<br />
and the number of c<strong>on</strong>trolled DCD d<strong>on</strong>ors had <strong>in</strong>creased c<strong>on</strong>siderably so that 37% of all deceased<br />
d<strong>on</strong>ati<strong>on</strong> comes from c<strong>on</strong>trolled DCD d<strong>on</strong>ors (and 63% from DBD d<strong>on</strong>ors). 23 It is likely that this will<br />
shift aga<strong>in</strong> over time and it is possible that some unc<strong>on</strong>trolled DCD programmes may be resumed.<br />
This <strong>in</strong><strong>for</strong>mati<strong>on</strong> is relevant to the legal framework because <strong>in</strong> 2000, when most of the DCD<br />
programmes used unc<strong>on</strong>trolled DCD, questi<strong>on</strong>s were raised about the lawfulness of tak<strong>in</strong>g the<br />
steps required to preserve the <strong>organ</strong>s be<strong>for</strong>e c<strong>on</strong>sent <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> had been obta<strong>in</strong>ed. This issue<br />
was clarified <strong>in</strong> the 2004 and 2006 legislati<strong>on</strong> and the law now clearly permits the tak<strong>in</strong>g of the<br />
m<strong>in</strong>imum steps necessary to preserve <strong>organ</strong>s <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> after death has been c<strong>on</strong>firmed. These<br />
<strong>in</strong>terventi<strong>on</strong>s may be undertaken be<strong>for</strong>e the register is checked or relatives’ c<strong>on</strong>sent (or authorisati<strong>on</strong>)<br />
<strong>for</strong> d<strong>on</strong>ati<strong>on</strong> is obta<strong>in</strong>ed but all steps must cease if it becomes known that c<strong>on</strong>sent (authorisati<strong>on</strong>)<br />
has not, or will not, be given <strong>for</strong> d<strong>on</strong>ati<strong>on</strong>. 24 Although this legal clarificati<strong>on</strong> was welcomed and<br />
co<strong>in</strong>cided with the <strong>in</strong>vestment of significant sums by UK Transplant (now the Organ D<strong>on</strong>ati<strong>on</strong> and<br />
Transplantati<strong>on</strong> directorate of NHS BT) <strong>in</strong>to develop<strong>in</strong>g DCD programmes around the country, 25<br />
by that stage unc<strong>on</strong>trolled DCD had already begun to decl<strong>in</strong>e <strong>for</strong> other reas<strong>on</strong>s. In fact, at that<br />
stage c<strong>on</strong>trolled DCD had become the standard practice, <strong>where</strong> d<strong>on</strong>ati<strong>on</strong> follows the c<strong>on</strong>trolled<br />
withdrawal of treatment and there is time to ensure that c<strong>on</strong>sent is obta<strong>in</strong>ed be<strong>for</strong>e the procedure<br />
takes place. This legal clarificati<strong>on</strong> will, however, be useful <strong>in</strong> the future should a decisi<strong>on</strong> be made<br />
to resume unc<strong>on</strong>trolled DCD.<br />
12<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
Liv<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong><br />
D<strong>on</strong>ati<strong>on</strong> of <strong>organ</strong>s from liv<strong>in</strong>g <strong>in</strong>dividuals requires prior approval by the Human Tissue Authority.<br />
The <strong>on</strong>ly excepti<strong>on</strong> to this rule is ‘dom<strong>in</strong>o’ d<strong>on</strong>ati<strong>on</strong>s <strong>where</strong> an <strong>organ</strong> is removed <strong>for</strong> the benefit of<br />
the d<strong>on</strong>or him or herself. This arises, <strong>for</strong> example, <strong>where</strong> a kidney is removed <strong>for</strong> cl<strong>in</strong>ical reas<strong>on</strong>s<br />
but is suitable <strong>for</strong> transplantati<strong>on</strong> <strong>in</strong>to another <strong>in</strong>dividual.<br />
Where the d<strong>on</strong>or is a healthy volunteer, the d<strong>on</strong>or and recipient must be <strong>in</strong>terviewed by an<br />
Independent Assessor who is accredited by the HTA. The Independent Assessor must be satisfied<br />
that the pers<strong>on</strong> giv<strong>in</strong>g c<strong>on</strong>sent to the d<strong>on</strong>ati<strong>on</strong> has been given and has understood the necessary<br />
<strong>in</strong><strong>for</strong>mati<strong>on</strong>, and that there is no evidence of reward or coerci<strong>on</strong> or evidence that the <strong>in</strong>dividual<br />
has been subjected to pressure to c<strong>on</strong>sent. The Assessor then submits a report to the HTA which<br />
decides whether to authorise the d<strong>on</strong>ati<strong>on</strong>. There are some cases <strong>where</strong> additi<strong>on</strong>al safeguards are<br />
<strong>in</strong> place, and each case must be c<strong>on</strong>sidered by a panel of at least three members of the HTA<br />
be<strong>for</strong>e approval is given. These cases are:<br />
• <strong>in</strong> England, Wales and Northern Ireland, <strong>where</strong> the d<strong>on</strong>or is an adult who lacks capacity or a<br />
child who lacks capacity to c<strong>on</strong>sent (<strong>on</strong>ly adults with capacity can be liv<strong>in</strong>g solid <strong>organ</strong> d<strong>on</strong>ors<br />
<strong>in</strong> Scotland, except <strong>where</strong> an adult who lacks capacity d<strong>on</strong>ates as part of a dom<strong>in</strong>o d<strong>on</strong>ati<strong>on</strong>)<br />
• ’paired‘ and ’pooled‘ d<strong>on</strong>ati<strong>on</strong>s which allow a d<strong>on</strong>or and recipient to pair up with <strong>on</strong>e or more<br />
other d<strong>on</strong>or and recipient pairs <strong>in</strong> an <strong>organ</strong> exchange. For example, d<strong>on</strong>or A’s <strong>organ</strong> goes to<br />
recipient B, d<strong>on</strong>or B’s <strong>organ</strong> goes to recipient C and d<strong>on</strong>or C’s <strong>organ</strong> goes to recipient A. This<br />
system can be used by d<strong>on</strong>ors who are <strong>in</strong>compatible (by ABO blood group or HLA type) with<br />
their chosen recipient.<br />
• d<strong>on</strong>ati<strong>on</strong> to a stranger (referred to as ‘n<strong>on</strong>-directed altruistic d<strong>on</strong>ati<strong>on</strong>’).<br />
The sec<strong>on</strong>d and third of these categories are collectively referred to as Nati<strong>on</strong>al Liv<strong>in</strong>g D<strong>on</strong>or<br />
Kidney Shar<strong>in</strong>g Schemes (NLDKSS).<br />
Mental capacity legislati<strong>on</strong><br />
Although there is specific legislati<strong>on</strong> cover<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> there are other legislative provisi<strong>on</strong>s<br />
that are also relevant. Legislati<strong>on</strong> relat<strong>in</strong>g to decisi<strong>on</strong> mak<strong>in</strong>g <strong>for</strong> adults who lack capacity, <strong>for</strong><br />
example (the Mental Capacity Act 2005 and Adults with Incapacity (Scotland) Act 2000) has<br />
had a significant impact <strong>on</strong> discussi<strong>on</strong>s about the cl<strong>in</strong>ical management of potential d<strong>on</strong>ors .26<br />
The legislati<strong>on</strong> requires that decisi<strong>on</strong>s taken <strong>on</strong> behalf of adults who lack capacity are made <strong>in</strong><br />
their best <strong>in</strong>terests (benefit <strong>in</strong> Scotland). Part of the assessment of best <strong>in</strong>terests <strong>in</strong>volves tak<strong>in</strong>g<br />
account of prior wishes and values; this <strong>in</strong>cludes tak<strong>in</strong>g account of any expressed wish to d<strong>on</strong>ate<br />
<strong>organ</strong>s after death. This legislati<strong>on</strong>, <strong>for</strong> example, provides the legal justificati<strong>on</strong> <strong>for</strong> tak<strong>in</strong>g some<br />
steps be<strong>for</strong>e death to facilitate d<strong>on</strong>ati<strong>on</strong>, <strong>where</strong> it is known the <strong>in</strong>dividual wished to d<strong>on</strong>ate<br />
<strong>organ</strong>s. This issue is discussed further <strong>in</strong> secti<strong>on</strong> 4.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 13
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
EU Organs Directive<br />
The EU Organs Directive aims to ensure high quality and safe standards <strong>for</strong> the d<strong>on</strong>ati<strong>on</strong>,<br />
procurement, transportati<strong>on</strong>, traceability and follow-up of human <strong>organ</strong>s throughout the European<br />
Uni<strong>on</strong>. 27 The Directive, which requires that all transplant centres’ compliance with the Directive is<br />
audited and c<strong>on</strong>trolled, must be <strong>in</strong>corporated <strong>in</strong>to UK legislati<strong>on</strong> by August 2012. The Human<br />
Tissue Authority has been nom<strong>in</strong>ated as the competent authority <strong>for</strong> the UK. 28 At the time of<br />
writ<strong>in</strong>g draft regulati<strong>on</strong>s were be<strong>in</strong>g c<strong>on</strong>sidered that would lead to the development of a<br />
regulatory mechanism as well as sett<strong>in</strong>g standards <strong>for</strong> the quality and safety of <strong>organ</strong>s <strong>for</strong><br />
transplantati<strong>on</strong>. 29 From August 2012 all <strong>organ</strong>isati<strong>on</strong>s <strong>in</strong>volved <strong>in</strong> the d<strong>on</strong>ati<strong>on</strong> or transplantati<strong>on</strong><br />
of <strong>organ</strong>s will need to be authorised by the HTA. It will be necessary to keep a record of liv<strong>in</strong>g<br />
and deceased d<strong>on</strong>ors, put <strong>in</strong> place a report<strong>in</strong>g system <strong>for</strong> serious adverse events and develop<br />
and implement an effective and proporti<strong>on</strong>ate system of penalties <strong>for</strong> breaches of the Directive.<br />
14<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
4 Develop<strong>in</strong>g the <strong>in</strong>frastructure<br />
Strategies to improve <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> rates require acti<strong>on</strong> <strong>on</strong> two fr<strong>on</strong>ts: develop<strong>in</strong>g the <strong>in</strong>frastructure<br />
with<strong>in</strong> which d<strong>on</strong>ati<strong>on</strong> takes place and <strong>in</strong>creas<strong>in</strong>g the number of d<strong>on</strong>ors. This secti<strong>on</strong> looks at the<br />
acti<strong>on</strong>s that have been taken, and the success that has been achieved, <strong>in</strong> the first of those areas.<br />
The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce<br />
In December 2006 the UK Government set up an Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce charged with<br />
identify<strong>in</strong>g barriers to <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> and transplantati<strong>on</strong> and recommend<strong>in</strong>g ways to overcome<br />
them, with<strong>in</strong> the exist<strong>in</strong>g operati<strong>on</strong>al and legal frameworks. The Task<strong>for</strong>ce took an objective and<br />
strategic approach, look<strong>in</strong>g <strong>in</strong> detail at every aspect of the transplant process, identify<strong>in</strong>g problems<br />
or barriers to d<strong>on</strong>ati<strong>on</strong> and recommend<strong>in</strong>g radical, comprehensive and far-reach<strong>in</strong>g changes. A key<br />
f<strong>in</strong>d<strong>in</strong>g of the Task<strong>for</strong>ce was the significant variability <strong>in</strong> per<strong>for</strong>mance between different regi<strong>on</strong>s <strong>in</strong><br />
terms of bra<strong>in</strong> stem test<strong>in</strong>g, referral of potential d<strong>on</strong>ors and local engagement. This was seen as a<br />
reflecti<strong>on</strong> of the ad hoc way <strong>in</strong> which the system had developed and the lack of a coherent nati<strong>on</strong>al<br />
strategy. The Task<strong>for</strong>ce recognised that d<strong>on</strong>ati<strong>on</strong> should no l<strong>on</strong>ger be viewed as an ‘opti<strong>on</strong>al extra’<br />
but must become a mandatory and usual part of the duty of care <strong>in</strong> every hospital and that this<br />
needed to be per<strong>for</strong>mance-managed. Furthermore, <strong>in</strong> order to be successful, Trust Chief Executive<br />
Officers (CEOs) or Chief Operat<strong>in</strong>g Officers (COOs) needed to take resp<strong>on</strong>sibility, and be accountable,<br />
<strong>for</strong> the identificati<strong>on</strong> and referral of potential d<strong>on</strong>ors with<strong>in</strong> their hospital. The Task<strong>for</strong>ce report was<br />
published <strong>in</strong> 2008 with 14 recommendati<strong>on</strong>s (see below) which, it believed, would <strong>in</strong>crease d<strong>on</strong>ati<strong>on</strong><br />
rates by 50% over a five-year period. 30 The Task<strong>for</strong>ce was adamant that the recommendati<strong>on</strong>s<br />
required both f<strong>in</strong>ancial and political commitment and must be implemented <strong>in</strong> full; partial<br />
implementati<strong>on</strong> was not an opti<strong>on</strong>.<br />
Recommendati<strong>on</strong>s of the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce<br />
1. A UK-wide Organ D<strong>on</strong>ati<strong>on</strong> Organisati<strong>on</strong> should be established.<br />
2. The establishment of the Organ D<strong>on</strong>ati<strong>on</strong> Organisati<strong>on</strong> should be the resp<strong>on</strong>sibility of<br />
NHS Blood and Transplant.<br />
3. Urgent attenti<strong>on</strong> is required to resolve outstand<strong>in</strong>g legal, ethical and professi<strong>on</strong>al issues<br />
<strong>in</strong> order to ensure that all cl<strong>in</strong>icians are supported and are able to work with<strong>in</strong> a clear<br />
and unambiguous framework of good practice. Additi<strong>on</strong>ally, an <strong>in</strong>dependent UK-wide<br />
D<strong>on</strong>ati<strong>on</strong> Ethics Group should be established.<br />
4. All parts of the NHS must embrace <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> as a usual not an unusual event. Local<br />
policies, c<strong>on</strong>structed around nati<strong>on</strong>al guidel<strong>in</strong>es, should be put <strong>in</strong> place. Discussi<strong>on</strong>s about<br />
d<strong>on</strong>ati<strong>on</strong> should be part of all end-of-life care when appropriate. Each Trust should have an<br />
identified cl<strong>in</strong>ical d<strong>on</strong>ati<strong>on</strong> champi<strong>on</strong> and a Trust d<strong>on</strong>ati<strong>on</strong> committee to help achieve this.<br />
5. M<strong>in</strong>imum notificati<strong>on</strong> criteria <strong>for</strong> potential <strong>organ</strong> d<strong>on</strong>ors should be <strong>in</strong>troduced <strong>on</strong> a UK-wide<br />
basis. These criteria should be reviewed after 12 m<strong>on</strong>ths <strong>in</strong> the light of evidence of their<br />
effect, and the comparative impact of more detailed criteria should also be assessed.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 15
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
6. D<strong>on</strong>ati<strong>on</strong> activity <strong>in</strong> all Trusts should be m<strong>on</strong>itored. Rates of potential d<strong>on</strong>or identificati<strong>on</strong>,<br />
referral, approach to the family and c<strong>on</strong>sent to d<strong>on</strong>ati<strong>on</strong> should be reported. The Trust<br />
d<strong>on</strong>ati<strong>on</strong> committee should report to the Trust Board through the cl<strong>in</strong>ical governance<br />
process and the medical director, and the reports should be part of the assessment of<br />
Trusts through the relevant healthcare regulator. Benchmark data from other Trusts<br />
should be made available <strong>for</strong> comparis<strong>on</strong>.<br />
7. Bra<strong>in</strong> stem death (BSD) test<strong>in</strong>g should be carried out <strong>in</strong> all patients <strong>where</strong> BSD is a likely<br />
diagnosis, even if <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> is an unlikely outcome.<br />
8. F<strong>in</strong>ancial dis<strong>in</strong>centives to Trusts facilitat<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> should be removed through the<br />
development and <strong>in</strong>troducti<strong>on</strong> of appropriate reimbursement.<br />
9. The current network of d<strong>on</strong>or transplant co-ord<strong>in</strong>ators (DTCs) should be expanded and<br />
strengthened through central employment by a UK-wide Organ D<strong>on</strong>ati<strong>on</strong> Organisati<strong>on</strong>.<br />
Additi<strong>on</strong>al co-ord<strong>in</strong>ators, embedded with<strong>in</strong> critical care areas, should be employed to<br />
ensure a comprehensive, highly skilled, specialist and robust service. There should be<br />
a close and def<strong>in</strong>ed collaborati<strong>on</strong> between DTCs, cl<strong>in</strong>ical staff and Trust d<strong>on</strong>ati<strong>on</strong><br />
champi<strong>on</strong>s. Electr<strong>on</strong>ic <strong>on</strong>-l<strong>in</strong>e d<strong>on</strong>or registrati<strong>on</strong> and <strong>organ</strong> offer<strong>in</strong>g systems should<br />
be developed.<br />
10. A UK-wide network of dedicated <strong>organ</strong> retrieval teams should be established to ensure<br />
timely, high-quality <strong>organ</strong> removal from all heartbeat<strong>in</strong>g and n<strong>on</strong>-heartbeat<strong>in</strong>g d<strong>on</strong>ors.<br />
The Organ D<strong>on</strong>ati<strong>on</strong> Organisati<strong>on</strong> should be resp<strong>on</strong>sible <strong>for</strong> commissi<strong>on</strong><strong>in</strong>g the retrieval<br />
teams and <strong>for</strong> audit and per<strong>for</strong>mance management.<br />
11. All cl<strong>in</strong>ical staff likely to be <strong>in</strong>volved <strong>in</strong> the treatment of potential <strong>organ</strong> d<strong>on</strong>ors should<br />
receive mandatory tra<strong>in</strong><strong>in</strong>g <strong>in</strong> the pr<strong>in</strong>ciples of d<strong>on</strong>ati<strong>on</strong>. There should also be regular<br />
update tra<strong>in</strong><strong>in</strong>g.<br />
12. Appropriate ways should be identified of pers<strong>on</strong>ally and publicly recognis<strong>in</strong>g <strong>in</strong>dividual<br />
<strong>organ</strong> d<strong>on</strong>ors, <strong>where</strong> desired. These approaches may <strong>in</strong>clude nati<strong>on</strong>al memorials, local<br />
<strong>in</strong>itiatives and pers<strong>on</strong>al follow-up to d<strong>on</strong>or families.<br />
13. There is an urgent requirement to identify and implement the most effective methods<br />
through which <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> and the ‘gift of life’ can be promoted to the general<br />
public, and specifically to the BME populati<strong>on</strong>. Research should be commissi<strong>on</strong>ed<br />
through Department of Health research and development fund<strong>in</strong>g.<br />
14. The Department of Health and the M<strong>in</strong>istry of Justice should develop <strong>for</strong>mal guidel<strong>in</strong>es<br />
<strong>for</strong> cor<strong>on</strong>ers c<strong>on</strong>cern<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>.<br />
Reproduced from: Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) Organs <strong>for</strong> Transplants. A report from the<br />
Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Department of Health, L<strong>on</strong>d<strong>on</strong>.<br />
The Task<strong>for</strong>ce’s mantra was that <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> should become ‘a usual not an unusual event’,<br />
emphasis<strong>in</strong>g that it should be seen as a standard part of end-of-life care <strong>for</strong> all suitable patients.<br />
It should be the norm that bra<strong>in</strong> stem tests are carried out <strong>on</strong> every patient <strong>where</strong> bra<strong>in</strong> stem<br />
death is a possible diagnosis, that all cases of bra<strong>in</strong> stem death or treatment withdrawal are<br />
referred to the d<strong>on</strong>or co-ord<strong>in</strong>ator, and that the Organ D<strong>on</strong>or Register is checked and the relatives<br />
approached <strong>in</strong> every case <strong>where</strong> d<strong>on</strong>ati<strong>on</strong> may be a possibility. The Task<strong>for</strong>ce recommended<br />
16<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
c<strong>on</strong>siderable restructur<strong>in</strong>g of the system, much of which had developed <strong>in</strong> an ad hoc fashi<strong>on</strong> at a<br />
local level. NHS Blood and Transplant was to become the s<strong>in</strong>gle nati<strong>on</strong>al <strong>organ</strong>isati<strong>on</strong> resp<strong>on</strong>sible<br />
<strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> and transplantati<strong>on</strong> and would directly employ an <strong>in</strong>creased number of d<strong>on</strong>or<br />
co-ord<strong>in</strong>ators. Cl<strong>in</strong>ical ‘d<strong>on</strong>ati<strong>on</strong> champi<strong>on</strong>s’ and d<strong>on</strong>ati<strong>on</strong> committees with<strong>in</strong> every Trust would<br />
ensure that d<strong>on</strong>ati<strong>on</strong> was c<strong>on</strong>sidered <strong>on</strong> a Trust-wide basis and at Board level. To ensure high-level<br />
engagement and oversight, <strong>in</strong>dividual hospital d<strong>on</strong>ati<strong>on</strong> rates, together with benchmark data from<br />
other Trusts <strong>for</strong> comparis<strong>on</strong>, would be provided to the Trust Board and would be c<strong>on</strong>sidered as<br />
part of the cl<strong>in</strong>ical governance process.<br />
The UK Health M<strong>in</strong>isters accepted all of the Task<strong>for</strong>ce’s recommendati<strong>on</strong>s and the UK Government<br />
appo<strong>in</strong>ted Mr Chris Rudge (<strong>for</strong>merly Medical Director of UK Transplant) as the first Nati<strong>on</strong>al Cl<strong>in</strong>ical<br />
Director <strong>for</strong> Transplantati<strong>on</strong> <strong>in</strong> England to lead the day-to-day implementati<strong>on</strong> of the recommendati<strong>on</strong>s<br />
and to chair a Programme Delivery Board that ma<strong>in</strong>ta<strong>in</strong>ed oversight of <strong>progress</strong> across the UK.<br />
Similar appo<strong>in</strong>tments were made <strong>in</strong> Scotland, Wales and Northern Ireland. In Scotland, the Cab<strong>in</strong>et<br />
Secretary <strong>for</strong> Health & Wellbe<strong>in</strong>g asked the Scottish Transplant Group to take resp<strong>on</strong>sibility <strong>for</strong><br />
oversee<strong>in</strong>g implementati<strong>on</strong> <strong>in</strong> Scotland. In 2008/09, £16.5 milli<strong>on</strong> was allocated to the NHS <strong>for</strong><br />
<strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> and transplantati<strong>on</strong> (of which £11.5milli<strong>on</strong> was new m<strong>on</strong>ey specifically related to<br />
the implementati<strong>on</strong> of the Task<strong>for</strong>ce report). A further £26.5 milli<strong>on</strong> was allocated <strong>for</strong> 2009/10. 31<br />
The UK Health M<strong>in</strong>isters made clear, however, that it expected to see improvements and would be<br />
closely m<strong>on</strong>itor<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> rates. In December 2011 the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce Programme<br />
Delivery Board published its f<strong>in</strong>al report, announc<strong>in</strong>g that all of the recommendati<strong>on</strong>s had been<br />
fully or substantially implemented. 32<br />
Cl<strong>in</strong>ical leads, specialist nurses and d<strong>on</strong>ati<strong>on</strong> committees<br />
A fundamental aim of the Task<strong>for</strong>ce was that every acute Trust <strong>in</strong> the country should have a<br />
d<strong>on</strong>ati<strong>on</strong> champi<strong>on</strong> (subsequently renamed cl<strong>in</strong>ical lead <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>), an ‘embedded’ d<strong>on</strong>or<br />
transplant co-ord<strong>in</strong>ator (subsequently renamed specialist nurse – <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>) and a d<strong>on</strong>ati<strong>on</strong><br />
committee, chaired by a n<strong>on</strong>-cl<strong>in</strong>ical champi<strong>on</strong>, act<strong>in</strong>g as a l<strong>in</strong>k between the transplant team and<br />
the Board or senior management of the Trust. 33 These local ‘collaboratives’ would ensure that<br />
<strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> was always c<strong>on</strong>sidered <strong>in</strong> appropriate cases, identify and remove barriers to<br />
d<strong>on</strong>ati<strong>on</strong> with<strong>in</strong> the Trust and raise awareness of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> with<strong>in</strong> hospitals and am<strong>on</strong>gst<br />
the local populati<strong>on</strong>. Thus a nati<strong>on</strong>al system of local collaboratives – based <strong>on</strong> the successful<br />
model <strong>in</strong> Spa<strong>in</strong> (see secti<strong>on</strong> 6) – was seen as key to maximis<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> potential.<br />
As part of its implementati<strong>on</strong> <strong>policy</strong>, NHS BT developed and executed a 12-m<strong>on</strong>th professi<strong>on</strong>al<br />
development programme <strong>for</strong> cl<strong>in</strong>ical leads and d<strong>on</strong>ati<strong>on</strong> committee chairs. 34 The programme aimed<br />
to provide participants with the skills necessary to implement the Task<strong>for</strong>ce’s visi<strong>on</strong> of mak<strong>in</strong>g<br />
d<strong>on</strong>ati<strong>on</strong> a normal part of end-of-life care. The tra<strong>in</strong><strong>in</strong>g focused <strong>on</strong> achiev<strong>in</strong>g the ‘six big w<strong>in</strong>s’:<br />
1. Increased c<strong>on</strong>sent/authorisati<strong>on</strong> rates<br />
2. Increased diagnosis of bra<strong>in</strong> stem death<br />
3. Increased d<strong>on</strong>ati<strong>on</strong> after cardiac death (now referred to as d<strong>on</strong>ati<strong>on</strong> after circulatory death)<br />
4. Increased rate of d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> emergency medic<strong>in</strong>e<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 17
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
5. Increased referral accord<strong>in</strong>g to m<strong>in</strong>imum notificati<strong>on</strong> criteria<br />
6. Increased quality and quantity of <strong>organ</strong>s from improved d<strong>on</strong>or management.<br />
A f<strong>in</strong>al part of the programme was the development of 12 regi<strong>on</strong>al d<strong>on</strong>ati<strong>on</strong> collaboratives <strong>in</strong> the<br />
UK to provide local teams with support, advice and a <strong>for</strong>um <strong>for</strong> the exchange of ideas.<br />
Cl<strong>in</strong>ical leads <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong><br />
The aim of the cl<strong>in</strong>ical lead posts is to have a senior cl<strong>in</strong>ician with<strong>in</strong> each Trust (or equivalent <strong>in</strong><br />
the devolved nati<strong>on</strong>s) who is resp<strong>on</strong>sible <strong>for</strong> ensur<strong>in</strong>g that <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> is seen as a priority,<br />
that the Task<strong>for</strong>ce’s recommendati<strong>on</strong>s are implemented and that procedures are <strong>in</strong> place to<br />
optimise potential d<strong>on</strong>or identificati<strong>on</strong> and management. The role is a strategic <strong>on</strong>e, focus<strong>in</strong>g<br />
<strong>on</strong> policies and process rather than <strong>on</strong> <strong>in</strong>dividual cases.<br />
Cl<strong>in</strong>ical leads are employed by the Trust <strong>for</strong> <strong>on</strong>e or two sessi<strong>on</strong>s per week with fund<strong>in</strong>g and<br />
tra<strong>in</strong><strong>in</strong>g provided by NHS BT. The vast majority of cl<strong>in</strong>ical leads are c<strong>on</strong>sultants <strong>in</strong> <strong>in</strong>tensive care.<br />
This <strong>in</strong>itially gave rise to some c<strong>on</strong>cerns about a potential c<strong>on</strong>flict of <strong>in</strong>terest <strong>where</strong> <strong>in</strong>tensivists are<br />
mak<strong>in</strong>g decisi<strong>on</strong>s about withhold<strong>in</strong>g or withdraw<strong>in</strong>g life-prol<strong>on</strong>g<strong>in</strong>g treatment, carry<strong>in</strong>g out bra<strong>in</strong><br />
stem tests to diagnose death and, at the same time, have a <strong>for</strong>mal positi<strong>on</strong> with<strong>in</strong> the Trust<br />
relat<strong>in</strong>g to <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Their goal, however, is not to maximise the number of d<strong>on</strong>ors – which<br />
could give rise to a c<strong>on</strong>flict of <strong>in</strong>terest – but to ensure that systems are <strong>in</strong> place so that the opti<strong>on</strong><br />
of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> is always available <strong>for</strong> patients and their relatives. The <strong>BMA</strong> supports this goal<br />
and believes that all doctors who care <strong>for</strong> dy<strong>in</strong>g patients should see the offer of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong><br />
as part of their role. Nevertheless, Trusts may decide that <strong>in</strong>troduc<strong>in</strong>g a <strong>for</strong>mal system to protect<br />
aga<strong>in</strong>st any percepti<strong>on</strong> of a c<strong>on</strong>flict of <strong>in</strong>terest is helpful, such as <strong>in</strong>troduc<strong>in</strong>g a <strong>for</strong>mal requirement<br />
<strong>for</strong> a sec<strong>on</strong>d cl<strong>in</strong>ical op<strong>in</strong>i<strong>on</strong> when cl<strong>in</strong>ical leads are mak<strong>in</strong>g decisi<strong>on</strong>s to withdraw life-prol<strong>on</strong>g<strong>in</strong>g<br />
treatment from some<strong>on</strong>e who may go <strong>on</strong> to be an <strong>organ</strong> d<strong>on</strong>or. 35 This may simply be a matter of<br />
<strong>for</strong>malis<strong>in</strong>g exist<strong>in</strong>g practice under which, <strong>for</strong> example, the ICU c<strong>on</strong>sultant and the referr<strong>in</strong>g<br />
c<strong>on</strong>sultant liaise closely over such decisi<strong>on</strong>s.<br />
Cl<strong>in</strong>ical leads have been appo<strong>in</strong>ted <strong>in</strong> all 226 d<strong>on</strong>at<strong>in</strong>g hospitals <strong>in</strong> the UK. 36 Most are employed<br />
<strong>for</strong> <strong>on</strong>e sessi<strong>on</strong> per week but a small number have additi<strong>on</strong>al resp<strong>on</strong>sibilities and have two sessi<strong>on</strong>s.<br />
This may be because they work <strong>in</strong> a large Trust, because they have additi<strong>on</strong>al commitments <strong>on</strong> a<br />
nati<strong>on</strong>al level or because they have taken <strong>on</strong> the role of Regi<strong>on</strong>al Cl<strong>in</strong>ical Lead <strong>for</strong> Organ D<strong>on</strong>ati<strong>on</strong>.<br />
The regi<strong>on</strong>al cl<strong>in</strong>ical leads, work<strong>in</strong>g with NHSBT regi<strong>on</strong>al managers, compile annual reports and<br />
d<strong>on</strong>ati<strong>on</strong> plans and ensure co-ord<strong>in</strong>ati<strong>on</strong> and collaborati<strong>on</strong> with<strong>in</strong> the regi<strong>on</strong>. A small number<br />
of extra cl<strong>in</strong>ical leads have been appo<strong>in</strong>ted <strong>in</strong> specialist areas such as paediatrics or emergency<br />
medic<strong>in</strong>e. It is important that hospitals genu<strong>in</strong>ely protect this time to enable cl<strong>in</strong>ical leads to<br />
fulfil their resp<strong>on</strong>sibilities.<br />
Through the Professi<strong>on</strong>al Development Programme cl<strong>in</strong>ical leads were provided with leadership and<br />
change management tra<strong>in</strong><strong>in</strong>g designed to encourage them to identify the barriers to the delivery<br />
of the six big w<strong>in</strong>s with<strong>in</strong> their regi<strong>on</strong>, to analyse the reas<strong>on</strong>s <strong>for</strong> these barriers and to develop and<br />
implement a series of objectives to overcome them. Part of the role of the cl<strong>in</strong>ical lead is to ensure<br />
18<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
the development of local educati<strong>on</strong>al and tra<strong>in</strong><strong>in</strong>g opportunities <strong>for</strong> all staff likely to be <strong>in</strong>volved<br />
with the care of a potential <strong>organ</strong> d<strong>on</strong>or, <strong>in</strong> l<strong>in</strong>e with the Task<strong>for</strong>ce’s recommendati<strong>on</strong> 11. This has<br />
been approached <strong>in</strong> different ways around the country with some us<strong>in</strong>g e-learn<strong>in</strong>g resources,<br />
d<strong>on</strong>or simulati<strong>on</strong> tra<strong>in</strong><strong>in</strong>g or face-to-face tra<strong>in</strong><strong>in</strong>g provided by cl<strong>in</strong>ical leads or specialist nurses.<br />
Specialist nurses – <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong><br />
In l<strong>in</strong>e with the Task<strong>for</strong>ce’s n<strong>in</strong>th recommendati<strong>on</strong>, specialist nurses (<strong>for</strong>merly called transplant<br />
co-ord<strong>in</strong>ators) are now employed and tra<strong>in</strong>ed directly by NHS BT. These <strong>in</strong>dividuals provide the vital<br />
l<strong>in</strong>k between the family of the deceased, the hospital <strong>where</strong> the d<strong>on</strong>or died and the transplant<br />
centres retriev<strong>in</strong>g and receiv<strong>in</strong>g the d<strong>on</strong>ated <strong>organ</strong>s. Organ d<strong>on</strong>ati<strong>on</strong> and transplantati<strong>on</strong> are<br />
logistically complex, as well as emoti<strong>on</strong>ally demand<strong>in</strong>g, and specialist nurses play a critical role <strong>in</strong><br />
mak<strong>in</strong>g them happen. The Task<strong>for</strong>ce assessed the way the system was <strong>organ</strong>ised and recognised<br />
that the workload and work<strong>in</strong>g methods of specialist nurses were unsusta<strong>in</strong>able, with some<br />
work<strong>in</strong>g up to 24 hours without a break. It suggested that the role should be split <strong>in</strong>to three<br />
dist<strong>in</strong>ct areas of work so that up to three <strong>in</strong>dividuals might attend each d<strong>on</strong>or:<br />
• discussi<strong>on</strong>s with the <strong>organ</strong> d<strong>on</strong>or’s family, cover<strong>in</strong>g c<strong>on</strong>sent and seek<strong>in</strong>g a medical and social<br />
history of the d<strong>on</strong>or;<br />
• obta<strong>in</strong><strong>in</strong>g cl<strong>in</strong>ical <strong>in</strong><strong>for</strong>mati<strong>on</strong>, register<strong>in</strong>g the d<strong>on</strong>or with NHS BT and mak<strong>in</strong>g arrangements<br />
<strong>for</strong> the <strong>organ</strong> retrieval;<br />
• participat<strong>in</strong>g <strong>in</strong> the retrieval process and liais<strong>in</strong>g with NHS BT over the allocati<strong>on</strong> of <strong>organ</strong>s.<br />
This has proved difficult to achieve <strong>in</strong> practice. The Task<strong>for</strong>ce also recommended that work relat<strong>in</strong>g<br />
to d<strong>on</strong>ati<strong>on</strong> and that related to recipient care should be separated.<br />
At the time of the Task<strong>for</strong>ce Inquiry there were about 100 d<strong>on</strong>or co-ord<strong>in</strong>ators work<strong>in</strong>g <strong>in</strong> 18 teams.<br />
There were also 12 ‘<strong>in</strong>-house’ co-ord<strong>in</strong>ators based full-time with<strong>in</strong> a s<strong>in</strong>gle critical care unit or<br />
Trust. The Task<strong>for</strong>ce recommended that their number needed to be <strong>in</strong>creased to around 250 and<br />
that all specialist nurses should be employed and tra<strong>in</strong>ed by NHS BT. By November 2011 the target<br />
of 250 specialist nurses, and support staff, employed by NHS BT had been achieved and there<br />
were plans to appo<strong>in</strong>t a further 20. 37 The <strong>in</strong>tenti<strong>on</strong> has been that all specialist nurses would be<br />
embedded with<strong>in</strong> the <strong>in</strong>tensive care unit and at the time of writ<strong>in</strong>g the vast majority were already<br />
work<strong>in</strong>g <strong>in</strong> this way. Specialist nurses work <strong>in</strong> regi<strong>on</strong>al teams and have 24-hour support from<br />
regi<strong>on</strong>al managers who, <strong>in</strong> turn, have support from a range of experts to ensure that any<br />
challeng<strong>in</strong>g ethical or legal situati<strong>on</strong>s can be addressed. Applicants are required to have experience<br />
with<strong>in</strong> emergency medic<strong>in</strong>e or critical care and to have significant local management experience.<br />
They are also required to hold a post-basic qualificati<strong>on</strong> <strong>in</strong> critical care and must be able to<br />
dem<strong>on</strong>strate appropriate skills <strong>in</strong> communicati<strong>on</strong> and <strong>organ</strong>isati<strong>on</strong>. The tra<strong>in</strong><strong>in</strong>g is both desk-based<br />
and practical and can take up to ten m<strong>on</strong>ths to complete. 38<br />
The specialist nurse’s ma<strong>in</strong> priority is to manage the d<strong>on</strong>ati<strong>on</strong> process. Another key aspect is the<br />
collecti<strong>on</strong> and <strong>in</strong>terpretati<strong>on</strong> of data <strong>for</strong> the potential d<strong>on</strong>or audit (see below). They also have an<br />
important educati<strong>on</strong>al role at a local level. In additi<strong>on</strong>, under the new local collaborative model,<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 19
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
the specialist nurse has a more clearly def<strong>in</strong>ed strategic role <strong>in</strong> develop<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> locally,<br />
work<strong>in</strong>g with the cl<strong>in</strong>ical lead and the d<strong>on</strong>ati<strong>on</strong> committee to identify any problems, review<br />
per<strong>for</strong>mance and seek soluti<strong>on</strong>s as well as rais<strong>in</strong>g the profile of d<strong>on</strong>ati<strong>on</strong> both with<strong>in</strong> the<br />
hospital and <strong>in</strong> the local community.<br />
D<strong>on</strong>ati<strong>on</strong> committees<br />
The Task<strong>for</strong>ce’s fourth recommendati<strong>on</strong> was that every acute Trust, and equivalent <strong>in</strong> the devolved<br />
nati<strong>on</strong>s, should appo<strong>in</strong>t a d<strong>on</strong>ati<strong>on</strong> committee chaired by a n<strong>on</strong>-cl<strong>in</strong>ical ‘d<strong>on</strong>ati<strong>on</strong> champi<strong>on</strong>’.<br />
By November 2011 this had been achieved with the establishment of about 200 committees.<br />
Committee chairs come from a range of backgrounds <strong>in</strong>clud<strong>in</strong>g <strong>organ</strong> transplant recipients,<br />
n<strong>on</strong>-executive directors and retired cl<strong>in</strong>ical staff. Committee membership varies depend<strong>in</strong>g up<strong>on</strong><br />
local need, and availability, but the cl<strong>in</strong>ical leads and specialist nurses are key members. Other<br />
members <strong>in</strong>clude members of the cl<strong>in</strong>ical team from emergency medic<strong>in</strong>e, paediatric <strong>in</strong>tensive care,<br />
neuro-<strong>in</strong>tensive care and the palliative care service, the end-of-life care pathway lead, an operat<strong>in</strong>g<br />
theatre representative and a hospital chapla<strong>in</strong>. 39 Some Trust Medical Directors also sit <strong>on</strong> the<br />
committees. The committees are resp<strong>on</strong>sible <strong>for</strong> ensur<strong>in</strong>g that d<strong>on</strong>ati<strong>on</strong> is <strong>in</strong>tegrated <strong>in</strong>to the core<br />
bus<strong>in</strong>ess of the hospital and report to the Trust Board <strong>on</strong> a regular basis. The level of <strong>in</strong>volvement<br />
and engagement of Board members varies but overall appears to have improved significantly s<strong>in</strong>ce<br />
the <strong>in</strong>troducti<strong>on</strong> of the new structures. 40<br />
Part of the role of the d<strong>on</strong>ati<strong>on</strong> committee is to assess the data from the potential d<strong>on</strong>or audit<br />
to identify when, and why, potential d<strong>on</strong>ors have been lost or overlooked and to recommend<br />
soluti<strong>on</strong>s to any problems identified. D<strong>on</strong>ati<strong>on</strong> committees have also been <strong>in</strong>volved with the<br />
development of local d<strong>on</strong>ati<strong>on</strong> policies, rais<strong>in</strong>g awareness about d<strong>on</strong>ati<strong>on</strong> locally and identify<strong>in</strong>g<br />
appropriate ways of h<strong>on</strong>our<strong>in</strong>g d<strong>on</strong>ors.<br />
D<strong>on</strong>or identificati<strong>on</strong> and referral<br />
In l<strong>in</strong>e with the Task<strong>for</strong>ce’s fifth recommendati<strong>on</strong>, standard nati<strong>on</strong>al d<strong>on</strong>or identificati<strong>on</strong> and referral<br />
criteria have been established so that all patients who meet the criteria <strong>for</strong> bra<strong>in</strong> stem test<strong>in</strong>g<br />
(apnoea, coma from known aetiology and unresp<strong>on</strong>sive, ventilated and fixed pupils) or <strong>where</strong> a<br />
cl<strong>in</strong>ical decisi<strong>on</strong> has been made to withdraw life-prol<strong>on</strong>g<strong>in</strong>g treatment should be referred to the<br />
specialist nurse. This appears to be work<strong>in</strong>g well <strong>for</strong> those who meet the criteria <strong>for</strong> bra<strong>in</strong> stem<br />
test<strong>in</strong>g but there is some anecdotal evidence that the criteria <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> follow<strong>in</strong>g circulatory<br />
death are subject to differ<strong>in</strong>g <strong>in</strong>terpretati<strong>on</strong> and require further clarificati<strong>on</strong>. 41 This is c<strong>on</strong>firmed by<br />
the potential d<strong>on</strong>or audit (see below) which shows a low d<strong>on</strong>or identificati<strong>on</strong> and referral rate <strong>for</strong><br />
these potential d<strong>on</strong>ors and so clarify<strong>in</strong>g the referral criteria must be seen as a priority.<br />
In December 2011 the Nati<strong>on</strong>al Institute <strong>for</strong> Health and Cl<strong>in</strong>ical Excellence (NICE) published a<br />
cl<strong>in</strong>ical guidel<strong>in</strong>e <strong>on</strong> improv<strong>in</strong>g d<strong>on</strong>or identificati<strong>on</strong> and c<strong>on</strong>sent rates <strong>for</strong> deceased <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong>. 42 The guidel<strong>in</strong>e states that the healthcare team should discuss the potential <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> with the specialist nurse <strong>in</strong> all cases <strong>where</strong> the follow<strong>in</strong>g criteria are met:<br />
• ‘def<strong>in</strong>ed cl<strong>in</strong>ical trigger factors <strong>in</strong> patients who have had a catastrophic bra<strong>in</strong> <strong>in</strong>jury, namely:<br />
• the absence of <strong>on</strong>e or more cranial nerve reflexes and<br />
20<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
• a Glasgow Coma Scale (GCS) score of 4 or less that is not expla<strong>in</strong>ed by sedati<strong>on</strong><br />
unless there is a clear reas<strong>on</strong> why the above cl<strong>in</strong>ical triggers are not met (<strong>for</strong> example because of<br />
sedati<strong>on</strong>) and/or a decisi<strong>on</strong> has been made to per<strong>for</strong>m bra<strong>in</strong>stem death tests, whichever is the earlier<br />
• the <strong>in</strong>tenti<strong>on</strong> to withdraw life-susta<strong>in</strong><strong>in</strong>g treatment <strong>in</strong> patients with a life-threaten<strong>in</strong>g or lifelimit<strong>in</strong>g<br />
c<strong>on</strong>diti<strong>on</strong> which will, or is expected to, result <strong>in</strong> circulatory death’. 43<br />
The research data analysed by NICE, 44 showed that the use of cl<strong>in</strong>ical triggers and a requirement to<br />
refer accord<strong>in</strong>g to standard criteria led to an <strong>in</strong>crease <strong>in</strong> both referrals and d<strong>on</strong>ors. It is hoped that<br />
implementati<strong>on</strong> of the NICE guidel<strong>in</strong>e will result <strong>in</strong> early and c<strong>on</strong>sistent d<strong>on</strong>or referral. This,<br />
comb<strong>in</strong>ed with the cl<strong>in</strong>ical lead and specialist nurse provid<strong>in</strong>g support and guidance to staff and<br />
the d<strong>on</strong>ati<strong>on</strong> committee <strong>in</strong>vestigat<strong>in</strong>g all cases <strong>where</strong> potential d<strong>on</strong>ors are lost, should lead to an<br />
<strong>in</strong>crease <strong>in</strong> referral rates and, subsequently, an <strong>in</strong>crease <strong>in</strong> d<strong>on</strong>ors across the UK.<br />
Cl<strong>in</strong>ical management of potential d<strong>on</strong>ors, be<strong>for</strong>e and after referral, is also an important issue.<br />
This <strong>in</strong>cludes decisi<strong>on</strong>s about the tim<strong>in</strong>g of withdrawal of treatment (which should take account of<br />
the <strong>in</strong>dividual’s wish to become a d<strong>on</strong>or <strong>where</strong> that is known), and the <strong>in</strong>itial stabilisati<strong>on</strong> and<br />
assessment of potential d<strong>on</strong>ors. Work is currently underway to develop and test an ‘<strong>in</strong>tensive care<br />
bundle’ to help <strong>in</strong>tensivists to provide cl<strong>in</strong>ical care to potential d<strong>on</strong>ors <strong>in</strong> a way that will maximise<br />
d<strong>on</strong>ati<strong>on</strong> potential. 45<br />
Nati<strong>on</strong>al Organ Retrieval Service<br />
Another key change recommended by the Task<strong>for</strong>ce was the <strong>in</strong>troducti<strong>on</strong> of nati<strong>on</strong>al <strong>organ</strong><br />
retrieval teams. It recognised that the system <strong>in</strong> place s<strong>in</strong>ce the 1990s, which required specialist<br />
teams from several different transplant centres to attend a s<strong>in</strong>gle d<strong>on</strong>or, was problematic and<br />
unsusta<strong>in</strong>able. The teams varied <strong>in</strong> size, compositi<strong>on</strong> and level of experience. Most had other<br />
cl<strong>in</strong>ical commitments and so were often unable to resp<strong>on</strong>d at short notice and they relied heavily<br />
up<strong>on</strong> staff and facilities at the d<strong>on</strong>or hospital. Organ retrieval had developed <strong>in</strong> an ad hoc fashi<strong>on</strong><br />
and was neither explicitly funded nor per<strong>for</strong>mance-managed. The Task<strong>for</strong>ce’s proposal was that<br />
regi<strong>on</strong>al multi-<strong>organ</strong> retrieval teams should be established that were virtually self-sufficient and<br />
available 24 hours a day, seven days a week without other elective commitments dur<strong>in</strong>g periods <strong>on</strong><br />
call <strong>for</strong> <strong>organ</strong> retrieval. They would be able to provide early expert advice <strong>on</strong> d<strong>on</strong>or management<br />
as well as provid<strong>in</strong>g an efficient, high quality retrieval service. It was envisaged that this change<br />
would <strong>in</strong>crease capacity (to cater <strong>for</strong> the anticipated 50% <strong>in</strong>crease <strong>in</strong> d<strong>on</strong>ors), <strong>in</strong>crease the number<br />
of <strong>organ</strong>s collected per d<strong>on</strong>or and improve the quality of the <strong>organ</strong>s available. The new multi<strong>organ</strong><br />
retrieval service has been <strong>in</strong> place s<strong>in</strong>ce April 2010 and, under the new system, Trusts that<br />
support retrieval teams risk the impositi<strong>on</strong> of f<strong>in</strong>ancial penalties <strong>for</strong> n<strong>on</strong>-retrieval caused by a lack<br />
of team availability. 46<br />
In March 2010 NHS BT published nati<strong>on</strong>al standards <strong>for</strong> <strong>organ</strong> retrieval from deceased d<strong>on</strong>ors. 47<br />
The standards <strong>in</strong>clude that a retrieval centre po<strong>in</strong>t of c<strong>on</strong>tact must be available 24 hours a day,<br />
be able to dispatch the retrieval team with<strong>in</strong> <strong>on</strong>e hour of notificati<strong>on</strong> (unless the team is already<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 21
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
committed to retrieval else<strong>where</strong>) and an <strong>on</strong>-call c<strong>on</strong>sultant surge<strong>on</strong> must be available <strong>for</strong> the<br />
retrieval team to c<strong>on</strong>sult dur<strong>in</strong>g the retrieval if necessary. The standards also specify that lead<br />
abdom<strong>in</strong>al surge<strong>on</strong>s must be capable of accurately assess<strong>in</strong>g and retriev<strong>in</strong>g all abdom<strong>in</strong>al <strong>organ</strong>s<br />
and lead cardiothoracic surge<strong>on</strong>s must be capable of assess<strong>in</strong>g and retriev<strong>in</strong>g hearts and lungs.<br />
Where they are work<strong>in</strong>g together the two teams should agree, <strong>in</strong> advance, how the retrieval<br />
operati<strong>on</strong> will proceed.<br />
Review of the new system after <strong>on</strong>e year, to 1 April 2011, highlighted a number of issues. It found<br />
that although teams were required to be available 365 days a year, <strong>in</strong>dividual cardiothoracic teams<br />
were <strong>on</strong>ly out retriev<strong>in</strong>g <strong>organ</strong>s <strong>on</strong> between n<strong>in</strong>e and 28% of days and abdom<strong>in</strong>al teams <strong>on</strong><br />
between 19 and 59% of days. 48 This raised c<strong>on</strong>cerns about the effective use of resources which<br />
is currently be<strong>in</strong>g reviewed. Cardiothoracic retrieval is be<strong>in</strong>g c<strong>on</strong>sidered as <strong>on</strong>e part of a broader<br />
review of cardiothoracic transplantati<strong>on</strong> led by the NHS Nati<strong>on</strong>al Specialist Commissi<strong>on</strong><strong>in</strong>g Group. 49<br />
Despite these logistical issues, some cl<strong>in</strong>ical leads have reported that the revised retrieval<br />
arrangements have had a major positive impact <strong>on</strong> the effectiveness of the system <strong>in</strong> their area. 50<br />
The <strong>organ</strong> allocati<strong>on</strong> and offer<strong>in</strong>g system<br />
All <strong>organ</strong>s that become available are allocated accord<strong>in</strong>g to set criteria determ<strong>in</strong>ed by advisory<br />
groups relat<strong>in</strong>g to specific <strong>organ</strong>s. The blood group, age and size of both the d<strong>on</strong>or and recipient<br />
and, <strong>in</strong> some cases, the tissue type are taken <strong>in</strong>to account to ensure the best possible match <strong>for</strong><br />
each patient.<br />
The Task<strong>for</strong>ce recommended improvements to the process of allocati<strong>on</strong> by the <strong>in</strong>troducti<strong>on</strong> of<br />
an electr<strong>on</strong>ic offer<strong>in</strong>g scheme which speeds up the match<strong>in</strong>g and allocati<strong>on</strong> process <strong>for</strong> d<strong>on</strong>ated<br />
<strong>organ</strong>s. The web-based system enables specialist nurses <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> to <strong>in</strong>put data allow<strong>in</strong>g<br />
recipient nurses to see <strong>on</strong>-screen, <strong>in</strong> real time, the <strong>organ</strong>s that are available, <strong>where</strong> they have been<br />
offered and when they have been accepted. This significantly reduces the time and work <strong>in</strong>volved<br />
<strong>in</strong> the allocati<strong>on</strong> process. The electr<strong>on</strong>ic offer<strong>in</strong>g system (EOS) has been trialled and widely adopted<br />
around the country. As a result of this review some improvements are be<strong>in</strong>g made to the system<br />
be<strong>for</strong>e its use is further expanded.<br />
The British Transplantati<strong>on</strong> Society (BTS) and the Intensive Care Society (ICS) have also called up<strong>on</strong><br />
NHS BT to c<strong>on</strong>sider the way <strong>in</strong> which <strong>organ</strong>s from DCD d<strong>on</strong>ors are currently offered to transplant<br />
units. They believe that the system would be streaml<strong>in</strong>ed and made more efficient if <strong>organ</strong>s were<br />
offered to transplant units simultaneously rather than sequentially. 51 At the time of writ<strong>in</strong>g this<br />
issue is under review by NHS BT. 52<br />
The potential d<strong>on</strong>or audit<br />
It was recognised many years ago that a crucial part of the process of improv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> rates is<br />
to understand the true potential <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> from deceased d<strong>on</strong>ors and the reas<strong>on</strong>s <strong>for</strong><br />
n<strong>on</strong>-d<strong>on</strong>ati<strong>on</strong>. In April 2003 UK Transplant (now the Organ D<strong>on</strong>ati<strong>on</strong> and Transplant directorate<br />
of NHS BT) began rout<strong>in</strong>ely collect<strong>in</strong>g data <strong>on</strong> all deaths <strong>in</strong> <strong>in</strong>tensive care units throughout the UK.<br />
It identified the key po<strong>in</strong>ts <strong>in</strong> the d<strong>on</strong>ati<strong>on</strong> process: bra<strong>in</strong> stem test<strong>in</strong>g, c<strong>on</strong>sider<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong>,<br />
speak<strong>in</strong>g to relatives and obta<strong>in</strong><strong>in</strong>g c<strong>on</strong>sent to d<strong>on</strong>ati<strong>on</strong>. Through analys<strong>in</strong>g these data UK<br />
22<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
Transplant was able to identify <strong>where</strong> d<strong>on</strong>ors were lost and thus areas that required attenti<strong>on</strong>.<br />
The data were illum<strong>in</strong>at<strong>in</strong>g. From 1 April 2003 to 31 March 2005 2,740 <strong>in</strong>dividuals’ deaths were<br />
diagnosed by bra<strong>in</strong> stem tests (<strong>in</strong>dividuals who were there<strong>for</strong>e identified as potential d<strong>on</strong>ors), of<br />
whom <strong>on</strong>ly 1,244 (45.4%) went <strong>on</strong> to d<strong>on</strong>ate. 53 D<strong>on</strong>ati<strong>on</strong> was c<strong>on</strong>sidered <strong>in</strong> 90% of cases and,<br />
of these, an approach was made to the <strong>next</strong> of k<strong>in</strong> <strong>for</strong> permissi<strong>on</strong> <strong>in</strong> 94% of cases. C<strong>on</strong>firm<strong>in</strong>g<br />
anecdotal evidence, the largest reas<strong>on</strong> <strong>for</strong> n<strong>on</strong>-d<strong>on</strong>ati<strong>on</strong> was found to be relative refusal which<br />
stood at 41% of those approached (rang<strong>in</strong>g from 35% am<strong>on</strong>gst the white populati<strong>on</strong> to 70%<br />
<strong>for</strong> ethnic m<strong>in</strong>orities). Another area <strong>where</strong> d<strong>on</strong>ors could have been lost was the failure to carry<br />
out bra<strong>in</strong> stem tests. In 4,166 patients bra<strong>in</strong> stem death was recorded as a possible diagnosis but<br />
<strong>in</strong> 1,309 (31.4%) of these, tests were not carried out. Although they are often l<strong>in</strong>ked, bra<strong>in</strong> stem<br />
death test<strong>in</strong>g was not <strong>in</strong>troduced to facilitate <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> but <strong>for</strong> the diagnosis of death <strong>in</strong><br />
situati<strong>on</strong>s <strong>where</strong> there had been severe neurological damage yet other vital <strong>organ</strong>s were be<strong>in</strong>g<br />
ma<strong>in</strong>ta<strong>in</strong>ed by high level medical <strong>in</strong>terventi<strong>on</strong>. It should, there<strong>for</strong>e, be the norm <strong>for</strong> bra<strong>in</strong> stem<br />
death test<strong>in</strong>g to be carried out <strong>on</strong> every patient <strong>where</strong> bra<strong>in</strong> stem death is a possible diagnosis<br />
unless there are there are cl<strong>in</strong>ical reas<strong>on</strong>s why this is not appropriate.<br />
The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce stressed that, <strong>in</strong> additi<strong>on</strong> to the actual number of d<strong>on</strong>ors, an important<br />
measure of success is the proporti<strong>on</strong> of those suitable <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> who are identified and whose<br />
pers<strong>on</strong>al, or family’s, wishes are ascerta<strong>in</strong>ed and followed. The number of transplants is clearly also an<br />
important measure of success. The Task<strong>for</strong>ce welcomed <strong>on</strong>go<strong>in</strong>g work by NHS BT to collect more<br />
detailed data and to expand the potential d<strong>on</strong>or audit to emergency departments. It recommended<br />
that the data <strong>for</strong> <strong>in</strong>dividual Trusts should be made publicly available and reviewed by the Trust Board.<br />
D<strong>on</strong>ati<strong>on</strong> after bra<strong>in</strong> stem death<br />
The new enhanced and expanded potential d<strong>on</strong>or audit has been <strong>in</strong> operati<strong>on</strong> s<strong>in</strong>ce October 2009.<br />
In the first full year (1 April 2010 to 31 March 2011), 1,141 patients’ deaths <strong>in</strong> <strong>in</strong>tensive care units<br />
were diagnosed by bra<strong>in</strong> stem tests and there were no absolute c<strong>on</strong>tra<strong>in</strong>dicati<strong>on</strong>s to d<strong>on</strong>ati<strong>on</strong>. 54<br />
Of these 617 (54%) went <strong>on</strong> to d<strong>on</strong>ate. The family was approached about d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> 93% of<br />
cases (<strong>in</strong> 20% of cases <strong>where</strong> relatives were not approached this was because the family had<br />
already stated that they would not c<strong>on</strong>sent be<strong>for</strong>e a <strong>for</strong>mal approach was made.) Overall the<br />
family refusal rate was 35%. Where the <strong>in</strong>dividual’s wish to d<strong>on</strong>ate was known the refusal rate<br />
dropped to 6% but when the relatives did not know the <strong>in</strong>dividual’s views it <strong>in</strong>creased to 50% 55 .<br />
Ethnicity rema<strong>in</strong>s highly significant <strong>in</strong> respect of refusal rates with a rate of 29% am<strong>on</strong>gst the<br />
white populati<strong>on</strong> and 77% am<strong>on</strong>gst the n<strong>on</strong>-white populati<strong>on</strong>.<br />
As <strong>in</strong> 2003 there were a number of cases, 467 (28%), <strong>where</strong> all of the criteria <strong>for</strong> bra<strong>in</strong> stem<br />
test<strong>in</strong>g were met but the tests were not carried out; the reas<strong>on</strong>s given <strong>for</strong> this varied but <strong>in</strong>cluded<br />
that the patient was haemodynamically unstable and that there was family pressure not to test. 56<br />
There were also cases, 258 (15%), <strong>where</strong> the referral criteria were met but the case was not<br />
referred to the specialist nurse. 57 In 30% of these cases the reas<strong>on</strong> given was that the patient<br />
was not identified as a potential d<strong>on</strong>or or d<strong>on</strong>ati<strong>on</strong> was not c<strong>on</strong>sidered. 58 In 91% of cases<br />
<strong>where</strong> c<strong>on</strong>sent was provided d<strong>on</strong>ati<strong>on</strong> proceeded. Where it did not proceed the ma<strong>in</strong> reas<strong>on</strong>s<br />
were that the <strong>organ</strong>s were deemed medically unsuitable by the recipient centres (25%) or the<br />
cor<strong>on</strong>er/procurator fiscal refused to give authorisati<strong>on</strong> (17%). 59<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 23
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
It is difficult to make a direct comparis<strong>on</strong> with the 2003 data because of the different way <strong>in</strong><br />
which the data are presented but there have clearly been some improvements, <strong>in</strong>clud<strong>in</strong>g a<br />
welcome reducti<strong>on</strong> <strong>in</strong> the refusal rate which decreased from 41% to 35%. D<strong>on</strong>ati<strong>on</strong> rates <strong>for</strong><br />
<strong>in</strong>dividual areas c<strong>on</strong>t<strong>in</strong>ue to show significant variati<strong>on</strong> although this could <strong>in</strong> part be due to<br />
factors such as the age, sex and ethnicity of the populati<strong>on</strong>.<br />
Summary of key data <strong>for</strong> DBD 2010/11 60<br />
Yes % No %<br />
Total number of deaths <strong>in</strong> ICU and emergency departments 29,060<br />
Criteria <strong>for</strong> bra<strong>in</strong> stem test<strong>in</strong>g and referral met 1,672<br />
Referred to specialist nurse (% of those meet<strong>in</strong>g test<strong>in</strong>g criteria) 1,414 84.6 15.4<br />
Bra<strong>in</strong> stem tests carried out (% of those meet<strong>in</strong>g criteria) 1,205 72.1 27.9<br />
Death c<strong>on</strong>firmed and no medical c<strong>on</strong>tra<strong>in</strong>dicati<strong>on</strong>s<br />
(ie. potential d<strong>on</strong>ors)<br />
1,141<br />
Family approached (% of potential) 1,057 92.6 7.4<br />
C<strong>on</strong>sent/authorisati<strong>on</strong> obta<strong>in</strong>ed (% of those <strong>where</strong> families approached) 682 64.5 35.5<br />
Solid <strong>organ</strong>s d<strong>on</strong>ated (% of those with c<strong>on</strong>sent) 617 90.5 9.5<br />
D<strong>on</strong>ati<strong>on</strong> after circulatory death<br />
Under the new system, data are also collected <strong>on</strong> d<strong>on</strong>ati<strong>on</strong> after circulatory death (DCD) follow<strong>in</strong>g<br />
the planned withdrawal of treatment. In 2010-2011, there were 2,875 potential d<strong>on</strong>ors whose<br />
imm<strong>in</strong>ent death was anticipated, treatment was withdrawn and there were no absolute<br />
c<strong>on</strong>tra<strong>in</strong>dicati<strong>on</strong>s to solid <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. 61 With these potential d<strong>on</strong>ors, the n<strong>on</strong>-referral rate<br />
was significantly higher at 56%. 62 As with d<strong>on</strong>ati<strong>on</strong> after bra<strong>in</strong> stem death, <strong>in</strong> 32% of cases the<br />
reas<strong>on</strong> given was that <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> was not c<strong>on</strong>sidered; the medical c<strong>on</strong>tra<strong>in</strong>dicati<strong>on</strong>s rate was<br />
also high am<strong>on</strong>gst this group at 34%. 63 The relatives were approached about d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> 47% of<br />
cases and am<strong>on</strong>g these the relative refusal rate was 49% (<strong>where</strong> the <strong>in</strong>dividual’s wish to d<strong>on</strong>ate<br />
was known the refusal rate dropped but <strong>on</strong>ly to 20% which is significantly higher than <strong>for</strong> DBD<br />
d<strong>on</strong>ors 64 ). Where c<strong>on</strong>sent (or authorisati<strong>on</strong>) was provided, d<strong>on</strong>ati<strong>on</strong> proceeded <strong>in</strong> 50% of cases.<br />
Of the cases <strong>where</strong> d<strong>on</strong>ati<strong>on</strong> did not proceed, <strong>in</strong> almost half this was because there was a<br />
prol<strong>on</strong>ged period between treatment withdrawal and death result<strong>in</strong>g <strong>in</strong> <strong>organ</strong> damage and <strong>in</strong><br />
a further 21% of cases the <strong>organ</strong>s were deemed medically unsuitable by the recipient centres. 65<br />
24<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
Summary of key data <strong>for</strong> DCD 2010/11 6<br />
Yes % No %<br />
Total number of deaths <strong>in</strong> ICU and emergency departments 29,060<br />
Referral criteria met (<strong>on</strong> ventilator, not BSD, imm<strong>in</strong>ent death expected) 7,192<br />
Referred to specialist nurse (% of those <strong>where</strong> referral criteria met) 3,188 44.3 55.7<br />
Treatment withdrawn and no medical c<strong>on</strong>tra<strong>in</strong>dicati<strong>on</strong>s<br />
(ie. potential d<strong>on</strong>ors)<br />
2,875<br />
Family approached (% of potential) 1,359 47.3 52.7<br />
C<strong>on</strong>sent/authorisati<strong>on</strong> obta<strong>in</strong>ed (%of those <strong>where</strong> family approached) 691 50.8 49.2<br />
Solid <strong>organ</strong>s d<strong>on</strong>ated (% of those with c<strong>on</strong>sent) 345 49.9 50.1<br />
Potential d<strong>on</strong>or rate<br />
Another important and <strong>in</strong>terest<strong>in</strong>g additi<strong>on</strong> to the data set is <strong>in</strong><strong>for</strong>mati<strong>on</strong> about the potential<br />
d<strong>on</strong>or rates per milli<strong>on</strong> populati<strong>on</strong> <strong>in</strong> the UK. 67 This allows us to assess what is the absolute<br />
maximum rate of d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK if all potential d<strong>on</strong>ors went <strong>on</strong> to d<strong>on</strong>ate (recognis<strong>in</strong>g, of<br />
course, that <strong>in</strong> practice this is unachievable). The data <strong>for</strong> 2010/11 show that over that period the<br />
rate of potential DBD d<strong>on</strong>ors was 18.4 per milli<strong>on</strong> populati<strong>on</strong>. The potential rate of DCD d<strong>on</strong>ors<br />
was 46.4 per milli<strong>on</strong> populati<strong>on</strong>. This is based <strong>on</strong> 2,875 potential DCD d<strong>on</strong>ors but it needs to be<br />
recognised that a significant percentage of those (probably around 43%) will be unable to d<strong>on</strong>ate<br />
because of an extended period between withdrawal of treatment and death. This reduces the<br />
potential DCD d<strong>on</strong>or rate to 26.4 per milli<strong>on</strong> populati<strong>on</strong>, giv<strong>in</strong>g a total potential deceased d<strong>on</strong>or<br />
rate of 44.8 per milli<strong>on</strong> populati<strong>on</strong>. The current d<strong>on</strong>ati<strong>on</strong> rate <strong>in</strong> the UK is 16.3. 68<br />
Cl<strong>in</strong>ical, legal and ethical guidance<br />
Over the last few years a number of guidel<strong>in</strong>es have been published <strong>on</strong> various aspects of <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> with a view to improv<strong>in</strong>g practice and c<strong>on</strong>sistency throughout the UK. Some of these<br />
documents predated the Task<strong>for</strong>ce. Others were published <strong>in</strong> direct resp<strong>on</strong>se to the Task<strong>for</strong>ce’s<br />
third recommendati<strong>on</strong> that outstand<strong>in</strong>g legal, ethical and professi<strong>on</strong>al issues should be resolved so<br />
that professi<strong>on</strong>als can work with<strong>in</strong> a clear and unambiguous framework of good practice. This<br />
secti<strong>on</strong> highlights the ma<strong>in</strong> po<strong>in</strong>ts <strong>in</strong> some of these key documents.<br />
The process of seek<strong>in</strong>g c<strong>on</strong>sent<br />
In additi<strong>on</strong> to identify<strong>in</strong>g standard referral criteria (see above), the NICE guidel<strong>in</strong>e <strong>on</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> 69 also provides detailed advice about the process of plann<strong>in</strong>g and seek<strong>in</strong>g c<strong>on</strong>sent based<br />
<strong>on</strong> analysis of the published research. This <strong>in</strong>cludes the recommendati<strong>on</strong> that the approach should<br />
be made by a multi-discipl<strong>in</strong>ary team made up of the medical and nurs<strong>in</strong>g staff <strong>in</strong>volved<br />
<strong>in</strong> the care of the patient led by an identifiable c<strong>on</strong>sultant, and the specialist nurse <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong>. A local faith representative should also be <strong>in</strong>cluded <strong>where</strong> that is likely to be the wish<br />
of the family. The guidance also states that the <strong>organ</strong> d<strong>on</strong>or register should be checked, and the<br />
d<strong>on</strong>or’s potential to d<strong>on</strong>ate should be identified, be<strong>for</strong>e the relatives are approached. Families<br />
should be allowed sufficient time to understand and accept the <strong>in</strong>evitability of death and to spend<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 25
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
time with the patient be<strong>for</strong>e the issue of d<strong>on</strong>ati<strong>on</strong> is raised unless the family <strong>in</strong>itiates discussi<strong>on</strong><br />
about d<strong>on</strong>ati<strong>on</strong> earlier. When the approach is made, it should be <strong>in</strong> positive terms and should<br />
avoid the use of negative or apologetic language (eg ‘I am sorry to have to ask you…’). The<br />
guidel<strong>in</strong>e also lists the <strong>in</strong><strong>for</strong>mati<strong>on</strong> that must be provided and the knowledge and skills required<br />
by those specialists approach<strong>in</strong>g relatives.<br />
The <strong>BMA</strong> supports these recommendati<strong>on</strong>s. It believes that <strong>in</strong><strong>for</strong>mati<strong>on</strong> about <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong><br />
should be given to families <strong>in</strong> a positive way that emphasises the huge difference d<strong>on</strong>ati<strong>on</strong> makes<br />
to people’s lives, and that families should be <strong>in</strong><strong>for</strong>med of the com<strong>for</strong>t that many families derive<br />
from the knowledge that their loved <strong>on</strong>e’s <strong>organ</strong>s have been used <strong>for</strong> d<strong>on</strong>ati<strong>on</strong>.<br />
Diagnosis of death<br />
In 2008 the Academy of Medical Royal Colleges published a code of practice <strong>for</strong> the diagnosis and<br />
c<strong>on</strong>firmati<strong>on</strong> of death. 70 This reviewed and updated the exist<strong>in</strong>g guidance <strong>on</strong> diagnos<strong>in</strong>g death by<br />
bra<strong>in</strong> stem tests <strong>in</strong> those over the age of three m<strong>on</strong>ths and also, <strong>for</strong> the first time, <strong>in</strong>cluded clear<br />
guidance <strong>on</strong> diagnos<strong>in</strong>g death follow<strong>in</strong>g cardio-respiratory failure. The <strong>in</strong>crease <strong>in</strong> d<strong>on</strong>ors follow<strong>in</strong>g<br />
circulatory death prompted the need <strong>for</strong> clear, nati<strong>on</strong>ally agreed guidance both about how death<br />
is diagnosed and also the necessary period between death be<strong>in</strong>g diagnosed and <strong>in</strong>terventi<strong>on</strong>s<br />
commenc<strong>in</strong>g with the aim of preserv<strong>in</strong>g <strong>organ</strong>s <strong>for</strong> d<strong>on</strong>ati<strong>on</strong>. The code specifies that <strong>where</strong> a<br />
patient has suffered cardio-respiratory arrest and attempts to resuscitate are either <strong>in</strong>appropriate<br />
or have been unsuccessful, the <strong>in</strong>dividual should be observed <strong>for</strong> five m<strong>in</strong>utes. After this time a set<br />
of basic tests should be undertaken to c<strong>on</strong>firm that death has occurred (<strong>in</strong>clud<strong>in</strong>g c<strong>on</strong>firm<strong>in</strong>g the<br />
absence of circulati<strong>on</strong> us<strong>in</strong>g an arterial l<strong>in</strong>e or electrocardiogram (ECG)) and the legal time of death<br />
should be recorded as the time the tests are undertaken.<br />
Bra<strong>in</strong> stem test<strong>in</strong>g has frequently been closely associated with <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> but the code of<br />
practice emphasises that bra<strong>in</strong> stem tests should be undertaken <strong>in</strong> all patients who might meet<br />
the criteria and that they should not be c<strong>on</strong>sidered <strong>on</strong>ly <strong>in</strong> cases of possible <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. The<br />
same recommendati<strong>on</strong> was made by the Task<strong>for</strong>ce. This is because it is good cl<strong>in</strong>ical practice to<br />
withdraw treatment that is no l<strong>on</strong>ger able to benefit patients. The Academy’s code of practice<br />
restates the requirement that the diagnosis of death follow<strong>in</strong>g bra<strong>in</strong> stem tests must be made<br />
by at least two medical practiti<strong>on</strong>ers who have been registered <strong>for</strong> more than five years and are<br />
competent <strong>in</strong> the c<strong>on</strong>duct and <strong>in</strong>terpretati<strong>on</strong> of bra<strong>in</strong> stem test<strong>in</strong>g, at least <strong>on</strong>e of whom must<br />
be a c<strong>on</strong>sultant. The set of tests should be c<strong>on</strong>ducted <strong>on</strong> two separate occasi<strong>on</strong>s but the legal<br />
time of death is after the first set has diagnosed that the patient is dead.<br />
D<strong>on</strong>ati<strong>on</strong> follow<strong>in</strong>g circulatory death<br />
S<strong>in</strong>ce around 2005 there has been a big <strong>in</strong>crease <strong>in</strong> the number of units provid<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> after<br />
circulatory death (see secti<strong>on</strong> 3) such that these d<strong>on</strong>ors now make up nearly 37% of all deceased<br />
d<strong>on</strong>ati<strong>on</strong>. 71 Yet this is <strong>on</strong>e area highlighted by the Task<strong>for</strong>ce <strong>where</strong> there rema<strong>in</strong>ed legal, ethical<br />
and cl<strong>in</strong>ical uncerta<strong>in</strong>ty and <strong>where</strong> additi<strong>on</strong>al guidance was required. S<strong>in</strong>ce the Task<strong>for</strong>ce report<br />
was published, three sets of guidance have been produced address<strong>in</strong>g different aspects of this type<br />
of d<strong>on</strong>ati<strong>on</strong>: legal guidance (from the Department of Health and Welsh Assembly Government, 72<br />
26<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
the Scottish Government 73 and the Department of Health, Social Services and Public Safety <strong>in</strong><br />
Northern Ireland 74 ) ethical guidance from the UK D<strong>on</strong>ati<strong>on</strong> Ethics Committee 75 and cl<strong>in</strong>ical<br />
guidance from the British Transplantati<strong>on</strong> Society and the Intensive Care Society. 76<br />
Tak<strong>in</strong>g steps be<strong>for</strong>e death to facilitate d<strong>on</strong>ati<strong>on</strong><br />
The <strong>BMA</strong>’s Medical Ethics Committee (MEC) discussed, <strong>in</strong> 2004 and aga<strong>in</strong> <strong>in</strong> 2010, the questi<strong>on</strong> of<br />
what, if any, steps could be taken be<strong>for</strong>e death to facilitate <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. On both occasi<strong>on</strong>s the<br />
MEC c<strong>on</strong>cluded that some steps – such as c<strong>on</strong>t<strong>in</strong>u<strong>in</strong>g fluids or oxygen and tak<strong>in</strong>g a blood sample<br />
<strong>for</strong> virology screen<strong>in</strong>g – would be both legally and ethically justified <strong>where</strong> it was known that the<br />
<strong>in</strong>dividual wished to d<strong>on</strong>ate <strong>organ</strong>s after death. The <strong>BMA</strong> there<strong>for</strong>e supports the view that <strong>where</strong><br />
an <strong>in</strong>dividual wanted to be an <strong>organ</strong> d<strong>on</strong>or, it is ethically acceptable to take steps to facilitate, or<br />
at least not to frustrate, the patient’s wish to d<strong>on</strong>ate <strong>organ</strong>s after death provided the steps are<br />
not c<strong>on</strong>trary to the patient’s <strong>in</strong>terests. The legal test that must be satisfied, however, is a ‘best<br />
<strong>in</strong>terests’ test; any <strong>in</strong>terventi<strong>on</strong>s <strong>in</strong>volv<strong>in</strong>g patients who lack capacity must be <strong>in</strong> their best <strong>in</strong>terests.<br />
In order to assess this, every case needs to be c<strong>on</strong>sidered <strong>in</strong>dividually to determ<strong>in</strong>e the <strong>in</strong>dividual’s<br />
wishes and the risk of caus<strong>in</strong>g any harm or distress to the patient or those close to the patient.<br />
In the <strong>BMA</strong>’s view, the level of evidence available about the <strong>in</strong>dividual’s wishes is an important<br />
factor <strong>in</strong> decid<strong>in</strong>g what <strong>in</strong>terventi<strong>on</strong> is appropriate. For example:<br />
a) those d<strong>on</strong>ors who have stated, <strong>in</strong> advance, that they would be will<strong>in</strong>g to undergo <strong>in</strong>vasive<br />
procedures to enhance the prospect of a successful transplant;<br />
b) those d<strong>on</strong>ors who have <strong>in</strong>dicated a wish to d<strong>on</strong>ate their <strong>organ</strong>s – by jo<strong>in</strong><strong>in</strong>g the Organ D<strong>on</strong>or<br />
Register or sign<strong>in</strong>g a d<strong>on</strong>or card;<br />
c) those d<strong>on</strong>ors <strong>where</strong> the relatives have authorised d<strong>on</strong>ati<strong>on</strong> <strong>on</strong> the basis of the d<strong>on</strong>or’s known<br />
wishes and beliefs;<br />
d) those d<strong>on</strong>ors <strong>where</strong> the relatives have authorised d<strong>on</strong>ati<strong>on</strong> <strong>on</strong> the basis of the d<strong>on</strong>or’s likely<br />
wishes and beliefs;<br />
e) those d<strong>on</strong>ors <strong>where</strong> there is no <strong>in</strong>dicati<strong>on</strong> of the d<strong>on</strong>or’s wishes but <strong>where</strong> the relatives have<br />
n<strong>on</strong>etheless authorised d<strong>on</strong>ati<strong>on</strong> as someth<strong>in</strong>g they wish to see happen.<br />
The further down this list <strong>on</strong>e goes, the more difficult it is to justify <strong>in</strong>vasive procedures <strong>on</strong> the<br />
basis of a ‘best <strong>in</strong>terests’ test.<br />
The first official guidance <strong>on</strong> this subject was published <strong>in</strong> November 2009, by the Department of<br />
Health and Welsh Assembly Government. 77 This document focused <strong>on</strong> the broad assessment of<br />
‘best <strong>in</strong>terests’ required under the Mental Capacity Act 2005, which takes account of medical,<br />
social, cultural and religious issues, focus<strong>in</strong>g <strong>on</strong> the <strong>in</strong>dividual’s own wishes and beliefs. It<br />
c<strong>on</strong>cluded that <strong>where</strong> it is known that the <strong>in</strong>dividual wanted to d<strong>on</strong>ate <strong>organ</strong>s after death, some<br />
acti<strong>on</strong>s to facilitate d<strong>on</strong>ati<strong>on</strong> could be <strong>in</strong> the pers<strong>on</strong>’s best <strong>in</strong>terests if they do not cause the pers<strong>on</strong><br />
harm or distress (<strong>in</strong>clud<strong>in</strong>g caus<strong>in</strong>g distress to family and friends) and would there<strong>for</strong>e be lawful.<br />
The type of <strong>in</strong>terventi<strong>on</strong>s c<strong>on</strong>sidered <strong>in</strong>cluded adjustments to the tim<strong>in</strong>g or place of death,<br />
ma<strong>in</strong>tenance or adjustment of exist<strong>in</strong>g treatments such as fluids or <strong>in</strong>otropes to ma<strong>in</strong>ta<strong>in</strong> patient<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 27
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
stability and blood sampl<strong>in</strong>g <strong>for</strong> the purpose of tissue typ<strong>in</strong>g or virology screen<strong>in</strong>g. Where it is not<br />
possible to ascerta<strong>in</strong> the <strong>in</strong>dividual’s wishes the guidance states that cl<strong>in</strong>icians would need ‘a<br />
compell<strong>in</strong>g reas<strong>on</strong>’ to take acti<strong>on</strong>s to facilitate d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the <strong>in</strong>dividual’s best <strong>in</strong>terests. Parallel<br />
guidance was issued <strong>in</strong> Scotland, <strong>in</strong> May 2010, <strong>in</strong> relati<strong>on</strong> to decid<strong>in</strong>g whether acti<strong>on</strong>s to enhance<br />
the chances of a successful d<strong>on</strong>ati<strong>on</strong> would be <strong>for</strong> the pers<strong>on</strong>’s ‘benefit’ as required by the Adults<br />
with Incapacity (Scotland) Act 2000. 78 In March 2011 similar guidance was published <strong>in</strong> Northern<br />
Ireland based <strong>on</strong> the comm<strong>on</strong> law pr<strong>in</strong>ciple of best <strong>in</strong>terests. 79<br />
In December 2011, the UK D<strong>on</strong>ati<strong>on</strong> Ethics Committee (UK DEC) – set up <strong>in</strong> resp<strong>on</strong>se to the<br />
Task<strong>for</strong>ce’s third recommendati<strong>on</strong> – published its first report, An ethical framework <strong>for</strong> c<strong>on</strong>trolled<br />
d<strong>on</strong>ati<strong>on</strong> after circulatory death. In relati<strong>on</strong> to this subject UK DEC took a similar positi<strong>on</strong> to the<br />
DH and <strong>BMA</strong>. 80 This report also provides a detailed ethical framework to guide practice throughout<br />
the d<strong>on</strong>ati<strong>on</strong> process.<br />
Cl<strong>in</strong>ical guidance<br />
In June 2010 the Department of Health hosted a c<strong>on</strong>sensus meet<strong>in</strong>g <strong>on</strong> d<strong>on</strong>ati<strong>on</strong> after circulatory<br />
death, follow<strong>in</strong>g which the Intensive Care Society (ICS) and the British Transplantati<strong>on</strong> Society (BTS)<br />
published jo<strong>in</strong>t cl<strong>in</strong>ical guidance. 81 The document highlighted the wide variati<strong>on</strong> <strong>in</strong> practice <strong>in</strong> both<br />
the care of potential DCD d<strong>on</strong>ors and the retrieval and transplantati<strong>on</strong> of <strong>organ</strong>s, and sought to<br />
provide clear cl<strong>in</strong>ical guidance <strong>for</strong> practice. The guidance stated very clearly that a decisi<strong>on</strong> to<br />
withdraw treatment must be completely separate from, and precede, any c<strong>on</strong>siderati<strong>on</strong> of <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong>. No measures to facilitate d<strong>on</strong>ati<strong>on</strong> should be <strong>in</strong>stituted be<strong>for</strong>e this decisi<strong>on</strong> has been<br />
made. The guidel<strong>in</strong>es covered issues such as suitability criteria <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> after circulatory death,<br />
the process of treatment withdrawal, the def<strong>in</strong>iti<strong>on</strong> of ‘optimal’ and ‘sub-optimal’ d<strong>on</strong>ors and the<br />
diagnosis of death and post mortem <strong>in</strong>terventi<strong>on</strong>s. Some areas were identified <strong>where</strong> further<br />
debate was needed be<strong>for</strong>e agreement could be reached such as the possibility of c<strong>on</strong>t<strong>in</strong>u<strong>in</strong>g<br />
ventilati<strong>on</strong> <strong>for</strong> a period of time <strong>in</strong> the belief that some of the patients will go <strong>on</strong> to fulfil the<br />
criteria <strong>for</strong> DBD rather than DCD.<br />
Requested allocati<strong>on</strong> of <strong>organ</strong>s<br />
In March 2010 the UK Health Adm<strong>in</strong>istrati<strong>on</strong>s, together with NHS BT and the Human Tissue<br />
Authority produced a <strong>policy</strong> document <strong>on</strong> requested allocati<strong>on</strong> of a deceased d<strong>on</strong>or <strong>organ</strong>. This<br />
followed a small number of requests by <strong>in</strong>dividuals or their families <strong>for</strong> <strong>organ</strong>s to be d<strong>on</strong>ated, after<br />
death, to a family member or close friend. At the time such requests were turned down because<br />
d<strong>on</strong>ati<strong>on</strong>s were required to be unc<strong>on</strong>diti<strong>on</strong>al, follow<strong>in</strong>g a case <strong>in</strong> 1998 <strong>where</strong> an <strong>in</strong>dividual’s family<br />
stipulated that <strong>organ</strong>s should be used <strong>on</strong>ly <strong>for</strong> white recipients. 82 The type of case envisaged by the<br />
<strong>policy</strong> document was <strong>where</strong> a family member or close friend of the potential d<strong>on</strong>or required a<br />
transplant and the d<strong>on</strong>or, or the d<strong>on</strong>or’s family, requested that they should be given priority. It was<br />
po<strong>in</strong>ted out, <strong>in</strong> debate <strong>on</strong> the issue, that liv<strong>in</strong>g d<strong>on</strong>ors can direct their d<strong>on</strong>ati<strong>on</strong> to a particular<br />
<strong>in</strong>dividual. In fact, <strong>in</strong> some of the cases c<strong>on</strong>sidered, the patient was <strong>in</strong> the process of becom<strong>in</strong>g<br />
a liv<strong>in</strong>g d<strong>on</strong>or <strong>for</strong> a family member or friend be<strong>for</strong>e the <strong>in</strong>cident that led to death.<br />
28<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
One of the fundamental pr<strong>in</strong>ciples of the UK’s <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> system is that <strong>organ</strong>s are d<strong>on</strong>ated<br />
freely, voluntarily and unc<strong>on</strong>diti<strong>on</strong>ally. In additi<strong>on</strong>, the Human Tissue (Scotland) Act 2006<br />
specifically prohibits <strong>in</strong>dividuals from attach<strong>in</strong>g c<strong>on</strong>diti<strong>on</strong>s to their d<strong>on</strong>ati<strong>on</strong>s. 83 When the <strong>BMA</strong>’s<br />
Medical Ethics Committee (MEC) discussed this issue <strong>in</strong> 2007 it c<strong>on</strong>cluded that the basic pr<strong>in</strong>ciples,<br />
that d<strong>on</strong>ati<strong>on</strong> should be unc<strong>on</strong>diti<strong>on</strong>al and that <strong>organ</strong>s should be allocated <strong>on</strong> the basis of cl<strong>in</strong>ical<br />
need, should be upheld. It believed, however, that there should be some flexibility to c<strong>on</strong>sider<br />
<strong>in</strong>dividual requests <strong>for</strong> directed d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> rare and excepti<strong>on</strong>al cases. The MEC did not, however,<br />
support allow<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> to be c<strong>on</strong>diti<strong>on</strong>al up<strong>on</strong> an <strong>organ</strong> go<strong>in</strong>g to a particular recipient. Rather<br />
it should be possible <strong>for</strong> families to request that c<strong>on</strong>siderati<strong>on</strong> is given to allocat<strong>in</strong>g the <strong>organ</strong> to<br />
a particular pers<strong>on</strong> who is genetically or emoti<strong>on</strong>ally close to the d<strong>on</strong>or. Whether that request is<br />
accepted would depend, at least <strong>in</strong> part, <strong>on</strong> the potential harms to others – <strong>for</strong> example, if there<br />
was some<strong>on</strong>e <strong>on</strong> the ‘super urgent’ list who would die without the <strong>organ</strong>, the family should be<br />
<strong>in</strong><strong>for</strong>med that it was not possible to meet their request and that the <strong>organ</strong> would be allocated <strong>on</strong><br />
the basis of cl<strong>in</strong>ical need. C<strong>on</strong>sent (or authorisati<strong>on</strong>) <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> must however be given<br />
irrespective of whether the request is accepted. To do otherwise, the MEC c<strong>on</strong>sidered, would be<br />
to submit to a <strong>for</strong>m of c<strong>on</strong>diti<strong>on</strong>ality that is not acceptable <strong>for</strong> this type of public service.<br />
The <strong>policy</strong> document, from the Health Departments and NHS BT, takes a very similar approach,<br />
stat<strong>in</strong>g that a request <strong>for</strong> directed d<strong>on</strong>ati<strong>on</strong> can be c<strong>on</strong>sidered <strong>where</strong>:<br />
• c<strong>on</strong>sent, or authorisati<strong>on</strong>, has been provided;<br />
• the c<strong>on</strong>sent or authorisati<strong>on</strong> is not c<strong>on</strong>diti<strong>on</strong>al <strong>on</strong> the request be<strong>in</strong>g met;<br />
• there are no others <strong>in</strong> desperately urgent cl<strong>in</strong>ical need of the <strong>organ</strong> who might be harmed by<br />
the <strong>organ</strong> go<strong>in</strong>g to the nom<strong>in</strong>ated <strong>in</strong>dividual (<strong>in</strong>dividuals <strong>on</strong> the urgent heart scheme or super<br />
urgent liver list will always be given priority);<br />
• the <strong>in</strong>dividual, <strong>in</strong> his or her lifetime, or the family after death, had requested d<strong>on</strong>ati<strong>on</strong> to a<br />
particular <strong>in</strong>dividual who is a family member or friend of l<strong>on</strong>g stand<strong>in</strong>g; and<br />
• the potential recipient is <strong>on</strong> the transplant wait<strong>in</strong>g list or meets the criteria <strong>for</strong> a transplant.<br />
As a safeguard, NHS BT established a mechanism to c<strong>on</strong>sider and approve <strong>in</strong>dividual requests<br />
that fall with<strong>in</strong> this framework. By November 2011, four requests had been made, three of which<br />
were approved (<strong>in</strong> the fourth case d<strong>on</strong>ati<strong>on</strong> was c<strong>on</strong>diti<strong>on</strong>al up<strong>on</strong> the request be<strong>in</strong>g met and<br />
so the agreed criteria were not met). For a variety of reas<strong>on</strong>s n<strong>on</strong>e of these d<strong>on</strong>ati<strong>on</strong>s actually<br />
went ahead. 84<br />
Guidance <strong>for</strong> cor<strong>on</strong>ers<br />
One of the problems identified by the Task<strong>for</strong>ce was the significant variati<strong>on</strong> <strong>in</strong> the decisi<strong>on</strong>s of<br />
cor<strong>on</strong>ers and procurators fiscal regard<strong>in</strong>g whether d<strong>on</strong>ati<strong>on</strong> could proceed <strong>in</strong> cases referred to<br />
them. It had been known <strong>for</strong> some time that some cor<strong>on</strong>ers refused permissi<strong>on</strong> <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> <strong>in</strong><br />
all cases of sudden or unexpla<strong>in</strong>ed death <strong>where</strong>as others would allow d<strong>on</strong>ati<strong>on</strong> of some <strong>organ</strong>s<br />
<strong>where</strong> this would not <strong>in</strong>terfere with their <strong>in</strong>vestigati<strong>on</strong>. The Task<strong>for</strong>ce recommended that<br />
discussi<strong>on</strong>s should take place and nati<strong>on</strong>al guidel<strong>in</strong>es should be developed <strong>in</strong> order to ensure<br />
c<strong>on</strong>sistency and to m<strong>in</strong>imise the number of cases <strong>where</strong> d<strong>on</strong>ati<strong>on</strong> is prevented. As a result, <strong>in</strong><br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 29
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
March 2010, the Department of Health, together with the M<strong>in</strong>istry of Justice, produced guidance<br />
<strong>for</strong> specialist nurses <strong>on</strong> work<strong>in</strong>g with cor<strong>on</strong>ers 84 and an aide-memoire <strong>for</strong> cor<strong>on</strong>ers. 85 These<br />
documents emphasise the importance of the cor<strong>on</strong>er or a deputy be<strong>in</strong>g available to make<br />
a decisi<strong>on</strong> <strong>in</strong> a timely manner and set out the <strong>in</strong><strong>for</strong>mati<strong>on</strong> the cor<strong>on</strong>er is likely to need prior to<br />
giv<strong>in</strong>g agreement to d<strong>on</strong>ati<strong>on</strong>. They expla<strong>in</strong> that it might be possible <strong>for</strong> the cor<strong>on</strong>er to agree to<br />
the removal of <strong>organ</strong>s from those parts of the body that are not likely to be significant <strong>in</strong> any<br />
subsequent post-mortem exam<strong>in</strong>ati<strong>on</strong> and that the cor<strong>on</strong>er may ask <strong>for</strong> a <strong>for</strong>ensic pathologist<br />
to be present dur<strong>in</strong>g <strong>organ</strong> retrieval. Cor<strong>on</strong>ers are advised that they may wish to discuss the<br />
possibility of d<strong>on</strong>ati<strong>on</strong> with the pathologist who will undertake the post-mortem exam<strong>in</strong>ati<strong>on</strong> and,<br />
<strong>where</strong> relevant, the police be<strong>for</strong>e mak<strong>in</strong>g a decisi<strong>on</strong>. Awareness of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> will also be<br />
<strong>in</strong>cluded <strong>in</strong> cor<strong>on</strong>ers’ tra<strong>in</strong><strong>in</strong>g. In spite of these developments there rema<strong>in</strong>s significant unexpla<strong>in</strong>ed<br />
variati<strong>on</strong> <strong>in</strong> cor<strong>on</strong>er’s refusals. Further work with cor<strong>on</strong>ers is <strong>on</strong>go<strong>in</strong>g <strong>in</strong> a further attempt to<br />
reduce the variati<strong>on</strong> <strong>in</strong> practice and the number of d<strong>on</strong>ors lost.<br />
In Scotland, there is a l<strong>on</strong>g-stand<strong>in</strong>g agreement between the Scottish Transplant Group and the<br />
Crown Office and Procurator Fiscal Service regard<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. This is currently be<strong>in</strong>g<br />
updated to take account of the development of DCD programmes.<br />
Liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong><br />
In May 2011 the British Transplantati<strong>on</strong> Society and the Renal Associati<strong>on</strong> produced the third<br />
editi<strong>on</strong> of their United K<strong>in</strong>gdom Guidel<strong>in</strong>es <strong>for</strong> Liv<strong>in</strong>g D<strong>on</strong>or Kidney Transplantati<strong>on</strong>. 87 The<br />
guidel<strong>in</strong>es cover cl<strong>in</strong>ical, ethical and legal aspects of liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> provid<strong>in</strong>g up-to-date and<br />
robust guidel<strong>in</strong>es <strong>for</strong> cl<strong>in</strong>icians <strong>in</strong>volved <strong>in</strong> this area of transplantati<strong>on</strong>.<br />
In additi<strong>on</strong>, <strong>in</strong> January 2012 NHS Blood and Transplant published its UK Strategy <strong>for</strong> Liv<strong>in</strong>g D<strong>on</strong>or<br />
Kidney Transplantati<strong>on</strong> with the aim of <strong>in</strong>creas<strong>in</strong>g the number of liv<strong>in</strong>g kidney d<strong>on</strong>or transplants.<br />
The key aims of the strategy are to:<br />
‘1. Increase transplant activity from liv<strong>in</strong>g kidney d<strong>on</strong>ors <strong>for</strong> both adult and paediatric recipients,<br />
ensur<strong>in</strong>g that d<strong>on</strong>or safety is c<strong>on</strong>sistently promoted through best cl<strong>in</strong>ical practice.<br />
2. Achieve optimum pre-emptive liv<strong>in</strong>g d<strong>on</strong>or kidney transplantati<strong>on</strong> rates and equity of access<br />
<strong>for</strong> patients with<strong>in</strong> each transplant centre across the UK.<br />
3. Maximise the opportunities <strong>for</strong> d<strong>on</strong>ors and recipients who wish to participate <strong>in</strong> the Nati<strong>on</strong>al<br />
Liv<strong>in</strong>g D<strong>on</strong>or Kidney Shar<strong>in</strong>g Schemes, which <strong>in</strong>clude paired/pooled d<strong>on</strong>ati<strong>on</strong>, n<strong>on</strong>-directed<br />
altruistic d<strong>on</strong>ati<strong>on</strong> and altruistic d<strong>on</strong>or cha<strong>in</strong>s.’ 88<br />
C<strong>on</strong>siderable emphasis is placed <strong>on</strong> the importance of hav<strong>in</strong>g appropriate, robust and transparent<br />
commissi<strong>on</strong><strong>in</strong>g arrangements <strong>in</strong> place to facilitate and encourage liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong>. In fact, NHS BT<br />
highlights the lack of streaml<strong>in</strong>ed commissi<strong>on</strong><strong>in</strong>g arrangements across the UK as the primary risk<br />
to the successful implementati<strong>on</strong> of the strategy.<br />
30<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
What more can or should be d<strong>on</strong>e?<br />
The last four years have seen momentous and significant changes to the <strong>in</strong>frastructure with<strong>in</strong><br />
which <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> takes place. This has resulted <strong>in</strong> more d<strong>on</strong>ors and more transplants be<strong>in</strong>g<br />
undertaken. This is cause <strong>for</strong> celebrati<strong>on</strong>, but not complacency: people are still dy<strong>in</strong>g and as l<strong>on</strong>g<br />
as more can be d<strong>on</strong>e, more should be d<strong>on</strong>e. Whilst the 14 recommendati<strong>on</strong>s of the Task<strong>for</strong>ce have<br />
been fully or significantly implemented, some still require work over a l<strong>on</strong>ger period of time and<br />
other areas should also be explored. Set out below are some areas <strong>where</strong> further work is needed<br />
to maximise the efficiency of the system to ensure that all potential d<strong>on</strong>ors who want to d<strong>on</strong>ate<br />
are able to do so. Most, if not all, of these issues are already be<strong>in</strong>g <strong>in</strong>vestigated but the momentum<br />
and enthusiasm that has built up from the Task<strong>for</strong>ce report must be ma<strong>in</strong>ta<strong>in</strong>ed <strong>in</strong> the l<strong>on</strong>ger term.<br />
Increas<strong>in</strong>g referrals<br />
Some of the recommendati<strong>on</strong>s of the Task<strong>for</strong>ce require changes to cl<strong>in</strong>ical practice and <strong>in</strong> the way<br />
<strong>in</strong> which health professi<strong>on</strong>als carry out their work. The re<strong>for</strong>ms that have taken place have been<br />
aimed at chang<strong>in</strong>g the m<strong>in</strong>dset of those work<strong>in</strong>g with dy<strong>in</strong>g patients, so that all health professi<strong>on</strong>als<br />
see d<strong>on</strong>ati<strong>on</strong> as part of their resp<strong>on</strong>sibility to their patients which will <strong>in</strong>evitably take time and<br />
require <strong>on</strong>go<strong>in</strong>g ef<strong>for</strong>t. This will <strong>in</strong>clude work<strong>in</strong>g with health professi<strong>on</strong>als based <strong>in</strong> emergency<br />
medic<strong>in</strong>e as well as those <strong>in</strong> <strong>in</strong>tensive care <strong>where</strong> potential d<strong>on</strong>ors have traditi<strong>on</strong>ally been<br />
identified. It is hoped that <strong>in</strong> the future:<br />
• all patients who meet the criteria <strong>for</strong> bra<strong>in</strong> stem test<strong>in</strong>g will have the tests undertaken,<br />
irrespective of whether they are c<strong>on</strong>sidered likely to be d<strong>on</strong>ors;<br />
• health professi<strong>on</strong>als’ acceptance and implementati<strong>on</strong> of cl<strong>in</strong>ical triggers and/or clear and<br />
unambiguous referral criteria will ensure the specialist nurse is c<strong>on</strong>sulted and <strong>in</strong>volved at an early<br />
stage <strong>in</strong> all possible cases; and<br />
• there are no more cases <strong>where</strong> the potential d<strong>on</strong>or audit reports that <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> was simply<br />
not c<strong>on</strong>sidered (failure to c<strong>on</strong>sider d<strong>on</strong>ati<strong>on</strong> <strong>where</strong> a pers<strong>on</strong> was <strong>on</strong> the ODR should be reviewed<br />
at a senior level <strong>in</strong> the hospital).<br />
Unlike most aspects of d<strong>on</strong>ati<strong>on</strong>, this is an area that could be subject to targets and possibly<br />
reward schemes such as the Commissi<strong>on</strong><strong>in</strong>g <strong>for</strong> Quality and Innovati<strong>on</strong> (CQIN) payment framework<br />
<strong>in</strong> England. A hospital could, <strong>for</strong> example, receive payments <strong>for</strong> achiev<strong>in</strong>g a 100% referral rate <strong>for</strong><br />
potential d<strong>on</strong>ors (based <strong>on</strong> clear and unambiguous referral criteria). Such an <strong>in</strong>centive would not<br />
result <strong>in</strong> a c<strong>on</strong>flict of <strong>in</strong>terest s<strong>in</strong>ce it is not about d<strong>on</strong>ati<strong>on</strong> rates, per se, but about giv<strong>in</strong>g all<br />
patients who are dy<strong>in</strong>g the opti<strong>on</strong> of d<strong>on</strong>ati<strong>on</strong> <strong>where</strong> that is a possibility. One Strategic Health<br />
Authority has <strong>in</strong>cluded <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>in</strong>dicators <strong>in</strong>to its CQIN framework and this is reported to<br />
have led to greater scrut<strong>in</strong>y of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> with<strong>in</strong> the Trust and also appears to be show<strong>in</strong>g<br />
improvements <strong>in</strong> those areas m<strong>on</strong>itored by the CQIN. NHS BT is c<strong>on</strong>sider<strong>in</strong>g how this <strong>in</strong>itiative<br />
could be expanded to other parts of the UK. 89<br />
One of the aims of the Task<strong>for</strong>ce was to remove dis<strong>in</strong>centives to d<strong>on</strong>ati<strong>on</strong> by recommend<strong>in</strong>g that<br />
hospitals are reimbursed <strong>for</strong> the cost of <strong>organ</strong> retrieval, re<strong>in</strong>stat<strong>in</strong>g a system that was abolished <strong>in</strong><br />
the late 1990s. The rati<strong>on</strong>ale <strong>for</strong> its aboliti<strong>on</strong> was that pay<strong>in</strong>g hospitals’ costs when they retrieved<br />
<strong>organ</strong>s made it appear that this was an ‘opti<strong>on</strong>al extra’ rather than part of the core bus<strong>in</strong>ess of<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 31
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
acute hospitals. The m<strong>on</strong>ey was, there<strong>for</strong>e, <strong>in</strong>cluded <strong>in</strong> the overall hospital budget but, <strong>in</strong> practice,<br />
did not reach its <strong>in</strong>tended dest<strong>in</strong>ati<strong>on</strong>. The re<strong>in</strong>troducti<strong>on</strong> of the payment <strong>for</strong> reimbursement needs<br />
to be m<strong>on</strong>itored to ensure the m<strong>on</strong>ey is reach<strong>in</strong>g the appropriate departments but, <strong>where</strong> it is<br />
work<strong>in</strong>g well, it is seen as welcome recogniti<strong>on</strong> of the work <strong>in</strong>volved <strong>in</strong> d<strong>on</strong>ati<strong>on</strong>. 90<br />
Reduc<strong>in</strong>g the relative refusal rates<br />
It has l<strong>on</strong>g been known that <strong>on</strong>e of the major problems <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> is the high rate of<br />
relative refusals. In the 2003 Potential D<strong>on</strong>or Audit, it stood at 41%; by 2010 it had reduced<br />
to 35% <strong>for</strong> DBD d<strong>on</strong>ors but this is still too high. In produc<strong>in</strong>g its guidance, NICE reviewed the<br />
published literature <strong>in</strong>clud<strong>in</strong>g identify<strong>in</strong>g the key factors that were associated with c<strong>on</strong>sent<br />
and with refusal.<br />
Factors associated with c<strong>on</strong>sent be<strong>in</strong>g given: 91<br />
• ‘understand<strong>in</strong>g that transplantati<strong>on</strong> was a proven procedure, had a high success rate,<br />
and knowledge of the benefits of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong><br />
• an understand<strong>in</strong>g of the term bra<strong>in</strong> death<br />
• acceptance of death, and c<strong>on</strong>fidence <strong>in</strong> the ‘diagnosis of death’<br />
• c<strong>on</strong>siderati<strong>on</strong> and knowledge of the deceased’s wishes (through carry<strong>in</strong>g a d<strong>on</strong>or card<br />
or discussi<strong>on</strong>)<br />
• earlier tim<strong>in</strong>g of request<br />
• <strong>in</strong>volv<strong>in</strong>g more family members with the decisi<strong>on</strong><br />
• the level of com<strong>for</strong>t with which the healthcare professi<strong>on</strong>al requested c<strong>on</strong>sent<br />
• good relati<strong>on</strong>ships between the family and the healthcare professi<strong>on</strong>als<br />
• satisfacti<strong>on</strong> with treatment (either of the family or the deceased)<br />
• c<strong>on</strong>gruence between the views of healthcare professi<strong>on</strong>als and the families at <strong>in</strong>itial approach<br />
• request <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> be<strong>in</strong>g <strong>in</strong>itiated by a healthcare professi<strong>on</strong>al (not a physician) with<br />
further discussi<strong>on</strong> with an <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> professi<strong>on</strong>al<br />
• request by different healthcare professi<strong>on</strong>als<br />
• more time spent with an <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> professi<strong>on</strong>al<br />
• knowledge of the impact of d<strong>on</strong>ati<strong>on</strong> <strong>on</strong> other processes, such as funeral arrangements<br />
• knowledge of the costs of d<strong>on</strong>ati<strong>on</strong><br />
• choice of <strong>organ</strong>s <strong>for</strong> d<strong>on</strong>ati<strong>on</strong><br />
• families be<strong>in</strong>g able to discuss both specific and wider issues and gett<strong>in</strong>g answers to questi<strong>on</strong>s.’<br />
32<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
Factors associated with a decisi<strong>on</strong> to refuse c<strong>on</strong>sent: 92<br />
• feel<strong>in</strong>gs of pressure to c<strong>on</strong>sent<br />
• feel<strong>in</strong>g emoti<strong>on</strong>ally overwhelmed<br />
• feel<strong>in</strong>g of surprise <strong>on</strong> be<strong>in</strong>g asked about c<strong>on</strong>sent<br />
• fear of caus<strong>in</strong>g more ‘suffer<strong>in</strong>g’ or disfigurement, and not want<strong>in</strong>g the deceased to have<br />
more medical <strong>in</strong>terventi<strong>on</strong><br />
• c<strong>on</strong>cern that d<strong>on</strong>ati<strong>on</strong> may cause more distress to family members<br />
• uncerta<strong>in</strong>ty about the deceased’s wishes<br />
• reluctance to accept the death<br />
• social resentment<br />
• lack of understand<strong>in</strong>g and c<strong>on</strong>fidence <strong>in</strong> the c<strong>on</strong>cept of bra<strong>in</strong>-stem death<br />
• lack of family c<strong>on</strong>sensus and the family be<strong>in</strong>g ‘upset’<br />
• family reticence<br />
• mak<strong>in</strong>g the decisi<strong>on</strong> be<strong>for</strong>e <strong>in</strong><strong>for</strong>mati<strong>on</strong> was provided by a healthcare or <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong><br />
professi<strong>on</strong>al<br />
• an absence of key decisi<strong>on</strong> makers<br />
• the length of the process<br />
• not lik<strong>in</strong>g the hospital or healthcare professi<strong>on</strong>als<br />
• feel<strong>in</strong>g that the medical care was not optimal<br />
• <strong>in</strong>itial approach by a healthcare professi<strong>on</strong>al<br />
• percepti<strong>on</strong> that the healthcare professi<strong>on</strong>al did not care or was not c<strong>on</strong>cerned, or the<br />
healthcare professi<strong>on</strong>al show<strong>in</strong>g a lack of respect<br />
• healthcare professi<strong>on</strong>als stat<strong>in</strong>g that the request was required<br />
• lack of knowledge of the impact of d<strong>on</strong>ati<strong>on</strong> <strong>on</strong> other processes, such as funeral<br />
arrangements<br />
• lack of detailed <strong>in</strong><strong>for</strong>mati<strong>on</strong> <strong>on</strong> the process of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>, <strong>in</strong>clud<strong>in</strong>g the tim<strong>in</strong>g of<br />
retrieval and <strong>in</strong><strong>for</strong>mati<strong>on</strong> <strong>on</strong> recipients<br />
• <strong>in</strong>itial percepti<strong>on</strong> of healthcare professi<strong>on</strong>als that the family were likely to refuse.’<br />
More research is needed <strong>in</strong> this area and careful c<strong>on</strong>siderati<strong>on</strong> should be given to determ<strong>in</strong><strong>in</strong>g<br />
what more can be d<strong>on</strong>e to make relatives more likely to c<strong>on</strong>sent. This might <strong>in</strong>clude:<br />
• c<strong>on</strong>t<strong>in</strong>ued attempts to raise awareness of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> and to encourage people to make<br />
their views known and to discuss the issue with<strong>in</strong> families (<strong>in</strong> Scotland, <strong>where</strong> there have been<br />
<strong>on</strong>go<strong>in</strong>g promoti<strong>on</strong>al campaigns about <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> the c<strong>on</strong>sent rate has risen to 86%. 93 )<br />
• more work with ethnic m<strong>in</strong>ority communities – <strong>where</strong> the refusal rate is particularly high – to<br />
understand the specific reas<strong>on</strong>s <strong>for</strong> this and to identify factors that would motivate these groups<br />
to d<strong>on</strong>ate<br />
• compulsory tra<strong>in</strong><strong>in</strong>g <strong>in</strong> bereavement <strong>for</strong> those who are likely to approach relatives<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 33
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
• improved tra<strong>in</strong><strong>in</strong>g about d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> both undergraduate and postgraduate educati<strong>on</strong> so that<br />
all health professi<strong>on</strong>als feel c<strong>on</strong>fident <strong>in</strong> identify<strong>in</strong>g potential d<strong>on</strong>ors and jo<strong>in</strong><strong>in</strong>g specialist nurses<br />
<strong>in</strong> discuss<strong>in</strong>g the issues with families<br />
• c<strong>on</strong>sider<strong>in</strong>g whether there would be any advantage <strong>in</strong> giv<strong>in</strong>g the family a short death certificate,<br />
c<strong>on</strong>firm<strong>in</strong>g that death has occurred, be<strong>for</strong>e <strong>organ</strong>s are removed. Provisi<strong>on</strong> <strong>for</strong> short death<br />
certificates was made <strong>in</strong> the Cor<strong>on</strong>ers and Justice Act 2009 but has not yet been implemented.<br />
The potential d<strong>on</strong>or audit (see above) shows that the relative refusal rate is particularly high<br />
am<strong>on</strong>gst black and ethnic m<strong>in</strong>ority populati<strong>on</strong>s. Work is <strong>on</strong>go<strong>in</strong>g to try to determ<strong>in</strong>e the reas<strong>on</strong><br />
<strong>for</strong> this and to ensure that this group is aware of the impact of their decisi<strong>on</strong>s <strong>on</strong> people with<strong>in</strong><br />
their community. 94 Black and ethnic m<strong>in</strong>ority groups are more likely to need a transplant but less<br />
likely to sign up to the <strong>organ</strong> d<strong>on</strong>or register. Even <strong>where</strong> people have <strong>in</strong>dicated their wish to<br />
d<strong>on</strong>ate, relatives are more likely to override their wishes. This is a very serious issue that needs<br />
to be addressed and work must c<strong>on</strong>t<strong>in</strong>ue to f<strong>in</strong>d <strong>in</strong>novative ways of reach<strong>in</strong>g these groups.<br />
Bra<strong>in</strong> stem death test<strong>in</strong>g <strong>in</strong> ne<strong>on</strong>ates<br />
The Academy of Medical Royal College’s code of practice <strong>on</strong> diagnos<strong>in</strong>g death 95 applies <strong>on</strong>ly to<br />
those over the age of three m<strong>on</strong>ths and there are currently no standard tests <strong>for</strong> diagnos<strong>in</strong>g bra<strong>in</strong><br />
stem death <strong>in</strong> ne<strong>on</strong>ates. This means that ne<strong>on</strong>atal hearts are not d<strong>on</strong>ated <strong>in</strong> the UK. There are<br />
bra<strong>in</strong> stem death test<strong>in</strong>g standards <strong>for</strong> ne<strong>on</strong>ates <strong>in</strong> other parts of Europe, however, and so<br />
currently ne<strong>on</strong>atal hearts are imported. 96 This is an area that requires attenti<strong>on</strong> so that the<br />
diagnosis of death <strong>in</strong> ne<strong>on</strong>ates is brought <strong>in</strong>to l<strong>in</strong>e with other countries.<br />
Agreed acceptance criteria <strong>for</strong> <strong>organ</strong>s<br />
C<strong>on</strong>siderati<strong>on</strong> needs to be given to the development and c<strong>on</strong>sistent applicati<strong>on</strong> of agreed<br />
acceptance criteria <strong>for</strong> <strong>organ</strong>s. Currently different criteria are used by different transplant surge<strong>on</strong>s<br />
and physicians and many <strong>organ</strong>s are refused without the surge<strong>on</strong> see<strong>in</strong>g the <strong>organ</strong>s. There may<br />
be good reas<strong>on</strong>s why <strong>organ</strong>s are refused but there need to be clear and c<strong>on</strong>sistent criteria to<br />
guide this decisi<strong>on</strong>. NHS BT is currently work<strong>in</strong>g to address this problem. 97<br />
Organ d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the NHS<br />
There is a widespread view that the re<strong>for</strong>ms that have taken place have been a major success and<br />
the <strong>BMA</strong> shares this view. It is also evident that those charged with implement<strong>in</strong>g the re<strong>for</strong>ms<br />
and tak<strong>in</strong>g th<strong>in</strong>gs <strong>for</strong>ward at a local level <strong>on</strong> a day-to-day basis dem<strong>on</strong>strate great enthusiasm<br />
and commitment. Over the last four years there have been c<strong>on</strong>siderable resources directed to<br />
implement<strong>in</strong>g the Task<strong>for</strong>ce report, both <strong>in</strong> terms of time and m<strong>on</strong>ey but th<strong>in</strong>gs are chang<strong>in</strong>g.<br />
The Programme Delivery Board, established to oversee implementati<strong>on</strong> of the Task<strong>for</strong>ce<br />
recommendati<strong>on</strong>s, has been disbanded and Mr Chris Rudge, Nati<strong>on</strong>al Cl<strong>in</strong>ical Director <strong>for</strong><br />
Transplantati<strong>on</strong>, who was resp<strong>on</strong>sible <strong>for</strong> the day-to-day management of the changes, retired at<br />
the end of August 2011 and will not be replaced. Some c<strong>on</strong>cerns have been expressed that, with<br />
the loss of this central driv<strong>in</strong>g <strong>for</strong>ce, changes <strong>in</strong> the Health Service <strong>in</strong> England, and reducti<strong>on</strong>s <strong>in</strong><br />
public sector spend<strong>in</strong>g throughout the UK, the momentum that has been developed could be lost.<br />
As a resp<strong>on</strong>se to some of these c<strong>on</strong>cerns a Transiti<strong>on</strong>al Steer<strong>in</strong>g Group has been established by<br />
34<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
the Department of Health. 98 This group, chaired by Mr Chris Rudge, has membership from the four<br />
Health Departments, NHS BT and the key professi<strong>on</strong>al groups <strong>for</strong> <strong>in</strong>tensive care, emergency<br />
medic<strong>in</strong>e and transplantati<strong>on</strong>. It is reassur<strong>in</strong>g that many of those work<strong>in</strong>g with<strong>in</strong> the system have<br />
stated str<strong>on</strong>gly that the momentum that has built up can and should be ma<strong>in</strong>ta<strong>in</strong>ed at a local<br />
level. They believe this can be achieved with strategic directi<strong>on</strong> and <strong>in</strong>put from NHS BT (which<br />
is lead<strong>in</strong>g the development of a post-2013 strategy) and support and encouragement via the<br />
structure of regi<strong>on</strong>al d<strong>on</strong>ati<strong>on</strong> collaboratives. 99 Whilst there is uncerta<strong>in</strong>ty about the future, there<br />
is also tremendous optimism that what has been achieved can be ma<strong>in</strong>ta<strong>in</strong>ed and developed.<br />
At the time of writ<strong>in</strong>g the process <strong>for</strong> commissi<strong>on</strong><strong>in</strong>g transplant services <strong>in</strong> England is unclear.<br />
The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce advised that the commissi<strong>on</strong><strong>in</strong>g of all transplant services should be<br />
undertaken <strong>on</strong> a nati<strong>on</strong>al basis – a view the <strong>BMA</strong> supports. There are also questi<strong>on</strong>s about how<br />
maximum benefit can be derived from the work that has been d<strong>on</strong>e by, <strong>for</strong> example, l<strong>in</strong>k<strong>in</strong>g<br />
commissi<strong>on</strong><strong>in</strong>g to per<strong>for</strong>mance, such as whether commissi<strong>on</strong>ers of acute hospital services could<br />
make their c<strong>on</strong>tracts dependent up<strong>on</strong> NICE guidel<strong>in</strong>es <strong>on</strong> referral and c<strong>on</strong>sent be<strong>in</strong>g followed.<br />
Whatever systems are put <strong>in</strong> place, <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> must c<strong>on</strong>t<strong>in</strong>ue to be managed and coord<strong>in</strong>ated<br />
<strong>in</strong> a coherent fashi<strong>on</strong> and to be seen as an <strong>in</strong>tegral part of the end-of-life care pathway.<br />
It is <strong>on</strong>ly if these changes are protected that the major advances that have been made can be<br />
ma<strong>in</strong>ta<strong>in</strong>ed and we can beg<strong>in</strong> to build <strong>on</strong> the new <strong>in</strong>frastructure.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 35
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
5 Increas<strong>in</strong>g the number of d<strong>on</strong>ors<br />
As we have seen over the last four years develop<strong>in</strong>g the <strong>in</strong>frastructure, as described <strong>in</strong> the previous<br />
secti<strong>on</strong>, can by itself <strong>in</strong>crease the d<strong>on</strong>ati<strong>on</strong> rate through better d<strong>on</strong>or identificati<strong>on</strong> and referral,<br />
improved systems <strong>for</strong> <strong>organ</strong> retrieval and allocati<strong>on</strong> and the expansi<strong>on</strong> of new types of d<strong>on</strong>ati<strong>on</strong><br />
such as d<strong>on</strong>ati<strong>on</strong> after circulatory death. Further improvement can be made by <strong>in</strong>creas<strong>in</strong>g the<br />
number of d<strong>on</strong>ors, <strong>in</strong> order to make maximum use of the <strong>in</strong>frastructure that is now <strong>in</strong> place.<br />
This secti<strong>on</strong> sets out a number of ways that have been suggested <strong>for</strong> achiev<strong>in</strong>g this <strong>in</strong>crease either<br />
with<strong>in</strong> the current opt-<strong>in</strong> system or by c<strong>on</strong>sider<strong>in</strong>g alternatives to it. Some of these <strong>in</strong>itiatives are<br />
relatively unc<strong>on</strong>troversial such as expand<strong>in</strong>g c<strong>on</strong>trolled DCD programmes to emergency departments<br />
and <strong>in</strong>creas<strong>in</strong>g publicity <strong>for</strong> the NHS Organ D<strong>on</strong>or Register. Others, such as the <strong>in</strong>troducti<strong>on</strong> of a<br />
regulated market, are more c<strong>on</strong>tentious. In fact the <strong>BMA</strong> does not support some of the opti<strong>on</strong>s set<br />
out <strong>in</strong> this report but has <strong>in</strong>cluded them <strong>on</strong> the basis that those c<strong>on</strong>sider<strong>in</strong>g how best to proceed<br />
should at least be aware of all of the opti<strong>on</strong>s. The <strong>BMA</strong>’s views are clearly set out below.<br />
Expand<strong>in</strong>g the pool of potential d<strong>on</strong>ors<br />
Expand<strong>in</strong>g c<strong>on</strong>trolled DCD programmes to emergency departments<br />
The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce emphasised that <strong>in</strong>tensive care should not be the sole focus <strong>for</strong><br />
<strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> and that all areas <strong>where</strong> end-of-life care is provided should be <strong>in</strong>cluded. Attenti<strong>on</strong><br />
has recently focused <strong>on</strong> emergency departments (EDs), <strong>where</strong> patients are admitted who are not<br />
expected to survive their <strong>in</strong>juries and d<strong>on</strong>ati<strong>on</strong> after circulatory death may be possible. Currently,<br />
<strong>in</strong> many such cases treatment is withdrawn <strong>in</strong> the ED and <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> is not c<strong>on</strong>sidered. It is<br />
hoped that by rais<strong>in</strong>g awareness am<strong>on</strong>gst those work<strong>in</strong>g <strong>in</strong> EDs (with the assistance of cl<strong>in</strong>ical<br />
leads, specialist nurses and d<strong>on</strong>ati<strong>on</strong> committees) and provid<strong>in</strong>g clear cl<strong>in</strong>ical guidel<strong>in</strong>es, d<strong>on</strong>ati<strong>on</strong><br />
could become an opti<strong>on</strong> <strong>for</strong> those admitted to the ED with no, or very little, hope of survival.<br />
Data collected via the potential d<strong>on</strong>or audit show that the number of potential DCD d<strong>on</strong>ors <strong>in</strong><br />
emergency departments has ranged between 155 and 207 <strong>in</strong> each of the three six m<strong>on</strong>th periods<br />
s<strong>in</strong>ce April 2010. The actual number of DCD d<strong>on</strong>ors <strong>in</strong> each of these periods, however, ranged<br />
from <strong>on</strong>ly 5 to 11. 100 Work to <strong>in</strong>crease the number of d<strong>on</strong>ors from this source is there<strong>for</strong>e<br />
c<strong>on</strong>sidered a priority. In the l<strong>on</strong>ger term attenti<strong>on</strong> will focus <strong>on</strong> other areas such as acute stroke<br />
units, medical assessment units and general medical wards so that <strong>in</strong>dividuals treated <strong>in</strong> those<br />
facilities may also have the opti<strong>on</strong> of d<strong>on</strong>ati<strong>on</strong>. It is also possible, <strong>in</strong> the future, that unc<strong>on</strong>trolled<br />
DCD from emergency departments might be c<strong>on</strong>sidered (see secti<strong>on</strong> 3).<br />
In October 2010, the Department of Health hosted a c<strong>on</strong>sensus meet<strong>in</strong>g follow<strong>in</strong>g which the<br />
College of Emergency Medic<strong>in</strong>e and the British Transplantati<strong>on</strong> Society published a report sett<strong>in</strong>g<br />
out ways of ensur<strong>in</strong>g that the opti<strong>on</strong> of d<strong>on</strong>ati<strong>on</strong> is available <strong>for</strong> those who die <strong>in</strong> the emergency<br />
department. 101 In practice this would mean that, <strong>for</strong> example <strong>where</strong> patients have catastrophic<br />
bra<strong>in</strong> <strong>in</strong>jury that is not survivable, rather than withdraw<strong>in</strong>g treatment <strong>in</strong> the ED, the cl<strong>in</strong>ical team<br />
would refer the patient to the specialist nurse and steps would be taken to establish the <strong>in</strong>dividual’s<br />
wishes regard<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong>. Wherever possible, potential d<strong>on</strong>ors would subsequently be transferred<br />
to a critical care sett<strong>in</strong>g <strong>for</strong> assessment, management and withdrawal of treatment.<br />
36<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
The report <strong>in</strong>cluded the follow<strong>in</strong>g recommendati<strong>on</strong>s:<br />
• all emergency departments (EDs) should c<strong>on</strong>sider the identificati<strong>on</strong> of a lead cl<strong>in</strong>ician with an<br />
<strong>in</strong>terest <strong>in</strong> d<strong>on</strong>ati<strong>on</strong> who should be represented <strong>on</strong> the Trust/Health Board D<strong>on</strong>ati<strong>on</strong> Committee<br />
• the potential <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> should be reviewed after each death <strong>in</strong> EDs and data from the<br />
Potential D<strong>on</strong>or Audit (see secti<strong>on</strong> 4) should be reviewed every six m<strong>on</strong>ths<br />
• local <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> policies should be developed <strong>for</strong> EDs, <strong>in</strong>clud<strong>in</strong>g the care of a ventilated<br />
patient and the transfer of patients to <strong>in</strong>tensive care <strong>for</strong> further assessment and management<br />
• exist<strong>in</strong>g tra<strong>in</strong><strong>in</strong>g and educati<strong>on</strong> programmes <strong>for</strong> ED staff should be supplemented by<br />
<strong>in</strong>corporat<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>in</strong>to Emergency Department <strong>in</strong>ducti<strong>on</strong> programmes and<br />
local/regi<strong>on</strong>al study days.<br />
The <strong>BMA</strong> supports these recommendati<strong>on</strong>s but recognises that due to resource c<strong>on</strong>stra<strong>in</strong>ts it may<br />
not always be possible <strong>for</strong> patients to be transferred from the emergency department to ICU when<br />
d<strong>on</strong>ati<strong>on</strong> is be<strong>in</strong>g c<strong>on</strong>sidered. This may be because there are no beds available or because the<br />
patients do not meet the admissi<strong>on</strong> criteria. This is an issue that needs to be explored further both<br />
to determ<strong>in</strong>e the number of d<strong>on</strong>ors lost because of the lack of ICU facilities and to identify<br />
soluti<strong>on</strong>s. This might <strong>in</strong>volve seek<strong>in</strong>g additi<strong>on</strong>al fund<strong>in</strong>g to <strong>in</strong>crease the number of <strong>in</strong>tensive care<br />
beds and/or <strong>in</strong>creased flexibility <strong>in</strong> terms of admissi<strong>on</strong> criteria or identify<strong>in</strong>g other suitable locati<strong>on</strong>s<br />
<strong>for</strong> assessment and management of those patients who are not be<strong>in</strong>g treated <strong>in</strong> ICU but wish to<br />
d<strong>on</strong>ate <strong>organ</strong>s after their death.<br />
Expand<strong>in</strong>g the type of <strong>organ</strong>s used from DCD d<strong>on</strong>ors<br />
The vast majority of <strong>organ</strong>s transplanted from d<strong>on</strong>ors follow<strong>in</strong>g circulatory death (DCD) are kidneys<br />
although some pancreases, livers and lungs have also been transplanted. 102 The possibility of heart<br />
d<strong>on</strong>ati<strong>on</strong> from DCD d<strong>on</strong>ors has also been raised follow<strong>in</strong>g three cases from the United States<br />
reported <strong>in</strong> 2008. The mean age of the d<strong>on</strong>ors was 3.7 days and the cause of death of all three<br />
was birth asphyxia. Decisi<strong>on</strong>s to withdraw life-prol<strong>on</strong>g<strong>in</strong>g treatment were made by the <strong>in</strong>tensive<br />
care team with the c<strong>on</strong>sent of the families. Treatment was withdrawn <strong>in</strong> the operat<strong>in</strong>g room <strong>where</strong><br />
cardiac functi<strong>on</strong> was m<strong>on</strong>itored. When cardiorespiratory functi<strong>on</strong> ceased, the first patient was<br />
observed <strong>for</strong> three m<strong>in</strong>utes be<strong>for</strong>e the <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> process was <strong>in</strong>itiated. On the advice of the<br />
ethics committee the observati<strong>on</strong> period was reduced to 75 sec<strong>on</strong>ds with the other two patients.<br />
The hearts were then removed and transplanted <strong>in</strong>to other babies. All three recipients survived.<br />
In the UK, the Academy of Medical Royal Colleges’ guidance <strong>on</strong> diagnosis of death (see secti<strong>on</strong> 3) 103<br />
states that the m<strong>in</strong>imum period of observati<strong>on</strong>, be<strong>for</strong>e death is declared, should be five m<strong>in</strong>utes<br />
follow<strong>in</strong>g cessati<strong>on</strong> of cardiorespiratory functi<strong>on</strong>. (This guidance applies <strong>on</strong>ly to those over 3<br />
m<strong>on</strong>ths of age, however; there are no UK guidel<strong>in</strong>es <strong>for</strong> diagnos<strong>in</strong>g death <strong>in</strong> ne<strong>on</strong>ates.) In 2009 a<br />
team from Papworth Hospital reported that they had recovered cardiac functi<strong>on</strong> <strong>in</strong> a human DCD<br />
d<strong>on</strong>or by us<strong>in</strong>g extracorporeal perfusi<strong>on</strong> 23 m<strong>in</strong>utes after cardiorespiratory arrest. 104 The paper’s<br />
authors suggested that this represents a potential source of <strong>in</strong>creased d<strong>on</strong>or supply <strong>for</strong> heart<br />
transplantati<strong>on</strong>.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 37
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
The fact that an <strong>in</strong>dividual is declared dead follow<strong>in</strong>g cessati<strong>on</strong> of cardio-respiratory functi<strong>on</strong> but<br />
the heart is subsequently restarted and transplanted <strong>in</strong>to another pers<strong>on</strong> is a difficult c<strong>on</strong>cept and<br />
<strong>on</strong>e that requires careful explanati<strong>on</strong>. Discuss<strong>in</strong>g this apparent c<strong>on</strong>tradicti<strong>on</strong>, the UK D<strong>on</strong>ati<strong>on</strong><br />
Ethics Committee’s c<strong>on</strong>sultati<strong>on</strong> report says:<br />
‘Some people feel uneasy about restor<strong>in</strong>g cardiac functi<strong>on</strong>, given that irreversible cessati<strong>on</strong><br />
of cardiac functi<strong>on</strong> is a key comp<strong>on</strong>ent of the diagnosis of death <strong>in</strong> the d<strong>on</strong>or. In<br />
physiological terms, cardiac functi<strong>on</strong> cannot be restored with<strong>in</strong> the orig<strong>in</strong>al biological<br />
system (ie the d<strong>on</strong>or) without artificial support. The diagnosis of death applies to that<br />
pers<strong>on</strong> as a whole, not to their <strong>in</strong>dividual <strong>organ</strong>s. There is there<strong>for</strong>e no ethical <strong>in</strong>c<strong>on</strong>sistency<br />
if the heart is re-started and transplanted to a recipient.’ 105<br />
Some <strong>in</strong>tensivists have expressed c<strong>on</strong>cerns about this practice however, questi<strong>on</strong><strong>in</strong>g whether<br />
frustrati<strong>on</strong> over the fall<strong>in</strong>g number of DBD d<strong>on</strong>ors has resulted <strong>in</strong> ‘<strong>in</strong>terventi<strong>on</strong>s that could<br />
jeopardise professi<strong>on</strong>al and public c<strong>on</strong>fidence <strong>in</strong> all <strong>for</strong>ms of d<strong>on</strong>ati<strong>on</strong>’ and argu<strong>in</strong>g that such<br />
practices are ‘at the very edge of acceptability.’ 106<br />
The <strong>BMA</strong>’s Medical Ethics Committee (MEC) c<strong>on</strong>sidered this issue <strong>in</strong> October 2010 and c<strong>on</strong>cluded<br />
that this was an acceptable and important area of research to pursue with a view to <strong>in</strong><strong>for</strong>m<strong>in</strong>g<br />
developments <strong>in</strong> cl<strong>in</strong>ical practice. DCD d<strong>on</strong>ors are patients <strong>in</strong> whom treatment has been withdrawn<br />
follow<strong>in</strong>g a cl<strong>in</strong>ical decisi<strong>on</strong> that attempts to prol<strong>on</strong>g life are no l<strong>on</strong>ger able to achieve any<br />
therapeutic goal and are not, there<strong>for</strong>e, <strong>in</strong> the patient’s best <strong>in</strong>terests. In pr<strong>in</strong>ciple, the MEC<br />
c<strong>on</strong>sidered there was no difference between transplant<strong>in</strong>g hearts from d<strong>on</strong>ors whose death had<br />
been diagnosed by bra<strong>in</strong> stem tests (DBD d<strong>on</strong>ors) and those whose death was diagnosed by<br />
cessati<strong>on</strong> of circulatory functi<strong>on</strong> (DCD d<strong>on</strong>ors). Nevertheless, the <strong>BMA</strong> believes that the pr<strong>in</strong>ciple<br />
of heart d<strong>on</strong>ati<strong>on</strong> follow<strong>in</strong>g circulatory death will need very careful explanati<strong>on</strong>, both to families<br />
and, more generally, to the public. A careful explanati<strong>on</strong> of the way <strong>in</strong> which death is diagnosed<br />
will be needed and an explanati<strong>on</strong> that a heart that has stopped beat<strong>in</strong>g can be restarted after<br />
the pers<strong>on</strong> has died and used <strong>for</strong> transplantati<strong>on</strong>. It might also be helpful to refer to fact that<br />
the first heart transplant, under Christian Barnard, was from a DCD d<strong>on</strong>or.<br />
More research is needed be<strong>for</strong>e this can be <strong>in</strong>troduced <strong>in</strong>to cl<strong>in</strong>ical practice but it represents a<br />
possibility of both <strong>in</strong>creas<strong>in</strong>g the number of hearts available <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> and also of facilitat<strong>in</strong>g<br />
the wishes of more people who wish to be d<strong>on</strong>ors, although the numbers are likely to be small<br />
<strong>for</strong> the <strong>for</strong>eseeable future.<br />
Expand<strong>in</strong>g liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong><br />
As described <strong>in</strong> secti<strong>on</strong> 2, the number of liv<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ors has <strong>in</strong>creased dramatically over the<br />
last decade and the number of liv<strong>in</strong>g d<strong>on</strong>ors is now higher than the number of deceased d<strong>on</strong>ors.<br />
The vast majority of liv<strong>in</strong>g d<strong>on</strong>ors d<strong>on</strong>ate a kidney (1,020) but <strong>in</strong> 2010/11, 25 liv<strong>in</strong>g d<strong>on</strong>ors (2.4%)<br />
d<strong>on</strong>ated part of their liver. 107 It is also possible <strong>for</strong> liv<strong>in</strong>g d<strong>on</strong>ors to d<strong>on</strong>ate lung lobes to those with<br />
end-stage lung disease although this is not current UK practice.<br />
38<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
With any <strong>for</strong>m of liv<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> the d<strong>on</strong>or undergoes major surgery and is exposed to risk<br />
of complicati<strong>on</strong>s <strong>for</strong> the benefit of another pers<strong>on</strong>. It is now widely accepted that the risk to which<br />
kidney d<strong>on</strong>ors are exposed is with<strong>in</strong> acceptable levels. With liver and lung d<strong>on</strong>ati<strong>on</strong>, however,<br />
the risks are significantly higher and this is likely to be a key factor <strong>in</strong> the low uptake of liv<strong>in</strong>g<br />
d<strong>on</strong>ati<strong>on</strong>. Nevertheless, NICE has reviewed the evidence of liv<strong>in</strong>g liver 108 and lung 109 d<strong>on</strong>ati<strong>on</strong><br />
and has c<strong>on</strong>cluded, <strong>in</strong> both cases, that the evidence <strong>on</strong> efficacy and the safety profile ‘appears<br />
adequate to support the use of this procedure’ <strong>for</strong> suitable recipients. Whilst there may be scope<br />
<strong>for</strong> more liv<strong>in</strong>g liver and lung d<strong>on</strong>ati<strong>on</strong>s, because of the level of risk associated with d<strong>on</strong>ati<strong>on</strong> this<br />
is not an ideal soluti<strong>on</strong> to the <strong>organ</strong> shortage problem. For some people await<strong>in</strong>g a transplant,<br />
however, who have a friend or relative will<strong>in</strong>g to d<strong>on</strong>ate, this may be an opti<strong>on</strong>. As with all liv<strong>in</strong>g<br />
d<strong>on</strong>ati<strong>on</strong>, those <strong>in</strong>dividuals c<strong>on</strong>sider<strong>in</strong>g liv<strong>in</strong>g liver or lung d<strong>on</strong>ati<strong>on</strong> need to be aware of the risks<br />
and complicati<strong>on</strong>s and must be act<strong>in</strong>g voluntarily and free from pressure. All cases of liv<strong>in</strong>g<br />
d<strong>on</strong>ati<strong>on</strong> need to be approved, <strong>in</strong> advance, by the Human Tissue Authority follow<strong>in</strong>g review by<br />
an <strong>in</strong>dependent assessor.<br />
Although already established, there is also c<strong>on</strong>siderable scope to extend liv<strong>in</strong>g kidney d<strong>on</strong>ati<strong>on</strong><br />
through expansi<strong>on</strong> of the Nati<strong>on</strong>al Liv<strong>in</strong>g D<strong>on</strong>or Kidney Shar<strong>in</strong>g Schemes. This <strong>in</strong>cludes<br />
paired/pooled d<strong>on</strong>ati<strong>on</strong>, n<strong>on</strong>-directed altruistic d<strong>on</strong>ati<strong>on</strong> and altruistic d<strong>on</strong>or cha<strong>in</strong>s. Altruistic<br />
d<strong>on</strong>or cha<strong>in</strong>s are <strong>where</strong> a n<strong>on</strong>-directed altruistic d<strong>on</strong>or opts to d<strong>on</strong>ate <strong>in</strong>to the paired/pooled<br />
scheme <strong>in</strong>stead of directly <strong>in</strong>to the nati<strong>on</strong>al d<strong>on</strong>or pool. The kidney is then matched with some<strong>on</strong>e<br />
<strong>in</strong> the paired/pooled scheme and the d<strong>on</strong>or registered with that recipient then d<strong>on</strong>ates to another<br />
recipient and so <strong>on</strong>.<br />
Many people are not aware that they could d<strong>on</strong>ate a kidney to a stranger and so more work<br />
rais<strong>in</strong>g awareness about this opti<strong>on</strong> could help to extend the scheme. A YouGov survey <strong>in</strong><br />
November 2011 found that 32% of people surveyed did not know that it was possible to d<strong>on</strong>ate<br />
a kidney altruistically to a stranger but that 8% would c<strong>on</strong>sider it. 110 Clearly not all of these would<br />
go <strong>on</strong> to d<strong>on</strong>ate but even a small number could have a significant impact. The <strong>BMA</strong> supports<br />
moves to raise awareness about altruistic n<strong>on</strong>-directed d<strong>on</strong>ati<strong>on</strong> but recognises that care is<br />
needed to ensure that <strong>in</strong>dividuals do not feel pressured to d<strong>on</strong>ate.<br />
Use of ‘higher risk’ d<strong>on</strong>or <strong>organ</strong>s<br />
No transplant is without risk but there are a number of factors that affect the level of this risk. 111<br />
These <strong>in</strong>clude factors that might affect the graft functi<strong>on</strong>, such as the age of the d<strong>on</strong>or, cause of<br />
death, type of d<strong>on</strong>or (DCD or DBD), body mass <strong>in</strong>dex and length of stay <strong>in</strong> ICU prior to d<strong>on</strong>ati<strong>on</strong>.<br />
There are also some factors that <strong>in</strong>crease the risk of a transmissible disease be<strong>in</strong>g passed <strong>on</strong> to the<br />
recipient such as previous use of <strong>in</strong>travenous drugs, high risk sexual behaviour or previous history<br />
of malignancy. These risks can be reduced by limit<strong>in</strong>g the criteria <strong>for</strong> d<strong>on</strong>or acceptance (by age,<br />
body mass <strong>in</strong>dex, exist<strong>in</strong>g medical c<strong>on</strong>diti<strong>on</strong>s etc) but every restricti<strong>on</strong> applied reduces the number<br />
of <strong>organ</strong>s available <strong>for</strong> transplantati<strong>on</strong>. C<strong>on</strong>versely extend<strong>in</strong>g the acceptance criteria (by allow<strong>in</strong>g<br />
older d<strong>on</strong>ors or those with exist<strong>in</strong>g malignancy <strong>for</strong> example) would <strong>in</strong>crease the pool of potential<br />
d<strong>on</strong>ors but also <strong>in</strong>crease the level of risk to which some recipients would be exposed. Introduc<strong>in</strong>g<br />
wider acceptance criteria would also <strong>in</strong>crease the likelihood of d<strong>on</strong>ors go<strong>in</strong>g through the d<strong>on</strong>ati<strong>on</strong><br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 39
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
procedure and n<strong>on</strong>e of the <strong>organ</strong>s be<strong>in</strong>g suitable <strong>for</strong> transplantati<strong>on</strong>. An appropriate balance<br />
there<strong>for</strong>e needs to be reached between risks and benefits when sett<strong>in</strong>g exclusi<strong>on</strong> criteria <strong>for</strong><br />
d<strong>on</strong>ati<strong>on</strong>. NHS Blood and Transplant has developed a list of absolute c<strong>on</strong>tra<strong>in</strong>dicati<strong>on</strong>s <strong>for</strong> d<strong>on</strong>ati<strong>on</strong><br />
and has advised that all potential d<strong>on</strong>ors who have n<strong>on</strong>e of these c<strong>on</strong>tra-<strong>in</strong>dicati<strong>on</strong>s should be<br />
referred even if the likelihood of any <strong>organ</strong>s be<strong>in</strong>g accepted appears low. 112 The <strong>BMA</strong> supports this<br />
approach but believes that <strong>where</strong> there is a reas<strong>on</strong>able possibility that n<strong>on</strong>e of the <strong>organ</strong>s will be<br />
suitable <strong>for</strong> transplantati<strong>on</strong>, this should be discussed <strong>in</strong> advance with the d<strong>on</strong>or family.<br />
NHS BT has also, jo<strong>in</strong>tly with the British Transplantati<strong>on</strong> Society, provided guidance <strong>on</strong> the<br />
<strong>in</strong><strong>for</strong>mati<strong>on</strong> that should be provided to those who need a transplant both be<strong>for</strong>e they go <strong>on</strong> the<br />
wait<strong>in</strong>g list and <strong>on</strong>ce an <strong>organ</strong> is offered. It makes clear, <strong>in</strong> relati<strong>on</strong> to the offer of an <strong>organ</strong>, that<br />
‘<strong>where</strong> the risks exceed those that are accepted with<strong>in</strong> current guidel<strong>in</strong>es (<strong>for</strong> example <strong>where</strong> the<br />
d<strong>on</strong>or has a primary <strong>in</strong>tra-cranial cancer or a recent history of malignancy such that there is a<br />
possibility of tumour transmissi<strong>on</strong>), this should be discussed with the potential recipient when<br />
the <strong>organ</strong> is offered.’ 113<br />
Elective ventilati<strong>on</strong><br />
Once a patient has been diagnosed as dead us<strong>in</strong>g bra<strong>in</strong> stem tests, artificial ventilati<strong>on</strong> is usually<br />
c<strong>on</strong>t<strong>in</strong>ued <strong>for</strong> a period of time to allow the family time to say goodbye or, if <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> has<br />
been authorised, <strong>for</strong> arrangements to be made <strong>for</strong> the <strong>organ</strong>s to be retrieved. Elective ventilati<strong>on</strong> is<br />
different <strong>in</strong> that it <strong>in</strong>volves start<strong>in</strong>g ventilati<strong>on</strong>, <strong>on</strong>ce it is recognised that the patient is close to<br />
death, with the specific <strong>in</strong>tenti<strong>on</strong> of facilitat<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. This system was <strong>in</strong>troduced, with<br />
strict c<strong>on</strong>trols, <strong>in</strong> Exeter <strong>in</strong> 1988 and led to a 50% <strong>in</strong>crease <strong>in</strong> the number of <strong>organ</strong>s suitable <strong>for</strong><br />
transplantati<strong>on</strong>. It was stopped abruptly <strong>in</strong> 1994, however, when the Department of Health<br />
advised that the practice was unlawful. 114<br />
The law requires that, when patients lack the capacity to c<strong>on</strong>sent, procedures or <strong>in</strong>terventi<strong>on</strong>s<br />
must be <strong>in</strong> their best <strong>in</strong>terests. The use of elective ventilati<strong>on</strong> is not <strong>in</strong>tended to be <strong>for</strong> the cl<strong>in</strong>ical<br />
benefit of the <strong>in</strong>dividual but to facilitate d<strong>on</strong>ati<strong>on</strong>. The Mental Capacity Act 2005, however, takes<br />
a broad approach to ‘best <strong>in</strong>terests’ (and a similar broad approach to ‘benefit’ is likely under the<br />
Adults with Incapacity (Scotland) Act 2000) and there has recently been a <strong>for</strong>mal recogniti<strong>on</strong> that<br />
tak<strong>in</strong>g some steps be<strong>for</strong>e death to facilitate d<strong>on</strong>ati<strong>on</strong> could be <strong>in</strong> an <strong>in</strong>dividual’s best <strong>in</strong>terests (see<br />
secti<strong>on</strong> 4). The <strong>BMA</strong> has l<strong>on</strong>g argued that <strong>where</strong> an <strong>in</strong>dividual had expressed a wish to d<strong>on</strong>ate<br />
<strong>organ</strong>s after death, some steps to facilitate that wish may be seen as <strong>in</strong> that pers<strong>on</strong>’s best <strong>in</strong>terests<br />
or benefit (or at least not c<strong>on</strong>trary to his or her <strong>in</strong>terests). Individuals who are sufficiently <strong>in</strong><strong>for</strong>med<br />
may also wish to give specific, advance c<strong>on</strong>sent, to permit elective ventilati<strong>on</strong> to take place. The<br />
UK D<strong>on</strong>ati<strong>on</strong> Ethics Committee has called <strong>for</strong> further debate <strong>on</strong> this issue, to more clearly def<strong>in</strong>e<br />
the appropriate balance between benefits and harms and the type of <strong>in</strong>terventi<strong>on</strong>s that could<br />
reas<strong>on</strong>ably be undertaken. 115 The <strong>BMA</strong> would also welcome further clarificati<strong>on</strong> <strong>on</strong> this issue.<br />
From an ethical perspective <strong>on</strong>e of the major c<strong>on</strong>cerns with elective ventilati<strong>on</strong> is the level of the<br />
risk to which the <strong>in</strong>capacitated adult may be exposed. Fears have been expressed that, <strong>in</strong> theory at<br />
least, elective ventilati<strong>on</strong> could <strong>in</strong>duce a persistent vegetative state (pvs). Although the chance of<br />
harm occurr<strong>in</strong>g is c<strong>on</strong>sidered to be very low, <strong>in</strong>duc<strong>in</strong>g pvs would be a very significant harm and,<br />
40<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
if elective ventilati<strong>on</strong> were to be permitted, very careful safeguards would be needed to m<strong>in</strong>imise<br />
this risk. This might <strong>in</strong>clude, <strong>for</strong> example, restrict<strong>in</strong>g elective ventilati<strong>on</strong> to those patients dy<strong>in</strong>g of<br />
sp<strong>on</strong>taneous <strong>in</strong>tracranial haemorrhage (s<strong>in</strong>ce these patients rarely, if ever, develop pvs) 116 and<br />
stat<strong>in</strong>g that artificial ventilati<strong>on</strong> must not be started until natural respiratory arrest has occurred. 117<br />
There are also practical difficulties associated with the lack of ICU beds and compet<strong>in</strong>g demands<br />
<strong>for</strong> limited resources. In the <strong>BMA</strong>’s view, priority would always need to be given to the use of<br />
<strong>in</strong>tensive care facilities <strong>for</strong> those who have a chance of recovery rather than <strong>for</strong> those who are<br />
be<strong>in</strong>g ventilated to facilitate d<strong>on</strong>ati<strong>on</strong>.<br />
Elective ventilati<strong>on</strong> is not an easy opti<strong>on</strong> but it has been shown to <strong>in</strong>crease d<strong>on</strong>ati<strong>on</strong> rates, and to<br />
facilitate the wishes of a group of patients who want to d<strong>on</strong>ate and would otherwise be unable to<br />
do so. The <strong>BMA</strong> is not call<strong>in</strong>g <strong>for</strong> the law to be changed to permit elective ventilati<strong>on</strong> but believes<br />
this may be an issue that would benefit from debate both to assess the cl<strong>in</strong>ical, legal and ethical<br />
issues raised and to assess public op<strong>in</strong>i<strong>on</strong> about its use.<br />
Ensur<strong>in</strong>g <strong>in</strong>dividuals’ wishes are known<br />
The potential d<strong>on</strong>or audit (see secti<strong>on</strong> 4) dem<strong>on</strong>strates that <strong>where</strong> an <strong>in</strong>dividual’s wishes are<br />
known the relatives, under the current opt-<strong>in</strong> system, are less likely to refuse c<strong>on</strong>sent to d<strong>on</strong>ati<strong>on</strong>.<br />
With DBD d<strong>on</strong>ors <strong>in</strong> 2010/11, the overall refusal rate was 35% but this dropped to 6% <strong>where</strong> the<br />
<strong>in</strong>dividual’s wishes were known (<strong>where</strong> the <strong>in</strong>dividual’s views were not known the refusal rate was<br />
50%). With d<strong>on</strong>ors follow<strong>in</strong>g circulatory death, the overall relative refusal rate was 49% but this<br />
dropped to 20% <strong>where</strong> it was known that the <strong>in</strong>dividual wanted to d<strong>on</strong>ate (the refusal rate was<br />
61% when the <strong>in</strong>dividual’s views were not known). 118 While there are still cases <strong>where</strong> the<br />
<strong>in</strong>dividual’s known wishes are overridden by relatives, the knowledge that relatives are less likely<br />
to refuse <strong>in</strong> these circumstances provides impetus to f<strong>in</strong>d ways of encourag<strong>in</strong>g people to th<strong>in</strong>k<br />
about d<strong>on</strong>ati<strong>on</strong> and make their views known.<br />
More publicity about the NHS Organ D<strong>on</strong>or Register<br />
The clearest way to record a wish to d<strong>on</strong>ate is to sign up to the NHS Organ D<strong>on</strong>or Register (ODR).<br />
The register is available to authorised <strong>in</strong>dividuals 24 hours a day, 365 days a year which means<br />
that when the family are approached they can be <strong>in</strong><strong>for</strong>med that their relative wanted to d<strong>on</strong>ate<br />
<strong>organ</strong>s after death. Over the years a lot of ef<strong>for</strong>t has g<strong>on</strong>e <strong>in</strong>to promot<strong>in</strong>g the ODR with high<br />
profile campaigns <strong>in</strong>volv<strong>in</strong>g celebrities and emphasis<strong>in</strong>g the real difference transplants make to<br />
people’s lives. There are currently 18.4 milli<strong>on</strong> people registered, represent<strong>in</strong>g 29% of the UK<br />
populati<strong>on</strong>. Whilst this is an impressive number, it does not compare with the 70-90% who say<br />
they support d<strong>on</strong>ati<strong>on</strong>.<br />
NHS BT has undertaken a number of campaigns, <strong>in</strong>clud<strong>in</strong>g <strong>in</strong> 2009 <strong>on</strong>e aimed specifically at the<br />
group of people who would be will<strong>in</strong>g to receive an <strong>organ</strong> if they needed <strong>on</strong>e, but have not<br />
thought about sign<strong>in</strong>g up to the register – ‘if you believe <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>, prove it’. Although<br />
such campaigns are pr<strong>in</strong>cipally aimed at encourag<strong>in</strong>g people to sign up to the register, another<br />
benefit is encourag<strong>in</strong>g people to th<strong>in</strong>k, and talk about, their wishes regard<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>.<br />
Such promoti<strong>on</strong>al campaigns have, however, been significantly restricted <strong>in</strong> England over recent<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 41
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
years <strong>where</strong>as <strong>in</strong> Scotland, the Government has c<strong>on</strong>t<strong>in</strong>ued to fund high-impact nati<strong>on</strong>al advertis<strong>in</strong>g<br />
and publicity campaigns. Indeed there is a statutory duty <strong>on</strong> Scottish M<strong>in</strong>isters, under the 2006<br />
Act, to promote <strong>in</strong><strong>for</strong>mati<strong>on</strong> and awareness about <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Scotland currently has the<br />
highest c<strong>on</strong>sent rate <strong>in</strong> the UK at 86%. 119<br />
A number of campaigns have been targeted at black and ethnic m<strong>in</strong>orities <strong>where</strong> the shortage of<br />
d<strong>on</strong>ors is particularly acute. Around 16% of people <strong>on</strong> the wait<strong>in</strong>g list <strong>for</strong> a d<strong>on</strong>or <strong>organ</strong> are from<br />
Asian communities but these communities make up <strong>on</strong>ly 1.4% of people <strong>on</strong> the Organ D<strong>on</strong>or<br />
Register. 120 Similarly, 8% of people <strong>on</strong> the wait<strong>in</strong>g list are from black communities, but these make<br />
up <strong>on</strong>ly 0.4% of those <strong>on</strong> the Register. 121 Research has found high levels of support <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> am<strong>on</strong>gst African-Caribbeans and South Asians but a lack of awareness of the specific<br />
need <strong>for</strong> <strong>organ</strong>s with<strong>in</strong> their community. 122 NHS BT has tried to address this problem by<br />
emphasis<strong>in</strong>g the way <strong>in</strong> which people with<strong>in</strong> their own community are suffer<strong>in</strong>g because of a lack<br />
of suitably matched d<strong>on</strong>ors. It also provides a series of leaflets <strong>on</strong> different faiths’ perspectives <strong>on</strong><br />
<strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> to correct some of the myths and misunderstand<strong>in</strong>gs about religious perspectives<br />
<strong>on</strong> d<strong>on</strong>ati<strong>on</strong>. 123 These targeted campaigns appear to be work<strong>in</strong>g 124 but more work is required<br />
to determ<strong>in</strong>e how to produce and dissem<strong>in</strong>ate this <strong>in</strong><strong>for</strong>mati<strong>on</strong> to maximum effect and also to<br />
identify barriers that are ‘cultural’ rather than ‘religious’.<br />
The <strong>BMA</strong> has, <strong>for</strong> many years, supported an opt-out system with safeguards <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong><br />
and is best known <strong>for</strong> its work <strong>in</strong> this area. It has also undertaken, or supported, many campaigns<br />
aimed at rais<strong>in</strong>g awareness of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> generally and encourag<strong>in</strong>g people to sign up to the<br />
Organ D<strong>on</strong>or Register. It ran campaigns encourag<strong>in</strong>g people to ‘have a heart <strong>on</strong> Valent<strong>in</strong>e’s Day’<br />
and to ‘sign <strong>on</strong>e more card this Christmas’ as well as us<strong>in</strong>g various mechanisms to encourage its<br />
own members to lead by example and make sure their own wishes about d<strong>on</strong>ati<strong>on</strong> were known.<br />
Encourag<strong>in</strong>g people to sign up to the ODR is an important comp<strong>on</strong>ent of a broader strategy to<br />
improve d<strong>on</strong>ati<strong>on</strong> rates but is not the answer to the <strong>organ</strong> shortage. There is not a direct l<strong>in</strong>k<br />
between the number of people <strong>on</strong> the ODR and the number of d<strong>on</strong>ors. One reas<strong>on</strong> <strong>for</strong> this is that<br />
the people who register are not wholly representative of the people who die and go <strong>on</strong> to d<strong>on</strong>ate.<br />
It will never be possible to get every<strong>on</strong>e who is will<strong>in</strong>g to d<strong>on</strong>ate <strong>organ</strong>s to sign up to the ODR<br />
but encourag<strong>in</strong>g as many people as possible to do so is important. It needs to be acknowledged,<br />
however, that as publicity <strong>for</strong>, and awareness of, the register <strong>in</strong>creases – and with no <strong>for</strong>mal<br />
mechanism to record an objecti<strong>on</strong> to d<strong>on</strong>ati<strong>on</strong> – there is a possibility that the relatives of those<br />
who have not signed up might <strong>in</strong>terpret that fact as a sign that the <strong>in</strong>dividual did not wish to<br />
d<strong>on</strong>ate. This could have a negative impact <strong>on</strong> attempts to reduce the relative refusal rate.<br />
‘Prompted choice’<br />
In December 2010 the Cab<strong>in</strong>et Office published a paper, Apply<strong>in</strong>g behavioural <strong>in</strong>sight to health,<br />
identify<strong>in</strong>g areas <strong>where</strong> what has been termed ‘prompted choice’ or ‘nudge theory’ could help<br />
to address significant health issues with<strong>in</strong> the populati<strong>on</strong>. The idea is to understand people’s<br />
behaviour and develop ways to ‘prompt people to make choices that are <strong>in</strong> l<strong>in</strong>e with their<br />
underly<strong>in</strong>g motivati<strong>on</strong>s’. 125 One of the examples used <strong>in</strong> the document was <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>.<br />
42<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
From 1 August 2011 people who wish to apply <strong>for</strong> a new, or renewed, driv<strong>in</strong>g licence <strong>on</strong>l<strong>in</strong>e<br />
have been required to answer a questi<strong>on</strong> about <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. 126 Under the previous scheme,<br />
through which more than 8.5 milli<strong>on</strong> people signed up, a questi<strong>on</strong> about sign<strong>in</strong>g up to the ODR<br />
was <strong>in</strong>cluded but it was possible to skip over it. Under the new scheme, the questi<strong>on</strong> must be<br />
answered be<strong>for</strong>e the applicant can move <strong>on</strong>. The opti<strong>on</strong>s given are:<br />
• Yes, I would like to register<br />
• I do not wish to answer this questi<strong>on</strong> now<br />
• I am already registered <strong>on</strong> the NHS Organ D<strong>on</strong>or Register.<br />
The Nuffield Council <strong>on</strong> Bioethics, whilst support<strong>in</strong>g the use of such a pilot scheme to assess the<br />
effectiveness of prompted choice, was c<strong>on</strong>cerned that applicants were given no opportunity to<br />
object to d<strong>on</strong>ati<strong>on</strong>. Its report argued that failure to give the opti<strong>on</strong> of express<strong>in</strong>g objecti<strong>on</strong><br />
‘significantly underm<strong>in</strong>es commitment to follow<strong>in</strong>g the wishes of the deceased and even, arguably,<br />
fails to comply with the spirit of current legislati<strong>on</strong> with its central focus <strong>on</strong> c<strong>on</strong>sent’. 127 Clearly, if<br />
the opti<strong>on</strong> to say ‘no’ is to be <strong>in</strong>cluded, there must be a clear and robust mechanism <strong>in</strong> place <strong>for</strong><br />
those objecti<strong>on</strong>s to be registered and acted up<strong>on</strong>. This would <strong>in</strong>volve either modificati<strong>on</strong> of the<br />
ODR to <strong>in</strong>clude the opti<strong>on</strong> to opt out of d<strong>on</strong>ati<strong>on</strong> or a new <strong>organ</strong> d<strong>on</strong>or register designed<br />
specifically to allow people to either opt <strong>in</strong>to or out of d<strong>on</strong>ati<strong>on</strong>.<br />
The use of driv<strong>in</strong>g licence applicati<strong>on</strong>s as a <strong>for</strong>m of prompted choice is not new. In the late 1990s,<br />
<strong>for</strong> example, licensed drivers <strong>in</strong> Texas and Virg<strong>in</strong>ia were required to state their views about d<strong>on</strong>ati<strong>on</strong><br />
be<strong>for</strong>e obta<strong>in</strong><strong>in</strong>g a licence. In Texas, <strong>where</strong> the choice was between d<strong>on</strong>ati<strong>on</strong> or n<strong>on</strong>-d<strong>on</strong>ati<strong>on</strong>, the<br />
system was aband<strong>on</strong>ed after 80% registered as n<strong>on</strong>-d<strong>on</strong>ors lead<strong>in</strong>g to an overall reducti<strong>on</strong> <strong>in</strong> the<br />
number of d<strong>on</strong>ors. 128 In Virg<strong>in</strong>ia, the opti<strong>on</strong>s were d<strong>on</strong>or, n<strong>on</strong>-d<strong>on</strong>or or undecided. In the first six<br />
m<strong>on</strong>ths of the programme, approximately <strong>on</strong>e milli<strong>on</strong> Virg<strong>in</strong>ia drivers were asked to declare a<br />
preference. Of these, 31% registered as d<strong>on</strong>ors, 45% as n<strong>on</strong>-d<strong>on</strong>ors and 24% were undecided. 129<br />
In spite of the negative resp<strong>on</strong>se to its first attempt, Texas <strong>in</strong>troduced a new law <strong>in</strong> January 2010<br />
requir<strong>in</strong>g clerks <strong>in</strong> the Department of Public Safety to ask all driver’s licence and ID card applicants<br />
whether they would like to register as <strong>organ</strong> d<strong>on</strong>ors. After six m<strong>on</strong>ths it was reported that nearly<br />
70,000 d<strong>on</strong>ors a m<strong>on</strong>th had jo<strong>in</strong>ed the register. 130 There have been similar news reports of a<br />
positive effect from a similar <strong>in</strong>itiative <strong>in</strong> Ill<strong>in</strong>ois. 131 In additi<strong>on</strong>, the New Jersey Hero Act 2008 states<br />
that, from 2013, <strong>in</strong>dividuals who apply <strong>for</strong>, or renew, their driv<strong>in</strong>g licence or ID card will be<br />
required to c<strong>on</strong>sider whether they wish to become a d<strong>on</strong>or. Two opti<strong>on</strong>s are offered: to sign up<br />
as an <strong>organ</strong> d<strong>on</strong>or or to ‘review <strong>in</strong><strong>for</strong>mati<strong>on</strong> about the life-sav<strong>in</strong>g potential of <strong>organ</strong> and tissue<br />
d<strong>on</strong>ati<strong>on</strong>, and the c<strong>on</strong>sequences when an <strong>in</strong>dividual does not make a decisi<strong>on</strong> to become an<br />
<strong>organ</strong> d<strong>on</strong>or and does not register or otherwise record a designated decisi<strong>on</strong>-maker.’ 132<br />
We await with <strong>in</strong>terest the outcome of the UK experience of this <strong>for</strong>m of prompted choice.<br />
If successful, this model could be repeated with other official documents such as apply<strong>in</strong>g <strong>for</strong><br />
a passport, complet<strong>in</strong>g tax returns, register<strong>in</strong>g with a GP or, subject to legal re<strong>for</strong>m, electoral<br />
registrati<strong>on</strong>.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 43
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
Mandated choice<br />
Mandated choice is a system <strong>where</strong>by all adults are required, by law, to decide <strong>in</strong> advance whether<br />
they wish to d<strong>on</strong>ate their <strong>organ</strong>s <strong>for</strong> transplantati<strong>on</strong> after death, with penalties imposed <strong>on</strong> those<br />
who refuse to state a view. Prompted choice (see above) is a modificati<strong>on</strong> of mandated choice and<br />
the boundaries between the two can sometimes be blurred. Mandated choice and a soft opt-out<br />
system with safeguards are the two alternatives to the status quo that are most frequently<br />
discussed and supported. There are a number of variati<strong>on</strong>s <strong>on</strong> the theme. Traditi<strong>on</strong>ally, it was<br />
suggested that every<strong>on</strong>e would be asked about d<strong>on</strong>ati<strong>on</strong> and must decide ‘yes’ or ‘no’ or face<br />
some penalty (whether a f<strong>in</strong>e, <strong>in</strong>ability to obta<strong>in</strong> a driv<strong>in</strong>g licence, rejecti<strong>on</strong> of tax returns or<br />
<strong>in</strong>eligibility <strong>for</strong> <strong>in</strong>clusi<strong>on</strong> <strong>on</strong> the electoral register and there<strong>for</strong>e <strong>in</strong>eligibility to vote). A more recent<br />
proposal is that <strong>in</strong>dividuals should be given the choice of three opti<strong>on</strong>s – ‘yes’, ‘no’ or ‘I want my<br />
family to decide’. 133<br />
The pr<strong>in</strong>ciple beh<strong>in</strong>d mandated choice is to <strong>in</strong>crease d<strong>on</strong>ati<strong>on</strong> rates whilst enhanc<strong>in</strong>g <strong>in</strong>dividual<br />
aut<strong>on</strong>omy by allow<strong>in</strong>g <strong>in</strong>dividuals themselves to make the decisi<strong>on</strong> and ensur<strong>in</strong>g that all <strong>in</strong>dividuals’<br />
wishes are known and respected. It aims to overcome the problem of apathy <strong>where</strong>by a large<br />
majority of <strong>in</strong>dividuals express will<strong>in</strong>gness to d<strong>on</strong>ate when asked, but do not make their wishes<br />
known by sign<strong>in</strong>g up to the Organ D<strong>on</strong>or Register or <strong>in</strong><strong>for</strong>m<strong>in</strong>g their relatives. Mak<strong>in</strong>g it compulsory<br />
<strong>for</strong> <strong>in</strong>dividuals to decide and record their wishes also gets over the problem of people not wish<strong>in</strong>g<br />
to th<strong>in</strong>k about their own mortality.<br />
A further aim of mandated choice is to transfer c<strong>on</strong>trol from the family to the <strong>in</strong>dividual. 134 Under<br />
this system, the views of the <strong>in</strong>dividual are usually b<strong>in</strong>d<strong>in</strong>g and so the relatives would have no<br />
right of veto 135 (unless the <strong>in</strong>dividual specifically asked them to choose), thus also overcom<strong>in</strong>g the<br />
high relative refusal rate, which currently stands at 35% (and 50% <strong>for</strong> those whose views are not<br />
known). The <strong>in</strong>tenti<strong>on</strong> of most advocates is that this would apply <strong>in</strong> practice, as well as <strong>in</strong> law, as<br />
opposed to the current system <strong>where</strong>by the relatives have no legal right of veto but, <strong>in</strong> practice,<br />
<strong>organ</strong>s are not removed aga<strong>in</strong>st the str<strong>on</strong>g and susta<strong>in</strong>ed wishes of the family (although some<br />
have suggested that the discreti<strong>on</strong> <strong>for</strong> allow<strong>in</strong>g family refusals <strong>in</strong> some cases should rema<strong>in</strong> 136 ).<br />
Although the b<strong>in</strong>d<strong>in</strong>g nature of the <strong>in</strong>dividual’s stated wish to d<strong>on</strong>ate is usually a key strand of<br />
mandated choice, it is difficult to see how this would work <strong>in</strong> practice, s<strong>in</strong>ce it is highly unlikely<br />
that most surge<strong>on</strong>s would be will<strong>in</strong>g to remove <strong>organ</strong>s <strong>in</strong> the face of str<strong>on</strong>g family objecti<strong>on</strong>s. The<br />
<strong>BMA</strong> believes that while attempts should be made to persuade the family to follow the <strong>in</strong>dividual’s<br />
previous wishes, the retrieval team should have the discreti<strong>on</strong> not to retrieve <strong>organ</strong>s <strong>in</strong> this situati<strong>on</strong><br />
(see secti<strong>on</strong> 3). When assess<strong>in</strong>g mandated choice, there<strong>for</strong>e, it must be recognised that this part of<br />
the system may be difficult to uphold <strong>in</strong> practice.<br />
Evidence of effectiveness<br />
There is very limited evidence available to assess the effectiveness of mandated choice <strong>in</strong> <strong>in</strong>creas<strong>in</strong>g<br />
d<strong>on</strong>ati<strong>on</strong> rates s<strong>in</strong>ce no country has adopted this model. ‘Prompted choice’ can be seen as a <strong>for</strong>m<br />
of mandated choice, although applied to <strong>on</strong>ly small secti<strong>on</strong>s of the populati<strong>on</strong> and without<br />
penalties. The first attempt at prompted choice <strong>in</strong> Texas (see above) could <strong>in</strong>dicate that when<br />
people are <strong>for</strong>ced to make a decisi<strong>on</strong> – ‘yes’ or ‘no’, they are more likely to take a negative<br />
44<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
approach. It is unclear, however, whether the same model was used <strong>in</strong> the later, more successful,<br />
attempt and so it is difficult to draw any firm c<strong>on</strong>clusi<strong>on</strong>s from this. More evidence may become<br />
available when data from the UK’s DVLA system are published.<br />
By <strong>in</strong>clud<strong>in</strong>g an opti<strong>on</strong> not to decide, or to leave the decisi<strong>on</strong> to the family, as has been suggested,<br />
there is less risk that people who are unhappy about be<strong>in</strong>g <strong>for</strong>ced to choose will say ‘no’, but if<br />
large numbers take this opti<strong>on</strong>, the situati<strong>on</strong> may be no better than currently. There is even a<br />
chance that the refusal rate could <strong>in</strong>crease if families <strong>in</strong>fer from their relatives’ decisi<strong>on</strong> not to<br />
sign up to the register, when given the opti<strong>on</strong>, that they were not committed to d<strong>on</strong>ati<strong>on</strong>.<br />
Ethical c<strong>on</strong>siderati<strong>on</strong>s<br />
There are clear benefits of know<strong>in</strong>g every <strong>in</strong>dividual’s wish about <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> rather than<br />
seek<strong>in</strong>g views from relatives, at a time of great distress and anxiety, or mak<strong>in</strong>g assumpti<strong>on</strong>s about<br />
what a pers<strong>on</strong> is likely to have wanted. In order to achieve this situati<strong>on</strong>, however, an element of<br />
coerci<strong>on</strong> is required and compell<strong>in</strong>g people to make choices can be seen to underm<strong>in</strong>e, rather than<br />
enhance, their aut<strong>on</strong>omy. There are precedents <strong>for</strong> requir<strong>in</strong>g people to make a choice, <strong>where</strong> it<br />
is felt there is a resp<strong>on</strong>sibility to do so, such as mandatory vot<strong>in</strong>g <strong>in</strong> Australia. In the same way,<br />
Chouhan and Draper argue ‘it may be seriously irresp<strong>on</strong>sible of people not to decide about <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> when the lives, and quality of life, of so many people depend up<strong>on</strong> this decisi<strong>on</strong>.’ 137<br />
Furthermore, they argue, <strong>in</strong>terfer<strong>in</strong>g with <strong>in</strong>dividual liberty, by mandat<strong>in</strong>g choice, can be justified<br />
by the benefit that is likely to accrue from <strong>in</strong>creas<strong>in</strong>g the number of d<strong>on</strong>ors available and thus the<br />
number of transplants that can be undertaken. There is very little ef<strong>for</strong>t, harm or <strong>in</strong>c<strong>on</strong>venience<br />
to the <strong>in</strong>dividual, they argue, but c<strong>on</strong>siderable potential benefit to others.<br />
The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce expressed some support <strong>for</strong> mandated choice but raised c<strong>on</strong>cerns<br />
about some of the practical difficulties and the costs which it c<strong>on</strong>sidered would be higher than<br />
implement<strong>in</strong>g and ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g an opt-out system (see below). 138 It also expressed c<strong>on</strong>cerns that<br />
the impositi<strong>on</strong> of a penalty <strong>on</strong> those who did not comply risked los<strong>in</strong>g public goodwill and<br />
challenged the c<strong>on</strong>cept of d<strong>on</strong>ati<strong>on</strong> based <strong>on</strong> a ‘gift relati<strong>on</strong>ship’. 139<br />
Practical c<strong>on</strong>siderati<strong>on</strong>s<br />
A number of practical issues would need to be addressed such as when <strong>in</strong>dividuals would be<br />
c<strong>on</strong>tacted, who would c<strong>on</strong>tact them, how people would express a view and what the punishment<br />
should be <strong>for</strong> fail<strong>in</strong>g to resp<strong>on</strong>d, as well as how they can change their m<strong>in</strong>d <strong>on</strong>ce their view is<br />
registered. It would not be possible just to add the names of those who say ‘yes’ to the exist<strong>in</strong>g<br />
Organ D<strong>on</strong>or Register, s<strong>in</strong>ce there would be no way to differentiate between those who said ‘no’<br />
and those who asked <strong>for</strong> the decisi<strong>on</strong> to be left to family members. This could lead to families<br />
be<strong>in</strong>g unwill<strong>in</strong>g to c<strong>on</strong>sent to d<strong>on</strong>ati<strong>on</strong>, <strong>in</strong> case their relative had chosen the ‘no’ opti<strong>on</strong>, and a<br />
subsequent <strong>in</strong>crease <strong>in</strong> the relative refusal rate. A specific database would, there<strong>for</strong>e need to be<br />
developed, c<strong>on</strong>ta<strong>in</strong><strong>in</strong>g the views of every adult with<strong>in</strong> the UK; this is a major and costly task.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 45
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
Public op<strong>in</strong>i<strong>on</strong><br />
Mandated choice received c<strong>on</strong>siderable public support <strong>in</strong> the deliberative events <strong>organ</strong>ised by the<br />
Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Of eight opti<strong>on</strong>s discussed, it was ranked fourth overall but was put <strong>in</strong><br />
the top three opti<strong>on</strong>s by 44% of participants and was ranked first by 22%. 140<br />
<strong>BMA</strong> view<br />
The <strong>BMA</strong> accepts that the pr<strong>in</strong>ciple beh<strong>in</strong>d mandated choice, that every<strong>on</strong>e’s views should be<br />
known and acted up<strong>on</strong>, is a good <strong>on</strong>e. It does not, however, have c<strong>on</strong>fidence that the system<br />
would work <strong>in</strong> practice, and has some c<strong>on</strong>cerns about the level of coerci<strong>on</strong> that would be<br />
required. If <strong>in</strong>dividuals are to be ‘mandated’ to make a choice, there must be some punishment<br />
<strong>for</strong> those that do not do so. Giv<strong>in</strong>g people the opti<strong>on</strong> not to make a choice, whilst superficially<br />
reassur<strong>in</strong>g, is unlikely to lead to any improvements over the status quo. In particular, the <strong>BMA</strong><br />
has c<strong>on</strong>cerns about:<br />
• the coercive nature of <strong>for</strong>c<strong>in</strong>g people to make a decisi<strong>on</strong> at a particular time<br />
• the risk that if people are required to make a choice when they do not want to, they may be<br />
more likely to say ‘no’<br />
• the situati<strong>on</strong> be<strong>in</strong>g no different than the status quo if people are given the opti<strong>on</strong> of not decid<strong>in</strong>g<br />
• the type of ‘punishment’ that might be appropriate or reas<strong>on</strong>able if <strong>in</strong>dividuals refuse to choose<br />
• the lack of any evidence show<strong>in</strong>g a positive associati<strong>on</strong> between mandated choice and d<strong>on</strong>ati<strong>on</strong><br />
rates.<br />
Opt-out with safeguards<br />
The <strong>BMA</strong> has l<strong>on</strong>g advocated an opt-out system with safeguards and c<strong>on</strong>t<strong>in</strong>ues to believe that<br />
this is the best opti<strong>on</strong> <strong>for</strong> the UK. Under an opt-out system every<strong>on</strong>e would be assumed to want<br />
to d<strong>on</strong>ate <strong>organ</strong>s after their death unless, hav<strong>in</strong>g received <strong>in</strong><strong>for</strong>mati<strong>on</strong> about the system, they<br />
had chosen to opt out of d<strong>on</strong>ati<strong>on</strong> dur<strong>in</strong>g their lifetime. Most supporters of this type of system,<br />
<strong>in</strong>clud<strong>in</strong>g the <strong>BMA</strong>, support what is often called a ‘soft’ system of opt-out. This system has built-<strong>in</strong><br />
safeguards, so that the family is always c<strong>on</strong>sulted and asked about any unregistered objecti<strong>on</strong> and<br />
there is scope not to proceed with d<strong>on</strong>ati<strong>on</strong> if this would cause severe distress to the family.<br />
(In practice the family needs to be <strong>in</strong>volved <strong>in</strong> order to provide <strong>in</strong><strong>for</strong>mati<strong>on</strong> about medical history<br />
etc and d<strong>on</strong>ati<strong>on</strong> is highly unlikely to proceed if the family is not available.) A few countries, such<br />
as Austria, operate a ‘hard’ opt-out system <strong>where</strong>by unless an <strong>in</strong>dividual has opted out of d<strong>on</strong>ati<strong>on</strong><br />
dur<strong>in</strong>g his or her lifetime <strong>organ</strong>s can be used <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> after death, with no role <strong>for</strong> the family.<br />
This system has not been proposed <strong>for</strong> the UK.<br />
The pr<strong>in</strong>ciple beh<strong>in</strong>d an opt-out system is that the default positi<strong>on</strong> should be to save lives and that,<br />
unless an <strong>in</strong>dividual objects to d<strong>on</strong>ati<strong>on</strong> their <strong>organ</strong>s should be used after death to benefit others.<br />
Under such a system <strong>in</strong>dividuals have exactly the same choice as under an opt-<strong>in</strong> system – to d<strong>on</strong>ate<br />
or not to d<strong>on</strong>ate – but the way that choice is registered differs, to give priority to d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the<br />
absence of objecti<strong>on</strong>. The system would work as follows.<br />
46<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
• Be<strong>for</strong>e the new system is <strong>in</strong>troduced there would be extensive and high profile publicity to<br />
ensure all members of society were aware of the <strong>for</strong>thcom<strong>in</strong>g change and to encourage them<br />
to c<strong>on</strong>sider their own wishes about d<strong>on</strong>ati<strong>on</strong> after their death.<br />
• A database would be established with mechanisms <strong>for</strong> people to easily and quickly opt out if<br />
that is their wish.<br />
• Once implemented, when some<strong>on</strong>e over the age of 16 dies and d<strong>on</strong>ati<strong>on</strong> is a possibility, the<br />
opt-out register must, by law, be checked and if the <strong>in</strong>dividual had opted out, d<strong>on</strong>ati<strong>on</strong> could<br />
not proceed.<br />
• As an extra safeguard, if the <strong>in</strong>dividual had not opted out, family members would be asked if<br />
they were aware of any unregistered objecti<strong>on</strong>.<br />
• If the relatives were not aware of any objecti<strong>on</strong>, they would be <strong>in</strong><strong>for</strong>med that d<strong>on</strong>ati<strong>on</strong> would<br />
proceed. There would, however, be scope not to proceed if it became evident that to do so<br />
would cause severe distress to the relatives.<br />
Those under the age of 16 and those who have not had capacity s<strong>in</strong>ce the system was <strong>in</strong>troduced,<br />
and there<strong>for</strong>e would not have had the opportunity to opt out, would be excluded from the system<br />
and specific c<strong>on</strong>sent from a qualify<strong>in</strong>g relative would c<strong>on</strong>t<strong>in</strong>ue to be required.<br />
The ma<strong>in</strong> practical change would be <strong>in</strong> the approach to relatives. Rather than ask<strong>in</strong>g them to make<br />
the decisi<strong>on</strong> (as currently happens when the <strong>in</strong>dividual’s views are not known), relatives would<br />
simply be asked if they were aware of any unregistered objecti<strong>on</strong>. The broader change would be<br />
to the philosophy around d<strong>on</strong>ati<strong>on</strong>, mak<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> the usual and expected th<strong>in</strong>g to happen<br />
when some<strong>on</strong>e dies. This is an outcome that has been widely champi<strong>on</strong>ed <strong>in</strong>clud<strong>in</strong>g by the Organ<br />
D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (mak<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> a usual not an unusual practice) and NHS BT (to promote<br />
<strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> as ‘expected behaviour’ am<strong>on</strong>gst UK citizens) 141 although different strategies<br />
have been recommended to achieve that outcome.<br />
Term<strong>in</strong>ology<br />
This system is often referred to as ‘presumed c<strong>on</strong>sent’ and this is the term the <strong>BMA</strong> has traditi<strong>on</strong>ally<br />
used. This term is, however, c<strong>on</strong>troversial with people argu<strong>in</strong>g that ‘presumed c<strong>on</strong>sent’ is not<br />
‘c<strong>on</strong>sent’ at all but someth<strong>in</strong>g rather different. The <strong>BMA</strong> has found that this has resulted <strong>in</strong> debate<br />
focus<strong>in</strong>g <strong>on</strong> the term<strong>in</strong>ology and thus detract<strong>in</strong>g from the important debate about the merits, or<br />
otherwise, of the system itself. Another term that is frequently used, and which is a simple descripti<strong>on</strong><br />
of the system is ‘opt-out’ – <strong>in</strong>dividuals who do not wish to d<strong>on</strong>ate need to opt out. In order to<br />
differentiate between those versi<strong>on</strong>s of opt-out that <strong>in</strong>volve the family and those that do not, the<br />
<strong>for</strong>mer is referred to as either ‘soft opt-out’ or ‘opt-out with safeguards’. In France the term<br />
‘presumed solidarity’ has been used. The <strong>BMA</strong>’s preferred term<strong>in</strong>ology is ‘opt-out with safeguards’.<br />
Evidence of effectiveness<br />
It is notoriously difficult to assess the impact of opt-out legislati<strong>on</strong> <strong>on</strong> d<strong>on</strong>ati<strong>on</strong> rates, because of<br />
the problem of separat<strong>in</strong>g out the effect of opt-out from other factors that are known to affect<br />
d<strong>on</strong>ati<strong>on</strong> rates. When analys<strong>in</strong>g the data to assess the impact of opt-out legislati<strong>on</strong>, there are two<br />
ma<strong>in</strong> types of research that can be undertaken, comparis<strong>on</strong>s between countries with an opt-out<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 47
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
system and those without, and compar<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> rates with<strong>in</strong> countries be<strong>for</strong>e the <strong>in</strong>troducti<strong>on</strong><br />
of an opt-out system and afterwards. It is not possible to do an experimental study or c<strong>on</strong>trolled<br />
trial, <strong>where</strong> other factors – such as the number of deaths from road traffic accidents – are manipulated<br />
or c<strong>on</strong>trolled, so it will never be possible to obta<strong>in</strong> a result show<strong>in</strong>g a clear cause and effect. The<br />
best result that can be obta<strong>in</strong>ed from this type of research is a positive associati<strong>on</strong> or correlati<strong>on</strong><br />
between an opt-out system and d<strong>on</strong>ati<strong>on</strong> rates.<br />
With support <strong>for</strong> an opt-out system be<strong>in</strong>g expressed by England’s Chief Medical Officer 142 and<br />
the then Prime M<strong>in</strong>ister, Gord<strong>on</strong> Brown, 143 the Government <strong>in</strong> 2007 asked the Organ D<strong>on</strong>ati<strong>on</strong><br />
Task<strong>for</strong>ce to undertake a review of opt-out and c<strong>on</strong>sider the potential impact of <strong>in</strong>troduc<strong>in</strong>g such<br />
a system <strong>in</strong> the UK. As part of this review the Task<strong>for</strong>ce commissi<strong>on</strong>ed the University of York to<br />
undertake an <strong>in</strong>dependent systematic review of all published studies. The review identified:<br />
• eight studies compar<strong>in</strong>g countries with an opt-out system and those without, four of which<br />
were ‘of sufficient methodological quality to provide reliable results.’ 144 All four of those studies<br />
found that opt-out law or practice was associated with <strong>in</strong>creased rates of d<strong>on</strong>ati<strong>on</strong><br />
and, <strong>in</strong> all except <strong>on</strong>e of these, the results were statistically significant.<br />
• five studies of countries be<strong>for</strong>e and after the <strong>in</strong>troducti<strong>on</strong> of opt-out legislati<strong>on</strong> which were<br />
methodologically sound. All of these studies reported an <strong>in</strong>crease <strong>in</strong> d<strong>on</strong>ati<strong>on</strong> rates follow<strong>in</strong>g<br />
the <strong>in</strong>troducti<strong>on</strong> of an opt-out system.<br />
The authors of the review c<strong>on</strong>cluded that:<br />
‘The available evidence suggests that presumed c<strong>on</strong>sent legislati<strong>on</strong> is associated with an<br />
<strong>in</strong>crease <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> rates, though the size of the associati<strong>on</strong> varied between studies.<br />
A number of other factors also appear to be associated with <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> rates, such as<br />
transplant capacity, GDP and health expenditure per capita.’ 145<br />
This c<strong>on</strong>firms the f<strong>in</strong>d<strong>in</strong>gs of studies c<strong>on</strong>ducted previously, 146 and s<strong>in</strong>ce the Task<strong>for</strong>ce’s report was<br />
published, 147 that hav<strong>in</strong>g an opt-out system is <strong>on</strong>e of a number of factors that are associated with<br />
higher d<strong>on</strong>ati<strong>on</strong> rates. The presence of that positive associati<strong>on</strong> <strong>in</strong> all the studies which met the<br />
criteria <strong>for</strong> the systematic review is, <strong>in</strong> the <strong>BMA</strong>’s view, the most c<strong>on</strong>v<strong>in</strong>c<strong>in</strong>g evidence that could<br />
be obta<strong>in</strong>ed from such a literature review, because these studies could not c<strong>on</strong>trol <strong>for</strong> possible<br />
c<strong>on</strong>found<strong>in</strong>g factors.<br />
The Task<strong>for</strong>ce <strong>in</strong>terpreted the York f<strong>in</strong>d<strong>in</strong>gs rather differently however, c<strong>on</strong>clud<strong>in</strong>g that ‘we found<br />
no c<strong>on</strong>v<strong>in</strong>c<strong>in</strong>g evidence that it would deliver significant <strong>in</strong>creases <strong>in</strong> the number of d<strong>on</strong>ated<br />
<strong>organ</strong>s’ and the report c<strong>on</strong>cluded that an opt-out system could ‘negatively impact <strong>on</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> numbers’. 148 This <strong>in</strong>terpretati<strong>on</strong> of the data was not universally shared. 149<br />
The <strong>BMA</strong> accepts that it is not easy to dem<strong>on</strong>strate a direct causal l<strong>in</strong>k between opt-out and<br />
d<strong>on</strong>ati<strong>on</strong> rates, because with observati<strong>on</strong>al studies it is difficult to exclude other factors that might<br />
have had an impact. Nevertheless, after review<strong>in</strong>g the evidence available the <strong>BMA</strong> c<strong>on</strong>cludes that<br />
48<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
there is a positive associati<strong>on</strong> between the two – that is to say that those countries that have an<br />
opt-out system tend to have higher d<strong>on</strong>ati<strong>on</strong> rates although it cannot be said <strong>for</strong> certa<strong>in</strong> what<br />
causes them.<br />
A study which did not meet the criteria of the York review looked at the differential rates of <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> between hospitals <strong>in</strong> Belgium which adopted the opt-out system and those which <strong>in</strong> the<br />
short-term did not. This was thus a ‘be<strong>for</strong>e and after’ study which did c<strong>on</strong>trol <strong>for</strong> factors such as<br />
<strong>in</strong>creased publicity surround<strong>in</strong>g the law change. It showed no <strong>in</strong>crease <strong>where</strong> the system was not<br />
changed and a significant <strong>in</strong>crease <strong>where</strong> it was changed. 150<br />
Ethical c<strong>on</strong>siderati<strong>on</strong>s<br />
Any system that has the potential to <strong>in</strong>crease the number of <strong>organ</strong>s available <strong>for</strong> d<strong>on</strong>ati<strong>on</strong>, and<br />
there<strong>for</strong>e the number of lives that can be saved, has str<strong>on</strong>g moral arguments to support it but<br />
there are other factors that need to be taken <strong>in</strong>to account.<br />
As menti<strong>on</strong>ed above, the central pr<strong>in</strong>ciple beh<strong>in</strong>d opt-out is that the default positi<strong>on</strong> should be<br />
to save lives. If people do not object, it is right that their <strong>organ</strong>s should be used <strong>for</strong> the benefit of<br />
others. That is not to say that we have a moral obligati<strong>on</strong> to d<strong>on</strong>ate, or that we have no <strong>in</strong>terest or<br />
rights <strong>in</strong> relati<strong>on</strong> to what happens to our bodies. Rather, if <strong>in</strong>dividuals have not <strong>in</strong>dicated any objecti<strong>on</strong><br />
to d<strong>on</strong>ati<strong>on</strong>, it is appropriate to assume they would want to act <strong>in</strong> an altruistic manner and help others.<br />
The <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> system <strong>in</strong> the UK is based <strong>on</strong> altruism and the noti<strong>on</strong> of a gift relati<strong>on</strong>ship.<br />
The ‘gift’ element of d<strong>on</strong>ati<strong>on</strong> can be important to those families who c<strong>on</strong>sent to d<strong>on</strong>ati<strong>on</strong>, and<br />
to those who receive <strong>organ</strong>s. It has been suggested that if the <strong>in</strong>dividual does not pers<strong>on</strong>ally, or via<br />
his or her family, pro-actively ‘volunteer’ the <strong>organ</strong>, it is no l<strong>on</strong>ger a gift. Under an opt-out system,<br />
however, <strong>in</strong>dividuals go through exactly the same thought process to decide not to opt out as<br />
they do <strong>in</strong> decid<strong>in</strong>g to opt <strong>in</strong>. Given the opti<strong>on</strong> to d<strong>on</strong>ate or not, a decisi<strong>on</strong> is made to act to help<br />
others, by not opt<strong>in</strong>g out of d<strong>on</strong>ati<strong>on</strong>; this is no less of a gift than an <strong>organ</strong> d<strong>on</strong>ated under an<br />
opt-<strong>in</strong> system. Undoubtedly some will th<strong>in</strong>k more about this than others and some people will<br />
choose not to th<strong>in</strong>k about it at all. Under an opt-out system, there is no way of know<strong>in</strong>g which of<br />
those who have not opted out would have taken positive steps to d<strong>on</strong>ate under an opt-<strong>in</strong> system.<br />
Some people will see the loss of this positive acti<strong>on</strong> to d<strong>on</strong>ate as a cause <strong>for</strong> c<strong>on</strong>cern. Whilst it<br />
may be seen as preferable <strong>for</strong> <strong>in</strong>dividuals – or their families – to take active steps to give <strong>organ</strong>s,<br />
we need to acknowledge that under the current system, <strong>organ</strong>s are be<strong>in</strong>g lost that could have<br />
saved lives when that would not have been the wish of potential d<strong>on</strong>ors. In the <strong>BMA</strong>’s view<br />
families should be encouraged to see the whole process of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> as a ‘gift’ which has<br />
the potential <strong>for</strong> very significant benefit to another pers<strong>on</strong>.<br />
A central questi<strong>on</strong> around opt-out systems <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> is whether they enhance or reduce<br />
aut<strong>on</strong>omy. Those who oppose such schemes suggest that the decisi<strong>on</strong> is be<strong>in</strong>g taken out of the<br />
hands of <strong>in</strong>dividuals and the government is tak<strong>in</strong>g and us<strong>in</strong>g <strong>organ</strong>s without c<strong>on</strong>sent. Individuals,<br />
and their families, are thus denied the right to make a pers<strong>on</strong>al decisi<strong>on</strong> and so their aut<strong>on</strong>omy is<br />
underm<strong>in</strong>ed. It is important to recognise, however, that under an opt-out system <strong>in</strong>dividuals have<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 49
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
Dur<strong>in</strong>g the Task<strong>for</strong>ce review of opt-out, some <strong>in</strong>tensivists raised c<strong>on</strong>cerns that patients might<br />
be afraid that ef<strong>for</strong>ts would not be made to save their own lives if they were c<strong>on</strong>sidered to be<br />
potential <strong>organ</strong> d<strong>on</strong>ors. This is a c<strong>on</strong>cern that we know is already held by some people under the<br />
current system, 153 and so it is not exclusive to opt-out. It could equally be argued that if people are<br />
<strong>on</strong> the Organ D<strong>on</strong>or Register – and thus <strong>in</strong>dicate a will<strong>in</strong>gness to d<strong>on</strong>ate – they might be seen as<br />
potential d<strong>on</strong>ors rather than as patients. The important po<strong>in</strong>t – irrespective of the c<strong>on</strong>sent system<br />
<strong>in</strong> place – is to ensure that patients and the public are aware of the clear separati<strong>on</strong> between the<br />
treat<strong>in</strong>g team and the transplant team and that patients and relatives are given sufficient<br />
<strong>in</strong><strong>for</strong>mati<strong>on</strong> about what is happen<strong>in</strong>g and why, to reassure them that all treatment decisi<strong>on</strong>s<br />
are made <strong>in</strong> patients’ best <strong>in</strong>terests.<br />
Public op<strong>in</strong>i<strong>on</strong><br />
Public support is crucial <strong>for</strong> an opt-out system to work. In 1999 the Department of Health<br />
commissi<strong>on</strong>ed a survey of public op<strong>in</strong>i<strong>on</strong> <strong>in</strong> which 28% supported a shift to an opt-out system<br />
with 50% opposed and 22% undecided. 154 S<strong>in</strong>ce then, however, a number of surveys have shown<br />
<strong>in</strong>creas<strong>in</strong>g support <strong>for</strong> such a shift. In October 2007 a YouGov survey commissi<strong>on</strong>ed by the <strong>BMA</strong><br />
showed that 64% of resp<strong>on</strong>dents would support an opt-out system with safeguards. 155<br />
The most recent and most comprehensive survey of public op<strong>in</strong>i<strong>on</strong> was undertaken <strong>in</strong> 2008 by the<br />
Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce which <strong>organ</strong>ised seven <strong>on</strong>e-day workshops around the UK each with<br />
about 50 participants. 156 Participants were polled at the beg<strong>in</strong>n<strong>in</strong>g of the event and aga<strong>in</strong> after<br />
receiv<strong>in</strong>g <strong>in</strong><strong>for</strong>mati<strong>on</strong>, watch<strong>in</strong>g video clips present<strong>in</strong>g arguments <strong>for</strong> and aga<strong>in</strong>st opt-out and<br />
hav<strong>in</strong>g the opportunity to ask questi<strong>on</strong>s and discuss the issue with a panel of experts. Be<strong>for</strong>e the<br />
event 65% supported a change <strong>in</strong> legislati<strong>on</strong> to opt-out. After receiv<strong>in</strong>g <strong>in</strong><strong>for</strong>mati<strong>on</strong> and hav<strong>in</strong>g<br />
the chance to c<strong>on</strong>sider the issue carefully, this <strong>in</strong>creased to 72% <strong>in</strong> favour of this change. The<br />
number who expressed ‘str<strong>on</strong>g support’ <strong>for</strong> such a change nearly doubled after the event from<br />
25% to 43%. 157<br />
The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce Report<br />
The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce, which reported <strong>in</strong> 2008, did not recommend a shift to an opt-out<br />
system at that time. 158 One of its c<strong>on</strong>cerns was the cost of implement<strong>in</strong>g the new system. It<br />
estimated set-up costs <strong>for</strong> the database of at least £10 milli<strong>on</strong> and £2 milli<strong>on</strong> per annum runn<strong>in</strong>g<br />
costs. The Task<strong>for</strong>ce also estimated that publicity around the new system would cost a further<br />
£25 milli<strong>on</strong> <strong>for</strong> a susta<strong>in</strong>ed three-year campaign. (This compares with £12.1milli<strong>on</strong> spent <strong>in</strong> the<br />
f<strong>in</strong>ancial year 2007/08 <strong>in</strong> c<strong>on</strong>necti<strong>on</strong> with the ban <strong>on</strong> smok<strong>in</strong>g <strong>in</strong> public places. 159 )<br />
The Task<strong>for</strong>ce c<strong>on</strong>cluded that the changes to the <strong>in</strong>frastructure it had recommended <strong>in</strong> its first<br />
report (see secti<strong>on</strong> 4) should be tried first and might make opt-out unnecessary. It there<strong>for</strong>e<br />
adopted a ‘wait and see’ strategy. The expert work<strong>in</strong>g groups established by the Organ D<strong>on</strong>ati<strong>on</strong><br />
Task<strong>for</strong>ce to c<strong>on</strong>sider the legal and ethical implicati<strong>on</strong>s of chang<strong>in</strong>g to a system of presumed<br />
c<strong>on</strong>sent advised, however, that there were ‘no fundamental legal or ethical barriers to <strong>in</strong>troduc<strong>in</strong>g<br />
a ‘soft’ opt out system, <strong>in</strong> which, as a safeguard, family members would be c<strong>on</strong>sulted about<br />
d<strong>on</strong>ati<strong>on</strong>.’ 160<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 51
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
In spite of the report’s c<strong>on</strong>clusi<strong>on</strong> the Welsh Assembly Government has pledged to <strong>in</strong>troduce an<br />
opt-out system with safeguards <strong>in</strong> Wales and a White Paper was published <strong>in</strong> November 2011. 161<br />
<strong>BMA</strong> view<br />
The <strong>BMA</strong> has supported a change <strong>in</strong> legislati<strong>on</strong> to opt-out with safeguards s<strong>in</strong>ce 1999. This <strong>policy</strong><br />
has been reaffirmed <strong>on</strong> many occasi<strong>on</strong>s s<strong>in</strong>ce. The ma<strong>in</strong> reas<strong>on</strong>s <strong>for</strong> the <strong>BMA</strong>’s support can be<br />
summarised as follows.<br />
• We believe that, as <strong>on</strong>e part of a broader strategy, a shift to an opt-out system will have a<br />
positive effect <strong>on</strong> d<strong>on</strong>ati<strong>on</strong> rates.<br />
• Studies show that a large majority of people would be will<strong>in</strong>g to d<strong>on</strong>ate but <strong>on</strong>ly 29% of the<br />
populati<strong>on</strong> are <strong>on</strong> the NHS Organ D<strong>on</strong>or Register or carry a d<strong>on</strong>or card. While this level of<br />
apathy exists despite people’s good <strong>in</strong>tenti<strong>on</strong>s, people will c<strong>on</strong>t<strong>in</strong>ue to die while wait<strong>in</strong>g <strong>for</strong><br />
d<strong>on</strong>or <strong>organ</strong>s.<br />
• The <strong>BMA</strong> supports the pr<strong>in</strong>ciple beh<strong>in</strong>d an opt-out system – that if people do not object to their<br />
<strong>organ</strong>s be<strong>in</strong>g used after death, they should be used to save lives.<br />
• Under an opt-out system <strong>in</strong>dividuals have exactly the same choice as <strong>in</strong> an opt-<strong>in</strong> system –<br />
to d<strong>on</strong>ate or not to d<strong>on</strong>ate.<br />
• The decisi<strong>on</strong> not to opt out of d<strong>on</strong>ati<strong>on</strong> is as much of a gift as a decisi<strong>on</strong> to opt <strong>in</strong>.<br />
• An opt-out system gives added protecti<strong>on</strong> to those who do not wish to d<strong>on</strong>ate and makes it<br />
more likely that those who are will<strong>in</strong>g to d<strong>on</strong>ate will be able to do so.<br />
• Organ d<strong>on</strong>ati<strong>on</strong> becomes the default positi<strong>on</strong> which, with public support, changes cultural<br />
expectati<strong>on</strong>s <strong>in</strong> society. This represents a more positive view of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> which is to be<br />
encouraged.<br />
• Overall an opt-out system is better <strong>for</strong> recipients (because more <strong>organ</strong>s will be available) better<br />
<strong>for</strong> d<strong>on</strong>ors (because it is more likely their wishes will be respected) and better <strong>for</strong> relatives<br />
(because it is more likely that the <strong>in</strong>dividual’s own wishes will be known).<br />
Reciprocity<br />
Under a system of reciprocity, those who d<strong>on</strong>ate <strong>organ</strong>s, or sign up to d<strong>on</strong>ate after their death,<br />
receive priority should they themselves require a transplant. One of the aims of this system is to<br />
overcome the problem of so-called ‘free-riders’ – those who would be will<strong>in</strong>g to accept an <strong>organ</strong>,<br />
should they need <strong>on</strong>e, but are not will<strong>in</strong>g themselves to d<strong>on</strong>ate (although, <strong>in</strong> practice, most people<br />
have simply not made a decisi<strong>on</strong> rather than actually be<strong>in</strong>g ‘unwill<strong>in</strong>g’ to d<strong>on</strong>ate). NHS Blood and<br />
Transplant highlighted this <strong>in</strong> its advertis<strong>in</strong>g campaign launched <strong>in</strong> 2009 follow<strong>in</strong>g surveys that<br />
showed that while 96% would accept an <strong>organ</strong> if they needed <strong>on</strong>e, <strong>on</strong>ly 27% had signed up to<br />
the Organ D<strong>on</strong>or Register. 162 This lack of reciprocity is not just an issue with <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>; NHS<br />
BT’s surveys also found that 55% of those questi<strong>on</strong>ed would accept a lift without offer<strong>in</strong>g <strong>on</strong>e <strong>in</strong><br />
return and half would borrow books but haven’t lent their own.<br />
52<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
In 2008 Israel became the first country to pass legislati<strong>on</strong> <strong>in</strong>corporat<strong>in</strong>g a system of reciprocity<br />
<strong>in</strong>to its <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> system. 163 Under the new system, which came <strong>in</strong>to effect <strong>in</strong> January 2010,<br />
priority is still given to those <strong>in</strong> urgent medical need of a heart, lung or liver. Where two candidates<br />
have equal cl<strong>in</strong>ical need, however, priority will be given to:<br />
• <strong>in</strong>dividuals who c<strong>on</strong>sent dur<strong>in</strong>g their life to d<strong>on</strong>ate <strong>organ</strong>s follow<strong>in</strong>g death and their first degree<br />
relatives<br />
• first degree relatives of people who d<strong>on</strong>ated <strong>organ</strong>s follow<strong>in</strong>g their death<br />
• <strong>in</strong>dividuals who become n<strong>on</strong>-directed liv<strong>in</strong>g d<strong>on</strong>ors (ie to strangers) and their first degree relatives.<br />
With<strong>in</strong> these categories a weight<strong>in</strong>g system is applied such that first degree relatives of those<br />
who have signed a d<strong>on</strong>or card have half the priority given to those who have signed a d<strong>on</strong>or card<br />
themselves. Those who have a first degree relative who d<strong>on</strong>ated after death and those who were<br />
n<strong>on</strong>-directed liv<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ors have <strong>on</strong>e and a half times the priority of those who have signed<br />
a d<strong>on</strong>or card.<br />
The <strong>in</strong>troducti<strong>on</strong> of the new system was preceded by a ‘massive, multil<strong>in</strong>gual, multimedia<br />
educati<strong>on</strong>al campaign designed and aimed at all levels of educati<strong>on</strong> <strong>in</strong> the public’ 164 with the aim<br />
of encourag<strong>in</strong>g people to sign an <strong>organ</strong> d<strong>on</strong>or card. The new <strong>policy</strong> applies to every<strong>on</strong>e, <strong>in</strong>clud<strong>in</strong>g<br />
those who have religious objecti<strong>on</strong>s to d<strong>on</strong>ati<strong>on</strong> (<strong>on</strong> the basis that if they oppose d<strong>on</strong>ati<strong>on</strong> they<br />
should neither give nor receive <strong>organ</strong>s). The <strong>policy</strong> is due to be reviewed after two years.<br />
A system of reciprocity also operates under United Network <strong>for</strong> Organ Shar<strong>in</strong>g (UNOS) guidel<strong>in</strong>es<br />
<strong>in</strong> the United States, <strong>where</strong>by any liv<strong>in</strong>g d<strong>on</strong>or is given priority <strong>for</strong> <strong>organ</strong>s from deceased d<strong>on</strong>ors<br />
should they need them at any stage <strong>in</strong> the future. This could be seen as act<strong>in</strong>g as an <strong>in</strong>centive to<br />
people to d<strong>on</strong>ate or it could be seen as remov<strong>in</strong>g a counter-<strong>in</strong>centive. If fear of failure of the<br />
rema<strong>in</strong><strong>in</strong>g kidney deters people from act<strong>in</strong>g as liv<strong>in</strong>g d<strong>on</strong>ors, then assur<strong>in</strong>g them that they would<br />
be given priority <strong>for</strong> an <strong>organ</strong>, should they need <strong>on</strong>e <strong>in</strong> future, might <strong>in</strong>crease the number of<br />
d<strong>on</strong>ors and there<strong>for</strong>e the number of lives saved and trans<strong>for</strong>med by a transplant.<br />
Evidence of effectiveness<br />
As menti<strong>on</strong>ed above, it is very difficult to obta<strong>in</strong> data show<strong>in</strong>g the impact of any <strong>in</strong>dividual factor or<br />
<strong>in</strong>itiative <strong>on</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> rates. A news article <strong>in</strong> the BMJ <strong>in</strong> 2011, <strong>for</strong> example, reported that the<br />
number of transplants fell by 20% <strong>in</strong> Israel <strong>in</strong> the previous year and that the number of people dy<strong>in</strong>g<br />
while wait<strong>in</strong>g <strong>for</strong> an <strong>organ</strong> <strong>in</strong>creased. 165 The reas<strong>on</strong> given <strong>for</strong> this fall, however, was the legal changes<br />
to the def<strong>in</strong>iti<strong>on</strong> of death <strong>in</strong> 2008. No menti<strong>on</strong> was made of the number of liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong>s or d<strong>on</strong>or<br />
registrati<strong>on</strong>s as an <strong>in</strong>dicator <strong>for</strong> how well the ‘reciprocity provisi<strong>on</strong>s’ <strong>in</strong> the Act have been received.<br />
In additi<strong>on</strong>, part of the measure of the success of this scheme is the number of people carry<strong>in</strong>g<br />
d<strong>on</strong>or cards and it is likely to take some time be<strong>for</strong>e any <strong>in</strong>crease <strong>in</strong> people sign<strong>in</strong>g up <strong>for</strong> d<strong>on</strong>ati<strong>on</strong><br />
is reflected <strong>in</strong> <strong>in</strong>creased d<strong>on</strong>ati<strong>on</strong> rates. The publicity surround<strong>in</strong>g the <strong>in</strong>troducti<strong>on</strong> of the scheme,<br />
however, could reas<strong>on</strong>ably be expected to have itself had a positive impact <strong>on</strong> d<strong>on</strong>ati<strong>on</strong> rates. It is<br />
there<strong>for</strong>e difficult to judge how much any improvements have been offset by the reducti<strong>on</strong> <strong>in</strong><br />
d<strong>on</strong>ors result<strong>in</strong>g from changes to the def<strong>in</strong>iti<strong>on</strong> of death.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 53
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
Ethical c<strong>on</strong>siderati<strong>on</strong>s<br />
The noti<strong>on</strong> of reward<strong>in</strong>g those who c<strong>on</strong>tribute to the public good has many attracti<strong>on</strong>s, not least<br />
because its focus is not simply <strong>on</strong> <strong>in</strong>creas<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> rates but also <strong>on</strong> mak<strong>in</strong>g the system fairer.<br />
Nevertheless, the offer of an <strong>in</strong>centive <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> is seen by some as underm<strong>in</strong><strong>in</strong>g the ‘gift<br />
relati<strong>on</strong>ship’ <strong>where</strong>by an <strong>in</strong>dividual, as an act of solidarity, d<strong>on</strong>ates an <strong>organ</strong> to another pers<strong>on</strong> <strong>for</strong><br />
no pers<strong>on</strong>al ga<strong>in</strong>. With systems of reciprocity, d<strong>on</strong>ors are encouraged to give <strong>in</strong> order to receive some<br />
(actual or potential) benefit, there<strong>for</strong>e emphasis<strong>in</strong>g self-<strong>in</strong>terest over pure altruism. A significant,<br />
but perhaps not the <strong>on</strong>ly, reas<strong>on</strong> <strong>for</strong> d<strong>on</strong>at<strong>in</strong>g is to ga<strong>in</strong> some pers<strong>on</strong>al advantage – <strong>in</strong> terms of<br />
priority <strong>for</strong> an <strong>organ</strong> <strong>in</strong> the future should <strong>on</strong>e be needed. The difference between these schemes<br />
and payment per se, however, is that the reward is not immediate and the <strong>in</strong>dividual may never<br />
need an <strong>organ</strong> and so never ga<strong>in</strong> any benefit.<br />
Offer<strong>in</strong>g <strong>in</strong>centives is frequently c<strong>on</strong>sidered to be coercive but it has been argued that any coerci<strong>on</strong><br />
<strong>in</strong> a reciprocity scheme <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> must be m<strong>in</strong>imal given that ‘all the benefits accrue to<br />
the <strong>in</strong>dividual while s/he is alive while the costs are exacted exclusively after his/her death’. 166 This,<br />
of course, <strong>on</strong>ly applies to systems that relate solely to deceased d<strong>on</strong>ati<strong>on</strong>. Even <strong>where</strong> the scheme<br />
<strong>in</strong>cludes liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong>, however, there is no guarantee of benefit s<strong>in</strong>ce the d<strong>on</strong>or may never be<br />
<strong>in</strong> the positi<strong>on</strong> of need<strong>in</strong>g an <strong>organ</strong> so the lack of any immediate benefit would appear to reduce,<br />
if not eradicate, c<strong>on</strong>cerns about coerci<strong>on</strong>.<br />
Such schemes also <strong>in</strong>troduce allocati<strong>on</strong> based partly <strong>on</strong> social, rather than solely cl<strong>in</strong>ical, factors.<br />
Those who act <strong>in</strong> a way we c<strong>on</strong>sider to be <strong>in</strong> the public good – by agree<strong>in</strong>g to d<strong>on</strong>ate – get the<br />
possibility of some future benefit, <strong>where</strong>as those who do not, risk be<strong>in</strong>g penalised by hav<strong>in</strong>g a<br />
lower priority <strong>in</strong> the event of need<strong>in</strong>g an <strong>organ</strong>. Although <strong>in</strong> practice cl<strong>in</strong>ical need would c<strong>on</strong>t<strong>in</strong>ue<br />
to be the pr<strong>in</strong>cipal factor <strong>in</strong> allocat<strong>in</strong>g <strong>organ</strong>s, and d<strong>on</strong>ati<strong>on</strong> status would <strong>on</strong>ly be c<strong>on</strong>sidered<br />
<strong>where</strong> two <strong>in</strong>dividuals have the same cl<strong>in</strong>ical need, <strong>in</strong>troduc<strong>in</strong>g any moral element to these<br />
judgements by c<strong>on</strong>sider<strong>in</strong>g d<strong>on</strong>or status could be seen as a step towards allocati<strong>on</strong> based <strong>on</strong> social<br />
worth or just deserts. Gill<strong>on</strong> warns that ‘[i]f past or present fault [thus] became an accepted<br />
criteri<strong>on</strong> <strong>for</strong> distributive justice <strong>for</strong> scarce medical resources, a very steep ‘logical slippery slope’<br />
would have been created.’ 177<br />
Practical c<strong>on</strong>siderati<strong>on</strong>s<br />
In establish<strong>in</strong>g a system of reciprocity, there would need to be some time-limits <strong>on</strong> registrati<strong>on</strong> to<br />
ga<strong>in</strong> entitlements. If not there would be noth<strong>in</strong>g to prevent those who are told they need an <strong>organ</strong><br />
transplant from sign<strong>in</strong>g up to the register <strong>in</strong> order to ga<strong>in</strong> immediate priority access to <strong>organ</strong>s. If<br />
this were possible, the <strong>in</strong>centive <strong>for</strong> those not requir<strong>in</strong>g a transplant to sign up would be removed<br />
– they could simply wait and see if they need an <strong>organ</strong>. In development of the Israeli law it was<br />
agreed that people should be registered <strong>for</strong> three years prior to their need <strong>for</strong> a transplant be<strong>in</strong>g<br />
identified <strong>in</strong> order to receive the benefit. As a transiti<strong>on</strong>al arrangement <strong>for</strong> the first year, any<strong>on</strong>e<br />
<strong>on</strong> the register would be given priority over those not <strong>on</strong> the register.<br />
Thought would need to be given to how children and adults lack<strong>in</strong>g capacity would fare with<strong>in</strong><br />
such a system. The most logical opti<strong>on</strong> would be to exclude them from the scheme and to reach<br />
54<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
a fair positi<strong>on</strong> about how their priority would be determ<strong>in</strong>ed relative to those with<strong>in</strong> the scheme.<br />
Alternatively, proxy advance decisi<strong>on</strong>s could be made by parents <strong>on</strong> behalf of children too young<br />
to make a pers<strong>on</strong>al choice. Similarly carers could make proxy decisi<strong>on</strong>s <strong>on</strong> behalf of adults lack<strong>in</strong>g<br />
capacity <strong>on</strong> the basis that it is clearly <strong>in</strong> their best <strong>in</strong>terests to receive priority access to <strong>organ</strong>s,<br />
should they need it, without caus<strong>in</strong>g them any significant harm. 168<br />
One of the practical difficulties of the scheme relates to the relative weight given to registrati<strong>on</strong> <strong>on</strong><br />
the Organ D<strong>on</strong>or Register and cl<strong>in</strong>ical needs. If greater weight is given to sign<strong>in</strong>g up to the Organ<br />
D<strong>on</strong>or Register, the <strong>in</strong>centive <strong>for</strong> people to sign up is large and the <strong>in</strong>crease <strong>in</strong> d<strong>on</strong>ors is likely to<br />
be significant. This means, however, that those who do not sign up are unlikely to receive <strong>organ</strong>s<br />
despite hav<strong>in</strong>g far greater cl<strong>in</strong>ical need than other people who have volunteered to be d<strong>on</strong>ors after<br />
their death. This is a very harsh punishment <strong>for</strong> people who may have failed to sign up because of<br />
apathy, because they are dis<strong>organ</strong>ised or because they do not want to c<strong>on</strong>fr<strong>on</strong>t their own mortality<br />
<strong>for</strong> example. This appears to c<strong>on</strong>travene a central pr<strong>in</strong>ciple <strong>in</strong> medical ethics that medical care<br />
should be provided, and scarce resources allocated, <strong>on</strong> the basis of cl<strong>in</strong>ical need and not <strong>on</strong> the<br />
actual or perceived blameworth<strong>in</strong>ess of the patient. 169 If priority is given to cl<strong>in</strong>ical need, however,<br />
as <strong>in</strong> Israel, and it is <strong>on</strong>ly when two people have exactly the same cl<strong>in</strong>ical need that their d<strong>on</strong>or<br />
status becomes relevant, there is less of an <strong>in</strong>centive to d<strong>on</strong>ate and there<strong>for</strong>e less likelihood of the<br />
scheme hav<strong>in</strong>g a significant impact <strong>on</strong> d<strong>on</strong>or rates. Some balance would need to be reached<br />
between these two factors <strong>in</strong> order <strong>for</strong> the system to be fair but also to be effective.<br />
A key aim of reciprocity systems is to <strong>in</strong>crease fairness by giv<strong>in</strong>g priority <strong>in</strong> terms of allocati<strong>on</strong> to<br />
those who are themselves will<strong>in</strong>g to d<strong>on</strong>ate. It is suggested that, s<strong>in</strong>ce so-called ‘free-rid<strong>in</strong>g’ is<br />
a ‘morally precarious positi<strong>on</strong>’, it is reas<strong>on</strong>able to counteract that by disadvantag<strong>in</strong>g those who<br />
choose not to sign up <strong>for</strong> d<strong>on</strong>ati<strong>on</strong>. 170 This may be seen as fair <strong>in</strong> relati<strong>on</strong> to the majority, but some<br />
thought needs to be given to those whose <strong>organ</strong>s are not suitable <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> – because of<br />
current illness, or past medical history, <strong>for</strong> example. This group will be unfairly disadvantaged<br />
because it is not that they are unwill<strong>in</strong>g to d<strong>on</strong>ate but that their <strong>organ</strong>s are simply not suitable.<br />
Public op<strong>in</strong>i<strong>on</strong><br />
In a 2004 survey of 336 adults <strong>in</strong> Greater L<strong>on</strong>d<strong>on</strong> (118 Asian, 112 African-Caribbean and 106<br />
white), participants were asked to rate the impact of a series of <strong>in</strong>itiatives <strong>on</strong> their will<strong>in</strong>gness to<br />
sign up to d<strong>on</strong>ate <strong>organ</strong>s after death. 171 The opti<strong>on</strong>s <strong>in</strong>cluded ga<strong>in</strong><strong>in</strong>g priority access to <strong>organ</strong>s, as<br />
well as cash payments at the time of sign<strong>in</strong>g up to the <strong>organ</strong> d<strong>on</strong>or register, reduced <strong>in</strong>surance<br />
premiums, ability to <strong>in</strong>fluence the characteristics of <strong>organ</strong> recipients and <strong>for</strong>mal recogniti<strong>on</strong> of<br />
d<strong>on</strong>ati<strong>on</strong>. Am<strong>on</strong>gst all groups the alternatives that were deemed most important <strong>on</strong> average<br />
were priority access to <strong>organ</strong>s should the need arise and upfr<strong>on</strong>t cash payments.<br />
A survey of 1,009 Scottish adults <strong>in</strong> 2004 found mixed op<strong>in</strong>i<strong>on</strong>s regard<strong>in</strong>g reciprocity schemes with<br />
42% <strong>in</strong> support, 43% neither agree<strong>in</strong>g nor disagree<strong>in</strong>g and 12% opposed to such schemes. 172<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 55
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
<strong>BMA</strong> view<br />
The <strong>BMA</strong> supports the approach of NHS BT <strong>in</strong> draw<strong>in</strong>g attenti<strong>on</strong> to the moral disparity of those<br />
who are not will<strong>in</strong>g to d<strong>on</strong>ate <strong>organ</strong>s after their death but would be will<strong>in</strong>g to accept an <strong>organ</strong> if<br />
they needed <strong>on</strong>e. It is appropriate to encourage people to th<strong>in</strong>k about this but the <strong>BMA</strong> does not<br />
support the type of reciprocity system <strong>in</strong>troduced <strong>in</strong> Israel because it breaches two fundamental<br />
pr<strong>in</strong>ciples that the <strong>BMA</strong> values, namely that:<br />
• d<strong>on</strong>ati<strong>on</strong> should be a gift freely and voluntarily given and there<strong>for</strong>e <strong>in</strong>dividuals should not be<br />
given an <strong>in</strong>centive to d<strong>on</strong>ate and<br />
• <strong>organ</strong>s should be allocated <strong>on</strong> the basis of cl<strong>in</strong>ical need and social or moral factors should not<br />
be taken <strong>in</strong>to account.<br />
A regulated market<br />
Most of the discussi<strong>on</strong> <strong>in</strong> this paper has focused <strong>on</strong> d<strong>on</strong>ati<strong>on</strong> after death but an <strong>in</strong>creas<strong>in</strong>g number<br />
of transplants are from liv<strong>in</strong>g d<strong>on</strong>ors. Currently the law permits liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> – <strong>in</strong>clud<strong>in</strong>g to<br />
strangers (see secti<strong>on</strong> 3) – but prohibits the sale of, or trade <strong>in</strong>, <strong>organ</strong>s. Intermittently, however,<br />
calls are made <strong>for</strong> the <strong>organ</strong> shortage to be addressed by allow<strong>in</strong>g people to sell their <strong>organ</strong>s.<br />
In August 2011, <strong>for</strong> example, a paper <strong>in</strong> the BMJ recommended that healthy <strong>in</strong>dividuals should<br />
be offered about £28,000 – the average annual <strong>in</strong>come <strong>in</strong> the UK – to d<strong>on</strong>ate a kidney to enable<br />
people to ‘do a k<strong>in</strong>d deed and make enough m<strong>on</strong>ey to, <strong>for</strong> <strong>in</strong>stance, pay off university loans.’ 173<br />
Whilst some supporters of paid <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> advocate a free market approach to <strong>organ</strong> sales, 174<br />
others believe that most of the c<strong>on</strong>cerns about the potential harmful effects of allow<strong>in</strong>g people<br />
to sell their <strong>organ</strong>s can be overcome through a regulated market.<br />
In <strong>on</strong>e possible model <strong>for</strong> a regulated market <strong>in</strong> the UK, the NHS would be the sole authorised<br />
purchaser and would buy <strong>organ</strong>s and tissue, <strong>for</strong> a fixed price, from will<strong>in</strong>g sellers <strong>in</strong> the same<br />
way as it does other goods such as dialysis mach<strong>in</strong>es or drugs. 175 Only those liv<strong>in</strong>g with<strong>in</strong> the<br />
geographical area covered by the scheme, who may there<strong>for</strong>e also benefit by receiv<strong>in</strong>g an <strong>organ</strong>,<br />
should be eligible to sell. The NHS purchaser would ensure appropriate screen<strong>in</strong>g, match<strong>in</strong>g and<br />
allocati<strong>on</strong> of <strong>organ</strong>s – to prevent the rich ga<strong>in</strong><strong>in</strong>g an unfair advantage at the expense of the poor.<br />
Allocati<strong>on</strong> would c<strong>on</strong>t<strong>in</strong>ue to be <strong>on</strong> the basis of need. John Harris, a str<strong>on</strong>g advocate <strong>for</strong> such a<br />
scheme, argues that those who agree to sell their <strong>organ</strong>s should be given priority <strong>in</strong> the allocati<strong>on</strong><br />
of <strong>organ</strong>s if they become patients <strong>in</strong> need of a transplant <strong>in</strong> the future. 176 He also argues that any<br />
payment made to sellers should not be liable to tax or reducti<strong>on</strong> of welfare benefits, as an added<br />
<strong>in</strong>centive to <strong>in</strong>dividuals to sell their <strong>organ</strong>s and thus benefit both themselves and others.<br />
Evidence of effectiveness<br />
Although it is widely recognised that the illegal sale of <strong>organ</strong>s is endemic <strong>in</strong> some parts of the<br />
world, 177 Iran is the <strong>on</strong>ly country to legally permit a market <strong>in</strong> human kidneys. 178 The system, <strong>in</strong><br />
operati<strong>on</strong> s<strong>in</strong>ce 1988, is run by the Dialysis and Transplant Patients Associati<strong>on</strong> (DTPA), a voluntary<br />
patient group. Potential vendors c<strong>on</strong>tact DTPA and are referred to a transplant centre <strong>for</strong><br />
evaluati<strong>on</strong> accord<strong>in</strong>g to the same medical criteria as liv<strong>in</strong>g d<strong>on</strong>ors who are not f<strong>in</strong>ancially<br />
compensated. The Iranian government provides a fixed compensati<strong>on</strong> of approximately US$1,200<br />
56<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
plus health <strong>in</strong>surance cover <strong>for</strong> <strong>on</strong>e year <strong>for</strong> c<strong>on</strong>diti<strong>on</strong>s directly related to the surgery. The vendor<br />
also receives remunerati<strong>on</strong> either from the recipient, the recipient’s family or <strong>on</strong>e of a number of<br />
charitable <strong>organ</strong>isati<strong>on</strong>s: this amount is usually between US$2,300 and US$4,500. Vendors must<br />
be aged between 20 and 35 years of age and must also have the c<strong>on</strong>sent of their <strong>next</strong> of k<strong>in</strong>. 179<br />
Analyses of the Iranian system 180 have found that:<br />
• by 1999 the wait<strong>in</strong>g list <strong>for</strong> kidneys had been elim<strong>in</strong>ated (subsequent reports, however, have<br />
claimed that this is <strong>on</strong>ly true <strong>for</strong> those who can af<strong>for</strong>d to pay <strong>for</strong> a live d<strong>on</strong>or, with others still<br />
be<strong>in</strong>g placed <strong>on</strong> a wait<strong>in</strong>g list <strong>for</strong> a deceased d<strong>on</strong>or 181 )<br />
• the l<strong>on</strong>g-term outcome <strong>for</strong> recipients does not appear to be significantly different whether the<br />
kidney came from a paid d<strong>on</strong>or or a liv<strong>in</strong>g related d<strong>on</strong>or<br />
• the regulated market has not reduced altruistic d<strong>on</strong>ati<strong>on</strong>; liv<strong>in</strong>g related d<strong>on</strong>ati<strong>on</strong> rates have<br />
rema<strong>in</strong>ed static and altruistic d<strong>on</strong>ati<strong>on</strong> after death has <strong>in</strong>creased over this period.<br />
It has also been found, however, that:<br />
• <strong>organ</strong> vendors are disproporti<strong>on</strong>ately impoverished and uneducated<br />
• the data <strong>on</strong> l<strong>on</strong>g-term outcomes <strong>for</strong> <strong>organ</strong> vendors are c<strong>on</strong>flict<strong>in</strong>g and <strong>in</strong>complete.<br />
Hippen, an advocate of such a scheme <strong>for</strong> the United States, suggests that less<strong>on</strong>s can be learned<br />
from the Iranian experience, to <strong>in</strong>troduce an ethical market <strong>in</strong> human <strong>organ</strong>s. He argues that<br />
altruism can persist and even flourish al<strong>on</strong>gside a kidney market, as it does <strong>in</strong> Iran. D<strong>on</strong>ors can still<br />
choose to d<strong>on</strong>ate altruistically and recipients can have the choice of an <strong>organ</strong> from some<strong>on</strong>e who<br />
was paid or who was d<strong>on</strong>at<strong>in</strong>g altruistically. L<strong>on</strong>g-term outcomes would need to be assessed and<br />
this would need to be built <strong>in</strong>to the system and careful attenti<strong>on</strong> would need to be given to the<br />
selecti<strong>on</strong> of vendors and to ensur<strong>in</strong>g that they are properly <strong>in</strong><strong>for</strong>med of the risk. Hippen rejects the<br />
argument that impoverished <strong>in</strong>dividuals are coerced by the offer of a f<strong>in</strong>ancial <strong>in</strong>centive <strong>on</strong> the<br />
grounds that ‘an offer cannot be coercive if the relati<strong>on</strong>ship is <strong>in</strong>itiated by the pers<strong>on</strong> <strong>in</strong> danger of<br />
be<strong>in</strong>g coerced’. 182<br />
Ethical c<strong>on</strong>siderati<strong>on</strong>s<br />
Central to the debate about permitt<strong>in</strong>g a regulated market are arguments around c<strong>on</strong>sent,<br />
coerci<strong>on</strong> and exploitati<strong>on</strong>. It is argued that aut<strong>on</strong>omous <strong>in</strong>dividuals should be free to do whatever<br />
they wish with their own bodily material, <strong>in</strong>clud<strong>in</strong>g sell<strong>in</strong>g it, provided that they are sufficiently<br />
<strong>in</strong><strong>for</strong>med, have given c<strong>on</strong>sent and are not harm<strong>in</strong>g any<strong>on</strong>e else. Society does not usually prevent<br />
<strong>in</strong>dividuals from mak<strong>in</strong>g their own decisi<strong>on</strong>s about <strong>where</strong> the balance of benefits and harms lies<br />
<strong>for</strong> them. Prohibit<strong>in</strong>g payment, <strong>in</strong> the absence of significant harm to the <strong>in</strong>dividual or others, could<br />
there<strong>for</strong>e be seen to <strong>in</strong>fr<strong>in</strong>ge the freedom and aut<strong>on</strong>omy of <strong>in</strong>dividuals. Kidney d<strong>on</strong>ati<strong>on</strong> <strong>in</strong>volves<br />
major surgery with a small, but <strong>in</strong>herent, risk of harm. The fear is that the people who are more<br />
likely to take up the opti<strong>on</strong> of sell<strong>in</strong>g <strong>organ</strong>s are those who are poor, impoverished or <strong>in</strong> serious<br />
f<strong>in</strong>ancial difficulties and who have few, if any, other opti<strong>on</strong>s. Essentially, those who need the<br />
m<strong>on</strong>ey will be more likely to expose themselves to these risks and may be tempted to dismiss<br />
or m<strong>in</strong>imise any c<strong>on</strong>cerns they have about it <strong>in</strong> order to ga<strong>in</strong> the m<strong>on</strong>ey they need. This raises<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 57
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
the scenario of d<strong>on</strong>ors act<strong>in</strong>g c<strong>on</strong>trary to their better judgement because of their f<strong>in</strong>ancial<br />
circumstances and the f<strong>in</strong>ancial <strong>in</strong>centive offered, lead<strong>in</strong>g to claims of exploitati<strong>on</strong> and coerci<strong>on</strong>.<br />
Although the offer of an <strong>in</strong>centive is not, <strong>in</strong> itself, exploitative, <strong>in</strong>dividuals may be exploited if,<br />
under different f<strong>in</strong>ancial circumstances, or with full <strong>in</strong><strong>for</strong>mati<strong>on</strong>, they would not have chosen<br />
to d<strong>on</strong>ate. Arguably, however, the coerci<strong>on</strong> <strong>in</strong> such cases is caused by their f<strong>in</strong>ancial situati<strong>on</strong>;<br />
prohibit<strong>in</strong>g payment <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> will not improve their situati<strong>on</strong> and limits the opti<strong>on</strong>s open to<br />
them. The idea that adults with capacity need to be protected from mak<strong>in</strong>g the ‘wr<strong>on</strong>g’ decisi<strong>on</strong>s<br />
by restrict<strong>in</strong>g the opti<strong>on</strong>s open to them has been challenged <strong>in</strong> other areas, <strong>in</strong>clud<strong>in</strong>g <strong>in</strong> the debate<br />
around women participat<strong>in</strong>g <strong>in</strong> egg-shar<strong>in</strong>g arrangements. 183 If people c<strong>on</strong>sider that sell<strong>in</strong>g an<br />
<strong>organ</strong> is the best opti<strong>on</strong> <strong>for</strong> them, and there are safeguards built <strong>in</strong>to the system so that the risks<br />
and payments are c<strong>on</strong>trolled and the rich cannot pay <strong>for</strong> preferential treatment at the expense<br />
of the poor, are there legitimate grounds to prevent <strong>in</strong>dividuals from tak<strong>in</strong>g this acti<strong>on</strong>? The<br />
Internati<strong>on</strong>al Forum <strong>for</strong> Transplant Ethics has po<strong>in</strong>ted out that vendors themselves are will<strong>in</strong>g to<br />
sell their <strong>organ</strong>s and see this as the best opti<strong>on</strong> open to them; their positi<strong>on</strong> may be worse if the<br />
opti<strong>on</strong> of sell<strong>in</strong>g a kidney is removed from them. They argue that:<br />
‘[i]f the rich are free to engage <strong>in</strong> dangerous sports <strong>for</strong> pleasure, or dangerous jobs <strong>for</strong> high<br />
pay, it is difficult to see why the poor who take the lesser risk of kidney sell<strong>in</strong>g <strong>for</strong> greater<br />
rewards – perhaps sav<strong>in</strong>g relatives’ lives – should be thought so misguided as to need<br />
sav<strong>in</strong>g from themselves.’ 184<br />
A further ethical c<strong>on</strong>siderati<strong>on</strong> stems from the ancient professi<strong>on</strong>al obligati<strong>on</strong> to <strong>in</strong>tervene <strong>on</strong>ly <strong>for</strong><br />
a patient’s net benefit and to impose harm or risk of harm <strong>on</strong>ly <strong>for</strong> the <strong>in</strong>tended net benefit of the<br />
patient. While it is widely accepted that, with appropriate c<strong>on</strong>sent, m<strong>in</strong>imal harm may be imposed<br />
by doctors <strong>for</strong> the benefit of others, c<strong>on</strong>temporary as well as ancient medical ethics would draw<br />
the l<strong>in</strong>e at impos<strong>in</strong>g substantial harm <strong>for</strong> the benefit of others, even if appropriate c<strong>on</strong>sent were<br />
given. D<strong>on</strong>ati<strong>on</strong> of a heart <strong>for</strong> the benefit of a loved <strong>on</strong>e would be an obvious example. In the<br />
case of kidney d<strong>on</strong>ati<strong>on</strong>, however, this c<strong>on</strong>cern would apply equally to unpaid liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> as to<br />
paid d<strong>on</strong>ati<strong>on</strong>. The current acceptance of liv<strong>in</strong>g kidney d<strong>on</strong>ati<strong>on</strong> implies that the level of harm and<br />
risk of harm <strong>for</strong> d<strong>on</strong>ors is morally acceptable whether paid or unpaid. C<strong>on</strong>versely, if the level of<br />
harm to paid kidney d<strong>on</strong>ors is too great to be ethically acceptable then the same c<strong>on</strong>clusi<strong>on</strong><br />
should exclude unpaid kidney d<strong>on</strong>ors.<br />
Mov<strong>in</strong>g from a system based <strong>on</strong> altruism to <strong>on</strong>e based <strong>on</strong> commerce, however, would represent<br />
a fundamental shift, rais<strong>in</strong>g the questi<strong>on</strong> of whether altruism is a ‘good’ <strong>in</strong> itself which we should<br />
strive to ma<strong>in</strong>ta<strong>in</strong> irrespective of the practical outcome of that shift. The Nuffield Council <strong>on</strong><br />
Bioethics stresses the importance of altruism ‘as underp<strong>in</strong>n<strong>in</strong>g important communal values that<br />
express someth<strong>in</strong>g very significant about the k<strong>in</strong>d of society <strong>in</strong> which we would wish medic<strong>in</strong>e<br />
and research to flourish.’ 185 There is also a pr<strong>in</strong>cipled argument that d<strong>on</strong>ati<strong>on</strong> and altruism are<br />
central to the NHS, which operates the <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> system. If we accept a move to commerce<br />
<strong>in</strong> this area, this could be viewed as <strong>on</strong>e step towards an overall reducti<strong>on</strong> <strong>in</strong> altruism <strong>in</strong> society,<br />
with people less will<strong>in</strong>g to help others unless there is some pers<strong>on</strong>al ga<strong>in</strong>. It has been argued <strong>for</strong><br />
58<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
example, that if a f<strong>in</strong>ancial motivati<strong>on</strong> is <strong>in</strong>troduced ‘the value of d<strong>on</strong>ati<strong>on</strong> would be underm<strong>in</strong>ed,<br />
because it would no l<strong>on</strong>ger stand <strong>for</strong> selfless motivati<strong>on</strong> or sacrifice <strong>on</strong> the part of the d<strong>on</strong>or, and<br />
nor would it express a sense of shared obligati<strong>on</strong>, of solidarity, to provide that which is essential<br />
<strong>for</strong> life or health’. 186 L<strong>in</strong>ked to this is c<strong>on</strong>cern about the way we perceive ourselves and others as<br />
human be<strong>in</strong>gs. Allow<strong>in</strong>g payment <strong>for</strong> an <strong>organ</strong> can be seen as treat<strong>in</strong>g that part of our bodies as<br />
a mere commodity to be traded. This could be seen to underm<strong>in</strong>e the noti<strong>on</strong> of human dignity<br />
and the moral obligati<strong>on</strong> to show respect <strong>for</strong> pers<strong>on</strong>s.<br />
Practical c<strong>on</strong>siderati<strong>on</strong>s<br />
Prop<strong>on</strong>ents have suggested that <strong>in</strong>troduc<strong>in</strong>g a regulated market <strong>in</strong> human <strong>organ</strong>s would be a<br />
pragmatic soluti<strong>on</strong> to the serious problem of the lack of <strong>organ</strong>s which is result<strong>in</strong>g <strong>in</strong> unnecessary<br />
deaths. We may c<strong>on</strong>sider voluntary d<strong>on</strong>ati<strong>on</strong>, with its emphasis <strong>on</strong> altruism, human dignity and<br />
m<strong>in</strong>imisati<strong>on</strong> of exploitati<strong>on</strong>, as far preferable. If that fails to ma<strong>in</strong>ta<strong>in</strong> supply, however, as a society<br />
a decisi<strong>on</strong> is needed about whether to uphold the pr<strong>in</strong>ciple of altruism and accept the<br />
c<strong>on</strong>sequences or to take a more pragmatic approach and take steps, such as the use of payment<br />
or <strong>in</strong>centives, to meet the shortfall. Some would argue that given the benefits that accrue from<br />
d<strong>on</strong>ati<strong>on</strong>, payment (if it were found to <strong>in</strong>crease d<strong>on</strong>ati<strong>on</strong>s) may be justified <strong>on</strong> utilitarian grounds.<br />
The c<strong>on</strong>sequence of not ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g the supply of <strong>organ</strong>s is not simply the unnecessary loss of life.<br />
It is well known that some patients, <strong>in</strong> desperati<strong>on</strong>, use unlawful, unregulated and sometimes<br />
unsafe arrangements <strong>in</strong> other countries. This not <strong>on</strong>ly puts their life at risk but also has a knock-<strong>on</strong><br />
effect <strong>on</strong> others, when limited NHS resources are required to deal with the c<strong>on</strong>sequences. A<br />
patient who was not at the top of the wait<strong>in</strong>g list <strong>for</strong> a transplant would, n<strong>on</strong>etheless, receive<br />
urgent medical treatment <strong>for</strong> complicati<strong>on</strong>s aris<strong>in</strong>g from sub-standard surgery undertaken <strong>in</strong> other<br />
countries. From the d<strong>on</strong>or’s perspective, it has been suggested that the c<strong>on</strong>t<strong>in</strong>ued shortage of<br />
<strong>organ</strong>s <strong>in</strong> developed countries, and the failure to take acti<strong>on</strong> to address it, provides a market <strong>for</strong>,<br />
and thus susta<strong>in</strong>s, the harmful and clearly exploitative practice of traffick<strong>in</strong>g <strong>organ</strong>s from<br />
develop<strong>in</strong>g countries. 187 Introduc<strong>in</strong>g an ethical market <strong>in</strong> <strong>organ</strong>s, it is suggested, may there<strong>for</strong>e help<br />
to prevent the greater harms of traffick<strong>in</strong>g as well as address<strong>in</strong>g the urgent need <strong>for</strong> more d<strong>on</strong>ors.<br />
One of the practical arguments that is frequently used aga<strong>in</strong>st payment <strong>for</strong> <strong>organ</strong>s is that paid<br />
d<strong>on</strong>ors would transmit more diseases than voluntary d<strong>on</strong>ors because of the type of pers<strong>on</strong> the<br />
payment would attract and the possibility that they would lie about any illnesses or risk factors <strong>in</strong><br />
order to get the m<strong>on</strong>ey. Data from blood d<strong>on</strong>ati<strong>on</strong> surveys appear to add weight to the argument<br />
that, at a global level, <strong>in</strong>centives might affect the quality of the d<strong>on</strong>ati<strong>on</strong> or lead to more potential<br />
d<strong>on</strong>ors be<strong>in</strong>g rejected <strong>for</strong> blood d<strong>on</strong>ati<strong>on</strong>. The World Health Organizati<strong>on</strong>’s 2007 Blood Safety<br />
Survey found that d<strong>on</strong>ors who gave blood voluntarily, and <strong>for</strong> altruistic reas<strong>on</strong>s, had the lowest<br />
prevalence of HIV, hepatitis viruses and other blood-borne <strong>in</strong>fecti<strong>on</strong>s, as compared to people who<br />
d<strong>on</strong>ate <strong>for</strong> family members or <strong>in</strong> return <strong>for</strong> payment. 188 In practice, however, with rout<strong>in</strong>e screen<strong>in</strong>g<br />
of d<strong>on</strong>ors <strong>for</strong> communicable disease it is unclear how big an issue this would be <strong>in</strong> the UK although<br />
it may still be a problem <strong>in</strong> countries that are not able to undertake full screen<strong>in</strong>g. One effect <strong>in</strong><br />
the UK, however, could be that more potential d<strong>on</strong>ors are rejected because of <strong>in</strong>fectious diseases<br />
and there<strong>for</strong>e the expected <strong>in</strong>crease <strong>in</strong> actual d<strong>on</strong>ors could be smaller than anticipated.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 59
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
Any payment <strong>for</strong> <strong>organ</strong>s, from liv<strong>in</strong>g or deceased d<strong>on</strong>ors, is specifically prohibited by the EU<br />
Organs Directive, which the UK has signed up to. It limits reimbursement to that which is ‘strictly<br />
limited to mak<strong>in</strong>g good the expenses and loss of <strong>in</strong>come related to the d<strong>on</strong>ati<strong>on</strong>’ 189 (This c<strong>on</strong>trasts<br />
with the EU Tissues and Cells Directive – which applies, <strong>for</strong> example, to gamete (egg or sperm)<br />
d<strong>on</strong>ati<strong>on</strong> – which also permits payment to make good ‘<strong>in</strong>c<strong>on</strong>veniences related to the d<strong>on</strong>ati<strong>on</strong>’.)<br />
Public op<strong>in</strong>i<strong>on</strong><br />
A survey of third-year medical students <strong>in</strong> Switzerland found that 27% would c<strong>on</strong>sider sell<strong>in</strong>g a<br />
kidney but 73% would not, under any circumstances. Of those who would c<strong>on</strong>sider sell<strong>in</strong>g, 66%<br />
would sell <strong>on</strong>ly to overcome a particularly difficult f<strong>in</strong>ancial situati<strong>on</strong>. 190 In this study, the median<br />
amount of m<strong>on</strong>ey expected <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> of a kidney was £20,500. In a 2004 survey of the<br />
Scottish public <strong>on</strong>ly 24% said the offer of payment <strong>for</strong> liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> would make them more<br />
likely to d<strong>on</strong>ate (51% said it would make no difference and 21% said it would make them less<br />
likely to do so). 191 The author po<strong>in</strong>ts out, however, that payment of <strong>on</strong>ly £2,000 was suggested<br />
and the results may have been different had the figure been higher. (Figures of up to £100,000<br />
have been suggested. 192 )<br />
<strong>BMA</strong> view<br />
The <strong>BMA</strong> believes that <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> should be a gift, freely and voluntarily given and does<br />
not support <strong>in</strong>centives or direct payment <strong>for</strong> d<strong>on</strong>ati<strong>on</strong>. The shift away from altruism and social<br />
solidarity <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> could have a broader impact <strong>on</strong> societal attitudes and c<strong>on</strong>tribute to<br />
an overall reducti<strong>on</strong> <strong>in</strong> altruism with<strong>in</strong> UK society. In additi<strong>on</strong>, liv<strong>in</strong>g kidney d<strong>on</strong>ati<strong>on</strong> carries a small<br />
but significant health risk; <strong>in</strong>troduc<strong>in</strong>g payment could lead to d<strong>on</strong>ors feel<strong>in</strong>g compelled to take<br />
these risks, c<strong>on</strong>trary to their better judgement, because of their f<strong>in</strong>ancial situati<strong>on</strong>.<br />
Payment of funeral expenses<br />
The offer of f<strong>in</strong>ancial <strong>in</strong>centives <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> has also been proposed as a way of <strong>in</strong>creas<strong>in</strong>g<br />
the number of deceased d<strong>on</strong>ors. In its report, Human bodies: d<strong>on</strong>ati<strong>on</strong> <strong>for</strong> medic<strong>in</strong>e and research, 193<br />
the Nuffield Council <strong>on</strong> Bioethics advocates a system <strong>where</strong>by the NHS offers to meet the funeral<br />
expenses of those people who sign up to the Organ D<strong>on</strong>or Register dur<strong>in</strong>g their lifetime and<br />
subsequently become d<strong>on</strong>ors. This is based <strong>on</strong> the system <strong>in</strong> place <strong>for</strong> those who d<strong>on</strong>ate their<br />
bodies to medical schools <strong>for</strong> educati<strong>on</strong>al purposes <strong>where</strong> cremati<strong>on</strong> fees are often paid. In these<br />
cases a medical school arrang<strong>in</strong>g cremati<strong>on</strong> is seen as an acknowledgement of the d<strong>on</strong>or’s<br />
c<strong>on</strong>tributi<strong>on</strong> to medical science and teach<strong>in</strong>g and has not proved c<strong>on</strong>troversial (although it is not<br />
clear how aware people are of this arrangement). The Nuffield Council proposes that payment of<br />
funeral expenses would similarly be seen as recogniti<strong>on</strong> of the c<strong>on</strong>tributi<strong>on</strong> a pers<strong>on</strong> and his or her<br />
family have made <strong>in</strong> allow<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> to proceed. The offer of funeral expenses may also act as<br />
a trigger to important c<strong>on</strong>versati<strong>on</strong>s with<strong>in</strong> families which would remove uncerta<strong>in</strong>ty around<br />
d<strong>on</strong>ati<strong>on</strong> and, <strong>in</strong> turn, help families to fulfil their loved <strong>on</strong>e’s wishes. Although it is not widely<br />
reported, and few details are available, a c<strong>on</strong>tributi<strong>on</strong> towards funeral expenses is offered to <strong>organ</strong><br />
d<strong>on</strong>ors <strong>in</strong> some regi<strong>on</strong>s <strong>in</strong> Spa<strong>in</strong>. 194 Payment to families <strong>for</strong> d<strong>on</strong>ors’ burial costs also <strong>for</strong>med part<br />
of the Israeli <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> law which came <strong>in</strong>to <strong>for</strong>ce <strong>in</strong> 2010 (see above).<br />
60<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
Evidence of effectiveness<br />
The Nuffield Council’s report acknowledges that there is no evidence of the effectiveness of its<br />
suggesti<strong>on</strong> and so proposes a pilot study <strong>in</strong> order to assess both public acceptance and its ability<br />
to c<strong>on</strong>tribute to <strong>in</strong>creased d<strong>on</strong>ati<strong>on</strong> rates. An analysis of the impact of this model <strong>in</strong> Spa<strong>in</strong>,<br />
undertaken some years ago by the Director of Organización Naci<strong>on</strong>al de Trasplantes (ONT), found<br />
no evidence that it led to <strong>in</strong>creased d<strong>on</strong>ati<strong>on</strong> rates although there are no published data about<br />
this. 195 At the time of writ<strong>in</strong>g there has been no published analysis of the impact of this provisi<strong>on</strong><br />
<strong>in</strong> the Israeli law.<br />
The outcome measures <strong>for</strong> a pilot scheme would need to be carefully c<strong>on</strong>sidered and structured<br />
<strong>in</strong> order to obta<strong>in</strong> mean<strong>in</strong>gful results. It would be difficult, <strong>for</strong> example, to identify an <strong>in</strong>crease <strong>in</strong><br />
relatives’ authorisati<strong>on</strong> because the refusal rate, <strong>where</strong> the <strong>in</strong>dividual is <strong>on</strong> the ODR, is <strong>on</strong>ly 6% so<br />
it would take a l<strong>on</strong>g time and would need to be a wide pilot area <strong>for</strong> enough cases to be <strong>in</strong>cluded<br />
to identify a statistically significant difference. Another outcome could be <strong>in</strong>creased d<strong>on</strong>or<br />
registrati<strong>on</strong>s, or the rate of <strong>in</strong>crease be<strong>for</strong>e and after the scheme is announced but, as menti<strong>on</strong>ed<br />
above, there is not a direct correlati<strong>on</strong> between the number <strong>on</strong> the register and the number of<br />
deceased <strong>organ</strong> d<strong>on</strong>ors. Another opti<strong>on</strong> would be to c<strong>on</strong>duct follow-up <strong>in</strong>terviews with relatives<br />
and the request<strong>in</strong>g staff to see what impact the availability of funeral expenses makes.<br />
Ethical c<strong>on</strong>siderati<strong>on</strong>s<br />
Many of the c<strong>on</strong>cerns that are raised <strong>in</strong> relati<strong>on</strong> to provid<strong>in</strong>g <strong>in</strong>centives <strong>for</strong> liv<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ors –<br />
around c<strong>on</strong>sent, coerci<strong>on</strong> and exploitati<strong>on</strong> (see above) – do not apply <strong>where</strong> the benefit is received<br />
after death. The d<strong>on</strong>or is not undertak<strong>in</strong>g any risk and does not benefit pers<strong>on</strong>ally from the m<strong>on</strong>ey.<br />
Whilst this represents a shift from the current system, which is based solely <strong>on</strong> noti<strong>on</strong>s of the<br />
comm<strong>on</strong> good (<strong>where</strong> the benefit is to unknown others), it can be argued that it n<strong>on</strong>etheless<br />
reta<strong>in</strong>s an altruistic focus because the acti<strong>on</strong> (ie sign<strong>in</strong>g up to the ODR) is still motivated by a<br />
desire to benefit others – the d<strong>on</strong>or’s family and heirs who will benefit from the payment after the<br />
<strong>in</strong>dividual’s death, as well as potential recipients of the <strong>organ</strong>s. Although not suggested by the<br />
Nuffield Council <strong>on</strong> Bioethics, the altruistic nature of the system could be <strong>in</strong>creased further by<br />
offer<strong>in</strong>g families the opti<strong>on</strong> of d<strong>on</strong>at<strong>in</strong>g the m<strong>on</strong>ey to a charity of their choice, if they felt they<br />
did not need the m<strong>on</strong>ey to cover the costs of the funeral.<br />
The Nuffield Council <strong>on</strong> Bioethics uses a ‘ladder of <strong>in</strong>terventi<strong>on</strong>’ as a tool to analyse various ways<br />
of promot<strong>in</strong>g and encourag<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong>. It sets out six levels of <strong>in</strong>terventi<strong>on</strong>:<br />
1. provid<strong>in</strong>g <strong>in</strong><strong>for</strong>mati<strong>on</strong> about the need <strong>for</strong> d<strong>on</strong>ati<strong>on</strong><br />
2. recogniti<strong>on</strong> of, and gratitude <strong>for</strong>, d<strong>on</strong>ati<strong>on</strong><br />
3. removal of barriers to d<strong>on</strong>ati<strong>on</strong> am<strong>on</strong>gst those already <strong>in</strong>cl<strong>in</strong>ed to d<strong>on</strong>ate<br />
4. an additi<strong>on</strong>al prompt or encouragement <strong>for</strong> those already <strong>in</strong>cl<strong>in</strong>ed to d<strong>on</strong>ate<br />
5. benefits <strong>in</strong> k<strong>in</strong>d to encourage those who would not otherwise d<strong>on</strong>ate<br />
6. f<strong>in</strong>ancial <strong>in</strong>centives that leave people better off by their decisi<strong>on</strong> to d<strong>on</strong>ate.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 61
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
It refers to levels 1-4 as ‘altruist-focused <strong>in</strong>terventi<strong>on</strong>s’ which act to ‘remove dis<strong>in</strong>centives from, or<br />
provide a spur to, those already <strong>in</strong>cl<strong>in</strong>ed to d<strong>on</strong>ate’ and to levels 5 and 6 as ‘n<strong>on</strong>-altruist-focused<br />
<strong>in</strong>terventi<strong>on</strong>s’ <strong>where</strong> ‘the reward offered to the potential d<strong>on</strong>or is <strong>in</strong>tended al<strong>on</strong>e to be sufficient<br />
to prompt acti<strong>on</strong>’. 196 The report makes clear that the step from altruist-focused to n<strong>on</strong>-altruistfocused<br />
<strong>in</strong>terventi<strong>on</strong>s should not necessarily be seen as mov<strong>in</strong>g from ethical to unethical although<br />
n<strong>on</strong>-altruist-focused <strong>in</strong>terventi<strong>on</strong>s may require more careful c<strong>on</strong>siderati<strong>on</strong>.<br />
A regulated market, as discussed <strong>in</strong> the preced<strong>in</strong>g secti<strong>on</strong>, would clearly be a level 6 <strong>in</strong>terventi<strong>on</strong>.<br />
The Nuffield Council suggests that the offer of funeral expenses to family members could be<br />
viewed as a level 4 <strong>in</strong>terventi<strong>on</strong>, act<strong>in</strong>g as an additi<strong>on</strong>al prompt to those who are already <strong>in</strong>cl<strong>in</strong>ed<br />
to d<strong>on</strong>ate, but acknowledges that it could be placed higher up the ladder. 197 It could be argued,<br />
<strong>for</strong> example, that the payment of funeral expenses is a f<strong>in</strong>ancial <strong>in</strong>centive that leaves people better<br />
off by their decisi<strong>on</strong> to allow d<strong>on</strong>ati<strong>on</strong> to proceed – a level 6 <strong>in</strong>terventi<strong>on</strong>. Or, it could be seen as<br />
a benefit <strong>in</strong> k<strong>in</strong>d (level 5 <strong>in</strong>terventi<strong>on</strong>) although it might be said that offer<strong>in</strong>g benefits <strong>in</strong> k<strong>in</strong>d <strong>for</strong><br />
someth<strong>in</strong>g that is a necessity – such as funeral expenses – is equivalent to giv<strong>in</strong>g m<strong>on</strong>ey, <strong>where</strong>as<br />
a benefit <strong>in</strong> k<strong>in</strong>d that is <strong>for</strong> a luxury or opti<strong>on</strong>al item is not.<br />
In any event, us<strong>in</strong>g this mechanism the Nuffield Council c<strong>on</strong>cludes that ‘[s]ystems based <strong>on</strong> altruism<br />
and systems <strong>in</strong>volv<strong>in</strong>g some <strong>for</strong>m of payment are not necessarily <strong>in</strong>compatible’ 198 even though they<br />
are normally seen as oppos<strong>in</strong>g approaches.<br />
The <strong>BMA</strong> agrees that an <strong>in</strong>dividual d<strong>on</strong>or’s motivati<strong>on</strong> could, under such a scheme, be both altruistic<br />
and f<strong>in</strong>ancial, and that the system would still be based <strong>on</strong> altruism – <strong>in</strong> terms of be<strong>in</strong>g motivated<br />
by a desire to benefit others (<strong>in</strong>clud<strong>in</strong>g the f<strong>in</strong>ancial positi<strong>on</strong> of <strong>on</strong>e’s relatives). Nevertheless, there<br />
would be a shift away from pure altruism <strong>in</strong> the sense of an act of social solidarity, <strong>where</strong> the<br />
motivati<strong>on</strong> is to help unknown recipients, to <strong>on</strong>e <strong>where</strong> the motivati<strong>on</strong> is to provide f<strong>in</strong>ancial<br />
benefit to specific members of <strong>on</strong>e’s family and heirs. The noti<strong>on</strong> of d<strong>on</strong>at<strong>in</strong>g to strangers as a<br />
comm<strong>on</strong> good, which is <strong>in</strong>herent <strong>in</strong> the current system, engenders c<strong>on</strong>siderable public support. It<br />
is unclear whether this type of shift <strong>in</strong> the c<strong>on</strong>cept of altruism would affect this support, but there<br />
is a risk that <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> might <strong>in</strong>creas<strong>in</strong>gly be seen as less of a ‘worthy cause’ if part of the<br />
motivati<strong>on</strong> is to benefit <strong>on</strong>e’s own family rather than to benefit society more generally. D<strong>on</strong>at<strong>in</strong>g<br />
<strong>organ</strong>s after death is seen as a good and positive th<strong>in</strong>g that people choose to do out of a sense<br />
of moral duty or a genu<strong>in</strong>e c<strong>on</strong>cern <strong>for</strong> other members of society. This public recogniti<strong>on</strong> of the<br />
selfless act of d<strong>on</strong>ati<strong>on</strong> could be damaged <strong>in</strong> a system that offers f<strong>in</strong>ancial reward to the d<strong>on</strong>or’s<br />
family, even <strong>where</strong> those rewards are decl<strong>in</strong>ed or, <strong>where</strong> accepted, were not the d<strong>on</strong>or’s pr<strong>in</strong>cipal<br />
motivati<strong>on</strong>. On a societal level, however, the system could be particularly beneficial <strong>for</strong> the poor,<br />
who are most anxious about cover<strong>in</strong>g their funeral costs, and so could be seen as another <strong>for</strong>m<br />
of solidarity.<br />
There is no empirical evidence about the likely effect of shift<strong>in</strong>g to a system <strong>where</strong> motivati<strong>on</strong> is<br />
based <strong>on</strong> both altruism and reward. It is possible that those who currently feel a str<strong>on</strong>g moral<br />
obligati<strong>on</strong> to d<strong>on</strong>ate <strong>organ</strong>s after death <strong>for</strong> the benefit of others may feel their gift is underm<strong>in</strong>ed<br />
<strong>in</strong> some way by the offer of payment. Those who do not qualify <strong>for</strong> the reward (because their<br />
62<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
loved <strong>on</strong>e had not signed up to the register <strong>for</strong> example) may feel less moral compulsi<strong>on</strong> to<br />
c<strong>on</strong>sent and could possibly even feel aggrieved that others are receiv<strong>in</strong>g payment <strong>for</strong> d<strong>on</strong>ati<strong>on</strong><br />
when they are not. Such reacti<strong>on</strong> is not <strong>in</strong>evitable, however, and those who are already motivated<br />
to d<strong>on</strong>ate but, <strong>for</strong> reas<strong>on</strong>s of apathy have not signed up to the ODR, may see the offer of funeral<br />
expenses (and the possibility of benefitt<strong>in</strong>g their family and heirs) as the necessary prompt. Or,<br />
they may view it simply as appropriate public recogniti<strong>on</strong> of their altruistic act.<br />
There is also a broader issue about what, if anyth<strong>in</strong>g, the offer of payment to families <strong>in</strong> return <strong>for</strong><br />
d<strong>on</strong>ated <strong>organ</strong>s would say about our society’s percepti<strong>on</strong> of the importance of social solidarity and<br />
whether, <strong>in</strong> reality, that matters. As a society, we benefit from noti<strong>on</strong>s of ‘the comm<strong>on</strong> good’ and<br />
selflessness. An important c<strong>on</strong>siderati<strong>on</strong> must there<strong>for</strong>e be whether the <strong>in</strong>troducti<strong>on</strong> of payment to<br />
the families of <strong>organ</strong> d<strong>on</strong>ors would represent a significant shift that could underm<strong>in</strong>e noti<strong>on</strong>s of<br />
social solidarity with<strong>in</strong> society or whether it is a small step <strong>in</strong> the directi<strong>on</strong> of commerce, reflect<strong>in</strong>g<br />
the reality of a chang<strong>in</strong>g society <strong>in</strong> which behaviour can be heavily <strong>in</strong>fluenced by <strong>in</strong>centives, whilst<br />
ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g its overall altruistic focus.<br />
Practical c<strong>on</strong>siderati<strong>on</strong>s<br />
Although the report does not go <strong>in</strong>to details, there would need to be a maximum c<strong>on</strong>tributi<strong>on</strong><br />
to prevent <strong>in</strong>dividuals seek<strong>in</strong>g elaborate funerals, way bey<strong>on</strong>d their pers<strong>on</strong>al means, at public<br />
expense. The offer of unlimited funds would be unaf<strong>for</strong>dable and unfair and could tip the balance<br />
significantly <strong>in</strong> favour of people d<strong>on</strong>at<strong>in</strong>g <strong>for</strong> f<strong>in</strong>ancial rather than purely altruistic motives. A moderate,<br />
standard grant towards funeral expenses as a <strong>for</strong>m of public recogniti<strong>on</strong> of the altruistic act of<br />
d<strong>on</strong>ors would be preferable. Even so, with a basic funeral <strong>in</strong> the UK cost<strong>in</strong>g around £2,500 to<br />
£3,000, 199 the cost could be quite significant, rais<strong>in</strong>g legitimate questi<strong>on</strong>s about whether this is the<br />
best use of resources. (On the basis of 1,000 d<strong>on</strong>ors per year, <strong>for</strong> example, of whom 33% were <strong>on</strong><br />
the ODR, the direct cost would be around £1 milli<strong>on</strong>). If it were evident that this would make a<br />
significant difference to d<strong>on</strong>ati<strong>on</strong> rates, it might be cost-effective but much more work is needed<br />
<strong>in</strong> this area.<br />
A relevant factor <strong>in</strong> the cost-benefit analysis is that the system is aimed at encourag<strong>in</strong>g people to<br />
sign up to the Organ D<strong>on</strong>or Register, rather than be<strong>in</strong>g aimed at encourag<strong>in</strong>g families to d<strong>on</strong>ate<br />
<strong>on</strong>ce a relatives’ death has occurred. As menti<strong>on</strong>ed above, there is not a clear correlati<strong>on</strong> between<br />
<strong>in</strong>creas<strong>in</strong>g numbers <strong>on</strong> the ODR and <strong>in</strong>creas<strong>in</strong>g numbers of d<strong>on</strong>ors and so this type of <strong>in</strong>centive<br />
may not produce significant improvements <strong>in</strong> d<strong>on</strong>ati<strong>on</strong> rates, at least <strong>in</strong> the short term. An alternative<br />
would be to offer the grant to any family that agrees to d<strong>on</strong>ati<strong>on</strong> irrespective of whether the<br />
deceased was <strong>on</strong> the ODR. Hav<strong>in</strong>g the type of two-stage approach recommended by the Nuffield<br />
Council, however, provides a level of protecti<strong>on</strong> <strong>for</strong> the patient. If families receive the grant <strong>for</strong><br />
agree<strong>in</strong>g to the d<strong>on</strong>ati<strong>on</strong> of <strong>organ</strong>s, there would be a clear <strong>in</strong>centive <strong>for</strong> the family to authorise<br />
d<strong>on</strong>ati<strong>on</strong> even if they knew that was not what their loved <strong>on</strong>e would have wanted.<br />
The <strong>in</strong>troducti<strong>on</strong> of such a system would also need to be carefully managed to ensure that people<br />
are not given false reassurance. The public generally has very little awareness that the majority of<br />
people do not die <strong>in</strong> situati<strong>on</strong>s <strong>where</strong> they would be able to d<strong>on</strong>ate <strong>organ</strong>s: people who die at<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 63
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
home or at the scene of an accident, or even <strong>on</strong> a general ward <strong>in</strong> hospital, are most unlikely to<br />
be able to d<strong>on</strong>ate solid <strong>organ</strong>s. Others will be unable to d<strong>on</strong>ate <strong>for</strong> medical reas<strong>on</strong>s. Research<br />
shows that around 46% of people have made no f<strong>in</strong>ancial provisi<strong>on</strong> <strong>for</strong> their funeral. 200 If people<br />
believe it is unnecessary to make such provisi<strong>on</strong> because they have signed up to the ODR, this<br />
figure could be much higher.<br />
Thought would also need to be given to whether it is the offer of d<strong>on</strong>ati<strong>on</strong> or the fact of d<strong>on</strong>ati<strong>on</strong><br />
that would trigger payment. If an <strong>in</strong>dividual was <strong>on</strong> the ODR and the family did not object but the<br />
<strong>organ</strong>s, <strong>on</strong>ce retrieved were not suitable <strong>for</strong> d<strong>on</strong>ati<strong>on</strong>, it is unclear whether the d<strong>on</strong>or’s family would<br />
be eligible <strong>for</strong> payment. To make payment c<strong>on</strong>diti<strong>on</strong>al up<strong>on</strong> <strong>organ</strong>s suitable <strong>for</strong> d<strong>on</strong>ati<strong>on</strong> be<strong>in</strong>g<br />
retrieved could be <strong>in</strong>terpreted as payment <strong>for</strong> the <strong>organ</strong>s themselves, rather than a payment <strong>in</strong><br />
recogniti<strong>on</strong> of their d<strong>on</strong>ati<strong>on</strong>. On the other hand, the cost of the system could <strong>in</strong>crease significantly<br />
if the payment were made <strong>on</strong> the basis of the offer of d<strong>on</strong>ati<strong>on</strong>, irrespective of whether d<strong>on</strong>ati<strong>on</strong><br />
proceeded or <strong>organ</strong>s suitable <strong>for</strong> transplantati<strong>on</strong> were received.<br />
Public op<strong>in</strong>i<strong>on</strong><br />
In 2004, the offer of a cash payment of £2,000 <strong>for</strong> funeral costs was <strong>in</strong>cluded <strong>in</strong> a survey of the<br />
Scottish public <strong>on</strong> factors likely to <strong>in</strong>fluence their decisi<strong>on</strong> to d<strong>on</strong>ate. 201 Overall 39% said the offer<br />
would make them more likely to d<strong>on</strong>ate, 49% said it would make no difference and 9% said it<br />
would make them less likely to d<strong>on</strong>ate.<br />
As part of its work <strong>on</strong> d<strong>on</strong>ati<strong>on</strong> the Nuffield Council <strong>on</strong> Bioethics set up a deliberative workshop<br />
with 43 members of the public to establish their views <strong>on</strong> the range of issues under<br />
c<strong>on</strong>siderati<strong>on</strong>. 202 Overall the public expressed str<strong>on</strong>g support <strong>for</strong> altruism <strong>in</strong> d<strong>on</strong>ati<strong>on</strong> and to<br />
the extent that <strong>in</strong>centives were supported, this was limited to those <strong>where</strong> altruism rema<strong>in</strong>ed<br />
the primary reas<strong>on</strong> <strong>for</strong> d<strong>on</strong>ati<strong>on</strong>. Offer<strong>in</strong>g a c<strong>on</strong>tributi<strong>on</strong> towards funeral expenses was seen as<br />
appeal<strong>in</strong>g because it was aimed at help<strong>in</strong>g the family, rather than the <strong>in</strong>dividual, and because<br />
it was seen as recogniti<strong>on</strong> of their c<strong>on</strong>tributi<strong>on</strong> rather than payment per se.<br />
A YouGov survey undertaken <strong>in</strong> the immediate aftermath of the publicati<strong>on</strong> of the Nuffield Council<br />
<strong>on</strong> Bioethics’ report <strong>in</strong> 2011 found mixed views about the general acceptability of the proposal. 203<br />
Of the 2,640 people questi<strong>on</strong>ed, 47% supported the suggesti<strong>on</strong>, 32% were opposed to it and<br />
21% said they did not know. Asked whether they thought it would make people more or less<br />
<strong>in</strong>cl<strong>in</strong>ed to sign up to the ODR, 56% said they thought it would <strong>in</strong>crease registrati<strong>on</strong>s, 1% said it<br />
would decrease registrati<strong>on</strong>s and 32% thought it would make no difference (11% did not know).<br />
Interest<strong>in</strong>gly, however, of those who were not <strong>on</strong> the register, 58% said it would make no difference<br />
to them pers<strong>on</strong>ally (28% said it would make them more likely to do so and 3% less likely).<br />
64<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
<strong>BMA</strong> views<br />
There are undoubtedly ethical issues, practical problems and cost-implicati<strong>on</strong>s of this proposal that<br />
need to be thoroughly <strong>in</strong>vestigated. Nevertheless, the <strong>BMA</strong> does not have major ethical c<strong>on</strong>cerns<br />
about offer<strong>in</strong>g funeral expenses to those <strong>on</strong> the Organ D<strong>on</strong>or Register who go <strong>on</strong> to d<strong>on</strong>ate <strong>organ</strong>s<br />
although we questi<strong>on</strong> the likely effectiveness of such a venture <strong>in</strong> <strong>in</strong>creas<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> rates. Mov<strong>in</strong>g<br />
away from a system based solely <strong>on</strong> altruism would <strong>on</strong>ly be worthwhile if there is good reas<strong>on</strong> to<br />
believe that it will achieve this aim. Whilst recognis<strong>in</strong>g the difficulty of devis<strong>in</strong>g a sufficiently robust<br />
study, if a pilot scheme could be devised that would measure the effectiveness of such a scheme,<br />
this would be worth explor<strong>in</strong>g further. Any research would also need to address public support<br />
and, if possible, the broader implicati<strong>on</strong>s, if any, of <strong>in</strong>troduc<strong>in</strong>g a system based <strong>on</strong> f<strong>in</strong>ancial as<br />
well as altruistic motivati<strong>on</strong>.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 65
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
6 The way <strong>for</strong>ward <strong>for</strong> <strong>policy</strong><br />
What can we learn from Spa<strong>in</strong>?<br />
Spa<strong>in</strong> c<strong>on</strong>sistently has the highest d<strong>on</strong>ati<strong>on</strong> rate <strong>in</strong> the world at around 34-35 d<strong>on</strong>ors per milli<strong>on</strong><br />
populati<strong>on</strong> (compared with 16 <strong>in</strong> the UK). It is there<strong>for</strong>e reas<strong>on</strong>able, when develop<strong>in</strong>g our own<br />
system, to look at the Spanish model to see what less<strong>on</strong>s can be learned.<br />
How does the Spanish system work?<br />
The law <strong>in</strong> Spa<strong>in</strong> permits <strong>organ</strong>s to be taken <strong>for</strong> transplantati<strong>on</strong> with the c<strong>on</strong>sent of the family<br />
or <strong>in</strong> the absence of any known objecti<strong>on</strong> by the deceased. It is technically an opt-out system<br />
although there is no opt-out register and families are relied up<strong>on</strong> to report any objecti<strong>on</strong> to the<br />
transplant co-ord<strong>in</strong>ator. In practice, c<strong>on</strong>sent is sought from relatives and the system there<strong>for</strong>e<br />
operates more <strong>in</strong> l<strong>in</strong>e with an opt-<strong>in</strong> system. 204 D<strong>on</strong>ati<strong>on</strong> rates <strong>in</strong>creased slightly after this legislati<strong>on</strong><br />
was <strong>in</strong>troduced <strong>in</strong> 1979 but did not beg<strong>in</strong> to <strong>in</strong>crease significantly until what has become known<br />
as ‘the Spanish model’ was <strong>in</strong>troduced <strong>in</strong> 1989. The Organización Naci<strong>on</strong>al de Trasplantes (ONT)<br />
was established <strong>in</strong> that year as part of the Spanish Department of Health and undertook a<br />
programme of ‘professi<strong>on</strong>alisati<strong>on</strong>’ of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> through a network of professi<strong>on</strong>als work<strong>in</strong>g<br />
at nati<strong>on</strong>al, regi<strong>on</strong>al and local level. When this programme started there were 25 transplant coord<strong>in</strong>at<strong>in</strong>g<br />
teams, but by 1999 this had <strong>in</strong>creased to 139 with <strong>on</strong>e <strong>in</strong> each hospital with the<br />
potential <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. 205 Most transplant co-ord<strong>in</strong>ators are medically qualified, usually<br />
<strong>in</strong>tensivists, work<strong>in</strong>g part-time <strong>in</strong> the transplant co-ord<strong>in</strong>ator role <strong>for</strong> two to three years at a time<br />
<strong>in</strong> order to avoid ‘burnout’; after this time they return to other jobs. 206<br />
The system is designed to ensure that the transplant co-ord<strong>in</strong>ators feel a sense of <strong>in</strong>volvement and<br />
accountability <strong>for</strong> per<strong>for</strong>mance. They are resp<strong>on</strong>sible <strong>for</strong> all aspects of the <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> process<br />
with<strong>in</strong> the hospital, <strong>in</strong>clud<strong>in</strong>g d<strong>on</strong>or identificati<strong>on</strong> which, given their positi<strong>on</strong><strong>in</strong>g with<strong>in</strong> the ICU,<br />
they are ideally placed to undertake. As part of the Spanish model all professi<strong>on</strong>als directly or<br />
<strong>in</strong>directly <strong>in</strong>volved <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> receive regular tra<strong>in</strong><strong>in</strong>g courses; it has been reported that<br />
s<strong>in</strong>ce 1991 more than 11,000 professi<strong>on</strong>als <strong>in</strong> Spa<strong>in</strong> have undertaken this tra<strong>in</strong><strong>in</strong>g. 207 Communicati<strong>on</strong><br />
with the public is also a large part of the strategy developed by ONT with a 24-hour teleph<strong>on</strong>e<br />
<strong>in</strong><strong>for</strong>mati<strong>on</strong> l<strong>in</strong>e <strong>for</strong> the press, public and professi<strong>on</strong>als <strong>in</strong> order to generate trust <strong>in</strong> the system<br />
and a positive overall view of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>.<br />
Spa<strong>in</strong> is an example of a country that has <strong>in</strong>creased its d<strong>on</strong>or rate, without implement<strong>in</strong>g its optout<br />
law. It is possible that the background of an opt-out system – which potentially leads to a<br />
more positive view of d<strong>on</strong>ati<strong>on</strong> with<strong>in</strong> society – could have had some <strong>in</strong>direct impact <strong>on</strong> the<br />
success of the new model. Abadie and Gay have suggested, <strong>for</strong> example, that the defaults <strong>in</strong><br />
legislati<strong>on</strong> might affect decisi<strong>on</strong>s made by families, even if they are not en<strong>for</strong>ced. 208 It is, however,<br />
generally accepted, <strong>in</strong>clud<strong>in</strong>g by the <strong>BMA</strong>, that Spa<strong>in</strong>’s success is not due to its legislati<strong>on</strong> but its<br />
<strong>organ</strong>isati<strong>on</strong>al model. For many years the UK has been look<strong>in</strong>g to the Spanish model to see how<br />
it could be adapted to the UK situati<strong>on</strong> and a number of the <strong>in</strong>itiatives suggested by the Organ<br />
D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce are based <strong>on</strong> practice <strong>in</strong> Spa<strong>in</strong>. The answer, however, is not simply to adopt<br />
more of the Spanish system. In fact, there are some aspects of the Spanish system that the UK<br />
either could not, or would not wish to, adopt.<br />
Some of Spa<strong>in</strong>’s per<strong>for</strong>mance, compared with the UK, can be put down to differences <strong>in</strong> resources<br />
or cl<strong>in</strong>ical practices between the two countries. These <strong>in</strong>clude: 209<br />
66<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
• the higher number of <strong>in</strong>tensive care beds <strong>in</strong> Spa<strong>in</strong> – 87.5 per milli<strong>on</strong> populati<strong>on</strong> compared<br />
with 27 per milli<strong>on</strong> populati<strong>on</strong> <strong>in</strong> the UK (exclud<strong>in</strong>g cor<strong>on</strong>ary care, ne<strong>on</strong>atal and burns units);<br />
• different admissi<strong>on</strong> criteria <strong>for</strong> ICU – with far fewer beds <strong>in</strong> the UK, those with a poor prognosis,<br />
who are there<strong>for</strong>e more likely to be potential d<strong>on</strong>ors, are less likely to be admitted to ICU;<br />
• end-of-life practices – <strong>in</strong> the UK it is c<strong>on</strong>sidered good practice to withdraw life-susta<strong>in</strong><strong>in</strong>g<br />
treatment be<strong>for</strong>e bra<strong>in</strong> stem tests are carried out if treatment is no l<strong>on</strong>ger benefitt<strong>in</strong>g the<br />
patient, <strong>where</strong>as this is less comm<strong>on</strong> <strong>in</strong> Spa<strong>in</strong>. This results <strong>in</strong> a far lower number of potential<br />
DBD d<strong>on</strong>ors <strong>in</strong> the UK. (Spa<strong>in</strong> has a d<strong>on</strong>or rate of 34-35 per milli<strong>on</strong> populati<strong>on</strong>, 95% of whom<br />
are DBD d<strong>on</strong>ors 210 <strong>where</strong>as the maximum number of potential DBD d<strong>on</strong>ors identified <strong>in</strong> the UK<br />
potential d<strong>on</strong>or audit was 18.4 per milli<strong>on</strong> populati<strong>on</strong>). This situati<strong>on</strong> could change with recent<br />
Spanish legislati<strong>on</strong> <strong>on</strong> withdrawal of life support which could make patient and family requests<br />
to withdraw ventilati<strong>on</strong> more comm<strong>on</strong>. 211<br />
• the use of ‘higher risk d<strong>on</strong>ors’ (see secti<strong>on</strong> 5). In 2009, 45% of Spanish d<strong>on</strong>ors were over 60<br />
years of age, compared with 30% <strong>in</strong> the UK. In 2009 no <strong>organ</strong>s could be transplanted from<br />
206 of the 1,606 d<strong>on</strong>ors (12.8%) <strong>in</strong> Spa<strong>in</strong>. 212<br />
Some aspects of the Spanish system have been subject to criticism although there is a significant<br />
level of ambiguity about how the system works <strong>in</strong> practice, such that it is difficult to know<br />
whether this criticism is justified. If the <strong>in</strong>terpretati<strong>on</strong> is correct there would appear to be some<br />
practices <strong>in</strong> Spa<strong>in</strong> that would c<strong>on</strong>flict with the general culture of care <strong>in</strong> the UK.<br />
• The tra<strong>in</strong><strong>in</strong>g <strong>for</strong> transplant co-ord<strong>in</strong>ators <strong>in</strong>cludes <strong>in</strong><strong>for</strong>m<strong>in</strong>g them how to challenge the most<br />
comm<strong>on</strong> reas<strong>on</strong>s families give <strong>for</strong> refus<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong>. As a result of this the role of the coord<strong>in</strong>ator<br />
has been <strong>in</strong>terpreted as to explicitly and actively ‘persuade’ the family to agree to<br />
d<strong>on</strong>ati<strong>on</strong>.<br />
• Transplant co-ord<strong>in</strong>ators are paid variable amounts based <strong>on</strong> the hours worked and so they are<br />
paid more when there are d<strong>on</strong>ors. This arrangement has been widely <strong>in</strong>terpreted as <strong>in</strong>centive<br />
b<strong>on</strong>us payments <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>, although those resp<strong>on</strong>sible <strong>for</strong> the system have reacted<br />
str<strong>on</strong>gly to ‘ill-<strong>in</strong><strong>for</strong>med’ criticism of this aspect of the Spanish model. In comment<strong>in</strong>g <strong>on</strong> this the<br />
ONT has, n<strong>on</strong>etheless, acknowledged that variable payment is a ‘favourable c<strong>on</strong>diti<strong>on</strong>’ <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong>. 213 It expla<strong>in</strong>s that, unlike <strong>in</strong> other countries, <strong>in</strong> Spa<strong>in</strong> ‘there are many doctors with low<br />
basic pay but with the prospect of a significant <strong>in</strong>crease l<strong>in</strong>ked to objectives.’ 214<br />
• The transplant co-ord<strong>in</strong>ator may also have cl<strong>in</strong>ical resp<strong>on</strong>sibility <strong>for</strong> the patient’s treatment <strong>in</strong><br />
<strong>in</strong>tensive care as well as identify<strong>in</strong>g potential d<strong>on</strong>ors and approach<strong>in</strong>g the family. This could be<br />
perceived as a c<strong>on</strong>flict of <strong>in</strong>terest, particularly if the transplant co-ord<strong>in</strong>ator then receives<br />
additi<strong>on</strong>al payment as a direct result of any d<strong>on</strong>ati<strong>on</strong> that proceeds.<br />
A number of other countries have adapted the Spanish model with great success. Modificati<strong>on</strong>s of<br />
it can be found <strong>in</strong> parts of the United States of America 215 and <strong>in</strong> Italy. 216 In Italy, both <strong>organ</strong>isati<strong>on</strong>al<br />
change, based <strong>on</strong> the Spanish model, and an opt-out system were <strong>in</strong>troduced <strong>in</strong> 1999. It has been<br />
reported that not all regi<strong>on</strong>s implemented both aspects of the legislati<strong>on</strong> but those that showed<br />
the greatest susta<strong>in</strong>ed <strong>in</strong>crease <strong>in</strong> deceased d<strong>on</strong>or activity rates are those that implemented both<br />
structural re<strong>for</strong>m and an opt-out system <strong>for</strong> deceased d<strong>on</strong>ati<strong>on</strong>. 217 The <strong>BMA</strong> has always argued<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 67
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
that an opt-out system al<strong>on</strong>e could not achieve the type of d<strong>on</strong>ati<strong>on</strong> rates we need and that this<br />
must be accompanied, or ideally preceded, by the development of a well-funded, well-<strong>organ</strong>ised<br />
<strong>in</strong>frastructure.<br />
Where <strong>next</strong> <strong>for</strong> public <strong>policy</strong>?<br />
The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce and those who have worked so hard to implement its<br />
recommendati<strong>on</strong>s deserve c<strong>on</strong>gratulati<strong>on</strong>s and c<strong>on</strong>siderable credit <strong>for</strong> their work. For the first time<br />
<strong>in</strong> the UK, the <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> system has been subject to rigorous review with a comprehensive,<br />
radical and logical approach and significant f<strong>in</strong>ancial <strong>in</strong>vestment. The key pr<strong>in</strong>ciple underp<strong>in</strong>n<strong>in</strong>g<br />
the Task<strong>for</strong>ce’s work – that d<strong>on</strong>ati<strong>on</strong> should be a usual part of end-of-life care – has been<br />
translated <strong>in</strong>to practical changes that have made, and will c<strong>on</strong>t<strong>in</strong>ue to make, a significant<br />
difference. Liv<strong>in</strong>g d<strong>on</strong>ati<strong>on</strong> has also c<strong>on</strong>t<strong>in</strong>ued to expand and a strategy has been developed<br />
to promote further growth. These changes will result <strong>in</strong> lives be<strong>in</strong>g saved and trans<strong>for</strong>med.<br />
We have much to celebrate but we cannot af<strong>for</strong>d to be complacent.<br />
The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce believed its re<strong>for</strong>ms would lead to a 50% <strong>in</strong>crease <strong>in</strong> deceased<br />
d<strong>on</strong>ors over the five year period to 2013, tak<strong>in</strong>g the UK to 19.6 d<strong>on</strong>ors per milli<strong>on</strong> populati<strong>on</strong>.<br />
The first three years saw an <strong>in</strong>crease of 25%, and it is projected that this <strong>in</strong>crease will rise to 34%<br />
<strong>in</strong> the fourth year to April 2012. 218 Although good <strong>progress</strong> has been made, it will be a significant<br />
challenge to achieve the target of 50% by 2013. Even if a 50% <strong>in</strong>crease is achieved it will not<br />
solve the problem and people will still be dy<strong>in</strong>g unnecessarily. In its strategic plan <strong>for</strong> 2011-14,<br />
NHS BT acknowledges that with a chang<strong>in</strong>g d<strong>on</strong>or profile, and <strong>in</strong>creas<strong>in</strong>g demand <strong>for</strong> d<strong>on</strong>ati<strong>on</strong>,<br />
‘the need to deliver the targets of the ODTF, and be able to susta<strong>in</strong> further <strong>in</strong>creases bey<strong>on</strong>d the<br />
time period that was set, become even more challeng<strong>in</strong>g’. 219<br />
As a society we need to c<strong>on</strong>sider whether, hav<strong>in</strong>g developed the <strong>in</strong>frastructure, we should be<br />
satisfied that we have d<strong>on</strong>e all we can and accept that we have reached the limit of our potential<br />
<strong>for</strong> d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK, or whether we should seek to build <strong>on</strong> what has already been achieved<br />
by shift<strong>in</strong>g our attenti<strong>on</strong> to additi<strong>on</strong>al ways of <strong>in</strong>creas<strong>in</strong>g the number of <strong>organ</strong> d<strong>on</strong>ors.<br />
In the <strong>BMA</strong>’s view, as l<strong>on</strong>g as more can be d<strong>on</strong>e, more should be d<strong>on</strong>e. We recognise that any<br />
significant <strong>policy</strong> change will <strong>on</strong>ly succeed if it has public and professi<strong>on</strong>al support and must be<br />
pursued carefully. But we must not shy away from this debate. Do<strong>in</strong>g noth<strong>in</strong>g is not a neutral<br />
act. Where lives are at stake a positive decisi<strong>on</strong> not to pursue further ga<strong>in</strong>s is <strong>on</strong>e that needs<br />
justificati<strong>on</strong>. We also cannot keep delay<strong>in</strong>g the issue. Given the significant time that would be<br />
needed to implement any major change, lost time will <strong>in</strong>evitably result <strong>in</strong> lost lives.<br />
We welcome debate <strong>on</strong> the range of possible opti<strong>on</strong>s <strong>in</strong>clud<strong>in</strong>g systems based <strong>on</strong> reciprocity,<br />
mandated choice or the payment of funeral expenses but the <strong>BMA</strong> rema<strong>in</strong>s firmly c<strong>on</strong>v<strong>in</strong>ced that<br />
a system of opt-out with safeguards is the best opti<strong>on</strong> and the <strong>on</strong>e that is most likely to have a<br />
positive effect.<br />
The <strong>BMA</strong> hopes that the publicati<strong>on</strong> of this report will encourage and facilitate debate – am<strong>on</strong>gst<br />
health professi<strong>on</strong>als, <strong>policy</strong>-makers and the public, with a view to reach<strong>in</strong>g broad agreement about<br />
the way <strong>for</strong>ward.<br />
68<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
7 Summary of key po<strong>in</strong>ts<br />
• S<strong>in</strong>ce the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce report was published <strong>in</strong> January 2008 there have been<br />
major changes and significant improvements to the <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> system <strong>in</strong> the UK.<br />
• The latest published data (2010/11) show that over the last three years, d<strong>on</strong>ati<strong>on</strong> rates from<br />
deceased d<strong>on</strong>ors have improved by 25% (compared with 2007/08). More recent data provided<br />
by NHS BT show that the total <strong>in</strong>crease is projected to rise to 34% by April 2012 (based <strong>on</strong><br />
d<strong>on</strong>ors up to 8 January 2012).<br />
• The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce believed that, with the changes it proposed, deceased d<strong>on</strong>or<br />
rates would <strong>in</strong>crease by 50% by 2013. Although good <strong>progress</strong> has been made it will be a<br />
significant challenge to achieve this target.<br />
• Whether or not the target of 50% is reached, people will still be dy<strong>in</strong>g unnecessarily while<br />
wait<strong>in</strong>g <strong>for</strong> an <strong>organ</strong> transplant.<br />
• Work must c<strong>on</strong>t<strong>in</strong>ue to maximise the impact of the changes that have taken place and to<br />
explore further avenues <strong>for</strong> improvement. This will <strong>in</strong>clude <strong>in</strong>creas<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> from<br />
emergency departments, extend<strong>in</strong>g the use of liv<strong>in</strong>g d<strong>on</strong>ors, <strong>in</strong>creas<strong>in</strong>g referrals, attempt<strong>in</strong>g to<br />
reduce the relative refusal rate and targeted campaigns <strong>for</strong> black and ethnic m<strong>in</strong>ority groups.<br />
• As a society we now need to c<strong>on</strong>sider whether, hav<strong>in</strong>g developed the <strong>in</strong>frastructure, we should<br />
be satisfied that we have d<strong>on</strong>e all we can or whether we should seek to build <strong>on</strong> what has<br />
already been achieved by shift<strong>in</strong>g our attenti<strong>on</strong> to additi<strong>on</strong>al ways of <strong>in</strong>creas<strong>in</strong>g the number<br />
of <strong>organ</strong> d<strong>on</strong>ors.<br />
• A range of opti<strong>on</strong>s have been suggested, <strong>in</strong>clud<strong>in</strong>g a system of opt-out with safeguards,<br />
mandated choice, reciprocity or some <strong>for</strong>m of <strong>in</strong>centive or compensati<strong>on</strong> <strong>for</strong> d<strong>on</strong>ors.<br />
• The <strong>BMA</strong> rema<strong>in</strong>s firmly c<strong>on</strong>v<strong>in</strong>ced that a system of opt-out with safeguards is the best opti<strong>on</strong><br />
<strong>for</strong> the UK and the <strong>on</strong>e that is most likely to be effective.<br />
• The <strong>BMA</strong> hopes that this report will encourage and facilitate <strong>in</strong><strong>for</strong>med debate am<strong>on</strong>gst<br />
professi<strong>on</strong>als, <strong>policy</strong>-makers and the public about how we take <strong>for</strong>ward public <strong>policy</strong> <strong>on</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 69
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
References<br />
1 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, p.2.<br />
2 NHS Blood and Transplant (2012) Achiev<strong>in</strong>g the 50% <strong>in</strong>crease <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>,<br />
26 January 2012. NHS BT, Bristol.<br />
3 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) Organs <strong>for</strong> Transplants. A report from the Organ<br />
D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Department of Health, L<strong>on</strong>d<strong>on</strong>, p.2.<br />
4 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, p.9.<br />
5 NHS Blood and Transplant (2011) Strategic Plan 2011-14. NHSBT, Wat<strong>for</strong>d, p.12.<br />
6 25 adults (reported <strong>in</strong> NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK.<br />
Activity Report 2010/11. NHS BT, Bristol, p.13) and 3 paediatric cases (data provided by<br />
NHS BT, 13 January 2012).<br />
7 Human Tissue Act 2004 s 43. Human Tissue (Scotland) Act 2006 s 13.<br />
8 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, p.1.<br />
9 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, p.13.<br />
10 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, p.1.<br />
11 See NHS Blood and Transplant website at: www.<strong>organ</strong>d<strong>on</strong>ati<strong>on</strong>.nhs.uk<br />
(accessed 1 February 2012).<br />
12 Department of Health (2010) Review of the Organ D<strong>on</strong>or Register. Report to the Secretary<br />
of State <strong>for</strong> Health by Professor Sir Gord<strong>on</strong> Duff FRCP, FMedSci, FRSE. DH, L<strong>on</strong>d<strong>on</strong>.<br />
13 NHS Blood and Transplant (2012) Organ D<strong>on</strong>or Register Development, 26 January 2012.<br />
NHS BT, Bristol.<br />
14 NHS Blood and Transplant website: www.<strong>organ</strong>d<strong>on</strong>ati<strong>on</strong>.nhs.uk (accessed 1 February 2012).<br />
15 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, p.78.<br />
16 Council of Europe (2011) Newsletter. Transplant 2011. Council of Europe, Strasbourg, p.4.<br />
17 British Medical Associati<strong>on</strong> (2009) Human Tissue Legislati<strong>on</strong> – Guidance from the <strong>BMA</strong><br />
Medical Ethics Department. <strong>BMA</strong>, L<strong>on</strong>d<strong>on</strong>.<br />
18 Human Tissue Authority (2009) Code of Practice 2 – D<strong>on</strong>ati<strong>on</strong> of solid <strong>organ</strong>s <strong>for</strong><br />
transplantati<strong>on</strong>. HTA, L<strong>on</strong>d<strong>on</strong>.<br />
19 For <strong>in</strong><strong>for</strong>mati<strong>on</strong> about who may give c<strong>on</strong>sent (authorisati<strong>on</strong>) see: British Medical<br />
Associati<strong>on</strong> (2009) Human Tissue Legislati<strong>on</strong> – Guidance from the <strong>BMA</strong> Medical Ethics<br />
Department. <strong>BMA</strong>, L<strong>on</strong>d<strong>on</strong>.<br />
20 Human Tissue Authority (2009) Code of Practice 2 – D<strong>on</strong>ati<strong>on</strong> of solid <strong>organ</strong>s <strong>for</strong><br />
transplantati<strong>on</strong>. HTA, L<strong>on</strong>d<strong>on</strong>, para 100.<br />
21 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol, p.6.<br />
22 Ipsos MORI (2010) HTA General Public Survey. Human Tissue Authority, L<strong>on</strong>d<strong>on</strong> p.4.<br />
23 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, p.3.<br />
24 Human Tissue Act 2004 s 43. Human Tissue (Scotland) Act 2006 s 13.<br />
70<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
25 UK Transplant (2006) UK plans to <strong>in</strong>crease <strong>organ</strong> transplant numbers to new levels. Press<br />
release, 29 November.<br />
26 Cogg<strong>on</strong> J, Brazier M, Murphy P et al. (2008) Best <strong>in</strong>terests and potential <strong>organ</strong> d<strong>on</strong>ors.<br />
BMJ 336, p.1346-7.<br />
27 Directive 2010/53/EU of the European Parliament and of the Council of 7 July 2010 <strong>on</strong><br />
standards of quality and safety of human <strong>organ</strong>s <strong>in</strong>tended <strong>for</strong> transplantati<strong>on</strong>.<br />
28 Department of Health (2011) Tissue authority to set EU transplant standards. Press release,<br />
10 March.<br />
29 Department of Health (2011) Public C<strong>on</strong>sultati<strong>on</strong> <strong>on</strong> Regulati<strong>on</strong>s to Transpose Organ<br />
Directive 2010/53/EU <strong>in</strong>to UK Legislati<strong>on</strong>. DH, L<strong>on</strong>d<strong>on</strong>. Human Tissue Authority (2011)<br />
Public c<strong>on</strong>sultati<strong>on</strong> <strong>on</strong> documentary framework <strong>for</strong> the quality and safety of human <strong>organ</strong>s<br />
<strong>in</strong>tended <strong>for</strong> transplantati<strong>on</strong>. HTA, L<strong>on</strong>d<strong>on</strong>.<br />
30 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) Organs <strong>for</strong> Transplants. A report from the Organ<br />
D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Department of Health, L<strong>on</strong>d<strong>on</strong>.<br />
31 The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce Implementati<strong>on</strong> Programme (2009) Work<strong>in</strong>g together to<br />
save lives. The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce Implementati<strong>on</strong> Programme’s Annual Report,<br />
2008/09. Department of Health, L<strong>on</strong>d<strong>on</strong>, p.12.<br />
32 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce Programme Delivery Board (2011) Work<strong>in</strong>g together to save<br />
lives. The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce Implementati<strong>on</strong> Programme’s F<strong>in</strong>al Report, 2011.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>.<br />
33 Murphy PG, Logan L. (2009) Cl<strong>in</strong>ical leads <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>: mak<strong>in</strong>g it happen <strong>in</strong><br />
hospitals. JICS 10(3), pp.174-8.<br />
34 Murphy PG, Logan L, Aldridge D. (2010) The Professi<strong>on</strong>al Development Programme <strong>for</strong><br />
Cl<strong>in</strong>ical Leads <strong>for</strong> Organ D<strong>on</strong>ati<strong>on</strong>. The Royal College of Anaesthetists’ Bullet<strong>in</strong> 64, pp.22-6.<br />
35 The UK D<strong>on</strong>ati<strong>on</strong> Ethics Committee recommends this safeguard <strong>for</strong> all decisi<strong>on</strong>s to<br />
withdraw life-prol<strong>on</strong>g<strong>in</strong>g medical treatment, whether or not <strong>on</strong>e of the cl<strong>in</strong>icians is the<br />
cl<strong>in</strong>ical lead <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. See: UK D<strong>on</strong>ati<strong>on</strong> Ethics Committee (2011) An ethical<br />
framework <strong>for</strong> c<strong>on</strong>trolled d<strong>on</strong>ati<strong>on</strong> after circulatory death. Academy of Medical Royal<br />
Colleges, L<strong>on</strong>d<strong>on</strong>, para 1.3.2.<br />
36 Logan L, NHS Blood and Transplant, Pers<strong>on</strong>al communicati<strong>on</strong>, 7 November 2011.<br />
37 Logan L, NHS Blood and Transplant, Pers<strong>on</strong>al communicati<strong>on</strong>, 7 November 2011.<br />
38 Turner J, Logan L, McGowan O. (2010) The role of the specialist nurse <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>.<br />
The Royal College of Anaesthetists’ Bullet<strong>in</strong> 64, pp.28-30.<br />
39 Murphy PG. (2008) Trust D<strong>on</strong>ati<strong>on</strong> Committees and Cl<strong>in</strong>ical D<strong>on</strong>ati<strong>on</strong> Champi<strong>on</strong>s – Letter<br />
to Acute Trust Medical Directors, 12 November. NHS BT.<br />
40 Pers<strong>on</strong>al communicati<strong>on</strong> with a range of D<strong>on</strong>ati<strong>on</strong> Committee Chairs and Cl<strong>in</strong>ical Leads,<br />
October-November 2011.<br />
41 Pers<strong>on</strong>al communicati<strong>on</strong> with a range of D<strong>on</strong>ati<strong>on</strong> Committee Chairs and Cl<strong>in</strong>ical Leads,<br />
October-November 2011.<br />
42 Nati<strong>on</strong>al Institute <strong>for</strong> Health and Cl<strong>in</strong>ical Excellence (2011) Organ D<strong>on</strong>ati<strong>on</strong> <strong>for</strong><br />
Transplantati<strong>on</strong>: improv<strong>in</strong>g d<strong>on</strong>or identificati<strong>on</strong> and c<strong>on</strong>sent rates <strong>for</strong> deceased <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong>. NICE cl<strong>in</strong>ical guidel<strong>in</strong>e 135. NICE, L<strong>on</strong>d<strong>on</strong>.<br />
43 Nati<strong>on</strong>al Institute <strong>for</strong> Health and Cl<strong>in</strong>ical Excellence (2011) Organ D<strong>on</strong>ati<strong>on</strong> <strong>for</strong><br />
Transplantati<strong>on</strong>: improv<strong>in</strong>g d<strong>on</strong>or identificati<strong>on</strong> and c<strong>on</strong>sent rates <strong>for</strong> deceased <strong>organ</strong><br />
d<strong>on</strong>ors. NICE cl<strong>in</strong>ical guidel<strong>in</strong>e 135. NICE, L<strong>on</strong>d<strong>on</strong>, para 1.1.2.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 71
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
44 Nati<strong>on</strong>al Institute <strong>for</strong> Health and Cl<strong>in</strong>ical Excellence (2011) Organ D<strong>on</strong>ati<strong>on</strong> <strong>for</strong><br />
Transplantati<strong>on</strong>: improv<strong>in</strong>g d<strong>on</strong>or identificati<strong>on</strong> and c<strong>on</strong>sent rates <strong>for</strong> deceased <strong>organ</strong><br />
d<strong>on</strong>ors. Guidel<strong>in</strong>es appendices. NICE, L<strong>on</strong>d<strong>on</strong>.<br />
45 NHS Blood and Transplant (2011) GIFT- News <strong>for</strong> the <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> and transplantati<strong>on</strong><br />
community. Issue 2, December 2011, NHS BT, Bristol.<br />
46 NHS Blood and Transplant (2010) Nati<strong>on</strong>al Organ Retrieval Service: Commissi<strong>on</strong><strong>in</strong>g Update<br />
(10/07). NHS BT, Bristol.<br />
47 NHS Blood and Transplant (2010) Nati<strong>on</strong>al Standards <strong>for</strong> Organ Retrieval from Deceased<br />
D<strong>on</strong>ors (10/26). NHS BT, Bristol.<br />
48 Data provided by NHS Blood and Transplant, January 2012.<br />
49 NHS Blood and Transplant (2011) M<strong>in</strong>utes of the eighteenth meet<strong>in</strong>g of the NHS Blood and<br />
Transplant Cardiothoracic Advisory Group at 12.30pm <strong>on</strong> Tuesday 15 March 2011 at The<br />
Royal College of Pathologists, L<strong>on</strong>d<strong>on</strong> (CTAG(M)(11)1), para 8.1. Available at:<br />
www.<strong>organ</strong>d<strong>on</strong>ati<strong>on</strong>.nhs.uk (accessed 24 January 2012). See also: NHS Specialised Services<br />
(2011) Nati<strong>on</strong>al Specialised Commissi<strong>on</strong><strong>in</strong>g Priorities, April 2011, pp.13-6. Available at:<br />
www.specialisedservices.nhs.uk (accessed 24 January 2012).<br />
50 Pers<strong>on</strong>al communicati<strong>on</strong> with a number of Cl<strong>in</strong>ical Leads, October-November 2011.<br />
51 Intensive Care Society, British Transplantati<strong>on</strong> Society (2010) D<strong>on</strong>ati<strong>on</strong> after circulatory<br />
death, p.26. Available at: www.bts.org.uk (accessed 30 January 2012).<br />
52 Evans G, NHS Blood and Transplant, Pers<strong>on</strong>al communicati<strong>on</strong>, 19 October 2011.<br />
53 Barber K, Falvey S, Hamilt<strong>on</strong> C et al. (2006) Potential <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the United<br />
K<strong>in</strong>gdom: audit of <strong>in</strong>tensive care records. BMJ 332, pp.1124-6.<br />
54 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, pp.82-9.<br />
55 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol, p.6.<br />
56 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol, p.4.<br />
57 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol, p.3.<br />
58 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol, p.5.<br />
59 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol, p.11.<br />
60 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol.<br />
61 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, pp.82-9.<br />
62 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol, p.3.<br />
63 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol, p.5.<br />
64 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol, p.6.<br />
72<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
65 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol, p.11.<br />
66 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol.<br />
67 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, p.84.<br />
68 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, p.7.<br />
69 Nati<strong>on</strong>al Institute <strong>for</strong> Health and Cl<strong>in</strong>ical Excellence (2011) Organ D<strong>on</strong>ati<strong>on</strong> <strong>for</strong><br />
Transplantati<strong>on</strong>: improv<strong>in</strong>g d<strong>on</strong>or identificati<strong>on</strong> and c<strong>on</strong>sent rates <strong>for</strong> deceased <strong>organ</strong><br />
d<strong>on</strong>ors. NICE cl<strong>in</strong>ical guidel<strong>in</strong>e 135. NICE, L<strong>on</strong>d<strong>on</strong>, para 1.1.2.<br />
70 Academy of Medical Royal Colleges (2008) A code of practice <strong>for</strong> the diagnosis and<br />
c<strong>on</strong>firmati<strong>on</strong> of death. AMRC, L<strong>on</strong>d<strong>on</strong>.<br />
71 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, p.1.<br />
72 Department of Health, Welsh Assembly Government (2009) Legal issues relevant to n<strong>on</strong>heartbeat<strong>in</strong>g<br />
<strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. DH, L<strong>on</strong>d<strong>on</strong>.<br />
73 Burns H. (2010) Guidance <strong>on</strong> legal issues relevant to d<strong>on</strong>ati<strong>on</strong> follow<strong>in</strong>g cardiac death.<br />
(SGHD/CMO(2010)11). The Scottish Government, Ed<strong>in</strong>burgh.<br />
74 Department of Health, Social Services and Public Safety (2011) Legal issues relevant to<br />
d<strong>on</strong>ati<strong>on</strong> after circulatory death (n<strong>on</strong>-heart-beat<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>) <strong>in</strong> Northern Ireland,<br />
DHSSPS, Belfast.<br />
75 UK D<strong>on</strong>ati<strong>on</strong> Ethics Committee (2011) An Ethical Framework <strong>for</strong> C<strong>on</strong>trolled D<strong>on</strong>ati<strong>on</strong> after<br />
Circulatory Death. Academy of Medical Royal Colleges, L<strong>on</strong>d<strong>on</strong>.<br />
76 Intensive Care Society, British Transplantati<strong>on</strong> Society (2010) D<strong>on</strong>ati<strong>on</strong> after circulatory<br />
death. Available at: www.bts.org.uk (accessed 30 January 2012).<br />
77 Department of Health, Welsh Assembly Government (2009) Legal issues relevant to n<strong>on</strong>heartbeat<strong>in</strong>g<br />
<strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. DH, L<strong>on</strong>d<strong>on</strong>.<br />
78 Burns H. (2010) Guidance <strong>on</strong> legal issues relevant to d<strong>on</strong>ati<strong>on</strong> follow<strong>in</strong>g cardiac death.<br />
(SGHD/CMO(2010)11). The Scottish Government, Ed<strong>in</strong>burgh.<br />
79 Department of Health, Social Services and Public Safety (2011) Legal issues relevant to<br />
d<strong>on</strong>ati<strong>on</strong> after circulatory death (n<strong>on</strong>-heart-beat<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>) <strong>in</strong> Northern Ireland.<br />
DHSSPS, Belfast.<br />
80 UK D<strong>on</strong>ati<strong>on</strong> Ethics Committee (2011) An Ethical Framework <strong>for</strong> C<strong>on</strong>trolled D<strong>on</strong>ati<strong>on</strong> after<br />
Circulatory Death. Academy of Medical Royal Colleges, L<strong>on</strong>d<strong>on</strong>.<br />
81 Intensive Care Society, British Transplantati<strong>on</strong> Society (2010) D<strong>on</strong>ati<strong>on</strong> after circulatory<br />
death. Available at: www.bts.org.uk (accessed 30 January 2012).<br />
82 Department of Health (2000) An <strong>in</strong>vestigati<strong>on</strong> <strong>in</strong>to c<strong>on</strong>diti<strong>on</strong>al <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. DH, L<strong>on</strong>d<strong>on</strong>.<br />
83 Human Tissue (Scotland) Act 2006 s 49.<br />
84 Evans G, NHS Blood and Transplant, Pers<strong>on</strong>al communicati<strong>on</strong>, 19 October 2011.<br />
85 Department of Health, Welsh Assembly Government, M<strong>in</strong>istry of Justice (2010) Guidance<br />
<strong>for</strong> d<strong>on</strong>or coord<strong>in</strong>ators – work<strong>in</strong>g with cor<strong>on</strong>ers. DH, L<strong>on</strong>d<strong>on</strong>.<br />
86 Department of Health, Welsh Assembly Government, M<strong>in</strong>istry of Justice (2010) Organ and<br />
Tissue D<strong>on</strong>ati<strong>on</strong>. An aide memoire <strong>for</strong> cor<strong>on</strong>ers. DH, L<strong>on</strong>d<strong>on</strong>.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 73
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
87 British Transplantati<strong>on</strong> Society, Renal Associati<strong>on</strong> (2011) United K<strong>in</strong>gdom Guidel<strong>in</strong>es <strong>for</strong><br />
Liv<strong>in</strong>g D<strong>on</strong>or Kidney Transplantati<strong>on</strong>, 3rd editi<strong>on</strong>. Available at: www.bts.org.uk (accessed 25<br />
January 2012).<br />
88 NHS Blood and Transplant (2012) UK Strategy <strong>for</strong> Liv<strong>in</strong>g D<strong>on</strong>or Kidney Transplantati<strong>on</strong>. NHS<br />
BT, Bristol.<br />
89 NHS Blood and Transplant (2012) Achiev<strong>in</strong>g the 50% <strong>in</strong>crease <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>, 26<br />
January 2012. NHS BT, Bristol.<br />
90 Pers<strong>on</strong>al communicati<strong>on</strong> with a range of D<strong>on</strong>ati<strong>on</strong> Committee Chairs and Cl<strong>in</strong>ical Leads,<br />
October-November 2011.<br />
91 Nati<strong>on</strong>al Institute <strong>for</strong> Health and Cl<strong>in</strong>ical Excellence (2011) Organ D<strong>on</strong>ati<strong>on</strong> <strong>for</strong><br />
Transplantati<strong>on</strong>: improv<strong>in</strong>g d<strong>on</strong>or identificati<strong>on</strong> and c<strong>on</strong>sent rates <strong>for</strong> deceased <strong>organ</strong><br />
d<strong>on</strong>ors. Cl<strong>in</strong>ical guidel<strong>in</strong>e 135: Appendices. NICE, L<strong>on</strong>d<strong>on</strong>, pp.80-1.<br />
92 Nati<strong>on</strong>al Institute <strong>for</strong> Health and Cl<strong>in</strong>ical Excellence (2011) Organ D<strong>on</strong>ati<strong>on</strong> <strong>for</strong><br />
Transplantati<strong>on</strong>: improv<strong>in</strong>g d<strong>on</strong>or identificati<strong>on</strong> and c<strong>on</strong>sent rates <strong>for</strong> deceased <strong>organ</strong><br />
d<strong>on</strong>ors. Cl<strong>in</strong>ical guidel<strong>in</strong>e 135: Appendices. NICE, L<strong>on</strong>d<strong>on</strong>, pp.81-2.<br />
93 NHS Blood and Transplant (2012) Achiev<strong>in</strong>g the 50% <strong>in</strong>crease <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>, 26<br />
January 2012. NHS BT, Bristol.<br />
94 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce Programme Delivery Board (2011) Work<strong>in</strong>g together to save<br />
lives. The Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce Implementati<strong>on</strong> Programme’s F<strong>in</strong>al Report, 2011.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, pp.26-8.<br />
95 Academy of Medical Royal Colleges (2008) A code of practice <strong>for</strong> the diagnosis and<br />
c<strong>on</strong>firmati<strong>on</strong> of death. AMRC, L<strong>on</strong>d<strong>on</strong>.<br />
96 NHS Specialised Services (2011) Nati<strong>on</strong>al Specialised Commissi<strong>on</strong><strong>in</strong>g Priorities, April 2011,<br />
p.14. Available at: www.specialisedservices.nhs.uk (accessed 24 January 2012).<br />
97 Evans G, NHS Blood and Transplant, Pers<strong>on</strong>al communicati<strong>on</strong>, 19 October 2011.<br />
98 NHS Blood and Transplant (2011) ODT e-Newsletter – News <strong>for</strong> the <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> and<br />
transplantati<strong>on</strong> community. Issue 1, September 2011. NHS BT, Bristol.<br />
99 Pers<strong>on</strong>al communicati<strong>on</strong> with a range of D<strong>on</strong>ati<strong>on</strong> Committee Chairs and Cl<strong>in</strong>ical Leads,<br />
October-November 2011.<br />
100 NHS Blood and Transplant (2012) Achiev<strong>in</strong>g the 50% <strong>in</strong>crease <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>,<br />
26 January 2012. NHS BT, Bristol.<br />
101 NHS Blood and Transplant, British Transplantati<strong>on</strong> Society, The College of Emergency<br />
Medic<strong>in</strong>e (2011) The role of emergency medic<strong>in</strong>e <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Report of a workshop,<br />
October 4th 2010. NHS BT, Bristol.<br />
102 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol p.7.<br />
103 Academy of Medical Royal Colleges (2008) A code of practice <strong>for</strong> the diagnosis and<br />
c<strong>on</strong>firmati<strong>on</strong> of death. AMRC, L<strong>on</strong>d<strong>on</strong>.<br />
104 Ayyaz A, White P, Dhital K et al. (2009) Cardiac recovery <strong>in</strong> a human n<strong>on</strong>-heart-beat<strong>in</strong>g<br />
d<strong>on</strong>or after extracorporeal perfusi<strong>on</strong>: source <strong>for</strong> human heart d<strong>on</strong>ati<strong>on</strong>? The Journal of<br />
Heart and Lung Transplantati<strong>on</strong> 28(3), pp.290-3.<br />
105 UK D<strong>on</strong>ati<strong>on</strong> Ethics Committee (2011) An Ethical Framework <strong>for</strong> C<strong>on</strong>trolled D<strong>on</strong>ati<strong>on</strong> after<br />
Circulatory Death. C<strong>on</strong>sultati<strong>on</strong>. Academy of Medical Royal Colleges, L<strong>on</strong>d<strong>on</strong>, para 104.<br />
106 Eyn<strong>on</strong> CA, Murphy PG, Smith M et al. (2010) Heart Transplantati<strong>on</strong> after declarati<strong>on</strong> of<br />
death by cardiorespiratory criteria. Journal of Heart and Lung Transplantati<strong>on</strong>. 29(2), pp.232-3.<br />
74<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
107 NHS Blood and Transplant (2011) Transplant Activity <strong>in</strong> the UK. Activity Report 2010/11.<br />
NHS BT, Bristol, p.7.<br />
108 Nati<strong>on</strong>al Institute <strong>for</strong> Health and Cl<strong>in</strong>ical Excellence (2006) Liv<strong>in</strong>g-d<strong>on</strong>or liver<br />
transplantati<strong>on</strong>. NICE, L<strong>on</strong>d<strong>on</strong>.<br />
109 Nati<strong>on</strong>al Institute <strong>for</strong> Health and Cl<strong>in</strong>ical Excellence (2006) Liv<strong>in</strong>g-d<strong>on</strong>or lung<br />
transplantati<strong>on</strong> <strong>for</strong> end-stage lung disease. NICE, L<strong>on</strong>d<strong>on</strong>.<br />
110 YouGov survey commissi<strong>on</strong>ed by Give a Kidney – One’s Enough. Available at:<br />
www.yougov.co.uk (accessed 2 February 2012).<br />
111 NHS Blood and Transplant, British Transplantati<strong>on</strong> Society (2011) Guidel<strong>in</strong>es <strong>for</strong> c<strong>on</strong>sent <strong>for</strong><br />
solid <strong>organ</strong> transplantati<strong>on</strong> <strong>in</strong> adults. NHS BT, Bristol.<br />
112 NHS Blood and Transplant (2011) GIFT – News <strong>for</strong> the <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> and transplantati<strong>on</strong><br />
community. Issue 2, December 2011. NHS BT, Bristol.<br />
113 NHS Blood and Transplant, British Transplantati<strong>on</strong> Society (2011) Guidel<strong>in</strong>es <strong>for</strong> c<strong>on</strong>sent <strong>for</strong><br />
solid <strong>organ</strong> transplantati<strong>on</strong> <strong>in</strong> adults. NHS BT, Bristol, p.5.<br />
114 NHS Executive (1994) Identificati<strong>on</strong> of potential d<strong>on</strong>ors of <strong>organ</strong>s <strong>for</strong> transplantati<strong>on</strong><br />
(HSG(94)41). 10 October.<br />
115 UK D<strong>on</strong>ati<strong>on</strong> Ethics Committee (2011) An Ethical Framework <strong>for</strong> C<strong>on</strong>trolled D<strong>on</strong>ati<strong>on</strong> after<br />
Circulatory Death. Academy of Medical Royal Colleges, L<strong>on</strong>d<strong>on</strong>, pp.57-8.<br />
116 Fabre J. (1999) Elective ventilati<strong>on</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Transplant Topics 1999(2), pp.15-9.<br />
117 Riad H, Nicholls A. (1995) Elective ventilati<strong>on</strong> of potential <strong>organ</strong> d<strong>on</strong>ors. BMJ 310, pp.714-5.<br />
118 NHS Blood and Transplant (2011) Potential D<strong>on</strong>or Audit. Summary report <strong>for</strong> the 12 m<strong>on</strong>th<br />
period 1 April 2010 - 31 March 2011. NHS BT, Bristol, p.6.<br />
119 NHS Blood and Transplant (2012) Achiev<strong>in</strong>g the 50% <strong>in</strong>crease <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>, 26<br />
January 2012. NHS BT, Bristol.<br />
120 NHS Blood and Transplant (2011) Celebrities back new campaign to urge Asian<br />
communities to jo<strong>in</strong> the NHS Organ D<strong>on</strong>or Register. News release, 19 October.<br />
121 NHS Blood and Transplant (2011) Celebrities back new campaign to urge black<br />
communities to jo<strong>in</strong> the NHS Organ D<strong>on</strong>or Register. News release, 19 October.<br />
122 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) Organs <strong>for</strong> Transplants. The supplement report.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, pp.150-7.<br />
123 NHS Blood and Transplant. Religious perspectives <strong>on</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Available at:<br />
www.<strong>organ</strong>d<strong>on</strong>ati<strong>on</strong>.nhs.uk (accessed 2 February 2012).<br />
124 NHS Blood and Transplant (2011) Campaign tackl<strong>in</strong>g shortage of <strong>organ</strong> d<strong>on</strong>ors from BME<br />
groups <strong>on</strong> target. News Release, 30 November.<br />
125 The Cab<strong>in</strong>et Office (2010) Apply<strong>in</strong>g behavioural <strong>in</strong>sight to health. The Cab<strong>in</strong>et Office,<br />
L<strong>on</strong>d<strong>on</strong>, p.4.<br />
126 Department of Health (2011) Licences to drive up <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Press release, 1 August.<br />
127 Nuffield Council <strong>on</strong> Bioethics (2011) Human bodies: d<strong>on</strong>ati<strong>on</strong> <strong>for</strong> medic<strong>in</strong>e and research.<br />
NCB, L<strong>on</strong>d<strong>on</strong>, p.10.<br />
128 Sim<strong>in</strong>off LA, Mercer MB. (2001) Public <strong>policy</strong>, public op<strong>in</strong>i<strong>on</strong> and c<strong>on</strong>sent <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong>. Cambridge Quarterly <strong>for</strong> Healthcare Ethics 10(4), pp.377-86.<br />
129 Klassen A, Klassen D. (1996) Who are the d<strong>on</strong>ors <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>? The family’s<br />
perspective <strong>in</strong> mandated choice. Ann Int Med 125, pp.70-3.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 75
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
130 George C. (2010) Texas ga<strong>in</strong>s ground <strong>on</strong> register<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>ors. Houst<strong>on</strong> Chr<strong>on</strong>icle, 27 July.<br />
131 Thaler R. (2009) Opt<strong>in</strong>g <strong>in</strong> vs Opt<strong>in</strong>g out. The New York Times, 26 September.<br />
132 New Jersey Hero Act 2008. Available at: www.njleg.state.nj.us (accessed 17 November 2011).<br />
133 Chouhan P, Draper H. (2003) Modified mandated choice <strong>for</strong> <strong>organ</strong> procurement. J Med<br />
Ethics 29, pp.157-62.<br />
134 Spital A. (1995) Mandated choice. A plan to <strong>in</strong>crease public commitment to <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong>. JAMA 273(6), pp.504-6.<br />
135 Spital A. (1996) Mandated choice <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>: Time to give it a try. Ann Int Med<br />
125, pp.66-9.<br />
136 Saunders J. (2010) Bodies, <strong>organ</strong>s and sav<strong>in</strong>g lives: the alternatives. Cl<strong>in</strong>ical Medic<strong>in</strong>e 10(1),<br />
pp.26-9.<br />
137 Chouhan P, Draper H. (2003) Modified mandated choice <strong>for</strong> <strong>organ</strong> procurement. J Med<br />
Ethics 29, pp.157-62: 159.<br />
138 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) The potential impact of an opt out system <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK – A report from the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Support<strong>in</strong>g In<strong>for</strong>mati<strong>on</strong>.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, Annex F, p.7.<br />
139 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) The potential impact of an opt out system <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK – A report from the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Support<strong>in</strong>g In<strong>for</strong>mati<strong>on</strong>.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, Annex F, p.7.<br />
140 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) The potential impact of an opt out system <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK – A report from the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Support<strong>in</strong>g In<strong>for</strong>mati<strong>on</strong>.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, Annex J, p.62.<br />
141 NHS Blood and Transplant (2011) Strategic Plan 2011-14. NHSBT, Wat<strong>for</strong>d, p.11.<br />
142 D<strong>on</strong>alds<strong>on</strong> L. (2007) 2006 Annual Report of the Chief Medical Officer. On the State of<br />
Public Health. Department of Health, L<strong>on</strong>d<strong>on</strong>, pp.26-33.<br />
143 Brown G. (2008) Organ d<strong>on</strong>ati<strong>on</strong>s help us make a difference. The Telegraph, 13 January,<br />
www.telegraph.co.uk (accessed 18 May 2011).<br />
144 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) The potential impact of an opt out system <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK. A report from the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Support<strong>in</strong>g In<strong>for</strong>mati<strong>on</strong>.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, Annex I, p.9.<br />
145 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) The potential impact of an opt out system <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK. A report from the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Support<strong>in</strong>g In<strong>for</strong>mati<strong>on</strong>.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, Annex I, p.66.<br />
146 Gimbel RW, Strosberg MS, Lehrman SE et al. (2003) Presumed c<strong>on</strong>sent and other predictors<br />
of cadaveric <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> Europe. Progress <strong>in</strong> Transplantati<strong>on</strong> 13, pp.17-23. Abadie A,<br />
Gay S. (2006) The impact of presumed c<strong>on</strong>sent legislati<strong>on</strong> <strong>on</strong> cadaveric <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>: a<br />
cross-country study. Journal of Health Ec<strong>on</strong>omics 25, pp.599-620.<br />
147 Horvat LD, Cuerden MS, Klim SJ et al. (2010) In<strong>for</strong>m<strong>in</strong>g the Debate: Rates of Kidney<br />
Transplantati<strong>on</strong> <strong>in</strong> Nati<strong>on</strong>s with Presumed C<strong>on</strong>sent. Ann Intern Med 153, pp.641-9.<br />
Mossialos E, Costa-F<strong>on</strong>t J, Rudisill C (2008) Does <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> legislati<strong>on</strong> affect<br />
<strong>in</strong>dividuals’ will<strong>in</strong>gness to d<strong>on</strong>ate their own or their relative’s <strong>organ</strong>s? Evidence from<br />
European Uni<strong>on</strong> survey data. BMC Health Service Research, 8, p.48. Available at:<br />
www.biomedcentral.com (accessed 24 November 2011).<br />
148 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) The potential impact of an opt-out system <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK – An <strong>in</strong>dependent report from the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce,<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, p.34.<br />
76<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
149 See, <strong>for</strong> example: Harris E. (2008) House of Comm<strong>on</strong>s Hansard, 20 November, Col 151WH.<br />
Rieu R. (2010) The potential impact of an opt-out system <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK. J<br />
Med Ethics 36, pp.534-8.Bird SM, Harris J. (2010) Time to move to presumed c<strong>on</strong>sent <strong>for</strong><br />
<strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. BMJ 340:c2188.<br />
150 Price D (2000) Legal and ethical aspects of <strong>organ</strong> transplantati<strong>on</strong>. Cambridge University<br />
Press, Cambridge, pp.89-90.<br />
151 Michielsen P. (1992) Organ shortage – what to do? Transplantati<strong>on</strong> Proceed<strong>in</strong>gs 24(6), p.2392.<br />
152 Csillag C. (1998) Brazil abolishes ‘presumed c<strong>on</strong>sent’ <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Lancet 352, p.1367.<br />
153 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) The potential impact of an opt out system <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK – A report from the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Support<strong>in</strong>g In<strong>for</strong>mati<strong>on</strong>.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, Annex J, p.16.<br />
154 Department of Health (1999) Survey shows that public prefers exist<strong>in</strong>g <strong>organ</strong> d<strong>on</strong>or<br />
scheme, Press Release, 2 July (1999/0405).<br />
155 British Medical Associati<strong>on</strong> (2007) Support grows <strong>for</strong> presumed c<strong>on</strong>sent. Press release,<br />
19 October.<br />
156 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) The potential impact of an opt out system <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK – A report from the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Support<strong>in</strong>g In<strong>for</strong>mati<strong>on</strong>.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, Annex J.<br />
157 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) The potential impact of an opt out system <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK – A report from the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Support<strong>in</strong>g In<strong>for</strong>mati<strong>on</strong>.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, Annex J, p.42.<br />
158 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) The potential impact of an opt out system <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK. An <strong>in</strong>dependent report from the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>.<br />
159 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) The potential impact of an opt out system <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK – A report from the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce. Support<strong>in</strong>g In<strong>for</strong>mati<strong>on</strong>.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, Annex G, p.7.<br />
160 Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) The potential impact of an opt out system <strong>for</strong> <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> the UK. An <strong>in</strong>dependent report from the Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce.<br />
Department of Health, L<strong>on</strong>d<strong>on</strong>, p.4.<br />
161 Welsh Government (2011) Proposals <strong>for</strong> legislati<strong>on</strong> <strong>on</strong> <strong>organ</strong> and tissue d<strong>on</strong>ati<strong>on</strong>: A Welsh<br />
Government White Paper, C<strong>on</strong>sultati<strong>on</strong> Document. WAG, Cardiff.<br />
162 NHS Blood and Transplant (2009) New research highlights need to bridge gap between<br />
good <strong>in</strong>tenti<strong>on</strong>s and acti<strong>on</strong>. News release, 2 November.<br />
163 Lavee J, Ashkenazi T, Gurman G et al. (2010) A new law <strong>for</strong> allocati<strong>on</strong> of d<strong>on</strong>or <strong>organ</strong>s <strong>in</strong><br />
Israel. The Lancet 375, pp.1131-3.<br />
164 Lavee J, Ashkenazi T, Gurman G et al. (2010) A new law <strong>for</strong> allocati<strong>on</strong> of d<strong>on</strong>or <strong>organ</strong>s <strong>in</strong><br />
Israel. The Lancet 375, pp.1131-3:1132.<br />
165 Traubmann T. (2011) Transplantati<strong>on</strong>s fall <strong>in</strong> Israel as new law takes effect. BMJ 342, p.195.<br />
166 Jarvis R. (1995) Jo<strong>in</strong> the club: a modest proposal to <strong>in</strong>crease availability of d<strong>on</strong>or <strong>organ</strong>s. J<br />
Med Ethics 21, pp.199-204.<br />
167 Gill<strong>on</strong> R. (1995) On giv<strong>in</strong>g preference to prior volunteers when allocat<strong>in</strong>g <strong>organ</strong>s <strong>for</strong><br />
transplantati<strong>on</strong> [Editorial]. J Med Ethics 21, pp.195-6:196.<br />
168 Gill<strong>on</strong> R. (1995) On giv<strong>in</strong>g preference to prior volunteers when allocat<strong>in</strong>g <strong>organ</strong>s <strong>for</strong><br />
transplantati<strong>on</strong> [Editorial]. J Med Ethics 21, pp.195-6.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 77
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
169 Gill<strong>on</strong> R. (1995) On giv<strong>in</strong>g preference to prior volunteers when allocat<strong>in</strong>g <strong>organ</strong>s <strong>for</strong><br />
transplantati<strong>on</strong> [Editorial]. J Med Ethics 21, pp.195-6.<br />
170 Eat<strong>on</strong> S. (1998) The subtle politics of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>: a proposal. J Med Ethics 24, pp.166-70.<br />
171 Bennett R, Savani S. (2004) Factors <strong>in</strong>fluenc<strong>in</strong>g the will<strong>in</strong>gness to d<strong>on</strong>ate body parts <strong>for</strong><br />
transplantati<strong>on</strong>. Journal of Health & Social Policy 18(3), pp.61-85.<br />
172 Haddow G. (2006) ‘Because you’re worth it?’ The tak<strong>in</strong>g and sell<strong>in</strong>g of transplantable<br />
<strong>organ</strong>s. J Med Ethics 32, p.326.<br />
173 Rabbitt Roff S. (2011) We should c<strong>on</strong>sider pay<strong>in</strong>g kidney d<strong>on</strong>ors. BMJ 343, p.321.<br />
174 Block WE. (2011) Organ transplant: us<strong>in</strong>g the free market solves the problem. J Cl<strong>in</strong>ic Res<br />
Bioeth 2(3), pp.2-3.<br />
175 Harris J, Er<strong>in</strong> C. (2002) An ethically defensible market <strong>in</strong> <strong>organ</strong>s. BMJ 325, pp.114-5.<br />
176 Harris J, Er<strong>in</strong> C. (2002) An ethically defensible market <strong>in</strong> <strong>organ</strong>s. BMJ 325, pp.114-5.<br />
177 See, <strong>for</strong> example: Jafarey A, Thomas G, Ahmad A et al. (2007) Asia’s <strong>organ</strong> farms. Ind J<br />
Med Ethics 4, pp.52-3.<br />
178 Hippen B. (2008) Organ sales and moral travails. Less<strong>on</strong>s from liv<strong>in</strong>g kidney vendor program<br />
<strong>in</strong> Iran. Policy Analysis No 614. 20 March. CATO Institute, Wash<strong>in</strong>gt<strong>on</strong>. Hippen B, Ross LF,<br />
Sade RM. (2009) Sav<strong>in</strong>g lives is more important than abstract moral c<strong>on</strong>cerns: f<strong>in</strong>ancial<br />
<strong>in</strong>centives should be used to <strong>in</strong>crease <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Ann Thorac Surg 88, pp.1053-61.<br />
179 Griff<strong>in</strong> A. (2007) Iranian <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> – kidneys <strong>on</strong> demand. BMJ 334, pp.502-5.<br />
180 Ghods AJ. (2002) Renal Transplantati<strong>on</strong> <strong>in</strong> Iran. Nephrology Dialysis Transplantati<strong>on</strong> 17,<br />
pp.222-8. Hippen B. (2008) Organ sales and moral travails. Less<strong>on</strong>s from liv<strong>in</strong>g kidney<br />
vendor program <strong>in</strong> Iran. Policy Analysis No 614. 20 March. CATO Institute, Wash<strong>in</strong>gt<strong>on</strong>.<br />
181 Griff<strong>in</strong> A. (2007) Iranian <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> – kidneys <strong>on</strong> demand. BMJ 334, pp.502-5.<br />
182 Hippen B. (2008) Organ sales and moral travails. Less<strong>on</strong>s from liv<strong>in</strong>g kidney vendor program<br />
<strong>in</strong> Iran. Policy Analysis No 614. 20 March. CATO Institute, Wash<strong>in</strong>gt<strong>on</strong>, p.7.<br />
183 British Medical Associati<strong>on</strong> (2012) Medical Ethics Today 3rd edn. Wiley Blackwell,<br />
Chichester, pp.334-6.<br />
184 Radcliffe-Richards J, Daar AS, Guttman RD et al <strong>for</strong> the Internati<strong>on</strong>al Forum <strong>for</strong> Transplant<br />
Ethics (1998) The case <strong>for</strong> allow<strong>in</strong>g kidney sales. The Lancet 351, pp.1950-2.<br />
185 Nuffield Council <strong>on</strong> Bioethics (2011) Human bodies: d<strong>on</strong>ati<strong>on</strong> <strong>for</strong> medic<strong>in</strong>e and research.<br />
NCB, L<strong>on</strong>d<strong>on</strong>, p.viii.<br />
186 Cited <strong>in</strong>: Nuffield Council <strong>on</strong> Bioethics (2011) Human Bodies: d<strong>on</strong>ati<strong>on</strong> <strong>for</strong> medic<strong>in</strong>e and<br />
research. NCB, L<strong>on</strong>d<strong>on</strong>, p.144.<br />
187 Hippen B, Ross LF, Sade RM. (2009) Sav<strong>in</strong>g lives is more important than abstract moral<br />
c<strong>on</strong>cerns: f<strong>in</strong>ancial <strong>in</strong>centives should be used to <strong>in</strong>crease <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Ann Thorac Surg<br />
88, pp.1053-61.<br />
188 World Health Organizati<strong>on</strong> (2009) Blood safety and availability – Facts and figures from the<br />
2007 Blood Safety Survey. Fact sheet No 279. WHO, Geneva.<br />
189 Directive 2010/53/EU of the European Parliament and of the Council of 7 July 2010 <strong>on</strong><br />
standards of quality and safety of human <strong>organ</strong>s <strong>in</strong>tended <strong>for</strong> transplantati<strong>on</strong>, Art 13.<br />
190 Rid A, Bachmann LM, Wettste<strong>in</strong> V et al. (2009) Would you sell a kidney <strong>in</strong> a regulated<br />
kidney market? Results of an exploratory study. J Med Ethics 35, pp.558-64.<br />
191 Haddow G. (2006) ‘Because you’re worth it?’ The tak<strong>in</strong>g and sell<strong>in</strong>g of transplantable<br />
<strong>organ</strong>s. J Med Ethics 32, pp.324-8.<br />
78<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
192 Smith L. (2011) Sale of human <strong>organ</strong>s should be legalised, say surge<strong>on</strong>s. The Independent,<br />
5 January, www.<strong>in</strong>dependent.co.uk (accessed 21 September 2011).<br />
193 Nuffield Council <strong>on</strong> Bioethics (2011) Human Bodies: d<strong>on</strong>ati<strong>on</strong> <strong>for</strong> medic<strong>in</strong>e and research.<br />
NCB, L<strong>on</strong>d<strong>on</strong>.<br />
194 Matesanz R. (2011) Pers<strong>on</strong>al communicati<strong>on</strong>, 3 November.<br />
195 Matesanz R. (2011) Pers<strong>on</strong>al communicati<strong>on</strong>, 3 November.<br />
196 Nuffield Council <strong>on</strong> Bioethics (2011) Human bodies: d<strong>on</strong>ati<strong>on</strong> <strong>for</strong> medic<strong>in</strong>e and research.<br />
NCB, L<strong>on</strong>d<strong>on</strong>, pp.5-7.<br />
197 Nuffield Council <strong>on</strong> Bioethics (2011) Human bodies: d<strong>on</strong>ati<strong>on</strong> <strong>for</strong> medic<strong>in</strong>e and research.<br />
NCB, L<strong>on</strong>d<strong>on</strong>, pp.174-5.<br />
198 Nuffield Council <strong>on</strong> Bioethics (2011) Human bodies: d<strong>on</strong>ati<strong>on</strong> <strong>for</strong> medic<strong>in</strong>e and research.<br />
NCB, L<strong>on</strong>d<strong>on</strong>, p.xviii.<br />
199 Smithers R. (2011) Families cutt<strong>in</strong>g funeral costs, survey reveals. The Guardian, 8 February.<br />
200 Smithers R. (2011) Families cutt<strong>in</strong>g funeral costs, survey reveals. The Guardian, 8 February.<br />
201 Haddow G. (2006) ‘Because you’re worth it?’ The tak<strong>in</strong>g and sell<strong>in</strong>g of transplantable<br />
<strong>organ</strong>s. J Med Ethics 32, pp.324-8.<br />
202 Op<strong>in</strong>i<strong>on</strong> leader (2010) Nuffield Council <strong>on</strong> Bioethics: Human bodies <strong>in</strong> medic<strong>in</strong>e and<br />
research. Report of deliberative workshop <strong>on</strong> ethical issues raised by the d<strong>on</strong>ati<strong>on</strong> of bodily<br />
material. Available at: www.nuffieldbioethics.org.uk (accessed 2 December 2011).<br />
203 Thomps<strong>on</strong> H, Campbell K. (2011) Free funerals <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ors? Available at:<br />
www.labs.yougov.co.uk (accessed 7 November 2011).<br />
204 Fabre J, Murphy P, Matesanz R. (2010) Presumed c<strong>on</strong>sent is unnecessary. BMJ 341, pp.922-4.<br />
205 Miranda B, Fernández Lucas M, de Felipe C et al. (1999) Organ d<strong>on</strong>ati<strong>on</strong> <strong>in</strong> Spa<strong>in</strong>. Nephrol<br />
Dial Transplant 14 [Suppl 3], pp.15-21.<br />
206 House of Lords European Uni<strong>on</strong> Committee (2008) Increas<strong>in</strong>g the supply of d<strong>on</strong>or <strong>organ</strong>s<br />
with<strong>in</strong> the European Uni<strong>on</strong>, 17th Report of Sessi<strong>on</strong> 2007-08, Vol l. HL Paper, 123-1. The<br />
Stati<strong>on</strong>ery Office, Norwich, para 193.<br />
207 Fabre J, Murphy P, Matesanz R. (2010) Presumed c<strong>on</strong>sent is unnecessary. BMJ 341, pp.922-4.<br />
208 Abadie A, Gay S. (2006) The impact of presumed c<strong>on</strong>sent legislati<strong>on</strong> <strong>on</strong> cadaveric <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong>: a cross-country study. Journal of Health Ec<strong>on</strong>omics 25, pp.599-620.<br />
209 Fabre J, Murphy P, Matesanz R. (2010) Presumed c<strong>on</strong>sent is unnecessary. BMJ 341, pp.922-4.<br />
210 House of Lords European Uni<strong>on</strong> Committee (2008) Increas<strong>in</strong>g the supply of d<strong>on</strong>or <strong>organ</strong>s<br />
with<strong>in</strong> the European Uni<strong>on</strong>, 17th Report of Sessi<strong>on</strong> 2007-08, Vol ll. HL Paper, 123-1. The<br />
Stati<strong>on</strong>ery Office, Norwich, p.135.<br />
211 Rodríguez-Arias D, Wright L, Paredes D. (2010) Success factors and ethical challenges of<br />
the Spanish Model of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Lancet 376, pp.1109-12.<br />
212 Rodríguez-Arias D, Wright L, Paredes D. (2010) Success factors and ethical challenges of<br />
the Spanish Model of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Lancet 376, pp.1109-12.<br />
213 Quoted <strong>in</strong>: Rodríguez-Arias D, Wright L, Paredes D. (2010) Success factors and ethical<br />
challenges of the Spanish Model of <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>. Lancet 376, pp.1109-12:1,1110.<br />
214 Matesanz R. (2003) Factors <strong>in</strong>fluenc<strong>in</strong>g the adaptati<strong>on</strong> of the Spanish Model of <strong>organ</strong><br />
d<strong>on</strong>ati<strong>on</strong>. Transpl Int 16, pp.736-41:738.<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk? 79
<strong>BMA</strong> MEDICAL ETHICS COMMITTEE<br />
215 Falvey S. (2007) Approach to <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> with<strong>in</strong> the US: f<strong>in</strong>d<strong>in</strong>gs from a visit to US<br />
Organ Procurement Organisati<strong>on</strong>s. In: Organ D<strong>on</strong>ati<strong>on</strong> Task<strong>for</strong>ce (2008) Organs <strong>for</strong><br />
Transplants. The Supplement Report. Department of Health, L<strong>on</strong>d<strong>on</strong>, pp. 203-5.<br />
216 Sim<strong>in</strong>i B. (2000) Tuscany doubles <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> rates by follow<strong>in</strong>g Spanish example.<br />
Lancet 355, p.467.<br />
217 Quigley M, Brazier M, Chadwick R. (2008) Editorial: The <strong>organ</strong>s crisis and the Spanish<br />
model: theoretical versus pragmatic c<strong>on</strong>siderati<strong>on</strong>s. J Med Ethics 34, pp.223-4.<br />
218 NHS Blood and Transplant (2012) Achiev<strong>in</strong>g the 50% <strong>in</strong>crease <strong>in</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong>,<br />
26 January 2012. NHS BT, Bristol.<br />
219 NHS Blood and Transplant (2011) Strategic Plan 2011-14. NHSBT, Wat<strong>for</strong>d, p.12.<br />
80<br />
<str<strong>on</strong>g>Build<strong>in</strong>g</str<strong>on</strong>g> <strong>on</strong> <strong>progress</strong>: <strong>where</strong> <strong>next</strong> <strong>for</strong> <strong>organ</strong> d<strong>on</strong>ati<strong>on</strong> <strong>policy</strong> <strong>in</strong> the uk?
<strong>BMA</strong> Medical Ethics Committee<br />
British Medical Associati<strong>on</strong>, <strong>BMA</strong> House, Tavistock Square, L<strong>on</strong>d<strong>on</strong>, WC1H 9JP<br />
www.bma.org.uk<br />
© British Medical Associati<strong>on</strong>, 2012<br />
CODE: 52368 / ETHICS / FEBRUARY 2012