Familial Hypercholesterolemia Presenting as Intracranial Xanthoma
Familial Hypercholesterolemia Presenting as Intracranial Xanthoma
Familial Hypercholesterolemia Presenting as Intracranial Xanthoma

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
C<strong>as</strong>e Report<br />
<strong>Familial</strong> <strong>Hypercholesterolemia</strong> <strong>Presenting</strong> <strong>as</strong><br />
<strong>Intracranial</strong> <strong>Xanthoma</strong><br />
Anita B<strong>as</strong>avaraj**, S Jadhav*, J Dhadwad*<br />
Abstract<br />
A 22 years female who w<strong>as</strong> diagnosed <strong>as</strong> having cholestseatoma of right ear w<strong>as</strong> referred to us for medical<br />
fitness. On examination she incidentally had evidence of tuberous and tendon xanthom<strong>as</strong>. She w<strong>as</strong> found to<br />
have hypercholesterolemia. On m<strong>as</strong>toid exploration a yellowish groomous m<strong>as</strong>s w<strong>as</strong> seen which w<strong>as</strong><br />
surrounded by foamy macrophages, suggestive of ‘m<strong>as</strong>toid xanthoma’. The purpose of this c<strong>as</strong>e presentation<br />
is to report occurrence of such rare c<strong>as</strong>e and importance of early detection that will warrant treatment with<br />
proper diet and medical management. This will stabilize lesions and delay complications. ©<br />
INTRODUCTION<br />
<strong>Intracranial</strong> xanthom<strong>as</strong> are rare entity. They occur<br />
among patients with hyperlipidemia which consists<br />
of several entities such <strong>as</strong> polygenic<br />
hypercholesterolemia, combined familial<br />
hyperlipoproteinemia and familial hypercholesterolemia.<br />
Pharmacologic agents along with dietary<br />
me<strong>as</strong>urement are the b<strong>as</strong>is of treatment. Medical<br />
treatment includes bile resins, niacin and statins that<br />
work indirectly to incre<strong>as</strong>e low-density receptors and<br />
reduce serum low- density lipoprotein levels. 2,3 These<br />
me<strong>as</strong>ures stabilize lesions and sometimes may cause<br />
regression.<br />
We present a c<strong>as</strong>e of intracranial xanthoma <strong>as</strong>sociated<br />
with type 2 familial hypercholesterolemia.<br />
CASE REPORT<br />
A 20 years female w<strong>as</strong> admitted with complaints of<br />
reduced hearing in the right ear with mucopurulent<br />
discharge since 3 months <strong>as</strong>sociated with occipital<br />
headache there; w<strong>as</strong> no history of fever, giddiness,<br />
convulsions or vomiting. She w<strong>as</strong> diagnosed <strong>as</strong> having<br />
a cholesteatoma and w<strong>as</strong> posted for modified radical<br />
m<strong>as</strong>toidectomy. She w<strong>as</strong> referred to us for medical fitness,<br />
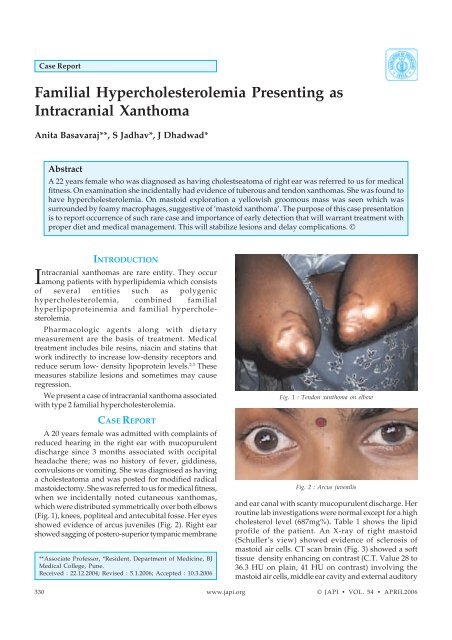
when we incidentally noted cutaneous xanthom<strong>as</strong>,<br />
which were distributed symmetrically over both elbows<br />
(Fig. 1), knees, popliteal and antecubital fosse. Her eyes<br />
showed evidence of arcus juveniles (Fig. 2). Right ear<br />
showed sagging of postero-superior tympanic membrane<br />
**Associate Professor, *Resident, Department of Medicine, BJ<br />
Medical College, Pune.<br />
Received : 22.12.2004; Revised : 5.1.2006; Accepted : 10.3.2006<br />
Fig. 1 : Tendon xanthoma on elbow<br />
Fig. 2 : Arcus juvenilis<br />
and ear canal with scanty mucopurulent discharge. Her<br />
routine lab investigations were normal except for a high<br />
cholesterol level (687mg%). Table 1 shows the lipid<br />
profile of the patient. An X-ray of right m<strong>as</strong>toid<br />
(Schuller’s view) showed evidence of sclerosis of<br />
m<strong>as</strong>toid air cells. CT scan brain (Fig. 3) showed a soft<br />
tissue density enhancing on contr<strong>as</strong>t (C.T. Value 28 to<br />
36.3 HU on plain, 41 HU on contr<strong>as</strong>t) involving the<br />
m<strong>as</strong>toid air cells, middle ear cavity and external auditory<br />
330 www.japi.org © JAPI • VOL. 54 • APRIL2006
Table 1 : Lipid profile of patient<br />
On admission<br />
8 months later<br />
Total chol 687 311<br />
HDL 73 62<br />
LDL 551 139<br />
VLDL 13 47<br />
Triglycerides 164 214<br />
Chylomicrons — 42<br />
Table 2 : Lipid profile of patient’s family<br />
Patient Father Mother Sister Brother<br />
Total chol 687 281 233 491 237<br />
HDL 73 38 39 42 44<br />
LDL 551 196 150 417 155<br />
VLDL 13 23 15.60 32 13.60<br />
Triglycerides 164 147 78 159 68<br />
the right sided facial palsy which had developed postoperatively<br />
h<strong>as</strong> recovered.<br />
DISCUSSION<br />
Fig. 3 : <strong>Intracranial</strong> xanthoma<br />
canal on the right side with erosion of the m<strong>as</strong>toid,<br />
temporal bone, anterior wall and sinus plate; this w<strong>as</strong><br />
thought to be a cholesteatoma, Periossicular soft tissue<br />
density w<strong>as</strong> noted, however the ossicular chain w<strong>as</strong><br />
preserved. A possibility of m<strong>as</strong>toid xanthoma (ectopic<br />
occurrence of fat) w<strong>as</strong> also kept in mind.<br />
During her tympanom<strong>as</strong>toid exploration it w<strong>as</strong> noted<br />
that, there w<strong>as</strong> erosion of the lateral wall of the m<strong>as</strong>toid<br />
antrum, posterior wall of the external auditory canal.<br />
The surgeons tried to remove the dise<strong>as</strong>e from middle<br />
ear by limited excision. Postoperatively, patient had a<br />
right lower motor neuron facial palsy.<br />
Histopathologic examination of the tissue removed<br />
during surgery revealed a yellowish groomous material.<br />
On microscopy it shows multiple cholesterol crystals<br />
surrounded by foamy macrophages, inflammation and<br />
calcification suggestive of m<strong>as</strong>toid- xanthoma. Other<br />
family members were also investigated for lipid profile<br />
(Table 2).<br />
Thus we had a patient of familial homozygous hypercholesterolemia<br />
(Type-II a) with rare presentation of<br />
intracranial xanthoma. She w<strong>as</strong> treated with Tab.<br />
Atorv<strong>as</strong>tatin 20 mg HS which w<strong>as</strong> incre<strong>as</strong>ed to 30 mg/<br />
day for better control. The patient soon developed statin<br />
induced proximal myopathy, hence the dose of<br />
atorv<strong>as</strong>tatin w<strong>as</strong> reduced to 20 mg/day and Tab.<br />
Ezetimibe 10mg w<strong>as</strong> added.<br />
Her current lipid profile 8 months later is given in<br />
Table 1, the cutaneous xanthom<strong>as</strong> have flattened and<br />
The heritable hyperlipidemia is of six types, I, IIa, IIb,<br />
III, IV and V. Subcutaneous xanthom<strong>as</strong> typically occur<br />
in patient with heritable hyperlipidemia. Types II and<br />
III hyperlipidemia are caused due to excess circulating<br />
lipoproteins and moderately elevated serum cholesterol<br />
levels. Accelerated atherosclerosis frequently occurs,<br />
resulting in premature coronary artery dise<strong>as</strong>e and<br />
stroke.<br />
Abnormal lipid storage in the setting of normal serum<br />
lipids may occur in conditions such <strong>as</strong> histiocytosis X,<br />
leading to xanthoma formation 4 and needs to be<br />
distinguished from xanthom<strong>as</strong> due to hyperlipidemia.<br />
Xanthom<strong>as</strong> develop because of lipid leakage from the<br />
v<strong>as</strong>cular into the surrounding tissue, where<br />
macrophages subsequently phagocytose these lipids.<br />
Because cholesterol is not degraded, it accumulates<br />
within these cells, creating “foamy” macrophages. The<br />
extracellular cholesterol crystallizes into clefts and<br />
induces an inflammatory reaction with giant cells and<br />
resultant fibrosis. 1 Systemic xanthom<strong>as</strong> most commonly<br />
occur along the Achilles, patellar, and extensor tendons<br />
of the hands, buttocks, elbows, eyelids, and hand<br />
cre<strong>as</strong>es. 3<br />
<strong>Intracranial</strong> xanthom<strong>as</strong> have been reported rarely<br />
among patients with hyperlipidemia, most commonly<br />
type II. <strong>Familial</strong> hypercholesterolemia h<strong>as</strong> a dominant<br />
inheritance pattern. Combined familial<br />
hyperlipoproteinemia occurs in 1% to 2% of the<br />
population and presents in the 3 rd to 4 th decade of life. It<br />
is usually not <strong>as</strong>sociated with xanthom<strong>as</strong>. It arises from<br />
a reduced number of hepatic low-density lipoprotein<br />
receptors, leading to reduced low density lipoprotein<br />
clearance from the blood.<br />
<strong>Intracranial</strong> and extracranial xanthom<strong>as</strong> can occur<br />
© JAPI • VOL. 54 • APRIL 2006 www.japi.org 331
in the temporal bone, 3 the skull b<strong>as</strong>e (clivus), 1 and over<br />
the cerebral convexities. Most occur in middle- aged and<br />
elderly patients, although they have been reported in<br />
young patients. 6 Because of their slow progression, they<br />
tend to present late in life. 3,4,6 Clinical presentation<br />
depends on lesion location and extent. Symptoms may<br />
include severe headache, 1 otorrhea, 6 cranial nerve<br />
palsies, tinnitus, 1-6 and otitis media.<br />
Although the diagnosis of an intracranial xanthoma<br />
may be suggested by its imaging appearance, the<br />
diagnosis is usually not considered because of its rarity.<br />
These are circumscribed, extraaxial m<strong>as</strong>ses that are<br />
hypodense to brain on unenhanced CT scans. 1 Osseous<br />
abnormalities include bony destruction and<br />
remodeling. 1,3,6 The MR imaging appearance of<br />
xanthom<strong>as</strong> is in part due to their high lipid content. On<br />
Unenhanced T1- weighted images, most are<br />
hyperintense, with corresponding heterogeneous low<br />
signal intensity on T-2 weighted images. After the IV<br />
administration of contr<strong>as</strong>t material, these lesions do not<br />
show significant enhancement.<br />
Pharmacological agents (bile resins, niacin, statins)<br />
used alone or in combination with dietary me<strong>as</strong>ures are<br />
the b<strong>as</strong>is of treatment of the hyperlipidemia. These may<br />
stabilize and sometimes, regress the lesions. So early<br />
medical intervention is important.<br />
REFERENCES<br />
1. Friedman O, Hockstein N, Willcox TO Jr, Keane WM.<br />
<strong>Xanthoma</strong> of the temporal bone: a unique c<strong>as</strong>e of this rare<br />
condition. Ear Nose Throat J 2000;79:433-6.<br />
2. Fukushima M, Marubay<strong>as</strong>hi T, Matsukado. A c<strong>as</strong>e of familial<br />
type IIa hyperlipoproteinemia with intracranial xanthoma.<br />
No To Shinkei 1984;36:375-81.<br />
3. Yamaha H, Kurata H, Nomura K. Adult Xantho<br />
granulomatous intracranial lesion involving familial<br />
hypercholesterolemia. Jpn J Med 1989;28:757-61.<br />
4. Jackler RK, Brackmann DE. <strong>Xanthoma</strong> of the temporal bone<br />
and skull b<strong>as</strong>e. Am J Otol 1987;8:111-5.<br />
5. Carr D, Thornes HM, Rutter AC, Finney RD, Turner PR.<br />
Sheehan's syndrome presenting with type III<br />
hyperlipoproteinaemia. Postgrad Med J 1987;63:1099-100.<br />
6. Bonhomme GR, Loevner LA, Yen DM, et al. Extensive<br />
<strong>Intracranial</strong> <strong>Xanthoma</strong> Associated with Type II<br />
Hyperlipidemia. Am J Neuroradiol 2000;21:353-5.<br />
Update Ayurveda ’06<br />
Date 22 nd – 24 th November 2006<br />
Venue : Nair Hospital Auditorium, D- Block, College Bldg., TN Medical College & BYL Nair Ch.<br />
Hospital, Mumbai Central, Mumbai – 400 008.<br />
The conference will include invited lectures from eminent scientists, Research workers, Academicians, Ayurvedic and<br />
Allopathic practitioners, <strong>as</strong> well <strong>as</strong> Industry stalwarts. L<strong>as</strong>t date for submission of abstracts (250 words) is 15 th September<br />
2006.<br />
For registration form and further details ple<strong>as</strong>e visit our website www.nair.edu<br />
For further information, ple<strong>as</strong>e contact:<br />
Dr. Supriya Bhalerao, Organizing Secretary – Update Ayurveda ’06<br />
Dr. Sharadini Dahanukar Advanced Centre for Ayurveda Research, Training & Services,<br />
Department of Clinical Pharmacology,<br />
TN Medical College and BYL Nair Ch. Hospital, Dr. AL Nair Road, Mumbai Central, Mumbai 400 008, INDIA.<br />
Contacts: 91-22-23014713; Telefax: 91-22-23050347 Email: clinpharm@vsnl.net<br />
332 www.japi.org © JAPI • VOL. 54 • APRIL2006