Five Cases of Aconite Poisoning - Journal of Analytical Toxicology
Five Cases of Aconite Poisoning - Journal of Analytical Toxicology
Five Cases of Aconite Poisoning - Journal of Analytical Toxicology

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Journal</strong> <strong>of</strong> <strong>Analytical</strong> <strong>Toxicology</strong>, Vol. 31, April 2007<br />
<strong>Five</strong> <strong>Cases</strong> <strong>of</strong> <strong>Aconite</strong> <strong>Poisoning</strong>: Toxicokinetics<br />
<strong>of</strong> Aconitines<br />
Yuji Fujita 1,2, Katsutoshi Terui 3, Megumi Fujita 1,2, Atsushi Kakizaki 2, Norio Sato 3, Kohei Oikawa 3, Hidehiko AokP,<br />
Katsuo TakahashP, and Shigeatsu Endo 3<br />
1<strong>Poisoning</strong> and Drug Laboratory Division, Critical Care and Emergency Center, Iwate Medical University Hospital, 3-16-1<br />
Honchoudori, Morioka, Iwate 020-0015, Japan; 2Department <strong>of</strong> Pharmacy, Iwate Medical University Hospital, 19-1 Uchirnaru,<br />
Morioka, Iwate 020-8505, Japan; and 3Department <strong>of</strong> Emergency Medicine, Iwate Medical University School <strong>of</strong> Medicine,<br />
19-1 Uchimaru, Morioka, Iwate 020-8505, Japan<br />
Abstract<br />
<strong>Aconite</strong> poisoning was examined in five patients (four males and<br />
one female) aged 49 to 78 years old. The electrocardiogram<br />
findings were as follows: ventricular tachycardia and ventricular<br />
fibrillation in case 1, premature ventricular contraction and<br />
accelerated idioventricular rhythm in case 2, AIVR in case 3, and<br />
nonsustained ventricular tachycardia in cases 4 and 5. The patient<br />
in case 1 was given percutaneous cardiopulmonary support<br />
because <strong>of</strong> unstable hemodynamics, whereas the other patients<br />
were treated with fluid replacement and antiarrhythmic agents.<br />
The main aconitine alkaloid in each patient had a half-life that<br />
ranged from 5.8 to 15.4 h over the five cases, and other detected<br />
alkaloids had half-lives similar to the half-life <strong>of</strong> the main alkaloid<br />
in each case. The half-life <strong>of</strong> the main alkaloid in case 1 was about<br />
twice as long as the half-lives in the other cases, and high values<br />
for the area under the blood concentration-time curve and the<br />
mean residence time were only observed in case 1. These results<br />
suggest that alkaloid toxicokinetics parameters may reflect the<br />
severity <strong>of</strong> toxic symptoms in aconite poisoning.<br />
Introduction<br />
<strong>Aconite</strong> is a well-known toxic plant <strong>of</strong> the genus Aconitum<br />
in the Ranunculaceae family. <strong>Aconite</strong> contains aconitine alkaloids<br />
such as aconitines, benzoylaconines and aconines, and<br />
the aconitines (aconitine, hypaconitine, jesaconitine, and<br />
mesaconitine) are the causative agents <strong>of</strong> aconite poisoning,<br />
since the toxicity <strong>of</strong> aconitines is much stronger than that <strong>of</strong><br />
other alkaloids (1). The LD50 value <strong>of</strong> aconitine in mice is reported<br />
to be 1.8 mg/kg when given orally (1), and the lethal<br />
dose <strong>of</strong> aconitine for humans is estimated to be 1-2 mg (2,3).<br />
Most cases <strong>of</strong> aconite poisoning have occurred in Japan and<br />
China. The common causes are ingestion <strong>of</strong> aconitine-containing<br />
Chinese herbal medicine (4-7) and mistaken ingestion<br />
<strong>of</strong> aconite instead <strong>of</strong> edible wild plants (8). <strong>Aconite</strong> has also<br />
been used in cases <strong>of</strong> suicide and homicide because <strong>of</strong> its high<br />
toxicity (9-11). Similar cases have been reported in Europe and<br />
the United States, although aconite-poisoning cases are relatively<br />
rare in these regions (12-14). Various toxic symptoms,<br />
such as nausea, vomiting, numbness and palsy <strong>of</strong> the extremities,<br />
and arrhythmia, are observed in aconite poisoning, with<br />
arrhythmia being the most typical symptom. <strong>Aconite</strong> poisoning<br />
<strong>of</strong>ten results in death due to cardiac arrest caused by a<br />
fatal arrhythmia such as ventricular fibrillation (Vf), and therefore<br />
an understanding <strong>of</strong> arrhythmias caused by aconite poisoning<br />
is <strong>of</strong> importance.<br />
There have been many pharmacological studies <strong>of</strong> aconitines<br />
(1,15-21), and the toxicity <strong>of</strong> these molecules is known to be<br />
due to their action on sodium channels in excitable<br />
membranes (16-19). In contrast, the toxicokinetics <strong>of</strong><br />
aconitines in humans have only been examined in two reports:<br />
a study <strong>of</strong> the distribution <strong>of</strong> aconitine alkaloids by Ito<br />
et al. (22) and measurement <strong>of</strong> the half-life <strong>of</strong> aconitine by<br />
Moritz et al. (14).<br />
Establishment <strong>of</strong> pharmacokinetics (toxicokinetics) parameters<br />
in aconite poisoning would be useful for improvement<br />
<strong>of</strong> clinical treatment <strong>of</strong> poisoning cases. Such parameters<br />
include half-life, area under the blood concentrationtime<br />
curve (AUC), clearance (CL), volume <strong>of</strong> distribution,<br />
and mean residence time (MRT). These parameters are typically<br />
used in dosage regimen design: the half-life may be used to<br />
determine the interval between doses, and CL can be used to<br />
achieve a target AUC that is appropriate in terms <strong>of</strong> efficacy and<br />
toxicity; CL is used, for example, in the formula-based calculation<br />
<strong>of</strong> the dosage <strong>of</strong> the anticancer agent carboplatin (23).<br />
We have developed a new method for rapid analysis <strong>of</strong><br />
aconitines in serum and urine, using liquid chromatography-mass<br />
spectrometry (LC-MS) (24). The method was applied<br />
to the determination <strong>of</strong> aconitines in serum collected<br />
from five patients with aconite poisoning who were admitted<br />
to the Critical Care and Emergency Center at Iwate Medical<br />
University. In this paper, we report the toxicokinetics parameters<br />
<strong>of</strong> aconitines calculated using serial serum concentrations<br />
from the five patients.<br />
1 32 Reproduction (photocopying) <strong>of</strong> editorial content <strong>of</strong> this journal is prohibited without publisher's permission.
<strong>Journal</strong> <strong>of</strong> <strong>Analytical</strong> <strong>Toxicology</strong>, Vol. 31, April 2007<br />
Methods<br />
Patients<br />
A summary <strong>of</strong> background data for the five patients with<br />
aconite poisoning is shown in Table I. The patients comprised<br />
Table I. Pr<strong>of</strong>iles <strong>of</strong> Patients with <strong>Aconite</strong> <strong>Poisoning</strong><br />
Ingested<br />
Height Weight Parts <strong>of</strong><br />
Case Age Gender (cm) (kg) <strong>Aconite</strong> ECG* Therapy<br />
I 53 male 158 63 root VT DF<br />
Vf PCPS<br />
2 69 male 165 75 root PVC, AIVR fluid replacement<br />
3 78 female - root AIVR fluid replacement<br />
4 49 male 180 85 leaf NSVT fluid replacement,<br />
antiarrhythmic<br />
5 58 male 158 60 root NSVT fluid replacement,<br />
antiarrhythmic<br />
* Abbreviations: ECG, electrocardiogram; VT, ventricular tachycardia; DF, defibrillation; Vf, ventricular<br />
fibrillation; PCPS, percutaneous cardiopulmonary support system; PVC, premature ventricular contraction;<br />
AIVR, accelerated idioventricular rhythm; and NSVT, nonsustained ventricular tachycardia.<br />
four males and one female, with ages ranging from 49 to 78<br />
years old and a mean age (• standard deviation) <strong>of</strong> 61.4 + 11.9<br />
years old. One <strong>of</strong> the patients had ingested aconite leaves and<br />
four patients had eaten roots. The electrocardiogram findings<br />
were as follows: ventricular tachycardia (VT) and Vf in patent<br />
1, premature ventricular contraction (PVC)<br />
and accelerated idioventricular rhythm (AIVR)<br />
in patient 2, AIVR in patient 3, and non-sustained<br />
ventricular tachycardia (NSVT) in pa-<br />
tients 4 and 5. All the patients recovered from<br />
the poisoning, with case 1 requiring additional<br />
percutaneous cardiopulmonary support<br />
(PCPS) because <strong>of</strong> unstable hemodynamics.<br />
Reagents<br />
Aconitine, mesaconitine, and hypaconitine<br />
were purchased from Wako Pure Chemical<br />
Industries (Osaka, Japan); jesaconitine<br />
was purchased from Sanwa Shoyaku (Utsunomiya,<br />
Japan); and methyllycaconitine<br />
was purchased from Sigma-Aldrich (St. Louis,<br />
MO) and used as an internal standard (I.S.).<br />
Formic acid <strong>of</strong> high-performance liquid<br />
chromatography (HPLC) grade and acetonitrile<br />
<strong>of</strong> LC-MS grade were purchased from<br />
100<br />
~--- LS.<br />
A<br />
tO0.<br />
.t--- LS.<br />
C-1<br />
A<br />
5o<br />
50<br />
~/Jeuc~nittne<br />
5<br />
m,~616<br />
m/z 632<br />
................. m/'.t 646<br />
L m/z 6"/6<br />
m/z 683<br />
, . . . . , ....<br />
l0<br />
, .... . ....<br />
15<br />
i .... , ....<br />
20<br />
, ....<br />
Retention time (min)<br />
..t<br />
el<br />
ae<br />
~ ~m/Z 616<br />
mlz 632<br />
____,.._____,,.~J X I ~ .Iz646<br />
._...7 L ,,I~ 676<br />
O" ~ . . . . . . . . . mlz 683<br />
5 tO 15 20<br />
Retention time (min)<br />
~.100<br />
q LS. 100<br />
B<br />
~--- LS.<br />
C-2<br />
A~itine ~ 50<br />
5<br />
J / J vr4~(~ -/z 616<br />
I ',. J\ I/ "~63:<br />
I x.~ i L ........ ~'z646<br />
/ L. m,~ a6<br />
................................. ,,,'z ~ 0<br />
10 15 20<br />
Retention time (min)<br />
5<br />
Jmcmilme<br />
....... ,t<br />
10 15 20<br />
Retention time (min)<br />
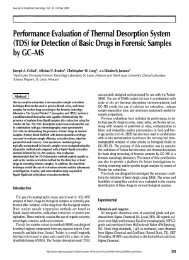
Figure I. Selected ion-monitoring chromatograms <strong>of</strong> aconitines. Selected ions for aconitine: m/z 646; hypaconitine: m/z 616; jesaconitine: m/z 676; mesaconitine:<br />
m/z 632; and methyllycaconitine (I.S.): m/z 683. Blank serum (A); spiked serum (I .0 nglmL) (B); patient sample (case I): 7 h after ingestion (C-I); and<br />
patient sample (case I ): 62 h after ingestion (C-2).<br />
m/Z 616<br />
m/Z 632<br />
m/Z 646<br />
m/Z 6'16<br />
m/Z 683<br />
133
<strong>Journal</strong> <strong>of</strong> <strong>Analytical</strong> <strong>Toxicology</strong>, Vol. 31, April 2007<br />
Kanto Kagaku (Tokyo, Japan). Other reagents were <strong>of</strong><br />
analytical reagent grade and were purchased from Wako Pure<br />
Chemical Industries.<br />
Sample preparation and equipment<br />
One milliliter <strong>of</strong> serum was mixed with 2.5 ng <strong>of</strong> I.S. and 2 mL<br />
<strong>of</strong> 0.025% (v/v) ammonia solution. The mixture was applied to<br />
i<br />
2<br />
Case 1<br />
3 i ..........................................<br />
9 : Acxmitine<br />
1<br />
!o<br />
-1<br />
-2<br />
-3<br />
-4<br />
3<br />
i 2<br />
1<br />
134<br />
!_l<br />
g0<br />
-2<br />
~-3<br />
[]<br />
9 : J~itine<br />
[] : Mesaconitine<br />
1() 20 3~) 40 5() 60 70<br />
Time after ingestion Cn)<br />
Case2<br />
r<br />
r<br />
: : Ae~nitine<br />
Jes~emfine<br />
: Mesaconifine<br />
, r i<br />
i<br />
Cue 4<br />
3 i ................................................................................................................................<br />
9 : Aconitiae<br />
1 9 : Jutine<br />
o 2'o 3'0 5o 7o<br />
Time after ingestion (h)<br />
Cue5<br />
~2 9 9 : Jeacceitine<br />
[] : Memumitine<br />
1<br />
9 -<br />
0 10 20 30 40 50 60 70 0 10 20 30 40 50 60 70<br />
Time after ingestion (h)<br />
Time after ingestion ~)<br />
Case 3<br />
9 : Aconithte<br />
; Hypac~mtine<br />
[] : Mesaconitine<br />
O 10 20 30 40 50 60 70<br />
Time after ingestion (11)<br />
Figure 2. Logarithmic serum concentrations <strong>of</strong> aconitines after ingestion <strong>of</strong> aconite. The lines in<br />
each graph indicate regression lines. A regression equation for each patient was obtained from<br />
logarithmically transformed serum aconitine concentrations and time after ingestion. Case 1:<br />
aconitine, y = -0.039x - 1.754 (R 2 = 0.992); jesaconitine, y = -0.045x + 0.216 (R 2 = 0.982).<br />
Case 2: aconitine, y = -0.186x + 0.370 (R 2 = 0.999); jesaconitine, y = -0.119x + 1.848 (R 2 =<br />
0.995); mesaconitine, y = -0.249x + 2.409 (R 2 = 0.998). Case 3: aconitine, y = -0.087x - 1.290<br />
(R 2 = 0.984); mesaconitine, y = -0.120x - 0.037 (R 2 = 0.993). Case 4: jesaconitine, y = -0.106x<br />
+ 0.429 (R 2 = 0.999). Case 5: aconitine, ,v= -0.086x - 1.552 (R 2 = 0.997); jesaconitine; y=<br />
-0.085x + 0.747 (R 2 = 0.990).<br />
an Extrelut NT3 column (Merck, Darmstadt, Germany) and the<br />
column was left to stand for 15 min at room temperature.<br />
Aconitines were then eluted with 15 mL <strong>of</strong> diethyl ether. The<br />
eluate was evaporated to dryness under a stream <strong>of</strong> nitrogen gas<br />
in a heat block at 40~ and dissolved in 0.2 mL <strong>of</strong> the mobile<br />
phase. The serum samples were stored at --80~ and measurernents<br />
were made within three days after sample collection.<br />
LC was performed on a Waters 2690 in-<br />
strument (Waters, Milford, MA). Separation<br />
was achieved using an XTerra RP18 column<br />
(150 x 2.l-ram i.d., 3.5-1Jm particle size, Waters)<br />
protected by a guard column (10 x 2.lmm<br />
i.d.) containing the same packing. The<br />
injection volume was set to 20 IJL, and the<br />
mobile phase was a mixture <strong>of</strong> 0.1% (v/v)<br />
formic acid in acetonitrile and 0.1% (v/v)<br />
formic acid in aqueous solution (24:76, v/v),<br />
with a flow rate <strong>of</strong> 0.2 mL/min. The column<br />
temperature was maintained at 40~<br />
MS was performed on a Micromass ZMD<br />
4000 instrument (Waters) operating in the<br />
electrospray ionization positive ion mode. The<br />
MS parameters were as follows: capillary potential,<br />
3.0 kV; cone voltage, 60 V; ion source<br />
temperature, 120~ drying gas temperature,<br />
350~ and nitrogen gas flow rate, 350 L/h.<br />
Measurements were carried out in the selected<br />
ion monitoring mode, and the mass-tocharge<br />
values <strong>of</strong> the monitoring ion were 646<br />
for aconitine, 616 for hypaconitine, 676 for jesaconitine,<br />
632 for mesaconitine, and 683 for<br />
methyllycaconitine (I.S.). The monitoring ion<br />
reflects the protonated alkaloid and formed<br />
the main peak for each alkaloid. No interfering<br />
endogenous substances were observed<br />
in blank serum samples.<br />
Toxicokinetics parameters <strong>of</strong> aconitines<br />
Concentrations <strong>of</strong> serum aconitines were<br />
plotted logarithmically against time after ingestion,<br />
and a serum concentration-time<br />
curve was obtained. The time <strong>of</strong> ingestion <strong>of</strong><br />
aconite is shown as 0 h, and the time after ingestion<br />
was obtained from the patient or their<br />
family. Regression analysis <strong>of</strong> these data was<br />
performed for each patient, using at least<br />
three concentration-time data points in the<br />
terminal log-linear phase. The elimination<br />
velocity constant (Kel) was calculated as Ke~ =<br />
slope, where the slope is that <strong>of</strong> the regression<br />
line. Serum half-lives for each alkaloid were<br />
calculated using the following equation: halflife<br />
= 0.693/Kel. AUC (from 0 to infinity) was<br />
calculated using the logarithmic trapezoidal<br />
method with extrapolation to infinity, and<br />
MRT was calculated as MRT = AUMC/AUC,<br />
where AUMC is the area under the moment<br />
curve from 0 to infinity.
<strong>Journal</strong> <strong>of</strong> <strong>Analytical</strong> <strong>Toxicology</strong>, Vol. 31, April 2007<br />
Results<br />
Aconitine, jesaconitine, and mesaconitine were detected in<br />
serum in cases 1, 2 and 5, and aconitine and jesaconitine were<br />
found in case 4. Jesaconitine was the main alkaloid (that is, the<br />
alkaloid with the highest serum concentration) in cases 1, 2, 4,<br />
and 5. In case 3, the main alkaloid was mesaconitine, and hypaconitine<br />
was detected only in case 3. Chrornatograms for<br />
blank serum, spiked serum and a patient sample (case 1) are<br />
shown in Figure 1. Logarithmic serum concentrations <strong>of</strong><br />
aconitines were plotted against time after ingestion for each<br />
case (Figure 2). The log concentration-time curves showed<br />
good linearity from 20 h after ingestion in case 1, from 8 h after<br />
ingestion in case 2, from 6 h after ingestion in case 3, from 12<br />
h after ingestion in case 4, and from 5 h after ingestion in case<br />
5.<br />
The toxicokinetics parameters for aconitines obtained from<br />
the log concentration-time curves are shown in Table II. In case<br />
1, the Kel values for aconitine and jesaconitine (the main alkaloid)<br />
were 0.039 h -1 and 0.045 h -1, respectively, and the halflives<br />
were 17.8 h and 15.4 h, respectively. In case 2, the Kel<br />
values for aconitine, jesaconitine (the main alkaloid) and<br />
mesaconitine were 0.186 h -1, 0.119 h -1, and 0.249 h -1, respectively,<br />
and the half-lives were 3.7 h, 5.8 h, and 2.8 h, respectively.<br />
In case 3, the Kel values for aconitine and mesaconitine<br />
(the mainalkaloid) were 0.087 h -1 and 0.120 h -1, respectively,<br />
and the half-lives were 8.0 h and 5.8 h, respectively. In case 4,<br />
the Kel for jesaconitine (the main alkaloid) was 0.106 h -1, and<br />
the half-life was 6.5 h. In case 5, the K~l values for aconitine and<br />
jesaconitine (the main alkaloid) were 0.086 h -1 and 0.085 h -1,<br />
and the half-lives were 8.1 h and 8.2 h, respectively.<br />
In case 1, the AUCs for aconitine and jesaconitine (the main<br />
alkaloid) were 5.1 ng.h/mL and 28.6 ng.h/mL, respectively,<br />
and the MRTs were 23.6 h and 22.6 h, respectively. In case 2,<br />
the AUCs for aconitine, jesaconitine (the main alkaloid) and<br />
mesaconitine were 3.1 ng.h/mL, 33.5 ng.h/mL and 13.0<br />
Table II. Toxicokinetics Parameters <strong>of</strong> Aconitines<br />
I~i* Half- AUC<br />
Case Aconitines (h ~ Life (h) (ng, h/mL) MET (h)<br />
1 Aconitine 0.039 17.8 5.1 23.6<br />
Jesaconitine* 0.045 15.4 28.6 22.6<br />
2 Aconitine 0.186 3.7 3.1 10.8<br />
Jesaconitine* 0.119 5.8 33.5 12.8<br />
Mesaconitine 0.249 2.8 13.0 9.7<br />
3 Aconitine 0.087 8.0 2.4 14.8<br />
Mesaconitine t 0.120 5.8 5.4 11.9<br />
4 Jesaconitine t 0.106 6.5 6.9 17.2<br />
5 Aconitine 0.086 8.1 2.7 10.9<br />
Jesaconitine t 0.085 8.2 26.1 11.5<br />
* Abbreviations: Kel, elimination velocity constant; AUC, area under the blood<br />
concentration-time curve; and MRT, mean residence time.<br />
~" Main alkaloid: the alkaloid with the highest serum concentration among the<br />
detected aconitines.<br />
ng.h/mL, respectively, and the MRTs were 10.8 h, 12.8 h and 9.7<br />
h, respectively. In case 3, the AUCs for aconitine and mesaconitine<br />
(the main alkaloid) were 2.4 ng.h/mL and 5.4 ng.h/mL, respectively,<br />
and the MRTs were 14.8 h and 11.9 h, respectively.<br />
In case 4, the AUC for jesaconitine (the main alkaloid) was 6.9<br />
ng.h/mL, and the MRT was 17.2 h. In case 5, the AUCs for<br />
aconitine and jesaconitine (the main alkaloid) were 2.7<br />
ng.h/mL and 26.1 ng.h/mL, respectively, and the MRTs were<br />
10.9 h and 11.5 h, respectively.<br />
Discussion<br />
In this study, we determined toxicokinetics parameters (halflife,<br />
AUC, MRT) for aconitines in five patients with aconite<br />
poisoning. Ito et al. (22) have studied the distribution <strong>of</strong> aconitine<br />
alkaloids in an autopsy case, and Moritz et al. (14) determined<br />
the half-life <strong>of</strong> aconitine in a poisoning case, but the<br />
current study is the first report <strong>of</strong> the toxicokinetics parameters<br />
<strong>of</strong> aconitines in patients with aconite poisoning. The halflives<br />
<strong>of</strong> the main alkaloid ranged from 5.8 to 15.4 h in the five<br />
patients, and the half-lives <strong>of</strong> other detected alkaloids were<br />
similar to the half-life <strong>of</strong> the main alkaloid in each case. The<br />
half-life <strong>of</strong> hypaconitine was not calculated, but it is likely that<br />
this value would have been similar to that <strong>of</strong> other alkaloids in<br />
the same case because all aconitines detected in each case had<br />
similar half-lives and aconitine alkaloids have closely related<br />
molecular structures.<br />
After a period <strong>of</strong> four times the half-life, 93.75% <strong>of</strong> the original<br />
amount <strong>of</strong> an agent has been eliminated from the body.<br />
Therefore, our results suggest that the main alkaloid is eliminated<br />
from the body over a period <strong>of</strong> 23-62 h. However, it has<br />
been reported that aconitines can be detected in urine until 7<br />
days after ingestion, but that they are not detectable in serum<br />
24 h after ingestion (10). Similarly, aconitines were detectable<br />
in urine in our cases after they became undetectable in serum<br />
(data not shown). Aconitines are distributed in high concentration<br />
to the liver and kidney (22), and therefore it appears<br />
that aconitines mainly migrate to the liver and kidney after absorption,<br />
and are then eliminated gradually from the body.<br />
The most important pathway appears to be via the kidney,<br />
given the detection <strong>of</strong> high concentrations <strong>of</strong> aconitines in<br />
urine (8,10) and the continuous detection <strong>of</strong> aconitines in<br />
urine after intoxication (10). Therefore, deterioration in renal<br />
function may lead to a delay in excretion <strong>of</strong> aconitines, and a<br />
corresponding increase in half-life. Among our patients, the<br />
half-life <strong>of</strong> the main alkaloid in case 1 was about 2 times longer<br />
than those in the other cases, but the renal function <strong>of</strong> the patient<br />
in case 1 was considered to be normal, since clinical data<br />
for serum creatinine and blood urea nitrogen were in the<br />
normal range. These results suggest that the prolonged half-life<br />
in case 1 was not due to deterioration <strong>of</strong> renal function. However,<br />
it is <strong>of</strong> note that cardiac output in case 1 was lower than<br />
that in the other cases, due to hemodynamic instability, and the<br />
patient required PCPS; therefore, the prolonged half-life in<br />
case 1 may have been due to decreased cardiac output, rather<br />
than to deterioration <strong>of</strong> renal function.<br />
135
<strong>Journal</strong> <strong>of</strong> <strong>Analytical</strong> <strong>Toxicology</strong>, Vol. 31, April 2007<br />
The AUC <strong>of</strong> the main alkaloid was larger in cases 1, 2, and 5<br />
compared to cases 3 and 4, whereas the MRT <strong>of</strong> the main alkaloid<br />
showed a tendency to prolong in cases 1 and 4 compared<br />
with the other cases. Therefore, only case I showed high values<br />
for both AUC and MRT. Because AUC reflects the amount <strong>of</strong> exposure<br />
and MRT reflects the time <strong>of</strong> exposure, these results<br />
suggest that a larger concentration <strong>of</strong> aconitines were acting<br />
on sodium channels for a longer time in case 1, compared to<br />
the other cases. In animal experiments, it has been reported<br />
that the toxic symptoms in aconite poisoning are dependent on<br />
the dose <strong>of</strong> aconitines (25), and our findings suggest that the<br />
extent <strong>of</strong> toxic symptoms is affected not only by amount <strong>of</strong> exposure<br />
to aconitines but also by time <strong>of</strong> exposure.<br />
The AUC values in cases 3 and 4 were low compared with the<br />
other cases. The patient in case 4 was the only one to ingest<br />
leaves <strong>of</strong> the plant. The content <strong>of</strong> aconitine alkaloids varies according<br />
to the part <strong>of</strong> the plant, growth region, season, and<br />
species (26-33), and the content in roots is higher than that <strong>of</strong><br />
stems and leaves; the level <strong>of</strong> aconitines in roots was about 10<br />
times that in stems (30), and about 300 times that in leaves<br />
(29). Therefore, our results suggest that the AUC in case 4 reflects<br />
the lower alkaloid content <strong>of</strong> leaves. The patient in case<br />
3 had ingested roots, but the AUC in this patient was low compared<br />
to other cases <strong>of</strong> root ingestion. Furthermore, in case 3<br />
the main alkaloid differed from that in the other cases, and this<br />
case was also the only one in which hypaconitine was detected<br />
and in which jesaconitine was not detected. The levels <strong>of</strong> aconitine,<br />
hypaconitine, jesaconitine, and mesaconitine in aconite<br />
vary according to the part <strong>of</strong> plant, the growing region, the<br />
aconite species, and the season (26-33); therefore our results<br />
suggest that the alkaloid level and composition in case 3 was<br />
influenced by one or more <strong>of</strong> these variables.<br />
Overall, the calculated toxicokinetics parameters may give an<br />
indication <strong>of</strong> the severity <strong>of</strong> toxic symptoms in aconite poisoning;<br />
however, a mechanistic study and calculation <strong>of</strong> toxicokinetics<br />
parameters in a larger numbers <strong>of</strong> patients are<br />
needed for full establishment <strong>of</strong> the relationship between toxic<br />
symptoms and toxicokinetics.<br />
References<br />
1. H. Sato, C. Yamada, C. Konno, Y. Ohizumi, K. Endo, and H.<br />
Hikino. Pharmacological actions <strong>of</strong> aconitine alkaloids. Tohoku<br />
J. Exp. Med. 128:175-187 (1979).<br />
2. F.E. Camps. Gradwohl's Legal Medicine. John Wright & Sons,<br />
Bristol, CT, 1968, p 674.<br />
3. E. Rentoul and H. Smith. Glaister's Medical Jurisprudence and<br />
<strong>Toxicology</strong>. Churchill Livingstone, Edinburgh, Scotland, 1973,<br />
pp 520-521.<br />
4. Y.T. Tai, RP.H. But, K. Young, and C.P. Lau. Cardiotoxicity after accidental<br />
herb-induced aconite poisoning. Lancet 340" 1254-1256<br />
(1992).<br />
5. P. Dickens, Y.T. Tai, RP.H. But, B. Tomlinson, H.K. Ng, and K.W.<br />
Yah. Fatal accidental aconitine poisoning following ingestion <strong>of</strong><br />
Chinese herbal medicine: a report <strong>of</strong> two cases. Forensic Sci. Int.<br />
67:55-58 (1994).<br />
6. RP.H. But, Y.T. Tai, and K. Young. Three fatal cases <strong>of</strong> herbal<br />
aconite poisoning. Vet. Hum. Toxicol. 36:212-215 (1994).<br />
7. C.C. Lin, T.Y.K. Chan, and J.F. Deng. Clinical features and man-<br />
agement <strong>of</strong> herb-induced aconitine poisoning. Ann. Emerg. Med.<br />
43' 574-579 (2004).<br />
8. N. Yoshioka, K. Gonmori, A. Tagashira, O. Boonhooi, M.<br />
Hayashi, Y. Saito, and M. Mizugaki. A case <strong>of</strong> aconitine poisoning<br />
with analysis <strong>of</strong> aconitine alkaloids by GC/SIM. Forensic<br />
Sci. Int. 81:117-123 (1996).<br />
9. A. Mori, M. Mukaida, I. Ishiyama, J. Hori, Y. Okada, M. Sasaki, K.<br />
Mii, and M. Mizugaki. Homicidal poisoning by aconite: report <strong>of</strong><br />
a case from the viewpoint <strong>of</strong> clinical forensic medicine. Jpn. ].<br />
Legal Med. (Nippon Hoigaku Zasshi) 44:352-357 (1990) (in<br />
Japanese, English abstract).<br />
10. K. Kurasawa, H. Ohfusa, H. Matsuo, K. Matsuzawa, E. Kishi, K.<br />
Matsubayashi, D. Maruyama, and M. Mizugaki. A case <strong>of</strong> "Torikabuto"<br />
intoxication with documented follow-up measurements <strong>of</strong><br />
Aconitum alkaloids in the urine. Jpn. J. Toxicol. (Chudoku<br />
Kenkyu) 6:185-188 (1993) (in Japanese, English abstract).<br />
11. Y. Ohno. The experimental approach to the murder case <strong>of</strong><br />
aconite poisoning. J. Toxicol. Toxin. Rev. 17:1-11 (1998).<br />
12. M. Imazio, R. Belli, F. Pomari, E. Cecchi, A. Chinaglia, G.<br />
Gaschino, A. Ghisio, R. Trinchero, and A. Brusca. Malignant<br />
ventricular arrhythmias due to Aconitum napellus seeds. Circulation<br />
102:2907-2908 (2000)..<br />
13. S.P. Elliott. A case <strong>of</strong> fatal poisoning with the aconite plant: quantitative<br />
analysis in biological fluid. ScL Justice 42:111-115 (2002).<br />
14. F. Moritz, P. Compagnon, I.G. Kaliszczak, Y. Kaliszczak, V.<br />
Caliskan, and C. Girault. Severe acute poisoning with homemade<br />
Aconitum napellus capsules: toxicokinetic and clinical<br />
data. Clin. Toxicol. 43:873-876 (2005).<br />
15. K. Peper and W. Trautwein. The effect <strong>of</strong> aconitine on the membrane<br />
current in cardiac muscle. Pflugers Arch Gesamte Physiol<br />
Menschen Tiere 296:328-336 (1967).<br />
16. W.A. Catterall. Cooperative activation <strong>of</strong> action potential Na+<br />
ionophore by neurotoxins. Proc. Natl. Acad. Sci. U.S.A. 72:<br />
1782-1786 (1975).<br />
17. W.A. Catterall. Neurotoxins as allosteric modifiers <strong>of</strong> voltagesensitive<br />
sodium channels. Adv. Cytopharmacol. 3:305-316<br />
(1979).<br />
18. W.A. Catterall. Neurotoxins that act on voltage-sensitive sodium<br />
channels in excitable membranes. Annu. Rev. Pharmacol. Toxicol.<br />
20:15-43 (1980).<br />
19. W.A. Catterall. Structure and function <strong>of</strong> voltage-sensitive ion<br />
channels. Science 242:50-61 (1988).<br />
20. J. Friese, J. Gleitz, U.T. Gutser, J.F. Heubach, T. Matthiesen, B. Wilffert,<br />
and N. Selve. Aconitum sp. alkaloids: the modulation <strong>of</strong><br />
voltage-dependent Na+ channels, toxicity and antinociceptive<br />
properties. Eur. J. Pharmacol. 337:165-174 (1997).<br />
21. A. Ameri. The effects <strong>of</strong> Aconitum alkaloids on the central nervous<br />
system. Prog. Neurobiol. 56:211-235 (1998).<br />
22. K. Ito, S. Tanaka, M. Funayama, and M. Mizugaki. Distribution <strong>of</strong><br />
Aconitum alkaloids in body fluids and tissues in a suicidal case <strong>of</strong><br />
aconite ingestion. J. Anal. Toxicol. 24:348-353 (2000).<br />
23. A.H. Calvert, D.R. Newell, L.A. Gumbrell, S. O'Reilly, M. Burnell,<br />
F.E. Boxall, Z.H. Siddik, I.R. Judson, M.E. Gore, and E. Wiltshaw.<br />
Carboplatin dosage: prospective evaluation <strong>of</strong> a simple formula<br />
based on renal function. J. Clin. Oncol. 7:1748-1756 (1989).<br />
24. Y. Fujita, M. Fujita, H. Niitsu, K. Oikawa, K. Terui, T. Akatsu, M.<br />
Kikuchi, N. Sato, H. Aoki, K. Takahashi, and S. Endo. A simple<br />
and rapid method for analysis <strong>of</strong> Aconitum alkaloids in serum and<br />
urine using liquid chromatography electrospray ionization mass<br />
spectrometry. J. Trad. Med. (Wakan lyakugaku Zasshi) 22:49-54<br />
(2005).<br />
25. S.D. Yakazu. Bibliographic studies on the intoxication <strong>of</strong> aconitine<br />
root (Uzu, Bushi). Part I. Jpn. J. Orient. Med. (Nippon Toyo<br />
Igaku Zasshi) 9:55-64 (1958) (in Japanese).<br />
26. F. Kurosaki, T. Yatsunami, T. Okamoto, and Y. Ichinohe. Separation<br />
and quantitative analysis <strong>of</strong> diterpene alkaloids in Japanese<br />
Aconitum roots. Yakugaku Zasshi 98:1267-1273 (1978) (in<br />
Japanese, English abstract).<br />
27. M. Nakano and T. Yamagishi. Quantitative analysis <strong>of</strong> aconitine<br />
136
<strong>Journal</strong> <strong>of</strong> <strong>Analytical</strong> <strong>Toxicology</strong>, Vol. 31, April 2007<br />
alkaloids in "Bushi" and "Uzu", aconiti tuber, by high performance<br />
liquid chromatography. Report <strong>of</strong> the Hokkaido Institute <strong>of</strong><br />
Public Health (Hokkaidoritsu Eisei Kenkyujoho), vol. 32, 1982, pp<br />
21-26 (in Japanese, English abstract).<br />
28. H. Hikino, S. Shiota, M. Takahashi, and M. Murakami. Seasonal<br />
dynamics <strong>of</strong> the accumulation <strong>of</strong> aconitine alkaloids in Aconitum<br />
carmichaeli roots. Shoyakugaku Zasshi 37:68-72 (1983)(in<br />
Japanese, English abstract).<br />
29. M. Mizugaki and K. Ito. A forensic toxicological study on<br />
Aconitum alkaloids. Res. Pract. Forensic Med. (Hoigaku No Jissai<br />
To Kenkyu) 44:1-16 (2001) (in Japanese, English abstract).<br />
30. M. Ogata, T. Itou, H. Tuji, and Y. Kasahara. Qualitative and quantitative<br />
analysis <strong>of</strong> aconitine analogs in Aconitum plants. Report<br />
<strong>of</strong> the Yamagata Prefectural Institute <strong>of</strong> Public Health (Yamagataken<br />
Eisei Kenkyujoho), vol. 36, 2003, pp 54-57 (in Japanese).<br />
31. M. Taki, T. Matsuba, M. Fukuchi, M. Aburada, and M. Okada.<br />
Comparison <strong>of</strong> seasonal variations on growth <strong>of</strong> Aconitum<br />
carmichaeli DEBX. and constituents <strong>of</strong> root tubers cultivated in<br />
Hokkaido and Ibaraki prefecture. Natural Medicines 58:55-63<br />
(2004) (in Japanese, English abstract).<br />
32. K. Okada and K. Kawaguchi. Change in chemical component<br />
characters within and among years <strong>of</strong> aconite. Natural Medicines<br />
59:36-41 (2005) (in Japanese, English abstract).<br />
33. Z.H. Jiang, Y. Xie, H. Zhou, J.R. Wang, Z.Q. Liu, Y.F. Wong, X.<br />
Cai, H.X. Xu, and L. Liu. Quantification <strong>of</strong> Aconitum alkaloids in<br />
aconite roots by a modified RP-HPLC method. Phytochem. Anal.<br />
16:415-421 (2005).<br />
Manuscript received July 5, 2006;<br />
revision received September 20, 2006.<br />
137