Lipoprotein Lipase Activity in Skeletal Muscle Is Related to Insulin ...
Lipoprotein Lipase Activity in Skeletal Muscle Is Related to Insulin ...
Lipoprotein Lipase Activity in Skeletal Muscle Is Related to Insulin ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Lipoprote<strong>in</strong></strong> lipase activity <strong>in</strong> skeletal muscle is related <strong>to</strong> <strong>in</strong>sul<strong>in</strong> sensitivity.<br />
T Pollare, B Vessby and H Lithell<br />
Arterioscler Thromb Vasc Biol. 1991;11:1192-1203<br />
doi: 10.1161/01.ATV.11.5.1192<br />
Arteriosclerosis, Thrombosis, and Vascular Biology is published by the American Heart Association, 7272 Greenville<br />
Avenue, Dallas, TX 75231<br />
Copyright © 1991 American Heart Association, Inc. All rights reserved.<br />
Pr<strong>in</strong>t ISSN: 1079-5642. Onl<strong>in</strong>e ISSN: 1524-4636<br />
The onl<strong>in</strong>e version of this article, along with updated <strong>in</strong>formation and services, is located on the<br />
World Wide Web at:<br />
http://atvb.ahajournals.org/content/11/5/1192<br />
Permissions: Requests for permissions <strong>to</strong> reproduce figures, tables, or portions of articles orig<strong>in</strong>ally published <strong>in</strong><br />
Arteriosclerosis, Thrombosis, and Vascular Biology can be obta<strong>in</strong>ed via RightsL<strong>in</strong>k, a service of the Copyright<br />
Clearance Center, not the Edi<strong>to</strong>rial Office. Once the onl<strong>in</strong>e version of the published article for which permission<br />
is be<strong>in</strong>g requested is located, click Request Permissions <strong>in</strong> the middle column of the Web page under Services.<br />
Further <strong>in</strong>formation about this process is available <strong>in</strong> the Permissions and Rights Question and Answerdocument.<br />
Repr<strong>in</strong>ts: Information about repr<strong>in</strong>ts can be found onl<strong>in</strong>e at:<br />
http://www.lww.com/repr<strong>in</strong>ts<br />
Subscriptions: Information about subscrib<strong>in</strong>g <strong>to</strong> Arteriosclerosis, Thrombosis, and Vascular Biology is onl<strong>in</strong>e<br />
at:<br />
http://atvb.ahajournals.org//subscriptions/<br />
Downloaded from http://atvb.ahajournals.org/ by guest on August 29, 2013
1192<br />
<strong>Lipoprote<strong>in</strong></strong> <strong>Lipase</strong> <strong>Activity</strong> <strong>in</strong> <strong>Skeletal</strong> <strong>Muscle</strong><br />
<strong>Is</strong> <strong>Related</strong> <strong>to</strong> Insul<strong>in</strong> Sensitivity<br />
T. Pollare, B. Vessby, and H. Lithell<br />
The relative effects of obesity, alone or <strong>in</strong> comb<strong>in</strong>ation with <strong>in</strong>sul<strong>in</strong> resistance and hyper<strong>in</strong>sul<strong>in</strong>emia<br />
(with or without diabetes), on lipoprote<strong>in</strong> concentrations, blood pressure, and other<br />
risk fac<strong>to</strong>rs for cardiovascular disease were <strong>in</strong>vestigated <strong>in</strong> 28 men (mean age, 63 years).<br />
Special attention was given <strong>to</strong> lipoprote<strong>in</strong> lipase (LPL) activity <strong>in</strong> tissues and <strong>to</strong> posthepar<strong>in</strong><br />
plasma LPL activity and hepatic lipase activity and their relation <strong>to</strong> <strong>in</strong>sul<strong>in</strong> resistance. The 28<br />
men fulfilled the entrance criteria of the study so that they could be allocated <strong>to</strong> one of the four<br />
groups (seven <strong>in</strong> each group): 1) normal body weight, normal fast<strong>in</strong>g <strong>in</strong>sul<strong>in</strong> level, and normal<br />
glucose <strong>to</strong>lerance (controls); 2) the same as <strong>in</strong> group 1 but with moderate obesity; 3) the same<br />
as <strong>in</strong> group 2 but with fast<strong>in</strong>g hyper<strong>in</strong>sul<strong>in</strong>emia; 4) the same as <strong>in</strong> group 3 but with<br />
non-<strong>in</strong>sul<strong>in</strong>-dependent diabetes mellitus. Glucose <strong>in</strong>fusion rate for the control group was<br />
8.1±2.1 mg/kg body wt/m<strong>in</strong> (mean±SD) at an <strong>in</strong>sul<strong>in</strong> <strong>in</strong>fusion rate of 56 milliunits/m 2 /m<strong>in</strong>.<br />
The average values <strong>in</strong> groups 2, 3, and 4 were 6.0±0.7, 3.2±0.5, and 1.9±1.0 mg/kg body<br />
wt/m<strong>in</strong>, respectively. Concentrations of very low density lipoprote<strong>in</strong>s as well as blood pressure<br />
and urate concentrations were highest and those of high density lipoprote<strong>in</strong>s were lowest <strong>in</strong> the<br />
two hyper<strong>in</strong>sul<strong>in</strong>emic groups (groups 3 and 4). <strong>Skeletal</strong> muscle LPL activity was 46 ±23,41 ±25,<br />
23 ±6, and 31 ±13 milliunits/g wet wt (mean±SD) <strong>in</strong> the four groups, respectively. There was a<br />
positive correlation between glucose <strong>in</strong>fusion rate and muscle LPL activity (r=0.58,/?
Pollare et al LPL <strong>Activity</strong> and Insul<strong>in</strong> Sensitivity 1193<br />
TABLE 1.<br />
Variable<br />
Selected Variables for the Study Population<br />
Body mass <strong>in</strong>dex (kg/m 2 )<br />
Waist <strong>to</strong> hip ratio<br />
Fast<strong>in</strong>g glucose<br />
concentration (mmol/1)<br />
Fast<strong>in</strong>g <strong>in</strong>sul<strong>in</strong><br />
concentration (milliunits/1)<br />
HbA lc (%)<br />
Intravenous glucose<br />
<strong>to</strong>lerance (%/m<strong>in</strong>)<br />
Glucose <strong>in</strong>fusion rate (mg/kg<br />
body wt/m<strong>in</strong>/milliunitxlOO)<br />
Normal-weight<br />
control<br />
24.0±1.5<br />
0.87 ±0.04<br />
5.3±0.5<br />
5.1±3.4<br />
5.0±0.4<br />
1.7±0.6<br />
9.7 ±2.9<br />
Subgroup<br />
Obese<br />
normo<strong>in</strong>sul<strong>in</strong>emic<br />
30.1 ±2.5*<br />
0.93 ±0.04<br />
5.2±0.3<br />
7.3±2.5<br />
4.6±0.5<br />
1.3 ±0.5<br />
6.8±1.6*<br />
Obese<br />
hyper<strong>in</strong>sul<strong>in</strong>emic<br />
31.7±4.6<br />
0.97±0.07<br />
5.7±0.4<br />
23.6±4.8t<br />
4.7 ±0.4<br />
1.3+0.4<br />
2.8+0.6*<br />
Obese<br />
diabetic<br />
30.4±2.6*<br />
0.99±0.05<br />
9.6±2.7*<br />
19.1 ±8.3*<br />
6.9±1.8f<br />
0.5 ±0.2*<br />
1.5 ±0.6*<br />
Values are mean±SD for selected variables <strong>in</strong> the four subgroups (n = 7 <strong>in</strong> each group). Comparisons were made<br />
between the obese groups and the normal-weight normo<strong>in</strong>sul<strong>in</strong>emic men.<br />
HbA lc , the glycosylated form of the major component of adult hemoglob<strong>in</strong> fraction Ai.<br />
*p
1194 Arteriosclerosis and Thrombosis Vol 11, No 5 September/Oc<strong>to</strong>ber 1991<br />
days, with an <strong>in</strong>terval of 2-3 days between each<br />
<strong>in</strong>vestigation. Dietary his<strong>to</strong>ry had revealed a fat <strong>in</strong>take<br />
of 32-38% of energy and of carbohydrates of 42-52%<br />
of energy. 6 For this particular study each participant<br />
was <strong>in</strong>structed <strong>to</strong> adhere <strong>to</strong> his regular diet but <strong>to</strong><br />
ma<strong>in</strong>ta<strong>in</strong> an <strong>in</strong>take of at least 250 g carbohydrates<br />
daily and <strong>to</strong> refra<strong>in</strong> from extreme physical exercise or<br />
<strong>in</strong>activity for at least 5 days before the <strong>in</strong>vestigation.<br />
Smokers were <strong>in</strong>structed not <strong>to</strong> smoke on the morn<strong>in</strong>g<br />
of the <strong>in</strong>vestigation. No other <strong>in</strong>structions regard<strong>in</strong>g<br />
diet or exercise were given dur<strong>in</strong>g the study. Blood<br />
samples were drawn, and ur<strong>in</strong>e specimens were collected<br />
after an overnight (12-hour) fast.<br />
Blood pressure and heart rate. Blood pressure was<br />
measured by mercury sphygmomanometry three times<br />
<strong>in</strong> the sup<strong>in</strong>e position after a rest of 10 m<strong>in</strong>utes and<br />
twice after 1 m<strong>in</strong>ute of stand<strong>in</strong>g. The mean of each of<br />
these sets of values was used <strong>in</strong> the analyses. A large<br />
cuff was used when appropriate. The pulse rate was<br />
recorded before each blood pressure measurement.<br />
Intravenous glucose <strong>to</strong>lerance test. The IVGTT was<br />
performed, as recently described <strong>in</strong> detail, 10 by <strong>in</strong>jection<br />
of 300 mg glucose/kg body wt. Plasma glucose<br />
was measured by the glucose oxidase method. Immunoreactive<br />
<strong>in</strong>sul<strong>in</strong> was assayed <strong>in</strong> plasma by use of a<br />
commercial radioimmunoassay kit (Phadeseph Insul<strong>in</strong><br />
RIA, Pharmacia, Uppsala, Sweden). Glucose<br />
<strong>to</strong>lerance was expressed as the k value, as described<br />
by Ikkos and Luft. 11 The peak <strong>in</strong>sul<strong>in</strong> response was<br />
def<strong>in</strong>ed as the mean of the values obta<strong>in</strong>ed at 2, 4,<br />
and 6 m<strong>in</strong>utes, and the <strong>in</strong>sul<strong>in</strong> <strong>in</strong>dex was def<strong>in</strong>ed as<br />
the ratio between the peak and basal plasma <strong>in</strong>sul<strong>in</strong><br />
values (mean of values at —10, -5, and 0 m<strong>in</strong>utes).<br />
The areas under the curves for glucose and <strong>in</strong>sul<strong>in</strong><br />
dur<strong>in</strong>g the IVGTT were calculated as the deviations<br />
from the basal value <strong>in</strong>tegrated over the sampl<strong>in</strong>g<br />
time. The average fast<strong>in</strong>g plasma <strong>in</strong>sul<strong>in</strong> and glucose<br />
concentrations were calculated from four samples<br />
taken on two separate days. The glycosylated form of<br />
the major component of adult hemoglob<strong>in</strong> fraction<br />
A, (HbA lc ) was measured by fast-performance liquid<br />
chroma<strong>to</strong>graphy (normal range, 3.5-6.0%). 12<br />
Clamp studies. The euglycemic hyper<strong>in</strong>sul<strong>in</strong>emic<br />
clamp technique, as <strong>in</strong>troduced by DeFronzo et al, 13<br />
was used and has recently been described <strong>in</strong> detail. 10<br />
The <strong>in</strong>sul<strong>in</strong> (Actrapid, Human, Novo, Denmark)<br />
<strong>in</strong>fusion rate was 56 milliunits/m 2 /m<strong>in</strong> <strong>in</strong> all subjects,<br />
result<strong>in</strong>g <strong>in</strong> a mean plasma <strong>in</strong>sul<strong>in</strong> concentration of<br />
102 milliunits/1 (range, 79-144 milliunits/1) dur<strong>in</strong>g<br />
the clamp studies. The target level of plasma glucose<br />
dur<strong>in</strong>g the clamp study was 5.3 mmol/1, and this level<br />
was ma<strong>in</strong>ta<strong>in</strong>ed by measur<strong>in</strong>g plasma glucose (Beckman<br />
Glucose Analyzer II, Beckman Instruments,<br />
Fuller<strong>to</strong>n, Calif.) every 5 m<strong>in</strong>utes and adjust<strong>in</strong>g the<br />
<strong>in</strong>fusion rate of the 20% glucose solution accord<strong>in</strong>gly.<br />
In all diabetics the desired plasma glucose level was<br />
atta<strong>in</strong>ed with<strong>in</strong> 60 m<strong>in</strong>utes from the start of the<br />
<strong>in</strong>sul<strong>in</strong> <strong>in</strong>fusion, except <strong>in</strong> two diabetic patients <strong>in</strong><br />
whom the clamp test was performed at a glucose level<br />
of about 5.7 mmol/1. Their results are <strong>in</strong>cluded <strong>in</strong> all<br />
calculations. Under steady-state conditions of euglycemia,<br />
the glucose <strong>in</strong>put (consist<strong>in</strong>g of exogenous<br />
glucose <strong>in</strong>fusion and endogenous glucose production)<br />
must equal the glucose use by all tissues of the<br />
body.<br />
Endogenous (hepatic) glucose production was<br />
quantified <strong>in</strong> persons from all four groups. Clamp<br />
studies were then performed <strong>in</strong> comb<strong>in</strong>ation with<br />
tritiated D-glucose (D[3- 3 H]glucose) <strong>to</strong> measure the<br />
effect of hyper<strong>in</strong>sul<strong>in</strong>emia on hepatic glucose production.<br />
The prim<strong>in</strong>g dose was 40 /iCi for diabetic<br />
patients and 20 p,Ci for normal subjects, and it was<br />
given as a 20-ml bolus <strong>in</strong>jection. The cont<strong>in</strong>uous<br />
<strong>in</strong>fusion provided 0.40 /nCi/m<strong>in</strong> for diabetic patients<br />
and 0.20 /iCi/m<strong>in</strong> for normal subjects. The duration<br />
of the D[3- 3 H]glucose <strong>in</strong>sul<strong>in</strong> before the start of<br />
<strong>in</strong>sul<strong>in</strong> <strong>in</strong>fusion was 120 m<strong>in</strong>utes <strong>in</strong> normal subjects<br />
and 180 m<strong>in</strong>utes <strong>in</strong> diabetic patients. Plasma samples<br />
for determ<strong>in</strong>ation of D[3- 3 H]glucose specific activity<br />
were obta<strong>in</strong>ed every 5 m<strong>in</strong>utes dur<strong>in</strong>g the last 30<br />
m<strong>in</strong>utes of the equilibration period, after which time<br />
the <strong>in</strong>sul<strong>in</strong> <strong>in</strong>fusion was begun. A steady state of<br />
glucose-specific activity was achieved by this method<br />
<strong>in</strong> each subject. Dur<strong>in</strong>g the <strong>in</strong>sul<strong>in</strong> clamp study<br />
plasma samples for D[3- 3 H]glucose specific activity<br />
were obta<strong>in</strong>ed at 15-m<strong>in</strong>ute <strong>in</strong>tervals until the last 30<br />
m<strong>in</strong>utes, at which time they were obta<strong>in</strong>ed at<br />
5-m<strong>in</strong>ute <strong>in</strong>tervals. D[3- 3 H]glucose activity was determ<strong>in</strong>ed<br />
after deprote<strong>in</strong>ization with Ba(OH) 2 -ZnSO 4<br />
and evaporation of water. 14 The specific activity of<br />
glucose was calculated by divid<strong>in</strong>g the D[3- 3 H]glucose<br />
activity by the plasma glucose concentration. D[3-<br />
3 H]glucose (5 Ci/mmol) was purchased from The<br />
Radiochemical Centre, Amersham, England.<br />
<strong>Lipoprote<strong>in</strong></strong> and Lipid Analyses<br />
TG and cholesterol concentrations <strong>in</strong> serum and<br />
lipoprote<strong>in</strong>s were determ<strong>in</strong>ed by enzymatic methods<br />
(Boehr<strong>in</strong>ger Mannheim, Mannheim, FRG) <strong>in</strong> a Multistat<br />
III F/LS (Instrumentation Labora<strong>to</strong>ries, Lex<strong>in</strong>g<strong>to</strong>n,<br />
Mass.). The analytical errors for the two<br />
methods were 1.4% and 1.7%, respectively. Very low<br />
density lipoprote<strong>in</strong>s (VLDLs) were separated by<br />
ultracentrifugation at a density of 1.006 g/ml. An<br />
MgCyphosphotungstic acid technique was applied<br />
<strong>to</strong> precipitate low density lipoprote<strong>in</strong>s (LDLs) from<br />
the bot<strong>to</strong>m fraction after ultracentrifugation. 15 The<br />
supernatant (high density lipoprote<strong>in</strong>, HDL) was<br />
analyzed for its contents of TG and cholesterol. HDL<br />
subclass 3 (HDL3) was separated from other lipoprote<strong>in</strong>s<br />
by ultracentrifugation of serum at a density of<br />
1.120 g/ml. The cholesterol and TG concentrations<br />
were measured <strong>in</strong> HDL3 (d> 1.120 g/ml), and the<br />
contents of these lipids <strong>in</strong> HDL2 were calculated as<br />
the difference between those <strong>in</strong> <strong>to</strong>tal HDL and<br />
HDL3. The lipid concentrations <strong>in</strong> LDL were calculated<br />
as the difference between those <strong>in</strong> the bot<strong>to</strong>m<br />
fraction after ultracentrifugation at a density of 1.006<br />
g/ml and those <strong>in</strong> HDL. Serum free fatty acids<br />
(FFAs) were determ<strong>in</strong>ed by an enzymatic colorimetric<br />
method supplied <strong>in</strong> a commercial kit (Wako<br />
Chemicals GmbH, Neuss, FRG) adapted for analysis<br />
Downloaded from http://atvb.ahajournals.org/ by guest on August 29, 2013
Pollare et al LPL <strong>Activity</strong> and Insul<strong>in</strong> Sensitivity 1195<br />
<strong>in</strong> the Multistat III centrifugal analyzer. Free glycerol<br />
was measured with a TG kit (Boehr<strong>in</strong>ger Mannheim),<br />
with omission of the saponification step after<br />
adaptation for use <strong>in</strong> the Multistat III.<br />
Analyses of <strong>Lipoprote<strong>in</strong></strong> <strong>Lipase</strong> Activities and the<br />
Intravenous Fat Tolerance Test<br />
Specimens of subcutaneous adipose tissue were<br />
obta<strong>in</strong>ed from the region lateral <strong>to</strong> the umbilicus<br />
(abdom<strong>in</strong>al site) by use of the technique described by<br />
Hirsch and Goldrick. 16 Biopsy samples of skeletal<br />
muscle tissue were taken from the lateral vastus<br />
muscle with an <strong>in</strong>strument described by Bergstrom. 17<br />
The tissue samples were s<strong>to</strong>red <strong>in</strong> liquid N 2 until<br />
analyzed. Each sample was weighed <strong>in</strong> the frozen<br />
condition and then <strong>in</strong>cubated <strong>in</strong> a reaction medium<br />
based on a glyc<strong>in</strong>e buffer (2.1 mol/1, pH 8.4) conta<strong>in</strong><strong>in</strong>g<br />
hepar<strong>in</strong> (240 IU/ml), a triole<strong>in</strong>-phospholipid<br />
emulsion, 18 album<strong>in</strong> (7.5 mg/ml), and serum (3%).<br />
The procedures have been described <strong>in</strong> detail elsewhere.<br />
19 " 21 The activity is expressed <strong>in</strong> milliunits (1<br />
milliunit=l nmol fatty acid released/m<strong>in</strong>) per gram<br />
wet weight of tissue.<br />
Plasma samples for determ<strong>in</strong>ation of lipase activities<br />
were drawn 40 m<strong>in</strong>utes after <strong>in</strong>travenous adm<strong>in</strong>istration<br />
of 100 IU hepar<strong>in</strong> (KabiVitrum, S<strong>to</strong>ckholm,<br />
Sweden) per kilogram body weight. 22 The activities of<br />
hepatic lipase and LPL were determ<strong>in</strong>ed by specific<br />
methods, with the use of glycerol tri[9,10(n)- 3 H]oleate<br />
as the substrate. 23 - 24 All samples were s<strong>to</strong>red at -70°C<br />
before analysis. The elim<strong>in</strong>ation rate of exogenous TG<br />
was determ<strong>in</strong>ed by the IVFTT, as described by Carlson<br />
and Rossner, 2526 with <strong>in</strong>jection of 1 ml 10%<br />
Intralipid (KabiVitrum) per kilogram body weight.<br />
Rout<strong>in</strong>e Hema<strong>to</strong>logy, Biochemistry, and Ur<strong>in</strong>alysis<br />
All other tests (sedimentation rate, hemoglob<strong>in</strong><br />
concentration, white blood cell count, platelet count,<br />
aspartate am<strong>in</strong>otransferase [ASAT], alan<strong>in</strong>e am<strong>in</strong>otransferase<br />
[ALAT], glutamyltransferase [GT],<br />
electrolyte balance, album<strong>in</strong>, creat<strong>in</strong><strong>in</strong>e, urate concentration<br />
<strong>in</strong> serum, and rout<strong>in</strong>e ur<strong>in</strong>alysis) were<br />
performed at the Department of Cl<strong>in</strong>ical Chemistry<br />
of the University Hospital, Uppsala.<br />
Calculations<br />
The <strong>to</strong>tal amount of glucose <strong>in</strong>fused serves as a<br />
measure of the subject's sensitivity <strong>to</strong> the prevail<strong>in</strong>g<br />
plasma <strong>in</strong>sul<strong>in</strong> concentration. The glucose <strong>in</strong>fusion<br />
rate dur<strong>in</strong>g the glucose clamp test is expressed per<br />
kilogram of body weight and adjusted for the mean<br />
<strong>in</strong>sul<strong>in</strong> concentration dur<strong>in</strong>g the clamp test (mg<br />
glucose/kg body wt/m<strong>in</strong>/milliunit/lxl00). 13<br />
The calculation of <strong>in</strong>sul<strong>in</strong> sensitivity is based on the<br />
assumption that endogenous hepatic glucose production<br />
is entirely suppressed (see "Results"). Ur<strong>in</strong>ary<br />
glucose losses were negligible under euglycemic conditions.<br />
Hepatic glucose production <strong>in</strong> the basal state<br />
(the last 30 m<strong>in</strong>utes of the pre-<strong>in</strong>sul<strong>in</strong>-<strong>in</strong>fusion period)<br />
was calculated by divid<strong>in</strong>g the rate of D[3-<br />
3 H]glucose <strong>in</strong>fusion (cpm/m<strong>in</strong>) by the steady-state<br />
level of glucose specific activity (dpm/mg). Dur<strong>in</strong>g<br />
the glucose and <strong>in</strong>sul<strong>in</strong> <strong>in</strong>fusions when glucose k<strong>in</strong>etics<br />
were not <strong>in</strong> a steady-state condition, the glucose<br />
appearance rate was calculated from Steele's equations<br />
<strong>in</strong> their derivative form, with a value of 0.65 for<br />
the pool fraction. The rate of endogenous (hepatic)<br />
glucose production was estimated by subtract<strong>in</strong>g the<br />
exogenous glucose <strong>in</strong>fusion rate from the <strong>to</strong>tal body<br />
glucose appearance rate, as calculated by the iso<strong>to</strong>pic<br />
tracer technique. 27 - 28<br />
Statistical Analyses<br />
Data are presented as mean±SD. An analysis of<br />
variance was performed, and all statistical comparisons<br />
among the four groups were calculated with Tukey's<br />
studentized range test. Pearson correlation coefficients<br />
were calculated. A stepwise regression analysis (maximum<br />
R 2 improvement method) was executed for some<br />
dependent variables, for example, posthepar<strong>in</strong> plasma<br />
LPL and hepatic lipase activity and LPL activity <strong>in</strong><br />
muscle and adipose tissue, with <strong>in</strong>sul<strong>in</strong> sensitivity measures,<br />
<strong>in</strong>sul<strong>in</strong> and glucose values, and anthropometric<br />
data as <strong>in</strong>dependent variables. In other series different<br />
lipoprote<strong>in</strong> and lipid concentrations were used as dependent<br />
variables, and the lipase activities were used as<br />
<strong>in</strong>dependent variables.<br />
Results<br />
The BMI and waist <strong>to</strong> hip ratio were significantly<br />
<strong>in</strong>creased <strong>in</strong> all the obese study groups compared<br />
with the normal-weight controls. In the groups of<br />
obese diabetic subjects, a significant <strong>in</strong>crease <strong>in</strong> the<br />
fast<strong>in</strong>g glucose concentration and HbA lc value and a<br />
reduction <strong>in</strong> glucose <strong>to</strong>lerance were noted (Table 1).<br />
The fast<strong>in</strong>g <strong>in</strong>sul<strong>in</strong> levels <strong>in</strong> the obese hyper<strong>in</strong>sul<strong>in</strong>emic<br />
and the obese diabetic groups did not differ<br />
from one another (p=0A5) but were significantly<br />
higher than <strong>in</strong> the other groups (/?
1196 Arteriosclerosis and Thrombosis Vol 11, No 5 September/Oc<strong>to</strong>ber 1991<br />
TABLE 2.<br />
Variable<br />
SBP sup<strong>in</strong>e<br />
SBP stand<strong>in</strong>g<br />
DBP sup<strong>in</strong>e<br />
DBP stand<strong>in</strong>g<br />
HR sup<strong>in</strong>e<br />
HR stand<strong>in</strong>g<br />
Blood Pressure Measurements<br />
Normal-weight<br />
control<br />
135 + 18<br />
128±18<br />
79±7<br />
79±10<br />
64±11<br />
70±ll<br />
for the Study Population<br />
Subgroup<br />
Obese<br />
normo<strong>in</strong>sul<strong>in</strong>emic<br />
142±16<br />
139±14<br />
82±9<br />
85 ±6<br />
69±6<br />
74±8<br />
Obese<br />
hyper<strong>in</strong>sul<strong>in</strong>emic<br />
149±13<br />
152±14t<br />
97±6*<br />
99±10 +<br />
67±8<br />
79±5<br />
Obese<br />
diabetic<br />
145±11<br />
144±llf<br />
87±7<br />
92±8*<br />
71±8<br />
82±9*<br />
Values are mean±SD for sys<strong>to</strong>lic (SBP) and dias<strong>to</strong>lic (DBP) blood pressure (mm Hg) and heart rate (HR,<br />
beats/m<strong>in</strong>) <strong>in</strong> the sup<strong>in</strong>e and stand<strong>in</strong>g positions for the four subgroups (n=7 <strong>in</strong> each group). For statistics, see footnote<br />
<strong>to</strong> Table 1.<br />
The steady-state levels of <strong>in</strong>sul<strong>in</strong> that were reached<br />
dur<strong>in</strong>g the euglycemic clamp test reflect the metabolic<br />
clearance rate of <strong>in</strong>sul<strong>in</strong>. In our study as <strong>in</strong><br />
others, 29 the mean steady-state <strong>in</strong>sul<strong>in</strong> concentrations<br />
were higher <strong>in</strong> the obese hyper<strong>in</strong>sul<strong>in</strong>emic and<br />
diabetic groups (116±15 and 124±20 milliunits/1,<br />
respectively) than <strong>in</strong> the normo<strong>in</strong>sul<strong>in</strong>emic groups<br />
(85±15 and 87±18 milliunits/1, respectively), which is<br />
consistent with a lower rate of metabolic <strong>in</strong>sul<strong>in</strong><br />
clearance <strong>in</strong> the two hyper<strong>in</strong>sul<strong>in</strong>emic groups.<br />
To evaluate the degree <strong>to</strong> which hepatic glucose<br />
production was <strong>in</strong>hibited with the present hyper<strong>in</strong>sul<strong>in</strong>emic<br />
clamp procedure <strong>in</strong> this k<strong>in</strong>d of subject, we<br />
studied hepatic glucose levels <strong>in</strong> two representatives<br />
from each group. The hepatic glucose output dur<strong>in</strong>g<br />
the last hour of the clamp study and the percentage<br />
suppression of hepatic glucose production are shown<br />
for each group separately. In normal-weight controls<br />
(n=2), these values were 2.02±0.15 and 0.11±0.04<br />
mg/kg body wt/m<strong>in</strong> and 95%, respectively; <strong>in</strong> the<br />
obese normo<strong>in</strong>sul<strong>in</strong>emic group (n=2), 2.29±0.10,<br />
0.14±0.04, and 94%; <strong>in</strong> the obese hyper<strong>in</strong>sul<strong>in</strong>emic<br />
group (n=2), 2.62±0.20, 0.20±0.03, and 92%; and <strong>in</strong><br />
the obese diabetic group (n=3), 2.87±0.10,0.34±0.02,<br />
TABLE 3. Serum Lipid Values for the Study Population<br />
Subgroup<br />
Normal-weight<br />
Obese<br />
control<br />
normo<strong>in</strong>sul<strong>in</strong>emic<br />
Variable<br />
Cholesterol (mmol/l)<br />
Serum<br />
VLDL chol<br />
LDL chol<br />
HDL chol<br />
HDLj chol<br />
HDL, chol<br />
5.53±0.77<br />
0.35±0.22<br />
4.11±0.74<br />
1.05+0.29<br />
0.40±0.28<br />
0.64±0.04<br />
5.87±1.07<br />
0.66 ±0.70<br />
4.18±1.41<br />
1.00±0.16<br />
0.28±0.14<br />
0.72±0.14<br />
Obese<br />
hyper<strong>in</strong>sul<strong>in</strong>emic<br />
5.76±0.87<br />
0.90±0.59*<br />
3.94±0.54<br />
0.86±0.16*<br />
0.25±0.11<br />
0.61 ±0.07<br />
Obese<br />
diabetic<br />
5.88±1.01<br />
0.93±0.56*<br />
4.01 ±0.94<br />
0.93±0.10<br />
0.30±0.10<br />
0.63±0.12<br />
Trigfycerides (mmol/l)<br />
Serum<br />
VLDLTG<br />
LDLTG<br />
HDLTG<br />
HDL2TG<br />
HDL3TG<br />
Plasma FFA<br />
Plasma glycerol<br />
1.42±0.59<br />
0.72±0.44<br />
0.49+0.15<br />
0.17±0.06<br />
0.08±0.05<br />
0.09±0.05<br />
0.41 ±0.18<br />
0.11+0.04<br />
2.14±1.51<br />
1.35±1.31<br />
0.51±0.21<br />
0.20±0.07<br />
0.06±0.09<br />
0.14±0.06<br />
0.50±0.14<br />
0.13±0.05<br />
2.91±1.21*<br />
2.05±0.92*<br />
0.53 ±0.25<br />
0.24±0.09*<br />
0.09±0.05<br />
0.15±0.04*<br />
0.50±0.10<br />
0.15±0.02*<br />
3.02±1.28*<br />
2.17±1.26*<br />
0.54±0.10<br />
0.26±0.07*<br />
0.08 ±0.09<br />
0.18±0.08t<br />
0.82 ±0.24*<br />
0.20±0.03*<br />
Other variables<br />
Urate<br />
ALAT<br />
GT<br />
333 ±63<br />
0.32±0.14<br />
0.29±0.21<br />
365+42<br />
0.40±0.09<br />
0.54±0.22<br />
434±155<br />
0.73 ±0.21*<br />
0.60±0.22<br />
326 ±77<br />
0.66±0.8t<br />
0.71 ±0.26*<br />
Values are mean±SD for serum lipoprote<strong>in</strong>, plasma free fatty acid, plasma free glycerol, and urate concentrations<br />
and for ALAT and GT enzyme activities for the four study groups (n=7 <strong>in</strong> each group). For statistics, see footnote<br />
<strong>to</strong> Table 1.<br />
VLDL, very low density lipoprote<strong>in</strong>; chol, cholesterol; LDL, low density lipoprote<strong>in</strong>; HDL, high density lipoprote<strong>in</strong>;<br />
TG, triglycerides; FFA, free fatty acids; ALAT, alan<strong>in</strong>e am<strong>in</strong>otransferase; GT, glutamyltransferase.<br />
Downloaded from http://atvb.ahajournals.org/ by guest on August 29, 2013
Pollare et al LPL <strong>Activity</strong> and Insul<strong>in</strong> Sensitivity 1197<br />
Insul<strong>in</strong><br />
sensitivity<br />
<strong>in</strong>dex<br />
10 1<br />
9<br />
8<br />
7<br />
6<br />
5<br />
4<br />
3<br />
2<br />
1<br />
f * * _ 1<br />
* * 4<br />
II<br />
1<br />
1<br />
1<br />
100 %<br />
1 2 3 4<br />
FIGURE 1. Bar graph show<strong>in</strong>g glucose <strong>in</strong>fusion rate (mg/kg<br />
body wt/m<strong>in</strong>/milliunitxlOO; adjusted for prevail<strong>in</strong>g <strong>in</strong>sul<strong>in</strong> concentration)<br />
dur<strong>in</strong>g the last hour of the clamp test <strong>in</strong> the four study<br />
groups: 1) normal-weight, normo<strong>in</strong>sul<strong>in</strong>emic, normoglycemic<br />
control group; 2) obese, normo<strong>in</strong>sul<strong>in</strong>emic, normoglycemic<br />
group; 3) obese, hyper<strong>in</strong>sul<strong>in</strong>emic, normoglycemic group; and 4)<br />
obese, hyper<strong>in</strong>sul<strong>in</strong>emic diabetic group. **p
1198 Arteriosclerosis and Thrombosis Vol 11, No 5 September/Oc<strong>to</strong>ber 1991<br />
TABLE 4.<br />
<strong>Lipase</strong> <strong>Activity</strong> Values for the Study Population<br />
Variable<br />
PHP HL activity (n=27)<br />
PHP LPL activity! (n=27)<br />
<strong>Muscle</strong> LPL activity! (n=26)<br />
Adipose tissue LPL activity! (n=26)<br />
k 2 dur<strong>in</strong>g IVFTT (%/m<strong>in</strong>) (/i=27)<br />
Normal-weight<br />
control<br />
8.4+3.0<br />
7.9+2.8<br />
46 ±23<br />
104+35<br />
4.3±2.4<br />
Subgroup<br />
Obese<br />
normo<strong>in</strong>sul<strong>in</strong>emic<br />
10.1±3.3<br />
7.7±2.9<br />
41 ±25<br />
101 ±37<br />
3.8±1.3<br />
Obese<br />
hyper<strong>in</strong>sul<strong>in</strong>emic<br />
11.8±4.2<br />
6.0±2.2<br />
23±6*<br />
100±23<br />
2.6+1.1<br />
Obese<br />
diabetic<br />
8.8±3.6<br />
6.5±2.0<br />
31±13<br />
96±34<br />
2.7±0.8<br />
Values are mean+SD for posthepar<strong>in</strong> plasma (PHP) lipoprote<strong>in</strong> lipase (LPL) activity, hepatic lipase (HL) activity,<br />
and lipoprote<strong>in</strong> lipase (LPL) activity <strong>in</strong> muscle and adipose tissue and for the k 2 value dur<strong>in</strong>g the <strong>in</strong>travenous fat<br />
<strong>to</strong>lerance test (IVFTT) <strong>in</strong> the four subgroups. For statistics, see footnote <strong>to</strong> Table 1.<br />
t <strong>Activity</strong> is expressed <strong>in</strong> milliunits (1 milliunit/1 = 1 nmol fatty acid released/m<strong>in</strong>) per gram wet weight of tissue or per<br />
milliliter plasma.<br />
group <strong>to</strong> the obese hyper<strong>in</strong>sul<strong>in</strong>emic group for posthepar<strong>in</strong><br />
LPL activity, skeletal muscle LPL activity, and k 2<br />
value and a gradual <strong>in</strong>crease for posthepar<strong>in</strong> hepatic<br />
lipase activity (Table 4). However, the diabetic group<br />
had not deteriorated more <strong>in</strong> any of these variables<br />
than the obese hyper<strong>in</strong>sul<strong>in</strong>emic group.<br />
Posthepar<strong>in</strong> Plasma Hepatic <strong>Lipase</strong> <strong>Activity</strong><br />
Hepatic lipase activity was strongly negatively correlated<br />
with LDL TG (r=0.58, p=0.001) and also<br />
with the TG concentration <strong>in</strong> HDL and HDL3 (Table<br />
5). Hepatic lipase activity was positively correlated<br />
with the <strong>in</strong>sul<strong>in</strong> area under the curve dur<strong>in</strong>g the<br />
IVGTT(r=0.41,p=0.03).<br />
Posthepar<strong>in</strong> Plasma <strong>Lipoprote<strong>in</strong></strong> <strong>Lipase</strong> <strong>Activity</strong><br />
LPL activity <strong>in</strong> posthepar<strong>in</strong> plasma was <strong>in</strong>versely<br />
correlated with TG concentration <strong>in</strong> serum and<br />
VLDL and positively with HDL3 cholesterol concentration<br />
(Table 5).<br />
In a stepwise regression model, 51% of the variation<br />
<strong>in</strong> posthepar<strong>in</strong> plasma LPL was expla<strong>in</strong>ed, the largest<br />
contributions com<strong>in</strong>g from the glucose <strong>in</strong>fusion rate<br />
dur<strong>in</strong>g the clamp test (partial R 2 =l9%) and fast<strong>in</strong>g<br />
blood glucose concentration (partial R 2 =14%).<br />
<strong>Lipoprote<strong>in</strong></strong> <strong>Lipase</strong> <strong>Activity</strong> <strong>in</strong> Adipose Tissue<br />
Adipose tissue LPL activity was not significantly<br />
correlated with any lipoprote<strong>in</strong> lipid variable (Table<br />
5). It was negatively correlated with HbAi c (r= -0.32,<br />
p=0.033).<br />
<strong>Lipoprote<strong>in</strong></strong> <strong>Lipase</strong> <strong>Activity</strong> <strong>in</strong> <strong>Skeletal</strong> <strong>Muscle</strong><br />
<strong>Muscle</strong> LPL activity was negatively correlated with<br />
TG concentrations <strong>in</strong> serum and VLDL and positively<br />
with LDL cholesterol concentration and <strong>in</strong>travenous<br />
fat <strong>to</strong>lerance (Table 6).<br />
<strong>Muscle</strong> LPL activity was positively correlated with<br />
the glucose <strong>in</strong>fusion rate dur<strong>in</strong>g the clamp test (Table<br />
6 and Figure 3) and negatively with <strong>in</strong>sul<strong>in</strong> concentration<br />
(Figure 4), ALAT, GT, and urate. In a stepwise<br />
regression model, 42% of the variation <strong>in</strong> muscle LPL<br />
activity was expla<strong>in</strong>ed by the glucose <strong>in</strong>fusion rate<br />
(partial R 2 =28.5%) and fast<strong>in</strong>g glucose concentration<br />
(partial i? 2 =13.5%). When these measures were accounted<br />
for, the addition of other variables did not<br />
contribute significantly <strong>to</strong> an improvement <strong>in</strong> the<br />
degree of explanation, <strong>in</strong>dicat<strong>in</strong>g, for example, that<br />
urate concentration, blood pressure, ALAT, and GT<br />
(Table 6) were not directly related <strong>to</strong> muscle LPL<br />
activity but <strong>to</strong> glucose <strong>in</strong>fusion rate (see below).<br />
Neither did the addition of serum TG concentration<br />
as an <strong>in</strong>dependent variable contribute significantly<br />
(p>0.6) <strong>to</strong> the model <strong>in</strong> the presence of glucose<br />
<strong>in</strong>fusion rate and fast<strong>in</strong>g <strong>in</strong>sul<strong>in</strong> concentration.<br />
Fractional Removal Rates<br />
The k 2 values of the IVFTT were negatively correlated<br />
with the serum TG. The k 2 value was positively<br />
correlated with glucose <strong>in</strong>fusion rate dur<strong>in</strong>g the<br />
clamp test and skeletal muscle LPL activity (Table 6).<br />
A stepwise regression analysis was performed with k 2<br />
as the dependent variable and LPL activities as the<br />
<strong>in</strong>dependent variables. Twenty-six percent of the<br />
variation <strong>in</strong> k 2 was expla<strong>in</strong>ed by skeletal muscle LPL<br />
activity. No other lipase activity improved the degree<br />
of explanation significantly. However, when glucose<br />
<strong>in</strong>fusion rate was added, the degree of explanation<br />
<strong>in</strong>creased significantly <strong>to</strong> 39%.<br />
Serum Triglycerides<br />
Serum TG levels were <strong>in</strong>versely correlated with<br />
posthepar<strong>in</strong> plasma LPL and skeletal muscle LPL<br />
activities and with glucose <strong>in</strong>fusion rate dur<strong>in</strong>g the<br />
clamp test (Table 5) and positively with ALAT<br />
(Table 6). A stepwise regression analysis was performed,<br />
with serum TG as the dependent variable<br />
and the different LPL activities, hepatic lipase activity,<br />
FFA concentration, and glucose <strong>in</strong>fusion rate<br />
dur<strong>in</strong>g the clamp test as the <strong>in</strong>dependent variables.<br />
Thirty-five percent of the variation <strong>in</strong> serum TG was<br />
expla<strong>in</strong>ed by LPL activity <strong>in</strong> posthepar<strong>in</strong> plasma,<br />
LPL activity <strong>in</strong> muscle tissue, and hepatic lipase<br />
activity, but when the effect of these variables was<br />
accounted for, neither adipose tissue LPL activity nor<br />
FFA concentration contributed significantly <strong>to</strong> an<br />
improvement <strong>in</strong> the degree of explanation.<br />
Downloaded from http://atvb.ahajournals.org/ by guest on August 29, 2013
Pollare et al LPL <strong>Activity</strong> and Insul<strong>in</strong> Sensitivity 1199<br />
TABLE 5. Correlation Coefficients Between Several Variables for the Study Population<br />
Variable<br />
PHP LPL activity<br />
PHP HL activity<br />
<strong>Muscle</strong> LPL activity<br />
AT LPL activity<br />
Serum TG<br />
r<br />
-0.47<br />
-0.30<br />
-0.39<br />
-0.07<br />
P<br />
VLDLTG<br />
0.013<br />
0.12<br />
0.047<br />
0.73<br />
r<br />
-0.51<br />
-0.22<br />
-0.44<br />
-0.10<br />
P<br />
VLDL chol<br />
0.006<br />
0.27<br />
0.024<br />
0.60<br />
r<br />
P<br />
LDLTG<br />
-0.47<br />
0.013<br />
-0.28<br />
0.13<br />
-0.38<br />
0.054<br />
-0.10<br />
0.59<br />
r<br />
0.04<br />
-0.58<br />
0.05<br />
0.23<br />
P<br />
LDL chol<br />
0.82<br />
0.001<br />
0.78<br />
0.22<br />
r<br />
0.26<br />
0.09<br />
0.52<br />
0.24<br />
P<br />
HDLTG<br />
0.18<br />
0.65<br />
0.006<br />
0.20<br />
r<br />
-0.12<br />
-0.42<br />
-0.15<br />
-0.15<br />
P<br />
HDL chol<br />
0.52<br />
0.028<br />
0.45<br />
0.41<br />
r<br />
0.30<br />
-0.04<br />
0.14<br />
0.03<br />
P<br />
HDL 3 TG<br />
0.12<br />
0.80<br />
0.49<br />
0.86<br />
r<br />
-0.32<br />
-0.37<br />
0.01<br />
-0.03<br />
P<br />
HDL 3 chol<br />
0.098<br />
0.056<br />
0.95<br />
0.85<br />
r<br />
0.51<br />
0.14<br />
0.27<br />
-0.05<br />
P<br />
0.006<br />
0.46<br />
0.16<br />
0.77<br />
r<br />
P<br />
HDL-2 chol<br />
r<br />
0.17<br />
0.39<br />
0.03<br />
-0.11<br />
0.57<br />
-0.14<br />
-0.20<br />
0.32<br />
P<br />
0.88<br />
0.49<br />
0.77<br />
0.73<br />
Correlation coefficients (r) between some variables for the study population (n=28). Statistical significance is<br />
<strong>in</strong>dicated below each r value.<br />
PHP, posthepar<strong>in</strong> plasma; LPL, lipoprote<strong>in</strong> lipase; HL, hepatic lipase; AT, adipose tissue; TG, triglycerides; VLDL,<br />
very low density lipoprote<strong>in</strong>; chol, cholesterol; LDL, low density lipoprote<strong>in</strong>; HDL, high density lipoprote<strong>in</strong>.<br />
-0.06<br />
0.14<br />
0.47<br />
0.07<br />
Free Fatty Acids<br />
Levels of FFAs were significantly <strong>in</strong>versely correlated<br />
with glucose <strong>in</strong>fusion rate and positively with<br />
HbA, c , ALAT, and GT values (Table 6). The mean<br />
value <strong>in</strong> the diabetic group was significantly higher<br />
than <strong>in</strong> the other three groups.<br />
Dias<strong>to</strong>lic Blood Pressure<br />
Dias<strong>to</strong>lic blood pressure was significantly positively<br />
correlated with <strong>in</strong>sul<strong>in</strong> concentration and <strong>in</strong>versely<br />
with glucose <strong>in</strong>fusion rate dur<strong>in</strong>g the clamp test<br />
(Table 6). Fifty-two percent of the <strong>in</strong>ter<strong>in</strong>dividual<br />
variation of dias<strong>to</strong>lic blood pressure taken while<br />
subjects were <strong>in</strong> the sup<strong>in</strong>e position was expla<strong>in</strong>ed by<br />
three fac<strong>to</strong>rs <strong>to</strong>gether: <strong>in</strong>sul<strong>in</strong> at 90 m<strong>in</strong>utes (partial<br />
R 2 =34%), glucose <strong>in</strong>fusion rate (partial R 2 =6%),<br />
and the k value at the IVGTT (partial R 2 =12%).<br />
Serum Alan<strong>in</strong>e Am<strong>in</strong>otransferase and<br />
Glutamyltransferase Concentrations<br />
Serum ALAT and GT concentrations were highest<br />
<strong>in</strong> the obese hyper<strong>in</strong>sul<strong>in</strong>emic group. The obese<br />
diabetic men (ALAT of 0.66±0.08 ;umol) and the<br />
obese hyper<strong>in</strong>sul<strong>in</strong>emic men (ALAT of 0.73 ±0.21<br />
)u,mol) had higher values than the other groups<br />
(p
1200 Arteriosclerosis and Thrombosis Vol 11, No 5 September/Oc<strong>to</strong>ber 1991<br />
TABLE 6. Correlation Coefficients Between Several Variables for the Study Population<br />
Variable<br />
ALAT<br />
r<br />
P<br />
GT<br />
r<br />
P<br />
HbA lc<br />
r<br />
P<br />
Urate<br />
r<br />
P<br />
k 2 (IVFTT)<br />
r<br />
P<br />
Serum <strong>in</strong>sul<strong>in</strong> (t=0)<br />
Glucose <strong>in</strong>fusion rate<br />
r<br />
P<br />
BMI<br />
r<br />
P<br />
<strong>Muscle</strong> LPL<br />
activity k 2 (IVFTT) Serum TG Plasma FFAs Serum ALAT DBP<br />
-0.38<br />
0.06<br />
-0.34<br />
0.09<br />
-0.03<br />
0.90<br />
-0.35<br />
0.08<br />
0.51<br />
0.01<br />
-0.4<br />
0.04<br />
0.54<br />
0.01<br />
-0.09<br />
0.67<br />
0.20<br />
0.32<br />
0.06<br />
0.77<br />
0.06<br />
0.77<br />
0.24<br />
0.22<br />
0.38<br />
0.05<br />
0.57<br />
0.002<br />
0.37<br />
0.06<br />
0.54<br />
0.003<br />
WHR<br />
r<br />
P<br />
-0.03<br />
0.88<br />
0.41<br />
0.03<br />
0.25<br />
0.20<br />
0.54<br />
0.004<br />
0.37<br />
0.05<br />
0.16<br />
0.41<br />
Correlation coefficients (r) between some variables for the study population. Statistical significance is <strong>in</strong>dicated<br />
below each r value.<br />
LPL, lipoprote<strong>in</strong> lipase; IVFTT, <strong>in</strong>travenous fat <strong>to</strong>lerance test; TG, triglycerides; FFAs, free fatty acids; ALAT,<br />
alan<strong>in</strong>e am<strong>in</strong>otransferase; DBP, dias<strong>to</strong>lic blood pressure; GT, glutamyltransferase; HbA lc , the glycosylated form of the<br />
major component of adult hemoglob<strong>in</strong> fraction A!; BMI, body mass <strong>in</strong>dex; WHR, waist <strong>to</strong> hip ratio.<br />
0.39<br />
0.03<br />
-0.06<br />
0.74<br />
-0.30<br />
0.12<br />
-0.70<br />
0.0001<br />
0.27<br />
0.17<br />
-0.54<br />
0.003<br />
0.17<br />
0.37<br />
0.52<br />
0.005<br />
0.46<br />
0.015<br />
0.77<br />
0.0001<br />
-0.14<br />
0.48<br />
-0.008<br />
0.97<br />
0.28<br />
0.15<br />
-0.58<br />
0.002<br />
0.33<br />
0.09<br />
0.59<br />
0.001<br />
0.16<br />
0.42<br />
0.06<br />
0.77<br />
0.20<br />
0.32<br />
0.64<br />
0.001<br />
0.70<br />
0.0001<br />
0.33<br />
0.08<br />
0.52<br />
0.005<br />
0.22<br />
0.27<br />
-0.02<br />
0.91<br />
0.32<br />
0.10<br />
-0.29<br />
0.15<br />
0.53<br />
0.004<br />
-0.55<br />
0.003<br />
0.25<br />
0.21<br />
low HDL cholesterol. 30 It has been recently suggested<br />
that hyper<strong>in</strong>sul<strong>in</strong>emia is a common denom<strong>in</strong>a<strong>to</strong>r<br />
for hypertension, obesity, and impaired glucose<br />
<strong>to</strong>lerance. 2 Hyper<strong>in</strong>sul<strong>in</strong>emia is the reflection and<br />
consequence of an <strong>in</strong>sul<strong>in</strong>-resistant state except for<br />
the diabetic condition, <strong>in</strong> which <strong>in</strong>sul<strong>in</strong> secretion<br />
does not match the pronounced <strong>in</strong>sul<strong>in</strong> resistance<br />
and "normal" or low <strong>in</strong>sul<strong>in</strong> concentration may prevail.<br />
1 The <strong>in</strong>sul<strong>in</strong>-resistant state thus may be regarded<br />
as the basis of a metabolic angiopathic syndrome,<br />
"syndrome X." 1<br />
In the present <strong>in</strong>vestigation for most of the fac<strong>to</strong>rs<br />
<strong>in</strong>vestigated, for example, blood pressure, lipoprote<strong>in</strong><br />
concentrations, liver enzyme activities, urate concentration,<br />
or glucose <strong>in</strong>fusion rate dur<strong>in</strong>g the clamp<br />
test, there was no clear dist<strong>in</strong>ction between the<br />
nonobese and obese subgroups, between the normo<strong>in</strong>sul<strong>in</strong>emic<br />
and hyper<strong>in</strong>sul<strong>in</strong>emic subgroups, or between<br />
the normoglycemic and hyperglycemic subgroups.<br />
The only exception was FFA concentration,<br />
which was significantly more elevated <strong>in</strong> the hyperglycemic<br />
group than <strong>in</strong> the other two obese groups. In<br />
the diabetic state adipocytes are <strong>in</strong>sul<strong>in</strong> resistant, 6<br />
and <strong>in</strong>sufficient <strong>in</strong>hibition of lipolysis <strong>in</strong> the adipocytes<br />
may expla<strong>in</strong> the higher concentration of FFAs.<br />
An elevated portal ve<strong>in</strong> concentration of fatty acids is<br />
associated with an <strong>in</strong>creased <strong>in</strong>sul<strong>in</strong> resistance <strong>in</strong> the<br />
liver, which may expla<strong>in</strong> the reduced <strong>in</strong>hibition of the<br />
glycogenolysis that causes hyperglycemia. 331 ' 32 Other<br />
variables were l<strong>in</strong>early related <strong>to</strong> measures of <strong>in</strong>sul<strong>in</strong><br />
resistance and are not particularly associated with<br />
any of the group characteristics.<br />
Dias<strong>to</strong>lic blood pressure was <strong>in</strong>versely correlated<br />
with the glucose <strong>in</strong>fusion rate (r= -0.55,p=0.003) and<br />
with the fast<strong>in</strong>g <strong>in</strong>sul<strong>in</strong> concentration (r=0.53,<br />
p=0.004), and as much as 52% of the <strong>in</strong>ter<strong>in</strong>dividual<br />
variation <strong>in</strong> dias<strong>to</strong>lic blood pressure could be expla<strong>in</strong>ed<br />
by <strong>in</strong>sul<strong>in</strong> concentration, glucose <strong>in</strong>fusion rate,<br />
and glucose <strong>to</strong>lerance. Several mechanisms l<strong>in</strong>k<strong>in</strong>g<br />
<strong>in</strong>sul<strong>in</strong> resistance <strong>to</strong> blood pressure regulation have<br />
been demonstrated. 33 In a prospective study the<br />
plasma <strong>in</strong>sul<strong>in</strong> concentration was an <strong>in</strong>dependent risk<br />
fac<strong>to</strong>r for development of hypertension <strong>in</strong> late-middleaged<br />
men dur<strong>in</strong>g a 10-year period, 34 which is the first<br />
Downloaded from http://atvb.ahajournals.org/ by guest on August 29, 2013
Pollare et al LPL <strong>Activity</strong> and Insul<strong>in</strong> Sensitivity 1201<br />
<strong>Muscle</strong><br />
LPL-activity, mu/g<br />
100<br />
80<br />
<strong>Muscle</strong><br />
LPL-activity, mu/g<br />
100 t<br />
80<br />
60<br />
r = 0.53<br />
p = 0.005<br />
0 3 6 9 12<br />
Glucose <strong>in</strong>fusion rate go'-i2O'<br />
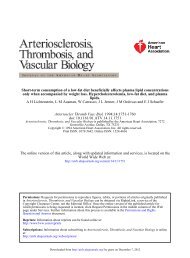
FIGURE 3. Scatterplot show<strong>in</strong>g the relation between muscle<br />
lipoprote<strong>in</strong> lipase (LPL) activity (mUlg) and glucose <strong>in</strong>fusion<br />
rate (adjusted for prevail<strong>in</strong>g <strong>in</strong>sul<strong>in</strong> concentration; mglkgbody<br />
wt/m<strong>in</strong>/mUx 100). n, Group 1; u,group 2; 9,group 3; and A,<br />
group 4 (see Figure 2, left panel).<br />
population-based support implicat<strong>in</strong>g <strong>in</strong>sul<strong>in</strong> as a fac<strong>to</strong>r<br />
contribut<strong>in</strong>g <strong>to</strong> the development of hypertension.<br />
Increased levels of ALAT and urate were found <strong>in</strong><br />
the groups with the most pronounced <strong>in</strong>sul<strong>in</strong> resistance<br />
<strong>in</strong> the present study and may be regarded as new<br />
characteristics of the <strong>in</strong>sul<strong>in</strong>-resistance syndrome.<br />
The VLDL secretion rate is related <strong>to</strong> the prevail<strong>in</strong>g<br />
<strong>in</strong>sul<strong>in</strong> concentration. 1 In the diabetic state the<br />
FFA concentration is the most important fac<strong>to</strong>r<br />
determ<strong>in</strong><strong>in</strong>g the VLDL secretion rate. 1 Both <strong>in</strong>sul<strong>in</strong><br />
and FFA concentrations are related <strong>to</strong> <strong>in</strong>sul<strong>in</strong> resistance.<br />
The results <strong>in</strong> the present study also show that<br />
the capacity for removal of circulat<strong>in</strong>g TGs is, <strong>to</strong> a<br />
large extent, related <strong>to</strong> <strong>in</strong>sul<strong>in</strong> resistance. The removal<br />
capacity was tested <strong>in</strong> a direct way by use of<br />
the IVFFT, which has been validated <strong>to</strong> reflect the<br />
catabolism of endogenous TG-rich lipoprote<strong>in</strong>s. 26<br />
Only muscle but not adipose tissue LPL activity<br />
contributed <strong>to</strong> an explanation of the <strong>in</strong>ter<strong>in</strong>dividual<br />
variation <strong>in</strong> fat <strong>to</strong>lerance (by 26%), and <strong>to</strong>gether with<br />
the glucose <strong>in</strong>fusion rate dur<strong>in</strong>g the clamp test, 39%<br />
of the variation was expla<strong>in</strong>ed. In the fast<strong>in</strong>g state<br />
about half of the hydrolysis dur<strong>in</strong>g the IVFTT takes<br />
place <strong>in</strong> skeletal muscle. 26 Our data demonstrat<strong>in</strong>g<br />
that muscle LPL activity has a key role <strong>in</strong> <strong>in</strong>travenous<br />
fat <strong>to</strong>lerance are therefore <strong>in</strong> agreement with those<br />
f<strong>in</strong>d<strong>in</strong>gs. This suggestion is further supported by the<br />
demonstration that 35% of the <strong>in</strong>ter<strong>in</strong>dividual variation<br />
of serum TG concentration was expla<strong>in</strong>ed by<br />
posthepar<strong>in</strong> plasma LPL, muscle LPL, and hepatic<br />
lipase activity <strong>to</strong>gether. The variations <strong>in</strong> both posthepar<strong>in</strong><br />
plasma LPL and muscle LPL activities were<br />
<strong>to</strong> a large degree expla<strong>in</strong>ed by glucose <strong>in</strong>fusion rate<br />
dur<strong>in</strong>g the clamp test.<br />
Also, other results <strong>in</strong>dicate that the regulation of<br />
muscle LPL activity may be related <strong>to</strong> <strong>in</strong>sul<strong>in</strong> action.<br />
For <strong>in</strong>stance, the decrease <strong>in</strong> <strong>in</strong>sul<strong>in</strong> concentrations<br />
dur<strong>in</strong>g physical exercise and the <strong>in</strong>creases dur<strong>in</strong>g diet<br />
experiments were associated with the reverse changes<br />
40<br />
20<br />
0 10 20 30 40<br />
Fast<strong>in</strong>g p-<strong>in</strong>sul<strong>in</strong>, mu/i<br />
FIGURE 4. Scatterplot show<strong>in</strong>g the relation between muscle<br />
lipoprote<strong>in</strong> lipase (LPL) activity (mU/g) and fast<strong>in</strong>g plasma<br />
(p-) <strong>in</strong>sul<strong>in</strong> concentration (mUll) <strong>in</strong> the study population.<br />
Symbols are the same as <strong>in</strong> Figure 3.<br />
<strong>in</strong> muscle LPL activity. 35 " 38 Use of a euglycemic<br />
hyper<strong>in</strong>sul<strong>in</strong>emic clamp test significantly decreased 39<br />
muscle LPL activity after 4 hours of moderate hyper<strong>in</strong>sul<strong>in</strong>emia.<br />
This demonstrates that <strong>in</strong>sul<strong>in</strong> itself (or<br />
the <strong>in</strong>creased glucose uptake <strong>in</strong> muscle cells dur<strong>in</strong>g<br />
hyper<strong>in</strong>sul<strong>in</strong>emia) downregulates muscle LPL activity.<br />
This may be <strong>in</strong>terpreted that the regulation of muscle<br />
LPL activity is not <strong>in</strong>sul<strong>in</strong> resistant and therefore, <strong>in</strong><br />
such a state when hyper<strong>in</strong>sul<strong>in</strong>emia prevails, LPL<br />
activity is downregulated.<br />
Adipose tissue LPL activity was not significantly<br />
different among the four obese and the normal-weight<br />
control groups. However, we did not measure cell size<br />
<strong>in</strong> adipose tissue. If that had been done, it may be<br />
assumed that the three obese groups would have had<br />
larger adipose cell sizes and would have expressed<br />
higher LPL activity per 10 6 cells. This is supported by<br />
a f<strong>in</strong>d<strong>in</strong>g from a previous study 40 <strong>in</strong> which there were<br />
significant correlations between hepar<strong>in</strong>-releasable<br />
ace<strong>to</strong>ne ether powder LPL activity expressed per cell<br />
and different <strong>in</strong>dexes of obesity. This correlation did<br />
not persist when ace<strong>to</strong>ne ether powder LPL activity<br />
S-ALAT,<br />
/ykat/l<br />
1.2 T<br />
r = -0.70<br />
p = 0.0001<br />
0 12 15<br />
Glucose <strong>in</strong>fusion rate 60. 120-<br />
FIGURE 5. Scatterplot show<strong>in</strong>g the relation between serum<br />
alan<strong>in</strong>e am<strong>in</strong>otransferase (S-ALAT) activity (/dcat/l) and<br />
glucose <strong>in</strong>fusion rate (adjusted for prevail<strong>in</strong>g <strong>in</strong>sul<strong>in</strong> concentration;<br />
mg/kg body wt/m<strong>in</strong>/mUxlOO). Symbols are the same<br />
as <strong>in</strong> Figure 3.<br />
Downloaded from http://atvb.ahajournals.org/ by guest on August 29, 2013
1202 Arteriosclerosis and Thrombosis Vol 11, No 5 September/Oc<strong>to</strong>ber 1991<br />
was expressed per gram. However, it may be questioned<br />
that LPL activity should be expressed per 10 6<br />
cells because we analyzed the hepar<strong>in</strong>-releasable<br />
(extracellular) part. Thus, by analogy, muscle LPL<br />
activity should have been expressed per 10 6 muscle<br />
fibers because muscle fiber size is also related <strong>to</strong><br />
obesity. However, we regard the significant correlations<br />
between TG concentration <strong>in</strong> serum and muscle<br />
LPL activity expressed per gram as an <strong>in</strong>dication of<br />
the importance of muscle LPL and as an <strong>in</strong>dication<br />
that this way of express<strong>in</strong>g the LPL activity is physiologically<br />
relevant.<br />
Hepatic lipase activity is known <strong>to</strong> be regulated by<br />
sex steroids. For example, dur<strong>in</strong>g treatment with estrogens,<br />
activity of this enzyme is decreased, but when<br />
estrogen is comb<strong>in</strong>ed with a gestagen with androgenic<br />
properties, hepatic lipase activity is upregulated, be<strong>in</strong>g<br />
reflected primarily <strong>in</strong> <strong>in</strong>creases and decreases, respectively,<br />
<strong>in</strong> HDL cholesterol concentrations. 41 " 43 However,<br />
an <strong>in</strong>verse relation between the degree of physical<br />
fitness (Vo 2max ) and hepatic lipase activity has<br />
been reported. 44 More physically fit men have lower<br />
<strong>in</strong>sul<strong>in</strong> concentrations than do less fit ones. 4546 These<br />
observations are compatible with the present f<strong>in</strong>d<strong>in</strong>g<br />
of a positive correlation between the area under the<br />
curve of <strong>in</strong>sul<strong>in</strong> concentrations and hepatic lipase<br />
activity. It is thus possible that <strong>in</strong>sul<strong>in</strong> (or <strong>in</strong>sul<strong>in</strong>related<br />
cellular functions) may also be <strong>in</strong>volved <strong>in</strong> the<br />
regulation of hepatic lipase activity. It may be suggested<br />
that the <strong>in</strong>creases <strong>in</strong> hepatic lipase activity may<br />
have been partly due <strong>to</strong> overexposure of the liver <strong>to</strong><br />
FFAs. This could <strong>in</strong>duce hepatic <strong>in</strong>sul<strong>in</strong> resistance,<br />
further dim<strong>in</strong>ish hepatic <strong>in</strong>sul<strong>in</strong> extraction, 3 - 31 - 32 and<br />
reduce the hepatic catabolism of sex steroids. 47<br />
In conclusion, this study has demonstrated that<br />
muscle LPL activity is correlated with the serum TG<br />
concentration <strong>in</strong> the fast<strong>in</strong>g state and <strong>in</strong>travenous fat<br />
<strong>to</strong>lerance, <strong>in</strong>dicat<strong>in</strong>g a role for impaired hydrolysis of<br />
circulat<strong>in</strong>g TGs <strong>in</strong> the hypertriglyceridemia of obesity<br />
and diabetes. Furthermore, muscle LPL activity was<br />
related <strong>to</strong> glucose <strong>in</strong>fusion rate, suggest<strong>in</strong>g that the<br />
hyper<strong>in</strong>sul<strong>in</strong>emia associated with <strong>in</strong>sul<strong>in</strong> resistance<br />
may have a downregulat<strong>in</strong>g effect on muscle LPL<br />
activity. The present results demonstrate that several<br />
risk fac<strong>to</strong>rs for coronary heart disease, such as serum<br />
TG and HDL cholesterol concentrations and blood<br />
pressure, are correlated with <strong>in</strong>sul<strong>in</strong> resistance, support<strong>in</strong>g<br />
the concept that <strong>in</strong>sul<strong>in</strong> resistance is an<br />
important underly<strong>in</strong>g pathogenic condition.<br />
References<br />
1. Reaven GM: Role of <strong>in</strong>sul<strong>in</strong> resistance <strong>in</strong> human disease.<br />
Diabetes 1988;3:1595-1607<br />
2. Modan M, Halk<strong>in</strong> H, Almog S, Lusky A, Eshkol A, Shefi M,<br />
Shitrit A, Fuchs Z: Hyper<strong>in</strong>sul<strong>in</strong>emia: A l<strong>in</strong>k between hypertension,<br />
obesity and glucose <strong>in</strong><strong>to</strong>lerance. / Cl<strong>in</strong> Invest 1985;75:<br />
809-817<br />
3. Reaven GM, Grenfield S: Diabetic hypertriglyceridaemia:<br />
Evidence for three cl<strong>in</strong>ical syndromes. Diabetes 1982;30(suppl<br />
2):66-75<br />
4. Task<strong>in</strong>en MR, Beltz WF, Harper I, Fields RM, Schonfeld G,<br />
Grundy SM, Howard BV: Effects of NIDDM on very-lowdensity<br />
lipoprote<strong>in</strong> triglyceride and lipoprote<strong>in</strong> B metabolism:<br />
Studies before and after sulfonylurea therapy. Diabetes 1986;<br />
35:1268-1277<br />
5. Rob<strong>in</strong>son DS: The function of the plasma triglycerides <strong>in</strong> fatty<br />
acid transport, <strong>in</strong> Flork<strong>in</strong> M, S<strong>to</strong>tz EH (eds): Comprehensive<br />
Biochemistry. Amsterdam, Elsevier Science Publish<strong>in</strong>g Co, Inc,<br />
1970, vol 18, pp 51-116<br />
6. Bol<strong>in</strong>der J, Lithell H, Skarfors E, Arner P: Effects of obesity,<br />
hyper<strong>in</strong>sul<strong>in</strong>emia, and glucose <strong>in</strong><strong>to</strong>lerance on <strong>in</strong>sul<strong>in</strong> action <strong>in</strong><br />
adipose tissue of sixty-year-old men. Diabetes 1986;35:282-290<br />
7. Lithell H, L<strong>in</strong>dgarde F, Hells<strong>in</strong>g K, Lundqvist G, Nygaard E,<br />
Vessby B, Salt<strong>in</strong> B: Body weight, skeletal muscle morphology,<br />
and enzyme activities <strong>in</strong> relation <strong>to</strong> fast<strong>in</strong>g serum <strong>in</strong>sul<strong>in</strong><br />
concentration and glucose <strong>to</strong>lerance <strong>in</strong> 48-year-old men. Diabetes<br />
1981;30:19-25<br />
8. Lithell H, Krotkiewski M, Kiens B, Wroblewski Z, Holm G,<br />
Strdmblad G, Grimby G, Bjorn<strong>to</strong>rp P: Non-response of muscle<br />
capillary density and lipoprote<strong>in</strong>-lipase activity <strong>to</strong> regular<br />
tra<strong>in</strong><strong>in</strong>g <strong>in</strong> diabetic patients. Diabetes Res 1985;2:17-21<br />
9. Grimby G, Wilhelmsen L, Bjorn<strong>to</strong>rp P, Salt<strong>in</strong> B, Tibbl<strong>in</strong> G:<br />
Habitual physical activity, aerobic power and blood lipids, <strong>in</strong><br />
Pernow B, Salt<strong>in</strong> B (eds): <strong>Muscle</strong> Metabolism Dur<strong>in</strong>g Exercise.<br />
New York, Plenum Publish<strong>in</strong>g Corp, 1971, pp 469-489<br />
10. Pollare T, Lithell H, Sel<strong>in</strong>us I, Berne C: Application of<br />
prazos<strong>in</strong> is associated with an <strong>in</strong>crease of <strong>in</strong>sul<strong>in</strong> sensitivity <strong>in</strong><br />
obese patients with hypertension. Diabe<strong>to</strong>logia 1988;31:<br />
415-420<br />
11. Ikkos D, Luft R: On the <strong>in</strong>travenous glucose <strong>to</strong>lerance test.<br />
Ada Endocr<strong>in</strong>ol (Copenh) 1957;25:312-334<br />
12. Jeppsson J-O, Jern<strong>to</strong>rp P, Sundkvist G, Englund H, Nylund V:<br />
Measurement of hemoglob<strong>in</strong> A]C by a new liquid-chroma<strong>to</strong>graphy<br />
assay: Methodology, cl<strong>in</strong>ical utility, and relation <strong>to</strong><br />
glucose <strong>to</strong>lerance evaluated. Cl<strong>in</strong> Chem 1986;32:1867-1872<br />
13. DeFronzo RA, Tob<strong>in</strong> JD, Andres R: Glucose clamp technique:<br />
A method for quantify<strong>in</strong>g <strong>in</strong>sul<strong>in</strong> secretion and resistance. Am<br />
JPhysiol 1979;237:E214-E223<br />
14. Altszuler N, Barkari A, Bjerknes C, Gottlieb B, Steele R:<br />
Glucose turnover values <strong>in</strong> the dog obta<strong>in</strong>ed with various<br />
species of labeled glucose. Am J Physiol 1975;229:1662-1667<br />
15. Siegler L, Wu TW: Separation of serum high-density lipoprote<strong>in</strong><br />
for cholesterol determ<strong>in</strong>ation: Ultracentrifugation vs precipitation<br />
with sodium phosphotungstate and magnesium chloride.<br />
Cl<strong>in</strong> Chem 1981;27:838-841<br />
16. Hirsch J, Goldrick RB: Serial studies on the metabolism of<br />
human adipose tissue: I. Lipogenesis and free fatty acid<br />
uptake and release <strong>in</strong> small aspirated samples of subcutaneous<br />
fat. / Cl<strong>in</strong> Invest 1964;43:1776-1792<br />
17. Bergstrom J: <strong>Muscle</strong> electrolytes <strong>in</strong> man. Scand J Cl<strong>in</strong> Lab<br />
Invest 1962;14(suppl):l-110<br />
18. Nilsson-Ehle P, Schotz MC: A stable radioactive substrate<br />
emulsion for assay of lipoprote<strong>in</strong> lipase. / Lipid Res 1976;17:<br />
536-541<br />
19. Lithell H, Boberg J: A method of determ<strong>in</strong><strong>in</strong>g lipoprote<strong>in</strong>lipase<br />
activity <strong>in</strong> human adipose tissue. Scand J Cl<strong>in</strong> Lab Invest<br />
1977;37:551-561<br />
20. Lithell H, Boberg J: Determ<strong>in</strong>ation of lipoprote<strong>in</strong>-lipase activity<br />
<strong>in</strong> human skeletal muscle tissue. Biochim Biophys Ada<br />
1978;528:58-68<br />
21. Arner P, Engfeldt P, Lithell H: Site differences <strong>in</strong> the basal<br />
metabolism of subcutaneous fat <strong>in</strong> obese women. / Cl<strong>in</strong><br />
Endocr<strong>in</strong>ol Metab 1981;53:948-952<br />
22. Boberg J, Carlson LA: Determ<strong>in</strong>ation of hepar<strong>in</strong>-<strong>in</strong>duced<br />
lipoprote<strong>in</strong> lipase activity <strong>in</strong> human plasma. Cl<strong>in</strong> Chim Ada<br />
1964;10:420-427<br />
23. Nilsson-Ehle P, Ekman R: Rapid, simple and specific assays<br />
for lipoprote<strong>in</strong> lipase and hepatic lipase. Artery 1977;3:<br />
194-209<br />
24. Nilsson-Ehle P, Garf<strong>in</strong>kel AS, Schotz MC: Lipolytic enzymes<br />
and plasma lipoprote<strong>in</strong> metabolism. Annu Rev Biochem 1980;<br />
49:667-693<br />
25. Carlson LA, Rossner S: A methodological study of an <strong>in</strong>travenous<br />
fat <strong>to</strong>lerance test with Intralipid emulsion. Scand J Cl<strong>in</strong><br />
Lab Invest 1972;29:271-280<br />
Downloaded from http://atvb.ahajournals.org/ by guest on August 29, 2013
Pollare et al LPL <strong>Activity</strong> and Insul<strong>in</strong> Sensitivity 1203<br />
26. Rossner S: Studies on an <strong>in</strong>travenous fat <strong>to</strong>lerance test:<br />
Methodological, experimental and cl<strong>in</strong>ical experiences with<br />
Intralipid®. Ada Med Scand 1974(suppl 564):l-24<br />
27. Steele R: Influences of glucose load<strong>in</strong>g and of <strong>in</strong>jected <strong>in</strong>sul<strong>in</strong><br />
on hepatic glucose output. Ann N YAcad Sci 1959;82:420-430<br />
28. Cowan JS, Hetenyi G: Glucoregula<strong>to</strong>ry responses <strong>in</strong> normal<br />
and diabetic dogs recorded by a new tracer method. Metabolism<br />
1971;20:360-372<br />
29. Davidson MB, Harris MD, Rosenberg CS: Inverse relationship<br />
of metabolic clearance rate of <strong>in</strong>sul<strong>in</strong> <strong>to</strong> body mass <strong>in</strong>dex.<br />
Metabolism 1987;36:219-222<br />
30. Ferrann<strong>in</strong>i E, Haffner SM, Stern MP: Essential hypertension:<br />
An <strong>in</strong>sul<strong>in</strong>-resistant state. / Cardiovasc Pharmacol 1990;<br />
15(suppl 5):S18-S25<br />
31. Stromblad G, Bjorn<strong>to</strong>rp P: Reduced hepatic <strong>in</strong>sul<strong>in</strong> clearance<br />
<strong>in</strong> rats with dietary-<strong>in</strong>duced obesity. Metabolism 1986;35:<br />
323-327<br />
32. Bevilacqua S, Bonadonna R, Buzzigioli G, Boni C, Ciociaro D,<br />
Maccari F, Giorico MA, Ferrann<strong>in</strong>i E: Acute elevation of free<br />
fatty acid levels leads <strong>to</strong> hepatic <strong>in</strong>sul<strong>in</strong> resistance <strong>in</strong> obese<br />
subjects. Metabolism 1987;36:502-506<br />
33. Ferrari P, Weidmann P: Insul<strong>in</strong>, <strong>in</strong>sul<strong>in</strong> sensitivity and hypertension.<br />
/ Hypertens 1990;8:491-500<br />
34. Skarfors ET, Lithell HO, Sel<strong>in</strong>us I: Risk fac<strong>to</strong>rs for development<br />
of hypertension: A ten-year longitud<strong>in</strong>al study <strong>in</strong> middleaged<br />
men. / Hypertens 1991;9:217-223<br />
35. Lithell H, Boberg J, Hells<strong>in</strong>g K, Lundqvist G, Vessby B:<br />
<strong>Lipoprote<strong>in</strong></strong>-lipase activity <strong>in</strong> human skeletal muscle and adipose<br />
tissue <strong>in</strong> the fast<strong>in</strong>g and the fed states. Atherosclerosis<br />
1978;30:89-94<br />
36. Lithell H, Jacobs I, Vessby B, Hells<strong>in</strong>g K, Karlsson J: Decrease<br />
of lipoprote<strong>in</strong> lipase activity <strong>in</strong> skeletal muscle <strong>in</strong> man dur<strong>in</strong>g<br />
a short term carbohydrate-rich dietary regime: With special<br />
reference <strong>to</strong> HDL-cholesterol, apolipoprote<strong>in</strong> and <strong>in</strong>sul<strong>in</strong><br />
concentrations. Metabolism 1982;31:994-998<br />
37. Lithell H, Karlstrom B, Sel<strong>in</strong>us I, Vessby B, Fellstrom B: <strong>Is</strong><br />
muscle lipoprote<strong>in</strong> lipase <strong>in</strong>activated by ord<strong>in</strong>ary amounts of<br />
dietary carbohydrates? Hum Nutr Cl<strong>in</strong> Nutr 1985;39C:289-295<br />
38. Task<strong>in</strong>en MR, Nikkila EA, Rheumen S, Gord<strong>in</strong> A: Effect of<br />
acute vigorous exercise on lipoprote<strong>in</strong> lipase activity of adipose<br />
tissue and skeletal muscle <strong>in</strong> physically active mm. Artery<br />
1980;6:471-483<br />
39. Kiens B, Lithell H, Mik<strong>in</strong>es KJ, Richter EA: Effects of <strong>in</strong>sul<strong>in</strong><br />
and exercise on muscle lipoprote<strong>in</strong> lipase activity <strong>in</strong> man and<br />
its relation <strong>to</strong> <strong>in</strong>sul<strong>in</strong> action. J Cl<strong>in</strong> Invest 1989;84:1124-1129<br />
40. Pykalis<strong>to</strong> OJ, Smith PH, Brunzell DJ: Determ<strong>in</strong>ants of human<br />
adipose tissue lipoprote<strong>in</strong> lipase: Effect of diabetes and obesity<br />
on basal- and diet-<strong>in</strong>duced activity. / Cl<strong>in</strong> Invest 1975;56:<br />
1108-1117<br />
41. Tikkanen MJ, Kuusi T, Vartianen E, Nikkila EA: Treatment<br />
of postmenopausal hypercholesterolaemia with estradiol.y4c/a<br />
Obstet Gynecol Scand Suppl 1979;88:83-88<br />
42. Tikkanen MJ, Nikkila EA, Kuusi T, Siponen S: High density<br />
lipoprote<strong>in</strong>-2 and hepatic lipase: Reciprocal changes produced<br />
by estrogen and norgestrel. J Cl<strong>in</strong> Endocr<strong>in</strong>ol Metab 1982;54:<br />
1113-1117<br />
43. Tikkanen MJ, Nikkila EA, Kuusi T, Siponen S: Effects of<br />
oestradiol and levonorgestrel on lipoprote<strong>in</strong> lipids and posthepar<strong>in</strong><br />
plasma lipase activities <strong>in</strong> normolipoprote<strong>in</strong>aemic women.<br />
Acta Endocr<strong>in</strong>ol 1982;99:630-635<br />
44. Stubbe I, Hansson P, Gustafson A, Nilsson-Ehle P: Plasma<br />
lipoprote<strong>in</strong>s and lipolytic enzyme activities dur<strong>in</strong>g endurance<br />
tra<strong>in</strong><strong>in</strong>g <strong>in</strong> sedentary men: Changes <strong>in</strong> high-density lipoprote<strong>in</strong><br />
subfractions and composition. Metabolism 1983;32:1120-1128<br />
45. Rosenthal M, Haskell WL, Solomon R, Widstrom A, Reaven<br />
GM: Demonstration of a relationship between level of physical<br />
tra<strong>in</strong><strong>in</strong>g and <strong>in</strong>sul<strong>in</strong>-stimulated glucose utilization <strong>in</strong> normal<br />
humans. Diabetes 1983;32:408-411<br />
46. Heath GW, Gav<strong>in</strong> JR, H<strong>in</strong>derliter JM, Hagberg JM, Bloomfield<br />
SA, Holloszy JO: Effects of exercise and lack of exercise<br />
on glucose <strong>to</strong>lerance and <strong>in</strong>sul<strong>in</strong> sensitivity. J Appl Physiol<br />
Environ Exerc Physiol 1983;55:512-517<br />
47. Haffner SM, Katz MS, Stern MP, Dunn JF: The relationship<br />
of sex hormones <strong>to</strong> hyper<strong>in</strong>sul<strong>in</strong>emia and hyperglycemia.<br />
Metabolism 1988;37:683-688<br />
KEY WORDS • lipoprote<strong>in</strong> lipase activity • <strong>in</strong>sul<strong>in</strong> sensitivity •<br />
<strong>in</strong>sul<strong>in</strong> • lipids • obesity • diabetes<br />
Downloaded from http://atvb.ahajournals.org/ by guest on August 29, 2013