Building for a brighter future - GHA Central
Building for a brighter future - GHA Central Building for a brighter future - GHA Central
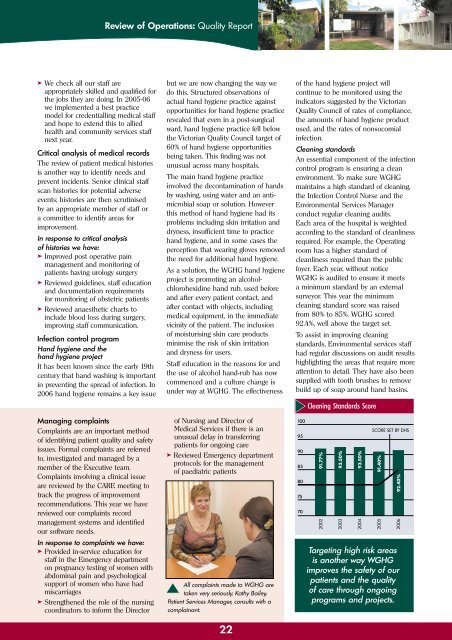
Review of Operations: Quality Report ➤ We check all our staff are appropriately skilled and qualified for the jobs they are doing. In 2005-06 we implemented a best practice model for credentialling medical staff and hope to extend this to allied health and community services staff next year. Critical analysis of medical records The review of patient medical histories is another way to identify needs and prevent incidents. Senior clinical staff scan histories for potential adverse events; histories are then scrutinised by an appropriate member of staff or a committee to identify areas for improvement. In response to critical analysis of histories we have: ➤ Improved post operative pain management and monitoring of patients having urology surgery ➤ Reviewed guidelines, staff education and documentation requirements for monitoring of obstetric patients ➤ Reviewed anaesthetic charts to include blood loss during surgery, improving staff communication. Infection control program Hand hygiene and the hand hygiene project It has been known since the early 19th century that hand washing is important in preventing the spread of infection. In 2006 hand hygiene remains a key issue Managing complaints Complaints are an important method of identifying patient quality and safety issues. Formal complaints are referred to, investigated and managed by a member of the Executive team. Complaints involving a clinical issue are reviewed by the CARE meeting to track the progress of improvement recommendations. This year we have reviewed our complaints record management systems and identified our software needs. In response to complaints we have: ➤ Provided in-service education for staff in the Emergency department on pregnancy testing of women with abdominal pain and psychological support of women who have had miscarriages ➤ Strengthened the role of the nursing coordinators to inform the Director but we are now changing the way we do this. Structured observations of actual hand hygiene practice against opportunities for hand hygiene practice revealed that even in a post-surgical ward, hand hygiene practice fell below the Victorian Quality Council target of 60% of hand hygiene opportunities being taken. This finding was not unusual across many hospitals. The main hand hygiene practice involved the decontamination of hands by washing, using water and an antimicrobial soap or solution. However this method of hand hygiene had its problems including skin irritation and dryness, insufficient time to practice hand hygiene, and in some cases the perception that wearing gloves removed the need for additional hand hygiene. As a solution, the WGHG hand hygiene project is promoting an alcoholchlorohexidine hand rub, used before and after every patient contact, and after contact with objects, including medical equipment, in the immediate vicinity of the patient. The inclusion of moisturising skin care products minimise the risk of skin irritation and dryness for users. Staff education in the reasons for and the use of alcohol hand-rub has now commenced and a culture change is under way at WGHG. The effectiveness of Nursing and Director of Medical Services if there is an unusual delay in transferring patients for ongoing care ➤ Reviewed Emergency department protocols for the management of paediatric patients All complaints made to WGHG are taken very seriously. Kathy Bailey, Patient Services Manager, consults with a complainant. 22 of the hand hygiene project will continue to be monitored using the indicators suggested by the Victorian Quality Council of rates of compliance, the amounts of hand hygiene product used, and the rates of nonsocomial infection. Cleaning standards An essential component of the infection control program is ensuring a clean environment. To make sure WGHG maintains a high standard of cleaning, the Infection Control Nurse and the Environmental Services Manager conduct regular cleaning audits. Each area of the hospital is weighted according to the standard of cleanliness required. For example, the Operating room has a higher standard of cleanliness required than the public foyer. Each year, without notice WGHG is audited to ensure it meets a minimum standard by an external surveyor. This year the minimum cleaning standard score was raised from80% to 85%. WGHG scored 92.4%, well above the target set. To assist in improving cleaning standards, Environmental services staff had regular discussions on audit results highlighting the areas that require more attention to detail. They have also been supplied with tooth brushes to remove build up of soap around hand basins. 100 95 90 85 80 75 70 Cleaning Standards Score 91.77% 2002 93.50% 2003 93.50% 2004 SCORE SET BY DHS 91.40% 2005 92.40% 2006 Targeting high risk areas is another way WGHG improves the safety of our patients and the quality of care through ongoing programs and projects.
Review of Operations: Quality Report In response to learning from others in healthcare across Australia, WGHG has: ➤ Reviewed blood transfusion practices in line with best practice models ➤ Introduced best practice use of pain relievers in the Emergency department ➤ Implemented the Surgical Consultative Council five step patient identification processes to help ensure we have the correct patient for the correct procedure A heightened awareness of procedures and encouragement to report, has resulted in staff reporting more errors in medication documents. This positive increase indicates errors are being picked up before the medications are given, preventing potential harm. Medication management In 2004-05, after a review of the most common forms of medication error, we concentrated on how medications could be unintentionally omitted. Improvement strategies implemented dramatically improved the number of errors relating to the omission of medications by 66%. In 2005-06 the focus was on errors relating to documentation. Medication incidents are regularly discussed at Nursing Council meetings and in the Medication Safety Working Party so that improvement strategies can be targeted in the most effective manner. This year: ➤ Clinical Nurse Managers changed handover processes to include checking of medications at the bedside for all Ward areas ➤ The medication management procedure was reviewed ➤ All nursing staff received in-service training on medication management procedures and general incident reporting ➤ In a “no-blame” culture, staff were actively encouraged to report all documentation errors detected. The data for 2005-06 now shows a 129% increase in the number of incidents reported (31 to 71). Of the 71 reported incidents in this category, only one had a minor outcome requiring medical review for the patient. Another project aimed at reducing medication errors by targeting the way medications are documented, commenced in 2004-05 when WGHG trialled a standardised national medication chart and provided feedback to the National Quality And Safety Council, National Medication Chart pilot project. This year the National Medication Chart was fully implemented at WGHG. Pharmacist Kenneth Ch’ng ensures the medications prescribed on the medication chart are the correct medication prior to discharge of patient Arthur Row. Falls Falls remain one of the top two incidents reported at WGHG. Falls projects, commenced last year, continue with best practice falls risk assessments and minimisation strategies being implemented in all clinical areas and extending into the community. As part of this, a new Admission and Discharge form that includes an initial falls screening tool was trialled and implemented. If the initial screen confirms a risk of falling a second more extensive tool is completed and falls reduction strategies implemented in the care planning. Analysis of the data shows we are making a difference. This year there has been a 17% decrease in the number of falls occurring in hospital resulting in minor injuries in the acute Types of Medication Errors Reported 80 70 60 50 40 30 20 10 0 2003/04 2004/05 2005/06 Omitted dose Documentation related Wrong dose Not detailed Wrong drug Duplicated dose Wrong rate IV therapy and Site issues Delayed dose Wrong patient Known allergy Wrong route Self administering Adverse drug reaction Drug intervention Incompatible blood product Overall the number of errors reported for 2005-2006, in nearly all categories, has increased. Staff have been provided with a series of incident reporting sessions to encourage reporting. This has improved the climate of reporting and has given us more opportunities to learn. 23
- Page 1 and 2: Building for a brighter future West
- Page 3 and 4: Overview: Year in Brief Significant
- Page 5 and 6: Overview: At a glance INFORMATION M
- Page 7 and 8: Overview: Year in Review Human Reso
- Page 9 and 10: Overview: Our Profile What we do Ho
- Page 11 and 12: Overview: Overall Performance Expen
- Page 13 and 14: Overview: Overall Performance Debto
- Page 15 and 16: Corporate Governance: Board of Dire
- Page 17 and 18: Corporate Governance: Organisation
- Page 19 and 20: Our People: Occupational Health and
- Page 21 and 22: Review of Operations: Environment a
- Page 23: Review of Operations: Quality Repor
- Page 27 and 28: Review of Operations: Quality Repor
- Page 29 and 30: Review of Operations: Acute (Hospit
- Page 31 and 32: Review of Operations: Acute (Hospit
- Page 33 and 34: Review of Operations: Aged Care Ser
- Page 35 and 36: Review of Operations: Community Ser
- Page 37 and 38: Review of Operations: Allied Health
- Page 39 and 40: Our Community: Volunteers We enjoy
- Page 41 and 42: Our Community: Donations and Sponso
- Page 43 and 44: Staff List: Our Staff Allied Health
- Page 45 and 46: Financial: Financial Results OPERAT
- Page 47 and 48: Financial: Financial Results STATEM
- Page 49 and 50: Financial: Financial Results Notes
- Page 51 and 52: Financial: Financial Results Notes
- Page 53 and 54: Financial: Financial Results Notes
- Page 55 and 56: Financial: Financial Results Notes
- Page 58 and 59: Financial: Financial Results Notes
- Page 60 and 61: Financial: Financial Results Notes
- Page 62 and 63: Financial: Financial Results Notes
- Page 64 and 65: Financial: Financial Results Notes
- Page 66 and 67: Financial: Financial Results Notes
- Page 68 and 69: Financial: Financial Results Notes
- Page 70 and 71: Financial: Financial Results Notes
- Page 72 and 73: Financial: Auditor General’s Repo
Review of Operations: Quality Report<br />
➤ We check all our staff are<br />
appropriately skilled and qualified <strong>for</strong><br />
the jobs they are doing. In 2005-06<br />
we implemented a best practice<br />
model <strong>for</strong> credentialling medical staff<br />
and hope to extend this to allied<br />
health and community services staff<br />
next year.<br />
Critical analysis of medical records<br />
The review of patient medical histories<br />
is another way to identify needs and<br />
prevent incidents. Senior clinical staff<br />
scan histories <strong>for</strong> potential adverse<br />
events; histories are then scrutinised<br />
by an appropriate member of staff or<br />
a committee to identify areas <strong>for</strong><br />
improvement.<br />
In response to critical analysis<br />
of histories we have:<br />
➤ Improved post operative pain<br />
management and monitoring of<br />
patients having urology surgery<br />
➤ Reviewed guidelines, staff education<br />
and documentation requirements<br />
<strong>for</strong> monitoring of obstetric patients<br />
➤ Reviewed anaesthetic charts to<br />
include blood loss during surgery,<br />
improving staff communication.<br />
Infection control program<br />
Hand hygiene and the<br />
hand hygiene project<br />
It has been known since the early 19th<br />
century that hand washing is important<br />
in preventing the spread of infection. In<br />
2006 hand hygiene remains a key issue<br />
Managing complaints<br />
Complaints are an important method<br />
of identifying patient quality and safety<br />
issues. Formal complaints are referred<br />
to, investigated and managed by a<br />
member of the Executive team.<br />
Complaints involving a clinical issue<br />
are reviewed by the CARE meeting to<br />
track the progress of improvement<br />
recommendations. This year we have<br />
reviewed our complaints record<br />
management systems and identified<br />
our software needs.<br />
In response to complaints we have:<br />
➤ Provided in-service education <strong>for</strong><br />
staff in the Emergency department<br />
on pregnancy testing of women with<br />
abdominal pain and psychological<br />
support of women who have had<br />
miscarriages<br />
➤ Strengthened the role of the nursing<br />
coordinators to in<strong>for</strong>m the Director<br />
but we are now changing the way we<br />
do this. Structured observations of<br />
actual hand hygiene practice against<br />
opportunities <strong>for</strong> hand hygiene practice<br />
revealed that even in a post-surgical<br />
ward, hand hygiene practice fell below<br />
the Victorian Quality Council target of<br />
60% of hand hygiene opportunities<br />
being taken. This finding was not<br />
unusual across many hospitals.<br />
The main hand hygiene practice<br />
involved the decontamination of hands<br />
by washing, using water and an antimicrobial<br />
soap or solution. However<br />
this method of hand hygiene had its<br />
problems including skin irritation and<br />
dryness, insufficient time to practice<br />
hand hygiene, and in some cases the<br />
perception that wearing gloves removed<br />
the need <strong>for</strong> additional hand hygiene.<br />
As a solution, the WGHG hand hygiene<br />
project is promoting an alcoholchlorohexidine<br />
hand rub, used be<strong>for</strong>e<br />
and after every patient contact, and<br />
after contact with objects, including<br />
medical equipment, in the immediate<br />
vicinity of the patient. The inclusion<br />
of moisturising skin care products<br />
minimise the risk of skin irritation<br />
and dryness <strong>for</strong> users.<br />
Staff education in the reasons <strong>for</strong> and<br />
the use of alcohol hand-rub has now<br />
commenced and a culture change is<br />
under way at WGHG. The effectiveness<br />
of Nursing and Director of<br />
Medical Services if there is an<br />
unusual delay in transferring<br />
patients <strong>for</strong> ongoing care<br />
➤ Reviewed Emergency department<br />
protocols <strong>for</strong> the management<br />
of paediatric patients<br />
All complaints made to WGHG are<br />
taken very seriously. Kathy Bailey,<br />
Patient Services Manager, consults with a<br />
complainant.<br />
22<br />
of the hand hygiene project will<br />
continue to be monitored using the<br />
indicators suggested by the Victorian<br />
Quality Council of rates of compliance,<br />
the amounts of hand hygiene product<br />
used, and the rates of nonsocomial<br />
infection.<br />
Cleaning standards<br />
An essential component of the infection<br />
control program is ensuring a clean<br />
environment. To make sure WGHG<br />
maintains a high standard of cleaning,<br />
the Infection Control Nurse and the<br />
Environmental Services Manager<br />
conduct regular cleaning audits.<br />
Each area of the hospital is weighted<br />
according to the standard of cleanliness<br />
required. For example, the Operating<br />
room has a higher standard of<br />
cleanliness required than the public<br />
foyer. Each year, without notice<br />
WGHG is audited to ensure it meets<br />
a minimum standard by an external<br />
surveyor. This year the minimum<br />
cleaning standard score was raised<br />
from80% to 85%. WGHG scored<br />
92.4%, well above the target set.<br />
To assist in improving cleaning<br />
standards, Environmental services staff<br />
had regular discussions on audit results<br />
highlighting the areas that require more<br />
attention to detail. They have also been<br />
supplied with tooth brushes to remove<br />
build up of soap around hand basins.<br />
100<br />
95<br />
90<br />
85<br />
80<br />
75<br />
70<br />
Cleaning Standards Score<br />
91.77%<br />
2002<br />
93.50%<br />
2003<br />
93.50%<br />
2004<br />
SCORE SET BY DHS<br />
91.40%<br />
2005<br />
92.40%<br />
2006<br />
Targeting high risk areas<br />
is another way WGHG<br />
improves the safety of our<br />
patients and the quality<br />
of care through ongoing<br />
programs and projects.


