

2008 Barcelona - European Society of Human Genetics
2008 Barcelona - European Society of Human Genetics
2008 Barcelona - European Society of Human Genetics

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Cytogenetics<br />
P02.215<br />
cytogenetic analysis <strong>of</strong> turner syndrome<br />
L. Letica, R. Lasan, I. Tonković Đurišević, K. Crkvenac Gornik, M. Burek, D.<br />
Begović;<br />
Division <strong>of</strong> <strong>Genetics</strong> and Metabolism, Department <strong>of</strong> Pediatrics, University<br />
Hospital Centre, Zagreb, Croatia.<br />
Turner syndrome is caused by the absence <strong>of</strong> all or part <strong>of</strong> the second<br />
sex chromosome . In our study on 100 female patients clinically diagnosed<br />
with Turner syndrome:<br />
46 patients were 45,X<br />
10 patients were mos 45,X/46, XX<br />
2 patients were mos 45,X/47, XXX/46,XX<br />
8 patients were mos 45,X/47, XXX<br />
31 patients had a structurally abnormal X chromosome (mainly isochromosome,<br />
deletion p or q arm, ring X chromosome) and 2 patients<br />
had a structurally changed Y chromosome<br />
The phenotype is variable and includes short stature and gonadal dysgenesis<br />
. Mental retardation is not a feature <strong>of</strong> Turner syndrome .<br />
Conventional cytogenetical G-banding method and Fluorescence in<br />
situ hybridization technique were considered in cultured peripheral<br />
blood .<br />
Postnatal recognation <strong>of</strong> the syndrome requires genetic counselling <strong>of</strong><br />
parents and supportive multidisciplinary treatment .<br />
P02.216<br />
the importance <strong>of</strong> women karyotyping in assisted reproduction<br />
G. Ozgon 1 , O. Oner 1 , C. Aslan 1 , B. Onal 1 , F. Fiorentino 1 , G. Karlikaya 2 , H. Karagozoglu<br />
2 , S. Kahraman 2 ;<br />
1 Genoma Turkey, istanbul, Turkey, 2 Memorial hospital, istanbul, Turkey.<br />
INTRODUCTION: Recent researches show that the infertility is related<br />
to both male and female genetics . Patients, who applied to our center,<br />
evaluated according to their indication and karyotypoes .<br />
Karyotpye analysis was applied for the patients with the indication<br />
such as; recurrent implantation failure (RIF), recurrent pregnancy lost<br />
(RPL), male factor and abnormal fetus history, female factors (primary<br />
amenore) .<br />
In this study, we aimed to demonstrate karytopes evaluation <strong>of</strong> the<br />
women who were referred to our cytogenetics laboratory .<br />
MATERIAL- METHOD: Chromosome preparations were made from<br />
72-h PHA-stimulated cell cultures from peripheral blood . Cell division<br />
was synchronized by a pulse <strong>of</strong> thymidine administered 21 h prior to<br />
harvesting . The thymidine block was released by washing the cells in<br />
fresh culture medium (RPMI 1640),also prewarmed to 37°C, for 3,5 h<br />
prior to harvesting . The culture was harvested using colcemid for 50<br />
min prior to harvesting . At least 20 GTG-banded (Giemsa stain) metaphase<br />
cells were analyzed for each patient .<br />
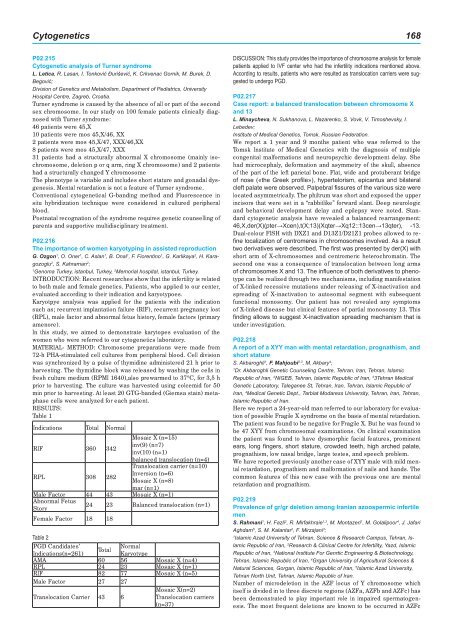
RESULTS:<br />
Table 1<br />
Indications Total Normal<br />
RIF 360 342<br />
Mosaic X (n=15)<br />
inv(9) (n=7)<br />
inv(10) (n=1)<br />
balanced translocation (n=4)<br />
RPL 308 282<br />
Translocation carrier (n=10)<br />
Inversion (n=6)<br />
Mosaic X (n=8)<br />
mar (n=1)<br />
Male Factor 44 43 Mosaic X (n=1)<br />
Abnormal Fetus<br />
Story<br />
24 23 Balanced translocation (n=1)<br />
Female Factor 18 18<br />
Table 2<br />
PGD Candidates’<br />
Indications(n=261)<br />
Total<br />
Normal<br />
Karyotype<br />
AMA 60 56 Mosaic X (n=4)<br />
RPL 24 23 Mosaic X (n=1)<br />
RIF 82 77 Mosaic X (n=5)<br />
Male Factor 27 27<br />
Translocation Carrier 43 6<br />
Mosaic X(n=2)<br />
Translocation carriers<br />
(n=37)<br />
DISCUSSION: This study provides the importance <strong>of</strong> chromosome analysis for female<br />
patients applied to IVF center who had the infertility indications mentioned above.<br />
According to results, patients who were resulted as translocation carriers were suggested<br />
to undergo PGD.<br />
P02.217<br />
case report: a balanced translocation between chromosome X<br />
and 13<br />
L. Minaycheva, N. Sukhanova, L. Nazarenko, S. Vovk, V. Timoshevsky, I.<br />
Lebedev;<br />
Institute <strong>of</strong> Medical <strong>Genetics</strong>, Tomsk, Russian Federation.<br />
We report a 1 year and 9 months patient who was referred to the<br />
Tomsk Institute <strong>of</strong> Medical <strong>Genetics</strong> with the diagnosis <strong>of</strong> multiple<br />
congenital malformations and neuropsychic development delay . She<br />
had microcephaly, deformation and asymmetry <strong>of</strong> the skull, absence<br />
<strong>of</strong> the part <strong>of</strong> the left parietal bone . Flat, wide and protuberant bridge<br />
<strong>of</strong> nose («the Greek pr<strong>of</strong>ile»), hypertelorism, epicantus and bilateral<br />
cleft palate were observed. Palpebral fissures <strong>of</strong> the various size were<br />
located asymmetrically . The philtrum was short and exposed the upper<br />
incisors that were set in a “rabbitlike” forward slant . Deep neurologic<br />
and behavioral development delay and epilepsy were noted . Standard<br />
cytogenetic analysis have revealed a balanced rearrangement:<br />
46,X,der(X)(pter→Xcen),t(X;13)(Xqter→Xq12::13cen→13qter), -13.<br />
Dual-colour FISH with DXZ1 and D13Z1/D21Z1 probes allowed to refine<br />
localization <strong>of</strong> centromeres in chromosomes involved. As a result<br />
two derivatives were described. The first was presented by der(X) with<br />
short arm <strong>of</strong> X-chromosomes and centromeric heterochromatin . The<br />
second one was a consequence <strong>of</strong> translocation between long arms<br />
<strong>of</strong> chromosomes X and 13. The influence <strong>of</strong> both derivatives to phenotype<br />
can be realized through two mechanisms, including manifestation<br />
<strong>of</strong> X-linked recessive mutations under releasing <strong>of</strong> X-inactivation and<br />
spreading <strong>of</strong> X-inactivation to autosomal segment with subsequent<br />
functional monosomy . Our patient has not revealed any symptoms<br />
<strong>of</strong> X-linked disease but clinical features <strong>of</strong> partial monosomy 13 . This<br />
finding allows to suggest X-inactivation spreading mechanism that is<br />
under investigation .<br />
P02.218<br />
A report <strong>of</strong> a XYY man with mental retardation, prognathism, and<br />
short stature<br />
S. Akbaroghli 1 , F. Mahjoubi 2,3 , M. Akbary 4 ;<br />
1 Dr. Akbaroghli Genetic Counseling Centre, Tehran, Iran, Tehran, Islamic<br />
Republic <strong>of</strong> Iran, 2 NIGEB, Tehran, Islamic Republic <strong>of</strong> Iran, 3 3Tehran Medical<br />
Genetic Laboratory, Taleganee St, Tehran, Iran, Tehran, Islamic Republic <strong>of</strong><br />
Iran, 4 Medical Genetic Dept., Tarbiat Modaress University, Tehran, Iran, Tehran,<br />
Islamic Republic <strong>of</strong> Iran.<br />
Here we report a 24-year-old man referred to our laboratory for evaluation<br />
<strong>of</strong> possible Fragile X syndrome on the basis <strong>of</strong> mental retardation .<br />
The patient was found to be negative for Fragile X . But he was found to<br />
be 47 XYY from chromosomal examinations . On clinical examination<br />
the patient was found to have dysmorphic facial features, prominent<br />
ears, long fingers, short stature, crowded teeth, high arched palate,<br />
prognathism, low nasal bridge, large testes, and speech problem .<br />
We have reported previously another case <strong>of</strong> XYY male with mild mental<br />
retardation, prognathism and malformation <strong>of</strong> nails and hands . The<br />
common features <strong>of</strong> this new case with the previous one are mental<br />
retardation and prognathism .<br />
P02.219<br />
Prevalence <strong>of</strong> gr/gr deletion among Iranian azoospermic infertile<br />
men<br />
S. Rahmani 1 , H. Fazli 2 , R. Mirfakhraie 1,3 , M. Montazeri 1 , M. Golalipoor 4 , J. Jafari<br />
Aghdam 5 , S. M. Kalantar 2 , F. Mirzajani 3 ;<br />
1 Islamic Azad University <strong>of</strong> Tehran, Science & Research Campus, Tehran, Islamic<br />
Republic <strong>of</strong> Iran, 2 Research & Clinical Centre for Infertility, Yazd, Islamic<br />
Republic <strong>of</strong> Iran, 3 National Institute For Genrtic Engineering & Biotechnology,<br />
Tehran, Islamic Republic <strong>of</strong> Iran, 4 Grgan University <strong>of</strong> Agricultural Sciences &<br />
Natural Sciences, Gorgan, Islamic Republic <strong>of</strong> Iran, 5 Islamic Azad University,<br />
Tehran North Unit, Tehran, Islamic Republic <strong>of</strong> Iran.<br />
Number <strong>of</strong> microdeletion in the AZF locus <strong>of</strong> Y chromosome which<br />
itself is divided in to three discrete regions (AZFa, AZFb and AZFc) has<br />
been demonstrated to play important role in impaired spermatogenesis<br />
. The most frequent deletions are known to be occurred in AZFc













