Hereditary Pelger-Huet Change
Hereditary Pelger-Huet Change
Hereditary Pelger-Huet Change

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Blood Cell Identification – Graded<br />
Case History<br />
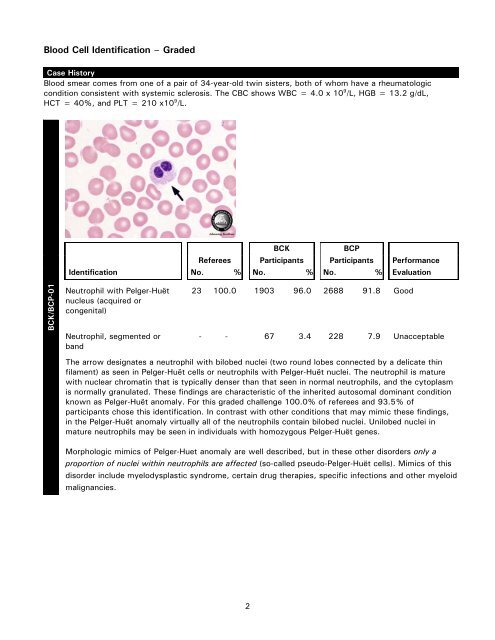
Blood smear comes from one of a pair of 34-year-old twin sisters, both of whom have a rheumatologic<br />
condition consistent with systemic sclerosis. The CBC shows WBC = 4.0 x 10 9 /L, HGB = 13.2 g/dL,<br />
HCT = 40%, and PLT = 210 x10 9 /L.<br />
BCK/BCP-01<br />
BCK BCP<br />
Referees Participants Participants Performance<br />
Identification No. % No. % No. % Evaluation<br />
Neutrophil with <strong>Pelger</strong>-Huët<br />
nucleus (acquired or<br />
congenital)<br />
Neutrophil, segmented or<br />
band<br />
23 100.0 1903 96.0 2688 91.8 Good<br />
- - 67 3.4 228 7.9 Unacceptable<br />
The arrow designates a neutrophil with bilobed nuclei (two round lobes connected by a delicate thin<br />
filament) as seen in <strong>Pelger</strong>-Huët cells or neutrophils with <strong>Pelger</strong>-Huët nuclei. The neutrophil is mature<br />
with nuclear chromatin that is typically denser than that seen in normal neutrophils, and the cytoplasm<br />
is normally granulated. These findings are characteristic of the inherited autosomal dominant condition<br />
known as <strong>Pelger</strong>-Huët anomaly. For this graded challenge 100.0% of referees and 93.5% of<br />
participants chose this identification. In contrast with other conditions that may mimic these findings,<br />
in the <strong>Pelger</strong>-Huët anomaly virtually all of the neutrophils contain bilobed nuclei. Unilobed nuclei in<br />
mature neutrophils may be seen in individuals with homozygous <strong>Pelger</strong>-Huët genes.<br />
Morphologic mimics of <strong>Pelger</strong>-<strong>Huet</strong> anomaly are well described, but in these other disorders only a<br />
proportion of nuclei within neutrophils are affected (so-called pseudo-<strong>Pelger</strong>-Huët cells). Mimics of this<br />
disorder include myelodysplastic syndrome, certain drug therapies, specific infections and other myeloid<br />
malignancies.<br />
2
Blood Cell Identification – Graded<br />
BCK/BCP-02<br />
BCK BCP<br />
Referees Participants Participants Performance<br />
Identification No. % No. % No. % Evaluation<br />
Eosinophil, any stage 23 95.0 1185 59.9 2879 99.0 Good<br />
Neutrophil, segmented or<br />
band<br />
Neutrophil with <strong>Pelger</strong>-Huët<br />
nucleus (acquired or<br />
congenital)<br />
1 5.0 398 20.1 10 0.3 Unacceptable*<br />
- - 287 14.5 9 0.3 Unacceptable<br />
The arrow designates an eosinophil that lies adjacent to a neutrophil with <strong>Pelger</strong>-<strong>Huet</strong> nucleus. The<br />
eosinophil was correctly identified by 95.0% of referees and 83.2% of BCK and BCP total participants.<br />
While both cells are of a similar size, the smaller pale salmon-colored specific granules of the neutrophil<br />
contrast with the distinctive uniform coarse orange-red granules of the eosinophil.<br />
In analyzing participant results, the Scientific Committee noted that BCK participants had a poorer<br />
performance (59.9%) compared to BCP participants (99.0%) in identifying the arrowed cell as an<br />
eosinophil. On review, slight color differences were noted between the Photomicrograph versus the<br />
Photopage for this graded challenge. *Hence, the Scientific Committee has decided that both<br />
“Neutrophil, segmented or band” and “Neutrophil with <strong>Pelger</strong>-<strong>Huet</strong> nucleus” are acceptable answers for<br />
BCK participants only (code 30 = Scientific Committee Decision). Participants using photomicrographs<br />
are reminded to view images using a slide projector in a darkened room or an illuminated, magnifying<br />
hand-held viewer.<br />
The majority of participants now subscribe to the CAP’s color photograph products for Blood Cell<br />
Identification. With the increasing use of digital imagery and the advancements of color enhancing<br />
technology, it is recommended that you consider enrolling in these products. The CAP’s color<br />
photograph products offer you larger images for more accurate resulting as well as a supplementary<br />
CD-ROM, giving you the ability to digitally project and view the images in greater detail. Please refer to<br />
the 2008 Surveys catalog for more information.<br />
3
Blood Cell Identification – Graded<br />
BCK/BCP-03<br />
4<br />
BCK BCP<br />
Referees Participants Participants Performance<br />
Identification No. % No. % No. % Evaluation<br />
Basophil, any stage 23 100.0 1972 99.5 2895 99.6 Good<br />
The arrow designates a basophil as correctly identified by 100.0% of referees and 99.6% of<br />
participants. All basophils are characterized by a moderate number of densely stained coarse granules<br />
of varying sizes and shapes. These granules appear larger than neutrophilic granules and often obscure<br />
the nucleus. An uneven distribution of granules or partial degranulation may be observed (not seen in<br />
this particular basophil). Depending on the Wright stain preparation, the granules may appear purple,<br />
red or a deep blue-black.
Blood Cell Identification – Graded<br />
BCK/BCP-04<br />
5<br />
BCK BCP<br />
Referees Participants Participants Performance<br />
Identification No. % No. % No. % Evaluation<br />
Lymphocyte 23 95.0 1790 90.3 2696 92.8 Good<br />
Plasma cell, morphologically<br />
mature<br />
Lymphocyte, reactive (to<br />
include plasmacytoid and<br />
immunoblastic forms)<br />
nRBC, normal or abnormal<br />
morphology (blood only)<br />
1 5.0 2 0.1 5 0.2 Unacceptable<br />
- - 100 5.0 85 2.9 Unacceptable<br />
- - 78 3.9 104 3.6 Unacceptable<br />
The arrow designates a lymphocyte as correctly identified by 95.0% of referees and 91.8% of<br />
participants. The lymphocyte is small in size with a scant amount of pale basophilic cytoplasm lacking<br />
granules. The nuclear:cytoplasmic ratio is high, and the cell is largely occupied by the oval nucleus<br />
containing diffusely dense chromatin.
Blood Cell Identification – Graded<br />
BCK/BCP-05<br />
6<br />
BCK BCP<br />
Referees Participants Participants Performance<br />
Identification No. % No. % No. % Evaluation<br />
Ovalocyte 23 100.0 1968 99.2 2882 99.2 Good<br />
The two arrows in this low-power view designate ovalocytes, as was correctly identified by 100.0% of<br />
referees and 99.2% of participants. Ovalocytes or elliptocytes are erythrocytes with blunt ends and<br />
parallel sides. The blood smears of normal individuals frequently contain small numbers of<br />
ovalocytes/elliptocytes. <strong>Hereditary</strong> ovalocytosis/elliptocytosis, however, will show a marked<br />
ovalocytosis in which more than 25% of erythrocytes are affected.
Discussion<br />
Originally described in 1928 by <strong>Pelger</strong> and first recognized as an autosomal dominant trait in 1931 by Huët,<br />
the <strong>Pelger</strong>-Huët anomaly is characterized by abnormal neutrophil nuclear segmentation and extremely<br />
coarse nuclear chromatin. In heterozygotes, this manifests as bilobed round nuclei connected by a thin<br />
filament as shown in the case above, whereas unilobed neutrophil nuclei are predominantly seen in<br />
homozygotes. Well known to hematopathologists and hematologists, this anomaly is generally easily<br />
recognized as virtually all neutrophils show these changes. Neutrophil function is normal in individuals with<br />
congenital <strong>Pelger</strong>-Huët anomaly. Recently, lamin B receptor mutations have been described in congenital<br />
<strong>Pelger</strong>-Huët anomaly.<br />
Acquired <strong>Pelger</strong>-Huët anomaly shares morphologic features resembling congenital <strong>Pelger</strong>-Huët anomaly, but<br />
only a proportion of neutrophils are affected. Additional clinical history and the extent of these morphologic<br />
features help clarify the etiology of these changes. Mimics of the <strong>Pelger</strong>-Huët anomaly are most frequently<br />
found in myeloid malignancies (e.g. myelodysplastic syndrome and acute myeloid leukemia), but have also<br />
been described in association with certain drugs, infections, and malignancies, among others. Neutrophil<br />
function may be abnormal in some patients with myeloid malignancies.<br />
Dysplastic changes in the peripheral blood of patients with myelodysplastic syndrome may be seen in white<br />
blood cells, platelets and/or erythrocytes. Morphologic findings in white cells include abnormal cytoplasmic<br />
granules, hypercondensed nuclear chromatin, and abnormal nuclear segmentation. Abnormal granulation<br />
includes hypogranular neutrophils, neutrophils with so-called toxic granulations and Dohle bodies or<br />
abnormally large granules. <strong>Change</strong>s in nuclear chromatin may show a typical hypercondensed pattern,<br />
visible in myeloid series cells, as well as lymphocytes. Abnormal nuclear segmentation, including<br />
hyposegmented and hypersegmented forms are also well described.<br />
Acquired <strong>Pelger</strong>-Huët anomaly has been described in association with certain antibiotics, chemotherapeutic<br />
agents, and immunosuppressive medications. The latter medications are used in transplant recipients and<br />
include mycophenolate mofetil (MMF), tacrolimus, and ganciclovir. The neutrophil abnormalities are<br />
reversible following discontinuation or reduction of medications.<br />
References:<br />
1. Constantino BT. <strong>Pelger</strong>-Huët anomaly—morphology, mechanism, and significance in the peripheral blood<br />
film. Lab Med 2005;36:103-107.<br />
2. Etzell JE, Wang E. Acquired <strong>Pelger</strong>-Huët anomaly in association with concomitant tacrolimus and<br />
mycophenolate mofetil in a liver transplant patient. Arch Pathol Lab Med 2006;130:93-96.<br />
3. Hoffman K, Dreger CK, Olins AL, et al. Mutations in the gene encoding the lamin B receptor produce an<br />
altered nuclear morphology in granulocytes (<strong>Pelger</strong>-Huët anomaly). Nat Genet 2002;31:410-414.<br />
4. Skendzel LP, Hoffman GC. The <strong>Pelger</strong> anomaly of leukocytes: forty-one cases in seven families. Am J<br />
Clin Pathol 1962; 37:294-301.<br />
5. Skubitz K. Qualitative disorders of leukocytes. In: Greer JP, Foerster J, Lukens JN, Rodgers GM,<br />
Paraskevas F, Glader B, eds. Wintrobe’s Clinical Hematology. 11th ed. Philadelphia, Pa: Lippincott Williams<br />
& Wilkins; 2004; 1802-1803.<br />
Tracy I George, MD, Vice-Chair<br />
Hematology and Clinical Microscopy Resource Committee<br />
7
Blood Cell Identification – Ungraded<br />
Case History<br />
Blood smear is from a 48-year-old female with a history of small bowel obstruction and enterocutaneous<br />
fistula. CBC data include: WBC = 35.2 x 10 9 /L, RBC = 2.87 x 10 12 /L, HGB = 8.8 g/dL, HCT = 25.5%,<br />
MCV = 89 fL, MCH = 30.1 pg, MCHC = 33.8 g/dL, RDW 14.6%, PLT = 230 x 10 9 /L. Differential results<br />
are as follows: Neutrophils = 96%; Lymphocytes = 2%; Monocytes = 1%; Eosinophils = 0%;<br />
Basophils = 1%.<br />
BCK/BCP-06<br />
BCK BCP<br />
Referees Participants Participants Performance<br />
Identification No. % No. % No. % Evaluation<br />
Leukocyte with phagocytized<br />
fungi<br />
Macrophage with<br />
phagocytized fungi,<br />
leishmania, or toxoplasma<br />
16 94.0 1472 77.6 2228 80.3 Educational<br />
1 6.0 369 19.5 455 16.4 Educational<br />
All four images demonstrate leukocytes with phagocytized fungi. These leukocytes with phagocytized<br />
fungi were correctly identified by 94.0% of the referees and 79.2% of the participants. Six percent of<br />
the referees and 17.6 % of the participants identified macrophage with phagocytized fungi, leishmania<br />
or toxoplasma". As macrophages are seen in the bone marrow, identifying this cell as a macrophage is<br />
not the best choice. The yeast are round to oval. Fungi are only rarely seen in the peripheral blood and<br />
usually the number of organisms is few. Intracellular fungi may be confused with precipitated stain<br />
overlying a leukocyte, large toxic granules, Dohle bodies or large bacterial cocci.<br />
8
Blood Cell Identification – Ungraded<br />
BCK/BCP-07<br />
BCK/BCP-08<br />
BCK BCP<br />
Referees Participants Participants Performance<br />
Identification No. % No. % No. % Evaluation<br />
Fungi, extracellular 16 94.0 1805 95.3 2631 94.7 Educational<br />
Neutrophil necrobiosis<br />
(degenerated neutrophil)<br />
1 6.0 40 2.1 87 3.1 Educational<br />
Extracellular fungi, as seen in this peripheral blood smear, can be seen in patients with severe<br />
disseminated infection or as a possible contaminant. Finding intracellular fungi supports the diagnosis of<br />
disseminated infection. The extracellular fungi were correctly identified by 94.0% of the referees and<br />
94.9% of the participants.<br />
BCK BCP<br />
Referees Participants Participants Performance<br />
Identification No. % No. % No. % Evaluation<br />
Eosinophil, any stage 17 100.0 1896 99.6 2770 99.0 Educational<br />
This classic eosinophil has a bilobed nucleus and abundant coarse, orange-red granules of uniform size.<br />
Eosinophils have a classic appearance and were correctly identified by 100.0% of the referees and<br />
99.2% of the participants.<br />
9
Blood Cell Identification – Ungraded<br />
BCK/BCP-09<br />
10<br />
BCK BCP<br />
Referees Participants Participants Performance<br />
Identification No. % No. % No. % Evaluation<br />
Basophil, any stage 17 100.0 1820 95.6 2727 97.5 Educational<br />
Basophils are recognized by the densely stained granules of varying sizes and shape, which most<br />
frequently stain blue-black. Basophils have a classic appearance and were correctly identified by<br />
100.0% of the referees and 96.8% of the participants.
Blood Cell Identification – Ungraded<br />
BCK/BCP-10<br />
11<br />
BCK BCP<br />
Referees Participants Participants Performance<br />
Identification No. % No. % No. % Evaluation<br />
Neutrophil, toxic (to include<br />
toxic granulation and/or Dohle<br />
bodies, and/or toxic<br />
vacuolization)<br />
Neutrophil necrobiosis<br />
(degenerated neutrophil)<br />
17 100.0 1785 93.7 2654 94.9 Educational<br />
- - 99 5.2 71 2.5 Educational<br />
The neutrophils in this image exhibit toxic changes with prominent cytoplasmic vacuoles in the two<br />
cells marked with the arrows. The third cell in the image has another commonly seen toxic change,<br />
namely, toxic granulation. Toxic changes in neutrophils are present in many clinical situations, with<br />
cytoplasmic vacuolation most associated with sepsis, as seen in this patient. Toxic neutrophils were<br />
correctly identified by 100.0% of the referees and 94.4% of the participants.
Discussion<br />
The CBC results and the peripheral blood smear images from this 48-year-old female with an<br />
enterocutaneous fistula demonstrate disseminated candidiasis. In BCK/BCP-06, all four photos are<br />
leukocytes with phagocytized fungi. The yeast forms are round to oval and have a pseudo-halo surrounding<br />
them. As is not uncommonly seen in sepsis, the leukocytes exhibit reactive changes, to include cytoplasmic<br />
vacuoles, as shown here. Image BCK/BCP-07 has extracellular fungi. When extracellular fungi are found in<br />
the peripheral blood they are usually associated with intracellular organisms. These findings indicate a<br />
serious systemic infection.<br />
Systemic candidiasis is the fourth most common cause of nosocomial bloodstream infections. Over the past<br />
20 years the number of blood stream infections related to Candida species has risen 5- to 10-fold. There is<br />
a significant associated morbidity and mortality with systemic infection, with some studies reporting the<br />
mortality as high as 40.0%. Approximately two-thirds of the cases are due to Candida albicans and the<br />
remainder to non-albicans species. Candida glabrata in older patients and Candida parapsilosis in the<br />
neonatal and pediatric population comprise the majority of the non-albicans systemic infections.<br />
Candida species form a part of the normal microbial flora of the mouth and gastrointestinal tract.<br />
Transmission of Candida is almost exclusively endogenous, with rare cases of transmission from a health<br />
care worker or medical equipment. Oropharyngeal infection and vulvovaginal infection are the most<br />
commonly seen Candida infections. Neonates, neutropenic patients, hematopoietic stem cell and organ<br />
transplant recipients and other immunocompromised patients are at higher risk for systemic Candida<br />
infection. These patients present with fever and chills, which are unresponsive to antibacterial therapy.<br />
Severe sepsis, septic shock and end-organ dysfunction (acute renal failure, altered mental status) can<br />
develop quickly in these patients, even with appropriate therapy. Progression to septic shock is associated<br />
with an overall higher mortality.<br />
The diagnosis of systemic candidiasis is made with blood culture or culture of infected tissue. A gram stain<br />
of blood cultures demonstrating the presence of pseudohyphae in clusters is helpful in distinguishing<br />
Candida albicans from non-albicans. Drug resistance is rare. Testing for susceptibility to fluconazole,<br />
itraconazole and flucytosine may be helpful, especially with infections due to non-albicans species.<br />
A peripheral blood smear with neutrophilia, extracellular and intracellular fungi, as seen in this patient, is an<br />
insensitive method for diagnosing systemic Candida infection. Detection of candidemia by peripheral blood<br />
smear examination requires a yeast concentration of 1 to 5 X105 CFU/mL or greater. As positive blood<br />
cultures take at least 2 days to turn positive, exploration of more rapid diagnostic methods is being<br />
explored. Conventional PCR assays offer increased sensitivity, but more recent studies utilizing multiplex<br />
real-time PCR show even greater promise. Multiplex real-time PCR requires a very small amount of blood or<br />
tissue, detects many Candida species and provides a sensitive and specific result much quicker than<br />
standard blood culture. Additional studies using this technology may help in earlier diagnosis and treatment.<br />
Treatment of invasive candidiasis is with intravenous (IV) Amphotericin B or IV or oral Fluconazole. Hospital<br />
surveillance, prophylaxis when indicated (patients with prolonged severe neutropenia or who receive a<br />
solid-organ transplant) and better diagnostic tests may facilitate an earlier clinical diagnosis and improved<br />
overall survival.<br />
12
References:<br />
1. Bassetti M, Trecarichi EM, Righi E, et al. Incidence, risk factors and predictors of outcome of<br />
candidemia. Survey in 2 Italian university hospitals. Diagn Microbiol Infect Dis 2007;58:325-331.<br />
2. Branda, JA, Ferraro MJ, Kratz A. Sensitivity of peripheal blood smear review for the diagnosis of<br />
Candida fungemia. Arch Pathol Lab Med 2007;131:97-101.<br />
3. Candidiasis. www.cdc.gov<br />
4. Gudlaugsson O, Gillespie S, Lee K, et al. Attibutable mortality of nosocomial candidemia, revisited. Clin<br />
InfectDis 2003;37:1172-1177.<br />
4. Harrington A, McCourtney K, Nowowiejski D, Limaye A. Differentiation of Candida albicans from nonalbicans<br />
yeast directly from blood cultures by Gram stain morphology. Eur J Clin Microbiol Infect Dis<br />
2007;26:325-329.<br />
5. Innings A, Ullberg M, Johansson A, et al. Multiplex real-time PCR targeting the RNase P RNA gene for<br />
detection and identification of Candida species in blood. J Clin Micro 2007;45:874-880.<br />
6. Pfaller MA, Diekema DJ. Role of sentinel surveillance of candidemia: trends in species distribution and<br />
antifungal susceptibility. J Clin Micro 2002; 40:3551-3557.<br />
7. Rex JH, Walsh TJ, Sobel JD, et al. Practice guidelines for the treatment of candidiasis. Infectious<br />
Diseases Society of America. Clin Infect Dis 2000;30:662-678.<br />
8. Wisplinghoff H, Seifert H, Wenzel RP, Edmond MB. Inflammatory response and clinical course of adult<br />
patients with nosocomial bloodstream infections caused by Candida spp. Clin Microbiol Infect<br />
2006;12:170-177.<br />
Deborah A. Perry, MD<br />
Hematology and Clinical Microscopy Resource Committee<br />
13