Biomechanical and histological comparison of self-drilling and self ...
Biomechanical and histological comparison of self-drilling and self ...
Biomechanical and histological comparison of self-drilling and self ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
ORIGINAL ARTICLE<br />
<strong>Biomechanical</strong> <strong>and</strong> <strong>histological</strong> <strong>comparison</strong> <strong>of</strong><br />
<strong>self</strong>-<strong>drilling</strong> <strong>and</strong> <strong>self</strong>-tapping orthodontic<br />
microimplants in dogs<br />
Yan Chen, a Hong-In Shin, b <strong>and</strong> Hee-Moon Kyung c<br />
Hohhot, China, <strong>and</strong> Daegu, Korea<br />
Introduction: The purpose <strong>of</strong> this study was to compare the influences <strong>of</strong> different implant modalities on<br />
orthodontic microimplants <strong>and</strong> surrounding tissues biomechanically <strong>and</strong> <strong>histological</strong>ly. Methods: Fifty-six<br />
titanium alloy microimplants placed on the buccal side <strong>of</strong> the maxillae <strong>and</strong> the m<strong>and</strong>ibles in 2 dogs were<br />
divided into 2 groups <strong>of</strong> 28; one group <strong>of</strong> microimplants was <strong>self</strong>-<strong>drilling</strong>, <strong>and</strong> the other was <strong>self</strong>-tapping.<br />
Approximately 200 g <strong>of</strong> continuous <strong>and</strong> constant forces were applied immediately between 2 microimplants<br />
by stretching closed nickel-titanium coil springs for 9 weeks. Peak insertion torque <strong>and</strong> removal torque were<br />
recorded immediately after the implants were placed <strong>and</strong> when the dogs were killed, respectively.<br />
Undecalcified sections <strong>of</strong> the microimplants <strong>and</strong> the surrounding tissues were studied with light microscope<br />
<strong>and</strong> fluorescent microscope. Results: Success rates were higher in the <strong>self</strong>-<strong>drilling</strong> group (93%) than in<br />
<strong>self</strong>-tapping group (86%). Higher peak insertion torque <strong>and</strong> peak removal torque values were seen in the<br />
<strong>self</strong>-<strong>drilling</strong> group in both the maxilla <strong>and</strong> the m<strong>and</strong>ible. A tendency to fracture was found in <strong>self</strong>-<strong>drilling</strong><br />
group. The percentage <strong>of</strong> bone-to-implant contact values was greater in the <strong>self</strong>-<strong>drilling</strong> group. Conclusions:<br />
Self-<strong>drilling</strong> microimplants can provide better anchorage <strong>and</strong> can be recommended for use in the maxilla <strong>and</strong><br />
in thin cortical bone areas <strong>of</strong> the m<strong>and</strong>ible. (Am J Orthod Dent<strong>of</strong>acial Orthop 2008;133:44-50)<br />
The <strong>self</strong>-tapping method <strong>of</strong> microimplant placement<br />
is an excellent approach in orthodontics,<br />
1,2<br />
although it has some shortcomings. Compared<br />
with the pretapping method, the <strong>self</strong>-tapping<br />
method <strong>of</strong>fers quicker placement, less damage to bone,<br />
3<br />
<strong>and</strong> a better grip in bone. A prerequisite for <strong>self</strong>tapping<br />
placement is pilot <strong>drilling</strong> to prepare a hole for<br />
the implant. 4 Particularly for interradicular microimplants,<br />
pilot <strong>drilling</strong> has potential dangers, such as<br />
damage to tooth roots, drill-bit breakage, over<strong>drilling</strong>,<br />
5-8<br />
<strong>and</strong> thermal necrosis <strong>of</strong> bone. Also, the process takes<br />
time.<br />
The growing dem<strong>and</strong> for absolutely rigid orthodontic<br />
anchorage has led to an expansion <strong>of</strong> implant<br />
technology. 8 <strong>drilling</strong> procedure is simpler <strong>and</strong> involves less use <strong>of</strong><br />
instruments.<br />
Recent advances in biomaterials have<br />
resulted in a new <strong>self</strong>-<strong>drilling</strong> implant system for rigid<br />
8<br />
internal fixation in maxill<strong>of</strong>acial surgery. The <strong>self</strong>-<br />
9<br />
Nevertheless, differences in biomechanical characteristics<br />
<strong>and</strong> mechanisms between <strong>self</strong>-<strong>drilling</strong> microimplants<br />
(SDIs) <strong>and</strong> <strong>self</strong>-tapping microimplants (STIs)<br />
in terms <strong>of</strong> how they are anchored to bone have not<br />
10-12<br />
been clarified. In previous animal <strong>and</strong> clinical<br />
studies, 13-16 osseointegrated dental implants have behaved<br />
like ankylosed teeth to provide orthodontic<br />
anchorage. In theory, SDIs might cause less damage to<br />
bone during placement; therefore, osseointegration<br />
17<br />
might happen earlier <strong>and</strong> be better than with STIs.<br />
Because primary stability is thought to be essential in<br />
achieving ideal bone-to-implant contact (BIC), clinical<br />
studies have shown significantly higher placement<br />
torque with SDIs,<br />
18 but no histologic data <strong>of</strong> BIC<br />
values have been shown. Based on the limited literature<br />
<strong>and</strong> clinical experiences,<br />
8,19 SDIs might have a relatively<br />
high anchorage value for the en-masse movement<br />
<strong>of</strong> anterior teeth, molar uprighting, <strong>and</strong> forward movement.<br />
Perhaps the BIC values at the interface can be<br />
enhanced with SDIs,<br />
17 aAssociate pr<strong>of</strong>essor, Oral Department, Attached Hospital <strong>of</strong> Inner Mongolia<br />
Medical University, Hohhot, China.<br />
bChairman <strong>and</strong> pr<strong>of</strong>essor, Department <strong>of</strong> Oral Pathology, School <strong>of</strong> Dentistry,<br />
Kyungpook National University, Daegu, Korea.<br />
cChairman <strong>and</strong> pr<strong>of</strong>essor, Department <strong>of</strong> Orthodontics, School <strong>of</strong> Dentistry,<br />
Kyungpook National University, Daegu, Korea.<br />
so that they can be expected to<br />
Reprint requests to: Hee-Moon Kyung, Department <strong>of</strong> Orthodontics, Dental<br />
School, Kyungpook National University, 188-1, Sam Duk 2 Ga, Jung Gu,<br />
Daegu, Korea 700-412; e-mail, hmkyung@knu.ac.kr.<br />
improve the anchorage <strong>of</strong> implants, especially in areas<br />
<strong>of</strong> low bone density, to increase the success rate.<br />
Submitted, September 2005; revised <strong>and</strong> accepted, January 2006.<br />
0889-5406/$34.00<br />
Copyright © 2008 by the American Association <strong>of</strong> Orthodontists.<br />
doi:10.1016/j.ajodo.2007.01.023<br />
The objectives <strong>of</strong> this study were to compare the<br />
biomechanical properties <strong>of</strong> microimplants with different<br />
<strong>drilling</strong> methods by measuring peak insertion torque<br />
44
American Journal <strong>of</strong> Orthodontics <strong>and</strong> Dent<strong>of</strong>acial Orthopedics<br />
Volume 133, Number 1<br />
(PIT) <strong>and</strong> peak removal torque (PRT) in an animal<br />
model, <strong>and</strong> to investigate the influence <strong>of</strong> <strong>self</strong>-<strong>drilling</strong><br />
<strong>and</strong> <strong>self</strong>-tapping techniques on BIC values under orthodontic<br />
force.<br />
MATERIALS AND METHODS<br />
Two adult female mongrel dogs (weight, 13 kg)<br />
were housed in the animal laboratory at Kyungpook<br />
National University Medical College in Daegu, Korea.<br />
All permanent teeth were erupted, <strong>and</strong> maxillary <strong>and</strong><br />
m<strong>and</strong>ibular growth was completed. The treatment <strong>of</strong> the<br />
experimental animals was approved by the ethics committee<br />
<strong>of</strong> the Medical College at Kyungpook National<br />
University.<br />
Fifty-six threaded microimplants (Absoanchor,<br />
Dentos, Daegu, Korea) made <strong>of</strong> titanium alloy (titanium,<br />
aluminum, vanadium) were used for this experiment<br />
<strong>and</strong> divided into 2 groups. The head <strong>of</strong> the<br />
microimplant was hexagonal to enable placement with<br />
h<strong>and</strong>-driver; it had a small hole for threads <strong>and</strong> ligature<br />
wires. SDIs, with a specially designed sharp tip <strong>of</strong><br />
conical shape with threads, served as the study group,<br />
<strong>and</strong> STIs with an ordinary tip served as the control<br />
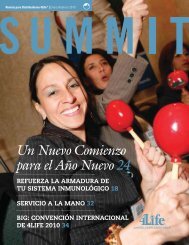
group (28 for each group). Size 1312-07—tapered with<br />
1.3 mm neck diameter, 1.2 mm diameter near the apex,<br />
<strong>and</strong> threaded intrabone part 7 mm—was chosen for this<br />
experiment (Fig 1). The 2 types <strong>of</strong> microimplants were<br />
the same size <strong>and</strong> shape (except for the tip), had the<br />
same placement angle <strong>and</strong> similar force magnitudes,<br />
<strong>and</strong> were intended for similar bone densities.<br />
The buccal side <strong>of</strong> the bilateral maxilla <strong>and</strong> m<strong>and</strong>ible<br />
<strong>of</strong> the dogs was chosen as the recipient site for<br />
symmetrically placing 2 groups <strong>of</strong> microimplants. The<br />
left side was for SDIs, <strong>and</strong> the right side was for STIs<br />
Chen, Shin, <strong>and</strong> Kyung 45<br />
Fig 1. Microimplants <strong>and</strong> h<strong>and</strong>-driver used in this<br />
study: A, STI with tip; B, SDI with tip; C, microimplant<br />
head; D, h<strong>and</strong>-driver.<br />
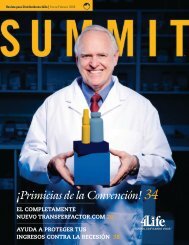
head <strong>of</strong> the microimplant remained outside the attached<br />
gingiva for connecting the nickel-titanium springs (Fig 2).<br />
Twenty-eight STIs were placed with the <strong>self</strong>-tapping<br />
method. A pilot hole was drilled first with a<br />
0.9-mm diameter round bur, as deep as the length <strong>of</strong><br />
in 1 dog (Fig 2). The left maxilla <strong>and</strong> the right m<strong>and</strong>iblemicroimplant<br />
thread part, with a h<strong>and</strong>piece at a speed<br />
received SDIs, <strong>and</strong> the right maxilla <strong>and</strong> the left <strong>of</strong> 500 rpm by <strong>drilling</strong> intermittently. Saline solution<br />
m<strong>and</strong>ible received STIs in the other dog. All microim- was used to keep the bur <strong>and</strong> drill cooled <strong>and</strong> the<br />
plant placement procedures were performed aseptically placement site lubricated. Then the microimplants were<br />
with a 90° implant placement angle to the long axis <strong>of</strong> manually placed with the same long h<strong>and</strong>-driver, ac-<br />
the teeth. Oral hygiene was achieved by rinsing each<br />
20<br />
cording to the technique described by Kyung et al.<br />
dog’s mouth biweekly with 0.2% chlorhexidine glu- Approximately 200 g <strong>of</strong> continuous <strong>and</strong> constant<br />
conate solution.<br />
horizontal force was immediately applied by stretching<br />
For the placement <strong>of</strong> the microimplants, the dogs nickel-titanium superelastic closed-coil springs (Tomy,<br />
were anesthetized with a cocktail composed <strong>of</strong> ket- Tokyo, Japan) between 2 microimplants for 9 weeks (Fig<br />
amine (Ketara; Yuhan, Seoul, Korea) at a dose <strong>of</strong> 10 2). The springs contacted the microimplants directly.<br />
mg per kilogram <strong>of</strong> body weight, xylazine (Rompun An operator who has placed more than 100 microim-<br />
Bayer Korea, Seoul, Korea) at 0.4 mg per kilogram <strong>of</strong> plants in patients <strong>and</strong> for animal experiments placed all<br />
body weight, <strong>and</strong> saline solution.<br />
the microimplants.<br />
Twenty-eight SDIs were placed with the <strong>self</strong>-drill- PIT—the force <strong>of</strong> the maximum clockwise moveing<br />
method. They were manually placed through the ment that stripped bone from screw insertion until it<br />
attached gingiva with a long h<strong>and</strong>-driver (Dentos, was perfectly placed—was measured with a precision<br />
Daegu, Korea) that was especially designed for these digital indicator (EMT, E-mobile tech 17000 series;<br />
microimplants, without pilot <strong>drilling</strong> <strong>and</strong> incision. The SEEC, Seoul, Korea) <strong>drilling</strong> after placement for all
46 Chen, Shin, <strong>and</strong> Kyung<br />
microimplants in the 2 groups. After 9 weeks <strong>of</strong> observation,<br />
PRT—the force <strong>of</strong> the maximum counterclockwise<br />
movement to loosen the microimplants—was<br />
measured with the same machine for 12 stable microimplants<br />
at symmetrical sites in each group.<br />
The stability <strong>of</strong> the microimplants was measured<br />
with dental tweezers; failure was defined if a microimplant<br />
could be moved in any direction after the 9-week<br />
observation period.<br />
A vital staining procedure was used for the animals.<br />
Oxytetracycline (15 mg per kilogram per day) was<br />
given intramuscularly for the first 4 days after the<br />
microimplants were placed. A subcutaneous injection<br />
<strong>of</strong> 1% calcein (15 mg per kilogram per day) was given<br />
at the fourth week, <strong>and</strong> 0.16% alizarin red (75 mg per<br />
kilogram per day) was injected intramuscularly at the<br />
seventh week.<br />
The anesthetized dogs were killed by intracardial<br />
perfusion with neutral 10% formaldehyde solution. The<br />
maxillary <strong>and</strong> m<strong>and</strong>ibular bones containing microimplants<br />
were dissected. The specimens were fixed in the<br />
same solution for more than 24 hours. After being washed<br />
with distilled water, each implant area was separated with<br />
a saw (D-54518, Proxxon; Woo Sung E&ICo,Ltd,<br />
Tokyo, Japan).<br />
Fourteen microimplants with surrounding tissue were<br />
selected for histologic evaluation from the 2 groups at<br />
symmetrically interradicular areas <strong>of</strong> the maxillae <strong>and</strong> the<br />
m<strong>and</strong>ibles <strong>of</strong> the 2 dogs. These specimens were infiltrated<br />
with vilanueva bone stain propylene oxide from a starting<br />
solution <strong>of</strong> 70% alcohol <strong>and</strong> stained. This procedure<br />
included 11 steps <strong>and</strong> lasted more than 3 weeks.<br />
Before being embedded in vilanueva bone stain<br />
propylene oxide, the specimens were dehydrated <strong>and</strong><br />
defatted with graded ethanol. Each embedded implant<br />
with bone was sectioned sagittally with a low-speed<br />
digital saw (Accutom-50; Struers, Ballerup, Denmark)<br />
into thicknesses <strong>of</strong> 500 m. These sections were<br />
ground with a grinding machine (Rotopol-35; Struers)<br />
until the implants <strong>and</strong> the surrounding tissues could be<br />
seen clearly. Microscope slides, prepared by mounting<br />
American Journal <strong>of</strong> Orthodontics <strong>and</strong> Dent<strong>of</strong>acial Orthopedics<br />
January 2008<br />
Fig 2. Placement <strong>of</strong> microimplants in dog jaw with force applied by nickel-titanium coil springs: A,<br />
SDI; B, STI.<br />
Table I. Comparison <strong>of</strong> peak insertion torque values<br />
between groups (in Ncm)<br />
Group (n 14 each group) STI SDI P<br />
Maxilla 3.5 2.1 5.6 1.1 .017<br />
M<strong>and</strong>ible 7.4 1.1 8.7 2.3 .029<br />
Significance, P .05.<br />
the flattened sections with low fluorescence, were<br />
observed with a light microscope <strong>and</strong> a fluorescent<br />
microscope.<br />
Histomorphometric analysis was performed on the<br />
digitized images from the microscope with a camera<br />
system (Olympus, Tokyo, Japan). The images obtained<br />
with 100-times magnification were combined into 1<br />
figure including the entire implant surface <strong>and</strong> analyzed<br />
with image analysis s<strong>of</strong>tware (Image & Microscope<br />
Technique, Goleta, Calif). For each microimplant, the<br />
bone contact sections were measured <strong>and</strong> expressed as<br />
percentages <strong>of</strong> BIC.<br />
Data are expressed as means <strong>and</strong> st<strong>and</strong>ard deviations.<br />
The differences between the SDI <strong>and</strong> STI groups<br />
were evaluated with the Student t test. A P value less<br />
than .05 was considered significant.<br />
RESULTS<br />
Not all the microimplants remained firm enough<br />
during the experimental period. In the STI group, the<br />
overall success rate was 86%; 4 microimplants loosened<br />
<strong>and</strong> tipped. Two failures occurred in the SDI<br />
group; 1 microimplant loosened, <strong>and</strong> another in the<br />
distal region <strong>of</strong> the m<strong>and</strong>ibular second molar fractured<br />
in the fourth week. The success rate was 93%.<br />
Mild inflammation <strong>and</strong> swelling <strong>of</strong> the alveolar<br />
gingivae were observed on both sides <strong>of</strong> the maxilla<br />
<strong>and</strong> the m<strong>and</strong>ible. They were more serious on the left<br />
side in both dogs.<br />
The <strong>comparison</strong> <strong>of</strong> the PIT values taken at the<br />
beginning <strong>of</strong> the experiment showed significant differ-
American Journal <strong>of</strong> Orthodontics <strong>and</strong> Dent<strong>of</strong>acial Orthopedics<br />
Volume 133, Number 1<br />
Table II. Comparison <strong>of</strong> peak removal torque values<br />
between groups (in Ncm)<br />
Group (n 6 each group) STI SDI P<br />
Maxilla 5.7 2.3 6.5 2.2 NS<br />
M<strong>and</strong>ible 6.1 0.5 7.1 2.0 NS<br />
NS, P .05.<br />
Fig 3. Bone implant interfaces: A, SDI; B, STI (20X<br />
original magnification).<br />
ences between the 3 groups in the maxilla <strong>and</strong> the<br />
m<strong>and</strong>ible (Table I).<br />
The <strong>comparison</strong> <strong>of</strong> mean PRT showed no statistically<br />
significant difference between the 2 groups after 9<br />
weeks (Table II).<br />
Histologic assessment showed good histocompatibility,<br />
with various bone structures interspersed with<br />
fibrous connective tissues around the microimplants in<br />
both groups (Fig 3). Better osseous tissue formation<br />
around the microimplants <strong>and</strong> greater original bone<br />
were seen in the SDI group than in STI group, as<br />
evidenced by calcein <strong>and</strong> oxytetracycline labeling.<br />
Remodeling <strong>and</strong> apposition were seen more in the SDI<br />
group than in STI group (Fig 4).<br />
BIC values are shown in Table III.<br />
DISCUSSION<br />
After the 9-week period, an important finding in<br />
this study was the high success rates <strong>of</strong> the SDI <strong>and</strong> the<br />
STI groups. The results confirmed our original deduction<br />
<strong>of</strong> greater success in the SDI group (93%) than in<br />
Chen, Shin, <strong>and</strong> Kyung 47<br />
the STI group (86%). Two microimplants failed in the<br />
SDI group; 1 loosened, <strong>and</strong> the other fractured in the<br />
fourth week. In a similar animal experiment, Kim <strong>and</strong><br />
Chang 21 observed a higher success rate in miniscrews<br />
in the drill-free group than in the drill group with a<br />
1-week healing period.<br />
The main reason for the failures might have been<br />
the poor initial stability caused by early loading <strong>and</strong> the<br />
exposed healing situation. This was confirmed in the<br />
19<br />
pig experiment <strong>of</strong> Heidemann et alwith<br />
a 100%<br />
success rate in the groups <strong>of</strong> <strong>self</strong>-<strong>drilling</strong> screws (SDS)<br />
<strong>and</strong> <strong>self</strong>-tapping screws (STS), which healed in a closed<br />
situation <strong>and</strong> without force.<br />
Because <strong>of</strong> early loading in our study, the microimplants<br />
stayed in the bone with mechanical interlock<br />
without bone <strong>and</strong> implant osseointegration at the be-<br />
1<br />
ginning <strong>of</strong> the experiment. Roberts et demonstrated<br />
al<br />
that immediate loading was deleterious to implant<br />
stability in their animal study. However, SDIs have<br />
been proven to have greater strength <strong>and</strong> highly mechanical<br />
friction with bone to keep initial stability <strong>and</strong><br />
to resist micromovement.<br />
19 Initial stability was be -<br />
lieved to play an important role in the success <strong>of</strong> our<br />
interradicular microimplants that healed in exposed<br />
situations. 22<br />
PIT, which exhibited the holding strength to resist<br />
loosening <strong>and</strong> loss <strong>of</strong> the implants, was measured at the<br />
beginning <strong>of</strong> the experiment for each microimplant in<br />
both groups. The mean PIT values <strong>of</strong> the SDIs in the<br />
maxilla <strong>and</strong> the m<strong>and</strong>ible were 5.6 <strong>and</strong> 8.7 Ncm,<br />
respectively. In the STI group, PIT values were 3.5<br />
Ncm for the maxilla <strong>and</strong> 7.4 Ncm for the m<strong>and</strong>ible. PIT<br />
values were found to be significantly different between<br />
the SDI <strong>and</strong> STI groups, both in the maxilla <strong>and</strong> the<br />
m<strong>and</strong>ible, but lower in the maxilla. Our results were<br />
similar to those from the clinical experiment <strong>of</strong> Schon<br />
et al 23 for craniomaxill<strong>of</strong>acial procedures; they found<br />
that insertion torque <strong>of</strong> the SDS was higher compared<br />
with that <strong>of</strong> the STS in humans. Microimplants with<br />
high PIT might have closer initial contact with bone<br />
<strong>and</strong> might be good for bone remodeling. From an anchorage<br />
perspective, the greater the contact between the<br />
surface <strong>of</strong> the microimplant threads <strong>and</strong> the cortical bone,<br />
24,25<br />
the higher the initial grip <strong>of</strong> microimplants would be.<br />
Fracture is a disadvantage <strong>of</strong> microimplants even<br />
when they are placed without excessive force. The<br />
results showed high PIT values for thin-diameter microimplants,<br />
<strong>and</strong> high bone density might be dangerous<br />
to SDIs. According to the principle <strong>of</strong> conservation <strong>and</strong><br />
transformation <strong>of</strong> energy, SDIs have higher pressure<br />
than STIs, <strong>and</strong> pretapped implants were placed after the<br />
pilot holes were drilled. Even though SDIs have many<br />
advantages, if the bone is dense, they should not to be
48 Chen, Shin, <strong>and</strong> Kyung<br />
Fig 4. Fluorescent microscope views <strong>of</strong> middle part <strong>of</strong> peri-implant bone at first molar area<br />
<strong>of</strong> 1 dog’s m<strong>and</strong>ible: A <strong>and</strong> B, SDI; C <strong>and</strong> D, STI (100X original magnification).<br />
Table III. Comparison <strong>of</strong> BIC values between groups<br />
Group SDI STI<br />
Maxilla 39.28% (n 4) 27.96% (n 4)<br />
M<strong>and</strong>ible 47.44% (n 3) 26.35% (n 3)<br />
American Journal <strong>of</strong> Orthodontics <strong>and</strong> Dent<strong>of</strong>acial Orthopedics<br />
January 2008<br />
in the m<strong>and</strong>ible in the STI group. Removal torque, as a<br />
biomechanical method to measure anchorage or endosseous<br />
integration in which greater forces are required to<br />
remove microimplants, might be associated with increases<br />
in the strength <strong>of</strong> osseous integration.<br />
Compared with STIs, SDIs showed good resistance<br />
to shear force with bone growing into the threads <strong>of</strong> the<br />
microimplants. The secondary bone healing response<br />
resulted in biomechanical bone interlocking, which<br />
developed sufficient interface to resist shear strength<br />
<strong>and</strong> was sufficient to withst<strong>and</strong> orthodontic loads.<br />
However, there was no statistically significant difference<br />
in PRT between the 2 <strong>drilling</strong> methods. This<br />
chosen. STIs should be considered instead. In the<br />
maxilla <strong>and</strong> areas with thin cortical bone in the m<strong>and</strong>ible,<br />
microimplants would penetrate easily. Failure<br />
due to stripping <strong>of</strong> bone was infrequent, so pilot <strong>drilling</strong><br />
was not necessary.<br />
Heidemann et al<br />
19 reported the increase <strong>of</strong> PIT <strong>and</strong><br />
shearing forces on the screw it<strong>self</strong>; fracture <strong>of</strong> the<br />
screws was caused in thick cortical bone in their<br />
in-vitro test. Ellis <strong>and</strong> Laskin<br />
24 believed that, if a screw<br />
was stressed sufficiently in tension or torsion, it ultimately<br />
would be broken. They thought that, if screws<br />
were subjected to torsion <strong>and</strong> flexion stress, they would<br />
fail at a lower tensile stress value.<br />
This was validated by an in-vitro trial <strong>of</strong> screws<br />
with diameters <strong>of</strong> 0.8 to 2.0 mm; the screw diameter<br />
was the major predictor for holding <strong>and</strong> breaking<br />
strength. 26 23<br />
was supported by the results <strong>of</strong> Schon et in al which<br />
the PRT value <strong>of</strong> the SDIs was similar to that <strong>of</strong> the<br />
STIs at the same location: 4 Ncm in the maxilla <strong>and</strong> 12<br />
Ncm in the m<strong>and</strong>ible. The PRT values in the SDI <strong>and</strong><br />
STI groups might suggest that certain factors associated<br />
with microimplants stimulate in-vivo incorporation <strong>of</strong><br />
bone. Several previous investigations pointed out that<br />
removal torque measurement usually gave concomitant<br />
29-31<br />
results with histomorphometric evaluation <strong>of</strong> BIC.<br />
The authors <strong>of</strong> that study emphasized that As time went on, the PRT values in the SDI <strong>and</strong> STI<br />
the larger the diameter <strong>of</strong> the screw, the better its groups might be similar, <strong>and</strong> it was not expected that<br />
holding strength in thick bone.<br />
SDIs would have greater PRT values than STIs. In<br />
The use <strong>of</strong> reverse torque for measuring the shear contrast to previous reports,<br />
force required to rupture the bone-microimplant interface<br />
provided important information concerning bone<br />
growing into the fixture surface. Our PRT values were<br />
6.5 Ncm in the maxilla <strong>and</strong> 7.1 Ncm in the m<strong>and</strong>ible in<br />
the SDI group, <strong>and</strong> 5.7 Ncm in the maxilla <strong>and</strong> 6.1 Ncm<br />
27-30 our lower PRT values<br />
might be explained by the small size <strong>of</strong> the microimplants<br />
<strong>and</strong> the short observation time.<br />
It has been widely accepted that osseointegrated<br />
implants can provide absolute anchorage for tooth<br />
movement. The BIC value is a parameter for the linear
American Journal <strong>of</strong> Orthodontics <strong>and</strong> Dent<strong>of</strong>acial Orthopedics<br />
Volume 133, Number 1<br />
surface <strong>of</strong> microimplants that is directly in contact with<br />
bone matrix <strong>and</strong> is calculated with s<strong>of</strong>tware <strong>and</strong> expressed<br />
as a percentage <strong>of</strong> the total microimplant surface. In this<br />
study, the mean BIC values in the SDI group were 39.28%<br />
in the maxilla <strong>and</strong> 47.44% in the m<strong>and</strong>ible. In the STI<br />
group, the mean BIC values were 27.96% <strong>and</strong> 26.35% in<br />
the maxilla <strong>and</strong> the m<strong>and</strong>ible, respectively. Because the<br />
BIC values were higher in the SDI group than in the STI<br />
group, this showed that the <strong>drilling</strong> method had an effect<br />
on bone-to-microimplant contact; this was further confirmed<br />
by PRT values <strong>and</strong> histologic findings <strong>of</strong> more<br />
original <strong>and</strong> new bone in the SDI group.<br />
BIC values <strong>of</strong> 93.8% in the SDS group <strong>and</strong> 81% in<br />
the STS group were found after 6 months <strong>of</strong> observation<br />
in pigs.<br />
19 Heidemann et al<br />
19 demonstrated that the<br />
BIC values in the SDS group were superior to those in<br />
the STS group because <strong>of</strong> the greater amount <strong>of</strong> original<br />
bone in the threads <strong>of</strong> the drill-free screws. Similarly, in<br />
21<br />
the study <strong>of</strong> Kim <strong>and</strong> Chang, the mean BIC value<br />
(43.68%) in the drill-free group was higher than in the<br />
drill group (23.41%) in dogs. Obviously, compared<br />
with previous studies, our results indicate that using<br />
SDIs without chemical <strong>and</strong> biologic modification<br />
caused less damage to bone, <strong>and</strong> the time <strong>of</strong> bone<br />
modeling <strong>and</strong> remodeling was reduced because the<br />
bone debris was transported <strong>and</strong> deposited on the bone<br />
surface around the implant tip because <strong>of</strong> the conical<br />
shaft.<br />
19<br />
Compared with the results <strong>of</strong> Heidemann et al, the<br />
BIC values in our study were lower. This difference<br />
could be an internal response <strong>of</strong> bone to the implant<br />
31<br />
time <strong>and</strong> the healing condition. Melsen <strong>and</strong> Costa<br />
observed BIC values <strong>of</strong> 10% to 58% after 6 months <strong>of</strong><br />
forcing without a healing period for miniscrews. They<br />
found that the BIC ratio increased with implantation<br />
time but was independent <strong>of</strong> the type <strong>of</strong> bone <strong>and</strong> the<br />
magnitude <strong>of</strong> force. Our results have elucidated the<br />
mechanism behind the behavior <strong>of</strong> cells on implant<br />
surfaces, <strong>and</strong> we report an increase in BIC contact by<br />
using different <strong>drilling</strong> methods.<br />
Because the numbers <strong>of</strong> dogs <strong>and</strong> microimplants<br />
were limited, this study might be regarded as a pilot.<br />
However, the results were unequivocal because the<br />
tested microimplants were placed symmetrically. Further<br />
studies with different force magnitudes after a<br />
short healing period are required for more discussion<br />
<strong>and</strong> definite results.<br />
CONCLUSIONS<br />
By comparing the biomechanical <strong>and</strong> histologic<br />
properties between SDIs <strong>and</strong> STIs, without a healing<br />
period, we found high success rates in both groups.<br />
Chen, Shin, <strong>and</strong> Kyung 49<br />
PIT, PRT, <strong>and</strong> BIC values were higher in the SDI group<br />
than in the STI group.<br />
We recommend using SDIs in the maxilla <strong>and</strong> the<br />
thin cortical bone areas <strong>of</strong> the m<strong>and</strong>ible because there is<br />
less damage <strong>and</strong> use <strong>of</strong> instruments. In areas <strong>of</strong> dense<br />
cortical bone, STIs <strong>and</strong> SDIs with larger diameters can<br />
be recommended.<br />
REFERENCES<br />
1. Roberts WE, Smith R, Zilberman Y. Osseous adaptation to<br />
continuous loading <strong>of</strong> rigid endosseous implants. Am J Orthod<br />
1984;68:95-111.<br />
2. Smalley WM, Shapiro PA, Hohi TH, Kokich VG, Bränemark PI.<br />
Osseointergrated titanium implants for maxill<strong>of</strong>acial protraction<br />
in monkeys. Am J Orthod Dent<strong>of</strong>acial Orthop 1988;94:285-95.<br />
3. Foley W, Frost D, Tucker M. The effect <strong>of</strong> repetitive screw hole<br />
use on the retentive strength <strong>of</strong> pretapped <strong>and</strong> <strong>self</strong>-tapped screws.<br />
Int J Oral Maxill<strong>of</strong>ac Surg 1990;48:264-7.<br />
4. Bahr W. Pretapped <strong>and</strong> <strong>self</strong>-tapping screw in the human midface.<br />
Int J Oral Maxill<strong>of</strong>ac Surg 1990;19:51-3.<br />
5. Park HS, Kwon OW, Sung JH. Micro-implant anchorage for<br />
forced eruption <strong>of</strong> impacted canines. J Clin Orthod 2004;38:297-<br />
302.<br />
6. Park HS, Kwon TG, Sung JH. Nonextraction treatment with<br />
microscrew implants. Angle Orthod 2004;74:539-49.<br />
7. Park HS, Kwon TG. Sliding mechanics with microscrew implant<br />
anchorage. Angle Orthod 2004;74:703-10.<br />
8. Paik CH, Woo YJ, Kim JS, Park JU. Use <strong>of</strong> miniscrew for<br />
intermaxillary fixation <strong>of</strong> lingual-orthodontic surgery patients.<br />
J Clin Orthod 2002;36:132-6.<br />
9. Paik CH, Woo YJ, Boyd RL. Treatment <strong>of</strong> an adult patient with<br />
vertical maxillary excess using miniscrew fixation. J Clin Orthod<br />
2003;37:423-8.<br />
10. Linder-Aronson S, Nordenram A, Anneroth G. Titanium implant<br />
anchorage in orthodontic treatment: an experimental investigation<br />
in monkeys. Eur J Orthod 1990;12:414-9.<br />
11. Roberts WE, Marshall KJ, Mozsary PG. Rigid endosseous<br />
implant utilized as anchorage to protract molars <strong>and</strong> close an<br />
atrophic extraction site. Angle Orthod 1990;60:135-52.<br />
12. Majzoub Z, Finotti M, Miotti F, Giardino R, Aldini NN, Cordioli<br />
G. Bone response to orthodontic loading <strong>of</strong> endosseous implants<br />
in the rabbit calvaria: early continuous distalizing forces. Eur<br />
J Orthod 1999;21:223-30.<br />
13. Odman J, Lekholm U, Jemt T, Bränemark PL, Thil<strong>and</strong>er B.<br />
Osseointergrated implants—a new approach in orthodontic treatment.<br />
Eur J Orthod 1988;10:98-105.<br />
14. Odman J, Lekholm U, Jemt T, Thil<strong>and</strong>er B. Osseointergrated<br />
implants as orthodontic anchorage in the treatment <strong>of</strong> partially<br />
edentulous adult patients. Eur J Orthod 1994;16:187-201.<br />
15. Roberts WE, Helm FR, Marshall KJ, Gongl<strong>of</strong>f RK. Rigid<br />
endosseous implants for orthodontic <strong>and</strong> orthopedic anchorage.<br />
Angle Orthod 1989;59:247-56.<br />
16. Wehrbein H, Feife H. Palatal implant anchorage reinforcement<br />
<strong>of</strong> posterior teeth: a prospective study. Am J Orthod Dent<strong>of</strong>acial<br />
Orthop 1999;116:676-86.<br />
17. Heidemann W, Gerlach KL, Grobel KH, Kollner HG. Drill free<br />
screws: a new form <strong>of</strong> osteosynthesis screw. J Craniomaxill<strong>of</strong>ac<br />
Surg 1998;26:163-8.<br />
18. Heidemann W, Gerlach KL. Clinical applications <strong>of</strong> drill free<br />
screws in maxill<strong>of</strong>acial surgery. J Craniomaxill<strong>of</strong>ac Surg 1999;<br />
27:252-5.
50 Chen, Shin, <strong>and</strong> Kyung<br />
19. Heidemann W, Terheyden H, Gerlach KL. Analysis <strong>of</strong> the<br />
osseous/metal interface <strong>of</strong> drill free screws <strong>and</strong> <strong>self</strong>-tapping<br />
screws. J Craniomaxill<strong>of</strong>ac Surg 2001;29:69-74.<br />
20. Kyung HM, Park HS, Bae SM. Development <strong>of</strong> orthodontic<br />
micro-implants for intraoral anchorage. J Clin Orthod 2003;37:<br />
321-8.<br />
21. Kim JW, Chang YL. Effects <strong>of</strong> <strong>drilling</strong> process in stability <strong>of</strong><br />
micro-implants used for the orthodontic anchorage. Korea<br />
J Orthod 2002;32:107-15.<br />
22. Sharawy M, Misch CE, Weller N, Tehemar S. Heat generation<br />
during implant <strong>drilling</strong>: the significance <strong>of</strong> motor speed. J Oral<br />
Maxill<strong>of</strong>ac Surg 2002;60:1160-9.<br />
23. Schon R, Gellrich NC, Gutwald R, Schramm A, Schmelzeisen R.<br />
Indication <strong>of</strong> <strong>self</strong>-<strong>drilling</strong> screws in craniomaxill<strong>of</strong>acial surgery.<br />
Int poster J Dent Oral Med 2000;2:poster 43.<br />
24. Ellis JA Jr, Laskin DM. Analysis <strong>of</strong> seating <strong>and</strong> fracturing torque<br />
<strong>of</strong> bicortical screws. J Oral Maxill<strong>of</strong>ac Surg 1994;52:483-6.<br />
25. You ZH, Bell W, Schneiderman E. <strong>Biomechanical</strong> properties <strong>of</strong><br />
small bone screw. J Oral Maxill<strong>of</strong>ac Surg 1994;52:1293-302.<br />
American Journal <strong>of</strong> Orthodontics <strong>and</strong> Dent<strong>of</strong>acial Orthopedics<br />
January 2008<br />
26. Johansson CB, Han CH, Wennerberg A, Albrektsson T. A<br />
quantitative <strong>comparison</strong> <strong>of</strong> machined commercially pure titanium<br />
<strong>and</strong> titanium-aluminum-vanadium implants in rabbit bone.<br />
Int J Oral Maxill<strong>of</strong>ac Implants 1998;13:315-21.<br />
27. Klokkevold PR, Johnson P, Dadgostari S, Caputo A, Davies JE,<br />
Nishimura RD. Early endosseous integration enhanced by dual<br />
acid etching <strong>of</strong> titanium: a torque removal study in the rabbit.<br />
Clin Oral Implants Res 2001;12:350-7.<br />
28. Han CH, Johansson CB, Wennerberg A, Albrektsson T. Quantitative<br />
<strong>and</strong> qualitative investigations <strong>of</strong> surface enlarged titanium <strong>and</strong><br />
titanium alloy implants. Clin Oral Implants Res 1998;9:1-10.<br />
29. Carssion L, Rostlund T, Albrektsson B. Removal torques for<br />
polished <strong>and</strong> rough titanium implants. Int J Oral Maxill<strong>of</strong>ac<br />
Implants 1988;3:21-4.<br />
30. Tjellstrom A, Jacobsson M, Albrektsson T. Removal torque <strong>of</strong><br />
osseointegrated crani<strong>of</strong>acial implants: a clinical study. Int J Oral<br />
Maxill<strong>of</strong>ac Implants 1988;3:287-9.<br />
31. Melsen B, Costa A. Immediate loading <strong>of</strong> implants used for<br />
orthodontic anchorage. Clin Orthod Res 2000;3:23-8.