Premature ejaculation - Keur der Wetenschap
Premature ejaculation - Keur der Wetenschap
Premature ejaculation - Keur der Wetenschap

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Behavioural Brain Research 92 (1998) 111–118<br />
<strong>Premature</strong> <strong>ejaculation</strong> and serotonergic antidepressants-induced delayed<br />
<strong>ejaculation</strong>: the involvement of the serotonergic system<br />
Marcel D. Waldinger a,d, *, Hemmie H.G. Berendsen b , Bertil F.M. Blok c , Berend Olivier d ,<br />
Gert Holstege c<br />
a Department of Psychiatry and Neurosexology, Leyenburg Hospital, Leyweg 275, 2545 CH The Hague, Netherlands<br />
b Department of Neuropharmacology, N.V. Organon, Oss, Netherlands<br />
c Department of Anatomy and Embryology, Faculty of Medicine, Uniersity of Groningen, Groningen, Netherlands<br />
d Department of Psychopharmacology, Rudolf Magnus Institute for Neurosciences, Faculty of Pharmacy, Utrecht Uniersity, Utrecht, Netherlands<br />
Abstract<br />
<strong>Premature</strong> <strong>ejaculation</strong> has generally been consi<strong>der</strong>ed a psychosexual disor<strong>der</strong> with psychogenic aetiology. Although still mainly<br />
treated by behavioural therapy, in recent years double-blind studies have indicated the beneficial effects of some of the<br />
serotonergic antidepressants (SSRIs) in delaying <strong>ejaculation</strong>. We describe here the neurophysiology and the peripheral neuroanatomy<br />
of <strong>ejaculation</strong> and provide a review of the involvement of serotonin in the central nervous system in relation to<br />
serotonergic nuclei and their projections. A hypothesis of the role of 5-HT 1A and 5-HT 2C receptors in premature <strong>ejaculation</strong> is<br />
postulated. © 1998 Elsevier Science B.V. All rights reserved.<br />
Keywords: <strong>Premature</strong> <strong>ejaculation</strong>; Serotonergic antidepressants; Sexual dysfunction<br />
1. Introduction<br />
<strong>Premature</strong> <strong>ejaculation</strong> is defined as a persistent or<br />
recurrent <strong>ejaculation</strong> with minimal sexual stimulation<br />
before, on or shortly after penetration and before the<br />
person wishes it [4]. Generally, premature <strong>ejaculation</strong><br />
was and still is consi<strong>der</strong>ed a psychosexual disturbance<br />
[1,41]. This led to the idea that the main option for<br />
treating premature <strong>ejaculation</strong> were behavioural therapies<br />
such as the stop-start technique [44], the squeeze<br />
technique [33] and other psychotherapeutic interventions<br />
[47]. However, in two longitudinal studies [17,27]<br />
it was shown that the initial positive effects of behavioural<br />
techniques disappear after 3 years.<br />
Pharmacotherapy was also used to delay the <strong>ejaculation</strong><br />
time. Initially, local anesthetic ointments were recommended<br />
[5,16,13], but later case reports and open<br />
trials described the beneficial effects of monoamine-oxi-<br />
* Corresponding author. Tel.: +31 70 3592086; fax: +31 70<br />
3295046.<br />
0166-4328/98/$19.00 © 1998 Elsevier Science B.V. All rights reserved.<br />
PII S0166-4328(97)00183-6<br />
dase inhibitors [6], clomipramine [24,23,43,3,26] and<br />
benzodiazepines [42]. However, the use of pharmacotherapy<br />
was consi<strong>der</strong>ed as ‘only’ suppressive for the<br />
disor<strong>der</strong>. The ‘real’ etiology was still thought to be<br />
psychogenic, which is probably one of the reasons that<br />
a neurobiological view regarding aetiology and pathogenesis<br />
is still lacking.<br />
The beneficial effects of the recently introduced selective<br />
serotonergic re-uptake inhibitor antidepressants<br />
(SSRIs), such as fluoxetine [15,55], paroxetine<br />
[55,52,54], and sertraline [34,55] for treating premature<br />
<strong>ejaculation</strong>, clearly indicates that the classical psychological<br />
view of premature <strong>ejaculation</strong> is no longer tenable<br />
as the only pathogenetic theory. Possibly,<br />
serotonin plays a role in the <strong>ejaculation</strong> process. It<br />
might as well be that genetic factors play a role in the<br />
etiology of premature <strong>ejaculation</strong> [56].<br />
This paper first describes the peripheral nervous<br />
pathways associated with the <strong>ejaculation</strong> process, then<br />
reviews the SSRI-induced ejaculatory retardation and<br />
describes some essential features of the serotonergic
112<br />
system. Finally, it will be postulated which serotonin<br />
receptor subtypes might be involved in premature<br />
<strong>ejaculation</strong>.<br />
2. Neurophysiology and peripheral neuroanatomy of<br />
<strong>ejaculation</strong><br />
Ejaculation occurs in two stages [7]. In the first stage,<br />
the emission phase, sympathetic impulses produce peristaltic<br />
smooth muscle contractions of the epididymis<br />
and vas deferens, moving sperm to the posterior (prostatic)<br />
urethra. At the same time, the seminal vesicles<br />
and prostate contract rhythmically, expelling seminal<br />
and prostatic fluid to mix with sperm. Finally, all these<br />
fluids mix with mucus already secreted by the bulbourethral<br />
glands. The combination of these fluids is<br />
known as semen [46]. The emission is subjectively experienced<br />
as ejaculatory inevitability, because at this point<br />
<strong>ejaculation</strong> cannot be stopped. It is immediately followed<br />
by the second phase, the expulsion or <strong>ejaculation</strong><br />
proper, in which semen is expelled out of the urethra by<br />
rhythmic contractions of pelvic floor muscles.<br />
The (preganglionic) sympathetic nerves, involved in<br />
the emission phase, originate from the intermediolateral<br />
columns of the spinal thoracolumbar cord from T10 to<br />
L2 [32] and travel via the sympathetic chain and hypogastric<br />
nerve (postganglionic) to the pelvic plexus (inferior<br />
hypogastric plexus) or via the sympathetic chain<br />
and pelvic nerve (nervi erigentes) to the pelvic plexus<br />
[18]. From the pelvic plexus the sympathetic nerves are<br />
mediated via the cavernous nerve to the vase deferentia<br />
[18].<br />
During emission the sphincter urethrae internus muscle<br />
(blad<strong>der</strong> neck) contracts by sympathetic influence,<br />
preventing the semen to enter the blad<strong>der</strong> (retrograde<br />
<strong>ejaculation</strong>). The second phase is initiated by pressure<br />
on the wall of the ampullae urethrae by the semen,<br />
giving rise to afferent impulses which reach the S2–S4<br />
sacral cord segments via the pudendal and pelvic nerves<br />
[40]. The expulsion is mediated by motoneurons in the<br />
nucleus of Onuf, which, by way of the pudendal nerve<br />
[45] produce co-ordinated contractions of the bulboand<br />
ischiocavernosus muscles of the pelvic floor. How<br />
the afferent impulses of the urethral wall are relayed to<br />
the motoneurons of Onuf’s nucleus is not known.<br />
The ejaculatory response is triggered by genital and<br />
cortical stimulation. In genital stimulation the afferent<br />
sensory impulses are mediated via touch receptors on<br />
the glans penis, which are connected with sensory fibers<br />
that travel in the dorsal penile and pudendal nerves and<br />
enter the sacral spinal cord. How cortical activation,<br />
such as visual and auditory impulses, reach the <strong>ejaculation</strong><br />
related systems is not known.<br />
M.D. Waldinger et al. / Behaioural Brain Research 92 (1998) 111–118<br />
3. Peripheral serotonin and the central nervous system<br />
The first indication of the presence of serotonin dates<br />
from more than 100 years ago, when a vasoconstrictive<br />
agent in blood was accidentally discovered, which later<br />
appeared to be present in serum. In the 1930s, an agent<br />
(enteramine) was discovered in the gut [20], but it was<br />
not clear whether this agent was the same as that found<br />
in serum. By the end of the 1940s this endogenous<br />
factor was identified. After purification it was called<br />
‘serotonin’ because of its ‘serum tonic’ properties. In<br />
1952, it became clear that serotonin or 5-hydroxytryptamine<br />
(5-HT; [39]) and enteramine were identical<br />
[19].<br />
4. Peripheral serotonin<br />
The majority of 5-HT is found in the enterochromaffin<br />
cells in the gastrointestinal tract, where it accounts<br />
for approximately 80% of total body 5-HT<br />
content [14,21]. In the periphery 5-HT acts as a vasoconstrictor<br />
and pro-aggregator when released from aggregating<br />
platelets, as a neurotransmitter in the enteric<br />
plexuses of the gut and as an autocrine hormone when<br />
released from enterochromaffin cells from the gut, pancreas<br />
and elsewhere [25,21]. Circulating 5-HT does not<br />
enter the brain because it cannot cross the blood–brain<br />
barrier.<br />
5. Serotonin in the central nervous system<br />
After the discovery that 5-HT occurred in the central<br />
nervous system also [51], Woolley and Shaw [57] postulated<br />
in 1954, a central role for 5-HT in psychiatric<br />
disor<strong>der</strong>s, in particular because the 5-HT agonist D-<br />
LSD exerted such a potent psychomimetic action. Reserpine,<br />
a drug given in serious hypertension, was<br />
found to induce a depressive mood. As reserpine induces<br />
an initial release of 5-HT from presynaptic terminals<br />
followed by the ceasing of 5-HT release, a relation<br />
was suggested between low 5-HT levels and depression.<br />
Further research has led to the hypothesis that a deficit<br />
in monoamines (including 5-HT) could lead to depression.<br />
This theory has led to the development of the<br />
selective serotonin re-uptake inhibitors (SSRIs) which<br />
proved to be effective antidepressants. The serotonin<br />
system in the brain was visualized using histochemical<br />
techniques (Falck–Hillarp techniques) in the 1960s.<br />
This relatively primitive localization method was<br />
strongly improved by the development of antibodies<br />
against 5-HT [48] and later still, by autoradiographic<br />
techniques, which made it possible to reveal detailed<br />
5-HT receptor locations.
M.D. Waldinger et al. / Behaioural Brain Research 92 (1998) 111–118 113<br />
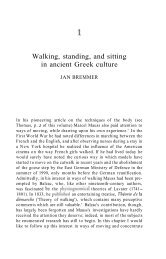
Fig. 1. A schematic representation of a serotonergic neuron and a post-synaptic neuron. All known 5-HT receptors and their putative localization<br />
are depicted (hypothetical).<br />
In 1979, using radioligand binding technology, two<br />
classes of 5-HT receptors in the CNS were shown [38].<br />
This was the start of an era in which a continuous<br />
stream of new 5-HT receptors has been detected.<br />
Presently, at least sixteen different 5-HT receptors have<br />
been found, cloned and the structure described (5-<br />
HT 1A, 5-HT 1B, 5-HT 1D, 5-HT 1D, 5-HT 1E, 5-HT 1F,<br />
5-HT 2A, 5-HT 2B, 5-HT 2C, 5-HT 3, 5-HT 4, 5-HT 5A, 5-<br />
HT 5B, 5-HT 6, 5-HT 7). A schematic representation of<br />
these different 5-HT receptors and their putative locations<br />
are depicted on a cartoon of a 5-HT presynaptic<br />
neuron and a post-synaptic neuron (Fig. 1).<br />
5.1. Serotonergic neurons<br />
Serotonergic cell bodies are present in the brainstem<br />
in the raphe nuclei and adjacent reticular formation<br />
(Fig. 2). There is a clear dichotomy in the 5-HT system<br />
neuronal cell groups. Firstly, a rostral part with cell<br />
bodies in the midbrain and rostral pons projecting to<br />
the forebrain. Secondly, a caudal part with cell bodies<br />
predominantly in the medulla oblongata with important<br />
projections to the spinal cord. Both parts also<br />
project to areas in the brainstem and the cerebellum<br />
[31].<br />
5.2. Rostral and caudal serotonergic cell groups<br />
The rostral part of the 5-HT system consists of the<br />
caudal linear nucleus and the dorsal and median raphe<br />
nuclei. The number of 5-HT cells in the dorsal raphe is<br />
the largest among all raphe nuclei and contains approx-<br />
imately 24 000 in the cat and 165 000 in man [50].<br />
Besides the raphe nuclei, a number of 5-HT neurons are<br />
present in the adjoining reticular formation of pons and<br />
midbrain. The caudal system contains the nuclei raphe<br />
magnus, pallidus and obscurus and some in the adjoining<br />
medullary reticular formation, solitary nucleus and<br />
the area of the nucleus (sub)coeruleus.<br />
5.3. Projections of the serotonergic cell groups<br />
5.3.1. Ascending projections<br />
The ascending 5-HT system consists of two more or<br />
less parallel projection pathways, presumably with different<br />
functions [50].<br />
The first system is called ‘Basket-axon’ system and<br />
originates in the median raphe nucleus. It has thick<br />
fibers (M-fibers) that branch into short, thin fibers and<br />
form large, round boutons (varicosities) with extensive<br />
synaptic contacts. These beaded axons often intensively<br />
embranch certain cortical cells (baskets) and form classical<br />
synaptic contacts.<br />
The second system originates in the dorsal raphe<br />
nucleus. It has thin fibers (D-fibers) with many spindlesized<br />
varicosities. These fibers branch extensively and<br />
diffusely and contain small fusiform boutons. However,<br />
these boutons do not seem to contain real synaptic<br />
structures.<br />
Both systems (M- and D-fibers) can be found together<br />
in most brain areas, but to a different extent.<br />
The cerebral cortex is the area where both systems<br />
co-exist extensively, whereas the striatum almost exclusively<br />
receives fine varicose D-fibers and the gyrus
114<br />
M.D. Waldinger et al. / Behaioural Brain Research 92 (1998) 111–118<br />
Fig. 2. A longitudinal view of rat brain with a schematic representation of the localization of the serotonergic cell bodies in the raphe nuclei and<br />
in the brain stem reticular formation and the corresponding classification into the B-groups and their projections. CB, cerebellum; mfb, medial<br />
forebrain bundle, CC, corpus callosum; OB, olfactory bulb; Cpu, caudate putamen; OC, optic chiasma; GP, globus pallidus; OT, olfactory<br />
tubercle; H, hypothalamus; Pit, pituitary gland; Hip, hippocampal region; Sc, superior colliculus; lc, locus coeruleus; SN, substantia nigra; LS,<br />
lateral septal nucleus; T, thalamus; MM, medial mammilary nucleus; V, ventrikel. For the 5-HT cell cluster, the 5-HT cells in structure<br />
(classification into the rostral (r) and caudal (c) serotonergic system according to Tork (1991) are as follows: B1, raphe pallidus nucleus (c), caudal<br />
ventrolateral medulla (c); B2, raphe obscurus nucleus (c); B3, raphe magnus nucleus (c), rostral ventrolateral medulla (c), lateral paragigantocellular<br />
reticular nucleus (c); B4, raphe obscurus, dorsolateral part (c); B5, median raphe nucleus, caudal part (r); B6, dorsal raphe nucleus, caudal<br />
part (r); B7, dorsal raphe nucleus, rostral part (r); B8, Median raphe nucleus, rostral part (r); caudal linear nucleus (r); B7, nucleus pontis oralis<br />
(r); B9, Nucleus pontis oralis (r); Supralemniscal region (r).<br />
dentatus primarily thick M-fibers. The functional role<br />
of these two 5-HT systems is rather unclear, although<br />
they display a differential sensitivity for certain substituted<br />
amphetamines like MDMA [37]. Such drugs destroy<br />
the fine varicose system but leave the thick,<br />
beaded system intact.<br />
5.3.2. Descending projections<br />
The caudal raphe nuclei project to the caudal brain<br />
stem and spinal cord. The raphe magnus nucleus predominantly<br />
projects to the dorsal horn and the nuclei<br />
raphe pallidus and obscurus to the ventral horn, intermediate<br />
zone and the intermediolateral cell column<br />
(IML) of the thoracolumbar and sacral spinal cord.<br />
The latter areas contain preganglionic sympathetic and<br />
parasympathetic motoneurons, respectively.<br />
5.3.3. Afferents of the caudal serotonergic raphe nuclei<br />
The afferents of the caudal raphe nuclei originate<br />
largely from medial structures in the so called limbic<br />
system. The most important are the mesencephalic periaqueductal<br />
grey and medial cell groups in hypothalamus<br />
and pre-optic area [28].<br />
5.3.4. Regulation<br />
Serotonergic neurons have various mechanisms to<br />
regulate their own activity, viz. somatodendritic autoreceptors<br />
(5-HT 1A receptors), presynaptic autoreceptors<br />
(5-HT 1B/1D receptors) and the 5-HT re-uptake process<br />
(5-HT transporter).<br />
5.3.4.1. Somatodendritic (5-HT 1A) autoreceptors. The<br />
5-HT 1A autoreceptors are present in high densities on<br />
the cell bodies and dendrites of serotonergic neurons in<br />
the raphe nuclei (Fig. 3). Upon activation of these<br />
receptors, the firing rate of the 5-HT neuron decreases.<br />
Un<strong>der</strong> normal physiological conditions endogenous 5-<br />
HT activates this 5-HT 1A autoreceptor. It is as yet not<br />
clear from where this endogenous 5-HT originates, but<br />
it is assumed that it <strong>der</strong>ives from somatodendritic release,<br />
which differs from synaptic release. Application<br />
of the selective 5-HT 1A receptor agonists (i.e. 8-OH-<br />
DPAT or flesinoxan) either systemically or locally in<br />
the raphe nuclei, inhibits the release of 5-HT in the<br />
synaptic cleft.<br />
5.3.4.2. 5-HT 1B/1D autoreceptors. This pre-synaptic receptor<br />
inhibits, after activation, the 5-HT release into<br />
the synaptic cleft. The 5-HT 1B/1D receptor is coupled to<br />
an inhibitory (GI-protein) transaction mechanism that<br />
apparently blocks the release of 5-HT from the synaptic<br />
vesicles in an as yet not un<strong>der</strong>stood manner. This<br />
feedback mechanism of the cell, where the released<br />
5-HT inhibits its own release, is a frequently occurring<br />
principle in neurotransmitter regulation and provides<br />
the system with the possibility to prevent overstimulation<br />
of (post)synaptic receptors.<br />
5.3.4.3. 5-HT re-uptake. If 5-HT is released into the<br />
synaptic cleft it should be removed again as fast as<br />
possible to prevent overstimulation of the<br />
(post)synaptic receptors (desensitization). The 5-HT<br />
neuron, therefore, possesses large quantities of 5-HT<br />
transporters (5-HTT), not only on the synaptic endings<br />
but also on the cell bodies and dendrites of serotonergic<br />
neurons. Apart from this 5-HT cell system, glial cells<br />
have also a transport system which presumably contributes<br />
to the remove of released 5-HT. After blockade<br />
of the 5-HT transporters via selective serotonin re-uptake<br />
inhibitors (SSRIs), the synaptic 5-HT increases,
M.D. Waldinger et al. / Behaioural Brain Research 92 (1998) 111–118 115<br />
Fig. 3. Schematic representation of acute and chronic activation SSRI administration and the effect on the 5-HT 1A autoreceptor.<br />
although this process is counteracted by activation of<br />
5-HT 1A autoreceptors, which are stimulated by enhanced<br />
5-HT and inhibit the 5-HT release.<br />
5.3.4.4. Acute and chronic administration of SSRIs. After<br />
acute administration of an SSRI all 5-HT transporters<br />
are blocked. This leads to high 5-HT levels in<br />
the extracellular space around the 5-HT cell bodies in<br />
the raphe nuclei, leading to activation of 5-HT 1A autoreceptors<br />
and thus to a decrease in the firing frequency<br />
of the cell and a decreased release of 5-HT in<br />
the synaptic cleft. This decreased release is (completely<br />
or partially) compensated by blockade of the<br />
5-HT re-uptake in the synaptic cleft. The net effect in<br />
the synaptic cleft is difficult to predict, both an increase<br />
in or lack of effect have been observed. If a<br />
post-synaptic increase occurs, activation of the presynaptic<br />
5-HT 1B/1D autoreceptor will further dampen<br />
the release process. In general, acute administration of<br />
SSRIs will presumably lead to a mild increase of 5-<br />
HT neurotransmission leading to some stimulation of<br />
all post-synaptic 5-HT receptors.<br />
After chronic administration a number of adaptive<br />
processes may play a role, although much is still quite<br />
speculative. Because the 5-HTTs are chronically<br />
blocked, a chronically enhanced level of 5-HT is<br />
present at somatodendritic level. This leads to desensitization<br />
of the 5-HT 1A receptors and consequently to<br />
lesser (or no) inhibition of the cell firing of the 5-HT<br />
neuron, leading to higher 5-HT release. Simultaneously,<br />
also the synaptic 5-HTTs are chronically<br />
blocked which means, together with the enhanced re-<br />
lease of 5-HT, to strongly enhanced synaptic levels of<br />
5-HT. It is possible, although not fully elucidated yet,<br />
that the 5-HT 1B/1D autoreceptors also desensitize,<br />
which might contribute to the process of enhanced<br />
5-HT neurotransmission. The net effect of chronic<br />
SSRI administration is thus a strongly enhanced 5-HT<br />
neurotransmission. Apparently, activation of one (or<br />
more) of the post-synaptic 5-HT receptors, contributes<br />
to the antidepressant and anxiolytic effects of the SS-<br />
RIs.<br />
6. <strong>Premature</strong> <strong>ejaculation</strong> and 5-HT<br />
Some of the SSRIs appear effective in inhibiting the<br />
premature <strong>ejaculation</strong> both after acute and chronic<br />
administration [55,52,54,53] whereas their antidepressant<br />
and anxiolytic effects only gradually emerge over<br />
time. This remarkably rapid onset is not well un<strong>der</strong>stood.<br />
It is suggested that acute blockade of 5-HT<br />
re-uptake enhances 5-HT transmission into the<br />
synapse. These acute synaptic effects occur within<br />
hours of administering antidepressant SSRIs. Since<br />
the rapid onset of postponement of <strong>ejaculation</strong> by<br />
SSRIs has a similar time course as the synaptic effects<br />
it is suggested that the postponement of <strong>ejaculation</strong> is<br />
mediated by the acutely enhanced 5-HT neurotransmission.<br />
Apart from their rapid onset of action, the question<br />
remains why SSRIs, such as paroxetine [55,52,54],<br />
fluoxetine [55], sertraline [34,55] and to a lesser extent<br />
also fluvoxamine [55] delay <strong>ejaculation</strong> time. Human<br />
<strong>ejaculation</strong> is peripherally activated by 1-noradrener-
116<br />
gic nerve stimulation. Since paroxetine has no sympatholytic<br />
effects, it is suggested that the effect of paroxetine<br />
on the delay of <strong>ejaculation</strong> is on the central<br />
nervous system.<br />
The involvement of the central serotonergic neurotransmission<br />
in human <strong>ejaculation</strong> has been investigated<br />
in animal studies. Induction of penile erections<br />
in rats and rhesus monkeys showed that responses<br />
due to SSRI treatment are identical to those seen<br />
after selective activation of 5-HT 2C receptors [49,8,12]<br />
and are different from the responses seen after 5-<br />
HT 1A and 5-HT 2A receptor stimulation [58,11,36,30].<br />
Moreover, a cross familiarization study showed that<br />
the drug stimuli of the SSRI’s fluoxetine and paroxetine<br />
most resemble those of a 5-HT 2C-receptor agonist<br />
[10]. Apparently, it seems that the responses from<br />
SSRI treatment in these animals are due to 5-HT 2C<br />
receptor activation [12,49]. Since paroxetine treatment<br />
results in <strong>ejaculation</strong> retardation, it is suggested that<br />
in humans premature <strong>ejaculation</strong> is caused by hyposensitivity<br />
of 5-HT 2C receptors. Such a concept<br />
would correspond with the results of rat studies in<br />
which the 5-HT receptor agonists D-LSD (D-lysergic<br />
acid diethylamide) and quipazine increase the <strong>ejaculation</strong><br />
latency [2]. Furthermore, DOI (2,5-dimethoxy-4iodophenyl-2-aminopropane)<br />
which equally stimulates<br />
5-HT 2A and 5-HT 2C receptors, also increases the <strong>ejaculation</strong><br />
latency [22], while the selective 5-HT 2A receptor<br />
agonist DOM (2,5-dimethoxy-4-methylamphetamine)<br />
does not have this effect [2].<br />
In male rats also another 5-HT subtype receptor<br />
seems to be involved in the <strong>ejaculation</strong> process. Activation<br />
of 5-HT 1A receptors by the selective 5-HT 1A<br />
receptor agonist 8-OH-DPAT (8-hydroxy-2-(di-npropylaminotetralin)<br />
shortens the <strong>ejaculation</strong> latency<br />
time and reduces the number of intermissions preceding<br />
<strong>ejaculation</strong> in animals [2]. The behavioral response<br />
to activation of 5-HT 1A receptors is attenuated or<br />
completely blocked by co-activation of 5-HT 2C receptors<br />
indicating that functional interactions between<br />
these receptors exists [9]. Extrapolating these findings<br />
from animal research to human premature <strong>ejaculation</strong><br />
one might speculate that premature <strong>ejaculation</strong> may<br />
be caused by the hypersensitive 5-HT 1A receptor.<br />
Treatment of premature <strong>ejaculation</strong> by an SSRI will<br />
then induce activation of the 5-HT 2C receptor and<br />
consequently decrease the function of the 5-HT 1A receptor<br />
or restore the balance between 5-HT 1A and<br />
5-HT 2C receptor function, resulting in an overall delay<br />
of <strong>ejaculation</strong>.<br />
However, the identification of which specific 5-HT<br />
receptor subtypes are involved in the human <strong>ejaculation</strong><br />
process is only possible by administration of subtype<br />
selective 5-HT ligands in patients with premature<br />
<strong>ejaculation</strong>. Unfortunately, these agents are not yet<br />
available for human use.<br />
M.D. Waldinger et al. / Behaioural Brain Research 92 (1998) 111–118<br />
7. SSRIs and their neurophysiological substrates of<br />
sexual side effects<br />
Although it is well known that SSRIs have sexual<br />
side effects in humans, such as retardation of <strong>ejaculation</strong><br />
and anorgasmia [35], the neural substrates involved<br />
in these effects are unknown. The bulk of<br />
psychopharmacological studies using SSRIs for depression,<br />
anxiety disor<strong>der</strong>s or the obsessive-compulsive<br />
disor<strong>der</strong> have investigated their effects on serotonergic<br />
neurons and their projections to cortical and subcortical<br />
structures. However, studying sexual effects of SS-<br />
RIs, such as their effect on <strong>ejaculation</strong>, necessitates<br />
studies not only on cortical and subcortical functions,<br />
but also on brainstem functions, spinal cord mechanisms<br />
and the peripheral nervous system.<br />
The recent description of the emotional motor system<br />
(EMS) by Holstege [28,29] might represent a neuroanatomical<br />
substrate for the emotional influences on<br />
basic neurogenital pathways. Further research into the<br />
relationship between the central serotonergic system<br />
and the EMS might illuminate the speculative idea<br />
that a threshold for <strong>ejaculation</strong> is set and modulated<br />
somewhere in the central nervous system and can be<br />
changed by SSRI treatment.<br />
References<br />
[1] Abraham K. Uber ejaculatio praecox, Zeitschr. f. ärztl. Psychoanalyse<br />
1917;IV:171–86.<br />
[2] Ahlenius S, Larsson K, Svensson L, Hjorth S, Carlsson A,<br />
Lindberg P, Wilkstrom H, Sanchez D, Arvidsson LE, Hacksell<br />
U, Nilsson JL. Effects of a new type of 5-HT receptor agonist on<br />
male rat sexual behavior. Pharmacol Biochem Behav<br />
1981;15:785–92.<br />
[3] Althof SE, Levine SB, Corty EW, Risen CB, Stern EB, Kurit<br />
DM. A double-blind crossover trial of clomipramine for rapid<br />
<strong>ejaculation</strong> in 15 couples. J Clin Psychiatry 1995;56:402–7.<br />
[4] American Psychiatric Association, Diagnostic and Statistical<br />
Manual of Mental Disor<strong>der</strong>s, 4th ed., Washington, DC: American<br />
Psychiatric Association, 1994.<br />
[5] Aycock L. The medical management of premature <strong>ejaculation</strong>. J<br />
Urol 1949;62:361–2.<br />
[6] Bennett D. Treatment of ejaculatio praecox with monoamine-oxidase<br />
inhibitors (letter). Lancet 1961;II:1309.<br />
[7] Benson G. Male sexual function: erection, emission and <strong>ejaculation</strong>.<br />
In: Knobil E, Neill JD, editors. The Physiology of Reproduction.<br />
New York: Raven Press, 1988.<br />
[8] Berendsen HHG, Broekkamp CLE. Drug-induced penile erections<br />
in rats: indications of serotonin 1B receptor mediation. Eur<br />
J Pharmacol 1987;338:191–5.<br />
[9] Berendsen HHG, Broekkamp CLE. Behavioural evidence for<br />
functional interactions between 5-HT-receptor subtypes in rats<br />
and mice. Br J Pharmacol 1990;101:667–73.<br />
[10] Berendsen HHG, Broekkamp CLE. Comparison of stimulus<br />
properties of fluoxetine and 5-HT receptor agonists in a conditioned<br />
taste aversion procedure. Eur J Pharmacol 1994;253:83–<br />
9.<br />
[11] Berendsen HHG, Jenck F, Broekkamp CLE. Selective activation<br />
of 5-HT 1A receptors induces lower lip retraction in the rat.<br />
Pharmacol Biochem Behav 1989;33:821–7.
[12] Berendsen HHG, Jenck F, Broekkamp CLE. Involvement of<br />
5-HT 1C-receptors in drug-induced penile erections in rats. Psychopharmacology<br />
1990;101:57–61.<br />
[13] Berkovitch M, Keresteci AG, Koren G. Efficacy of prilocainelidocaine<br />
cream in the treatment of premature <strong>ejaculation</strong>. J<br />
Urol 1995;154:1360–1.<br />
[14] Bertacinni G, Chieppa S. Urinary excretion of 5-hydroxyindoleacetic<br />
acid after removal of the large intestine in man.<br />
Lancet 1960;1:881.<br />
[15] Crenshaw R, Prozac and <strong>Premature</strong> Ejaculation, Annual Meeting<br />
of the American Association of Sex Educators, Counselors<br />
and Therapists, Orlando, FL, 1992.<br />
[16] Damrau F. <strong>Premature</strong> <strong>ejaculation</strong>: use of ethyl aminobenzoate<br />
to prolong coitus. J Urol 1963;89:936–9.<br />
[17] DeAmicis LA, Goldberg DC, LoPiccolo J, Friedman J, Davies<br />
L. Clinical follow-up of couples treated for sexual dysfunction.<br />
Arch Sexual Behav 1985;14:467–89.<br />
[18] de Groat WC, Steers WD. Autonomic regulation of the urinary<br />
blad<strong>der</strong> and sexual organs. In: Loewy AD, Spyer KM,<br />
editors. Central Regulation of Autonomic Functions. Oxford:<br />
Oxford University Press, 1990:310–33.<br />
[19] Erspamer V. Asero, Identification of enteramin, the specific<br />
hormone of the enterochromaffin cell system. Nature<br />
1952;169:800–1.<br />
[20] Erspamer V. Pharmakologische studien uber enteramin; einige<br />
Eigenschaften des enteramins, sowie uber die abgrenzung des<br />
enteramins von den an<strong>der</strong>en kreislauf wirksamen gewebsprodukten.<br />
Arch f Exp Path Pharmacol 1940;196:336–90.<br />
[21] Farthing MJG. 5-Hydroxytryptamine and 5-hydroxytryptamine-3<br />
receptor antagonists. Scand J Gastroenterol<br />
1991;26:92–100.<br />
[22] Foreman MM, Hall JL, Love RL. The role of the 5-HT 2<br />
receptor in the regulation of sexual performance of male rats.<br />
Life Sci 1989;45:1263–70.<br />
[23] Girgis SM, El-Haggen S, El-Hermouzy SA. A double-blind<br />
trial of clomipramine in premature <strong>ejaculation</strong>. Andrologia<br />
1982;29:364–8.<br />
[24] Goodman RE. An assessment of clomipramine (Anafranil) in<br />
the treatment of premature <strong>ejaculation</strong>. J Int Med Res<br />
1980;8(S3):53–9.<br />
[25] Grahame-Smith DG. Serotonin (5-hydroxytryptamine, 5-HT).<br />
Q J Med 1988;67:459–66.<br />
[26] Haensel SM, Rowland DL, Kallan KTHK, Slob AK.<br />
Clomipramine and sexual function in men with premature <strong>ejaculation</strong><br />
and controls. J Urol 1996;156:1310–5.<br />
[27] Hawton K, Catalan J, Martin P, Fagg J. Long-term outcome<br />
of sex therapy. Behav Res Ther 1986;24:665–75.<br />
[28] Holstege G. Descending motor pathways and the spinal motor<br />
system: limbic and non-limbic components. Progr Brain Res<br />
1991;87:307–412.<br />
[29] Holstege JC. The ventro-medial medullary projections to spinal<br />
motoneurons: ultrastructure, transmitters and functional aspects.<br />
In: Holstege G, Bandler R, Saper C, editors. The Emotional<br />
Motor System. Progr Brain Res, vol. 107. Amsterdam:<br />
Elsevier, 1996:159–82.<br />
[30] Hoyer D, Clarke DE, Fozard JR, Hartig PR, Martin EJ,<br />
Mylecharane PR, Saxena PR, Humphrey PPA. International<br />
Union of Pharmacology classification of receptors for 5-hydroxytryptamine<br />
(serotonin). Pharmacol Rev 1994;46:157.<br />
[31] Jacobs BL, Azmitia EC. Structure and function of the brain<br />
serotonin system. Physiol Rev 1992;72:165–229.<br />
[32] Marberger H. The mechanisms of <strong>ejaculation</strong>. In: Coutinho<br />
EM, Fuchs F, editors. Physiology and Genetics of Reproduction;<br />
Basic Life Sciences, vol. 4. New York: Plenum Press,<br />
1974.<br />
M.D. Waldinger et al. / Behaioural Brain Research 92 (1998) 111–118 117<br />
[33] Masters WH, Johnson VE. <strong>Premature</strong> <strong>ejaculation</strong>. In: Masters<br />
WH, Johnson VE, editors. Human Sexual Inadequacy. Boston,<br />
MA: Little, Brown and Co., 1970:92–115.<br />
[34] Mendels J, Camera A, Sikes C. Sertraline treatment for premature<br />
<strong>ejaculation</strong>. J Clin Psychopharmacol 1995;15:341–6.<br />
[35] Meston CM, Gorzalka BB. Psychoactive drugs and human<br />
sexual behavior: The role of serotonergic activity. J Psychoactive<br />
Drugs 1992;24:1–40.<br />
[36] Molewijk HE, van <strong>der</strong> Heyden JAM, Olivier B. Lower lip<br />
retraction is selectively mediated by activation of the 5-HT1A<br />
receptor. Eur J Neurosci 1989;214(2):121–36.<br />
[37] Molliver ME, Berger UV, Mamounas LA, Molliver DC,<br />
O’Hearn E, Wilson MA. Neurotoxicity of MDMA and related<br />
compounds: anatomical studies. Ann NY Acad Sci<br />
1990;600:640–64.<br />
[38] Peroutka SJ, Sny<strong>der</strong> SH. Multiple serotonin receptors: differential<br />
binding of [ 3 H]5-hydroxytryptamine, [ 3 H]lysergic acid diethylamide<br />
and [ 3 H]spiroperidol. Mol Pharmacol<br />
1979;16:687–99.<br />
[39] Rapport MM. Serum vasoconstrictor (serotonin) V. Presence<br />
of creatinine in the complex. A proposed structure of the vasoconstrictor<br />
principle. J Biol Chem 1949;180:961–9.<br />
[40] Retief PJM. Physiology of micturition and <strong>ejaculation</strong>. S Afr<br />
Med J 1950;24:509.<br />
[41] Ruff GA, St Lawrence JS. <strong>Premature</strong> <strong>ejaculation</strong>: past research<br />
progress, future directions. Clin Psychol Rev 1985;5:627–39.<br />
[42] Segraves RT. Treatment of premature <strong>ejaculation</strong> with Lorazepam.<br />
Am J Psychiatry 1987;144:1240.<br />
[43] Segraves RT, Saran A, Segraves K, Maguire E. Clomipramine<br />
versus placebo in the treatment of premature <strong>ejaculation</strong>: a<br />
pilot study. J Sex Marital Ther 1993;19:198–200.<br />
[44] Semans JH. <strong>Premature</strong> <strong>ejaculation</strong>: a new approach. S Afr<br />
Med J 1956;49:353.<br />
[45] Semans JH, Langworthy OR. Observations on the neorophysiology<br />
of sexual function in the male cat. J Urol 1938;40:836.<br />
[46] Singer C, Weiner WJ. Male sexual response cycle. In: Singer<br />
CS, Weiner WJ, editors. Sexual Dysfunction, a Neuro-Medical<br />
Approach. Armonk: Futura, 1994:30–1.<br />
[47] St. Lawrence JS, Madakasira S. Evaluation and treatment of<br />
premature <strong>ejaculation</strong>: a critical review. Int J Psychiatry Med<br />
1992;22:77–97.<br />
[48] Steinbush HWM. Distribution of serotonin-immunoreactivity<br />
in the central nervous system of the rat-cell bodies and terminals.<br />
Neuroscience 1981;4:557–618.<br />
[49] Szele FG, Murphy DL, Garrick NA. Effects of fenfluramine,<br />
m-chlorophenylpiperazine and other serotonin-related agonists<br />
and antagonists on penile erections in non-human primates.<br />
Life Sci 1988;43:1297–303.<br />
[50] Tork I. Anatomy of the serotonergic system. Ann NY Acad<br />
Sci 1990;600:6–35.<br />
[51] Twarag BM, Page IH. Serotonin content of some mammalian<br />
tissues and urine and a method for its determination. Am J<br />
Physiol 1953;174:157–61.<br />
[52] Waldinger MD, Hengeveld MW, Zwin<strong>der</strong>man AH. Paroxetine<br />
treatment of premature <strong>ejaculation</strong>: a double-blind, randomized,<br />
placebo-controlled study. Am J Psychiatry 1994;151:<br />
1377–9.<br />
[53] Waldinger MD, Hengeveld MW, Zwin<strong>der</strong>man AH, Olivier B.<br />
An empirical operationalization study of the DSM-IV Diagnostic<br />
Criteria for <strong>Premature</strong> Ejaculation, 1997 (submitted).<br />
[54] Waldinger MD, Hengeveld MW, Zwin<strong>der</strong>man AH. Ejaculation-retarding<br />
properties of paroxetine in patients with primary<br />
premature <strong>ejaculation</strong>: a double-blind, randomized, dose-response<br />
study. Br J Urol 1997;79:592–5.
118<br />
[55] Waldinger MD, Hengeveld MW, Zwin<strong>der</strong>man AH, Olivier B.<br />
The effect of SSRI antidepressants on <strong>ejaculation</strong>: a doubleblind,<br />
randomised, placebo-controlled study with fluoxetine,<br />
fluvoxamine, paroxetine and sertraline. J Clin Psychopharmacol<br />
1997 (in press).<br />
[56] Waldinger MD, Rietschel M, Nothen NM, Hengeveld MW,<br />
Olivier B. Familial occurrence of primary premature <strong>ejaculation</strong>.<br />
M.D. Waldinger et al. / Behaioural Brain Research 92 (1998) 111–118<br />
.<br />
Psychiatr Genet 1997 (in press).<br />
[57] Woolley DW, Shaw E. A biochemical and pharmacological<br />
suggestion about certain mental-disor<strong>der</strong>s. Proc Natl Acad Sci<br />
1954;40:228–31.<br />
[58] Yap CY, Taylor DA. Involvement of 5-HT2 receptors in the<br />
wetdog shake behaviour induced by 5-hydroxytryptophan in the<br />
rat. Neuropharmacology 1983;22:801–4.