Gonozyme
Gonozyme
Gonozyme

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
J0^^!\<br />
vgfp^v<br />
Principles and methods<br />
CRITICAL REVIEW<br />
Anthony J. Barletta, M.D.<br />
January, 1985<br />
<strong>Gonozyme</strong>"<br />
<strong>Gonozyme</strong>1" (Abbott Laboratories) is a solid-phase enzyme immunoassay (EIA) for<br />
the rapid detection of gonococcal antigens in clinical specimens. In this system, a<br />
specially treated polystyrene bead adsorbs gonococcal antigen present in the test<br />
solution. The bead is washed to remove unbound material, incubated first with<br />
rabbit antibody to Neisseria gonorrhoeae, and subsequently with goat anti-rabbit<br />
serum antibody which is conjugated to horseradish peroxidase. The presence of this<br />
enzyme on the bead surface is detected by a final incubation of the washed bead<br />
with a peroxidase substrate (O-phenylenediamine containing hydrogen peroxide). If<br />
the specimen is positive, a yellow-orange color reaction occurs. The intensity of the<br />
color reaction is quantitated with a spectrophotometer (measured optical density at<br />
492 nm) and is proportional to the quantity of gonococcal antigen adsorbed by the<br />
bead. The mean absorbance of three negative controls plus 0.190 is the<br />
recommended cutoff of positivity (2).<br />
Summary of clinical evaluations<br />
Several clinical evaluations of this assay have been published in the recent literature<br />
(see references). These compare <strong>Gonozyme</strong> results with those of standard culture<br />
techniques and/or direct microscopy of Gram-stained smears, utilizing the<br />
percentage of positive cultures as an estimate of gonococcal disease prevalence.<br />
The available data indicate that the <strong>Gonozyme</strong>1" assay is capable of rapidly<br />
detecting gonococcal antigen in urethral and endocervical swab specimens as was<br />
intended by the manufacturer, although some results indicate lower sensitivity,<br />
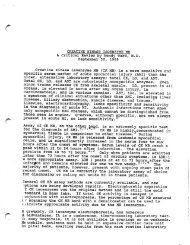
specificity, and predictive values than were initially obtained (Table I). In general,<br />
the reported sensitivity and specificity of EIA are comparable to those of the Gram<br />
stain in males, whereas in females EIA appears more sensitive though less specific<br />
than Gram stain (1,3,6,13,16,18,20).<br />
Technical advantages and limitations<br />
Numerous selective culture media and transport systems have been developed for<br />
the isolation of gonococci. When a single swab specimen is collected, cultures can<br />
optimally detect close to 95% of male urethral infections and 85% of female<br />
cervical infections (4). Available culture techniques have several drawbacks<br />
including: 1) loss of viability of gonococci under suboptimal transport or growth<br />
conditions, 2) inability to grow the organisms after initiation of antibiotic therapy,<br />
3) failure to culture vancomycin-sensitive strains or other strains with fastidious<br />
growth characteristics, and 4) a time requirement of up to 2 to 3 days before results<br />
are available (4).
Page 2<br />
EIA systems are theoretically not affected by sensitivity of gonococci to<br />
vancomycin or loss of viability in specimen transport. Organisms are rendered non<br />
viable by the specimen preservative and dilution buffer included in the test kit.<br />
This, however, precludes susceptibility testing and the identification of<br />
penicillinase-producing gonococci if EIA is utilized as the sole diagnostic test.<br />
Infections with small numbers of organisms may yield false negative results, and<br />
there is at least a theoretical potential for false positive results in evaluating<br />
patients for test of cure after therapy, due to detection of non-viable organisms.<br />
<strong>Gonozyme</strong> has not yet been evaluated with pharyngeal or rectal specimens. Crossreacting<br />
antigens from other Neisseria species and enteric organisms may pose<br />
problems for its usefulness in evaluating specimens from these sites (3,21). Calcium<br />
alginate or dacron swabs should not be used for collecting EIA specimens (2).<br />
Does the <strong>Gonozyme</strong> EIA improve upon current diagnostic methods?<br />
For males with urethritis, the Gram stain remains an inexpensive technique<br />
providing rapid, accurate results when performed by experienced personnel (3,20).<br />
In a hypothetical cost-benefit analysis, it seems difficult to justify substituting<br />
<strong>Gonozyme</strong> for routine screening or first evaluation of symptomatic males. In<br />
asymptomatic males the sensitivity of the Gram stain drops to 40-60% compared<br />
with culture (8). In this group <strong>Gonozyme</strong> would be of greater potential value,<br />
r especially when specimens require transport to a referral laboratory. Note however<br />
that the test's sensitivity and positive predictive value in Stamm's series are lowest<br />
(67 and 30% respectively) in men without urethral discharge in whom the prevalence<br />
of disease was only 2% (20). This is in keeping with Bayes Theorem stating that<br />
without perfect specificity, the predictive value of a positive test declines rapidly<br />
with decreasing prevalence of disease in the test population.<br />
Patients with asymptomatic gonorrhea presumably have fewer gonococci and hence<br />
less antigen per swab. Loss of antigen in preparing Gram-stain smears and streaking<br />
cultures plates prior to antigen assay may be a factor in reducing sensitivity of the<br />
test in patients with few organisms to begin with. Along these lines, Schachter et<br />
al. have demonstrated significant decreases in EIA sensitivity with multiple uses of<br />
the same swab prior to inoculating the <strong>Gonozyme</strong> transport medium, and<br />
recommends use of separate swabs for Gram-stains or cultural duplication (18).<br />
In women with cervical gonorrhea diagnosis is confounded by the non-specific signs<br />
and symptoms of infection and the relatively poor sensitivity of cervical Gram-stain<br />
(approximately 42%) (3). A rapid diagnostic test more sensitive than the Gram-stain<br />
would be of particular value in females who are at greatest risk of complication<br />
from delayed therapy. In a recent study conducted at a sexually transmitted disease<br />
clinic, 7.3% of women with gonococcal cervicitis not treated at the first visit<br />
developed pelvic inflammatory disease before the followup visit after a mean<br />
interval of 7 days (11).<br />
Although more sensitive, EIA is not equivalent in speed or cost to the Gram stain —<br />
^^ the assay takes approximately one hour and would likely be performed in batches<br />
f^ once or twice daily. The reported sensitivity of <strong>Gonozyme</strong> in detecting cervical
n<br />
Page 3<br />
gonorrhea in some series seems unacceptably low for screening high risk populations<br />
such as those encountered in sexually transmitted disease clinics. The available<br />
data also indicate that the <strong>Gonozyme</strong> assay lacks sufficient positive predictive<br />
value to replace culture as the definitive diagnostic test in female populations with<br />
a low disease prevalence.<br />
A positive <strong>Gonozyme</strong> assay is considered sufficient evidence of gonorrhea in males,<br />
and is as accurate as a Gram-stain. As stated by the manufacturer, however,<br />
positive <strong>Gonozyme</strong> results in females should be regarded only as presumptive and<br />
confirmed by appropriate methods (2).<br />
References<br />
1. Aardoom HA, DeHoop D, Iserief COA, et al.: Detection of Neisseria<br />
gonorrhoeae antigen by a solid-phase enzyme immunoassay. Br J Vener Dis<br />
58:359-362, 1982.<br />
2. Abbott Laboratories, North Chicago, Illinois: <strong>Gonozyme</strong> Diagnostic Kit:<br />
Enzyme immunoassay for the detection of Neisseria gonorrhoeae in urogenital<br />
swab specimens (package insert). September 1983.<br />
3. Burns M, Rossi PH, Cox DW, et al.: A preliminary evaluation of the<br />
<strong>Gonozyme</strong> test. Sex Transm Dis 10:180-183, 1983.<br />
4. Carlson BL, Haley MS, Tisei NA, McCormack WM: Evaluation of four methods<br />
for isolation of Neisseria gonorrhoeae. J Clin Microbiol 12:301-303, 1980.<br />
5. Dans PE, Rothenberg R, Holmes KK: Gonococcal serology: how soon, how<br />
useful, and how much? J Infect Dis 135:330-334, 1977.<br />
6. Danielsson D, Moi H, Forslin L: Diagnosis of urogenital gonorrhea by<br />
detecting gonococcal antigen with a solid phase enzyme immunoassay<br />
(<strong>Gonozyme</strong>). J Clin Pathol 36:674-677, 1983.<br />
7. Demetriou E, Sackett R, Welch DF, Kaplan DW: Evaluation of an enzyme<br />
immunoassay for detection of Neisseria gonorrhoeae in an adolescent<br />
population. JAMA 252:247-250, 1984.<br />
8. Handsfield HH, Lipman JP, Harnisch E, et al.: Asymptomatic gonorrhea in<br />
men. Diagnosis, natural course, prevalence and significance. N Engl J Med<br />
290:117-123, 1974.<br />
9. Judson FN: A clinic-based system for monitoring the quality of techniques for<br />
the diagnosis of gonorrhea. Sex Transm Dis 5:141-145, 1978.<br />
10. Judson FN, Maltz AB: A rational basis for the epidemiologic treatment of<br />
gonorrhea in a clinic for sexually transmitted diseases. Sex Transm Dis<br />
5:89-92, 1978.
Page 4<br />
11. Lossick JG, Smeltzer MP, Curran JW: The value of the cervical Gram stain in<br />
the diagnosis and treatment of gonorrhea in women in a venereal disease<br />
clinic. Sex Transm Dis 9:124-127, 1982.<br />
12. Martin R, Wentworth BB, Coopes S, Larson EH: Comparison of Transgrow and<br />
<strong>Gonozyme</strong> for the detection of Neisseria gonorrhoeae in mailed specimens. J<br />
Clin Microbiol 19:893-895, 1984.<br />
13. Manis RD, Harris B, Geiseler PJ: Evaluation of <strong>Gonozyme</strong>, an enzyme<br />
immunoassay for the rapid diagnosis of gonorrhea. J Clin Microbiol<br />
20:742-746, 1984.<br />
14. Mirrett S, Reller LB, Knapp JS: Neisseria gonorrhoeae strains inhibited by<br />
vancomycin in selective media and correlation with auxotype. J Clin<br />
Microbiol 14:94-99, 1981.<br />
15. Nachamkin I, Sondheimer SJ, Barbagallo S, Barth S: Detection of Neisseria<br />
gonorrhoeae in cervical swabs using the <strong>Gonozyme</strong> enzyme immunoassay.<br />
Am J Clin Pathol 82:461-465, 1984.<br />
16. Papasian CJ, Bartholomew WR, Amsterdam D: Validity of an enzyme<br />
immunoassay for detection of Neisseria gonorrhoeae antigens. J Clin<br />
Microbiol 19:347-350, 1984.<br />
17. Rudrik JT, Waller JM, Britt EM: Efficacy of an enzyme immunoassay with<br />
uncentrifuged first voided urine for detection of gonorrhea in males. J Clin<br />
Microbiol 20:577-578, 1984.<br />
18. Schachter J, McCormack WM, Smith RF, et al.: Enzyme immunoassay for<br />
diagnosis of gonorrhea. J Clin Microbiol 19:57-59, 1984.<br />
19. Sng EH, Rajan VS, Yeo K, Goh A: The recovery of Neisseria gonorrhoeae from<br />
clinical specimens: effects of different temperatures, transport times, and<br />
media. Sex Transm Dis 9:74-78, 1982.<br />
20. Stamm WE, Cole B, Fennell C, et al.: Antigen detection for the diagnosis of<br />
gonorrhea. J Clin Microbiol 19:399-403, 1984.<br />
21. Tramont EC, Sandoff JC, Artenstein MS: Cross-reactivity of Neisseria<br />
gonorrhoeae and the nature of the antigens involved in the bacteriocidal<br />
reaction. J Infect Dis 130:240-246, 1974.
Table I. Clinical evaluations of <strong>Gonozyme</strong>1" EIA compared with culture in the detection of N. gonorrhoeae from urethral and endocervical swab specimens.<br />
Author<br />
Aardoom et al.<br />
Abbott, Inc.<br />
Hums et al.<br />
Janielsson et al.<br />
Demetriou et al.<br />
ivlanis et al.<br />
Nachamkin et al.<br />
Papasian et al.<br />
Rudriok et al.<br />
Schachter et al.<br />
Stainm et al.<br />
Sex Sensitivity (%)<br />
F ( p r o s t i t u t e s ) 6 2 - 1 0 0<br />
F ( c o n t a c t s ) 6 0 - 9 8<br />
M ( u r e t h r i t i s ) 9 0 - 1 0 0<br />
F ( h i g h r i s k ) 8 7 . 2<br />
F ( l o w r i s k ) 1 0 0<br />
M ( h i g h r i s k ) 9 3 . 2<br />
F 8 8 . 5<br />
M 1 0 0<br />
F 9 0 . 9<br />
M 8 3<br />
M (corrected for FP cultures) 85.7<br />
F 8 7 . 5<br />
M 1 0 0<br />
F 9 6 . 4<br />
M 9 7 . 1<br />
F 8 7 . 2<br />
Al<br />
F 79.2<br />
M 97.3<br />
F 86.7<br />
:V1 100<br />
M (FVU) 91.6<br />
F (Boston - 1 culture) 70<br />
F (Boston - 2 cultures) 38.5<br />
F (Richmond - I culture) 86.8<br />
.vi (Boston + Richmond) 93.3<br />
F 78<br />
M (Total) 94<br />
M (w/ urethral discharge) 95<br />
M (w/o urethral discharge) 67<br />
-1|<br />
Specificity (%)<br />
91-99<br />
76-97<br />
81-100<br />
95.5<br />
97.4<br />
98.3<br />
94.3<br />
96.8<br />
100<br />
94.3<br />
96.6<br />
98<br />
100<br />
86.5<br />
96.9<br />
89.1<br />
87.2<br />
95.8<br />
93.7<br />
97.6<br />
97.9<br />
97.7<br />
94.1<br />
97.9<br />
100<br />
98<br />
98<br />
98<br />
98<br />
Positive<br />
Predictive<br />
Value (%)<br />
78.6<br />
76.5<br />
100<br />
82.5<br />
25<br />
96.8<br />
90.5<br />
97<br />
100<br />
66.7<br />
80<br />
85.7<br />
100<br />
62.2<br />
94.3<br />
37.2<br />
71.3<br />
96.5<br />
(76.5)<br />
(95.8)<br />
(91.7)<br />
94.4<br />
71.4<br />
97<br />
100<br />
85<br />
90<br />
97<br />
30<br />
Negative<br />
Predictive<br />
Value (%)<br />
98.9<br />
94.6<br />
100<br />
96.9<br />
100<br />
99.1<br />
93.6<br />
100<br />
99.3<br />
97.7<br />
97.7<br />
98.2<br />
100<br />
99.0<br />
98.4<br />
Disease<br />
Prevalence<br />
(% culture-positive)<br />
11.8<br />
27.7<br />
67.3<br />
16.96<br />
0.85<br />
34.8<br />
-<br />
7.3<br />
11.9<br />
Total<br />
No. of<br />
Patients<br />
102<br />
54<br />
52<br />
1,892<br />
236<br />
985<br />
368<br />
71<br />
150<br />
101<br />
14.3 782<br />
57<br />
18.8<br />
34.9<br />
591<br />
295<br />
98.9 6.9 1,588<br />
91.3<br />
96.8<br />
(93.7)<br />
(100)<br />
(98)<br />
86<br />
80<br />
90<br />
89.4<br />
96<br />
99<br />
97<br />
99<br />
28.6 252<br />
54.3 208<br />
(19.2) 78<br />
(35.9) 44<br />
(20) 120<br />
35.3 68<br />
27.6 47<br />
44.2 86<br />
64.1 117<br />
15 723<br />
16<br />
36<br />
2<br />
1,171<br />
-<br />
-
Table § Clinical evaluations of <strong>Gonozyme</strong> EIA compared with ^ture in the detection of N. gonorrhoeae from urethral |endocervical swab specimt |<br />
Author<br />
Aardoom et al.<br />
Abbott, Inc.<br />
Burns et al.<br />
Danielsson et al.<br />
Demetriou et al.<br />
Manis et al.<br />
Nachamkin et al.<br />
Papasian et al.<br />
Rudrick et al.<br />
Schachter et al.<br />
Stamm et al.<br />
F (prostitutes)<br />
F (contacts)<br />
M (urethritis)<br />
F (high risk)<br />
F (low risk)<br />
M (high risk)<br />
F<br />
M<br />
S e x S e n s i t i v i t y ( % ) S p e c i fi c i t y ( % )<br />
F MM (corrected for F P cultures)<br />
F M<br />
F<br />
M<br />
F M<br />
F<br />
M<br />
F<br />
M<br />
M (FVU)<br />
F (Boston - 1 culture)<br />
F (Boston - 2 cultures)<br />
F (Richmond - 1 culture)<br />
M (Boston + Richmond)<br />
F<br />
M (Total)<br />
M (w/ urethral discharge)<br />
M (w/o urethral discharge)<br />
62-100<br />
60-98<br />
90-100<br />
87.2<br />
100<br />
98.2<br />
88.5<br />
100<br />
90.9<br />
83<br />
85.7<br />
87.5<br />
100<br />
96.4<br />
97.1<br />
87.2<br />
79.2<br />
97.3<br />
86.7<br />
100<br />
91.6<br />
70<br />
38.5<br />
86.8<br />
93.3<br />
78<br />
94<br />
95<br />
67<br />
91-99<br />
76-97<br />
81-100<br />
95.5<br />
97.4<br />
98.3<br />
94.3<br />
96.8<br />
100<br />
94.3<br />
96.6<br />
98<br />
100<br />
86.5<br />
96.9<br />
89.1<br />
PPositive o s i t i v e N e g a t i v e '<br />
'<br />
"<br />
"<br />
D<br />
i s e<br />
Negative<br />
e<br />
a s<br />
s<br />
e<br />
Predictive Predictive ' (% culture-positive)<br />
Prevalence<br />
Value (%) Value (%) ;<br />
78.6<br />
76.5<br />
100<br />
82.5<br />
25<br />
96.8<br />
90.5<br />
97<br />
100<br />
66.7<br />
80<br />
85.7<br />
100<br />
62.2<br />
94.3<br />
37.2<br />
98.9<br />
94.6<br />
100<br />
96.9<br />
100<br />
99.1<br />
93.6<br />
100<br />
99.3<br />
97.7<br />
97.7<br />
98.2<br />
100<br />
99.0<br />
98.4<br />
11.8<br />
27.7<br />
67.3<br />
16.96<br />
0.85<br />
34.8<br />
-<br />
7.3<br />
11.9<br />
Total<br />
No. of<br />
Patients<br />
102<br />
54<br />
52<br />
1,892<br />
236<br />
985<br />
368<br />
71<br />
150<br />
101<br />
14.3 782<br />
57<br />
18.8<br />
34.9<br />
591<br />
295<br />
98.9 6.9 1,588<br />
87.2 71.3 91.3 28.6 252<br />
95.8 96.5 96.8 54.3 208<br />
93.7 (76.5) (93.7) (19.2) 78<br />
97.6 (95.8) (100) (35.9) 44<br />
97.9 (91.7) (98) (20) 120<br />
97.7 94.4 86 35.3 68<br />
94.1 71.4 80 27.6 47<br />
97.9 97 90 44.2 86<br />
100 100 89.4 64.1 117<br />
98 85 96 15 723<br />
98 90 99 16 1,171<br />
98 97 97 36 -<br />
98 30 99 2 -