Immunological Assay of CKMB
Immunological Assay of CKMB
Immunological Assay of CKMB

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
TEST<br />
<strong>Immunological</strong> <strong>Assay</strong> <strong>of</strong> <strong>CKMB</strong><br />
THEORETICAL CONSIDERATIONS<br />
TEST EVALUATION<br />
Sara Bodner, M.D.<br />
A combination <strong>of</strong> creatine kinase (CK) and lactate dehydrogenase isoenzymes<br />
provide the best laboratory indication <strong>of</strong> myocardial infarction, and the classic<br />
method <strong>of</strong> determining these isoenzymes is electrophoresis (1). Recently developed<br />
immunologic assays for these isoenzymes are quicker and less expensive than<br />
electrophoresis (2). One such assay is an immunochemical method for <strong>CKMB</strong><br />
determinations combining an immunoinhibition step with a immunoprecipitation step<br />
(3).<br />
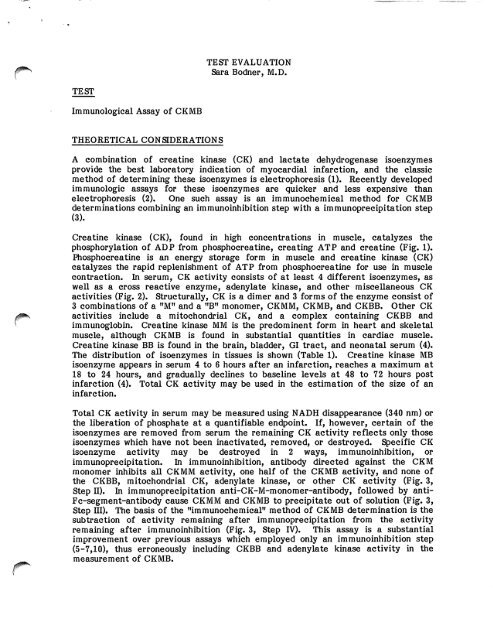
Creatine kinase (CK), found in high concentrations in muscle, catalyzes the<br />
phosphorylation <strong>of</strong> ADP from phosphocreatine, creating ATP and creatine (Fig. 1).<br />
Phosphocreatine is an energy storage form in muscle and creatine kinase (CK)<br />
catalyzes the rapid replenishment <strong>of</strong> ATP from phosphocreatine for use in muscle<br />
contraction. In serum, CK activity consists <strong>of</strong> at least 4 different isoenzymes, as<br />
well as a cross reactive enzyme, adenylate kinase, and other miscellaneous CK<br />
activities (Fig. 2). Structurally, CK is a dimer and 3 forms <strong>of</strong> the enzyme consist <strong>of</strong><br />
3 combinations <strong>of</strong> a "M" and a "B" monomer, CKMM, <strong>CKMB</strong>, and CKBB. Other CK<br />
activities include a mitochondrial CK, and a complex containing CKBB and<br />
immunoglobin. Creatine kinase MM is the predominent form in heart and skeletal<br />
muscle, although <strong>CKMB</strong> is found in substantial quantities in cardiac muscle.<br />
Creatine kinase BB is found in the brain, bladder, GI tract, and neonatal serum (4).<br />
The distribution <strong>of</strong> isoenzymes in tissues is shown (Table 1). Creatine kinase MB<br />
isoenzyme appears in serum 4 to 6 hours after an infarction, reaches a maximum at<br />
18 to 24 hours, and gradually declines to baseline levels at 48 to 72 hours post<br />
infarction (4). Total CK activity may be used in the estimation <strong>of</strong> the size <strong>of</strong> an<br />
infarction.<br />
Total CK activity in serum may be measured using NADH disappearance (340 nm) or<br />
the liberation <strong>of</strong> phosphate at a quantifiable endpoint. If, however, certain <strong>of</strong> the<br />
isoenzymes are removed from serum the remaining CK activity reflects only those<br />
isoenzymes which have not been inactivated, removed, or destroyed. Specific CK<br />
isoenzyme activity may be destroyed in 2 ways, immunoinhibition, or<br />
immunoprecipitation. In immunoinhibition, antibody directed against the CKM<br />
monomer inhibits all CKMM activity, one half <strong>of</strong> the <strong>CKMB</strong> activity, and none <strong>of</strong><br />
the CKBB, mitochondrial CK, adenylate kinase, or other CK activity (Fig. 3,<br />
Step II). In immunoprecipitation anti-CK-M-monomer-antibody, followed by anti-<br />
Fc-segment-antibody cause CKMM and <strong>CKMB</strong> to precipitate out <strong>of</strong> solution (Fig. 3,<br />
Step HI). The basis <strong>of</strong> the "immunochemical" method <strong>of</strong> <strong>CKMB</strong> determination is the<br />
subtraction <strong>of</strong> activity remaining after immunoprecipitation from the activity<br />
remaining after immunoinhibition (Fig. 3, Step IV). This assay is a substantial<br />
improvement over previous assays which employed only an immunoinhibition step<br />
(5-7,10), thus erroneously including CKBB and adenylate kinase activity in the<br />
measurement <strong>of</strong> <strong>CKMB</strong>.
00&*^<br />
JfjP^v<br />
CLINICAL APPLICATIONS<br />
Page 2<br />
Creatine kinase (CK) isoenzyme determinations have a major impact upon the<br />
diagnosis <strong>of</strong> myocardial infarction, and several studies have been done to determine<br />
whether immunochemical methods are as sensitive, specific, and efficient as<br />
electrophoresis in making this diagnosis (Table 2) (5-7). The standard against which<br />
these tests were compared were multiparameter laboratory determinations<br />
combined with clinical information, and assessed by a panel <strong>of</strong> experts. While these<br />
studies were imperfect (e.g., lacking a "gold" standard <strong>of</strong> diagnosis, and occasionally<br />
using electrophoretic CK and LDH determinations to establish the diagnosis) they<br />
indicate that the newer immunochemical method is as useful clinically in the<br />
diagnosis <strong>of</strong> myocardial infarction as electrophoresis. One study also demonstrates<br />
a 94.4% agreement between <strong>CKMB</strong> immunochemical and electrophoretic<br />
determinations. Because the CK immunochemical assay performs as well as the<br />
more expensive, more time-consuming electrophoretic method, it is gaining<br />
increased acceptance among pathologists and clinicians (2,8).<br />
Alternative methods for measuring CK isoenzymes include column chromatography,<br />
and radioimmunoassay. Column chromatography is even more time-consuming than<br />
electrophoresis and does not always adequately resolve CKMM, <strong>CKMB</strong>, and CKBB.<br />
The radioimmunoassay is very sensitive, but expensive, and exposes personnel to the<br />
hazards <strong>of</strong> radiation (12).<br />
TECHNICAL CONSIDERATIONS<br />
Most methods presently in use for total CK determinations may be adapted for use<br />
in <strong>CKMB</strong> immunochemical determinations. Serum pretreated with antibody and<br />
centrifugation as outlined in the immunochemical assay (Fig. 3) may be run in the<br />
same way as a total CK, and with a simple arithmetic computation the <strong>CKMB</strong> result<br />
can be calculated (R <strong>CKMB</strong> =2X (tube 2 - tube 1) (Fig. 3). Since 2 measured CK<br />
activities are being subtracted, a sensitive spectrophotometer must be used for<br />
h!fh.est accuraey- The small quantities resulting after subtraction may also create<br />
difficulties in precision and accuracy in the lower range <strong>of</strong> normal. Finally, some<br />
reagents used in total CK determinations are not compatible with substrates and<br />
reagents presently being used in the immunochemical assay. For example: the only<br />
immunochemical <strong>CKMB</strong> assay now on the market is produced by Roche. It is<br />
compatible with their (Roche) reagents for total CK determinations. Beckman's<br />
assay for total CK using the enzyme module on the Astra is also compatible with the<br />
(Roche) immunochemical assay for <strong>CKMB</strong>. On the other hand, KDA's reagents for<br />
total CK determinations result in imprecise results when combined with the (Roche)<br />
immunochemical assay for <strong>CKMB</strong> (13). To ensure highest precision and accuracy,<br />
the appropriate methods for CK determinations and sensitive spectrophotometers<br />
must be used.<br />
CONCLUSION<br />
For many years the gold standard in the diagnosis <strong>of</strong> acute myocardial infarction has<br />
been the combination <strong>of</strong> CK and LDH isoenzyme electrophoresis. Recently<br />
f developed immunochemical methods have demonstrated sensitivity, specificity,
*PpSs>\<br />
yfP**^<br />
Page 3<br />
efficiency, and predictive values comparable to those <strong>of</strong> electrophoresis in clinical<br />
trials. These immunochemical methods are also less time-consuming and less<br />
expensive than electrophoretic methods. Because <strong>of</strong> the economic pressures on<br />
medical care it appears likely that immunochemical methods will at least undergo<br />
further scrutiny, and possibly in part supplant electrophoretic methods in the<br />
diagnosis <strong>of</strong> acute myocardial infarction.<br />
REFERENCES<br />
1. Galen RS, Ruffel JA, Gambino R. Diagnosis <strong>of</strong> acute myocardial infarction<br />
relative efficiency <strong>of</strong> serum enzyme and isoenzyme measurements. JAMA<br />
232(2), 1975.<br />
2. Wu AHB, Bowers GN. Evaluation and comparison <strong>of</strong> immunoinhibition and<br />
immunoprecipitation methods for differentiating MB from BB and macro forms<br />
<strong>of</strong> creatine kinase CK isoenzymes in patients and healthy individuals. Clin<br />
Chem 28:2017-2021, 1982.<br />
3. Wicks R, Usatequi-Gomez M, Miller M, Warshaw M. Immunochemical<br />
determination <strong>of</strong> CK-MB isoenzyme in serum. II. An enzymatic approach.<br />
Clin Chem 28(l):54-58, 1982.<br />
4. Pesa MA. The CK isoenzymes: findings and meanings. Laboratory<br />
Management, October, 1982.<br />
5. Ali M, Laraia S, Angeli R, Fayemi O, Braun EV, Davis E, Palladino PH.<br />
Immunochemical CK-MB assay for myocardial infarction. Am J Clin Pathol<br />
77(5):573-579, 1982.<br />
6. Seckinger DL, Vezquez A, Rosenthal PK, Mendizabal RC. Cardio isoenzyme<br />
methodology and the diagnosis <strong>of</strong> acute myocardial infarction. Am J Clin<br />
Pathol 80(2):164-169, 1983.<br />
7. Bruno DL, Chitwood J, Koller K, Hill KE, Mostrom J, Savoy J. Creatine<br />
kinase-MB activity: Clinical and laboratory studies <strong>of</strong> immunochemical<br />
technique with optimized enzymatic assay. Ann Clin Lab Sci 13(l):59-65.<br />
1983.<br />
8. Statland BE. CK isoenzymes. MLO, June 1982, pp 14-15.<br />
9. Galen RS. Tips on technology. MLO, September 1981, pp 13-14.<br />
10. Obzansky D, Lott JA. Clinical evaluation <strong>of</strong> an immunoinhibitor procedure for<br />
creatine kinase-MB. Clin Chem 26(1):150-152, 1980.<br />
11. Sobel BE, Brenahan GF, Shell WI, et al. Estimation <strong>of</strong> infarct size in man and<br />
its relation to prognosis. Circulation 46:640-648, 1972.<br />
12. Lott JA, Stung JM. Clin Chem 26:124-150, 1980.<br />
13. Personal communication. Technical representative. H<strong>of</strong>fman Roche, Inc.<br />
Nutley, New Jersey.
Table I. Distribution <strong>of</strong> CK and CK isoenzymes in Various Tissues<br />
Tissue Range <strong>of</strong><br />
Total CK<br />
(U/gm tissue)<br />
Range <strong>of</strong> CK Isoenzymes<br />
M M M B B B<br />
(%)<br />
Skeletal muscle 1080-3050 96-100 0-4 0<br />
Heart muscle 190-692 58-36 15-42 . 0-1<br />
Brain 73-200 0 0 100<br />
Bladder 162 2 6 92<br />
Placenta 250 19 1 80<br />
Gastrointestinal<br />
tract<br />
145 3-4 0-2 96<br />
Thyroid 32-34 4-79 0-6 15-96<br />
Uterus 9-38 2-20 2-20 60-96<br />
Kidney 10-18 10 0 90<br />
Lung 11-13 26-60 0-1 2-14<br />
Prostate 8-9 4-40 3-4 56-93<br />
Spleen 2-7 0-74 0 26-100<br />
Liver 3-4 0-90 0-6 4-100<br />
Pancreas 3 14 1 85
^ ) '")<br />
Table 2. Studies Comparing Electrophoretic and Immunochemical Methods<br />
in the Diagnosis <strong>of</strong> MI<br />
Ref/Method #Pts 3 Pts w/ MI Sensitivity Specificity PV(+) PV(-) Efficiency Precision<br />
(5)Ali 215 45<br />
Immunochemical Method 95.5 95.3 95.3<br />
Electrophoretic Method 93.3 94.7 94.4<br />
(6) Sukmger<br />
Immunochemical Method<br />
Electrophoretic Method<br />
(7) Bruns<br />
Immunochemical Method<br />
180 36<br />
99 27<br />
100<br />
88<br />
93 78<br />
79<br />
100 97 94 5 to 12%<br />
100<br />
94<br />
95<br />
89<br />
(u = 39)
1 "1 1<br />
Figure I.<br />
Creatinec,^<br />
P h o s p h o c r e a t i n e - | - A n p ^ ^ A T P + C r e a t i n e<br />
Kinase<br />
Figure II.<br />
CK^, • CKtilo , CK<br />
CK Total = olH/IM + UIVMB + olBB + CK(mitochondrial) + Adenylate Kinase<br />
+ O t h e r s
F Ijre III.<br />
ISOMUNE — CK PROCEDURE<br />
I. Add 200 |iI <strong>of</strong> patient's serum to each <strong>of</strong> two test tubes<br />
m<br />
qO AK<br />
OQ<br />
Tubel<br />
iQQl<br />
»O0<br />
Tubel<br />
AK<br />
qQ<br />
AK<br />
OB<br />
Tube 2 (Blank tube)<br />
Add 200 ul <strong>of</strong> solid phase<br />
anti-goat IgG, mix and<br />
incubate 5 min. at ambient<br />
temperature<br />
Tube 2 (Blank tube)<br />
Solid phase<br />
anti-goat IgG<br />
Anti-MM<br />
serum<br />
1.<br />
Add 250 ul <strong>of</strong> anti-MM serum,<br />
JL mix and incubate for 20 min.<br />
at ambient temperature<br />
/<br />
A<br />
anti-MM<br />
w.<br />
|Q0]<br />
Tubel<br />
AK<br />
1001 AK<br />
■ O g -<br />
QQ<br />
Tubel<br />
Add 50 ul <strong>of</strong> anti-MM serum,<br />
mix and incubate for 5 min.<br />
at ambient temperature<br />
AK<br />
Tube 2 (Blank tube)<br />
Centrifuge for 5 min. at 1000 x g<br />
Tube 2 (Blank tube)<br />
Subtract the enzyme activity in the supernate <strong>of</strong> the blank<br />
tube from that <strong>of</strong> tube 1
Figure II. Fibrinogen Degradation (22)<br />
Fibrinogen<br />
Plasmm<br />
Fibrinogen<br />
Degradation<br />
Products<br />
Thrombin<br />
Fibrin monomer<br />
and macromolecular complexes<br />
non-crosslinked Fibrin<br />
Monomer<br />
Plasmm<br />
non-crosslinked<br />
Fibrin Degradation<br />
Products<br />
Modified from Colman and Hirsch (page 155)<br />
xnia<br />
crosslmked Fibrin<br />
Plasmm<br />
crosslmked<br />
Fibrin Degradation<br />
Products