

A systematic review of the effectiveness of adalimumab
A systematic review of the effectiveness of adalimumab
A systematic review of the effectiveness of adalimumab

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
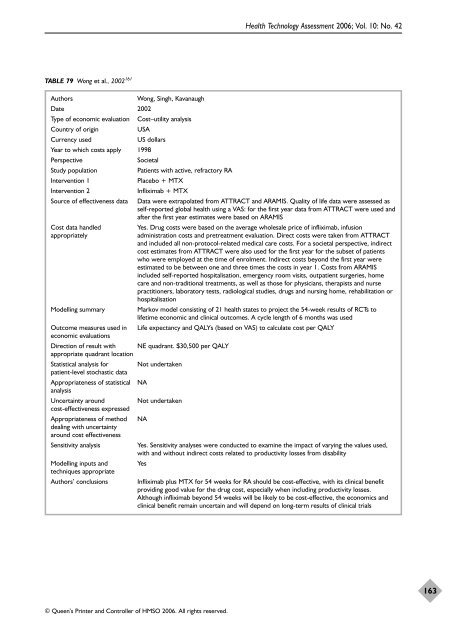
TABLE 79 Wong et al., 2002 161<br />
© Queen’s Printer and Controller <strong>of</strong> HMSO 2006. All rights reserved.<br />
Health Technology Assessment 2006; Vol. 10: No. 42<br />
Authors Wong, Singh, Kavanaugh<br />
Date 2002<br />
Type <strong>of</strong> economic evaluation Cost–utility analysis<br />
Country <strong>of</strong> origin USA<br />
Currency used US dollars<br />
Year to which costs apply 1998<br />
Perspective Societal<br />
Study population Patients with active, refractory RA<br />
Intervention 1 Placebo + MTX<br />
Intervention 2 Infliximab + MTX<br />
Source <strong>of</strong> <strong>effectiveness</strong> data Data were extrapolated from ATTRACT and ARAMIS. Quality <strong>of</strong> life data were assessed as<br />
self-reported global health using a VAS: for <strong>the</strong> first year data from ATTRACT were used and<br />
after <strong>the</strong> first year estimates were based on ARAMIS<br />
Cost data handled Yes. Drug costs were based on <strong>the</strong> average wholesale price <strong>of</strong> infliximab, infusion<br />
appropriately administration costs and pretreatment evaluation. Direct costs were taken from ATTRACT<br />
and included all non-protocol-related medical care costs. For a societal perspective, indirect<br />
cost estimates from ATTRACT were also used for <strong>the</strong> first year for <strong>the</strong> subset <strong>of</strong> patients<br />
who were employed at <strong>the</strong> time <strong>of</strong> enrolment. Indirect costs beyond <strong>the</strong> first year were<br />
estimated to be between one and three times <strong>the</strong> costs in year 1. Costs from ARAMIS<br />
included self-reported hospitalisation, emergency room visits, outpatient surgeries, home<br />
care and non-traditional treatments, as well as those for physicians, <strong>the</strong>rapists and nurse<br />
practitioners, laboratory tests, radiological studies, drugs and nursing home, rehabilitation or<br />
hospitalisation<br />
Modelling summary Markov model consisting <strong>of</strong> 21 health states to project <strong>the</strong> 54-week results <strong>of</strong> RCTs to<br />
lifetime economic and clinical outcomes. A cycle length <strong>of</strong> 6 months was used<br />
Outcome measures used in Life expectancy and QALYs (based on VAS) to calculate cost per QALY<br />
economic evaluations<br />
Direction <strong>of</strong> result with NE quadrant. $30,500 per QALY<br />
appropriate quadrant location<br />
Statistical analysis for Not undertaken<br />
patient-level stochastic data<br />
Appropriateness <strong>of</strong> statistical NA<br />
analysis<br />
Uncertainty around Not undertaken<br />
cost-<strong>effectiveness</strong> expressed<br />
Appropriateness <strong>of</strong> method NA<br />
dealing with uncertainty<br />
around cost <strong>effectiveness</strong><br />
Sensitivity analysis Yes. Sensitivity analyses were conducted to examine <strong>the</strong> impact <strong>of</strong> varying <strong>the</strong> values used,<br />
with and without indirect costs related to productivity losses from disability<br />
Modelling inputs and Yes<br />
techniques appropriate<br />
Authors’ conclusions Infliximab plus MTX for 54 weeks for RA should be cost-effective, with its clinical benefit<br />
providing good value for <strong>the</strong> drug cost, especially when including productivity losses.<br />
Although infliximab beyond 54 weeks will be likely to be cost-effective, <strong>the</strong> economics and<br />
clinical benefit remain uncertain and will depend on long-term results <strong>of</strong> clinical trials<br />
163













